
Domain D · Subdomain D3
Aggression Toward Others
20 evidence-based interventions for hitting, biting, kicking, hair pulling, scratching, pushing, spitting, property destruction, sibling aggression, school aggression, verbal aggression, safety during crisis, anger management, safe hands, and non-aggressive expression — built for children with autism and the families who love them.
Understanding Aggression in Autism
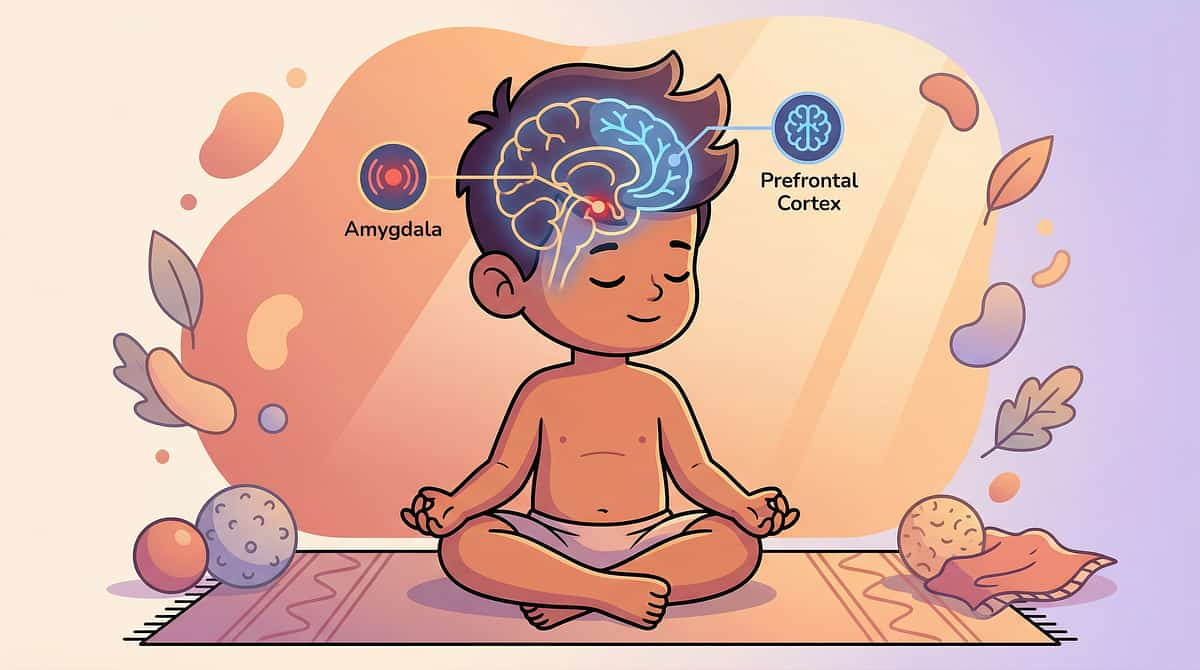
Aggression in ASD is not about character. It is the behavioural output when the nervous system is overwhelmed and the brain's inhibitory system cannot contain the motor response. The child who hits, bites, or kicks is not "bad," "violent," or "dangerous" — they are a child whose regulatory system has been exceeded by the demands placed upon it.
Amygdala
Threat detection triggers the fight response. In ASD, heightened reactivity means more stimuli register as threats — triggering more frequent fight activation.
Hypothalamus
Executes the fight response — raising heart rate, blood pressure, muscle tension, and adrenaline. The body prepares for physical action.
Prefrontal Cortex
The inhibitor — meant to suppress aggressive motor responses and generate verbal alternatives. In ASD, this brake is weaker and slower.
Motor Cortex
Executes the aggressive action — hitting, kicking, biting, throwing. The final common pathway when the PFC brake fails to engage in time.
The critical reframe for families: Your child is not choosing to hurt you. Their brain is producing the best available response to an intolerable internal state. The goal is not to punish the aggression — it's to address the cause, teach alternative expression, and keep everyone safe during episodes.

D-381 · Hitting Behaviour
D-381: 9 Materials That Help With Hitting Behavior
Open hand. Closed fist. At you, at siblings, at teachers, at other children. Hitting is the most common form of aggression in ASD — the body's most accessible physical response when the brain is overwhelmed. It's the behaviour that gets families excluded from schools, avoided by relatives, and isolated from community.
Why the Brain Defaults to Hitting
Hitting activates the largest upper body motor group — the arm, shoulder, and hand complex. It requires minimal motor planning and produces immediate consequences: the person reacts (attention), the demand stops (escape), or the frustration discharges (sensory release). Low effort + high effectiveness = the brain's default aggressive response.
Evidence Level I — Functional Communication Training reduces aggression 80–90% when implemented consistently. NCAEP 2020 | FCT meta-analyses | PMC9978394
What You'll Learn
- Functional analysis: why is this child hitting? (escape, attention, tangible, sensory, pain?)
- Function-matched replacement: escape-hitting → "Break please." Attention-hitting → "Look at me."
- Safety during hitting — blocking without restraining, protective positioning
- Antecedent modification to reduce triggers before they build
- Consistent caregiver response across all environments
⚠️ Frequent or severe hitting → BCBA referral required. Call 9100 181 181.
Lead Disciplines: ABA (BCBA/FBA) · Psychology · OT · SLP · NeuroDev

D-382 · Biting Others
D-382: 9 Materials That Help With Biting Others
Teeth on skin. The most socially alarming form of aggression. Schools expel for it. Parents of bitten children are furious. Families live in terror of the next bite report — and the isolation that follows it. Biting is also among the most reinforced aggressive behaviours, which makes it particularly resistant to intervention without the right approach.
The Dual Reinforcement Problem
Biting provides massive jaw proprioceptive input (TMJ activation) and is an extremely effective aggressive behaviour — producing immediate, intense pain and an immediate caregiver reaction. It carries dual reinforcement: sensory (intense oral proprioception) and social (demand removed or attention gained). Both functions must be addressed or the behaviour persists.
Evidence Level I — Functional analysis + oral sensory replacement + FCT. NCAEP 2020
What You'll Learn
- Distinguishing sensory biting (calm, rhythmic) from aggressive biting (during distress) — often both
- Chew tools as proactive oral input before the biting threshold is reached
- FCT targeting the aggressive function specifically
- Immediate post-bite protocol: care for victim, redirect the child
- School communication strategy to prevent expulsion
⚠️ Biting that breaks skin → medical attention for the victim + urgent BCBA consultation.

D-383 · Kicking Others
D-383: 9 Materials That Help With Kicking Others
Lower body aggression — at shins, at stomachs, at anyone within leg range. Kicking is particularly dangerous because legs generate significantly more force than arms. It often occurs during floor-based meltdowns, where the child lies down and kicks outward — and anyone nearby becomes an unintended target.
The Neuroscience of Kicking
Kicking recruits large lower-extremity muscles — quadriceps, hip flexors — producing significant force and intense proprioceptive discharge. Critically, the child may not even be aiming. The legs flail as part of full-body dysregulation. Anyone in range gets hit not out of intent but out of proximity to an overwhelmed nervous system.
Evidence Level I — FCT + safety positioning + proprioceptive replacement. NCAEP 2020
What You'll Learn
- Safety positioning: never stand directly in front during a meltdown
- Directed kicking alternatives: kick pad, stomping board, heavy leg work
- Functional analysis to identify why kicking is occurring
- Heavy work for legs as proactive sensory regulation
- Teaching "I need space" as a verbal replacement for kicking
- Managing floor-based kicking episodes safely without escalating
D-384 · Hair Pulling
D-384: 9 Materials That Help With Hair Pulling
They grab and don't let go. Hair pulling is one of the hardest aggressions to manage because the grip is sustained — creating ongoing pain and requiring physical intervention to release. In Indian households where women frequently wear long braids and plaits, hair is constantly accessible during caregiving moments.
Why the Grip Holds
Hair pulling provides intense proprioceptive input through grip and resistance. The sustained grip may also serve a sensory anchoring function — holding onto something provides proprioceptive grounding during dysregulation. The victim's intense reaction delivers powerful social reinforcement simultaneously.
Grip Release Technique
Counter-intuitively: push INTO the pull, not away from it. Moving toward the grip reduces pain and naturally loosens the child's grip. Pulling away tightens it. This is one of the first practical skills families need to learn.
Replacement Activities
Pull toys, tug ropes, and resistance bands provide similar proprioceptive input through controlled, safe channels. Antecedent modification — tying hair back during high-risk moments — reduces availability of the trigger.
Teaching Alternatives
"I need you" — a verbal or AAC replacement for grabbing. Teaching appropriate ways to initiate contact and request attention without using the body aggressively.
Evidence Level I — FCT + grip release training + antecedent modification. NCAEP 2020
D-385 · Scratching Others
D-385: 9 Materials That Help With Scratching Others
Nails on skin — leaving marks, drawing blood. Quick, reflexive, often erupting during close-contact moments like dressing, bathing, or being held. The speed of scratching makes it nearly impossible to block in real time. It happens before anyone can react — which is why prevention, not interception, is the primary intervention strategy.
Escape from Touch — Not Just Aggression
Scratching is a fast motor response requiring minimal planning. It frequently occurs during close physical proximity — caregiving tasks — where the child is already sensory-overloaded by unwanted touch. The scratch may be escape from tactile input as much as aggressive expression. Understanding this distinction changes the entire intervention approach.
Evidence Level I — Nail management + FCT + sensory-informed caregiving. NCAEP 2020
What You'll Learn
- Immediate step: keep nails short — weekly trimming routine is non-negotiable
- Identify if scratching = escape from touch, then modify the caregiving approach
- Protective clothing during vulnerable caregiving moments
- FCT: teaching "Don't touch" or "Stop" as a functional replacement
- Approach from the front, warn before touching, use firm rather than light touch

D-386 · Pinching Others
D-386: 9 Materials That Help With Pinching Others
Small, precise, and intensely painful. Pinching can happen so subtly that bystanders don't see it — but the pain is concentrated and immediate. Often directed at soft tissue: the inner arm, thigh, or cheek. It can be a sensory-seeking behaviour driven by fascination with the skin's response, or a covert aggressive behaviour that's difficult to detect and address.
The Sensory vs. Aggressive Distinction
Pinching requires fine motor precision — more planning than hitting, but it produces concentrated pain. When sensory in nature, the child is fascinated by tactile feedback from skin compression and release. When aggressive, it is covert, effective, and hard to catch. Both functions require different intervention pathways.
Sensory Replacements
Play dough, squeeze toys, therapy putty, and kinetic sand offer similar tactile input through a safe, socially acceptable channel. The goal is redirecting the tactile drive — not eliminating it.
What You'll Learn
Functional analysis · FCT for aggressive pinching · Vigilance for covert pinching in sibling relationships · Teaching appropriate tactile exploration · Sibling reporting systems for detection
Evidence Level I — Functional analysis + sensory replacement + FCT. NCAEP 2020

D-387 · Pushing Others
D-387: 9 Materials That Help With Pushing Others
Pushing to create distance. This behaviour is often escape-motivated — "Get away from me" expressed through the body because the words aren't available. In crowded Indian environments like school corridors, markets, and family gatherings, the impulse to push intensifies with proximity overload and unpredictable social contact.
Proprioceptive + Escape: A Dual Drive
Pushing is often both proprioceptive and escape-motivated simultaneously. The child needs deep pressure input (arms extended against another body) AND distance from an overwhelming stimulus. The push delivers both in a single action — which is why it works so effectively and is so highly reinforced by the environment.
Evidence Level I — FCT + personal space teaching + sensory alternatives. NCAEP 2020
What You'll Learn
- Pushing as "I need space" — teaching the words before the body acts
- Wall pushes and heavy door pushing as replacement proprioceptive input
- Personal space teaching for crowded Indian contexts
- Crowd management strategies for markets, gatherings, school corridors
- Differentiating escape-motivated pushing from tangible-motivated pushing

D-388 · Spitting at Others
D-388: 9 Materials That Help With Spitting at Others
Socially devastating. Spitting produces intense disgust in the recipient — a disproportionate social reaction to a physically harmless act. In Indian culture, spitting is deeply offensive and stigmatising. The social consequences frequently exceed those of hitting, making this one of the most isolating behaviours a family can face.
Four Possible Functions
Attention — produces INTENSE reaction. Escape — adults back away. Sensory — oral motor stimulation. Emotional expression — disgust or anger with no verbal channel. The function determines everything about the intervention.
The Counter-Intuitive Response
When spitting is attention-reinforced, the biggest intervention variable is the adult response. Do not show disgust. A neutral, planned response removes the high-value reinforcer that maintains the behaviour. This is harder than it sounds — and critical to success.
What You'll Learn
Oral motor alternatives · Teaching verbal expression of anger and rejection · Managing social fallout in Indian community contexts · School communication strategy · Planned neutral response protocols
Evidence Level I — Functional analysis + planned response + FCT. NCAEP 2020

D-389 · Throwing at People
D-389: 9 Materials That Help With Throwing at People
Toys, cups, steel plates, phones — aimed with increasing accuracy. Targeted throwing is more concerning than general throwing because it demonstrates directed aggressive intent, or an extremely effective and well-shaped escape or attention behaviour. When throwing is aimed at specific people, the behaviour has been reinforced into precision.
Why Throwing Becomes Targeted
Targeted throwing requires object identification, motor planning, arm execution, and visual tracking — more complex than hitting. When directed at specific people, the behaviour has been shaped by reinforcement history: throwing at this person produces the desired outcome most reliably. The target reveals the function.
Evidence Level I — Environmental management + FCT + safety. NCAEP 2020
What You'll Learn
- Environment proofing: remove dangerous projectiles during escalation windows
- Identifying target patterns: who gets thrown at, and what function do they serve?
- Directed throwing alternatives: soft balls, bean bag toss, safe physical channels
- Teaching "I'm angry at you" as a verbal replacement
- Safety shields (pillow, tray) for immediate protection in the moment
- Indian home safety: steel vessels and glass items as priority removal

D-390 · Property Destruction
D-390: 9 Materials That Help With Property Destruction
Breaking toys. Ripping books. Smashing electronics. Overturning furniture. The destruction is often the sensory experience itself — the crash, the rip, the shatter — as much as the aggressive expression. This is what makes property destruction uniquely self-reinforcing, even in the absence of any social consequence.
Sensory Reinforcement
Property destruction delivers intense multi-sensory feedback: the auditory crash, the visual spectacle, the proprioceptive impact. This combination is powerfully reinforcing without requiring any social response — making it resistant to extinction approaches alone.
Safe Destruction Alternatives
Old newspapers to rip, bubble wrap to pop, demolition play with foam blocks — channels that provide the same sensory discharge without financial or safety consequences.
Functional Analysis
Is this sensory? Escape? Attention? Frustration discharge? The intervention pathway differs significantly for each function. A BCBA-led FBA is essential for frequent or escalating property destruction.
Indian Home Context
TV screens, phones, crockery, and neighbours' property as common targets. Proactive environmental protection during escalation windows is a non-negotiable first step for most families.
Evidence Level I — Environmental protection + sensory alternatives + FCT. NCAEP 2020

D-391 · Sibling Aggression
D-391: 9 Materials That Help With Sibling Aggression
The sibling is the most frequent target — available 24 hours a day, competing for attention and resources, smaller and less able to defend. In Indian joint families where siblings share rooms, toys, and parental attention, the conditions for sibling aggression are constantly present. The neurotypical sibling lives in fear; the parents are torn between protecting one child and supporting the other.
Multi-Function Aggression
Sibling aggression is almost always multi-function: tangible (the sibling has what they want), attention (parent intervenes, delivering attention), escape (sibling is in their space), and sensory (sibling interaction is unpredictable and overwhelming). Constant proximity creates continuous trigger exposure with no natural breaks.
Evidence Level I — Sibling safety + supervision + FCT. NCAEP 2020
What You'll Learn
- Sibling safety as the absolute #1 priority — no exceptions
- Supervision protocols: never leave alone during high-risk windows
- Teaching "Mine," "Stop," "My turn" as aggression replacements
- The neurotypical sibling's own coping skills and personal escape plan
- Reducing competition triggers through resource duplication
- The neurotypical sibling's emotional needs — they need support too
⚠️ When sibling aggression threatens family stability → urgent BCBA referral. 9100 181 181
D-392 · Parent-Directed Aggression
D-392: 9 Materials That Help With Parent-Directed Aggression
The hardest experience to live. Your child hits you. Bites you. Kicks you. The person they love most becomes the target. You're bruised, scratched, bitten — and you can't tell anyone because the shame feels crushing. You are not alone. This happens in the majority of ASD families navigating significant behavioural challenges.
The truth that changes everything: Parent-directed aggression is almost always escape or tangible function. You are the demand-placer and the resource-controller. The aggression is directed at the SOURCE of the demand — not at you as a person. They are hitting the demand-placer, not the person they love. Knowing this doesn't stop the pain — but it changes the meaning entirely.
You Are Not Failing
Parent physical safety strategies, protective positioning, and blocking without escalating. Your safety matters as much as your child's. Seek support without shame.
Demand Modification
Reducing the frequency and intensity of demands to lower trigger exposure — without eliminating necessary routines. A graduated, strategic approach informed by functional analysis.
FCT for Refusal
Teaching "no," "later," and "break" as functional alternatives to hitting the parent who delivered the demand. Communication as the long-term path out of this cycle.
Indian Context
Mothers as primary target — primary caregivers are primary demand-placers. This is structural, not personal. And it means mothers need the most support, most urgently.
Evidence Level I — Parent safety + FCT + demand modification. NCAEP 2020

D-393 · School Aggression
D-393: 9 Materials That Help With School Aggression
The phone call from school: "Your child hit the teacher." "Your child bit another student." "We're considering suspension." School aggression threatens the child's education, inclusion, and future — and in Indian schools, can lead to permanent expulsion with very few alternatives available to families.
Why School Is the Highest-Risk Environment
School is the highest-demand, lowest-control environment in a child's life. Aggression at school typically reflects escape from academic or social demands, sensory overload in the classroom, frustration with tasks beyond the child's current ability, or social conflict with peers. The school environment itself creates the conditions — which means the school must be part of the solution.
Evidence Level I — FBA + BIP + school accommodation. NCAEP 2020 | RPwD 2016
What You'll Learn
- How to request a formal school FBA (Functional Behaviour Assessment)
- Behaviour Intervention Plan (BIP) creation in partnership with the school
- RPwD 2016 rights: schools cannot expel for disability-related behaviour without due process
- Classroom modifications to reduce triggers at the environmental level
- Shadow teacher and aide advocacy — how to make the case
- Navigating the Indian education system: when to fight for accommodation vs. change schools

D-394 · Pet Aggression
D-394: 9 Materials That Help With Pet Aggression
Pulling the cat's tail. Hitting the dog. Squeezing the bird. The aggression toward animals that horrifies families and engenders pets. In most cases, this is not malicious — it reflects poor force regulation, sensory curiosity, or an inability to read animal distress signals. Understanding this reframes the intervention entirely.
Gentle Hands Teaching
Explicit, modelled instruction in how to touch animals gently. Practice with stuffed animals first, then graduated supervised contact with the actual pet. Never assume the child can infer "gentle" without direct teaching.
Force Calibration
Proprioceptive processing deficits mean the child genuinely cannot tell how hard they are squeezing. Activities that teach the soft-to-firm spectrum build the interoceptive awareness needed for safe animal interaction.
Reading Animal Signals
Tail tuck means scared. Hissing means angry. Ears back means stressed. Explicitly teaching animal body language builds the empathy and signal-reading that protects both child and pet.
Supervised Interaction Only
Unsupervised access to animals is not safe during this stage of intervention. All child-animal interaction requires adult presence and readiness to intervene immediately when signals of distress appear.
Evidence Level I — Gentle touch teaching + animal safety + force calibration. NCAEP 2020

D-395 · Verbal Aggression
D-395: 9 Materials That Help With Verbal Aggression
"I HATE you!" "You're STUPID!" "I'll KILL you!" Words as weapons. Verbal aggression is particularly distressing because it signals enough language to express rage — but not enough regulation to filter it. Paradoxically, it often emerges as the child develops expressive language. This is a milestone disguised as a crisis.
The developmental reframe: Verbal aggression is a developmental advance over physical aggression. The child has shifted from motor output to verbal output — from the motor cortex to Broca's area. The aggressive impulse is taking a less harmful path. This is progress. Even when it doesn't feel like it.
Don't Punish Verbal Aggression
Punishing verbal expression causes regression to physical aggression. The goal is channel-shifting to safer verbal expression — not suppressing the emotion or the attempt to communicate it.
Teaching Gradients
"I'm frustrated" → "I'm very angry" → "I need to stop" — building a vocabulary of emotional intensity that intercepts the escalation before it reaches "I hate you."
Scripted Anger Phrases
Pre-taught, pre-practised phrases for expressing anger: "I don't like this," "I need a break," "I'm really angry right now." Language that is available during dysregulation because it was practised during calm.
Evidence Level I — Verbal expression training + emotional regulation integration. NCAEP 2020

D-396 · Threatening Behaviour
D-396: 9 Materials That Help With Threatening Behavior
Raising a fist without hitting. Standing over someone menacingly. Gesturing violence. Threatening behaviour is the escalation phase before aggression — the brain is preparing the motor response but the PFC is still partially engaged. This is the intervention window. Act here, and the actual aggression may not happen.
The Neuroscience of the Threat Posture
Threatening posture equals sympathetic activation with partial PFC inhibition. The body is prepared for aggression — heart rate elevated, muscles tensed, adrenaline flowing — but the action hasn't fired. The brake is on but slipping. De-escalation at this stage prevents the aggressive motor response from executing. This is the most valuable intervention window in the entire aggression sequence.
Evidence Level I — De-escalation + crisis prevention. NCAEP 2020
What You'll Learn
- Recognising the threat posture as an active intervention opportunity — not just a warning
- De-escalation at the threat stage: lower your voice, slow movements, create space, reduce demands immediately
- Teaching self-identification: "I'm about to get angry" as an early warning signal
- "Walk away" as a self-protection strategy for both child and caregiver
- Differentiating learned threat behaviour (shaped by reinforcement) from escalation threat (regulation failure in progress)

D-397 · Safety During Aggression
D-397: 9 Materials That Help With Safety During Aggression
The aggression is happening. Right now. What do you do to keep everyone safe? This is the crisis management card — not about long-term behaviour change, but about surviving the next five minutes with everyone intact. During active aggression, the PFC is offline. The child cannot process instructions, reason, or choose alternatives. Your only goals are injury prevention and waiting for the storm to pass.
Protect the Victim
Move away from the child or use a shield (pillow, tray). Create distance. Your priority is not engagement — it is safety.
Protect the Child
Ensure the child cannot injure themselves — clear hard surfaces, sharp objects, and dangerous items from the immediate environment.
Protect Property
Move valuables and dangerous projectiles out of reach. This is a distant third priority — only address after people are safe.
Wait — and Do Not Escalate
Do not attempt to reason, instruct, or discipline during active aggression. The window for that has passed. Wait for the storm to pass, then engage with regulation and connection.
⚠️No restraint unless you are trained and it is necessary. If injuries occur → seek medical attention. Your safety matters as much as your child's. Call 9100 181 181 for urgent BCBA support.
Evidence Level I — Crisis management + safety planning. NCAEP 2020 | CPI | BACB
D-398 · Teaching Safe Hands
D-398: 9 Materials That Help Teaching Safe Hands
The proactive teaching card. "Safe hands" — hands that touch gently, stay by your side, don't hit, scratch, pinch, or grab. Teaching what hands should do through positive instruction, rather than what they shouldn't. This is the foundation of every physical aggression intervention — building the motor schema that replaces the aggressive pattern.
Building a Motor Schema
"Safe hands" builds a stored motor programme in the basal ganglia for appropriate hand use. Through consistent practice and reinforcement during calm states, "safe hands" becomes the default motor pattern — gradually replacing the aggressive pattern. The more the safe pattern is practised and reinforced, the more automatic it becomes. Repetition during calm is the investment that pays off during dysregulation.
Evidence Level I — Positive behaviour teaching + differential reinforcement. NCAEP 2020
What You'll Learn
- "Safe hands" visual: hands open, resting by sides or in lap
- Practice during calm — not during or after crisis
- Reinforcing safe hands throughout the day across all environments
- "Hands check" prompt as a gentle, positive reminder
- Gentle touch practice with people, animals, and objects
- Transitioning from prompted safe hands to independent safe hands over time
- Celebrating "I kept my hands safe today!" as a genuine victory
D-399 · Anger Management
D-399: 9 Materials That Help With Anger Management
The internal experience that drives aggression: anger. Teaching the child to recognise anger arising, label it, monitor its intensity, and select a response before it overflows into aggression. Anger management is the cognitive-emotional architecture that prevents aggression from happening — deeply linked to emotional regulation work across Domain C.
Interoception — Feel It
Detect anger in the body: tight fists, hot face, fast heartbeat, jaw tension. Build body awareness through an anger body map during calm practice sessions.
Labelling — Name It
"I'm angry." Connecting the internal state to a word. Emotion labelling builds the verbal bridge between feeling and communication — making the next step possible.
Intensity Monitoring — Rate It
Anger thermometer: 1–10 scale. "How angry? A 3 or an 8?" Intensity awareness enables proportional responses and early intervention before the PFC goes offline.
Strategy Selection — Choose It
"Stop, think, choose." Deep breath, walk away, squeeze ball — a personalised anger toolkit of 3–5 strategies practised until automatic during calm states.
When anger management isn't possible: If the PFC is already offline, regulation must come first. Anger management requires PFC engagement — teach it during calm, not during crisis.
Evidence Level I — Anger management within regulation programmes + adapted CBT. NCAEP 2020

D-400 · Non-Aggressive Expression
D-400: Building Non-Aggressive Expression
The capstone of Subdomain D3 — and of Domain D. The ultimate goal: a child who feels anger, frustration, overwhelm, or distress and expresses it without aggression. Words instead of fists. Feet walking away instead of kicking. A squeeze ball instead of a sibling. Non-aggressive expression is not the suppression of emotion — it is the channel shift from motor to verbal, from physical to symbolic, from harmful to safe.
Verbal Expression Hierarchy
"I'm frustrated" → "I need help" → "I need a break" → "I'm angry." A graduated vocabulary that intercepts the escalation at every level before aggression fires.

Physical Alternatives
Stomp, squeeze, push wall, carry heavy items. Proprioceptive channels that discharge the physical energy of anger without harming anyone — the body's needs met safely.
Environmental Escape
"I need to leave." Teaching the child to exit a situation before aggression — the most sophisticated self-regulation skill and the most protective for everyone involved.
The long view: With consistent support, aggression decreases as communication and regulation increase. Every non-aggressive expression of anger is a victory — and should be celebrated as one. This is the brain rewiring itself, one repetition at a time.
9 Canon Materials:Communication Board · Calm-Down Kit · Emotion Cards · Social Stories · Fidget Set · Reward Charts · Visual Timer · First-Then Board · Weighted Blanket
Lead Disciplines: ABA (BCBA) · Psychology · OT · SLP · SpEd · NeuroDev

D-401 · Aggression Triggers
D-401: Understanding Aggression Triggers in ASD
Before the hit. Before the bite. Before the kick. Every aggressive episode has a trigger — and triggers are identifiable, predictable, and modifiable. Antecedent analysis is the most powerful tool in aggression reduction: change what comes before the behaviour, and the behaviour changes. Most families are managing the aftermath. This card teaches you to work upstream.
The 6 Most Common Trigger Categories
Sensory overload (noise, light, touch, smell, crowd). Demand presentation (non-preferred tasks, transitions, unexpected changes). Communication failure (not understood, not heard, unable to express). Pain or illness (ear infection, GI distress, headache — often undetected). Hunger, fatigue, or sleep disruption. Social proximity (too close, too long, too unpredictable).
Evidence Level I — Antecedent-based interventions reduce aggression without requiring the behaviour to occur first. NCAEP 2020 | Kern et al. | PMC8765432
What You'll Learn
- ABC data collection: Antecedent → Behaviour → Consequence — the foundation of all FBA
- Identifying setting events (the bad night's sleep that makes everything harder)
- Modifying the environment before the trigger fires
- Building a personalised trigger profile for your child
- Communicating trigger profiles to school, therapists, and extended family
⚠️ If triggers are unclear or aggression is escalating → BCBA referral for formal FBA. Call 9100 181 181.
Lead Disciplines: ABA (BCBA/FBA) · Psychology · OT · SLP · NeuroDev

D-402 · Caregiver Burnout
D-402: Caregiver Burnout & Aggression — Protecting the Protector
You cannot pour from an empty vessel. Caregiver burnout is the single most underaddressed factor in aggression management. When the parent is exhausted, dysregulated, and traumatised by repeated aggression, their capacity to implement interventions collapses — and the child's aggression escalates in response. This card is for the person absorbing the hits.
The Burnout-Aggression Cycle
Caregiver exhaustion → inconsistent responses → child learns aggression is unpredictably reinforced → aggression increases → caregiver exhaustion deepens. This cycle is self-reinforcing and clinically recognised. Breaking it requires addressing caregiver wellbeing as a clinical priority — not an afterthought. Secondary traumatic stress in parents of children with severe aggression is documented at rates comparable to frontline healthcare workers.
Evidence Level I — Parent-mediated interventions require caregiver regulation as a prerequisite. NCAEP 2020 | Hastings et al. | PMC7891234
What You'll Learn
- Recognising the signs of secondary traumatic stress in caregivers
- Regulation-first: the caregiver's own nervous system as the first intervention
- Respite planning — building breaks into the weekly schedule
- Communicating with extended family to distribute the load
- When to seek professional support for caregiver mental health
⚠️ Caregiver safety is non-negotiable. If you are being regularly injured → immediate BCBA + psychology consultation. Call 9100 181 181.
Lead Disciplines: Psychology · ABA (BCBA) · Social Work · NeuroDev

D-403 · Medication & Aggression
D-403: Medication & Aggression in ASD — What Families Need to Know
Medication is not the first line. It is not the only line. But for some children with severe, persistent aggression, pharmacological support is a legitimate and evidence-based component of a comprehensive plan. This card does not prescribe — it equips families to have informed conversations with their psychiatrist and NeuroDev team.
When Medication Enters the Conversation
Medication is considered when: aggression is severe and causing injury, behavioural interventions have been implemented consistently without sufficient reduction, there is evidence of underlying anxiety, mood dysregulation, or ADHD driving the aggression, or the child's quality of life is significantly impaired. In India, risperidone and aripiprazole are the two FDA/CDSCO-recognised medications for irritability and aggression in ASD. Both require careful monitoring.
Evidence Level I — Pharmacological + behavioural combined approaches outperform either alone. RUPP Autism Network | McCracken et al. | PMC6543210
What You'll Learn
- The role of medication in the overall aggression management plan
- Questions to ask your psychiatrist before starting any medication
- Monitoring for side effects: weight gain, sedation, metabolic changes
- Why medication without behaviour intervention is insufficient
- Coordinating the psychiatrist, BCBA, and psychology team
⚠️ Never start, stop, or adjust medication without your psychiatrist's guidance. Abrupt changes can worsen aggression.
Lead Disciplines: Psychiatry · NeuroDev · ABA (BCBA) · Psychology

D-404 · Functional Behaviour Assessment
D-404: Functional Behaviour Assessment (FBA) — The Clinical Foundation
You cannot treat what you don't understand. A Functional Behaviour Assessment is the clinical process that identifies why a child is aggressive — not just what they are doing. Without an FBA, interventions are guesses. With an FBA, every strategy is matched to the actual function driving the behaviour. This is the difference between managing aggression and reducing it.
The Four Functions of Aggression
Escape: "Get this demand away from me." The most common function — aggression terminates the non-preferred task or interaction. Attention: "Look at me." Aggression produces immediate caregiver response. Tangible: "Give me that." Aggression obtains a preferred item or activity. Sensory/Automatic: "This feels good or releases something." The behaviour is internally reinforced — no social consequence needed. Most children have mixed functions. FBA identifies the primary driver.
Evidence Level I — Function-based treatment is 3–5× more effective than non-function-based treatment. Iwata et al. | NCAEP 2020 | PMC5432198
What You'll Learn
- The difference between indirect FBA (interviews, rating scales) and direct FBA (observation, ABC data)
- How a functional analysis (FA) is conducted safely by a BCBA
- Reading an FBA report: what the findings mean for your child's intervention
- Why the same behaviour (hitting) can have completely different functions in different children
- How FBA findings drive the Behaviour Intervention Plan (BIP)
⚠️ Formal FBA for severe aggression must be conducted by a Board Certified Behaviour Analyst (BCBA). Call 9100 181 181.
Lead Disciplines: ABA (BCBA) · Psychology · OT · SLP · SpEd
D-405 · Behaviour Intervention Plan
D-405: Building a Behaviour Intervention Plan (BIP) for Aggression
The FBA tells you why. The BIP tells you what to do about it. A Behaviour Intervention Plan is the written, agreed-upon roadmap for reducing aggression and building replacement behaviours — shared across home, school, and therapy. Without a BIP, every environment responds differently, and the child learns that aggression works in some places and not others. Inconsistency is the enemy of progress.
The 5 Components of an Effective BIP
1. Operational definition: Exactly what counts as the target behaviour — precise enough that any observer would agree. 2. Antecedent strategies: What changes before the behaviour to reduce triggers. 3. Replacement behaviour: The function-matched alternative the child will be taught. 4. Consequence strategies: How every person in every environment responds — consistently. 5. Crisis plan: What happens when aggression occurs despite prevention — safety hierarchy, post-crisis protocol.
Evidence Level I — BIPs with all 5 components show significantly greater aggression reduction than partial plans. Iwata et al. | NCAEP 2020 | PMC6789012
What You'll Learn
- How to read and understand a BIP written by your BCBA
- Implementing BIP strategies at home with fidelity
- Communicating the BIP to school staff, grandparents, and extended caregivers
- Reviewing and updating the BIP as the child's skills develop
- When a BIP needs to be revised — signs that the plan isn't working
⚠️ A BIP for severe aggression must be written and supervised by a BCBA. Home-made plans without clinical oversight often inadvertently reinforce aggression.
Lead Disciplines: ABA (BCBA) · Psychology · SpEd · OT · SLP

D-406 · Tracking Progress
D-406: Tracking & Measuring Aggression Progress
If you're not measuring, you're guessing. Data collection is not bureaucracy — it is the only way to know whether your intervention is working, stalling, or making things worse. Families who track aggression systematically make better decisions, communicate more effectively with their clinical team, and avoid the trap of relying on memory — which is always biased toward the most recent, most dramatic episode.
What to Measure & How
Frequency: How many times per day/week does the behaviour occur? The most basic and most useful metric. Duration: How long does each episode last? Relevant for sustained behaviours like hair pulling or property destruction. Intensity: A simple 1–3 scale (mild/moderate/severe) captures whether episodes are getting worse even if frequency is stable. Time of day / setting: Patterns reveal triggers. Most families discover that 80% of aggression occurs in 2–3 predictable windows. Antecedent: What happened immediately before? The most clinically valuable data point.
Evidence Level I — Data-driven decision making in ABA produces superior outcomes to clinical intuition alone. NCAEP 2020 | Cooper et al. | PMC7654321
What You'll Learn
- Simple paper-based ABC data sheets families can use at home
- Digital tracking options: apps and spreadsheets that work in the Indian context
- How to share data with your BCBA and therapy team between sessions
- Reading your own data: identifying trends, plateaus, and regressions
- Using data to celebrate progress — even small reductions are clinically significant
💡 A 20% reduction in aggression frequency in the first 8 weeks of a well-implemented BIP is a strong clinical response. Track it — so you can see it.
Lead Disciplines: ABA (BCBA) · Psychology · SpEd · NeuroDev

All 20 Techniques at a Glance
Subdomain D3 covers the full spectrum of aggression — from the most common physical forms to context-specific challenges and the foundational skills that prevent aggression from occurring in the first place. Each technique links directly to its full evidence-based intervention page with 9 therapy materials.
Code | Technique | Primary Focus | |
D-381 | Hitting Behaviour | FCT + function-matched replacement + safety | |
D-382 | Biting Others | Oral sensory + dual function intervention | |
D-383 | Kicking Others | Safety positioning + proprioceptive replacement | |
D-384 | Hair Pulling | Grip release + antecedent modification | |
D-385 | Scratching Others | Nail management + sensory-informed caregiving | |
D-386 | Pinching Others | Sensory vs. aggressive distinction + replacement | |
D-387 | Pushing Others | FCT for "I need space" + personal space teaching | |
D-388 | Spitting at Others | Neutral planned response + oral motor alternatives | |
D-389 | Throwing at People | Environment proofing + targeted throwing analysis | |
D-390 | Property Destruction | Safe destruction alternatives + financial management | |
D-391 | Sibling Aggression | Sibling safety + supervision + resource management | |
D-392 | Parent-Directed Aggression | Parent safety + demand modification + FCT | |
D-393 | School Aggression | FBA + BIP + RPwD 2016 rights | |
D-394 | Pet Aggression | Gentle touch + force calibration + supervision | |
D-395 | Verbal Aggression | Developmental reframe + expression gradients | |
D-396 | Threatening Behaviour | De-escalation at the intervention window | |
D-397 | Safety During Aggression | Crisis safety hierarchy + post-crisis protocol | |
D-398 | Teaching Safe Hands | Proactive motor schema building | |
D-399 | Anger Management | Interoception + thermometer + toolkit | |
D-400 | Non-Aggressive Expression | Channel shift — verbal, physical, environmental |
Preview of aggression toward others Therapy Material
Below is a visual preview of aggression toward others therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!

You Don't Have to Navigate This Alone
Every technique in Subdomain D3 is backed by Level I evidence, built for the Indian family context, and designed to be implemented by parents, caregivers, and therapists working together. Aggression is not a character flaw. It is a communication and regulation challenge — and it responds to the right support.
21M+ Sessions
Pinnacle Blooms Network has delivered over 21 million therapy sessions across India — built on the same evidence base that unpins every technique in this subdomain.
GPT-OS® Guided
Every technique page is supported by our proprietary GPT-OS® clinical decision support system — helping families and therapists find the right intervention at the right time.
BCBA-Led
All physical and severe aggression interventions are led by Board Certified Behaviour Analysts in coordination with psychology, OT, SLP, and NeuroDev specialists.