
9 Materials That Help Weaning from Bottle
When your toddler won't let go — a clinically validated, parent-tested protocol to bridge the gap to cup drinking. Evidence-based feeding therapy from Pinnacle Blooms Network®, India's largest pediatric therapy consortium.

ACT I — EMOTIONAL ENTRY
When the bottle won't let go.
It is 10:45 pm. Your three-year-old is asking — demanding — for the bottle. Not because they are hungry. The bottle is the only thing standing between sleep and a 45-minute meltdown. You have tried sippy cups, straw cups, water bottles with funny animals on them. All rejected. Your pediatrician said "wean by 18 months." Your dentist is worried about teeth. And you are exhausted, guilty, and wondering why every other child at playgroup seems to have made this transition effortlessly while yours cannot let go.
You are not failing. Your child's nervous system, emotional regulation, and oral motor development are all speaking — and the bottle is the only language that feels safe to them right now. This page is your decoding guide.
Technique: Structured Bottle-to-Cup Transition Using Multi-Domain Therapy Materials | Episode: E-464 | Feeding & Mealtime Independence Series
Reviewed by: Feeding Therapist • SLP • OT • ABA/BCBA • NeuroDev Pediatrician | FREE National Helpline: 9100 181 181 — Available 24×7 in 16+ languages

ACT I — THE NUMBERS
The numbers behind the struggle.
You are among millions of families navigating this exact transition. In India alone, Pinnacle's 70+ centers report that bottle weaning difficulty is among the top 5 feeding concerns for children aged 12 months to 4 years — across neurotypical children and those with autism, sensory processing differences, and developmental delays.
25–40%
Struggle with transition
of toddlers experience significant difficulty moving from bottle to cup
62%
Sensory-linked
of bottle-dependent children aged 2+ show sensory-linked oral preferences, not just habit
3×
Higher caries risk
dental caries risk in children using bottles beyond 18 months compared to those weaned on time
"Prolonged bottle use is not a parenting failure. It is a clinical signal that needs a clinical response." — Pinnacle Feeding Therapy Consortium
Global data reinforces urgency: WHO & UNICEF link bottle use beyond 24 months to iron-deficiency anaemia risk; the AAP recommends complete weaning by 12–18 months; and pooled milk around teeth during prolonged feeding is the primary driver of Early Childhood Caries.
ACT I — THE SCIENCE
It is not stubbornness. It is wiring.
The Neuroscience
The bottle nipple creates a highly specific sensory experience: soft silicone texture against the lips and tongue, slow controlled liquid flow, rhythmic suckling that activates the parasympathetic nervous system — the calming system. For children who experience the world intensely, this sensory cocktail is uniquely regulating.
When you remove the bottle, you are not just removing a cup. You are removing a self-regulation tool that the child's nervous system has learned to depend on.
Three Things Keeping Your Child Attached
Sensory Comfort
The nipple texture, temperature, and flow feel "right" in a way other cups simply don't match.
Emotional Security
The bottle has become a transitional object — like a lovey — signaling safety at bedtime and during stress.
Skill Gap
Cup and straw drinking require genuinely different oral motor skills your child may simply not have learned yet.
This is a wiring difference and a skill gap — not a behavior choice. All three are addressable with the right materials and approach.

ACT I — DEVELOPMENT
The developmental map of drinking.
Most children complete the bottle-to-cup transition between 12–18 months. Understanding where this sits on the developmental timeline helps parents see the clear path forward — and why delay is a waypoint, not a dead end.
6–9 Months
Open cup introduction (caregiver assisted)
9–12 Months
Straw drinking introduction possible
12–18 Months
Bottle weaning recommended (AAP guidelines)
18–24 Months
Independent cup drinking begins to be established
24 Months+
Full cup independence — caregiver target
You are navigating the transition zone. For children with sensory processing differences, ASD, oral motor delays, or anxiety profiles, this transition may be 6–18 months delayed — and a clear therapeutic path exists for each profile. Prolonged bottle use often co-occurs with food selectivity, dental concerns, and iron-deficiency anaemia. A feeding therapy assessment addresses all simultaneously.

ACT I — EVIDENCE
Clinically validated. Home-applicable. Parent-proven.
Evidence Grade: Level II — Multiple systematic reviews, RCTs, and clinical consensus support this approach.
PRISMA Systematic Review (2024) — PMC11506176
Multi-disciplinary feeding intervention meets evidence-based practice criteria in pediatric populations.
Meta-analysis, World J Clin Cases (2024) — PMC10955541
Structured sensory-motor intervention effectively promotes adaptive behavior and oral motor skills across 24 studies.
Padmanabha et al., Indian J Pediatr (2019)
Home-based, caregiver-administered interventions demonstrate significant outcomes in Indian pediatric populations.
WHO Nurturing Care Framework (2018) — PMC9978394
Caregiver-mediated early intervention in the home setting is the most impactful developmental lever available.
"The 9 materials on this page are not products. They are precision therapeutic tools selected from 20 million sessions of clinical evidence." — Pinnacle Blooms Consortium

ACT II — THE TECHNIQUE
Structured Bottle-to-Cup Transition Protocol
What It Is
A systematic, multi-layered therapeutic approach — nicknamed "The Bottle Bridge" — that addresses the three root causes of bottle dependency simultaneously: sensory preferences, emotional attachment, and oral motor skill gaps. Uses 9 specific therapeutic materials in a graduated framework rather than abrupt removal.
Who It Is For
Children aged 12 months to 4 years experiencing bottle dependency beyond age-appropriate windows — with particular application for children with autism, sensory processing differences, anxiety, oral motor delays, or a history of multiple failed weaning attempts.
At a Glance
Age Range: 12 months – 4 years
Frequency: Daily practice | 5–15 min per session
Timeline to outcome: 4–12 weeks (individual variation)
Domain Badges
- 🍽️ Feeding & Oral Motor
- 🧠 Sensory Processing
- 💬 Speech-Language Development
- ❤️ Self-Regulation
- 🔄 Behavioral-Routine Management
ACT II — THE TEAM
Five disciplines. One coordinated approach.
This technique crosses therapy boundaries because the child's nervous system doesn't organize by therapy type. At Pinnacle, the FusionModule™ integrates all five disciplines into a single converged feeding therapy pathway — one coordinated plan, not five separate ones.
Speech-Language Pathologist (SLP)
Primary lead for oral motor assessment, straw training, cup drinking skill development, and evaluation of speech impacts from prolonged bottle use.
Occupational Therapist (OT)
Sensory processing assessment, sensory-respectful cup introduction, routine and transition support, fine motor aspects of cup holding.
ABA / BCBA Therapist
Behavioral structure: scheduled bottle access, reinforcement for cup use, visual schedules, extinction of demand-based bottle giving.
Special Educator
Generalization to school and childcare settings, teacher communication templates, routine embedding across environments.
NeuroDev Pediatrician
Medical evaluation for iron deficiency anaemia, dental referral, nutritional guidance, and underlying developmental assessment.

ACT II — TARGETS
Precision targets. Not a random activity.
🎯 Primary Target
Bottle Dependency Elimination — Child drinks all fluids from cups within timeline; requests bottle fewer than once per day within 4–6 weeks; tolerates milk from cup with no distress.
🔵 Secondary Targets
- Straw drinking competence (used for life)
- Open cup lip control and liquid management
- Sleep independence without bottle as cue
- Tolerance of transitions without meltdown
- Self-soothing with age-appropriate alternatives
⚪ Tertiary Targets
- Oral motor maturation supporting speech sound production
- Dental health protection (ECC prevention)
- Iron nutritional status improvement
- Feeding independence for school-readiness
- Self-regulation skills that generalize beyond feeding

ACT II — MATERIALS 1–3
9 Materials. 9 Therapeutic Purposes.
Every material below is clinically selected. Each addresses a different root cause of bottle dependency. You do not need all 9 at once — start with 2–3 based on your child's profile. Call 9100 181 181 for personalized guidance.
Material 1 — Soft Spout Transition Cup
Canon Category: Oral Motor Tools — Transitional Cups
The sensory bridge. Silicone spout mimics the feel of a bottle nipple while introducing the cup format. The jump from soft nipple to hard sippy spout is too large for sensory-sensitive children — this cup closes that gap.
Price range: ₹300–800 | Search on Amazon.in →
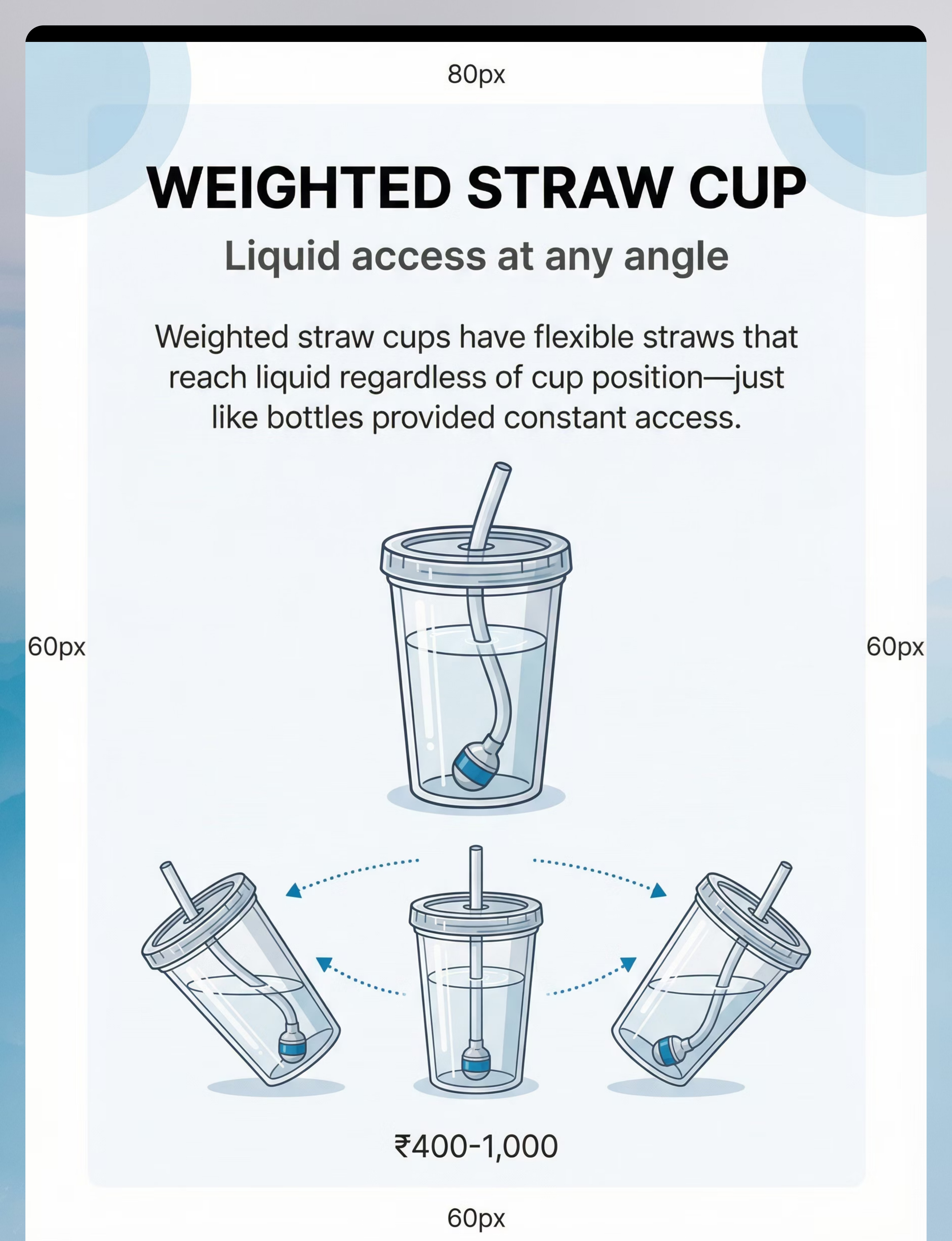
Material 2 — Weighted Straw Cup
Canon Category: Oral Motor Tools — Straw Cups
Straw drinking is developmentally more mature than bottle suckling. Weighted straws reach liquid at any cup angle — maintaining the "always available" quality the bottle had. Once straw drinking is learned, this becomes the bottle's true replacement.
Price range: ₹400–1,000 | Search on Amazon.in →
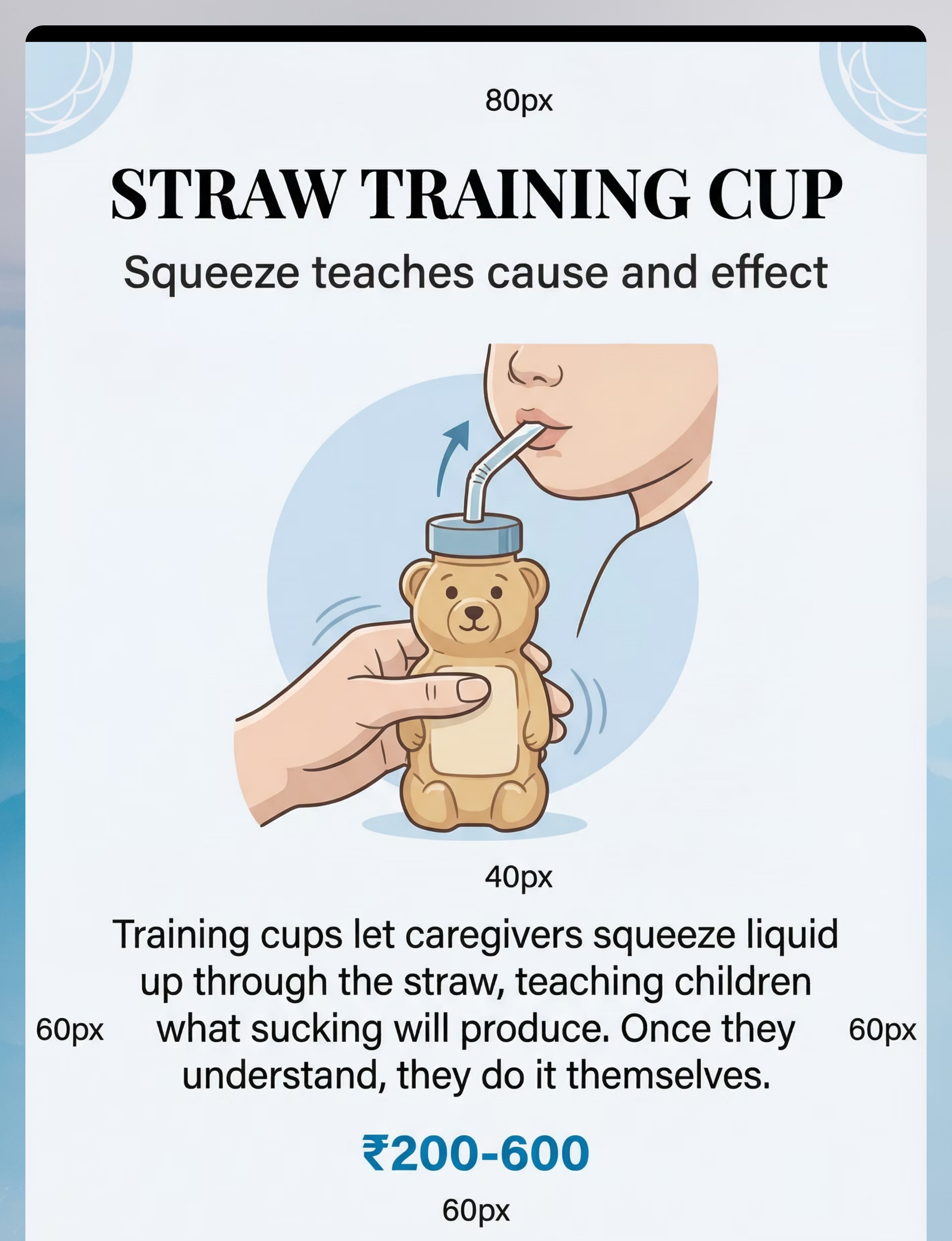
Material 3 — Straw Training Cup (Honey Bear)
Canon Category: Oral Motor Tools — Straw Training
Children can't accept straws if they don't understand how straws work. The honey bear squeeze bottle teaches cause-and-effect: caregiver squeezes → liquid appears → child learns to suck. A classic SLP tool.
Price range: ₹200–600 | Search on Amazon.in →

ACT II — MATERIALS 4–6
Materials 4, 5 & 6 — Cup, Character & Comfort
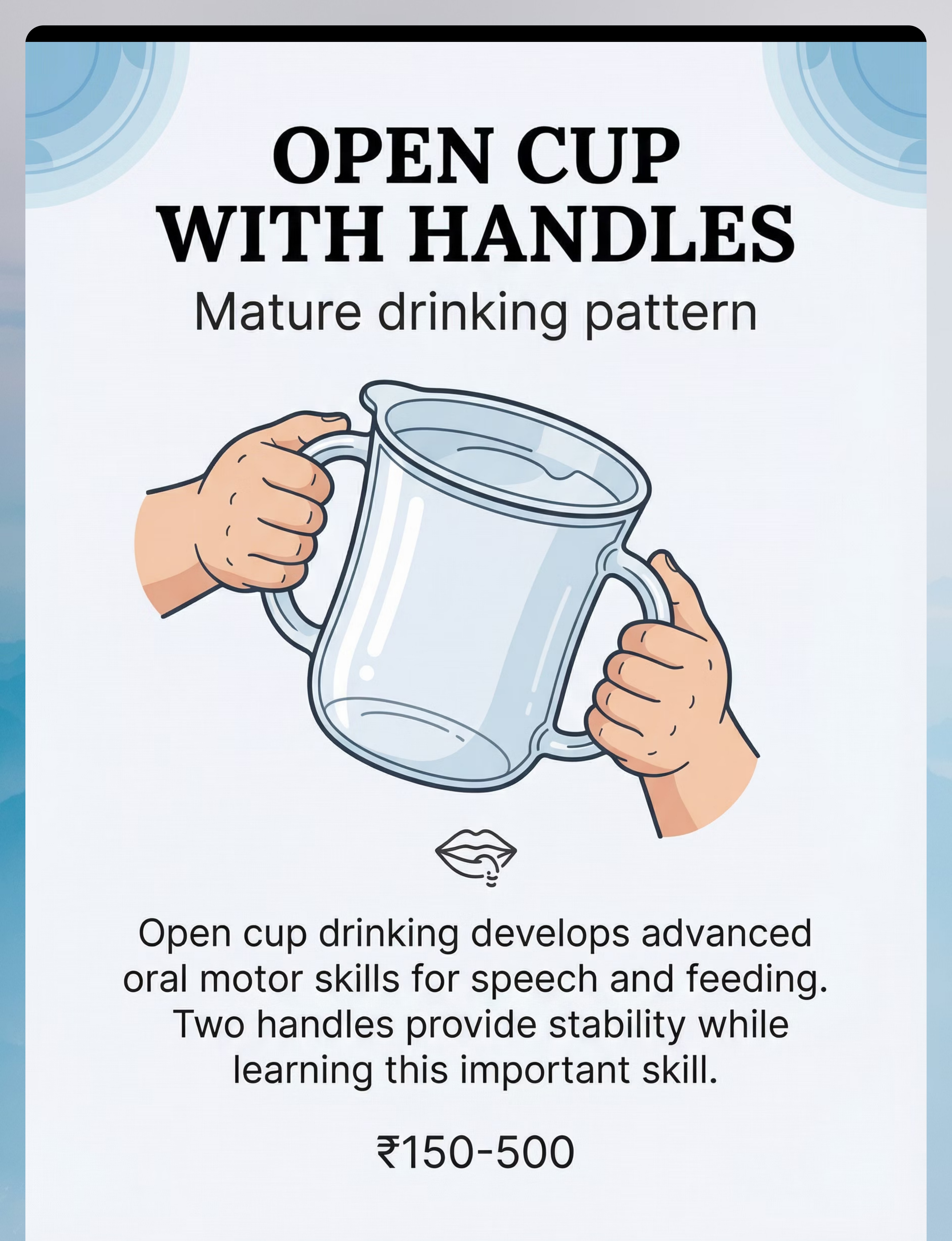
Material 4 — Open Cup with Two Handles
Canon Category: Oral Motor Tools — Open Cups
The most mature drinking pattern. Builds lip closure and liquid flow control that supports both feeding independence and speech sound development. Two handles provide stability for early learners.
Price range: ₹150–500 | Search on Amazon.in →
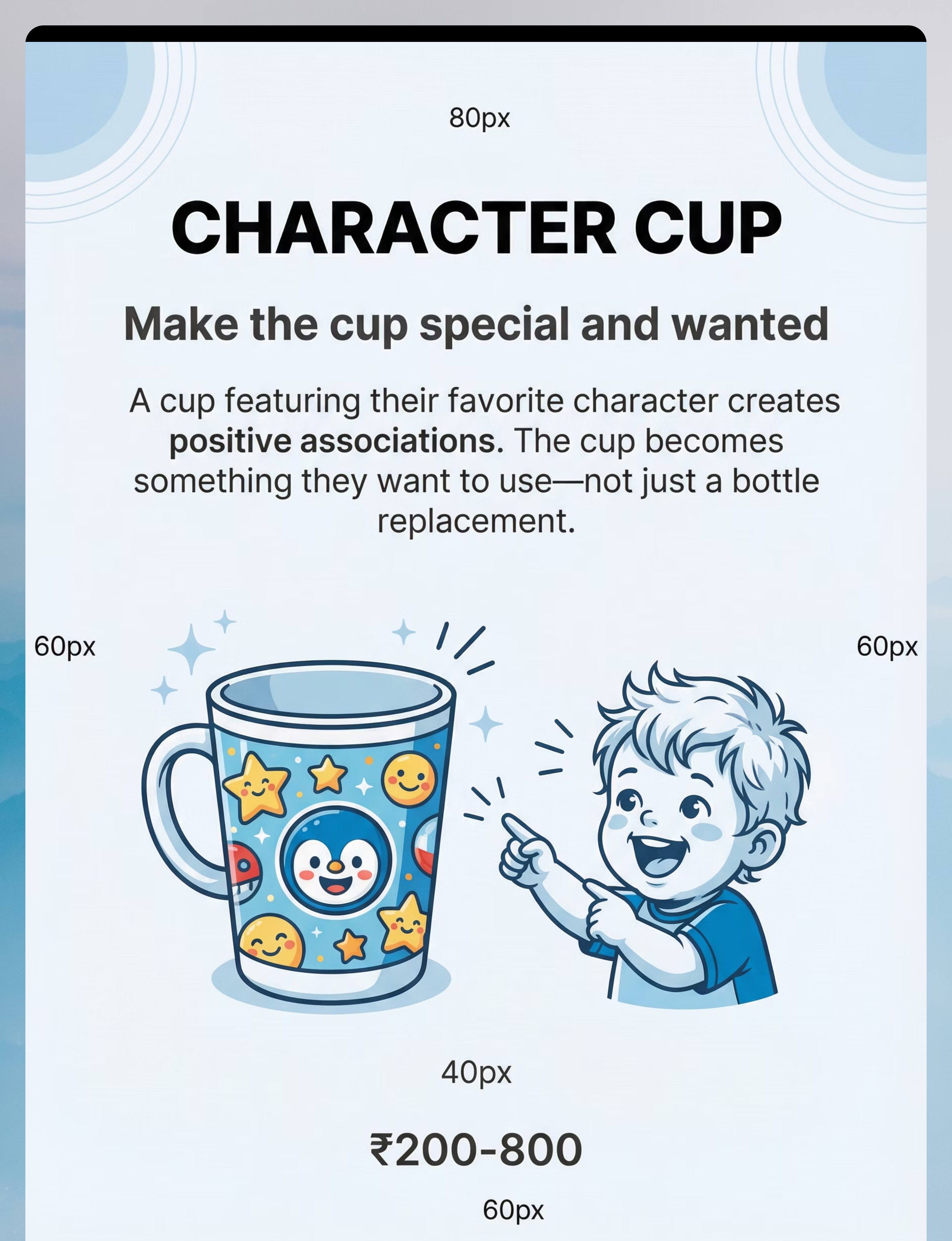
Material 5 — Character Cup
Canon Category: Motivation & Engagement Materials
Motivation matters. A cup featuring your child's beloved character creates positive association and ownership. The cup becomes something they want to use — not just a bottle replacement. Crucial for the emotional component of weaning.
Price range: ₹200–800 | Search on Amazon.in →
Material 6 — Comfort Lovey / Transitional Object
Canon Category: Transition Objects / Comfort Items
The bottle is often not about milk — it is about comfort. A new lovey introduced during bottle times transfers the soothing role as the bottle phases out. Non-negotiable for children with sleep-onset bottle dependency.
Price range: ₹200–1,000 | ₹425 — Comfort Transition Object on Pinnacle Canon →

ACT II — MATERIALS 7–9
Materials 7, 8 & 9 — Schedule, Timer & Story
Material 7 — Visual Schedule (Bottle Reduction Schedule)
Canon Category: Visual Supports — Daily Schedules
Bottle weaning feels arbitrary without structure. A visual schedule shows when bottles happen and when they don't — making reduction transparent and predictable rather than a daily battle. Essential for children with autism and routine dependency.
Price range: ₹100–400 (or DIY — see Card 14) | Search on Amazon.in →
Material 8 — Visual Timer / Sand Timer
Canon Category: Visual Supports — Timers
Verbal time limits feel arbitrary and trigger resistance. A visible timer externalizes the limit: the timer says bottle time is ending — not the parent. Reduces confrontation and teaches self-regulation beautifully.
Price range: ₹100–600 | Search on Amazon.in →
Material 9 — Social Story (Bottle to Cup Growing-Up Story)
Canon Category: Social Communication Tools — Narrative Books
For children aged 2+, a personalized social story frames weaning as growing up — not losing something. "Big kids drink from cups" becomes something to aspire to. Can be DIY-created with your child's name and photos.
Price range: ₹100–400 (or DIY) | Search on Amazon.in →

ACT II — ACCESSIBILITY
Every family can start today. Zero-cost options for every material.
WHO/UNICEF Equity Principle: Effective early intervention must not be income-dependent. Every technique on this page has a zero-cost alternative that applies the same therapeutic mechanism.
Material | ₹0 / DIY Alternative | Why It Works | |
Soft Spout Cup | Cut tip of an old silicone bottle nipple, attach to a small regular cup with tape | Same silicone texture principle | |
Weighted Straw Cup | Standard steel straw in a small steel cup with preferred liquid; help child learn angle | Same straw-drinking skill | |
Straw Training | Any cleaned squeeze bottle (ketchup-style) with straw attached — squeeze liquid up | Identical cause-effect teaching | |
Open Cup | Any small steel tumbler or clay cup with a safe lip edge | Same oral motor development | |
Character Cup | Decorate any cup with child's favorite sticker or printout; involve child in decorating | Same ownership + motivation | |
Comfort Lovey | Any soft cloth item, fabric from parent's clothing tied to stuffed toy | Same comfort-transfer attachment | |
Visual Schedule | Printed or drawn pictures glued to cardboard with velcro; phone photos work | Same predictability principle | |
Visual Timer | Any kitchen timer placed visibly; count down verbally with hand signals | Same externalized limit | |
Social Story | Handwritten or printed booklet with child's name and your own photos | Same narrative growth framing |
When the clinical-grade material is non-negotiable: For children with significant sensory processing differences or oral motor delays, the precise tactile properties of a professional soft-spout cup or straw training cup matter. If multiple DIY attempts fail, the clinical material is likely needed — call 9100 181 181.

ACT II — SAFETY
Read before every session.
🔴 DO NOT PROCEED — Consult a Professional
- Child has known swallowing difficulty (dysphagia) or history of aspiration
- Child shows signs of significant weight loss or dehydration
- Child has structural oral differences not yet professionally assessed
- Weaning attempts trigger self-injurious behavior or severe distress (4+ hours)
- Child is under active treatment for an acute illness
🟡 MODIFY — Proceed with Adjustments
- Child is unwell, teething, or recently disrupted — slow down; do not advance stage
- Child is in a high-stress period — hold at current cup tolerance; do not remove bottles
- Caregiver consistency is not possible this week — pause reduction until all caregivers are aligned
🟢 PROCEED — When All Apply
- Child is regulated, well-rested, recently fed
- Environment is calm and familiar
- All household caregivers are briefed on the current step
- You have at least 15 uninterrupted minutes
Material safety: Check all cups for cracks, spout tears, or straw damage before every use. Straw diameter must be appropriate for child's age — if liquid flows too fast, cover end partially with finger. Comfort lovey must meet age-appropriate safe sleep guidelines if used at bedtime.

ACT II — SETUP
The right environment multiplies success.
Space Setup
Primary position: Child seated at table or highchair
- Left side: Preferred liquid cup (start cup)
- Right side: Character cup (aspirational cup)
- Behind/beside: Visual schedule — visible to child
- Timer: On table, within child's sight line
- Comfort lovey: On or beside chair — available if needed
Remove: TV/screens if they distract from cup engagement; other bottles (keep out of sight during practice sessions); sippy cups the child has already rejected.
Environmental Recommendations
Lighting: Natural or warm — avoid harsh overhead lights, which are dysregulating for sensory-sensitive children.
Sound: Quiet preferred, or gentle familiar background music. No competing audio demands.
Temperature: Liquid temperature matters enormously. Start with child's preferred temperature. Many children accept cups more readily with warm liquid initially.
Timing: Best sessions: post-nap, mid-morning snack time, or 30 minutes before a meal — not during hunger peak.
Position the bottle visibly but not immediately accessible — present in the visual schedule but not within grab-reach.

ACT III — EXECUTION
60-second pre-session readiness check. Every time.
The best session is one that starts right. A 5-minute successful session is worth more than a 30-minute forced one. Run this check before you begin.
Readiness Indicator | ✅ Ready | 🔴 Not Ready | |
Child has eaten within the last 90 minutes | Fed and settled | Severely hungry — will not accept cup | |
Child has slept recently | Well rested | Overtired — reverts to comfort-seeking immediately | |
Child appears calm or regulated | Calm baseline | Already in meltdown or transition dysregulation | |
Environment is calm and familiar | Home routine | Novel environment — hold practice | |
No illness or physical discomfort signs | Well, comfortable | Even mild teething or cold — reschedule 24 hours | |
Caregiver is calm and not rushed | Relaxed | Caregiver anxiety transfers — give yourself 5 minutes first |
✅ 5–6 Indicators Met
GO — Full session as planned
✅ 3–4 Indicators Met
MODIFY — Shorter session, no new materials introduced
✅ 0–2 Indicators Met
POSTPONE — Brief calming activity instead. No cup pressure today.

ACT III — STEP 1
Step 1 of 6: Invite — never command.
What to Do
Introduce the cup into the environment without placing any demand for drinking. Show the cup, talk about it positively, let the child touch it. No pressure for mouth contact yet.
What to Say (Exact Script)
"Look what I found! This is [Child's Name]'s special cup. Want to see it? It has [favourite character] on it! Let's have it near us while we [eat/play/sit together]."
For younger children: Simply place cup on table within reach. Let curiosity lead.
Reading Acceptance Cues
Reaches for cup or leans toward it
Strong readiness signal — proceed to Step 2.
Looks at cup and returns to activity
Neutral — proceed gently at low demand.
Pushes cup away or turns head
Accept this. Try again in 10 minutes with zero pressure. Today may be cup-present-only.
Body language: Sit at child's level. Relaxed posture. Make cup interaction look enjoyable — sip from your own cup simultaneously. Timing: 30–60 seconds of invitation before next step.

ACT III — STEP 2
Step 2 of 6: Engage — let the cup become familiar.
Child has accepted the cup's presence. Now introduce the liquid — making the experience positive, exploratory, and zero-demand initially. "Should we put [preferred drink] in your special cup? Let's see..."
🔵 Sensory-Sensitive Child
Start with the Soft Spout Cup. Let child mouth the silicone spout without liquid first. Familiar texture creates safety before any drinking demand is placed.
🟡 Skill-Gap Child
Start with the Straw Training Cup. Hold honey bear to lips, squeeze gently — liquid appears. Child learns cause-and-effect: this is straw learning in action.
🟢 Emotionally-Attached Child
Start with the Character Cup during a calm, positive moment — not during a high-need moment. Build positive associations first; cup competence follows.
Reinforcement cue: The moment the child touches lips to cup — even briefly, even without drinking — praise immediately: "Yes! You touched your cup! That's exactly right. You're such a brave kid!" Timing: 1–3 minutes. End before the child loses interest.

ACT III — STEP 3
Step 3 of 6: The core drinking trial.
Graduated introduction of actual drinking from the chosen cup. Not full bottle replacement yet — brief, successful trials are the goal at this stage.
Soft Spout Cup
Offer cup with a small amount of liquid. Spout at lips — let child manage the flow. First trials: even 1–2 sips = complete success. Do not push for more.
Straw Training Cup (Honey Bear)
Place straw at child's lips. Squeeze a tiny amount of liquid up. Watch for tongue position. On next trial, squeeze less. Then stop squeezing and wait for child to
ACT III — STEP 4
Step 4 of 6: Dosage and variation.
Target Repetitions
Days 1–3
1 brief cup trial per session (success = any lip contact)
Days 4–7
2–3 sip trials per session
Week 2+
Gradual volume and frequency increase based on child's lead
"3 successful sips today > 10 forced sips that end in meltdown. Dosage is quality, not quantity."
Variation Strategies
Change liquid temperature
If room-temperature rejected, try slightly warm or cold
Change setting
Once accepted at highchair, try floor, small table, snack in garden
Change the cup
Once soft spout accepted → character cup → straw cup
Model drinking
Sit beside child and drink from an identical cup yourself
Pair with preferred activity
Have cup present during favourite show, book time, or play

ACT III — STEP 5
Step 5 of 6: Make success feel worth it.
Timing rule: Reinforcement must come within 3 seconds of the desired behavior. After 3 seconds, the child has moved on.
"YES! You drank from your cup! I am SO proud of you! That was amazing!"
Verbal Praise
Specific, not generic: "You drank from your straw cup!" lands far better than "Good job."
Physical Celebration
High five, hug, spin, clap together — match your child's preferred physical connection.
Visual Reward
Sticker on a chart, star drawn, coloring a bottle-to-cup journey chart. Sticker Reward Chart ₹364 →
Token System
5 cup sips = one token = preferred activity. Star Token System ₹589 →
"Celebrate the attempt, not just the perfect outcome. Every lip-touch is progress."

ACT III — STEP 6
Step 6 of 6: End every session intentionally.
No session ends abruptly. The cool-down transitions the child from cup practice back to their normal routine without the abruptness that triggers protest. Consistent endings teach that transitions are safe.
Transition Warning (2 Min Before End)
"Two more sips, then we're all done with cup practice. You're doing so well."
Visual Timer use: Start timer as you say "two more." Child watches time ending. When timer finishes: "Timer says all done! Great cup work today. Time for [next activity]."
If the Child Resists Ending
"I know. Cup time is done for now. We'll do more tomorrow. Here's your [lovey/book/toy]."
Do not extend session past cool-down. Ending is part of the protocol.
Cool-Down Routine (Choose One)
Put cup together on "special shelf" — not hidden, just in its home
Offer comfort lovey if child reaches for bottle
Move immediately to a preferred, low-demand activity
Sing a familiar transition song or phrase used consistently
After session: If a scheduled bottle time follows, it remains on the visual schedule. Structure, not cold turkey. The child sees: cup practice → normal routine → scheduled bottle (if still in weaning phase).

ACT III — DATA
Within 60 seconds of session end — record these 3 things.
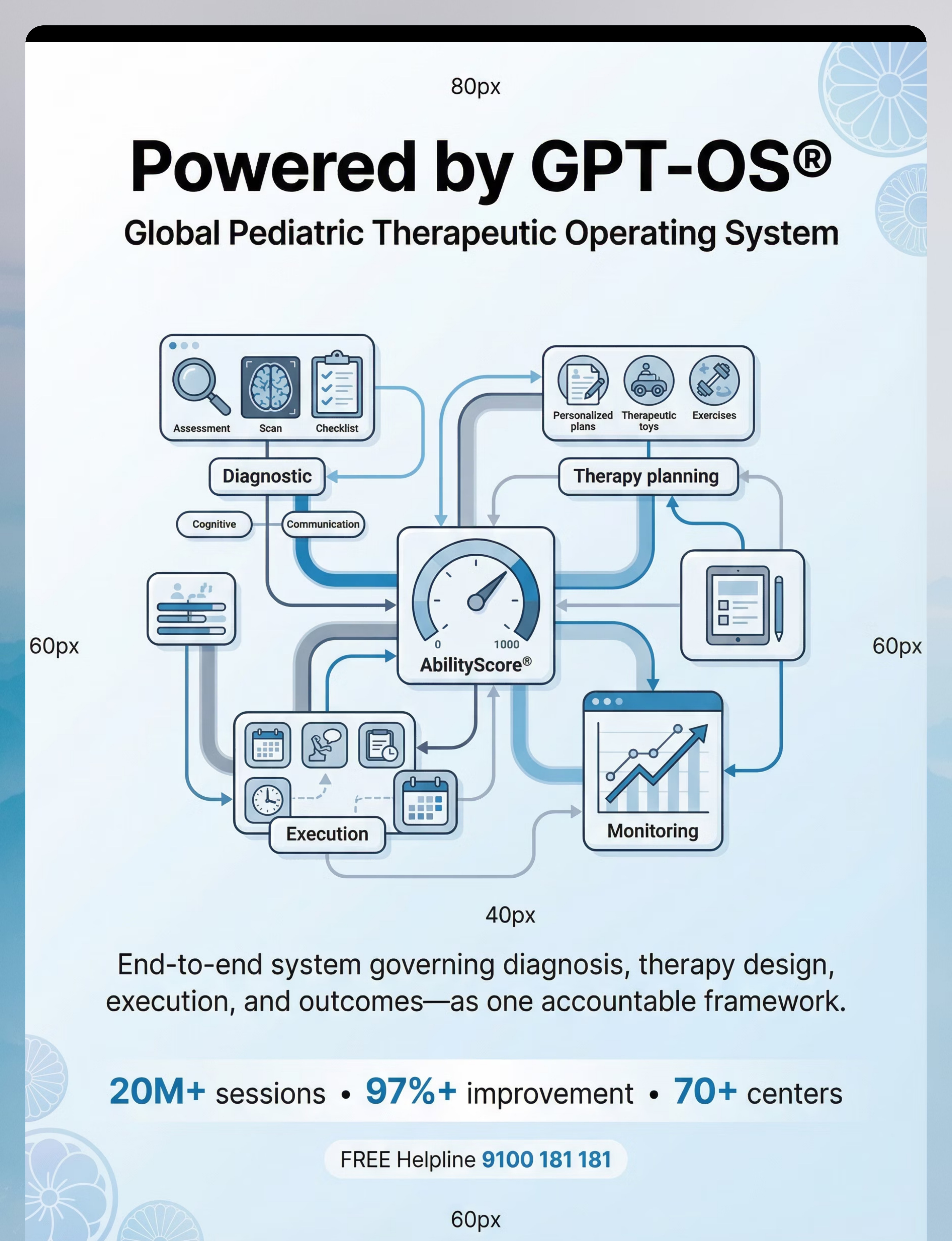
"60 seconds of data now saves hours of guessing later." Your session data feeds directly into your child's Feeding Independence Readiness Index on the GPT-OS® dashboard, tracking progression from Stage 1 (complete bottle dependency) to Stage 5 (full cup independence).
1. Cup Trials Completed
[ 0 ] [ 1 ] [ 2 ] [ 3 ] [ 4 ] [ 5+ ]
2. Child's Best Response Today
- Refused cup entirely
- Lip contact only
- 1–2 sips
- 3–5 sips
- Drank full small amount voluntarily
3. Bottle Requests Today
Count of requests before, during, and after session. This trending number is your most powerful progress signal.

ACT III — TROUBLESHOOTING
Real sessions are messy. Here's your fix guide.
"Session abandonment is not failure — it is data. Every difficult session tells you something the next session needs."
Child completely refused and melted down
Why: Cup introduced at wrong time, or cup type's sensory properties were wrong. Next session: Return to cup-present-only. Try a different cup type with preferred juice, zero demand to drink. Reassess readiness checklist.
Child accepted cup then grabbed bottle and refused to give back
Why: Bottle still within reach during cup practice, or no visual schedule structure yet. Next session: During cup practice, bottles are physically out of sight. Visual schedule shows cup time → next activity.
Child won't drink milk from any cup — only water
Why: Extremely common. Milk has specific comfort associations tied to the bottle that water does not. Keep water from cup as a win. Introduce warm milk in character cup at a neutral snack time — not bedtime.
Bedtime bottle is completely non-negotiable
Why: Bedtime bottle is a sleep association, not thirst. It is the last to be weaned. First wean all daytime bottles, then establish lovey, then move milk to cup at earlier snack, then lovey replaces bottle at sleep. Allow 4–8 weeks for this phase specifically.
Grandparents or babysitter giving bottle during weaning
Why: Caregiver inconsistency is the single biggest cause of weaning stall. One bottle given outside the plan resets a week of progress. Use Card 32's Family Guide PDF and request a caregiver alignment call at 9100 181 181.
Stuck at same stage after 3 weeks
Why: A hidden factor — sensory, oral motor, or behavioral — is maintaining the block. This is the clinical referral signal. Three weeks of honest, consistent effort without movement = feeding therapy assessment needed. Call 9100 181 181.
ACT III — ADAPT
Your child's profile. Your personalized version.
Easier Version
Cup present, no drinking demand (days 1–5). Cup as toy during water play. Straw training with preferred juice only, zero milk pressure. One 3-minute session per day maximum.
Core Version
Follow Steps 1–6 as described. 5–10 minute sessions, 1–2 times daily. Graduated volume increase week by week. Track on daily tracker.
Advanced Version
Full cup meals for all daytime drinking. Open cup practice alongside straw cup. Bedtime bottle weaning phase begins. Child self-selects cup from two options.
Child Profile | Key Modification | |
Sensory-sensitive, texture-focused | Soft spout → hard spout only after 2 weeks acceptance. Warm liquid to start. Silicone straw preferred over plastic. | |
Emotionally attached, comfort-seeking | Lovey always available. Character cup introduced with ceremony. No bottle weaning during bedtime disruptions. | |
Oral motor skill gap | Honey bear straw training 5 minutes before every meal for 2 weeks. Open cup with 5ml water only. SLP involvement recommended. | |
Routine-rigid, autism profile | Visual schedule 1–2 weeks before any bottle removal. Social story nightly for 2 weeks before beginning. No simultaneous changes. | |
Typically developing older toddler (2.5–4 years) | Narrative approach: "Bottle Fairy," giving bottles away, graduation ceremony. Child agency in choosing their new cup. |


ACT IV — PROGRESS ARC
Week 3–4: The child begins to anticipate.
~40% — Stage 3: Increasing Cup Use. The behavioral shift in Week 3–4 signals that new neural pathways are consolidating. You may notice you're more confident now, too. Your instincts are calibrating. Trust them.
✅ Consolidation Indicators
- Child reaches for their character cup at snack time without being prompted
- Cup drinking occurring voluntarily 2–3 times per day for water or juice
- Comfort lovey is established at bedtime alongside bottle
- Child references visual schedule without meltdown when bottle is not scheduled
- Straw training no longer requires parent squeezing — child initiates suction
- Daytime bottle requests have decreased — child accepts "cup time" with less protest
🔑 Behavioral Signals of Neural Pathway Formation
- Child brings cup to parent to be filled (proactive use — massive signal)
- Child begins copying parent's cup drinking at meals
- Child's language around "cup" becomes positive or neutral (not immediately negative)
▶ When to Increase Intensity
If Week 3–4 consolidation is solid → remove one daytime bottle from the visual schedule (the easiest one — typically mid-morning or afternoon). Replace with cup. One change at a time.

ACT IV — PROGRESS ARC
Week 5–8: The bottle becomes optional.
~75–90% — Stage 4: Advancing Independence. This is the phase families remember. The shift from "requires cup practice" to "chooses cup" is a genuine developmental milestone.
✅ Mastery Criteria
- All daytime bottles eliminated; cups used independently for water, juice, and emerging milk
- Child selects their cup from two options presented
- Cup drinking persists in multiple settings: home, grandparents', childcare
- Bottle requests are infrequent and can be redirected
- Open cup trials possible with small volumes at structured snack times
- Comfort lovey used independently at bedtime without bottle prompt
🌍 Generalization Indicators
- Child drinks from straw at restaurant without difficulty
- Child accepts cup of water from unfamiliar person (school, clinic)
- Child asks for "cup" rather than "bottle" on waking
Before starting bedtime bottle weaning: Only begin when ALL daytime bottles are eliminated AND the lovey is established as a comfort object. Rushing bedtime weaning before this is the most common cause of full regression.

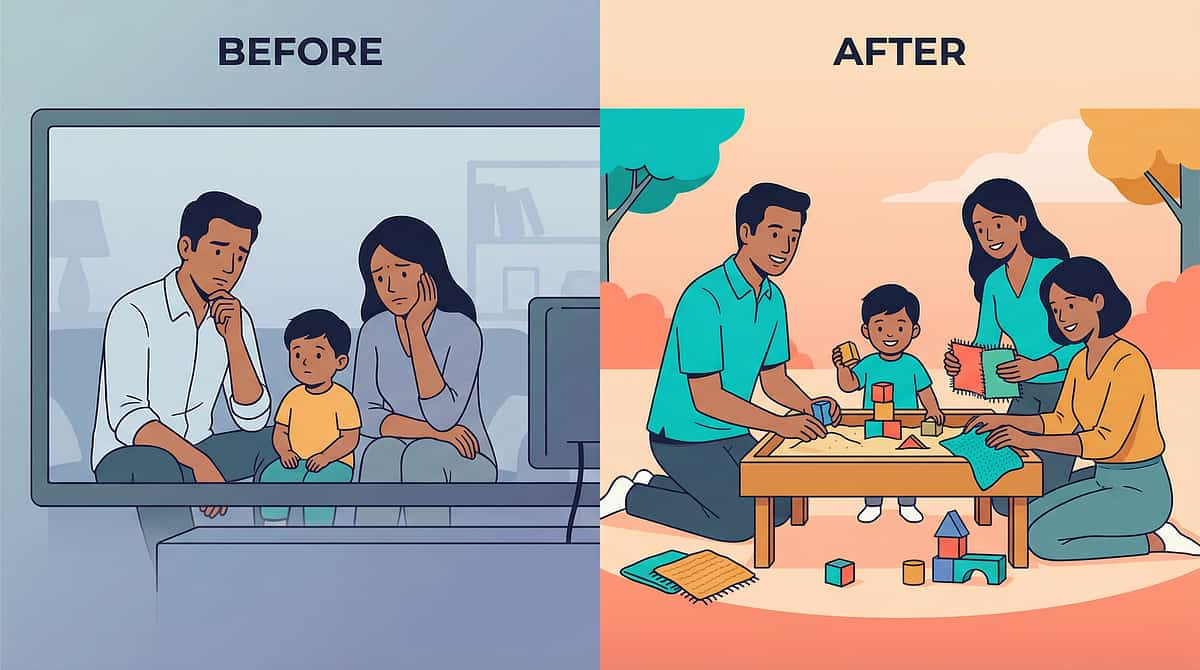
ACT IV — CELEBRATE
You did this. Your child grew because of your consistency.
This was not easy. Bottle weaning for a child with strong attachment, sensory preferences, or developmental differences is one of the most emotionally demanding transitions a family faces. Every refused cup, every night you stayed firm, every morning you kept the visual schedule — it all compounded into this.
Dental Protection
Protection from Early Childhood Caries that would have affected growing teeth.
Oral Motor Foundation
Skills that will serve their speech and feeding for life — now established.
Self-Regulation
Self-soothing without an external feeding object — a genuine developmental milestone.
Nutritional Balance
Iron-rich solids can now meet their needs — milk volume no longer displacing nutrition.
📸 Journal prompt: Take a photo of your child drinking from their cup today. Write one sentence: "On [date], [child's name] drank from a cup independently for the first time."
ACT IV — RED FLAGS
Even in progress — know when to pause and ask.
🔴 Red Flag | Why It Matters | What To Do | |
Child not drinking enough fluid (reduced wet nappies, dry lips) | Risk of dehydration — weaning progressed too quickly | Offer bottle immediately; slow pace significantly; consult pediatrician | |
Child gags, chokes, or coughs consistently when drinking from cups | Possible dysphagia or oral motor challenge requiring clinical assessment | Stop cup practice; SLP feeding evaluation urgently needed | |
Child loses more than 0.5 kg during weaning attempt | Nutritional refusal — child choosing not to eat or drink rather than use cup | Return to previous stage; feeding therapist assessment | |
Severe self-injurious behavior or prolonged distress (2+ hours daily) | Emotional dysregulation exceeding home management capacity | Pause all active weaning; call 9100 181 181; behavioral support needed | |
Three or more weeks of consistent effort with zero progress | Clinical factors present requiring professional identification | Feeding therapy referral — call 9100 181 181 |
🏠 Self-Resolve
Minor regression, illness-related. Return to previous stage for 3–5 days.
📱 Teleconsult
No progress for 2+ weeks, behavioral escalation. Book at pinnacleblooms.org/teleconsult
🏥 Clinic Visit
Red flags above, suspected medical/oral motor factors. Call 9100 181 181

ACT IV — PATHWAY
Where you were. Where you are. Where you're going.
E-464 sits within a carefully sequenced feeding independence series. Each technique builds directly on the skills established in the previous one.
E-462
Slow Eating / Prolonged Meals
E-463
Eating Too Fast / Speed Regulation
★ E-464
Bottle Weaning — YOU ARE HERE
E-465
Cup Drinking Skills Development
E-466 → E-469
Straw Drinking | Open Cup | Sleep Transitions | Pacifier Weaning
Long-term developmental goal this feeds: Full Feeding Independence → School Readiness → Social Participation in Mealtimes → Oral Motor Foundation for Clear Speech
ACT IV — RELATED TECHNIQUES
Other techniques in your Feeding & Mealtime toolkit.
You already own the visual schedule, timer, and comfort lovey for these techniques — they transfer directly. Each technique below shares materials and therapeutic mechanisms with E-464.
Technique | Difficulty | Primary Material | |
🟡 Core | Open Cup / Weighted Straw Cup | ||
🟡 Core | Honey Bear / Straw Training Tools | ||
🔴 Advanced | Open Cup with Handles | ||
🔴 Advanced | Comfort Lovey / Visual Schedule | ||
🟢 Intro | Social Story / Comfort Lovey | ||
🟡 Core | Visual Timer / Structured Routine |
ACT IV — DEVELOPMENTAL MAP
Bottle weaning is one piece of your child's complete developmental journey.
E-464 sits within Domain E — Feeding & Mealtime Independence, connected directly to Domains B (oral communication), C (self-regulation for transitions), D (behavioral routine management), and G (speech-language oral motor).
"Bottle weaning is not just feeding therapy. It is self-regulation, oral motor, behavioral, and emotional development — all at once." This is why the FusionModule™ coordinates SLP, OT, ABA, and feeding therapy simultaneously rather than sequentially.
ACT V — COMMUNITY
Three families. The journey you're on.
Family 1 — Chennai | 3 years 4 months | Autism diagnosis
Before: Completely bottle-dependent for milk — five times daily including twice at night. Every cup thrown across the room. Dentist reported two front teeth already affected.
Approach: Soft spout cup introduced alongside bottle (not instead of) for 2 weeks, zero demand. Visual schedule + honey bear straw training with juice + comfort elephant at bedtime. Graduated reduction over 8 weeks.
After: Daytime bottles gone by week 8. Uses weighted straw cup for milk. Bedtime bottle became milk-in-cup with the elephant. No more crying. Dentist is happy.
"We spent 18 months fighting the bottle. 8 weeks with the right system and it was done."
Family 2 — Hyderabad | 2 years 8 months | Sensory processing differences
Before: Would accept water from cups — but milk only from the bottle. Every cup spout texture felt wrong. She'd gag and push them away.
After: Warm milk in soft silicone spout cup was the unlock. Graduated to straw cup in 3 more weeks. "The temperature and texture were the keys we'd been missing."
Family 3 — Delhi | 3 years 9 months | Typically developing
Before: Cold turkey attempted twice. Both times — 3 days of screaming and refusing all food and drink. Gave up.
After: Social story + bottle fairy ceremony + child-selected character cup. "He waved goodbye to the bottles himself. That was 3 months ago. Never asked for one again."
📌 From the Therapist's Notes (SLP, Pinnacle Feeding Team): "Parents who fail at bottle weaning have almost always tried only the behavioral approach — just removing the bottle — without addressing the sensory or comfort dimensions. When you address all three, the transition is rarely the battle parents dread."

ACT V — COMMUNITY
You are not navigating this alone.
Isolation is the enemy of consistent implementation. Families who connect with peer communities during feeding transitions show significantly higher adherence and lower caregiver burnout.
WhatsApp Parent Group
Active parents sharing day-by-day progress, material tips, and encouragement. Real-time support from families navigating the same transition.
Pinnacle Parent Forum
Moderated by Pinnacle feeding therapists at pinnacleblooms.org/community/feeding. Searchable by technique code E-464.
Local Parent Meetup
Find parents in your city navigating the same journey. pinnacleblooms.org/events
Peer Mentoring
Connect with a parent who has successfully completed bottle weaning with a child profile similar to yours. Request via 9100 181 181.
"Your experience — even the hard weeks — will help a family currently on Day 3. Consider sharing your journey when you reach the other side."
ACT V — PROFESSIONAL SUPPORT
Home is powerful. Professional support multiplies it.
Pinnacle Blooms Network® — 70+ Centers Across India. For E-464 Bottle Weaning, request these specialists:
Specialist | What They Provide | |
🗣️ Pediatric SLP / Feeding Therapist | Oral motor assessment, straw training, cup drinking skill evaluation, speech-feeding connection | |
💆 Pediatric OT | Sensory processing profile for oral/tactile, transition routine support | |
🎯 BCBA/ABA Therapist | Behavioral structure for bottle reduction, reinforcement systems, caregiver consistency coaching | |
🧬 NeuroDev Pediatrician | Iron levels, dental referral, developmental monitoring, underlying factor assessment |
Can't travel to a center?Book Teleconsultation → Available in 16+ languages. Some private insurance plans cover pediatric feeding therapy under developmental disorder coverage.
ACT V — RESEARCH
For the parent who wants to go deeper.
PRISMA Systematic Review (2024) — PMC11506176
Children journal — 16 studies (2013–2023) confirm multi-disciplinary feeding intervention meets evidence-based practice criteria for pediatric populations including ASD.
Meta-analysis (2024) — PMC10955541
World Journal of Clinical Cases — 24 studies confirm sensory-motor intervention promotes oral motor skills, adaptive behavior, and feeding-related outcomes across diverse pediatric populations.
Padmanabha et al., Indian J Pediatrics (2019)
DOI: 10.1007/s12098-018-2747-4 — Indian RCT validating home-based, caregiver-administered interventions in Indian pediatric settings, with significant measured developmental outcomes.
WHO Care for Child Development Package (2023) — PMC9978394
Caregiver-mediated early intervention implemented across 54 low- and middle-income countries; household-based approaches demonstrate robust effectiveness.
NCAEP Evidence-Based Practices Report (2020)
Visual supports, structured behavioral protocols, and video modeling: all classified evidence-based for autism. Foundation for visual schedule and social story components of this protocol.
ACT V — SHARE
The more people who understand this, the more consistent the result.
One parent following this protocol while a grandparent gives bottles on demand is the #1 cause of prolonged weaning difficulty. Share this resource with everyone in your child's life — including the one-page simplified version below.
📖 The Grandparent/Caregiver Version
"We are helping [child's name] learn to drink from cups. This is recommended by [their] pediatrician and supported by [their] therapists."
When you are with [child's name]:
- ✅ Offer liquids in the cups shown to you
- ✅ Do NOT give a bottle unless child is showing red flags (severe distress, refuses all fluids)
- ✅ If asked for a bottle, redirect: "Your cup is right here. Let's have your special cup."
- ✅ If unsure, call [parent's number]
"This consistency makes the difference between 3 weeks and 3 months."
Share This Page
Page URL: techniques.pinnacleblooms.org/feeding/weaning-from-bottle-E-464
For School & Childcare
A pre-formatted teacher communication letter for school and childcare providers is available — ensures the same cup-first approach is maintained across all environments your child spends time in.
Preview of 9 materials that help weaning from bottle Therapy Material
Below is a visual preview of 9 materials that help weaning from bottle therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!
ACT VI — FAQs & CLOSE
Real questions from parents at Pinnacle centers.
My child is 3.5 years old and still has a bottle. Is it too late?
It is not too late. Children have successfully weaned at ages 4 and even 5 with the right approach. The older the child, the more the narrative approach (social stories, child agency) becomes the primary lever — but dental and oral motor urgency increases with each year. Call 9100 181 181 for an age-specific plan.
Should I just go cold turkey?
For children with minimal sensory attachment and strong cognitive understanding, cold turkey can work quickly. For children with sensory preferences, autism, anxiety, or comfort-object attachment, cold turkey typically results in temporary drinking refusal (dehydration risk), prolonged distress, and full regression. If cold turkey has already failed twice, the graduated multi-material approach is clinically indicated.
My child drinks water from cups but only milk from the bottle. What's happening?
This is extremely common. Milk has specific sensory-emotional associations tied to the bottle's comfort role that water does not. Establish cup competence with water and juice first, then introduce milk from cup in the character cup at a neutral snack time — not at bedtime. Gradual dilution (90% milk + 10% water, then 80-20, etc.) in the cup can also bridge this transition.
Is the bottle affecting my child's speech?
Direct causation is not confirmed. What is established: bottle nipple suckling uses oral motor patterns that differ from those required for speech sounds. Extended use of immature oral motor patterns can delay mature pattern development. An SLP assessment will evaluate whether speech-oral motor connections warrant specific intervention.
How do I know if my child needs a feeding therapist vs. handling this at home?
Home management suits mild-moderate bottle attachment with no suspected oral motor delays and some cup acceptance history. Clinical referral is indicated when multiple consistent attempts have failed; child shows oral motor difficulty (gagging, coughing); autism, sensory differences, or anxiety disrupts home management; or dental concerns are already present. When in doubt — call 9100 181 181.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | GSTIN: 36AAGCB9722P1Z2. FREE National Helpline: 9100 181 181 — 24×7 | 16+ Languages.Medical Disclaimer: This content is educational and does not replace individualized feeding assessment and intervention with licensed feeding therapists, SLPs, OTs, or pediatricians. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.