
Untitled card
View more
The Recognition Moment
ACT I — THE STORY "The mashed potatoes were perfect — not a single lump. But before the spoon even touched their lips, they saw the bowl and started gagging. Another meal turned into a war. Another night I cried after bedtime. I don't know if this is sensory, behavioral, or if something is wrong with their mouth. I just know my child is shrinking their world of food — one texture at a time." You are not failing. Your child's nervous system is speaking — loudly, and in the only language it knows. This is not willfulness. This is neurology. FREE National Autism Helpline: 9100 181 181 — Available 24x7 in 16+ languages. Pinnacle Blooms Consortium® | Episode E-454 | Feeding & Mealtime Skills | Ages 1–12 years






- Oral sensory hypersensitivity — reducing gag threshold to age-appropriate levels
- Texture tolerance range — expanding from 1–2 safe textures to a full texture spectrum
- Oral motor skill development — chewing patterns, bolus formation, jaw strength
- Mealtime anxiety — reducing anticipatory distress and visual-triggered refusal
- Food variety — expanding accepted foods through systematic chaining
- Mixed texture tolerance — building capacity for foods with multiple consistencies
- Social eating participation — birthday parties, school lunches, family meals
- Nutritional adequacy — reducing reliance on smooth/limited textures
- Self-regulation — child learns to anticipate and manage own texture responses
- Independence — child develops self-advocacy about food preferences vs. aversions
- Reduction in gag frequency per meal (trackable in GPT-OS®)
- Increase in number of accepted food textures (Texture Diversity Index)
- Reduced pre-meal anxiety behaviors
- Willingness to touch/interact with previously refused textures








Material | Commercial | Zero-Cost DIY Alternative | |
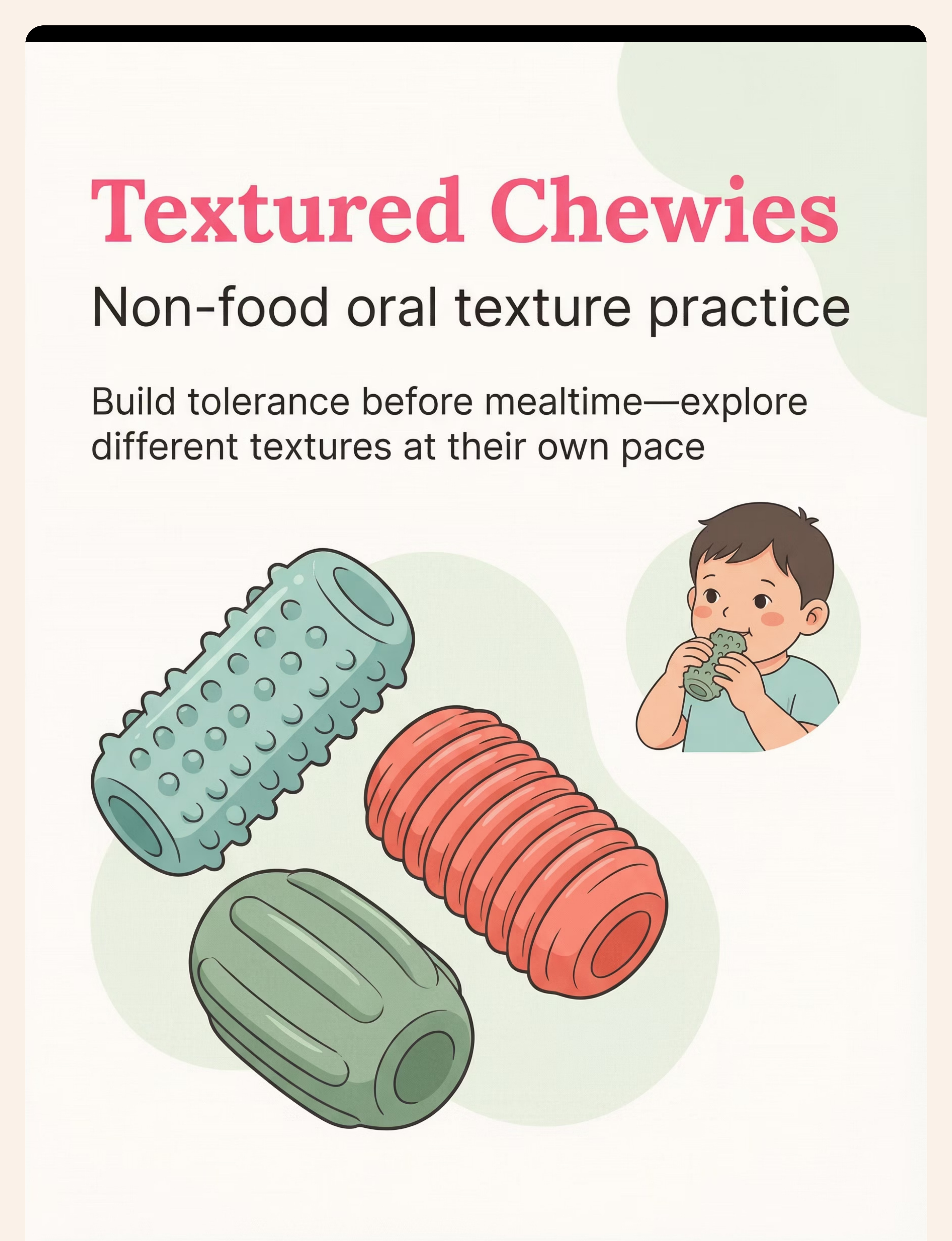
Textured Chewy | ₹300–1,200 | Silicone teething ring (toddlers) or washcloth twist | |
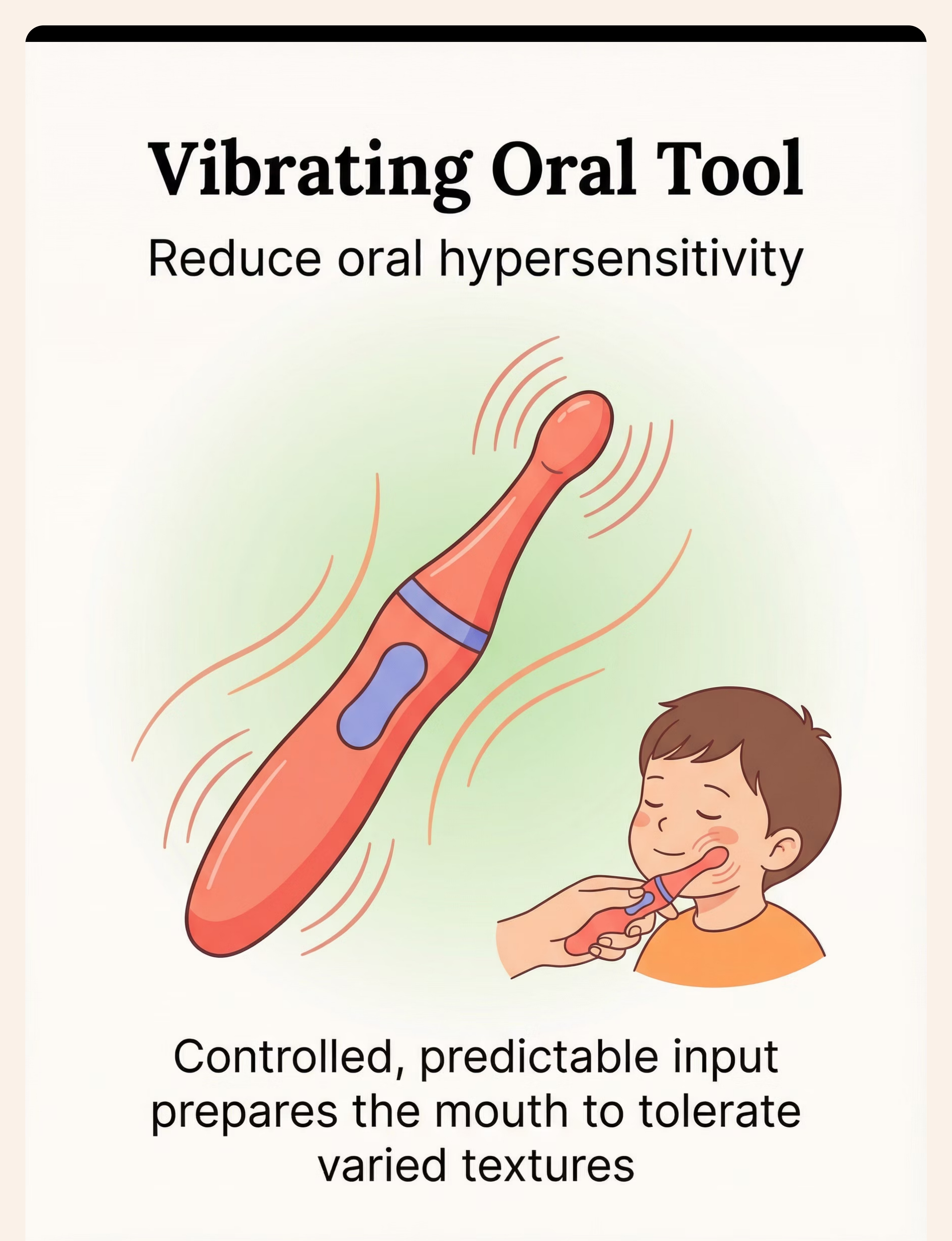
Vibrating Tool | ₹500–2,000 | Electric toothbrush (off-brand ₹150–300) on lips/cheeks | |
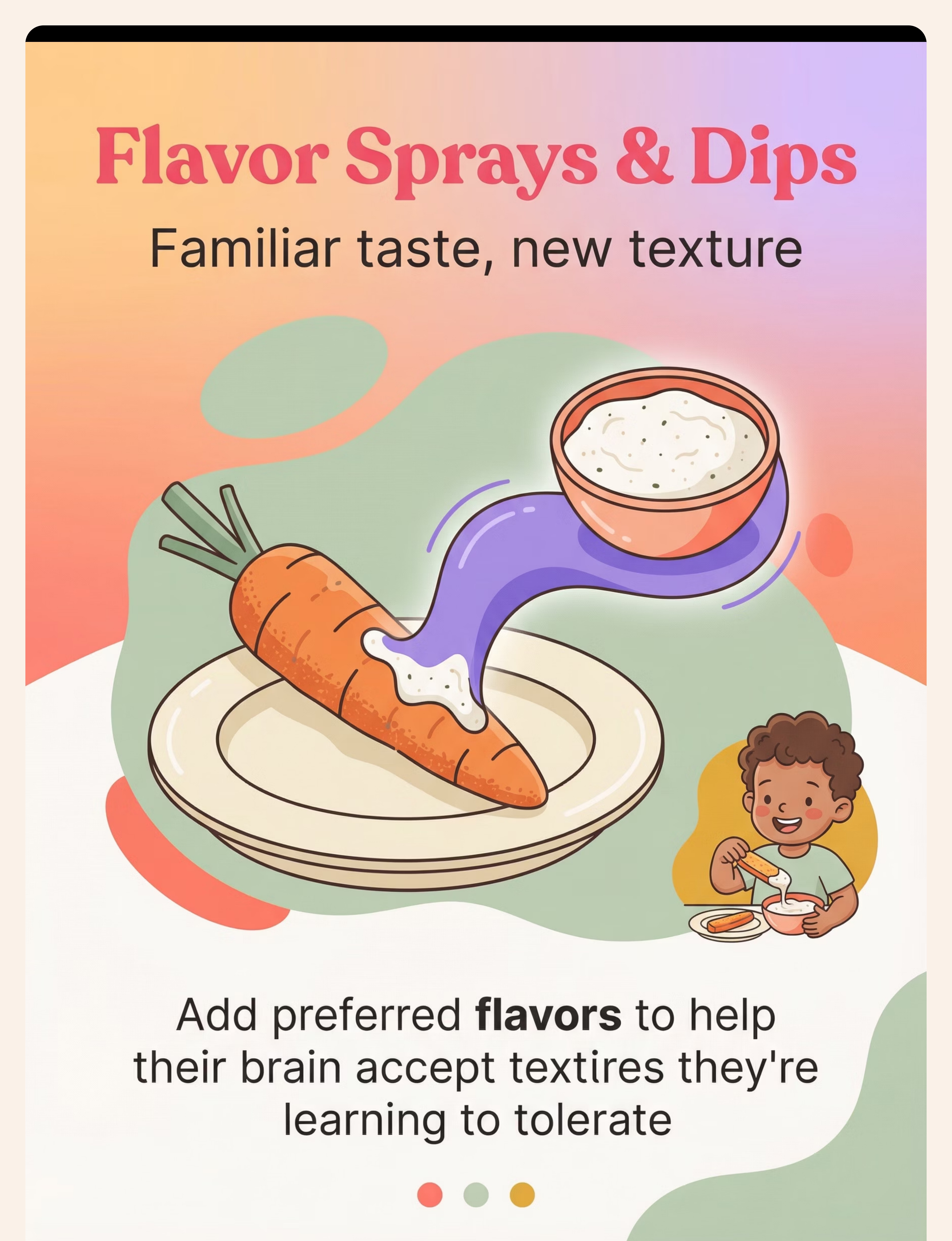
Flavor Dips | ₹200–800 | Kitchen condiments they already like — butter, ketchup, sugar | |
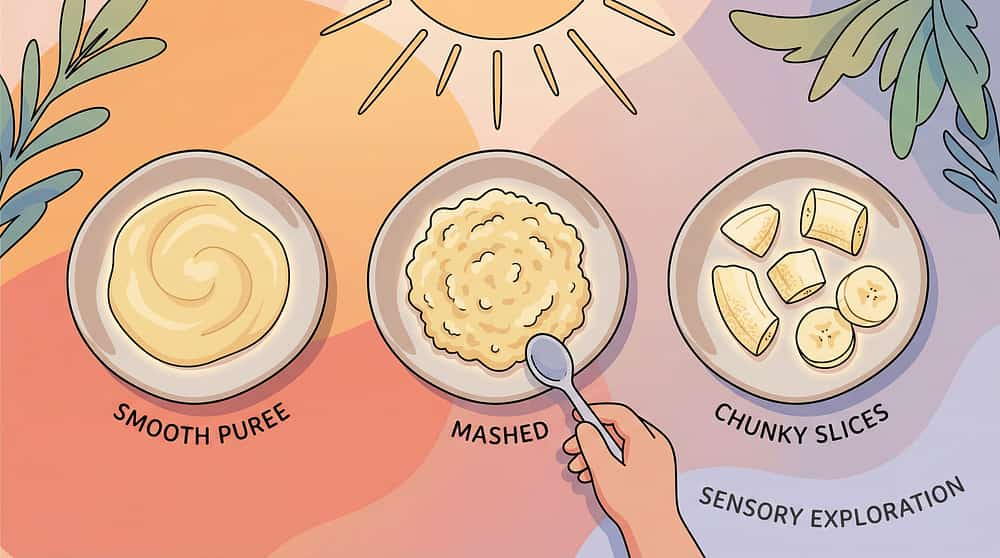
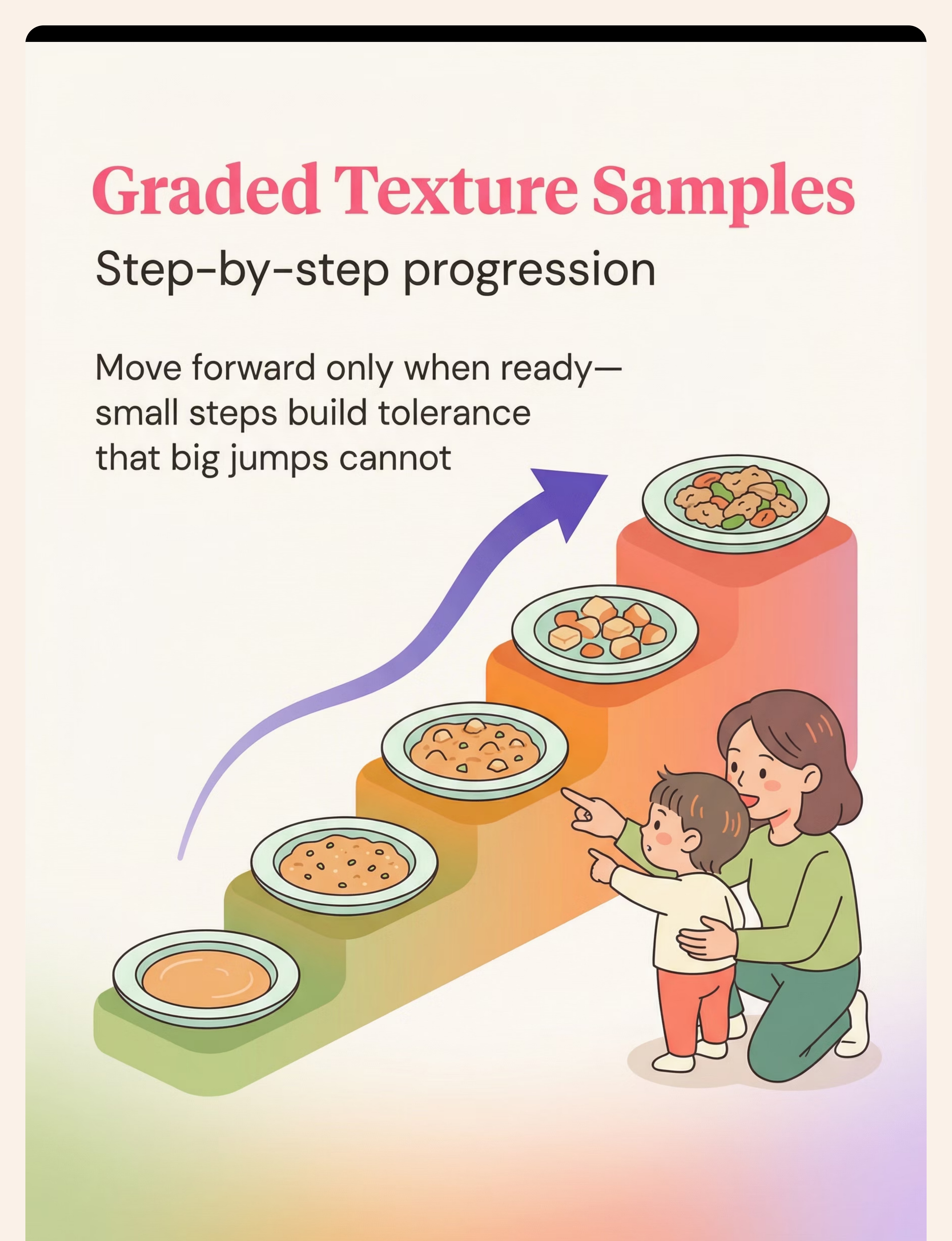
Texture Ladder | Food costs only | Same food prepared 5 ways from smooth to chunky | |
Food Interaction Tools | ₹100–500 | Kitchen toothpicks, regular tongs, fork for mashing | |
Sensory Play | ₹200–1,000 | Homemade play dough, rice bin, cooked pasta, cornstarch gloop | |
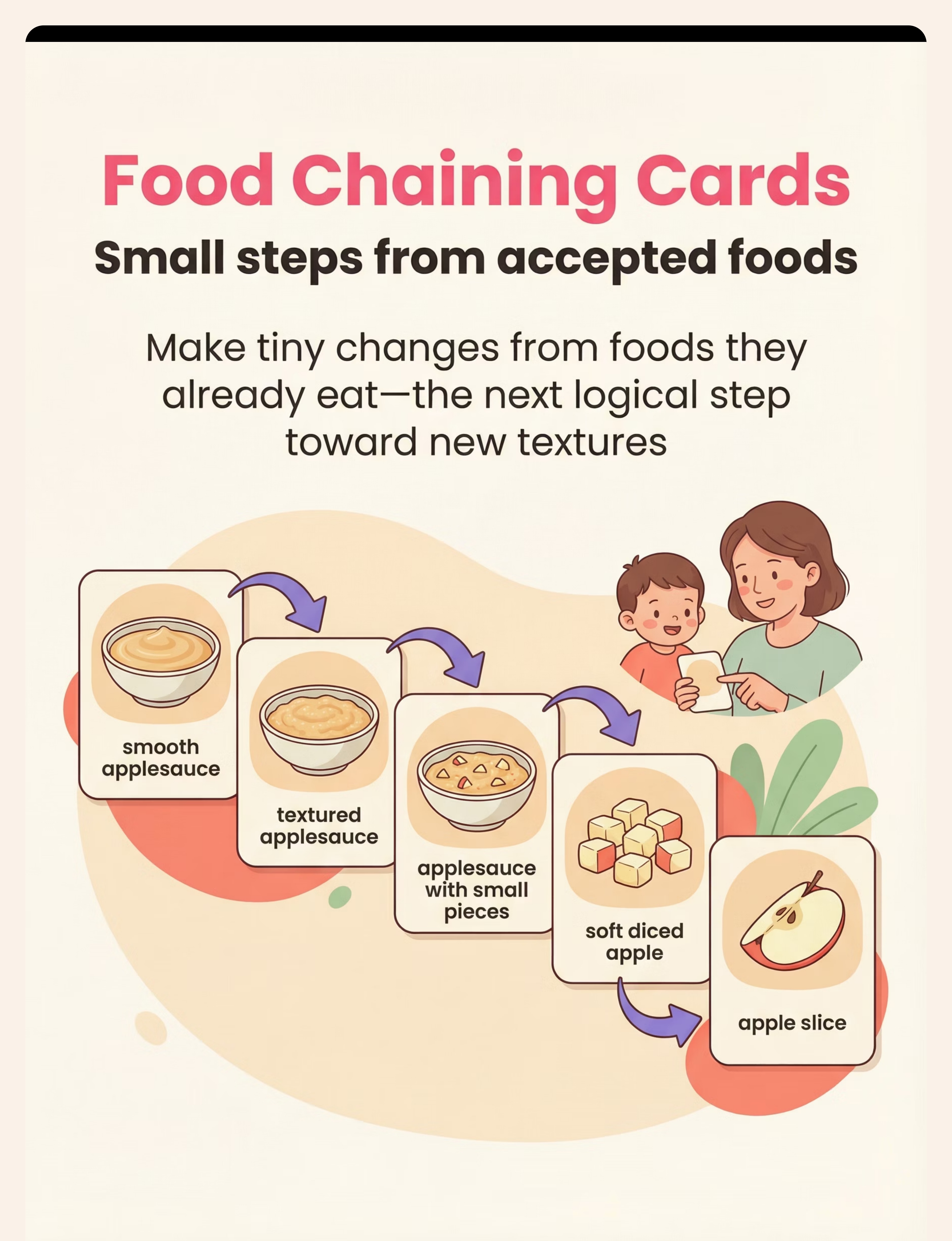
Food Chaining Cards | ₹500–1,500 | Paper + crayon drawings or phone photos, laminate with tape | |
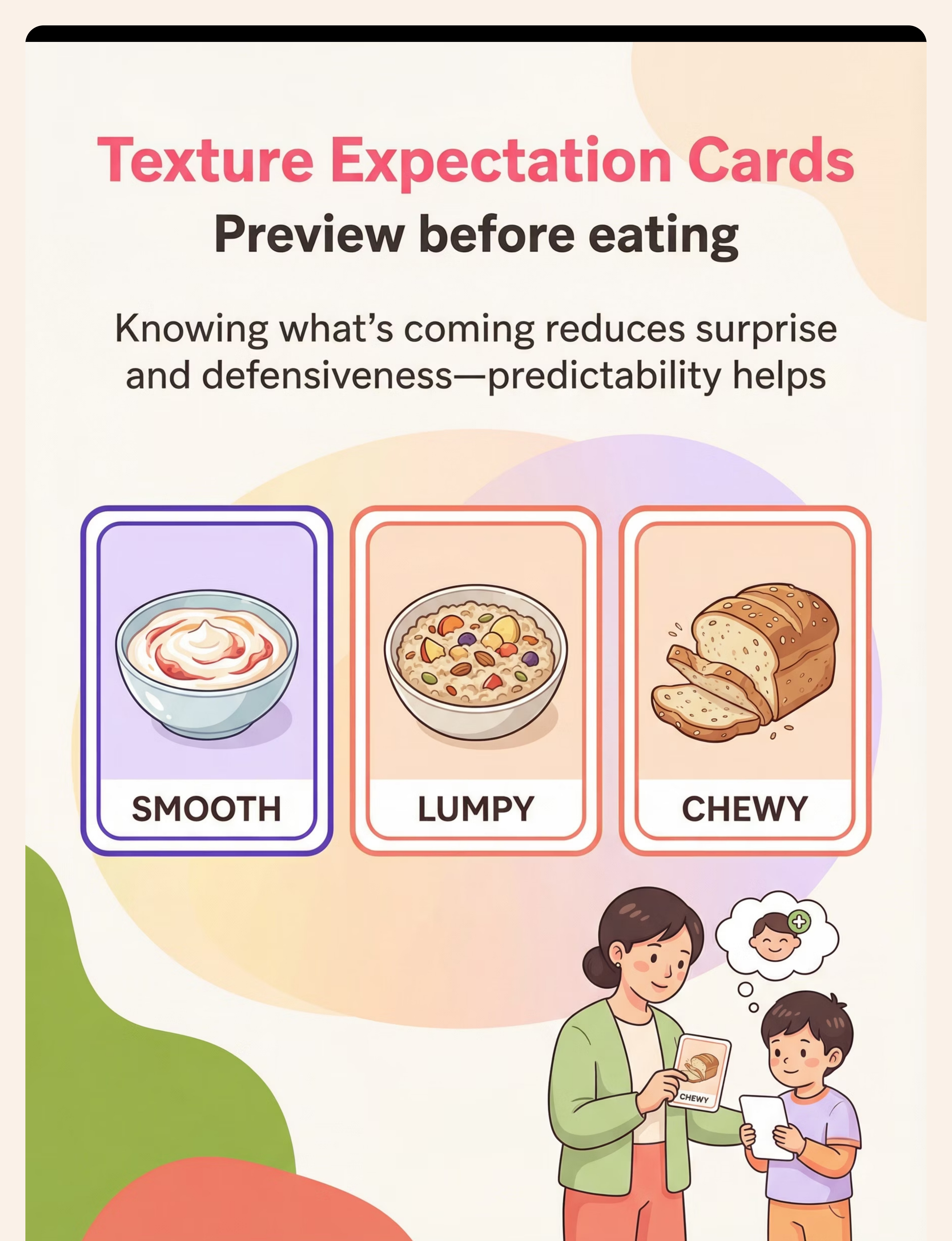
Texture Expectation Cards | ₹200–800 | Print food photos + laminate or use plastic sheet protector | |
Oral Motor Games | ₹200–1,000 | Bubbles (₹30), party blowers, regular straws + water |

- Active vomiting, diarrhea, or GI distress
- Fever or illness
- Suspected structural oral issue — consult SLP/ENT first
- Significant weight loss or nutritional concerns — medical evaluation FIRST
- Child in acute distress or post-meltdown (within 30 minutes)
- Suspected ARFID requiring clinical diagnosis — refer to feeding specialist
- Child is tired, excessively hungry, or overstimulated
- Previous meal ended badly — allow 3+ hours recovery
- New food being introduced — use only familiar materials
- Heightened sensory sensitivity today — use lighter-intensity materials
- Child is fed, rested, and in a calm/available regulatory state
- Environment is prepared and distraction-free
- Parent is regulated and pressure-free
- Materials are clean, intact, and age-appropriate

Step 1: The Invitation — Oral Sensory Warm-Up
ACT III — STEP 1 OF 6 ⏱ 10–15 minutes Begin With the Body — Not the Food "Hey [name], want to do our mouth games before we eat? Pick your chewy/buzzy thing." The oral sensory warm-up is not optional — it is the sensory preparation that makes subsequent food introduction possible. Administer using the textured chewy and/or vibrating tool before any food appears. Acceptance Cues — Child Is Ready Relaxed jaw, reduced facial tension Self-directed engagement with tool Verbal or gestural signal of readiness Resistance Cues — Back Off Turning away or hand-blocking Vocalizing distress Increased body tension

"Look what we have today — [food name]. Can you see what it looks like? What do you think the texture is?"
- ❌ Jumping more than one micro-step at a time
- ❌ Mixing a new texture with a new taste simultaneously
- ❌ Pressuring "just one more bite" after a distress signal
- ❌ Praising eating the texture while ignoring the interaction


Step 6: The Cool-Down
ACT III — STEP 6 OF 6 ⏱ 2–3 minutes End Right — Protect Tomorrow's Session No session ends abruptly. The cool-down protects the child's regulatory state and preserves the positive association with future mealtimes. How you end this session determines how the child enters the next one. Transition warning (30–60 sec out) "Two more tries, then all done with our texture work." Visual timer Show 1–2 minutes remaining with visual timer tool or phone countdown. Put-away ritual Child helps put away interaction tools — builds agency and closure. Proprioceptive input Push hands against table, bear hug, 5 chair push-ups — brief heavy work to regulate. Transition to safe food Offer 1–2 completely accepted foods for the remainder of the meal. Final celebration "Our texture practice is done! You did amazing today." "Texture practice is done. Now it's just regular eating time."

- Session date + duration (minutes)
- Today's target texture
- Highest interaction level: Proximity / Tool-touch / Finger-touch / Lips / Lick / Tiny taste / Bite
- Gag count: 0 / 1 / 2 / 3+
- Child distress level: 0–10
- Ready to advance? Yes / Not yet / Regressed
- Feeding Independence Readiness Index
- Oral Sensory Tolerance Readiness Index
- Texture Diversity Readiness Index
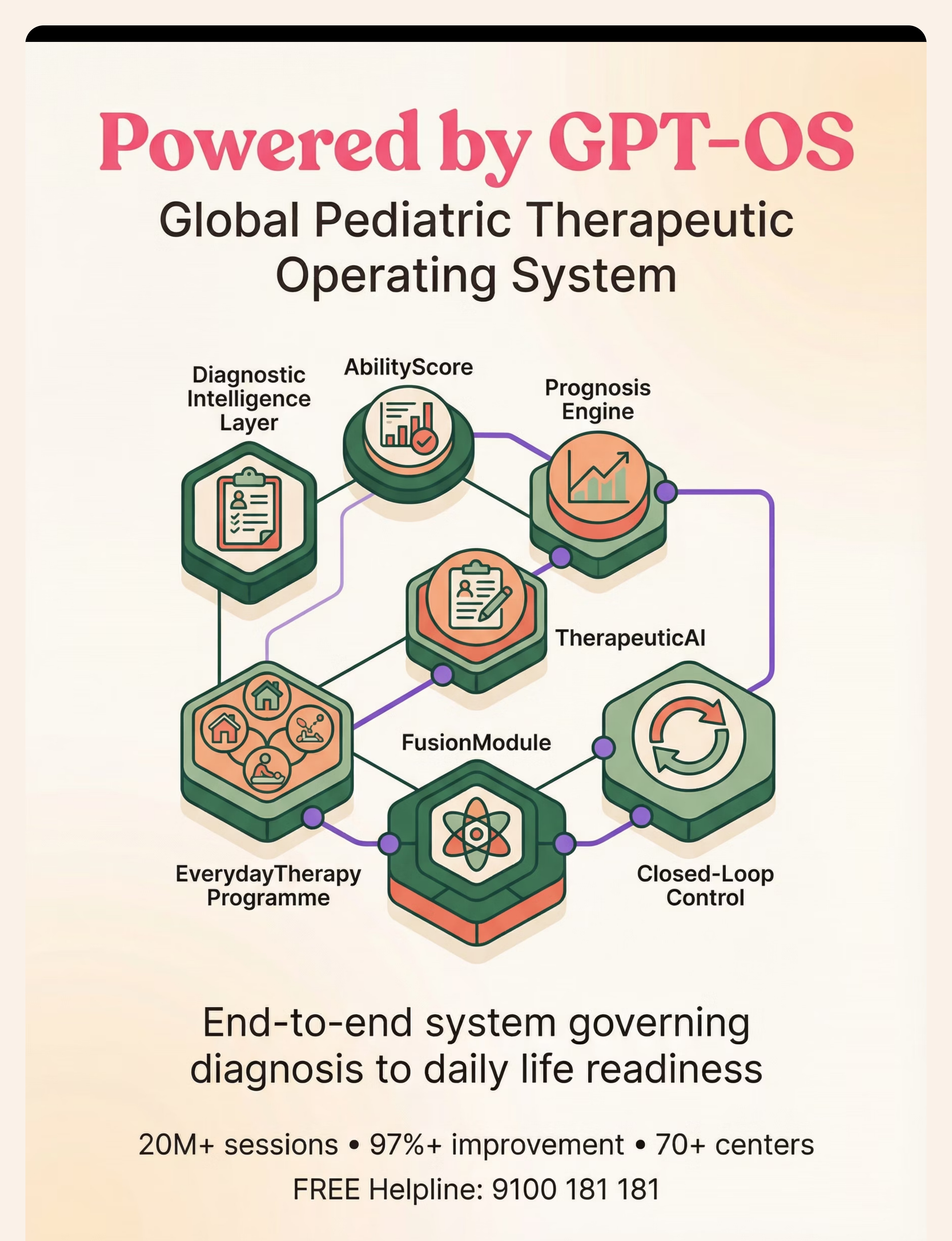
- TherapeuticAI® personalized next-step recommendations

When Sessions Go Wrong — Clinical-Grade Troubleshooting
ACT IV — TROUBLESHOOTING Problem Likely Cause Solution Child gags immediately on seeing food Visual aversion is the trigger Start with food completely off the table. Introduce texture expectation card first. Progress: food in room → on plate → engagement. Accepted textures yesterday refused today Sensory fluctuation / state-dependent Go back one step. Check readiness. Use oral warm-up longer. State fluctuates — it's normal. No progress after 4 weeks Steps are too large Break into even smaller micro-steps. Consult SLP/OT. Review food chaining — is the gap too big? Child only accepts flavor dip, not texture Taste dependency developing Reduce dip amount by 10% each session. Goal is texture tolerance, not flavor bridge dependence. Gagging frequency increasing Over-exposure / advancing too fast Immediately reduce texture challenge. Increase oral warm-up time. Allow more sessions at current level. Parent getting frustrated Caregiver burnout This is real and valid. Call 9100 181 181. Parent regulation is a prerequisite to child progress. Sibling disruption Environmental control Session timing must be protected. Sibling in another room or with another caregiver. Escalate to professionals if: Weight loss or growth concerns | No texture expansion after 6–8 weeks | Gagging leading to vomiting regularly | Suspected ARFID. Pinnacle assessment path: AbilityScore® → Comprehensive Feeding Evaluation → FusionModule™ OT + SLP + Behavioral intervention.

- ✅ Child tolerates oral sensory warm-up without distress
- ✅ Engages with texture expectation cards willingly
- ✅ Gag frequency may INCREASE slightly before decreasing — desensitization is working
- ✅ Interacts with target texture via tool (not yet touching)
- ✅ 2–3 "proximity without distress" moments per session
- ❌ Actual eating of new textures
- ❌ Zero gag events
- ❌ Consistent acceptance across all meals
"If your child tolerates the texture for 3 seconds longer than last week — that is real, measurable, neurological progress."

Weeks 3–4: Neural Pathways Are Forming
ACT IV — PROGRESS Progress: ████████░░ 40% Weeks 3–4 mark a visible shift. When you see your child approach the target food with curiosity instead of dread — even once — you are watching new neural pathways form. The brain is literally rewiring its "this is dangerous" classification of that texture. Child begins to anticipate the oral warm-up positively Gag frequency drops 20–30% from baseline Child uses food interaction tools spontaneously (without prompting) First instances of voluntary finger-touch to target texture Child starts to categorize textures using expectation card language Slight generalization: tolerance of texture in unexpected settings Advance one micro-step when: Child completes current texture level without distress for 3 consecutive sessions. Reduce flavor dip support slightly when child initiates food interaction spontaneously.
"Around week 6, something clicked. He poked the banana piece with his pick, then just... put it in his mouth. No drama. Like it was the most normal thing. I cried." — Parent, Pinnacle Network (Illustrative case; outcomes vary)
Mastery Is Not a Destination — It's a Continuous Expansion
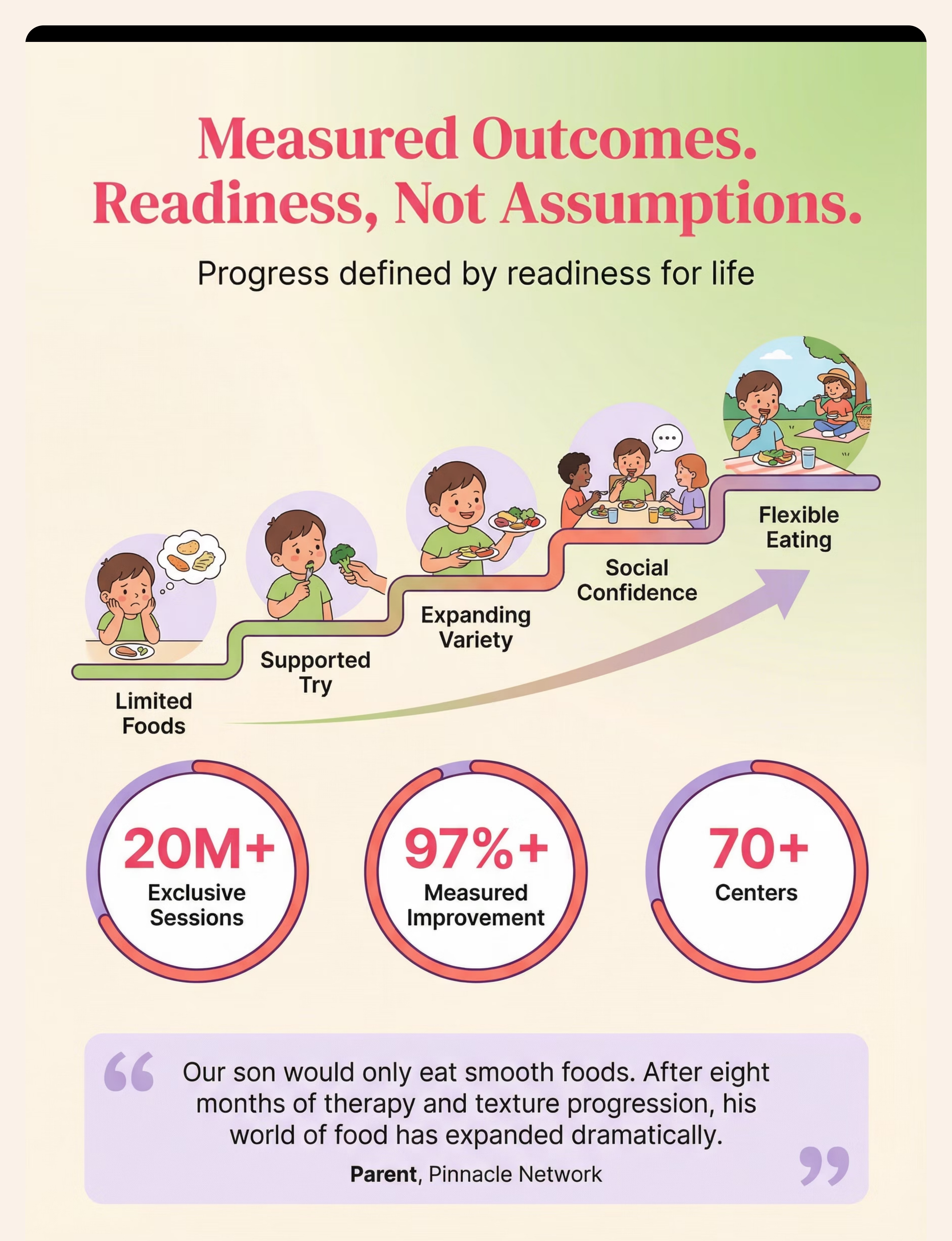
ACT IV — MASTERY Stage 1 Tolerates oral sensory warm-up tools with positive engagement Stage 2 Interacts with target food without immediate distress Stage 3 Takes tiny tastes of new texture voluntarily Stage 4 Eats portion of target texture within a familiar food chain Stage 5 Generalizes texture tolerance to social eating settings — birthday parties, school lunches, family meals "Our son would only eat completely smooth foods — purees, yogurt, specific crackers. Eight months of consistent texture work, food chaining, and oral sensory prep. He now eats mashed food with pieces, soft fruits, and is working on mixed textures. His world of food has expanded dramatically." — Parent, Pinnacle Network (Outcomes vary) AbilityScore® Readiness Progression: Severe restriction → Emerging tolerance → Developing variety → Advancing independence → Flexible eating

E-453: New Food Refusal — food introduction hierarchy + trust-building
Reel | Title | Level | Materials You Already Have | |
E-452 | Mealtime Refusal | Intro | Sensory tools, Visual cards | |
E-453 | New Food Refusal | Intro | Food chaining cards | |
E-457 | Gagging on Textures | Core | All E-454 materials ✓ | |
E-458 | Chewing Difficulty | Core | Oral motor tools | |
E-472 | Food Chaining Deep Dive | Advanced | Food chaining cards | |
E-482 | Mixed Food Aversion | Advanced | Texture expectation cards |

— Priya M., Hyderabad(Outcomes vary)
— Arjun K., Bengaluru(Outcomes vary)
— Meena R., Chennai(Outcomes vary)

Available 24x7
- AbilityScore® Assessment → pinnacleblooms.org/assessment
- Feeding-specific evaluation → Request via helpline
- Center locator → pinnacleblooms.org/centers

- Gag threshold pattern — which textures trigger, at what frequency
- Oral warm-up effectiveness — does duration correlate with session success?
- Food chaining velocity — sessions needed to advance one micro-step
- Flavor bridge dependency — is the child becoming reliant on dips?

This web page is the full clinical expansion of the Reel. Video modeling is classified as evidence-based practice for autism (NCAEP 2020) — multi-modal learning (visual + text + demonstration) improves parent skill acquisition.
- Reel ID: E-454
- Domain: E — Feeding & Mealtime Skills
- Series position: Episode 454 of 999
- Duration: 75–85 seconds
- Therapist: Pinnacle Feeding Therapy Consortium Lead
- ← E-453: 9 Materials That Help With New Food Refusal
- → E-455: 9 Materials That Help When Foods Can't Touch
- → E-457: 9 Materials That Help With Gagging on Textures
#FoodTextureAversion #SensoryFeeding #PinnacleBlooms #GPT_OS


Your Child's Texture World Can Expand — Start Today
ACT VI — START NOW Validated by the Pinnacle Blooms Consortium® | Occupational Therapy • Speech-Language Pathology • ABA • Special Education • NeuroDevelopmental Pediatrics • Feeding Therapy 🟢 Start This Technique Today Launch your GPT-OS® E-454 Guided Session and begin building your child's texture tolerance with a personalized, data-driven home program. Start E-454 Guided Session 🟡 Book a Feeding Therapy Assessment Schedule at your nearest Pinnacle center for a comprehensive feeding evaluation with our OT + SLP + Feeding Specialist consortium. Book Assessment ⚪ Explore the Next Technique Ready to go further? Explore related techniques in the Feeding & Mealtime Skills cluster — your E-454 materials work for all of them. Browse Domain E Sessions Delivered Measured Improvement Centers Across India Countries Served FREE National Autism Helpline: 9100 181 181 — 24x7 | 16+ languages | Always free, always available.
Preview of 9 materials that help with food texture aversions Therapy Material
Below is a visual preview of 9 materials that help with food texture aversions therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.


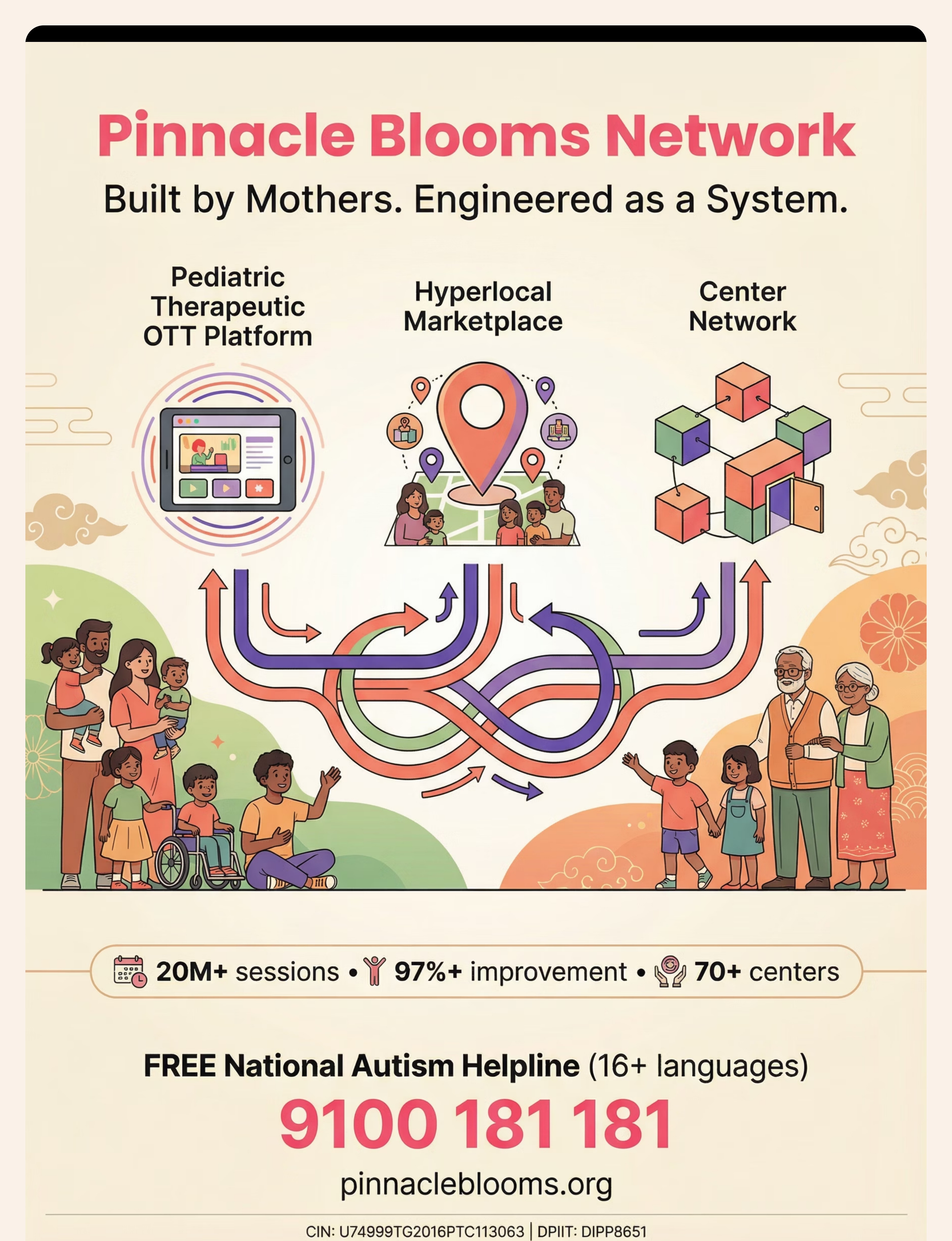






"From fear to mastery. One texture at a time. One mealtime at a time. One child at a time." — Pinnacle Blooms Network®, Built by Mothers. Engineered as a System.