- Proprioceptive sensors in hand
- Spinal cord relay
- Cerebellum coordination
- Motor cortex command
- Arm movement execution
- Spoon-to-mouth delivery
Age | Typical Milestone | What "Messy" Means Here | |
6–9 months | Hand-to-mouth with fingers | Very messy — completely normal | |
12–15 months | Begins spoon use (fist grip) | Significant spilling — expected | |
18–24 months | Improving spoon aim, fork introduction | Moderate mess — still normal | |
2–3 years | Proficient spoon/fork | Minor mess, mostly contained | |
3–4 years | Refined, neat eating | Minimal mess | |
4+ years | Age-appropriate independence | Occasional spills only |


Domain | Age Range | Frequency | Duration | Lead Discipline | |
Feeding + Fine Motor | 18 months–10 years | Every mealtime | Ongoing | Occupational Therapy |

"The brain doesn't organize by therapy type. Eating involves sensory, motor, behavioral, oral, and postural systems simultaneously — which is exactly why our consortium approach works." — Pinnacle Blooms OT + Feeding Consortium

- Food consistently reaching mouth
- Plate remaining on table during scooping
- Clothes remaining relatively clean by meal end
- Spoon held with 3-finger or palm grip
- Wrist not rotating excessively mid-arc
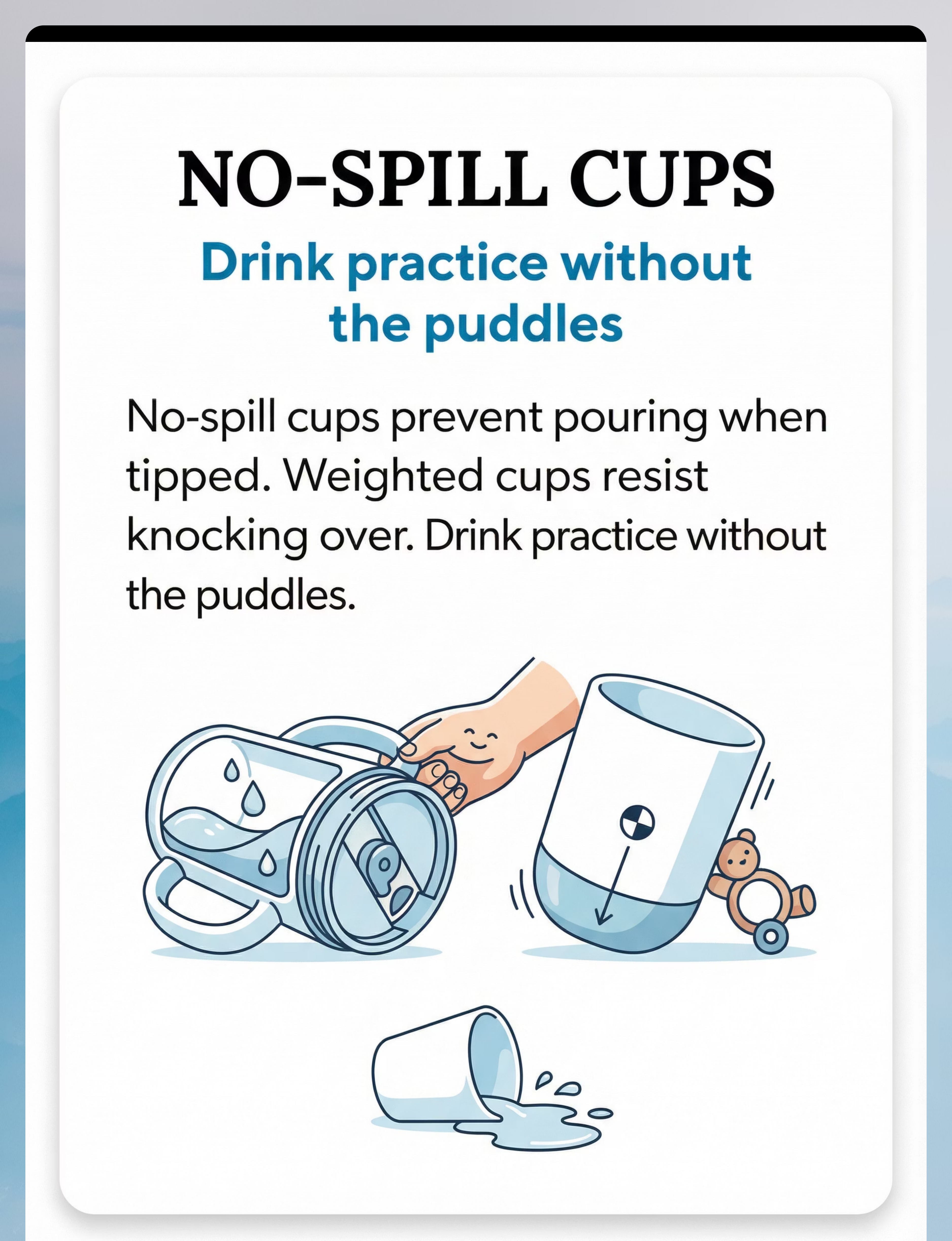
- Cup held without spilling
- Child eating at school without shame






Commercial Option | Zero-Cost DIY Alternative | |
Weighted utensils (₹400–1,200) | Wrap handle of regular spoon with wet sand-filled tape OR use a stainless steel heavy ladle — the weight principle is identical | |
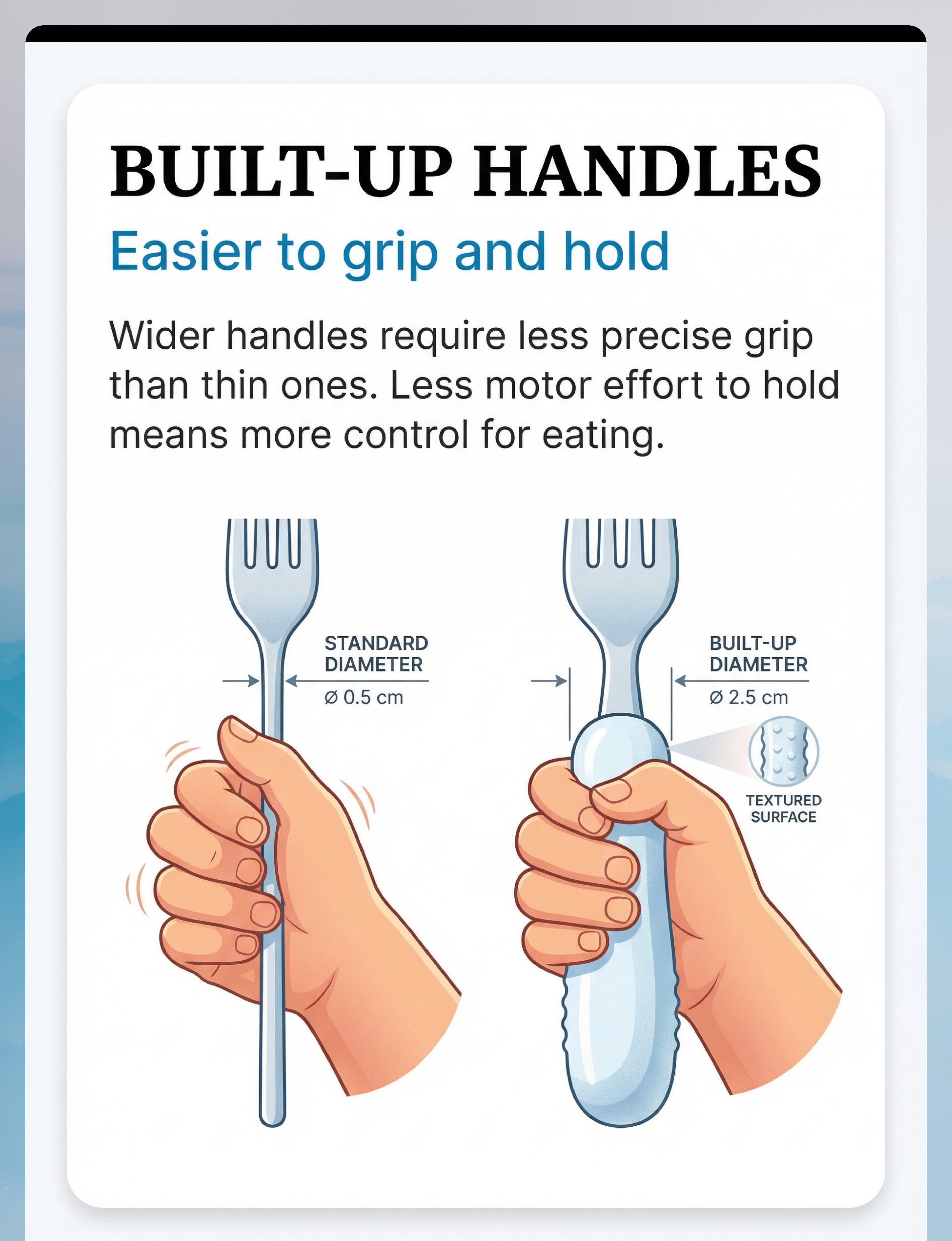
Built-up handle (₹200–800) | Wrap regular spoon handle tightly with several layers of rubber band or cloth tape until diameter fills child's palm | |
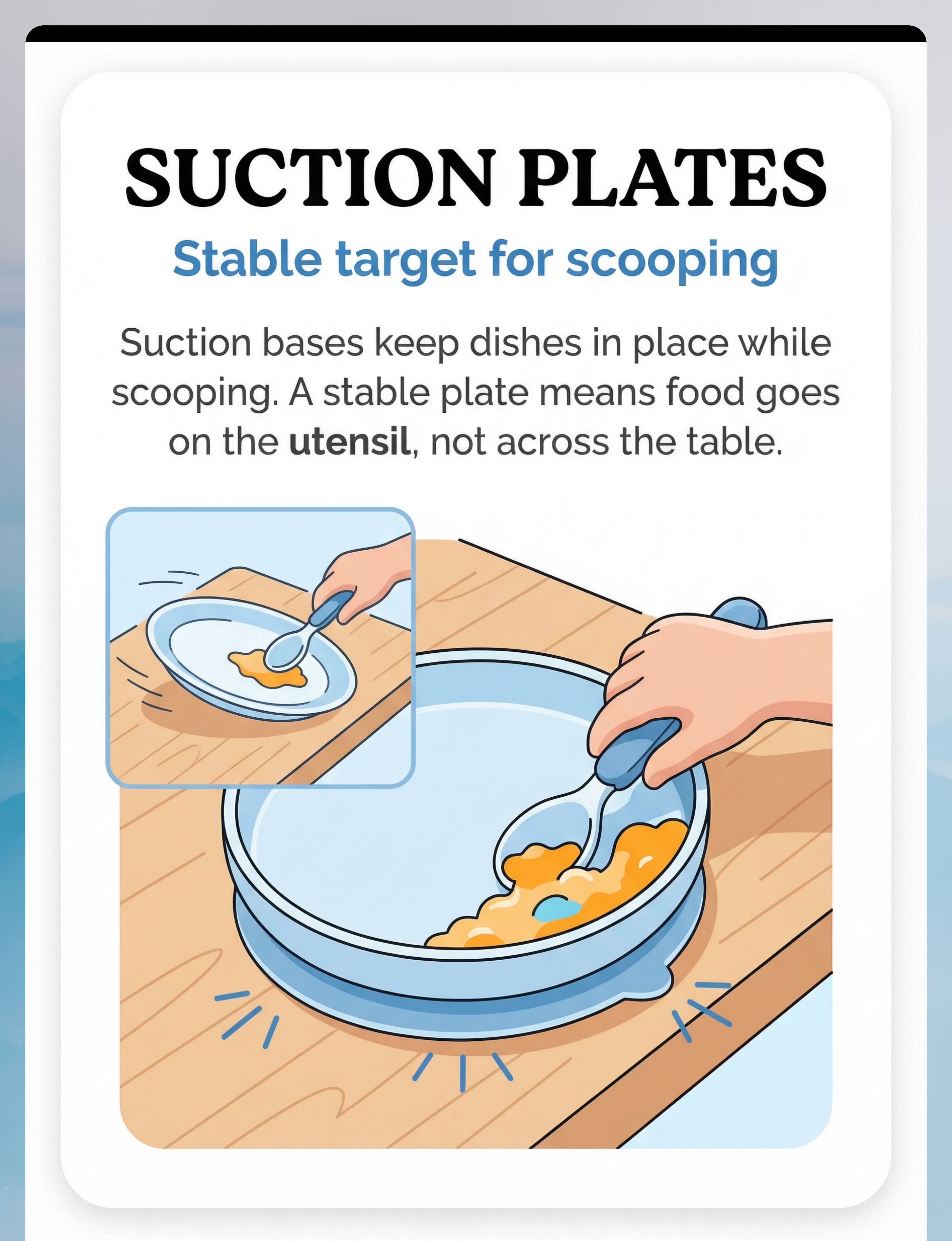
Suction plate (₹300–1,000) | Place regular plate on damp non-slip rubber mat (same fixation principle) OR use heavy steel thali | |
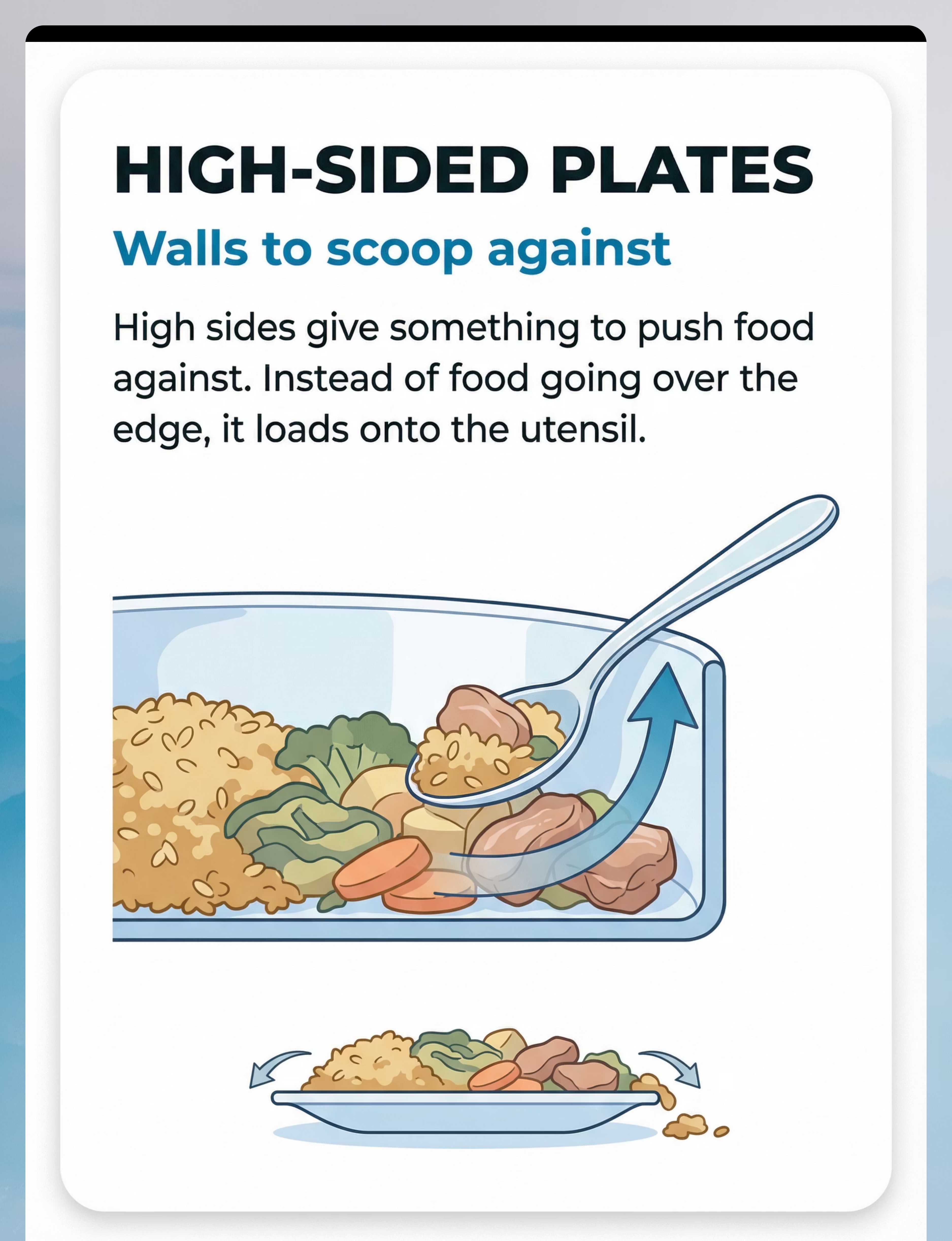
High-sided bowl (₹200–700) | Use any deep kadai/steel bowl rather than a flat plate — same "wall to scoop against" | |
Non-slip placemat (₹200–600) | Lay a damp kitchen towel or yoga mat piece under the plate | |
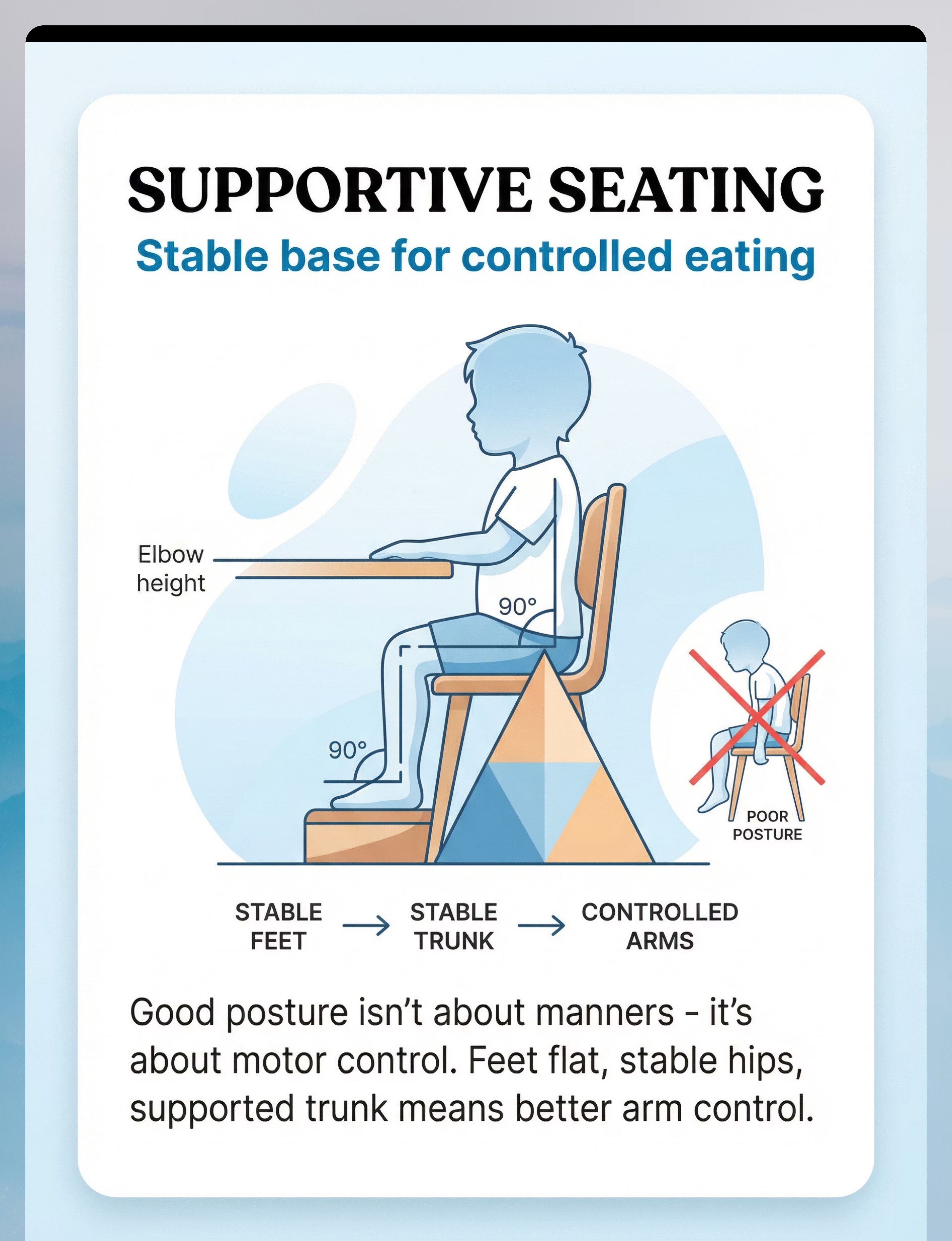
Foot support (₹500–3,000) | Stack 2–3 firm cushions or books under feet — measure to ensure hips at 90° | |
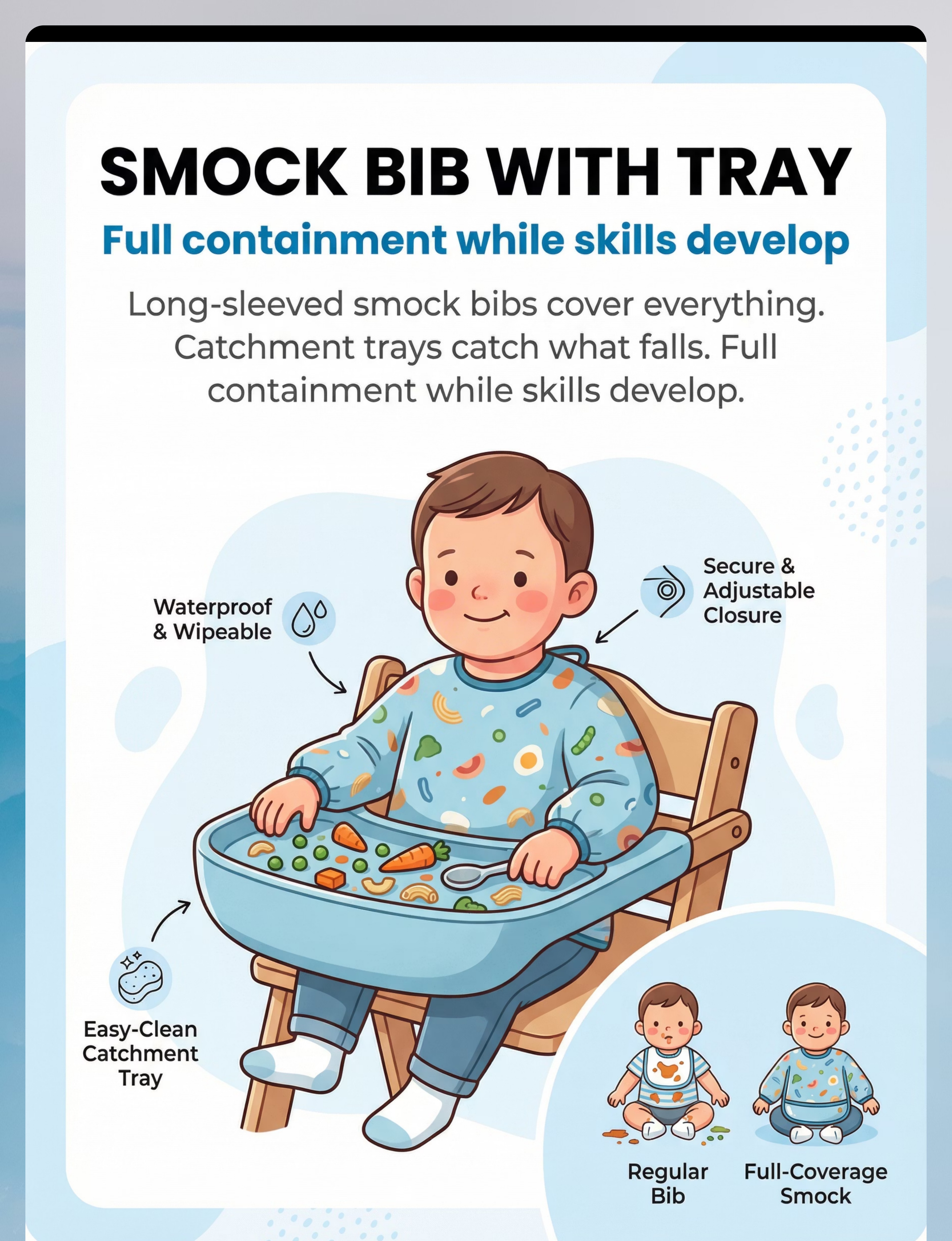
Smock bib (₹300–1,200) | Use an old adult T-shirt worn backwards as full-coverage protection |

- Child has dysphagia (swallowing disorder) — seek SLP assessment first
- Child recently had a severe mealtime meltdown (within last 2 hours) — wait for regulated state
- Child has significant hypotonia — consult OT before introducing weighted utensils (increased fatigue risk)
- Any choking incident in last 72 hours — seek medical evaluation first
- Child has oral motor challenges — add SLP coordination
- Child has strong sensory aversion to specific textures — pair with desensitization protocol
- Child is under 18 months — use age-appropriate modifications only
- Weighted utensils: watch for arm fatigue in children with low tone; start with 5-minute use windows
- Child is in a calm, regulated state
- Not within 30 minutes of a recent meal
- Materials are clean, food-safe, and age-appropriate
- Parent/caregiver is calm and non-reactive to mess during the learning phase

- Feet flat on floor or footrest (not dangling)
- Hips at approximately 90°
- Table surface at elbow height when arms are relaxed
- Trunk supported — not slumping into table
- Chair pulled in close — no leaning forward
- Suction plate/high-sided bowl on non-slip mat
- Cup at 2 o'clock position (dominant side)
- Parent seated at 90° to child, not directly opposite
- Smock bib and backup utensils within parent's reach
- Lighting: Bright, natural light preferred. No flickering fluorescent. Reduce glare from windows.
- Sound: Calm background. No TV during early skill-building phase.
- Temperature: Comfortable. Avoid distracting cold/heat.
- Remove from space: TV/screen, distracting toys, excessive background noise
Step 1: The Invitation (30–60 Seconds)
ACT III · STEP 1 Parent Script "[Child's name], it's lunchtime! Look, I have your special [spoon/bowl] ready. Come sit in your chair." Display the adapted material casually — not with excessive emphasis. Let the child see it as a normal part of the mealtime routine, not a medical device. Body Language Guidance Relaxed, open posture At child's eye level where possible Warm, matter-of-fact tone — not anxious or performatively cheerful Move slowly near the materials — no sudden movements ✅ Acceptance Cues — What to Look For Child moves toward chair Looks at materials with curiosity Sits down willingly Reaches for food or utensil ⚠️ Resistance Cues — What to Do Child refuses chair → Offer choice: "Do you want to sit here or here?" (2 acceptable options) Child grabs/throws material → Calmly retrieve. "The spoon stays on the table." Crying/avoidance → Assess if hunger-related or anxiety. If anxiety, use Modify protocol. Do not rush this phase. A child who arrives regulated at the table eats better — every time.
"Look at your special spoon — feel how it feels different in your hand. Now let's try scooping your [food]."
- Place utensil handle-first, close to dominant hand
- Do not force grip — let child pick up naturally
- For suction plate: press down in child's view so they see it "sticking" — demystifies the mechanism
- For smock bib: put on before food arrives, make it part of the pre-meal routine, not a reactive response to mess

- Parent holding plate steady (defeats the purpose of suction) → Remove hands
- Wiping child's face mid-bite (disrupts motor flow) → Wait for natural pauses
- Rushing child → Adaptive equipment use takes longer initially — this IS the practice
Weeks | Equipment Combination | Challenge Level | |
1–2 | Suction plate + Smock bib + Supportive seating | Foundation | |
3–4 | Add appropriate utensil (built-up OR curved OR weighted) | Add 1 tool | |
5–6 | Add no-spill cup | Add drink management | |
7–8 | Begin fading smock bib for 1 meal/day | Begin independence |
"3 successful bites with the adaptive spoon > 10 unsuccessful attempts with a standard spoon. Every successful repetition trains the motor pathway. Every failed one does the opposite."

- "You got the food all the way to your mouth — that was great holding!"
- "Look, your plate didn't move at all when you scooped!"
- Immediate thumbs-up with eye contact
- Clap once + big smile
- Token/star on visual chart
- Sticker chart (immediate visual token) — ₹364–589 on Amazon.in
- Preferred food as natural reinforcer (next bite of favorite item)
- Praise + physical comfort (high-five, shoulder squeeze) for children who enjoy touch
- Break card redemption if token economy is in place

- "Two more bites, then all done."
- "One more bite, then we clean up."
- "All done! Great eating today."
- "Can you put the spoon on the plate?"
- "Let's take off your bib together"
- Suction plate: let child "pop" the suction — often motivating proprioceptive feedback
- "Five seconds on the timer, then all done" — use visual timer
- Do not extend mealtime indefinitely — this creates negotiation patterns
- Natural consequence: "When the timer beeps, mealtime is over"
- Hand washing with warm water (proprioceptive + calming)
- Quiet preferred activity at table
- Gentle cleanup together
Data Point | What to Record | Options | |
Mess Level Today | How much mess relative to without equipment? | 1 (same) → 5 (much less) | |
Tool That Helped Most | Which material had most visible effect? | [List all 9] | |
Child Regulation | Child's emotional state at end of meal | Calm / Neutral / Distressed |
Troubleshooting: When It's Not Working
ACT III · TROUBLESHOOT Nine specific problems and their evidence-based solutions. Every challenge has a reason — and a fix. Problem Why It's Happening Solution Child refuses adaptive utensil Novelty aversion / sensory difference Introduce alongside preferred food. Let child hold it without eating for 3 days first. Suction plate immediately removed Exploration instinct / frustration Use stronger suction. Introduce during snack (less pressure). Pair with preferred food. Weighted utensil causes fatigue Weight too heavy / low muscle tone Switch to lighter option. Use only for first 5 minutes of meal. Feet come off footrest constantly Habit / not attending to body position Use visual marker on footrest. Physical prompt to replace feet calmly. Smock bib resisted Tactile sensitivity / routine disruption Introduce before meal for 5 days without food. Use preferred design. No improvement after 3 weeks Underlying cause not yet addressed Get OT assessment — may be postural or oral motor issue requiring targeted therapy. Works at home, not at school Generalization failure Send equipment to school. Coordinate with teacher using sharing templates. Child getting worse with equipment Wrong tool for this child's pattern Reassess which specific motor barrier is primary. Consult OT. Parent burning out Over-structured approach Simplify to 1–2 tools for 4 weeks. Reduce sessions. Sustainable > perfect.

Personalizing This for Your Child
ACT III · ADAPTATION Every child's messy eating has a different root cause. Match the tool to the cause — not to what's most popular or most recommended in general. If your child... Primary tool to start Has shaky, uncontrolled movements Weighted utensils (proprioceptive feedback) Drops utensils / can't maintain grip Built-up handle utensils (grip support) Tips food off spoon mid-arc Curved/angled utensils (reduce wrist rotation) Pushes plate while scooping Suction plate (anchors dish) Can't load spoon — food escapes plate High-sided bowl (scooping wall) Slumps, unstable at table Foot support + seating adjustment FIRST Spills drinks more than food No-spill cup + weighted cup General mess while skills develop Smock bib with catchment tray Age Adaptations 18 months–2 years: Focus on seating + suction plate. Utensils are secondary. 2–4 years: Introduce adaptive utensils once seating is optimized. 4–6 years: Begin systematic fading of supports as motor skills develop. 6–10 years: Focus on specific remaining barriers (often wrist control or proprioception). Sensory Profile Adaptations Sensory Seeker: Weighted utensils often very effective immediately. More proprioceptive feedback = better control. Sensory Avoider: Introduce materials gradually. Novelty aversion is real — don't force. Build tolerance with slow, low-pressure exposure. Difficulty Scaling ← Easier: Start with smock bib + suction plate only (containment + stability) → Harder: Remove smock bib for 1 meal/day, begin with open cup for 1 drink/day

- Child accepts adaptive materials without major resistance (3–5 days in)
- Plate remains in place more consistently (suction plate immediate effect)
- Slightly less food on floor (containment tools working)
- Child may eat more slowly — this is fine; they are using more cognitive attention for the motor task
- Dramatically neater eating across the board
- Independent, fluent utensil use
- Generalization to other settings


Week 5–8: Mastery Indicators
ACT IV · WEEK 5–8 For E-462 Adaptive Mealtime Protocol, mastery is defined by observable, measurable outcomes — not impressions or feelings. Food Reaches Mouth Successful bite rate at mastery threshold Cleanup Time Reduced Mealtime cleanup time reduced compared to pre-intervention baseline Consecutive Mealtimes Mastery criteria met for 5 consecutive mealtimes before beginning tool fading 🏆 Full Mastery Criteria Food reaching mouth successfully in 70–80% of attempts Child accepts all adaptive materials without resistance Meals completed without parent intervention on equipment Some spontaneous generalization (eating neatly at grandparent's house or school) When to Move vs. Stay ✅ Mastery met for 5 consecutive mealtimes → Begin systematic fading of one tool ✅ Mastery across 2 settings → Technique generalized, consider progression to E-463 ⏸️ Inconsistent mastery (good week/bad week) → Continue 2 more weeks before fading
"The motor pathways your child built at this table are permanent. They took 5–8 weeks to form and will last a lifetime. This is what real therapy looks like."


- E-463 (Eating Too Fast) — If mealtime speed becomes next primary challenge
- E-466 (Utensil Use Difficulties) — For advanced utensil refinement after basic mess is controlled
- E-470 (Self-Feeding Independence) — Full independence sequence
- If E-462 approach didn't resonate → Try E-461 (texture sensitivity may be driving avoidance)
- Or E-460 (overstuffing may be a linked motor pattern)






"Your experience with E-462 helps the family who finds this page next week. Consider sharing your journey." → Submit your story at pinnacleblooms.org
- 🔵Pediatric Occupational Therapist — primary lead: fine motor, postural, adaptive equipment
- 🟢Pediatric Feeding Therapist (SLP) — if oral motor component is significant
- 🟡BCBA/ABA Therapist — if behavioral resistance to mealtimes is primary

- Rate of mess reduction → calibrates motor intervention dosage
- Which tools worked → refines adaptive equipment recommendations for similar children
- Timeline to consolidation → improves population-level prognosis accuracy
- Parent adherence patterns → adjusts recommendation complexity
▶️ E-462: 9 Materials That Help With Messy Eating | Feeding & Mealtime Independence Series | Episode 462 | Duration: 60–75 seconds
- ← E-461: Food Texture Sensitivity
- → E-463: Eating Too Fast
Preview of 9 materials that help with messy eating Therapy Material
Below is a visual preview of 9 materials that help with messy eating therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.