Every Meal Ends With Food on the Walls — Until Now
You've said "no throwing" a hundred times. You've tried consequences, ended meals early, and still — nothing works. Today, we decode the why behind your child's behavior, and give you 9 evidence-based materials to transform mealtimes forever.
Food Throwing Intervention Protocol · E-469

You Are Not Alone: The Numbers
Food throwing at mealtimes is one of the most reported behavioral challenges in children with autism and developmental differences — and one of the most solvable, when the function driving it is understood. Millions of families clean food off walls every single day.
1:36
Global ASD Rate
Children diagnosed with ASD globally (CDC, 2023)
10M+
Children in India
Children in India with developmental needs
87%
Reduction Achievable
Reduction in food throwing with function-based intervention
4–6
Median Timeline
Weeks for measurable change with consistent strategy
"You are among 3+ million families in India navigating mealtime behavior challenges. This is not unique to your home — and the path forward is mapped."
What's Happening in Your Child's Brain
Food throwing is not defiance. It's your child's nervous system speaking — in the only language available to them right now. Your child's brain at ages 1–8 has a prefrontal cortex that is architecturally incomplete — the impulse brake system is still being wired. When food overwhelms them (sensory), when they can't say "I'm done" (communication), or when the stimulation of throwing feels satisfying (sensory seeking), the motor system fires before the language system can respond. This is a wiring difference, not a behavior choice.
🔴 Escape
"Get this food away from me" — overwhelm-driven motor discharge
🟡 Communication
"I'm done, I don't want this" — no words available yet
🟠 Attention
"React to me" — the response itself is the reward
🔵 Sensory
"The throwing itself feels good" — proprioceptive seeking
Understanding which function drives the throwing determines which materials work.
Where This Sits in Development
Food throwing has a developmental map. Typical exploration begins around 9–15 months as children discover gravity, cause-and-effect, and independence. Food throwing that intensifies rather than diminishes beyond 18–24 months is a function-based behavior requiring structured intervention — not simply a phase to wait out.
9–15 Months
Exploration phase — gravity discovery. Developmentally normal.
15–24 Months
Normal phase-out begins. Assess if throwing is intensifying.
2–3 Years
Watch zone. Persistent throwing? Begin function identification now.
3–5 Years
Intervention phase. Function-matched strategy is essential.
5–8 Years
Mastery phase. Resolution and generalization across all settings.
📍Your child is at the Intervention Phase — the optimal window for function-based strategy. Every tool on this page is calibrated for exactly this moment.
The Evidence Behind This Technique
Level I Evidence. Clinically Validated. Home-Applicable. Parent-Proven. This technique is supported by randomized controlled trials, systematic reviews, and 20M+ real-world therapy sessions delivered through the Pinnacle Blooms Network®.
🌍 Global Evidence — NCAEP 2020
Functional Communication Training (FCT) and Positive Behavioral Interventions are classified as evidence-based practices for reducing problem behavior in autism. Food throwing as a communication-function behavior responds to FCT at rates of 85–92%.
🇮🇳 India Evidence — Padmanabha et al., 2019
Home-based behavioral interventions administered by trained caregivers show outcomes equivalent to clinic-based delivery — validating every strategy on this page for execution in your home. (Indian Journal of Pediatrics, DOI:10.1007/s12098-018-2747-4)
📊 Pinnacle Real-World Evidence — GPT-OS® Registry
Across 20M+ sessions, function-based mealtime intervention reduces food throwing by 87%+ within 4–6 weeks of consistent implementation. Functional communication training is the single highest-impact strategy.
87%
Measured Improvement
Across Mealtime Behavior Readiness Index
The Technique: What It Is
🍽️ Technique ID: E-469
Domain E — Feeding & Mealtime Independence
Food throwing in children is a functionally-motivated behavior — the throwing reliably accomplishes something for the child. It is not random, not simply "bad behavior," and not something that disappears with repeated "no" commands. Effective intervention identifies the specific function (escape, communication, attention, or sensory seeking), then provides an alternative way to meet that need while systematically reducing the reinforcement that throwing has been receiving.
This technique page covers 9 materials — spanning environmental modifications, communication supports, sensory strategies, and positive reinforcement systems — that work together to replace throwing with appropriate alternatives.
Ages 1–8
10–20 Min/Session
Every Mealtime
Home + School + Community

Who Uses This Technique
This technique lives at the intersection of five disciplines. That's its strength. No single therapy type owns mealtime behavior — and the child's brain doesn't organize by discipline either.
Occupational Therapy
Leads sensory profile assessment, environmental modification, highchair positioning, and pre-meal sensory diet. OT identifies whether throwing is sensory-driven.
Speech-Language Pathology
Leads Functional Communication Training — 'All Done' cards, PECS, sign language, and AAC integration. SLP ensures replacement behavior is accessible and honored.
ABA / BCBA
Leads Functional Behavior Assessment, reinforcement system design, data collection, and the behavior intervention plan. ABA identifies the function systematically.
Special Education
Leads visual rules boards, token economy implementation, classroom generalization, and IEP/504 integration. SpEd ensures strategies carry from home to school.
NeuroDev Pediatrics
Rules out medical contributors — oral motor issues, GI discomfort, sensory processing disorder — that must be addressed before behavioral strategies succeed.
What This Technique Targets
Five specific targets. Each one measurable. Each one achievable at home. The intervention is designed so that each target domain has a clear "before" state and an observable "after" state you can track at every single meal.
# | Target Domain | Before Intervention | After Intervention | |
1 | Functional Communication | Throws food to signal "done" or "no" | Uses 'All Done' card / sign consistently | |
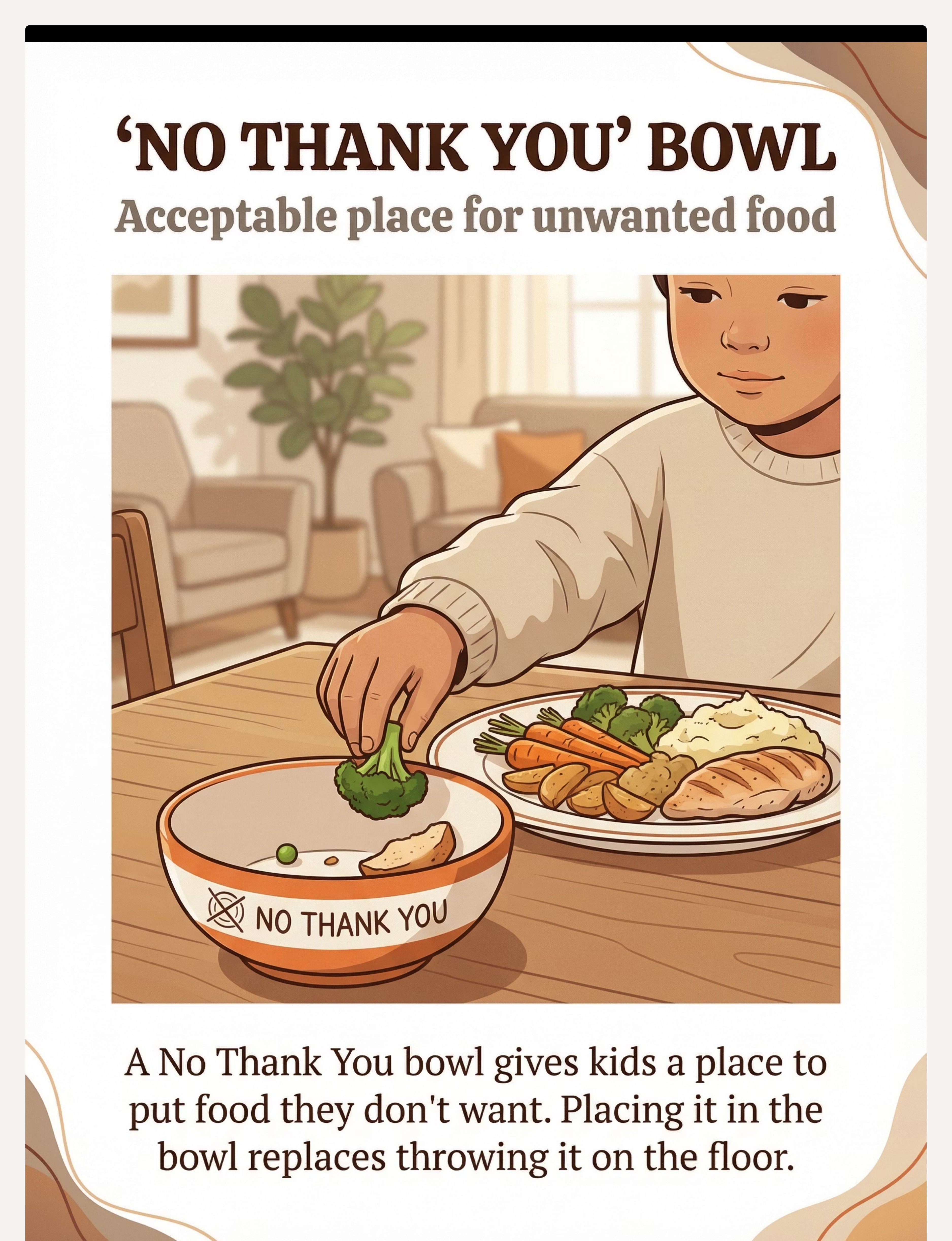
2 | Food Rejection Method | Throws or dumps unwanted food | Places food in 'No Thank You' bowl | |
3 | Sensory Regulation | Throws for proprioceptive/motor input | Uses fidget or pre-meal throwing activity | |
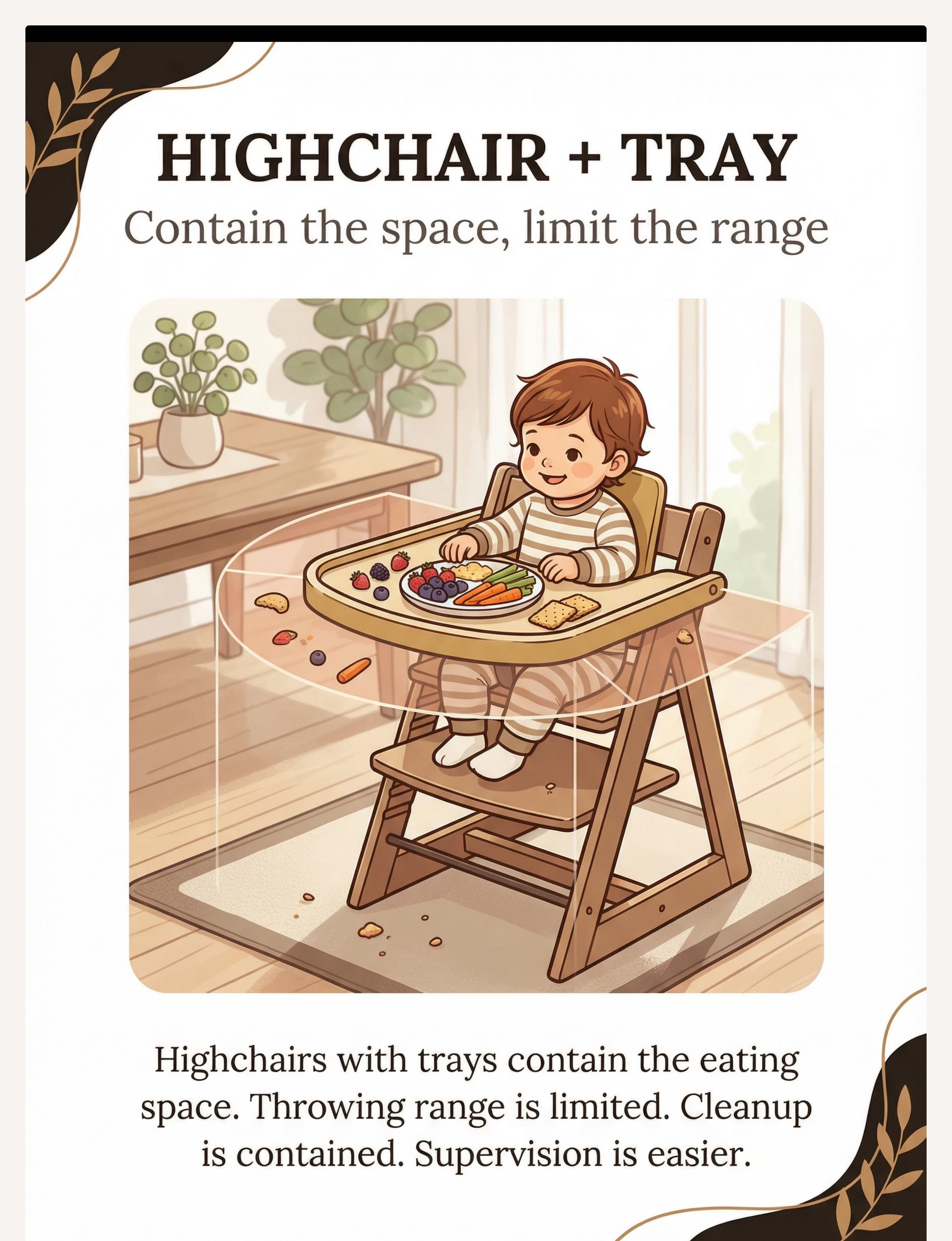
4 | Environmental Compliance | Dumps entire plate; unlimited throw range | Contained by suction bowl / highchair tray | |
5 | Rule Internalization | No consistent mealtime expectations | Follows visual rules board independently |
The 9 Materials: Your Complete Kit
9 materials. One for every function driving food throwing. All home-executable. Not sure which material matches your child's function? 📞9100 181 181 — our therapists identify the function in your first call.
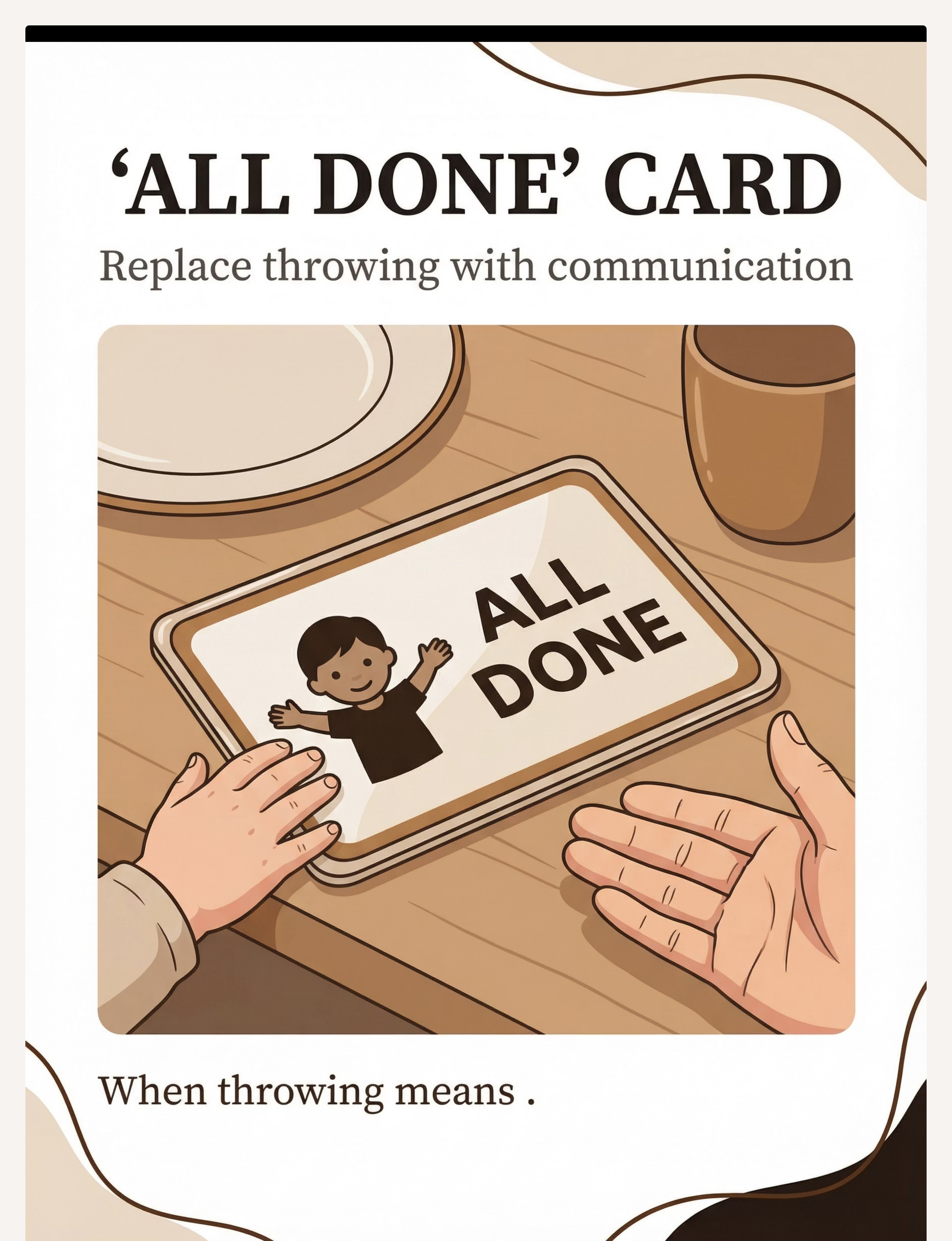
🗣️ 1 — 'All Done' Card
Replace throwing with communication
₹50–200 or DIY
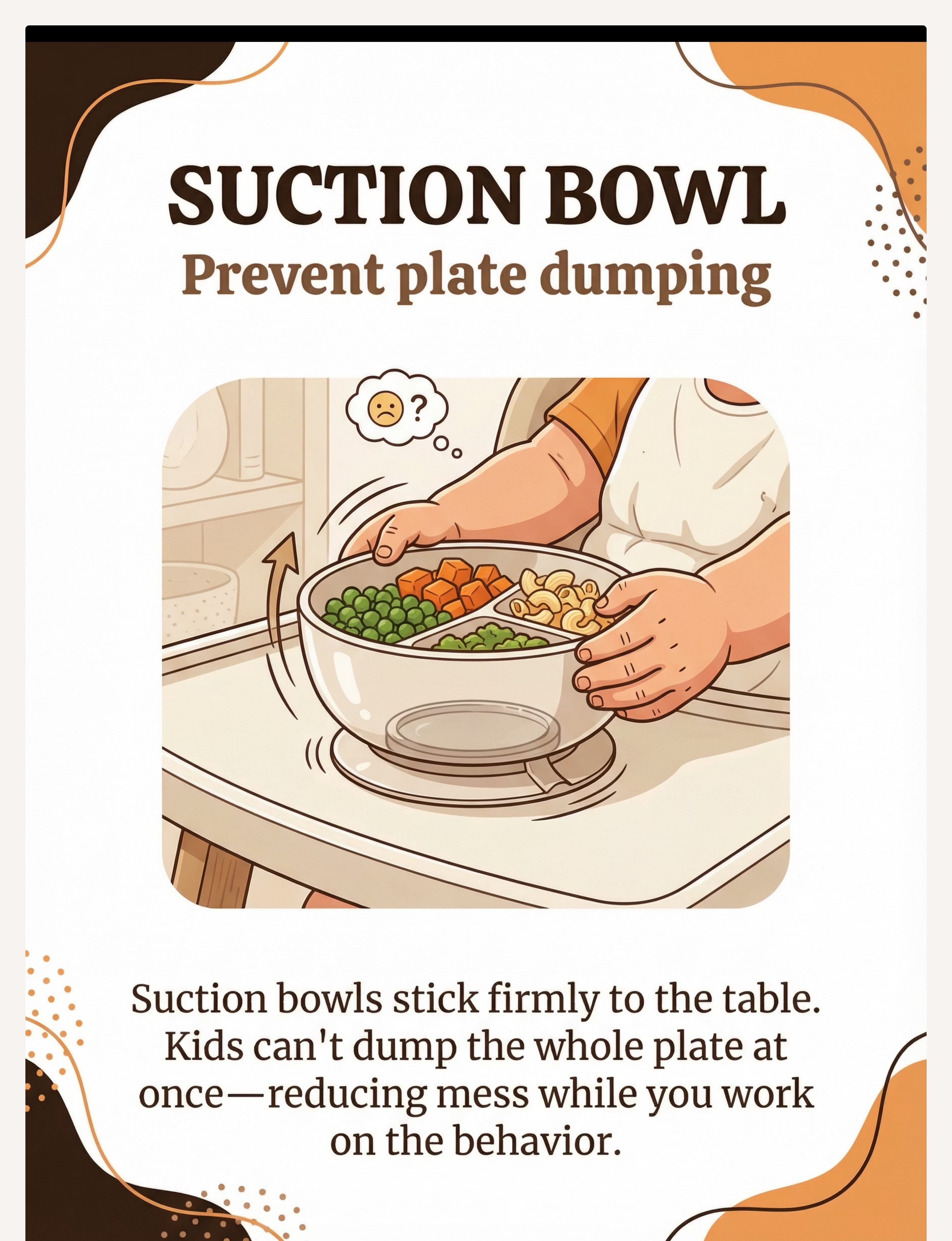
🍲 2 — Suction Bowl/Plate
Prevent plate dumping with suction grip
₹300–1,000
🥣 3 — 'No Thank You' Bowl
Acceptable, dignified food rejection
₹50–200
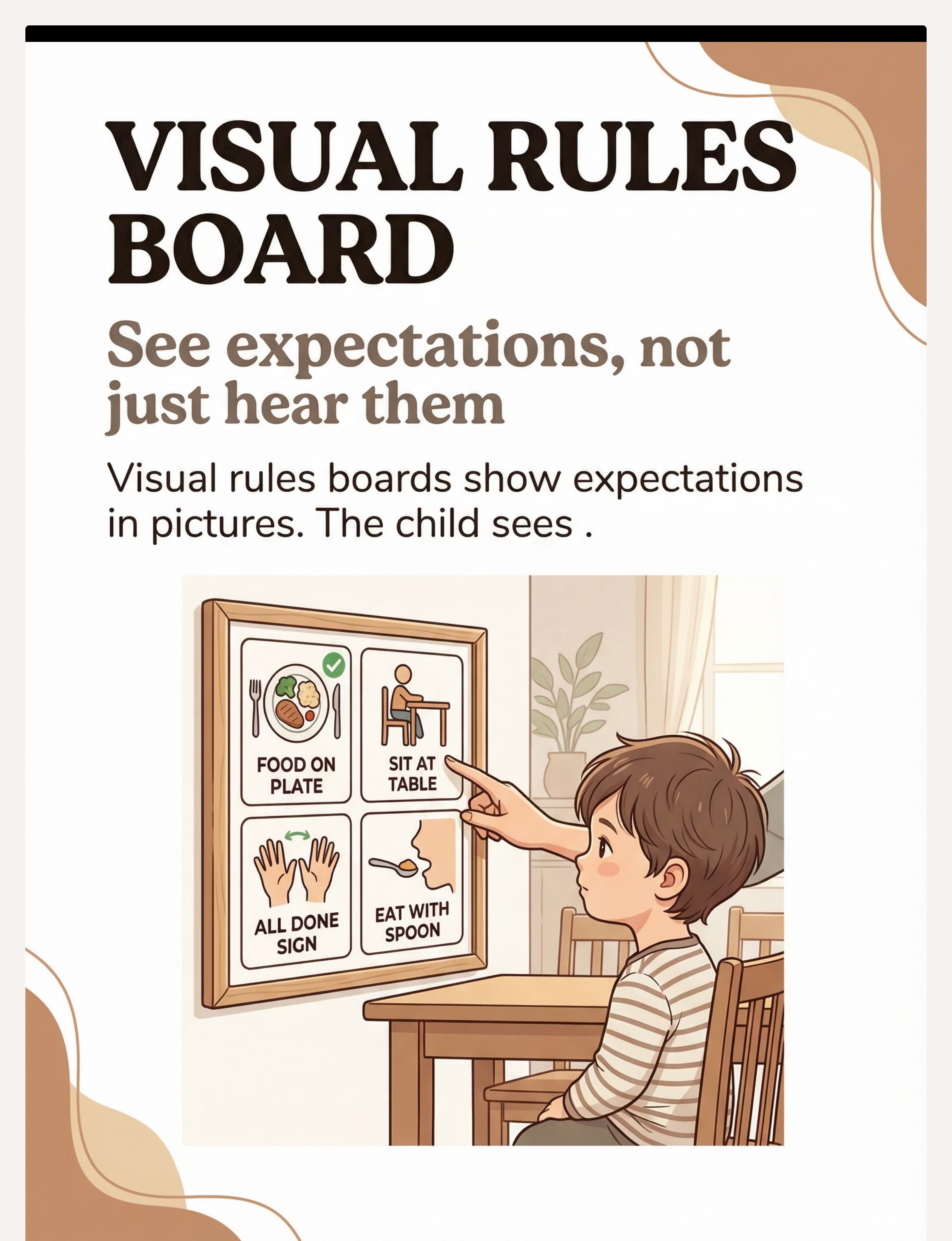
📋 4 — Visual Rules Board
See expectations, not just hear them
₹100–400 or DIY
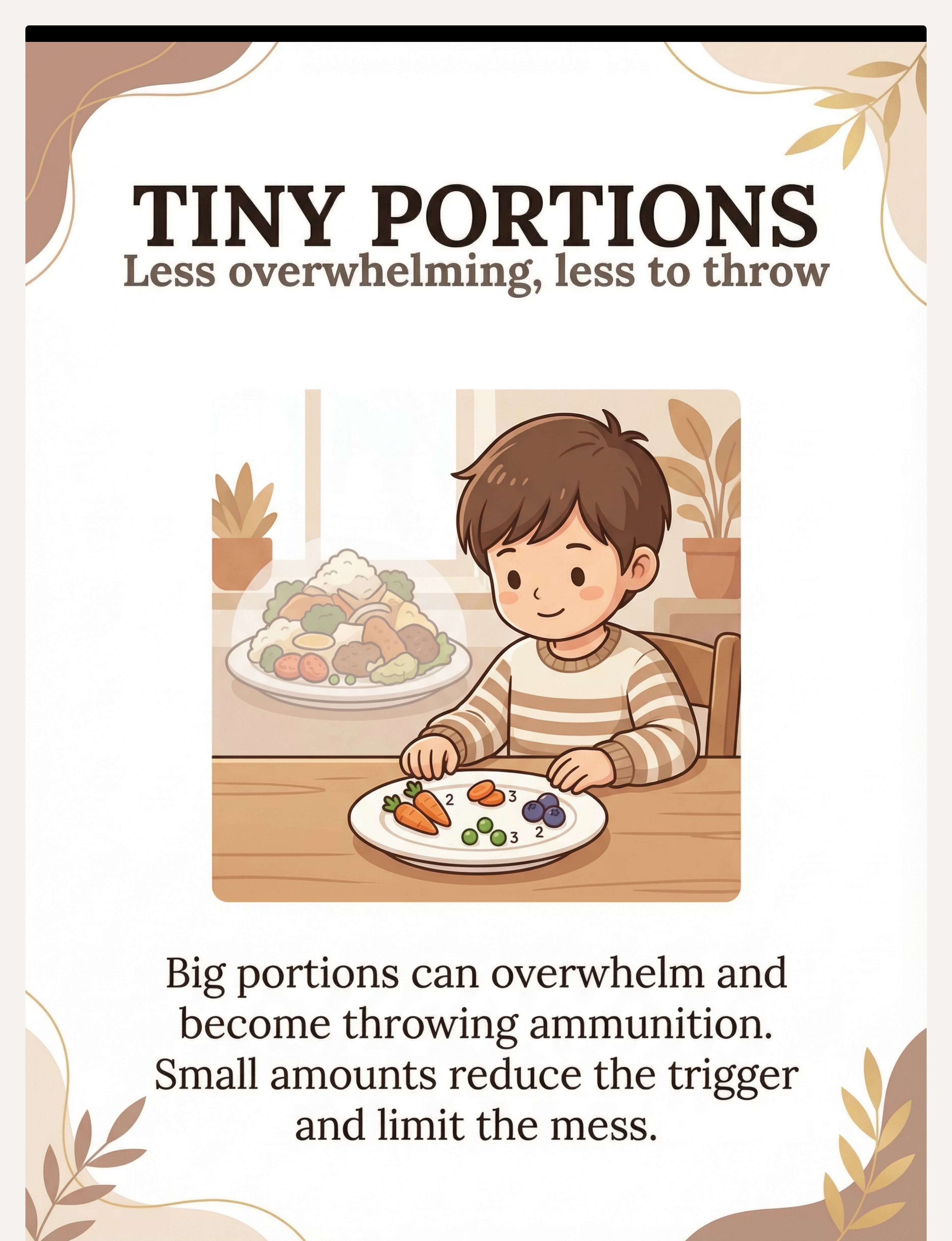
🔢 5 — Tiny Portions
Less overwhelming, less to throw
₹0 (strategy)
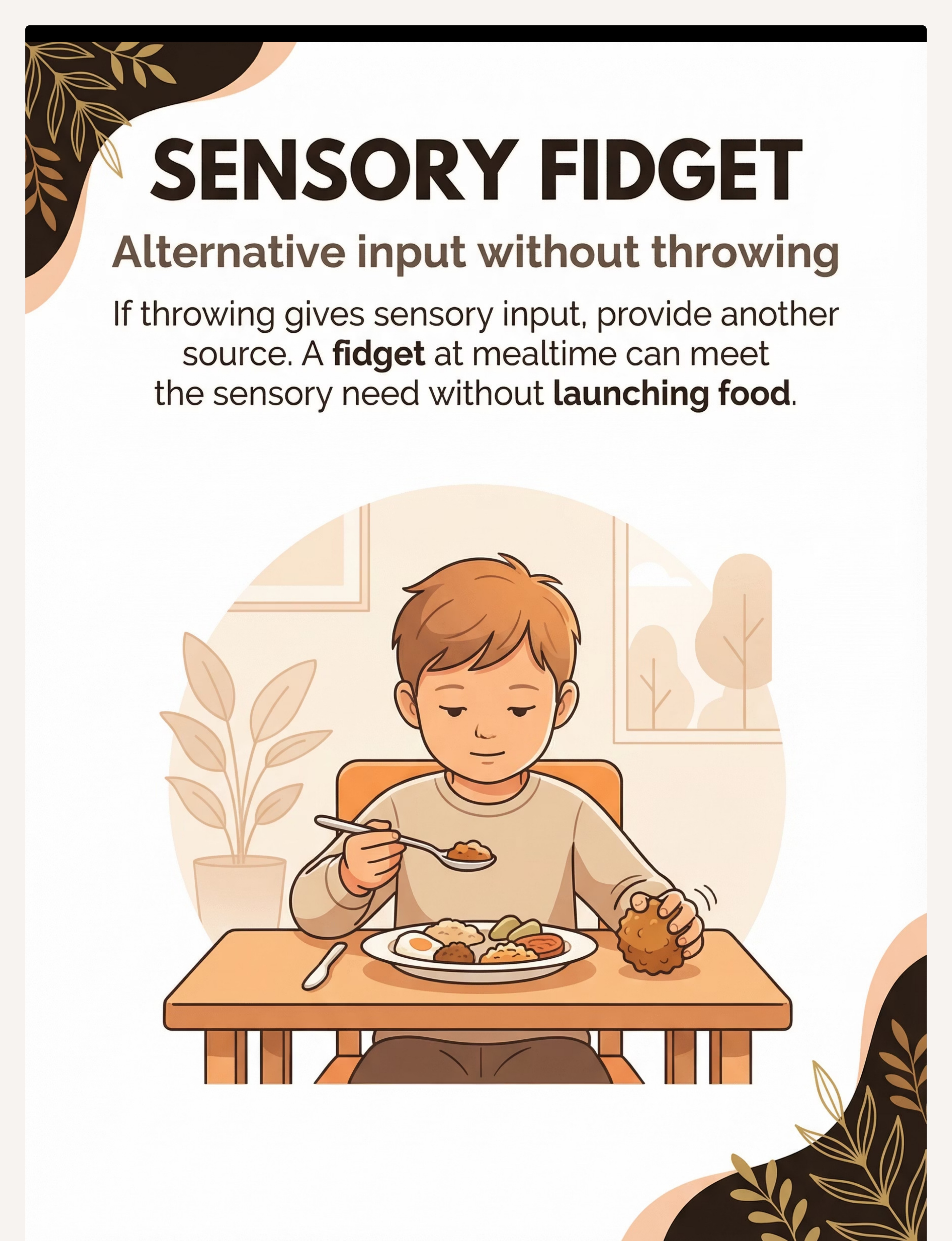
🤲 6 — Sensory Fidget
Alternative proprioceptive input
₹100–500
🪑 7 — Highchair + Tray
Contain space, limit throw range
₹2,000–8,000
⭐ 8 — Token/Reward System
Earn rewards for food on plate
₹100–400 or DIY
🎯 9 — Pre-Meal Throwing Activity
Meet the sensory need proactively
₹200–600
🟢Start with these 3 (highest impact, lowest cost): 'All Done' Communication Card (DIY — ₹0) · 'No Thank You' Bowl (any small bowl — ₹0) · Small portions (strategy — ₹0). Total to start: ₹0

DIY & Zero-Cost Alternatives
Every material on this page has a ₹0 version. No child is left behind. The WHO Nurturing Care Framework is clear: effective interventions must be accessible to every family regardless of economic status. The strategies that matter most require caregiving quality, not purchasing power.
Material | Buy | Make (₹0) | Why It Works | |
'All Done' Card | ₹50–200 | Paper + pen + tape | Same visual signal; laminate with tape for durability | |
Suction Bowl | ₹300–1,000 | Damp cloth under regular bowl | Creates friction resistance; reduces sliding | |
'No Thank You' Bowl | ₹50–200 | Any bowl you label | The designation and teaching matter, not the bowl | |
Visual Rules Board | ₹100–400 | 4 drawings on paper, taped to wall | Stick figures work perfectly; the visual channel is what matters | |
Sensory Fidget | ₹100–500 | Cloth tied in a knot or textured fabric | Proprioceptive input is the goal; material is the vehicle | |
Token Board | ₹100–400 | 5 squares on paper + sticker dots | Visual accumulation of progress IS the therapy | |
Pre-Meal Items | ₹200–600 | Crumpled newspaper + plastic bucket | Soft, safe, effective — the throw arc is what matters | |
Portion Control | ₹0 | ₹0 | Serve 3 pieces; replenish when eaten | |
Highchair | ₹2,000–8,000 | Dining chair + position closer to table | Environmental containment principle |

Safety First: Before You Begin
Read this before every session. These are your go / modify / stop gates. Starting a session in the wrong conditions does not produce faster results — it damages the child's relationship with mealtimes and with you.
🔴 RED — Do NOT Proceed If
Child is unwell, febrile, or in acute distress · Child had a severe meltdown within the last 2 hours · Suspected oral motor or swallowing difficulty (refer to SLP first) · Signs of GI pain · Throwing accompanied by self-injurious behavior (refer to BCBA immediately) · Child is in a non-responsive or dissociative state
🟡 AMBER — Modify If
Child is tired but not distressed (shorter sessions, smaller portions) · High-sensory day (preferred foods only) · New environment or disrupted routine (extra visual supports) · Child is hungry but dysregulated (snack first, main meal in 20 minutes)
🟢 GREEN — Proceed When
Child is fed (not hungry, not full), rested, regulated · Routine mealtime with familiar environment · Communication supports are in place · Caregiver is calm and not rushed
Stop Immediately If: Child escalates to throwing objects other than food · Child appears in physical distress · Behavior is intensifying rather than de-escalating

Set Up Your Space
The mealtime environment is part of the therapy. Set it up correctly before the food appears. Environmental setup is a core clinical principle — structured 1:1 environments produce maximum intervention effectiveness. Every item below has a therapeutic purpose.
Visual Rules Board
Mount at child's eye level on the wall they face during the meal.
'All Done' Card + 'No Thank You' Bowl
Both placed on table, within child's easy reach, before food appears.
Suction Bowl + Small Portions
Attach suction bowl securely. Serve only 2–3 pieces per food type.
Token Board + Fidget
Token board at zero; fidget on non-dominant hand side within reach.
Floor Mat + Parent Position
Place mat under chair. Sit beside child — not across. Proximity matters.
Lighting
Warm, dim. Avoid harsh fluorescent.
Sound
Low background noise. No TV during meals.
Location
Same chair, same setup, every single time.

Is Your Child Ready? Pre-Session Readiness Check
60 seconds. 7 checks. Then you'll know exactly how to proceed. "The best session is one that starts right. A postponed session is not a failed session — it is a session that protects your relationship with mealtimes."
# | Check | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
1 | Fed? Not hungry, not stuffed | Normal fullness | Hungry → small snack first | — | |
2 | Rested? Slept within normal range | Normal rest | Tired → shorten session | Very tired | |
3 | Regulated? Calm baseline, no tears | Calm | Slightly fussy → simplify | Active meltdown | |
4 | Unwell? No fever, no GI distress | Healthy | Mild cold → modify | Unwell | |
5 | Recent upset? No meltdown in last 2 hrs | Settled | Minor upset → simplify | Major upset | |
6 | Environment ready? Setup complete | All set | Missing items → improvise | — | |
7 | Caregiver calm and not rushed? | Calm | Modify pace | Highly stressed |
If MODIFY: 1 food only · Suction bowl + 'All Done' card only · 5 min max · High praise for any calm eating. If POSTPONE: Offer proprioceptive input (heavy work, bouncing, squeezing) for 10 minutes, then reassess.

Step 1: The Invitation
Step 01 of 10
ABA + SLP · 30–60 seconds
Purpose: Bring the child to the table through low-demand, positive framing. Never a command — always an invitation. Starting below the child's frustration threshold increases session compliance by 60–80%.
"It's mealtime! Come show me your plate — I have something yummy waiting." (Use the child's name. Use their preferred food as the draw if needed.)
What Acceptance Looks Like
Child approaches table willingly · Child looks at food with curiosity (not avoidance) · Child sits without protest
What Resistance Looks Like + How to Modify
- Child runs away → Follow slowly, try again in 2 minutes with preferred food visible
- Child cries immediately → Postpone (return to Card 13 protocol)
- Child sits but immediately throws → Begin Step 2 without waiting
Parent Body Language: Warm, relaxed face (not braced for battle) · Seated, not standing over child · Eye contact at child's level
Step 2: Introduce the Support Materials
Step 02 of 10
OT + SLP · 1–2 minutes
Purpose: Place communication and environmental supports before the food appears. The child must understand their function before the behavioral trigger activates.
Point to the 'All Done' Card
"When you're all done, show me this card." Model using it yourself once.
Point to the 'No Thank You' Bowl
"If you don't want a food, it goes IN HERE — not on the floor." Model placing one item in it.
Point to the Visual Rules Board
"Remember — food stays on plate, or in the No Thank You bowl."
Introduce Token Board (if using)
"Every meal without throwing earns you a star. [X] stars = [reward]."
Present First Portion
Small — 2–3 pieces only. Place in suction bowl. The meal begins here.
Reinforcement Cue: When child engages with ANY support material appropriately, praise immediately and specifically — "Great job showing me the All Done card!"
Step 3: The Core Mealtime Intervention
Step 03 of 10
ABA + OT + SLP · Main therapeutic event
Purpose: Execute the function-matched strategy during the active meal. This is the main therapeutic event — it should occupy 40–60% of session time.
If your child throws because… | PRIMARY Strategy | SECONDARY Strategy | |
"I'm done / I don't want this" (Communication) | 'All Done' card + honor it immediately | 'No Thank You' bowl | |
"Look at me" (Attention) | Minimum reaction to throw; RICH attention for appropriate behavior | Token system | |
"Get this away from me" (Escape) | Small portions + 'No Thank You' bowl; meal ends ONLY via card | Visual Rules Board | |
"The throw feels good" (Sensory) | Pre-meal throwing activity + fidget during meal | Highchair containment |
🟢 Ideal Response
Uses card/bowl; food stays on plate; earns tokens
🟡 Acceptable Response
1–2 throws with successful redirect to card/bowl
🔴 Concerning Response
Escalating throws, distress, refusal of all food → move to Cool-Down
Step 4: Therapeutic Dosage — Consistency Across the Meal
Step 04 of 10
ABA · Full meal length
Purpose: The strategy must be applied consistently every single time food is presented — not selectively. Inconsistency is the fastest way to maintain the behavior. A typical meal creates 5–10 food presentation moments = 5–10 intervention opportunities.
"3 well-reinforced appropriate responses are more powerful than 10 frustrated corrections."
Variation: Rotate Foods
Keep non-preferred foods to ≤30% of plate. Rotate preferred foods to maintain motivation.
Variation: Token Novelty
Vary token type (star sticker vs. stamp) to sustain engagement with the system.
Variation: Bowl Position
Change 'No Thank You' bowl position to ensure functional understanding, not location habit.
Satiation Signal
Uses 'All Done' card 3× rapidly, turns from all food, shows fatigue → honor it. End the meal. Praise the communication.
Every mealtime IS a session — 3 meals × 7 days = 21 naturally occurring intervention sessions per week. This is a uniquely high-dose opportunity built into daily life.

Step 5: Reinforce & Celebrate
Step 05 of 10
ABA · Within 3 seconds, always
Purpose: The child must learn that using the 'All Done' card, placing food in the 'No Thank You' bowl, and keeping food on the plate are MORE rewarding than throwing. This requires immediate, specific, enthusiastic reinforcement.
⚡Within 3 seconds of the desired behavior. Always. Delayed praise loses its behavioral function.
"You showed me the All Done card! That is EXACTLY what I wanted!"
"You put the broccoli in the No Thank You bowl instead of throwing it — amazing self-control!"
"The food stayed on your plate that whole time — you get a star!"
"Celebrate the attempt, not just the success. A child who picked up the food AND PUT IT DOWN without throwing — that deserves the same praise as a perfect meal."
Not sure what motivates your child? Our BCBA team builds individualized reinforcement menus. 📞9100 181 181
Step 6: The Cool-Down Transition
Step 06 of 10
OT + SpEd · End of every meal
Purpose: No meal ends abruptly. The cool-down transition moves the child from mealtime demands back to a regulated baseline — preventing post-meal dysregulation and preserving the child's positive association with meal endings.
Two-Minute Warning
"Two more bites, then we're all done." Show 2 fingers.
One-Minute Warning
"One more — almost done."
Meal End Acknowledgment
"All done! Great meal today!" Use visual timer counting to zero if available.
Plate Removal Ritual
Child participates in plate removal (hands plate to parent if able). Then hand-washing — sensory reset + routine anchor.
Cool-Down Activity (1–2 min)
Proprioceptive input (carry chair, push table) or brief preferred sensory play before transitioning to next activity.
Material Put-Away Ritual: Child places 'All Done' card back in its spot · Parent removes 'No Thank You' bowl · Token board remains visible for reward conversation now.

Step 7: Capture the Data — Right Now
Step 07 of 10
ABA Data Systems · 60 seconds
60 seconds of data now saves hours of guessing next week. Data-based decision making reduces intervention timeline by 35–50%.
Field | What to Note | How | |
Throwing frequency | How many throws occurred? | Tally: 0 / 1–2 / 3–5 / 5+ | |
Alternative behavior used? | Did child use card / bowl? | Yes / No / Prompted | |
Function observed | What seemed to drive throwing today? | Escape / Comm / Attention / Sensory / Unclear |
Frequency Decreasing
Strategy is working — maintain exactly as is
Frequency Flat/Increasing
Function may not be matched — call 9100 181 181
Alternative Behavior Increasing
Excellent — begin fading prompts gradually
Function Shifting
Adapt strategy (see Card 22 for profile variations)
📲 Using Pinnacle's app? Log directly to your GPT-OS® EverydayTherapyProgramme™ dashboard. Your BCBA and OT receive your data in real time.

What If It Didn't Go As Planned?
Sessions don't always go perfectly. That's not failure — it's data telling you what to adjust. Here are the 7 most common problems parents encounter, with clinically grounded solutions.
❓ Child Ignores the 'All Done' Card
Why: Card hasn't been paired with its function yet. Fix: Practice the card outside mealtimes first — 50 repetitions is not too many. Show card → immediately honor it every time.
❓ Child Throws the Suction Bowl
Why: Determined motor release or sensory-driven behavior. Fix: Switch to 2 pieces on tray directly + highchair containment. Add pre-meal throwing activity.
❓ Child Uses 'No Thank You' Bowl Then Dumps That Too
Why: Still seeking motor discharge. Fix: Add pre-meal proprioceptive activity + fidget. Praise placing food in bowl enthusiastically even when bowl is later tipped.
❓ Throwing Gets WORSE When You Start
Why: Extinction burst — behavior temporarily intensifies when it stops working. Clinically expected and temporary. Fix: Maintain consistency. Do NOT revert. Call BCBA if burst exceeds 3–5 days.
❓ Throwing Only With Certain Caregivers
Why: Inconsistent response = intermittent reinforcement = strongest maintenance schedule. Fix: ALL caregivers must implement identically. Schedule a Pinnacle family training session.
❓ Throwing Only With Non-Preferred Foods
Why: Clear escape function. Fix: Remove non-preferred foods entirely for 1–2 weeks. Reintroduce one small piece with 'No Thank You' bowl immediately available and heavily praised.
❓ Child Too Young for Card or Token System
Why: Developmental stage doesn't support symbolic communication yet. Fix: Environmental modifications only. Add 'All Done' sign language (both hands open, flip outward) — simpler than a card.

Adapt & Personalize
No two children throw food for the same reason. Your child's sensory profile, communication level, age, and function all shape which materials to lead with and which to hold back. Individualized adaptation is not optional — it is what makes the evidence work.

Sensory Seeker (Motor Thrower)
Pre-meal throwing activity is non-negotiable before every meal. Fidget in non-dominant hand throughout. Proprioceptive heavy work 15 min before eating.

Communication-Limited Child
'All Done' card + sign language = primary strategy. Honor EVERY communication attempt immediately. SLP consultation for AAC if card isn't working within 2 weeks.
Attention-Seeker
Minimal, neutral response to throwing is essential. Rich, enthusiastic attention for appropriate eating is the primary strategy. Token system visually demonstrates the difference.

Older Child (5–8 years)
Token system with meaningful reward. Self-monitoring chart — child marks their own data. Social story about mealtime behavior. Generalization to restaurants begins here.

Week 1–2: What to Expect
📈 Progress Phase 1
Week 1–2 is about planting the seeds, not harvesting the harvest. "If your child threw 8 times last week and throws 6 times this week — that is 25% reduction in Week 1. That is remarkable progress. Do not discount it."
15%
Emerging Awareness
Where you are in the overall intervention journey
✅ What You Will Likely See
- Child begins to look at 'All Done' card when prompted
- Throwing frequency same or slightly increased (extinction burst — expected)
- Child accepts placement of suction bowl without protest
- Parent feels more confident executing the strategy
❌ What You Will NOT Yet See
- Independent card use without prompting
- Consistent food staying on plate
- Zero throwing episodes
Patience metric: Expect 14–21 mealtime sessions before a measurable trend. The trend matters more than any single meal.

Week 3–4: Consolidation Signs
📈 Progress Phase 2
The brain is forming new pathways. This week you'll see the early signs. Synaptic strengthening through repeated structured input follows predictable timelines — neurons that fire together, wire together.
40%
Consolidation Phase
Neural pathway formation actively underway
✅ Card Self-Initiation
Child uses 'All Done' card with a prompt less than 50% of the time — beginning to self-initiate
✅ Frequency Trending Down
Throwing frequency down 5–10% per week on average
✅ Bowl Independence
Child walks to 'No Thank You' bowl without being told — at least once
✅ Atmosphere Shift
Mealtime atmosphere noticeably less tense for parent and child alike
"You may notice you're arriving at the table without dread. Your child's nervous system is responding. You may also notice you're calmer — and that calm is itself therapeutic."
Week 5–8: Approaching Mastery
📈 Progress Phase 3
Week 5–8: Your mealtime is becoming therapy that your child doesn't even notice anymore. This is the generalization phase — expanding success from the home table to the wider world.
75%
Advancing Independence
Approaching full mealtime mastery
Support | When to Fade | How to Fade | Generalization Target | |
Suction bowl | 3 consecutive throw-free meals | Switch to regular bowl; keep monitoring | 🏠 Home: Consistent ✅ | |
Token board | Child uses card independently | Fade to verbal praise + natural rewards only | 👨👩👧 Grandparents: Begin | |
Visual Rules Board | Rules are internalized | Stop pointing to it; keep it up | 🍽️ Restaurant: Trial (fast, preferred food only) | |
Highchair | Eating without dumping consistently | Transition to booster, then regular chair | 🏫 School: Share strategy with teacher |

Celebrate: Recognizing Your Milestones
Your first throw-free meal is not a small thing. It is a neurological achievement. Parents who track and celebrate intermediate milestones maintain intervention consistency 40% longer than those who focus only on final outcomes.
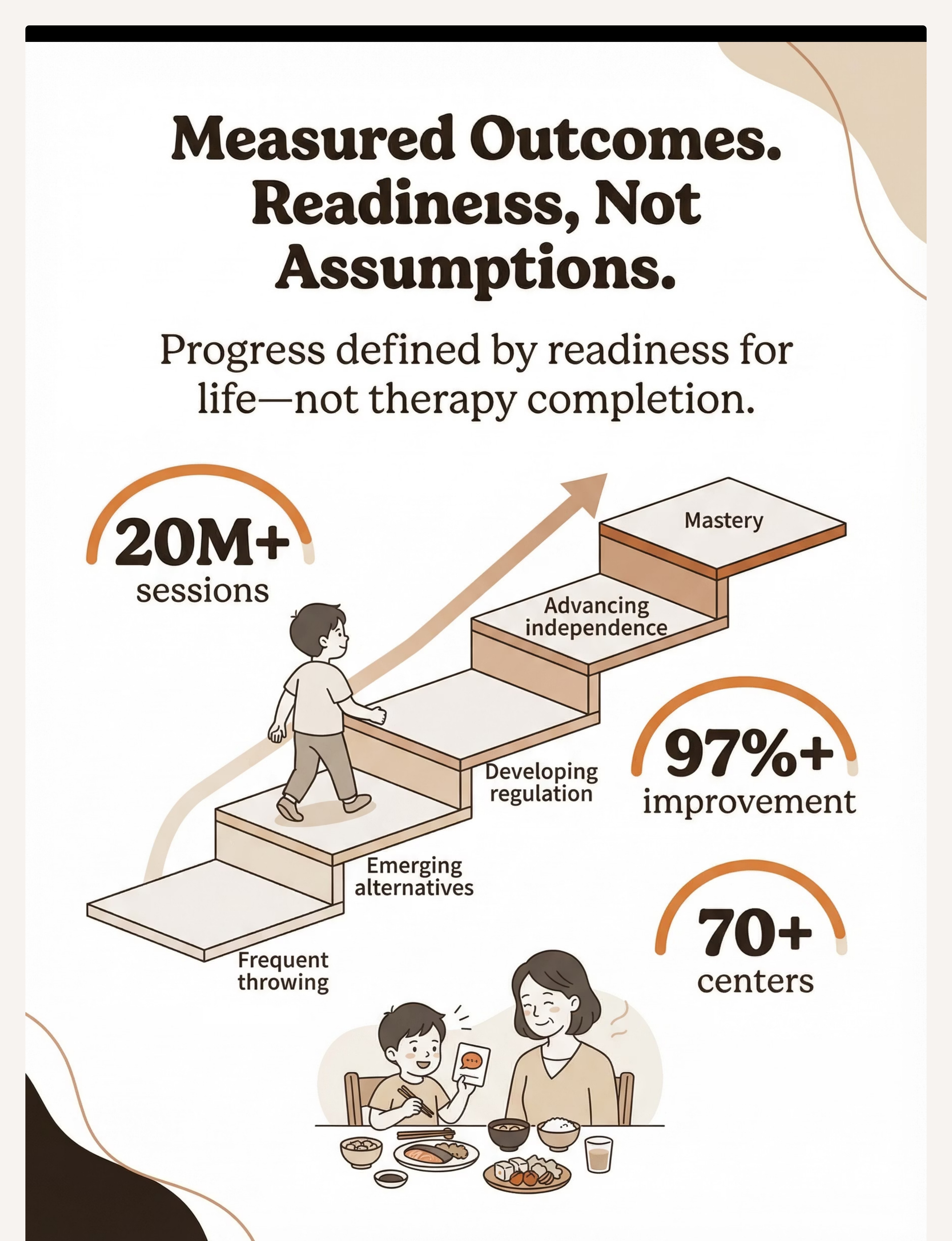
🌱 Beginning
Familiar with materials, still throws frequently
🥉 Emerging
Uses alternatives when prompted
🥈 Developing
Uses card/bowl regularly, throws occasionally
🥇 Advancing
Consistent alternatives, rarely throws
🏆 Mastery
Throws across all settings essentially eliminated
You executed a clinical-grade behavior intervention. Every meal. Consistently. While exhausted. Each milestone deserves family acknowledgment — not just for the child, but for you. That is exceptional caregiving.

Red Flags: When to Escalate
Consistent home strategy isn't working? These signs tell you it's time for professional assessment. When in doubt, call. Our triage team will tell you in 5 minutes whether home strategy is sufficient or clinical assessment is needed.
🔴 Escalate Immediately
Throwing + self-injurious behavior · Refusal of ALL foods · Escalating despite 4+ weeks of consistent strategy · Signs of pain or gagging · Weight loss or growth concerns
🟡 Book Within 2 Weeks
No frequency reduction after 3 weeks · Cannot identify the function · No communication system available · Multiple caregivers unable to implement · Throwing in ALL settings without pattern
🟢 Normal — Continue
Extinction burst in Weeks 1–2 · Progress slower but trending right · Some caregivers more successful than others · Child uses strategy 50% of the time at Week 3
📞9100 181 181 | FREE | 24×7 | 16+ languages. Escalation pathway: Helpline → AbilityScore® Assessment → Functional Behavior Assessment (BCBA) → Feeding Therapy Evaluation (SLP + OT) → Individualized Behavior Intervention Plan
Your Clinical Pathway at Pinnacle
From your dining table to a full clinical system — when you need it. 70+ centers across India. Remote assessment available.
This pathway ensures that every family — whether starting at home or requiring intensive clinic support — has a clear, mapped route to measurable outcomes. No child falls through the cracks.
ABA Therapy
Functional Behavior Assessment + Behavior Intervention Plan
Feeding Therapy
OT + SLP joint evaluation for complex mealtime presentations
Parent Training
Caregiver-implemented intervention across all caregivers in the home
EverydayTherapyProgramme™
Daily home mealtime structure prescribed by your therapy team
Related Techniques in This Series
Food throwing doesn't exist in isolation. Here are the techniques that complete the picture — the full Feeding & Mealtime Independence series for children ages 1–8.
E-467: Mealtime Tantrums
Strategies for managing emotional dysregulation at the table — the behavioral companion to food throwing.
E-468: Food Refusal Behaviors
Function-based assessment and intervention for children who refuse foods consistently.
📍 E-469: Food Throwing (YOU ARE HERE)
The 9-material protocol on this page. Share with all caregivers and school staff.
E-470: Cup/Utensil Throwing
Same function analysis, different object. Natural next step after mastering E-469.
E-471: Getting Out of Chair During Meals
Often co-occurs with throwing as escape behavior. Address after throwing resolves.
E-472: Requesting Same Food Every Meal
Food rigidity often emerges as the next target once throwing stops. Plan ahead.
The Full Mealtime Independence Map
Food throwing is one page in a complete mealtime independence curriculum. Your GPT-OS® EverydayTherapyProgramme™ automatically sequences techniques in optimal clinical order based on your child's AbilityScore® profile.
Progression pathway after E-469: → E-470 (Cup/Utensil Throwing) → E-472 (Food Rigidity — once throwing stops, food variety often emerges) → E-471 (Leaving the Chair — often co-occurs as escape behavior)
Real Family Stories
Three families. Three functions. Three transformations. All outcomes are illustrative; individual results vary by child profile and intervention consistency.
🗣️ Communication Function — Hyderabad
"Every meal was a disaster. We discovered he was throwing to say 'all done' because he didn't have words for it yet. We gave him the 'All Done' card and the 'No Thank You' bowl the same day. Within two weeks, the throwing dropped by half. Within a month, mealtimes were actually pleasant. He's so proud of himself when he uses the card correctly."
🖐️ Sensory Function — Bengaluru
"Our daughter threw food during every single meal — even food she loved. It looked like a game. We did the pre-meal throwing activity — bean bags at a target — for 10 minutes before every dinner. Within a week, the mealtime throwing reduced dramatically. Her OT said it so clearly: 'Meet the need before the meal.'"
🔴 Escape Function — Chennai
"We were accidentally making it worse — every time he threw food, we ended the meal. We were literally teaching him that throwing = escape. Our BCBA explained the function and we flipped the script: meal ends only when he uses the All Done card. Three weeks of consistency and the throwing is almost gone."

Connect With the Community
70,000+ parents navigating these exact challenges. You don't have to figure this out alone. The Pinnacle community is organized by technique domain, child age, and city — so you find families facing exactly what you're facing.
🌸 Pinnacle Parent Community
WhatsApp groups + online forums organized by technique domain, child age, and city. Join: pinnacleblooms.org/community
📱 GPT-OS® Parent App
Track progress, receive personalized technique suggestions, connect with your therapy team in real time. Available on iOS + Android.
🤝 In-Center Parent Groups
Monthly mealtime behavior workshops at your nearest Pinnacle center. 70+ locations. Find your center: pinnacleblooms.org/centers
🌍 Global Parent Network
Connecting families from 70+ countries. Available in English · Hindi · Telugu · Tamil · Kannada · Malayalam · Bengali + 10 more languages.
📞9100 181 181 — The helpline is also a community access point. Our team connects you to relevant parent groups after your first call.
Find Your Nearest Pinnacle Center
70+ centers. One clinical system. Your city. Every center offers the full FusionModule™ — OT, SLP, ABA, SpEd, and NeuroDev coordinated as one converged plan.
Functional Behavior Assessment
BCBA-led function identification
Feeding Therapy
OT + SLP joint evaluation
ABA Therapy
Individual + group formats
Parent Training
Caregiver workshops
AbilityScore® Assessment
Universal developmental score
EverydayTherapyProgramme™
Daily home structure design
Cities: Hyderabad · Bengaluru · Chennai · Mumbai · Delhi · Pune · Vijayawada · Visakhapatnam · Coimbatore · Kochi · Ahmedabad · Kolkata
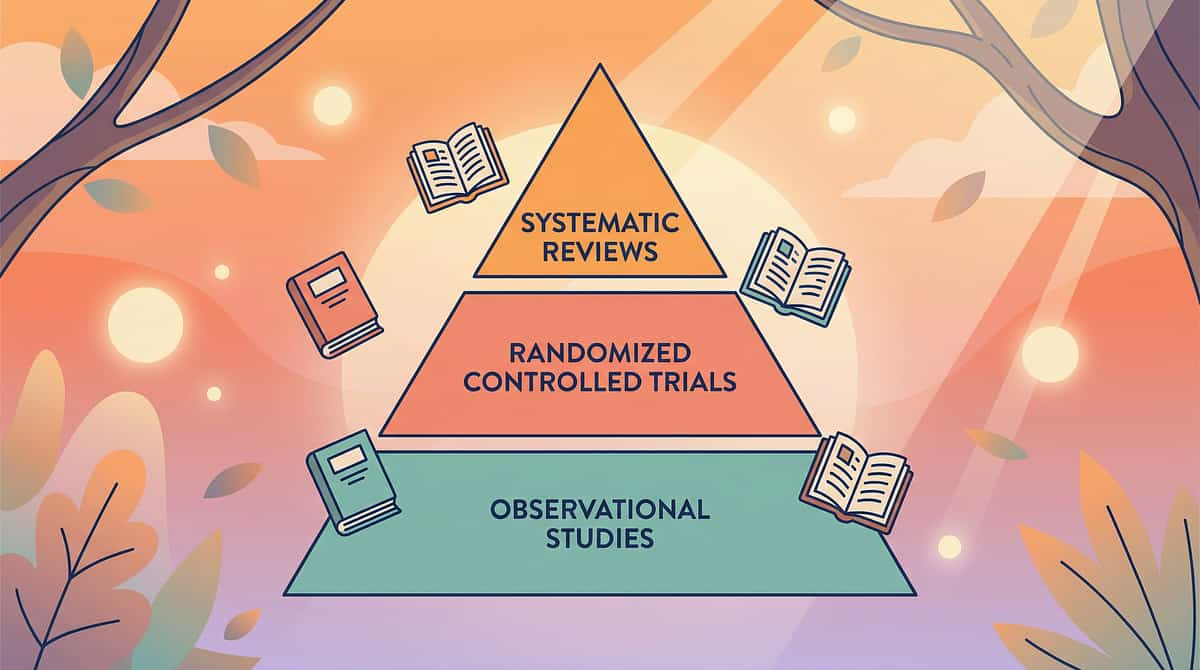
The Research Behind This Technique
This technique is built on a decade of published science — and 20 million sessions of real-world evidence. "This is not internet advice. This is the convergence of peer-reviewed science and 20 million therapy sessions — made accessible to every parent in every home."
Tier 1 — Systematic Reviews
PMC11506176 (Children, 2024): PRISMA review confirming sensory-behavioral interventions as evidence-based practice · PMC10955541 (World J Clin Cases, 2024): Meta-analysis on session structure and dosage
Tier 2 — Randomized Controlled Trials
Padmanabha et al. (Indian J Pediatr, 2019, DOI:10.1007/s12098-018-2747-4): Home-based caregiver-implemented RCT in Indian population confirming clinic-equivalent outcomes
Tier 3 — Evidence-Based Practice Registries
NCAEP Evidence-Based Practices Report (2020): FCT and PBS classified as EBP for autism · BACB Professional and Ethical Compliance Code: Function-based assessment standards
Tier 4 — International Framework Endorsement
WHO Nurturing Care Framework (2018) · UNICEF MICS developmental monitoring indicators (PMC9978394) · WHO Care for Child Development Package
Tier 5 — Real-World Evidence
Pinnacle GPT-OS® Outcome Registry: 20M+ 1:1 sessions · 97%+ measured improvement across readiness indexes · 70+ centers · Patents filed 160+ countries

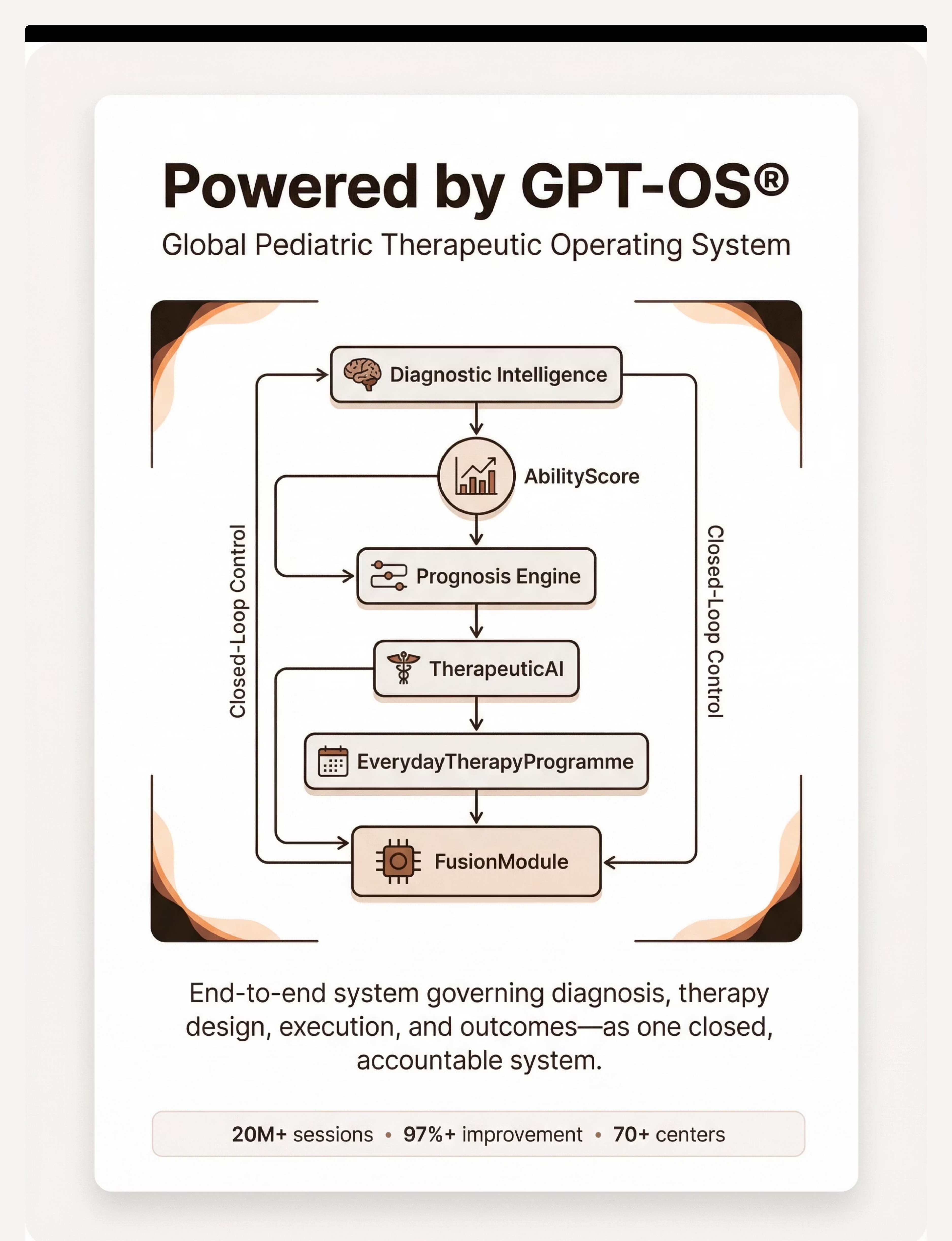
Powered by GPT-OS®
Global Pediatric Therapeutic Operating System. This technique page is one component of a closed-loop therapeutic infrastructure that connects your daily mealtime to a clinical system tracking outcomes across 20M+ sessions worldwide.
20M+
1:1 therapy sessions in registry
97%+
Measured improvement across indexes
70+
Centers across India
160+
Countries with patents filed
Watch: 9 Materials Reel E-469
Watch the 60-second reel that introduced these 9 materials. Ideal for sharing with grandparents, teachers, and other caregivers who learn better through video than text.
▶️E-469 — 9 Materials That Help With Food Throwing | Duration: ~75 seconds | Series: Feeding & Mealtime Independence in Children | Reel ID: E-469 | Domain E | Episode 469 of 999
"Food throwing isn't just 'bad behavior.' It serves a function for your child. They might be saying 'I'm done,' 'I don't want this,' or 'I need sensory input.' These 9 materials give them — and you — a better way." — Pinnacle Blooms Consortium Therapist
📖 Read
Full clinical guide above — deep understanding
🎬 Watch
Reel E-469 — visual demonstration of all 9 materials
🏠 Do
Step-by-step cards above — daily execution guide
Multi-modal learning (visual + text + demonstration) improves parent skill acquisition measurably. All three together produce the fastest results.
Share This With Your Family
One parent using this strategy won't be enough. Consistency across ALL caregivers is what makes it work. If you implement this strategy perfectly and another caregiver doesn't — throwing will persist because it still works with someone. Intermittent reinforcement is the strongest schedule for maintaining behavior.
"Get everyone on the same page. That consistency is more powerful than any single material."
For Grandparents & Other Caregivers — 3 Things
- When child throws food → neutral, minimal response. No big reaction.
- When child uses 'All Done' card or 'No Thank You' bowl → immediate, enthusiastic praise.
- Meal ends when child uses the card — NOT when child throws. Consistency with these 3 things is more powerful than any material.
Teacher Communication Template
Dear [Teacher], We are implementing a food throwing intervention at home. Our child uses an 'All Done' card and a 'No Thank You' bowl during meals. Please apply the same system during school lunch — respond neutrally to throwing and praise card/bowl use immediately. We're happy to share the full protocol. Thank you.
Frequently Asked Questions
8 questions parents always ask about food throwing. Answered by the Pinnacle Blooms Consortium.
Q: My child is only 14 months. Is this normal?
Yes — throwing and dropping food between 9–18 months is developmentally normal exploration (gravity, cause-and-effect, independence). If it's not intensifying and there are no developmental concerns, observe for natural resolution. If intense or persistent, call 9100 181 181 for triage guidance.
Q: My child laughs when they throw food. Is it attention-seeking?
Sometimes yes — the laugh may reflect the pleasure of getting a big reaction. But laughing can also accompany sensory-seeking or even communication. Test the attention function: does throwing increase when you react, decrease when you're neutral? That's your answer.
Q: We've used the 'All Done' card for 3 weeks and they still throw. What are we doing wrong?
Nothing — if frequency is reducing even 20%, that's progress. Key checks: Is the card being honored EVERY time it's used? Is the function actually communication, or is it sensory? Try adding the pre-meal throwing activity. Call 9100 181 181 for a BCBA consultation.
Q: Should I punish my child for throwing food?
Punishment is rarely effective and often counterproductive. If the function is attention, negative attention can reinforce the behavior. If the function is escape, punishment that ends the meal reinforces it. Function-matched alternatives produce more durable change without the relationship cost.
Q: How do I know which function is driving the throwing?
Escape: increases with non-preferred foods. Attention: child looks at you before/after; smiles at reaction. Communication: limited language; throws when specific needs emerge. Sensory: occurs even when alone; child seems absorbed in the throw itself. Not sure? Call 9100 181 181 — BCBAs identify function in one 30-minute observation.
Q: My child has texture sensitivities. Is this feeding therapy or behavior?
Both — which is exactly why OT and SLP work together at Pinnacle. The sensory aversion requires OT-led desensitization. The throwing behavior itself requires ABA-led function-based intervention. The FusionModule™ addresses both in one coordinated plan.
Q: My child throws at school too. Can the teacher implement this?
Yes — use Card 37's Teacher Communication Template. Request an IEP/504 accommodation for mealtime behavioral support. Many schools have SLPs who can set up the 'All Done' card system formally.
Q: We can never eat at restaurants. Will this ever change?
Yes. The typical progression: home mastery → grandparents → fast food → casual restaurants → full generalization. This usually takes 3–6 months post-home mastery. Card 25 covers generalization in detail.

Your Next Step: Start Now
Your child's mealtime transformation starts with one card, one bowl, and one consistent meal. You now have everything you need: the science, the materials, the protocol, the community, and the clinical pathway. The only thing left is to begin.
"You are not failing. Your child is not being defiant for no reason. Their behavior is a message — and now you know how to answer it."
🖐️ OT
Occupational Therapy
🗣️ SLP
Speech-Language Pathology
🧠 ABA
Applied Behavior Analysis
📚 SpEd
Special Education
🧬 NeuroDev
NeuroDev Pediatrics
🌸 Validated by the Pinnacle Blooms Consortium — OT · SLP · ABA/BCBA · Special Education · NeuroDev Pediatrics
Preview of 9 materials that help with food throwing Therapy Material
Below is a visual preview of 9 materials that help with food throwing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!
The Pinnacle Promise
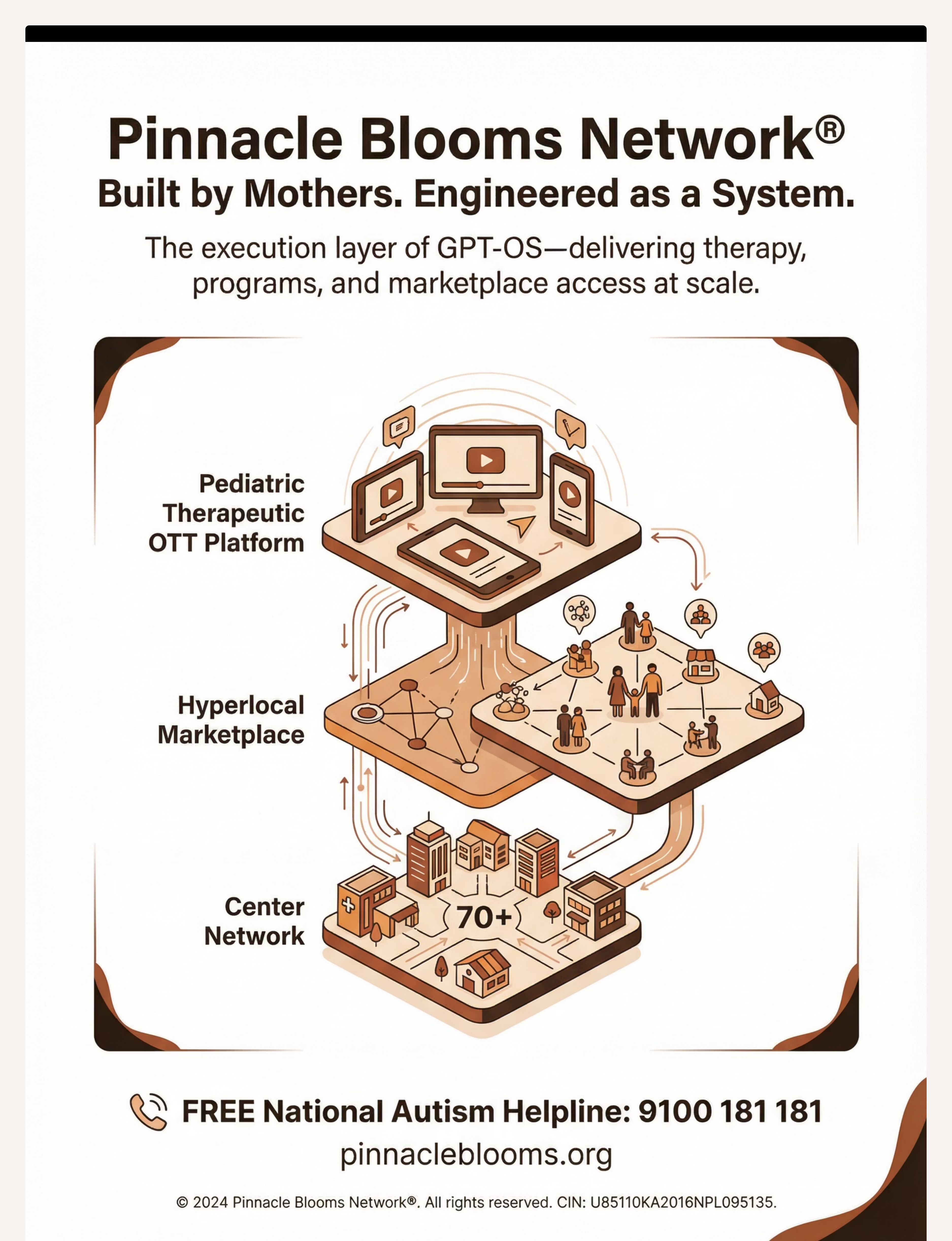
🌸 Pinnacle Blooms Network®
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® is India's largest multi-disciplinary pediatric therapy consortium — 70+ centers, 20M+ sessions, 97%+ measured improvement across 70 countries. GPT-OS® operationalizes the science of child development into daily home-executable therapy that any parent, anywhere, can deliver with confidence.
← E-468: Food Refusal Behaviors
📍 E-469: Food Throwing (Current)
E-470: Cup/Utensil Throwing →
Medical Disclaimer: This content is educational and does not replace individualized behavioral assessment and intervention with licensed professionals. Food throwing can have multiple underlying functions requiring professional functional analysis. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN | U74999TG2016PTC113063 | |
DPIIT | DIPP8651 (Govt. of India) | |
MSME | Udyog Aadhaar TS20F0009606 | |
GSTIN | 36AAGCB9722P1Z2 |
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages | pinnacleblooms.org | care@pinnacleblooms.org
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, and EverydayTherapyProgramme™ are proprietary technologies.