
When Their Mouth Says No Before They Can Try
Texture Acceptance Therapy — 9 Materials That Change Everything
You are not failing. Your child's oral sensory system is overwhelmed, not defiant. There is a neurological reason for every gag. And there is a systematic path forward.
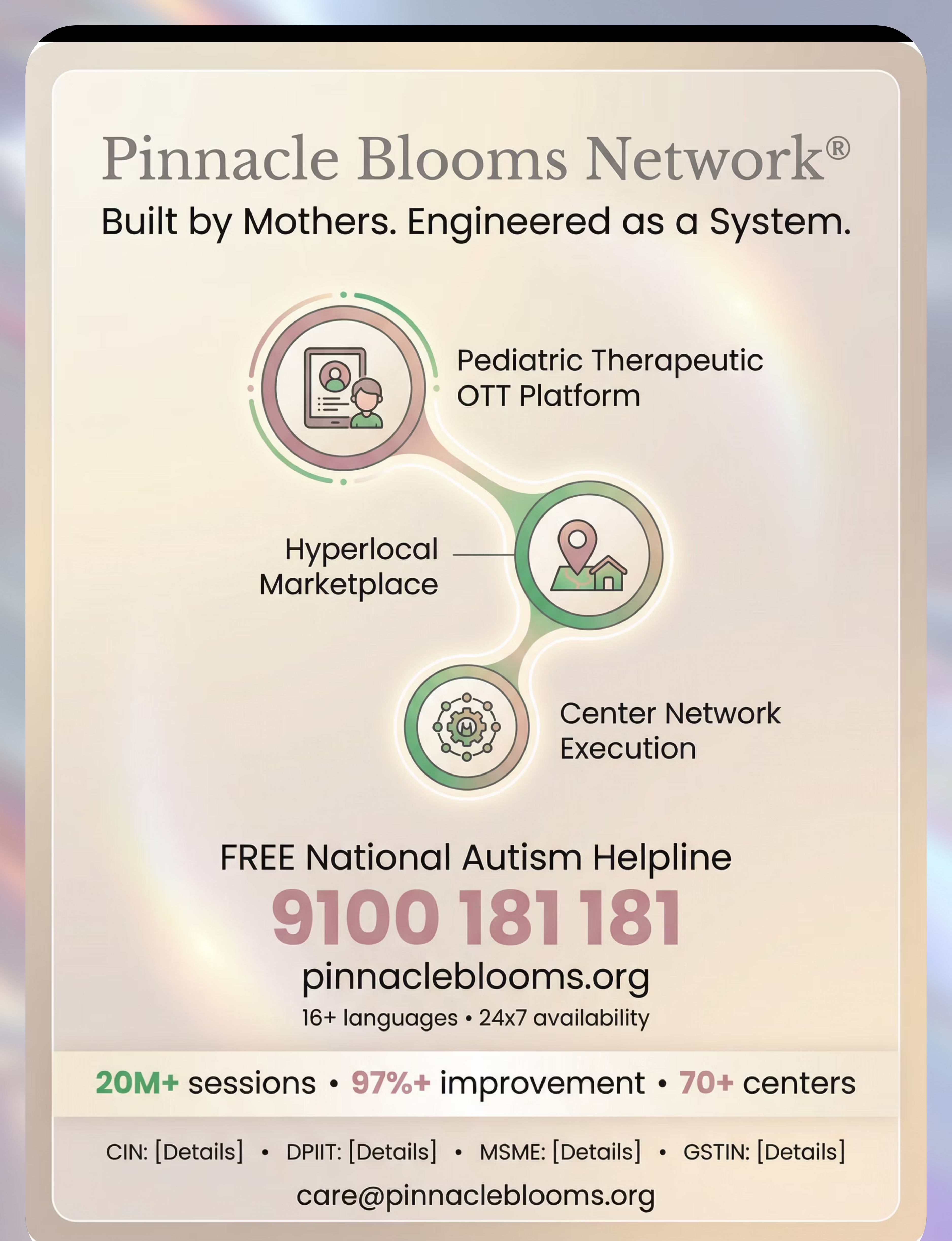
🏛️ Pinnacle Blooms Network® | OT • SLP • ABA • SpEd • NeuroDev • CRO
📍 70+ Centers | 20M+ Sessions | 97%+ Measured Improvement
📞 FREE Helpline: 9100 181 181
📍 70+ Centers | 20M+ Sessions | 97%+ Measured Improvement
📞 FREE Helpline: 9100 181 181

The Numbers Behind the Gagging
You are among millions of families navigating this exact mealtime challenge — in India and across 70+ countries. The gag reflex triggering on safe food textures is one of the most commonly reported feeding concerns in pediatric therapy clinics worldwide. Your child's response is neurologically predictable. And it is therapeutically addressable.
80%
ASD + Oral Sensory
of children diagnosed with ASD experience oral sensory processing difficulties (PRISMA Systematic Review, 2024 — PMC11506176)
1/37
Children in India
are on the autism spectrum (WHO Global Autism Prevalence Data + India HMIS 2023)
89%
Show Improvement
of children with texture-based feeding difficulties show measurable improvement with systematic oral desensitization therapy (Feeding Matters Clinical Outcome Data, 2023)
In a country where food is culture, where shared meals are love, where texture is embedded in every regional cuisine — a child stuck on purees faces not just nutritional limitation but social isolation. Pinnacle's 70+ center network has supported tens of thousands of Indian families through exactly this journey.
📞FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
Why Texture Triggers a Gag: The Neuroscience
The Neural Pathway
The gag reflex is governed by cranial nerve IX (glossopharyngeal) and X (vagus). In typical development, the gag reflex trigger point migrates posteriorly — from the front of the tongue in infancy to the back third by age 2–3. This migration is driven by oral sensory experience: touching, mouthing, and chewing a variety of textures.
In children with oral sensory over-responsivity, the somatosensory cortex amplifies texture signals 3–5× beyond typical thresholds. The thalamus interprets texture as threat-level input. The brainstem activates the gag reflex as a protective response — even when the food is completely safe to swallow.
The child is not choosing to gag. Their nervous system is doing exactly what it was designed to do — it is simply calibrated incorrectly for the texture level being presented.
What This Means for Your Family
Think of your child's mouth as a security alarm with the sensitivity dial turned up too high. The alarm goes off for a falling leaf when it should only go off for a fire. Every gag is the alarm triggering. The food is not dangerous — but the oral system has been trained to believe it is.
The goal of feeding therapy is not to override the alarm. It is to gradually recalibrate the sensitivity dial — so that textures register as "safe input" rather than "threat." This is done through systematic oral desensitization: introducing texture in carefully graduated steps, starting outside the mouth and moving inward, never forcing, always following the child's tolerance.
"This is a wiring calibration issue, not a behavioral choice. Your child cannot simply decide not to gag — any more than you can decide not to blink when something approaches your eye. The nervous system acts before conscious thought." — Pinnacle SLP-Feeding Consortium

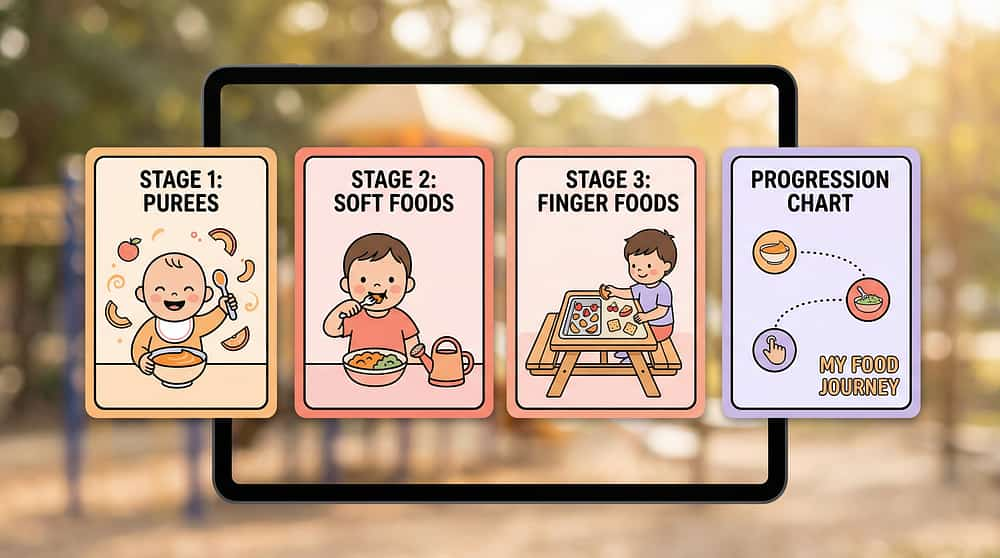
The Texture Development Timeline
4–8 Months
Thin liquids, smooth purees (Stage 1)
8–12 Months
Thick purees + soft lumps, mashed table foods, dissolvables
12–18 Months
Soft cubed foods, soft mixed textures in diverse settings
2–3 Years
Crunchy/chewy foods + soft pieces, meat, bread
3–5 Years
Complex mixed textures in all settings
← Gag reflex naturally migrates from front to back of tongue across this entire period →
A child gagging on textures past 12 months is showing signs that the natural gag reflex migration has been interrupted or delayed. This is not permanent — but it does require targeted intervention. Children with texture-based feeding difficulties frequently also experience tactile sensitivity, auditory sensitivity, delayed oral motor skills, anxiety around mealtimes, and broader sensory processing differences.
Your child is at a waypoint — not a destination. The oral system retains neuroplasticity across childhood. With systematic desensitization, the gag trigger point can be moved backward. The developmental pathway is open.
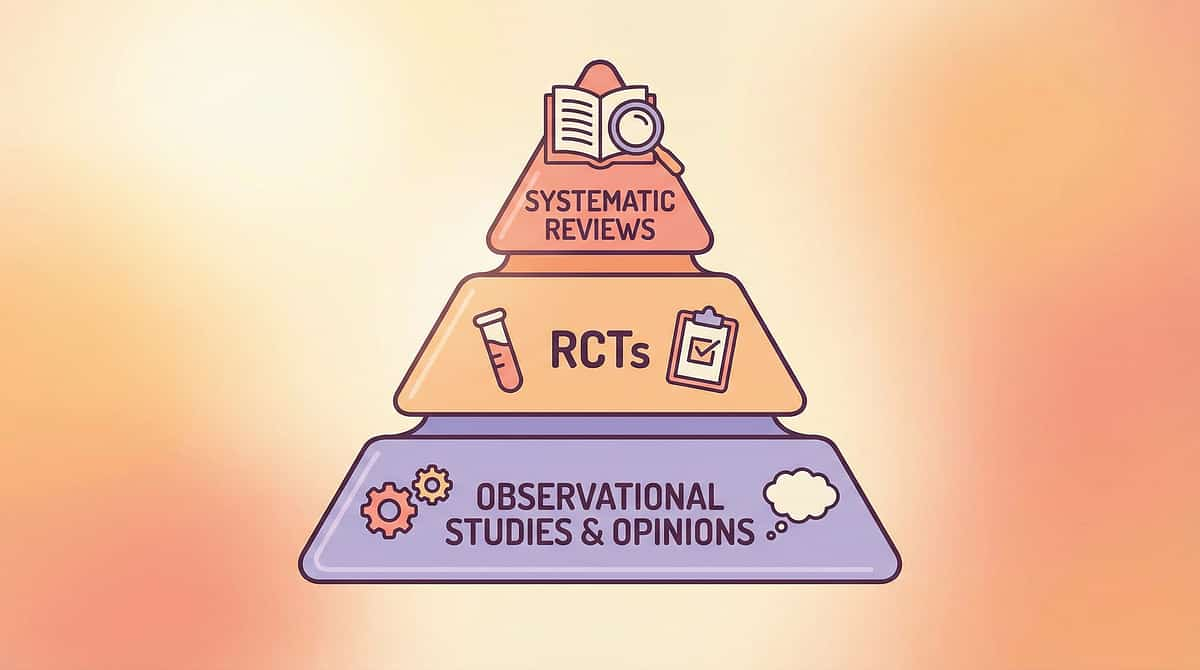
The Science Backing This Approach
Evidence Grade: Level I–II
Systematic Reviews + RCTs
16 studies | 2013–2023
87% Confidence Rating
16 studies | 2013–2023
87% Confidence Rating
Systematic oral desensitization using graduated texture exposure, oral motor tools, and sensory diet principles is classified as an evidence-based practice for children with ASD by the National Clearinghouse on Autism Evidence and Practice (NCAEP, 2020).
"Clinically validated. Home-applicable. Consortium-proven. This is the standard of care for texture-based feeding difficulties at Pinnacle's 70+ center network across India."
Key Studies
PRISMA Meta-Analysis (2024)
16 studies confirm sensory integration intervention meets evidence-based practice criteria in ASD. → PMC11506176
World J Clinical Cases (2024)
24 studies demonstrate SI therapy promotes adaptive behavior, sensory processing, and functional skills. → PMC10955541
Indian RCT (2019)
Home-based sensory interventions by trained parents showed significant outcomes in Indian pediatric populations. → DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Caregiver-administered interventions show population-level efficacy across 54 countries. → PMC9978394
The Technique
E-457 | Domain E: Oral Motor & Feeding
Oral Texture Desensitization Therapy
Parent-Friendly Name: "Teaching the Mouth That Textures Are Safe"
Oral Texture Desensitization Therapy is a systematic, graduated approach to helping a child's oral sensory system reduce its hypersensitive response to food textures. Beginning with non-food oral tools and progressing through a carefully sequenced texture hierarchy, this technique recalibrates the gag reflex trigger point, builds oral motor tolerance, and establishes positive associations with texture — enabling the child to advance from smooth purees toward age-appropriate foods. Implemented as part of a feeding therapy program guided by an SLP or OT, with consistent home carryover by parents.
Domain
Oral Motor & Feeding
Age Band
6 months – 10 years
Duration
10–20 min/session
Frequency
Daily (home) + 2–3×/week (therapy)
🎬 This technique is the deep-dive companion to: E-457: 9 Materials That Help With Gagging on Textures | Feeding & Mealtime Development in Children | Episode 457
🔗techniques.pinnacleblooms.org/oral-motor-feeding/gagging-on-textures-E457
🔗techniques.pinnacleblooms.org/oral-motor-feeding/gagging-on-textures-E457

The Consortium Behind This Technique
The brain does not organize by therapy type. A child's gag reflex is influenced by sensory processing, oral motor skills, learned fear responses, and medical history. Treating only one domain while ignoring others is why many families fail to see progress. Pinnacle's FusionModule™ integrates all five disciplines simultaneously.
Speech-Language Pathologist (Primary Lead)
Assesses the oral motor mechanism, identifies whether gagging is sensory, motor, structural, or behavioral in origin, and designs the desensitization hierarchy. Administers oral massage, vibration tools, and texture progression protocols.
Occupational Therapist
Addresses the broader sensory processing context. Evaluates the child's full sensory profile and ensures the oral sensory diet is integrated into whole-body regulation strategies — creating the regulated state that makes desensitization possible.
ABA / BCBA
Addresses anxiety, avoidance behaviors, and negative food associations. Applies systematic desensitization hierarchies, reinforcement of approach behaviors, and reduction of anticipatory anxiety responses.
Special Educator
Coordinates generalization to school settings — lunch environments, cafeterias, food-related classroom activities. Ensures feeding progress is maintained across environments.
Neurodevelopmental Paediatrician
Provides medical clearance, rules out structural causes (GERD, anatomical abnormalities, aspiration risk), and coordinates with gastroenterology or ENT if indicated. Medical factors must be addressed before behavioral/sensory intervention.

Precision Targets: What Changes and Why
Primary Target
Oral Sensory Over-Responsivity
Observable indicator: Child no longer gags when common food textures touch the front or middle of tongue. Gag trigger moves progressively posterior.
Observable indicator: Child no longer gags when common food textures touch the front or middle of tongue. Gag trigger moves progressively posterior.
Secondary Targets
- Mealtime anxiety reduction — child approaches meals without anticipatory distress
- Oral motor skill development — lateralizing tongue, developing chewing patterns
- Gag trigger repositioning — from anterior (front) to posterior (back third)
- Caregiver confidence — parent executes home protocol without anxiety
Tertiary Developmental Gains
- Nutritional variety — wider texture range expands dietary adequacy
- Social eating — child participates in family and peer meals
- Language development — oral motor patterns support articulation directly
- Sensory regulation — oral sensory diet creates regulated nervous system baseline
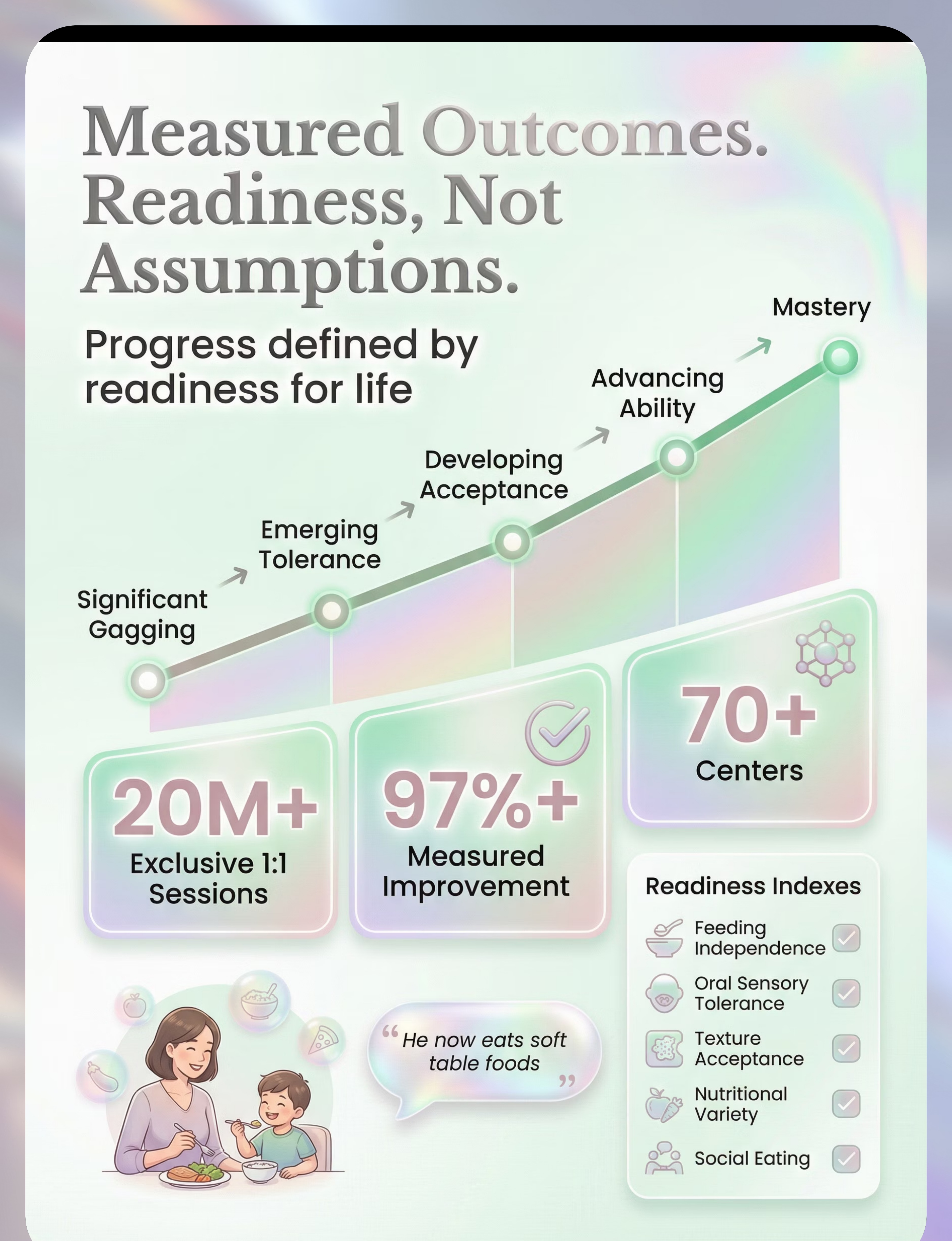
GPT-OS® Readiness Indexes Tracked
- Texture Acceptance Readiness Index
- Oral Sensory Tolerance Readiness Index
- Feeding Independence Readiness Index
- Nutritional Variety + Social Eating Readiness Index

9 Materials That Help With Gagging on Textures
Clinically specified by the Pinnacle Feeding Therapy Consortium. Each material addresses a specific layer of the desensitization pathway.

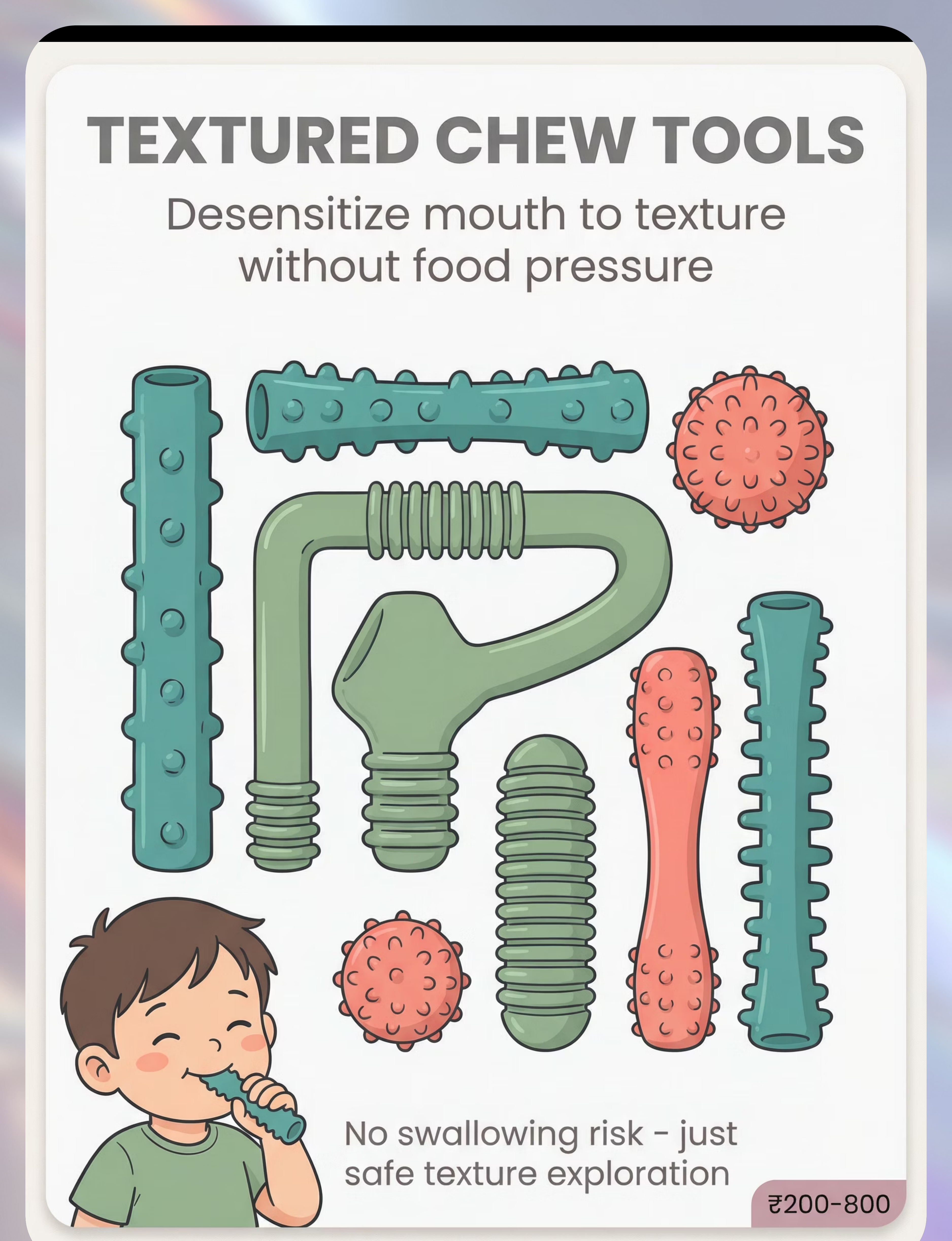
1. Textured Oral Sensory Chew Tools
Bumpy, ridged, nubby surfaces provide safe non-food texture input with zero swallowing risk. Regular use helps move the gag trigger point posteriorly. ₹200–800 | Search Amazon.in →
2. Vibrating Oral Motor Tool
Vibration provides organizing sensory input to the oral cavity. Used externally (lips, cheeks) then internally (gums, tongue) to reduce oral hypersensitivity before meals. ₹1,500–3,000 | Search Amazon.in →

3. Textured Feeding Spoons
Textured spoons with subtle bumps/ridges provide subliminal texture exposure with every bite of accepted smooth food — building tolerance without changing the food itself. ₹300–800 | Search Amazon.in →

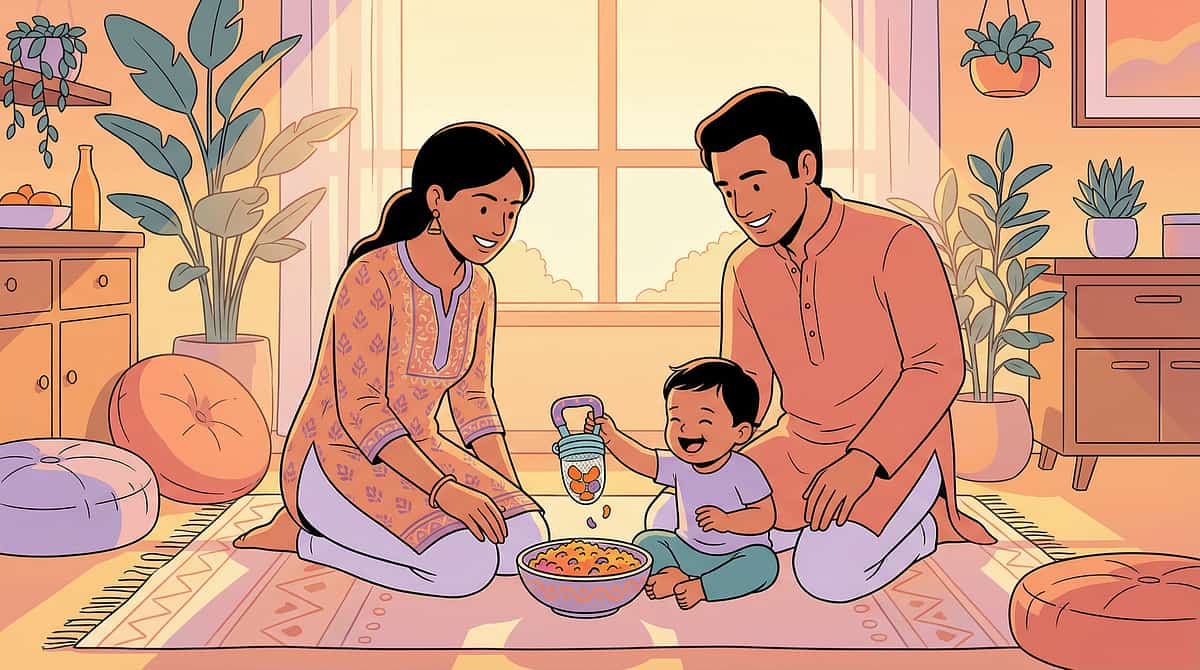
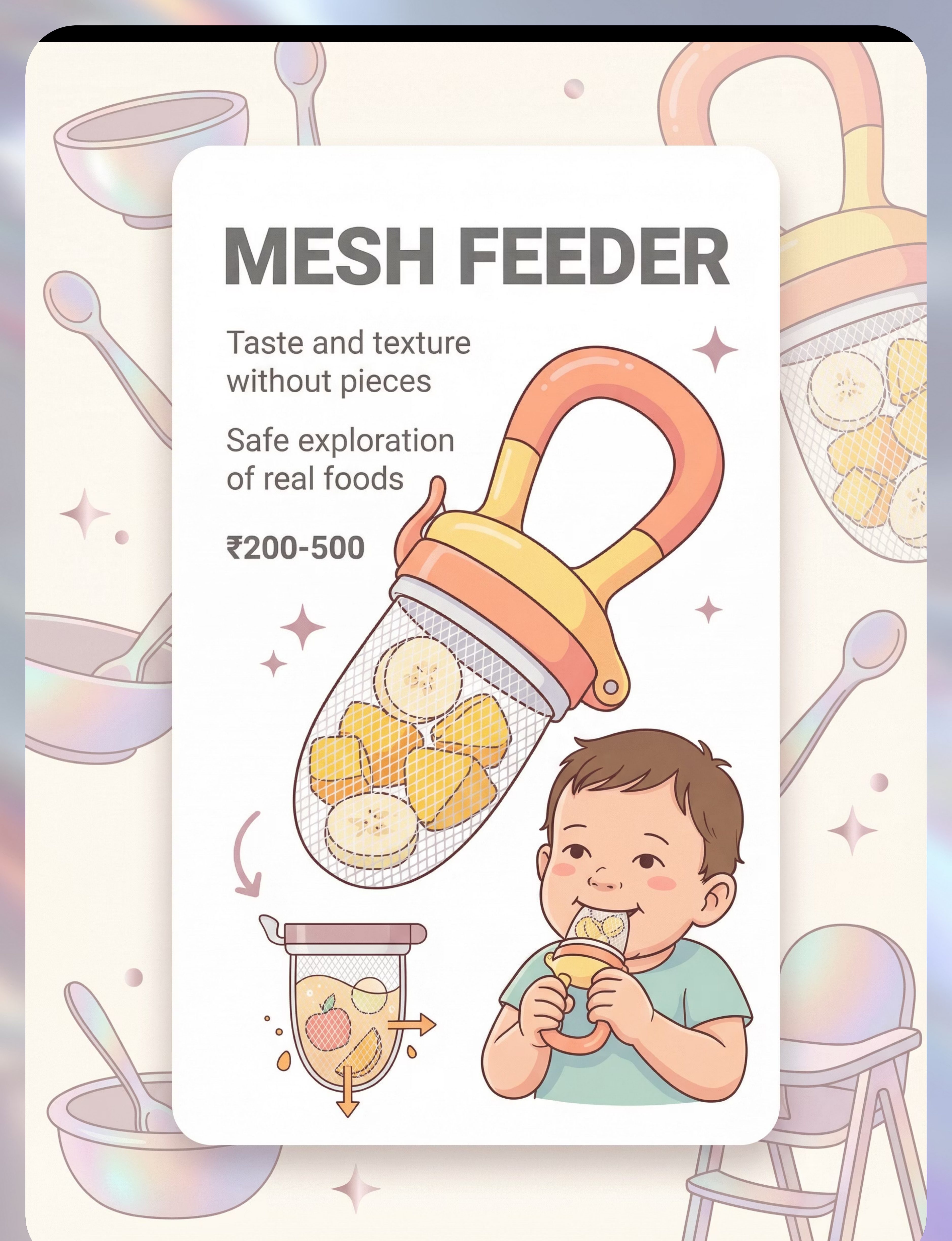
4. Mesh Feeder / Fresh Food Feeder
Allows children to experience the taste and texture sensation of real foods without the risk of pieces triggering gagging. A critical bridge between smooth purees and actual food textures. ₹200–500 | Buy on Amazon.in →

5. Dissolvable Puff Snacks
Dissolvable puffs look and feel like real food but dissolve with saliva — no chewing required. Often the first "real" texture children with significant gag responses can tolerate. Success here builds enormous confidence. ₹150–400 | Search Amazon.in →
Materials 6–9: Completing the Kit
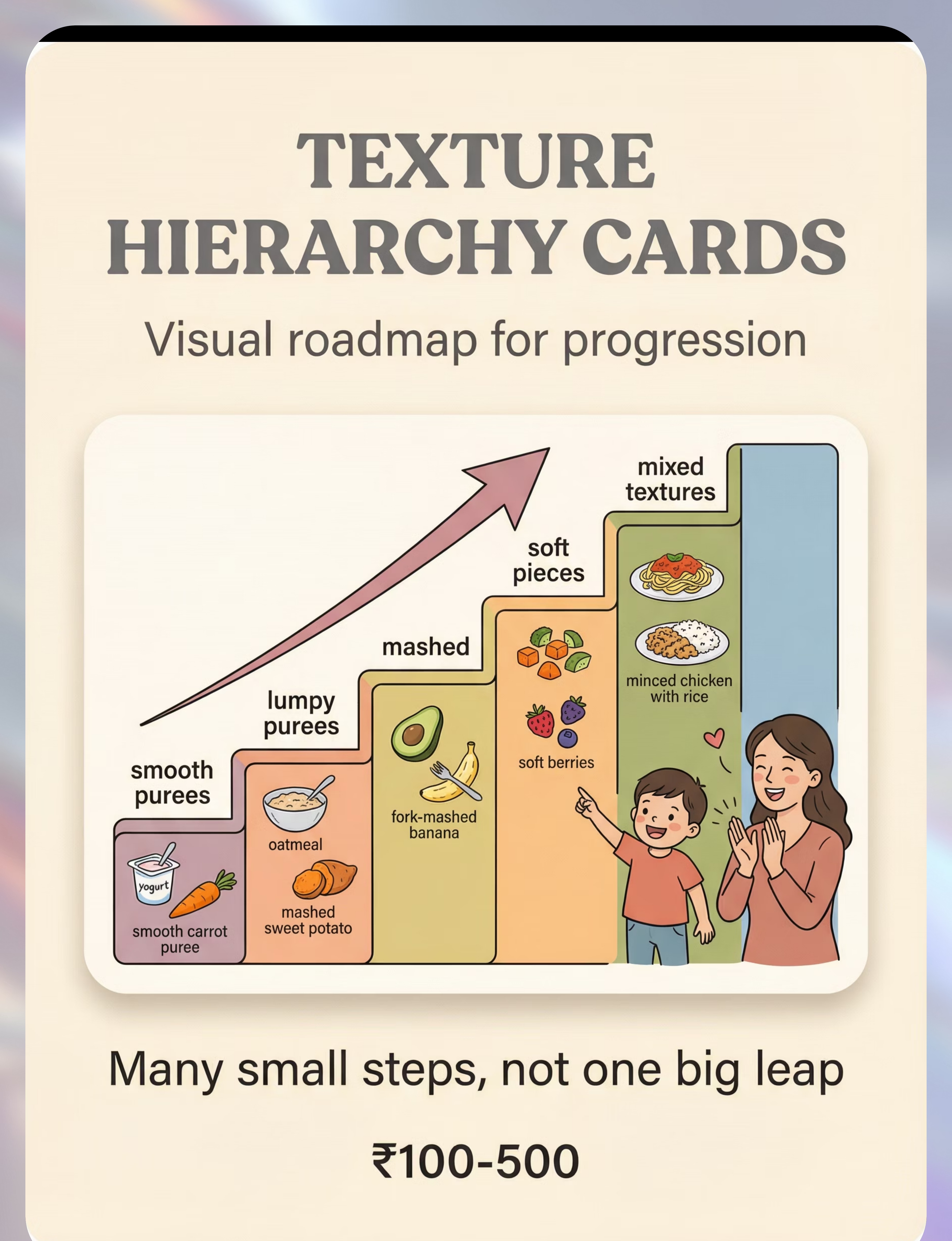
6. Texture Hierarchy Cards / Visual Guides
Visual roadmap showing parents and children exactly where they are, where they've been, and where they're going across 11 texture levels. Progress tracking reduces anxiety and celebrates incremental wins. ₹100–500 | Search Amazon.in → | 📥 Free printable at pinnacleblooms.org/resources

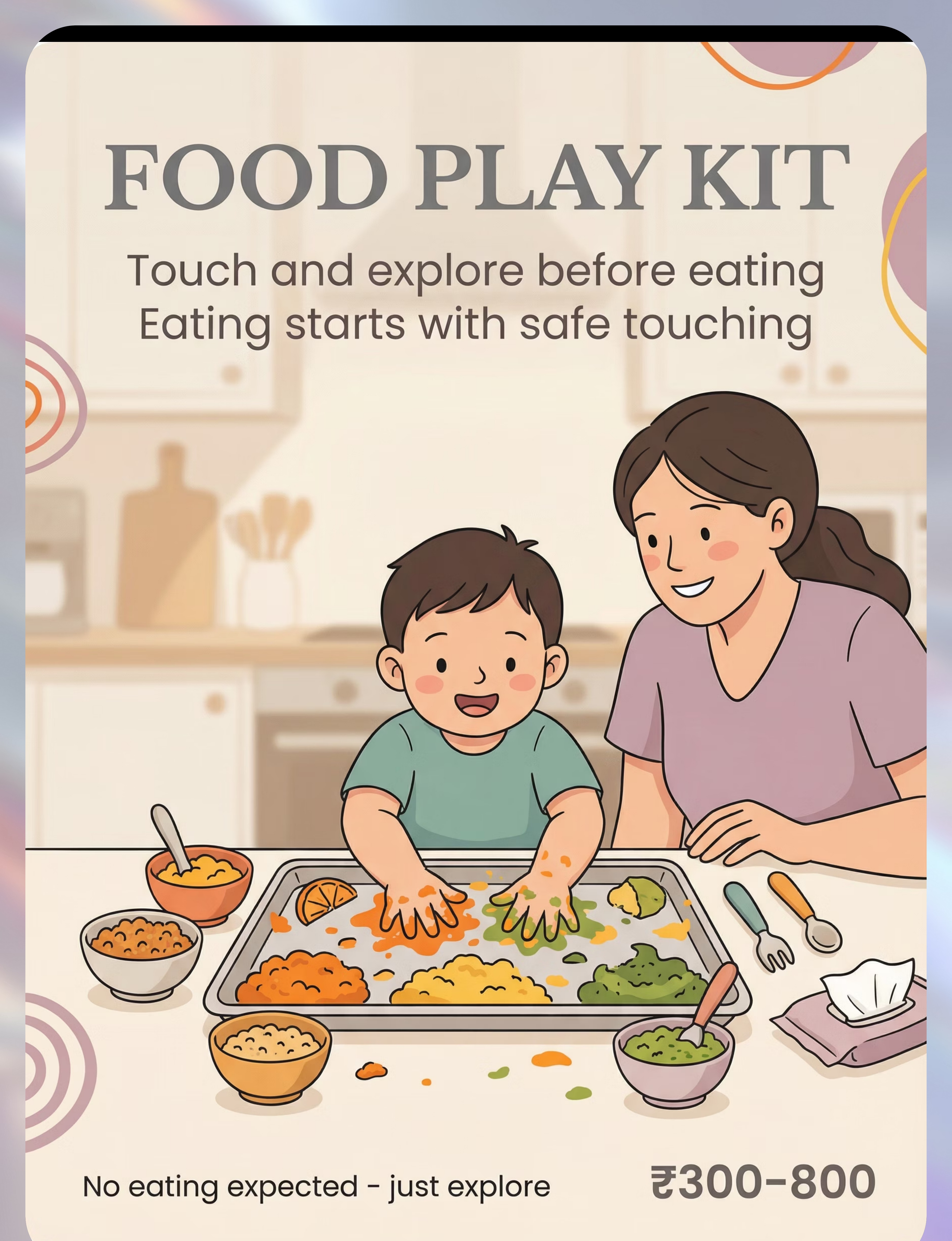
7. Food Play / Sensory Exploration Kit
A food play kit (large tray, small bowls, child utensils, wipes) enables mess-friendly texture exploration with zero eating expectation. Play is the first step on the exposure hierarchy — the journey to eating starts with safe touching. ₹300–800 | Search Amazon.in →

8. Oral Massage Tools (NUK / Finger Brush)
Gentle, firm pressure inside and outside the mouth via NUK brushes and finger brushes helps desensitize the oral cavity and move the gag reflex trigger point further back on the tongue. Used before meals as oral preparation. ₹200–600 | Search Amazon.in →⚠️ Professional guidance strongly recommended

9. Texture Progression Foods (Commercially Staged)
Commercially staged foods (Stage 1 → Stage 3) provide consistent, controlled textures the child can learn to trust. Unpredictable texture is anxiety-triggering — consistency is the foundation of texture acceptance. ₹200–1,000 | Search Amazon.in →
🏷️Total Starter Kit Investment: Essential starter ~₹700–1,600 (Chew tools + Puffs + Food play setup) | Full therapeutic kit ~₹3,000–7,000 | All materials clinically specified by the Pinnacle Feeding Therapy Consortium.

Zero-Cost Texture Therapy: Every Material Has a Household Substitute
WHO/UNICEF principle in action: Every family, regardless of economic access, can begin this intervention today with household items.
Material | Clinical Grade | Household Substitute | Why It Works | |
Chew Tools | Textured chew tubes ₹200–800 | Food-grade silicone toothbrush with textures; clean dry pasta pre-chewing practice | Same textured surface principle — oral sensory input without food | |
Vibrating Tool | Z-Vibe ₹1,500–3,000 | Electric toothbrush (child-safe, soft bristle) used externally on cheeks/lips | Vibration input achieves same normalization effect | |
Textured Spoon | Maroon therapy spoon ₹300–800 | Silicone baby spoon with small bumps/texture pattern | Subliminal texture exposure on every accepted bite | |
Mesh Feeder | Commercial mesh feeder ₹200–500 | Clean muslin cloth tied around soft fruit piece | Same barrier principle — taste/texture without pieces | |
Dissolvable Puffs | Commercial baby puffs ₹150–400 | Thin rice crackers that dissolve quickly; roti crisped and soaked to dissolve point | Identical dissolution mechanism | |
Texture Cards | Printed hierarchy ₹100–500 | Hand-drawn staircase chart with food photos at each level | Same visual progression map | |
Food Play Kit | Commercial kit ₹300–800 | Large steel thali/baking tray + steel katoris + kitchen spoons | Same exploration container concept | |
Oral Massage | NUK brush ₹200–600 | Clean finger wrapped in soft washcloth; gentle firm pressure | Fingertip pressure achieves same desensitization | |
Staged Foods | Commercial ₹200–1,000 | Home-blended stages: smooth → add tiny soft pieces → mash → soft cubes | Controlled texture achievable at home with planning |
Non-Negotiable Clinical Grades: When a child has significant aspiration risk, medical feeding history, or severe gagging leading to vomiting — professional-grade oral tools and SLP supervision are essential safety requirements and are not substitutable.
Safety Gate — Read Before Every Session
🔴 Red Light — Do Not Proceed
- Child has history of aspiration or choking episodes
- Child is losing weight or failing to grow
- Child vomits more than 2–3 times per week related to feeding
- Child has diagnosed/suspected GERD that is not controlled
- Child has had NG tube, G-tube, or extended NICU stay
- Child has breathing difficulties during or after feeding
- Gagging leads consistently to vomiting and significant distress
🟡 Amber Light — Modify Session
- Child has not been assessed by a feeding therapist
- Gagging is so severe it prevents any oral intake
- Child shows extreme anticipatory anxiety before food
- Other sensory sensitivities are extreme and unmanaged
- Child is younger than 6 months
🟢 Green Light — Proceed
- Child has had feeding evaluation and medical clearance
- Gagging is texture-specific (not present with all foods)
- Child can eat some foods safely
- You are following guidance from your child's feeding therapist
- Session is low-demand, child-paced, and non-forceful
Absolute Stop Signs During Session:🛑 Child becomes intensely distressed | 🛑 Gagging leads to vomiting | 🛑 Signs of choking or airway compromise | 🛑 Child's skin color changes | 🛑 Child becomes completely dysregulated
📞9100 181 181 — Pinnacle FREE National Helpline for immediate guidance | 🏥 Nearest Pinnacle center: pinnacleblooms.org/centers

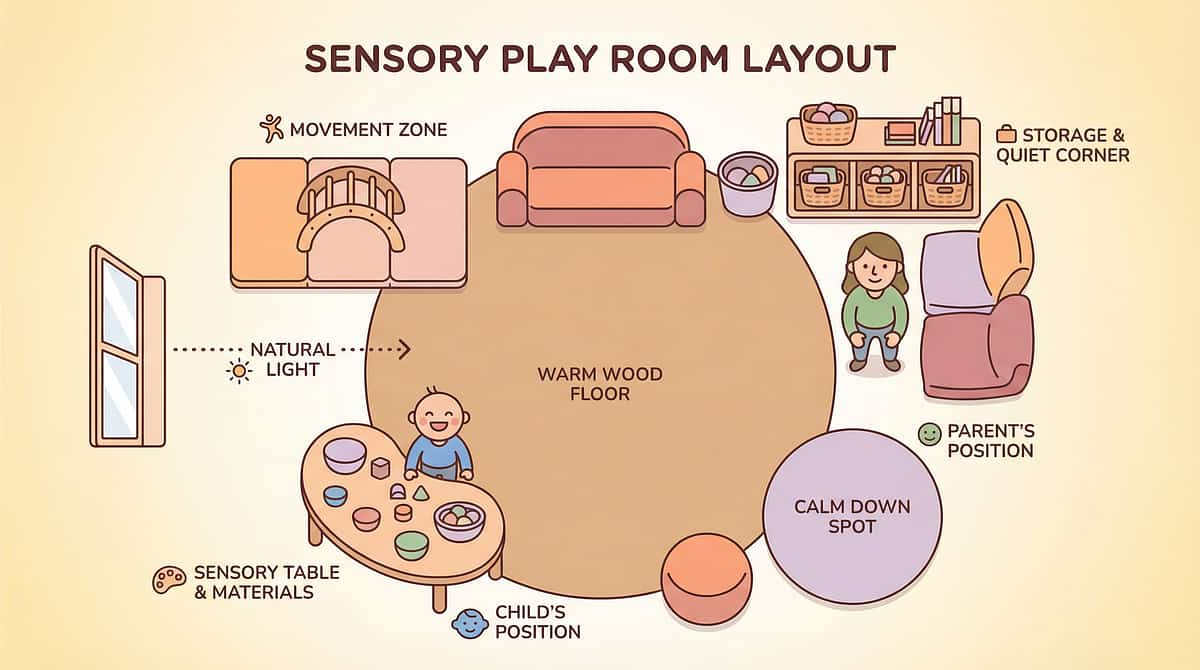
The Texture Therapy Space Setup

Child Positioning: High chair or adapted seat. Feet flat on footrest (90-90-90: hips-knees-ankles). Upright — never reclined for texture work. This is a safety and sensory regulation requirement.
Lighting: Warm, consistent natural light or warm LED. Avoid harsh overhead fluorescent lighting, which increases sensory stress baseline.
Sound: Quiet, or very soft familiar background music. No TV, no competing noise. The child needs to focus on oral sensation.
Setup Checklist
- Left side of table: Pre-session oral tools (chew tool, vibrating tool, massage brush)
- Right side: Session materials (today's food play setup OR next texture level)
- Behind child: Food play tray (for later in session)
- Nearby: Wipes — normalize mess cleanup
- Remove: TV, tablets, busy toys, strong food smells, distracting siblings, pets
Session Timing
Not immediately after a stressful activity. Not when child is overtired or unwell. Best sessions occur when the child is regulated and alert — approximately 1–2 hours after waking, or 1 hour before peak tiredness.
Temperature: Room comfortable — extreme heat or cold changes sensory reactivity.

Pre-Session Readiness Check (60 Seconds)
Run through this check before every session. It takes 60 seconds and determines whether you have a full session, a modified session, or a rest day.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Child is fed (not hungry, not overfull) | Yes | Slightly hungry | Hungry or very full | |
Child has rested adequately | Rested | Mildly tired | Overtired | |
No meltdown in last 30 minutes | No recent | 30+ min ago | Recent meltdown | |
No signs of illness | None | Mild cold, stable | Fever/acute illness | |
Child is in regulated state | Calm/alert | Slightly elevated | Dysregulated | |
Environment is set up correctly | Ready | Minor adjustments | Needs full reset | |
Parent is calm and confident | Yes | Slightly anxious | Very anxious |
All Green → Full Session
Proceed with complete protocol. Child and environment are optimally ready.
Any Amber → Modified Session
Shortened version: oral tool warm-up only (no food). 5 minutes. Maintain positive ending. Note which indicator was amber.
Any Red → Postpone Today
Alternative calming activity: proprioceptive input, preferred sensory activity. No feeding session today. This is data-informed decision making.
"The best session is one that starts right. A 5-minute session that ends positively is worth infinitely more than a 20-minute session that ends in gagging and tears."

Step 01 of 06
Step 1: The Invitation — The Session Begins Here
The Exact Opening Script
"[Child's name], want to play with our special tools? Come see what I have."
Do NOT say: "Today we're going to eat." | "You have to try this." | "Just taste it."
This is an invitation, never a command. The child must feel they are choosing to engage. Choice is the foundation of feeding therapy — forced feeding creates lasting aversion.
Body Language Guidance
- Get to child's eye level
- Relaxed, open posture — not leaning in intensely
- Genuine smile, not strained
- Breathe slowly and evenly (children mirror parent's regulation state)
Reading the Child's Response
What acceptance looks like:
- Child moves toward you or the materials
- Child makes eye contact or reaches for tools
- Child's body is open (not hunched, not turned away)
- Child makes positive vocalizations
What resistance looks like — and how to respond:
- Child moves away → Reduce demand: "Just look. You don't have to touch."
- Child shows distress → Return to preferred activity. End positively.
- Child ignores → Try preferred sensory input first to increase engagement, then re-invite.
⏱️Timing: 30–60 seconds for the invitation phase
Step 02 of 06
Step 2: Oral Tool Warm-Up — Pre-Feeding Preparation
Before any food texture is introduced, the mouth needs to be prepared. This 3–5 minute oral warm-up is the foundation of every session.
Material Introduction Script
"Look — this tool has bumpy texture. Let's see what it feels like on your cheek. Like a little massage."
Critical Rule
If child shows any significant resistance at any phase, return to the previous phase immediately. Never proceed to a phase the child is not comfortable with.
Child Response Indicators
- Engagement: Child leans in, opens mouth, touches tool voluntarily
- Tolerance: Child allows contact without significant distress (mild initial resistance is normal)
- Avoidance: Child turns away, pushes tool, shows distress → Reduce intensity immediately
Reinforcement Cue: The moment the child tolerates ANY oral tool contact: immediate warm verbal praise within 3 seconds. "You did it! That was brave!"
⏱️Timing: 3–5 minutes total

Step 03 of 06
Step 3: The Texture Exposure — The Therapeutic Core
This is the active ingredient. What happens in this step determines progress. Choose the appropriate level for your child today.
Level 1 — Food Play Only
Place small amount of textured food on tray. Demonstrate touching it yourself. Invite child to touch with one finger: "Can you give it a poke?" Celebrate ANY touching. No eating expectation.
Level 2 — Mesh Feeder Exploration
Place soft fruit in mesh feeder. Child sucks/mouths the mesh experiencing texture safely. No pieces, no gagging risk. Celebrate any mouthing.
Level 3 — Dissolvable Puffs
Place one puff on table. Child may look, touch, lick — in any order. Do NOT place in child's mouth. Celebrate every step toward the mouth.
Level 4 — Smooth Food + Textured Spoon
Child's accepted smooth food served with textured feeding spoon. Over many meals, oral system adapts to the spoon's subliminal texture exposure without any change to the food itself.
Common Errors to Avoid:❌ Placing food in child's mouth without consent ❌ Continuing when child shows clear refusal ❌ Commenting negatively on gagging ("Oh no, don't gag!") ❌ Showing your own anxiety ❌ Rushing to higher levels before consolidating current level
⏱️Timing: Core action occupies 5–10 minutes of a 15–20 minute session
⏱️Timing: Core action occupies 5–10 minutes of a 15–20 minute session

Step 04 of 06
Step 4: Dosage — How Much Is Enough?
3 high-quality, positive repetitions at a child's genuine tolerance level are worth more than 15 forced, distressed repetitions. Quantity without quality does not build neural tolerance — it builds fear.
Target Repetitions by Level
- Oral tool warm-up: 2–3 repetitions of full face-to-mouth sequence
- Food play touches: 3–5 voluntary touches of today's texture
- Mesh feeder: 2–3 mouthing episodes, each 10–30 seconds
- Dissolvable exploration: 3–5 contact opportunities (look, touch, lick, bite)
Variation Options to Maintain Engagement
- Change the tool (bumpy → ridged → smooth chew tool)
- Change the food in the mesh feeder (banana → mango → melon)
- Change your script ("Try it on your nose!" creates laughter — laughter reduces tension)
- Change the game (poking vs. squishing vs. drawing patterns in food)
Satiation Indicators
The child has had enough for today when:
- Child becomes distracted and disengaged (not distressed — just done)
- Child pushes materials away gently
- Child gets up or turns to leave
- Session has reached 15–20 minutes
Satiation ≠ Failure
A child's satiation point is information. Record it. Over weeks, the satiation point will extend as comfort increases. This is progress data, not disappointment.
Sensory integration therapy: 2–3 sessions/week for 8–12 weeks is the typical professional protocol.

Step 05 of 06
Step 5: Reinforce the Brave Mouth
Every attempt at texture engagement — however small — deserves immediate, specific, enthusiastic reinforcement. Not "good job" (vague). Specific: "You TOUCHED the bumpy food! That was SO brave!"
Timing is everything: Within 3 seconds of the desired behavior. Immediate reinforcement links the texture exposure to the positive experience at the neural level.
For Touching a Texture
"You touched it! Your brave hand touched the bumpy food!"
For Mouthing the Mesh Feeder
"Your mouth tried the texture! That was amazing!"
For Licking a Dissolvable
"You licked it! Your tongue is so brave!"
For Tolerating Oral Tool
"Your mouth is getting so strong and brave!"
Reinforcement Menu
- Social: Clapping, spinning, high-five, chase game (10 seconds)
- Tangible: Sticker on chart, small preferred item
- Activity: 30 seconds of favorite screen, song, jump on trampoline
- Sensory: Preferred sensory input (squeeze, swing, deep pressure)
Token Economy
Each successful texture engagement earns a token/sticker. Accumulate 5 tokens → access preferred reward. Visual token board makes the system concrete and predictable.
Celebrate the Attempt, Not Just the Success: A child who tried and gagged still made a brave attempt. "You tried! That was so brave. We'll try again another day."
Step 06 of 06
Step 6: The Cool-Down — End Well Every Time
Why the Cool-Down Matters
The last 2 minutes of a session determine how the child feels about the next session. A session that ends abruptly can create anxiety about beginning the next one. A session that ends predictably and positively creates anticipatory comfort.
Transition Warning Script
"Two more, and we're all done with texture time."
Then 1 minute: "One more, and then we clean up."
30-second warning: "Almost done — last one!"
Then 1 minute: "One more, and then we clean up."
30-second warning: "Almost done — last one!"
Closing Script
"We're done with texture time. You were so brave today. What should we do now?"
(Give choice of 2 preferred activities)
Cool-Down Activity Options (1–2 minutes)
- Preferred calming sensory input (deep pressure, proprioceptive input)
- Simple put-away ritual: child places tools back in their container
- Short preferred song or rhyme
- Transition object: "Now it's time for [preferred next activity]."
The Put-Away Ritual
Having the child participate in cleaning up (wiping the tray, putting the chew tool in its case, stacking the bowls) provides session closure, proprioceptive input (calming), builds a sense of agency and competence, and creates a predictable ending ritual.
Visual Timer
Use a visual timer throughout the session so the child can see time remaining. Predictability dramatically reduces resistance. 🛒Visual Timer — Amazon.in

60 Seconds of Data Right Now → Months of Progress Insight Later
Do this within 60 seconds of ending the session. The data is most accurate right now.
Field 1: Highest Level Reached Today
Level 1: Food play/touching | Level 2: Mesh feeder | Level 3: Dissolvables | Level 4: Textured spoon with accepted food | Level 5: New texture in mouth
Field 2: Gag Episodes
Number of gag episodes during session: ___
Triggered by: ___________________
Triggered by: ___________________
Field 3: Child's State Rating (1–5)
1 = Highly distressed | 2 = Moderately distressed | 3 = Neutral | 4 = Calm and tolerating | 5 = Engaged and enjoying
What This Data Reveals Over Time
- Trend in highest level reached (should increase over weeks)
- Gag count trending (should decrease over weeks)
- State rating trending (should increase)
- Day/time/environment patterns in best vs. hardest sessions
- Data that guides your therapist's protocol adjustments
📥unknown link
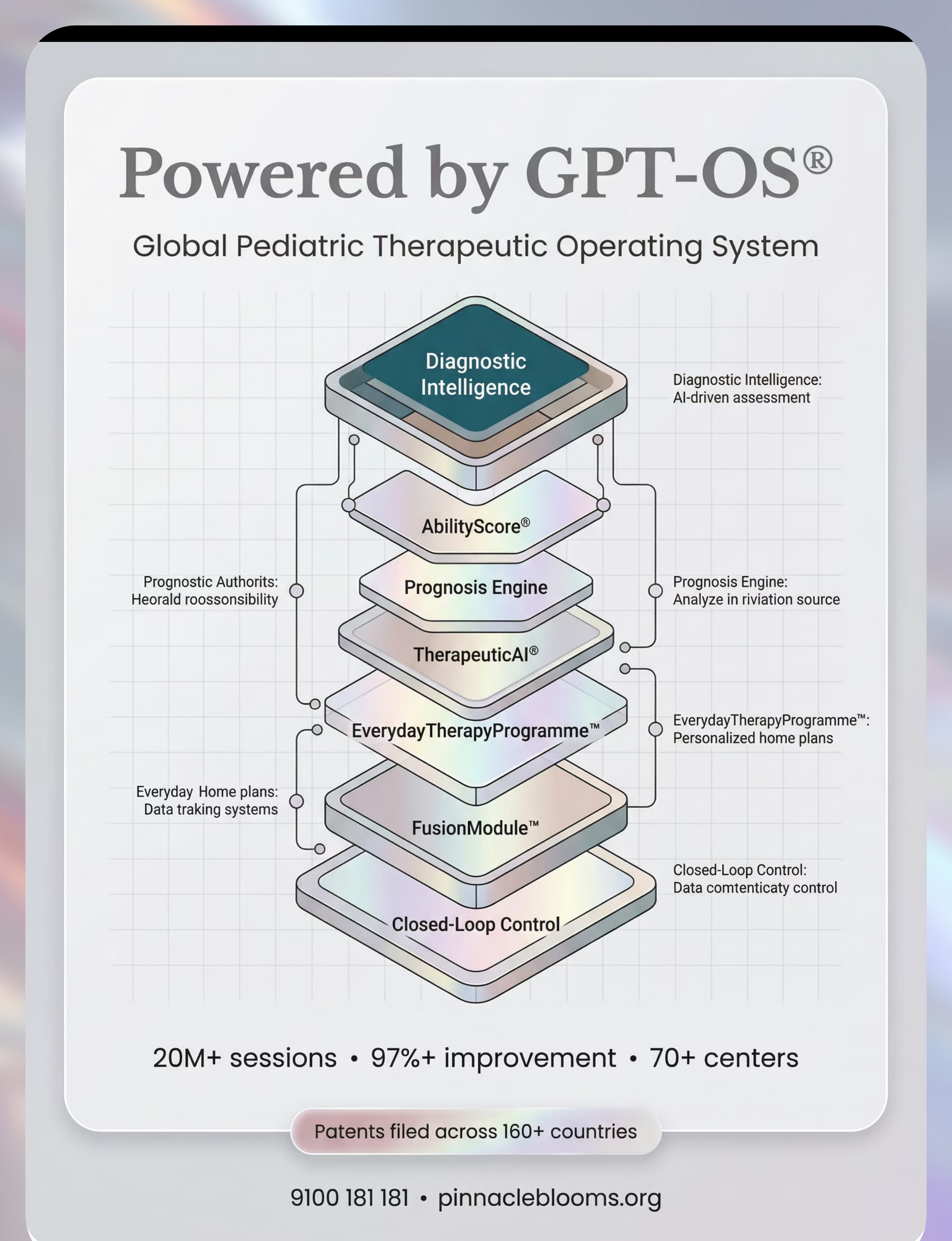
GPT-OS® In-App Tracker
If using the Pinnacle GPT-OS® platform, navigate to EverydayTherapyProgramme™ → Session Log → E-457. The app timestamps, sequences, and surfaces patterns automatically — routing your data to the TherapeuticAI® dashboard for personalized recommendations.
Real Sessions, Real Challenges — Solutions for Each
Session abandonment is not failure. It is data. Every imperfect session teaches you something that makes the next one better.
❓ Child gagged on the first texture attempt today
What happened: The texture level was too advanced, or the oral warm-up was insufficient. The warm-up is non-negotiable.
Next time: Double the oral warm-up time. Reduce texture level by one step. Celebrate that the session happened at all.
Next time: Double the oral warm-up time. Reduce texture level by one step. Celebrate that the session happened at all.
❓ Child refused to touch the oral tools at all
What happened: Oral hypersensitivity extends to tools, not just food. The oral system is in a highly defensive state.
Next time: Start with external face touch (cheeks, not mouth). Use preferred comfort toy as intermediary. May need vibration externally first. Consult SLP.
Next time: Start with external face touch (cheeks, not mouth). Use preferred comfort toy as intermediary. May need vibration externally first. Consult SLP.
❓ Child ate fine for two days then gagged again today
What happened: This is completely normal — progress is not linear. Factors like sleep, illness, stress, or environmental change affect sensory thresholds.
Next time: Return to the last successful level. One bad day does not erase previous progress. Track triggers in data.
Next time: Return to the last successful level. One bad day does not erase previous progress. Track triggers in data.
❓ Zero progress toward higher levels for weeks
What happened: The progression pace needs professional recalibration. Some children have a narrower tolerance window and need clinic-level intensity.
Next time: Book a feeding therapy session review. GPT-OS® data will show the plateau to your therapist.
Next time: Book a feeding therapy session review. GPT-OS® data will show the plateau to your therapist.
❓ Child gags when they even SEE textured food
What happened: Anticipatory gagging — a conditioned fear response. Months of gagging experiences have created a sight-triggered anxiety response.
Next time: Visual exposure hierarchy first: food in the room → food on the table → food on the plate. Textures are not touched at this stage. This can take weeks.
Next time: Visual exposure hierarchy first: food in the room → food on the table → food on the plate. Textures are not touched at this stage. This can take weeks.
❓ Parent became anxious and the session deteriorated
What happened: Child mirrored parent's anxiety state and dysregulated. Parent stress is a direct antecedent to child resistance.
Next time: Parent regulation first. 3 deep breaths before entering the feeding space. Your calm is the child's permission to feel safe.
Next time: Parent regulation first. 3 deep breaths before entering the feeding space. Your calm is the child's permission to feel safe.
Every Child Is Different — Personalize the Protocol
For Bad Days — Reduce Demand
- Oral warm-up only — no food in the room
- Child's preferred sensory input first (5 minutes)
- Parent and child sit at table together with preferred food — no texture work
- Make it a "just play" session — no progression expectations
For Breakthrough Days — Child Is Regulated
- Extend the session by 5 minutes (not more)
- Try introducing the next level's material (introduce, don't demand)
- Celebrate extensively and document everything
Sensory Seeker Profile
If child seeks oral sensory input (mouths objects): Use firmer, more intense textures on chew tools. Begin with strongly flavored dissolvables. Food play with interesting textures (slime-like foods) may be more engaging.
Sensory Avoider Profile
If child pulls away from all oral contact: Begin exclusively external. Use preferred temperature. Keep sessions shorter (5–7 minutes initially). More repetitions at each level before moving on.
Age-Based Modifications
- 6–18 months: Oral tool exploration and mesh feeders only
- 18 months–3 years: Add food play and dissolvable puffs
- 3–6 years: Full protocol; add texture hierarchy cards and visual tracking
- 6–10 years: Child can participate in planning — "Which texture do you want to try today?"
Week 1–2: The First Signs of Change
15%
Early Progress
Week 1–2 benchmark — foundational tolerance forming
✅ Child tolerates oral warm-up 30 seconds longer than Week 1
This is measurable neural adaptation. Celebrate it.
✅ Child approaches the food play tray without immediate refusal
The approach itself is progress — before Week 1, they may have refused to be near the tray at all.
✅ Gag count in sessions is decreasing (even by 1–2 episodes)
Fewer gags = the threshold is moving. This is the primary metric.
✅ Child's state rating is 3+ more frequently
Neutral tolerance is the bridge to active engagement. It comes before enjoyment.
"If your child tolerates the oral warm-up for 5 seconds longer than they did last week — that is real, measurable, clinically meaningful progress. The neural pathway is forming. You may not see it yet. It is happening."

Week 3–4: Neural Pathways Are Forming
40%
Consolidation Phase
Week 3–4 benchmark — first desensitization tier consolidating
🔵 Child Anticipates the Routine
They remember the sequence: face massage → oral tool → food play. The predictability itself is calming their nervous system before texture contact.
🔵 Oral Tool Contact Accepted Consistently
This is the key consolidation sign. Acceptance across 3–4 consecutive days means the first desensitization tier is consolidating.
🔵 Food Play Duration Increasing
Child is spending longer touching/exploring textured foods before reaching their tolerance limit. The exposure window is widening.
🔵 Spontaneous Approach Outside Sessions
Child picks up the chew tool or mesh feeder independently, outside scheduled session time. This is generalization beginning.
You may notice that you are now more confident facilitating sessions. You're reading your child's tolerance signals accurately. You're adjusting in real time. This is a clinical skill — and you are learning it.
Week 5–8: Mastery Is Within Reach
75%
Mastery Phase
Week 5–8 benchmark — Tier 1 foundation being achieved
Oral Tool Acceptance
Child accepts full face-to-mouth oral warm-up sequence daily with no significant distress — for 5 consecutive sessions.
Food Play Mastery
Child initiates touching textured foods spontaneously during food play sessions.
Dissolvable Mastery
Child eats dissolvable puffs from the plate for 3 consecutive sessions.
Gag Threshold Moved
Gag episodes per session consistently 0–1 (down from multiple gags at session start).
Generalization Beginning
Skill appearing in at least one other context (different caregiver, different room).
🏆TIER 1 MASTERY UNLOCKED: Oral Desensitization Foundation | E-457 | Pinnacle GPT-OS® | Texture Acceptance: EMERGING
Mastery here means the oral sensory system's baseline sensitivity has reduced enough to begin actual food texture progression. Tiers 2–4 build the texture hierarchy on top of this foundation.
Mastery here means the oral sensory system's baseline sensitivity has reduced enough to begin actual food texture progression. Tiers 2–4 build the texture hierarchy on top of this foundation.

You Did This. Stop and Feel This.
This card is for you, the parent. The therapist. The grandmother who sat through a hundred sessions. The person who showed up, every day, even when it felt impossible.
Your child can now touch textured food. Their mouth accepts input that once triggered an immediate gag. You sat with the mess, the anxiety, the setbacks, the sessions that didn't go well — and you kept coming back. This is not a small thing. For a child whose nervous system was telling them that all texture was danger — this is a profound neurological shift. You made this happen.
Family Celebration Suggestions
- Take a family photo with the texture tools
- Create a "brave mouth" journal entry
- Let the child choose their celebration meal — even if it's all smooth foods, that's okay
- This achievement deserves marking
Journal Prompt
Write one paragraph about the change you've seen in the last 6–8 weeks. Date it. Read it on the hard days ahead. Progress is rarely linear but the trend line is real.
Share Your Journey
Your experience is not just yours. The parent who sees your story may start the protocol they've been delaying for months. Consider sharing your journey. Every texture story shared is a family helped.
Tag: @PinnacleBloomsNetwork
#BraveMouth | #TextureJourney | #PinnacleGPTOS
#BraveMouth | #TextureJourney | #PinnacleGPTOS

Clinical Safety Guardrails — Know When to Pause
Even in the celebration zone, these signs mean: pause, consult, and get professional guidance before continuing.
🚨 Red Flag | What It Looks Like | Action | |
Gagging leading to vomiting is INCREASING despite 4+ weeks of protocol | More vomiting episodes than Week 1 | SLP + GI evaluation urgently | |
Child is losing weight or growth slowing | Weight curve flattening | Paediatric nutrition + feeding therapy urgent review | |
Child develops new avoidance behaviors beyond textures | Refusing all eating, hiding food, extreme mealtime anxiety | Behavioral + feeding specialist assessment | |
Child gags on foods they previously tolerated | Regression on safe foods | Medical evaluation (GERD, aspiration, illness) | |
Child becomes significantly more distressed with each session | Sessions getting harder, not easier | SLP reassessment of protocol | |
Any choking, change in breathing, or aspiration signs | Coughing, wet/gurgly voice after eating | IMMEDIATE medical evaluation |
Tier 1 Support
📞FREE Helpline 9100 181 181
Initial guidance and triage | 24×7
Initial guidance and triage | 24×7
Tier 2 Support
🖥️ Teleconsultation with Pinnacle SLP-Feeding Specialist — same-day available
Tier 3 Support
🏥 In-center assessment at nearest Pinnacle center — pinnacleblooms.org/centers
Your Child's Texture Development Roadmap
Texture Hierarchy — 11 Levels
Thin Liquids
Smooth Purees
Thick Purees
Purees with Soft Lumps
Mashed Foods
Soft Dissolvables ← Most E-457 Children Working Here
"This technique is one essential station on a longer journey. Mastering E-457 opens the pathway to E-458 (chewing), to dietary variety, to social eating, to nutritional independence. Each technique builds the neural foundation for the next."
Other Techniques in the Feeding & Mealtime Domain
Browse the full feeding library — find techniques that work with materials you already own.
Technique | Code | Canon Materials | Link | |
Refusing New Foods | E-455 | Food Exploration Tools | ||
Limited Diet / Food Selectivity | E-456 | Food Exploration Tools + Visual Supports | ||
Gagging on Textures | E-457 | Oral Motor Chews + Food Exploration | YOU ARE HERE | |
Chewing Development | E-458 | Oral Motor Chews + Chewable Tools | ||
Swallowing Difficulties | E-459 | Oral Motor Tools + Positioning | ||
Oral Sensory Seeking During Meals | E-465 | Oral Motor Chews + Sensory Tools |
Materials You Already Own: If you purchased the E-457 kit, you already have materials for ✓ E-458 (same oral motor chew tools) ✓ E-465 (same sensory oral tools) ✓ E-455/456 (same food exploration and food play setup)
One Technique. One Domain. One Piece of a Larger Plan.
Your Current Position
Domain E: Feeding & Mealtime Development | Technique E-457: Gagging on Textures
Progress: Building Tier 1 Foundation (Oral Desensitization)
Progress: Building Tier 1 Foundation (Oral Desensitization)
Connected Domains
Work on E-457 directly feeds:
- Domain A (Sensory Processing): Oral sensory work generalizes to broader sensory regulation
- Domain C (Emotional Regulation): Mealtime calm generalizes to emotional baseline
- Domain K (Independence): Self-feeding skills require texture acceptance as foundation
See Your Child's Full Profile
📞FREE National Helpline: 9100 181 181
Map your child's full developmental plan
Map your child's full developmental plan

Families From the Pinnacle Network — Their Texture Journey
Anonymized clinical narratives. Identifying details changed to protect privacy. Outcomes are specific to these families; individual results vary.
Family 1 — Chennai, Tamil Nadu | Child: M, Age 3.5 at Start
Before: M had never successfully eaten anything beyond smooth Stage 1 purees. Any lump — even microscopic — triggered an immediate gag followed by vomiting. Mealtimes lasted 5–10 minutes before ending in tears. M had never chewed.
The Journey (14 months): Month 1–2: Oral warm-up only. M refused any oral tool contact for the first 3 weeks. Breakthrough in Week 4 when therapist used a flavored chew tube M's own mother warmed in her hands. Month 3–6: Mesh feeder established — first fruit flavors and textures explored. Month 7–10: The first time M let a puff dissolve on his tongue without gagging, his mother cried at the session. Month 11–14: Soft mashed banana, then soft cooked potato, then small soft pieces.
After: M eats soft table foods consistently. Still works on texture variety — but the foundation is built.
"Three years of being told he'd grow out of it. He didn't. What actually worked was understanding WHY his mouth said no — and then patiently, systematically, teaching it that texture was safe."
Family 2 — Hyderabad, Telangana | Child: R, Age 5 at Start
Before: R's gag reflex triggered from SIGHT of textured food. Extreme anticipatory anxiety. Limited to 4 foods. Had previously had a choking episode that created lasting fear.
The Journey (18 months): Medical clearance first — GERD identified and treated. Months 1–3: Exclusively visual exposure hierarchy. R sat near textured food without touching. Months 4–8: Food play with gloves, then bare hands. Oral warm-up established. Months 9–18: Slow progression through dissolvables, then soft mashed foods.
After: R eats 11 foods across 3 texture levels. Social eating at school resumed.
"R's case illustrates why rushing texture introduction without addressing anticipatory anxiety first makes things worse. We spent 3 months just on visual exposure before touching a single food. That foundation made everything else possible."
Pinnacle Network Aggregate Data
- Median time to first dissolvable tolerance: 11 weeks with daily home protocol
- 89% show measurable progress on Texture Acceptance Readiness Index within 20 weeks
- 73% achieve soft table food acceptance within 18 months with consistent therapy
You Don't Have to Figure This Out Alone
Isolation is the enemy of adherence. The families who make the most consistent progress are the ones who are connected to others on the same journey.
E-457 Parent Community — WhatsApp
"Texture Journey" — families navigating gagging and texture aversion together. Topics: daily wins, setbacks, material tips, therapist questions.
unknown link
unknown link
Pinnacle Parent Forum
Moderated by Pinnacle SLP-Feeding therapists. Evidence-based discussions.
forum.pinnacleblooms.org/feeding/texture-gagging
forum.pinnacleblooms.org/feeding/texture-gagging
Local Pinnacle Parent Meetups
Monthly feeding therapy parent groups at Pinnacle centers. Find your nearest center:
pinnacleblooms.org/centers
pinnacleblooms.org/centers
Peer Mentoring
"Texture Veteran" parents — families 2+ years ahead in the journey — available for 1:1 connection.
Request a mentor →
Request a mentor →
"Your experience is not just yours. The parent who sees your story may start the protocol they've been delaying for months. Consider sharing your journey. Every texture story shared is a family helped."
Home + Clinic = Maximum Impact
Home-based intervention works best when anchored by professional guidance. This is your access point to Pinnacle's clinical network.
Therapist Matching — E-457 Specialists
For texture-based feeding difficulties, you need:
- 🗣️SLP with Feeding Specialization (primary)
- 🤲OT with Sensory Integration Certification (secondary)
70+ centers across India | Hyderabad, Bangalore, Chennai, Mumbai, Delhi, Pune + Tier 2/3 cities
Teleconsultation — For Remote Families
- ✅ Video session with feeding-specialized SLP
- ✅ Session observation and real-time coaching
- ✅ Protocol design for your home setup
What to Bring to Your First Appointment
- Session tracking data (E-457 tracking sheet)
- Video of a typical mealtime (even 2 minutes is helpful)
- List of foods currently accepted
- Medical history relevant to feeding
Insurance and Funding
Feeding therapy services may be covered under:
- Central/state disability benefit schemes
- RBSK (Rashtriya Bal Swasthya Karyakram)
- Private health insurance (check your policy)
📞FREE National Helpline: 9100 181 181 | 24×7 | 16+ languages
The Evidence Behind Every Card on This Page
For the curious parent, the questioning grandparent, the skeptical co-parent. The research is here.
📋 PRISMA Meta-Analysis — Children (2024)
16 studies, 2013–2023: Sensory integration intervention is evidence-based practice for children with ASD. Oral sensory desensitization meets Level I evidence criteria. → PubMed: PMC11506176
📋 World Journal of Clinical Cases — Meta-Analysis (2024)
24 studies: Sensory integration therapy effectively promotes adaptive behavior, sensory processing, and functional outcomes. → PubMed: PMC10955541
📋 Indian Journal of Pediatrics — RCT (2019)
Home-based sensory interventions with parent training: significant outcomes in Indian pediatric population. → DOI: 10.1007/s12098-018-2747-4
📋 WHO Nurturing Care Framework (2018)
Population-level evidence for caregiver-delivered early intervention across 54 countries. → WHO NCF: PMC9978394 | nurturing-care.org
📋 NCAEP Evidence-Based Practices Report (2020)
Visual supports and sensory-based interventions classified as evidence-based for autism. → NCAEP.org
📋 ASHA Practice Portal — Pediatric Feeding & Swallowing
Oral sensory desensitization recognized clinical practice for texture-based feeding difficulties. → ASHA Portal

Your Data. Your Child's Personalized Pathway.
What GPT-OS® Learns From E-457 Data
- The child's current gag threshold level
- Rate of threshold change over time (fast responder vs. gradual)
- Time-of-day patterns (morning vs. evening session quality differences)
- Material-specific tolerance variations (which of the 9 materials is advancing fastest)
- Environmental factors correlated with better sessions
Privacy Assurance
Your child's data is secured under ISO 27001 standards. All data is de-identified for population analysis. You control your data — export or delete at any time.
Population-Level Benefit
When thousands of families contribute E-457 session data, GPT-OS® identifies which material sequences work fastest for which sensory profiles, which texture hierarchy progressions are most sustainable, and which family structures need different support types.
Your child's data helps every child like yours.

The Reel That Brought You Here

🎬 Episode E-457
Title: 9 Materials That Help With Gagging on Textures
Series: Feeding & Mealtime Development in Children
Domain: Domain E — Oral Motor & Feeding
Duration: 75–85 seconds
Cover tagline: "When their mouth says no before they can try"
Series: Feeding & Mealtime Development in Children
Domain: Domain E — Oral Motor & Feeding
Duration: 75–85 seconds
Cover tagline: "When their mouth says no before they can try"
The Reel gives you a 60-second visual introduction to all 9 materials — this web page is the deep-dive companion. Watch the Reel to see each material, then come back here for the full clinical context, protocol, and progress tracking.
Related Reels in the Feeding Series
E-455: 9 Materials That Help With Refusing New Foods
E-456: 9 Materials That Help With Food Selectivity
E-458: 9 Materials That Help With Chewing Development
A-013: 9 Materials That Help With Grass Texture Aversion
Follow for More
📱 Instagram: @PinnacleBloomsNetwork
📱 YouTube: youtube.com/PinnacleBloomsNetwork
📱 Facebook: facebook.com/PinnacleBloomsNetwork
📱 YouTube: youtube.com/PinnacleBloomsNetwork
📱 Facebook: facebook.com/PinnacleBloomsNetwork
Consistency Across All Caregivers Multiplies Impact
If one caregiver does the protocol and five don't, the child gets mixed signals. Sharing this page is therapy.
Share This Page
The 1-page Family Guide covers: what the technique is, what to say and NOT say around textured food, the 6-step protocol summary, emergency stop signs, and the helpline number 9100 181 181.
"Explain to Grandparents" Version
"[Child's name] is learning to be comfortable with different food textures. Their mouth is extra sensitive and needs time to adjust. Please don't comment on their eating, don't try to make them eat textured foods, and don't show concern or worry at mealtimes. Just eating your own food normally near them is the most helpful thing you can do."
Teacher / School Communication Template
"[Child's name] is currently in feeding therapy for oral texture sensitivity. At school meals, please: (1) Allow them to eat their brought foods, (2) Do not encourage them to try unfamiliar textures at school, (3) Inform me if any gagging episodes occur during school meals. Thank you for supporting their therapeutic progress."

Questions We Hear From Every Family
❓ Is this gagging psychological or sensory — and does it matter?
It matters for treatment design. Most children have a sensory component (oral hypersensitivity) — and many also develop a psychological component (anticipatory anxiety) after months of aversive gagging. Both can coexist. A professional feeding evaluation will identify the balance. Pinnacle's FusionModule™ — integrating SLP, OT, and ABA — addresses both simultaneously and is more effective than single-discipline treatment.
❓ How long will texture therapy take?
For significant texture gagging, expect 6–18 months of consistent work to reach soft table food tolerance. Factors: severity of gagging, duration of aversion, consistency of home practice, professional therapy intensity. Progress is not linear. Set your horizon to 12 months and celebrate every step along the way.
❓ My child has had the same 9 foods for 2 years. Have we passed a critical window?
No. The oral system retains neuroplasticity throughout childhood and into adolescence. There is no age at which texture therapy stops being effective. Longer aversion duration means a longer recovery journey — but every family in Pinnacle's data who has committed to consistent protocol has seen measurable improvement.
❓ Should I stop trying to introduce textures at home while doing therapy?
During the initial stabilization phase (first 4–8 weeks), your therapist may advise a "mealtime pressure-free zone." Mealtimes become purely about calories and positive association. You follow the clinic protocol ONLY in designated therapy sessions. This is not giving up — it is strategic removal of a trigger to allow desensitization to work without constant re-traumatization.
❓ My child eats crunchy textures but gags on soft/lumpy. Why?
Crunchy textures are predictable — they're either crispy or not. Soft/lumpy textures are unpredictable — they change during chewing, surprising the oral system mid-bite. Many children tolerate crunchy precisely because it's predictable. Treatment focuses specifically on the unpredictable texture category.
❓ Is ARFID the same as what we're dealing with?
ARFID is a diagnostic category that can include texture-based feeding difficulties as one presentation. Not all children with texture gagging have ARFID — the diagnosis depends on severity, nutritional impact, and psychosocial impact. If your child's diet is significantly nutritionally inadequate, an ARFID evaluation may be appropriate. Call 9100 181 181 to discuss.
❓ What if the feeding therapist says my child needs a G-tube?
G-tube recommendations are made when oral feeding cannot safely meet nutritional needs. G-tube is NOT the end of oral feeding therapy — many children on G-tubes continue oral feeding therapy and eventually wean. If a G-tube is being discussed, request a second opinion and ensure a complete medical workup. Call 9100 181 181 for guidance.
❓ Can I do E-457 without a therapist?
Some families start with home protocol components before accessing professional therapy. The home protocol in this page is designed to be parent-safe. However — if your child has significant vomiting from gagging, weight concerns, or medical feeding history — professional assessment is the safety gate. Use this page to prepare and supplement professional therapy, not to replace it.
Didn't find your answer? → Ask GPT-OS® | 📞FREE Helpline: 9100 181 181 | → Book Teleconsultation
Preview of 9 materials that help with gagging on textures Therapy Material
Below is a visual preview of 9 materials that help with gagging on textures therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

Their Mouth Can Learn That Textures Are Safe.
The Journey Starts With One Step Today.
You've read the science. You've seen the protocol. You have the materials list. What happens next is determined by what you do in the next 10 minutes.
🏛️ Validated by the Pinnacle Blooms Consortium
🤲 OT | 🗣️ SLP | 🧠 ABA | 📚 SpEd | 👶 NeuroDev | 🔬 CRO
20M+ Sessions | 97%+ Improvement | 70+ Centers
20M+ Sessions | 97%+ Improvement | 70+ Centers
From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7, personalized, multi-disciplinary pediatric therapy center — accessible to every family, in every language, at every income level, in every geography.
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7, personalized, multi-disciplinary pediatric therapy center — accessible to every family, in every language, at every income level, in every geography.
Medical Disclaimer: This content is educational and informational. It does not replace professional feeding evaluation and therapy by licensed speech-language pathologists, occupational therapists, or feeding specialists. Severe or worsening feeding difficulties require medical evaluation. Please consult a pediatric feeding specialist for persistent texture aversion, weight concerns, or feeding that compromises nutritional adequacy.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT Startup India: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, and FusionModule™ are proprietary marks of Pinnacle Blooms Network®.
📞9100 181 181 | care@pinnacleblooms.org | pinnacleblooms.org | techniques.pinnacleblooms.org
GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, and FusionModule™ are proprietary marks of Pinnacle Blooms Network®.
📞9100 181 181 | care@pinnacleblooms.org | pinnacleblooms.org | techniques.pinnacleblooms.org