
Community Navigation
40 evidence-based interventions for children with autism — equipping them to move through shops, temples, parks, airports, restaurants, and every corner of the real world. Subdomain J1 | Domain J: Community & Independence | Pinnacle Blooms Network®
Subdomain J1
40 Techniques
Level I Evidence

Why Community Navigation Is the Hardest Domain
The World Wasn't Designed for ASD Brains. So We Prepare ASD Brains for the World.
Every skill built across Domains A–I — sensory regulation, communication, social interaction, executive function, motor skills, emotional control — was building toward this moment: leaving the controlled environments of home, school, and therapy, and entering the uncontrolled community. Shops, temples, parks, pools, theatres, airports, salons. Places that don't accommodate, don't slow down, and don't adjust their sensory profile for one child.
Community navigation is the field test of every skill learned in every domain. It is the most complex, most demanding, and most important frontier in the autism intervention journey.
Sensory Unpredictability
Community spaces are UNPREDICTABLE. A shop might suddenly play loud music. A market might have an unexpected smell. A state of heightened vigilance that is exhausting.
Social Complexity
Community settings have UNWRITTEN social rules: voice volume in a library, queue behaviour, greeting shopkeepers, sitting still in a movie — each venue has its own unspoken social code.
Executive Demand
Community navigation requires SUSTAINED executive function: following a plan, inhibiting impulses, managing time, switching between activities — all simultaneously, in an unfamiliar environment.
Duration Uncertainty
"How long will this take?" At home, the visual schedule answers. In the community, queues are unpredictable, appointments run late, traffic delays return home. Uncertainty → anticipatory anxiety.

Section 1 of 4
Shopping & Services
Section 1: Shopping & Services
Cards 01–08 cover the most frequent and functionally critical community environments — stores, grocery shops, queues, restaurants, places of worship, medical appointments, the dentist, and the hair salon. These are the settings families navigate every single week.
Store Visits & Shopping Behaviour (J-841, J-842)
Visual overload, sensory triggers, impulse management, and purposeful participation in the shopping environment.
Grocery Shopping (J-843)
The community navigation training ground — predictable layout, repetition, and meaningful participation.
Waiting in Lines (J-844)
The universal community challenge — PFC endurance with no visible finish line.
Restaurant, Temple, Medical & Salon (J-845–J-851)
Behavioural expectations, sensory preparation, and structured engagement across every service setting.

J-841 + J-842: Store Visits & Shopping Behaviour
Paired Card
Level I Evidence
The shop presents a perfect storm: visual overload (products everywhere), auditory input (music, announcements, other shoppers), olfactory intensity (cleaning products, food aisles, cosmetics), tactile temptation (EVERYTHING within reach), and social demand (navigating other shoppers, interacting with staff). Shops are designed by marketing science to overwhelm executive function — the typical adult's PFC barely manages a shopping trip without impulse purchases. The ASD child's PFC is simultaneously fighting: sensory overload + impulse control + social navigation + following the parent + waiting in the checkout queue.
What You'll Learn — J-841: Store Visits
- Social story + visual shopping list (child participates in making it)
- Sensory preparation: headphones, fidget in pocket
- Duration limit: "We're buying 5 things, then leaving"
- Store jobs: child carries basket, finds items from list — PURPOSE reduces aimless anxiety
- Indian shops: kirana (familiar, quick) → supermarket → street market (maximum sensory)
What You'll Learn — J-842: Shopping Behaviour
- "Walking feet, looking eyes, hands in pockets" rule
- Impulse management: "Today we buy what's on the list. You choose ONE extra."
- Queue waiting: fidget, countdown, first-then ("FIRST we pay, THEN car")
- Staff interaction: brief, scripted, supported ("Excuse me, where is...?")
Evidence:📊 Level I — Community-based social skill intervention. NCAEP 2020 | PMC10955541
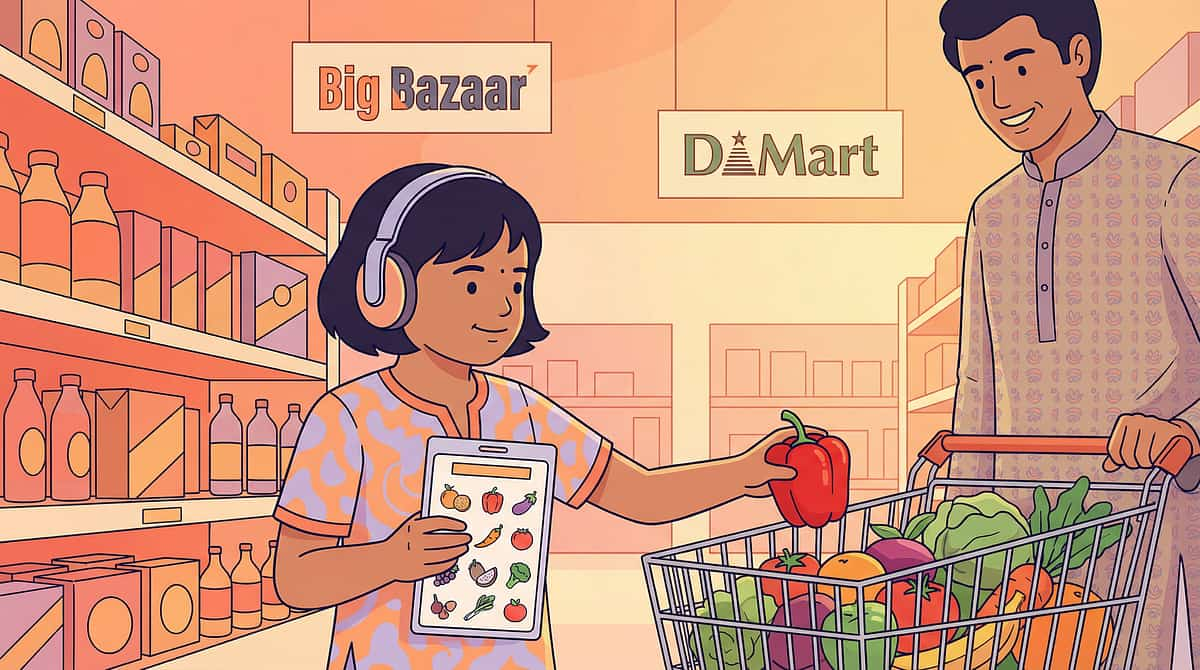
J-843: Grocery Shopping
Dedicated Card
Level I Evidence
Grocery shopping is the most frequent community outing for most families — weekly or more. And that frequency is its greatest therapeutic asset. Grocery stores offer a systematic layout (aisles = predictable), repetitive visits (familiarity builds over time), and a practical purpose that allows the child to participate meaningfully. The combination of predictability + repetition + purpose makes grocery shopping the ideal community skill development training ground.
1
Carry the List
Child holds picture grocery list — visual mission, sense of purpose and role.
2
Find the Items
Child locates items from list — decision-making, aisle navigation, visual scanning.
3
Place in Cart
Child places items in cart — functional motor + participatory role in family task.
4
Wait & Pay
Checkout queue: fidget, countdown, first-then. Gradual progression to assisted payment.
5
Carry the Bag
Child carries one bag to car — completion of the task, proprioceptive input, pride in contribution.
Sensory preparation matters: map which aisles to avoid (cleaning products = olfactory overload), time visits for early morning (quieter), and apply familiar tools — headphones in louder stores. Indian context: vegetable market (open air, sensory intense but brief) vs. BigBazaar/DMart (large format, air-conditioned, structured).

J-844: Waiting in Lines
Dedicated Card
Level I Evidence
The universal community challenge. Every community setting has a queue: billing counter, ticket window, restaurant host, bank, post office, temple darshan, doctor reception. Waiting requires standing still, tolerating proximity to strangers, managing boredom, inhibiting impulses, and tolerating the uncertainty of duration — for an unknown amount of time. The PFC must maintain inhibition for an indefinite period. Unknown endpoint → amygdala escalation over time. The longer the wait, the harder the inhibition, the more likely the meltdown. Waiting is a PFC endurance test with no visible finish line.
The Waiting Kit — Always Carry
- Fidget tool (pocket-sized, quiet)
- Small preferred toy or activity
- Phone/tablet with preferred video (last resort)
- Preferred snack
- Visual "we are number X" card for numbered queues
Strategies That Work
- Let the child sit if possible — standing adds motor demand to cognitive demand
- Counting game, I-spy, song while waiting
- Progress visualization: numbered queues = visible finish line
- Indian queues: temple, government offices, hospitals — often long and unpredictable. ALWAYS carry the waiting kit.

J-845: Restaurant Behaviour
Dedicated Card
Level I Evidence
Restaurant behaviour requires the child to monitor multiple simultaneous social rules — voice volume (moderate, not loud), body position (seated, not wandering), eating behaviour (utensils, mess management), social interaction (waiter, other diners), and time management (meal has a beginning, middle, and end). Each rule requires PFC monitoring. The rules are implicit — nobody posts them on the wall.
Visual Restaurant Rules
Sit in chair · Use inside voice · Eat your food · Wait nicely. Review the social story before entering — "When we go to a restaurant, we..."
Ordering Skills
Practice at home: "I would like [item] please." Use visual menu if available. Parent orders if child can't yet — no pressure on this skill until communication is ready.
Waiting for Food
Dedicated restaurant activity bag (different from other bags — build the association). Familiar food ordered — no pressure to try new items during community visits.
Leaving Routine
"When we finish eating, we pay and go to the car." Clear endpoint. Older children can place the tip — functional maths and social participation.

J-846 + J-847: Temple Behaviour & Religious Services
Paired Card
Level I Evidence
Religious participation presents a unique challenge: specific motor sequences (folding hands, bowing, sitting cross-legged) must be executed simultaneously with inhibition (quiet, still, respectful) and sensory tolerance (incense, bells, chanting). The child must execute behavioural sequences while managing sensory overload — a genuine dual demand on the nervous system.
J-846: Temple Behaviour
- Visual sequence: enter → shoes off → queue → darshan → prasad → circle → exit
- Practice folding hands at home before visit
- Sit-or-stand practice for duration tolerance
- Sensory protection: earplugs for bells during aarti
- Gradual exposure: attend briefly → build duration over visits
J-847: Religious Services
- Social story specific to the service (puja, mass, namaaz, ardas)
- Duration preparation — "We stay for 20 minutes, then we can go"
- Participation grading: attend part, not all, and build from there
- Quiet activity for longer services
- Indian religious diversity: each faith community has unique sensory profile and expectations — prepare SPECIFICALLY for each

J-848 + J-849: Waiting Rooms & Doctor Office Behaviour
Paired Card
Level I Evidence
Medical visits combine sustained inhibition in a novel environment with the challenge of allowing physical touch by an unfamiliar person. The waiting room brings sick children, unfamiliar toys, and olfactory triggers. The examination demands following rapid verbal instructions, tolerating uncomfortable procedures, and communicating symptoms — all while managing a high-anxiety context.
Waiting Room Strategies
- Dedicated medical waiting bag (different from other bags — builds the association)
- Sit in less crowded area of the waiting room
- Visual timer for estimated wait
- First-Then: "FIRST doctor, THEN [preferred reward]"
Doctor Office Behaviour
- Visual sequence: sit → doctor talks → stethoscope → ears → mouth → done
- Practice compliance at home with play doctor kit
- Communication card: "It hurts here" with body picture diagram
Indian Context
- Government hospital: long waits, crowded — extended preparation required
- Private clinic: shorter wait, calmer — good starting point for first medical visits
- Prepare DIFFERENTLY for each setting

J-850: Dentist Office Behaviour
Dedicated Card
Level I Evidence
The oral cavity is the highest sensitivity zone in the human body — with more cortical representation than almost any comparable area. Instruments in the mouth trigger the gag reflex (brainstem), tactile defensiveness (somatosensory cortex), and pain anticipation anxiety (amygdala). The child must inhibit every instinct to close the mouth and pull away. This is one of the most neurologically demanding community experiences on this entire subdomain.
The Tell-Show-Do method is essential: the dentist TELLS what's next, SHOWS the tool, then DOES the procedure — no surprises. Give the child a hand-raise signal meaning "stop" — this grants CONTROL, which dramatically reduces anxiety. At home, practice with an electric toothbrush for vibration familiarity and mouth-open exercises. Desensitisation at home is what makes the dental chair possible.

J-851: Haircut Salon
Dedicated Card
Level I Evidence
For many ASD children, haircuts are the #1 most feared community activity. Scissors near ears. Buzzer vibrating against skull. Cape around neck — a tactile restriction. A stranger touching the head. Water sprayed on hair. Mirror reflecting an unfamiliar appearance mid-cut. The haircut combines tactile hypersensitivity (head/neck), close-range auditory (scissors clicking beside ear, buzzer humming against skull via bone conduction), visual distortion (watching yourself change), and proprioceptive restriction — all simultaneously, all in a confined chair.
1
Home Desensitisation
Practice at home: comb through hair, touch around ears, cape on shoulders, buzzer sound from phone. Build tolerance before any salon visit.
2
Gradual Salon Exposure
First visit: sit in chair only. Second: cape on. Third: 3 snips. Fourth: 10 snips. Build to full cut over multiple sessions — no rush.
3
Salon Selection
Quiet salon, first appointment of the day (no other clients), ASD-experienced barber. Indian neighbourhood barber is often ideal — familiar, flexible, willing to go slowly and take breaks.
4
During the Cut
Headphones block buzzer. Tablet provides distraction. Parent in sight at all times. Child on parent's lap if needed — this is valid and therapeutic, not a regression.
Section 2 of 4
Community Spaces
Section 2: Community Spaces
Cards 09–16 cover the wider community — banks, post offices, libraries, cinemas, zoos, museums, amusement parks, and outdoor play spaces. These environments range from the sensory-minimal (library) to the sensory-maximal (amusement park), and each teaches a different constellation of community skills.
Functional Life Skill Spaces
Bank (J-852), Post Office (J-853) — transaction skills, queue management, adult environment navigation for older children and adolescents.
Low-Sensory Gateway Spaces
Library (J-854) — the most ASD-friendly community space. Success here builds confidence for harder environments.
High-Sensory Leisure Spaces
Movie Theater (J-855), Zoo (J-856), Museum (J-857), Amusement Park (J-858) — preparation and graded exposure are essential.
Daily Community Spaces
Park (J-859) and Playground (J-860) — where all developmental domains converge in unstructured, real-world application every single day.
J-852: Bank Visits & J-853: Post Office Visits
Dedicated Cards — Functional Life Skills
Level I Evidence
For older children and adolescents, bank and post office visits are functional life skills — not just community outings. Both environments teach a transferable community transaction sequence: enter → identify service → queue → interact with staff → complete transaction → collect receipt → leave. Mastering the post office generalises directly to the bank, telecom office, and government service environments. The skills compound.
J-852: Bank Visits
- Bank social story + visual sequence of the full visit
- Practice counter interaction at home through role-play
- Token system and form-filling support (pre-filled where possible)
- Progressive skill: accompany → participate → assisted independent → independent
- Indian banking: UPI/digital payments are ASD-friendlier — predictable, minimal social interaction
J-853: Post Office Visits
- Post office social story + visual sequence
- Practice at home: writing address, licking stamp, handing envelope
- Purpose-led visit: "We are sending a birthday card to cousin — YOU are posting it"
- Role-play the counter interaction before arriving
- Indian post office: neighbourhood post office as low-stakes first practice, Speed Post for simpler transactions

J-854: Library Visits
Dedicated Card
Level I Evidence
The library is potentially the most ASD-friendly community space that exists. Quiet. Structured. Predictable layout. Books on special interests freely available. Rules that are explicit (whisper, no running, return books). Low sensory load (quiet, often dim lighting, minimal olfactory triggers), high structure, interest-based engagement, and minimal social demand. The library can be the gateway community experience — success here builds the confidence and nervous system regulation to tackle harder environments.
Introduction Strategy
Social story before first visit. Visit during the quietest hours. Brief the librarian — they are natural allies and can be enormously helpful. Issue the child their own library card — that ownership matters.
Library Behaviour
Whisper voice practice at home. Walking feet only. Sit to read — model and practise. Return books to the cart independently as a purposeful task.
Library as Regulation Space
When the world is overwhelming, the library is a REFUGE. Teach the child to name it as a safe space — "Can we go to the library?" is a powerful self-advocacy skill.

J-855: Movie Theater & J-856: Zoo Visits
Dedicated Cards
Level I Evidence
J-855: Movie Theater
Dark room. Loud sound system reaching 85–100 dB. Giant screen. Strangers sitting close. No pause button. Movie theatres are sensory extremes — but with preparation, many children learn to enjoy them.
- First movie: choose FAMILIAR title already watched at home
- Aisle seat (escape route) + noise-cancelling headphones + earplugs
- Arrive AFTER previews — the loudest part of any cinema visit
- Parent reassures: "We can leave any time" — reduces anticipatory anxiety
- Gradual: watch 30 min → leave. Next time: 45 min. Build duration slowly.
- Indian cinema: check PVR/INOX sensory-friendly screenings, matinee for smaller crowds
J-856: Zoo Visits
Outdoor, walking-intensive, animal encounters. For children with animal interests, the reward system is engaged throughout — producing better community skill generalisation than non-interest outings.
- Zoo preparation: visual map, duration plan (5–6 exhibits only, not the whole zoo), rest stops, snack schedule, sun protection
- Zoo behaviour: stay on path, don't touch barriers, quiet near animals
- Interest leverage: "We'll see the elephants AFTER we walk past the birds nicely"
- Indian zoos: early morning visit — cooler, less crowded. Avoid weekends.

J-857: Museum Visits & J-858: Amusement Parks
Dedicated Cards
Level I Evidence
J-857: Museum Visits
For visual-spatial learners, museums are paradise. For tactile-seeking children, a room full of fascinating objects they CANNOT touch is a PFC endurance test. The key is matching exhibit type to sensory profile.
- Preparation: website preview, exhibit map, choose 3–4 galleries maximum
- "Look with eyes, not hands" rule + fidget in pocket (redirects touch impulse)
- Interactive science centres: hands-on exhibits = ASD-IDEAL (touch is encouraged)
- Duration: 45–60 minutes initially — leave while it's still positive
- Indian museums: Salar Jung, National Museum, Birla Planetarium, regional science centres with interactive sections
J-858: Amusement Parks
Maximum everything: noise, lights, crowds, rides, queues, heat. Every sensory channel at PEAK simultaneously for hours. Some ASD children love specific rides (vestibular seekers). Others cannot tolerate the environment at all. Know your child's profile first.
- Weekday visit (less crowd), map with chosen rides (max 5), headphones, sunglasses
- Frequent rest breaks in quiet areas — build these into the plan, not as reactive breaks
- Disability access: accessibility passes to skip queues — ESSENTIAL for ASD children
- Ride selection: match to sensory profile — vestibular seekers vs. sensory avoiders need different ride lists
- Indian parks: Wonderla, Imagica, EsselWorld — check accessibility policies

J-859 + J-860: Park Visits & Playground Behaviour
Paired Card
Level I Evidence
Parks and playgrounds are the daily community space — the location where all developmental domains converge in unstructured, real-world application. Motor skills (climbing, swinging, sliding), social skills (turn-taking, group play), sensory processing (vestibular from swings, proprioceptive from climbing), and communication (requesting turns, joining play) all activate simultaneously. The playground is where every domain is tested without a therapist, a schedule, or a controlled environment.
J-859: Park Visits
- Timing: visit during quieter hours — morning or evening in India — to reduce social stress during early skill building
- Choose a REGULAR park — familiarity builds comfort and predictability
- Parent as facilitator (not director) — provide scaffolding without overriding the child's autonomy
- Transition preparation: "We leave when the visual timer finishes"
J-860: Playground Behaviour
- Turn-taking for swings and slide — visual wait card helps ("It's my turn after them")
- "Can I play?" script — practised, role-played, then supported in real context
- Safety rules: hold on, wait your turn, feet first on slide
- Managing when equipment is occupied: "I'm waiting — that's okay"
- Parent identifies potential play partners and facilitates introductions gently

Section 3 of 4
Outings & Travel
Section 3: Outings & Travel
Cards 17–22 move into the wider world of outings and travel — water environments, social visits, air and ground transport, long car journeys, and overnight stays. These cards deal with the most extended, least predictable, and most demanding community experiences. Preparation is everything here.
Water Environments
Beach (J-861) and Pool (J-862) — therapeutic sensory input with critical water safety emphasis.
Social Visits
Extended family (J-863) and friend house visits (J-864) — novel environments with layered social demands.
Air Travel
Airplane (J-865) — sensory capsule at 35,000 feet with no exit for 2–12 hours.
Ground Transport
Train (J-866), Bus (J-867), Long Car (J-868) — public transport skills and road trip strategies.
Overnight Stays
Hotel stays (J-869) and new place adjustment (J-870) — sleep, routine, and environmental adaptation.

J-861 + J-862: Beach Visits & Pool Visits
Paired Card
Level I Evidence
Water environments provide powerful sensory input — hydrostatic pressure (whole-body proprioceptive input, deeply calming for many), vestibular challenge (waves, floating), temperature input, and continuous tactile stimulation. For sensory seekers, water is therapeutic. For sensory avoiders, it is overwhelming. Water environments tend to be binary — children strongly love them or strongly fear them. Neither response is wrong; both require different preparation strategies.
⚠️Water Safety Is Paramount: ASD children are at significantly HIGHER drowning risk — wandering behavior, attraction to water, and reduced danger perception create a critical safety profile. NEVER leave unsupervised near any water. Water safety skills (floating, edge-holding) are the FIRST skills to teach.
J-861: Beach Visits
- Gradual approach: observe → feet in water → wading → playing in waves
- Sand desensitisation: touch dry sand first, then wet sand, then walk on it
- Sun protection plan prepared before arrival (not applied at beach = meltdown trigger)
- Quiet beach section away from main crowd for early visits
- Never forced — respect a strong "no" and try again another time
J-862: Pool Visits
- Temperature preparation — test with hands before entering
- Gradual entry using steps (not jumping in)
- Flotation aids during learning phase
- Build comfort with face wet slowly — no surprises
- Pool rules as visual card: walk, no pushing, stay in shallow end

J-863 + J-864: Extended Family Visits & Friend House Visits
Paired Card
Level I Evidence
Visiting someone else's home combines an unfamiliar environment (sensory recalibration of a novel space) with layered social expectations: greeting, conversation, playing with other children, eating offered food (which may not be preferred), and tolerating an uncertain duration. Other people's houses have other people's rules — and the child must navigate social expectations in an unfamiliar sensory environment simultaneously. Double cognitive load.
J-863: Extended Family Visits
Preparation before arriving: who's there (photos help), what to expect, how long we'll stay. Greeting script practised at home. Quiet space identified in advance. Familiar snack packed from home. Duration limit agreed and communicated: "We'll stay for one hour." Indian joint family visits: multiple relatives, unexpected questions, food pressure — prepare specifically for this social gauntlet.
J-864: Friend House Visits
Play plan prepared: what will they do? Sharing preparation addressed beforehand. House rules briefed by parent. Parent present (or nearby) initially, fading involvement gradually. Different cultural practices at friend's home — food, routines, customs — briefed as part of visit preparation.
Leaving Routine — Both Visits
"When Amma says it's time, we say bye and go." Clear, practised, predictable endpoint. Plan for decompression time after visit — community participation is regulating work and the nervous system needs recovery time.

J-865: Airplane Travel
Dedicated Card
Level I Evidence
Airplane travel is a confined sensory capsule at 35,000 feet with no escape. Constant engine noise at 80–85 dB. Ear pressure changes during altitude shifts (painful for sensory-sensitive children). Confined seating for 2–12 hours. Shared armrests. Seatbelt requirement. Unpredictable turbulence. Unfamiliar food. And all of this is preceded by airport navigation: check-in, security, gate waiting, and boarding. Comprehensive preparation is not optional — it is the entire intervention.
Airport Preparation
- Social story: check-in → security → gate → board → seat → takeoff → fly → land → exit
- Visit airport beforehand if possible — just to walk through, no flight required
- Airline assistance: request pre-boarding and specific seat selection (window seat = wall to lean on, less social exposure)
- Indian airlines: IndiGo/Air India accessibility services available — request in advance
During the Flight
- Noise-cancelling headphones: ESSENTIAL — the single most important tool for air travel
- Ear pressure management: chewing gum or swallowing during ascent and descent
- Activity bag: tablet loaded with preferred content, snacks, comfort item
- Domestic flights first: IndiGo Chennai–Bangalore is a better first flight than Mumbai–London

J-866 + J-867: Train Travel & Bus Travel
Paired Card
Level I Evidence
Public transport is a daily reality in India — and a critical community independence skill. Train and bus travel involve shared spaces, unpredictable schedules, crowded conditions, and strangers in close proximity. Indian public transport adds its own intensity: extreme crowding during peak hours, heat, open windows carrying wind and dust and horn noise. Metro systems offer the most ASD-friendly entry point — clean, air-conditioned, structured, predictable.
J-866: Train Travel
- Long-distance: lower berth selection (easy exit), familiar bedding from home, visual journey schedule
- Metro: predictable, air-conditioned — the ideal starting point for public transport skill development
- Rajdhani/Shatabdi: premium, less crowded — good stepping stone before general class
- Visual schedule of train journey: departure → travel → arrival → exit
J-867: Bus Travel
- Route familiarity: travel same route repeatedly to build predictability
- Seating strategy: front seats, near door, window for sensory grounding
- Headphones + holding on (proprioceptive grounding during motion)
- Exit preparation: "We get off at the next stop" — give warning, no surprises
- Ticket/card handling as functional skill: Oyster-style metro cards are easier than cash transactions
J-868: Long Car Travel
Dedicated Card
Level I Evidence
Long car travel means 3–12 hours of physical confinement. Indian road trips add: unpredictable road quality, constant horn noise, motion sickness risk, highway dhaba stops with unfamiliar food and toilets, and the duration uncertainty of Indian traffic and road conditions. The child's PFC must manage boredom, regulate behaviour, and sustain itself for hours — a genuine endurance demand that requires deliberate preparation and strategy.
Timing Strategy
Night travel: child sleeps through most of the journey. Early morning departure: cooler, less traffic, cooler temperament. Avoid peak-heat midday starts on long trips.
Activity Rotation
Screen → music → sensory game → snack → nap → screen. Rotate every 30–45 minutes. Monotony is the enemy of regulation on long journeys.
Motion Sickness
Window seat, look outside (not at screen), ginger candy, stop immediately if nausea signals appear. Vestibular-visual conflict worsens with screen use in a moving vehicle.
Rest Stop Preparation
Highway dhaba stops: toilet visual social story prepared in advance, familiar snack packed (don't rely on dhaba food), Fastag for smooth toll transitions — avoid cash fumbling at tolls.

J-869 + J-870: Hotel Stays & New Place Adjustment
Paired Card
Level I Evidence
Sleeping in an unfamiliar bed in an unfamiliar room. The brain's "first night effect" — where one hemisphere stays more alert in novel environments — is documented in neurotypical adults. In ASD, this effect is likely amplified: poorer sleep quality, increased nighttime waking, possible regression in behaviour. New place adjustment extends beyond hotels to any unfamiliar living space — a grandparent's house, a rental apartment, a relative's home during a family event.
J-869: Hotel Stays
- Bring bedding from home: child's own pillow and blanket — familiar olfactory and tactile anchors
- Maintain EXACT bedtime routine — same sequence, same timing, new location
- Request quiet room: away from elevator, lobby, and pool area
- Bring nightlight and check for sensory triggers (AC noise, curtain light leak)
- Indian hotels: inspect OYO/budget rooms first. Request ground floor. Ask for extra blanket.
J-870: New Place Adjustment
- Systematic exploration upon arrival: room by room, parent as tour guide
- Identify key locations immediately: bathroom, kitchen, sleeping area, exit
- Set up familiar items FIRST: comfort object, bedding, visual schedule posted
- Visual schedule: what happens here, what time, in what order — predictability reconstructed in new environment

Section 4 of 4
Classes, Inclusion & Mastery
Section 4: Classes, Inclusion & Mastery
Cards 23–30 move into the richest territory: structured community classes, sports programs, creative arts, movement therapies, martial arts, summer camps, and the philosophical capstone — community inclusion and public behaviour. These are the domains where participation becomes identity, and where the skills of every preceding card become a way of life.
Structured Community Classes
Community classes (J-871) and sports programs (J-872) — the ideal midpoint between therapy and fully unstructured social interaction, with interest-based motivation.
Creative Arts
Music (J-873) and Art (J-874) — accessing ASD strengths in pattern recognition, detail focus, and systematic processing through structured creative expression.
Movement Therapies
Swimming (J-875) and Dance (J-876) — whole-body sensory-motor activities with profound therapeutic benefit and social synchrony development.
Mastery & Independence
Martial arts (J-877), Summer camps (J-878), Community inclusion (J-879), and Public behaviour (J-880) — the full journey toward autonomous community participation.

J-871: Community Classes & J-872: Sports Programs
Dedicated Cards
Level I Evidence
J-871: Community Classes
Community classes are the gateway to structured social participation outside school. They offer lower social demand than unstructured play (instructor provides structure and rules), higher social exposure than 1:1 therapy (real peers, real group dynamics), and interest-based motivation.
- Class selection: match interest AND sensory tolerance — visit before enrolling
- Talk to instructor about ASD before the first class
- First class: parent present, partial participation fully accepted
- Instructor briefing: one-page child profile with strategies that work
- Indian options: Shiamak dance, art classes, coding classes, yoga (structured, regulated — excellent for ASD)
J-872: Sports Programs
Sports naturally integrate multiple therapeutic domains: motor skills, social skills (teamwork, sportsmanship), emotional regulation (winning and losing), executive function, and sensory regulation through sustained proprioceptive and vestibular input.
- Progression: individual sport first (swimming, running, cycling, martial arts) → paired (badminton, tennis) → team (cricket, football)
- Coach education: ASD awareness, patience with skill acquisition, modified rules if needed
- Competition management: winning/losing social stories prepared in advance
- Indian sports: cricket coaching (universal access), swimming (therapeutic + skill), kabaddi

J-873 + J-874: Music Classes & Art Classes
Paired Card
Level I Evidence
Creative classes access ASD strengths directly. Music engages temporal cortex and cerebellum (rhythm processing), the reward system (melody enjoyment), and bilateral brain engagement (auditory + motor coordination). Art activates parietal cortex (visual-spatial processing), motor cortex (fine motor control), and emotional expression through a nonverbal medium — critically important for children whose feelings exceed their words. Both domains reward pattern recognition, detail focus, and systematic processing.
J-873: Music Classes
- Instrument selection: match interest AND sensory tolerance — keyboard (structured, systematic), drums (deeply proprioceptive), vocals (requires auditory comfort)
- Group vs. individual lessons: individual first, then small group as skills develop
- Music as regulation tool: establish a "calm song" as portable sensory tool
- Indian context: Carnatic/Hindustani music training — highly structured, systematic learning style — an excellent fit for ASD learners
J-874: Art Classes
- Medium exploration: painting, clay, collage, digital art — try several before committing
- Art as communication: "Draw how you feel when you can't find the words"
- Sensory art options: finger painting, textured collage — therapeutic tactile engagement
- Portfolio building: visible evidence of growth builds confidence and identity
- Indian context: Rangoli as art therapy — geometric, pattern-based, highly structured, culturally meaningful

J-875 + J-876: Swimming Lessons & Dance Classes
Paired Card
Level I Evidence
Swimming and dance are whole-body sensory-motor activities with profound therapeutic depth. Swimming provides hydrostatic pressure (proprioceptive — deeply calming), bilateral coordination, breath regulation that improves vagal tone, and water as an intrinsic sensory regulation medium. Dance develops rhythm (cerebellar timing), motor planning (sequencing body movements), imitation (mirror neuron activation), social synchrony (moving WITH others), and heightened body awareness through interoception and proprioception.
⚠️Water Safety: Swimming lessons must begin with safety skills — floating and edge-holding — BEFORE any stroke technique. ASD children must NEVER be unsupervised near water at any stage of skill development.
J-875: Swimming Lessons
- Water comfort progression: feet → wading → chest → floating → swimming — honour each step
- 1:1 instructor initially — group lessons only when water comfort is established
- Safety skills FIRST: floating, edge-holding, roll-to-back — non-negotiable
- Therapeutic swimming: OT-guided aquatic therapy available through Pinnacle network
J-876: Dance Classes
- Movement to music as natural reward — start with free dance before structured choreography
- Structured choreography: predictable sequences are ASD-friendly — repetition builds mastery
- Performance opportunities: recitals build confidence and community belonging
- Indian classical dance: Bharatanatyam — highly structured, systematic learning, deep proprioceptive input, culturally rich — excellent fit for ASD learners
J-877: Martial Arts
Dedicated Card
Level I Evidence
Martial arts may be the single most ASD-optimal structured activity available. Structured, predictable, individually paced, proprioceptively rich, respect-based, and confidence-building. The belt system provides a clear, visible, tangible progression — exactly the kind of external motivation structure that ASD learners thrive with.
Predictable Structure
Every class follows the same format: bow → warm-up → technique → practice → cool-down → bow. No surprises. The brain knows exactly what's coming next.
Individual Progression
Belt system: clear, visual, tangible milestones. The child competes against their own previous performance — not against others. Intrinsically motivating.
Proprioceptive Input
Heavy work throughout — deep joint compression, resistance, and impact. Powerful sensory regulation embedded in every session.
Self-Regulation Curriculum
Emotional control is CORE curriculum in martial arts — bowing, listening, discipline, and respect are explicitly taught skills, not implicit expectations.
Style recommendations: Karate (striking, systematic katas — highly structured), Judo (grappling, deep proprioceptive), Taekwondo (kicking, bilateral coordination). Indian options: karate most accessible across cities, Kalaripayattu (Kerala traditional martial art — deeply proprioceptive and ceremonially structured). Look for instructors with special needs experience and willingness to modify pacing.
Preview of community navigation Therapy Material
Below is a visual preview of community navigation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!

J-878: Summer Camps + J-879 & J-880: Community Inclusion & Public Behaviour
Dedicated + Capstone Paired Cards
Level I Evidence
J-878: Summer Camps
Summer camp is the ultimate community integration test: new environment, new people, new schedule, sustained group activity, peer interaction, and extended independence from primary caregiver — for hours or days at a time. With appropriate support, camp accelerates social development significantly.
- Day camp first → build to residential
- ASD-specific camps: structured, trained staff
- Practice independence skills at home: toileting, eating, dressing without parent
- Daily parent-counsellor communication channel agreed before camp begins
- Indian options: ASD-specific camps in Hyderabad, Bangalore, Mumbai, Chennai — growing rapidly
J-879 + J-880: The Capstone — Inclusion & Public Behaviour
Community inclusion and public behaviour are not the end of the journey — they ARE the journey. Every successful community experience adds to the child's library of "I did it" moments. That library is confidence. That confidence is independence. That independence is life.
- Every child has the RIGHT to be in public spaces — RPwD 2016 enshrines this
- Context-specific rules: library voice, restaurant sitting, shop walking — generalised systematically
- Self-monitoring: "Am I using the right behaviour for this place?"
- Repair when things go wrong: apology, recovery, try again — model this explicitly
- Parent scripts: prepared responses for "What's wrong with your child?" — community education in real time
The formula is always: PREPARE → PROTECT → PARTICIPATE → PROCESS. Every shop visited, every park played in, every temple attended, every plane boarded — each one builds the library of "I did it." That library is confidence. That confidence is independence. That independence is life.