
Every Behavior Is Communication. Your Child Is Telling You Something.
Your child isn't being "bad." Their behavior is the loudest language they have.
The hitting that comes from nowhere. The head-banging that terrifies you. The running away the moment you look away. The endless lining up of objects for hours. The screaming that fills every public space. Behind every challenging behavior is a function — a need being expressed through the only channel available. Understanding that function is the first step to transformation.
You are about to access 110+ clinically validated behavior intervention techniques — each designed for home implementation, evidence-graded, and developed by the world's largest pediatric therapy consortium.
🏥 India's #1 Autism Therapy Chain
70+ Centers | 21M+ Sessions
97%+ Measured Improvement

You Are Not Alone — The Numbers Speak
Challenging behavior is one of the most common — and most exhausting — experiences for families raising a child with autism or a developmental difference. Research confirms what you already know: you are far from alone.
94%
Experience Challenging Behavior
of parents of children with ASD report at least one form of challenging behavior — Research in Autism Spectrum Disorders, 2023
50-70%
Exhibit Aggressive Behaviors
exhibit aggressive behaviors at some point during childhood — Journal of Applied Behavior Analysis, 2022
30%
Require Structured Intervention
engage in self-injurious behavior requiring structured, professional intervention — Systematic Review, 2021
These numbers aren't meant to overwhelm — they are meant to reassure. Every one of these families found a path forward. So will you.
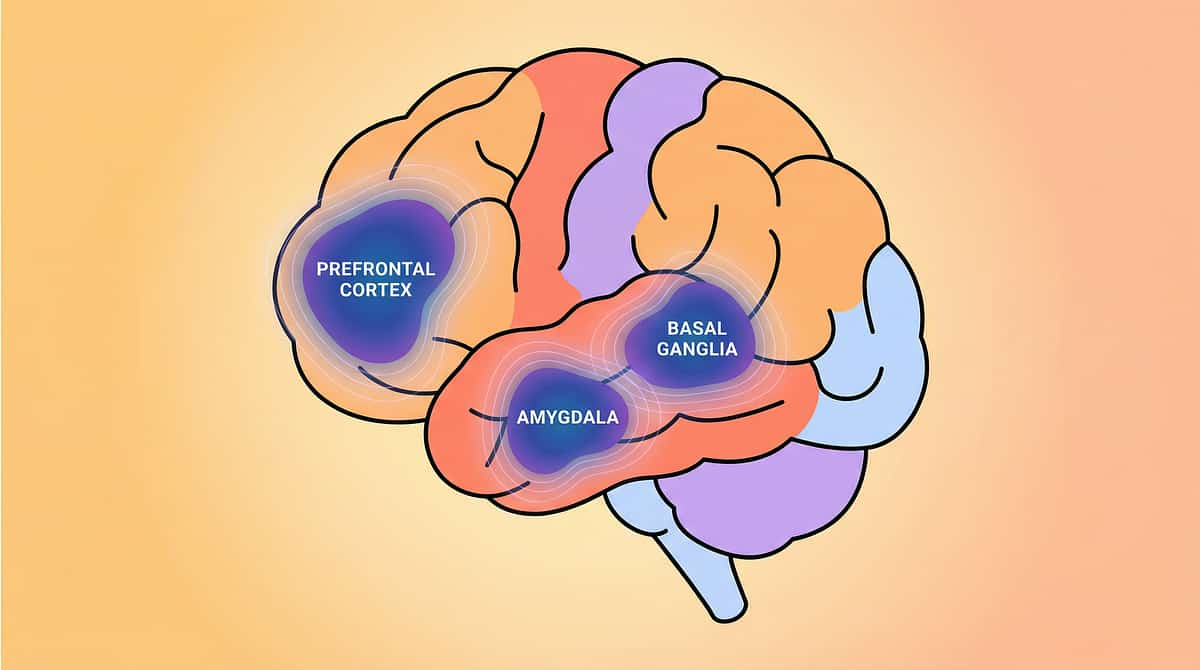
The Behavior Brain — Decoded for Parents
Every challenging behavior your child shows is rooted in neurology, not defiance. Understanding the brain regions involved transforms how you see — and respond to — your child's most difficult moments.
The EATS Model — The Function Equation
Every behavior serves one of 4 functions: Escape, Attention, Tangible, or Sensory. Your child's challenging behavior isn't random — it's a strategy that works for them, even when it doesn't work for you.
The Prefrontal Cortex — The Impulse Brake
Controls impulse inhibition, planning, and consequence evaluation. In autism, maturation may follow a different timeline. When this brake is underdeveloped, children act on impulse before considering outcomes.
The Basal Ganglia — The Habit Engine
Drives repetitive behaviors and routine patterns. Stimming, ritualistic behaviors, and insistence on sameness originate here — neurological patterns providing regulation and predictability, not conscious choices.
The Amygdala — The Threat Detector
Triggers fight-or-flight when the child feels threatened, overwhelmed, or unable to communicate. Most aggressive behaviors are fear-based, not malice-based.
The Reward Circuitry — The Motivator
Dopamine-driven learning determines which behaviors get repeated. If hitting produces escape from a demand, the brain logs: "Hitting = effective strategy." Understanding this circuit is how we replace behaviors without ignoring the need.
This is brain architecture, not bad character. Your child is solving problems with the tools they have. Your job — with our guidance — is to give them better tools.
Evidence: ABA foundational literature | PMC8234840 | BACB Ethics & Standards

Clinically Validated. Globally Recognized. Home-Applicable.
The techniques in this library aren't drawn from opinion or anecdote — they represent the gold standard of behavioral science, graded by evidence level and adapted for home implementation by a multi-disciplinary consortium.
Level I — ABA Evidence Base
Applied Behavior Analysis has the largest and most rigorous evidence base of any autism intervention, spanning 50+ years. NCAEP (2020) classifies FBA, FCT, antecedent-based interventions, reinforcement, extinction, differential reinforcement, self-management, and response interruption as evidence-based.
Positive Behavioral Supports (PBS)
Endorsed by the WHO for community-based implementation, PBS provides the overarching framework of prevention over punishment — building environments where challenging behavior is less likely to occur.
Parent-Implemented Intervention
Systematic reviews confirm that parents trained in ABA principles achieve behavior reduction outcomes comparable to clinical implementation for most challenging behaviors — making home-based programs powerful and proven.
Indian Context
BCBA-supervised programs across Pinnacle centers demonstrate significant behavior reduction with culturally adapted, function-based interventions validated for Indian family environments.
References: NCAEP 2020 | BACB Standards 5th Ed | PMC8234840 | WHO mhGAP Guidelines | Cochrane Review: Early Intensive Behavioral Intervention
6 Subdomains. 110 Techniques. Evidence-Based. Home-Executable.
Domain D: Behavior is organized into six focused subdomains, each addressing a distinct cluster of challenges. Every technique is ordered from foundational to advanced — so you always know where to start.
🔍 Understanding & Preventing Behavior
20 Techniques | Reels D-341 to D-360
Identify triggers, decode functions, and build environments where behavior challenges are less likely to occur.
🔄 Stimming & Repetitive Behaviors
20 Techniques | Reels D-361 to D-380
Understand, redirect, and channel repetitive behaviors into functional, regulated alternatives.
👊 Aggression Toward Others
20 Techniques | Reels D-381 to D-400
Reduce hitting, biting, and aggressive outbursts through functional communication and de-escalation.
⚠️ Self-Injurious Behavior
15 Techniques | Reels D-401 to D-415
Address head-banging, self-biting, and other self-harm with safety-first, function-based strategies.
🚨 Other Challenging Behaviors
25 Techniques | Reels D-416 to D-440
Tackle property destruction, elopement, tantrums, noncompliance, and more with targeted protocols.
💤 Attention and Sleep
10 Techniques | Reels D-441 to D-450
Build focus, reduce impulsivity, and establish the sleep routines that make all other progress possible.

Subdomain D1
20 Techniques | D-341 to D-360
🔍 Understanding & Preventing Behavior
You've tried everything — changing your tone, adjusting the routine, offering choices — but the meltdown still comes. You can see it building in your child's eyes, but you don't know how to stop it. You replay the day wondering: What was the trigger? What did I miss? The exhaustion isn't just physical — it's the weight of not knowing, of feeling one step behind a behavior you can't decode. Beneath this, your child's nervous system is responding to environmental demands that exceed their current regulation capacity. The behavior is the signal, not the problem.
This subdomain gives you the science of why behaviors occur and the practical tools to prevent them before they escalate. When you understand the function driving a behavior, you become your child's most powerful intervention.
Techniques Covered in This Subdomain:
- Functional Behavior Assessment (FBA) — identifying the ABCs (Antecedent–Behavior–Consequence)
- Antecedent modification and environmental arrangement
- Proactive visual schedules and first-then boards
- Behavior prediction using the EATS model (Escape, Attention, Tangible, Sensory)
- Trigger identification and mitigation protocols
- Priming strategies for transitions and demand introduction
- Reinforcement mapping and preference assessments
- Behavior Intervention Plan (BIP) fundamentals for home
- Proactive communication supports before escalation
- Data collection for pattern recognition
Lead Discipline: ABA (BCBA)
Supporting: OT · SLP · SpEd · NeuroDev
Subdomain D2
20 Techniques | D-361 to D-380
🔄 Stimming & Repetitive Behaviors
He spins the same toy wheel for forty minutes. She flaps her hands when excited, distressed, or simply present. He repeats the same phrase, the same question, the same scene from a movie — hundreds of times a day. You worry what it looks like in public. You wonder if stopping it is the right thing, or if that makes it worse. You feel torn between acceptance and intervention, unsure where the line is. The truth is that stimming and repetitive behaviors are neurological self-regulation — the basal ganglia producing predictable, sensory-rewarding patterns that help the child's nervous system achieve equilibrium. They are not meaningless, and they are not permanent without support.
This subdomain helps you understand when stimming is adaptive, when it interferes, and exactly how to redirect or replace it with functional, socially flexible alternatives — without shame or suppression.
Techniques Covered in This Subdomain:
- Sensory reinforcement profiling — identifying the sensory input driving the stim
- Non-contingent reinforcement (NCR) to reduce stim-driven behavior
- Response Interruption and Redirection (RIRD) protocols
- Competing stimulation and replacement behavior training
- Structured stim breaks within daily routine
- Sensory diet integration with OT guidance
- Vocal and motor stim differentiation and intervention
- Echolalia — functional vs. non-functional and intervention pathways
- Perseverative speech reduction strategies
- Social acceptability training for flexible stim management
Lead Discipline: ABA (BCBA)
Supporting: OT · SLP · SpEd · NeuroDev

Subdomain D3
20 Techniques | D-381 to D-400
👊 Aggression Toward Others
The bite marks on your arm. The scratches on your face. The moment your child lunged at their sibling — and the look on their sibling's face afterward. You love your child completely and unconditionally, and you are also frightened, exhausted, and ashamed to admit how hard this is. You've stopped going to certain places. You've started managing every interaction to prevent the next explosion. You are not failing as a parent — you are managing a child whose amygdala is firing in threat-response mode before their prefrontal cortex can intervene. Aggression is almost always fear, overwhelm, or communication failure — rarely anger for its own sake.
This subdomain equips you with evidence-based, safety-first strategies to reduce aggressive behavior systematically — without physical punishment, without shame, and with measurable outcomes.
Techniques Covered in This Subdomain:
- Functional Communication Training (FCT) as the primary replacement pathway
- Crisis de-escalation protocols for in-the-moment aggression
- Antecedent-based demand modification and predictability building
- Differential Reinforcement of Other Behavior (DRO)
- Differential Reinforcement of Incompatible Behavior (DRI)
- Safe physical redirection and protective positioning
- Emotion regulation pre-teaching using visual tools
- Token economy systems for positive behavior building
- Environmental restructuring to reduce aggression triggers
- Sibling and caregiver safety protocols
Lead Discipline: ABA (BCBA)
Supporting: OT · SLP · SpEd · NeuroDev

Subdomain D4
15 Techniques | D-401 to D-415
⚠️ Self-Injurious Behavior
Watching your child bang their head against the wall or floor is one of the most terrifying experiences a parent can face. The bruises. The moments where you throw yourself between your child and a hard surface. The way time slows down and your heart stops. You've been told "they won't really hurt themselves" — but you've seen the marks, and you don't believe it. You are right to take this seriously. Self-injurious behavior (SIB) is most commonly driven by sensory-seeking (the impact produces neurological input the child craves), escape from demands, or social communication when no other channel is available — but it requires structured, supervised intervention.
This subdomain provides the most carefully graded, safety-first protocols in the entire behavior library — designed to reduce SIB while identifying and honoring the underlying need.
Techniques Covered in This Subdomain:
- Medical ruling-out protocol — pain sources, GI, ear infection, sensory thresholds
- SIB function assessment — sensory automatic vs. socially mediated
- Non-contingent sensory reinforcement for automatic SIB
- Protective equipment use without inadvertent reinforcement
- Functional Communication Training as SIB replacement
- Response blocking with redirection — safe, systematic protocols
- Sensory alternative provision — crash pads, proprioceptive input
- Environmental modification to reduce high-risk opportunities
- Extinction protocols with safety modifications
- Crisis escalation pathway and when to seek immediate help
⚠️ If your child's SIB is escalating in frequency, intensity, or duration, or if injury is occurring, contact Pinnacle's clinical helpline at 9100 181 181 before implementing any protocol independently.
Lead Discipline: ABA (BCBA)
Supporting: OT · NeuroDev · SpEd

Subdomain D5
25 Techniques | D-416 to D-440
🚨 Other Challenging Behaviors
He runs out the front door the moment it opens. She tears apart everything on the shelf during a tantrum. He refuses every transition, every request, every "no" — with an explosion that lasts an hour. She destroys her schoolwork the moment she makes an error. These behaviors don't fit neatly into aggression or self-injury — but they are just as disruptive, just as exhausting, and just as isolating. They represent your child's most creative — if destructive — problem-solving strategies. Each one has a function. Each one has an evidence-based response.
With the largest technique count of any subdomain, this library addresses the full spectrum of challenging behaviors not covered elsewhere — from elopement to noncompliance to property destruction — with the same clinical rigor applied across the entire domain.
Techniques Covered in This Subdomain:
- Elopement prevention — environmental, behavioral, and communication-based strategies
- Tantrum management using structured extinction and reinforcement
- Noncompliance reduction through demand fading and choice-making
- Property destruction — FBA-based replacement behavior training
- Food refusal and mealtime behavior protocols
- Toileting-related behavior challenges
- Public behavior — preparation, priming, and community access protocols
- Pica — ingestion of non-food items, safety and intervention
- Task refusal and work avoidance in structured settings
- Separation anxiety behaviors and transition resistance
Lead Discipline: ABA (BCBA)
Supporting: OT · SLP · SpEd · NeuroDev

Subdomain D6
10 Techniques | D-441 to D-450
💤 Attention and Sleep
He can't sit for more than 30 seconds — not for meals, not for therapy, not for a story. She hasn't slept through the night in three years. You survive on fragmented rest and fractured focus, and you know that everything else — the progress, the learning, the emotional regulation — depends on foundations that simply aren't there yet. Attention and sleep are not peripheral to behavior management: they are the biological bedrock on which every other intervention rests. When sleep is disrupted and sustained attention is impossible, every challenging behavior becomes harder to manage and every skill is harder to acquire.
This subdomain targets the two most foundational regulatory systems — sustained attention and sleep architecture — with behavioral protocols that have been validated for use with children with ASD and related developmental differences.
Techniques Covered in This Subdomain:
- Attention building through structured reinforcement schedules
- Graduated attention span extension protocols
- Sleep hygiene behavioral routines — consistent schedule, environment cues
- Bedtime fading and sleep restriction protocols
- Night-waking behavioral response protocols
- Sensory sleep environment modifications
- Visual bedtime routine supports
- Co-sleeping transition protocols
- Impulse control pre-teaching for attention regulation
- Melatonin coordination with behavioral protocols (medical consultation required)
Lead Discipline: ABA (BCBA)
Supporting: OT · NeuroDev · SLP
Domain D: Behavior — Complete Subdomain Index
Use this index to navigate directly to any subdomain. Techniques are ordered from foundational to advanced within each subdomain — start with the first technique in your chosen area.
# | Subdomain | Techniques | Reel Range | Link | |
D1 | Understanding & Preventing Behavior | 20 | D-341 to D-360 | ||
D2 | Stimming & Repetitive Behaviors | 20 | D-361 to D-380 | ||
D3 | Aggression Toward Others | 20 | D-381 to D-400 | ||
D4 | Self-Injurious Behavior | 15 | D-401 to D-415 | ||
D5 | Other Challenging Behaviors | 25 | D-416 to D-440 | ||
D6 | Attention and Sleep | 10 | D-441 to D-450 | ||
Total | All Behavior Subdomains | 110 | D-341 to D-450 |
Behavior Connects Across the Developmental Spectrum
Domain D: Behavior does not exist in isolation. Challenging behaviors are both influenced by — and directly influence — every other area of your child's development. Effective intervention means understanding these connections.
Domain A: Sensory Processing → Behavior
Sensory over- or under-responsivity is one of the most common drivers of challenging behavior. A child who hits because a sound is overwhelming needs sensory support, not just a behavior plan. Sensory and behavior interventions must be co-designed.
Domain B: Communication → Behavior
The most powerful behavior intervention is often a communication one. When a child cannot express needs, discomfort, or preferences verbally or via AAC, behavior becomes the default language. Functional Communication Training bridges this gap directly.
Domain C: Social-Emotional Development → Behavior
Emotional regulation deficits directly amplify behavioral challenges. A child who cannot identify, tolerate, or express emotions will express them through behavior. Social-emotional and behavioral programming must be explicitly linked.
Domain E: Daily Living Skills → Behavior
Behavioral challenges most frequently cluster around transitions and daily routines — getting dressed, mealtimes, bathing, bedtime. Building daily living skills reduces the demand load that triggers behavioral escalation.
Domain H: School & Academic → Behavior
Task avoidance, noncompliance, and classroom aggression are frequently escape-motivated behaviors driven by academic demands that exceed the child's current skill level. Behavior plans must account for curriculum accommodation.
Domain K: Family & Caregiver Support → Behavior
Caregiver burnout, inconsistent implementation, and family stress are among the most significant predictors of behavior intervention failure. Family well-being is not separate from the child's progress — it is foundational to it.

Drafted by a Multi-Disciplinary Consortium
No single discipline can address the full complexity of behavioral challenges in autism. Every technique in this library was reviewed, graded, and validated by specialists across six disciplines — ensuring that clinical rigor, safety, and real-world applicability are built in from the ground up.
Clinical Research Organization (CRO)
Evidence grading, systematic review analysis, PubMed citation mapping, and regulatory compliance across all 110+ techniques.
NeuroDevelopmental Pediatricians
Neurological pathway validation, medical safety review, comorbidity management, and pharmacological interaction screening.
Occupational Therapists (OT)
Sensory-motor integration, environmental modification, daily living skill protocols, and sensory diet design.
Speech-Language Pathologists (SLP)
Communication integration, AAC protocol design, functional communication training, and social communication support.
Board Certified Behavior Analysts (BCBA)
Functional behavior assessment, data-driven programming, reinforcement system design, and extinction protocol safety.
Special Educators (SpEd)
Academic integration, IEP and IFSP goal mapping, structured teaching, inclusion strategy design, and classroom behavior support.

About Pinnacle Blooms Network®
India's Largest Autism & Child Development Therapy Ecosystem
Founded by Dr. Koti Reddy Saripalli — technology pioneer (India's first Java Community Process member, Asia's first Microsoft Certified Solution Developer) who pivoted to pediatric healthcare after his own son's misdiagnosis. A system built from a father's love and an engineer's precision.
70+
Therapy Centers
Across India, with 500+ licensed therapists
21M+
Therapy Sessions
~70 clinical data points documented per session
97%+
Improvement Rate
Measured via AbilityScore® across enrolled families
70+
Countries Served
Families from across the globe trust Pinnacle
Mission: Empowering 900 million kids, parents and families worldwide to be self-sufficient and part of the mainstream world.
GPT-OS® — The World's First Pediatric Therapeutic Operating System
SaMD under CDSCO
13+ Patents (IPO & WIPO)
ISO 13485:2016
ISO/IEC 27001:2022
Layer 1: AbilityScore®
Universal 0–1000 developmental metric across 400+ data points and 25 gold-standard assessments. A single number that captures your child's complete developmental profile.
Layer 2: TherapeuticAI®
21M+ sessions and 1.47B data points powering personalized intervention intelligence. The largest pediatric therapy dataset in the world, working for your child.
Layer 3: Personal Development Kernel (PDK)
A living developmental profile for your child — continuously updated as skills emerge, behaviors shift, and contexts change.
Layer 4: Everyday Therapy Program (ETP)
9 goals + 9 techniques per session, personalized daily for your child's current profile and home environment.
For Behavior, GPT-OS® delivers:
- 🎯 Behavior profile mapping across all 6 subdomains
- 📊 Technique recommendation based on profile, age, and available materials
- 📈 Week-by-week progress tracking calibrated to evidence-based timelines
- 🔄 Adaptive pathway adjustment as your child progresses

Core Therapy Materials for Behavior Interventions
Every technique page in Domain D references specific materials that support implementation. These Canon Materials are curated for clinical relevance, home accessibility, and alignment with evidence-based protocols.
Material | Primary Use in Behavior Intervention | Catalogue | |
Visual Schedule Board (Daily Routine) | Antecedent modification, predictability building, transition management | ||
First-Then Visual Card | Demand compliance, motivation, noncompliance reduction | ||
Emotion Regulation Cards | Pre-teaching emotional states, de-escalation, aggression prevention | ||
Token Board & Reinforcement System | Positive behavior reinforcement, token economy implementation | ||
Sensory Break Kit (Proprioceptive Tools) | Stimming alternatives, SIB sensory replacement, regulation support | ||
Bedtime Visual Routine Strip | Sleep behavior protocols, bedtime resistance reduction | ||
Behavior Data Collection Sheet | ABC recording, FBA data, progress monitoring | ||
Communication Board (Basic Needs) | Functional Communication Training, aggression/SIB replacement | ||
Transition Warning Timer (Visual) | Elopement prevention, transition resistance, tantrum reduction | ||
Weighted Sensory Tools | Self-regulation support, stimming management, sleep readiness |

⚠️ Safety First — Behavior Intervention Red Flags: The following signs require immediate professional consultation before continuing any home intervention.
⚠️ Safety First — Behavior Intervention Red Flags
🔴 Escalating Self-Injury with Physical Harm
If head-banging, self-biting, or skin-picking results in visible injury, bruising, or bleeding — or is increasing in frequency and force — do not manage this independently. Immediate clinical assessment is required.
🔴 Aggression Resulting in Injury to Others
If your child's aggressive behavior causes injury to siblings, caregivers, or peers — bites that break skin, scratches requiring treatment, or pushing that results in falls — escalate to in-person consultation immediately.
🔴 Pica — Ingestion of Non-Food Items
Any ingestion of non-food materials (dirt, paint, paper, clothing, small objects) is a medical emergency risk. Behavior intervention must be coordinated with a physician and a BCBA simultaneously.
🔴 Elopement with Road or Water Access Risk
If your child has run into traffic, toward water, or into unfamiliar environments — or is at risk of doing so — implement environmental safety measures immediately and contact your clinical team before behavioral protocols are introduced.
🔴 Behavioral Regression After Previous Progress
A sudden and significant regression in behavior — especially after a period of clear improvement — may indicate a medical cause (pain, illness, medication change). Rule out medical factors before adjusting behavioral programming.
🔴 Complete Sleep Loss (48+ Hours)
If your child has not slept in 48 or more hours, behavioral sleep protocols alone are insufficient. Medical and neurodevelopmental consultation is required urgently — sleep deprivation compounds every behavioral and regulatory challenge.
Escalation Pathway:
Step 1: Self-Resolve
Pause intervention → ensure physical safety → provide sensory regulation tools → document the incident
Step 2: Teleconsult
Pinnacle National Helpline — 9100 181 181 (16+ languages, 24/7 availability)
Step 3: In-Person
Find your nearest Pinnacle center for urgent clinical review and BIP revision
Your Behavior Intervention Journey — The 12-Week Arc
Evidence-based behavior change follows a predictable trajectory. Understanding this arc helps you stay consistent during the difficult early weeks — when change is happening beneath the surface before it's visible in behavior.
Most families notice the first meaningful shift between weeks 3 and 5 — this is when the brain's reinforcement circuitry begins to register the new behavioral pathway as more effective than the challenging one. Consistency in weeks 1–4 is what makes weeks 8–12 possible. Trust the arc.
What Every Technique Page Delivers
Each of the 110 technique pages follows the Pinnacle 40-Card Narrative Architecture — a clinically structured, parent-accessible format that takes you from recognition to implementation to mastery.
1
Recognition Moment
Your specific daily struggle, written from lived experience — so you know immediately you're in the right place. No clinical jargon. Just your reality, decoded.
2
Neuroscience Explained
What's happening in your child's brain during this behavior — explained in plain language, with the specific brain regions and mechanisms involved.
3
Evidence Grade
Level I–IV evidence grading with PubMed citations, NCAEP classification, and consortium consensus — so you know exactly how well-proven the technique is.
4
Step-by-Step Protocol
10–15 minute daily sessions, written for home implementation. Clear setup, implementation, and response instructions with troubleshooting for the most common obstacles.
5
Materials & Progress
Specific material recommendations with purchase links, progress indicators, safety notes, and a clear progression pathway to the next technique in the sequence.
PubMed-Referenced
WHO/UNICEF-Aligned
Consortium-Drafted
GPT-OS® Integrated

Real Families, Real Outcomes
Behind every technique in this library is a family who needed it. These stories represent thousands more across Pinnacle's network of 70+ centers.
"We finally understood WHY he was hitting."
"Our son's aggression was making every family outing impossible. We were isolating ourselves completely. At Pinnacle, the BCBA helped us do a Functional Behavior Assessment at home — and we discovered every episode was escape-motivated. Within 6 weeks of Functional Communication Training, the hitting reduced by 70%. By week 12, he could say 'I need a break' instead. We had our family back."
— Parent, Pinnacle Blooms Network, Hyderabad
"The head-banging stopped. We still cry when we think about it."
"Our daughter's SIB was the most terrifying thing I have ever experienced as a mother. We were told it was 'attention-seeking' and to ignore it — but we couldn't. The Pinnacle team identified it as sensory-automatic, gave us a proprioceptive replacement protocol and a crash pad, and taught us non-contingent sensory reinforcement. By week 8, incidents had dropped from 15 per day to fewer than 2. Month 3: zero. I cannot describe the relief."
— Parent, Pinnacle Blooms Network, Bengaluru
"Sleep changed everything else."
"My son hadn't slept through the night in four years. Neither had I. Behavior therapy alone wasn't working because we were both too exhausted to implement anything consistently. The Pinnacle sleep protocol — visual routine, bedtime fading, and weighted blanket — got him sleeping 7 hours within 5 weeks. His daytime behaviors improved dramatically within days. I had no idea sleep was this connected to everything."
— Parent, Pinnacle Blooms Network, Chennai
Domain D Research Index — Behavior Evidence Base
Every technique in this library is grounded in peer-reviewed evidence. The following citations represent the foundational research base for Domain D: Behavior interventions.
NCAEP (2020).Systematic Review of Evidence-Based Practices for Autism Spectrum Disorder. National Clearinghouse on Autism Evidence and Practice. Classifies ABA-derived interventions as Level I evidence for behavior challenges in ASD.
Cochrane Collaboration (2018).Early Intensive Behavioral Intervention (EIBI) for Young Children with Autism Spectrum Disorders. PMC6513645. Meta-analysis supporting parent-implemented behavioral intervention efficacy.
Fitzpatrick, S. E. et al. (2023).Prevalence and correlates of challenging behavior in autism spectrum disorder. Research in Autism Spectrum Disorders. Systematic review establishing 94% prevalence of challenging behavior in ASD.
WHO (2018).Nurturing Care Framework for Early Childhood Development. WHO/UNICEF/World Bank. Provides global community-based behavior support framework. PMC9978394.
BACB (2020).Ethics Code for Behavior Analysts, 6th Edition. Behavior Analyst Certification Board. Standards for safe, ethical behavior intervention implementation.
Lakhan, R. (2015).Behavioral interventions for challenging behavior in autism in India: A systematic review. Indian Journal of Psychiatry. PMC4375809. Documents culturally adapted FBA outcomes in Indian pediatric populations.
NICE (2013, updated 2021).Autism Spectrum Disorder in Under 19s: Support and Management. CG170. UK national clinical guidelines for behavior intervention in ASD.
Wacker, D. P. et al. (2013).Conducting Functional Communication Training via Telehealth. PMC3671583. Demonstrates parent-implemented FCT efficacy for behavior reduction in community settings.
Rehabilitation Council of India (RCI).Guidelines for Behavior Management in Persons with Autism and Intellectual Disabilities. Regulatory framework governing behavior intervention practice in India.
IAP (Indian Academy of Pediatrics) (2017).Consensus Statement on ASD Management in Indian Clinical Practice. Endorses ABA-based behavior intervention as primary evidence-based approach for Indian pediatric settings.
Explore All 12 Intervention Domains
Domain D: Behavior is one of twelve interconnected intervention domains in the Pinnacle Blooms Network® library. Each domain contains subdomains, technique pages, and home protocols — all built on the same evidence standards.
Domain | Name | Link | |
A | 🎯 Sensory Processing | ||
B | 🗣️ Communication | ||
C | 💛 Social-Emotional Development | ||
D | 🧩 Behavior | ||
E | 🏠 Daily Living Skills | ||
F | 🏃 Motor Skills | ||
G | 🎮 Play & Cognitive Skills | ||
H | 📚 School & Academic | ||
I | 🔄 Transitions & Life Events | ||
J | 🌍 Community & Outings | ||
K | 👨👩👧 Family & Caregiver Support | ||
L | 🏥 Therapy Implementation |

Why Pinnacle GPT-OS® for Behavior?
There is a meaningful difference between generic advice and a system built on 1.47 billion clinical data points. Here is what that difference looks like in practice.
Dimension | Typical Approach | Pinnacle GPT-OS® | |
Evidence | Single therapist's training and experience | Consortium: CRO + OT + SLP + BCBA + SpEd + NeuroDev | |
Personalization | Generic protocol applied uniformly | AI-mapped profile across all 6 behavior subdomains | |
Continuity | 1–2 hours per week in clinic | 24/7 home protocols + clinic sessions, seamlessly integrated | |
Materials | Whatever happens to be available | Canon Materials with purchase links and implementation protocols | |
Progress | Subjective clinical notes | Data-driven milestones via AbilityScore® (0–1000 scale) | |
Intelligence | Individual therapist's experience | 1.47 billion data points via TherapeuticAI® | |
Improvement | Variable, often unreported | 97%+ measured improvement rate |

For Therapists, Educators & Pediatricians
The Pinnacle behavior library is designed for dual use: parent-accessible home implementation and clinical reference for allied health professionals. Every technique page includes PubMed citations, evidence grades, and protocol fidelity checklists suitable for professional documentation.
IEP/IFSP Integration
Map technique pages directly to behavioral goals in your student's or client's plan. Every subdomain is indexed by functional goal area.
Parent Handouts
Each technique page functions as a shareable parent handout with plain-language instructions, visual supports, and progress monitoring guides.
Research Index
Use the Domain D Research Index for clinical documentation, continuing education, supervision notes, and funding justification.
Professional Training
Pinnacle offers certified professional training, school consultation, and parent training programs delivered by BCBA-supervised clinical teams.
Professional Resources:Teacher Training · Certified Courses · Parent Training · School Training · Careers at Pinnacle

Behavior — Frequently Asked Questions
The questions parents ask most. Answered with the clarity and honesty you deserve.
Can I really do this at home without a therapist present?
Yes — for most challenging behaviors, parent-implemented behavioral interventions have been shown in systematic reviews to produce outcomes comparable to clinician-delivered treatment. Our protocols are specifically designed for home implementation with 10–15 minute daily sessions. For severe behaviors (significant SIB, dangerous elopement, pica), we recommend starting with a telehealth session with a Pinnacle BCBA before implementing independently.
How quickly will I see results?
Most families report early signs of change between weeks 3 and 5 — but behavioral change follows a non-linear path. Expect a possible temporary increase in the challenging behavior during the first 1–2 weeks of intervention (an "extinction burst" — a sign the protocol is working). By week 8, most families see 40–70% reduction. By week 12, behaviors are typically manageable and decreasing. Consistency during the early weeks is the single most important factor in outcomes.
What age range are these techniques suitable for?
The techniques in Domain D are evidence-graded for children aged 18 months through 18 years. Each technique page specifies the appropriate age range, developmental prerequisites, and adaptations for different profiles. Many techniques are also adapted for adults with autism through Pinnacle's adult services pathway.
Where do I start? There are 110 techniques — I'm overwhelmed.
Start with the subdomain that matches your most urgent daily challenge. Within that subdomain, begin with Technique 1 — they are ordered foundational to advanced. You do not need all 110 techniques. Most families effectively implement 5–8 techniques from 2–3 subdomains. Our GPT-OS® assessment will recommend your personalized starting point within minutes.
Where do I get the materials referenced in each technique?
Every technique page links directly to the relevant Canon Materials at materials.pinnacleblooms.org. Materials include visual supports, sensory tools, reinforcement systems, and data collection sheets — all selected for availability in Indian markets and international shipping where applicable. Many techniques can also be started with materials you already have at home.
When should I stop trying at home and seek professional help?
If a behavior poses a safety risk (SIB causing injury, dangerous elopement, pica, or aggression causing injury to others) — seek professional consultation before or alongside home implementation, not instead of it. If you've been implementing consistently for 4 weeks without any observable change, a Functional Behavior Assessment by a BCBA is strongly recommended. Call our helpline: 9100 181 181.
Internationally Aligned. Nationally Regulated. Globally Trusted.
Every technique in the Pinnacle behavior library is developed and maintained in alignment with the world's leading clinical, regulatory, and humanitarian bodies — ensuring that what we recommend meets the highest standards of evidence, ethics, and safety.
Global Clinical Standards
✅ WHO Nurturing Care Framework (2018) · ✅ WHO CCD Package (PMC9978394) · ✅ UNICEF MICS · ✅ NCAEP 2020 · ✅ NICE CG170 · ✅ SIGN Guidelines
Indian Regulatory Compliance
✅ CDSCO SaMD Classification · ✅ Indian Academy of Pediatrics (IAP) · ✅ Rehabilitation Council of India (RCI) · ✅ Rights of Persons with Disabilities Act (RPwD) 2016
Quality & Intellectual Property
✅ ISO 13485:2016 (Medical Devices) · ✅ ISO/IEC 27001:2022 (Information Security) · ✅ 13+ Patents filed with IPO & WIPO · ✅ BACB Ethics Standards
CIN: U85110TG2019PTC132498 | Bharath Healthcare Laboratories Pvt Ltd
Start Your Child's Behavior Journey — Now
You don't need to have everything figured out. You don't need to start with all 110 techniques. You need one next step — and here it is.
Step 1: Identify Your Starting Point
Identify the behavior challenge causing the most daily disruption. Scroll up to the 6 subdomain cards and find the one that matches your child's most pressing need. That is your entry point.
Step 2: Enter Your Subdomain
Enter your chosen subdomain. Begin with Technique 1 — techniques are ordered foundational to advanced. Read the recognition moment. See yourself there. Then follow the protocol.
Step 3: Gather, Implement, Track
Gather the recommended materials, implement the daily 10–15 minute session, and track progress weekly using the data sheet on each technique page. Adjust using the troubleshooting guide when needed.
Join 2 Million+ Families on This Journey
You are not navigating this alone. The Pinnacle Blooms Network® community spans 70+ countries, 2 million+ families, and a network of parents, therapists, and educators who understand exactly what you are going through — and who have found a path forward.
Website & Resources
pinnacleblooms.org — Your complete resource hub for autism, ABA, speech, OT, and developmental therapy in India and beyond.
News & Updates
Latest Clinical News — Research summaries, policy updates, and technique additions from the Pinnacle consortium, updated regularly.
Parent Resources
Parent & Family Resources — Curated guides, workshop recordings, caregiver well-being tools, and community connection for families navigating developmental differences.
National Helpline
9100 181 181 — Available in 16+ languages, 24/7. Clinical triage, technique guidance, crisis support, and center referral — one call away.
Every Behavior Has a Reason. Every Reason Has a Solution.
Built by Mothers. Engineered as a System. Governed by Science.
70+ Centers
Across India, delivering the same evidence-based standard of care
21M+ Sessions
A dataset that makes every recommendation smarter and more precise
97%+ Improvement
Measured. Documented. Reproducible. Not a promise — a result.
Consortium: CRO · SLP · OT · BCBA · SpEd · NeuroDevelopmental Pediatricians
Powered by GPT-OS® — AbilityScore® · TherapeuticAI® · Everyday Therapy Program
Preview of behavior Therapy Material
Below is a visual preview of behavior therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!