Attention & Sleep
10 evidence-based interventions for children with autism — covering sitting still, fidgeting, attention difficulty, easy distraction, impulsivity, sleep initiation, night waking, bedtime resistance, sleep routine, and sensory sleep environment. Subdomain D6 | Pinnacle Blooms Network®
Domain D: Behaviour
D-441 to D-450
21M+ Sessions
Section 1: Attention & Body Regulation
The Attention Network — Why "Pay Attention" Doesn't Work
Attention is not a single skill — it's a network of three interconnected systems that can each be independently affected in autism. Understanding this neuroscience transforms how we teach, support, and respond to attention challenges.
Alerting Network
Brainstem reticular formation → thalamus. Maintains arousal and wakefulness. The baseline "on" state that keeps the brain ready to receive information.
Orienting Network
Superior parietal → temporal-parietal junction. Directs attention to relevant stimuli. The "Look at THIS" system — responsible for shifting focus appropriately.
Executive Attention
Anterior cingulate → dorsolateral PFC. Sustained focus, conflict monitoring, distraction inhibition. The "Stay focused, ignore THAT" command centre.
In ASD, attention is not simply "poor" — it is differently distributed. Hyperfocus on preferred topics coexists with inability to attend to non-preferred tasks. The system allocates resources based on interest and sensory salience, not social or task demands. ASD+ADHD comorbidity affects 30–80% of children — compounding the challenge significantly.

D-441 · Card A
Recognition + Neuroscience
Can't Sit Still — The Moment & The Neuroscience
"Sit down." They sit. Three seconds later — up. Rocking the chair. Sliding off. Standing. Wandering. Returning. Sitting. Up again. School demands 6+ hours of stillness. Their body demands movement. This collision between institutional expectation and neurological need defines their school experience — and it is not defiance. It is neurology.
The Neuroscience
Sitting still requires the active suppression of the motor system — a PFC computation that consumes significant cognitive energy. For many children with ASD (especially with ADHD comorbidity), this "stillness" computation costs so much that nothing remains for the actual task. The paradox: demanding stillness reduces attention. Allowing movement increases attention. The body must move so the brain can think.
The Evidence
Level I Evidence
Movement breaks and sensory seating consistently improve attention and on-task behaviour. Active seating — wobble cushions, therapy balls — outperforms rigid seating for attention in children with ASD+ADHD.
NCAEP 2020 | Sensory seating research | ADHD+ASD attention studies
D-441 · Card B
Intervention Strategy
Can't Sit Still — Intervention Strategy
The Paradigm Shift: Stop demanding stillness. Start providing structured movement that enables attention.
1
Movement Breaks
5-minute gross motor activity every 20–30 minutes — jumping jacks, wall pushes, running in place, yoga pose. Schedule these as non-negotiable parts of the learning session.
2
Active Seating
Wobble cushion (₹500–1500), therapy ball chair, move-n-sit disc, or T-stool. These allow micro-movements while seated, satisfying the body's movement need without leaving the work area.
3
Heavy Work First
10 minutes of intense proprioceptive input before sitting tasks — carrying books, climbing, animal walks. This creates a calmer nervous system for 20–30 minutes of seated focus.
4
Alternative Seating
Standing desk, kneeling position, lying prone, or floor seating. The rigid chair is the worst option for many children with ASD. Expand what "seated work" looks like.
Reframing for teachers: "They are not misbehaving — they are regulating. Allow movement, get better attention." The child can also be given a "body break" card they can use independently when they need movement — building self-advocacy from the start.

D-441 · Card C
Home Protocol + Action
Can't Sit Still — Your Home Protocol
This daily structure transforms homework from a battle into a workable routine. Heavy work before seated tasks is the single highest-impact change most families can make.
School Accommodation
Under RPwD 2016, request: active seating, scheduled movement breaks, standing desk option, seating near aisle for easy exit, and sensory tools at desk (fidget, wobble cushion). A letter from your OT makes this request formal and effective.
9 Canon Materials
Lead:🤲 OT · 📋 ABA | SpEd · NeuroDev (ADHD assessment)

D-442 · Card A
Recognition + Neuroscience
Constant Fidgeting — The Moment & The Neuroscience
Clicking pens. Tapping fingers. Chewing sleeves. Picking at skin. Twirling hair. Bouncing legs. Fiddling with everything. The hands and body are in constant low-level motion. Teachers call it "distracting." The truth: for many children with ASD+ADHD, fidgeting IS the attention strategy. Stop the fidget — lose the attention.
The Neuroscience
Fidgeting provides sub-threshold sensory stimulation that maintains arousal in the alerting network. Research shows children with ADHD who fidget more perform better on cognitive tasks. The fidget provides just enough input to keep the brainstem reticular formation activated — maintaining the "on" state. Taking away the fidget is like cutting the engine's idle: the system stalls.
The Evidence
Level I Evidence
Fidget tools consistently improve on-task behaviour and learning outcomes in ASD+ADHD populations. The evidence base for classroom-appropriate fidget tools is strong and growing.
NCAEP 2020 | Fidget research in ADHD+ASD
D-442 · Card B
Intervention Strategy
Constant Fidgeting — Intervention Strategy
Classroom Fidgets
Under-desk resistance band on chair legs, silent putty, tangle toy, smooth stone, textured pencil grips, velcro strip under desk surface. Silent and invisible to classmates.
Fidget Hierarchy
Silent/invisible fidgets for classroom → larger fidgets for home → unrestricted movement during breaks. Match the fidget intensity to the environment and demand level.
Quiet Fidget Rules
Teach: fidget doesn't make noise, doesn't leave the desk, doesn't distract others. When fidgeting disrupts peers — redirect to a quieter fidget, not to NO fidget.
Teacher Education
Indian classroom context: 40+ students, strict discipline culture. Teacher education on fidget benefits is essential — share research, frame as a learning tool, not a toy.

D-442 · Card C
Home Protocol + Action
Constant Fidgeting — Your Home Protocol
Fidget Kit by Context
School kit (₹350): Silent putty (₹100), smooth stone (₹0 — find one outdoors), resistance band on chair (₹200), textured pencil grip (₹50)
Home kit: Fidget spinner, tangle toy, stress ball, therapy putty, kinetic sand — more variety, more intensity allowed
Car/travel kit: Small fidget in pocket, chew necklace, rubber band on wrist
Daily Protocol
✅ Fidget available during ALL seated tasks — homework, meals, screen time, car rides
✅"Hands busy" strategy: provide something to the hands before the hands find their own solution (hair, skin, clothing)
✅ Regular heavy work breaks to reduce overall fidget intensity throughout the day
D-443 · Card A
Recognition + Neuroscience
Attention Difficulty — The Moment & The Neuroscience
"Pay attention!" — the most useless instruction in education. They can't. Not because they're lazy, defiant, or unintelligent — because the executive attention network cannot sustain focus on non-preferred, non-salient tasks. They'll focus on dinosaurs for 3 hours. They can't focus on math for 3 minutes. The attention exists — it is allocated differently.
The Neuroscience
Attention difficulty in ASD reflects the interest-driven nervous system: the reward system (nucleus accumbens) determines attentional allocation. Preferred topic = high dopamine = unlimited attention. Non-preferred task = low dopamine = attention collapses. This is NOT voluntary. The child cannot "choose" to find math interesting any more than you can choose to find a blank wall fascinating.
The Intervention Principle
Make the task more rewarding — do not demand more attention. Embed non-preferred content within preferred interests. Use reinforcement, task chunking, and visual supports to artificially raise the dopamine signal around low-interest tasks.
NCAEP 2020 — Level I Evidence

D-443 · Card B
Intervention Strategy
Attention Difficulty — Intervention Strategy
Interest-Based Learning
Embed non-preferred tasks within the child's preferred interest: counting with dinosaurs, reading about trains, math through cricket statistics. The interest provides the dopamine the task cannot.
Task Chunking + Visual Progress
Break large tasks into tiny visible segments. Three problems → break → three problems → break. Visible progress (tokens, checkboxes) sustains motivation across chunks.
Environmental Arrangement
Reduce all distractions: face the wall, clear desk, headphones for noise, study carrel. Use highlighting, colour-coding, and reading windows to focus visual attention on the task.
Timer-Based Attention Building
Start at the child's actual current capacity (even 2 minutes). Build by 30 seconds at a time. Celebrate every successful focus burst with a token or praise.
⚠️ADHD Assessment: If attention difficulty is pervasive across ALL contexts and interests, a NeuroDev evaluation for ADHD comorbidity is essential. Medication may significantly improve attentional capacity and quality of life.

D-443 · Card C
Home Protocol + Action
Attention Difficulty — Your Home Protocol
Homework Setup
📚 Clear desk — only current task visible
🎧 Noise-reducing headphones
⏰ Visual timer — start with achievable time
🏆 Token after each completed chunk
🏃 Movement break between chunks
🦕 Interest integration wherever possible
🎧 Noise-reducing headphones
⏰ Visual timer — start with achievable time
🏆 Token after each completed chunk
🏃 Movement break between chunks
🦕 Interest integration wherever possible
Attention Building Progression
Weeks 1–2: 3-minute focus → break → 3 minutes (6 min total work per 20-min session)
Weeks 3–4: 5-minute focus → break → 5 minutes
Weeks 5–8: 8-minute focus → break → 8 minutes
Goal: 15–20 minutes sustained attention — realistic and achievable for ASD+ADHD

D-444 · Card A
Recognition + Neuroscience
Easy Distraction — The Moment & The Neuroscience
Every sound. Every movement. Every change in the environment. Their attention is pulled away by everything — the fan's hum, a bird outside, someone walking past the door, their own passing thoughts. The distractibility is exhausting — for them and for everyone trying to teach them.
The Neuroscience
Distractibility reflects a filtering deficit in the thalamic gating system. Normally, the thalamus acts as a sensory gate — filtering irrelevant input and passing only relevant information to the cortex. In ASD+ADHD, this gate is too open: everything gets through. The brain cannot determine which stimuli are relevant (teacher's voice) vs. irrelevant (traffic outside). ALL stimuli arrive at the cortex with equal priority.
What This Means in Practice
The child is not being rude or lazy when they look at the window. Their brain is genuinely processing that stimulus with the same urgency as the teacher's instruction. The solution is environmental: reduce the number of stimuli competing for attention, rather than demanding the child filter what their brain cannot filter.
NCAEP 2020 — Level I Evidence
D-444 · Card B
Intervention Strategy
Easy Distraction — Intervention Strategy
Distraction Audit
List every distraction in the learning environment — visual, auditory, tactile, olfactory — and systematically reduce each one. Start with the loudest or most frequently pulling distractors.
Auditory Management
Noise-reducing headphones, white noise machine, quiet workspace, earplugs during independent work. Match solution to child's auditory profile — some need white noise, others need silence.
Visual Management
Study carrel (three-sided partition), face wall, remove posters from workspace, minimize visual clutter. Seating position matters: away from windows, doors, and high-traffic areas.
Internal Distraction
"Parking lot" for wandering thoughts: write the distracting thought on a sticky note, "park" it on the side of the desk, and return to the task. Thought captured = brain released.
Attention anchors — a physical object representing "I'm working now" (special pencil, attention badge) — create a tangible signal to the nervous system that focus mode is active. Teach self-monitoring with a "Am I focused?" visual cue card on the desk.

D-444 · Card C
Home Protocol + Action
Easy Distraction — Your Home Protocol
Distraction-Free Study Zone
📍 Dedicated workspace — same place every day
🧱 Study carrel or DIY partition (₹500: cardboard box sides)
🔇 Noise management: headphones, closed door, white noise app
📱 Screens off and out of sight
🪟 Window blocked or curtained during study
🧹 Clear desk — only current task visible
🧱 Study carrel or DIY partition (₹500: cardboard box sides)
🔇 Noise management: headphones, closed door, white noise app
📱 Screens off and out of sight
🪟 Window blocked or curtained during study
🧹 Clear desk — only current task visible
Indian Home Reality Adaptations
Joint family noise → headphones + designated quiet time block (agree with family)
Shared room → cardboard partition creates a visual "workspace island"
Small apartment → designated corner with visual boundaries (mat, low shelf)
Power cuts → torch + battery-operated white noise, backup plan prepared in advance

D-445 · Card A
Recognition + Neuroscience
Impulsivity — The Moment & The Neuroscience
They grab before asking. They run before looking. They speak before thinking. They touch before considering. The gap between impulse and action — which in most people is a fraction of a second of PFC computation — is absent. The thought and the action are the same thing. Impulsivity is the invisible disability that causes the most social damage.
The Neuroscience
Impulsivity = PFC inhibitory failure. The PFC should: detect the impulse → evaluate the consequence → inhibit the motor response → generate an alternative. This entire computation should happen in 200–500 milliseconds. In ASD+ADHD, the PFC computation is too slow — the motor cortex fires before the PFC can evaluate and inhibit. The child is not choosing to be impulsive; the brake is too slow for the engine.
The Critical Distinction
Impulsivity is neurological, not moral. The child does not decide to grab, run, or interrupt — the action happens before the decision can be made. Punishment after the fact is ineffective because the brain never had the opportunity to choose differently. The intervention must happen before the impulse fires.
NCAEP 2020 — Level I Evidence

D-445 · Card B
Intervention Strategy
Impulsivity — Intervention Strategy
1
STOP–THINK–DO
Visual prompt at every decision point — desk, wall, door, wristband. Practiced during calm until the three-step pause becomes automatic and habitual.
2
Build the Pause
Physical STOP signal (hand up, red card) practiced repeatedly during calm. Start with 3-second waits and build to 10 → 30 → 1 minute with a visual timer.
3
Environmental Reduction
Remove temptation structurally: food not visible if they grab food; physical barriers at exits if they run. Environmental design is faster than teaching for immediate safety.
4
Impulse Control Games
Red Light/Green Light, Simon Says, Freeze Dance — daily fun practice of "stop on command." The game trains the exact neural pathway (motor inhibition on signal) needed for impulse control.
⚠️ADHD Medication Assessment: If impulsivity is severe, pervasive, and creating safety risks, a NeuroDev evaluation for medication is essential. Stimulant medication can significantly improve impulse control and reduce daily harm.

D-445 · Card C
Home Protocol + Action
Impulsivity — Your Home Protocol
Daily Practice Protocol
🛑 "Stop-Think-Do" visual posted at: front door, homework desk, dining table, and in school bag
🎮 One impulse control game per day — 5 minutes: Red Light/Green Light, Simon Says, Freeze Dance
⏱️ Waiting practice: timer-based waiting during preferred activities ("wait 10 seconds, then you can have it")
🏆Celebrate every successful pause — "You stopped and asked! That's amazing!" Positive reinforcement builds the pause faster than anything else.
Safety Priority
For dangerous impulsivity — road-running, grabbing hot items, jumping from heights — environmental barriers come first, teaching comes second.
Never rely on a child's in-the-moment impulse control for safety. Design the environment so the dangerous action is physically impossible, then teach the safer alternative in a low-stakes context.

Section 2: Sleep
The Sleep Circuit — Why Children with Autism Can't Fall Asleep
Sleep disorders affect 50–80% of children with ASD — one of the highest comorbidity rates in all of pediatric medicine. Understanding why sleep is neurologically harder in autism is the first step toward fixing it — and fixing sleep improves every other domain.
Suprachiasmatic Nucleus
The brain's master circadian clock. May show atypical rhythms in ASD, making the body's natural sleep-wake timing less reliable and consistent.
Pineal Gland & Melatonin
Melatonin production is often reduced, delayed, or irregularly timed in ASD — making sleep onset biologically harder even when the child is exhausted and the environment is perfect.
Amygdala/Anxiety Circuit
Anxiety activates arousal systems that actively oppose sleep. The child cannot sleep because the brain won't allow it — it is in threat-detection mode, not rest mode.
Sensory System
Every bedtime sensory input — sheet texture, room temperature, light level, ambient noise, pyjama fabric — can trigger discomfort that prevents the body from reaching the sensory neutrality sleep requires.
Why sleep matters for everything: One night of poor sleep reduces PFC function by 30–40%, directly increasing meltdowns, aggression, SIB, attention difficulties, and emotional dysregulation. Fixing sleep can improve every other domain. Sleep is not a luxury — it is infrastructure.

D-446 · Card A
Recognition + Neuroscience
Sleep Initiation — The Moment & The Neuroscience
Bedtime: 8 PM. Eyes finally close: 11 PM. Three hours of lying awake, tossing, stimming, getting up, requesting water, asking questions, crying. Sleep onset insomnia — the inability to fall asleep — affects 40–80% of children with ASD. Parents are exhausted. The child is exhausted. And tomorrow's behaviour will directly reflect tonight's sleep failure.
The Neuroscience
Sleep initiation requires four simultaneous conditions that are each harder in ASD: melatonin release (often reduced or delayed), arousal system deactivation (difficult when anxiety or sensory issues maintain sympathetic activation), PFC executive shutdown (the thinking brain must quiet — hard when thoughts loop), and sensory comfort (body must reach sensory neutrality — nearly impossible when bedding, temperature, or noise are aversive).
The Evidence
Level I Evidence
Sleep hygiene combined with melatonin supplementation and sensory sleep environment optimisation represents the strongest evidence-based package for sleep initiation in ASD.
NCAEP 2020 | Sleep in ASD meta-analyses | Melatonin RCTs

D-446 · Card B
Intervention Strategy
Sleep Initiation — Intervention Strategy
Sleep Hygiene Protocol
Consistent bedtime (same time ±15 minutes every night including weekends), screen curfew 60 minutes before bed — blue light actively suppresses melatonin — cool dark room, quiet environment. Consistency is more important than the exact time chosen.
Melatonin Supplementation
Evidence supports 1–3mg melatonin 30–60 minutes before desired sleep time. Start with 0.5mg and titrate slowly. ⚠️ Always consult NeuroDev before starting — dosing, timing, and formulation (liquid vs. tablet, immediate vs. extended-release) all matter significantly.
Calming Bedtime Routine
Deep pressure (massage, weighted blanket), quiet activity (reading, gentle music), reduced lighting (dimmer or lamp only), aromatherapy (lavender — mild evidence, test tolerance first).
Anxiety Management
"Worry box" for pre-sleep anxiety (write the worry, put it in the box, it's handled until morning), relaxation scripts, consistent reassurance language. When sleep onset consistently exceeds 60 minutes → formal sleep evaluation.
D-446 · Card C
Home Protocol + Action
Sleep Initiation — Your Home Protocol
The power of this protocol comes from its unwavering consistency. The sequence itself becomes the sleep signal — the brain begins releasing melatonin when the routine starts, not when the clock strikes bedtime.
Indian Home Adaptations
Joint family noise → white noise machine or fan. Shared bedroom → visual partition, individual routine. Summer heat → fan + light cotton sheet. Power cuts → battery-operated white noise, battery fan. Monsoon → adjust for humidity with light cotton options.
9 Canon Materials

D-447 · Card A
Recognition + Neuroscience
Night Waking — The Moment & The Neuroscience
2 AM. They're awake. Fully awake. Playing, stimming, calling out, coming to your bed, turning on lights. Sleep maintenance insomnia — they fall asleep but cannot stay asleep. The child loses hours of restorative sleep. The parents lose all of theirs.
The Neuroscience
Sleep cycles include brief natural awakenings between 90-minute NREM/REM cycles. Neurotypical children briefly wake → self-soothe → return to sleep without full consciousness. ASD children wake → fully activate (sensory system online, arousal system engaged) → cannot self-soothe → fully awake for hours. Reduced melatonin + anxiety + sensory alertness = cycle after cycle of complete waking.
The Key Insight
The problem is not the waking — natural brief waking happens in everyone. The problem is the child's inability to self-soothe back to sleep once awake. Every intervention targets this transition: making the return to sleep automatic, uneventful, and boring enough to not trigger full activation.
NCAEP 2020 — Level I Evidence

D-447 · Card B
Intervention Strategy
Night Waking — Intervention Strategy
Boring Night Protocol
If they wake, environment stays dark, quiet, and completely boring. Parent presence is calm and silent — no play, no conversation, no screens, no kitchen visits. The environment must communicate: nothing interesting is available at 2 AM.
Extended-Release Melatonin
Discuss with NeuroDev: extended-release formulations maintain melatonin levels through the night, reducing mid-cycle waking. This is different from immediate-release which only helps with sleep onset.
Night Light Choice
RED or AMBER night lights only. Blue and white light actively suppresses melatonin resurgence — using a standard white night light makes returning to sleep biologically harder.
In-Bed Self-Soothing Kit
Weighted blanket, soft music on a quiet loop, comfort object, sensory toy already in the bed. The child's tools for returning to sleep should be within arm's reach without needing to call for help.
Keep a sleep diary: track wake times, duration, triggers, and context. Patterns identified over 2–3 weeks provide the most actionable information for your NeuroDev team.

D-447 · Card C
Home Protocol + Action
Night Waking — Your Home Protocol
Night Waking Response Protocol
🌙 They wake → Do NOT turn on main lights (red night light only)
🤫 Minimal interaction: "It's nighttime. Back to sleep." — same words every time
🚫 No screens. No play. No kitchen. No conversation.
🧸 Guide back to bed → weighted blanket → comfort object → white noise
📝 Record: time awake, time back to sleep, what was observed → share with NeuroDev at next review
Parent Survival Strategy
Tag-team with a partner when possible to protect at least one adult's sleep quality. Accept that you will lose sleep during the intervention period — this is not forever.
Night waking most often improves within 4–8 weeks of a consistent approach combined with melatonin optimisation. Document your progress — the improvement motivates continued consistency.

D-448 · Card A
Recognition + Neuroscience
Bedtime Resistance — The Moment & The Neuroscience
"No bed!" Running from the bedroom. Curtain calls — one more water, one more toilet, one more hug, one more story. Bedtime becomes a two-hour negotiation. Bedtime resistance is distinct from sleep initiation difficulty (D-446): this child CAN fall asleep — they DON'T WANT TO. The transition from activity to bed is the hardest transition of the day.
The Neuroscience
Bedtime resistance reflects multiple converging factors: transition difficulty (ending preferred activity is aversive), separation anxiety (leaving parent), fear of dark, FOMO, and most importantly — conditioned avoidance. When bedtime has been paired with frustration and demands repeatedly, the bed itself becomes an aversive stimulus. The child is not being difficult; they are avoiding something their nervous system has learned to associate with distress.
The Evidence
Level I Evidence
Bedtime fading combined with a positive bedtime routine and graduated extinction represents the strongest evidence-based approach to bedtime resistance in ASD.
NCAEP 2020 — Behavioural sleep interventions
D-448 · Card B
Intervention Strategy
Bedtime Resistance — Intervention Strategy
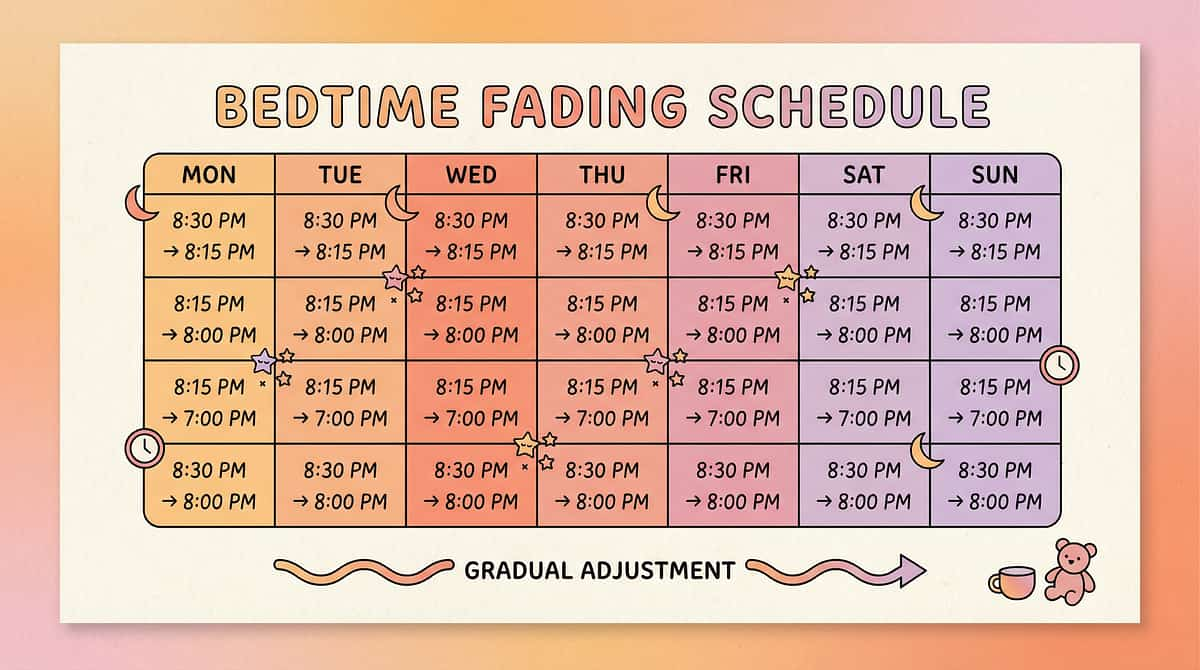
1
Bedtime Fading
Temporarily SET bedtime to when they actually fall asleep (even 10 PM) — zero resistance at the real sleep time. Once falling asleep quickly, move 15 minutes earlier every 3–4 days until target bedtime is reached.
2
Positive Bedtime Routine
Re-pair the bed with positive associations: make bedtime the BEST part of the day — special stories, massage, one-on-one undivided attention, favourite calming activity. The bed must stop being aversive before behaviour changes.
3
Visual Bedtime Schedule
Picture sequence of every step eliminates negotiation — "the schedule says teeth next, not the parent." The schedule becomes the authority, removing the interpersonal power struggle entirely.
4
The Bedtime Pass
Give the child ONE physical pass for one additional request after lights out. After the pass is used — no more. This gives perceived control while structurally limiting the curtain calls that reinforce bedtime avoidance.
D-448 · Card C
Home Protocol + Action
Bedtime Resistance — Your Home Protocol
Bedtime Fading Schedule
📊Week 1: Set bedtime at current actual sleep time — no resistance because they're genuinely tired
📊Week 2: Move 15 minutes earlier. Maintain the full positive routine.
📊Weeks 3–8: Continue 15-minute shifts every 3–4 days until target bedtime is reached.
Positive Routine Template
🛁 Bath → 👕 Pyjamas → 🪥 Teeth → 📖 2 stories (child's choice) → 💆 Massage/deep pressure → 🧸 Comfort object → 🌙 Goodnight script → 💡 Lights off → 🎵 White noise
Bedtime Pass rules: One card. One extra request. After it's used — no more until morning. Celebrate when they use it wisely.
D-449 · Card A
Recognition + Neuroscience
Sleep Routine — The Master Sleep Card
If there is ONE intervention from this entire sleep section that changes everything, it is this one. A consistent, predictable, sensory-informed sleep routine — repeated identically every night — is the single most effective non-pharmacological sleep intervention for autism. The routine IS the treatment.
The Neuroscience
A sleep routine builds a conditioned chain in the basal ganglia: step 1 → step 2 → step 3 → ... → sleep. After enough repetitions, the chain becomes automatic — each step triggers the next, and the final step triggers sleep onset. The brain begins melatonin release not at a clock time, but at the start of the routine — because the routine has become the brain's primary sleep cue. One disrupted night begins to reset the chain.
The Evidence
Level I Evidence
A consistent bedtime routine is the #1 sleep recommendation for ASD across all major clinical guidelines — NCAEP 2020, AAP sleep guidelines, and every major sleep-in-ASD meta-analysis. No other single intervention has stronger consensus.

D-449 · Card B
Intervention Strategy
Sleep Routine — Intervention Strategy
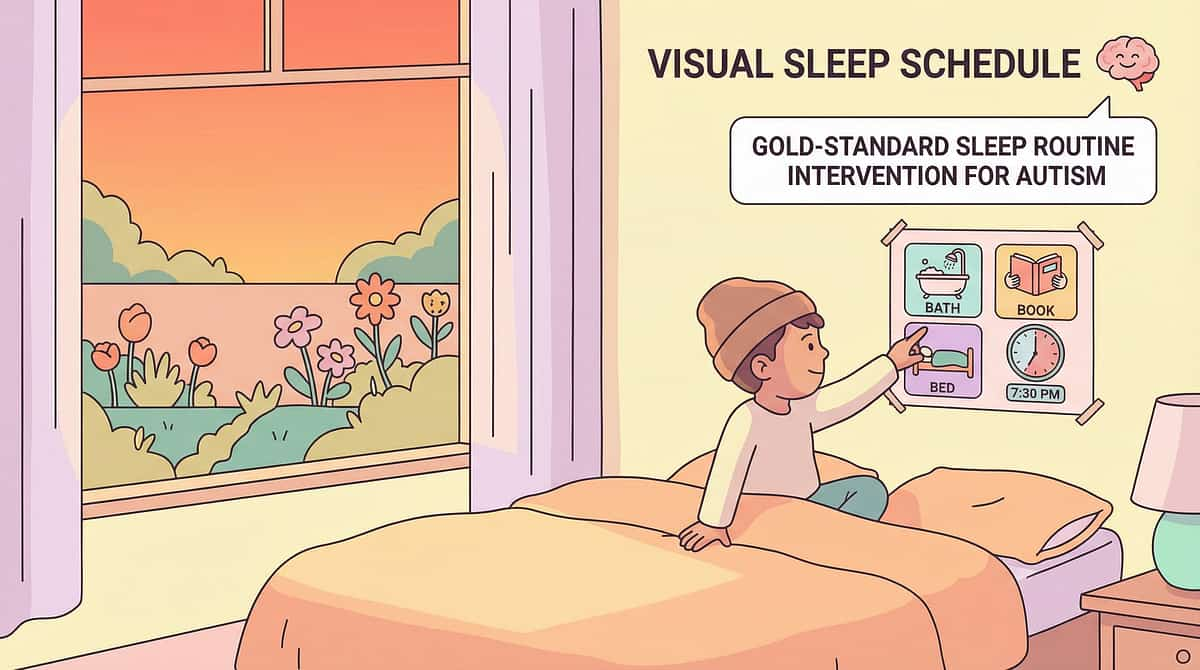
Visual Sleep Schedule
Picture-based schedule in the bedroom. Same order every night, no exceptions, no negotiations. The schedule is the authority — it removes the parent from the negotiation entirely.
Routine Components
Transition activity → hygiene → sensory-friendly clothing → connection (story/massage/song) → environmental setup (lights/noise/temperature) → sleep cue (final words/action) → sleep. Duration: 20–30 minutes total.
Consistency Rules
Same routine on weekdays AND weekends. Same order. Same goodnight words. Same person (ideally) — or the same script given to every caregiver so the words never change even when the face does.
Travel Routine Kit
Portable kit for novel environments: comfort object, favourite story, white noise app, preferred pyjamas, laminated routine card. Maintain as much of the routine as physically possible away from home.
When routine becomes extremely rigid — child melts down if a single step is missed — apply flexibility-building strategies (D-374) to the sleep context. The goal is a predictable, calming routine, not an inflexible ritual that creates its own anxiety.

D-449 · Card C
Home Protocol + Action
Sleep Routine — Your Home Protocol
Visual Sleep Routine Template (print, laminate, and post in bedroom)
1
Bath/Wash 🛁
2
Pyjamas 👕
3
Teeth + Toilet 🪥
4
Melatonin 💊
5
Story/Song 📖
6
Deep Pressure 💆
7
Weighted Blanket 🧸
8
White Noise 🎵
9
Goodnight Words 🌙
Non-negotiables: Same time (±15 minutes). Same order. Every night. For a minimum of 4 weeks before evaluating effectiveness — the basal ganglia chain needs time to build.

D-450 · Card A
Recognition + Neuroscience
Sensory Sleep Environment — The Bedroom as Sensory Minefield
The sheet is wrong. The pillow is wrong. The room is too bright. Too dark. The fan is too loud. The silence is too quiet. The pyjamas itch. The blanket is too heavy. The blanket is too light. The bedroom is a sensory minefield — and every single sensory discomfort prevents the brain from transitioning into sleep. This is the capstone of Domain D.
The Neuroscience
Sleep requires the sensory system to reach a state of sensory neutrality — neither over-stimulated nor under-stimulated. For the ASD sensory system, this neutral zone is extremely narrow. Achieving it requires simultaneous optimisation of six sensory channels: visual, auditory, tactile, temperature, proprioceptive, and olfactory. All six must be addressed — optimising five while leaving one problematic can prevent sleep entirely.
The Evidence
Level I Evidence
Sensory sleep environment optimisation is supported by NCAEP 2020, sensory processing and sleep research, and the clinical consensus across OT, sleep medicine, and ASD-specialist practice globally.

D-450 · Card B
Intervention Strategy
Sensory Sleep Environment — Intervention Strategy
Visual
Blackout curtains (₹500–2000) or foil on windows. RED or amber night light only — no blue or white. No screens visible from the bed. Complete visual control of the sleep environment.
Auditory
White noise machine or fan for consistent masking sound, or complete silence with earplugs/headband headphones. Match strictly to the child's auditory profile — some need sound, some need silence.
Tactile
Test bedding textures with the child: jersey cotton, silk, bamboo. Seamless pyjamas. Weighted blanket at 10% body weight. Compression sheet or sleep sack for proprioceptive input during the night.
Temperature
Cool room (18–22°C ideal). Fan + light sheet, or AC where available. Indian summer: cooling is a priority investment — it is not a comfort upgrade, it is a sleep necessity.
Proprioceptive
Weighted blanket, body pillow, sleeping bag or compression sheet, tight-fitting sleep clothes. Proprioceptive input during sleep reduces arousal and supports sustained sleep cycles.
Olfactory
Neutral environment — remove all strong smells including agarbatti/incense during sleep hours. Lavender pillow spray has mild evidence and good tolerance in most children (test first).
D-450 · Card C
Home Protocol + Action
Sensory Sleep Environment — Your Home Protocol
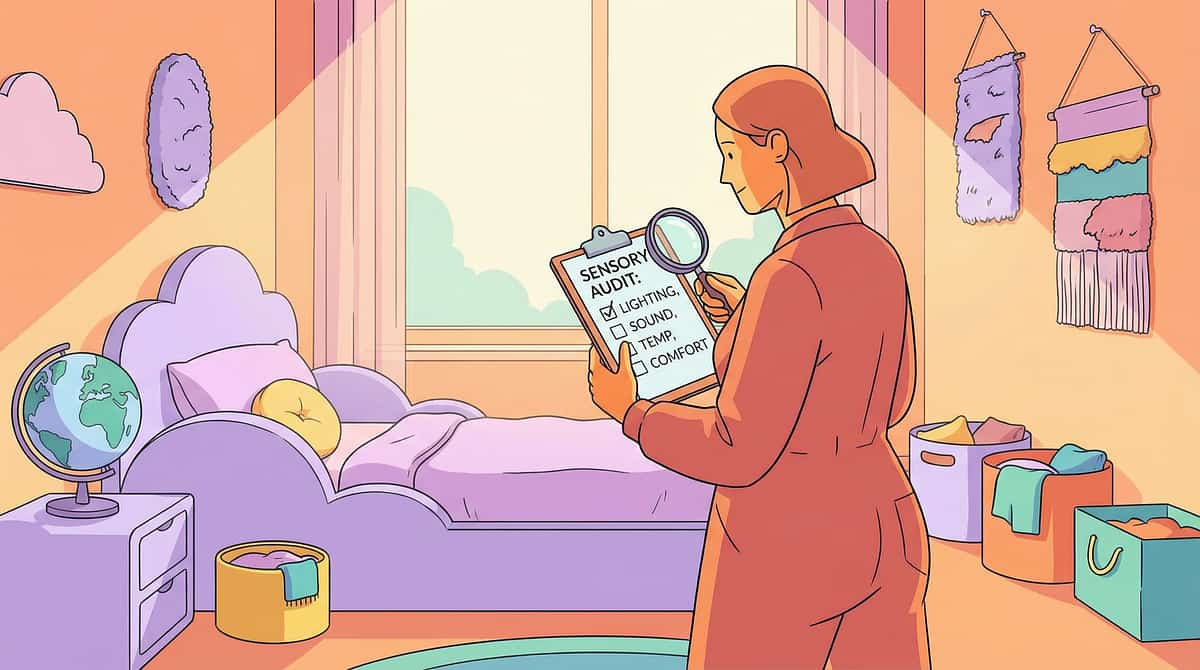
Bedroom Sensory Audit — Assess, Identify, Solve
Sense | Common Issue | Solution | ₹ Budget | |
Visual | Too bright | Blackout curtains + red night light | ₹500–2000 | |
Auditory | Too noisy or too quiet | White noise machine or fan | ₹500–1500 | |
Tactile | Sheet texture aversive | Jersey cotton fitted sheet | ₹300–800 | |
Temperature | Too hot (Indian summer) | Ceiling fan + light cotton | ₹0 (existing fan) | |
Proprioceptive | Under-compressed | Weighted blanket (10% body weight) | ₹1500–4000 | |
Olfactory | Strong smells at night | Remove agarbatti, neutral environment | ₹0 |
Investment Priority Order
1️⃣ Weighted blanket — biggest sleep impact per rupee
2️⃣ Blackout curtains
3️⃣ White noise machine or fan
4️⃣ Sensory pyjamas (seamless)
5️⃣ Bedding upgrade (jersey cotton)
2️⃣ Blackout curtains
3️⃣ White noise machine or fan
4️⃣ Sensory pyjamas (seamless)
5️⃣ Bedding upgrade (jersey cotton)
9 Canon Materials
Lead:🤲 OT (Sensory Sleep) · 🧠 Psychology (Sleep Behaviour) · NeuroDev (Melatonin/Medication) · 📋 ABA · SpEd
Sleep Is the Foundation — The Domain D Capstone
Fix sleep → behaviour improves across every domain. Every rupee invested in sleep environment saves hundreds in behavioural intervention. Sleep is not a luxury — it is infrastructure.
50-80%
ASD Children Affected
Proportion of children with autism experiencing significant sleep disorders — one of the highest comorbidity rates in all of pediatric medicine.
30-40%
PFC Function Lost
Reduction in prefrontal cortex function after just one night of poor sleep — directly increasing meltdowns, aggression, attention difficulty, and emotional dysregulation.
4 wks
Minimum Trial Period
The minimum time a consistent sleep routine must be followed before evaluating effectiveness. The brain's conditioned chain needs repetition to become automatic.

All 10 Techniques at a Glance — Subdomain D6
Each technique below links to its full 40-card deep-dive page with 9 canon therapy materials, step-by-step protocols, school accommodation letters, and GPT-OS® clinical decision support.

D-441: Can't Sit Still
Movement as attention strategy. Active seating, heavy work protocols, and school accommodation.

D-442: Constant Fidgeting
Fidgeting as attention tool. Silent classroom fidgets and the hierarchy from school to home.

D-443: Attention Difficulty
Interest-driven attention, task chunking, and the progression from 2-minute to 20-minute focus.

D-444: Easy Distraction
Thalamic gating deficit. Environmental distraction audit, study carrel, parking lot technique.

D-445: Impulsivity
PFC inhibitory failure. Stop-Think-Do framework, waiting practice, and impulse control games.

D-446: Sleep Initiation
Melatonin delay and arousal system activation. The 8 PM protocol and four-condition sleep model.

D-447: Night Waking
Sleep cycle activation in ASD. The boring night protocol and extended-release melatonin strategy.

D-448: Bedtime Resistance
Conditioned avoidance. Bedtime fading, positive re-pairing, and the bedtime pass technique.

D-449: Sleep Routine
The master sleep card. Basal ganglia conditioning, 9-step visual template, consistency rules.

D-450: Sensory Sleep Environment
Six-channel sensory audit. The budget-ranked investment guide for the optimal sleep bedroom.
Preview of attention sleep Therapy Material
Below is a visual preview of attention sleep therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!

Domain D: Behaviour — Complete
Subdomain D6: Attention & Sleep completes all 110 techniques across Domain D. Each subdomain addresses a distinct cluster of behavioural challenges with the same evidence-based, neuroscience-grounded approach — from understanding and prevention through to the most complex attention and sleep presentations.
D1: Understanding & Preventing
20 techniques · D-341 to D-360 · ✅ Complete
D2: Stimming & Repetitive
20 techniques · D-361 to D-380 · ✅ Complete
D3: Aggression Toward Others
20 techniques · D-381 to D-400 · ✅ Complete
D4: Self-Injurious Behaviour
15 techniques · D-401 to D-415 · ✅ Complete
D5: Other Challenging Behaviours
25 techniques · D-416 to D-440 · ✅ Complete
D6: Attention & Sleep
10 techniques · D-441 to D-450 · ✅ Complete
GPT-OS® Clinical Support
Access Pinnacle Blooms' AI-powered clinical decision support for real-time protocol guidance, individualised recommendations, and case consultation across all 110 Domain D techniques.