

- OT • SLP • ABA • SpEd
- NeuroDevelopmental Pediatrics
- Feeding Specialists
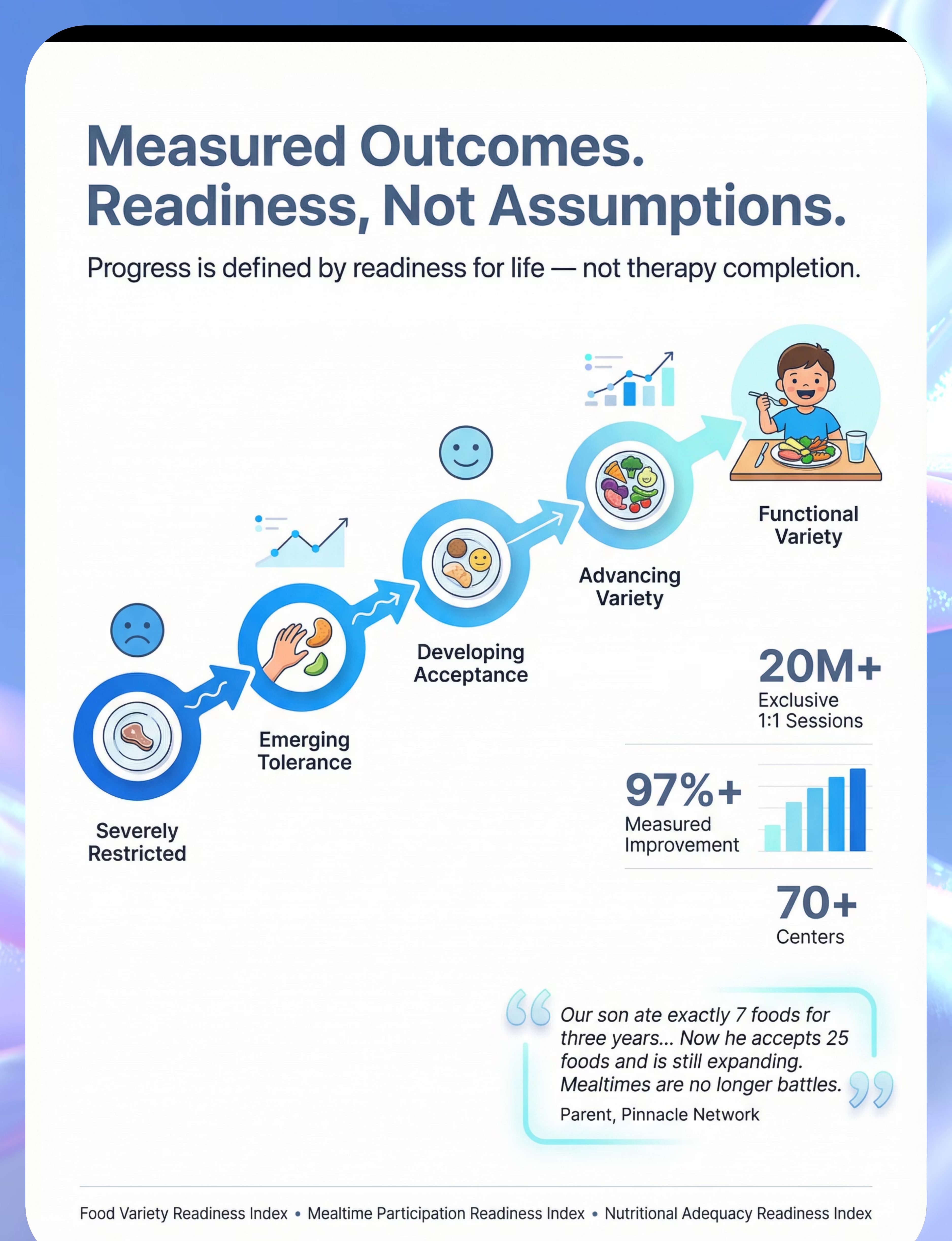
- 20M+ 1:1 therapy sessions
- 97%+ measured improvement rate

"You are among millions of families navigating this exact challenge. The science has caught up. The tools exist. The path forward is clear."
This Is a Wiring Difference. Not a Behavior Problem.
The Neuroscience In children with very limited food repertoire, the brain's sensory processing pathways — including the gustatory cortex (taste), somatosensory cortex (texture), olfactory bulb (smell), and visual cortex — process food stimuli with amplified intensity. What a neurotypical child experiences as "mild bitterness" registers as overwhelming. What feels like normal texture feels like sandpaper or slime. Neuroimaging studies confirm atypical sensory processing in the insula and anterior cingulate cortex — regions governing both taste and threat response. Frontiers in Integrative Neuroscience (2020) | PMC11506176 In Parent Language Imagine eating while wearing headphones set to maximum volume, with a spotlight shining directly in your eyes, and someone is constantly touching your arm. That's the sensory experience of mealtime for many selective eaters. Their refusal is protective. Their selectivity makes complete neurological sense. The goal is not to force through the refusal. The goal is to gradually reduce the threat signal — one tiny, patient step at a time. "This is a wiring difference, not a behavior choice. Intervention works by building new neural pathways through safe, repeated, low-pressure exposure — not through force, rewards for eating, or punishment." — Pinnacle Blooms Consortium, Feeding Therapy Division

- The feeding relationship is the first context where a child experiences safety, connection, and control
- Disruption of the feeding relationship has cascading developmental impacts
- All 5 nurturing care components intersect at the feeding relationship
- Sensory processing disorder
- Autism spectrum conditions
- Anxiety disorders & ADHD
- Oral motor difficulties
- GI disorders (reflux, eosinophilic esophagitis)
Clinically Validated. Home-Applicable. Parent-Proven.
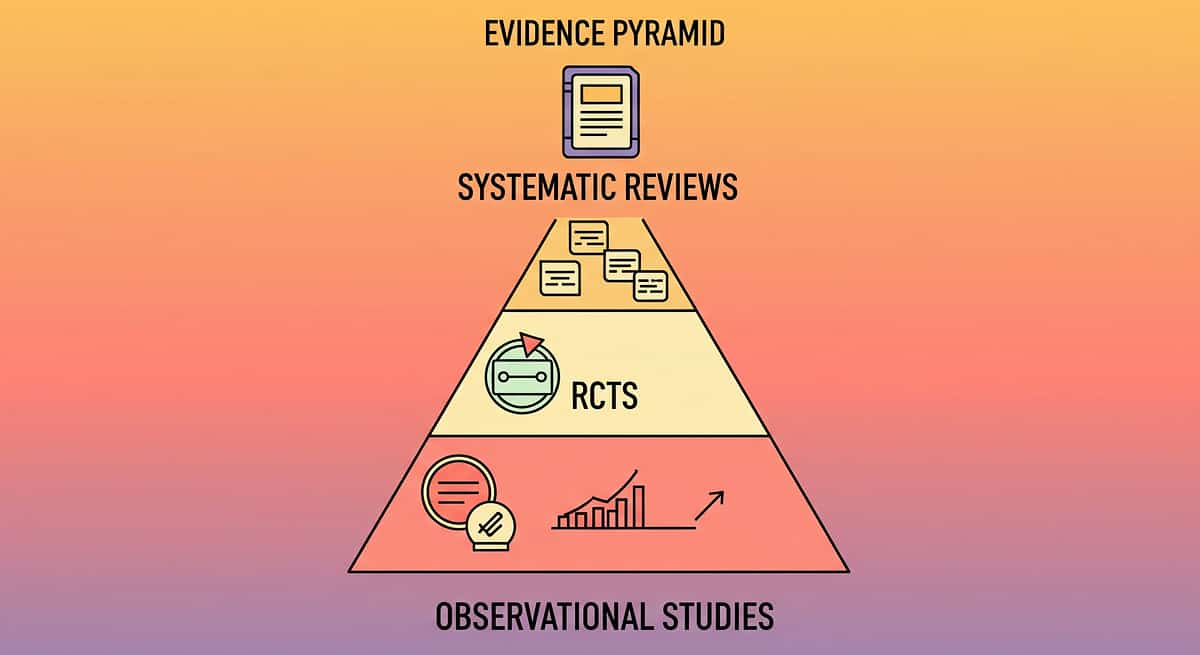
🛡️ Level I Evidence — Systematic Review + Meta-Analysis Study Finding Source PRISMA Systematic Review (2024) Sensory integration intervention is evidence-based practice for autism across 16 studies (2013–2023) PMC11506176 Meta-analysis, World J Clin Cases (2024) Feeding intervention promotes food acceptance, adaptive eating behavior, and reduced food-related anxiety across 24 studies PMC10955541 Indian RCT (2019) Home-based sensory feeding interventions demonstrate significant outcomes in Indian pediatric population DOI: 10.1007/s12098-018-2747-4 SOS Approach to Feeding 6–18 months of systematic exposure → average 20–30 new foods accepted Dr. Kay Toomey WHO CCD Package Caregiver-delivered feeding intervention produces measurable outcomes in 54 LMICs PMC9978394 Key Finding: Food chaining + sensory desensitization + removal of mealtime pressure = the evidence-based triple approach for very limited food repertoire. Pinnacle real-world evidence: 20M+ sessions | 97%+ improvement rate via GPT-OS®.

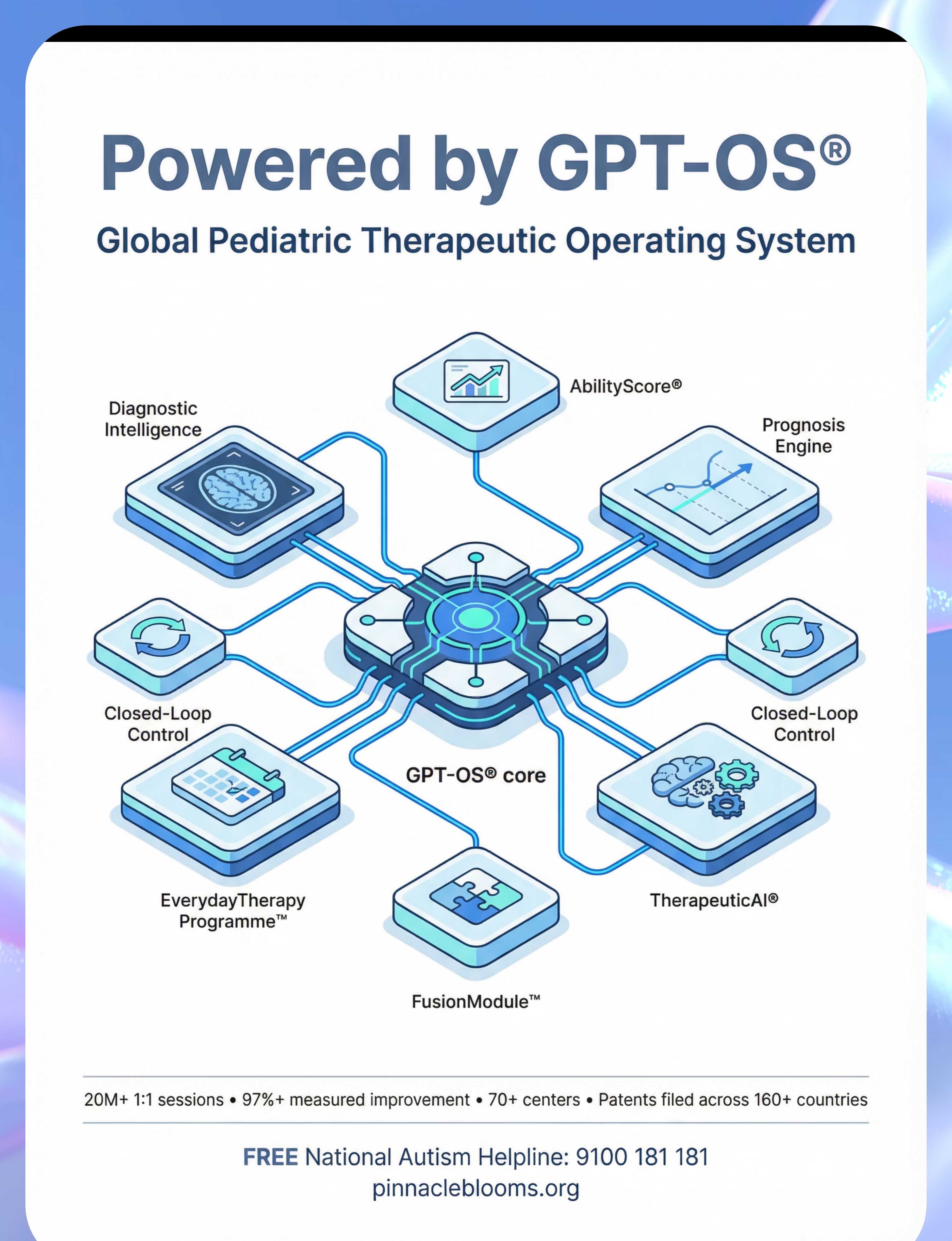
"The brain doesn't organise by therapy type. Effective feeding intervention requires all five disciplines working from a single integrated plan — which is what GPT-OS® FusionModule™ delivers." — Pinnacle Blooms Consortium
- Food Variety Readiness Index
- Mealtime Participation Readiness Index
- Nutritional Adequacy Readiness Index
- Social Eating Readiness Index
- Feeding Independence Readiness Index
- Sensory Processing Regulation — Generalised improvement in sensory tolerance beyond food
- Autonomy & Self-Efficacy — Child develops agency over their relationship with food
- Family Quality of Life — Meal planning stress reduces; family can eat out and travel








Every Family Can Start Today. Zero Budget Required.
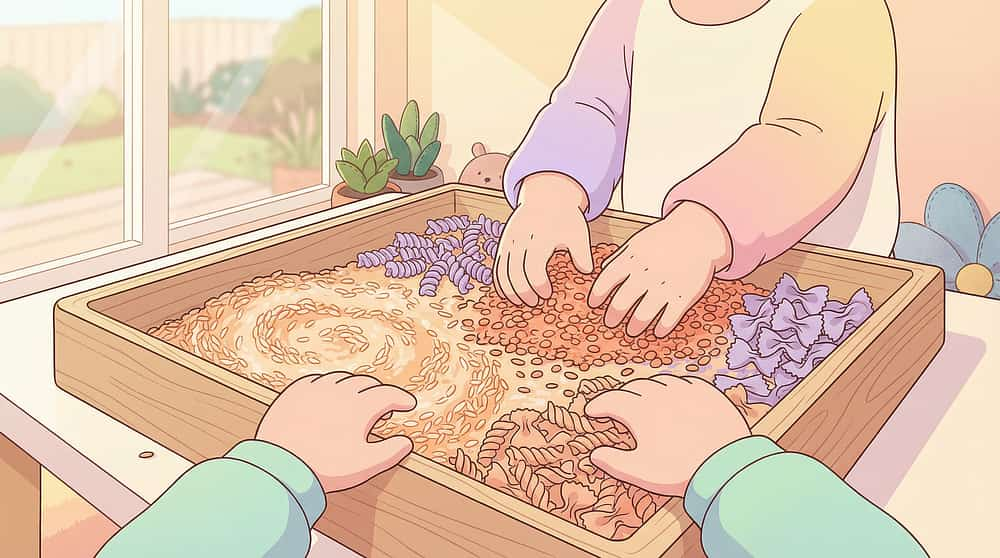
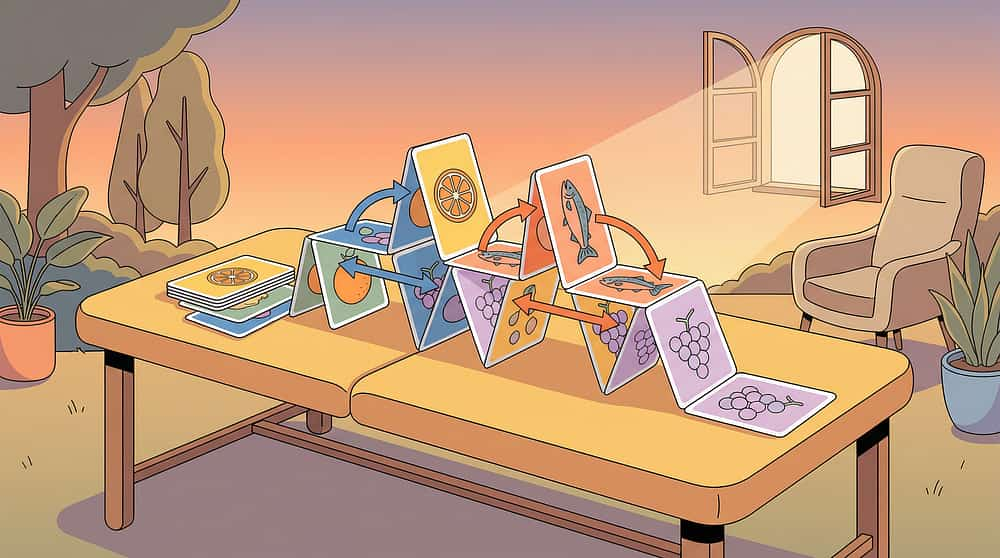
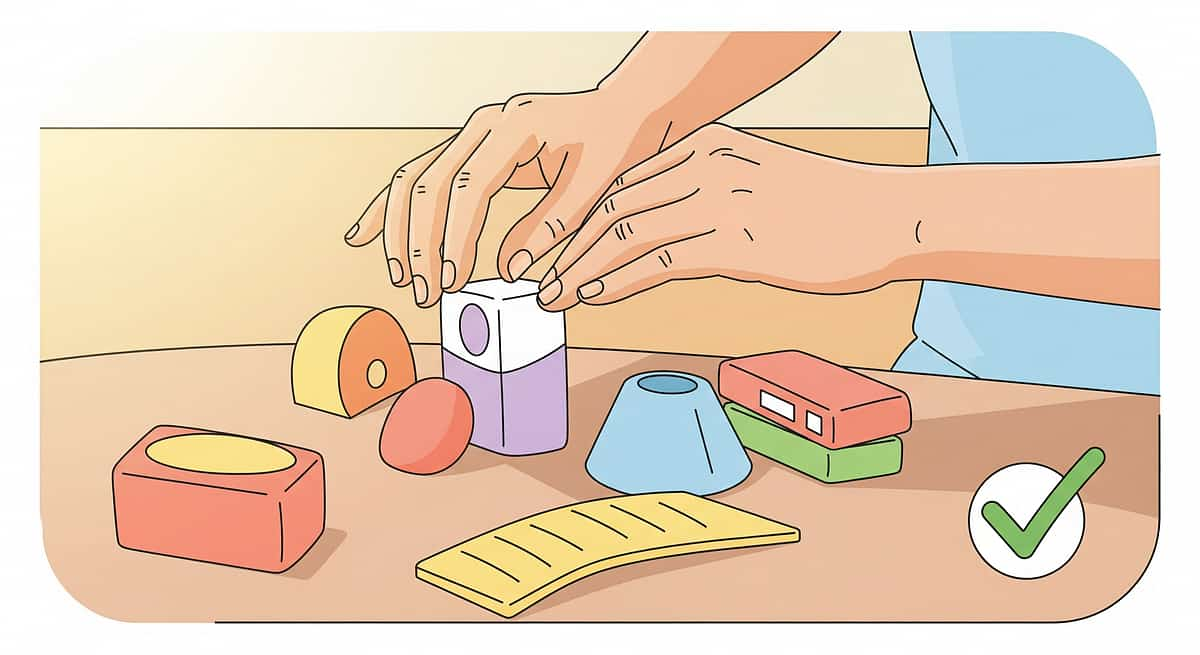
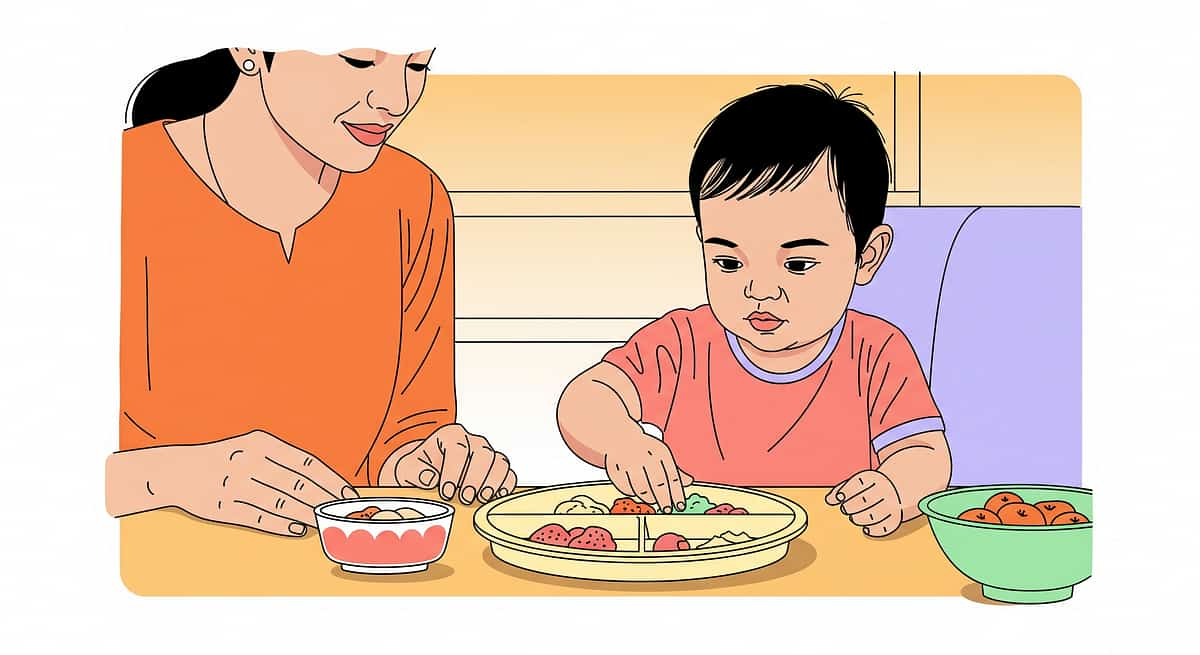
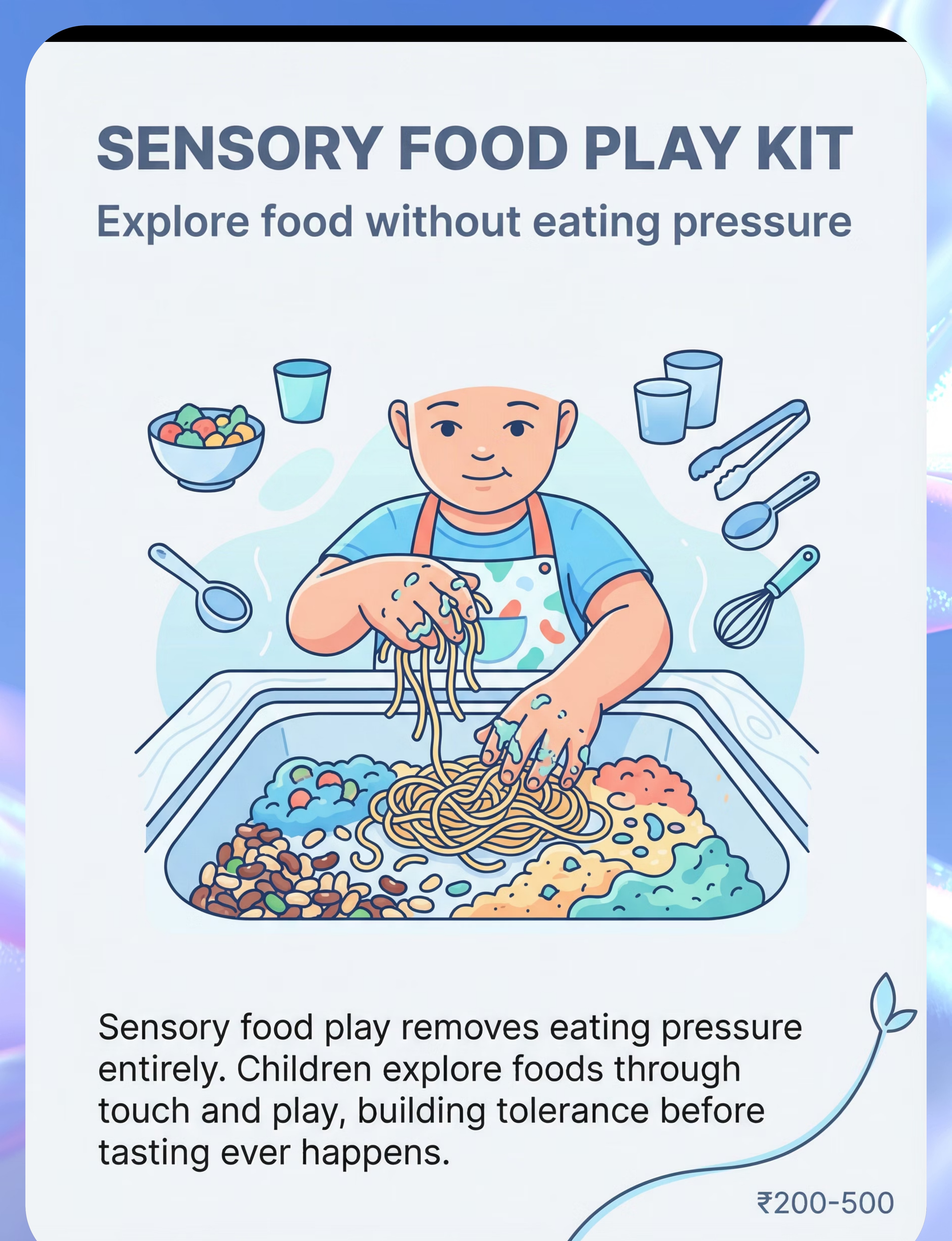
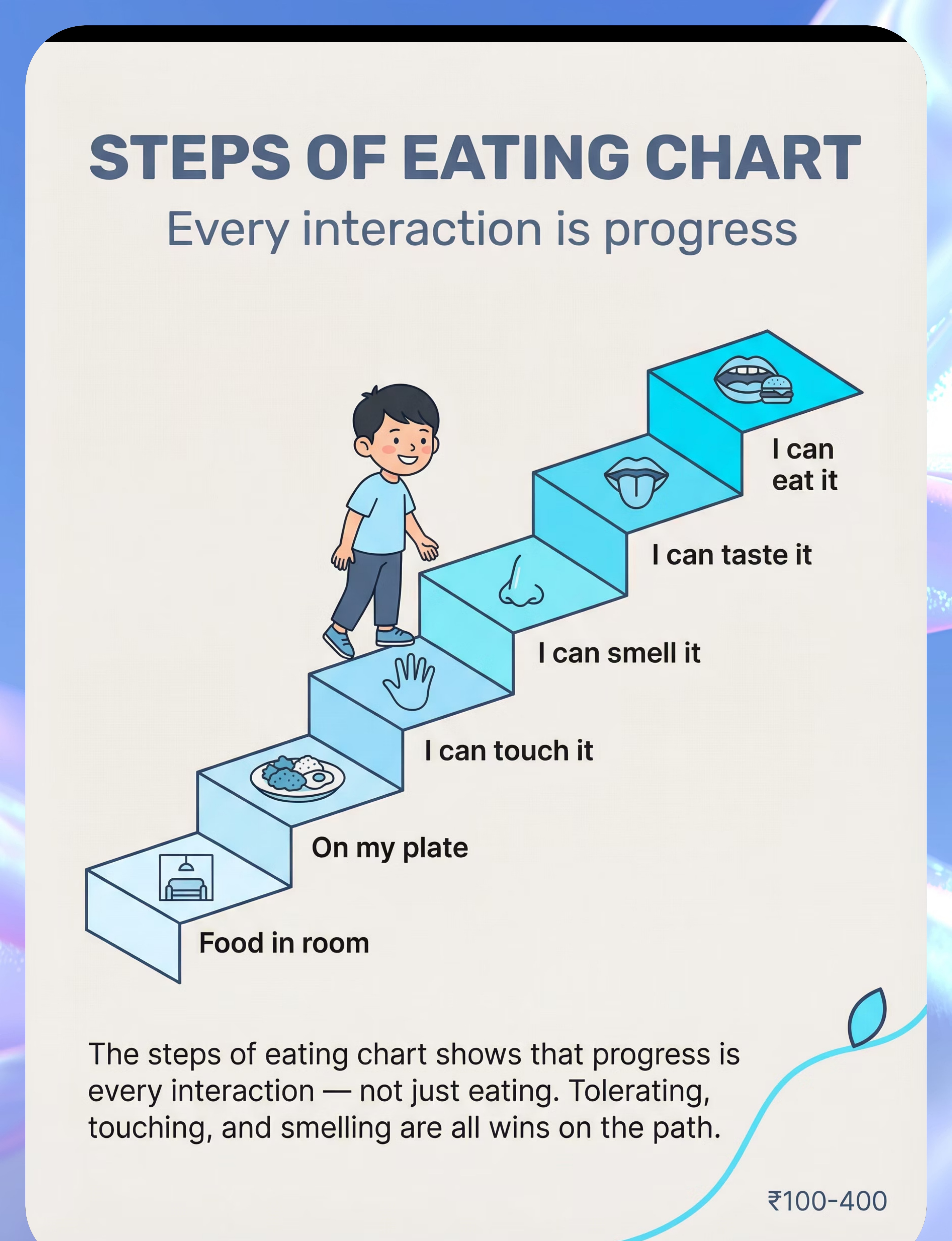
"The best intervention is the one a family can actually access and execute. This page serves families from Bengaluru apartments to rural Bihar homes." — WHO/UNICEF Equity Principle Material Buy This DIY Today Divided Plates Silicone 3-section plate ₹250–500 3 small bowls or a thali with katoris. One katori = learning zone. Food Chaining Cards Printed laminated cards ₹300–600 Index cards + food photos from magazines or phone. Map chains in a notebook. Sensory Food Play Kit Sensory tray + tools ₹300–700 A steel plate, dry dal, cooked rice, pasta. Use the kitchen floor. No special tools needed. Steps of Eating Chart Printed visual chart ₹100–300 Draw 10 steps on paper. Stick on fridge. Use stickers to track progress. Oral Motor Tools Chewy tube ₹500–1,500 Consult your OT first. Some children can use clean silicone teethers. Professional guidance essential. Tiny Serving Tools Baby spoon set ₹150–400 Use the smallest spoon in your kitchen. Medicine droppers for liquids. Toothpicks for single pieces. Food Learning Books Picture books ₹200–600 Print food images from internet. Create a "food book" with the child. Free social story templates online. Food Bridge Cards Card set ₹300–600 Two columns on paper: accepted food / new food / what they share. Child can colour and decorate. Environment Kit Ergonomic chair + dimmer ₹800–3,000 Rolled towel under feet. Remove TV from mealtime. Consistent seating. Dim overhead light with curtains. "The therapeutic mechanism is in the approach, not the price of the material. A ₹0 paper chart used consistently outperforms a ₹2,000 tool used once."

🚦 Safety Gate: Read This Before Starting
🔴 STOP — Medical Clearance Required If: Child gags, vomits, or coughs regularly during eating (possible swallowing disorder) Child has lost significant weight or shows signs of nutritional deficiency You suspect food-related pain (GI disorder, reflux, eosinophilic esophagitis) History of choking requiring Heimlich manoeuvre Fewer than 5 accepted foods with severe anxiety/panic at mealtimes Known food allergy — all new foods must be screened first 🟡 MODIFY — Consult Specialist First If: Child drops accepted foods frequently (food "jags") Growth concerns flagged by pediatrician Child is tube-fed or has feeding device Previous force-feeding history Significant co-occurring anxiety disorder 🟢 PROCEED — Home Protocol Safe When: Medical causes have been ruled out Child is maintaining weight adequately Selectivity is primarily sensory/anxiety-based Child can be present at mealtimes without panic Parent can commit to low-pressure, no-force approach ⚠️ Material Safety: All plates/tools must be food-grade and age-appropriate. Supervise all sensory food play. No oral motor tools without OT guidance. Toothpicks/food picks for children 5+ only, always supervised. Stop the session immediately if child gags, enters true panic, or shows any sign of allergic reaction.📞 9100 181 181 — Speak to a medical professional before starting if any red flags apply

- Turn off TV, music with lyrics, loud background noise
- Dim harsh overhead fluorescent lights (warm lighting preferred)
- Reduce strong cooking smells during the meal (cook 20 min before serving)
- Remove visual clutter from the table
- Child's feet fully supported — activates postural stability and reduces sensory seeking
- Chair height: elbows at table level
- Consistent seat — same chair, same position, every meal
- Same sequence every meal: wash hands → sit → see what's on the table → eat → done
- Predictability = safety = willingness to engage with challenge
- No comments about eating or not eating
- No "just one bite" — this phrase can set back progress weeks
- Adults eat the same/similar food without drawing attention
- Neutral face when child ignores learning food

Indicator | ✅ Green — Proceed | ⚠️ Modify | 🔴 Postpone | |
Fed recently? | Light snack 45 min ago | — | Very full or very hungry | |
Rested? | Alert, not overtired | Slightly tired | Melting down from exhaustion | |
Regulated? | Calm baseline | Some energy, manageable | Active meltdown / shutdown | |
Recent illness? | Healthy | Mild cold | Fever, vomiting, GI upset | |
Emotional state? | Content/playful | Slightly anxious | Severe distress/anxiety | |
Major event today? | Typical day | Minor disruption | Significant stressor (new school, medical procedure) |
"The best feeding session is one that starts right. A session that ends in calm — even with no eating — advances progress."

"It's food time! Come and see what's here today."
- ❌ "Today we're going to try this new food"
- ❌ Point at the learning food
- ❌ Express hope or expectation
- ❌ Ask "Can you try just one bite?"
- Place divided plate with safe foods + one learning food in its section
- Sit beside (not opposite) your child
- Begin eating your own food or doing an activity
- Do NOT draw attention to the learning food
- Wait 30–60 seconds for the child to arrive and settle
- "Mm, this is warm."
- "This has a bit of crunch."
- If child looks at learning food: "Yep, that's [food name]" — then return to your own food
- If child touches learning food spontaneously: say nothing. Let the exploration happen organically.
"You looked right at it. That's really something."
"You touched it! That's a big deal."
- Child turns away repeatedly
- Increased fussiness beyond manageable
- Session has reached 10+ minutes for food play
- Always end while mood is still positive
- Minimum 5–10 successful exposures at current step
- Child shows neutral response (no distress or curiosity) at current step
- Then — and only then — introduce the next incremental change
"3 engaged, willing interactions with a food are worth more therapeutically than 10 forced, distress-filled ones. Always end before resistance peaks." — The 3-Good-Rep Principle

- Any forward movement on the steps of eating hierarchy
- Sitting at the table without protest
- Tolerating learning food on plate without pushing it away
- Engaging with food play
- Using steps-of-eating vocabulary: "I can look at it"
- "Good eating!" (implies eating was the goal)
- Reward charts specifically for eating new foods (creates pressure)
- "Just one more bite" after reinforcing (erodes trust)
- Compare to siblings

Meal: Breakfast / Lunch / Dinner / Food Play
Learning food presented: ___________
Step reached today (circle): 1 / 2 / 3 / 4 / 5 / 6 / 7 / 8 / 9 / 10 / 11
Child's mood at start: Calm / Neutral / Anxious / Distressed
Child's mood at end: Calm / Neutral / Anxious / Distressed
Any spontaneous interaction with learning food? Y / N
Notes: ___________
- Total exposures this week: ___
- Highest step reached this week with this food: ___
- New foods added to accepted list this week: ___
- Any foods dropped from accepted list: ___
Problem | Likely Cause | Solution | |
Child refuses to sit at table | Too much anxiety around food context | Begin at a different location. Snack on floor first. Gradually move toward table over weeks. | |
Child pushes plate off table | Learning food section too threatening | Move to food-in-room only stage. Learning food on a shelf 2 meters away during meals. | |
No progress after 6 weeks | Steps too large OR unaddressed medical/sensory issue | Make steps smaller. Get feeding assessment. Rule out medical cause. | |
Child drops an accepted food suddenly | Sensory over-exposure or mild aversion triggered (food jag) | Don't panic. Maintain availability without pressure. Most jagged foods return in 2–8 weeks. | |
Family pressure ("just make them eat") | Misunderstanding of feeding therapy approach | Share this page with family. Pressure paradoxically worsens selectivity — this is clinical fact. | |
Different behaviour at school/grandparents | Environment and approach inconsistency | All caregivers must use same approach. Use family sharing tools from the Share card. | |
Child accepts food at clinic, refuses at home | Environmental/contextual factors | Recreate clinic conditions at home. Involve the treating therapist in home session design. | |
Parent feels hopeless/exhausted | This is a marathon, not a sprint | This is normal and valid. Progress happens invisibly before it becomes visible. Call 9100 181 181. |

- Start with food in room, not on plate
- Use clear containers so food is visible but contained
- Allow child to smell from distance before any proximity
- Extra slow progressions — weeks per step, not days
- Reduce other sensory demands at mealtimes (noise, lighting)
- Oral motor preparation before meals (chewy tube, vibrating tool)
- Use firmer textures for new food introductions
- Physical activity break immediately before meal
- Strong flavours may be more acceptable than bland ones

- Child stops pushing plate away when learning food is present → Real progress
- Mealtime distress slightly reduced → Real progress
- Child glances at learning food without immediate panic → Real progress
- Child participates in food play session without significant resistance → Real progress
- Child eating the new food
- Any expressed interest in tasting
- Dramatic change in food variety
"If your child tolerates the learning food on their plate for 3 seconds longer than last week — that is genuinely significant neural progress."

"You may notice you're less tense at mealtimes. That matters enormously. Your regulated nervous system directly regulates your child's."

Weeks 5–8 often include setbacks — a food jag, a bad meal, a regression during illness or stress. This is not failure. The neural pathways built in weeks 1–4 don't disappear. Resume the protocol after recovery.

- A child who eats everything
- Neurotypical eating variety
- Eating without any selectivity
- A nutritionally adequate diet — even if still selective
- Family mealtimes that are not battlegrounds
- A child with vocabulary and skills to engage with new foods over their lifetime
"Our son ate 7 foods for three years. After 8 months of this approach, he accepts 25 foods. More importantly, mealtimes are no longer battles. He knows how to meet new foods." — Parent, Pinnacle Network

- Child loses weight or shows growth faltering during the protocol
- Accepted foods continue to drop (repertoire shrinking, not stable or growing)
- Child shows increased anxiety beyond mealtimes — generalised food anxiety affecting daily life
- Gagging or vomiting increases in frequency
- Child stops eating altogether (more than 1 day without adequate intake)
- Signs of nutritional deficiency: extreme fatigue, pale skin, hair loss, dental issues
- Child's distress intensifies rather than reduces over 4 weeks of consistent protocol
- Family cannot maintain low-pressure approach (escalation of mealtime conflict)
Our Feeding Specialists can assess your child's situation and connect you with appropriate resources — in your language, 24×7.
- E-451 — Extreme Picky Eating (overlap technique with different entry angle)
- B-Series — Social Communication (if food selectivity co-occurs with communication avoidance)
- C-Series — Emotional Regulation (if anxiety is primary driver)
- Divided Plates → works with E-451, E-453, E-455
- Steps of Eating Chart → works with E-453, E-454
- Sensory Food Play Kit → works with E-450, E-454
Explore the Full Feeding Mastery Series
Technique Code Difficulty Key Material Extreme Picky Eating E-451 🟢 Entry Divided Plates Very Limited Food Repertoire E-452 🟡 Core Food Chaining Cards New Food Refusal E-453 🟡 Core Steps of Eating Chart Food Texture Aversions E-454 🟠 Intermediate Sensory Food Play Kit Foods Can't Touch E-455 🟠 Intermediate Divided Plates + Social Stories Gagging & Food Refusal E-456 🔴 Advanced Oral Motor Tools

GPT-OS® sees all 12 domains simultaneously. A single intervention on this page is valuable. A coordinated 12-domain plan is transformational.
- Child has fewer than 15 accepted foods
- Home protocol has been consistent for 8 weeks without progress
- Any of the red flags from the Red Flags card apply
- You want supervised, accelerated progress
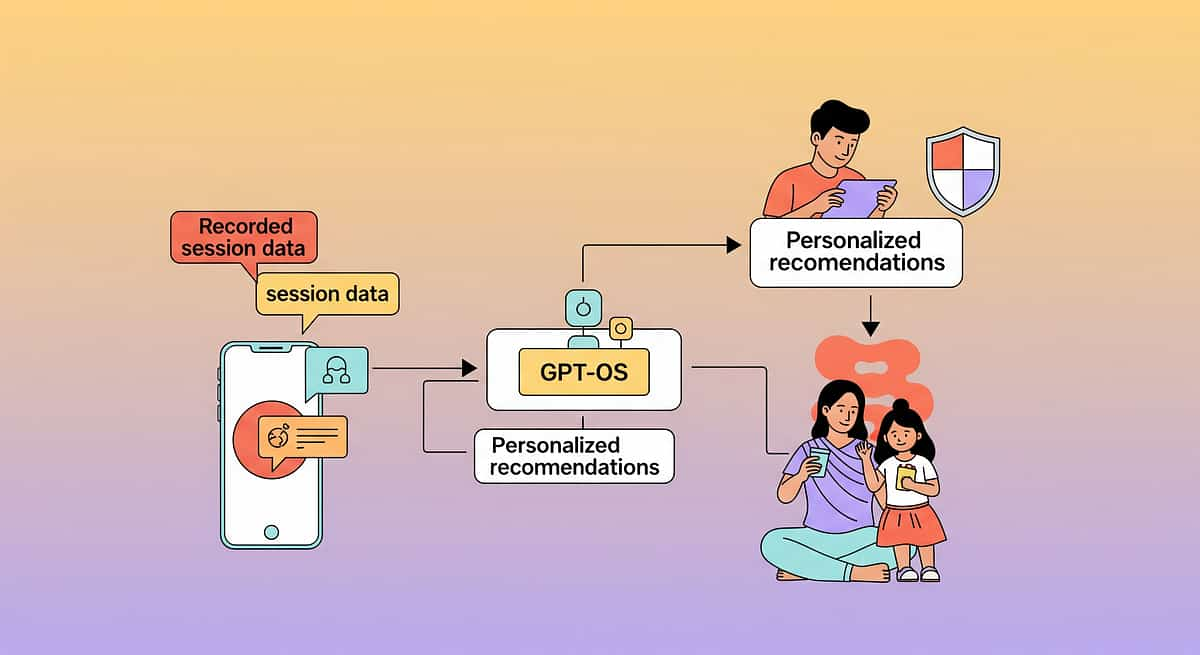
- Current step on the steps-of-eating hierarchy for each target food
- Rate of chain progression (fast, typical, slow — determines next protocol)
- Sensory sensitivity pattern (informs which new foods to chain toward)
- Optimal session timing and frequency for your child
Watch: 9 Materials That Help With Very Limited Food Repertoire
Reel E-452 Feeding & Mealtime Challenges in Children — Episode 452 Series Domain E | Feeding & Mealtime Series | 999 Reels Master Duration 75–85 seconds Neighbouring Reels in the Series: ← E-451 Extreme Picky Eating E-452 (You Are Here) Very Limited Food Repertoire E-453 → New Food Refusal E-454 → Food Texture Aversions Our Consortium Feeding Specialists walk you through all 9 materials — what each one is, exactly how to use it, and what progress looks like when you do. 📞 9100 181 181 — Call if you have questions after watching | @pinnacleblooms | #FeedingTherapy #LimitedFoodRepertoire

One Parent Knowing This Helps. Every Caregiver Knowing This Transforms.
"Caregiver consistency across all feeding contexts multiplies therapeutic impact. One pressure-free mealtime followed by a forced-eating lunch at grandparents' house sets back progress significantly." — WHO CCD Package, Caregiver Training Module WhatsApp Share "Found this page on feeding therapy for [child's name]'s food challenges — really helpful. Please read before the next time you feed them." For Grandparents — Simple Version "When a new food is on the plate: say nothing. Do not encourage, do not comment, do not ask them to try it. Just eat your own food. That's the whole approach. We'll explain why it works when we next meet." For School / Teacher Communication "Our child is in feeding therapy for severe food selectivity. Please serve their packed lunch without comment on what they eat or don't eat. No encouragement to try other foods. This is a medical approach." Download Family Guide PDF — 1 page, FREE Download School Letter Template
Preview of 9 materials that help with very limited food repertoire Therapy Material
Below is a visual preview of 9 materials that help with very limited food repertoire therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.











"From a world where families face their child's developmental challenges alone, frightened, and without tools — to a world where every parent, in every home, in every country, has access to the same precision, science, and support that the world's best therapy centres provide. One technique at a time. One family at a time. At population scale." — Pinnacle Blooms Network®, Mission Statement
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is educational. It does not replace individualised feeding assessment and intervention with licensed feeding specialists, occupational therapists, speech-language pathologists, and healthcare professionals. Consult specialists for persistent or severe feeding challenges. Individual results may vary.