Feeding & Eating — 40 Evidence-Based Interventions for Autism
Picky eating · Food texture aversions · Oral motor challenges · Mealtime meltdowns · Self-feeding independence. Built for families, therapists, and program leads — grounded in neuroscience, delivered with warmth.
Subdomain E1
Domain E: Daily Living
Pinnacle Blooms Network®
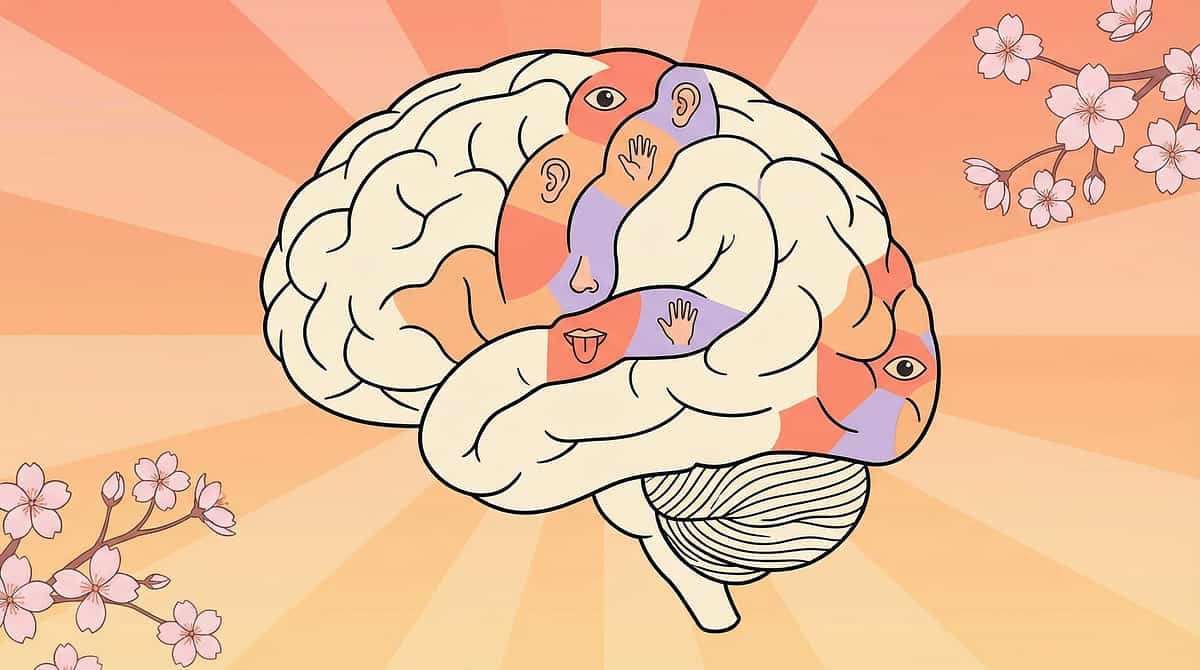
The Neuroscience Behind Food Selectivity
Food selectivity in ASD is not a choice — it is a neurological condition driven by sensory processing, oral motor function, anxiety, and rigid thinking patterns. Between 70–90% of children with ASD have significant feeding challenges. Understanding the brain systems involved is the first step to helping.
Oral Sensory (CN V)
Processes texture, temperature, pressure — may be hypersensitive (gagging), hyposensitive (stuffing), or narrowly discriminating.
Gustatory Cortex
Taste processing heightened — mild flavours become overwhelming. The insula amplifies every signal.
Amygdala
Food neophobia — new food = unknown = genuine FEAR response. Not stubbornness. A real threat signal.
Interoception
Hunger and fullness detection (insular cortex) may be impaired — children truly may not feel hunger cues.
Every food has FIVE sensory dimensions: texture, taste, temperature, smell, and appearance. ALL FIVE must fall within the child's narrow acceptable range. One dimension outside range → rejection.

⚠️ Critical Safety Principles
Before exploring any technique on this page, every caregiver and therapist must understand the non-negotiable foundations of safe feeding intervention.
🚫 Never Force-Feed
Forced feeding causes lasting feeding trauma and permanently worsens selectivity. There is no exception to this rule.
🚫 Never Punish Food Refusal
Punishment creates conditioned aversion — the table becomes a threat environment. It does not expand food repertoire.
⚠️ Under 20 Foods → Nutritional Assessment
Fewer than 20 foods in repertoire requires urgent dietitian evaluation for nutritional gaps and supplementation planning.
⚠️ Gagging + Weight Loss → Urgent SLP Referral
Gagging combined with failure to thrive or weight loss is a clinical emergency requiring immediate speech-language pathology evaluation.
Section 1
Cards 01–12
Food Selectivity & Sensory
The foundation of all feeding work — understanding and addressing the sensory roots of food selectivity, texture aversion, new food refusal, and oral motor challenges that shape what a child will and will not accept at the table.
1
E-451
Extreme Picky Eating
2
E-452
Limited Food Repertoire
3
E-453
New Food Refusal
4
E-454
Food Texture Aversions
5
E-455–456
Presentation & Plate Rigidity
6
E-457–467
Gagging, Chewing, Motor & Sitting

E-451 + E-452
Food Selectivity
Extreme Picky Eating · Limited Food Repertoire
The moment: Five foods. That's it — rice, bread, chips, biscuits, milk. Even those must be the right brand, right temperature, right plate. Mealtime feels like a battlefield.
The Neuroscience
Extreme picky eating in ASD is multi-system: oral sensory rejection (CN V hypersensitivity), amygdala food neophobia, basal ganglia sameness insistence, and impaired interoception. The brain is not being defiant — it is protecting the child from perceived sensory danger.
The Evidence
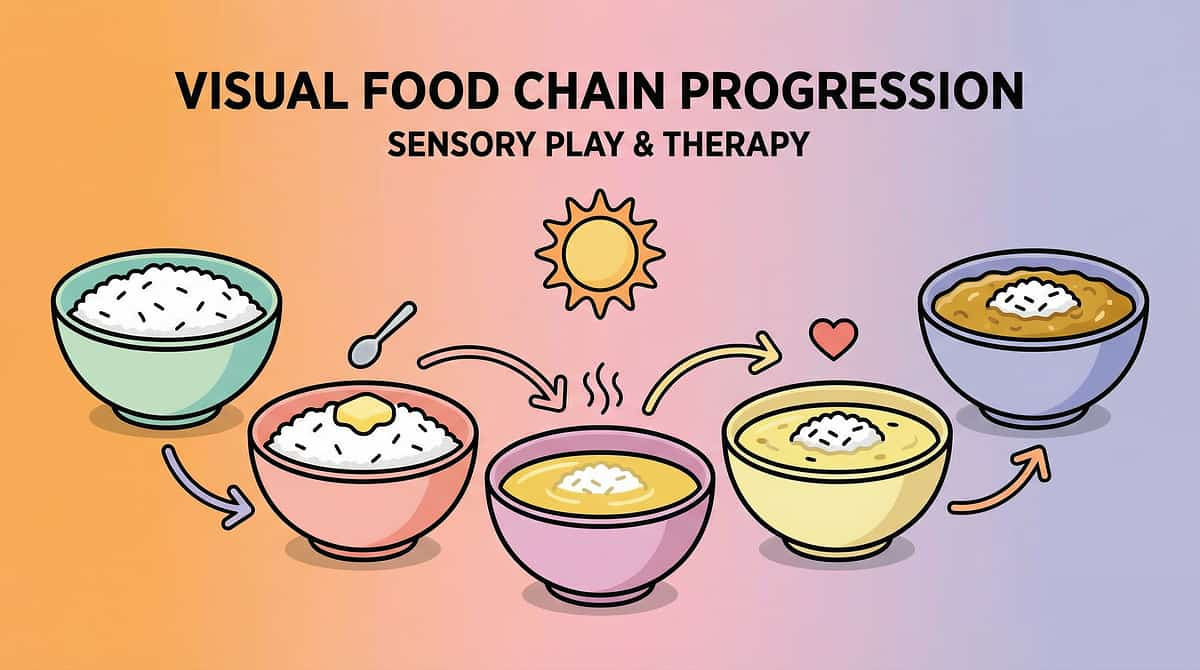
📊Level I — SOS Approach to Feeding and Food Chaining: gradual, non-force exposure to expand repertoire safely over time.
NCAEP 2020 | SOS (Toomey) | Food Chaining (Fraker) | PMC10955541
Lead Clinicians
🗣️ SLP (Feeding) · 🤲 OT (Oral Sensory) | 📋 ABA · NeuroDev · Dietitian
Build a Food Inventory
Document every accepted food with its sensory properties.
Apply the SOS 32-Step Hierarchy
Tolerate food in room → on plate → touch → smell → taste → eat.
Set Realistic Timelines
Expansion takes months, not days. Celebrate every step.
The moment: Only white foods. Only crunchy. Only room-temperature. Only one brand. A repertoire so narrow that nutritional gaps are inevitable — and a supply chain disruption becomes a family crisis.
The Neuroscience
Sensory narrow-banding combined with sameness insistence and amygdala neophobia creates a rigid "safe food list." Everything outside it registers as danger — not preference.
Food Chaining Strategy
Start with an accepted food → make one TINY sensory change → if accepted, change slightly more. Chain from accepted to new through micro-steps the brain can tolerate.
Indian Safe Foods
Plain rice, roti, papad, plain dosa, idli, plain milk — common starting anchors for Indian families building food chains.
Level I Evidence
Food Chaining (Fraker et al.) is the primary evidence-based method for expanding limited repertoires gradually and safely.

E-453 + E-454
New Food Refusal & Texture Aversions
New Food Refusal · Food Texture Aversions
The moment: Won't look. Won't touch. Won't smell. May cry, gag, or leave the table at the mere sight of unfamiliar food. You stopped trying months ago — but the window for expansion is still open.
Why It Happens
Amygdala food neophobia drives new food refusal. Neurotypical children need 10–15 exposures to accept a new food. Children with ASD often require 50–200+ exposures — and every exposure MUST be non-threatening, or it reinforces the fear rather than reducing it.
The SOS Hierarchy
Room → table → plate → utensil touch → finger touch → smell → lip → lick → tiny taste → bite → eat. One new food at a time. A "learning plate" removes eating demands entirely — explore, don't require.
Indian festival foods — Diwali sweets, Holi colours, Pongal rice — are natural, low-pressure exposure opportunities. Celebration context reduces anticipatory anxiety.
The moment: Smooth — yes. Lumpy — NEVER. Crunchy — yes. Slimy — gagging. Mixed textures — panic. Texture is the number one reason children with ASD reject food — not taste.
Texture Hierarchy
Smooth/Pureed: Yoghurt, blended dal, smooth purees — the entry point for oral tolerance work.
Soft Solid: Soft idli, banana, ripe mango — predictable texture, manageable challenge.
Firm Solid: Toasted bread, paneer cubes, cooked carrot — builds lateral jaw movement.
Crunchy: Papad, rice cakes, apple slices — provides proprioceptive feedback that many children seek.
Oral desensitisation — gum massage, textured spoon, vibrating toothbrush — is conducted outside meals, reducing the oral system's reactivity before the child comes to the table. Level I — NCAEP 2020 | SOS Approach.
E-455 + E-456
Food Presentation Rigidity
Foods Can't Touch · Specific Plate Requirements
E-455: Foods Can't Touch
If dal touches rice before the child decides — meltdown. If sabzi juice crosses into roti zone — plate pushed away. The brain's prediction system demands EXACT visual arrangement. Any violation = error = rejection.
The Indian thali is a natural divided plate. Steel katoris (₹100–300) provide affordable, culturally familiar compartmentalisation.
E-456: Specific Plate Requirements
Only the blue plate. Only THAT steel bowl. Only the Mickey Mouse cup. Container matters as much as contents — brand packaging and vessel shape form part of the brain's multi-sensory food template.
Strategy: Keep backup plates for travel and school. Introduce "same family" vessels — same colour, slightly different shape — as gradual flexibility practice.
Gradual proximity reduction: 3 cm apart → 2 cm → 1 cm → touching
When rigidity protects nutrition — accommodate it first, flex it later
Decant new brand into old familiar container as bridge strategy

E-457
⚠️ Clinically Significant
9 Materials That Help With Gagging on Textures
⚠️ CLINICALLY SIGNIFICANT: Gagging — sometimes vomiting — at sight, smell, touch, or taste of certain textures is not drama. It is a hypersensitive protective reflex requiring clinical attention.
The Neuroscience
The gag reflex (CN IX + CN X) is anteriorised — it fires at the lips and tongue tip instead of the normal posterior location. The threshold is set too low. One reason: the brain over-predicts danger from oral input, triggering the reflex prematurely and at lower-intensity stimuli than typical.
Clinical Response
Gagging is protective, not voluntary. Never push through gagging. Gag desensitisation is SLP-guided only — systematic posterior progression over weeks to months, matched to the child's gag tolerance level.
⚠️ Gagging + weight loss/failure to thrive → URGENT SLP feeding evaluation.
Managing the environment: respond to vomiting calmly, clean without big reaction, and avoid creating secondary anxiety around gagging episodes. The calm response is itself therapeutic. 📊Level I — NCAEP 2020 | SOS Approach.

E-458 + E-459
Chewing & Pocketing
Chewing Difficulty · Pocketing Food
E-458: Chewing Difficulty
Food comes out partially chewed or swallowed in chunks. The jaw cannot execute the rotary chewing pattern. Chewing requires coordinated bilateral jaw movement (CN V motor), tongue lateralisation (CN XII), and cheek tension (CN VII) — each a separate motor computation that must be learned.
Intervention: Chewy tubes with graded resistance, crunchy foods for lateral jaw practice (papad, carrot sticks, apple), lateral chewing exercises guided by SLP.
E-459: Pocketing Food
Food goes in but stays in cheeks — "pocketed" without swallowing. Found 30 minutes after the meal. This is a choking and aspiration risk requiring immediate attention.
Intervention: Vibrating toothbrush on cheeks, cheek massage before meals, "check your cheeks" verbal cue every 3–4 bites. Oral hyposensitivity means the brain literally does not detect food in the cheeks.
⚠️ Swallowing unchewed food = CHOKING RISK. SLP involvement is mandatory for both chewing difficulty and consistent food pocketing. 📊 Level I — NCAEP 2020.
E-460 + E-461
Overstuffing & Utensils
Mouth Overstuffing · Utensil Use
E-460: Mouth Overstuffing
Entire portion shoved in at once. Cheeks bulging. Choking risk at every meal. This is oral proprioceptive hyposensitivity — the mouth cannot detect "full." Combine that with impulse control deficits and possible food anxiety (eat fast before it's removed) and overstuffing becomes a predictable, multi-cause behaviour.
Key:⚠️ All caregivers should be trained in the Heimlich manoeuvre.
E-461: Utensil Use
Utensil use requires fine motor precision, hand-eye coordination, oral motor coordination, and proprioceptive calibration — each an independent computation. Progression: fingers → loaded spoon → self-scooping → fork stabbing.
Adaptive utensils (weighted, angled — ₹300–800 on Amazon India) significantly lower the motor demand during early stages.
Small portions on plate (3–4 bites, refill) to reduce overstuffing volume
Model and cue: bite → pause → chew → swallow before next bite
Practice utensils with preferred foods first — motivation drives motor learning

E-462 + E-463
Messy Eating & Cup Drinking
Messy Eating · Cup Drinking
E-462: Messy Eating
Food everywhere — face, hands, clothes, floor. Proprioceptive awareness deficit means the child cannot feel food on their face, and tactile hyposensitivity means they are not bothered by it. Without the signal, there is no self-correction. A mirror at the table, face awareness exercises, and vibrating toothbrush on cheeks and lips before meals all build the sensory feedback loop needed for cleaner eating.
E-463: Cup Drinking
Spilling from cups. Unable to coordinate sip-swallow. Still on a sippy cup at age 6+. Cup drinking requires lip seal (CN VII), jaw grading, sip volume control, sip-swallow coordination, and arm stability — each independent.
Progression: Closed spout → straw → open cup with thick liquid → open cup thin liquid. Nosey cups (cut-out design) allow the child to see the liquid level without tipping.
The Indian steel tumbler is a culturally meaningful milestone — building cup drinking skills connects the child to family mealtime traditions. 📊Level I — NCAEP 2020.
E-464 + E-465
Bottle Weaning & Self-Feeding
Weaning from Bottle · Self-Feeding
E-464: Weaning from Bottle
Still on bottle at 4, 5, 6+ years. Beyond nutrition, the bottle provides oral sensory comfort through rhythmic sucking — a genuine parasympathetic calming mechanism. Removal means oral sensory distress and comfort loss, not defiance. Eliminate one feed per week (least preferred first), replace with a chew toy or straw cup, and remove the bedtime bottle last.
E-465: Self-Feeding
Still parent-fed at an age when peers eat independently. Self-feeding requires motor planning, hand-eye coordination, sensory tolerance of touching food, and motivation. If parent-feeding is faster and cleaner — why self-feed?
Celebrate messy self-feeding over clean parent-feeding. Progress: hand-over-hand → hand-under-hand → guided → independent.
Indian context: grandparent resistance ("Let me feed the child") reflects deep cultural love — but lovingly explain that independence at the table builds independence for life. Grandparents are powerful allies when they understand the why.

E-466 + E-467 + E-469
Eating Speed, Sitting & Food Throwing
Eating Speed · Sitting for Meals · Food Throwing
E-466: Eating Speed
Meals take 90 minutes (too slow) — or 3 minutes (too fast, choking). Slow eating signals oral motor processing difficulty or sensory avoidance. Fast eating signals oral hyposensitivity or food anxiety. Slow: 30-minute max rule. Fast: Visual timer pacing, one-item plating, utensil-down cue between bites.
E-467: Sitting for Meals
Eats on the run — standing, walking, in front of the TV. Never at the table, or sits for 30 seconds and bolts. The table is the highest-demand mealtime environment: sitting + food sensory + oral motor + social all at once.
Key strategies:
- Proper Seating Setup: Feet flat (footrest essential), hips at 90°, table at elbow height. Good posture dramatically reduces the postural demand that competes with eating.
- Start Small, Build: Begin with 2 minutes of sitting as the goal — not a full meal. First-then board: "First sit 3 minutes, then play." Build duration by 30 seconds every few days.
- Reduce Table Load: Fewer dishes, quieter environment, dimmer light. Remove TV. Indian floor-sitting (on a mat or low table) may be MORE stable for some children — use it.
- Level I — Structured mealtime + environmental support. NCAEP 2020.
E-469: Food Throwing
Plate launched. Rice on walls. Dal on floor. Roti frisbeed. Food throwing serves a function — escape (meal ends), sensory (visual + auditory feedback of crash), attention (intense parental reaction), or communication ("done" / "don't want").
Key response: Identify the function. Offer an "all done" card as replacement. Serve small portions. Use a suction plate (₹300–600). Calm, minimal reaction — big reactions reinforce the behaviour.
Section 2
Cards 13–20
Mealtime Behaviour & Strategies
Mealtime behaviour is inseparable from the sensory and emotional experience of eating. These cards address the behavioural layer — meltdowns, school refusal, brand rigidity, and the overarching frameworks for making every meal calmer, safer, and more expansive.
E-468
Mealtime Meltdowns
E-471
School Eating Refusal
E-470 + E-476
Location & Colour Rigidity
E-472
Food Chaining
E-473 + E-474
Sensory Introduction & Positive Mealtimes
E-475 + E-477
Brand Rigidity & Temperature Preferences

E-468
Mealtime Meltdowns
9 Materials That Help With Mealtime Meltdowns
The moment: Food hits the table and screaming starts. The meltdown is ABOUT food — but not about hunger or taste. It is anticipatory anxiety, sensory overwhelm, demand to eat, unpredictability. Mealtime has become a trauma trigger.
The Neuroscience
Conditioned food/table aversion — the amygdala associates the table with distress. Elevated cortisol suppresses appetite. Escape behaviour ends the meal and is reinforced. The cycle deepens with every difficult mealtime.
Positive mealtimes reverse the conditioning. Table = pleasant → amygdala relaxes → appetite returns → exploration increases.
Division of Responsibility (Satter)
The single most powerful mealtime framework: Parent decides WHAT is served, WHEN meals happen, and WHERE eating occurs. Child decides WHETHER to eat and HOW MUCH.
This division eliminates food battles entirely — because the parent is no longer in the child's lane. Always serve at least one safe food alongside new foods. The child always has something they can eat.
E-470 + E-471 + E-476
Location, School & Colour Rigidity
School Eating Refusal · Location-Specific Eating · Food Colour Requirements
E-471: School Eating Refusal
The moment: Tiffin comes home untouched. Every single day. Six to eight hours without food. Then home starving, melting down. School eating refusal wrecks behaviour, attention, and learning for the entire school day.
Why School Is Different: Cafeteria sensory environment (noise, smells, crowding), social anxiety around eating before peers, location-specific eating (E-470), temperature change (tiffin no longer warm), and peak demand overload combine to make school eating uniquely difficult.
Accommodation Strategies: Quiet eating space or smaller group, extended lunch time, a familiar eating companion. These are reasonable RPwD 2016 accommodations — families can formally request them.
Tiffin Optimisation: Room-temperature-acceptable safe foods, insulated container for preferred warm foods, familiar vessel (same box used at home). Gradual school eating: 1 bite → 2 → half → full over weeks.
E-470: Location-Specific Eating
Eats at home — refuses at school. Eats at grandma's — refuses at restaurants. Eating is LOCATION-DEPENDENT. The basal ganglia encodes eating as context-specific: home + thali + TV + chair = eating. Change any variable and the system breaks.
Strategy: Portable mealtime kit (plate, utensil, placemat travel with child). Gradual expansion: living room → table → balcony → park → restaurant.
E-476: Food Colour Requirements
Only white foods. Only beige. Anything green → refused. The visual cortex tags certain colours as "unsafe" — an evolutionary signal (bright colours = potential poison). The amygdala rejects based on colour ALONE, before taste or texture are ever processed.
Strategy: Exposure OUTSIDE food first (green play dough, green paint). Colour chaining: white rice → rice with tiny green coriander → gradually more green. Hidden vegetables blended into accepted foods.
E-472
The Master Expansion Strategy
9 Materials That Help With Food Chaining
The moment: This is THE master food expansion strategy — the clinical tool that makes everything else possible. Start with an accepted food → change ONE sensory property by a TINY amount → if accepted, change slightly more → chain from accepted to completely new food through micro-steps.
Each micro-step falls WITHIN the brain's tolerance window — the change is small enough that the amygdala does not trigger neophobia. Step by step, the tolerance window expands. Indian food chains: plain rice → rice + ghee → rice + dal water → rice + thin dal → rice + thick dal. Cost: ₹0 — requires only patience and precision. 📊Level I — Food Chaining (Fraker et al.)

E-473 + E-474
Sensory Introduction & Positive Mealtimes
Sensory Food Introduction · Making Mealtimes Positive
E-473 — Sensory Food Introduction
The moment: Food as PLAY — not eating demand. Before a child can eat a food, they must tolerate it through all sensory channels. Playing with food is not "bad manners" — it is therapy.

Visual + Tactile Exploration
Painting with yoghurt, stamping with cut fruit — builds visual tolerance before oral tolerance is even attempted.

Building & Sorting
Building with vegetables, sorting foods by colour — olfactory and visual exposure in zero-pressure context.

Indian Sensory Play
Rangoli with lentils, dosa batter mixing, chapati rolling, rice sorting — culturally rooted food exploration.
A "learning plate" at every meal — a small plate with the new food, no requirement to eat — normalises the food's presence without demand. Messy food play happens outside mealtimes to prevent contamination of the eating context. 📊Level I — SOS Approach (Toomey).
E-474 — Making Mealtimes Positive
The moment: Mealtime is the worst part of the day — pressure, crying, gagging, throwing, begging, bribing, threatening. This card resets the mealtime relationship. Goal: mealtimes the child wants to attend, even if they eat only three bites.
The Satter Division of Responsibility: Parent provides WHAT is served, WHEN meals happen, and WHERE eating occurs. Child decides WHETHER to eat and HOW MUCH. This single framework eliminates ALL food battles — because the parent is no longer fighting in the child's domain.
Building Positive Association: Fun at the table outside meals — conversation, simple games, music. Remove ALL pressure. Celebrate attendance over consumption. The 20-minute maximum meal rule prevents the table from becoming an endurance event. When cortisol drops and the table feels safe, appetite and exploration naturally follow.

E-475 + E-477 + E-483
Brand, Temperature & Sauce Rigidity
Food Brand Rigidity · Temperature Preferences · Sauce and Dip Aversion
E-475: Food Brand Rigidity
The moment: Only Parle-G. Only Amul milk. Only Maggi noodles. Only THAT brand of bread. Brand discontinued? Crisis. Travelling? Potential starvation. Brand rigidity is one of the most practically disruptive feeding challenges families face.
Why It Happens: Brand packaging + flavour + texture create a multi-sensory template in the basal ganglia. The brain identifies food as a UNIT — package + taste + texture together. Change the package and the brain suspects the food itself has changed.
Transition Strategy: Decant new brand into old familiar container first. If accepted with old container, gradually introduce the new packaging alongside. Side-by-side presentation builds comparison tolerance.
Supply Chain Preparedness: Build flexibility BEFORE the crisis — don't wait for a brand to be discontinued. Indian dependencies: Parle-G, Amul, Britannia, Maggi — each has a specific transition pathway.
E-477: Temperature Preferences
The moment: Only cold. Only room temperature. Only piping hot. Any deviation → refusal. Thermoreceptors (CN V) may be hypersensitive — warm feels "burning." OR temperature serves a sensory regulation function (cold numbs oral hypersensitivity). Indian hot food culture combined with school tiffin at room temperature creates daily conflict.
Strategy: Gradual range expansion (cold → cool → room → slightly warm). Insulated tiffin containers for preferred warm temperature.
E-483: Sauce and Dip Aversion
The moment: No ketchup. No chutney. No curd on rice. Wet condiments CONTAMINATE the safe base food — because they change multiple sensory properties simultaneously (texture, temperature, appearance, taste). Each application creates a sensorially DIFFERENT food, triggering neophobia.
Strategy: Always serve sauce on the side. Dipping progression: touch → finger taste → tiny dot on food → small amount. Chutney varieties as graded exposure. Raita as a texture bridge.
Section 3
Cards 21–24
Food Group Aversions
When entire food groups are rejected, nutritional risk escalates rapidly. These cards address the most clinically significant aversions — liquids, vegetables, proteins, and fruits — with evidence-based, India-contextualised strategies for each.
E-478: Liquid Refusal
Dehydration risk in Indian summers. Strategies for flavoured water, vessel choice, and high-water foods.
E-479: Vegetable Aversion
The most nutritionally impactful aversion. Hidden strategies, food chaining, Indian vegetable hierarchy.
E-480: Protein Aversion
The most dangerous nutritional deficit. Texture-driven strategies and Indian protein ranking by acceptance.
E-481 + E-486: Fruit Introduction & Bite Size
Building from banana → mango → variety. Bite size calibration as an oral proprioceptive skill.

E-478
Liquid Refusal
9 Materials That Help With Liquid Refusal
The moment: Won't drink water. Won't drink juice. Only milk from a bottle. Dehydration risk is real — especially in Indian summers at 40°C+. Constipation (extremely common in ASD) and UTI risk compound the concern.
Flavour the Water
Lemon, cucumber, or fruit infusion — subtle flavour can bridge the gap between plain water and something the child will accept. Avoid artificial flavourings.
Experiment with Temperature
Some children accept only ice-cold water (sensory numbing), others only room temperature. Temperature preference is a legitimate variable — use it.
Change the Vessel
Straw bottle, sports bottle, open cup — vessel shape changes the sensory experience of drinking significantly.
High-Water Foods
Watermelon, cucumber, curd, coconut water, buttermilk — Indian summer foods that provide significant hydration.
⚠️ Dehydration signs in Indian summer: dark urine, lethargy, dry lips, sunken eyes → seek medical attention. Do not manage dehydration with feeding strategies alone.
E-479 + E-480
⚠️ Urgent Nutritional Risk
Vegetable Aversion · Protein Aversion
The moment: Zero vegetables. None. The most nutritionally impactful food aversion. Indian cuisine offers enormous variety — but variety means nothing if all vegetables are rejected.
Why Vegetables Are So Hard
Vegetables combine multiple challenging sensory dimensions simultaneously: fibrous textures, bitter flavour compounds (the TAS2R38 receptor may be more sensitive in ASD), strong smells, and alarming colours (green is particularly rejected). They fail on multiple sensory dimensions at once — which is why they are among the most universally refused foods.
Indian Strategies
Hidden: Lauki in roti dough, spinach in dal, carrot in paratha, beetroot in dosa batter — nutrients without confrontation.
Chaining: Potato → sweet potato → carrot → peas → beans.
Blended Indian dishes: Palak paneer blended smooth, mixed veg soup blended, vegetable paratha with finely grated vegetables.
Supplement micronutrients while building acceptance — don't wait for vegetables to close the nutritional gap.
The moment: Won't eat chicken, fish, eggs, paneer, dal, or beans. Protein aversion is the most dangerous nutritional deficit — impacting growth, muscle development, immune function, and brain development. In vegetarian Indian families where dal AND paneer are both refused, the risk becomes critically narrow.
Protein Texture Hierarchy
Smooth
Blended dal, egg custard, milk-based protein — entry point for maximum oral tolerance.
Soft
Scrambled egg, mashed dal, soft-cooked dal — minimal chewing demand.
Firm
Paneer cubes, chicken tikka, thick dal — requires lateral chewing.
Fibrous
Tandoori, grilled chicken, whole legumes — full oral motor engagement.
Indian protein acceptance ranking: milk > curd > dal water > thin dal > thick dal > paneer > egg > chicken. Start from the top of this hierarchy. Level I — NCAEP 2020.
⚠️ Zero protein in repertoire → URGENT dietitian referral. Do not address with feeding strategies alone — supplementation must begin immediately.

E-481 + E-486
Fruit Introduction & Bite Size
Fruit Introduction · Bite Size Teaching
E-481: Fruit Introduction
Won't eat fruit — or only one (usually banana). Missing vitamins, fibre, and natural sugars. Fruits should be the easiest group (sweet, soft) — but texture variability, seeds, skin, and juice-on-hands make them sensorially complex. Variable textures within a single fruit overwhelm the sensory prediction system.
Indian fruit chain: Banana → chikoo → mango → papaya → watermelon. Preparation matters: peeled, deseeded, uniform pieces. Smoothies as a bridge. Mango season = natural introduction window.
E-486: Bite Size Teaching
Bites too big (choking risk) or too small (meals take forever). Bite size calibration requires jaw proprioception, oral spatial awareness, visual estimation, and motor planning — each independent. When any one fails, bite size becomes random.
Intervention: Pre-cut food to target size. "Big bite / little bite" teaching with visual demonstration. Model → bite → match. Chewy tube for jaw grading calibration between meals.

Section 4
Cards 25–30
Advanced Strategies & Independence
The final section brings together the master frameworks — mixed food tolerance, systematic desensitisation, oral sensory programming, swallowing safety, utensil mastery, and the capstone of all feeding work: independent meals across all environments.
E-482
Mixed Food Aversion — from single-ingredient to complex Indian dishes
E-484
Building Food Tolerance — the master 11-step hierarchy
E-485
Oral Sensory Needs — the oral diet that underpins all feeding progress
E-487
Swallowing Difficulty — medical priority, aspiration risk
E-488 + E-489
Spoon & Fork Mastery — fine motor to independent utensil use
E-490
Independent Meals — the capstone of Subdomain E1
E-482
Mixed Food Aversion
9 Materials That Help With Mixed Food Aversion
The moment: Single ingredient only. No biryani. No pulao. No khichdi. No sandwich. Indian cuisine celebrates complex mixed dishes — and almost all of them are impossible.
The Neuroscience
Mixed foods bring texture unpredictability (each bite is different), visual complexity (ingredients unidentifiable), and simultaneous multi-sensory overwhelm. The brain cannot PREDICT what the next bite will feel like → the amygdala labels the entire dish "unsafe."
The Mixing Progression
Single foods → two visible but touching → partially mixed → fully mixed → three-component dishes. Transparent mixing (child watches preparation) reduces unpredictability. Deconstructed versions of complex dishes — biryani components served separately — honour the flavours while reducing sensory challenge. Start with khichdi: the simplest Indian mix.

E-484
The Master Tolerance Framework
9 Materials That Help Building Food Tolerance
The master tolerance card. Before eating, a child must TOLERATE — in the room, on the table, on the plate, near the face, touching the lips. Building tolerance means systematically moving a food from "threat" to "neutral" in the amygdala's database.
Each non-threatening exposure WEAKENS the amygdala's threat response. Exposure → no bad outcome → recalibrate → "less dangerous" → next exposure → eventually neutral → then acceptable. This requires dozens of exposures and ZERO pressure. Multiple foods can be worked at different stages simultaneously. Allow 3–6 months per food for severely selective children. Sticker charts per food per step make progress visible. 📊Level I — NCAEP 2020 | SOS Approach.

E-485
Oral Sensory Needs
9 Materials That Help With Oral Sensory Needs
The moment: The oral sensory programme card — linking feeding to the broader sensory system. Oral seeking (chewing everything), oral avoidance (rejecting textures), and oral discrimination all affect feeding. An oral sensory diet outside mealtimes improves feeding DURING mealtimes.
Chew Tools
Chewy tubes and chewellery throughout the day provide consistent oral proprioceptive input that regulates the system.
Vibrating Toothbrush
3× daily on gums, cheeks, and tongue. Systematic desensitisation that reduces reactivity at mealtimes.
Blowing Activities
Whistles, bubbles, pinwheels — builds oral motor strength and breath control with zero food required.
Straw Drinking
Builds lip seal, tongue retraction, and graded sucking — foundational oral motor skills for safe cup drinking.
Match input to profile: oral seekers need intense input (harder chewy tools, crunchier snacks). Oral avoiders need gradual desensitisation starting with the lowest-intensity stimuli. SLP and OT collaborate on this programme. 📊Level I — NCAEP 2020.

E-487 + E-488 + E-489
⚠️ Medical Priority & Utensil Mastery
Swallowing Difficulty · Spoon Feeding Transition · Fork Use
⚠️ MEDICAL PRIORITY. Food goes in but doesn't go down. Holding food for minutes. Spitting instead of swallowing. Coughing or choking during swallowing. SLP evaluation is mandatory — this is not a home-management-first presentation.
E-487: Swallowing Difficulty
The Neuroscience: Swallowing involves 50+ muscles coordinated by CN V, VII, IX, X, and XII across four phases: oral prep → oral transport → pharyngeal → oesophageal. Dysfunction at ANY phase = dysphagia. Pharyngeal dysphagia carries ASPIRATION RISK — food entering the airway can cause aspiration pneumonia.
Aspiration Warning Signs:⚠️ Coughing or choking during swallowing. Wet or gurgly voice after eating. Recurrent chest infections or pneumonia. Food or liquid coming from the nose. Refusing previously accepted foods suddenly.
Any of these signs → URGENT SLP referral for swallowing evaluation (MBSS or FEES). Texture modification is determined by the SLP, not the caregiver.
E-488 + E-489: Spoon & Fork Mastery
E-488: Spoon Feeding Transition: From parent-spoon-feeding to self-scooping — each step (scooping, balancing, transporting, inserting) is a separate motor challenge. Grasp progression: palmar → digital → tripod. Wrist supination for scooping. Lip closure around spoon.
Progression: Loaded spoon → scooping from bowl → scooping from plate → fully independent. Backward chaining (parent does all EXCEPT the last step) is particularly effective. Practice with thick foods: dahi, kheer, halwa — they forgive imprecise scooping.
E-489: Fork Use: Spoon mastered → fork next. Stabbing and spearing require a different motor pattern — downward force rather than rotation. Targeted hand-eye coordination, force calibration (enough to pierce, not break food), wrist stability.
Progression: Stabbing large soft food (paneer cube) → small food (peas) → scooping with fork → cutting with fork edge. Paneer cubes are the ideal Indian practice food — soft enough to pierce, firm enough to stay on the tines.
Indian context: fork use is less culturally mandated than spoon use. Prioritise spoon mastery first and fork by functional need — school, social settings, specific food types.
E-490
Subdomain E1 Capstone
9 Materials That Help With Independent Meals
The moment: The capstone of Subdomain E1. Independent meals — sitting at the table, using utensils, eating a nutritionally adequate meal, managing bite size, chewing and swallowing safely, drinking from a cup, cleaning up, and participating in social context. Independence at the table is the foundation for independence in life.
7
Systems Integrated
Oral sensory, oral motor, fine motor, gross motor, executive function, social skills, and self-regulation — all converge at the independent meal.
40
Techniques in E1
Every technique in Subdomain E1 contributes to this single capstone goal — independence at the table, in every environment.
21M+
GPT-OS® Sessions
Pinnacle Blooms Network's evidence-based feeding resources, informed by millions of therapy sessions.
Build One Skill at a Time
Track each component of independent meals separately — utensils, sitting duration, bite size, cup drinking. Celebrate granular progress.
Generalise Across All Environments
Long-term goal: independent eating at home, school, restaurants, and family functions. Use the portable mealtime kit and systematic generalisation techniques.
The Feeding Journey Is Possible
From 5 foods to functional nutrition — with patience, science, and zero force, it happens. Celebrate every new food, every new skill, every meal where they sat and ate.
Preview of feeding eating Therapy Material
Below is a visual preview of feeding eating therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!