
When they eat fine at home — but the lunchbox comes back untouched. Every. Single. Day.
It's 3:30 PM. You open the lunchbox. The sandwich is still whole. The fruit is untouched. The crackers are still sealed. Everything exactly as you packed it — again. And by the time you get home they're ravenous, cranky, falling apart. You watched them eat a full breakfast. You'll watch them eat a full dinner. But lunch — at school — simply doesn't happen.
E-471 | Domain: FEED-SCHOOL
🍱 School Eating Refusal Support Protocol
"You are not failing. Your child's nervous system is telling you something important about the school environment — and it can be addressed."

You Are Not Alone
The lunchbox coming home full is one of the most-searched parenting concerns in pediatric feeding therapy. Context-specific eating — where a child eats well at home but refuses food at school — affects millions of families worldwide. India's NFHS-5 and Pinnacle Blooms Network® clinical data from 20M+ sessions across 70+ centers confirm school eating refusal as one of the highest-volume feeding concerns presenting to pediatric OT and feeding therapy.
25–35%
Context-Specific Eating
of school-age children with neurodevelopmental differences experience context-specific eating difficulties
40M
Children in India
have some degree of feeding challenge — placing school eating refusal among the top 5 pediatric feeding concerns
80%+
Autism + Sensory
of children with autism experience sensory processing difficulties that directly affect eating behaviour, including environment-dependent refusal
You are among millions of families navigating this exact challenge. The lunchbox is not coming home full because your child is choosing to be difficult. Something specific about the school environment is creating a neurological barrier to eating.
What's Happening in Your Child's Brain
The Clinical Mechanism
When a child encounters an overwhelming environment — a cafeteria with 80–90 decibels of ambient noise, visual chaos, unpredictable social dynamics, and time pressure — the sympathetic nervous system activates a fight-or-flight response. Digestion is physiologically suppressed, appetite signals are overridden, the vagal brake disengages, and cortisol rises. This is not "refusing to eat." This is the nervous system doing exactly what it evolved to do in threatening environments.
Why the Cafeteria Is "Too Much"
- 🔊Auditory overwhelm: School cafeterias regularly exceed 80–90 dB — equivalent to a lawnmower. Neurologically equivalent to a fire alarm for sensitive children.
- 👁️Visual chaos: Dozens of bodies moving, colours, trays — the visual cortex is overwhelmed, leaving no processing capacity for food.
- ⏱️Time pressure anxiety: "I won't have enough time" triggers the same physiological response as a real threat.
- 👥Social surveillance: Fear of eating "wrong" in front of peers activates the same neural circuits as physical danger.
This is not defiance. This is neuroscience.

Where School Eating Refusal Sits in Development
The peak emergence window for school eating refusal is ages 5–9 years — exactly when children transition from home-based eating to full school participation. For children with sensory differences, anxiety, autism spectrum traits, or feeding challenges, this transition is the highest-risk period for context-specific refusal to emerge.
Birth–12m
Oral motor foundations established
1–3 years
Expanding food variety begins at home
3–5 years
Social eating introduction
5–9 years ◄ PEAK ZONE ►
School eating refusal peak — cafeteria transition highest-risk period
9–12 years
Building toward environmental flexibility
What commonly co-occurs: Sensory Processing Differences, Anxiety, Autism Spectrum Disorder, ADHD, and Selective/Avoidant Eating patterns. This challenge sits within the WHO Nurturing Care Framework's Early Learning and Responsive Caregiving components — both identified as modifiable through targeted parent-led intervention.

The Evidence Behind These Materials
⚖️ Evidence Grade: Level II
Systematic Reviews + RCTs + Multi-Centre Clinical Data
Clinically validated. Home-applicable. Parent-proven. These 9 materials are not random products — each addresses a specific, research-identified mechanism that blocks eating in the school environment.
Study | Finding | Relevance to E-471 | |
PRISMA Systematic Review, Children (2024) — PMC11506176 | 16 studies confirm sensory integration as evidence-based practice for ASD | Headphones, calming tools, gradual exposure — directly validated | |
Meta-analysis, World J Clin Cases (2024) — PMC10955541 | SI therapy promotes adaptive behaviour across 24 studies | Environmental modification, bento logistics, familiar utensils | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory interventions achieve significant outcomes in Indian pediatric population | All 9 materials are home/school-applicable | |
NCAEP Evidence-Based Practices (2020) | Visual supports, gradual exposure, social narratives classified as EBP for autism | Visual timers, social story cards, gradual exposure — directly validated |
📞FREE Helpline: 9100 181 181 — speak to a feeding therapist today. Available 24×7 in 16 languages.
The Technique: What It Is
🍱 School Eating Refusal Support Protocol
Also known as: The Lunchbox Bridge
Formal Definition: School eating refusal describes a pattern in which children who eat adequately at home consistently refuse or are unable to eat in the school environment. This is a context-specific eating difficulty — the child's ability to eat is intact; the school environment creates barriers that override that ability.
Plain English: Your child is not "choosing not to eat." Their nervous system — responding to sensory overwhelm, social anxiety, time pressure, or environmental unpredictability — has blocked the physiological capacity to eat in that specific context. The evidence-based response is to identify the specific barrier and remove or accommodate it, not to push through it.
🎯 Domain
Feeding Therapy / OT / ABA
👤 Age Band
4–12 years
⏱️ Session
Daily (school lunch)
📅 Frequency
Every school day
🏆 Outcome
School Eating Readiness Index

The Consortium Behind These Materials
School eating refusal crosses therapy boundaries because the school cafeteria doesn't recognize therapy types. A child overwhelmed by noise needs OT. A child frozen by anxiety needs ABA + psychology. A child whose food changes temperature needs a feeding therapist's logistics. The Pinnacle consortium deploys all five disciplines simultaneously through FusionModule™.
Occupational Therapist (OT) — Primary Lead
Addresses sensory processing differences, environmental modification, mealtime positioning, tool selection, and gradual desensitisation of cafeteria stimuli. OT assesses the sensory profile and prescribes specific materials from the 9 listed.
Feeding Therapist (OT/SLP Specialty)
Addresses food texture preferences, temperature sensitivity, lunchbox packing strategies, and the mealtime motor sequence. Evaluates whether food logistics are the primary barrier.
ABA Therapist / BCBA
Designs gradual exposure hierarchy, reinforcement schedules, data collection protocols, and consistency between home and school environments.
Special Educator (SpEd)
Creates social stories, manages school-teacher communication, formal accommodation documentation (IEP/504 equivalent), and classroom-based eating support.
Child Psychologist / NeuroDev Pediatrician
Addresses underlying anxiety evaluation, school-based mental health coordination, medical contraindications, and formal diagnostic workup if needed.
Precision Targets: What These 9 Materials Address
Target | What you'll see at Week 2 | What you'll see at Week 8 | |
Successful eating | 3–5 bites at school | Full lunch consumed | |
Reduced anxiety | Less resistance to packing lunchbox | Willingly approaches cafeteria | |
Tool independence | Uses headphones with prompting | Independently manages accommodation | |
Parent-school alignment | First accommodation conversation complete | Formal plan in place |

9 Materials That Bridge Home and School Eating
Each material targets a specific, identified barrier. Match the material to your child's barrier. Below is your complete sourced, priced, ready-to-implement guide.
Noise-Reducing Headphones / Ear Defenders
📍 Sensory Supports (Auditory) | 💰 ₹500–₹3,000 | 🎯 Cafeteria auditory overwhelm
Insulated Bento-Style Lunchbox
📍 Feeding Logistics Equipment | 💰 ₹800–₹2,500 | 🎯 Food temperature change, texture degradation
Visual Timer
📍 Visual Schedule Materials | 💰 ₹300–₹1,500 | 🎯 Time pressure anxiety, freeze response
Preferred Utensils and Familiar Eating Tools
📍 Feeding Logistics / Sensory Comfort | 💰 ₹200–₹800 | 🎯 Unfamiliarity friction
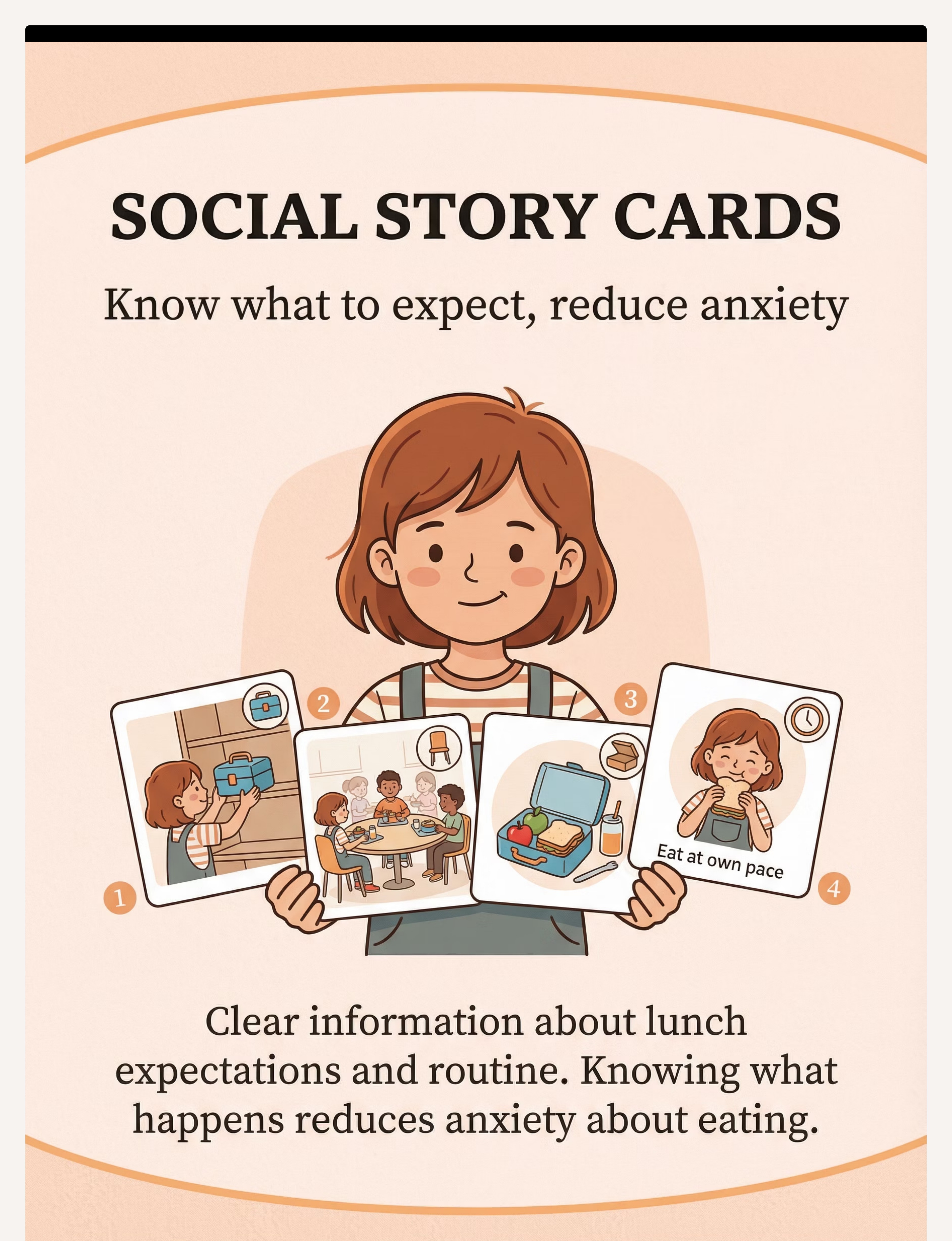
Social Story Cards / Visual Script
📍 Social Narrative Tools | 💰 ₹0–₹1,500 | 🎯 Predictability anxiety, unwritten social rules
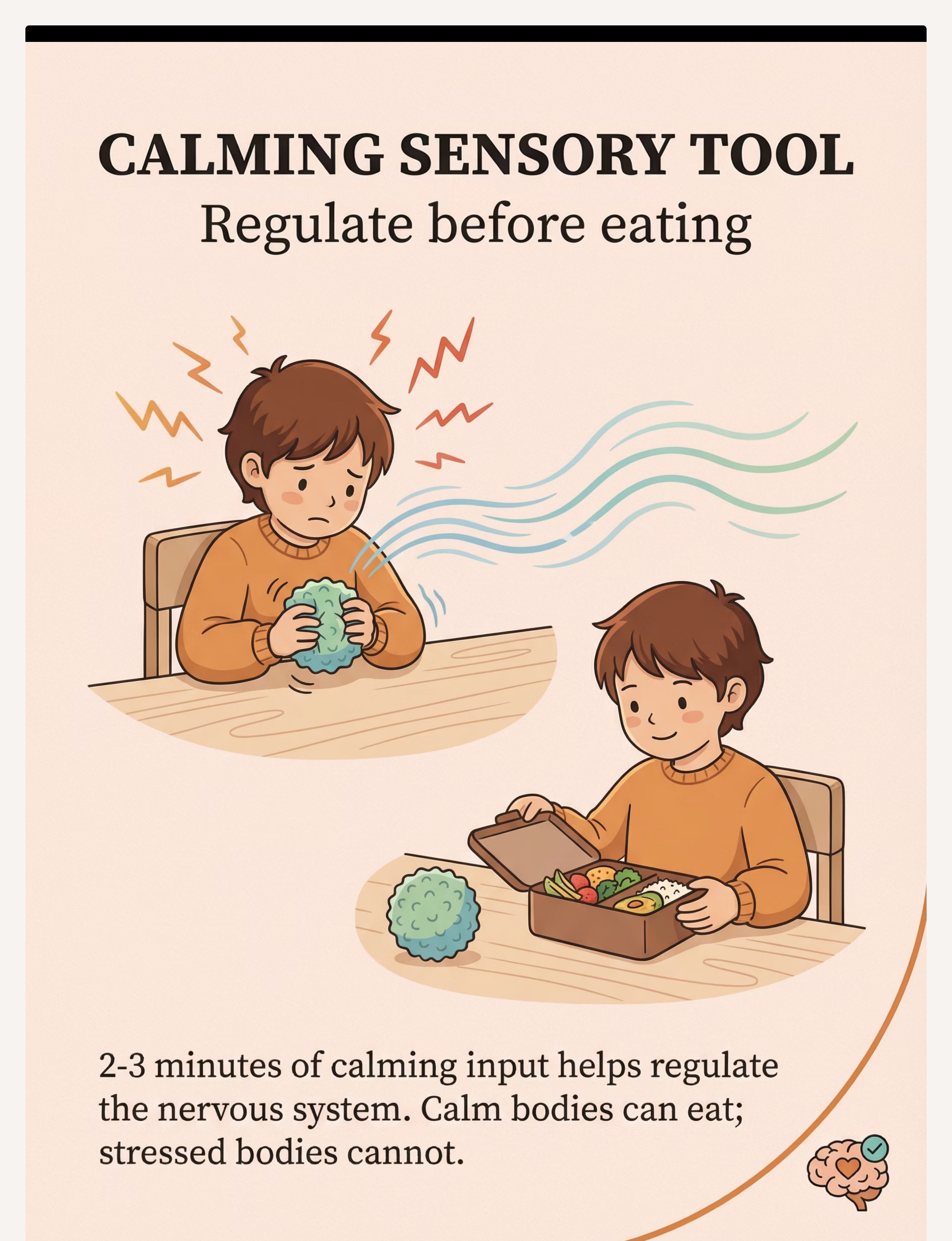
Calming Sensory Tool for Pre-Meal Regulation
📍 Calming Sensory Tools | 💰 ₹100–₹800 | 🎯 Dysregulation arriving at lunch from morning demands
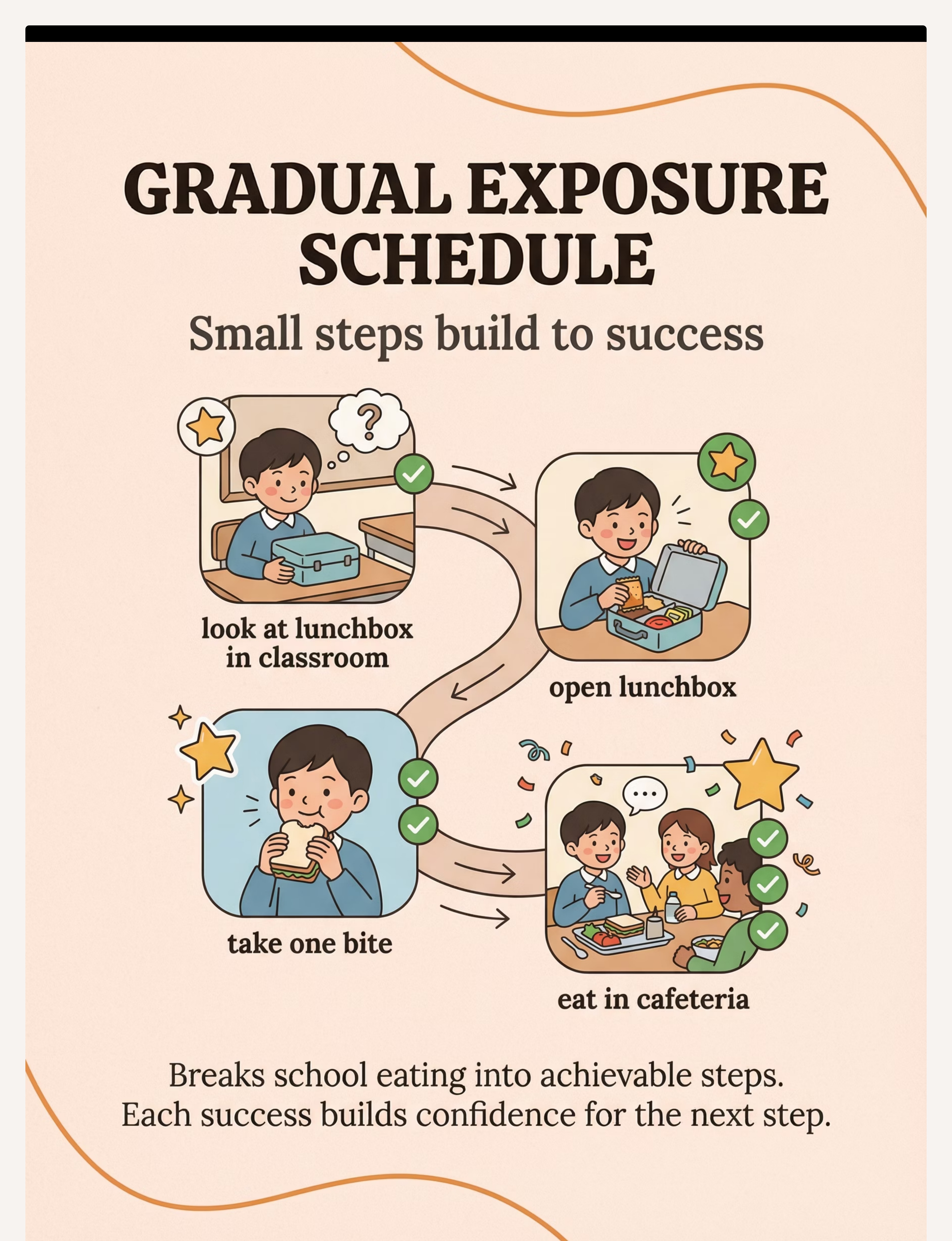
Gradual Exposure Photo Schedule
📍 Visual Schedule / Gradual Desensitisation | 💰 ₹200–₹800 | 🎯 Anxiety-driven avoidance gap
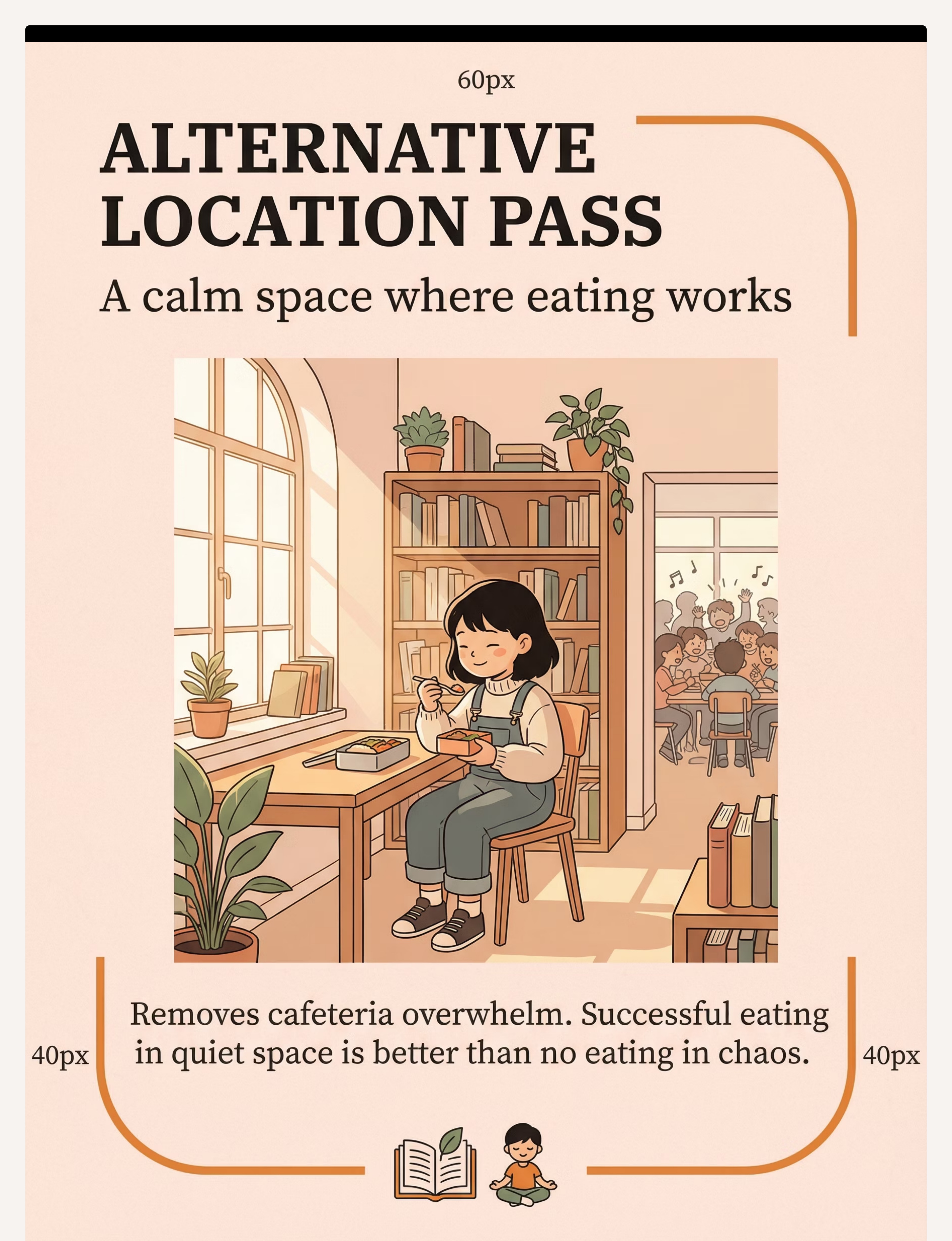
Alternative Eating Location Pass
📍 Environmental Accommodation Tools | 💰 ₹0 | 🎯 Cafeteria environment exceeds tolerance
Home-to-School Transition Object
📍 Transition Objects / Comfort Items | 💰 ₹0–₹300 | 🎯 Psychological distance between home and school

Material 1: Noise-Reducing Headphones
Why It Works
School cafeterias are among the loudest environments children encounter. For children with auditory sensitivities, this noise activates fight-or-flight and physiologically blocks digestion. Headphones reduce auditory input to manageable levels, allowing the nervous system to calm enough for eating to occur.
What to Look For
Child-sized, lightweight, comfortable ear cup padding, NRR 22–27 dB, foldable for lunchbox storage. Options with passive noise reduction (no electronics needed for basic function).
School Coordination Note
Most schools readily accommodate sensory headphones when framed as a "sensory regulation tool" — not a medical device. Normalize with peers: "these help me eat better."
DIY / Zero-Cost Alternative
Soft foam earplugs (₹20–50 at pharmacy) as a discreet alternative. Test at home first for comfort. Not as effective for severe sensitivity but adequate for moderate cases.
🛒 Search on Amazon.in: children ear defenders noise reducing headphones
Material 2: Insulated Bento Lunchbox
Why It Works
Food packed at 7 AM may be soggy, room-temperature, or touching other foods by 12 PM — creating a sensory barrier for children with texture/temperature sensitivities. Insulated compartment boxes maintain food temperature and prevent mixing, keeping foods as close to home-presentation as possible.
What to Look For
Genuine thermal insulation (test: pack food, wait 5 hours, check temp), 3–5 separate compartments with leakproof seals, child-openable latches, BPA-free food-safe materials, fits in standard school bag.
DIY / Zero-Cost Alternative
Separate small stainless containers with individual lids inside a larger bag. Wrap hot-food containers in newspaper insulation. ₹0 if you already have separate containers.
🛒 Search on Amazon.in: insulated bento lunchbox kids compartments thermal

Materials 3 & 4: Visual Timer + Familiar Utensils
⏱️ Material 3 — Visual Timer
Why it works: Abstract time ("you have 20 minutes") creates anxiety in children who cannot intuitively track time. A visual timer transforms invisible time into concrete, visible countdown — reducing uncertainty and the freeze response. Can also be used therapeutically: "You only need to try eating for 10 minutes."
What to look for: Visual time representation — shrinking red disc (Time Timer style) or sand timer. Silent or near-silent. Portable, lunchbox-sized if possible.
DIY: Sand timer from craft store (₹50–100). Draw a clock face showing "lunch ends here." 💰 ₹300–₹1,500
🥄 Material 4 — Familiar Utensils
Why it works: A child who always eats with a specific fork at home may experience just enough friction from unfamiliar school utensils to tip from reluctant eating to complete refusal. Familiar utensils carry the psychological safety of the home eating context.
What to look for: Duplicate set of home-used utensils. Child's preferred fork, spoon, cup. Matching the handle grip, weight, and material they use successfully at home.
DIY: Pack home cutlery in a small labelled pouch in the lunchbox. Already in your kitchen — ₹0. 💰 ₹200–₹800
Material 5: Social Story Cards / Visual Script
Why It Works
Children with anxiety or autism experience "unwritten rule" overwhelm at school lunch: Where do I sit? What do I do? What's expected? Social story cards provide a visual, concrete sequence of what happens during school lunch, removing uncertainty and freeing cognitive resources for eating.
What to Look For
Personalized cards using photos of the child's actual school cafeteria/lunch space. Sequence: pack → carry → find seat → open lunchbox → eat → pack up. Laminated for durability.
DIY / Zero-Cost
Photograph your child's actual school lunch sequence. Print and laminate at any print shop (₹30–50 for 4 cards). Ring-bind and place in lunchbox. Personalised photos outperform commercial versions — your child's brain recognises their own environment.
💰 ₹0 (DIY) to ₹1,500 (commercial) | 🛒 Search: social story cards visual schedule laminated

Material 6: Calming Sensory Tool for Pre-Meal Regulation
Children arrive at lunch dysregulated from 4 hours of school demands. An overstimulated nervous system suppresses appetite. 2–3 minutes of calming sensory input before opening the lunchbox shifts the system from alert to regulated — making eating physiologically possible.
What to Look For
Small enough for lunchbox. Child's preferred calming input: squeeze ball, therapy putty, textured stone, fidget cube, or koosh ball. Test at home to confirm it's calming (not alerting) for your specific child.
Pinnacle Canon Products
Animal soft toys — for children who need a comfort object during regulation. Small, lunchbox-friendly.
DIY / Zero-Cost
Small smooth stone from garden. Piece of soft velvet fabric. Beeswax or playdough rolled into a ball. Tactile input quality matches commercial products.
💰 ₹100–₹800 | 🛒 Search on Amazon.in: stress ball fidget toy calming sensory children

Material 7: Gradual Exposure Photo Schedule
Anxiety responds to gradual, successful exposure — not forced leaps. A photo schedule breaks the journey from "won't open lunchbox" to "eating comfortably in cafeteria" into 10–15 achievable micro-steps. Each success builds neural confidence for the next step.
This 11-step hierarchy is a guide — your child's therapist may adjust the number of steps and pace based on their individual profile. The key principle: each step must be successful before advancing. No rushing. 💰 ₹200–₹800 (printing + laminating) | DIY total cost: ₹50–80.

Materials 8 & 9: Location Pass + Transition Object
🏫 Material 8 — Alternative Eating Location Pass
Why it works: Sometimes the cafeteria is the insurmountable barrier, regardless of other supports. A written accommodation allowing the child to eat in a quieter space (classroom, library, counsellor's office) removes the impossible barrier immediately. Successful eating anywhere at school is better than no eating in the cafeteria.
How to implement: Written request to class teacher + school counsellor. One sentence: "Please allow [child's name] to eat lunch in [alternative space] with supervision as a sensory accommodation." Many schools agree within 24 hours.
💰 ₹0 — School coordination only.
🏠 Material 9 — Home-to-School Transition Object
Why it works: For some children, the core barrier is the psychological distance between home (safe eating context) and school (unsafe eating context). A meaningful object from home bridges this gap, providing emotional connection to home safety — which can reduce anxiety enough for eating to occur.
What to use: Family photo in waterproof sleeve. Parent's handwritten note (new one each day, or laminated favourite). Small comfort object that fits in pocket. Animal soft toys — small comfort plush that travels in lunchbox.
💰 ₹0–₹300 | DIY: Parent writes a 3-sentence note each morning. Total cost: ₹0 + 2 minutes.

Material Selector Guide: Match Material to Barrier
Not every child needs all 9 materials. The most effective approach is identifying your child's primary barrier and starting with the 2 materials that address it most directly. Use this guide to find your starting point.
If the primary barrier is... | Start with... | |
Cafeteria noise | Material 1 (Headphones) + Material 8 (Alternative Location) | |
Food temperature / texture change | Material 2 (Insulated Bento) + Material 4 (Familiar Utensils) | |
Time pressure anxiety | Material 3 (Visual Timer) + Material 5 (Social Story) | |
General anxiety / unpredictability | Material 5 (Social Story) + Material 7 (Gradual Exposure) | |
Dysregulation arriving at lunch | Material 6 (Calming Tool) + Material 1 (Headphones) | |
Overwhelming cafeteria environment | Material 8 (Alternative Location) + Material 7 (Gradual Exposure) | |
Homesickness / psychological safety | Material 9 (Transition Object) + Material 5 (Social Story) |
When in doubt, start with Material 1 and Material 8 — these address the two most common barriers and have the fastest observable impact.

Every Family Can Start Today — Zero to Low Cost Options
WHO/UNICEF Equity Principle
"Evidence-based intervention should not be gated by income. Every child deserves access to effective feeding support." — WHO Nurturing Care Framework, 2018
Material | ₹0 DIY Version | Why It Works the Same | |
Noise-Reducing Headphones | Foam pharmacy earplugs (₹20) | Reduces auditory input by ~20 dB — sufficient for moderate sensory sensitivity | |
Insulated Bento Box | 3 separate stainless containers + newspaper insulation | Temperature retention for 3–4 hours achievable with layered insulation | |
Visual Timer | Sand timer (₹50) or smartphone screen timer | Visual time representation — identical neurological function | |
Familiar Utensils | Pack home cutlery in zip-lock bag | Already in your kitchen | |
Social Story Cards | Phone photos of school + printed sequence (₹30) | Personalised photos outperform commercial versions | |
Calming Sensory Tool | Smooth stone, pinecone, or rolled beeswax | Tactile input quality matches commercial products | |
Alternative Location Pass | Handwritten note from parent to teacher | Schools rarely require formal documentation for simple accommodations | |
Transition Object | Parent's daily handwritten note (₹0) | Written parental message reduces separation anxiety and eating inhibition |
When clinical-grade is non-negotiable: For children with severe auditory hypersensitivity (ASD + auditory processing disorder), professional-grade NRR 27+ dB ear defenders significantly outperform DIY foam earplugs. When DIY options don't produce improvement after 2 weeks, upgrade to clinical-grade.
Safety Gate: Read This Before Beginning
🔴 RED — Do Not Proceed Without Professional Evaluation If:
- Child has a diagnosed swallowing disorder (dysphagia) — feeding materials require SLP supervision
- Child has lost significant weight due to school eating refusal (>5% body weight in 4 weeks)
- Child shows signs of severe anxiety disorder, selective mutism, or panic attacks around school eating
- Child is under 4 years — school eating protocols require age-specific modification
- Child has any oral-motor disorder affecting chewing or swallowing
🟠 AMBER — Modify and Monitor If:
- Child has a history of food allergy — verify all lunchbox contents align with allergy management plan
- Child has sensory sensitivities to headphone pressure — trial shorter durations, softer ear cup materials
- Child resists the calming tool itself — switch to a different sensory modality
- Child becomes more anxious when visual timer is introduced — switch to verbal time cues only
🟢 GREEN — Safe to Proceed When:
- Child has been medically cleared for feeding difficulties
- Child is adequately hydrated and fed at home (breakfast eaten)
- School has been informed and is cooperative
- Parent has reviewed all 9 materials and selected the ones matching the identified barrier
⚠️Emergency — Stop If You See: Child becomes severely distressed or shows panic at school | Child refuses to enter school building due to lunch-related anxiety | Child reports physical pain when eating at school | Child's behaviour significantly worsens after implementing materials.
Your Morning Setup: The 5-Minute Lunchbox Ritual
The school eating refusal protocol begins at home, the night before and each morning. Your kitchen or preparation space needs to become a consistent ritual space — predictable, calm, child-involved. Predictability in the morning reduces the anxiety that carries forward to school.
Evening Before — Materials Prep
Fill insulated bento box compartments, place familiar utensils in utensil pouch, write tomorrow's transition note. Involve child: let them choose one item from accepted foods. Child-involved packing = more invested eating.
Evening Before — Tools Ready
Place calming tool in lunchbox or front pocket of school bag. Charge/prepare headphones if electronic version. Review social story cards with child: "Tomorrow at lunch, here's what will happen..." (2-minute preview).
Morning — T–15 Minutes
Review gradual exposure schedule together. Mark yesterday's progress. Acknowledge last step achieved. Keep tone calm and encouraging — not performative.
Morning — T–5 Minutes
Place transition object in lunchbox pocket or school bag. Parent to child: "This comes with you today. It will remind you that you're a great eater at home."
At School Drop-Off
Brief, confident goodbye. Avoid lingering or expressing parental anxiety — the child reads your emotional state. Your calm signals: this is manageable.

Pre-Session Readiness: The 60-Second Check
Before introducing any new material for the first time, take 60 seconds to assess your child's readiness. Introducing new materials on difficult days increases the chance of rejection and sets back progress. Maintaining existing successes on hard days is itself meaningful progress.
Check | ✅ Green | 🟠 Modify | 🔴 Postpone | |
Child's general mood this morning | Calm, cooperative | Slightly irritable | Severely dysregulated, meltdown | |
Breakfast eaten | Full breakfast | Partial | Refused entirely | |
Sleep last night | Good sleep | Moderate | Very poor sleep | |
Upcoming school stressors | Typical school day | Minor test | Field trip, assembly, major test | |
Child's attitude to school today | Neutral or positive | Mild reluctance | Significant school resistance |
4–5 ✅ → GO
Introduce the new material today as planned
3 ✅ → MODIFY
Introduce at lower intensity; pair with highest-comfort food
1–2 ✅ → POSTPONE
Today: maintain existing materials only. No new introductions.
Step 1: The Invitation — Never a Demand
Step 1 of 6
Every protocol begins with an invitation — never a command. The child is brought into the lunchbox ritual through low-demand, playful engagement. No pressure. No performance expectation. The ABA principle at work: Pairing — establishing positive association with the lunchbox activity before any demand is placed.
"Hey — let's pack your lunch together. You pick one thing you like. What should we put in the first compartment?"
Body Language
- Kneel or sit at child's height — do not tower
- Open body posture — no crossed arms
- Match your energy to theirs
- No visible clock-watching or hurry signals
Reading Cues
- ✅Acceptance: Moves toward lunchbox, picks up food item, nods, engages
- 🟠Walks away: Give 60 seconds, try again with simpler invitation ("Just one thing — you choose")
- 🔴Physical protest: Today is a Postpone day (return to Readiness Check)
- 🟡Silent but compliant: Proceed very gently — this is engagement

Step 2: The Engagement — Material Introduction
Step 2 of 6
Introduce the new support material as a helpful tool — not a medical intervention. Language matters enormously. Below are scripts for each material type, tailored to feel natural and empowering for your child.
For Headphones
"These are your special school eating headphones. They make the lunchtime noise quieter so you can focus on your food. Want to try them for a second?"
For Visual Timer
"This is your lunch timer. It shows you exactly how much time you have. You'll always know. Let's set it to 15 minutes — see how it works?"
For Transition Object
"I'm going to put this in your lunchbox. When you open it at school and see it, it's me saying — you've got this. You eat great at home. You can eat at school too."
For Social Story Cards
"Let's look at your lunch story. First you'll [card 1]... then [card 2]... and then you eat. Easy. You know exactly what's coming."
Reinforcement Cue: Any positive engagement with the material = immediate, specific praise: "Yes! You put the headphones on. That's exactly right." Reinforce the approach, not the outcome.

Step 3: The Therapeutic Action — School-Side Execution
Step 3 of 6
The therapeutic action occurs at school, during lunch. Your preparation at home creates the conditions for this moment to succeed. Each material functions differently in the school environment — here is what happens with each.
If Using Headphones
Child puts on headphones before entering cafeteria or upon sitting. Teacher/aide has been briefed. Child eats with auditory input reduced.
If Using Alternative Location
Child proceeds to agreed quiet location with lunchbox. Teacher/aide checks in. Child eats without cafeteria stimulus.
If Using Visual Timer
Timer is set when child sits. Child can see time remaining. No adult pressure — the timer provides structure without social demand.
If Using Gradual Exposure
Today's target step is the only expectation. If today's step is "open the lunchbox and look inside for 2 minutes," that is success.
Parent's Role During School Hours: Your role is complete once the child leaves home with all materials. Trust the setup. Do not call the school to check during lunch. Debrief at pickup with curiosity, not anxiety: "How was lunch today? Tell me something about it."

Step 4: Repeat and Vary — Consistency Over Intensity
Step 4 of 6
School eating refusal improves through daily, consistent, low-pressure exposure — not weekly intensive sessions. Target: every school day, full lunch period. Minimum effective trial: 10 consecutive school days before evaluating material effectiveness.
"10 consistent school lunch days with the right materials outperform 2 'perfect' sessions followed by 8 abandoned attempts."
Week | Primary Material | Variation Introduced | |
Week 1 | Headphones only | Establish baseline with one material | |
Week 2 | Headphones + Visual timer | Add time structure | |
Week 3 | Headphones + Timer + Familiar utensils | Add comfort layer | |
Week 4 | Introduce calming sensory tool pre-lunch | Address dysregulation arrival | |
Week 5+ | Gradual exposure steps advancing | Begin systematic environment expansion |
Satiation Watch: If child actively rejects a material that previously worked, this is a signal — the material is no longer needed (progress!), or the material is causing new anxiety (adapt). Do not force.

Step 5: Reinforce and Celebrate Every Success
Step 5 of 6
The window for effective reinforcement is at pickup — not hours later. What to reinforce (in therapeutic priority order): 1) Using the support material, 2) Any eating attempt, 3) Staying in the eating environment, 4) Communicating about lunch experience.
Script: Material Use
"You used your headphones at lunch? That is such a smart move — that's exactly what they're for!"
Script: Any Eating
"You took three bites today? That's more than yesterday. Your body got some fuel. I'm really proud."
Script: Brave Attempt
"You opened your lunchbox today even though it was scary. That took courage."
Reinforcement Menu: Verbal praise (always — immediate, specific) | High-five or fist bump at pickup | 5 minutes of child's chosen activity at home | Rosette Imprint Reward Jar — 5 tokens = special activity | 1800+ Reward Stickers Book — sticker for each "brave lunch day."

Step 6: The Cool-Down — School-to-Home Debrief
Step 6 of 6
The cool-down phase for school eating refusal happens during the after-school transition. How this debrief goes shapes tomorrow's willingness. The goal: curiosity without pressure, celebration without performance expectation.
First 3 Minutes — No Lunch Talk
Allow the child to decompress from school demands. Offer water and their post-school snack. No immediate questions about lunch.
Minutes 3–7 — Curious Enquiry
"Tell me one thing about lunch today." (Not: "Did you eat?" — these create performance anxiety)
Minutes 7–10 — Celebrate Any Positive
Whatever the child reports — use any positive element as reinforcement material for tomorrow's packing ritual.
Evening — Update Schedule
Mark today's progress on the exposure schedule. Write tomorrow's transition note if using. "I'm writing your tomorrow note. What do you want it to say?"
What to do if the lunchbox came home full again: Breathe. This is data, not failure. Ask: "Which material wasn't available today? Which step in the exposure schedule are we at?" Do not escalate. Tomorrow is another day.
60 Seconds of Data Now Saves Hours of Guessing Later
After 10 school days of data, patterns emerge: "Headphones days = higher intake. No-headphone days = near zero." → Noise is the primary barrier. "Monday and Tuesday always better than Thursday-Friday." → Fatigue accumulates — adjust Friday expectations. "Week 3 consistently better than Week 1." → Progress is happening even when it feels invisible.
Field 1: Estimated Intake
% of lunchbox eaten (0%, 25%, 50%, 75%, 100%)
Example: "25%"
Example: "25%"
Field 2: Materials Used
Which of the 9 materials were in play today
Example: "Headphones ✓, Utensils ✓"
Example: "Headphones ✓, Utensils ✓"
Field 3: Child's State at Pickup
1–5 scale: 1=severely dysregulated, 5=calm and engaged
Example: "3"
Example: "3"
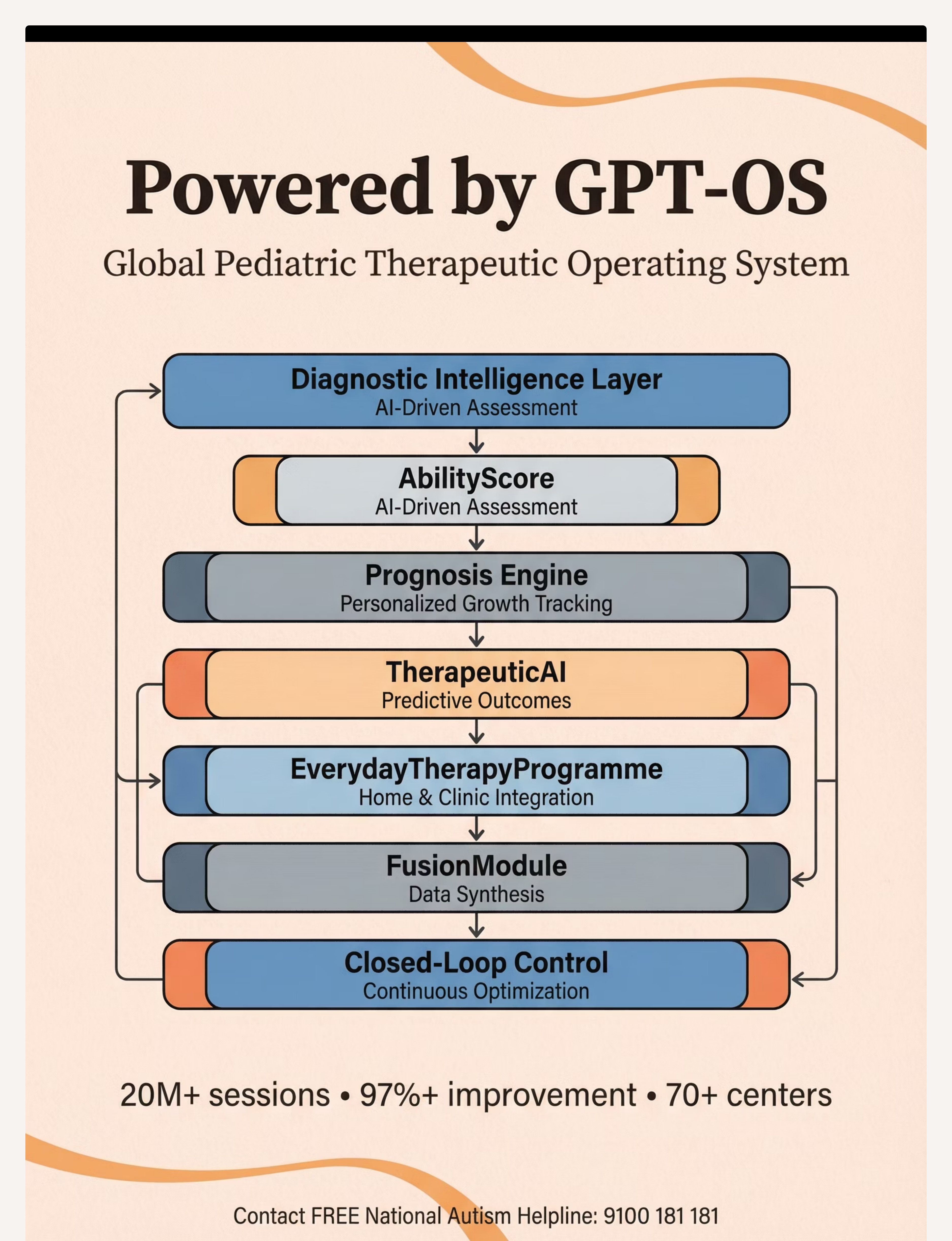
📱Digital: Note in phone immediately at pickup. Even a voice memo works. | 📋Paper: Weekly tracking sheet — 5 rows (Mon–Fri), 3 columns. | 🖥️GPT-OS® Tracker: Log to your GPT-OS® feeding programme dashboard at pinnacleblooms.org/gpt-os
The Reality Card: When Things Don't Go as Expected
"Session abandonment is not failure — it's data. Every unsuccessful lunch tells you something specific about the remaining barrier."
Lunchbox Still Came Home Completely Untouched Despite Materials
Return to barrier identification. Ask the teacher: "Where does [child] sit? What happens the moment they sit down? Do they even open the lunchbox?" The data changes the next action. The identified barrier may remain more powerful than the current material, or a new barrier has emerged.
Child Uses Headphones at Home but Refuses Them at School
Social self-consciousness — "other kids will notice/laugh." This is common at ages 8–12. Reframe headphones as "cool" rather than medical. Try discreet foam earplugs instead. Work with teacher to normalize their use with the class.
Gradual Exposure Progressed Well, Then Suddenly Regressed
A disruption occurred — substitute teacher, different seating, a social incident, a sick day that broke routine. Step back 2–3 steps on the exposure schedule. Regression is not starting over — it's a brief consolidation. Typical recovery: 3–5 days.
Child Eats Fine in Alternative Location but Refuses Cafeteria
The alternative location is working — the cafeteria remains overwhelming. Evaluate: is cafeteria participation a necessary goal? For some children, a supported quiet eating space is the appropriate permanent accommodation. Successful eating in a quiet space > no eating in cafeteria.
School Won't Agree to Any Accommodations
Request written documentation of the refusal. Provide our Teacher Communication Template (Card 37). Escalate to school principal. If child has diagnosis: formal accommodation through IEP equivalent. Call 9100 181 181 — Pinnacle's advocacy team can help.
Every Child Is Different: Personalise These Materials
For the Sensory Avoider (Over-Responsive)
- Start with Material 8 (Alternative Location) — full cafeteria removal first
- Use highest-rated NRR headphones (NRR 27+)
- Make the gradual exposure schedule slower — more intermediate steps
- Keep lunchbox very simple: 2 foods maximum initially
For the Sensory Seeker (Under-Responsive)
- Cafeteria may actually be stimulating rather than overwhelming — check if noise helps focus
- Focus on Materials 2, 3, 4 (logistics) rather than noise reduction
- Calming tool may need to be proprioceptive (heavy pressure, resistance band)
Age-Based Modifications
Age | Primary Materials | Key Adjustments | |
4–6 years | Materials 2, 4, 9 | Keep packing ritual very simple; child-chosen 1 food per day | |
7–9 years | Materials 1, 3, 5, 7 | Introduce exposure schedule; child participates in step design | |
10–12 years | Materials 1, 8, 7 (discreet) | Prioritise child's voice on accommodation visibility; peer awareness matters |
Severity Scaling
Mild (25–50% at school) | Moderate (<25%) | Severe (complete, 4+ weeks) | |
Materials 2, 3, 4 likely sufficient | Materials 1, 5, 7, 8 | All 9 materials + professional evaluation | |
2–4 week improvement expected | 6–8 week programme | 8–12 weeks + therapy support |
Week 1–2: What to Expect
Progress Arc — Act IV
Week 1–2 often brings frustration — because change is happening beneath the surface before it appears in behaviour. Neural pathways are forming. The nervous system is learning that school lunch is slightly safer than before. This happens before behaviour shifts.
✅ These ARE Progress at This Stage
- Child allows lunchbox to be packed with new materials without protest
- Child carries headphones to school even if not using them yet
- Lunchbox comes back with evidence of opening (disarranged contents)
- Child eats 1–2 items even if returning most
- Child mentions lunch at pickup without distress
- Teacher reports child "sat calmly" during lunch (even without eating)
❌ These Are NOT Expected Yet
- Full lunch eaten consistently
- Child requesting to sit in cafeteria
- No need for support materials
"If your child tolerates the familiar utensils in the lunchbox for a week without removing them — that's real, measurable progress."
What to Track This Week: Which material is being accepted? Which is being refused? This directly informs Week 3–4 planning. Progress bar: ████░░░░░░░░░░░░░░░░ 15%

Week 3–4: Consolidation Signs
Progress Bar: ████████░░░░░░░░░░░░ 40%
Neural Pathway Consolidation
Child anticipates the packing ritual — comes to the kitchen without being called. Refers to their school materials: "I need my eating headphones." Reduced resistance at lunchbox-packing time.
Measurable Changes
Intake has increased from 0% to 10–25% consistently. Child reports less distress at school lunch ("it's okay," "it's a bit better"). Recovery time after school is shorter.
Generalisation Seeds
Child may spontaneously reach for calming sensory tool in other anxiety contexts. May comment on noise level in other settings. Shows preference for certain lunchbox foods — engagement increasing.
Parent Milestone: By Week 4, you'll notice you're more confident in the morning packing ritual. That confidence transfers to your child. Parental anxiety about school eating is itself a barrier — your growing calm is therapeutic.

Week 5–8: Mastery Indicators
Progress Bar: ███████████████░░░░░ 75% → Mastery Zone
🏆 Primary Mastery
Child eats 50–100% of packed lunch on ≥4/5 school days per week, for 3 consecutive weeks, with current supports in place.
🏆 Secondary Mastery
Child independently manages own support materials (headphones on/off, timer set, calming tool used) without adult prompting.
🏆 Tertiary Mastery
Child can eat in cafeteria (with supports) OR eat in alternative location comfortably — has choice and uses it appropriately.
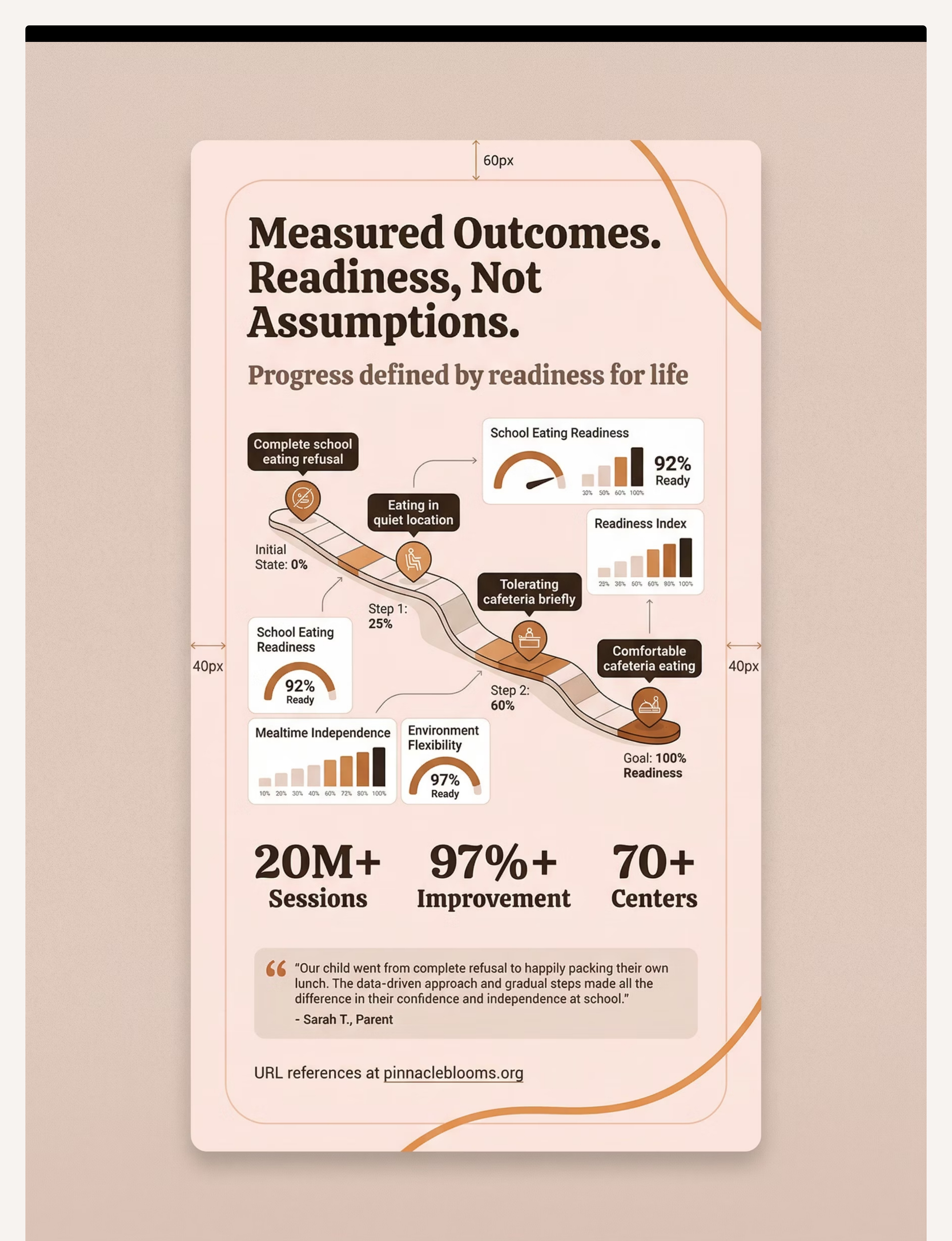
GPT-OS® Readiness Scores at Mastery: School Eating Readiness Index: Target 85%+ | Mealtime Independence: Target 80%+ | Environment Flexibility: Target 70%+
Maintenance Check: If supports are reduced or forgotten for 3 days — does eating hold? If yes → readiness to fade supports. If no → maintain and continue building.
🎉 Celebrate This Win — Your Commitment Made This Happen
YOU DID THIS. Seven weeks ago, the lunchbox came home untouched every day. Your child was hungry, dysregulated every afternoon, and the school eating situation felt impossible. You identified the barrier. You sourced the materials. You established the morning ritual. You communicated with the school. You tracked the data. You adjusted when things didn't work. You stayed consistent when you wanted to give up.
🍽️ Special Dinner
Dinner of child's choice: "You've been working so hard at school lunch. Tonight, you choose."
📸 Photo Milestone
Photograph child with their full, empty lunchbox — the reverse of your starting photo. A powerful visual record of the journey.
📔 Journal Prompt
"Write or draw the moment you noticed eating at school was getting easier."
"When a child who previously couldn't eat at school starts eating consistently, we see changes beyond nutrition. Afternoon behaviour improves. Academic focus sharpens. Anxiety about school in general often reduces. The lunchbox was a window into the whole school experience — fixing it fixes more than just hunger." — Pinnacle Feeding Therapy Clinical Notes

⚠️ Red Flags: When to Pause and Seek Professional Evaluation
🔴 Complete Refusal Beyond 6 Weeks of Consistent Material Use
Underlying barrier may require clinical assessment — possible anxiety disorder, sensory processing disorder, or undiagnosed ASD. Book assessment. Call 📞9100 181 181 for feeding therapy referral.
🔴 Physical Symptoms — Stomach Aches, Nausea, Vomiting
May indicate medical cause (GI motility, food sensitivity) or severe anxiety somatisation. Pediatrician evaluation first, then feeding therapist.
🔴 Weight Loss or Nutritional Concerns
School eating refusal is now affecting growth and development. Escalation required immediately: Pediatrician + registered dietitian + feeding therapist — concurrent, not sequential.
🟠 Eating Refusal Now Appearing at Home Too
School eating refusal has broadened; possible feeding disorder development. Feeding therapist evaluation within 2 weeks.
🟠 Child Refusing to Attend School Due to Lunch Anxiety
School avoidance driven by lunch has emerged. Child psychologist referral + school team meeting required.
🟠 No Improvement After 4 Weeks of Correct Implementation
Materials selected may not match the actual barrier. OT sensory assessment + feeding evaluation needed to identify the correct mechanism.
📞FREE HELPLINE: 9100 181 181 | Available 24×7 | 16 Languages
Escalation pathway: Self-monitor with tracking data → Teleconsultation (9100 181 181) → In-clinic OT/Feeding assessment → Multi-disciplinary evaluation if needed
Escalation pathway: Self-monitor with tracking data → Teleconsultation (9100 181 181) → In-clinic OT/Feeding assessment → Multi-disciplinary evaluation if needed
Your Developmental GPS: Before, Now, and Next
School eating refusal (E-471) sits within a broader developmental series. Understanding where you are and where you're headed gives the work meaning and direction.
E-469
Mealtime Anxiety (Pre-school)
E-470
Food Texture Sensitivities
◄ E-471 ►
School Eating Refusal — YOU ARE HERE
E-472
Social Eating Challenges
E-473
Restaurant & Public Eating
If your child responded best to... | Your next technique is... | |
Environmental reduction (headphones, quiet space) | E-472: Social Eating Challenges — expand to peer contexts gradually | |
Anxiety reduction (social stories, gradual exposure) | E-469 advanced: Mealtime Anxiety deep-work | |
Logistics (bento, utensils) | E-473: Restaurant and Public Eating — extend logistics to novel contexts | |
All materials working well | E-472: The full social eating context is ready to address |
Explore the Feeding & Mealtime Challenges Series
Domain E: Feeding Therapy | Episodes 469–550. Each technique builds on the last, following the developmental pathway from early anxiety to full environmental flexibility in eating.

🟡 E-469 — Mealtime Anxiety
Difficulty: Core | 🍱 Calming Sensory Tools, Visual Timers

🟠 E-470 — Food Texture Sensitivities
Difficulty: Core | 🛁 Texture Exploration, Bento Logistics

🔵 E-472 — Social Eating Challenges
Difficulty: Core-Advanced | 👥 Social Stories, Gradual Exposure
🟣 E-473 — Restaurant & Public Eating
Difficulty: Advanced | 🍽️ Noise Reduction, Environment Tools

This Technique Is One Piece of a Larger Plan
School eating refusal rarely exists in isolation. In Pinnacle's clinical data, it co-presents most frequently with Domain A (Sensory) in 78% of cases, Domain C (Emotional Regulation) in 64% of cases, and Domain D (Flexibility/Transitions) in 52% of cases.
Your child's feeding work in Domain E is connected to their sensory regulation (A), emotional wellbeing (C), and daily living skills (H). The GPT-OS® platform coordinates all active domains into one integrated plan rather than isolated interventions.

From the Pinnacle Clinical Files: Families Who've Navigated This
Illustrative clinical narratives. Outcomes vary by child profile, barrier type, and intervention consistency.
🌟 The Noise Barrier — 6-year-old boy
Before: Lunchbox returned 95% full for 14 consecutive weeks. School suggested child was "not hungry." OT assessment identified auditory hypersensitivity. Noise-reducing headphones introduced. After (Week 10): eating 50% in cafeteria with headphones.
"We didn't know the cafeteria noise was physically overwhelming his nervous system. Once we understood that, the headphones felt obvious. His afternoon behaviour transformed — he was no longer running on empty every day."
🌟 The Anxiety Barrier — 9-year-old girl
Before: Complete lunch refusal for 3 months. Mild ASD, social anxiety. Fear of eating "wrong" in front of peers. Social story cards personalized to her school's cafeteria. 17-step gradual exposure schedule. After (Week 8): eating in cafeteria 3/5 days.
"The social story cards were the breakthrough. She finally had a script for what to do. The anxiety was about not knowing — and the cards gave her certainty."
🌟 The Logistics Barrier — 7-year-old boy
Before: Refusing packed lunch — "it doesn't taste right." No diagnosis. Texture sensitivity — foods getting warm, sandwiches getting soggy. Insulated bento box, familiar home utensils, small ice pack. After (Week 2): Full lunch consumed consistently. No further intervention needed.
Therapist's Note: This is the fastest-resolution profile — a logistics barrier masquerading as refusal. When the food tastes as it should, the child eats.
Preview of 9 materials that help with school eating refusal Therapy Material
Below is a visual preview of 9 materials that help with school eating refusal therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Connect, Get Help, and Share
🟢 Connect With Other Parents
Join WhatsApp Group: School Eating Challenges — Parents India. Moderated by Pinnacle feeding therapy team. Peer Mentor Programme: connect 1-on-1 with a parent who has successfully navigated this.
📞 Your Professional Support Team
OT, Feeding Therapist, Child Psychologist, and Special Educator available at 70+ Pinnacle centers. Teleconsultation available nationally.
FREE: 9100 181 181 | 24×7 | 16 Languages
📥 Share With Caregivers
Downloadable: Family Guide PDF, Teacher Communication Template, School Accommodation Request Letter.
Frequently Asked Questions
Why is school lunch specifically the problem if my child eats well everywhere else?
School lunch combines auditory overwhelm, visual chaos, social performance pressure, time constraints, and separation from safe adults — all simultaneously. After-school care typically involves smaller groups, familiar adults, and a calmer environment. Identify your child's primary barrier and address it directly.
How do I get the school to agree to accommodations like eating in the classroom?
Key phrase: "My child has a sensory processing difference that makes the cafeteria environment too stimulating for eating. Could we trial [specific accommodation] for 4 weeks and review?" If school resists: provide our Teacher Communication Template, escalate to the principal, or call 9100 181 181.
We've been trying for 3 months with no improvement. Is professional help needed?
Yes. Professional evaluation is indicated at 4–6 weeks without improvement. At 3 months with no improvement, this is a definitive signal for clinical assessment. Call 9100 181 181. Common findings: undiagnosed sensory processing disorder, anxiety disorder, or a medical cause.
My child eats 1–2 bites and then stops. Is that progress?
Yes — significantly. From zero to 1–2 bites is a neural pathway breakthrough. Build on this by ensuring those bites are the most preferred foods, reinforcing them enthusiastically, and gradually — over weeks — expecting 3, then 4, then 5 bites. Do not rush past this stage.
Should I send the same foods every day or vary the lunchbox?
For children with anxiety or sensory sensitivities, predictability is protective during the early weeks. Send the same 2–3 high-acceptance foods consistently for the first 3–4 weeks. Variation can be introduced gradually — one new item per week, placed in a separate compartment, with zero expectation of eating it initially.
🍱 Start This Technique Today
Begin your personalised E-471 programme. GPT-OS® guides you step by step.
📞 Book a Feeding Therapy Consultation
Speak to a specialist. Get a personalised barrier assessment and material plan.
→ Next: E-472 Social Eating Challenges
When school eating is improving, prepare for the next challenge in the series.
✅Validated by the Pinnacle Blooms Consortium — OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • Feeding Therapy • CRO
20M+ sessions • 97%+ measured improvement • 70+ centers • Evidence-based • WHO/UNICEF aligned
20M+ sessions • 97%+ measured improvement • 70+ centers • Evidence-based • WHO/UNICEF aligned
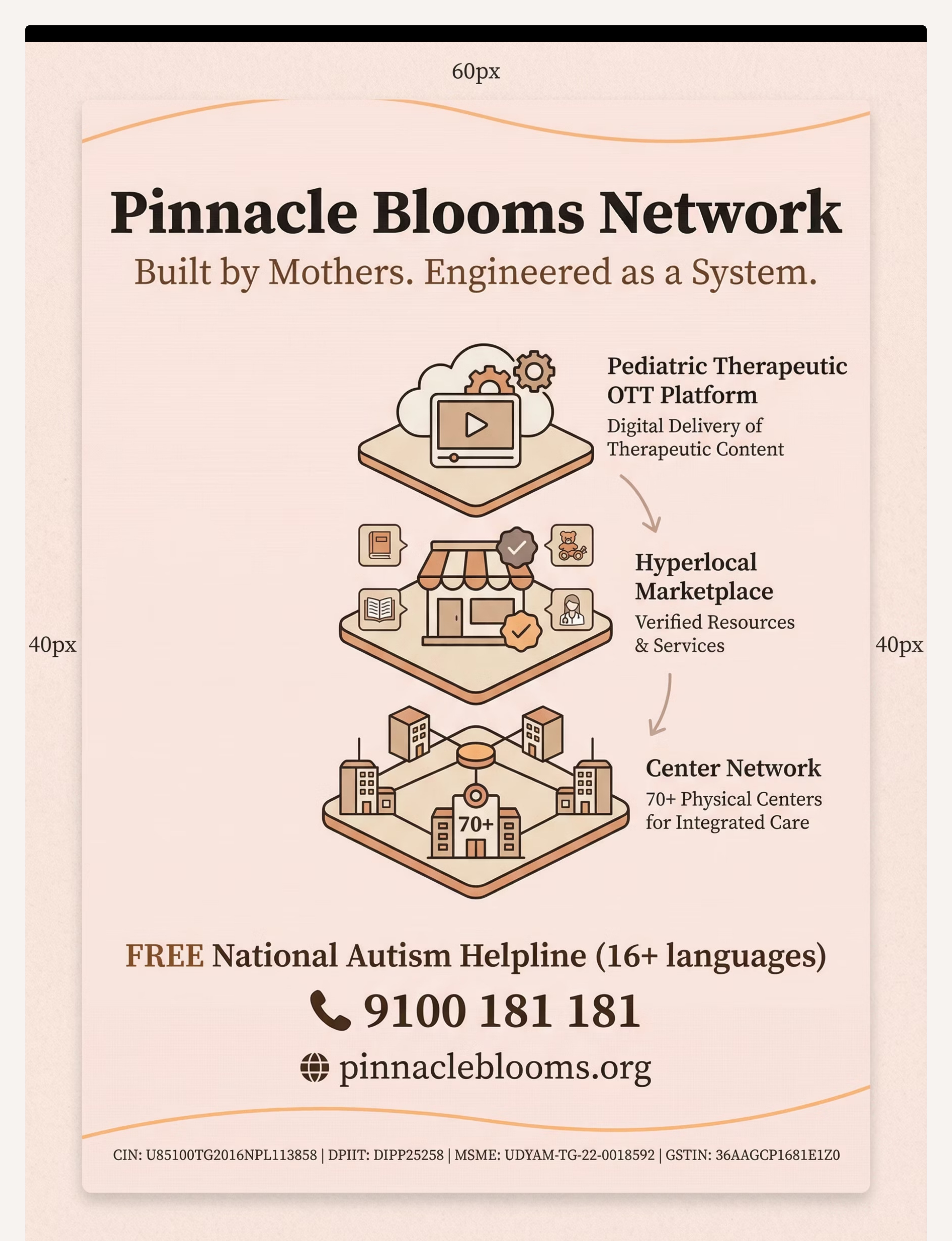
📞FREE National Autism Helpline: 9100 181 181 | 16 Languages | 24×7 | pinnacleblooms.org
🌸PINNACLE BLOOMS NETWORK® — Built by Mothers. Engineered as a System.
OT • SLP • ABA/BCBA • SpEd • NeuroDev • Feeding Therapy • CRO • Pediatricians • WHO • UNICEF • Families Across 70+ Countries
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content generated under GPT-OS® Content Engine. Consortium-reviewed. Evidence-linked. Technique code E-471. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is educational and does not replace individualised assessment and intervention with licensed feeding therapists, occupational therapists, psychologists, or pediatricians. Professional evaluation is recommended for persistent eating difficulties. Individual results may vary.
🌸PINNACLE BLOOMS NETWORK® — Built by Mothers. Engineered as a System.
OT • SLP • ABA/BCBA • SpEd • NeuroDev • Feeding Therapy • CRO • Pediatricians • WHO • UNICEF • Families Across 70+ Countries
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content generated under GPT-OS® Content Engine. Consortium-reviewed. Evidence-linked. Technique code E-471. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is educational and does not replace individualised assessment and intervention with licensed feeding therapists, occupational therapists, psychologists, or pediatricians. Professional evaluation is recommended for persistent eating difficulties. Individual results may vary.