

- Impulse control differences — the brain's prefrontal inhibition system can't pause the "reach for food" impulse in time.
- Anxiety-driven urgency — a history of food insecurity or mealtime pressure creates a biological drive to eat fast before food disappears.
"This is a wiring difference — not a behavior choice. The brain is speaking a different sensory language." — Pinnacle Blooms Consortium, OT + SLP Division
Study | Finding | Reference | |
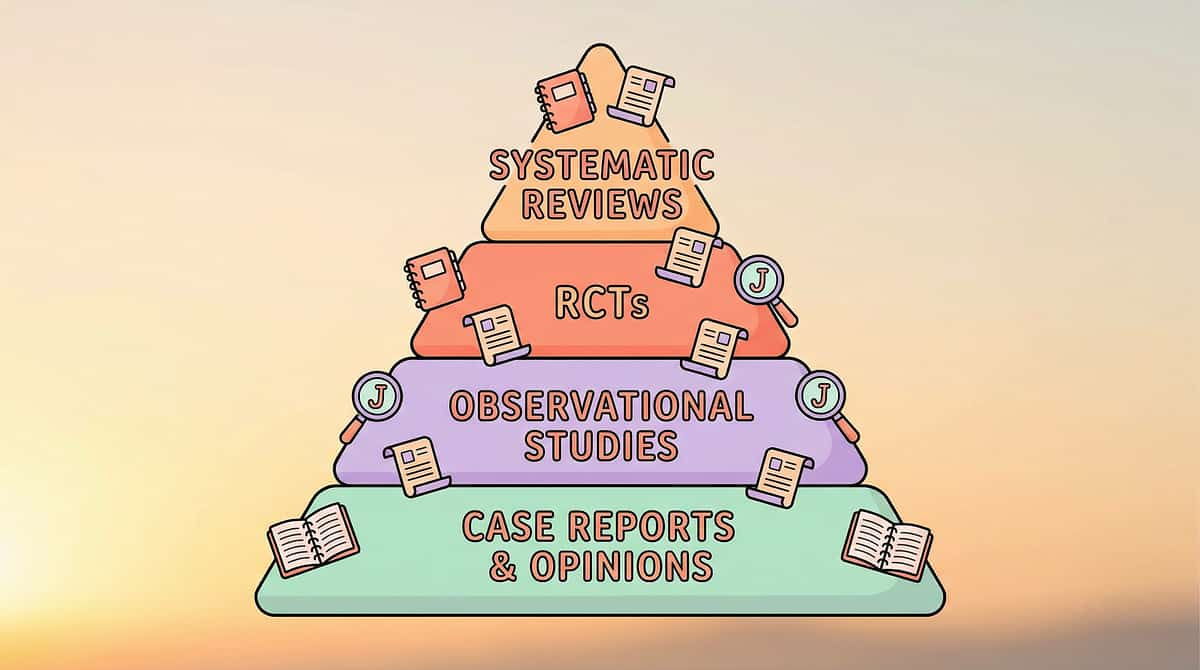
PRISMA Systematic Review 2024 | 16 studies confirm SI intervention is evidence-based for ASD | PMC11506176 | |
Meta-analysis World J Clin Cases 2024 | SI therapy effective for sensory processing, adaptive behavior, motor skills | PMC10955541 | |
Indian RCT (Padmanabha 2019) | Home-based sensory interventions showed significant outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP 2020 | Visual supports classified as evidence-based practice for autism | NCAEP Report | |
WHO CCD Package 2023 | Household-material interventions effective across 54 LMICs | PMC9978394 |
- 🏷️Domain: Feeding & Oral Motor
- 🎯Age: 2–12 years
- ⏱️Session: At every meal
- 📍Setting: Home + School
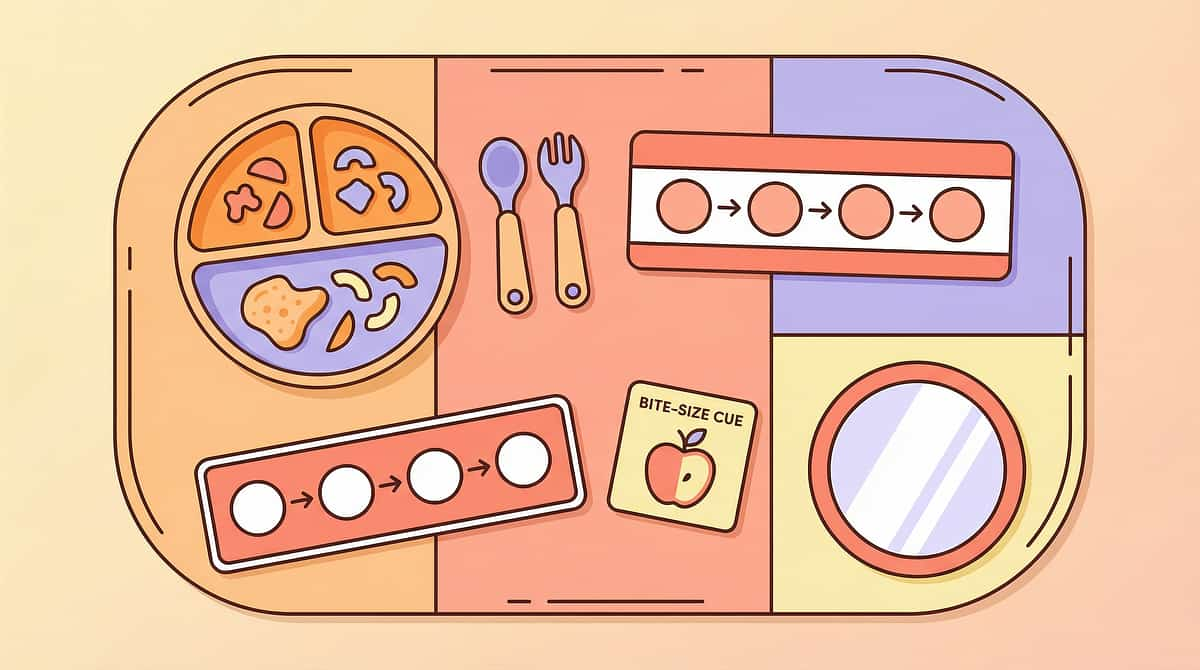
- 📦Materials: Feeding Tools | Oral Motor Materials | Visual Supports | Sensory Equipment


- Accepts smaller bites without distress
- Slows pace with visual support present
- Does not protest portion control systems
- Chews adequately before swallowing
- Demonstrates emerging self-monitoring
- Reduces gagging/choking episodes
- Eats at table with peers without constant monitoring
- Generalizes safe eating to school, restaurants, grandparents' homes
- Mealtimes become calm rather than hypervigilant







Zero Budget? Zero Barrier. Every Child Deserves This.
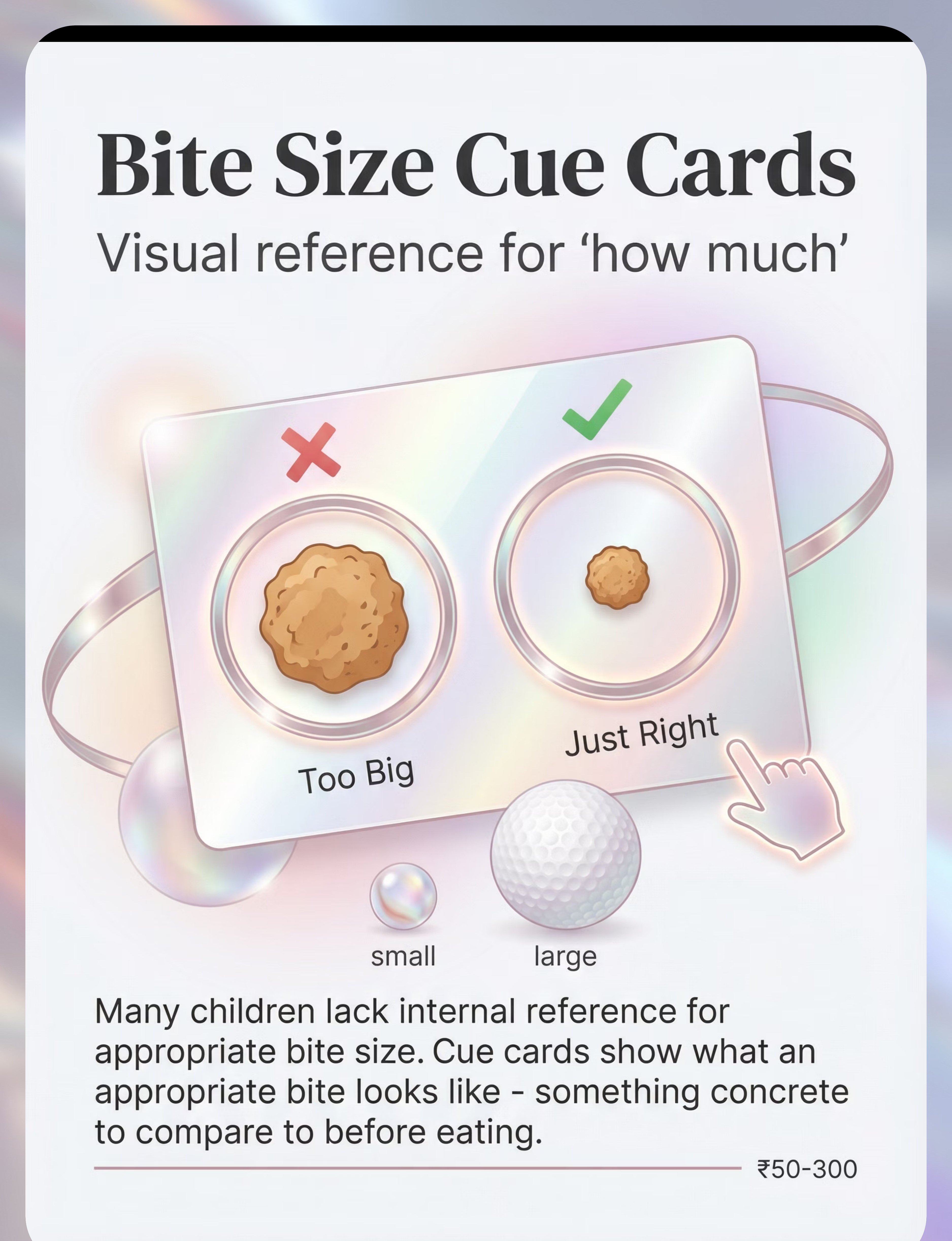
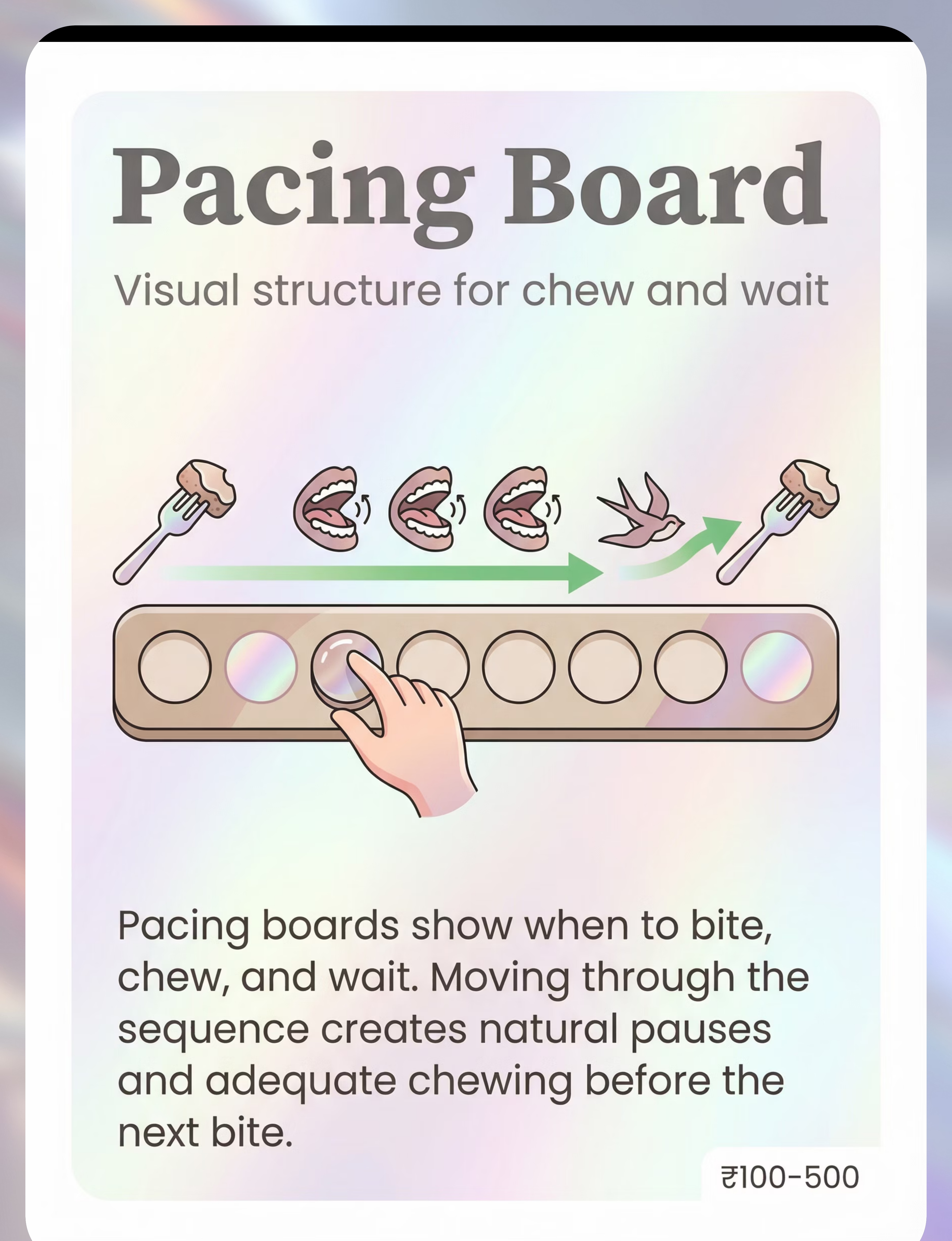
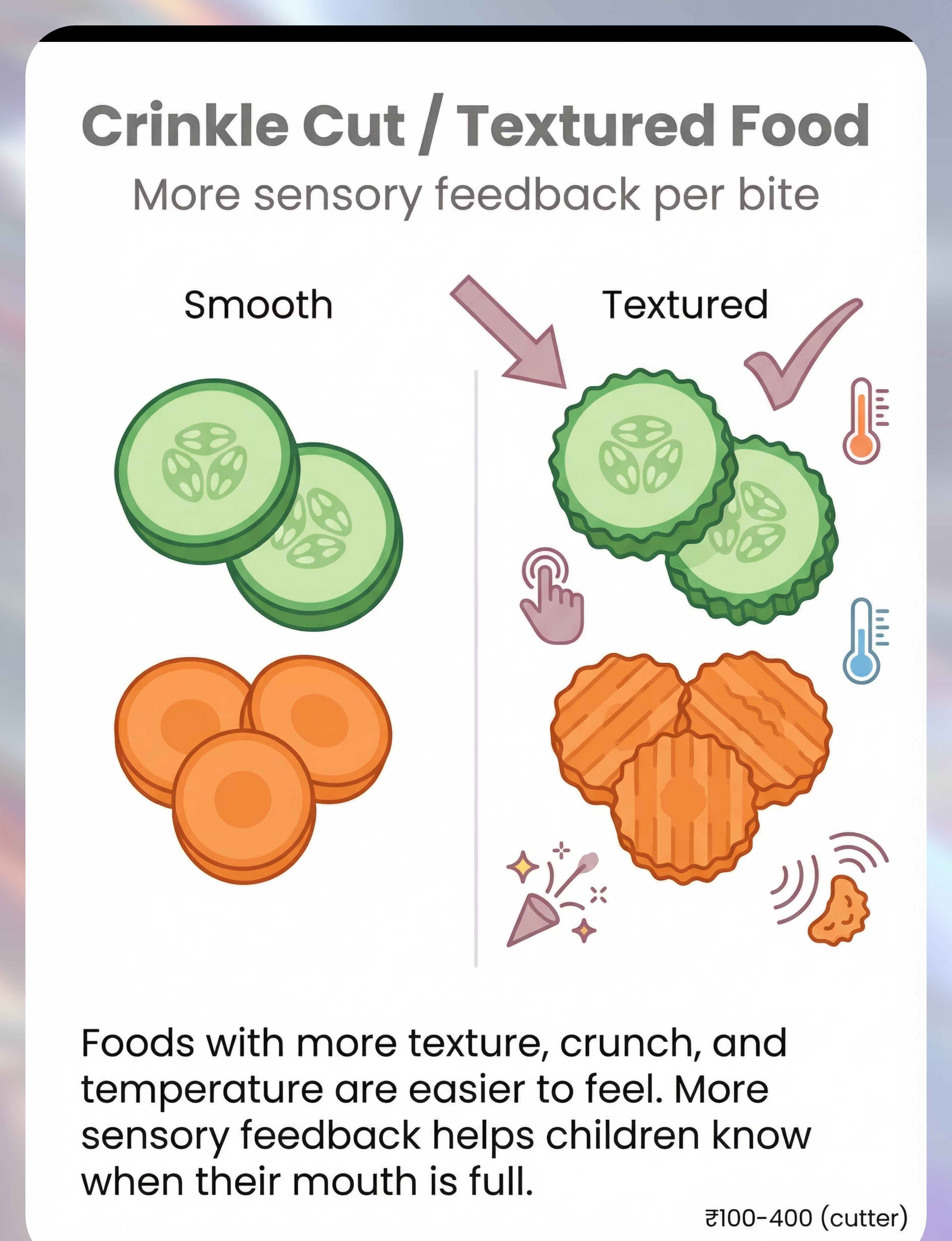
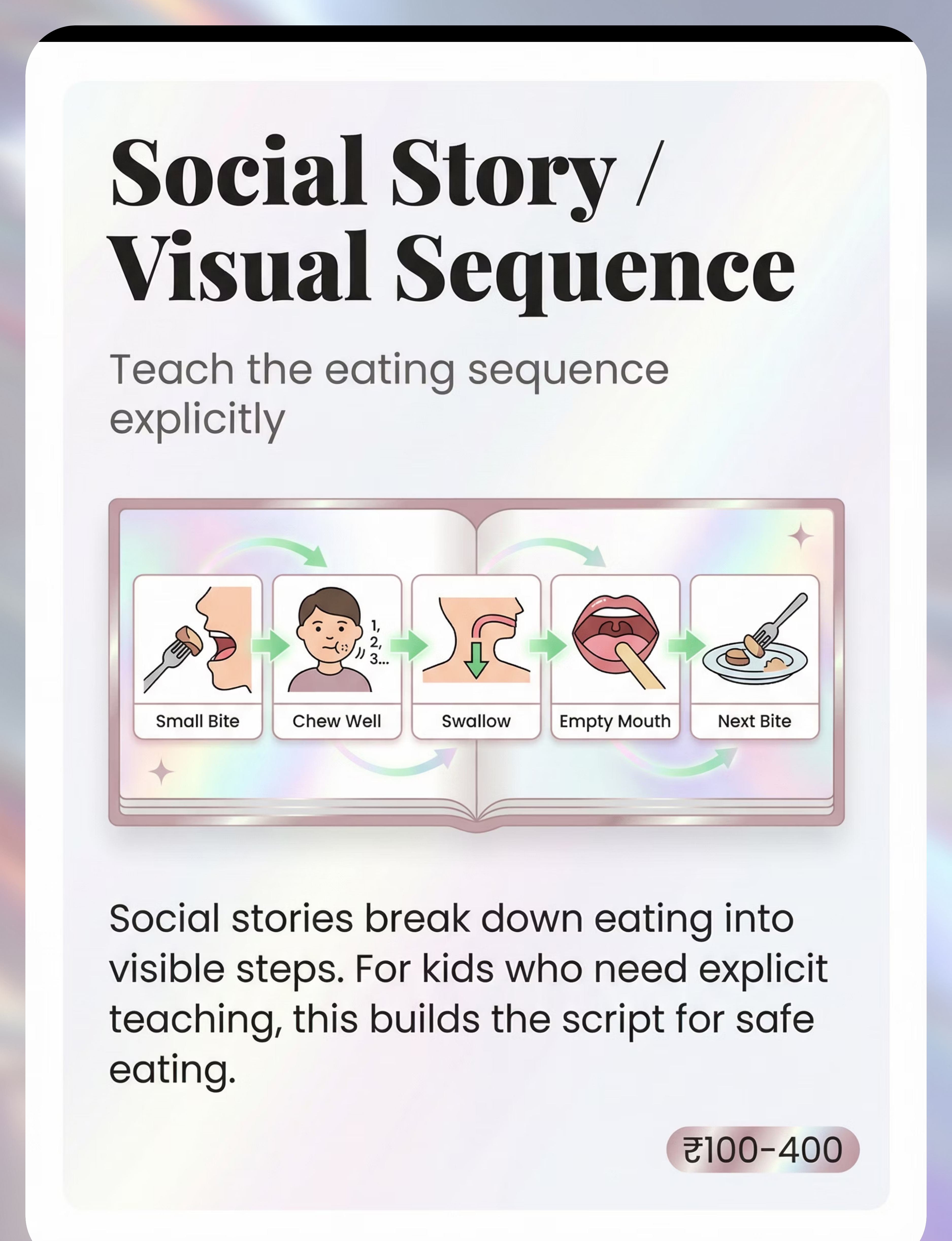
ACT II — EQUITY & ACCESS The WHO Nurturing Care Framework explicitly prioritizes context-specific, equity-focused interventions. These substitutes work because they engage the same sensory and behavioral mechanisms as their commercial counterparts. Every family, regardless of income, can begin today. Material Buy This DIY This (₹0) Divided Plate Compartment plate ₹200–800 Use a tiffin box with 3–4 compartments. Any plate + small bowls for sections. Small Utensils Child spoon set ₹100–400 A dessert spoon or tea spoon from any kitchen — literally the smallest spoon in your drawer. Bite Size Cue Cards Printed laminated cards ₹50–300 Hand-draw on paper: circle showing "bite this big" — stick it at the child's meal spot. Pacing Board Purchased board ₹100–500 Row of 8 stickers on cardboard. Child touches one per chew. Make in 5 minutes. One-Piece Tray Small tray ₹100–400 A small saucer, the lid of a container, or a folded napkin for one piece at a time. Mealtime Mirror Safety mirror ₹100–500 Any small mirror that won't break easily, propped against a book or cup at eye level. Oral Sensory Tools Z-Vibe ₹300–1,500 A clean, soft toothbrush used in a circular motion on cheeks/tongue before meals. Crinkle Cutter Kitchen tool ₹100–400 A fork dragged across soft vegetables creates texture ridges. Free and effective. Social Story Printed cards ₹100–400 Draw 5 stick figures: Bite → Chew → Chew × 10 → Swallow → Empty mouth → Next bite.

- Child is gagging severely or choking at most meals
- Wet/gurgling voice after eating, chronic cough during/after meals, recurrent chest infections
- Child is losing weight or refusing to eat entirely
- Overstuffing is getting worse, not stable or better
- Child is tired, recently upset, or post-meltdown — simplify to one-piece presentation only
- Child is very hungry — give a small safe snack first
- New food being introduced — use maximum support structure
- High-risk foods (whole grapes, hot dogs, popcorn) — modify or avoid until bite-size control improves
- Child is alert, calm, and reasonably well-regulated
- You have 15–20 minutes without major interruption
- At least one safety material is in place (small utensils OR one-piece presentation)
- You know the pediatric Heimlich maneuver
- Table cleared of all items except session materials
- TV / music / screens OFF
- Child seated with good postural support — feet on floor or footrest
- Small utensils in place — large utensils removed from table
- Bite size cue card at child's eye level
- Pacing board positioned on child's dominant hand side
- Mirror positioned if using (stable, unbreakable)
- Parent sitting to child's side, not directly opposite — less confrontational
- Oral sensory tool used for 1–2 minutes PRE-meal if applicable
- Extra food in small portions
- Paper towel
- Water
- All distractions
- Large utensils
- Full serving dishes (keep food out of reach)

Check | Go ✅ | Modify ⚠️ | Postpone ❌ | |
Alertness | Awake, responsive | Drowsy but present | Falling asleep | |
Emotional state | Calm / happy | Mildly frustrated | Crying / meltdown | |
Recent stress | None in last 30 min | Minor incident | Major meltdown <30min | |
Hunger level | Normal hunger | Very hungry | Just ate / not hungry | |
Physical | No illness signs | Minor sniffles | Fever / vomiting / pain |

"[Child's name], it's time for lunch. Come sit with me — I have your special [favourite food] ready."
- Kneel or sit at child's level before approaching
- Warm, calm facial expression — no tension
- Gesture toward the chair, not toward yourself
- Keep voice 20% quieter than your normal speaking voice
- Materials are already set up — don't mention them yet
- Child ignores: Wait 15 seconds, offer again once
- Child says no: "Okay. The food will be here. Come when you're ready." (Wait up to 5 minutes)
- Child protests: Use a transition object — "You can bring your toy/fidget to the table"


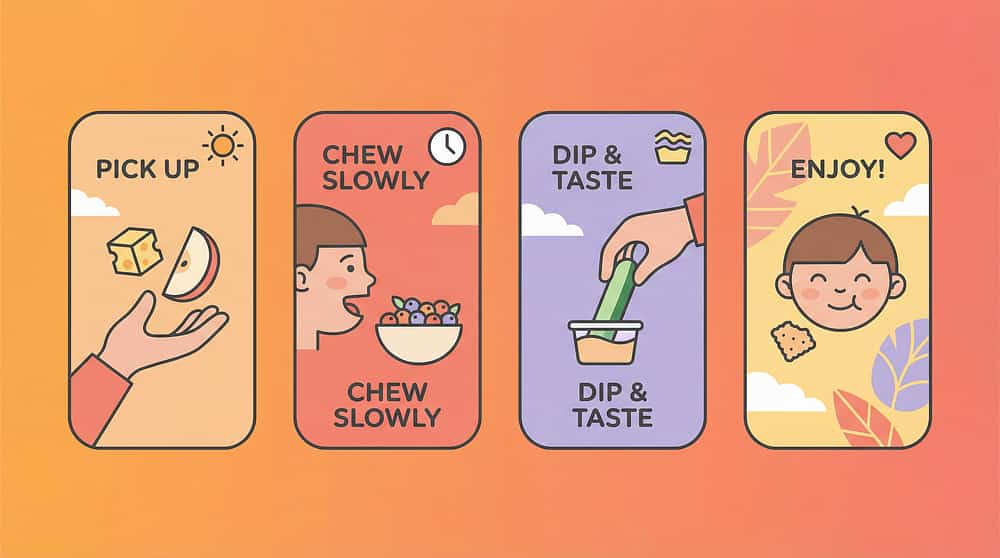
The 5-Part Eating Sequence — Teach It Until It's Automatic
STEP 3 OF 6 This is the core of the intervention. The sequence converts an unconscious, dysregulated behavior into a conscious, scaffolded routine — and with repetition, it becomes internalized habit. Target duration: 10–15 minutes of active eating. A. LOOK 👁️ Child checks the bite size cue card before picking up food. Parent: "Check your card — is your bite that size?" B. ONE PIECE 🍽️ Child picks up ONE piece (utensil limits what can be picked up). Parent: "Good — just one." C. CHEW ✅ Child chews. Move pacing board marker one space per chew. Target: 10–15 chews. Parent: silent, or counting quietly — not directing. D. SWALLOW + CHECK 👄 Child swallows, then opens mouth to show "empty" (or self-checks in mirror). Parent: "Empty? Good. Ready for the next one." E. WAIT ⏸️ One brief pause before the next piece. Use a 3-second visual timer. Parent: "Three... two... one... next piece." If concerning behavior: Child abandons sequence, becomes distressed, repeatedly grabs extra food. → Reduce to one-piece presentation only. Remove all food from view except what is in front of child. Don't reprimand — quietly manage.
- Every meal where overstuffing is a risk = opportunity for practice
- Minimum: 2 structured mealtimes per day
- Maximum: All 3 main meals, if family can sustain the structure
- Child slows naturally without prompting
- Child pushes food away and covers plate (genuine signal)
- Child's eating pace has noticeably slowed from the beginning of the meal
Food | Modification | |
Soft foods (rice, dal, idli) | Extra emphasis on small utensil — deep spoon replaced with tea spoon | |
Crunchy foods (carrot, cucumber) | Serve crinkle-cut — more sensory feedback per bite | |
Preferred foods (child's favourites) | Highest-risk — use maximum structure | |
Mixed meals | Divide sections in plate — sequence through one section at a time |
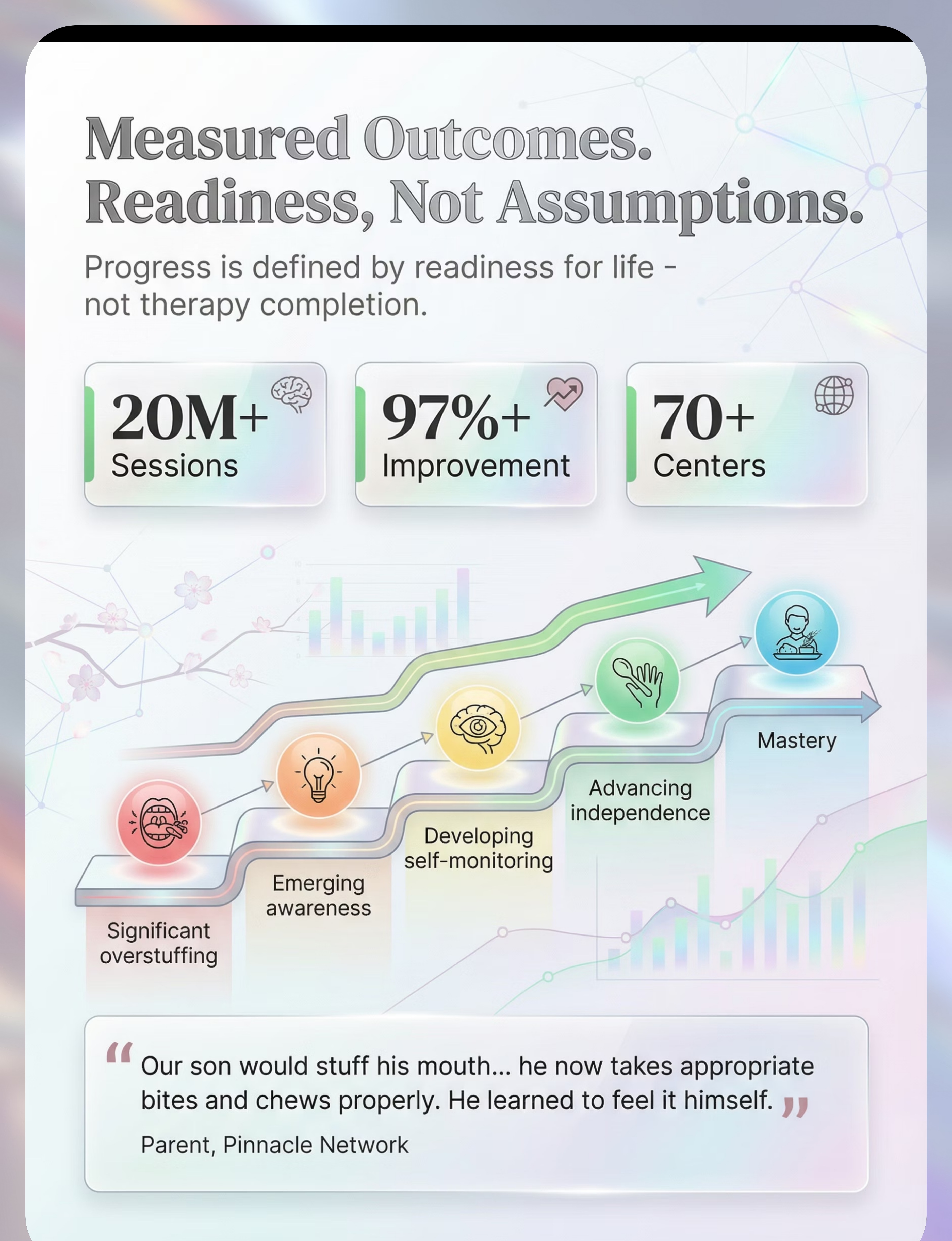
"3 bites taken with awareness and correct pacing are worth more than a full plate eaten with stuffing. Measure quality of eating, not quantity of food consumed."

Every Meal Deserves a Gentle Ending
STEP 6 OF 6 How a mealtime ends matters as much as how it begins. A predictable, calm close reduces the anxiety that can accumulate across a meal — and sets the emotional tone for the next mealtime before it has even begun. Transition Warning (2 minutes before end) "Two more bites, then we're all done." Use a mini sand timer — visual and tactile. Child Finishes Last Bite Using the Sequence Child places utensils down. Parent: "Meal complete. You did beautifully." Child Helps Put Pacing Board Away Participation builds ownership. This small act reinforces that the system belongs to the child, not just the parent. Brief Sensory De-escalation if Needed Hand squeeze, deep breath together, or 30 seconds of quiet. Offer water. Brief quiet activity — no screens for 5 minutes. Awareness-Building Conversation If child used mirror: "Did you notice your bites were smaller today?" This gentle reflection builds metacognitive awareness over time. If child resists ending: Resist removing plate suddenly — this increases food anxiety. Instead: "The food is going to the kitchen now. There will be more at [next meal time]. You did great." Remove plate calmly and without emotion.

- Bite Size (1–5 scale): 1 = constant stuffing → 5 = consistent small bites
- Pacing (1–5 scale): 1 = rapid, no pausing → 5 = paused between bites
- Gagging/Choking Episodes: 0 / 1 / 2 / 3+
- □ Divided plate □ Small utensils □ Cue card
- □ Oral tool (pre-meal) □ Pacing board
- □ One-piece tray □ Mirror
- □ Textured food □ Social story

Problem | Root Cause | Solution | |
Child refuses divided plate | Novelty aversion / rigidity | Introduce empty plate first. Add food section by section over days. | |
Child removes pacing board from table | Sensory aversion or doesn't understand purpose | Move board to child's non-dominant side. Narrate it casually. Model it yourself. | |
Bite size improves at home, but not at school | Environment inconsistency | Send small utensils to school. Share cue card with teacher. Call school support: 9100 181 181. | |
Child stuffs MORE when given small portions | Anxiety about food scarcity | Reassure food availability: keep visible refill ready. Announce: "There's more coming." | |
Mirror becomes distraction / play | Mirror-seeking behavior | Remove mirror. Replace with parent's verbal feedback: "Look at your bites — how big are they?" | |
Oral sensory tools rejected | Tactile aversion | Start with a soft toothbrush. Very brief 10-second touch. Build tolerance slowly. | |
Social story is ignored / child tears it | Engagement issue | Animate it — act it out with food at the table. Draw it together as a game, not a lesson. |
Sensory Profile | Priority Materials | |
Oral hyposensitive (can't feel food) | Oral sensory tools first + textured food + small utensils | |
Impulsive (can feel, but can't pause) | Pacing board + one-piece presentation + token economy | |
Anxious about food scarcity | Environment reassurance + small portions with visible refills | |
Motor planning difficulty | Social story + visual sequence + divided plate |

- Child tolerates materials without major protest (first win)
- Occasional compliance with one-piece presentation
- No change yet in self-regulation — that's expected and normal
- Parent confidence growing — you know what to do
- Self-initiated bite size regulation
- Pacing without verbal prompts
- Transfer to other settings (school, restaurants)

Milestone | When | How to Celebrate | |
First meal with no gagging | Week 1–3 | Verbal recognition + sticker on family chart | |
First meal with self-paced eating | Week 3–6 | Special preferred activity after dinner | |
First time child corrects own bite size | Week 5–10 | "You did that yourself. I'm amazed." — make it memorable | |
First meal without pacing board | Week 6–12 | Document it — take a note of the date | |
First meal at restaurant with appropriate bites | Week 8–16 | Family celebration — this is generalization | |
First full week with no stuffing | Week 12–24 | This is mastery entering. Honor it fully. |
Sign | Urgency | Professional to Contact | |
Choking/gagging at multiple meals per week despite intervention | URGENT | Pediatrician → Feeding Therapist + SLP | |
Wet/gurgly voice consistently after eating | URGENT | SLP for swallowing evaluation (VFSS) | |
Food consistently coming back up from mouth | HIGH | SLP + Gastroenterologist | |
No reduction in overstuffing after 8 weeks of consistent intervention | MODERATE | Feeding Therapist + OT | |
Child becoming more anxious/distressed at mealtimes (not less) | MODERATE | Feeding Therapist + Psychologist | |
Weight loss or significant nutritional restriction | HIGH | Pediatrician + Dietitian |

You Don't Have to Figure This Out Alone
ACT V — CONNECT The families navigating the same mealtimes, the same challenges, and the same hopes are right here. Moderated by Pinnacle feeding therapists. Active daily. Available in 16+ languages. Pinnacle Parent Community Join the Feeding & Mealtime Independence parent group — moderated by Pinnacle feeding therapists. Active daily. 16+ languages. pinnacleblooms.org/community/feeding → Pinnacle GPT-OS® Platform Access EverydayTherapyProgramme™ — daily home-executable feeding interventions, personalized to your child's profile. pinnacleblooms.org/gpt-os → Free Helpline — 24×7 📞 9100 181 181 — 16+ languages | Free. Ask anything. No appointment needed. First call free, always.
Study | Key Finding | Access | |
PRISMA SR 2024: Children with ASD & SI | 16 studies — SI intervention evidence-based practice | PMC11506176 | |
World J Clin Cases Meta-analysis 2024 | SI therapy: social skills, adaptive behavior, motor skills | PMC10955541 | |
WHO Care for Child Development Package | Household intervention validated 54 LMICs | PMC9978394 | |
Padmanabha et al. Indian J Pediatr 2019 | Home-based SI interventions: significant outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP Evidence-Based Practices 2020 | Visual supports & video modeling: evidence-based for autism | ncaep.fpg.unc.edu | |
ASHA Clinical Guidelines | Feeding and swallowing disorders in children | asha.org | |
SOS Approach to Feeding (Toomey) | Sequential Oral Sensory framework — gold standard | sosapproach-conferences.com |
- Which materials your child responds to
- What time of day / hunger level triggers worst stuffing
- Whether primary driver is sensory, behavioral, or anxiety-based
- Personalized fading schedule recommendations

Share This Page — Consistency Across Caregivers Multiplies Impact
ACT V — SHARE When grandparents, teachers, and all family members use the same approach, the child's nervous system receives consistent, coherent input — and learns faster. Caregiver alignment is not a nice-to-have; it's a clinical accelerator. 📱 Share on WhatsApp "Our child is working on bite size control with these 9 therapy materials — [link]. The divided plate and small utensils alone made a difference in week 1." 👵 Explain to Grandparents "Our child takes too much food into their mouth at once — it's not greedy, it's that their mouth doesn't send the 'full' signal. Use small spoons, give one piece at a time, don't rush them. Say 'good job chewing' when they slow down." 🏫 Teacher Communication Template "Dear [Teacher], our child is working on bite size regulation. At home we use: small utensils, a divided plate, and visual cue cards. Please can meals be supervised and the same small utensils be used at school? Thank you." 📄 Download 1-Page Family Summary — PDF 📧 Share via Email

You Have Everything You Need. Start This Meal Differently.
ACT VI — START NOW The 9 materials on this page cost between ₹0 and ₹1,500 total. You already have most of them in your home. The science is clear. The pathway is laid out. The only step left is the first one. 🟢 Start This Technique Today — Launch GPT-OS® Session 📞 Book a Consultation — 9100 181 181 | Free | 24×7 ▶ Explore Next Technique — E-461: Food Texture Sensitivity ✦ Validated by the Pinnacle Blooms Consortium | OT • SLP • ABA • SpEd • NeuroDev • Feeding Therapy • WHO/UNICEF Aligned | 📞 9100 181 181 | Free | 24×7 | 16+ Languages
Preview of 9 materials that help with mouth overstuffing Therapy Material
Below is a visual preview of 9 materials that help with mouth overstuffing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







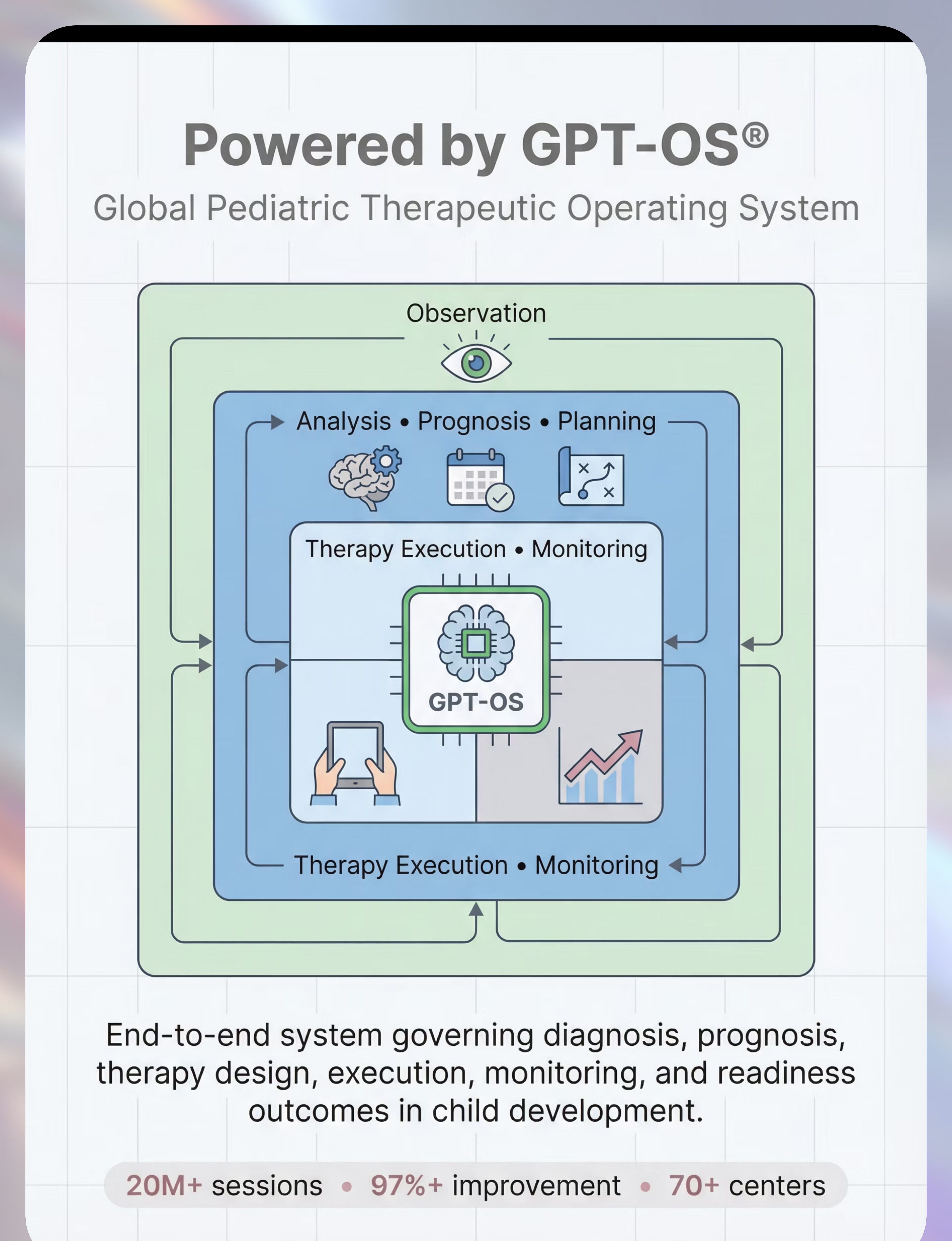






The Pinnacle Promise
PINNACLE BLOOMS NETWORK® "From fear to mastery. One technique at a time." — Pinnacle Blooms Network® Pinnacle exists to transform every home into a proven, scientific, 24×7 personalized pediatric therapy environment — powered by GPT-OS® and delivered by the world's most integrated pediatric consortium. 1:1 Sessions Delivered Measured Improvement Centers Across India Countries Served ← Return to Top Card 01 — The Recognition Moment → Next Technique E-461: Food Texture Sensitivity Browse All Feeding Techniques techniques.pinnacleblooms.org Medical Disclaimer: This content is educational and informational. It does not replace individualized feeding assessment and intervention by licensed feeding therapists, speech-language pathologists, or occupational therapists. Mouth overstuffing can have multiple underlying causes requiring professional evaluation. Choking is a serious risk; implement safety measures and seek professional guidance for persistent feeding difficulties. Individual outcomes vary by child profile, underlying cause, and intervention specificity. © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 📞 9100 181 181 | FREE National Autism Helpline | 16+ languages | 24×7 | pinnacleblooms.org | care@pinnacleblooms.org