
Dressing & Grooming
30 evidence-based interventions for children with autism — independent dressing, buttons, zippers, shoe tying, sensory clothing issues, hair brushing, toothbrushing, bathing, and self-care motivation. Subdomain E3 | Pinnacle Blooms Network®
Neuroscience Primer
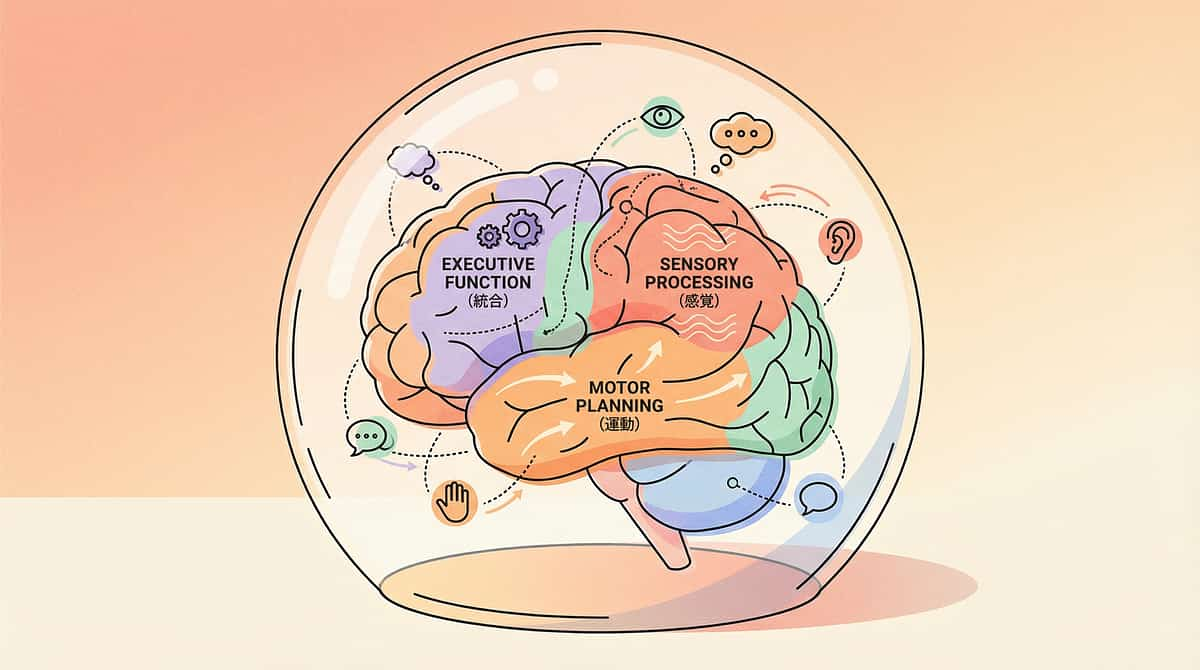
Why Dressing & Grooming Are So Hard in ASD
Self-care in ASD is delayed by an average of 2–4 years compared to neurotypical peers. A 7-year-old with ASD may have the self-care independence of a 3–4 year old — not because of intelligence, but because every self-care task demands the simultaneous coordination of systems that are each independently challenged in ASD.
Motor Planning
Dyspraxia affects 50–80% of ASD children, making multi-step motor sequences effortful and error-prone.
Sensory Processing
Tags, seams, brush bristles, water on face — each a potential sensory assault on a sensitized nervous system.
Bilateral Coordination
Buttons, zippers, and shoe tying all require both hands doing different things simultaneously.
Executive Function
Initiation, working memory, self-monitoring — the PFC demands of a 15-step morning routine are enormous.

Section 1 of 4 · Dressing Skills — Cards 01–09 cover the full spectrum of dressing independence — from putting on a shirt to managing sensory clothing challenges and weather-appropriate choices.
E-521
Independent Dressing
The Moment
Every morning: "Arms up. Head through. No, other arm. Turn it around. That's backward. Pull down. Now pants." You dress them. Every day. Every item. And you wonder: will they ever dress themselves? The answer is YES — with task analysis, chaining, practice, and adaptive strategies.
The Evidence
📊Level I — Task analysis + chaining (backward or forward) is the gold standard for dressing independence in ASD. NCAEP 2020 | PMC10955541
What You'll Learn
- Dressing task analysis — every item broken into smallest teachable steps
- Backward chaining: parent does everything except the last step → child completes → SUCCESS → fade backward
- Forward chaining: child does first step → parent completes → gradually child does more
- Which chaining method to use and when
- Practice with the SAME clothes daily to reduce variability
- Indian school uniform dressing sequence
Lead Clinicians
🤲 OT (Motor Planning / Fine Motor) · 📋 ABA | SpEd · NeuroDev

E-522
Button Skills
Buttons require the most sophisticated bilateral hand coordination of ANY dressing task. One hand holds the fabric steady while the other threads the button through the hole — each hand performing a completely different role simultaneously. School uniforms, formal wear, and many Indian garments demand this skill every single day.
1
Large Buttons on Practice Board
Begin with an oversized dressing frame (₹200–500 or DIY) — removes the challenge of wearing the garment while learning.
2
Large Buttons on Own Shirt — Laid Flat
Practice on the child's actual shirt while it lies on a table — adds familiarity without the body-orientation challenge.
3
Buttons While Wearing
Finally, practice with the shirt on the body. Start with UNBUTTONING (pulling apart is easier and provides satisfying sensory feedback).
4
Progressively Smaller Buttons
Large → medium → small → shirt buttons. Indian kurta and sherwani buttons are excellent cultural daily-practice opportunities.

E-523
Zipper Skills
The Motor Challenge
Insert tab into slider. Hold the bottom. Pull up. Three separate motor actions in precise coordination. The initial insertion is the hardest step — a tiny tab into a tiny slider requires visual-motor precision that most ASD children need explicit, scaffolded teaching to acquire.
The Evidence
📊Level I — Fine motor progression + practice activities. NCAEP 2020
Zipper Progression
- Pull up (already connected) → pull down → connect + pull up → fully independent
- Zipper pull adaptation: attach ribbon, ring, or large pull tab (₹0 — dramatically easier to grip)
- Practice jacket laid flat on table before practicing on body
- Jacket off hook → zip → put on (separating motor demands into manageable chunks)
- Indian daily practice: school bag zippers, jacket zippers, pencil case zippers
E-525
Backward Dressing
The Moment
Shirt on backward. Pants backward. Shoes on wrong feet. Inside out. Every garment with a 50% chance of being wrong. Backward dressing reflects body schema confusion — the child's internal map of their body doesn't reliably match the spatial orientation of clothing.
The Neuroscience
Correct orientation requires body schema (knowing front from back on your own body), visual-spatial processing (reading clothing cues), and mental rotation (if I see the tag, it goes at the BACK). ASD challenges all three simultaneously.
Practical Orientation Strategies
- Tag = back (or cut tags and mark front with fabric pen or sticker)
- Design or picture = front
- "Lay out and step in" method: shirt face-down on bed, arms in sleeves, flip over head
- Shoe matching: colour dots on inner edges (dots touch = correct feet)
- Indian school uniform: label placement, belt buckle as front marker
E-526
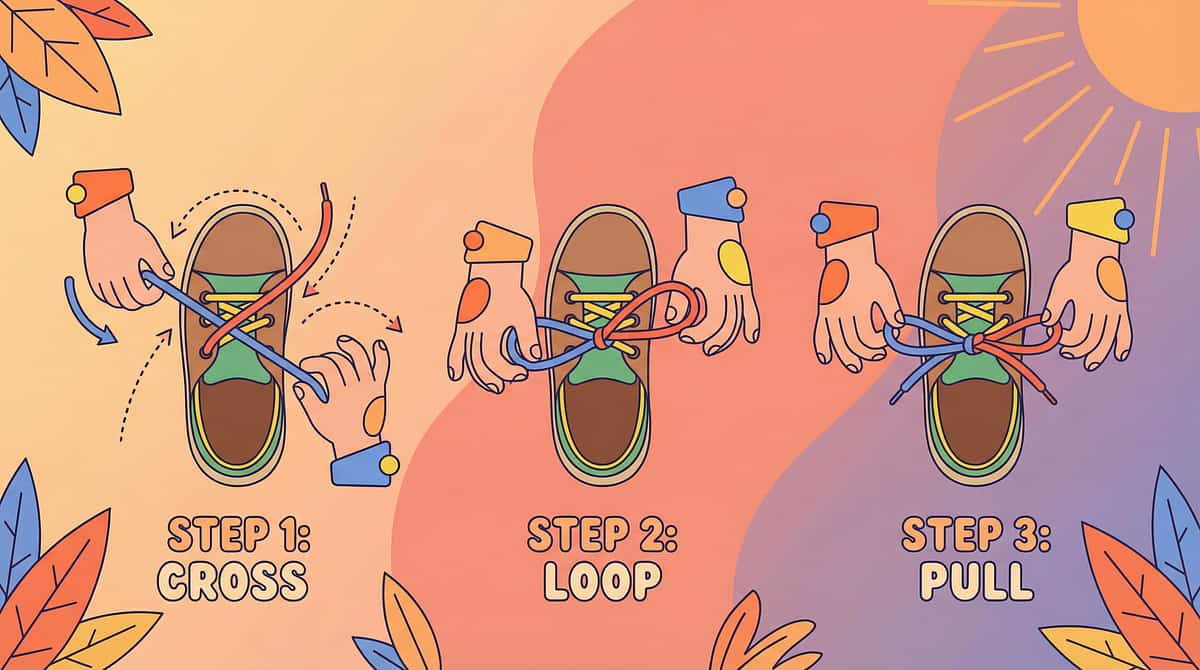
Shoe Tying
The Everest of dressing skills. Shoe tying requires the highest bilateral coordination, finest motor precision, and most complex sequencing of any daily living task. Average mastery age in neurotypical children is 6–7 years. In ASD, it is often 9–12 or later — and that is completely acceptable, because effective alternatives exist.
Use Alternatives First
Velcro shoes, slip-ons, elastic laces (convert any shoe to slip-on — ₹100–300), toggle laces. Independence matters more than convention.
Two-Colour Lace Method
Different colour for each lace visually separates the two simultaneous sequences — the most effective teaching method for ASD learners.
Bunny Ears Method
Both laces form loops that are then tied together — a simpler bilateral pattern than the traditional wrap-around method.
Practice Off the Foot
Practice on a shoe placed on a table facing away from the child — removes the added complexity of working on a surface below their body.
⚠️ Do NOT make shoe tying a daily battle. Adaptive alternatives are a valid, permanent solution. Independence always takes priority over convention.

E-527
Clothing Sensory Issues
This Is Not Pickiness
Tags scratch. Seams dig. Socks feel wrong. The collar is too tight. For a child with tactile hypersensitivity, putting on clothes is genuinely painful — a continuous, low-grade sensory assault that lasts all day, every day. The somatosensory cortex amplifies every fabric signal: tags become blades, seams become ridges, tight clothing becomes compression.
Immediate Solutions
- Cut ALL tags — do this for every new garment
- Turn socks inside out so seams sit on the outside
- Seamless underwear and flat-seam clothing
- Soft cotton only — wash new clothes 3–5 times before first wear
- Compression-fit garments (deep pressure = calming; light touch = irritating)
- Indian fabric: soft handloom cotton preferred; avoid polyester in heat

E-528
Single Outfit Rigidity
Only THAT shirt. Only THOSE pants. The same outfit every day. If it's in the wash — meltdown. If it wears out — crisis. Outfit rigidity is sameness insistence applied to clothing. The basal ganglia has encoded one specific outfit — its precise fabric, fit, weight, and colour — as neurologically SAFE, and the brain rejects all alternatives as a genuine threat, not a preference.
Buy Multiples
Purchase 3–5 identical sets of the preferred outfit. This investment prevents daily crisis and maintains the sensory template while enabling washing.
"Same But Slightly Different"
Exact same style in a slightly different colour → exact same colour from a slightly different brand. Reduce one variable at a time.
Involve the Child
Giving the child agency in selection significantly reduces rigidity. A choice between two approved options builds flexibility within safety.
Use School Uniform as Practice
The Indian school uniform is a built-in daily alternative — different from home clothes and socially sanctioned, making it an ideal flexibility bridge.

E-529
Weather-Appropriate Clothes
The Challenge
Refuses a jacket in winter. Insists on long sleeves in 40°C summer. Wears sandals in the rain. Weather-appropriate dressing requires interoception (feeling hot or cold internally), abstract weather concepts, cognitive flexibility (today's clothes differ from yesterday's), and tolerance for weather-specific garments with new textures and fits.
Visual Weather-Dressing Chart
- Sunny ☀️ → cotton, shorts, sandals
- Rainy 🌧️ → raincoat, closed shoes, umbrella
- Cold 🧥 → sweater, jacket, socks
Teaching the Routine
Window check → look at chart → choose clothes. Teach temperature feeling: "Is your body hot or cold?" → match to clothing choice. Indian seasons require specific attention: monsoon prep, summer cotton, Delhi pollution masks, winter layering.

Section 2 of 4 · Grooming & Hygiene
E-530
Hair Brushing
The brush touches the scalp and the screaming starts. Hair brushing combines tactile input (bristles on a sensitised scalp), proprioceptive input (pulling force during detangling), genuine pain from tangles, and duration (repeated strokes over several minutes). For tactile-defensive children, the brain begins anticipating pain the moment the brush is visible — conditioned avoidance before bristle ever touches hair.
Brush Selection
Wide-tooth comb first (minimal scalp contact), wet brush or Tangle Teezer (designed for pain-free detangling), then soft bristle brush as tolerance builds.
Technique Adjustment
Start at ends and work upward — this dramatically reduces pulling sensation and is the single most effective technique change.
Desensitisation First
Deep pressure scalp massage BEFORE brushing, or a vibrating scalp massager. Proprioceptive input prepares the nervous system for what follows.
Desensitisation First
Indian Context
Oil hair before brushing — the traditional coconut oil application reduces friction and is a culturally familiar sensory routine that eases the transition.

E-531
Haircut Preparation
The Crisis
Haircut day equals crisis day. The salon delivers: an unfamiliar environment, a stranger touching their head, buzzing clippers at 60–70 dB directly at the ear, a restrictive cape, scissors near the face, and hair falling on sensitised skin. Some families haven't cut their child's hair in years. This is understandable — and completely addressable with systematic desensitisation.
Desensitisation Pathway
- Salon visit with NO haircut — just observe
- Sit in the chair — nothing else
- Cape on — still nothing else
- Play hairdresser at home (comb through hair, pretend scissors)
- First cut: one single snip
- Gradually increase duration over multiple sessions
Sensory Accommodations
Noise-cancelling headphones during clippers · Preferred show on phone · Favourite toy · Deep pressure before the session · Finding an ASD-friendly barber or arranging home haircuts.
E-532
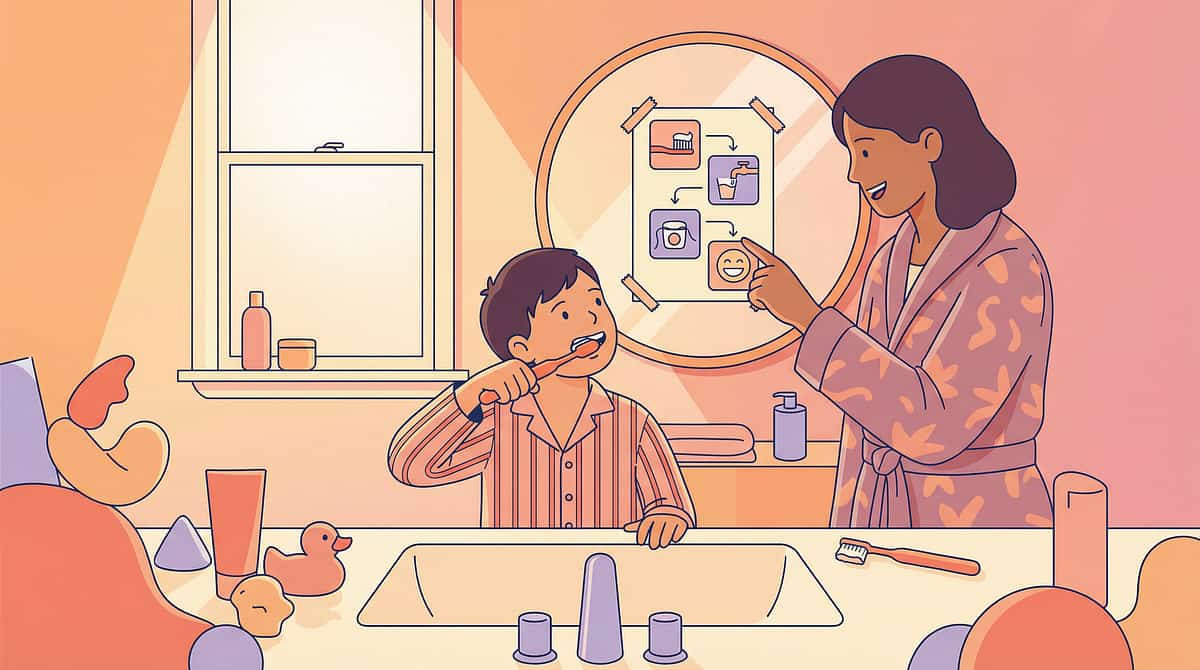
Toothbrushing
Open mouth. Foreign object enters. Bristles scrape gums. Mint paste burns the tongue. A frothy substance fills the mouth. For orally defensive children, toothbrushing is daily torture — and when avoided, dental health suffers catastrophically. Cavities accumulate. Dental visits become surgical procedures under general anaesthesia. This is a medical priority, not a preference battle.
Finger on Gums
Begin with a clean finger applying gentle pressure to the gum line — no tools, no paste. Build oral touch tolerance from the ground up.
Finger with Cloth
Wrap a soft cloth over the finger. Slightly different texture, same predictable control and pressure.
Finger Brush
Silicone finger brush — soft, controllable, no long handle entering the mouth unpredictably.
Soft Toothbrush
Front teeth only initially → sides → back teeth → tongue. Expand gradually over weeks, not days.
Toothpaste progression: start WITHOUT paste → unflavoured paste → mild fruit → mild mint. Indian options include Meswak, Himalaya herbal, and child-specific mild formulations. Electric toothbrushes suit some children — vibration provides deep pressure input that feels calming rather than invasive.
⚠️ Dental health is a MEDICAL PRIORITY. Untreated cavities cause chronic pain that directly escalates behaviour. Never deprioritise toothbrushing.

E-533
Face Washing
Why the Face Is Different
The face has the HIGHEST density of tactile receptors in the entire body (trigeminal nerve distribution). Water on the face triggers tactile overwhelm, temperature shock, and startle as water unpredictably enters eyes, nose, and mouth. Some children experience face-wetting as a drowning-like sensation — not a metaphor, but a genuine neurological experience of threat.
Graduated Exposure
- Dry cloth on face → damp cloth → wet cloth
- Splash water on cheeks → full face wash
- Wet wipes as controlled, predictable alternative for severe aversion
- Micellar water on cotton pad (no rinsing required)
- Deep pressure — firm hand press on cheeks — before washing
- Warm water is usually tolerated significantly better than cold
E-538 · Hand Washing
Beyond post-toilet handwashing, this focuses on generalised hand hygiene across all contexts — before meals, after outdoor play, after touching animals, when hands are visibly dirty.
Context-Specific Visual Reminders
Handwashing trigger visuals posted in the kitchen, at the back door, and near the pet area. The visual does the prompting — the adult steps back.
Sensory-Friendly Soap
Test preferred texture (bar vs. foam vs. gel), preferred temperature, and unscented vs. mild scent.
Hand Sanitiser as Backup
When a sink is unavailable, hand sanitiser maintains hygiene. Some children prefer the quick, controlled sensation of gel sanitiser over running water.
E-539 · Nose Blowing
Nose blowing requires closing the mouth completely, directing airflow out through the nostrils, calibrating force, and tolerating tissue on sensitive nasal skin.
- Blow out a candle (oral airflow practice)
- Blow through a straw (directed airflow)
- Blow a cotton ball across a table
- Blow with MOUTH CLOSED — air exits through nose
- Blow tissue held near nose and watch it move
- Blow INTO the tissue — task complete

E-534
Nail Cutting
The most feared grooming task. Nail cutting combines tactile pressure on the most sensitive fingertips in the body, the sharp CLIP sound (sudden auditory stimulus), visual threat of a metal tool near fingers, and a primal anxiety that something is being CUT OFF — all while being required to hold completely still. The amygdala threat response fires simultaneously across three sensory channels.
Desensitisation Sequence
Touch nails → press nails → hold clipper nearby → clipper touches nail → ONE nail cut → gradually more nails per session over weeks.
Strategic Timing
After bath (nails softest), during preferred screen activity, or in deep sleep for the youngest children. Choose the moment of lowest resistance.
Filing as Alternative
Electric nail file produces no clipping sound and applies gentler, more predictable pressure — often far better tolerated than clippers.
One Nail Per Day
Ten days for a complete set. This approach dramatically reduces the anticipatory anxiety of a full nail-cutting session.

E-535
Bath Time
Two Very Different Challenges
Bath time presents opposing profiles. Avoiders experience water as unpredictable tactile input across the entire body simultaneously — overwhelming, threatening, and impossible to escape. Seekers experience the bath as a 45-minute sensory paradise — water play, splashing, pouring — and ending the bath triggers a meltdown from transition and loss of preferred input.
For Avoiders
- Wet cloth → standing in shallow water → sitting → pouring
- Non-slip mat provides physical stability, which creates safety
- Bath toys, bubbles, or colour tablets as motivating additions
- Indian bucket bath may be LESS overwhelming than shower — controlled pouring vs. continuous stream
For Seekers
- Visual timer for bath duration
- 5-minute and 2-minute transition warnings
- Post-bath sensory activity as a bridge to the next routine step
E-537 · Lotion Application
Wet. Cold. Slimy. For tactile-defensive children, lotion is aversive on every sensory dimension: temperature (cold), texture (wet and spreading), coverage (across large body surfaces), and the residual feeling that persists for hours.
Why Lotion Feels Wrong
Light touch receptors fire intensely at the sliding sensation, and the slippery feeling simply does not resolve — ongoing sensory input the nervous system cannot habituate to easily.
Practical Adaptations
- Cream (thicker, less slimy) or gel, spray, or powder — test formats to find tolerance;
- Warm lotion in hands first — eliminates the cold shock entirely;
- Apply with firm, deep pressure rather than light spreading strokes;
- Teach self-application — control over the experience dramatically reduces aversion;
- Indian context: coconut oil and traditional body oils are often better tolerated than commercial lotions due to familiar smell and texture profile.

E-536
Hair Washing
Water over the head. Shampoo in eyes. Suds running down the face. Head tilting backward. Hair washing combines face-wetting aversion (E-533), vestibular disorientation from head tilting, chemical eye sting, and scalp sensitivity (E-530) — making it the single most distressing part of bath time for many ASD children.
Rinse Visor Shield
₹100–200 — creates a physical barrier preventing water from reaching the face. One of the highest-impact, lowest-cost adaptations available.
Tilt Forward Instead of Back
Rinsing into a bowl held in the child's hands, or leaning forward over the tub — eliminates vestibular disorientation and keeps water off the face.
Countdown Before Rinse
"3-2-1-water" gives predictability and eliminates startled responses. Child can also hold a dry cloth over eyes during the rinse.
Indian Context
Weekly coconut oil pre-treatment softens the hair washing experience — oil application is a familiar, calming ritual that also reduces shampoo friction.

E-537
Lotion Application
Why Lotion Feels Wrong
Wet. Cold. Slimy. For tactile-defensive children, lotion is aversive on every sensory dimension: temperature (cold), texture (wet and spreading), coverage (across large body surfaces), and the residual feeling that persists for hours. Light touch receptors fire intensely at the sliding sensation, and the slippery feeling simply does not resolve — ongoing sensory input the nervous system cannot habituate to easily.
Practical Adaptations
- Cream (thicker, less slimy) or gel, spray, or powder — test formats to find tolerance
- Warm lotion in hands first — eliminates the cold shock entirely
- Apply with firm, deep pressure rather than light spreading strokes
- Teach self-application — control over the experience dramatically reduces aversion
- Indian context: coconut oil and traditional body oils are often better tolerated than commercial lotions due to familiar smell and texture profile

E-538
Hand Washing
Beyond post-toilet handwashing (E-519), this technique focuses on generalised hand hygiene across all contexts — before meals, after outdoor play, after touching animals, when hands are visibly dirty. The skill may already exist, but it must be extended across environments and made automatic through habit architecture rather than repeated adult prompting.
Context-Specific Visual Reminders
Handwashing trigger visuals posted in the kitchen (before meals), at the back door (after outdoor play), and near the pet area. The visual does the prompting — the adult steps back.
Sensory-Friendly Soap
Test preferred texture (bar vs. foam vs. gel), preferred temperature, and unscented vs. mild scent. The right product removes the sensory barrier to compliance.
Hand Sanitiser as Backup
When a sink is unavailable, hand sanitiser maintains hygiene. Some children actually prefer the quick, controlled sensation of gel sanitiser over running water.

E-539
Nose Blowing
A Surprisingly Complex Skill
Nose blowing requires closing the mouth completely, directing airflow out through the nostrils (most air naturally exits through the mouth), calibrating force (enough to expel mucus, not enough to hurt ears), managing one nostril at a time, and tolerating the tactile sensation of tissue on sensitive nasal skin. Most ASD children learn this years after their peers and benefit from explicit, scaffolded teaching.
Precursor Activity Progression
- Blow out a candle (oral airflow practice)
- Blow through a straw (directed airflow)
- Blow a cotton ball across a table
- Blow with MOUTH CLOSED — air exits through nose
- Blow tissue held near nose and watch it move
- Blow INTO the tissue — task complete
Mirror practice lets the child see breath fog. Soft tissues and wet wipes are effective for building tissue tolerance before the full blowing task.

Section 3 of 4 · Routines & Methods
E-540
Morning Routine
Wake up. Toilet. Wash face. Brush teeth. Get dressed. Eat breakfast. Pack bag. Shoes on. Leave. Nine or more steps, every morning, under time pressure — the daily executive function test. The morning routine demands arousal regulation, sequential execution, motor planning for multiple tasks, time awareness, and smooth transitions between tasks. All of this with reduced prefrontal cortex function (mornings represent the lowest cortisol point and the slowest PFC activation of the day).
Visual Morning Schedule
Photo-based, posted at child eye-height in the bedroom and bathroom. The child moves a marker through each step. The schedule is the prompt — not the parent.
Same Order Every Day
The basal ganglia automates repeated sequences. Identical order = reduced cognitive load = fewer meltdowns over time.
Prepare the Night Before
Clothes laid out, bag packed, lunch ready. Every decision removed from the depleted morning brain.
Reinforce Independent Completion
Celebrate the days the routine runs without prompting. The reinforcer for completing independently matters more than any individual step.

E-541
Bedtime Routine
Self-Care at End of Day
This card focuses on the SELF-CARE components embedded in the bedtime routine: undressing, pyjamas, toilet, teeth, and face wash. End-of-day executive function is at its absolute lowest — depleted by a full day of regulation. The bedtime self-care sequence must be simple enough to execute on severely diminished cognitive reserves, and automated enough that it runs on habit rather than willpower.
Bedtime Self-Care Sequence
- Undress and place clothes in laundry
- Put on pyjamas
- Toilet visit
- Brush teeth
- Wash face
- Into bed — transition to sleep routine (E-449)
A separate visual schedule for bedtime self-care (distinct from the sleep routine visual) maintains clarity. Build independence backward — one step at a time using backward chaining on depleted reserves.

E-543
Task Analysis
Method Card #1. Task analysis — breaking any complex task into its smallest individually teachable steps — is the FOUNDATION of all self-care teaching in ASD. Without it, you are asking a child to execute something they cannot visualise, sequence, or plan. With it, you transform an impossible task into a series of achievable moments.
Example — "Put on shirt": (1) Pick up shirt (2) Find tag/back (3) Hold bottom opening (4) Put head through (5) Pull down (6) Find right sleeve (7) Push right arm through (8) Find left sleeve (9) Push left arm through (10) Pull down to waist. What looks like one action is actually ten.
Do the Task Yourself First
Perform the task slowly and narrate every micro-movement. This reveals steps that are automatic for adults but must be explicitly taught to the child.
Create a Visual Task Analysis
Photograph your child performing each step. Child-specific photos are significantly more effective than generic clip art or illustrations.
Test and Adjust
If the child fails a step consistently, it is too large. Break it into smaller sub-steps. The task analysis is a living document, not a fixed template.
E-544
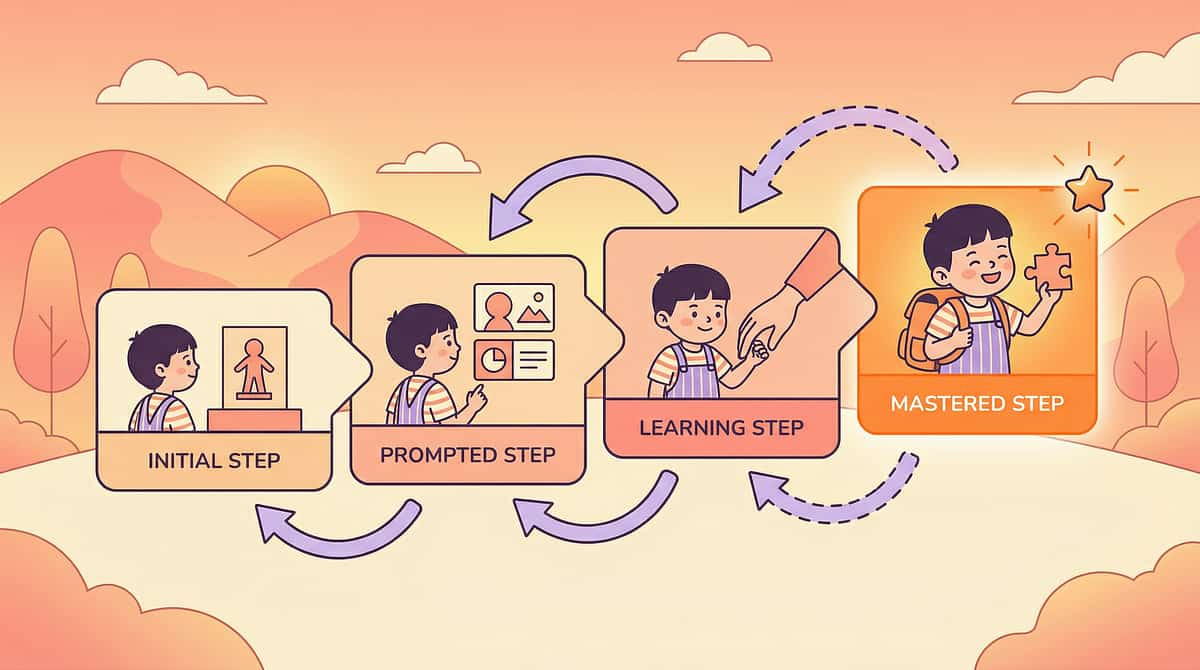
Backward Chaining
Method Card #2
Backward chaining is the gold standard for most ASD self-care skills. The parent completes ALL steps except the last one → the child does the LAST step → SUCCESS. The child experiences task completion from the very first teaching session. Completion activates the reward system (nucleus accumbens). Every session ends with the child having finished the task — building a powerfully positive association with the activity.
Toothbrushing Example
- Parent brushes entire mouth → child does ONE final brush and spits → reinforce
- Parent brushes most → child does last 5 seconds and spits → reinforce
- Parent brushes first half → child completes second half → reinforce
- Child brushes entire mouth independently
Common Mistakes
Fading too fast is the most frequent error. Each step must be fully mastered — consistently independent across multiple sessions — before adding the previous step. Track data: which steps are independent, which are prompted.
E-545 · Forward Chaining
Forward chaining inverts the sequence: the child does the FIRST step independently → the parent completes the rest. Then the child does the first TWO steps → parent completes. Building from beginning to end. Forward chaining works best when the first step is the easiest, the task builds in complexity from start to finish, or the child is motivated by INITIATING rather than completing.
Best Fit: Forward
Tasks where the first step is easiest and initiation is the motivator — e.g., putting on shoes (step in first, then parent fastens).
Best Fit: Backward
Tasks where completion is the motivator and the ending feels most rewarding — e.g., pulling a shirt fully down, spitting after brushing.
Combining Both
Some tasks benefit from teaching both the first AND last steps, then meeting in the middle. Match the method to the child's motivational profile and the task's natural shape.
E-546
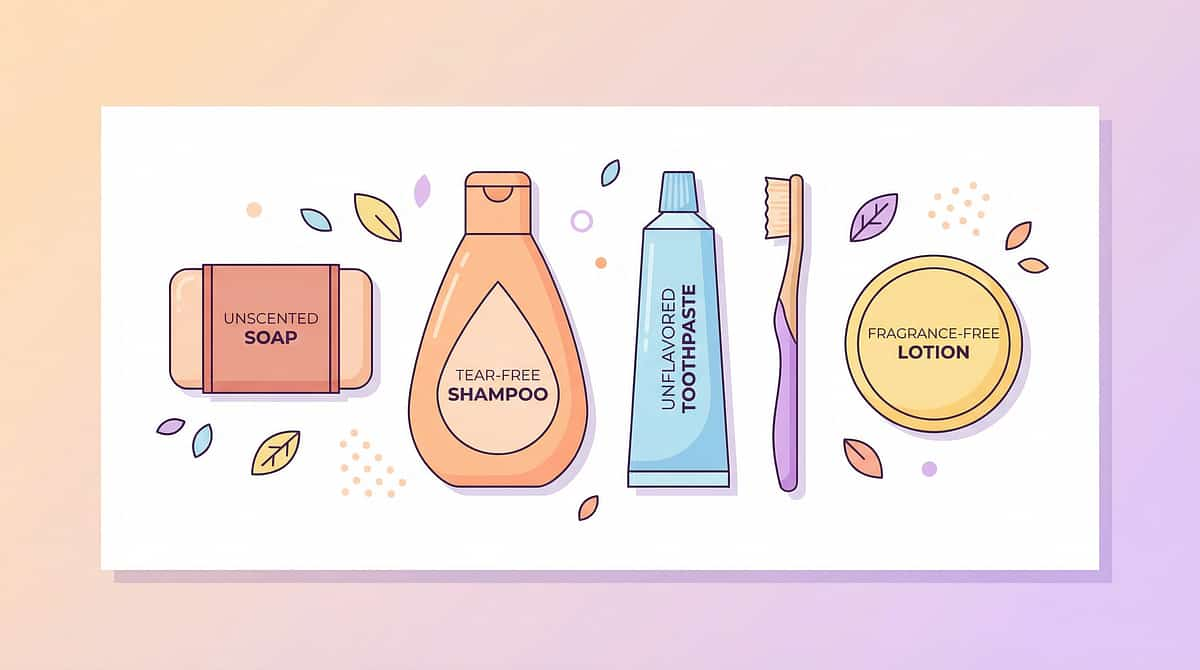
Sensory-Friendly Products
Commercial grooming products are engineered for neurotypical sensory systems. For ASD children, strong fragrances trigger olfactory assault, mint and chemical tastes create oral burning, foaming agents produce tactile overwhelm, and cold application creates temperature shock. Sensory-friendly product alternatives reduce the sensory load of the product itself — so that the SKILL can be learned without the product itself being the barrier.
Toothpaste
Unflavoured → mild fruit → training paste (no fluoride, safe to swallow initially). Indian options: Himalaya children's, Meswak, herbal formulations.
Soap & Shampoo
Unscented bar or liquid soap. Tear-free, unscented shampoo or conditioner-only washing method. Test foam vs. gel format for tactile preference.
Lotion & Sunscreen
Cream vs. gel vs. spray vs. powder for lotion. Sunscreen stick (no spreading) or mineral spray. Eliminate the spreading sensation entirely when possible.
Deodorant
Unscented only. Roll-on vs. spray format test. Introduced at puberty onset with clear task analysis and reinforcement (see E-549 for full programme).
Section 4 of 4 · Adaptive & Advanced
E-547
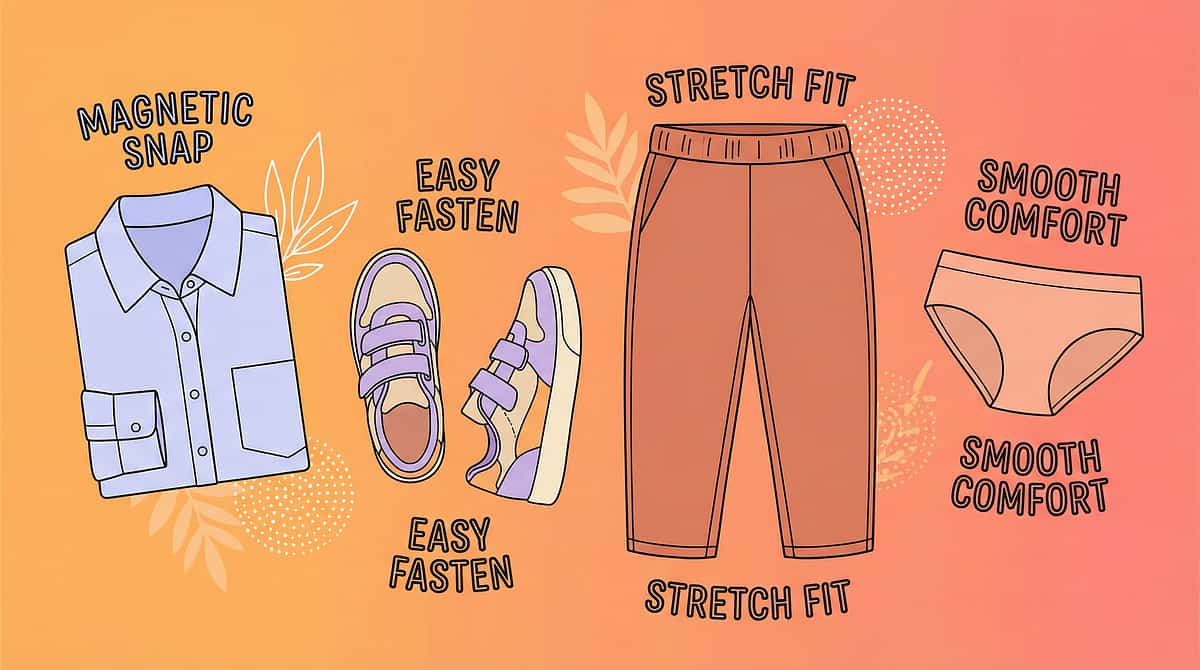
Adaptive Clothing
When standard clothing is the barrier to independence, adaptive clothing IS the solution — not a workaround, not a compromise, but the evidence-based engineering of garments to enable the independence that standard design prevents. Adapting the clothing is not giving up. It is building the conditions for success.
Adaptive Closures
Magnetic buttons look identical to regular buttons but require a fraction of the fine motor precision. Velcro sewn over buttons. Elastic waistbands replacing belt buckles. Pull-on shoes. Available in India: magnetic button retrofits ₹200–500.
Sensory-Adaptive Fabrics
Seamless, tagless, compression-fit, flat-seam underwear. Clothing engineered to eliminate the tactile features that generate distress — addressing E-527 at the garment level.
School Uniform Adaptations
A formal letter to school requesting adaptive uniform accommodations — documented, professional, and supported by occupational therapy assessment. Most schools in India will comply when properly approached.

E-548
Visual Routine Schedules
The Most Effective Independence Tool
Visual routine schedules — photo-based, laminated, posted at child eye-height in the relevant location — are the single most effective tool for self-care independence across all of ASD research. When the schedule is mastered, it replaces the parent as the instruction-giver. The child reads the wall. The parent steps back. Independence happens.
Why Visuals Work
They leverage ASD visual processing strengths, provide external working memory, support sequencing, enable self-prompting, and deliver the predictability the nervous system craves.
Creating Effective Schedules
- Use photos of YOUR child performing each step — most effective by far
- Laminate and mount at the child's eye height, in the exact location the task occurs
- Child physically moves a marker or checks off each completed step
- One dedicated schedule per routine: morning, bathroom, bedtime
- App-based schedules available for older children who use tablets
Fading Timeline
Visual schedule → mental checklist over months or years. The schedule may be needed long-term — this is entirely fine and represents successful independent functioning.

E-549
Grooming for Older Kids
Puberty arrives and the grooming stakes multiply dramatically. Body odour. Acne. Menstruation. Shaving. Body hair. The 12-year-old who doesn't use deodorant is socially excluded. The teenager who cannot manage menstrual hygiene loses school attendance. Age-appropriate grooming is not vanity — it is a social survival skill with direct consequences for peer inclusion, academic participation, and mental health.
Deodorant
Build into post-bath visual routine. Test stick vs. roll-on vs. spray for sensory tolerance. Unscented only to start. Introduce before body odour becomes a social issue.
Acne Management
Simple two-step routine: wash and moisturise. Introduce during morning face wash. Dermatologist involvement when needed — do not let skin conditions escalate without professional support.
Shaving
Electric razor is significantly safer and far less sensorially intense than a blade. Task analyse every step. Practice on arm before face — lower stakes, builds confidence and motor pattern.
Menstrual Hygiene
Full task analysis for pad use. Cycle tracking with visual calendar. School management kit (spare pads, bag, protocol). Teach before first period — preparation eliminates crisis.

E-550
Self-Care Motivation
The capstone of Subdomain E3. They CAN do it — they've been taught every skill. But they WON'T do it unless prompted. Every single time. Motivation is the gap between CAPABILITY and INDEPENDENCE. Closing this gap — making self-care truly self-initiated — is the final frontier of dressing and grooming intervention.
The Neuroscience of the Gap
Self-care motivation requires three converging factors: internal drive (social awareness of why grooming matters), habit formation (basal ganglia automation — the routine runs without conscious decision), and positive reinforcement history (self-care has been associated with good outcomes rather than battles and stress). All three must be actively built.
Closing the Gap
- Reinforce independent initiation, not just completion — "You started getting dressed WITHOUT me asking!" is the most powerful praise
- Self-monitoring checklists: child tracks own daily completion
- Premack principle: "When you're dressed, we go to the park"
- Fade verbal prompts → visual only → fully self-initiated over time
- For older children: peer motivation — wanting to look and feel like peers
Visual Schedule System
Social Stories
Reward Charts
Visual Timer
Calm-Down Kit
Emotion Cards
Lead:🤲 OT (Motor/Sensory) · 📋 ABA (Motivation/Chaining) | SpEd · NeuroDev · Psychology
Preview of dressing grooming Therapy Material
Below is a visual preview of dressing grooming therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!

The Independence Principle
Every skill a child learns independently is a skill a caregiver no longer has to provide. Self-care independence is not just about the child — it reduces caregiver burden, builds the child's self-esteem, enables full school participation, and lays the foundation for adult independence. The distance between parent and child at the mirror IS the measure of progress.
E-542 · Building Self-Care Independence
The master independence card. Bringing together every dressing and grooming skill into a comprehensive programme — the goal being a child who can manage their own body with minimal or no adult assistance. Self-care independence is the visible output of motor planning maturation, sensory tolerance development, executive function growth, and self-monitoring capacity converging over time.
20%
Full Assist
Adult completes the entire task.
40%
Partial Assist
Child and adult share the steps.
60%
Verbal Prompt Only
Adult cues each step verbally.
80%
Visual Prompt Only
Schedule does the cueing.
100%
Independent
Child self-initiates and completes.
2-4
Years Behind
Average self-care delay in ASD compared to neurotypical peers — not a measure of intelligence
30
Techniques
Evidence-based interventions across Subdomain E3 — one for every challenge in dressing and grooming
21M+
Sessions
Pinnacle Blooms Network® clinical experience powering every technique in this library