"If the juice from the fruit touches the bread, the bread is 'contaminated.' If the vegetables touch the chicken, the whole plate is rejected. I've tried reasoning with them. I've tried explaining that it all goes to the same stomach anyway. But logic doesn't help. This isn't about being difficult — when foods touch, the reaction is visceral. Genuine distress, sometimes gagging, sometimes shutdown. I'm exhausted." — Parent, navigating sensory-based feeding

"You are among the estimated 8–10 million families in India alone managing sensory-based feeding differences."
Not Picky. Not Defiant. Neurological.
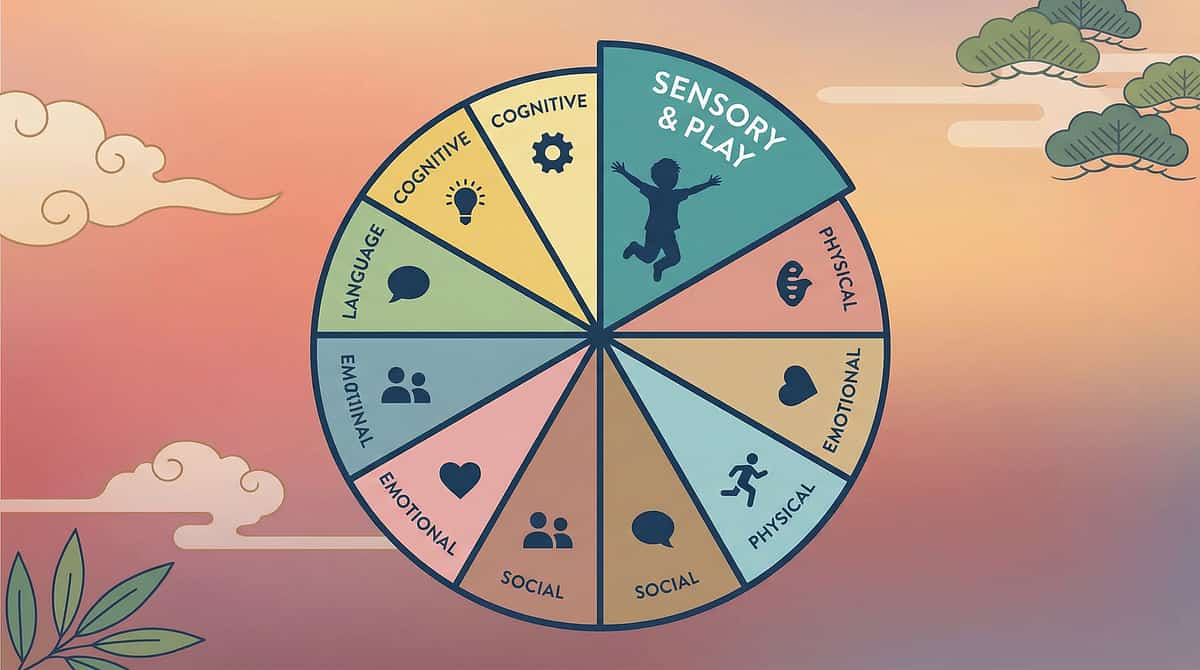
The Science What's Happening in the Brain Somatosensory Cortex Processes texture and temperature signals from every bite Amygdala Threat detection and anxiety response — flags mixed foods as dangerous Insula Interoception and disgust responses — registers aversion viscerally Prefrontal Cortex Prediction/expectation mismatch — mixed foods = unpredictable = unsafe Plain English: What This Means for Your Child Sensory Unpredictability When foods touch, the brain can't predict each bite's texture, taste, or smell — and flags the unpredictable bite as potentially dangerous. Tactile Defensiveness A wet food touching a dry food "contaminates" it with an aversive texture — a genuine threat signal. Visual Processing The visual disorganization of mixed foods creates anxiety before eating even begins. Rigidity as Control In an overwhelming sensory world, food separation rules provide one area of predictability. "This is a wiring difference, not a behavior choice." The distress your child experiences when foods touch is as real as the distress you'd feel touching something that genuinely repulses you. You cannot logic your way out of sensory responses — neither can they. 📚 Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660
- Autism Spectrum Disorder (ASD)
- Sensory Processing Disorder (SPD)
- ARFID (Avoidant/Restrictive Food Intake Disorder)
- Anxiety Disorders
- OCD spectrum features
- ADHD

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade LEVEL I–II EVIDENCE — Systematic Review + RCT Level. Multiple systematic reviews confirm sensory-based accommodations reduce mealtime distress and support feeding outcomes in sensory-sensitive children. Study Finding Source PRISMA Systematic Review (2024) Sensory integration is evidence-based practice for ASD; 16 articles, 2013–2023 PMC11506176 Meta-analysis, 24 studies (2024) SI therapy promotes adaptive behavior, social skills, sensory processing, motor skills PMC10955541 Indian RCT, Padmanabha et al. (2019) Home-based sensory interventions show significant outcomes; parent-administered DOI: 10.1007/s12098-018-2747-4 NCAEP (2020) Visual supports + structured environmental accommodations: evidence-based practices NCAEP EBP Report WHO NCF (2018) Responsive caregiving + sensory-appropriate accommodations: global evidence base nurturing-care.org These are not trends or tips. They are clinically validated, research-backed materials recommended by occupational therapists, feeding specialists, and pediatric developmental teams across 70+ countries. 📞 9100 181 181

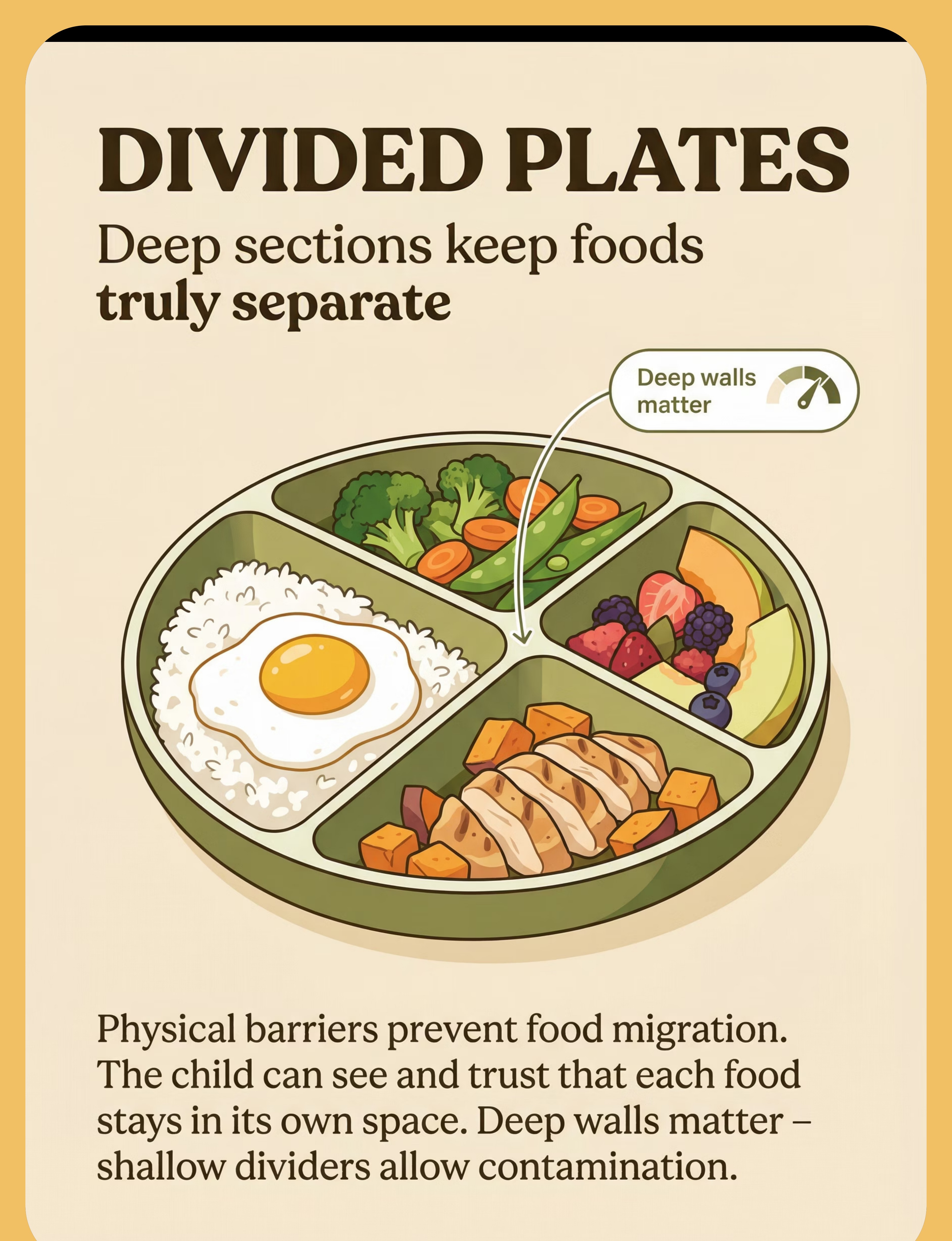
- 🍽️ Divided Plates (Deep Sections)
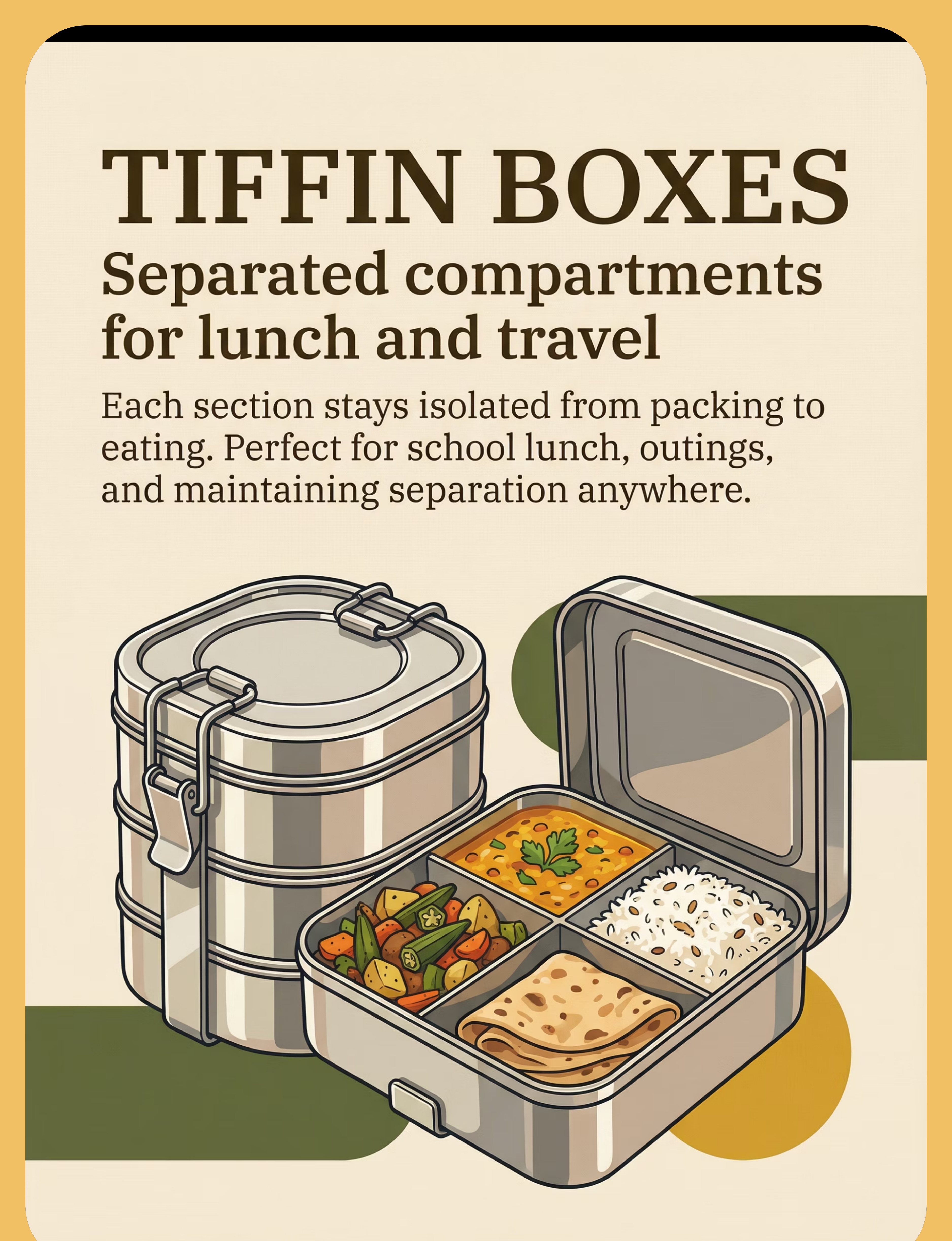
- 🥡 Stainless Steel Tiffin Boxes
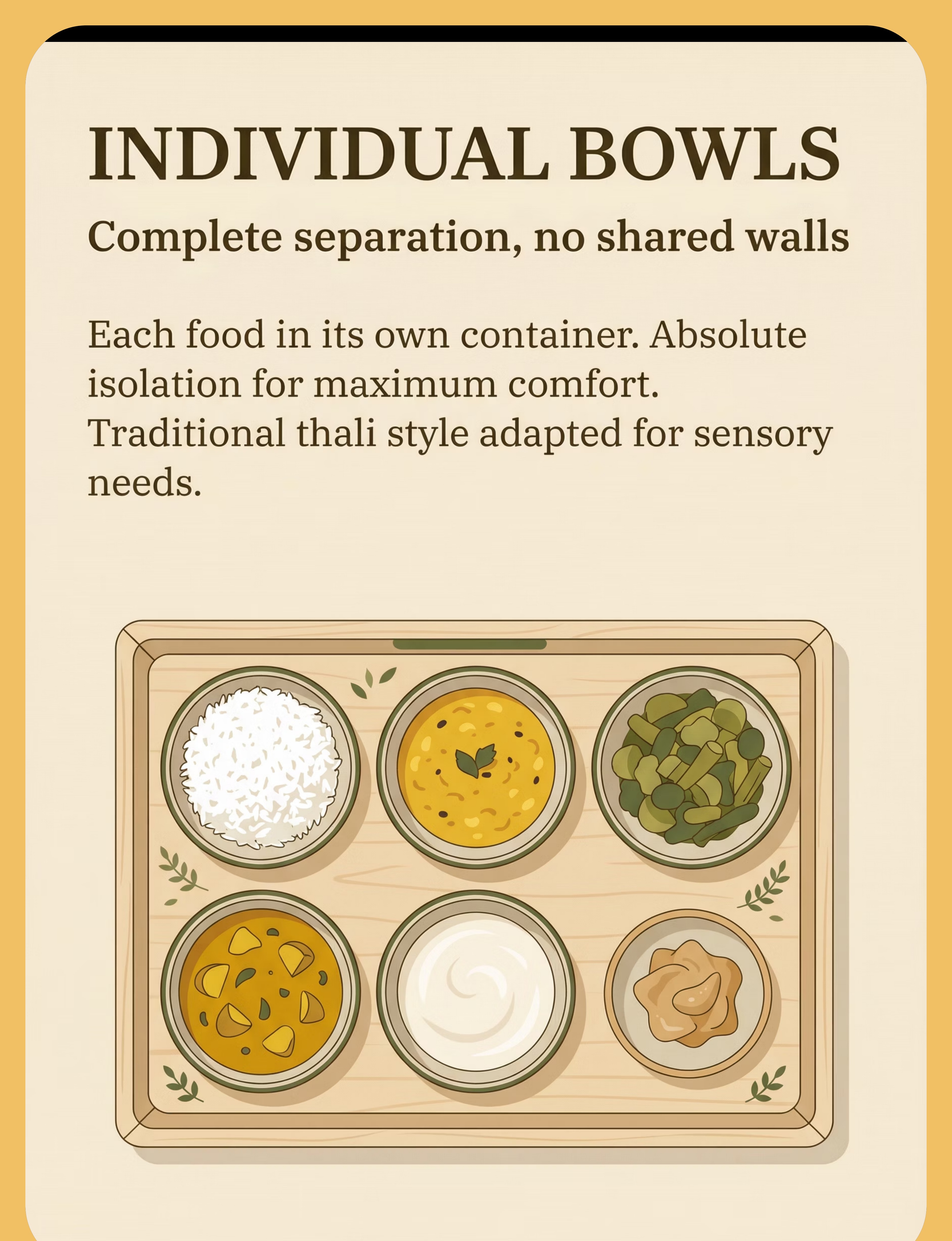
- 🥣 Individual Bowls / Katoris
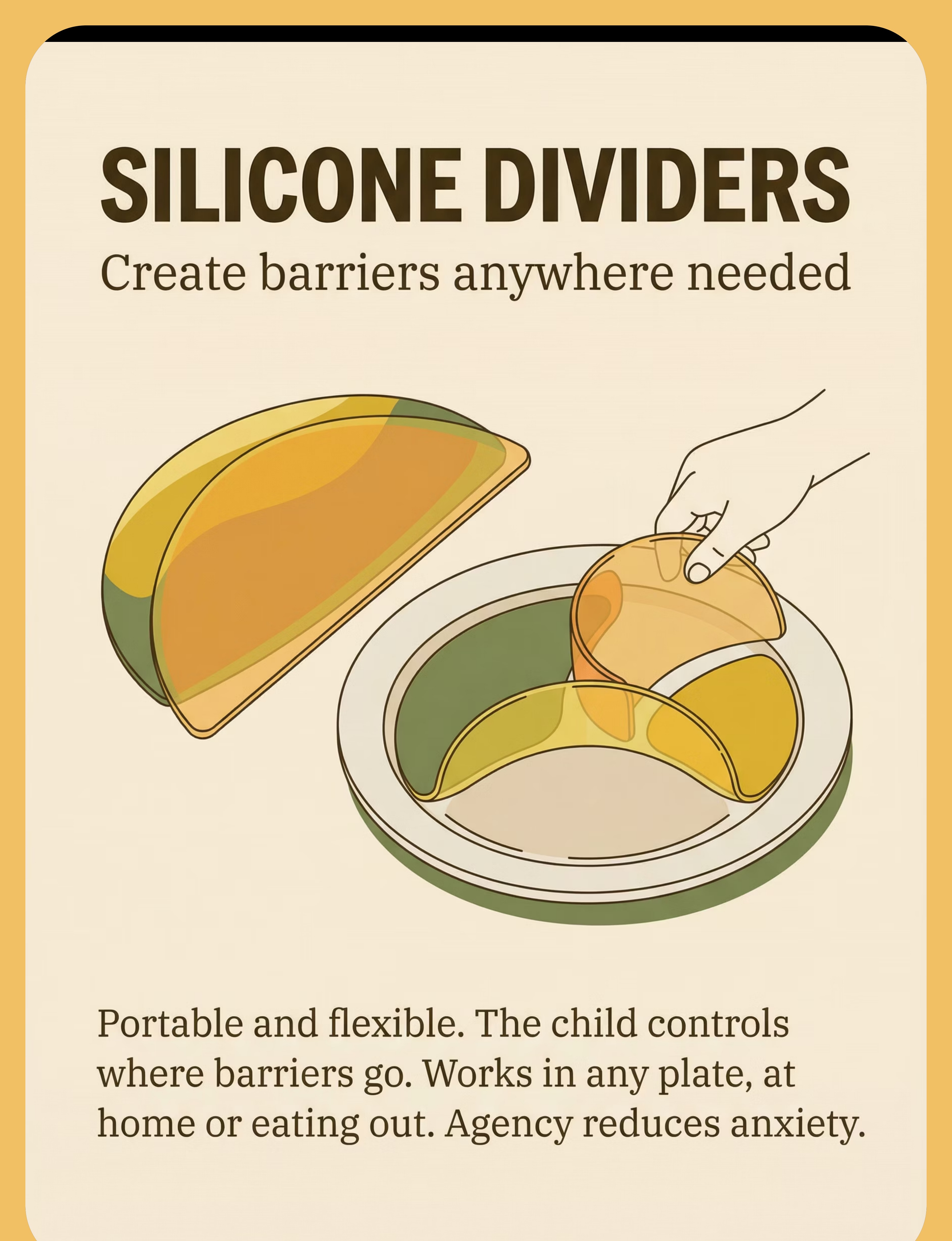
- 🟡 Silicone Food Dividers
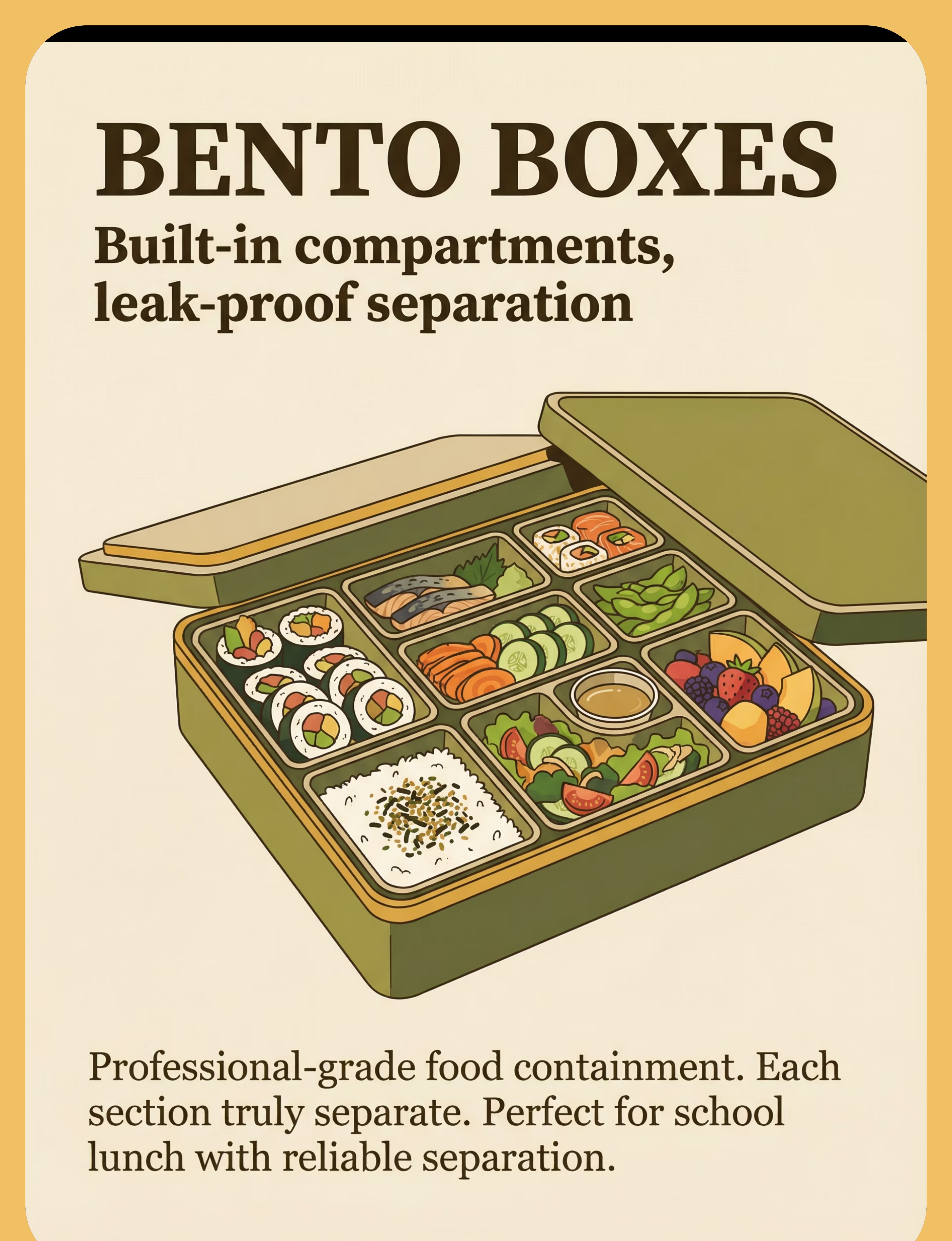
- 📦 Bento Box Containers
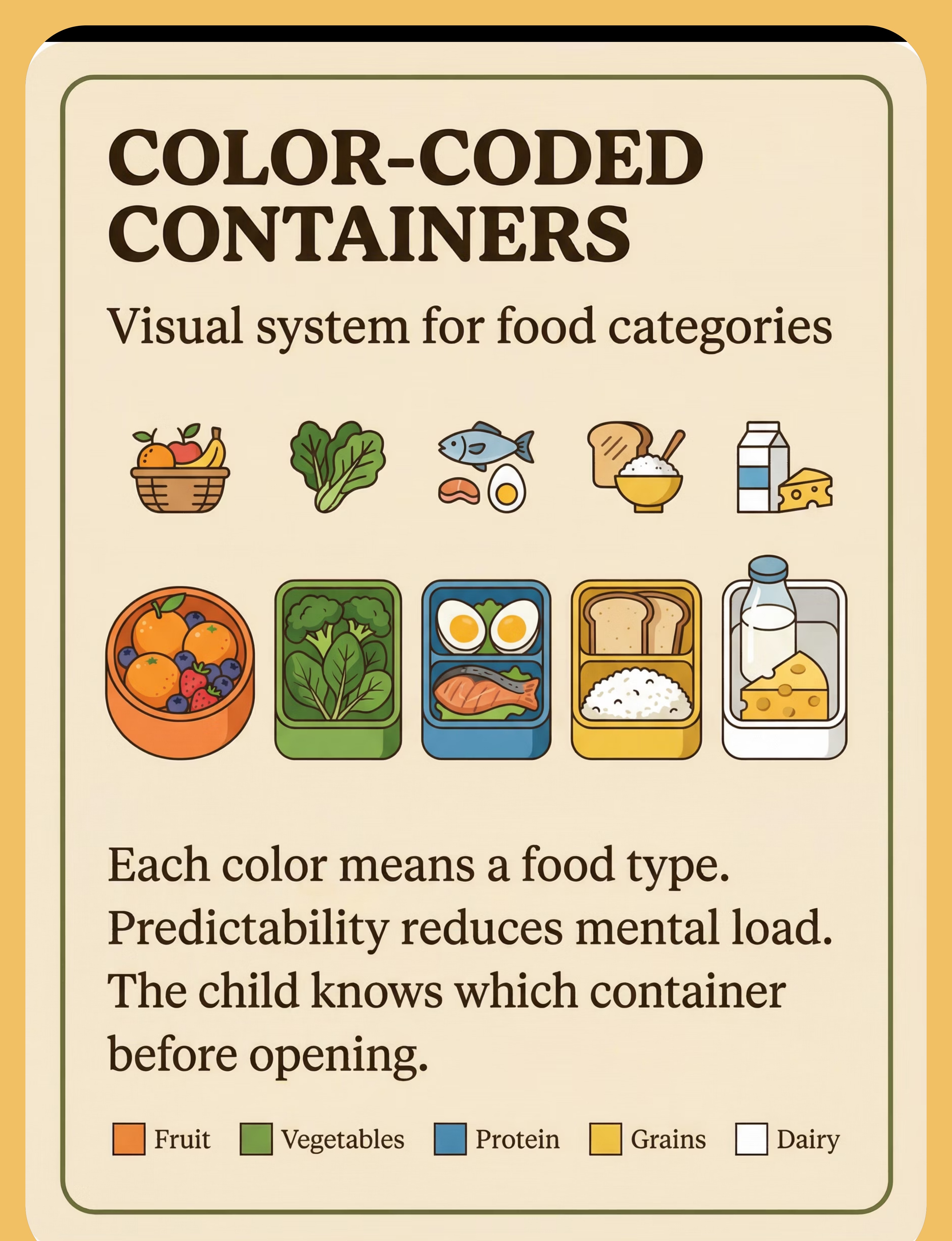
- 🎨 Color-Coded Containers
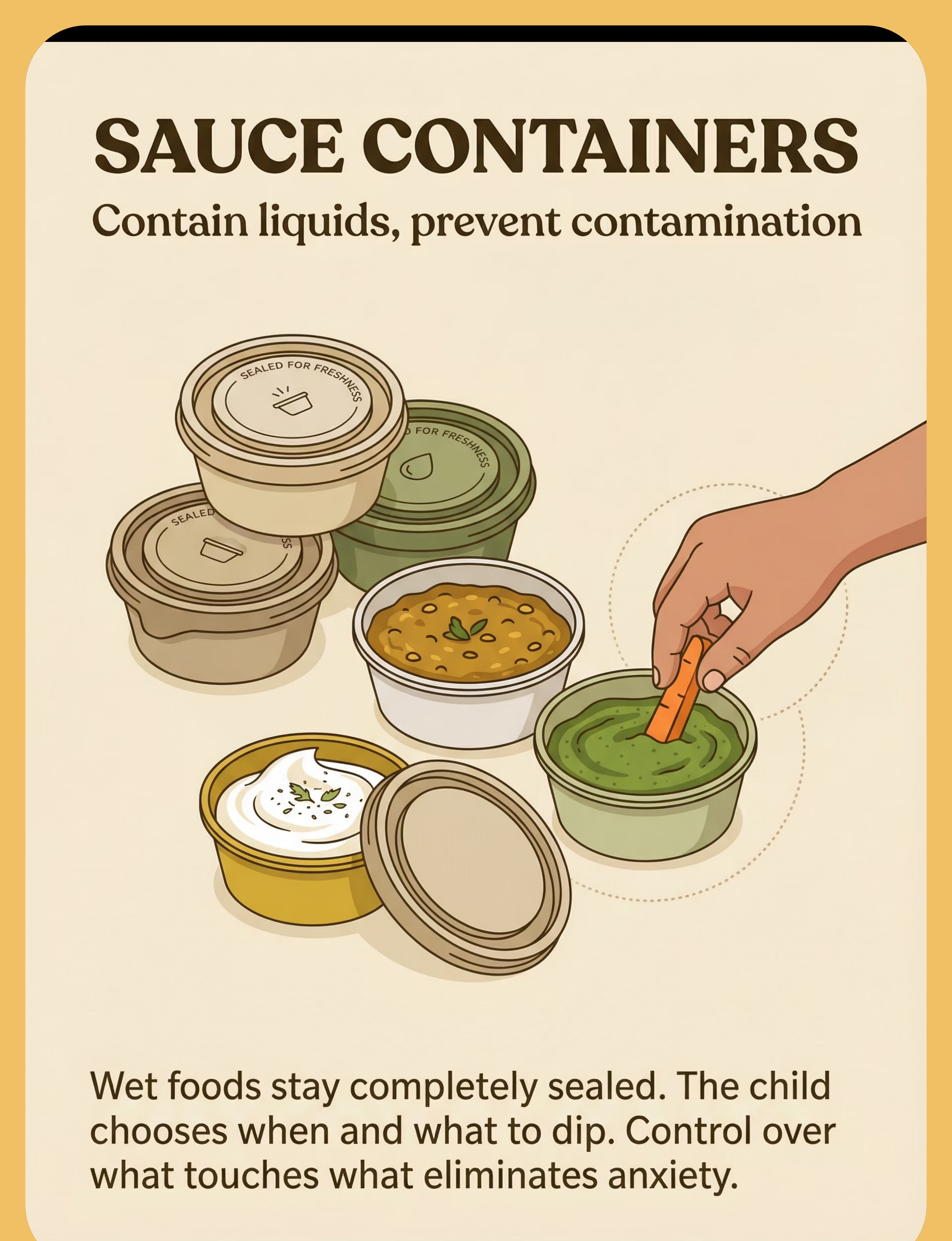
- 🥫 Sauce/Dip Containers with Lids
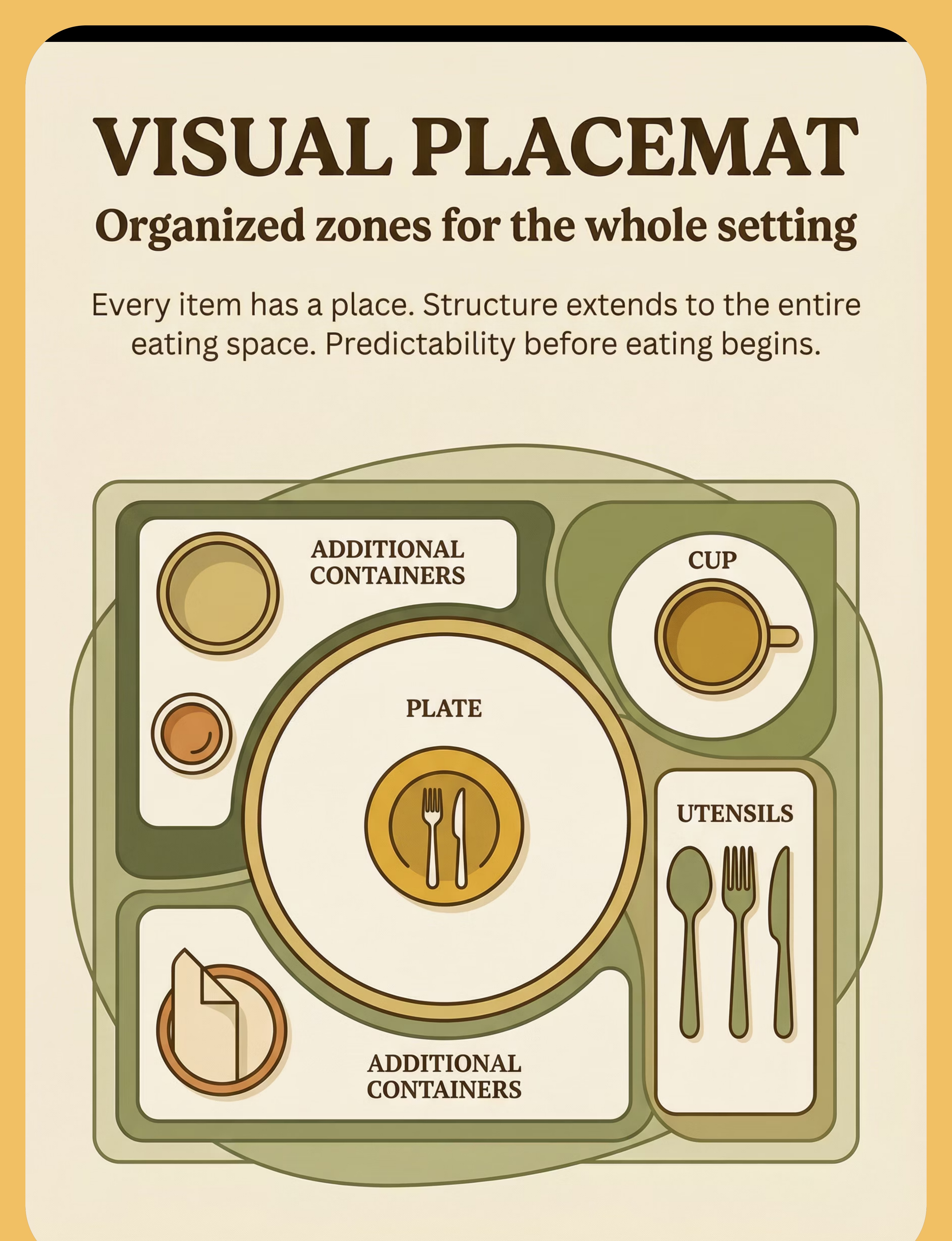
- 🗺️ Visual Placemat with Zones
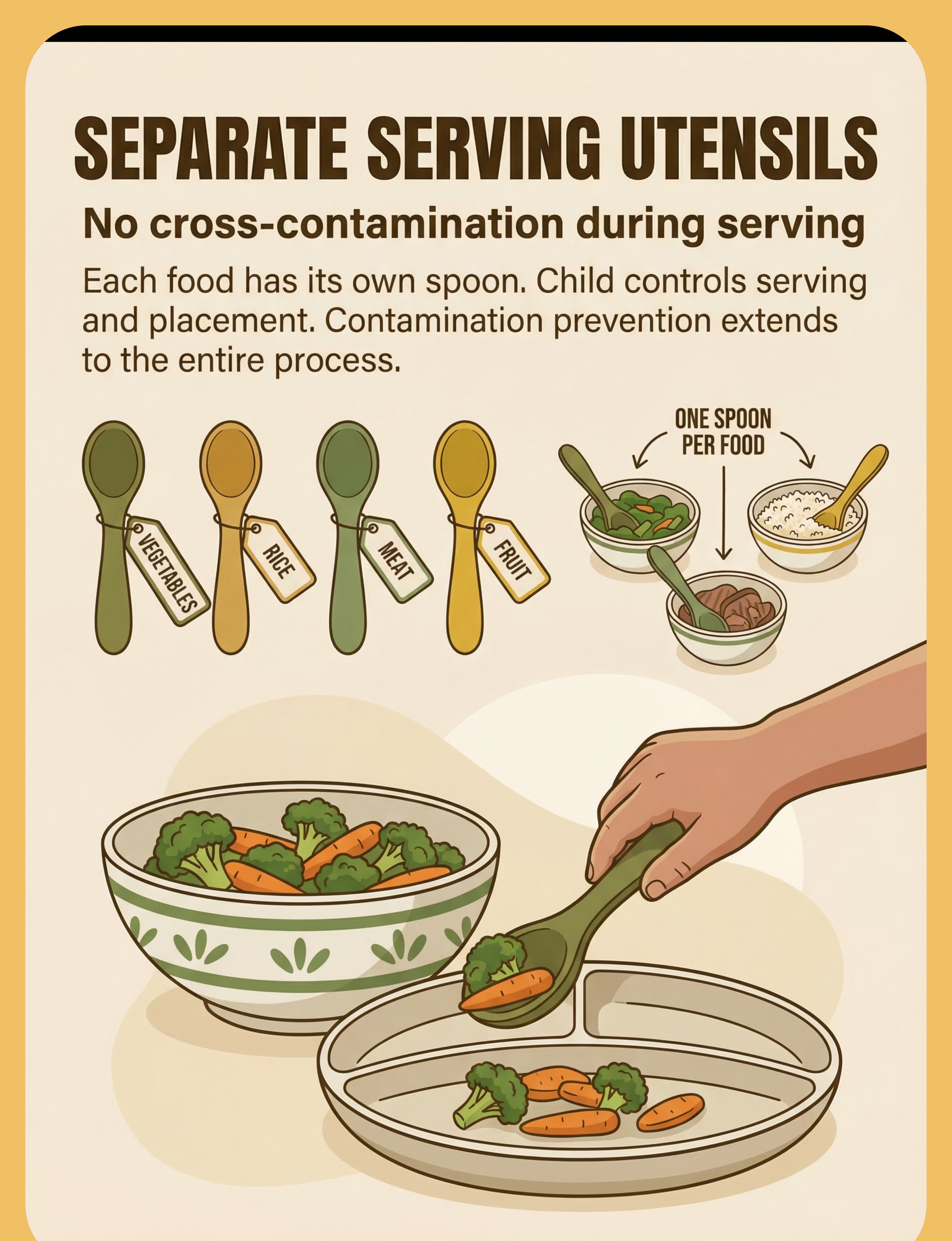
- 🥄 Child-Size Serving Utensils

- NeuroDevelopmental Pediatrician — Rules out medical causes, monitors growth, oversees integrated plan
- Pediatric Dietitian — Ensures nutritional adequacy within accepted foods
- Parent/Caregiver — The most critical member. Daily execution partner.
- ✅ Child completes meals without distress
- ✅ Child accepts foods in separated format previously rejected
- ✅ Mealtime duration under 30 minutes
- ✅ Child engages in table conversation during meals
- ✅ Child self-serves without parental intervention

9 Materials That Work With Their Brain, Not Against It
The 9 Materials 1. Divided Plates — Deep Sections 🍽️ ₹300–1,000 — Physical barriers the child can see and trust. Foods stay in their own territory, always. Pinnacle Recommends: Stainless steel or silicone, minimum 1.5cm wall height, 3–5 compartments. 2. Stainless Steel Tiffin Boxes 🥡 ₹200–800 — The school lunch solution. Compartmentalized, leak-proof, travels from home to lunchroom with separation intact. Pinnacle Recommends: Traditional Indian tiffin with 3–5 compartments; test seal before school use. 3. Individual Bowls / Katoris 🥣 ₹150–500 (set) — Maximum separation: each food in its own vessel, no shared walls, no contamination risk. Pinnacle Recommends: Matching stainless steel katoris on a tray — thali-style eating, adapted for sensory needs. 4. Silicone Food Dividers 🟡 ₹200–600 (set) — Portable barriers that fit any plate. The child places them — agency reduces anxiety. Pinnacle Recommends: Food-grade BPA-free silicone, tall enough to prevent migration, carry in child's bag. 5. Bento Box Containers 📦 ₹400–1,500 — Japanese-origin compartmentalized boxes — leak-proof, organized, school-appropriate, trusted separation. Pinnacle Recommends: Prioritize truly separate compartments. Test leak-proof before school. 6. Color-Coded Containers 🎨 ₹300–800 (set) — Orange = fruit, green = vegetables, blue = protein. Visual predictability reduces cognitive load. Pinnacle Recommends: Establish system with child's input. Consistent daily use builds reliable structure. 7. Sauce/Dip Containers with Lids 🥫 ₹100–400 (set) — Wet items are the biggest contamination risk. Sealed containers eliminate the threat — child dips by choice. Pinnacle Recommends: Silicone containers with secure lids for dal, raita, chutney, yogurt, sauce. 8. Visual Placemat with Zones 🗺️ ₹150–500 — Structure extends beyond the plate. Every item has a designated space — predictability before eating begins. Pinnacle Recommends: Laminated, wipeable, consistent design. Same placemat every meal. 9. Child-Size Serving Utensils 🥄 ₹150–400 (set) — Dedicated spoon per food — contamination is prevented before it even reaches the plate. Pinnacle Recommends: 6–8 small matching spoons/forks. Color-code by food type optionally. 🛒 Minimum Effective Setup (₹650–1,800 total): Divided plate with deep sections + Sauce containers with lids + Tiffin box for school. This trio solves 80% of food separation challenges at home and school immediately.

Commercial Option | DIY / Zero-Cost Alternative | Why It Works | |
Divided plate (₹300–1,000) | Regular plate with a washed bottle cap or small steel katori placed between foods | Creates physical barrier — same principle as divided sections | |
Tiffin with compartments (₹200–800) | Wrap each food in a separate small steel vessel from your kitchen set | The physical separation is what matters, not the vessel brand | |
Individual katoris (₹150–500) | Any set of 4–6 small matching bowls from your kitchen | Matching bowls reduce visual chaos — household sets work perfectly | |
Silicone dividers (₹200–600) | A folded piece of parchment paper or banana leaf placed between foods | Provides a visible, physical barrier the child can see and trust | |
Bento box (₹400–1,500) | Pack each food in its own small tiffin — multiple small steel boxes | Complete compartmentalization achieved with household items | |
Color-coded containers (₹300–800) | Mark existing containers with colored tape or rubber bands | The visual coding system is the intervention, not the container brand | |
Sauce containers (₹100–400) | Small steel katori with a small plate placed on top | Contains wet items — purpose is liquid isolation | |
Visual placemat (₹150–500) | Draw zones on a large piece of paper, laminate with clear tape, use daily | The predictable spatial structure is the therapeutic element | |
Separate utensils (₹150–400) | Select 6–8 matching spoons from your existing set, designate one per food | Designation and consistency are the intervention, not the spoon brand |
🚦 Read This Before Every Session
Safety First 🔴 RED — ABSOLUTE STOP SIGNS Do NOT proceed if: Child is in active meltdown or severely dysregulated state Child is ill, in pain, or unusually fatigued Child has not eaten for an extended period (hunger intensifies distress) Child shows signs of medical feeding difficulty (gagging on all foods, failure to gain weight) Anyone is pressuring or forcing food — stop immediately ⚠️ AMBER — MODIFY & PROCEED WITH CARE Child is mildly dysregulated — simplify to 2 foods only in most trusted vessels Child had a difficult day — reduce variety, maintain separation, reduce duration New environment — bring portable tools; don't force eating Caregiver is stressed — take a breath before serving; children detect caregiver anxiety ✅ GREEN — PROCEED Child is calm, rested, and in a regulated state Familiar environment with familiar foods in familiar vessels All tools are set up BEFORE child comes to table No time pressure on mealtime duration Everyone at table is calm Material Safety Checklist ☑️ All containers food-grade (stainless steel, BPA-free silicone, or food-safe plastic) ☑️ No small parts that are choking hazards for child's age ☑️ Silicone dividers: child is age-appropriate (supervised with under-3s) ☑️ Hot foods: ensure containers are appropriate for temperature ☑️ Child can open lids independently if needed at school 🚨 Emergency Stop: Stop the session if child gags uncontrollably, vomits, becomes severely distressed, refuses all food, or shows signs of aspiration. Consult a feeding therapist or pediatrician immediately. 📞 9100 181 181 — FREE, available 24×7 if you are concerned 📚 Indian Journal of Pediatrics RCT (2019) | DOI: 10.1007/s12098-018-2747-4

- Clear the table — remove all unnecessary items, distractions, screens
- Place the placemat in the child's established position
- Set up all containers BEFORE child comes to table — no serving in front of child
- Pre-fill sauce containers and seal before child arrives
- Arrange each food in its designated section/container — verify no cross-contact
- Place serving utensils for self-serving if child is able
- Set up drink in child's preferred cup in top-right zone
- Only then invite the child — do not call child while still arranging
- ❌ Mixed dishes (casseroles, stir-fries, curries with mixed ingredients)
- ❌ Any container that has previously caused distress
- ❌ Screens and devices (unless used as calming support — OT decision)
- ❌ Pressure or commentary about eating ("just try one bite" is a mealtime dysregulator)
- 💡Lighting: Warm, even — no harsh fluorescent
- 🔊Sound: Quiet or familiar background; no TV with commercials
- 🌡️Temperature: Comfortable — extremes increase sensory sensitivity
- ⏱️Time: Minimum 20 minutes, no rush to end
Check | ✅ Go | ⚠️ Modify | 🛑 Postpone | |
Last meal timing | 2–4 hours ago (hungry but not starving) | More than 4 hours ago (very hungry, lower tolerance) | Has just eaten; not hungry | |
Regulation state | Calm, engaged, responsive | Slightly elevated; mildly dysregulated | Meltdown, crying, severely dysregulated | |
Sleep status | Well-rested | Mildly tired | Severely overtired | |
Recent events | No recent triggers | Minor upset within last hour | Major meltdown or trauma in last 2 hours | |
Physical comfort | No apparent illness or pain | Slight discomfort | Illness, teething pain, headache | |
Environment | Familiar, quiet setting | Slight disruption | Completely unfamiliar or highly noisy | |
Caregiver state | Calm, patient | Slightly stressed | Highly stressed, rushed |
"The best session is one that starts right. A skipped meal in a dysregulated state is better than a forced meal that creates trauma associations with eating."
"[Child's name], your plate is ready. Everything has its own space — [food A] is here, [food B] is here, [food C] is here. Nothing is touching. Come see."
- Child approaches table and begins visual inspection
- Caregiver says: "Can you check that everything is in its own space?"
- Child points to or names each food — acknowledge: "Yes, the rice is right there. The dal is in its own container. Nothing is touching."
- If child requests a change — DO IT without commentary
- Once child signals readiness, meal begins
- Never force or carry child to table
- Check readiness indicators (Card 13) — likely a postpone situation
- Offer a visual schedule showing what comes after eating
- Check if hunger level is adequate

Step 3: The Meal Itself — The Separation System in Action
Step 3 🟠 OT Primary The Core Therapeutic Event: The child eating calmly from properly separated foods IS the therapeutic event. Every calm, distress-free meal actively rebuilds positive neural associations between eating and safety, reduces the amygdala's threat response, and establishes the neurological baseline from which gradual flexibility work will eventually be possible. Caregiver Action Child Target Stay present but not hovering Eating from at least one food item Minimal commentary — silence is therapeutic Remaining at table for at least 10 minutes If sauce container needs opening — do so slowly, away from plate Tolerating others' mixed food at same table If food accidentally touches — calmly offer replacement or clean section Completing the meal without significant distress Celebrate effort, not consumption: "I see you trying that" Not requiring caregiver intervention to manage plate Child Response Spectrum ✅ Ideal Eats all foods, stays calm, shows no distress ✅ Acceptable Eats 1–2 foods fully, tastes others, finishes in own time ⚠️ Watch Inspects excessively, eats very little, but stays calm 🛑 Concerning Distress despite correct setup — review Card 13 readiness indicators Duration: 15–25 minutes typical. Do not extend beyond 30 minutes. 📚 Meta-analysis (World J Clin Cases, 2024) | PMC10955541
- Frequency: 2–3 main meals per day using the full separation system
- Duration: 8–12 weeks minimum before expecting measurable tolerance changes
- Repetition principle: Predictable, identical setup every meal — novelty is the enemy of sensory safety
"3 calm meals > 10 pressured ones" — quality of the mealtime environment matters more than how much was eaten
- New safe food in its own container — one new food in its own separate vessel, no pressure to eat
- Slightly larger sections — same foods, slightly more in each section
- Different vessel — same food, new container (prepare child verbally)
- Foods on same tray but further apart — first step toward eventual proximity
- Child pushes away from table
- Child indicates "all done" (verbally or via sign)
- Eating pace slows significantly
- Child begins to play with food rather than eat it

- "I noticed you stayed calm even when the dal was next to the rice — that took real strength."
- "You tried the carrot today. That's progress."
- "You finished your lunch. Let's celebrate."
- "See, that wasn't so bad!" — invalidates their sensory experience
- "If you eat more, you'll get dessert" — creates food-reward associations

- Do NOT remove food from table forcibly
- Give 2-minute warning via visual timer
- Acknowledge: "I know you want more. There will be food at [next meal]."
- Consistent practice over 2–3 weeks reduces end-of-meal resistance
- Today's date + meal (breakfast / lunch / dinner)
- Distress level (0–5 scale): 0 = completely calm, 5 = severe meltdown
- Eating completion (0–100%): approximate % of food offered that was eaten

Session Abandonment Is Not Failure — It's Data
Troubleshooting ❓ Foods touched accidentally. Child refused entire meal. 🔑 Prevention: Pre-fill ALL containers before child comes to table. For wet foods: sealed sauce containers. For the immediate situation: calmly offer to replace the affected food if possible. Never minimize: "It's fine, it barely touched." Their experience is real. ❓ Child accepted meals for 3 weeks, then suddenly rejected everything. 🔑 Regression is normal, especially with illness, schedule change, school transition, or new family stress. Return to the most basic, trusted setup. No new foods. No variations. Regression typically resolves in 1–2 weeks. ❓ New caregiver doesn't follow the system and child now refuses to eat. 🔑 See Card 37 for family sharing resources. The system works only when applied consistently across all caregivers. Brief the school/care-provider with the printed protocol. For school lunch: send identical setup every day. ❓ Child's rules are getting stricter — now certain foods can't be on the same table. 🔑 This is escalating rigidity — seek professional OT/feeding therapy evaluation. This pattern suggests underlying anxiety is driving the food rules. Call 9100 181 181 for assessment guidance. ❓ Child eats at home but refuses to eat at school/restaurants. 🔑 Pack identical school setup from home (same divided tiffin, same setup). For restaurants: bring portable silicone dividers and sauce containers. Practice at a quiet, familiar restaurant first. Build up gradually. ❓ Child is not gaining weight despite eating during separated meals. 🔑 This is a medical red flag — consult pediatrician urgently. A pediatric dietitian can assess whether nutrition within accepted foods is adequate. ❓ I'm consistent, it's been 3 months, but distress levels haven't changed. 🔑 Professional evaluation needed. The child may need formal sensory integration therapy, ARFID-specific treatment, or anxiety treatment in addition to accommodation. Contact our feeding specialists: 9100 181 181. OT • SLP • ABA • SpEd Consortium Validated
Parameter | Easier Version | Standard | Harder Version (when ready) | |
Separation level | Individual katoris — maximum separation | Divided plate with deep sections | Divided plate with shallow dividers | |
Foods introduced | Only 2–3 known safe foods | Usual range of safe foods | Include 1 new food in own container | |
Sauce handling | All wet foods removed or sealed | Sealed sauce containers on tray | Sauce in small section of divided plate | |
Caregiver presence | Caregiver at table throughout | Caregiver nearby | Caregiver in room but not at table | |
Meal duration | 10–15 minutes | 20–25 minutes | Up to 30 minutes with timer |
- Ages 2–4: Finger food friendly; maximum separation; caregiver at table throughout
- Ages 5–8: Self-serving; token economy; visual timer visible
- Ages 9–12: Independent setup practice; portable tools for independence; peer lunch navigation

- Child comes to table without being chased or carried
- Child inspects plate and does NOT immediately leave
- Mealtime lasts longer than 5 minutes
- Child eats at least one food from the plate
- Distress score drops from 4–5 to 3–4 (reduced, not eliminated)
- Caregiver reports one meal that felt "calmer than usual"
- Child still inspects plate extensively — this is building trust, not obsession
- Child still refuses some foods — separation tolerance ≠ food variety increase yet
- Some meals still end in distress — 1–2 difficult meals per week is normal
Week 1–2 often feel like "nothing is working." They are. The nervous system doesn't change in 14 days. What you are building is trust — and trust takes time. Your consistency is the therapy.

Weeks 3–4: Neural Pathways Are Forming
Progress Arc Weeks 3–4 Progress Milestone Weeks 3–4: Consolidation and ownership of the system Anticipation Child begins to anticipate the mealtime setup — may come to table without prompting Ownership Child asks for specific containers/vessels — signals ownership of the system Duration Mealtime duration extends naturally — 20+ minutes now possible Variety Eating variety within accepted foods improves — eats more different safe foods Generalization Seeds — Watch for These Spontaneous Behaviors "Can I have the green bowl for my dal at school too?" — child is generalizing the system Child sets up own place at table before being asked — child is internalizing the protocol Child shows sauce container to sibling and explains it — child is self-advocating Parent Milestone: "You may notice you're more confident too. Your instincts about your child's readiness are becoming sharper. That's a clinical skill you've developed."
- Mealtime is calm — consistently, predictably, across most meals
- Child eats adequately — nutrition is no longer a crisis concern
- Child can tolerate minor variations in setup without major distress
- Portable system works — school lunch, outings, family gatherings manageable
- Child self-advocates: "I need my divided plate"
- Caregiver reports mealtime stress level dropped significantly
- ✅ Functional calm eating with accommodation
- ✅ Adequate nutrition within accepted foods
- ✅ Self-management of separation needs across settings
- ❌ Does NOT mean eating all foods mixed
- ❌ Does NOT mean the preference for separation disappears
- ❌ Does NOT mean the work is "finished"

Before | Now | |
Distress 4–5 at every meal | Distress 1–2 at most meals | |
Meals lasting 5 minutes (rejection) | Meals lasting 20–25 minutes (completing) | |
Eating less than 30% of what was offered | Eating more than 70% of what was offered | |
Daily meltdowns at mealtimes | Rare episodes with known triggers |
"The Pinnacle Blooms Consortium has witnessed thousands of mealtimes transform through this exact protocol. What you've accomplished is not small. It is the foundation for everything that comes next." — Pinnacle Blooms Feeding Therapy Team
- Weight loss or failure to gain weight → Pediatrician urgently
- Accepted foods decreasing over time → Feeding therapist urgently
- Extreme distress with full accommodation correctly applied → OT + Feeding specialist
- Food rules expanding beyond the plate (can't be cooked in same pan) → Anxiety/OCD evaluation
- Nutritional deficiency symptoms (fatigue, pallor, poor growth) → Pediatrician + Dietitian
- Gagging or vomiting regularly even on accepted foods → Medical + Feeding evaluation
- Mealtime terror despite months of accommodation → Multi-disciplinary evaluation
- Social isolation (refuses all food outside home) → ARFID evaluation
- New food refusals appearing (was eating 10 foods, now only eating 6)
- Night waking related to food anxiety
- Sibling imitating the food rules
- Caregiver burnout becoming severe
- ← E-453: Texture Sensitivity and Food Aversion
- ← E-454: New Food Introduction Resistance
- → E-456: Utensil Use Development
- → E-460: Mealtime Sensory Overload
- ↔ Domain A: Sensory Processing
- ↔ Domain C: Emotional Regulation
More Techniques for Feeding Independence
Feeding Series Technique Code Difficulty Materials You Already Have Texture Sensitivity & Food Aversion E-453 Foundation ✅ Katoris, dividers New Food Introduction Resistance E-454 Foundation ✅ Divided plate, bento You Are Here: Foods Can't Touch E-455 Foundation ✅ Full starter kit Utensil Use Development E-456 Foundation ✅ Serving utensils from this technique Self-Feeding Independence E-457 Intermediate ✅ Setup from this technique Mealtime Sensory Overload E-460 Foundation ✅ Placemat, visual supports 🛒 "You Already Own These Materials": With the starter kit from E-455, you have materials for 4 other techniques in this cluster — your investment works across the feeding series. → Browse Full Feeding Series: techniques.pinnacleblooms.org/feeding-sensory
- Feeding Independence Readiness Index (direct impact)
- Sensory Regulation Readiness Index (indirect impact)
- Mealtime Participation Readiness Index (direct impact)
- AbilityScore® — tracked across all 12 domains
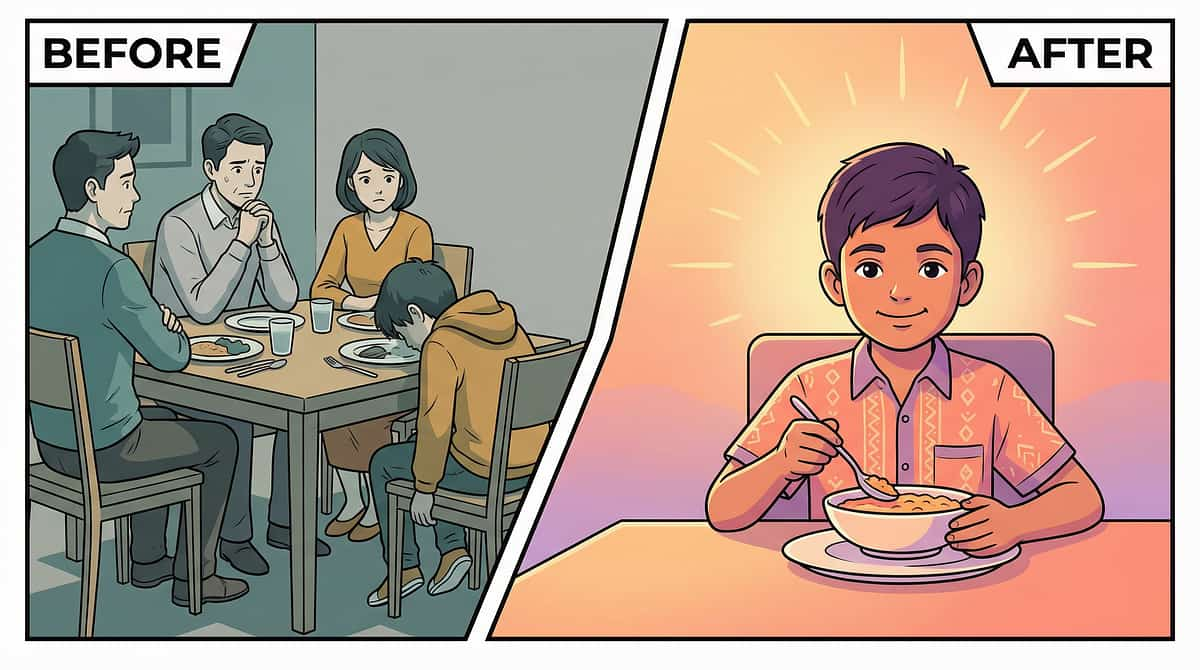
From Battleground to Mealtime Peace
Parent Stories "Mealtimes were a battlefield. If any food touched another food, our son would refuse the entire meal and melt down. We were exhausted from managing every plate. The feeding therapist helped us understand this was sensory-based, not defiance. We got divided plates with deep sections, separate containers for sauces, and let him serve himself. Within weeks, mealtimes were calmer. He's still not eating mixed foods, but he's eating — calmly, adequately, and without daily meltdowns. That's progress." — Parent, Pinnacle Network Distress Score From distress 4–5/5 at every meal to 1–2/5 at most meals Meal Duration (min) From 5-minute rejections to 20–25 minutes completing meals Foods Per Meal From fewer than 3 foods to 5–7 separated foods eaten per meal "I spent three years thinking I was a terrible mother because my daughter wouldn't eat. The divided plate changed everything. She inspects it, approves it, and eats. Simple solution to what seemed like an impossible problem." — Parent, Hyderabad | Pinnacle Network Parent Community Outcomes vary by child profile, underlying factors, and intervention approach. → Join 50,000+ Pinnacle parents: pinnacleblooms.org/community
You Don't Have to Navigate This Alone
Community Pinnacle Parent WhatsApp Community 50,000+ parents sharing daily mealtime wins, setups, material reviews, and peer support. → pinnacleblooms.org/whatsapp-community GPT-OS® Parent Forum Share data, ask questions, get therapist-moderated answers. → pinnacleblooms.org/forum #SeparationSetup — Share Your Setup Parents sharing divided plate configurations, tiffin setups, and mealtime wins. @PinnacleBloomsNetwork on Instagram, YouTube, Facebook, Twitter. Feeding Support Circle Monthly virtual group sessions facilitated by Pinnacle OT and feeding therapists. → pinnacleblooms.org/feeding-circle "Finally found a tiffin with truly separate compartments!" | "My daughter set up her own placemat today — milestone!" | "Sauce container changed everything — dal stays away from roti" 📞 9100 181 181
# | Study | Finding | Link | |
1 | PRISMA Systematic Review, Children (2024) | Sensory integration is evidence-based practice for ASD; 16 articles, 2013–2023 | PMC11506176 | |
2 | Meta-analysis, World J Clin Cases (2024) | SI therapy promotes adaptive behavior, social skills, sensory processing, motor skills; 24 studies | PMC10955541 | |
3 | Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory interventions: significant outcomes, RCT | DOI: 10.1007/s12098-018-2747-4 | |
4 | NCAEP (2020) | Visual supports + structured accommodation: EBP for autism | NCAEP EBP Report | |
5 | WHO Nurturing Care Framework (2018) | Responsive caregiving + sensory-appropriate environments: global evidence | nurturing-care.org | |
6 | WHO/UNICEF CCD Package (2023) | Home-based caregiver interventions implemented in 54 countries | PMC9978394 |

- Distress trajectory (decreasing = good; plateau or increasing = escalation trigger)
- Eating completion percentage correlation with setup variables
- Generalization patterns (does improvement at home transfer to school?)
- Next-technique readiness signal (when to introduce E-456)
- Divided plates in action — real mealtime demonstrations
- Tiffin box compartmentalization for school lunch
- Silicone dividers — how to place and use
- Sauce containers — preventing liquid contamination
- Visual placemat — full mealtime setup in 60 seconds
- 📱 Instagram: @PinnacleBloomsNetwork
- ▶️ YouTube: @PinnacleBloomsNetwork
- 📘 Facebook: @PinnacleBloomsNetwork
Consistency Across Caregivers Multiplies Impact
Share & Generalize WHO CCD Package: Multi-caregiver training is critical for intervention generalization. If the separation system works at home but not at school, or with one parent but not the other, the gains are cut in half. Share This Page 📱 WhatsApp — Share this page directly with family members 📧 Email — Send to teachers, grandparents, care providers 🔗 Copy Link — techniques.pinnacleblooms.org/feeding-sensory/foods-cant-touch-food-separation-e455 Downloadable Resources 📄 Family Guide — Foods Can't Touch: 1-page simplified protocol for grandparents, relatives, and care providers 📄 School Lunch Protocol Card: Pocket-sized card for school lunch supervisors and teachers WhatsApp Message Template "Hi [Name], I wanted to share something important about [child's] mealtimes. The therapist has helped us understand that [child] needs foods to be separated — this is neurological, not behavioral. Here's the setup we use: [link]. Could you follow the same setup when you feed them? It makes a huge difference. Thank you." Grandparent-Simplified Explanation "Your grandchild's brain processes mixed or touching foods as uncomfortable — the same way some of us feel about certain textures. When foods are separated properly, they can eat calmly and well. Please follow the same setup we use at home." 📚 PMC9978394 (WHO CCD Package — multi-caregiver implementation)

Preview of 9 materials that help when foods cant touch Therapy Material
Below is a visual preview of 9 materials that help when foods cant touch therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.