
"You remade the meal because the peas touched the rice. Again."
It wasn't about the peas. It was never about the peas. Your child needs their plate a specific way — and until you understand why, every meal is a battle you didn't choose.
🍽️ Specific Plate Requirements — Intervention Technique E-456
"You are not failing. Your child's nervous system is telling you exactly what it needs. Let's decode it together." — Pinnacle Blooms Consortium | OT + SLP + ABA + SpEd + NeuroDev
📞FREE Helpline: 9100 181 181 | 16+ languages | Available 24×7

You Are Among Millions of Families Navigating This
1/3
Children with ASD
have food presentation requirements
80%
Autistic Children
show sensory processing differences affecting eating
2.7M
Families in India
dealing with rigid mealtime behaviors
Specific plate requirements — foods must not touch, exact plate color, precise portion appearance — are among the most commonly reported feeding challenges in children with autism, ARFID, sensory processing disorder, and anxiety. This is not a parenting failure. This is a neurological reality affecting families on every continent.
India Data: An estimated 18 million children in India have developmental conditions with sensory-feeding components. Pinnacle Blooms Network® serves families across all 28 states and 8 UTs.
References: PMC11506176 (PRISMA 2024); PMC10955541 (Meta-analysis, World J Clin Cases 2024); Padmanabha et al., Indian J Pediatr 2019

This Is Not Pickiness. This Is Neuroscience.
What's Happening in the Brain
- Visual Cortex (V1/V4) — Hyper-processes plate color and food arrangement
- Interoception Pathways — Over-amplifies tactile food-touching signals
- Amygdala — Triggers threat response when presentation deviates
- Prefrontal Cortex — Immature regulation → can't override the signal
In Plain English
When your child's food touches another food, or the "wrong" plate is used, their nervous system isn't being dramatic — it is genuinely processing this as a threat.
The visual cortex in some children processes plate color, food arrangement, and portion appearance with extraordinary intensity. What you see as "just a plate," their brain sees as a complex, high-stakes environment.
Tactile anticipation circuits fire before food is even touched — the expectation of mixed textures triggers anxiety responses identical to real discomfort.
This is a wiring difference, not a willpower deficit. The child cannot choose to "just eat it" any more than you can choose not to flinch when something flies at your eyes.
🧠 Neurological Basis
Not Behavioral Defiance

Your Child's Journey — Mapped on the WHO Developmental Timeline
Your child is most likely in the Age 3–7 zone — the period when plate and presentation requirements are most intense and when structured intervention yields the greatest returns. Intervention now — using the right materials and graduated exposure — redirects this trajectory toward functional mealtime independence.
Conditions That Commonly Co-Occur With Specific Plate Requirements
Autism Spectrum Disorder
60–80% prevalence of food presentation rigidity
ARFID
Avoidant/Restrictive Food Intake Disorder — presentation is a core feature
Anxiety Disorders
Predictability needs drive plate requirements
Sensory Processing Disorder
Visual/tactile sensitivity drives all presentation needs
References: WHO Care for Child Development Package (2023) — PMC9978394; WHO/UNICEF Nurturing Care Framework 2018

Clinically Validated. Home-Applicable. Parent-Proven.
⭐ Level I–II Evidence
Systematic Reviews + RCTs
Study | Finding | Source | |
PRISMA Systematic Review 2024 | 16 studies confirm sensory-based feeding intervention is evidence-based practice for ASD | PMC11506176 | |
Meta-analysis, World J Clin Cases 2024 | OT + sensory integration promotes adaptive behavior in 24 studies | PMC10955541 | |
Indian RCT, Padmanabha 2019 | Home-based sensory interventions show significant outcomes | DOI:10.1007/s12098-018-2747-4 | |
WHO CCD Package 2023 | Caregiver-implemented structured environments reduce feeding anxiety | PMC9978394 | |
NCAEP 2020 | Visual supports + structured mealtime = evidence-based for autism | NCAEP 2020 |
✅ OT-Validated
✅ ABA-Aligned
✅ Feeding Specialist Endorsed
✅ Parent-Executable at Home

🍽️ The Plate Architecture System — What This Technique Is
Domain E: Feeding & Mealtime
Age 2–12 Years
Daily Implementation
What it is: A structured occupational therapy approach that first accommodates a child's specific plate and food presentation requirements — using precisely selected materials — and then systematically builds mealtime flexibility through graduated exposure, so the child can eat adequately today while expanding tolerance over time.
What It Does
Eliminates the daily mealtime war by removing the sensory triggers that prevent eating, while creating a therapeutic pathway toward functional independence across home, school, and community settings.
Who It's For
Children aged 2–12 with food touching anxiety, specific plate color/material requirements, portion overwhelm, food arrangement rigidity, or mealtime ritualistic behaviors. Relevant for ASD, ARFID, SPD, and anxiety-driven feeding challenges.
📋 Divided Plates
📋 Bento Systems
📋 Portion Tools
📋 Silicone Separators
📋 Visual Presentation Guides

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
🟢 Occupational Therapist (Primary Lead)
Core sensory processing assessment; evaluates visual, tactile, and proprioceptive contributions to plate requirements. Selects specific materials, designs graduated exposure hierarchy, and builds flexibility protocol.
🔵 Speech-Language Pathologist
Evaluates oral motor contributions to food texture/presentation sensitivity. Assesses whether mixing aversion relates to taste-texture interaction vs. visual processing. Designs texture-separation strategies.
🟠 ABA / BCBA
Identifies the function of plate requirement behaviors. Designs reinforcement schedules for flexibility attempts. Builds gradual exposure data collection systems.
🟣 Special Educator
Supports school lunch compliance using portable systems. Creates teacher communication tools. Ensures presentation accommodations in IEP/individualized plans.
NeuroDev Pediatrician: When plate requirements are severe, escalating, or compromising nutrition — our NeuroDevelopmental Pediatricians assess for underlying ARFID, OCD components, or autism diagnoses requiring comprehensive treatment planning.

Precision Over Guesswork — What This Technique Is Actually Targeting
Target | "I see it working when…" | Indicator | |
Anxiety Reduction | Child approaches the table without pre-meal distress | Primary ✅ | |
Nutritional Intake | Meal completion rate increases to 70%+ | Primary ✅ | |
Tolerance Building | Child tolerates minor variations 1–2x per week | Secondary ✅ | |
Portability | Child can eat from school bento without meltdown | Secondary ✅ |

Material 1: Divided Plates With Compartments
📋 Canon: Feeding Equipment
Pinnacle Recommends ✅
Foods in their own spaces — no touching. Physical barriers create the safety your child needs. Each food has its own designated space, eliminating anxiety about contamination between foods. This is the single most impactful material in the entire toolkit for most children with plate requirements.
DIY Alternative (₹0)
Silicone cupcake liners placed on a regular plate — functionally identical, zero cost, available from existing kitchen supplies. Wash and reuse daily.

Material 2: Consistent Plate Set (Same Plate Every Time)
📋 Canon: Feeding Equipment
Consistency Protocol ✅
Predictability creates safety. Multiple identical plates ensure the "right" plate is always available and clean. The plate becomes part of the eating ritual that signals safety to your child's nervous system — just seeing it on the table begins the calming process before the first bite is taken.
Critical tip: Buy 3–4 identical plates immediately. If the design is discontinued, photograph it and search for exact matches before it becomes unavailable. Many families report the break of the "special plate" as a crisis that was entirely preventable with backups.
DIY Alternative (₹0)
The existing preferred plate IS your consistent set. Buy 2–3 more of the same design while still available. ₹300–600 investment that prevents future crises.

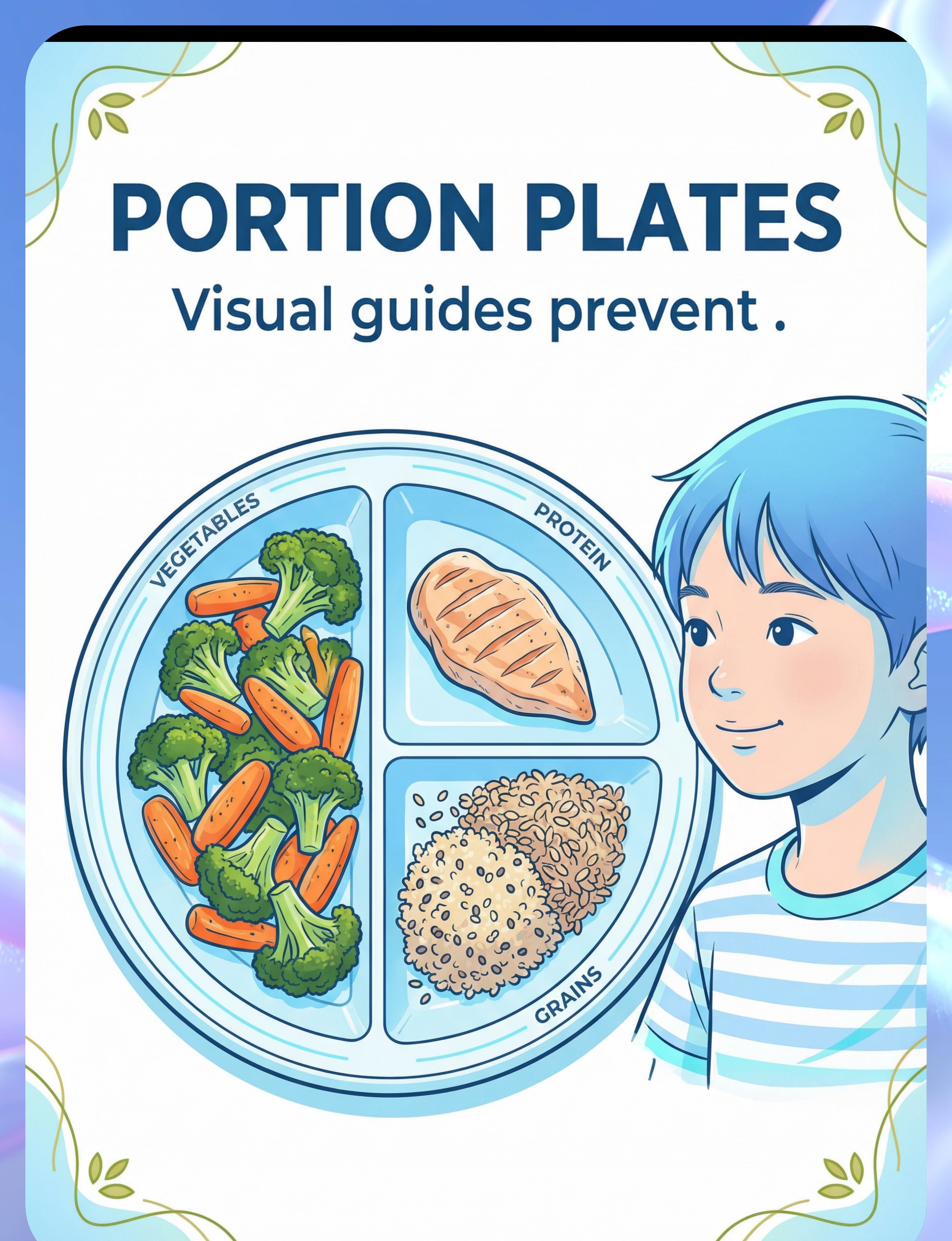
Material 3: Portion Control Plates With Visual Guides
📋 Canon: Feeding Equipment
Portion Support ✅
Visual guides prevent "too much" overwhelm. Predictable portion appearance prevents pre-meal visual overwhelm. The child knows exactly how the plate will look before food is even placed — removing the surprise element that triggers anxiety. When the amount and arrangement are consistent, the brain signals safety rather than threat.
DIY Alternative (₹0)
Draw portion zones on existing plate with a food-safe marker, or use a placemat with drawn portions. Completely functional and free.

Material 4: Bento Box — Multi-Compartment
📋 Canon: Feeding Equipment
School-Ready ✅
Multiple compartments, complete separation. Multiple small compartments provide variety with total organization. This is the essential tool for school lunches where presentation control is otherwise limited. It extends the therapeutic home environment into the school setting, enabling children to eat successfully in contexts their parents can't directly manage.
DIY Alternative (₹0)
Repurpose a multi-section steel tiffin (every Indian household has one). Individual stainless katoris work identically to bento compartments. Add silicone cupcake liners for additional separation.

Material 5: Color-Specific Plates and Bowls
📋 Canon: Feeding Equipment
Visual Preference Support ✅
The right color supports eating. Plate color significantly affects how food looks to visual processors. Some children are deeply anchored to a specific plate color — using any other color introduces a sensory variable that competes with the child's ability to attend to the food itself. Matching their preference removes a barrier before food is even served.
Why color matters: For children with visual hyper-reactivity, the contrast between food color and plate color, the pattern on a plate, or an unexpected hue can trigger the same threat-assessment process as a food touching another food. Solid, preferred colors eliminate this variable entirely.
DIY Alternative (₹0)
Use available solid-color plates in the preferred color. Retire patterned crockery from the child's mealtime rotation immediately.

Material 6: Silicone Food Separators & Divider Cups
📋 Canon: Feeding Equipment
Portable Intervention ✅
Create divisions on any plate — the most versatile tool in this toolkit. Silicone separators turn any plate into a divided plate. They are portable for restaurants, relatives' homes, and school. This single material is what enables therapy to travel with your child, transforming an unfamiliar eating environment into a manageable one.
DIY Alternative (₹80–150)
Small silicone muffin cups placed on a regular plate are functionally identical. A pack of 12 from any kitchen store — the most affordable therapy tool available.

Material 7: Clear / Transparent Plates
📋 Canon: Feeding Equipment
Visual Clarity Tool ✅
See everything — no hidden surprises. Transparency provides maximum visual information. Some children feel safer when they can see exactly what's on their plate from every angle — including underneath. The ability to fully visually inspect the food before committing to eating reduces the anticipatory anxiety that prevents engagement.
DIY Alternative (₹0)
A glass Pyrex pie dish from the existing kitchen ensures full visibility from all sides. A borosilicate glass lid turned upside-down also works. Zero cost from existing supplies.

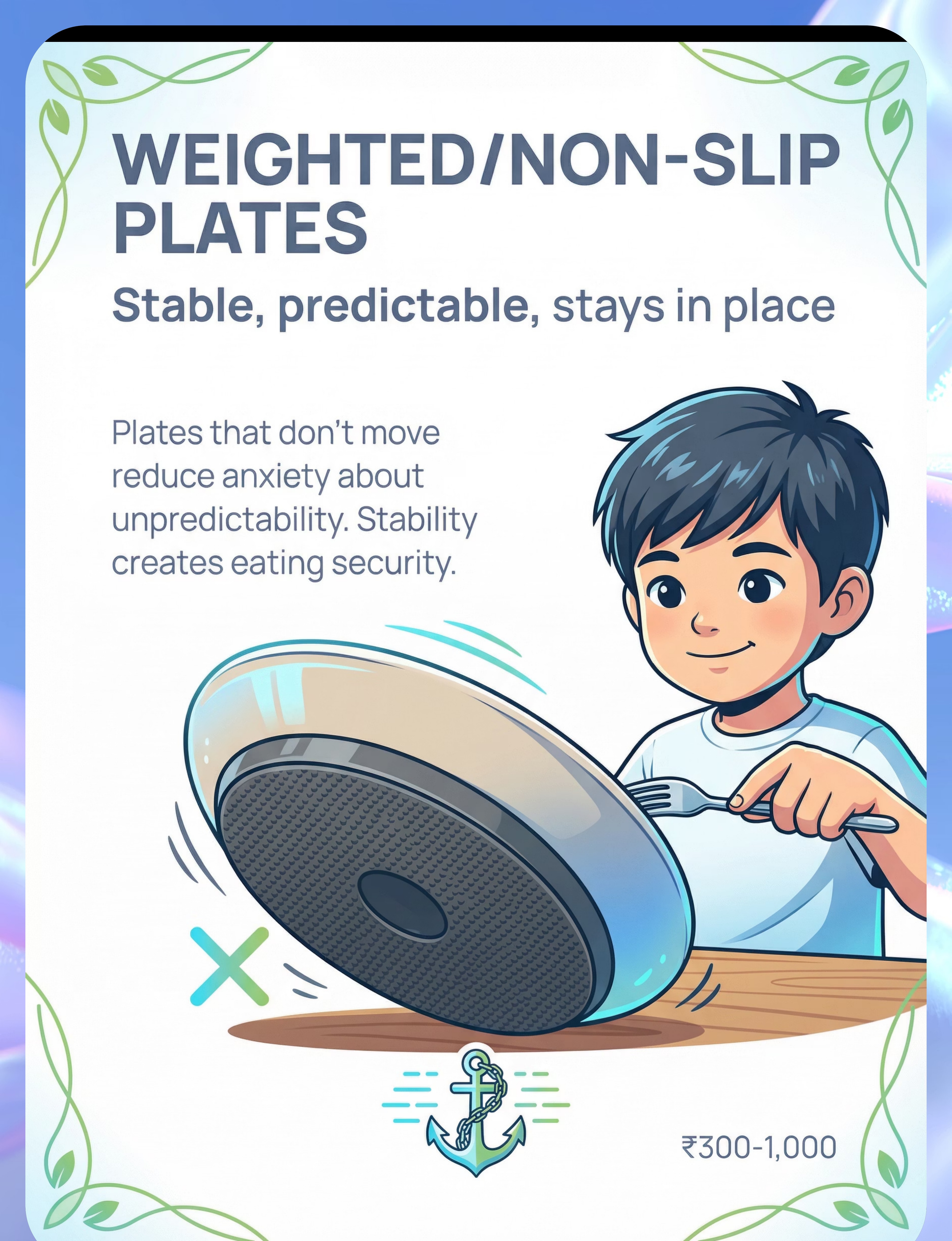
Material 8: Weighted / Non-Slip Plates
📋 Canon: Feeding Equipment
Stability Support ✅
Stable, predictable, stays in place. Plates that don't move reduce anxiety about environmental unpredictability. For children sensitive to sensory uncertainty, a plate that shifts when touched is a micro-stressor that compounds meal anxiety. Stability creates eating security — the plate becomes a grounded, reliable anchor in the sensory landscape of mealtime.
DIY Alternative (₹0)
A damp kitchen towel under any plate prevents movement. A cut piece of non-slip shelf liner (₹30 from hardware store) is absolutely functional and reusable for years.

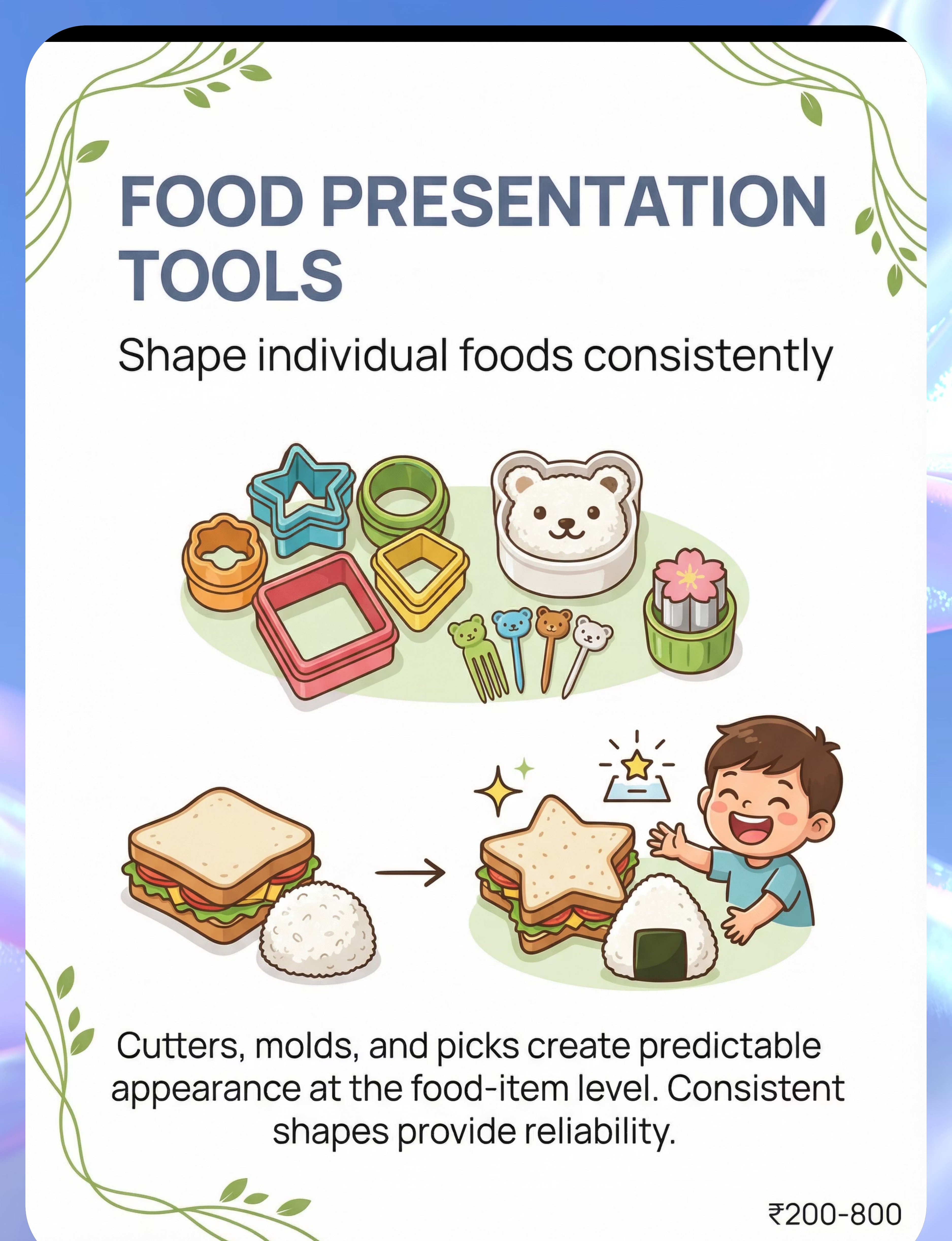
Material 9: Food Presentation Tools — Cutters, Molds & Picks
📋 Canon: Feeding Equipment
Food-Level Consistency ✅
Shape individual foods consistently. Cutters, molds, and picks create predictable appearance at the food-item level. A sandwich that's always the same shape, a carrot that's always a circle — item-level consistency removes the final layer of presentation anxiety. Combined with a correctly set-up plate, food-level consistency completes the sensory safety system.
DIY Alternative (₹0)
The mouth of a cup creates circular shapes. A glass or mug rim cuts perfect circles in sandwiches. Plastic bottle caps for small circles on soft foods. Consistency of shape is the goal — the tool is secondary.
💡Your Foundational Trio: Start with Materials 1, 2, and 6 (Divided Plate + Consistent Set + Silicone Separators) — ₹600–1,400 total investment. 📞9100 181 181 — Ask our OT team which materials suit your child's specific profile.

⚠️ Material Safety & Clinical Precautions
❌ Avoid These
- Glass plates for children under age 6 (breakage risk)
- Food picks with sharp ends unsupervised (choking/puncture)
- Painted plate surfaces that chip into food (toxicity)
- Suction plates on rough/uneven surfaces (sudden pop-off risk)
- Pressuring child to use new materials without gradual introduction
- Forcing flexibility without a graduated protocol in place
- Skipping nutritional backup when attempting flexibility challenges
✅ Safe Practices
- Food-grade, BPA-free, dishwasher-safe materials only
- Food-safe silicone for all separators and cups
- Tempered glass only if glass is used (age 8+)
- Always have the "safe" plate available during flexibility attempts
- Introduce new materials at low-stress meals, not challenging ones
- Never compromise nutrition for flexibility training
⚠️ Clinical Precaution: Escalating rigidity requires professional evaluation. If plate requirements are becoming more restrictive over time, nutrition is compromised, or mealtime distress is severe — this is a clinical signal. Contact Pinnacle Blooms at 9100 181 181 or consult an OT/feeding specialist immediately.

₹0 Alternatives: Every Family Can Start Today
WHO/UNICEF Equity Principle
Pinnacle operates on the principle that evidence-based intervention should not be gated by purchasing power. Every material in this protocol has a zero-cost home alternative, validated by OT teams across 70+ centers.
Divided Plate (₹0)
Line a regular thali with 3–4 silicone muffin cups. Same physical separation, zero cost. Wash and reuse daily.
Consistent Set (₹0)
The existing preferred plate IS your consistent set. Photograph it; buy extras while available.
Portion Guide (₹0)
Cut a paper plate in 3 sections as a placement guide. Trace sections with food-safe marker on existing crockery.
Bento (₹0–₹80)
A multi-section steel tiffin. Individual stainless katoris work identically to bento compartments.
Silicone Separators (₹80–₹150)
A set of 12 silicone muffin cups from any kitchen store — portable food separators and sauce holders.
Non-Slip Base (₹0)
A damp kitchen towel under any plate. A cut piece of non-slip shelf liner (₹30 from hardware store). Absolutely functional.
"The goal of every Pinnacle-developed material list is a world where no parent ever hears: 'I couldn't do the therapy because I couldn't afford the tools.'"

Before the Meal Begins: Your Pre-Session Setup Checklist
📍 Physical Setup
- Preferred plate(s) clean and available
- Backup identical plate available if #1 is unavailable
- Silicone separators or dividers placed correctly
- Foods prepared in required shapes/portions BEFORE plating
- Plate placed on non-slip surface
- Child's seat at correct height (feet flat, 90° hip angle)
🔇 Sensory Environment
- Room lighting: comfortable (not harsh fluorescent)
- Background noise minimized
- Strong food smells from other dishes removed or covered
- No visual clutter on the table
🧘 Parent Prep
- Your own calm state (regulated parent = regulated child)
- Reinforcement ready (verbal praise script rehearsed)
- Data tracking method ready (phone note or paper tally)
- 15–20 minutes of protected time
"The best meal session is one that starts with the space right."

The 60-Second Pre-Meal Readiness Assessment
🟢 GO — All Signals Present
- Child has been calm for ≥10 minutes
- No recent sensory overload event
- Not overtired or excessively hungry
- Recent successful meal memory (positive association)
- Your own emotional state: calm and patient
🟡 MODIFY — Some Signals Present
- Child is slightly heightened but manageable
- → Serve only "safe" foods in known configuration
- → Reduce food variety to minimum acceptable
- → Shorten mealtime expectation to 10 minutes
🔴 POSTPONE — Dysregulation Present
- Child is in meltdown, post-crisis, or overtired
- → Offer a small, safe snack informally (no table ritual)
- → Do not attempt flexibility work today
- → Regulate first; meal can wait 15–20 minutes
"A 10-minute successful meal is worth infinitely more than a 45-minute battle. No parent should push through when the child isn't ready."

Step 1: The Invitation
🟢 STEP 1 OF 6
⏱️ 30–60 Seconds
Objective: Bring the child to the table through playful, low-demand engagement — not a command.
"[Child's name], lunch is ready! Look — your blue plate is there with the rice on one side and the chicken on the other side, exactly how you like it. Come see!"
Body Language Guidance
- Crouch to child's eye level
- Warm, not urgent, tone
- Point to the correctly set plate — preview reduces surprise
- Give 30-second processing time before repeating
Acceptance Cues to Watch For
- Makes eye contact or looks toward table
- Moves toward table even slowly
- Reduces body tension
- Any positive vocalization
Resistance Response: Do NOT escalate to command. Offer one modification: "Do you want to carry your plate to the table?" If still resistant: return to the 60-Second Readiness Check (Go/Modify/Postpone).

Step 2: The Engagement
🟢 STEP 2 OF 6
⏱️ 1–3 Minutes
Objective: Child is at table. Now deepen engagement with the correctly configured plate.
"Here's your plate — see how the rice is right here [point] and it's not touching the chicken over here [point]? Just the way you like it."
Presentation Guidance
- Place plate in child's correct orientation (specific food positions)
- Announce foods by position before child has to assess — reduces visual search anxiety
- Do NOT rearrange anything after placing
Signal | Meaning | Response | |
Child looks at plate approvingly | Engagement ✅ | Praise and step back | |
Begins eating within 60 sec | High engagement ✅ | Maintain silence, reinforce with a smile | |
Checks each compartment | Assessment mode — normal | Allow; don't rush | |
Points to a problem | Communication ✅ | Fix it; praise the communication | |
Pushes plate away | Avoidance | Troubleshoot (see Card 33) |

Step 3: The Therapeutic Action
🟢 STEP 3 OF 6
⏱️ 10–20 Minutes
The active ingredient of this technique is consistent, accurate execution of the child's plate requirements — not despite your frustration with them, but because meeting them is the therapeutic intervention. Every correctly presented plate trains the child's nervous system that mealtimes are safe, predictable, and manageable.
Phase A — Accommodation
Weeks 1–4. Meet all plate requirements exactly. No flexibility challenges. Goal: establish mealtime as safe. Measure: meal completion rate.
Phase B — Micro-Variations
Weeks 5–8. Introduce one tiny variation per week at low-stress meals. Narrate: "The rice is almost in its spot — a little bit different today. That's okay."
Phase C — Graduated Exposure
Weeks 9–12+. Systematically reduce accommodation level while building coping skills. Goal: functional flexibility for real-world settings.
Child Response Spectrum:Ideal — Eats full meal, no distress. Acceptable — Eats majority with minor distress; recovers and continues. Concerning — Refuses entire meal or escalates to meltdown → see Troubleshoot card.

Step 4: Repeat & Vary
🟢 STEP 4 OF 6
Therapeutic Dosage
- Frequency: Every meal (3× daily) — plate requirements are inherently a daily activity
- Flexibility challenges: 1–2× per week maximum (Phases B and C)
- Satiation rule: When child shows escalating distress for 2 consecutive attempts, pause for 3–5 days
The Principle
"3 successful meals with Level 1 variation → unlock Level 2. 3 consecutive distressed meals → step back one level. This is not failure — it is calibration."
Level | Variation | Example | |
0 | No variation (accommodation) | Exact requirements met every time | |
1 | Same plate, food position shifted 1cm | Rice moved 1cm from usual spot | |
2 | Same plate type, slightly different shade | Same design, different color run | |
3 | Lower divider walls | Silicone cup instead of solid compartment | |
4 | Different plate, familiar food setup | Different plate but same food arrangement | |
5 | Any plate with portable separators | Unfamiliar restaurant plate + silicone separators |

Step 5: Reinforce & Celebrate
🟡 STEP 5 OF 6
⚡ Within 3 Seconds
The Golden Rule: Reinforce within 3 seconds of the desired behavior.
For completing a meal: "You sat down and ate your whole plate! That was really good eating. I'm proud of you."
For tolerating a variation: "The rice was in a slightly different spot today and you kept eating. That was brave. Really, really brave."
For communicating a problem: "Thank you for telling me the food was wrong instead of getting upset. That was amazing. Let's fix it together."
Social
High-five, hug, specific verbal praise
Activity
5 extra minutes preferred screen time; choose next game
Token
Star on chart; 5 stars = special treat
Natural
"You ate well, now let's do your favorite thing"
📞9100 181 181 — Our ABA team can design a custom reinforcement schedule for your child.

Step 6: The Cool-Down
🟢 STEP 6 OF 6
Transition Time
Objective: No meal ends abruptly. Transition the child from mealtime back to their regular activity safely — the ending of a meal is as therapeutically important as the beginning.
If Child Resists Ending
- Offer one more small acceptable item ("One more piece of chicken, then done")
- Do NOT extend the meal into a second engagement cycle
- Transition to preferred activity as quickly as possible
What to Avoid
- Abrupt removal of plate without warning
- Extending mealtime beyond 25 minutes regardless of completion
- Commenting on what wasn't eaten during cool-down

60 Seconds of Data = Months of Insight
Data captured today becomes the evidence that shows you — and your therapist — whether the protocol is working, whether to advance to the next variation level, and whether professional consultation is needed. Without data, you're navigating blind. With 60 seconds per meal, you have a clinical record.
📋 Pinnacle Meal Tracker (4 Fields)
- Date & Meal (breakfast / lunch / dinner)
- Meal completion % (0–100%)
- Distress level today (1–5 scale)
- Flexibility attempt today? Yes/No → Level attempted + outcome
📝 Paper Tally Alternative (₹0)
Date: _______ | Meal: B / L / D
Completion: 0% | 25% | 50% | 75% | 100%
Distress: 1 | 2 | 3 | 4 | 5
Variation attempted: Y / N | Outcome: ✅ / ❌
Completion: 0% | 25% | 50% | 75% | 100%
Distress: 1 | 2 | 3 | 4 | 5
Variation attempted: Y / N | Outcome: ✅ / ❌
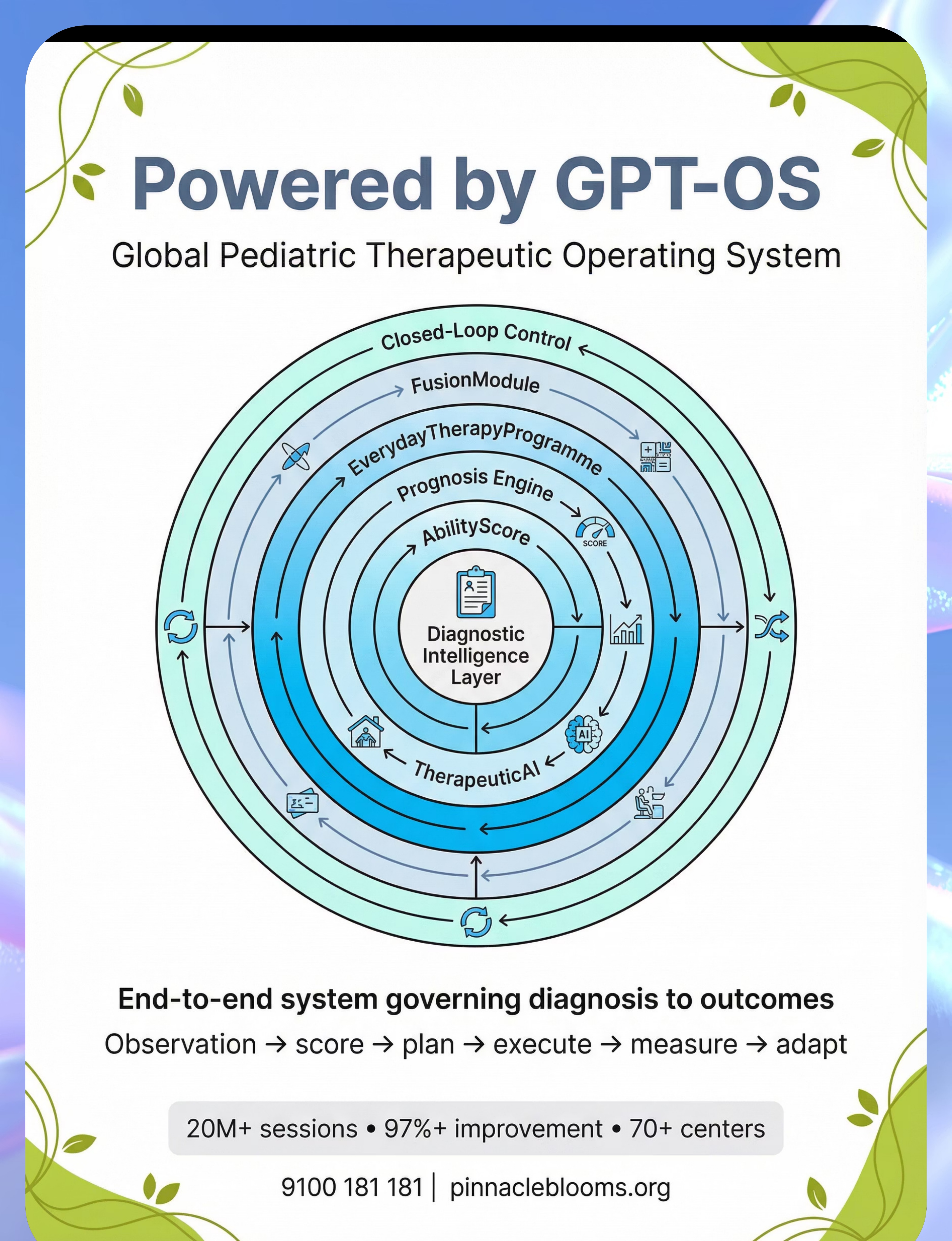
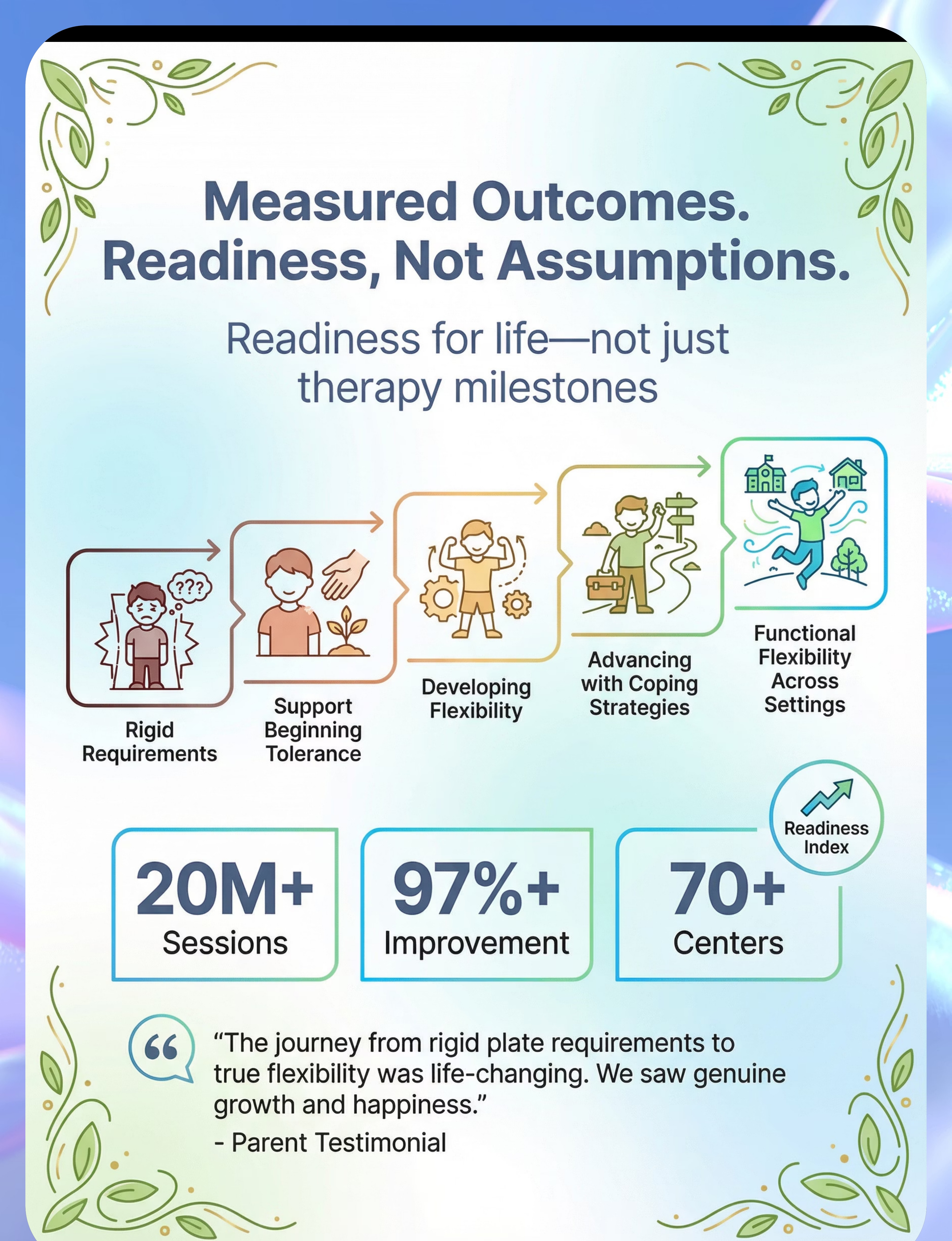
GPT-OS® Integration: This data, when entered into your GPT-OS® session, feeds the Feeding Flexibility Readiness Index and informs personalized progression recommendations. Download the Pinnacle Meal Tracker PDF at techniques.pinnacleblooms.org/feeding/E-456/tracker

Common Obstacles — and Exactly What to Do
🔴 Problem | 🟢 Solution | |
Child refuses the divided plate itself | Introduce plate while empty; let child examine and touch it for 3–5 days before food is placed. | |
Requirements escalating — more rules each week | This is a stress response signal. Review whether accommodation is sufficient and consistent. Consider professional consultation. | |
Works at home, fails at school | Pack bento + silicone separators + familiar spoon. Create a school communication card with plate requirements. | |
Works for one parent, not the other | Share this page. Ensure all caregivers follow identical plate setup. Inconsistency increases rigidity. | |
Child accepts the plate but eats very little | The plate architecture is working. Volume is a separate goal. Consult SLP/feeding specialist for intake expansion. | |
Flexibility attempt triggered meltdown | Stepped too fast. Return to full accommodation for 7 days. Retry with a smaller variation than attempted. | |
Child only eats 2–3 foods regardless of plate | This is ARFID territory. The plate protocol is supportive but professional feeding therapy is essential. |
📞9100 181 181 — If you're facing persistent, severe plate requirement escalation, our OT and feeding specialist team is available on the FREE National Helpline. 24×7 | 16+ Languages.

This Technique Is a Framework — Not a Script. Personalize It.
By Sensory Profile
- Visual Processor: Prioritize color-specific plates, clear plates, portion guides. Flexibility path: same design in adjacent color.
- Tactile Anxious: Prioritize deep-walled divided plates, tall silicone separators. Sauce always in separate cup. Flexibility path: slowly lower divider height over months.
- Overwhelmed: Smaller plate sizes, portion plates, bento with small compartments. Start with 3 items maximum visible.
By Age
- Age 2–4: Full accommodation; no flexibility pressure; build mealtime safety
- Age 5–7: Begin micro-variations; involve child in plate setup
- Age 8–12: Teach self-advocacy; introduce portable solutions; build school/social meal strategies

Week 1–2: What to Expect
Early Accommodation Phase
🔵 15% Progress
✅ In Weeks 1–2, Look For:
- Reduced pre-meal protests when plate is set up correctly
- Child approaching the table without prompting (on correct plate days)
- Meal completion rate improving from baseline
- You feeling more confident about the setup protocol
❌ What Is NOT Progress Yet
- Flexibility — we are in full accommodation phase only
- Eating new foods — this comes much later
- Eating at other people's homes without preparation
"If your child completes 50% more of their meal when requirements are met vs. not met — that is your first proof that this protocol is working. Write it down."
Weeks 1–2 can feel like you're just "giving in." You're not. You're establishing neurological safety. The flexibility comes later, and it comes from safety — not from pressure.

Week 3–4: Consolidation Signs
Consolidation Phase
🔵 40% Progress
✅ Watch for These Signs
- Child begins anticipating correctly set plate — less pre-meal checking behavior
- Child can tell you (verbally or by pointing) what they need if something is wrong
- Meal completion consistently above 70%
- Occasional tolerance of very minor setup errors without full meltdown
🧠 Neural Pathway Formation
The fact that your child can now tell you what's wrong instead of melting down immediately is a neural pathway forming. The prefrontal cortex is building regulatory capacity over the amygdala's threat response. This is real, measurable neurological progress.
Begin Phase B If All Three Are True:
- Meal completion >70% for 7 consecutive days
- Pre-meal distress has reduced significantly
- Child is communicating about requirements rather than just reacting
"You may notice that you're more confident too — that you know exactly how to set up the plate, what to say, and how to read your child. That parent confidence is therapeutic in itself."

Week 5–8: Mastery Indicators
🏅 Mastery Approaching
🔵 75% Progress
Criterion | Observable Indicator | Measurement | |
Accommodation mastery | Eats >80% of meals with correct setup without distress | 10 of last 14 days | |
Communication | Reports plate problems without meltdown | 90% of the time, 2 weeks | |
Micro-flexibility | Tolerates Level 2 variation at low-stress meals | 3 successful attempts | |
Portability | Can eat from bento/silicone separators at school or relative's home | 2 separate settings |
🏆 Mastery Unlocked Criteria: When your child can eat successfully from a correctly-set-up plate across HOME + SCHOOL + ONE OTHER SETTING — that is Domain E, Technique E-456, mastered.
Stay at Current Level If:
Mastery criteria not yet met in all settings. There is no shame in taking more time — the pace is the child's.
Advance to E-457 When:
Mealtime is stable and positive across ≥2 settings. Utensil skills become the next frontier.

🏆 You Did This.
Every meal you set up correctly. Every time you swallowed your frustration and got the blue plate instead of the green one. Every night you searched for divided plates that were the right size. Every time you packed the bento and carried the silicone separators to Grandma's house.
That was therapy. That was science. That was love in its most practical, unglamorous, and powerful form.
Your child's nervous system is safer because of you. That is not small. That is everything.
📸Family Celebration Suggestion: Choose any celebration your child loves — this is their milestone too. Name it. Mark it. Document it. Photo prompt: "The plate that changed mealtimes" — photograph your child's successful setup and share it with the Pinnacle community.
E-456 | Accommodation + Flexibility Foundation Established

⚠️ Trust Your Instincts — These Signs Mean Pause and Seek Help
🚩 Red Flag | Why It Matters | What To Do | |
Requirements becoming MORE specific each week, not less | Escalating rigidity = increasing anxiety — protocol alone insufficient | Book OT consultation; free teleconsult available | |
Child is losing weight or refusing to eat despite correct setup | Nutritional compromise is a medical signal | Contact pediatrician AND feeding specialist urgently | |
Child is gagging, vomiting, or showing pain during meals | May indicate oral motor or GI component | Medical evaluation + OT/SLP joint assessment | |
Plate requirements spread to school to point of refusing to eat there | Generalization of anxiety — clinical intervention needed | ARFID evaluation + behavioral health referral | |
Mealtime meltdowns lasting >30 minutes despite full accommodation | Indicates co-occurring anxiety disorder | Psychological evaluation + OT collaboration | |
Requirements suddenly appear or dramatically worsen | Possible acute stressor, medical issue, or trauma response | Pediatrician evaluation; clinical review |
📞9100 181 181 — Free 24×7 | 16+ Languages | Our clinical team will guide escalation appropriately. Self-resolve → Pinnacle Teleconsult (free) → Clinic Visit → Medical Referral.

You Are Here — Your Developmental GPS
E-454
Mealtime Sensory Sensitivities — foundational sensory tolerance work
E-455
Expanding Food Variety — food acceptance broadening
◄ E-456 ►
YOU ARE HERE — Specific Plate Requirements
E-457
Utensil Skill Development — next mealtime independence domain
E-458
Social Eating & Family Meals — community and peer settings
Next Level Options
- If plate anxiety is primary → E-460: Mealtime Anxiety and Rigidity
- If mealtime is stable → E-457: Utensil Skill Development
- If school eating is the challenge → E-461: Eating in Community Settings
Long-Term Goal
Functional mealtime independence — eating across home, school, and community settings with personal preferences acknowledged and coping strategies in place.

Other Techniques in Domain E: Feeding & Mealtime Independence

🍽️ E-454 — Mealtime Sensory Sensitivities
Managing the full spectrum of mealtime sensory triggers — sound, smell, texture, temperature, visual environment.

🥄 E-455 — Expanding Food Variety
Graduated food introduction and food chaining for selective eaters — from 3 foods to 30.

🍴 E-457 — Utensil Skill Development
Building spoon, fork, and chopstick competency alongside sensory regulation during eating.

👨👩👧 E-458 — Social Eating & Family Meals
Strategies for family mealtimes, restaurant eating, and peer lunch settings.

Real Families Who Walked This Path Before You
"Our son would only eat from a specific blue plate, with everything in exact positions. We got divided plates and duplicates of his preferred plate. For school, we pack his bento with silicone separators. Two years later, he still prefers separation but can eat from unfamiliar plates at restaurants. The rigidity isn't gone, but it's manageable."
— Parent, Pinnacle Hyderabad Network
"I was so embarrassed that my daughter would have a meltdown at family dinners over the plate. Once I understood it was neurological — not behavioral — I stopped being embarrassed and started problem-solving. The bento box changed our lives. It took 6 months but we got there."
— Mother of 7-year-old, Pinnacle Bangalore Network
"The hardest part was convincing my husband this wasn't spoiling. This page — the neuroscience card especially — helped us align. We both follow the same protocol now. That consistency alone made a 40% difference in meal completion."
— Father, Pinnacle Chennai Network
Illustrative cases; individual outcomes vary by child profile, underlying condition, and intervention specificity.

Frequently Asked Questions
Is meeting my child's plate requirements reinforcing the rigidity?
No — not in the short term and not when done with a therapeutic plan. Meeting sensory and anxiety-driven requirements reduces distress, enabling eating. Forced flexibility without support increases rigidity and food refusal. The protocol: accommodate first (so nutrition isn't compromised), then systematically build flexibility with graduated exposure.
My child only uses one specific plate. What if it breaks?
This is exactly why the protocol recommends purchasing 3–4 identical plates immediately. If the original is discontinued, photograph it and search for exact matches before it becomes unavailable. Many families report the break of the "special plate" as a preventable crisis.
How long before my child eats from an unfamiliar plate at a restaurant?
Timeline varies significantly by child profile. Average reported by Pinnacle OT teams: 6–18 months from starting the protocol to functional flexibility in 2+ settings. Portable silicone separators make restaurants possible much sooner as an interim solution.
Is this autism-specific, or do neurotypical children have plate requirements too?
Mild food-touching preferences are common in neurotypical young children (ages 2–5) and typically resolve without intervention. When requirements are consistent regardless of hunger level, escalating over time, causing mealtime distress, and preventing eating — professional evaluation is warranted regardless of diagnosis.
My child's plate requirements are very different at home vs. school. Why?
This reflects context-dependent regulation. Home = high safety, therefore more rigid requirements. School = survival mode, therefore sometimes more flexible. Use portable tools (bento, silicone separators) to extend home-level accommodation to school settings.
Can I just use silicone muffin cups on a regular plate instead of buying divided plates?
Yes — absolutely. Silicone cupcake liners on a regular plate are functionally equivalent to a divided plate for most children. This is the DIY alternative recommended in this protocol. Start with what you have; upgrade to purpose-built materials if needed.
My OT says to not accommodate the requirements. This page says to accommodate first. Why?
Clinical approaches vary based on individual assessment. Your OT has information about your child's specific profile that a general educational resource doesn't. The evidence base increasingly supports accommodation-first for anxiety-driven feeding challenges. Discuss the research evidence from Cards 5 and this page with your OT directly.
Where can I get professional help for this?
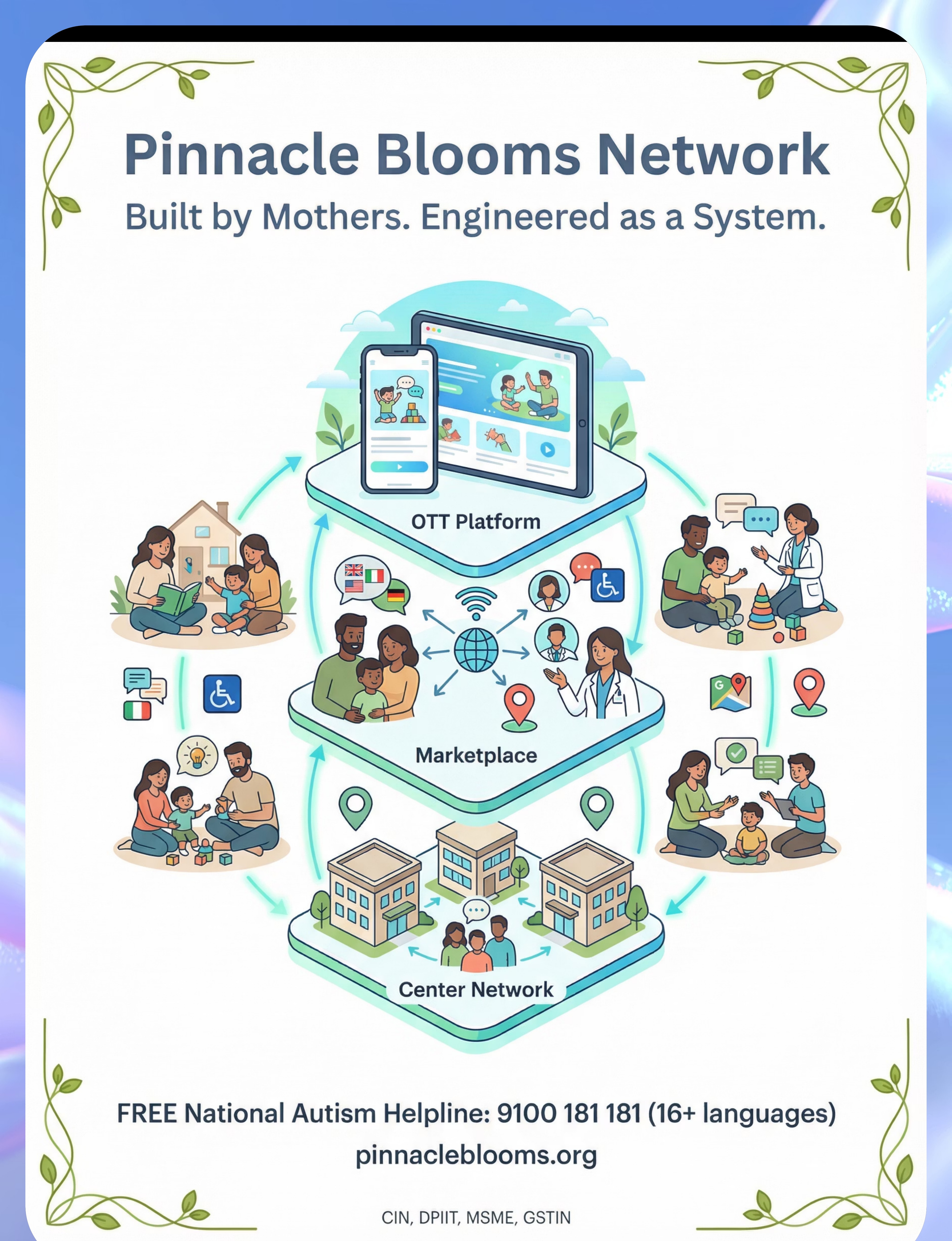
Pinnacle Blooms Network: 📞9100 181 181 (FREE, 24×7, 16+ languages) | pinnacleblooms.org | Book an OT or Feeding Specialist consultation at your nearest center or via teleconsult.
Preview of 9 materials that help with specific plate requirements Therapy Material
Below is a visual preview of 9 materials that help with specific plate requirements therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.











Link copied!

From Reading to Doing — Your Child's Next Mealtime Can Be Different
Every technique on this page is ready to use today — no special equipment required to begin, no waiting for a clinic appointment. Start with Material 1 (divided plate or silicone muffin cups), use Step 1 (The Invitation), and follow the 60-second readiness check. Your child's next meal is the first session.
🟢 OT
🔵 SLP
🟠 ABA
🟣 SpEd
🔴 NeuroDev
🏛️ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO
20M+ Sessions • 70+ Centers • 160+ Countries
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO
20M+ Sessions • 70+ Centers • 160+ Countries
🌐techniques.pinnacleblooms.org | 📞 FREE National Helpline: 9100 181 181 (16+ languages, 24×7) | ✉️ care@pinnacleblooms.org
This content is educational. It does not replace individualized feeding assessment and intervention with licensed occupational therapists, feeding specialists, or healthcare professionals. Specific plate requirements may be part of broader conditions including autism, ARFID, anxiety disorders, or sensory processing disorders requiring comprehensive evaluation. Consult pediatric specialists for persistent feeding concerns. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique E-456 | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2