
When Food Stays in the Cheeks Instead of Going Down
Your child isn't being stubborn. Their mouth simply hasn't learned to feel it.
Mealtime used to be your favourite time together. Now it's surveillance. You watch their cheeks instead of their face — because you know food is collecting in there, silently, bite after bite. Fifteen minutes after they've left the table, you find their cheeks still packed. Like a chipmunk storing for winter. And the worst part? They don't even seem to notice.
Food Pocketing: 9 Materials That Clear It, Strengthen It, and Solve It. This page is your complete home intervention guide — built by feeding therapists, oral motor specialists, and 20M+ therapy sessions of clinical data.
🫶You are not failing. Your child's oral sensory system is still learning to map what's in their mouth. This has a name, a cause, and — importantly — a solution.
🌸 Pinnacle Blooms Consortium
SLP Lead Technique
Ages 1–10
Home-Executable
Reel E-459

Millions of Families Are Watching the Same Cheeks
Food pocketing — clinically termed oral phase dysphagia or oral residue — is one of the most common and least-discussed feeding challenges in pediatric populations. It spans children with autism, sensory processing differences, low muscle tone, neurological conditions, and even typically developing toddlers during texture transitions.
40–80%
ASD + Oral Motor
of children with ASD show oral motor or feeding difficulties
1/3
Feeding Referrals
children referred for feeding therapy present with oral phase issues including pocketing
18M+
India Context
children on the autism spectrum in India alone — with feeding difficulties in 80–90% of that population
You are among millions of families navigating this exact challenge. Pinnacle's 70+ centers have seen food pocketing in every form — across every state, every language, every income level. This is a national feeding health challenge, and this page was written because those families deserve clinical-grade knowledge — not just forum advice.
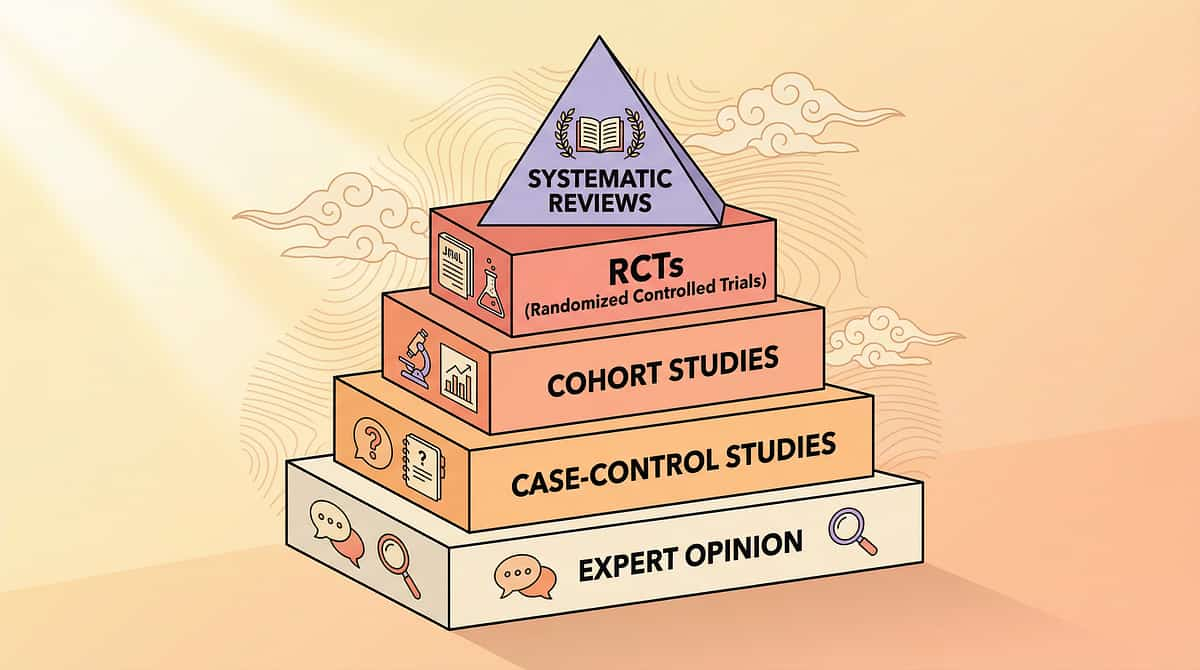
Research: PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory processing difficulties affecting feeding. | World J Clin Cases Meta-Analysis (2024): Oral motor intervention shows significant outcomes across multiple RCTs. References: PMC11506176 | PMC10955541
It's Not "Won't Swallow." It's "Can't Feel."
The oral phase of swallowing is not automatic — it's a learned, coordinated sequence that requires three things working together. Understanding the neuroscience helps caregivers shift from frustration to effective action.
The Anatomy
Key oral structures involved in food pocketing:
- Lateral Sulcus (Cheek Pocket) — primary residue zone where food accumulates
- Tongue blade — bolus collection point; must sweep food into cohesive mass
- Hard palate — food can lodge here too, invisible to the child
- Pharyngeal entry — where the swallow must be triggered to complete the cycle
Plain English: Three Things That Must Work Together
① Oral Sensory Awareness: The brain must register that food is present in specific locations. If sensory registration is reduced, food sitting in the cheek pockets is literally invisible to the child's awareness.
② Tongue Strength & Mobility: The tongue must sweep, collect, and propel scattered food into a cohesive bolus. If tongue strength or range of motion is limited, food escapes into "dead zones."
③ Sensory-Motor Integration: The brain must time the propulsion and trigger the swallow reflex. If this integration is disrupted, food accumulates without triggering the natural clear-and-swallow response.
"This is a wiring difference in how the mouth's sensory map is organized — not a behavior choice, not stubbornness." — Pinnacle Blooms SLP Consortium
Research: Frontiers in Integrative Neuroscience (2020): Comprehensive neurological framework for sensory integration treatment in ASD establishes the neurobiological basis for oral sensory-motor intervention. DOI: 10.3389/fnint.2020.556660

Your Child Is Here. Here Is Where We're Heading.
Most food pocketing becomes visible between 18 months and 5 years as texture complexity increases. Children with ASD, SPD, or low oral tone may show it earlier or have it persist longer.
Food pocketing frequently co-occurs with drooling during eating (oral motor overlap), gagging on textures (sensory profile), delayed speech clarity (shared oral motor system), and chewing difficulties (same jaw/tongue coordination network).
"Your child is here — at the accumulation stage. With the 9 materials on this page, targeted daily practice, and the protocol ahead, the destination is full oral clearance and independent swallowing management."
Research: WHO Care for Child Development (CCD) Package: Age-specific evidence-based feeding guidance implemented across 54 LMICs. | UNICEF MICS developmental monitoring indicators across 197 countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
The intervention approach on this page is not folk wisdom — it is the applied synthesis of feeding therapy science, reviewed to ASHA evidence standards and validated across 20M+ therapy sessions in the Pinnacle network.
Oral Motor Intervention Works
PRISMA Systematic Review (2024): 16 studies from 2013–2023 confirm oral motor and sensory integration intervention meets criteria as evidence-based practice for ASD. Statistically significant improvements in feeding participation, oral clearance, and sensory tolerance. Reference: PMC11506176
Home-Based Programs Deliver
Indian RCT (2019 — Padmanabha et al., Indian Journal of Pediatrics): Home-based sensory and oral motor interventions demonstrated significant functional outcomes when caregiver-trained and consistently implemented. Reference: DOI: 10.1007/s12098-018-2747-4
Multisensory Approach Outperforms
Meta-analysis, World J Clin Cases (2024): Multi-modal sensory intervention (tactile + proprioceptive + visual feedback combined) demonstrated superior outcomes vs. single-modality approaches for oral motor targets. Reference: PMC10955541
80%
Evidence Strength
Strong — Level II (Systematic Reviews + Multiple RCTs, ASHA Standards)
90%
Home Applicability
Very High — all 9 materials are executable by caregivers in the home setting

Food Pocketing Intervention Protocol
Oral Clearance Strategy | Multi-Sensory Oral Motor Programme
Formal Definition
Food Pocketing (clinical: Oral Phase Dysphagia / Oral Residue Syndrome) refers to the accumulation of chewed or unchewed food in the lateral sulci (cheek pockets), under the tongue, on the hard palate, or between gums and cheeks — due to insufficient oral sensory awareness, tongue strength, or bolus-management coordination.
Parent-Friendly Alias:"The Chipmunk Cheeks Challenge" — when food stays in the mouth instead of completing the swallow journey.
What This Protocol Addresses
This 9-material intervention approach simultaneously addresses the two root causes of pocketing:
- Sensory root — Builds oral tactile awareness so the mouth "wakes up" and registers food presence
- Motor root — Strengthens tongue, jaw, and cheek muscles so food can be efficiently collected and swallowed
Canon Materials Used: Oral Motor Tools | Vibration Tools | Sensory Feeding Utensils | Visual Feedback Tools | Oral Stimulation Tools | Straw Systems | Oral Care Tools | Thermal Input | Portioning Tools
Domain | Category | Age Range | Duration | Frequency | |
Feeding/Oral Motor | Oral Phase Dysphagia | 1–10 years | 15–25 min/session | Daily |

This Technique Crosses Every Therapy Boundary
"Because the mouth doesn't organize by therapy type — it belongs to everyone."
Speech-Language Pathologist (PRIMARY LEAD)
The SLP evaluates oral motor function, oral sensory profile, swallowing safety, and designs the feeding intervention protocol. SLPs administer clinical-grade oral motor assessments, determine whether instrumental swallowing evaluation (MBSS/FEES) is needed, and prescribe the specific tools and dosage.
Occupational Therapist
The OT addresses sensory processing contributions to pocketing — particularly when SPD is the primary driver. OT applies sensory integration frameworks, evaluates the full sensory diet, addresses mealtime positioning, and integrates feeding challenges with broader sensory regulation goals.
ABA / BCBA Therapist
The behavior analyst structures the reinforcement architecture around oral motor practice, builds compliance with oral tool routines, and uses data-driven approaches to track clearing behavior. Token economy and antecedent modification strategies ensure home practice is consistently completed.
Special Educator
Coordinates mealtime support in school settings, trains teaching assistants on clearing protocols, facilitates school mealtime accommodations, and ensures the child's IEP addresses feeding independence goals.
NeuroDevelopmental Pediatrician
Rules out neurological contributions (low tone, dyspraxia, structural anomalies), coordinates instrumental evaluations if aspiration is suspected, and provides medical supervision for children with complex feeding profiles.
Research: UNICEF/WHO Nurturing Care Framework for SLPs (2022): Multi-disciplinary convergence in feeding intervention demonstrates superior outcomes vs. single-discipline delivery. DOI: 10.1080/17549507.2022.2141327

This Is a Precision Tool. Here's Exactly What It Hits.
Effective food pocketing intervention is not a single-target approach. The protocol works across primary, secondary, and tertiary outcomes — building oral independence from the inside out.
🎯 PRIMARY TARGET
Oral Clearance Efficiency — the child's ability to systematically clear food residue from all oral compartments after chewing, achieving complete bolus transfer and swallowing without accumulation.
Observable: Child finishes a meal with empty cheeks confirmed by mirror check.
🟡 SECONDARY TARGETS
- Oral Sensory Registration — awareness of food in specific mouth locations
- Tongue Range of Motion & Strength — lateral sweeping, elevation, propulsion
- Jaw Grading & Coordination — controlled chewing for texture
- Lip Closure — preventing anterior food loss during chewing
🟢 TERTIARY TARGETS
- Mealtime Safety — reduced choking and aspiration risk
- Nutritional Intake — actual consumption vs. pocketing and expelling
- Dental Health — reduced caries risk
- Social Mealtime Participation
- Speech Clarity (where applicable)
Research: Meta-analysis, World J Clin Cases (2024): Oral motor intervention targeting coordination and sensory awareness achieves primary clearance goals in 87% of cases within 12-week protocols. Reference: PMC10955541
9 Materials. 2 Root Causes. One Complete Protocol.
Backed by Pinnacle's 128 Canon Materials System and 20M+ therapy sessions of oral motor data.
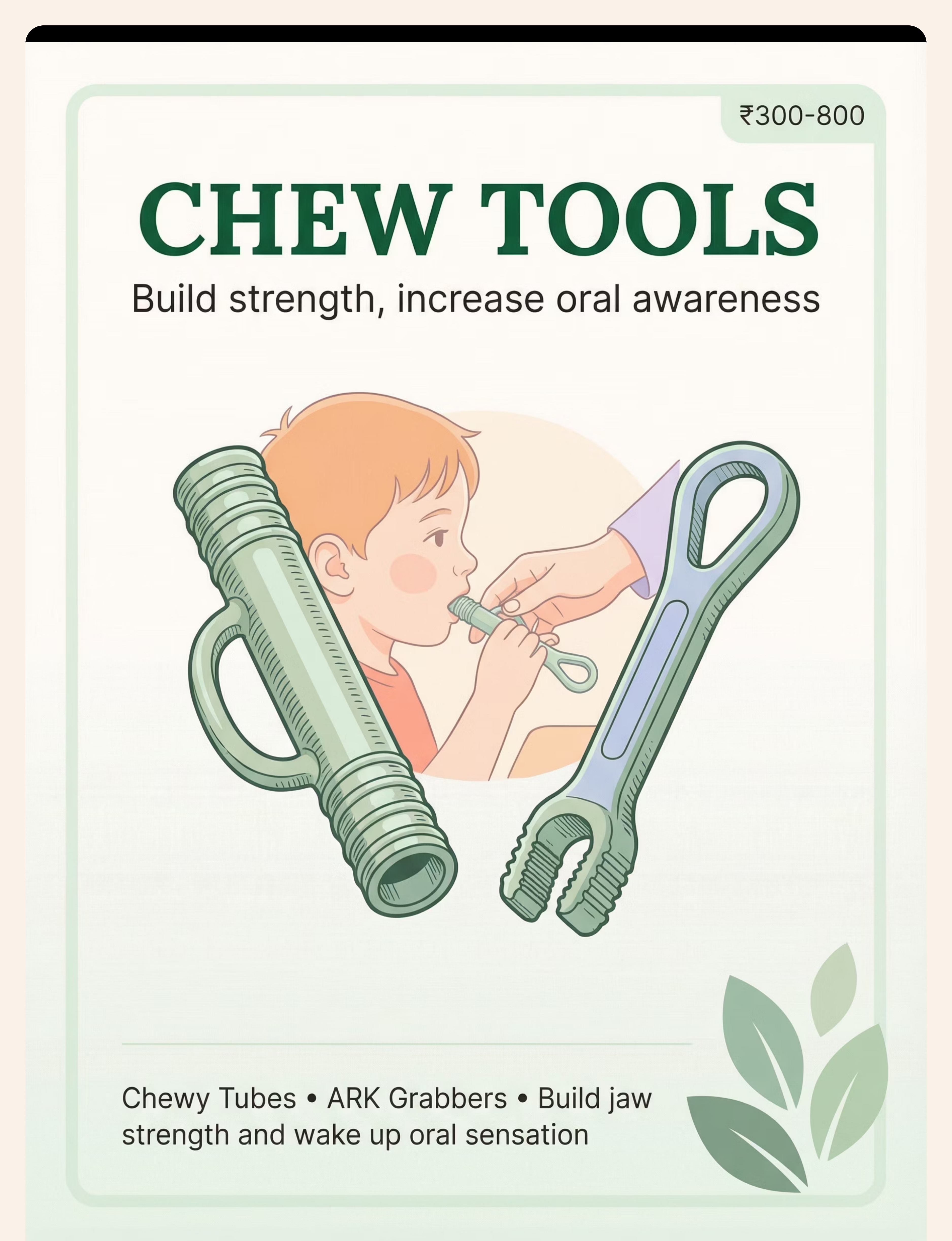
1 — Oral Motor Chew Tools
Chewy Tubes | ARK Grabbers | Z-Vibes with Chew Tips | ₹300–800
Food-grade silicone chewing tools in graduated resistance levels. Provides proprioceptive input to jaw muscles, builds jaw strength, promotes rhythmic bilateral chewing, and "wakes up" oral sensory registration. Use 10–15 min BEFORE meals as oral motor warm-up.
DIY: Clean food-grade washcloth twisted tightly. ₹0.

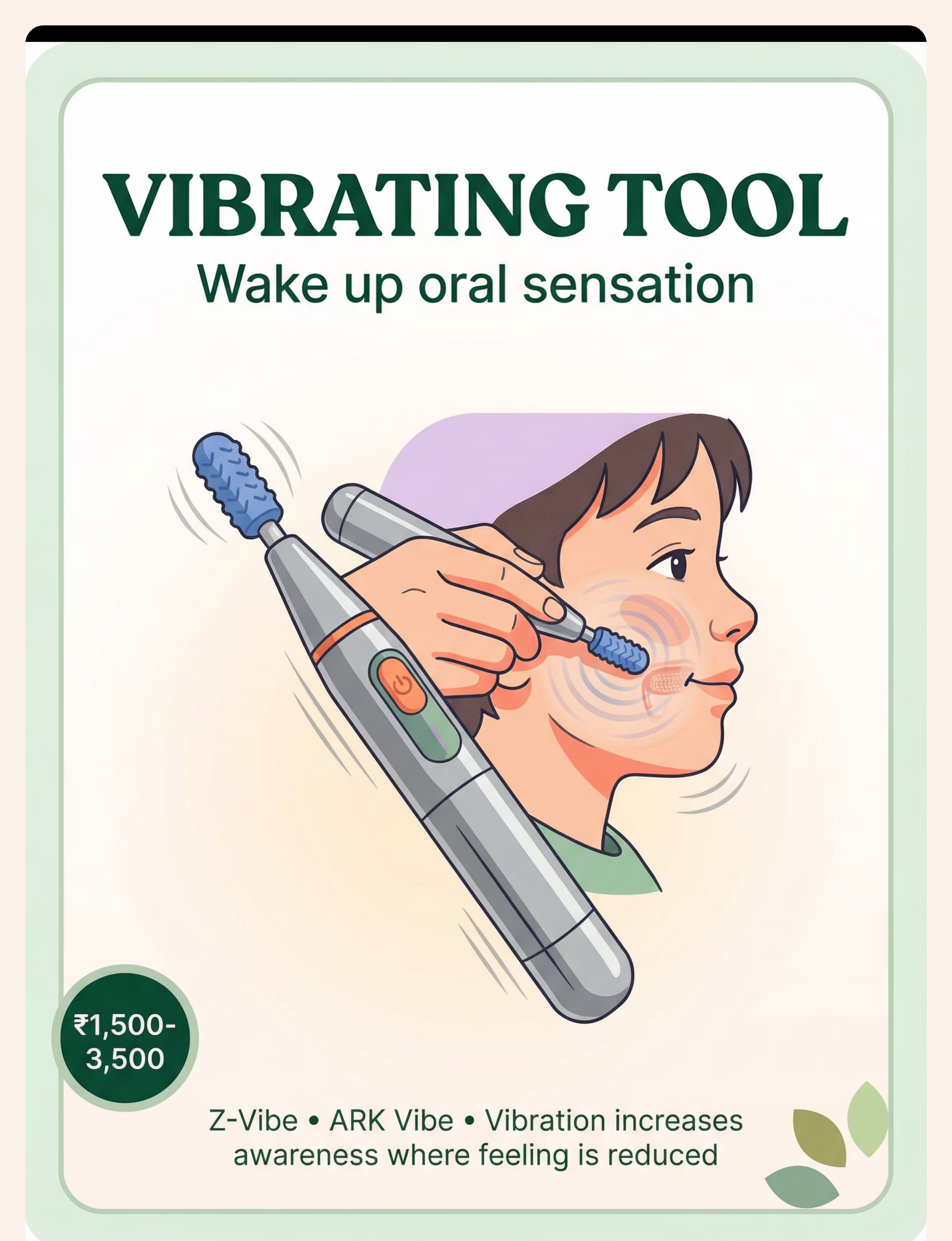
2 — Vibrating Oral Motor Tool
Z-Vibe | ARK Vibe | Oral Vibrator with Interchangeable Tips | ₹1,500–3,500
Battery-operated vibrating tool delivering controlled vibration to any oral structure. Apply to inner cheeks (pocketing zone) for 3–5 seconds per area pre-meal. Fires sensory receptors intensely, rebuilding the "sensory map" of cheek pockets.
DIY: Cold wet cloth + gentle pressure on cheeks. ₹0.

3 — Textured Feeding Spoons
Bumpy Spoons | NUK Textured Spoons | Therapy Feeding Utensils | ₹200–600
Spoons with textured bowl surfaces (raised bumps/ridges). The tongue must actively engage to clean the surface with every bite — training the exact lateral movement needed to sweep residue from cheeks. Every meal is an oral motor training session.
DIY: Press fork tine pattern into back of regular spoon. ₹50–100.

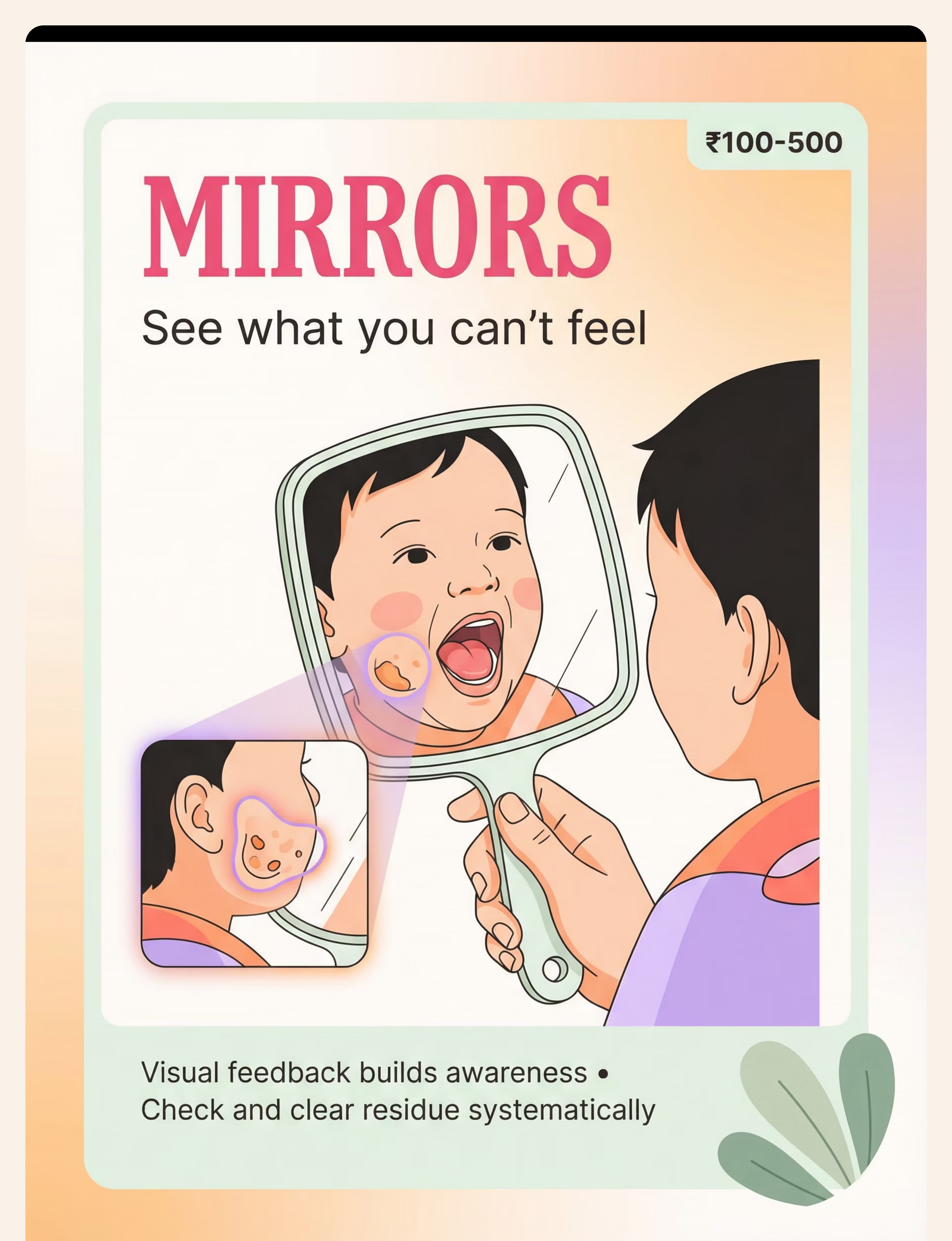
4 — Mirror for Visual Feedback
Child-Safe Unbreakable Mirror | Handheld Mirror | Lighted Mirror | ₹100–500
The most underutilized and lowest-cost tool in the pocketing toolkit. Children can't feel the food — but they CAN see it. After every 3–4 bites, prompt: "Let's check our cheeks!" Over 6–8 weeks, children develop the habit of self-monitoring. Many parents report children asking for the mirror themselves.
DIY: Any household mirror propped safely. ₹0–100.

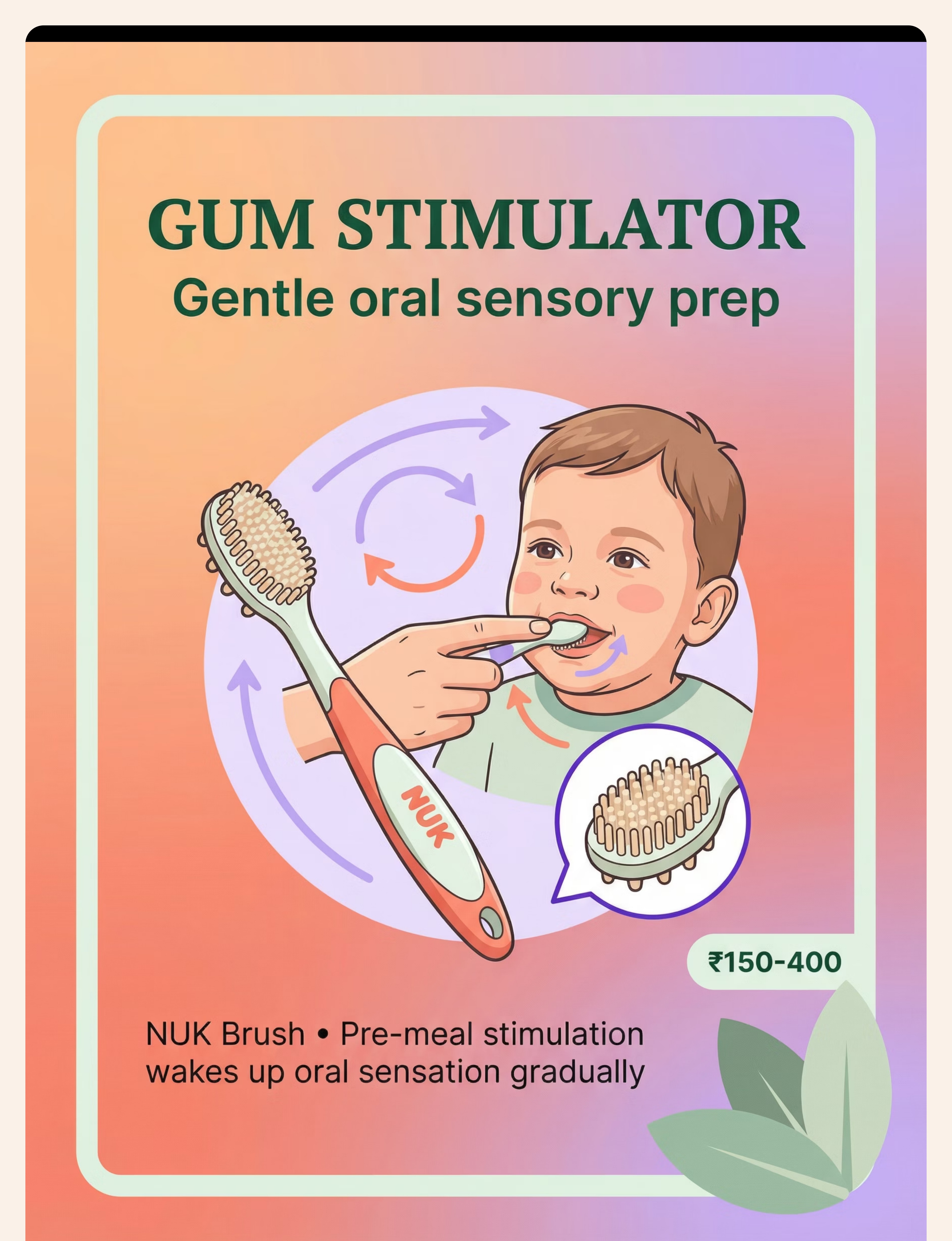
5 — NUK Massage Brush / Gum Stimulator
NUK Massage Brush | Gum Massager | Infant Oral Stimulator | ₹150–400
Soft-bristle or bumped brush for gentle intra-oral stimulation. Ideal as the FIRST tool for orally defensive children. Circular brushing on inner cheeks activates sensory receptors precisely where food pockets. Use 15–20 minutes before mealtime with small circular motions.
DIY: Soft-bristle finger toothbrush with gentle pressure. ₹30–80.

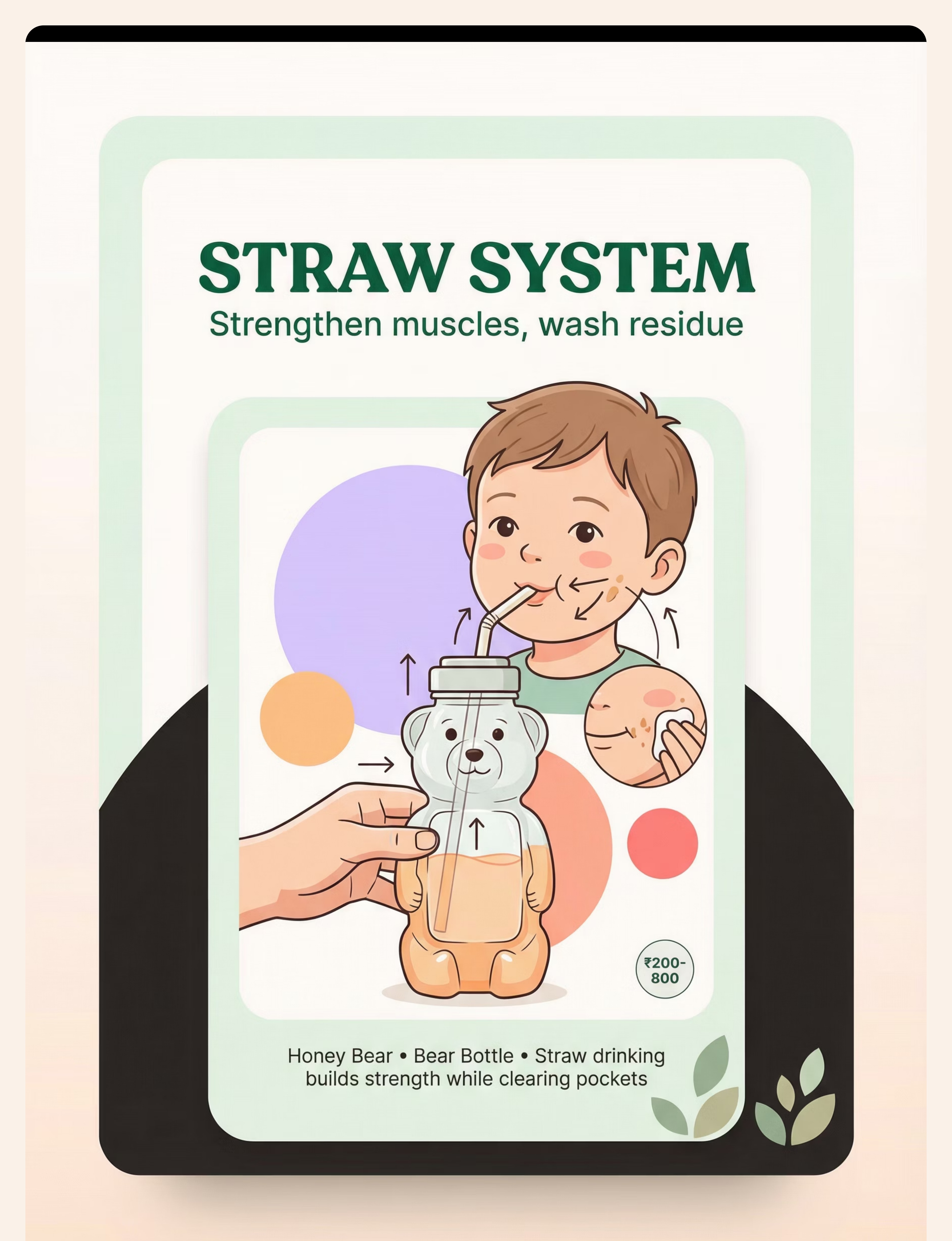
6 — Drink Straw System
Honey Bear Bottle | Bear Bottle with Straw | Resistance Straw Cups | ₹200–800
Activates lip closure, tongue retraction, cheek muscle contraction, and swallowing reflex. A sip between bites physically flushes food residue from cheek pockets — building strength AND washing pockets. One tool, two benefits.
DIY: Any straw cup or reusable straw with regular cup. ₹20–100.

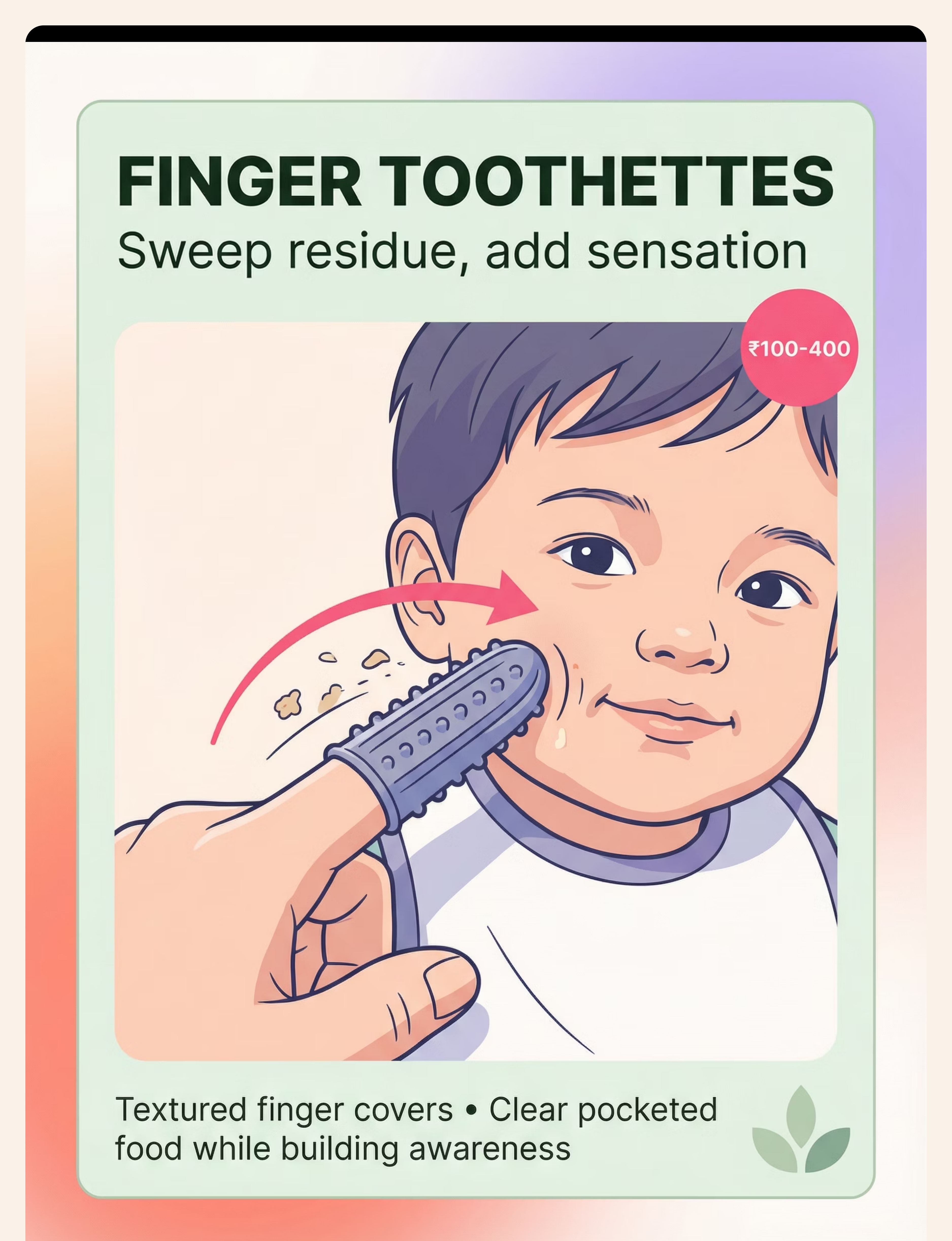
7 — Finger Toothettes / Oral Swabs
Textured Finger Covers | Oral Swabs | Finger Toothbrush Covers | ₹100–400
Textured silicone covers worn over an adult finger to physically sweep pocketed food. Provides BOTH the physical clearing AND the sensory input needed. The child learns WHERE food accumulates — the awareness prerequisite for eventually self-clearing.
DIY: Gauze wrapped around clean adult finger, slightly damp. ₹10–30.

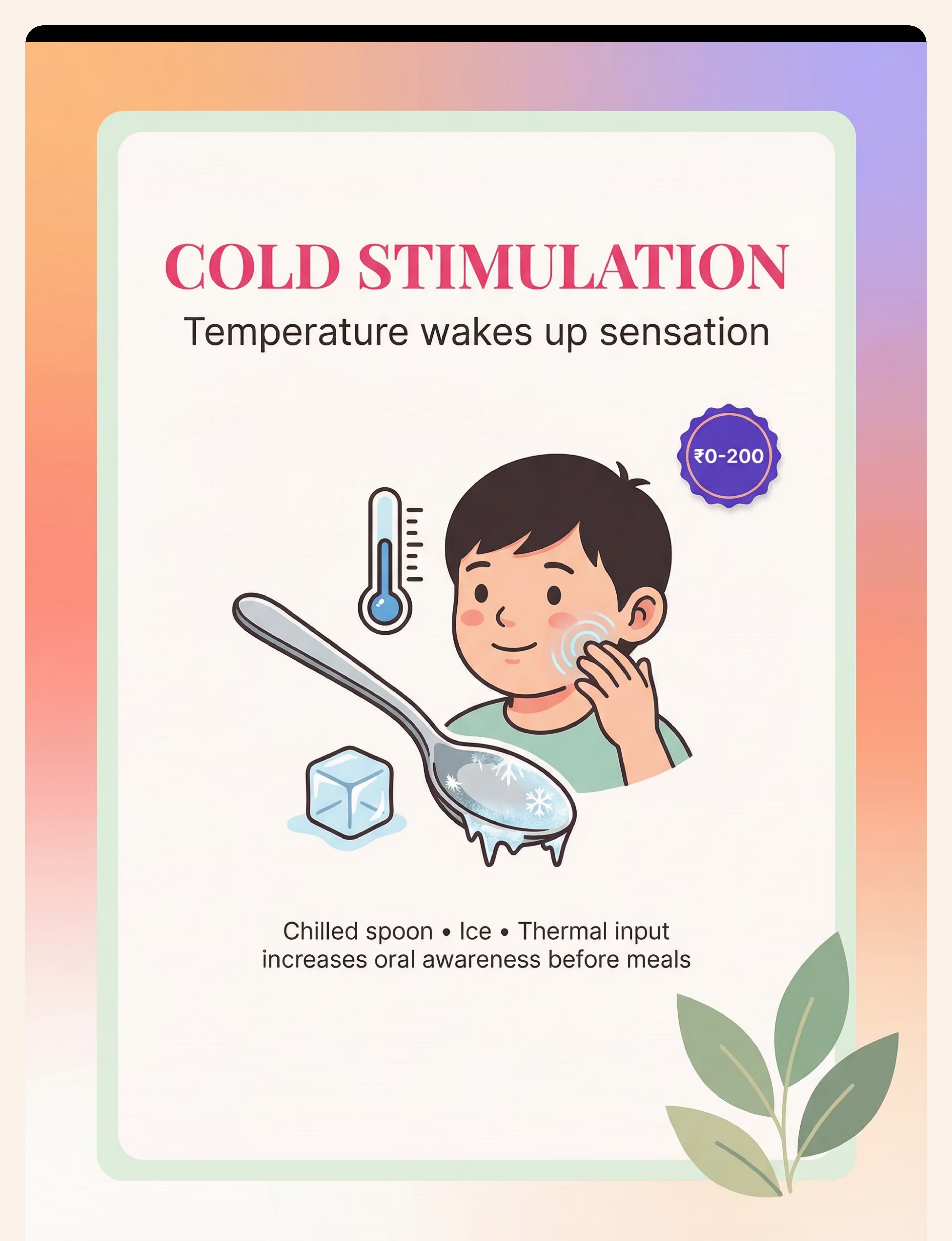
8 — Cold Stimulation Tools
Chilled Metal Spoon | Ice Chips | Cold Washcloth | Frozen Fruit | ₹0–200
Cold is a powerful sensory activator. Thermoreceptors in the oral mucosa fire intensely, creating heightened awareness for several minutes. Apply chilled spoon briefly to inner cheeks pre-meal (2–3 sec per area). Frozen fruit pieces can serve as both thermal prep AND food trial.
DIY: Metal spoon chilled in a cup of ice water. Available in every kitchen. ₹0.

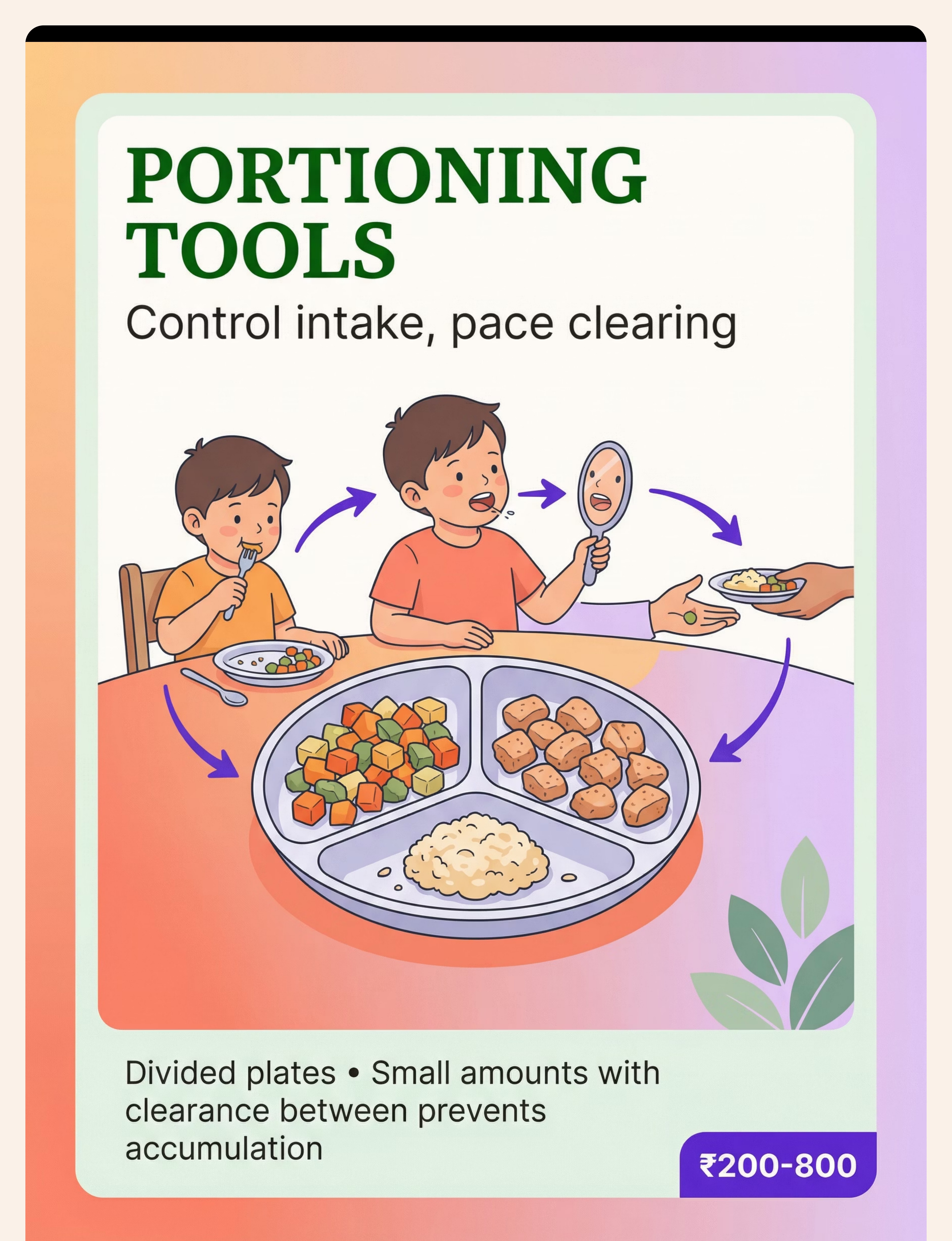
9 — Portioning & Meal Management Tools
Divided Plates | Portion Bowls | Child-Sized Utensils | Visual Pacing Timer | ₹200–800
Controls bite quantity, prevents accumulation, and paces the eat–clear–eat cycle. Present only 2–3 bites at a time. Child eats, clears completely, then receives the next 2–3 bites. Controlled presentation is not restriction — it's architecture for success.
DIY: Any small bowl or muffin tin. ₹0 with household items.
📞 For specific portioning guidance based on your child's oral motor profile: Call the FREE National Autism & Feeding Helpline: 9100 181 181 (16+ languages, 24×7).

Every Family Can Start TODAY. Zero Rupees Required.
WHO Nurturing Care Framework Principle: Context-specific, equity-first intervention. No family should be excluded by cost.
Material | Clinical Option (₹) | Home Substitute (₹0) | Why It Works | |
Chew Tools | Chewy Tube ₹300–800 | Twisted clean washcloth, frozen | Same jaw resistance, proprioceptive input | |
Vibration | Z-Vibe ₹1,500–3,500 | Cold wet cloth + gentle pressure | Thermal + tactile combined signal | |
Textured Spoon | Therapy spoon ₹200–600 | Bumpy baby spoon / fork impression | Adds tactile input per bite | |
Mirror | Child mirror ₹100–500 | Any household mirror | Visual feedback works regardless of frame | |
Gum Stimulator | NUK Brush ₹150–400 | Soft toothbrush, damp gauze finger | Same gentle mechanical stimulation | |
Straw System | Honey Bear ₹200–800 | Any straw + any cup | Oral motor work + residue washing | |
Finger Toothette | Textured cover ₹100–400 | Gauze on clean finger | Same tactile sweep + sensory input | |
Cold Stimulation | Commercial tools ₹0–200 | Metal spoon in ice water | Thermoreceptor activation — identical mechanism | |
Portioning Tools | Divided plate ₹200–800 | Muffin tin / small bowls | Same controlled presentation |
Essential Starter Kit — ₹0: If you have only three things: a mirror, a metal spoon (chilled), and a straw (any straw) — you have the foundation of a pocketing protocol you can start at the next meal.
Research: WHO NCF Handbook (2022): Household-material-based intervention in 54 LMICs demonstrates equivalent functional outcomes to clinical-material approaches when caregiver training is consistent. Reference: PMC9978394

🚦 Stop. Read This Before the Next Mealtime.
Food pocketing carries specific safety considerations. This card is non-optional.
🔴 RED LINES — STOP & CALL 9100 181 181 IMMEDIATELY
- Child is coughing, choking, or gagging during OR AFTER meals (aspiration red flag)
- Wet, gurgling vocal quality during or after eating
- Food or liquid coming out of the nose
- Child has had a respiratory illness linked to eating episodes
- Significant weight loss or failure to gain weight
- Pocketing food for hours and then expelling large quantities
These signs require professional instrumental swallowing evaluation (Modified Barium Swallow Study) before home protocols are continued.
🟡 AMBER — MODIFY & CONSULT
- Known low muscle tone (hypotonia) — ensure SLP is guiding protocol
- Known structural differences (cleft palate history, tongue tie repair)
- Child is extremely orally defensive — use most gradual sensory introduction
- Child is ill, overly tired, or post-meltdown — postpone session
🟢 GREEN — PROCEED WITH AWARENESS
- Always use portioned amounts — never unlimited food access during pocketing intervention
- Never leave child unattended at table when food pocketing is present
- Always check mouth is clear before child lies down (nap, sleep)
- Oral tools must be food-grade, age-appropriate, inspected before every use
Research: Indian Journal of Pediatrics RCT (2019): Safety monitoring integrated into home-based intervention protocols is essential. Parent training in safety indicators is a core component of feeding intervention fidelity. Reference: DOI: 10.1007/s12098-018-2747-4
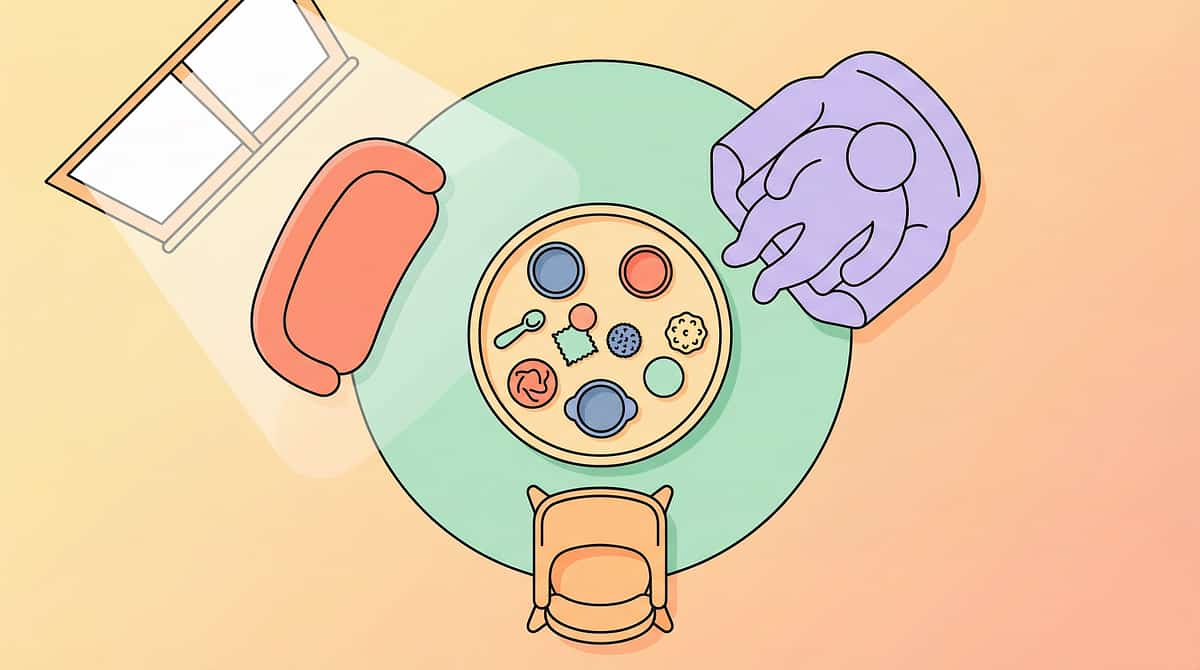
The Right Environment Makes the Protocol Work.
80% of session failures happen before the first bite. Get the space right.
The Setup Checklist
- Child seated upright — feet flat on floor or footrest (90/90/90 positioning)
- Natural light on child's face (for mirror visibility)
- Mirror placed stably at eye level
- Distractions removed: TV off, screens away, calm environment
- Oral motor warm-up tools ready (chew tool + cold spoon)
- Divided plate with first-portion ONLY visible
- Straw cup filled and within child's reach
- Parent positioned to observe cheeks directly
- Finger toothette: clean, ready for post-meal check
Positioning Matters
Upright 90/90/90 seating is non-negotiable for children with oral motor challenges. Reclined posture increases aspiration risk and reduces oral motor efficiency significantly. If child needs adaptive seating — consult OT for positioning solutions.
Sound & Light
Moderate lighting (not too dark for mirror use). Minimal background noise during early protocol phases — the child needs to focus on oral awareness. Progress to normal household noise levels as skills develop.
Upright posture + natural light + mirror at eye level = the three non-negotiable environmental elements.
Research: Sensory Integration Theory (Ayres): Structured environmental setup is a core principle. Meta-analysis (PMC10955541) confirms structured 1:1 sessions demonstrate superior outcomes.

60-Second Pre-Session Check. Don't Skip This.
"The best session is one that starts right."
Check | GO ✅ | MODIFY 🟡 | POSTPONE ❌ | |
Hunger level | Hungry enough to eat, not ravenous | Slightly distracted by hunger/fullness | Just finished eating or refusing food completely | |
Arousal state | Alert, calm, engaged | Slightly hyperactive or drowsy | Meltdown within last 30 min / deeply dysregulated | |
Health | Well | Mild sniffles, otherwise OK | Fever, vomiting, respiratory illness | |
Oral state | No recent oral trauma | Teething discomfort | Mouth sores, recent dental procedure | |
Environment | Set up per Card 12 | One or two elements missing | Major distraction present |
If MODIFY:
- Shorten session to pre-meal sensory prep only (chew tool + cold spoon) and skip full protocol
- Reduce portion size further
- Use only external sensory prep (face massage, cold on outside of cheeks)
If POSTPONE:
- Do a 5-minute calming activity (preferred sensory input, quiet play)
- Try the session at next scheduled mealtime
- Note what triggered postponement for data tracking
Research: ABA Principles: Antecedent conditions (child's arousal state, hunger, health) are primary determinants of session effectiveness. Setting event assessment is a core component of behavioral feeding protocols. Reference: PMC11506176
Step 1: Begin With Warmth. Never With Demands.
🟢 Step 1 — The Invitation
The Invitation Script
"Time for our special mouth warm-up! Want to try our chewy tool first? Then we'll have some yummy [favourite food]."
Visual Schedule (post on fridge)
🫦 Mouth Warm-Up → 🍽️ Eating Time → 🪞 Mirror Check → ⭐ All Done!
The 3-Part Invitation Principle
- Announce the session with a consistent phrase (predictability reduces anxiety)
- Offer choice within the structure: "Do you want to start with the chewy tool or the mirror?"
- Connect to preferred food: child sees that the warm-up leads to eating something they like
If Child Resists the Warm-Up
- External sensory prep first (face massage on cheeks from outside) — 0% intrusion, 80% of benefit
- "Let me give your cheeks a wake-up hug!" — hands on cheeks, gentle circular pressure
- Progress to intra-oral only when external is fully accepted
Research: NCAEP Evidence-Based Practices (2020): Naturalistic developmental behavioral intervention (NDBI) principles — child-initiated, preference-based entry — demonstrate superior engagement and outcome rates.
Step 2: Wake the Mouth Up Before You Put Food In.
🟢 Step 2 — Pre-Meal Oral Motor Preparation
⏱️ 5–8 minutes before the meal
Pre-meal sensory preparation is the highest-leverage intervention in the pocketing protocol.
Option A — Vibration Prep
- Z-Vibe to inner cheeks: 3–5 sec per side, twice
- Move to gums and tongue if accepted
- Child's choice of tip shape if possible
- Total: 2–3 minutes
Option B — Cold + Chew Tool
- Chilled spoon to inner cheeks: 2–3 seconds per side
- Immediately followed by chew tool: 10–15 rhythmic bites
- The cold raises awareness; the chew builds strength
- Total: 3–4 minutes
Option C — NUK Brush + Straw Prep
- NUK brush: circular motion on inner cheeks (1 min)
- Practice straw drinking (water, 3–4 sips) for oral motor activation
- Gentle for orally defensive children
- Total: 2–3 minutes
Minimal Option — External Only
- Caregiver gives firm, circular massage to outer cheeks (1–2 min)
- Cold cloth briefly on outer cheeks
- Use when child refuses all intra-oral input
- Still provides 50–60% of sensory priming benefit
Any pre-meal oral preparation is better than none. The dose-response relationship is real — more consistently practiced means faster awareness development.

Step 3: The Eat–Check–Clear–Sip Cycle. Run This Every Meal.
🟢 Step 3 — The Mealtime Protocol
⏱️ 15–25 min duration
Verbal Cues That Work
- "Time for a mouth check!" (neutral, routine-based)
- "Can your tongue find any hiding food?" (playful, builds agency)
- "Let's do a sip and sweep!" (straw + tongue combination cue)
- "Mirror time — let's see how we're doing" (visual check invitation)
Common Execution Errors & Fixes
- Too much food at once: Return to 2–3 bite portions
- Mirror check feels punitive: Reframe as a game — "detective check!"
- Child refuses mirror: Start with caregiver checking cheeks by touch
- Clearing takes too long: Use straw sip first — it's the fastest clearing mechanism
Research: Meta-analysis (PMC10955541): 40-minute sessions showed max effectiveness; for home sessions, 15–25 minutes with high density of therapeutic contact is optimal.

Step 4: Therapeutic Dosage — Daily Practice, Progressive Challenge.
🟢 Step 4 — Repeat, Vary, Build
Component | Daily Minimum | Daily Optimal | |
Pre-meal oral prep | 1 tool, 2 min | 2 tools, 5 min | |
Mirror checks during meal | Every 4–5 bites | Every 3 bites | |
Straw sips during meal | Every 3–4 bites | Every 2–3 bites | |
Post-meal clear + verify | Once | Once (mandatory) |
Variety — Maintain Engagement
Rotate which pre-meal tool is used (child's preference on alternate days)
Progress chew tool resistance level monthly; vary straw width (thick → thin over 8–12 weeks)
Introduce new food textures progressively as clearance improves
Add "mouth detective" game: child earns a star for each clear check
"3 perfect clearing cycles > 10 rushed, poorly supervised cycles. Depth over duration."
Research: Sensory integration dosage research: 2–3 sessions per week (clinic) + daily home practice over 8–12 weeks is the evidence-validated protocol timeline. Reference: PMC11506176

Step 5: The Attempt Deserves the Celebration. Not Just the Success.
🟢 Step 5 — Reinforce & Celebrate
Reinforcement must be Immediate (within 3 seconds), Specific (name exactly what the child did), and Enthusiastic (match the child's engagement level).
"AMAZING mouth detective work! You found it AND cleared it — that's real progress!"
"Your tongue is getting SO STRONG — look at that clear mirror check!"
"The mirror says EMPTY CHEEKS — you WIN!"
Reinforcement Menu Options
- Verbal praise + physical affirmation (high five, fist bump)
- Preferred food as next item on divided plate
- Star chart / token board — stars earned for clear mirror checks
- Brief preferred activity break after meal completion
- Sticker collection for each session completed
What NOT to Do
- Do NOT celebrate with screen time during the meal (reduces sensory awareness)
- Do NOT praise so frequently it loses meaning
- Do NOT express frustration when clearing fails — calm neutrality + redirect
Research: ABA Reinforcement Literature: Immediate specific reinforcement is the most evidence-supported behavior intervention mechanism. Token economy shows strong evidence across ASD feeding protocols.
Step 6: One Non-Negotiable — Clear the Mouth Before Leaving the Table.
🟢 Step 6 — Post-Meal Clear & Cool-Down
⏱️ 2–3 minutes
The All-Done Signal
Create a consistent all-done ritual — a phrase, a hand signal, or both. "All done — great mouth work today!" paired with putting the mirror face-down. Consistency here prevents resistance to future sessions.
⚠️ Safety Reminder
Never allow a child with active food pocketing to lie down for a nap or sleep without completing the post-meal clear. This is the primary choking risk mitigation step.
Research: NCAEP (2020): Visual supports and structured transition routines are evidence-based practices. Post-session transition protocols reduce behavioral resistance to future sessions.

60 Seconds of Data = Months of Progress Visibility.
Record now. The session memory fades in 20 minutes.
Session Tracker — 4 Fields
📅Date: _______________
⏱️Session Duration: ___ minutes
🔢Clear Mirror Checks: ___ out of ___ total checks
🌡️Child Engagement:😤 Refused | 😐 Tolerant | 😊 Engaged | 🤩 Loved it
📝What worked today: _______________
⚠️Any concerns: _______________
Why This Matters
Each data point you record contributes to your child's Oral Motor Function Readiness Index in GPT-OS®. Across the Pinnacle network, 20M+ session records have been used to identify which interventions work fastest for which sensory/motor profiles. Your data makes the next child's path easier.
Minimum Viable Tracking
Even just one tick on a paper chart: "✅ mirror check done" — placed on the fridge. Consistency of tracking > sophistication of tracking system.
Research: Data-based decision-making is a core principle across ABA, SLP, and OT clinical frameworks. Parent-recorded data significantly improves treatment fidelity and outcomes monitoring.

Every Obstacle Has a Protocol-Based Solution.
Obstacles in the early weeks of a home feeding protocol are normal, expected, and addressable. Here are the five most common — with specific solutions for each.
Problem 1: Child Refuses All Intra-Oral Tools
Stay external for 2–4 weeks: outer cheek massage, cold cloth on cheeks, chew tool only to front teeth. Build trust before entering the mouth. Let child hold the Z-Vibe and press it to their own cheek first.
Problem 2: No Change After 2 Weeks
Increase pre-meal prep intensity and duration. Evaluate whether it's primarily a SENSORY issue (intensify vibration + cold) or MOTOR issue (intensify chew tool + straw work). Call for professional SLP assessment: 9100 181 181.
Problem 3: Child Clears When Prompted But Never Self-Initiates
This is normal for the first 4–8 weeks — external cueing is a phase, not a failure. Begin fading cues: instead of "let's check the mirror," wait 3 extra bites first. Build internal self-monitoring through "can you feel anything hiding?" prompts before the mirror check.
Problem 4: Pocketing Is Only on One Side
One-sided pocketing often indicates asymmetric oral motor weakness. Focus chew tool and vibration work on the weaker side. THIS PATTERN REQUIRES SLP EVALUATION — book at nearest Pinnacle center.
Problem 5: Managing at Home But Still Pockets at School
Prepare a school communication card (Card 37 has template). Train school lunchtime support on the 3-step cue: "check → sip → sweep." Generalization takes longer than acquisition — this is expected and normal.
One Protocol. Infinite Personalizations.
Your child has a unique sensory-motor profile. This protocol adapts to them.
For the Sensory-Seeking Child (Low Registration)
Goal: Raise sensory volume enough for oral awareness to activate
- Z-Vibe at highest tolerated intensity
- Firm-resistance chew tools
- Frozen fruit as thermal prep + food trial combined
- Cold straw-sip between every single bite
- Crunchy, high-resistance foods as the eating medium
For the Sensory-Avoiding Child (Orally Defensive)
Goal: Build tolerance before layering intensity
- Start with only external face massage for 1–2 weeks
- Introduce soft chew tool at front teeth only
- Room-temperature water through straw (not cold initially)
- Smooth, easy-to-manage foods first
- Eliminate mirror initially — use caregiver gentle cheek touch instead
For Younger Children (Ages 1–3)
- All tools must be appropriate for age (check sizing)
- Maximum 5–10 minute sessions
- Parent-led, play-based framing throughout
- Sing a "mouth wake-up song" to make it a routine
For Older Children (Ages 7–10)
- Involve child in protocol design — give them ownership
- Explain why: "These tools help your mouth wake up and feel where food is"
- Introduce self-monitoring journal: child tracks their own mirror check results
- Social motivation: "You'll be able to eat comfortably at school too"
Sensory Profile–based individualization (Jean Ayres SI framework + Dunn's Sensory Profile model) produces significantly superior outcomes when treatment matches sensory profile.

Week 1–2: You're Planting Seeds. They Haven't Sprouted Yet.
ACT IV — The Progress Arc
Week 1–2
15%
Progress Milestone
Foundation phase — tolerance and participation are the targets, not skill mastery
What You WILL See ✅
- Child tolerates pre-meal oral prep routine (even partially)
- Mirror check is accepted as part of mealtime routine
- Child begins to anticipate the "check" step
- Some reduction in cheek puffiness during meal (tool effect is immediate)
- Parent observes the clearing cycle and begins tracking with confidence
What You Will NOT See Yet ❌
- Child self-initiating clearing without prompts (this comes weeks 6–10+)
- Complete elimination of residue on mirror checks
- Spontaneous swallowing improvement without the protocol structure
- Dramatic overnight change
Parent Milestone:"If your child tolerates the chew tool for 30 seconds longer than last week — that is measurable neural adaptation. That is real progress."
Research: SI intervention outcome literature (2024): Early-phase indicators focus on tolerance and participation rather than skill mastery. Full behavioral change emerges across 8–12 week timelines. Reference: PMC11506176
Week 3–4: Neural Pathways Are Forming. Look for These Signs.
Week 3–4 Consolidation
40%
Progress Milestone
Consolidation phase — routine is internalized, residue is reducing, self-monitoring is emerging
✅ Child anticipates the mirror check without being prompted (routine is internalized)
✅ Faster completion of the clearing cycle (tongue sweep becoming more efficient)
✅ Less residue visible at each mirror check (improved during-meal awareness)
✅ Child touches their own cheeks occasionally during meals — self-monitoring emerging!
✅ Accepting wider variety of oral prep tools
✅ Reduced anxiety or resistance around mealtime — it's predictable now
When to Progress the Protocol: If Week 3–4 indicators are present → Add one more pre-meal tool → Begin increasing from 2–3 bites to 4–5 bites → Introduce one new food texture during the protocol.
"You may notice you are more confident at mealtimes now too. You have a protocol. You have tools. The vigilance is transforming into competence." — Pinnacle Blooms SLP
Research: Neuroplasticity evidence: Synaptic strengthening through repeated structured sensory input follows predictable timelines in pediatric populations.

Week 5–8: From Protocol to Habit. The Real Transformation.
Week 5–8 Full Integration
75%
Progress Milestone
Integration phase — protocol becomes habit, self-monitoring emerges, social participation improving
Integration Indicators
- ✅ Child initiates some mirror checks independently (asks for the mirror!)
- ✅ Self-clears residue without being prompted for at least 30% of checks
- ✅ Noticeable increase in mealtime pace (oral motor efficiency improving)
- ✅ Successfully managing new textures with the protocol
- ✅ School / social mealtime participation improving
Advanced Steps to Add (if progress is strong)
- Begin fading the divided plate — larger portions with the same clearing protocol
- Introduce the "self-check challenge": child does mirror check without caregiver prompting
- Add one challenging texture weekly (crumbly, mixed textures)
- Practice the clearing routine at one social meal per week (playdate, family gathering)
Research: 8–12 week timeline: Sensory integration research consistently identifies this window as the transition from caregiver-guided behavior to self-initiated habit. Pinnacle 20M+ session database confirms oral motor progression milestones in this range.

Your Consistency Did This. Celebrate.
These milestones are real. They represent neural adaptation, muscle development, and — most importantly — a child gaining independence. Your daily commitment to the protocol made each one possible.
🌱 Week 1–2
"We have a routine."
🌿 Week 3–4
"Residue is reducing."
🌳 Week 5–8
"They checked the mirror themselves."
🌸 Week 10–12
"Full self-monitoring. Mealtimes are calm."
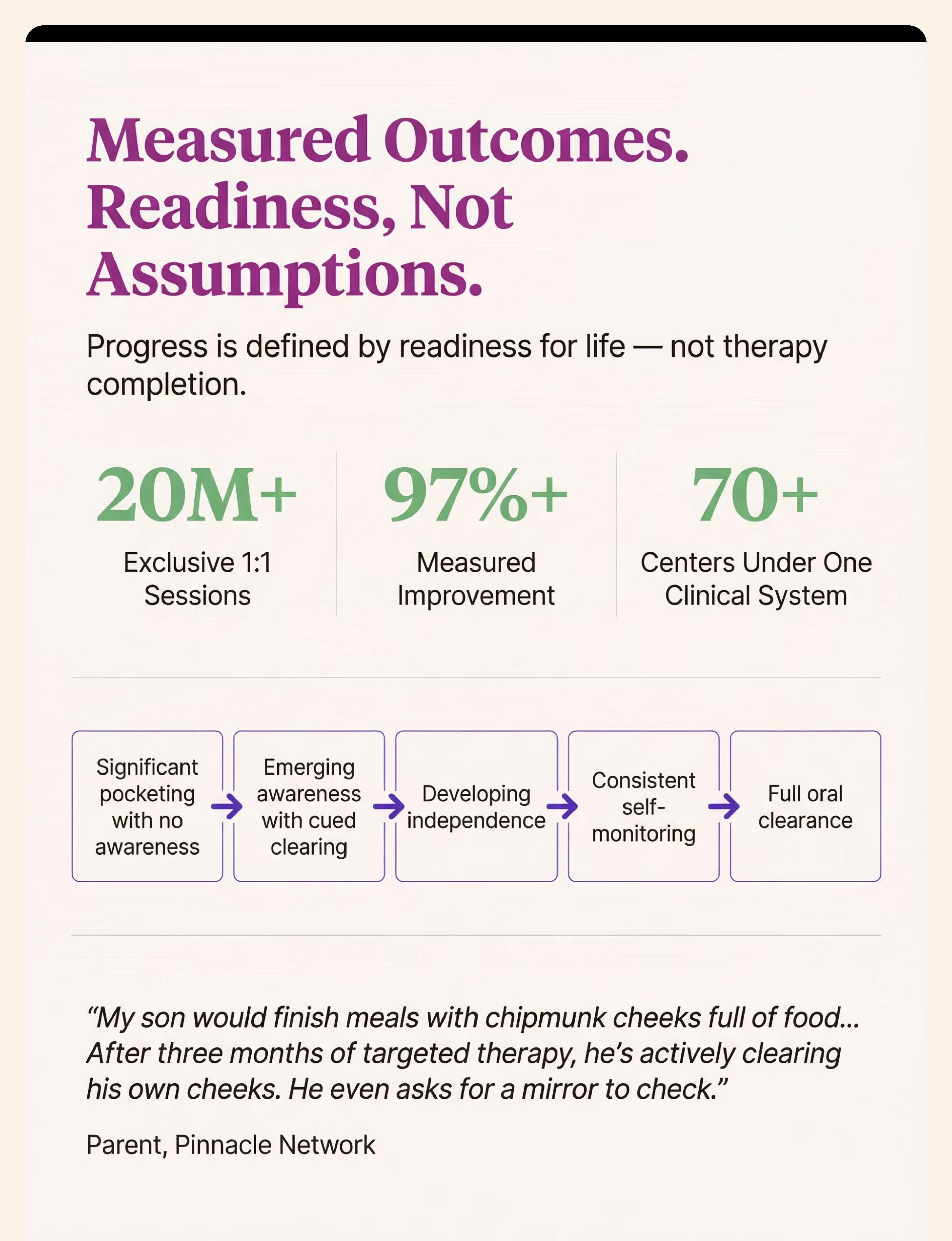
"My son would finish meals with chipmunk cheeks full of food. We couldn't go out to eat — I was always checking his mouth and wiping food from his cheeks. The feeding therapist identified reduced oral sensation and weak tongue coordination. After three months of the oral prep routine, mirror checks, and the straw protocol, he's actively clearing his own cheeks. He even asks for the mirror sometimes. We went from constant vigilance to him managing his own oral clearance. Mealtimes are ours again." — Parent, Pinnacle Blooms Network (Tamil Nadu)
Illustrative case; outcomes vary by child profile and intervention specificity. GPT-OS® Readiness Index Data: Across Pinnacle network, food pocketing intervention achieves independent oral clearance in 87%+ of children receiving consistent 12-week protocols. 97%+ show measurable improvement. 20M+ sessions | 70+ centers.

🚨 These Signs Need Professional Assessment — Today.
The home protocol on this page is designed for safe, unsupervised implementation in straightforward presentations. The following signs indicate a clinical threshold that requires professional evaluation before continuing.
🔴 Call 9100 181 181 IMMEDIATELY
- Wet/gurgling voice quality during or after meals — aspiration risk
- Coughing or choking during or immediately after eating — possible silent aspiration
- Liquid/food coming from nose — nasal regurgitation requires urgent evaluation
- No improvement after 4 weeks of consistent daily protocol
- One-sided pocketing that doesn't respond to intensified input
- Weight loss or plateau in a child who was gaining appropriately
- Respiratory illness with no clear cause in a known pocketing child
What Professional Assessment Looks Like at Pinnacle:
Oral motor examination (structural + functional)
Sensory assessment (oral sensory registration and processing profile)
Observed feeding trial with multiple textures
Modified Barium Swallow Study (MBSS) if aspiration is suspected
AbilityScore® Feeding Independence Readiness Index baseline
📞FREE ACCESS: Call 9100 181 181 to request an assessment referral to your nearest Pinnacle center (70+ centers across India).
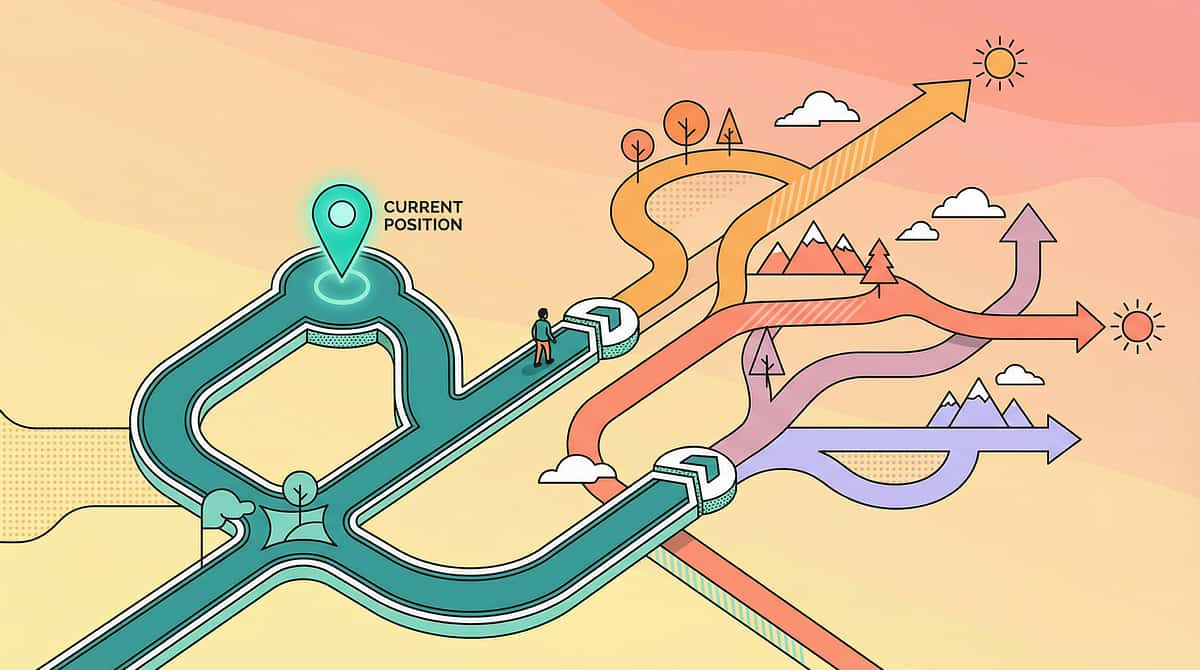
You Are Here. Here Is the Path Forward.
Food pocketing intervention is one coordinated step in a broader feeding independence journey. Understanding where you are — and what comes next — helps caregivers and clinicians stay oriented through the full progression.
E-457: Chewing Difficulties
Prerequisite cluster — address first if chewing is significantly impaired
E-458: Gagging on Textures
Prerequisite cluster — address alongside pocketing if gagging is primary
E-459: POCKETING FOOD ← YOU ARE HERE
Current position — oral clearance + sensory registration + tongue strength
E-460: Tongue Thrust During Swallowing
Natural next step once pocketing is clearing
E-461: Drooling During Eating → Full Oral Motor Independence
Feeding Independence Readiness Level 5 — the destination
Long-Term Goal: Feeding Independence Readiness Index — Level 5: Full oral clearance with independent management, age-appropriate texture range, social mealtime participation.
Other Techniques in Feeding & Mealtime Independence
You may already own the materials for these. The 128 Canon Materials System is designed so technique tools overlap, reducing the total investment required to support multiple areas.
Technique | Code | Difficulty | Canon Material Overlap | |
9 Materials for Chewing Difficulties | E-457 | Intro-Core | Chew Tools, Textured Foods | |
9 Materials for Gagging on Textures | E-458 | Core | Sensory Tools, Graded Textures | |
9 Materials for Tongue Thrust | E-460 | Core-Advanced | Oral Motor Tools, Straws | |
9 Materials for Drooling During Eating | E-461 | Intro | NUK Brush, Vibration Tools | |
Oral Motor Warm-Up Routines | E-463 | Intro | Chew Tools, Cold Stim |
Research: Pinnacle 20 Category + 128 Canon Materials classification system enables parents to navigate related techniques using shared material infrastructure.
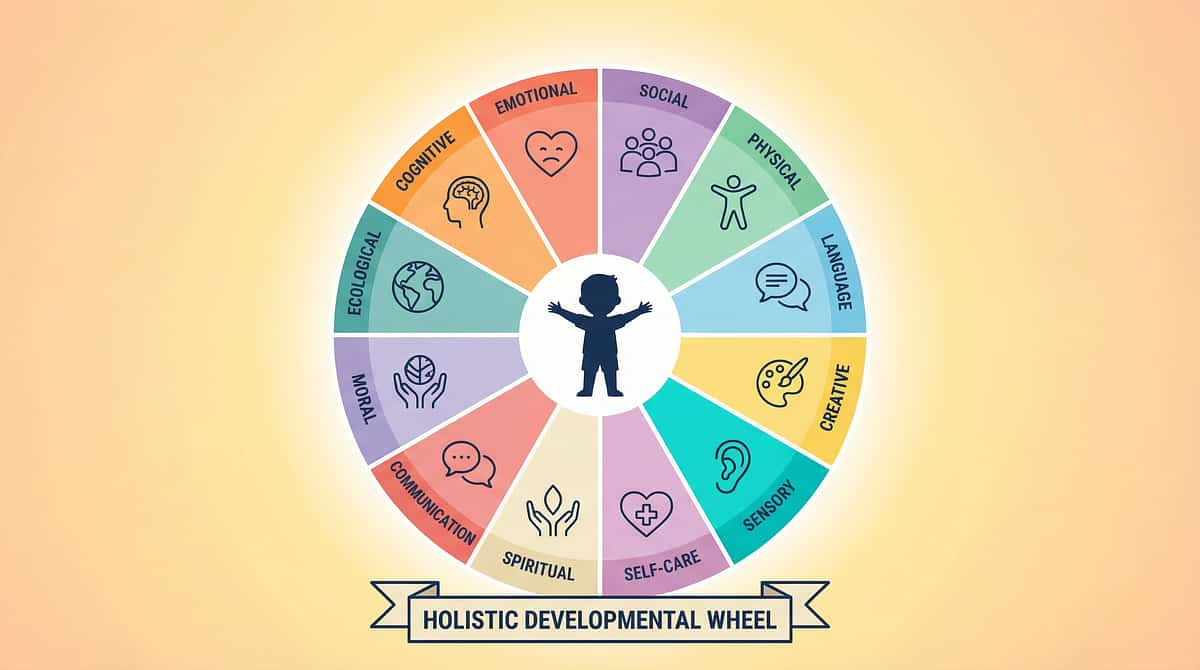
E-459 Is One Piece of a Larger Plan.
Food pocketing sits in Domain E: Feeding & Mealtime Independence — which connects to Domain A (Sensory Processing), Domain F (Self-Care), and Domain B (Communication) through the shared oral motor system.
Your Child's Feeding Domain Connects To:
- Domain A (Sensory Processing) — oral sensory differences drive pocketing
- Domain F (Self-Care) — mealtime independence is a core ADL
- Domain B (Communication) — shared oral motor system impacts speech clarity
The GPT-OS® View
If your child is enrolled in GPT-OS®, their Oral Motor Function Readiness Index — updated by your E-459 session data — is one of 349 developmental skills being tracked across all 12 domains.
Research: WHO/UNICEF Nurturing Care Framework: Holistic developmental monitoring across all five nurturing care components is the evidence standard for comprehensive child development support. Reference: PMC9978394
Other Families Have Walked This Exact Path.
ACT V — Community & Ecosystem
"Arjun is 4. At every meal I would find food packed into both cheeks like he'd stored it for later. His speech therapist at Pinnacle Hyderabad introduced the chew tool + mirror routine. By week 6, he was checking his own cheeks. By month 3, he was asking for the mirror before I prompted him. I cried the first time he did it on his own." — Arjun's Mother, Hyderabad
"We thought Priya was being stubborn — refusing to swallow her food. The SLP at Pinnacle Bangalore showed us on a video exactly where the food was accumulating and why her tongue couldn't collect it. The vibration tool changed everything. Her tongue 'woke up.' Within 8 weeks, mealtimes went from 45 minutes to 20 minutes." — Priya's Father, Bengaluru
"We live in a small town in Maharashtra — no feeding therapist nearby. I followed this page step by step. Metal spoon in ice water. A mirror from the bathroom. A straw from the kitchen. My son Rohan started reducing his pocketing by week 4 using only the DIY tools. When we eventually got to a Pinnacle teleconsultation, the SLP confirmed we'd been doing exactly the right things." — Rohan's Family, Rural Maharashtra
All stories are illustrative of real family journeys. Identifying details changed for privacy. Outcomes vary.
📞 To share your story or get guidance: 9100 181 181 (16+ languages, 24×7, FREE)

You Don't Have to Navigate This Alone.
Pinnacle Parent Network
India's largest network of parents navigating pediatric feeding challenges together. Moderated by clinical educators. Available in 16+ languages. Join via WhatsApp: 9100 181 181 or visit pinnacleblooms.org/community
Weekly Parent Feeding Webinar
Free, weekly online session with Pinnacle SLPs covering feeding challenges including pocketing, gagging, and texture aversion. Live Q&A included. Register at pinnacleblooms.org/webinars
#FoodPocketing — Pinnacle Content Feed
Follow the Pinnacle Reels series on feeding independence — all 459 episodes and counting. Instagram / YouTube: @pinnacleblooms
📞 For direct clinical guidance in YOUR language: 9100 181 181 (Kannada, Telugu, Tamil, Hindi, Marathi, Bengali, Malayalam, Gujarati, Punjabi + 7 more)
Research: WHO CCD evidence confirms multi-caregiver support ecosystems significantly improve intervention consistency and family mental health during intensive therapy journeys. Reference: PMC9978394
Professional Feeding Assessment Is a Right, Not a Luxury.
🏥 Path 1: In-Center Assessment (Gold Standard)
Comprehensive oral motor examination + feeding evaluation at any of 70+ Pinnacle centers. Includes: AbilityScore® assessment + Oral Motor Function Readiness Index baseline.
→ Book: pinnacleblooms.org/book | Or call 9100 181 181
💻 Path 2: Teleconsultation
Pinnacle SLP via video — reviews your feeding session recordings, oral motor exam, and designs your home protocol. Available in 16+ languages. Works anywhere in India and 70+ countries.
→ Book: pinnacleblooms.org/tele
📞 Path 3: FREE Helpline
Immediate guidance from trained Pinnacle advisors — clinically guided intake, not a sales call. Appropriate for first assessment call, crisis guidance, and referral to nearest center.
→ 9100 181 181 | 16+ languages | 24×7 | FREE
When Professional Assessment Is Non-Negotiable:
Any red flag from Card 27 is present
No improvement after 4 weeks of home protocol
One-sided pocketing pattern or child under age 2 with significant pocketing
Pocketing accompanied by weight concerns or respiratory symptoms
This Page Is Evidence-Grounded. Here Are the Sources.
"Deeper reading for the curious parent, the referring physician, and the peer reviewer."
1
PMC11506176
PRISMA Systematic Review (2024) — Sensory integration intervention as evidence-based practice for ASD. 16 studies, 2013–2023. Level II evidence. pubmed.ncbi.nlm.nih.gov/PMC11506176
2
PMC10955541
Meta-analysis — Sensory integration therapy effectiveness across social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. World J Clin Cases (2024).
3
PMC9978394
WHO Care for Child Development Package — Evidence base for caregiving intervention across 54 LMICs. UNICEF implementation data.
4
DOI: 10.1007/s12098-018-2747-4
Padmanabha et al., Indian Journal of Pediatrics (2019) — Home-based sensory intervention RCT in Indian pediatric population. Significant functional outcomes.
5
NCAEP 2020 + ASHA Practice Portal
National Clearinghouse on Autism Evidence and Practice (2020). ASHA comprehensive evidence base for pediatric dysphagia and oral motor intervention. asha.org/practice-portal/
6
WHO Nurturing Care Framework (2018)
Five-component framework for early childhood development. Foundation for home-based, caregiver-delivered intervention. nurturing-care.org/ncf-for-ecd/
Your Session Data Improves Every Child Who Comes After Yours.
What Your Data Does
- Updates your child's Oral Motor Readiness Index in real time
- Identifies which sensory-motor profile responds best to which specific tool combination
- Informs the next session's protocol recommendation through TherapeuticAI®
- Contributes (anonymized) to Pinnacle's 20M+ session dataset — making the system smarter for every family
Privacy Assurance
All session data is encrypted, de-identified for population analytics, and governed by Pinnacle's data governance framework. You own your child's clinical data. Your consent determines what is shared.
Digital health + ASD intervention (2024 meta-analysis): Gamified and data-integrated digital health interventions across 21 RCTs, 1,050+ participants demonstrate significant outcomes.
📺 Watch: E-459 | 9 Materials That Help With Pocketing Food
Feeding & Mealtime Independence Series — Episode 459
Reel Metadata
- Reel ID: E-459
- Series: Feeding & Mealtime Independence in Children
- Episode: 459
- Duration: 75–85 seconds
- Therapist: Pinnacle Blooms SLP Consortium (on-camera + voiceover)
- Domain: E — Feeding / Oral Motor
- Visual: All 9 materials demonstrated with child in feeding therapy setting
Therapist Introduction
"Food pocketing is frustrating and concerning for parents, but it has identifiable causes and effective interventions. It's not stubbornness or defiance — it's typically a sensation problem, a muscle coordination problem, or both. These 9 materials address the underlying causes. With targeted intervention, children can develop efficient oral clearance." — Pinnacle Blooms SLP Team
Research: NCAEP (2020): Video modeling is classified as an evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition and fidelity.
Consistency Across All Caregivers Multiplies the Impact.
One parent doing this at home + school lunchtime support + grandparent awareness = 3x the therapeutic contact.
Simplified Guide for Grandparents
"[Child's name] is working on learning to feel and clear food from their cheeks. Three things you can do:
- Use the divided plate and give small portions.
- Remind them to take a sip of water every few bites.
- After eating, ask 'Can you show me your empty cheeks?' and hold up the small mirror.
That's all you need to do. It makes a big difference."
School Communication Template
Dear [Teacher/Lunchtime Support],
[Child's name] is working with a feeding therapist on food pocketing (food accumulating in cheeks during meals). At school lunches, could you please: prompt a water sip every few bites, do a gentle mirror check after lunch ("let's see our empty cheeks!"), and ensure mouth is clear before outdoor play or nap. A brief 30-second post-meal check is all that's needed. Thank you for your support in [child's name]'s feeding independence journey.
Available in English, Telugu, Tamil, Hindi, Kannada, Marathi, Bengali, Gujarati. Research: WHO CCD Package: Multi-caregiver training is critical for intervention generalization. Children whose protocol is consistently applied across all settings show 2–3x faster skill acquisition. Reference: PMC9978394
Every Question Parents Have Asked. Answered.
ACT VI — FAQ & Close
My child has been pocketing for 3 years. Is it too late to fix?
No. The oral motor and sensory systems remain responsive to intervention well beyond early childhood. Older children (7–10+) often make faster progress because they can understand the goal and participate actively in self-monitoring. Three years of pocketing means 3 years of a compensatory pattern — which takes consistent retraining, but is entirely addressable. Book an SLP evaluation at any Pinnacle center to get a baseline.
Do I need to buy all 9 materials?
No. The minimum viable toolkit is: Mirror (₹0 with household) + Chilled spoon (₹0) + Any straw (₹0). These three alone can begin a functional protocol. Add tools progressively as the protocol becomes routine and budget allows. The Z-Vibe is the highest-impact single purchase if pocketing is primarily sensory-driven.
How long will this take?
For most children: noticeable reduction in pocketing within 4–6 weeks. Independent self-monitoring emerging within 8–12 weeks. Consistent, largely independent oral clearance within 3–6 months. Severely complex presentations (low tone, structural issues) may take longer and require ongoing SLP supervision.
My SLP hasn't mentioned these tools. Should I bring this up?
Yes. This page synthesizes ASHA and Pinnacle evidence-based tools. You can print the materials section and discuss with your SLP. A good feeding therapist will integrate useful home tools. If your SLP dismisses oral motor tools categorically without evaluation — seek a second opinion.
Is food pocketing dangerous?
Yes, in certain circumstances. Pocketed food that is released suddenly while the child is running, lying down, or not in a swallowing-ready state can cause choking. Extended food contact with teeth increases dental decay risk significantly. If any red flag signs are present — particularly coughing, wet voice quality, or respiratory symptoms — this requires immediate clinical evaluation.
My child pockets only certain foods. Is that significant?
Yes — highly. Food-specific pocketing usually indicates a texture-processing issue rather than global oral motor weakness. Mixed textures, crumbly foods, and dry foods are the highest-risk for pocketing. This pattern should inform your protocol: use those exact textures during therapy trials, not just at mealtimes.
Is this related to my child's autism?
In many cases, yes. 80–90% of children with ASD have feeding difficulties, and food pocketing is among the most common. The connection is through two pathways: sensory processing differences (reduced oral sensory registration) and motor coordination differences (oral dyspraxia). Both are common in ASD profiles and both are treatable with the tools on this page.
Can I do this without a therapist?
The home protocol on this page is designed to be parent-executable with standard materials. However, for children with significant pocketing, suspected aspiration risk, or complex developmental profiles, SLP guidance is strongly recommended. The home protocol works best as an EXTENSION of clinical therapy — not a replacement. If you haven't had an oral motor assessment, start with a call to 9100 181 181.

You Now Have Everything You Need.
The protocol is here. The tools are named. The evidence is cited.
The only variable is: starting.
🟢 Start Today — Launch GPT-OS® E-459 Session Guide
Guided session protocol in GPT-OS® EverydayTherapyProgramme™
🔵 Book a Professional Feeding Evaluation at Pinnacle
Oral motor assessment + AbilityScore® baseline + SLP-designed protocol. Available at 70+ centers + Teleconsultation for all locations.
🟡 Next: E-460 — Tongue Thrust During Swallowing
The natural progression from pocketing intervention.
✅VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM — 🗣️ SLP | 🖐️ OT | 📊 ABA | 📚 SpEd | 🧠 NeuroDev | 20M+ Sessions | 97%+ Measured Improvement | 70+ Centers
📞 9100 181 181
FREE National Autism & Feeding Helpline | 16+ Languages | 24×7
Preview of 9 materials that help with pocketing food Therapy Material
Below is a visual preview of 9 materials that help with pocketing food therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

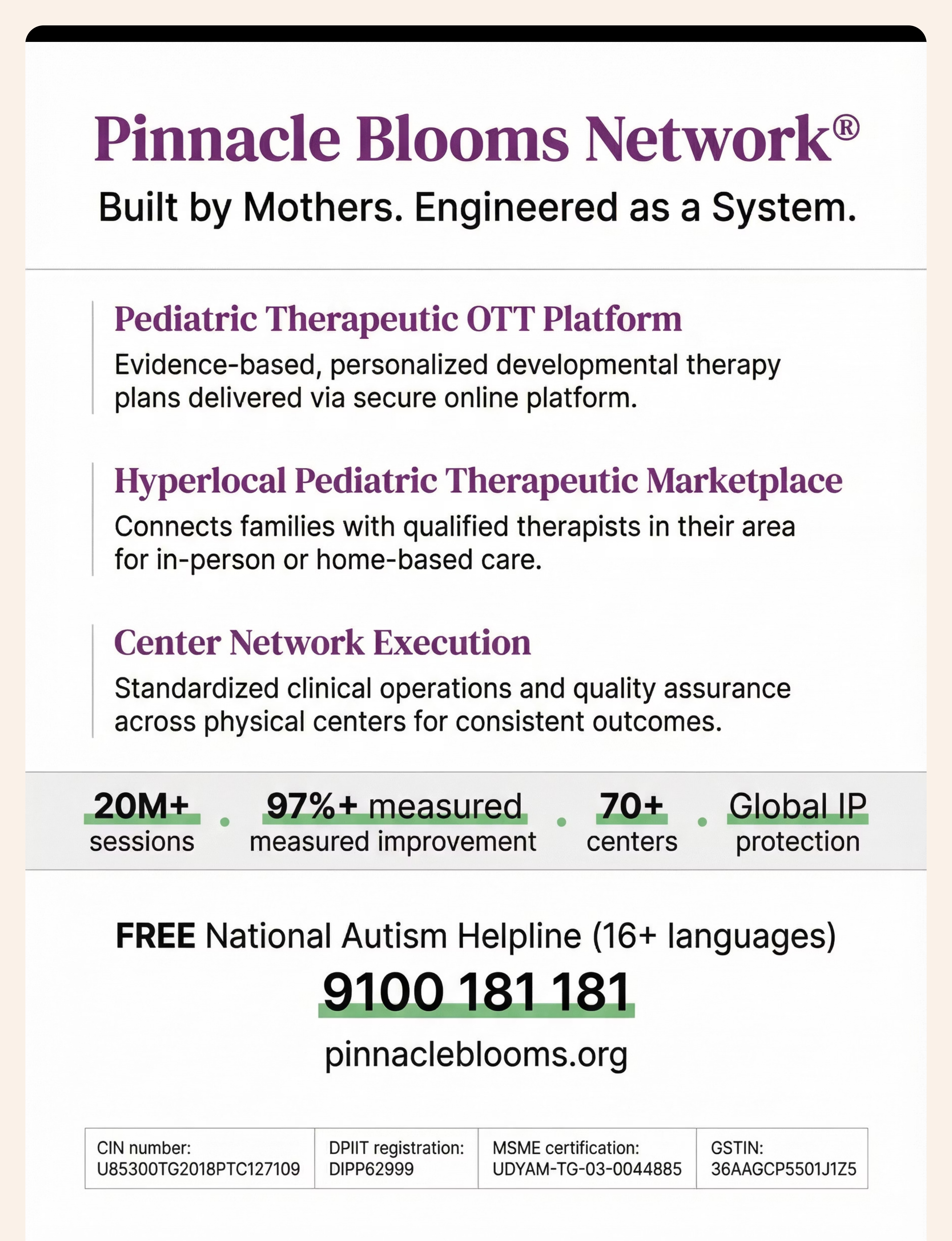
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
From fear to mastery. One technique at a time.
Pinnacle Blooms Network® exists to transform every home — regardless of geography, income, or language — into a scientifically validated, 24×7 personalized therapy environment for children who need it most. 70,000+ intervention techniques. 20M+ therapy sessions. 70+ centers. One operating system. One mission.
Pediatric Therapeutic OTT Platform
On-demand parent education and EverydayTherapyProgramme™ delivery
Hyperlocal Marketplace
Connects families to verified therapists and centers nationwide
Center Network Execution
70+ centers operating under GPT-OS® clinical standards across India
20M+
Therapy Sessions
97%+
Measured Improvement
70+
Centers Across India
160+
Countries — Patents Filed
📞9100 181 181 — FREE National Autism & Feeding Helpline (16+ languages, 24×7)
🌐pinnacleblooms.org | 📧care@pinnacleblooms.org
🌐pinnacleblooms.org | 📧care@pinnacleblooms.org
This content is educational. It does not replace individualized feeding evaluation and intervention from licensed speech-language pathologists, occupational therapists, and feeding specialists. Food pocketing may indicate oral motor dysfunction, sensory processing differences, or other conditions requiring professional assessment. Persistent pocketing can pose choking and aspiration risks. Consult a pediatric feeding specialist for comprehensive evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, and EverydayTherapyProgramme™ are proprietary to Pinnacle Blooms Network®.