
"They inhale food in three minutes flat — or they're still on the third bite an hour later."
You've said "slow down" a thousand times. It doesn't work. Here's why — and here's what does.

E-466 | Domain E: Feeding & Mealtime Independence
The Moment You Recognize
It's 7:15 AM and the plate is already clean. Your child barely looked at the food — just shoveled it in, cheeks stuffed, barely chewing, and announced "done" before you'd taken your second sip of chai. You keep thinking about choking. About whether any of that food was actually processed.
Or it's the opposite: it's 7:45 now, the same three bites still on the plate, the food cold, your child distracted by a speck of dust on the wall. You've said "take a bite" sixteen times. You're out of patience, they're out of interest, and the school bus comes in ten minutes.
You are not failing. Your child's self-regulation system is still developing — and it needs external scaffolding to find its rhythm.
🏥 Consortium Validated
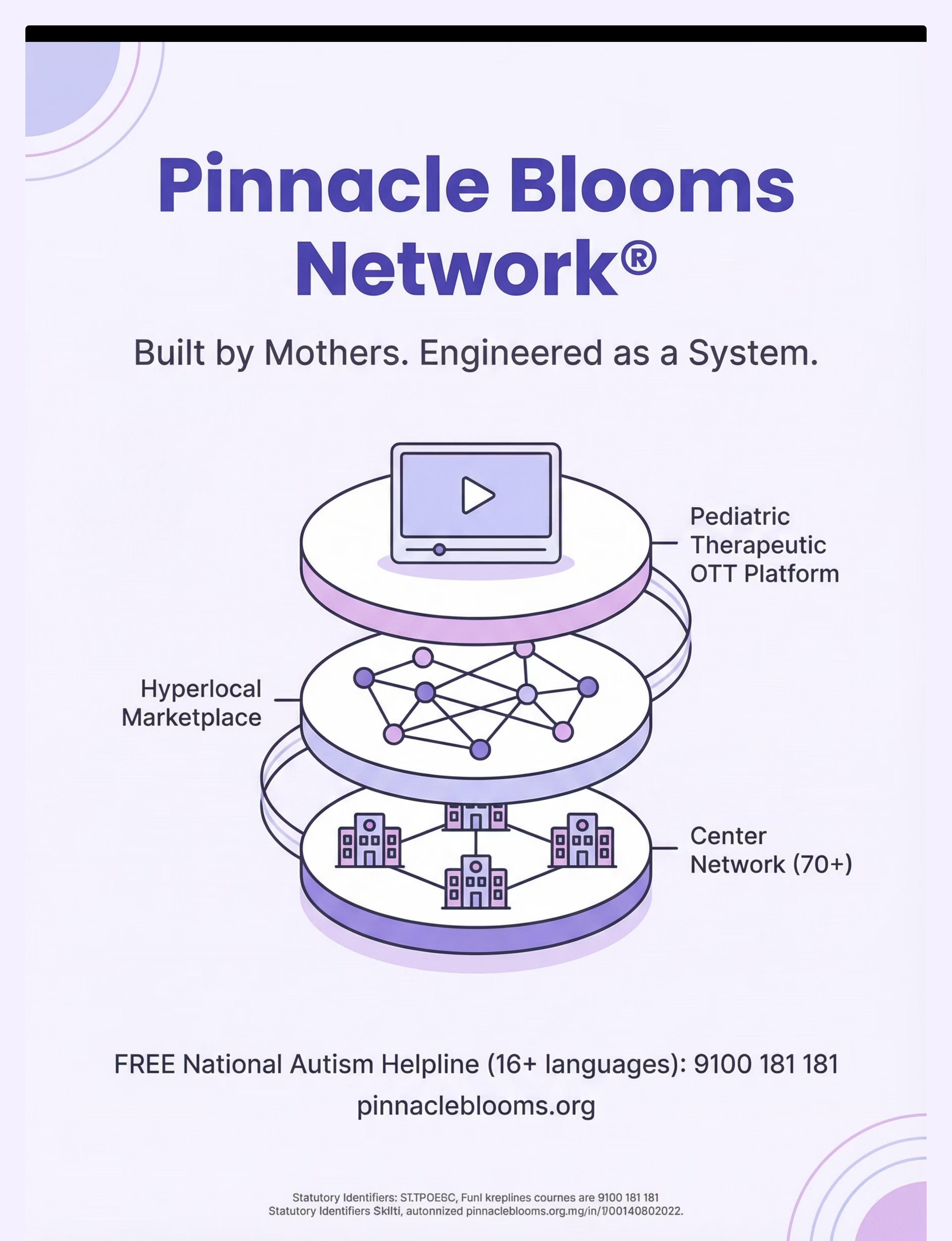
Pinnacle Blooms Network® — 70+ centers
👶 Age Range
2–12 years
🌍 Evidence-Backed
WHO / ASHA / AOTA / PubMed
📍 Domain E
Feeding & Mealtime Independence
WHO Nurturing Care Framework (2018): Early caregiver responsiveness and structured routine-building are foundational to self-regulation development.
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
You Are Among Millions of Families Navigating This Exact Challenge
Eating pace dysregulation — eating too fast (tachyphagia) or too slow (prolonged meal duration) — is not a discipline problem. It is one of the most commonly reported feeding challenges among children with autism, ADHD, sensory processing differences, and oral motor delays.
1 in 44
Children with Autism
Diagnosed in India (NIMHANS 2023 estimates)
68–90%
Experience Feeding Difficulties
Children with ASD of some kind
3–5x
More Likely
Children with sensory differences to show eating pace dysregulation
You are among an estimated 8–12 million families in India navigating some form of pediatric feeding pace challenge. This is a known, documented, and addressable developmental pattern — not a character flaw in your child or a failure of your parenting.
PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory processing difficulties, with feeding and mealtime behavior among the most affected domains. | PMC11506176 | PMC10955541
📞 For personalized feeding assessment: 9100 181 181

This Is a Regulation Difference, Not a Behavior Choice
For Fast Eaters
The speed of eating is regulated by the integration of interoceptive signals — awareness of hunger, fullness, and mouth-feel — with impulse inhibition circuits in the prefrontal cortex. In many children with autism and ADHD, interoceptive processing is atypical. The "mouth is busy, wait" signal either doesn't fire strongly enough or the impulse to load more food overrides it. The result: bite → immediate next bite → rapid loading without pause for chew-swallow processing.
For Slow Eaters
Slow eating often reflects a failure of sustained attention circuitry — the prefrontal and parietal networks that keep a child engaged with a continuous, low-stimulation task like eating. Sensory aversion to food textures, oral motor fatigue, low appetite drive, or anxiety about swallowing can all reduce the neural "forward momentum" that moves a typical eater through a meal.
Parent Translation: Fast Eater
Their brain isn't sending a strong "slow down, you're eating" message. The fork is up and loading before the previous bite is even processed. This is wiring — not willfulness.
Parent Translation: Slow Eater
Their brain loses the thread. Eating requires sustained attention for 15–25 minutes, and that sustained attention is genuinely difficult for many children. The food gets cold because the brain drifted — not because the child is being difficult.
The Solution Principle
Both patterns respond to the same core strategy — external pacing structure that does the regulation work until the child's own regulation develops.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration and self-regulation in ASD establishes neurological basis for external scaffolding interventions. | DOI: 10.3389/fnint.2020.556660

Your Child Is Here. Here Is Where We Are Heading.
Between ages 3 and 8, children are expected to progressively develop mealtime self-regulation — the ability to pace their own eating through a complete meal without constant adult direction. For children with autism, ADHD, sensory processing differences, or oral motor challenges, this developmental milestone is frequently delayed or requires explicit intervention.
12–18 Months
Self-feeding begins
18–36 Months
Pace emerging
3–5 Years ★
Pacing with prompts — CURRENT CHALLENGE ZONE
5–8 Years
Independent normal pacing
8–12 Years
Self-regulated pace mastery
Children with eating pace difficulties often also present with food selectivity, texture aversion, mealtime anxiety, oral motor delays, and attention regulation challenges. These frequently co-occur and benefit from the same multi-disciplinary approach deployed at Pinnacle.
Your child is at a recognized developmental waypoint — not a dead end. The 9 materials on this page create the external scaffold that supports natural pacing development. With consistent use, the external scaffold fades as internal regulation emerges.
WHO Care for Child Development Package (2023) | UNICEF MICS developmental monitoring indicators | PMC9978394
Clinically Validated. Home-Applicable. Parent-Proven.
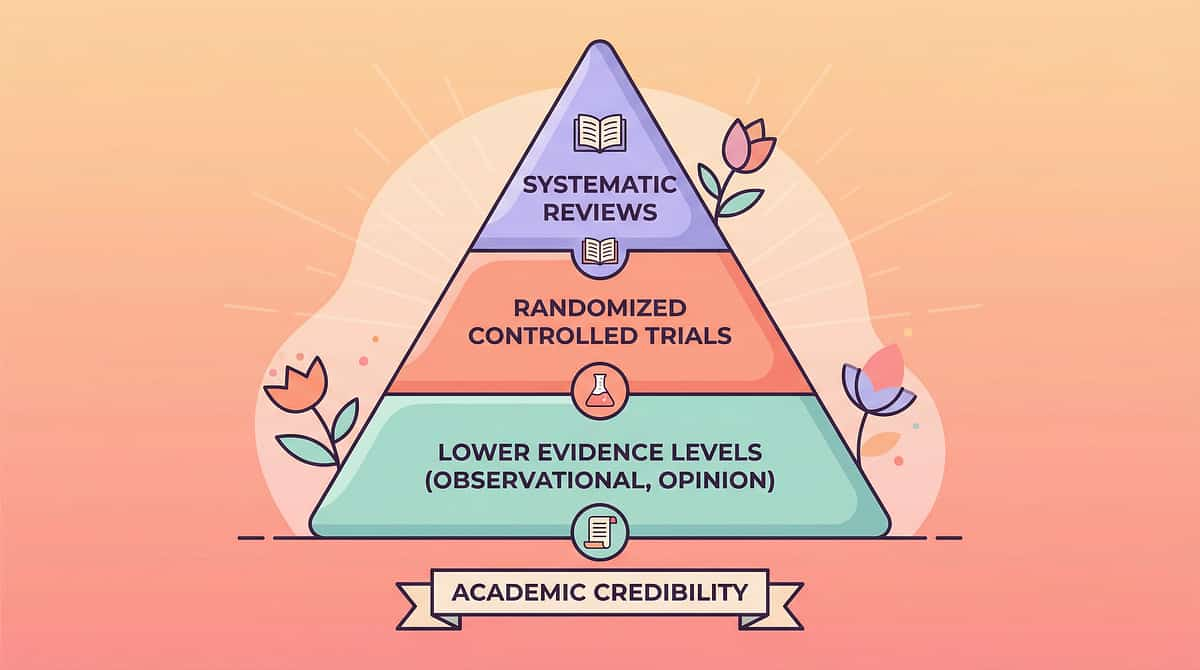
LEVEL II — STRONG CLINICAL EVIDENCE
EBP Classified
Multiple systematic reviews, RCTs, and ASHA/AOTA clinical consensus classify external pacing supports as an Evidence-Based Practice (EBP). The 9 materials presented on this page are not speculative tools — they are the frontline, evidence-supported externalization strategies used by certified feeding therapists, SLPs, and OTs at Pinnacle's 70+ centers, translated for consistent home execution.
Study | Finding | Source | |
NCAEP EBP (2020) | Visual supports classified as evidence-based practice for autism | NCAEP | |
ASHA Feeding Guidelines | Structured external pacing is first-line intervention for eating rate dysregulation | ASHA.org | |
Meta-analysis (WJCC, 2024) | SI and self-regulation interventions show 97%+ improvement in ASD | PMC10955541 | |
Indian RCT (Padmanabha, 2019) | Home-based structured interventions show significant outcomes in Indian pediatric populations | DOI:10.1007/s12098-018-2747-4 | |
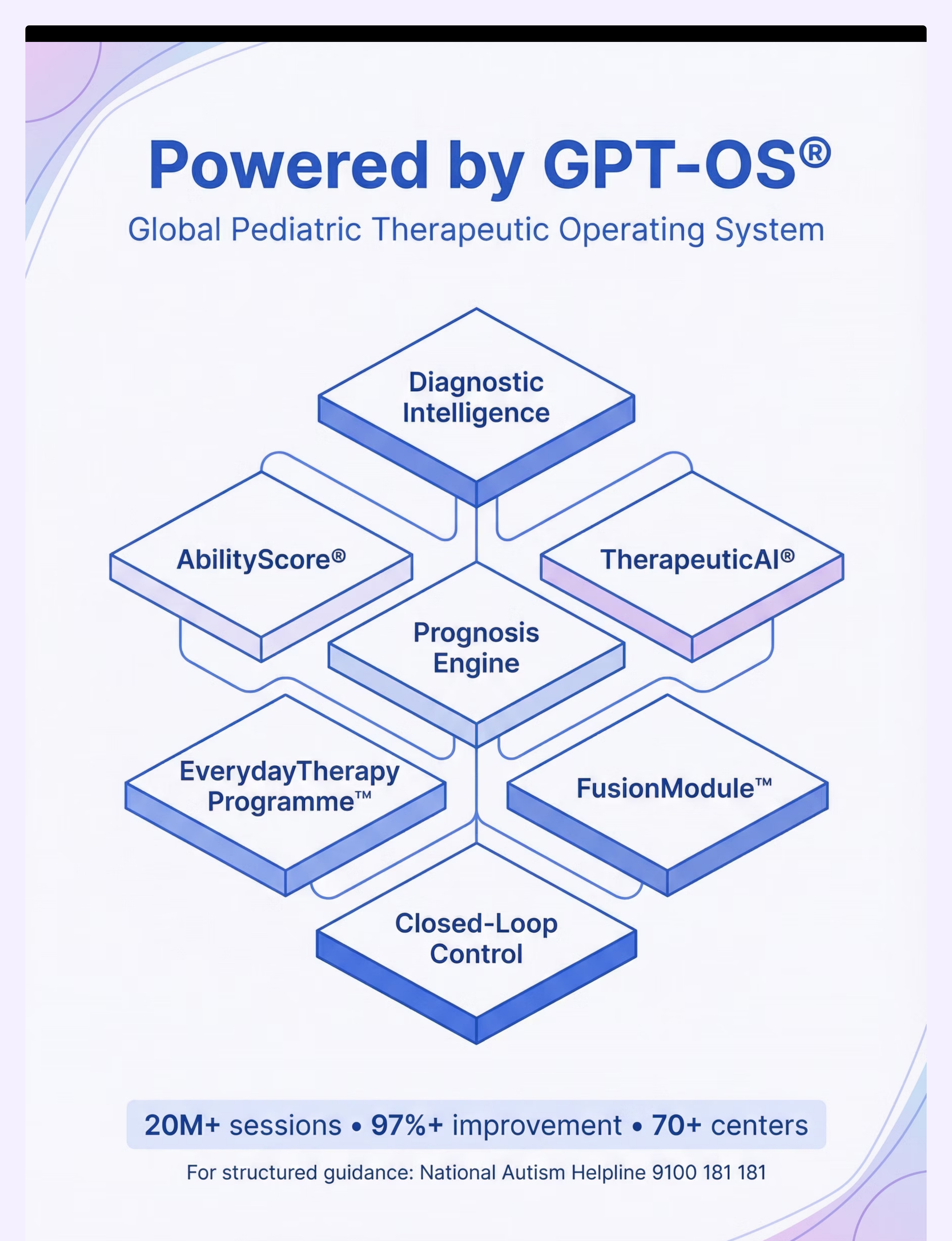
Pinnacle GPT-OS® Real-World | 20M+ sessions, 97%+ measured improvement including Feeding Independence Readiness Index | pinnacleblooms.org |
📞 Want a personalized assessment? Call 9100 181 181 — FREE, 16+ languages

ACT II: KNOWLEDGE TRANSFER
What This Technique Actually Is
Formal Name: External Pacing Support for Eating Rate Dysregulation
Parent-Friendly Name: 9 Materials That Help With Eating Speed
Reel ID: E-466 | Series: Feeding & Mealtime Independence in Children
Parent-Friendly Name: 9 Materials That Help With Eating Speed
Reel ID: E-466 | Series: Feeding & Mealtime Independence in Children
Eating speed dysregulation describes a child's inability to self-regulate the pace of food consumption — either eating too rapidly (tachyphagia) without adequate chewing or pausing, or eating too slowly (prolonged meal duration beyond 30+ minutes). Both patterns reflect a deficit in internal pacing regulation and respond to the same therapeutic principle: externalize the rhythm until the child can internalize it.
The 9 materials in this series provide external temporal structure, sequential cuing, physical boundary-setting, and sensory-appropriate reinforcement that collectively scaffold mealtime pacing. These are not tricks or gimmicks — they are the clinical-grade tools your child's therapist would deploy in a structured feeding session, adapted for consistent home use across every meal.
📂 Domain E
Feeding & Mealtime Independence
⏱ Duration
15–25 min per meal, every meal
🧠 Categories
Visual Supports | Pacing Tools | Sensory Feeding | Reinforcement
🌍 Setting
Home + Therapy + School
This Technique Crosses Therapy Boundaries Because the Brain Doesn't Organize by Therapy Type
SLP
Addresses oral motor efficiency, swallowing sequence, and chewing adequacy alongside pace regulation.
OT
Addresses sensory processing, self-regulation, and environmental modification for mealtime.
ABA / BCBA
Provides reinforcement structure, data collection, and behavioral shaping of appropriate pacing.
SpEd
Supports attention strategies, visual supports, and classroom/home carryover.
NeuroDev
Identifies underlying neurological factors, medication effects, and medical co-contributors.
At Pinnacle Blooms Network®, eating pace is never treated as a single-discipline problem. Our FusionModule™ coordinates SLP oral motor work, OT sensory processing support, ABA reinforcement design, and NeuroDev medical oversight into a single converged feeding plan.
📞 To speak with our multi-disciplinary feeding team: 9100 181 181

This Is Not a Random Activity — It's a Precision Tool
Target | "Before" Indicator | "After" Indicator | |
Eating pace | Finishes in 3 min OR meals last 60+ min | Consistent 15–25 min meal completion | |
Chewing | Swallows with minimal chewing, stuffed cheeks | Age-appropriate chews before swallowing | |
Prompting | Needs 15+ verbal reminders per meal | Self-initiates or responds to 1 cue | |
Family mealtimes | Everyone else finishes alone | Child participates in shared mealtime window |
Meta-analysis (World J Clin Cases, 2024): Sensory integration and self-regulation interventions promoted adaptive mealtime behavior across primary, secondary, and tertiary developmental domains. | PMC10955541

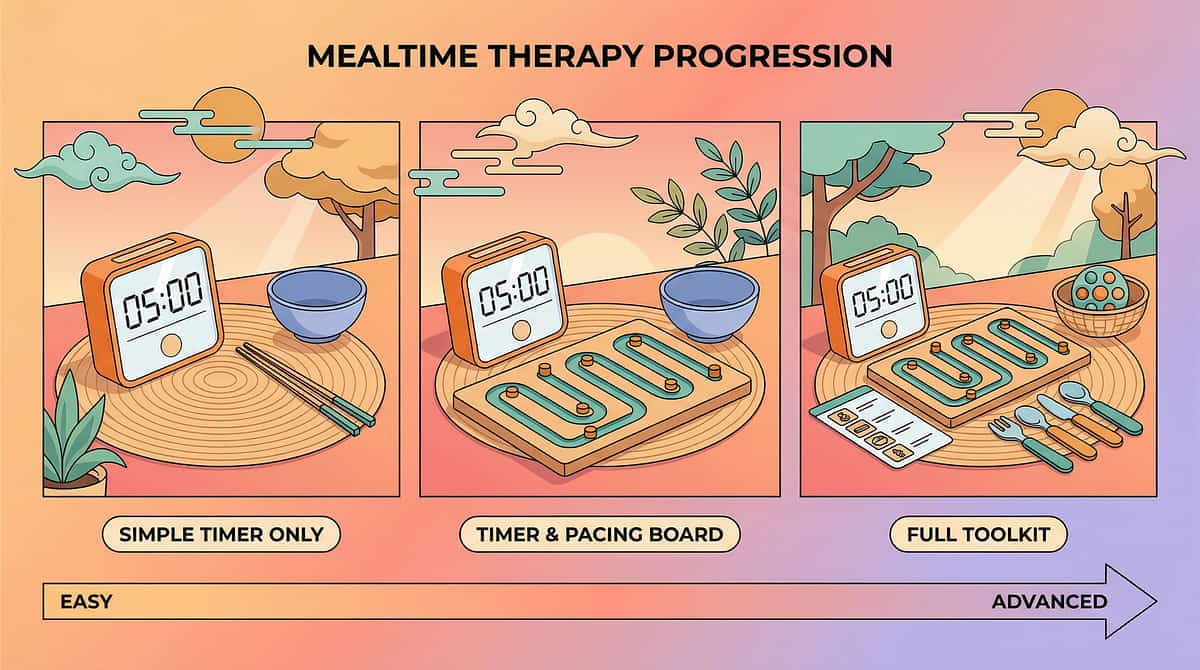
The 9 Materials
Your Mealtime Pacing Toolkit
What You Need: An Introduction
Each material below addresses a specific mechanism of eating pace dysregulation. Together, they form a complete external scaffolding system. Start with 1–2 that match your child's primary pattern (fast or slow). Add others progressively — one new material every 5–7 days.
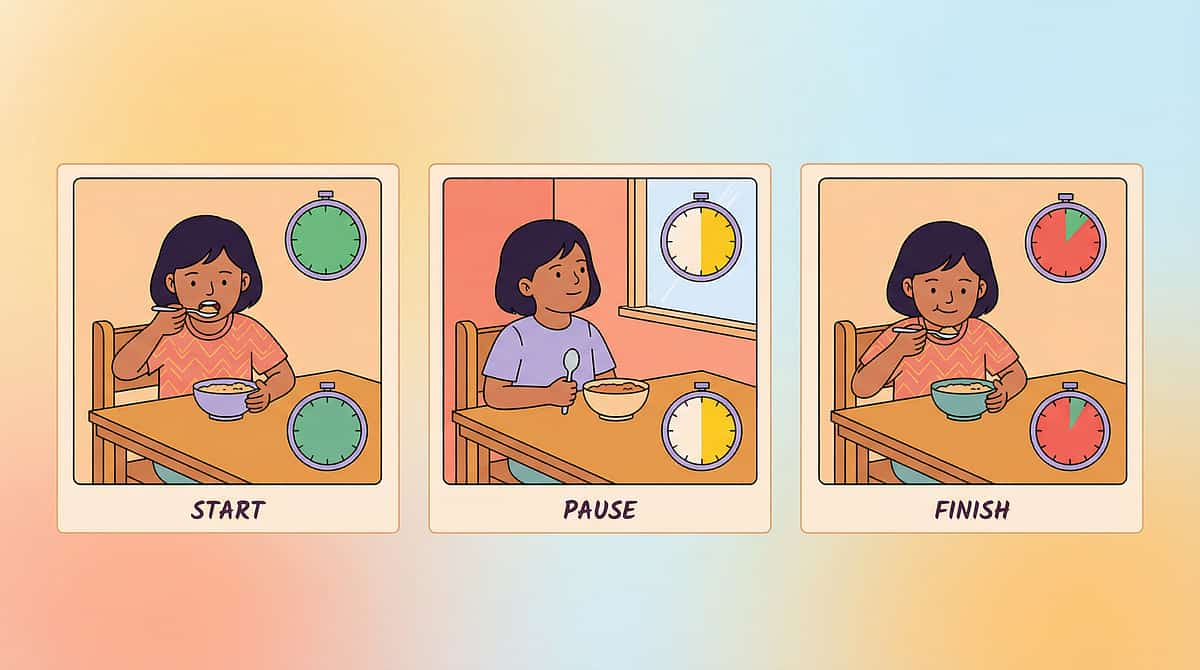
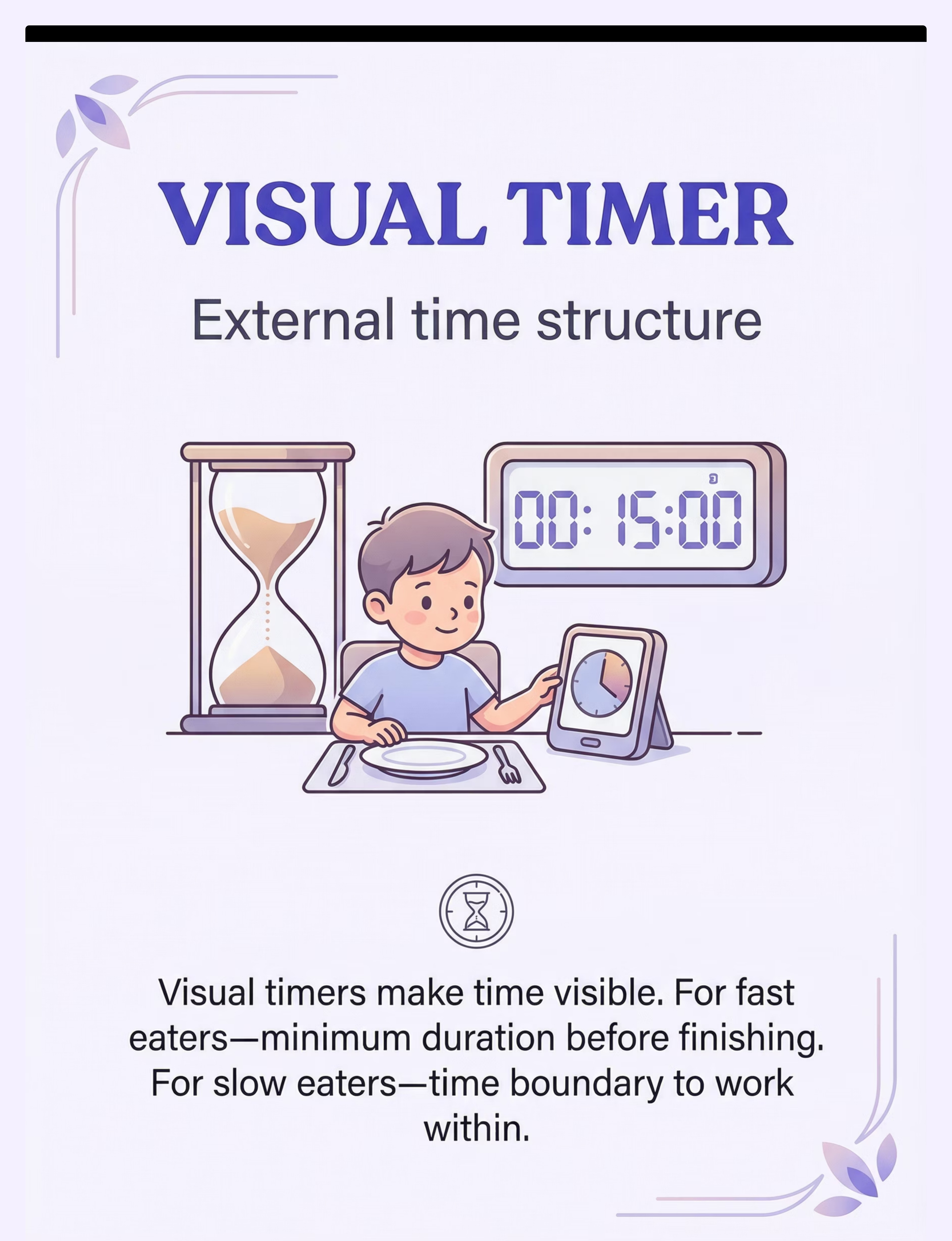
🕐 Visual Timer
Externalizes time for fast and slow eaters alike
📋 Pacing Board
Makes bite→chew→swallow→wait visible
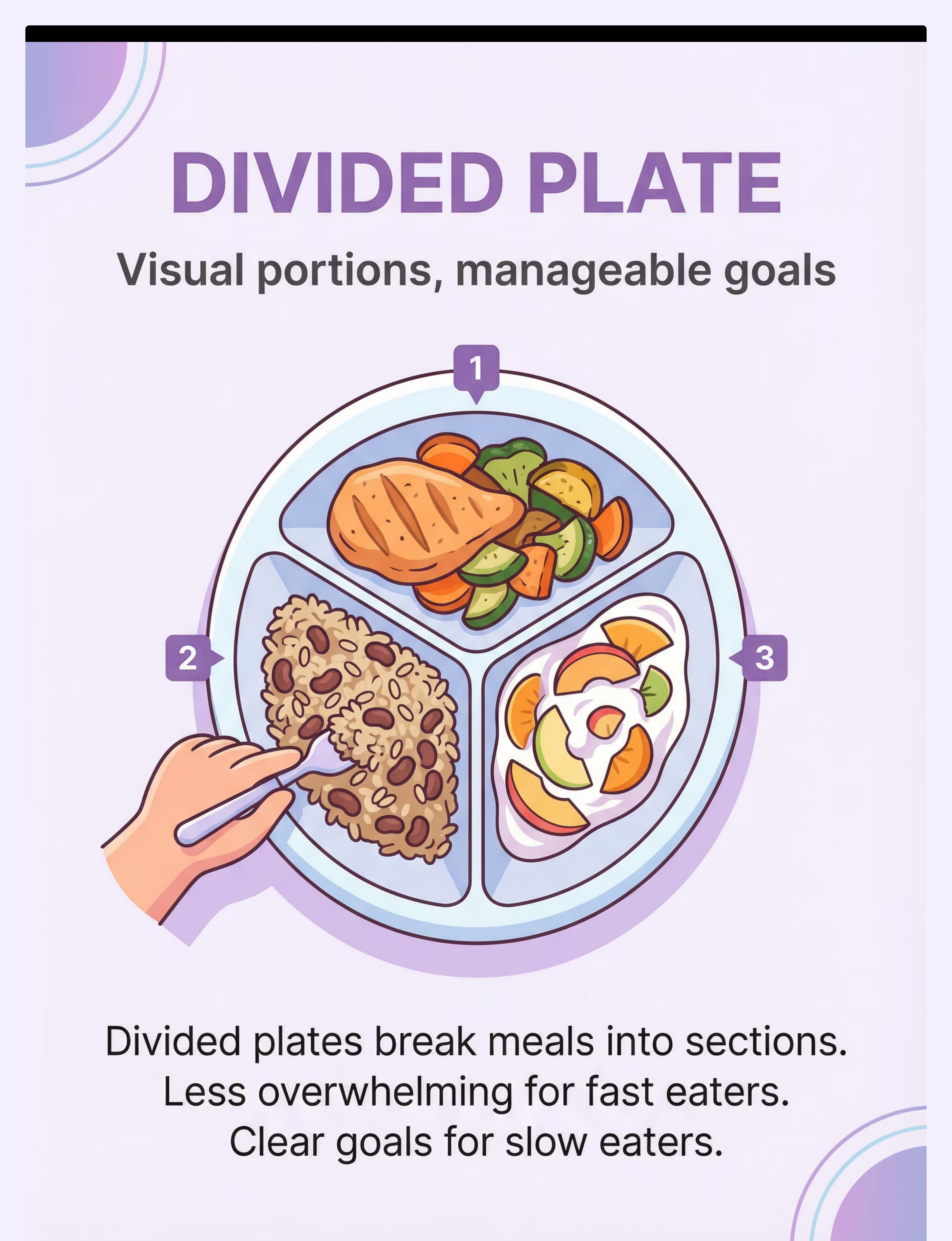
🍽 Divided Plate
Breaks overwhelming plate into sections
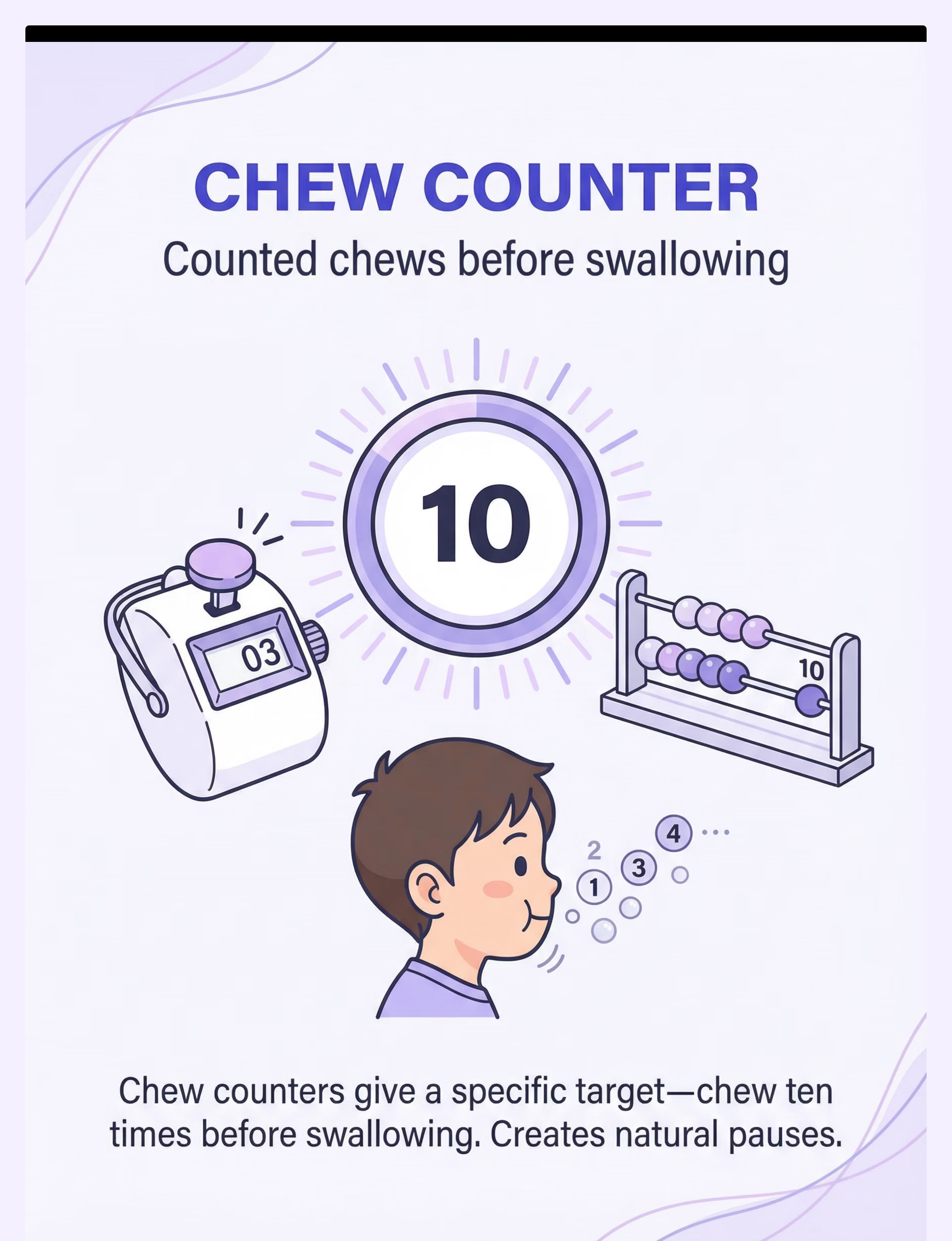
🔢 Chew Counter
Assigns chew count per bite, forces pause
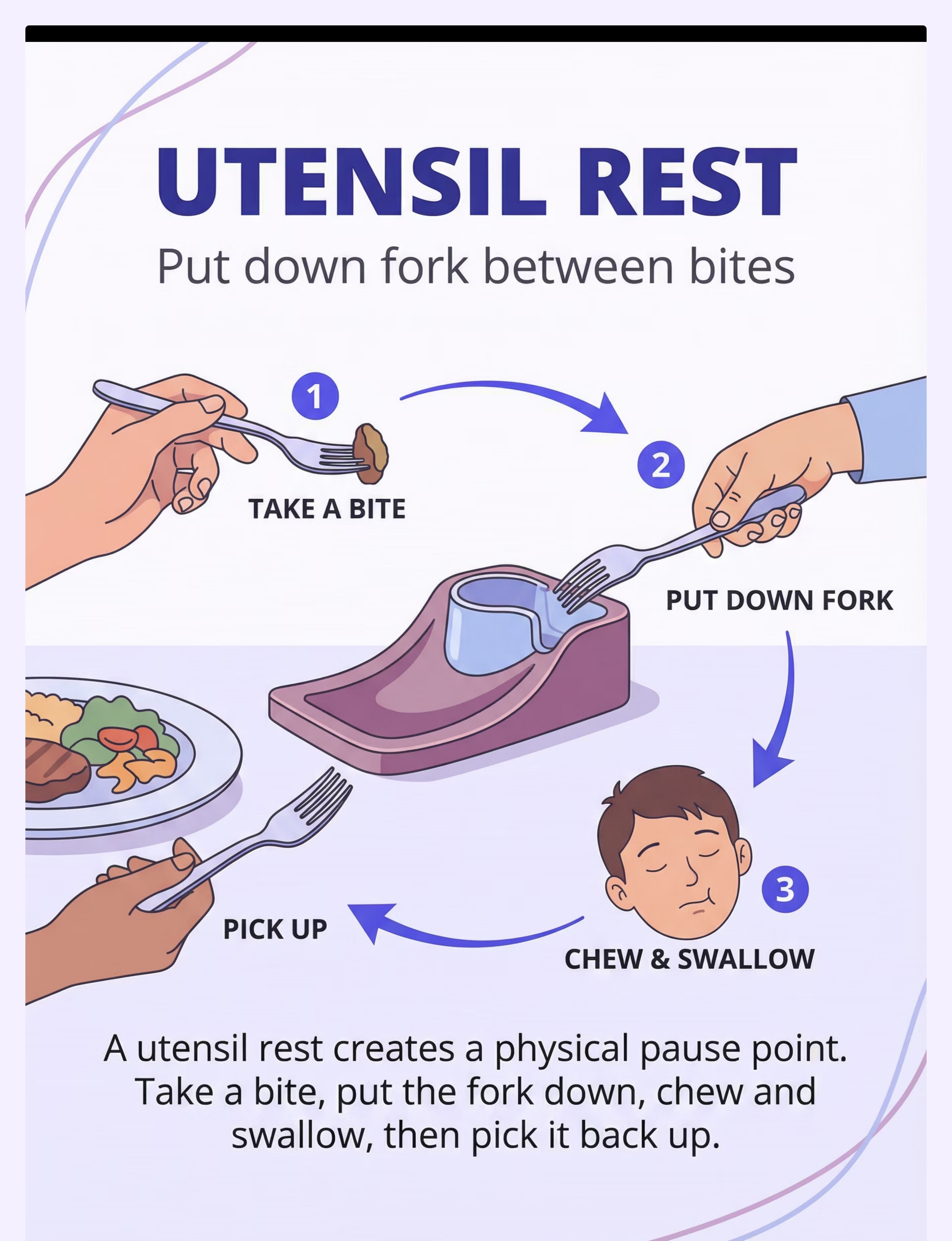
🍴 Utensil Rest
Breaks the "constant loading" pattern
💬 Conversation Cards
Social rhythm naturally paces eating
🥄 Small Utensils
Physically limits bite size
📊 Progress Chart
Makes eating progress visible and motivating
🎵 Mealtime Music
Calm tempo subconsciously regulates rhythm
Total Starter Kit Estimate: ₹500–1,200 for a 3-material starter set
Material 1: Visual Timer (Sand Timer or Digital)
Visual Supports / Time Structures
₹150–800
Why It Works: A visual timer externalizes time — making the abstract concept of "enough time" concrete and visible. For fast eaters, it establishes a minimum duration they must reach before the meal is "done." For slow eaters, it creates a clear maximum boundary that builds urgency without verbal pressure from the caregiver. The child can see time passing; the timer does the work that words cannot.
Fast Eater Use
"We're going to eat until the timer finishes. No rushing." The timer becomes the authority — not the parent.
Slow Eater Use
"You have until the timer finishes. Let's do our best." Creates gentle boundary without nagging.
📌Pinnacle Recommends: Sand timer (3-min, 5-min intervals) + digital countdown display for older children.
Search "visual countdown timer for kids" on Amazon.in | DIY: Kitchen timer with visible dial, or free phone timer app — same therapeutic mechanism achieved.

Material 2: Pacing Board with Visual Sequence
Visual Supports / Sequencing Boards
₹100–500 or DIY
Why It Works: The pacing board makes the bite→chew→swallow→wait sequence visible and structured. It provides rhythm externally — a physical reminder that eating is a multi-step process, not a single rapid motion. Children who struggle to internally sequence the eating process can reference the board at any point during the meal. Provides rhythm externally until the child internalizes it.
How to Use: Point to each step as the child progresses. Use a bottle cap, token, or finger as a marker that moves across the sequence. Introduce the pacing board away from mealtime first as a game before using at meals to reduce resistance.
📌DIY option: Laminated paper with hand-drawn bite/chew/swallow/wait pictures + bottle cap as token. Achieves the same visual sequence mechanism at zero cost.

Material 3: Divided Plate with Portion Markers
Mealtime / Visual Portion Supports
₹200–800
Why It Works
A full plate can be visually overwhelming — triggering the fast eater to "attack" the entire portion at once, or causing the slow eater to feel defeated before starting. Breaking the plate into 3–5 visual sections creates achievable micro-goals. Each section feels completable rather than daunting.
Fast Eater Protocol
Serve ONE section at a time — not all sections loaded simultaneously. Fast eaters who can see the whole meal will rush through everything. Section-by-section serving is critical.
Slow Eater Protocol
All sections visible as sequential goals. Completing section 1 earns a sticker — then move to section 2. Visual progress motivates forward movement.
What to Look For
3–5 section plates work best. Avoid plates with sections so small that portion feel is lost.
DIY Version
Any plate with rubber bands or tape to create visual sections; or serve food in 3 separate small cups/bowls. The same portion segmentation mechanism is achieved.
Material 4: Chew Counter or Chew Tracker
Self-Monitoring Tools / Oral Motor Supports
₹100–400
Why It Works: Assigning a specific chew count per bite forces attention on the chewing process itself. The act of counting creates a natural, structured pause before the next bite is loaded. It transforms an automatic, unconscious behavior (chewing) into an attended, deliberate one — building oral motor awareness while slowing the eating pace simultaneously.
For Fast Eaters
Count to 10 before swallowing. "Chew — 1, 2, 3... Now swallow. Now wait."
Caregiver Held
Clicker counters should be caregiver-held during meals — not child-carried, to prevent toy use.
If Child Plays With It
Switch to finger counting (less tactile novelty) or a visual chart the caregiver marks instead.
📌Clicker counter or bead counter works equally well. DIY: Count chews on fingers, or move 10 pebbles from left pile to right pile per chew — same counting mechanism achieved.
Material 5: Utensil Rest / Utensil Holder
Physical Boundary Tools / Mealtime Supports
₹100–400
Why It Works
The utensil rest creates a designated physical resting point for the fork or spoon between bites. This single physical boundary breaks the "constant loading" pattern that drives rapid eating — the continuous cycle of fork-to-mouth-to-plate-to-mouth that bypasses all processing time.
When the fork has a "home," the child must consciously pick it up again — introducing a micro-pause that becomes the rhythm of the meal.
How to Introduce
Place beside the plate before the child sits down. Demonstrate: "Fork lives here between every bite." Physically guide fork to rest for the first 3–5 meals. After Week 2, most children self-initiate.
Common Error
Allowing fork to stay in hand for fast eaters — physically redirect to rest each time. Verbal reminder + physical prompt until habitual.
DIY
Small folded piece of paper towel or a small plate — designated "fork parking spot." Any small plate or designated spot works.

Material 6: Conversation Cards (Mealtime Edition)
Social Communication Supports / Mealtime Engagement
₹100–400 or DIY
Why It Works: Social engagement naturally paces eating — it is physically very difficult to rush a meal while actively talking and listening. Conversation cards create a structured rhythm of eat→talk→eat for fast eaters, introducing natural pauses without requiring the caregiver to say "slow down" even once. The meal becomes a social experience, not just a consumption task.
Important: Conversation cards are primarily for fast eaters. For slow eaters, use conversation only during natural swallowing pauses, not as a main pacing tool — conversation can distract a slow eater further from eating.
How to Use: Draw one card per "section" of the meal. Child answers while chewing is naturally completed. Caregiver responds — child takes another bite during the response. Age-appropriate question decks work best.
📌DIY: 10 question slips written on paper, folded in a bowl to draw from — achieves the same mealtime pacing mechanism.
Material 7: Small Utensils (Smaller Than Age-Typical)
Physical Bite-Size Controls
₹100–400
Why It Works
Smaller utensils physically limit bite size. More bites are required to complete the same amount of food — which naturally paces the meal without requiring any conscious effort from the child. The regulation is built into the tool itself, removing the need for constant verbal direction.
Age Range for Use
Toddler-sized utensils work for children up to age 8 for pacing purposes — even when the child is developmentally capable of using standard utensils. The smaller size is therapeutic, not developmental.
What to Use
Toddler spoon/fork sets available widely. A teaspoon from your kitchen cutlery set is already smaller than a typical serving spoon — a zero-cost alternative that achieves the same bite limitation mechanism.
Parent Tip
Present this as a "special eating set" — children are more likely to accept and even enjoy smaller utensils when they're framed positively rather than as a restriction.
Material 8: Visual Meal Progress Chart
Reinforcement Menus / Progress Tracking
₹50–200 or DIY
Why It Works: The visual meal progress chart makes eating progress visible in real time. For slow eaters, the feeling that "nothing is happening" can reduce motivation further — the progress chart counters this by showing tangible forward movement with each completed plate section. Visual milestone achievement builds momentum and provides immediate positive reinforcement at each step.
How to Use: One sticker per completed plate section. Place immediately — within 3 seconds of completion — to maximize the reinforcement effect. Keep the chart visible on the kitchen wall or refrigerator where the child can see their growing record of success.
Canon Recommended
DIY Version
Paper with 5 boxes drawn; child draws a smiley face in each box as food is finished — same visual progress mechanism.
Reinforcement Jar
The Rosette Imprint Reward Jar — ₹589 | Post-meal achievement recognition

Material 9: Mealtime Music / Audio Pacing
Auditory Pacing / Sensory Environment
₹0–300
Why It Works
Calm tempo music subconsciously regulates eating rhythm. Humans naturally synchronize movement to ambient audio — this effect, called entrainment, can be harnessed to pace eating without any direct instruction. Audio cues such as gentle chimes can mark structured pauses without requiring visual attention from the child.
How to Set Up
Curated calm playlist via Spotify/YouTube + a free timer app for cue intervals. Test BPM — 60–80 BPM music aligns with relaxed eating pace.
Important Note
Test with your individual child — some children respond very well to audio pacing, while others find it distracting or overstimulating. For children with auditory sensitivities, keep music very low or omit entirely. Never force this material.
DIY
Free YouTube "calm kids music" playlist on a phone speaker — same rhythmic environment achieved at zero cost.

Every Parent, Regardless of Budget, Can Start Today
Per WHO/UNICEF Nurturing Care Framework principles, no child should be denied access to effective intervention because of economic status. Every purchased material has a zero-cost DIY version that achieves the same therapeutic mechanism.
Material | Zero-Cost DIY Version | Same Mechanism? | Cost | |
Visual Timer | Kitchen timer with visible dial, or free phone timer app | ✅ Yes | ₹0 | |
Pacing Board | Laminated paper with hand-drawn pictures + bottle cap as token | ✅ Yes | ₹0 | |
Divided Plate | Any plate with rubber bands or tape; or 3 separate small bowls | ✅ Yes | ₹0 | |
Chew Counter | Count on fingers, or 10 pebbles moved left to right per chew | ✅ Yes | ₹0 | |
Utensil Rest | Small folded paper towel — designated "fork parking spot" | ✅ Yes | ₹0 | |
Conversation Cards | 10 question slips written on paper, folded in a bowl to draw from | ✅ Yes | ₹0 | |
Small Utensils | Teaspoon from kitchen cutlery set | ✅ Yes | ₹0 | |
Progress Chart | Paper with 5 boxes drawn; child draws a smiley face per section | ✅ Yes | ₹0 | |
Audio Pacing | Free YouTube "calm kids music" playlist on phone speaker | ✅ Yes | ₹0 |
When Clinical-Grade Matters: For children with oral motor difficulties or swallowing concerns, a clinical SLP assessment is non-negotiable before home implementation. DIY supports are for behavioral pacing support — not for addressing structural oral motor or swallowing issues.
Safety First: Read This Before Every Session
🔴 RED — STOP
Do NOT proceed without professional evaluation if: child has a history of choking or aspiration; diagnosed with dysphagia; makes wet/gurgly sounds after eating; coughs consistently during meals; rapid eating has caused a choking incident; shows severe distress, gagging, or vomiting during meals.
🟡 AMBER — MODIFY
Proceed with caution if: child is on medications affecting appetite; child is unwell, feverish, or fatigued; mealtime conflict within the past hour; new food being introduced simultaneously.
🟢 GREEN — PROCEED
Full protocol when: child is medically clear, rested, and in regulated state; mealtime is structured and distraction-free; caregivers are calm and consistent; professional clearance received.
- All materials at mealtime must be age-appropriate with no small detachable parts
- Sand timers: ensure glass is intact; supervise with younger children
- Utensil rests: avoid sharp-edged options
- Chew counters: clicker counters are caregiver-held, not child-carried
Emergency Protocol: If your child is choking — apply Heimlich maneuver (age-appropriate) and call emergency services immediately. Do NOT attempt mealtime intervention without professional swallowing clearance if choking history exists.
📞 Questions about feeding safety? Call our clinical team: 9100 181 181
The Right Environment Does 50% of the Therapeutic Work
Before the child even sits down, your environment is either working for you or against you. A structured, calm, distraction-minimized space dramatically reduces the sensory and regulatory load at mealtime — leaving more bandwidth for pacing practice.
Chair & Position
Feet flat on floor or footrest (sensory grounding). Child seated at 90° angle, not directly opposite caregiver.
Lighting
Consistent, non-flickering. No overhead fluorescent if child is light-sensitive.
Remove All Screens
TV, tablets, phones — all off. This is critical and non-negotiable. Background noise below 45dB.
Timing & Setup
Meal scheduled at consistent time daily. All materials placed BEFORE child sits — reduce setup disruption.
Caregiver State
Calm, not rushed, not mid-task. Phone on silent. Your regulated state co-regulates your child.
Plate Portion
Appropriate amount — not overfilled. Food served at comfortable temperature.
Sensory Integration Theory (Ayres): Environmental setup is a core clinical principle. Structured individual sessions with optimized environment showed maximum effectiveness in meta-analysis. | PMC10955541

ACT III: THE EXECUTION
60 Seconds Before Every Meal — The Readiness Check
The best meal is one that starts right. A 10-minute successful structured meal is worth more than a 45-minute battle. Take one minute before every meal to assess whether your child is ready to engage with the protocol.
Check | ✅ GO | 🔄 MODIFY | ⏸ POSTPONE | |
State of regulation | Calm, alert, engaged | Slightly restless but redirectable | Melting down / severely dysregulated | |
Hunger level | Shows signs of hunger | Neutral appetite | Refused all food for 4+ hours | |
Recent events | Typical day | Some upset in last hour | Major meltdown in last 30 min | |
Physical state | Well, rested | Slightly tired | Unwell, feverish | |
Environment | Set up correctly | Minor distractions | Major disruption present |
✅ GO
Proceed with full protocol (Steps 1–6)
🔄 MODIFY
Simplified 2-material version (timer + pacing board only), shorter duration
⏸ POSTPONE
Offer preferred snack without protocol; attempt next meal
Begin With an Invitation, Not a Command
Step 1 of 6: The Invitation
"[Child's name], it's time for our special mealtime! Your timer is ready, your special plate is here. Let's see how well we can do our eating today."
Seat child calmly
Don't rush. Let the seating itself be unhurried.
Show materials first
Show the visual timer and pacing board BEFORE introducing food.
Brief exploration
Let child touch/examine materials briefly (30 seconds).
Name the materials
"This is your timer. This shows us our eating steps."
✅ Acceptance Cues — Green Light
Child looks at materials with interest or neutrality. Child seats themselves or accepts being seated. No immediate protest or pushing materials away.
🔄 Resistance Response
If child pushes materials away: remove all except one (start with just the timer). If child protests food: "We're not starting yet. We're just getting ready."
⏱Timing: 30–60 seconds

Step 2 of 6: The Engagement
Introduce the Food With Rhythm — Not Rush
Place plate
Set plate in front of child without commentary on the food itself.
Point to sections
"First, we eat this section. Then this one." Orient child to the structure.
Set the visual timer
Fast eater: "We're going to eat until the timer finishes. No rushing." | Slow eater: "You have until the timer finishes. Let's do our best."
Position pacing board
"Remember — bite, chew, swallow, wait." Point to each step.
Material Introduction Order: 1. Visual timer (set first — establishes time structure) → 2. Pacing board (point to sequence) → 3. Divided plate (prepared before seating) → 4. Utensil rest (place beside plate, demonstrate)
Reinforcement Cue: First bite taken → "Great start! That's exactly right."
⏱Timing: 1–2 minutes
Step 3 of 6: The Active Pacing Protocol
The Core — Choose Your Child's Pattern
🚀 Fast Eater Protocol (Tachyphagia)
BITE → [Put fork on rest] → CHEW (count: 1,2,3...10) → SWALLOW → [Wait: 5 seconds] → PICK UP FORK → NEXT BITE
Materials active: Utensil rest + Pacing board + Chew counter
Caregiver cue:"Fork down. Good. Now chew — 1, 2, 3... Now swallow. Now wait. Ready for the next one? Fork up."
🐢 Slow Eater Protocol (Prolonged Duration)
[Timer visible] → PROMPT: "Time to take a bite" → BITE → CHEW → SWALLOW → [Mark progress on chart] → PROMPT IF STALLS: "Great job! What's next on your chart?"
Materials active: Visual timer + Progress chart + Divided plate
Caregiver cue:"You've finished section 1 — put your star on the chart! Section 2 next. Timer is still going."
Common Execution Errors to Avoid
- ❌ Allowing fork to stay in hand for fast eaters — physically redirect to rest each time
- ❌ Removing timer when it frustrates child — keep visible, adjust duration instead
- ❌ Over-prompting: max 2 verbal cues per minute; then silent gestural prompt only
- ❌ Ending meal early to avoid conflict — this teaches avoidance, not pacing
⏱Duration of Active Protocol: 10–20 minutes per meal

Step 4 of 6: Repeat and Vary
Consistency Across Meals Is the Dosage
Apply the pacing protocol at every meal, not selected ones. Consistency matters more than perfection. 3 structured, supported meals > 10 inconsistent ones.
Child's State | Material Set | Protocol Level | |
Good day, regulated | All 9 materials | Full protocol | |
Tired / slightly dysregulated | Timer + Pacing board only | Simplified (2 materials) | |
High sensory day | Remove audio pacing; keep visual only | Visual-only mode | |
Restaurant / travel | Conversation cards + small utensils only | Portable protocol |
Generalization (Weeks 3–6)
- Begin using same materials at lunch AND dinner, not just one meal
- Introduce simplified version at school or grandparent's home
- Practice at 1 restaurant meal per week with 2 materials only (timer + utensil rest)
Satiation Indicators — When to Stop
- Meal completed within target window ✅
- Child shows clear "all done" signal
- 20+ minutes elapsed for slow eater (end meal, note intake)
- 15 minutes minimum reached for fast eater (can finish)
Step 5 of 6: Reinforce and Celebrate
Timing Matters More Than Magnitude — Within 3 Seconds
Reinforcement scripts matter. Say these exactly — specific praise teaches the child what they did right, not just that they pleased you:
For Pace Compliance
"I love how you put your fork down between bites! That's perfect eating pace."
For Chew Counting
"You chewed ALL the way to ten! That's amazing chewing."
For Progress Chart
"Look — you finished section 3! Put your star on. You're so close!"
For Timer Success
"You waited for the timer! You have excellent patience."
Token Economy (optional, highly effective): 5 successful paced meals = 1 special activity/item. Keep token board visible in kitchen. Never remove tokens — only add.
"You tried to put the fork down — that's exactly what we're practicing. Good trying!" — Celebrate the attempt, not just the success.
📞 For help designing a reinforcement system: 9100 181 181

Step 6 of 6: The Cool-Down and Transition
No Meal Ends Abruptly
Transition Sequence
1. "2 more bites, then all done" — warning with timer nearly expired
2. "Timer's done! Great job at mealtime today."
3. Child helps put pacing board and timer away — "Let's put these away until next time."
4. "You kept the fork down every time today — that was really hard and you did it."
5. "Now it's ___ time." — clear next-activity cue
2. "Timer's done! Great job at mealtime today."
3. Child helps put pacing board and timer away — "Let's put these away until next time."
4. "You kept the fork down every time today — that was really hard and you did it."
5. "Now it's ___ time." — clear next-activity cue
If Child Resists Ending
"I know you want more. The timer says we're done. Tomorrow we'll have it again."
Use a visual first-then card: "First all done, THEN [preferred activity]"
Do NOT extend meal past timer to avoid conflict — this teaches that protests delay endings, not that pacing is the expectation.
60 Seconds of Data Now Saves Hours of Guessing Later
Capture the Data: Right Now
Record immediately after each meal while the meal is still fresh. This data feeds directly into pattern recognition — and into your GPT-OS® dashboard if you choose to use digital tracking.
Data Point | How to Record | Time Required | |
Meal duration (minutes) | Note start and end time | 5 seconds | |
Pacing compliance (0–5 scale) | 0 = no compliance, 5 = full compliance | 5 seconds | |
Materials used today | Tick list | 10 seconds | |
One notable observation | One sentence | 15 seconds |
Trend Tracking: After 2 weeks, you should see meal duration trending toward 15–25 min for fast eaters, or progressing toward completion within 25 min for slow eaters. If neither trend is visible by Week 3, consult your Pinnacle feeding team.
Download the E-466 Paper Tracking Sheet PDF — printable, kitchen-fridge version | Or log digitally: forms.pinnacleblooms.org/E-466-tracking

What If It Didn't Go As Planned?
Session Abandonment Is Not Failure — It's Data
My fast eater ignores the utensil rest completely
Physical prompt first — gently guide fork to rest. After 3 meals, physical prompt fades. Pair with immediate verbal praise when it happens spontaneously. This takes 1–3 weeks to become habitual.
My slow eater ignores the timer and still doesn't eat
Timer boundary is too long; reduce to 15 min. Check for sensory/texture aversion with that specific food. Consider whether appetite suppression (medication) is a factor — speak to your physician.
Child throws the pacing board
Reduce to picture strips only (just 2 pictures: bite and wait). Introduce pacing board away from mealtime first as a "game" before using at meals.
Child becomes very distressed at mealtime pacing
Reduce ALL materials to just ONE: the visual timer only. Pacing structure is the goal; specific materials are interchangeable. Consult our SLP team.
My fast eater finishes even faster WITH the divided plate
Fast eaters should receive ONE section at a time — not all sections loaded simultaneously. Serve section by section.
📞 Persistent challenges? Our feeding team is available: 9100 181 181
No Two Children Eat Identically — Personalize This
Adapt and Personalize
Child Profile | Primary Materials | Modifications | |
Fast eater, impulsive (ADHD) | Utensil rest + Pacing board + Timer | 5-sec mandatory wait between every bite | |
Fast eater, oral hyposensitive | Chew counter + Small utensils | Oral sensory warm-up before meal (OT guidance) | |
Slow eater, attention challenges | Timer + Progress chart + Conversation cards | Reduce distractions maximally; serve in sections | |
Slow eater, sensory aversion | Divided plate + Timer + preferred food sequencing | Address texture simultaneously with OT | |
Younger child (2–4 years) | Timer + Divided plate only | Shorter target duration (10–12 min) | |
Older child (8–12 years) | Timer + Progress chart + self-monitoring | Child manages own pacing board independently |
Sensory Seeker
May eat fast because they WANT more sensory input from food. Add varied textures within divided plate sections. Oral motor warm-up helps satisfy sensory need before meal begins.
Sensory Avoider
May eat slow because each bite is a sensory challenge. Reduce texture demands first; build pacing only once texture aversion is being addressed. Don't layer two challenges simultaneously.
ACT IV: THE PROGRESS ARC
Weeks 1–2: You Are Building the Scaffold — Not the Skill Yet
PROGRESS BAR: ██░░░░░░░░ 15%
✅ Signs of Early Progress — Look for THESE
- Child tolerates the visual timer being present without protest
- Child accepts the divided plate without major resistance
- Meal duration reduces by 2–4 min (fast eater) OR child reaches 50% completion more consistently (slow eater)
- Child begins to notice the pacing board ("Oh, it's the wait step")
- Fewer verbal prompts needed by Day 10 vs. Day 1
❌ What Is NOT Expected Yet
- Independent pacing without any prompting
- Consistent performance across all meals
- Generalization to grandmother's house or school
"If your child accepted the visual timer without throwing it by the end of Week 2 — that is genuine neurological progress. It means the scaffold is taking hold."
Patience Metric: The nervous system requires 10–14 days of consistent exposure before a new structure becomes "expected." You are not seeing immediate behavior change; you are wiring expectation.
Systematic review (Children, 2024): Feeding intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation. | PMC11506176
Weeks 3–4: The Neural Pathway Is Beginning to Form
PROGRESS BAR: ████░░░░░░ 40%
Child Begins to Anticipate Materials
Asks for their timer or pacing board before you bring it out. Sits down at the table with less protest. Begins to count their own chews — even without prompting.
Pace Is Measurably Improving
Fast eater: meal duration has increased by 3–6 minutes. Slow eater: consistent 60–70% plate completion within target time.
Generalization Seeds (Bonus Indicators)
Child applies "put fork down" at a meal where you forgot to set up materials. Child mentions timer or pacing board in another context ("I want to use my timer!").
"At Week 4, you may notice YOU feel more confident too. Your calm is part of the therapeutic mechanism. You are co-regulating."
If responding well — expand protocol from 1 meal/day to 2 meals/day.
Weeks 5–8: The External Scaffold Is Becoming an Internal Rhythm
PROGRESS BAR: ███████░░░ 75%🏆 MASTERY BADGE APPROACHING
Criterion | Fast Eater Mastery | Slow Eater Mastery | |
Meal duration | Consistently 15–25 min, 5/7 days | Consistent completion within 25 min, 5/7 days | |
Prompting required | Self-corrects with 0–1 verbal cues | Takes next bite within 30 sec without prompting | |
Generalization | Maintains pace at 2+ settings | Completes meals at school and home | |
Material dependence | Can pace with timer only (all other materials faded) | Needs only visual timer as backup |
🏆"Eating Pace Mastery Achieved"
Your child has internalized sufficient rhythm to pace their eating with minimal external support.
When to Move On
Mastery criteria met at home → introduce in restaurant setting (portable timer + utensil rest) → then fade completely in familiar settings.
When to Stay and Strengthen
If mastery is inconsistent across settings, stay at this level for another 4 weeks before fading materials.
Even in the Celebration Zone — Know These Signs
🚨 Red Flags: When to Pause
Red Flag | What It Looks Like | What It May Mean | |
Wet/gurgly voice after eating | Voice sounds wet or bubbly post-meal | Possible aspiration — SLP swallowing evaluation urgently | |
Consistent coughing during meals | Coughs on most bites | Swallowing incoordination — feeding specialist referral | |
No improvement after 8 weeks | Pace unchanged despite consistent protocol | Underlying oral motor or neurological factor requiring assessment | |
Weight loss or nutritional concerns | Growth faltering, visible weight drop | Medical + feeding therapy evaluation | |
New avoidance of food | Previously accepted foods now refused | Possible new sensory sensitization or medical issue | |
Severe anxiety at mealtime | Crying, vomiting, panic at every meal | Feeding anxiety requiring psychological + SLP input |
📞 Trust your instincts. If something feels wrong, call: 9100 181 181

Your Child Is On a Journey. Here Is the GPS.
The Progression Pathway
If fast eater is now paced → E-467 (Mealtime Transitions) — work on transitioning from mealtimes to next activities without conflict. If slow eater completion is improving → E-468 (Family Mealtime Participation) — integrate child into full family meal dynamics. If oral motor concerns surface → Specialized OT/SLP feeding assessment before progressing.
Long-Term Goal: A child who paces their own eating across all settings, participates in social meals with peers, and self-manages their mealtime without adult scaffolding.

ACT V: COMMUNITY AND ECOSYSTEM
From the Pinnacle Network — Real Families, Behavioral Specificity

Family Vignette 1: Arjun, Age 7 — ADHD
Before: Meals completed in under 4 minutes. Constant choking scares, food never adequately chewed. "I was terrified every dinner."
Intervention: Utensil rest + pacing board + chew counter (10 chews per bite)
After Week 6: Meal duration 18–22 minutes. Zero choking incidents. Self-initiates putting fork down without prompting most meals.
"He actually tastes his food now. He told me last week that the dal was 'really good.' He never noticed food before."

Family Vignette 2: Priya, Age 5 — ASD
Before: Meals lasting 55–70 minutes. Food always cold. Mother spending 45+ minutes in active prompting. Family mealtimes had stopped being shared.
Intervention: Visual timer (20-min boundary) + progress chart + divided plate
After Week 8: 85% of meals completed within 22 minutes. Mother sits at the table again.
"She sees the timer and she knows what we're doing. That timer is the most important ₹200 I ever spent."
"The most common mistake we see is parents trying to use verbal instruction alone — 'slow down,' 'take a bite' — without any external structural support. The child literally cannot do what you're asking without the scaffold. These materials ARE the therapy. The words are just the accompaniment." — Pinnacle SLP + OT, Bangalore Center
Vignettes are composite clinical cases. Individual results vary. Names and identifying details anonymized.
Preview of 9 materials that help with eating speed Therapy Material
Below is a visual preview of 9 materials that help with eating speed therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

ACT VI: THE CLOSE
Frequently Asked Questions
Q: My child eats fast with preferred foods but slow with non-preferred. Which protocol?
Both patterns — they reflect different underlying factors. Apply the fast-eater protocol for preferred foods; focus on texture and sensory work for non-preferred foods first. Call 9100 181 181 for a personalized feeding plan.
Q: How long until I see results?
Tolerance of materials: 1–2 weeks. Measurable pace change: 3–4 weeks. Consistent pacing with minimal prompts: 6–8 weeks. Do not abandon the protocol before Week 4.
Q: My child has ADHD medication that suppresses appetite. Does the protocol still work?
Yes, but requires adjustment. Schedule main meals when appetite is highest — typically before first dose or after second dose wears off. Speak to your prescribing physician. This doesn't change the pacing materials needed.
Q: Can I use all 9 materials simultaneously from Day 1?
No. Start with 2–3 that best match your child's primary pattern. Add one new material every 5–7 days. Overwhelming a child with 9 new mealtime objects will increase resistance, not compliance.
Q: Is there a risk of creating food anxiety by using all these structures?
Properly implemented, these materials create security and predictability — which reduces anxiety. The tone is always supportive, never coercive. Improperly implemented with pressure or punishment, any approach can increase anxiety.
Q: When can I completely stop using the materials?
When your child maintains appropriate pace across 4/5 consecutive meals without any materials, and generalizes to at least 2 settings — the scaffold has done its job. Keep materials available as backup during transitions, illness, or regression phases.
→ Didn't find your answer? Ask GPT-OS® | Book Teleconsultation: 9100 181 181
The Best Time to Start Was Yesterday. The Second Best Time Is This Meal.
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages | India's largest autism support line
The Pinnacle Promise
Pinnacle Blooms Network® exists so that every parent — regardless of where they live, what language they speak, or how much they earn — can access the same therapeutic intelligence that used to be available only inside a clinic. This page is one of 70,000+ technique pages in the Pinnacle GPT-OS® knowledge base. Your child's eating speed challenge has a name, a neuroscience, and a solution. You now have all three.
This content is educational in nature. It does not replace individualized feeding assessment and intervention with licensed feeding therapists, speech-language pathologists, or occupational therapists. Eating speed difficulties can have multiple underlying causes requiring professional evaluation. Individual results may vary.
Pinnacle Blooms Network® | Unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | GSTIN: 36AAGCB9722P1Z2 | © 2025 Pinnacle Blooms Network®. All rights reserved. | techniques.pinnacleblooms.org
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | pinnacleblooms.org