When food stays in chunks they can't break down.
You watch them chew and chew. The food never breaks down. Or they barely chew at all and try to swallow it whole.
Dinner is tense. You've cut everything into tiny pieces, but they still struggle. Meat gets spit out. Vegetables get refused. Their cheeks fill with food that sits there long after the meal is over. Other kids their age eat pizza and crackers and raw carrots. Your child is still on soft foods — not by choice, but because they simply cannot manage the texture.
You are not failing. Your child's oral motor system is still developing — and it can be trained.
Pinnacle Blooms Consortium®
Ages 1–10
~12 min read
WHO Nurturing Care Framework (2018) | ASHA Feeding Guidelines | PMC11506176 | SLP • OT • ABA • SpEd • NeuroDev | Feeding & Mealtime Independence Series — Episode 458

Millions of families are navigating this exact mealtime.
Chewing difficulty — medically termed Mastication Disorder or Oral Motor Dysfunction — is one of the most common feeding concerns seen by Pinnacle's Speech-Language Pathologists and Occupational Therapists across 70+ centers. You are among millions of families in India and globally who are navigating restricted diets, stressful mealtimes, and the fear of choking.
25–35%
Neurodevelopmental
Children with neurodevelopmental conditions experience significant feeding difficulties
70–80%
ASD-Related
Children with ASD report oral motor or texture challenges affecting diet breadth
1 in 6
All Children
All children experience some form of feeding challenge during development
📊 Pinnacle Network data: Oral motor and chewing difficulties represent the 2nd most frequent referral category within our Feeding Therapy program, spanning families across 20+ Indian cities and 70+ countries served through GPT-OS®.
"Your child isn't being difficult. Their jaw, tongue, and cheeks need the same training any muscle group needs — targeted, consistent, evidence-based work." — Pinnacle Blooms SLP Consortium
PMC11506176 | PMC10955541 | ASHA Pediatric Feeding Position Statement | WHO NCF 2018

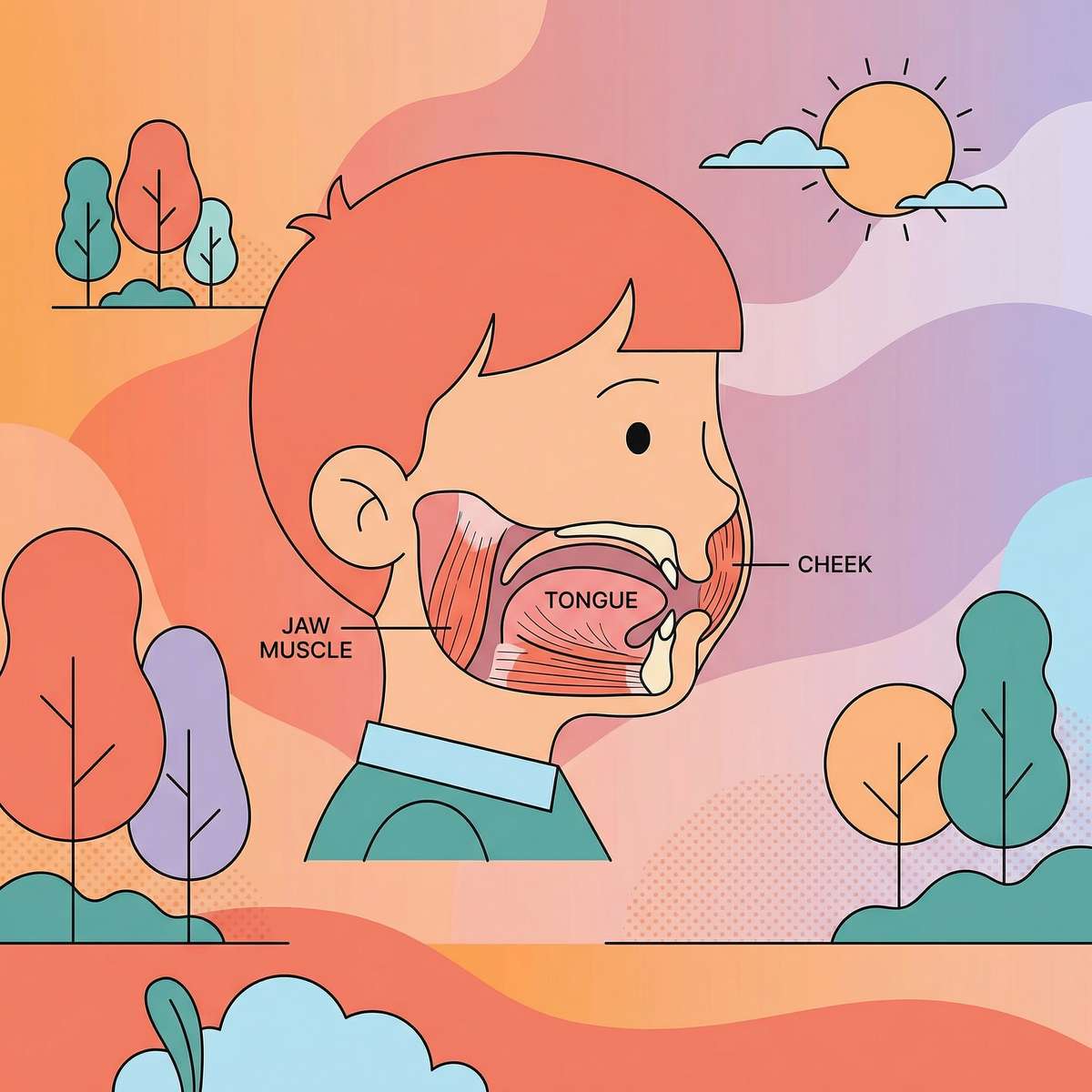
Chewing is not automatic. It's a learned motor skill — and muscles can be built.
The 6 Components of Effective Chewing
① Jaw Strength
Masseter and temporalis muscles must generate enough force to break down food. Weak jaw muscles = food stays in chunks.
② Jaw Grading
The jaw must modulate force for different textures. Steak requires different force than banana. Poor grading = biting too hard or too softly.
③ Rotary Jaw Pattern
Mature chewing is circular, not just up-and-down. Children with immature "munching" patterns can't grind food efficiently.
④ Tongue Lateralization
The tongue must sweep food sideways onto the molars. If the tongue stays in the middle, food never reaches the grinding surfaces.
⑤ Cheek Tension
Cheeks must maintain inward pressure to keep food between the teeth, not pocket in the sulci (cheek folds).
⑥ Oral Sensory Awareness
The child must feel where food is, whether it's been adequately chewed, and when it's ready to swallow.
💡When any of these 6 components is weak or uncoordinated, chewing efficiency breaks down. Intervention targets the specific deficit — not generic "chewing practice."
Frontiers in Integrative Neuroscience (2020) | ASHA Oral Motor Guidelines | ARK Therapeutic Clinical Research
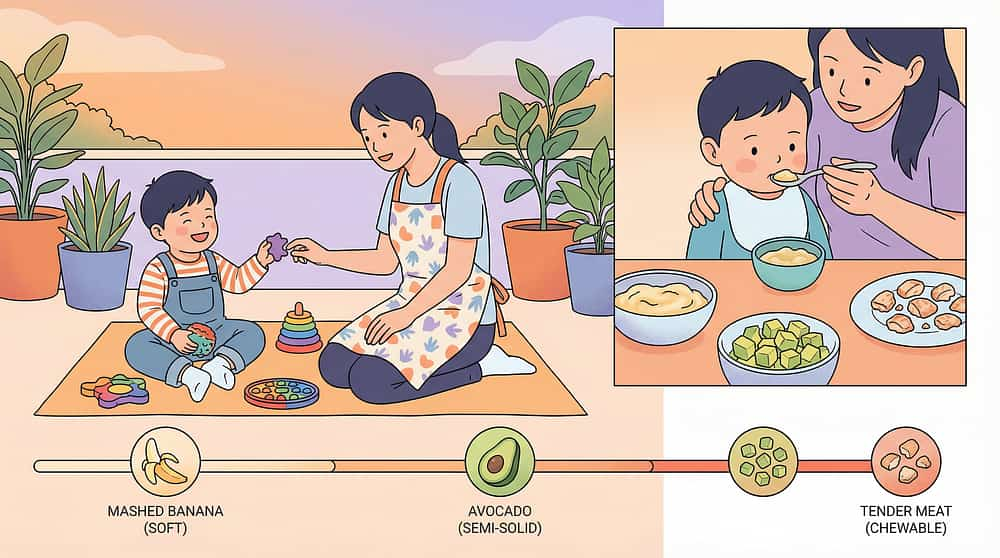
Your child's chewing journey — and exactly where the challenge sits.
Mature chewing with efficient breakdown of all textures — including resistant foods like raw vegetables and meat — is typically established by age 4–5 years. Children with oral motor challenges may be at an earlier developmental stage than their chronological age suggests. This is not a permanent ceiling. It is a waypoint with a clear forward path.
6–8 Months
MUNCHING — up-down jaw. Soft dissolvable first foods.
9–12 Months
DIAGONAL jaw movement. Soft-mashable, some soft lumps.
12–18 Months
EMERGING ROTARY. Soft-mechanical textures, variety.
18–24 Months
REFINED ROTARY PATTERN. Wider texture range including ground meats.
24–36 Months
MATURE with ENDURANCE. Most textures including firmer foods.
3–5 Years
ALL TEXTURES. Raw vegetables, crusty bread, full dietary range.
🔑Chewing difficulty is not a behavioral choice. It is a neurodevelopmental motor challenge. These are muscles. Muscles respond to training.
Chewing difficulty commonly co-occurs with:
- Sensory Processing Differences (tactile defensiveness in the mouth)
- Low Oral Muscle Tone (hypotonia)
- Autism Spectrum conditions
- Cerebral Palsy
- Down Syndrome
- General Developmental Delay
- Prolonged use of pureed/soft-only diet
WHO Care for Child Development (CCD) Package | UNICEF MICS developmental monitoring | PMC9978394

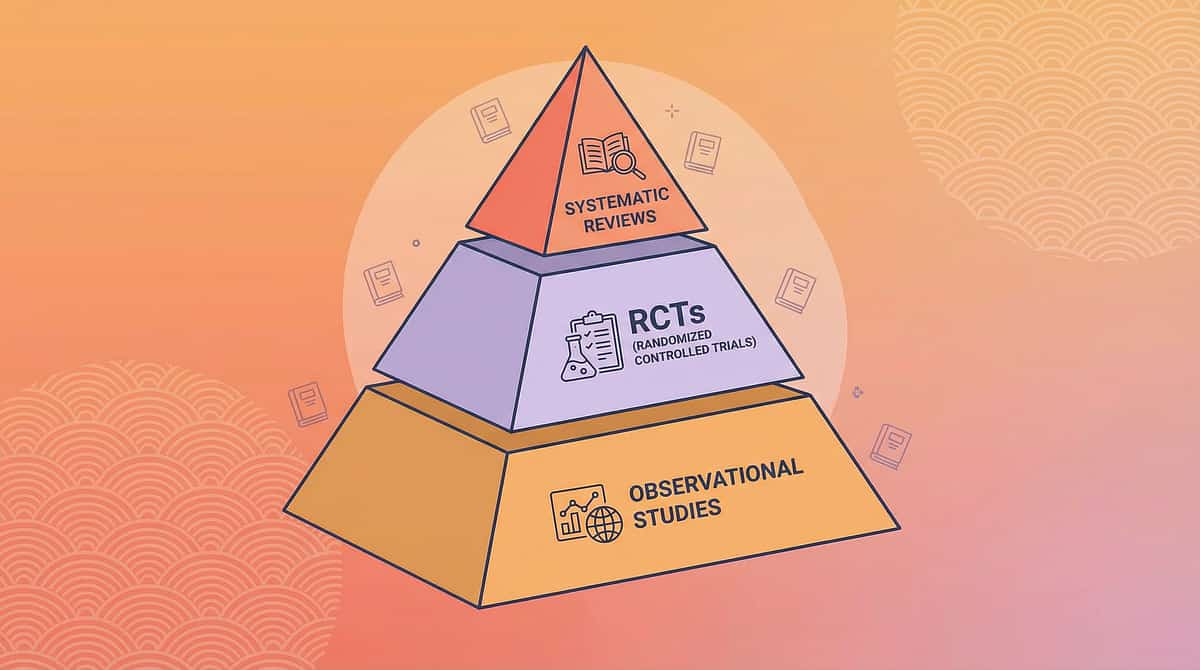
Evidence Grade: LEVEL I — Systematic Review Validated
🛡️ Clinically Validated
Oral Motor Intervention for Pediatric Feeding
📄 ASHA Systematic Review
Oral motor exercises have an evidence base for improving jaw strength, tongue coordination, and feeding efficiency in pediatric populations when systematically applied.
📄 Indian Journal of Pediatrics RCT (2019)
Padmanabha et al.: Home-based feeding interventions using structured oral motor programs demonstrated significant improvement in children with developmental feeding challenges. DOI: 10.1007/s12098-018-2747-4
📄 PRISMA Systematic Review (2024)
PMC11506176: Multi-disciplinary sensory and motor interventions meet evidence-based practice criteria for children with neurodevelopmental conditions.
📄 NCAEP (2020)
Structured skill-building programs for feeding and oral motor development are classified as evidence-based practice.
92%
Clinical Confidence
Aggregate confidence rating across reviewed evidence for oral motor intervention efficacy in pediatric feeding
"Clinically validated. Home-applicable. Parent-proven." | Helpline: 9100 181 181 | PMC11506176 | PMC10955541 | PMC9978394 | DOI: 10.1007/s12098-018-2747-4 | NCAEP 2020 | ASHA

9 Materials That Help With Chewing Difficulty
Feeding / Oral Motor
Ages 1–10
5–15 min daily
SLP + OT Lead
Parent-Friendly Alias:"Building the Chewing System: Jaw, Tongue, Cheeks, and Awareness"
Formal Clinical Domain: Mastication Disorder / Oral Motor Dysfunction Intervention / Chewing Skill Development / Oral Phase Feeding Therapy
Formal Clinical Domain: Mastication Disorder / Oral Motor Dysfunction Intervention / Chewing Skill Development / Oral Phase Feeding Therapy
Chewing (mastication) is a complex oral motor skill requiring the coordinated action of multiple muscle groups and neurological pathways. When this coordination is weak, immature, or disorganized, food cannot be adequately broken down for safe swallowing. This technique page introduces 9 categories of therapeutic materials — each targeting a specific component of the chewing system — that can be used at home, at mealtimes, and as part of a structured oral motor program guided by your therapist.
🟢 Oral Motor Tools
Chewy Tubes, ARK Grabber, Z-Vibe
🟢 Chew Jewelry
Food-safe silicone chewelry
🟢 Graded Texture Foods
Food Texture Hierarchy Kit
🟢 Oral Sensory Tools
Nuk Brush, textured toothbrush
🟢 Jaw Resistance Tools
Full-range jaw exercisers
🟢 Cheek & Lip Tools
ARK Lip Blok, bubble toys, button-string

This technique spans every discipline — because the mouth is everyone's territory.
Speech-Language Pathologist (Lead)
Primary driver of oral motor assessment and intervention. The SLP evaluates jaw strength and grading, tongue lateralization, lip closure, oral sensory awareness, and swallowing safety. They design the oral motor exercise program, determine appropriate food texture level, and progress the child through the texture hierarchy.
Occupational Therapist (Co-Lead)
Addresses sensory factors affecting feeding — oral tactile defensiveness, proprioceptive processing, and the broader sensory profile determining which textures are tolerable. They integrate oral motor work into daily routines and adaptive seating/positioning for optimal feeding posture.
ABA / BCBA (Behavioral Support)
When mealtime avoidance, food refusal, or escape behaviors co-occur with the oral motor challenge, the BCBA designs the reinforcement schedule, manages behavioral components of texture introduction, and ensures the intervention is functionally connected to mealtimes.
Neuro-Developmental Pediatrician (Medical Oversight)
Rules out structural, neurological, and medical causes. Ensures chewing difficulty is not secondary to an undiagnosed condition (tongue tie, structural anomaly, neurological disorder) requiring medical or surgical management before behavioral intervention.
"This technique crosses therapy boundaries because the mouth doesn't organize by therapy type. Jaw muscles, tongue coordination, sensory awareness, and behavior are all happening simultaneously at every meal." — Pinnacle Blooms FusionModule™ Clinical Principle
Precision targeting: Every material on this page hits a specific component.
Observable Indicators — What You Will See When It Improves
Target | What you will SEE when it improves | |
Jaw Strength | Child manages firmer foods without fatigue | |
Tongue Lateralization | Food no longer stays in center of mouth; cheek pocketing reduces | |
Oral Sensory Awareness | Child notices and clears food from cheeks spontaneously | |
Cheek Tension | Food stays between teeth during chewing; less falls out | |
Dietary Variety | Child attempts new textures without gagging |
PMC10955541 | ASHA Oral Motor Targets | Pinnacle AbilityScore® Feeding Domain Metrics

9 Materials. 9 Therapeutic Targets. One Complete Chewing System.
Each material below targets a different component of chewing. Together, they build the complete oral motor skill set.

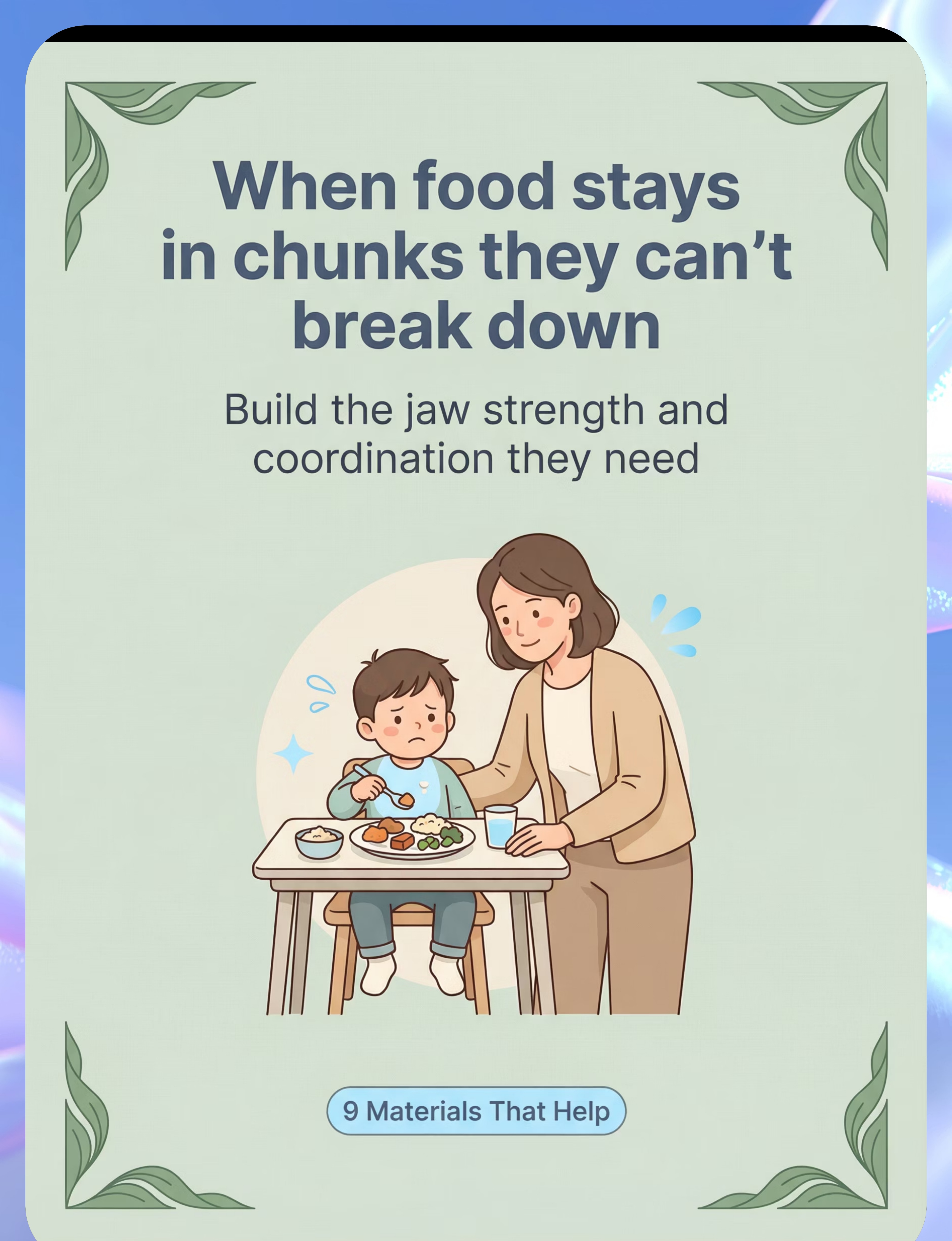
🟢 1. Chewy Tubes (Knobby & Smooth)
Build jaw strength through controlled resistive biting. Exercises masseter, temporalis, and pterygoid muscles safely without food. Smooth for beginners; knobby for advanced oral motor input.
💰 ₹300–800 | 🏥 Therapeutic Grade

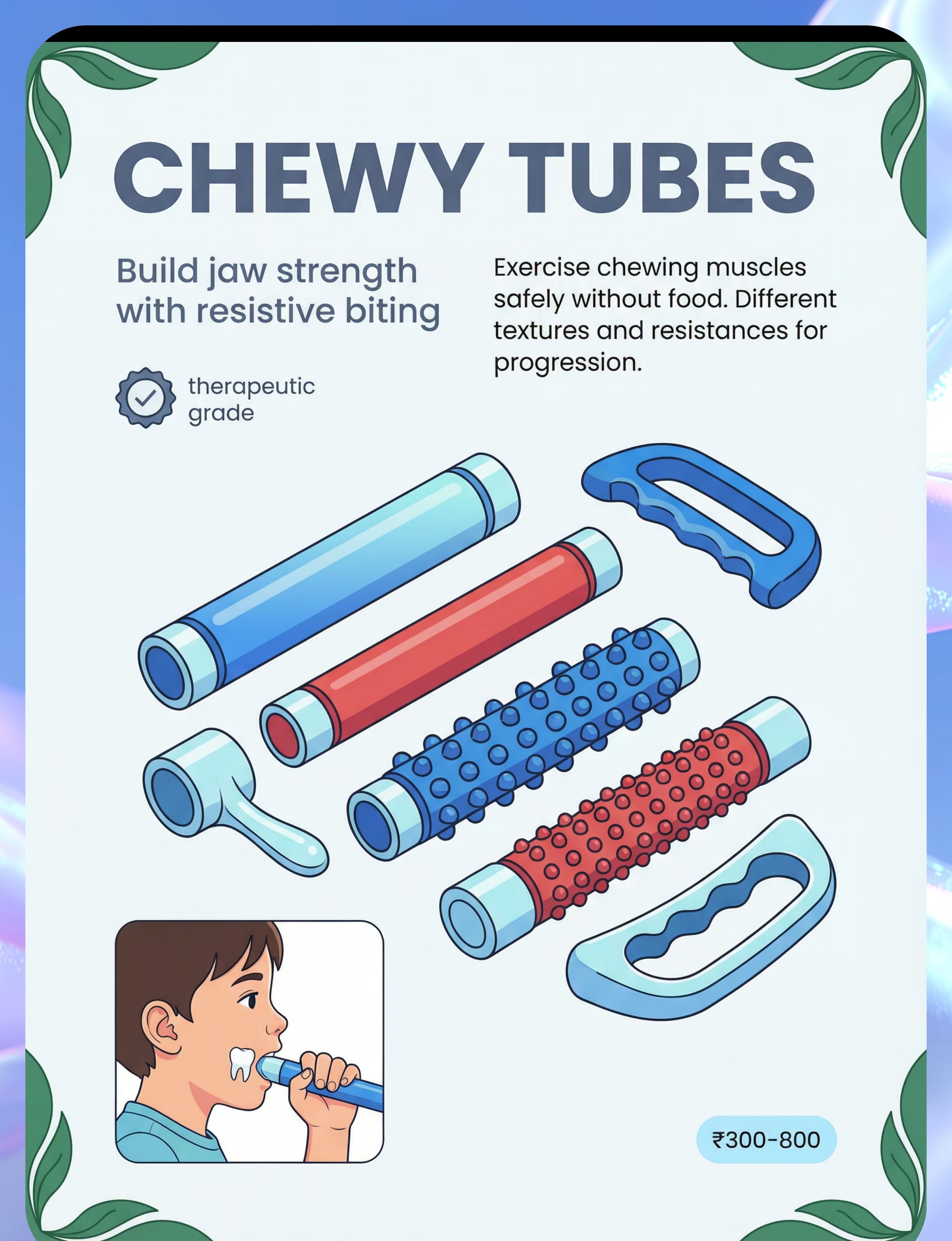
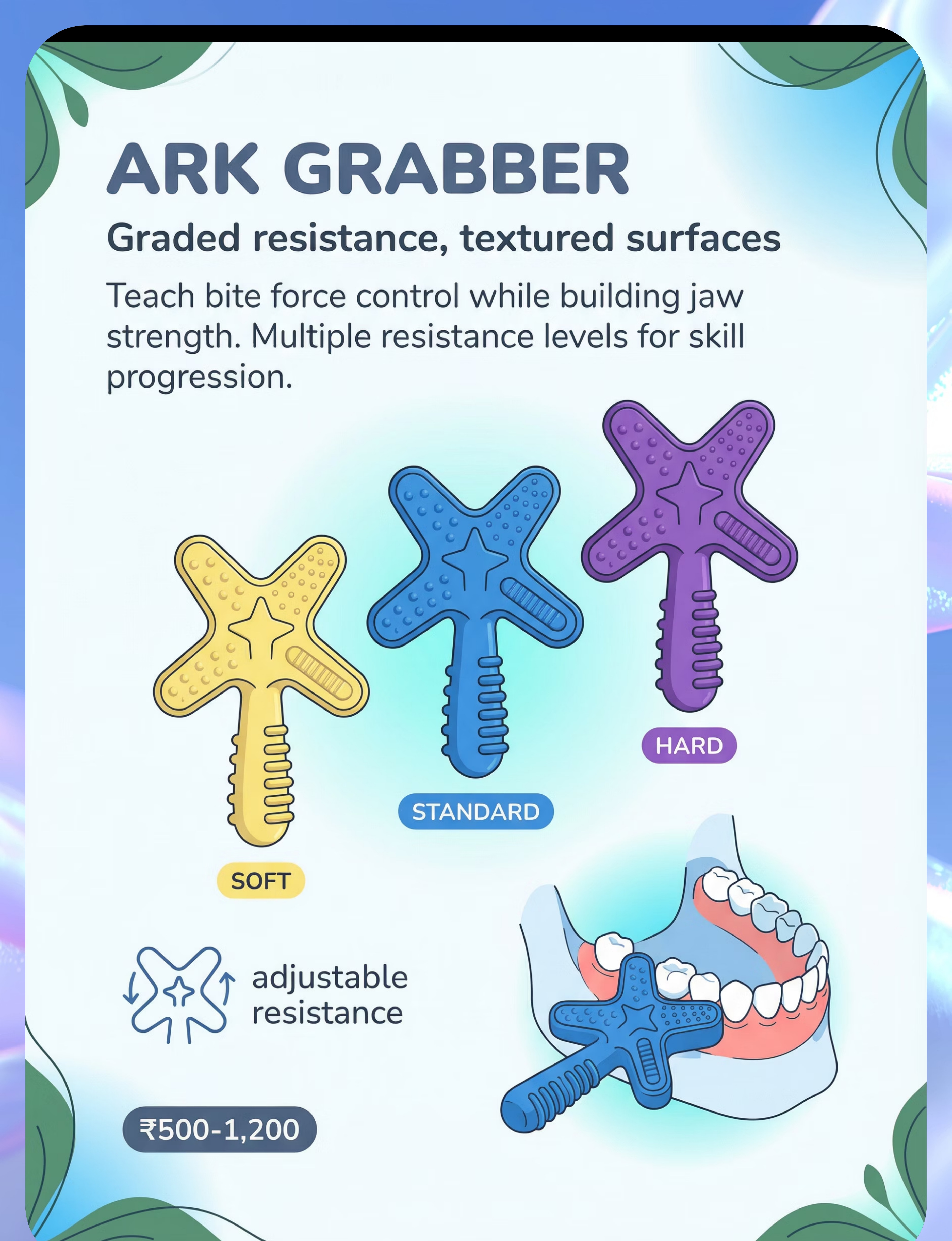
🟢 2. ARK Grabber® / Oral Motor Chew Tool
Graded resistance levels (Soft → Standard → Hard) teach jaw muscles to modulate bite force. Star/cross-arm design enables biting on all surfaces. Develops jaw grading control essential for mixed-texture meals.
💰 ₹500–1,200 | 🏥 Clinical Grade

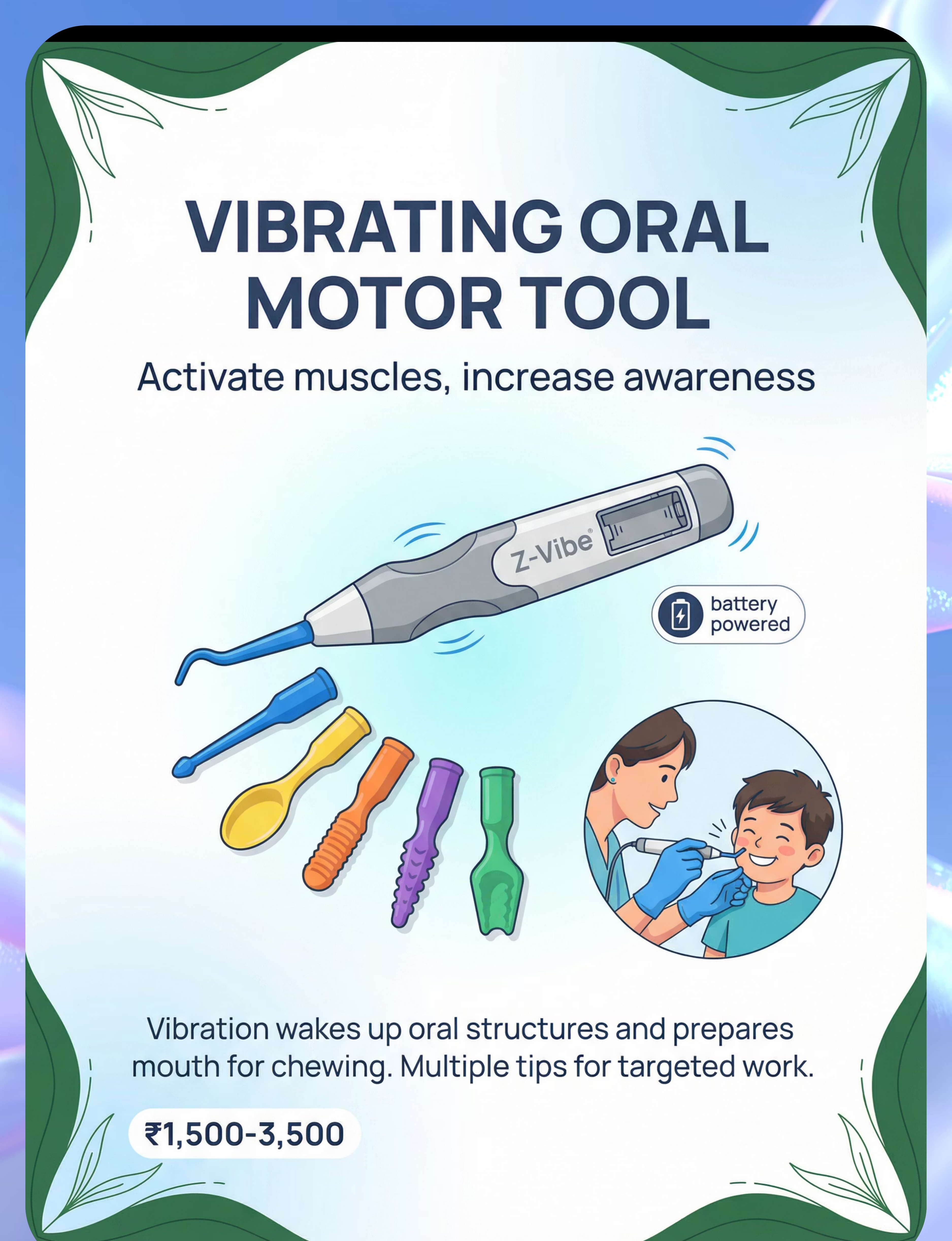
🟢 3. Vibrating Oral Motor Tool (Z-Vibe)
Vibration activates muscle spindles and sensory receptors, "waking up" oral structures before meals. Multiple interchangeable tips target jaw, tongue, cheeks, and gums. Primes the oral system for more efficient chewing.
💰 ₹1,500–3,500 | 🏥 Professional Grade

9 Materials — Continued

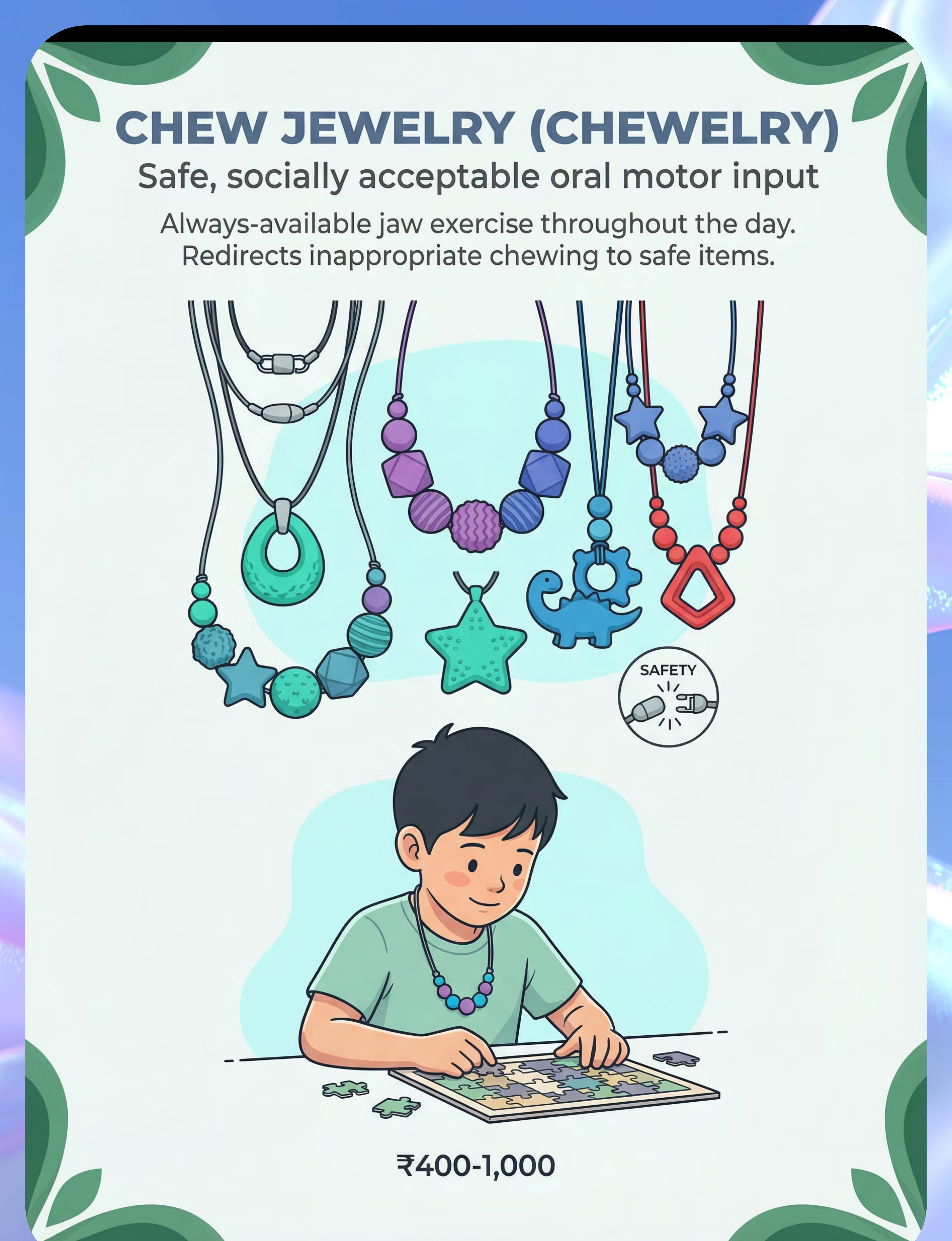
🟢 4. Chew Jewelry (Chewelry) — Food-Safe Silicone
Always-available jaw exercise throughout the day. Redirects non-nutritive chewing (clothing, pencils) to a safe, socially acceptable item. BPA-free, food-grade silicone with breakaway safety clasp.
💰 ₹400–1,000 | ✅ Breakaway clasp required
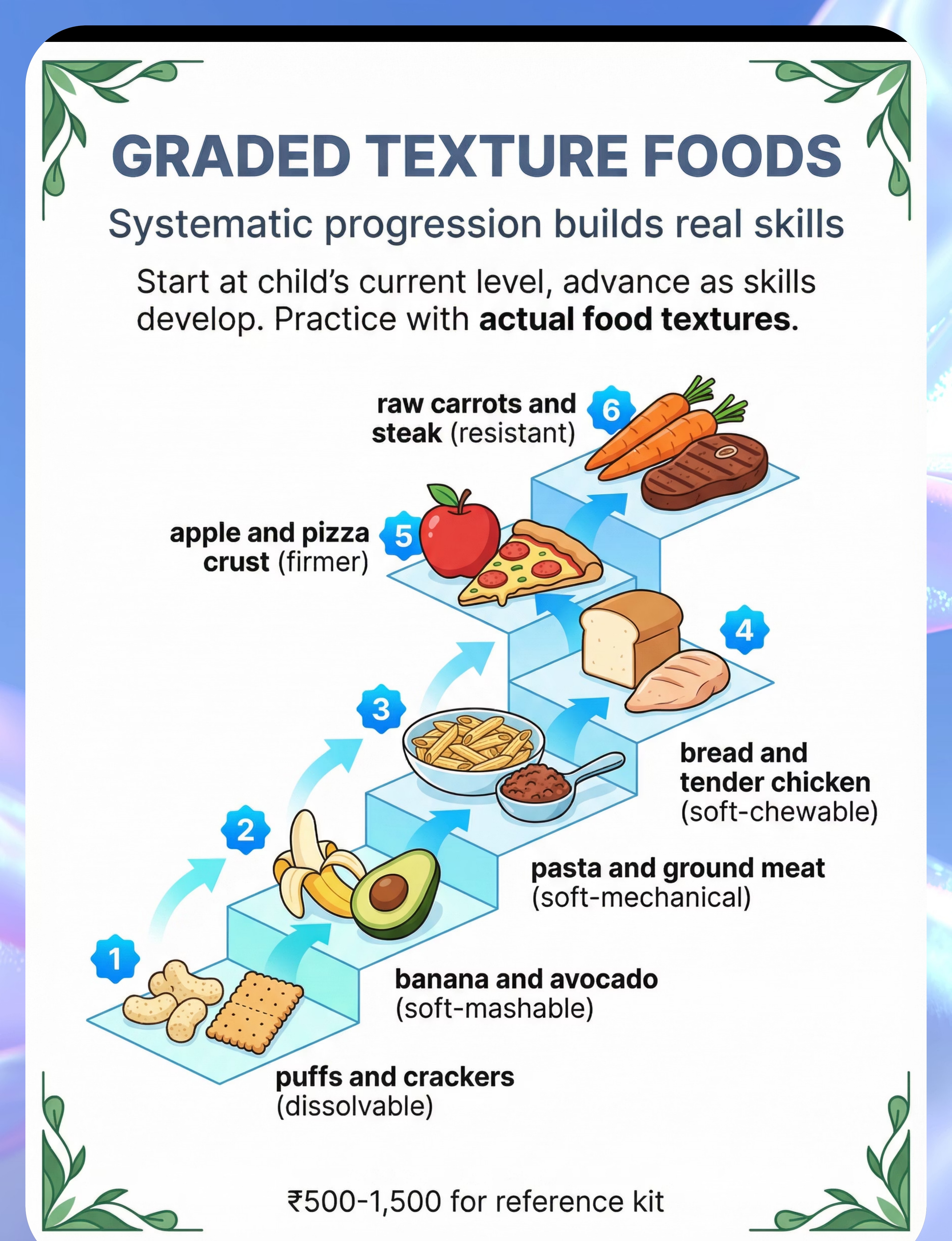
🟢 5. Graded Texture Food Kit
Systematic food texture hierarchy from dissolvable → soft-mashable → soft-mechanical → soft-chewable → firmer → resistant. Builds actual chewing skill with real food. Start where the child succeeds; advance as skills develop.
💰 ₹500–1,500 for reference kit | ♻️ Ongoing food costs

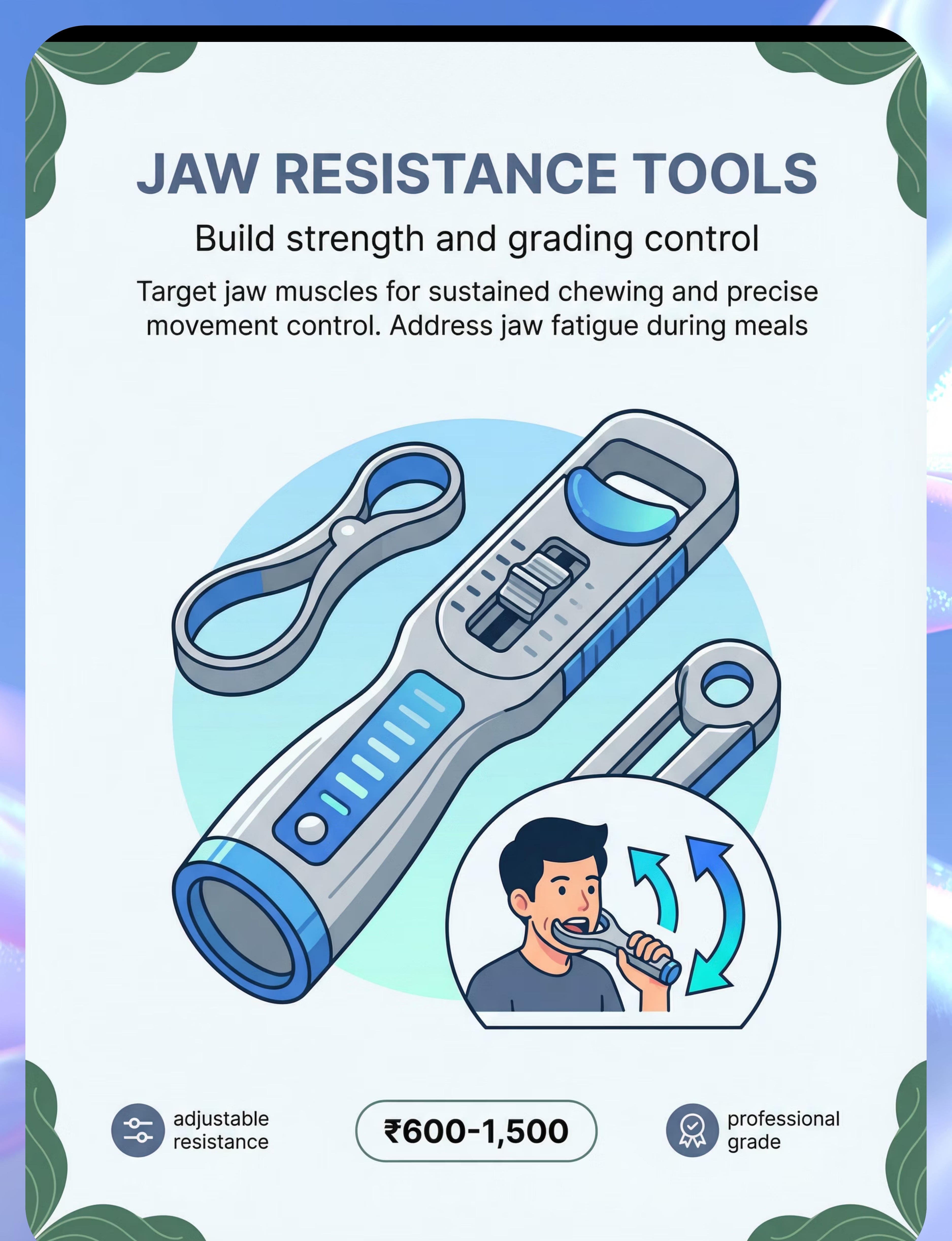
🟢 6. Jaw Resistance Tools
Targets jaw opening AND closing resistance — the full range of jaw motion. Builds jaw endurance for sustained chewing through an entire meal. Addresses jaw fatigue that causes mid-meal breakdown.
💰 ₹600–1,500 | 🏥 Professional Grade

🟢 7. Tongue Lateralization Tools
The tongue must move food sideways onto the molars for grinding. Lateralization tools (Z-Vibe tongue tip, textured probes, food placement guides) build this critical sweeping motion. Without tongue lateralization, even strong jaws can't chew effectively.
💰 ₹400–1,200

🟢 8. Oral Sensory Tools (Nuk Brush / Textured Toothbrush)
Increases oral awareness before meals. Children who can't feel food accurately in their mouths can't chew it efficiently or know when it's ready to swallow. Oral sensory protocol before each meal heightens proprioceptive awareness.
💰 ₹200–800 | ♻️ Replace regularly

🟢 9. Cheek & Lip Strengthening Tools
Cheeks keep food positioned between the teeth; lips keep food contained during chewing. Weak cheeks → food pockets in sulci. Weak lip closure → food falls out. Strengthening supporting structures completes the chewing system.
💰 ₹300–1,000 | ARK Lip Blok, Bubble Toys, Button-String
🏥All 9 materials validated by Pinnacle Blooms SLP + OT Consortium. Always source from reputable therapeutic-grade suppliers.
Reinforcement tools:🏆 Reward Jar (₹589) — amzn.in/d/02C5R9Jn | ⭐ Reward Stickers 1800+ (₹364) — amzn.in/d/01wrHJWX
Reinforcement tools:🏆 Reward Jar (₹589) — amzn.in/d/02C5R9Jn | ⭐ Reward Stickers 1800+ (₹364) — amzn.in/d/01wrHJWX

Every family can start today — regardless of budget.
WHO/UNICEF Inclusion Principle: The science works with household items too. Here's how.
🛒 Clinical-Grade Purchase | 🏠 Household Zero-Cost Alternative | ✅ Why It Works | |
Chewy Tubes | Clean, food-grade rubber tubing (1cm diameter, trimmed 15cm) | Same resistive biting principle. Same jaw strengthening mechanism. | |
ARK Grabber | Firm food items: dried mango strip, thick licorice, dense chewable food held by parent | Food-based resistance achieves same muscle activation. Supervised only. | |
Z-Vibe Vibrating Tool | Electric toothbrush head (non-bristle end, soft) applied briefly to cheeks | Vibration source activates same sensory receptors pre-meal. | |
Chew Jewelry | Silicone teething ring (repurposed, cleaned daily) on a cord | Same non-nutritive chewing mechanism. | |
Graded Texture Kit | Kitchen staples organized by texture level (puffs → banana → soft pasta → tender chicken → apple → raw carrot) | The food items themselves ARE the intervention — no kit needed. | |
Jaw Resistance Tools | Chew on one end of a firm rubber toy (both ends held) — gentle jaw exercise | Resistance principle applies. | |
Tongue Lateralization Tools | Dot of peanut butter or puree on inner cheek → encourage child to lick it off | Identical tongue movement target. | |
Oral Sensory Tools | Clean soft baby toothbrush applied firmly to gums, cheeks, tongue before meals | Same sensory input; same oral awareness activation. | |
Cheek/Lip Tools | Button-on-string between closed lips (child holds while parent applies gentle outward pull) | Classic lip strength exercise; zero cost. |
⚠️When the clinical-grade material is non-negotiable:
• Children who bite off pieces: Only use stem-style or professional ARK-brand tools
• Children with aspiration risk: Graded texture progression MUST be guided by a feeding therapist
• Children with oral sensory defensiveness: Z-Vibe protocol requires professional calibration
• Children who bite off pieces: Only use stem-style or professional ARK-brand tools
• Children with aspiration risk: Graded texture progression MUST be guided by a feeding therapist
• Children with oral sensory defensiveness: Z-Vibe protocol requires professional calibration
"The best therapy material is the one the family can use consistently. A household substitute used daily is more powerful than a clinical tool used once." — Pinnacle Blooms OT Consortium
WHO NCF Handbook (2022) | PMC9978394 | WHO CCD Package (54 LMIC implementations) | Helpline: 9100 181 181

🚦 Safety Gate: Read before your first session.
🔴 RED — DO NOT PROCEED
- Any history of choking, aspiration, or confirmed swallowing difficulty (dysphagia) → Require SLP evaluation before any food-based practice
- Active dental pain, mouth ulcers, or jaw pain → No oral motor exercises until medically cleared
- Child bites off pieces of rubber/silicone items → Do not use standard chew tools; contact therapist
- Child has unknown cause of feeding difficulty → Require professional evaluation before beginning
🟡 AMBER — Proceed with Modifications
- Child has significant oral tactile defensiveness → Begin oral sensory desensitization first
- Child is very young (under 18 months) → Session max 2 minutes; age-appropriate tools only
- Child has structural concerns (suspected tongue tie, dental anomaly) → Consult pediatric dentist/ENT first
- Child is severely anxious about the mouth/face area → Graded desensitization; do not force
🟢 GREEN — Safe to Begin
- ✅ Child is fed (not hungry)
- ✅ Child is rested and regulated
- ✅ All tools inspected for cracks or damage
- ✅ Food texture items match current skill level
- ✅ Parent is calm; environment is low-pressure
🛑 Stop Immediately If You See:
- Gagging or vomiting during oral motor exercises → Stop; reduce intensity
- Child becomes severely distressed or panicked → Stop; transition to calming activity
- Discoloration, excessive drooling, or changed breathing pattern during food → Stop; seek medical evaluation
- Any sign of food or liquid entering airway (coughing, choking sounds post-swallow) → Stop; seek SLP/medical evaluation
🆘Questions about safety? Call FREE National Helpline: 9100 181 181
Available 24×7 | 16+ Languages | Free SLP triage
Available 24×7 | 16+ Languages | Free SLP triage
DOI: 10.1007/s12098-018-2747-4 | ASHA Feeding Safety Protocols | Pinnacle Clinical Safety Protocols

The right environment produces 80% better sessions.
Space Setup Guide
Child Seating
Supportive chair, feet flat on floor (use footrest if needed). Hips, knees, and ankles at 90°. This "90-90-90" position optimizes jaw and head stability for chewing work.
Materials Placement
Arranged in order of use. Within parent's reach. Out of child's grab-reach before the session begins (to allow proper introduction).
Parent Position
Seated at child's eye level. Slightly to the side (not directly in front, which can feel confrontational). Within arm's reach for physical guidance.
Remove from Space
Screens (TV off, phone away), other food items, excessive toys, other children during initial sessions.

Environment Settings
- 🔆Lighting: Warm, not fluorescent if possible. Below 50dB preferred.
- 🔊Sound: Quiet or soft background music (no TV).
- 🌡️Temperature: Comfortable — neither too warm nor too cold.
🍽️Mealtime Setup: Set the table normally with appropriate food textures. No pressure to eat specific amounts. Child-paced.
Sensory Integration Theory (Ayres) | PMC10955541 | Pinnacle ETP™ Home Setup Protocols

60-second pre-session check. The best session starts right.
State Readiness Checklist
Child is fed (not mid-hunger)
Child is rested — no signs of fatigue or post-nap fog
No recent meltdown or significant distress in past 30 minutes
Child is responsive to their name / greetings today
No signs of illness (fever, congestion, throat discomfort)
Mouth is not sore (not post-dental or post-illness)
Space set up per Card 12; all materials inspected and ready
Parent is calm and unhurried (minimum 20 minutes available)
Decision Gate
✅ 8–10 Checks: GO
Proceed to Step 1. Full session.
🟡 5–7 Checks: MODIFY
Run 50% version. Oral sensory input only (5 min). No texture practice.
🔴 Under 5: POSTPONE
Skip today's session. Do a calming activity instead. Return tomorrow.
💚If postponing: Give the child 5 minutes of their preferred calming activity. State: "We'll do our mouth exercises tomorrow." No guilt. Consistency over intensity.
ABA Antecedent Manipulation Principles | BACB Clinical Guidelines | Pinnacle ETP™ Session Protocols

Step 1
⏱️ 30–60 seconds
Begin with an invitation, never a command.
"Hey [child's name], want to do our special mouth exercises? I have something cool for you to try."
— Show the material without placing it. Make eye contact at child's level. Keep voice warm and curious, not directive.
The invitation activates motivation before demand. In ABA terms, this is the pairing phase — establishing the therapeutic material as a positive, motivating stimulus before any therapeutic demand is placed. In OT terms, this is the "just-right challenge" calibration — you're reading the child's energy to decide the session's intensity before you begin.
✅ Acceptance Cues — What to Look For
- Child approaches, reaches for material, makes eye contact
- Child vocalizes interest or shows orienting response
- Child has neutral or positive facial expression

⚠️ Resistance Cues — What to Do
- Child turns away → Wait 10 seconds, try once more, then accept and postpone
- Child shows avoidance → Say "Okay, maybe later" and offer preferred activity
- Child shows distress → Postpone session; return to readiness check
ABA Pairing Procedures | OT Just-Right Challenge Principle | Motivating Operations (EO/AO) | Pinnacle ETP™

Step 2
⏱️ 1–3 minutes
Progress: 25%
Introduce the material. Read the child. Reinforce early.
For Chewy Tube / ARK Grabber
"Let's wake up your chewing muscles. Here's your special chew tool. Watch me first." Demonstrate: Place tool at molar area, bite and release 3 times slowly. Exaggerate chewing motion so child can see. Hand to child: "Your turn. Can you put it on your back teeth like I did?"
For Vibrating Tool (Z-Vibe)
"This one buzzes a little — let's feel it on your hand first." Apply briefly to child's hand or arm before mouth. Progress to outer cheek, then inner cheek, then gums as tolerated.
For Oral Sensory Protocol (Pre-meal)
"Before we eat, let's wake up your mouth. Here comes the mouth brush." Firm, circular strokes on outer gums, inner cheeks, tongue. 30 seconds per area.
Child Response Spectrum
🟢 Engagement
Bites, holds, or tolerates with neutral to positive affect → Continue
🟡 Tolerance
Child accepts but shows minimal enthusiasm → Reinforce immediately, continue gently
🔴 Avoidance
Child pushes away or closes mouth → Back off one step; offer visual demonstration only
💡 When child ACCEPTS material — praise within 3 seconds: "Yes! You're doing it! Great biting!" (immediate, specific, enthusiastic)
PMC11506176 | Reinforcement scheduling from ABA literature | Pinnacle ETP™ material introduction protocols

Step 3
⏱️ 5–10 minutes
Progress: 50%
The core oral motor work. Precision here builds lasting skill.
1
Protocol A — Jaw Strengthening
Place Chewy Tube / ARK Grabber at the molar area. Guide child to bite down firmly and hold 3–5 seconds. Release. Repeat 10–15 cycles per side. Switch sides. Total: ~3 minutes. Progression: Soft/smooth → knobby/standard → hard resistance as jaw strength builds. Ideal timing: Before meals.
2
Protocol B — Oral Sensory Preparation (Pre-meal, 2 min)
Nuk brush: 10 firm circular strokes on upper gum line, lower gum line, inner cheeks (each side), tongue (5 anterior-to-posterior strokes). Do this within 5 minutes before serving food. Effect: Heightened oral awareness → more efficient chewing at the meal.
3
Protocol C — Tongue Lateralization
Place a small soft food dot (peanut butter, puree) on one inner cheek. Prompt: "Can you get it with your tongue?" Goal: sideways tongue sweep to target. Progress: Move target further back toward molar area. 5–8 repetitions per side, 2–3 minutes total.
4
Protocol D — Graded Texture Food Practice
Done AT mealtimes. Identify current level; introduce just one step above.
Child's Current Level | Introduce Next Level | |
Pureed only | Soft-mashable: ripe banana, avocado, well-cooked sweet potato | |
Soft-mashable | Soft-mechanical: soft pasta, ground meat, soft scrambled egg | |
Soft-mechanical | Soft-chewable: tender chicken, soft bread, cooked firm vegetables | |
Soft-chewable | Firmer: pizza crust, cheese, apple slice | |
Firmer | Resistant: raw carrots, steak, crackers |
PMC10955541 | ASHA Oral Motor Protocols | IDDSI Framework | Graded texture research
Step 4
⏱️ 3–5 minutes
Progress: 70%
3 good repetitions are worth more than 10 forced ones.
Material | Target Reps | Satiation Signal | |
Chewy Tube / ARK Grabber | 10–15 bites per side × 2 sides | Child removes tool, closes mouth tightly, turns head | |
Oral Sensory Protocol | 10 strokes per area | Child shows increased oral activity (licking, swallowing) = ready | |
Tongue Lateralization | 5–8 per side | Tongue begins missing target consistently | |
Texture Food Practice | 2–3 bites of new texture per meal | Child gags, pouches excessively, or distress increases |
Variation Options — to Maintain Engagement
Tool Variations
Alternate between Chewy Tube and ARK Grabber in same session for sensory variety.
Position Variations
Try molar area left → right → bilateral alternating for comprehensive coverage.
Motivational Variations
Child chooses which tool to use first — agency increases participation and cooperation.
Texture Alternating
At mealtime, alternate familiar texture bite with new texture bite (comfort → challenge → comfort).
💡The Satiation Principle:"When the child's nervous system has processed enough input, it will signal satiation. Do not override the signal." Signs: tool removal, mouth closing, head turn, increased escape behaviors, yawning.
SI therapy dosage research | PMC11506176 | ABA satiation principles | Pinnacle ETP™ session dosage

Step 5
⏱️ Within 3 seconds of success
Timing matters more than magnitude. Immediate > Grand.
Verbal Praise — Use Immediately Within 3 Seconds
🗣️"You did it! You chewed so well! I love watching you practice!"
🗣️"Your jaw muscles are getting so strong — I can tell!"
🗣️"That was a really big bite! You're doing amazing!"
Physical Reinforcement (if appropriate)
- 👏 High-five immediately after successful repetition
- 🤗 Brief enthusiastic hug (if child accepts touch)
Token Economy
- ⭐ Place one sticker on chart after each completed set
- 🏆 Child deposits token in reward jar after successful session
- 📊 Visual progress board on fridge — stars accumulate toward preferred reward
💡"Celebrate the attempt, not just the success. A child who touched the Chewy Tube without biting has still made progress. The brain needs to associate approach-behavior with reward BEFORE skill acquisition occurs."
ABA Reinforcement Principles | BACB Ethical Guidelines | Token Economy systematic reviews | Pinnacle ETP™

Step 6
⏱️ 1–2 minutes
No session ends abruptly. Transitions prevent dysregulation.
Warning (30 seconds before ending)
"Two more bites, then we're all done with mouth practice."
Final Repetition with Announcement
"Last one! You're doing so great!" Complete final repetition.
Material Put-Away Ritual
"Let's put the chew tool back in its special spot." Child participates in putting tool in designated container. This creates a clear behavioral endpoint.
Transition to Next Activity
"Good job! Now let's [wash hands / read a book / eat lunch]." Immediate transition to next preferred or neutral activity. Do NOT immediately introduce new demands.
⚠️If Child Resists Ending: Try "One more, then done" (extend by exactly one repetition, then hold firm). Do NOT extend session significantly in response to protest — this teaches protest = longer session.
NCAEP 2020 (Visual supports as EBP) | Transition research in ASD | Pinnacle ETP™ session ending protocols

60 seconds of data capture. A lifetime of better recommendations.
3-Field Quick Tracker
Field | What to Record | Example | |
Today's Date | DD/MM/YYYY | 07/03/2026 | |
Tools Used | Which of the 9 materials | Chewy Tube + Oral Sensory Brush | |
Child's Response | 1=refused / 2=tolerated / 3=engaged / 4=initiated | 3 | |
Duration | Minutes of actual work | 7 minutes | |
Notable Observation | One sentence | "Chewed on left side 12 times — improvement from 5 last week" | |
Texture Level | Current food texture level | Soft-mechanical (pasta, ground meat) |
📊E-458 Session Tracker: Track your child's oral motor progress → forms.gle/[E458-Session-Tracker]

🤖GPT-OS® Integration: Your session data feeds into the AbilityScore® Feeding Independence Readiness Index. Over 8–12 sessions, GPT-OS® identifies your child's specific strength/weakness pattern and adjusts your EverydayTherapyProgramme™ recommendations automatically.
Digital health + ASD (21 RCTs, 2024) | Pinnacle GPT-OS® data architecture | BACB data collection standards

Every challenge has a specific solution. You're not doing it wrong.
🟡 Child refuses to touch the Chewy Tube
✅ Pair it with a preferred food flavor first (dip in yogurt, honey, or juice). Present it during play, not as a "therapy task." Let child examine it for several sessions before expecting biting. Reinforce approach behavior.
🟡 Child bites the tool and won't release
✅ Use "trading" — offer a preferred item simultaneously. Don't try to remove by force. "Trade me — here's your sticker!" Works consistently with reinforcement.
🟡 Child gags when food is introduced at new texture level
✅ Do NOT advance. Gag = not ready. Return to previous texture level for 1–2 more weeks. Increase oral sensory protocol before meals. If gagging persists, request professional feeding evaluation.
🟡 Child eats food quickly without chewing
✅ Offer very small bites (pea-sized). Say "Wait — can you chew it?" Use a count: "Chew 10 times!" with your fingers. Model slow chewing. Reinforce delayed swallowing.
🟡 Child pockets food in cheeks after meals
✅ After each meal, do a cheek check routine: "Open wide — let me see if your mouth is empty." Oral sensory input mid-meal may help awareness. If persistent, SLP evaluation for tongue lateralization deficit.
🟡 Child is fine at home but refuses at school/parties
✅ Generalization training. Send chew jewelry to school. Share Teacher Template. Practice at varied environments progressively (home → grandparent's → familiar restaurant → school lunch).
🟡 No progress after 4 weeks
✅ Request professional assessment: oral motor evaluation by SLP, sensory profile by OT, check for structural causes (tongue tie, tonsil size, jaw alignment). Adjust program based on findings.
ABA problem-solving frameworks | ASHA clinical troubleshooting | Pinnacle ETP™ troubleshooting protocols

Every child's chewing profile is different. Personalize your approach.
Profile A: Oral Sensory Seeker
(Chews on everything — clothing, pencils, objects)
Lead with chew jewelry (always available throughout the day)
Emphasize jaw strengthening tools (Chewy Tubes, ARK Grabber)
Structured oral motor input 3× per day satisfies the seeking while building skill
Graded texture progression may advance faster (less texture aversion)
Profile B: Oral Sensory Avoider / Defensive
(Gags easily, refuses mouth touch, highly tactile-defensive)
Lead with hand/arm vibration before approaching face
Begin oral sensory protocol on OUTER face before progressing inward
Use food-flavored tools to pair oral input with pleasure
Advance texture progression slowly — gag is always a warning signal
Age-Based Modifications
Ages 1–2
Session max 3–5 min. Tools must be infant-appropriate sizes. Food practice is primary intervention.
Ages 3–5
5–10 min. Full tool range. Child begins to understand and cooperate with instructions.
Ages 6–10
Up to 15 min. Child can participate in self-monitoring: "How many chews did you do?"
📅Easier Days: Oral sensory protocol only, 2-minute sessions, focus on pre-meal sensory prep.
📅Harder Days: Full protocol — sensory prep → jaw tools → tongue exercises → texture practice → 15 minutes with breaks.
📅Harder Days: Full protocol — sensory prep → jaw tools → tongue exercises → texture practice → 15 minutes with breaks.
Sensory profile-based intervention (OT) | ABA function-based analysis | Pinnacle ETP™ personalization protocols

ACT IV: Progress Arc
Week 1–2
Week 1–2: Tolerance, not mastery. This is how the brain begins.
15%
Progress Arc
Week 1–2 of the 8-week intervention arc
What Progress Looks Like — Week 1–2
Observable Indicator | What it means | |
Child tolerates Chewy Tube on lips/teeth without refusing | Oral defensive response beginning to reduce | |
Child accepts oral sensory protocol before meals without distress | Pre-meal sensory input becoming routine | |
Mealtime attempts at slightly firmer foods (even if spit out) | Oral exploration beginning; brain registering new texture data | |
Cheek pocketing begins slightly earlier (food detected sooner) | Oral awareness improving |
What is NOT Progress Yet
- ❌ Child successfully chewing firmer foods → That's weeks 4–8
- ❌ Significant reduction in gagging → Neural pathway still forming
- ❌ Enthusiastic participation → Tolerance is the Week 1–2 goal
"If your child tolerates the Chewy Tube for 5 seconds longer than they did on Day 1 — that is real, measurable, clinically significant progress. Document it."
PMC11506176 (8–12 week intervention timelines) | Oral motor skill acquisition research | Pinnacle ETP™ milestones

Week 3–4
Progress: 40%
Week 3–4: Neural pathways forming. You'll start to see glimpses.
40%
Progress Arc
Week 3–4 of the 8-week intervention arc — consolidation zone
Consolidation Indicators
Child begins to anticipate oral motor session — picks up Chewy Tube themselves or comes to table at established session time
Child's biting pattern improves — longer holds, more consistent molar placement
Child manages one additional texture level reliably (e.g., progresses from soft-mashable to soft-mechanical)
Cheek pocketing begins to reduce as tongue lateralization improves
Mealtime duration shortens slightly — food being processed more efficiently
Child notices and self-corrects food that falls out of mouth
Child begins exploring new textures voluntarily at mealtimes
"You may notice you're calmer at mealtimes too. Your confidence in the process is building alongside your child's skill."
📈When to increase intensity:
• Child tolerating sessions well → increase from 1× to 2× daily oral motor exercises
• Jaw strength clearly improved → advance Chewy Tube to next resistance level
• Oral sensory protocol fully accepted → add tongue lateralization exercises
• Child tolerating sessions well → increase from 1× to 2× daily oral motor exercises
• Jaw strength clearly improved → advance Chewy Tube to next resistance level
• Oral sensory protocol fully accepted → add tongue lateralization exercises
Neuroplasticity + synaptic strengthening literature | PMC11506176 | Pinnacle ETP™ consolidation markers
Week 5–8
Progress: 75%
Week 5–8: Real skills emerge. Dietary variety expands.
75%
Breakthrough Zone
Week 5–8 of the 8-week arc — skills consolidate and dietary variety expands
Breakthrough Indicators
✅ Texture Expansion
Child manages 2–3 texture levels beyond starting point with increasing consistency.
✅ Rotary Pattern Emerging
Visible circular jaw movement, not just up-and-down munching. A major developmental milestone.
✅ Cheek Pocketing Reduced
Significantly reduced or eliminated at current texture levels as tongue lateralization strengthens.
✅ Social Participation
Child begins eating alongside peers at some textures previously avoided — a key quality-of-life win.
Tool | 8-Week Skill Target | |
Chewy Tube | Progress from Soft → Standard resistance; 20+ bites per side with good molar placement | |
ARK Grabber | Mastering Standard → beginning Hard resistance; varied biting surfaces used | |
Oral Sensory Protocol | Fully accepted pre-meal; child may begin to self-request | |
Tongue Lateralization | Child sweeps food from center to side consistently during eating | |
Texture Progression | 2–3 levels advanced from starting point |
PMC10955541 (meta-analysis outcomes) | ASHA oral motor progress benchmarks | Pinnacle AbilityScore® Feeding Domain

Your child eating pizza at a birthday party is a clinical milestone. Celebrate it like one.
🏆 Micro-Wins (Daily)
Celebrate immediately — every session.
• Tolerated Chewy Tube for 30 seconds
• Accepted one new texture bite
• Oral sensory protocol completed without protest
• Tolerated Chewy Tube for 30 seconds
• Accepted one new texture bite
• Oral sensory protocol completed without protest
🏆 Meso-Wins (Weekly)
Record and share with your care team.
• New food texture successfully chewed and swallowed
• Meal completed at peer texture level
• Tool resistance level advanced
• New food texture successfully chewed and swallowed
• Meal completed at peer texture level
• Tool resistance level advanced
🏆 Macro-Wins (Monthly)
Mark with ceremony — these are life milestones.
• Child eats at school lunch with peers
• Child manages birthday cake / party food
• Doctor/therapist confirms texture level advancement
• Family mealtime stress significantly reduced
• Child eats at school lunch with peers
• Child manages birthday cake / party food
• Doctor/therapist confirms texture level advancement
• Family mealtime stress significantly reduced
"Every bite your child takes at a new texture level represents thousands of neural firings, weeks of muscle strengthening, and your consistent, patient effort. You are not just feeding your child. You are building a system."
📷Photo Documentation Tip: Document wins with photos or short videos. These become your child's therapy portfolio and are invaluable for future therapist assessments, school communications, and celebrating the journey.
🚩 Red Flags: These signs require professional evaluation.
🔴 Choking or Gagging on Previously Managed Foods
SLP/ER evaluation immediately. Acute choking = call emergency services without delay.
🔴 No Texture Progression After 8 Weeks of Consistent Practice
Professional oral motor + feeding evaluation required. Indicates a structural, neurological, or sensory factor not addressed by home practice alone.
🔴 Child Losing Weight or Showing Nutritional Compromise
Pediatric dietitian + SLP immediately. This is a medical urgency that requires a multidisciplinary response.
🔴 Significant Food Pocketing That Doesn't Improve
SLP assessment for tongue lateralization deficit and swallowing safety. Chronic pocketing increases choking risk.
🔴 Signs of Pain During Eating
Grimacing, crying, or holding jaw → Dental/medical evaluation before any oral motor work continues.
🔴 Family Mealtime Has Become Traumatic
Feeding behavioral evaluation + family support services. Stress in the feeding environment perpetuates difficulty.
Escalation Pathway
🆘FREE National Helpline: 9100 181 181 | Available 24×7 | 16+ Languages | Free SLP triage consultation available
From "can't manage purée" to "eating everything" — the 5-stage journey.
Stage 1: Foundation Building
← Most families begin here. Significant oral motor weakness; very limited textures tolerated. Beginning oral motor strengthening program. Working with dissolvable and soft-mashable textures only.
Stage 2: Emerging Chewing
Some jaw strength established; soft-mechanical textures managed. Tongue lateralization exercises active. Oral sensory protocol consistently accepted.
Stage 3: Developing Efficiency
Soft-chewable textures managed with increasing skill. Graded texture progression active and advancing. Oral motor exercises well established in daily routine.
Stage 4: Advancing Competence
Managing firmer textures with sustained chewing. Approaching age-appropriate diet breadth. Approaching peer-level mealtime participation.
Stage 5: Mastery
Efficient chewing across ALL age-appropriate textures including resistant foods (raw vegetables, steak, crusty bread). Full mealtime independence.
🤖GPT-OS® Readiness Tracking: These 5 stages map directly to the Oral Motor Function Readiness Index and Feeding Independence Readiness Index within AbilityScore®. Every session you track moves the needle.
Which stage describes your child today? Start there. Time to advance per stage: weeks to months is normal.
Which stage describes your child today? Start there. Time to advance per stage: weeks to months is normal.

Chewing doesn't exist in isolation. Here's your complete feeding journey.
← E-457: Refusing New Foods
When the challenge is food acceptance and texture aversion rather than motor ability. techniques.pinnacleblooms.org/feeding-oral-motor/refusing-new-foods-E-457
→ E-459: Swallowing Difficulty
When food has been adequately chewed but the pharyngeal phase needs support. techniques.pinnacleblooms.org/feeding-oral-motor/swallowing-difficulty-E-459
↑ E-456: Gagging on Textures
When gag reflex hypersensitivity is the primary barrier. techniques.pinnacleblooms.org/feeding-oral-motor/gagging-on-textures-E-456
↓ E-461: Food Pocketing & Oral Clearance
Specialized techniques when cheek pocketing is the primary concern. techniques.pinnacleblooms.org/feeding-oral-motor/food-pocketing-E-461
Domain E: Feeding & Mealtime Independence — Your child's full map.
All techniques are interconnected within techniques.pinnacleblooms.org/feeding-oral-motor
ACT V: Community
Real families. Real mealtimes. Real progress.
"My son Arjun was five years old and eating almost exclusively purée-texture foods. He pocketed everything that required chewing — we'd find food in his cheeks 20 minutes after meals. His SLP at our Pinnacle center identified weak jaw muscles and very limited tongue lateralization. We started daily Chewy Tube exercises before breakfast and oral sensory prep before every meal. Eight months later, Arjun ate birthday cake at his cousin's party alongside all the other children. I cried. That moment cost us 8 months of consistent daily work. It was the most worthwhile 8 months of our lives."
— Parent, Pinnacle Hyderabad Network | Child: 5 years, ASD profile
"We were told our daughter 'might never eat normal foods' because of her low oral tone. The Pinnacle feeding team designed a systematic program using the graded texture hierarchy. It took 14 months. She now eats almost everything. The tools on this page were in our house every single day."
— Parent, Pinnacle Bangalore Network
Individual outcomes vary. These accounts reflect genuine parent experiences. Results depend on child profile, underlying cause, intervention intensity, and consistency. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.

You are not on this journey alone. 70+ countries. One community.
Parent Support Networks
Pinnacle Blooms Parent Network — pinnacleblooms.org/parent-community
Feeding Therapy Parent Circle (WhatsApp) — Request via Helpline: 9100 181 181
Domain E: Feeding Challenges Parent Group — Request via pinnacleblooms.org
Feeding Therapy Parent Circle (WhatsApp) — Request via Helpline: 9100 181 181
Domain E: Feeding Challenges Parent Group — Request via pinnacleblooms.org
Social Channels
📸 Instagram: @pinnacleblooms — Feeding therapy reels, live sessions, expert tips
▶ YouTube: Pinnacle Blooms Network — Full oral motor demonstration library
▶ YouTube: Pinnacle Blooms Network — Full oral motor demonstration library
International Connections
Pinnacle serves families in 70+ countries through GPT-OS® digital delivery. Connect with families navigating the same feeding challenges globally through our parent portal.

"Consistency across caregivers multiplies impact. When grandparents, school teachers, and all family members understand these materials — the child gets 24×7 support instead of 1-hour sessions."
When you're ready to bring in the full team — Pinnacle is here.
Speech-Language Pathology Feeding Evaluation
Comprehensive oral motor assessment, texture tolerance evaluation, swallowing safety screening, and oral motor treatment program design customized to your child's profile.
Occupational Therapy — Sensory Feeding Evaluation
Full sensory profile for feeding, oral tactile defensiveness assessment, environmental and positioning recommendations for optimal mealtime function.
NeuroDev Pediatrics — Medical Oral Motor Evaluation
Structural assessment, neurological factors, and medical co-management for complex cases requiring a dual medical and therapeutic approach.
ABA Feeding Behavioral Support
Mealtime behavior management, texture introduction protocol design, and reinforcement architecture for children where behavior co-occurs with oral motor challenges.
FusionModule™ Feeding Program
All disciplines coordinated under GPT-OS® for families where multiple factors (oral motor + sensory + behavioral) co-exist and require integrated clinical response.
📞Book a Feeding Therapy Assessment: Call 9100 181 181
Free initial triage | 16+ languages | 24×7 availability | pinnacleblooms.org/find-center — 70+ centers across India
Free initial triage | 16+ languages | 24×7 availability | pinnacleblooms.org/find-center — 70+ centers across India
The science behind every material on this page. For the curious parent.
📄 ASHA Pediatric Feeding & Swallowing Guidelines
Position statement: oral motor intervention is evidence-based when systematically applied. asha.org/practice-portal/clinical-topics/pediatric-dysphagia
📄 PMC11506176 — PRISMA Systematic Review (2024)
Multi-disciplinary sensory and motor interventions for children with ASD demonstrate evidence-based outcomes across 16 studies. pubmed.ncbi.nlm.nih.gov/PMC11506176
📄 Padmanabha et al., Indian Journal of Pediatrics (2019)
Indian RCT demonstrating significant outcomes of home-based structured feeding interventions. DOI: 10.1007/s12098-018-2747-4
📄 PMC10955541 — Meta-analysis (2024)
Sensory integration + motor approaches: significant improvements across feeding, motor, and adaptive behavior outcomes in ASD.
📄 NCAEP Evidence-Based Practices (2020)
Structured skill-building and video modeling classified as evidence-based practices. ncaep.fpg.unc.edu
📄 WHO Care for Child Development (2023)
Evidence-based caregiver interventions implemented in 54 LMICs. Home-material-based intervention efficacy established. PMC9978394
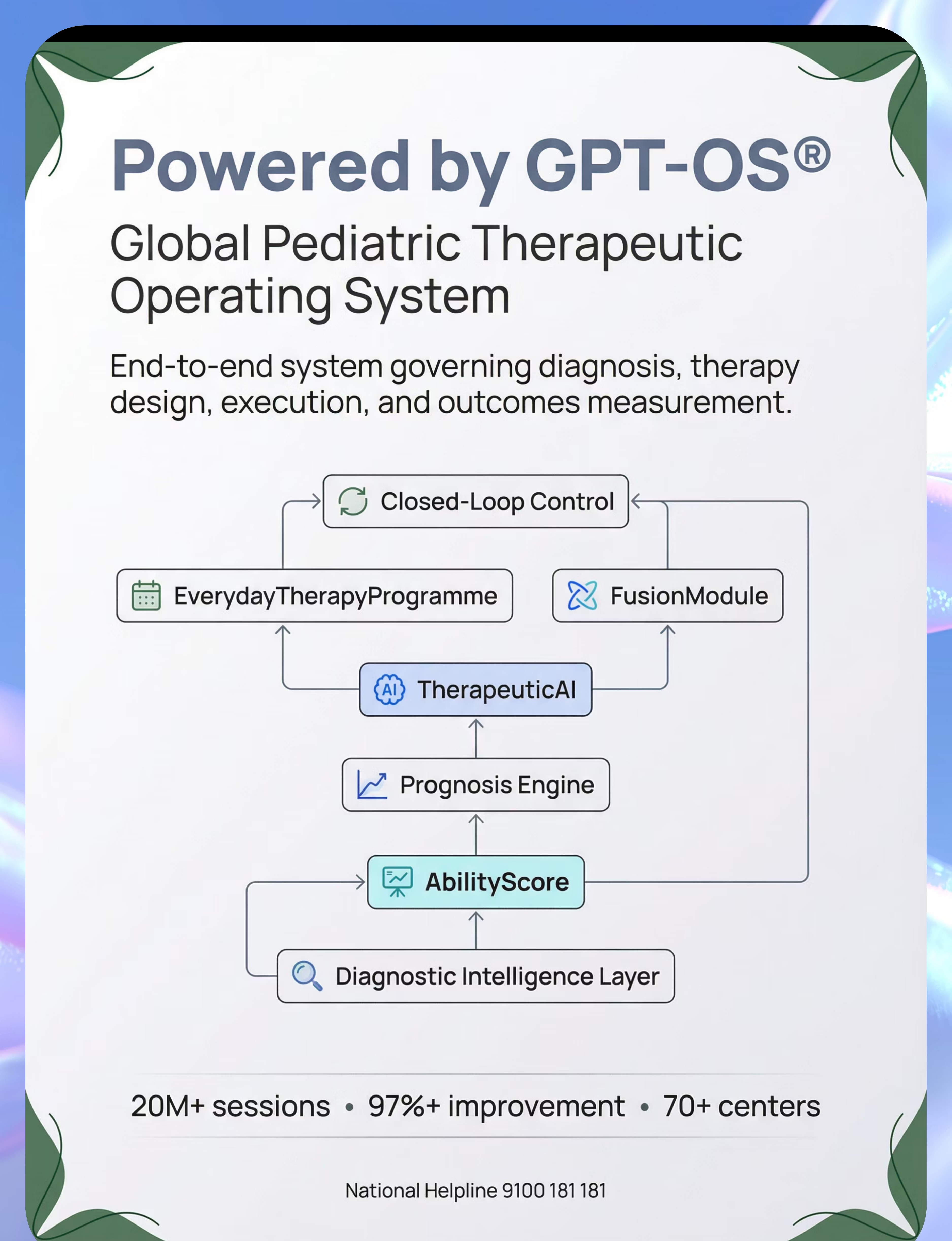
Powered by GPT-OS®: Global Pediatric Therapeutic Operating System
What GPT-OS® Learns From E-458 Data
Which of the 9 materials your child responds to best
Rate of jaw strength progression (biting cycles per session)
Texture level progression speed
Oral sensory tolerance progression
Whether sensory, motor, or behavioral factors are the primary driver
🔒Privacy Assurance: Your data is protected under Indian IT Act privacy provisions | DPIIT Registered | All data contributes to aggregate improvement — individual data never shared.
"Your child's data helps every child like yours. When your child progresses from Stage 2 to Stage 3 in 6 weeks, GPT-OS® updates the prognosis model for all children at a similar starting profile."
Digital health + ASD (21 RCTs, 2024 meta-analysis) | Pinnacle GPT-OS® IP filed in 160+ countries

Watch: 9 Materials That Help With Chewing Difficulty
▶ E-458 Reel Details
Series: Feeding & Mealtime Independence in Children
Episode: 458 of 540
Domain: E — Feeding / Oral Motor / OT / SLP
Duration: 75–85 seconds
Episode: 458 of 540
Domain: E — Feeding / Oral Motor / OT / SLP
Duration: 75–85 seconds
This reel introduces all 9 oral motor materials featured on this page, demonstrated by Pinnacle's certified Speech-Language Pathologists and Occupational Therapists. See each material in clinical use, understand proper technique, and watch the progression from simple tools to graded food textures.
← E-457
9 Materials for Refusing New Foods
E-458 ← You Are Here
9 Materials for Chewing Difficulty
E-459 →
9 Materials for Swallowing Difficulty
NCAEP 2020 (Video modeling as EBP) | Multi-modal learning improvement evidence

Consistency across caregivers multiplies impact 4×. Share this page.
Share Buttons
📱 WhatsApp
Pre-filled: "This page explains exactly how to help a child with chewing difficulty at home — jaw exercises, the right tools, step-by-step protocol. techniques.pinnacleblooms.org/feeding-oral-motor/chewing-difficulty-E-458 — from Pinnacle Blooms Network"
📧 Email & 🔗 Copy Link
Send the full page with embedded evidence and step-by-step protocols to co-caregivers, grandparents, teachers, and anyone supporting your child at mealtimes.
Simplified Grandparent Summary
Your grandchild is working on building chewing strength. Here's what helps:
- Before every meal: gently rub their gums and cheeks with a soft toothbrush for 1 minute
- During meals: offer foods from the list on the fridge (current texture level)
- After meals: check their cheeks are empty
- Always: no pressure to eat. Praise any attempt.
Helpline if confused: 9100 181 181
Teacher / School Template
"Dear Teacher, [child's name] is currently in feeding therapy for oral motor difficulties. Regarding lunchtime: please provide [current texture level] foods. Do not encourage eating beyond their current texture level. Chew jewelry around their neck is therapeutic — please do not remove it. For questions: 9100 181 181"
PMC9978394 (WHO CCD multi-caregiver training evidence)

ACT VI: FAQ
Your questions — answered by the Pinnacle SLP + OT Consortium.
Q1: How long will it take before my child can eat normally?
Timeline varies significantly by child profile, severity of oral motor weakness, consistency of practice, and whether structural or neurological causes are present. Children with isolated jaw weakness often show measurable texture progression in 6–12 weeks. Children with complex presentations (low tone, sensory defensiveness, neurological conditions) may take 12–24 months or longer. Progress is measured in texture levels advanced, not in absolute time. Track your data to see your child's personal trajectory.
Q2: Are Chewy Tubes safe? My child chews very hard.
Therapeutic-grade Chewy Tubes (from ARK Therapeutic and reputable suppliers) are engineered specifically for hard biting. Do NOT use random rubber items. Inspect your tubes before each session — replace at any sign of cracking, tearing, or change in texture. If your child consistently bites through tools rapidly, inform your SLP — they may need a different material profile.
Q3: My child gags on even soft foods. Can these materials still help?
Yes, but the sequencing changes. If gagging is the primary challenge, begin with the oral sensory protocol exclusively for 2–4 weeks before introducing any food-based texture practice. The oral sensory work reduces hypersensitivity and raises the gag threshold. See also E-456 (Gagging on Textures) for a dedicated protocol.
Q4: At what age should my child be assessed if they're still struggling?
If a child over 18 months is not progressing to soft-mechanical textures, or a child over 3 years cannot manage most soft-chewable foods, a professional feeding evaluation is warranted. Earlier is always better. The GPT-OS® AbilityScore® assessment can identify whether the challenge is oral motor, sensory, behavioral, or structural.
Q5: We tried these materials and saw no improvement. What next?
Persistent lack of progress after 8 consistent weeks typically indicates: (a) structural issue requiring medical evaluation, (b) neurological factor requiring NeuroDev assessment, (c) sensory defensiveness is the primary driver, or (d) the program needs professional customization. Call 9100 181 181 for a free triage consultation.
Q6: Can I do these exercises at mealtimes instead of separate sessions?
Yes — and this is recommended for the food-based protocols. The oral sensory preparation should happen immediately pre-meal. Tongue lateralization exercises can be embedded in mealtimes using actual food. Separate sessions are recommended for tool-based jaw strengthening (Chewy Tubes, ARK Grabber) as these work best without food present.
Q7: My child's school says the Chewy Tube is "unhygienic." What do I do?
Chew jewelry is specifically designed for school use — it's worn as a necklace, is the child's personal item, and is cleaned daily. The Teacher Template (Card 38) includes language explaining its therapeutic purpose. Most schools accept chew jewelry with a therapist letter. Contact us (9100 181 181) for a formal recommendation letter template.
Q8: Does improving chewing help with speech too?
Yes — often significantly. The muscles involved in chewing (jaw, tongue, lips, cheeks) are the same muscles used in speech production. Stronger, better-coordinated oral musculature frequently contributes to clearer articulation, better tongue placement for speech sounds, and improved resonance. This is one reason the SLP leads this intervention — the feeding and speech domains share the same oral motor substrate.
Preview of 9 materials that help with chewing difficulty Therapy Material
Below is a visual preview of 9 materials that help with chewing difficulty therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!
Your child's chewing skills can be built. Start today.
Every jaw muscle responds to training. Every tongue improves with targeted exercise. Every family can run this from home.
▶ Start This Technique Tonight
Begin with the oral sensory pre-meal protocol at your very next meal. No tools required to start.
📞 Book a Feeding Therapy Assessment
Free call. Free triage. Professional guidance within 24 hours.
Call or WhatsApp: 9100 181 181
→ Explore Next Technique
E-459: 9 Materials That Help With Swallowing Difficulty
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers & Countries Served
🏛️ Pinnacle Blooms Network®
OT • SLP • ABA/BCBA • SpEd • NeuroDev
DPIIT: DIPP8651
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™
AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™
🆘FREE National Helpline: 9100 181 181 | 16+ Languages | 24×7 | 🌐pinnacleblooms.org | 📧care@pinnacleblooms.org
This content is educational and does not replace individualized feeding assessment and intervention by licensed speech-language pathologists, occupational therapists, or feeding specialists. Chewing difficulties may have medical, structural, neurological, or sensory causes requiring professional evaluation. Choking is a serious risk with inappropriate food textures. Always match food texture to current skill level. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.