
Safety Skills — 10 Evidence-Based Interventions for Children with Autism
Danger awareness, road safety, water safety, body safety, and emergency skills — explicitly taught, systematically practiced, and endlessly reinforced. Subdomain E4 | Pinnacle Blooms Network®
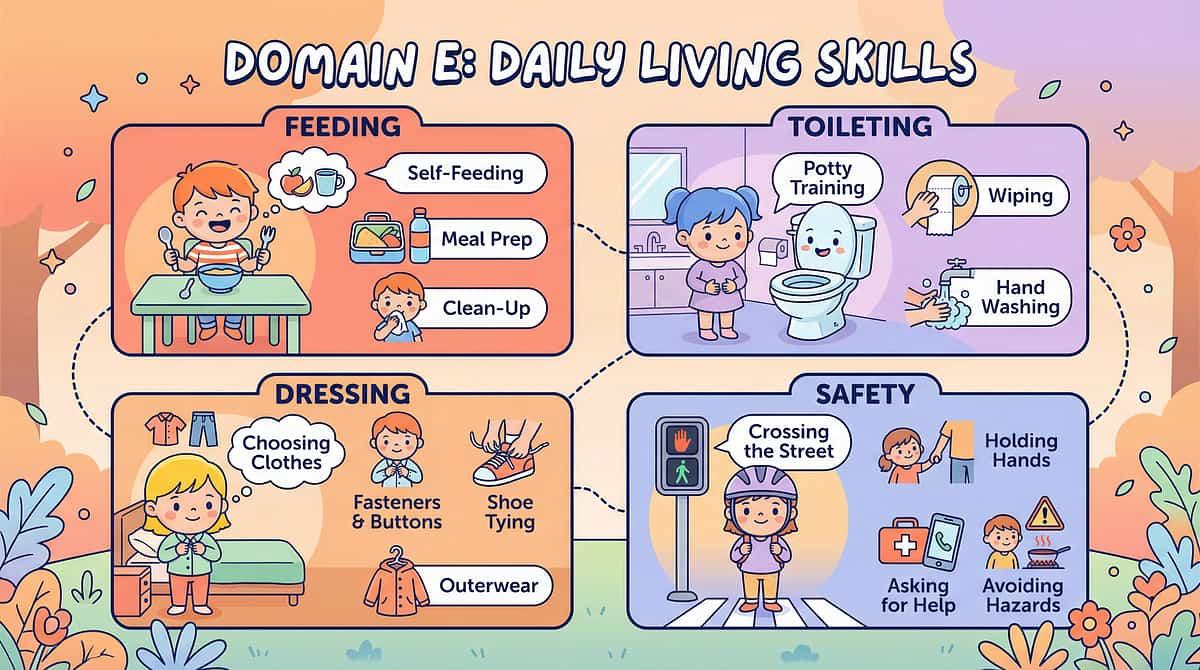
Domain E: Daily Living
E4: Safety Skills
10 Techniques

⚠️ Why Safety Skills Are a Life-or-Death Priority
Children with autism spectrum disorder face significantly elevated risks of accidental injury and death. Drowning is the #1 cause of death in children with ASD under 14. Traffic accidents, burns, poisoning, and exploitation follow closely behind. These are not hypothetical risks — they are daily realities for families navigating a world not designed with their children's safety profile in mind.
What makes this uniquely challenging is that safety learning in neurotypical children happens incidentally — through casual observation, fear responses, and social feedback. In ASD, each of these pathways is compromised. Safety skills must be explicitly taught, systematically rehearsed, and continuously maintained. This subdomain provides the clinical roadmap to do exactly that.
160×
More likely to drown than neurotypical peers
3–4×
Higher risk of abuse for children with disabilities
#1
Cause of ASD death under 14: drowning
10
Evidence-based techniques across 30 structured cards
The Neuroscience Behind the Safety Gap
Five distinct neurological gaps explain why safety is disproportionately harder for children with ASD — and why each must be addressed with targeted intervention rather than assumed to develop naturally.
Hazard Recognition Gap
Visual cortex + Hippocampus: Incidental safety learning is reduced. Danger recognition must be explicitly taught through structured, repeated exposure to visual and contextual cues.
Risk Assessment Gap
Orbitofrontal cortex: The OFC may underestimate real danger or overestimate harmless situations. Calibration is off — and must be corrected through direct instruction.
Impulse Inhibition Gap
Prefrontal cortex: The brake is too slow. A child can be in the road before the brain fully processes the danger signal. Automaticity — not thinking — is the goal.
Fear Calibration Gap
Amygdala: Reduced fear of genuine dangers (heights, traffic, water) coexists with extreme fear of harmless stimuli (toilets, balloons). The alarm system is miscalibrated.
Social Safety Gap
mPFC + Theory of Mind: Stranger danger requires understanding intentions. Theory of mind deficits lead to indiscriminate trust — making exploitation far more likely.

10 Techniques in This Subdomain
Subdomain E4 covers the full spectrum of safety skills — from environmental hazard awareness to personal information recall. Each technique is organized across three structured cards: Recognition + Neuroscience (A), Strategy + Intervention (B), and Home Protocol + Materials + Action (C).

Section 1: Environmental Safety
E-551 · Danger Awareness
E-551: Danger Awareness
The Moment
They walk toward the road without flinching. Reach for the hot stove without hesitation. Approach the barking dog without fear. The absence of danger awareness is one of the most terrifying parental experiences — watching your child move toward harm with zero recognition that harm exists. Because for their brain, it genuinely doesn't.
Level I Evidence — Explicit danger recognition teaching with visual supports, video modelling, and in-vivo practice. NCAEP 2020 | NAA Big Red Safety Box | PMC9978394
E-551: The Neuroscience of Danger Recognition
Danger awareness requires three sequential computations that must all be functioning and linked together. When any one fails, the child moves into danger as if it simply doesn't exist.
In many children with ASD, the amygdala fails to generate a fear signal strong enough to interrupt ongoing motor behavior. Without all three steps linked — recognition → fear → action — the child walks into danger as if it doesn't exist. Teaching must address all three stages explicitly and simultaneously.

E-551: Danger Awareness — Intervention Strategy
This technique builds a comprehensive danger vocabulary and discrimination skill set — teaching children to identify, categorize, and respond to hazards across all environments.
Build Danger Vocabulary
Teach HOT, SHARP, ROAD, DEEP, FIRE, STOP — each with a visual card, verbal label, and sign. Consistent multi-modal pairing accelerates encoding.
Danger Category Training
Teach by hazard type: things that BURN (stove, iron, diyas, hot water), CUT (knives, glass), CRUSH (traffic), DROWN (pools, tanks, rivers), and FALL (heights, balconies). Photo card discrimination — "DANGER or SAFE?" — 50+ trials per category.
Emotional Pairing
Teach the child to FEEL the alarm: "When you see THIS → your body says STOP." Linking the visual cue to an internal physical response is what creates an automatic reaction.
Generalise Across ALL Settings
Danger recognition locked to one location is not safety. Practice in-vivo in controlled conditions, then community settings under close supervision. Video modelling bridges the gap.
⚠️Environmental protection is always the FIRST layer. Lock the gate. Fence the pool. Guard the stove. Teaching is the second layer — it does NOT replace physical barriers.

E-551: Your Home Protocol — Danger Awareness
Daily Practice
- "DANGER or SAFE?" sorting game — 5 min daily with photo cards
- Community walks: point out dangers in real time ("See the car? DANGER. We STOP.")
- Video modelling: watch safety videos, pause and discuss responses
Home Danger Audit
- Kitchen: Stove guards, knife locks, hot water temp limiter
- Bathroom: Non-slip mats, locked medications, drained buckets
- Balcony: Mesh/grill, no climbable furniture near railing
- Electrical: Outlet covers, cord management
- Road access: High door locks, gate locks, door alarm
9 Canon Materials:Visual Schedule · Social Stories · Communication Board · Video Modeling · First-Then Board · Reward Charts · Emotion Cards · Calm-Down Kit · Visual Timer
Lead Professionals: ABA (BCBA) · Psychology | SpEd · OT · NeuroDev

E-552: Stop and Wait — Intervention Strategy
STOP must bypass PFC decision-making and activate a direct auditory-motor pathway: sound → auditory cortex → basal ganglia → motor cortex → FREEZE. This requires thousands of practice repetitions and must work even when the prefrontal cortex is offline during meltdown, excitement, or impulsive chase.
1
STOP
Motor freeze — not a verbal instruction to think about. Immediate, automatic. Say "STOP" → child freezes → IMMEDIATE powerful reinforcer. 50+ trials per week.
2
WAIT
Hold position after the freeze. STOP (freeze) → WAIT (hold) → "OKAY" (resume). Three-part chain practiced as a unit across all settings.
3
EVERYWHERE
Home, park, near roads, school, during running, during play — STOP must work in every environment with every person who gives the command.
Game-based practice: Red Light/Green Light (daily), Freeze Dance, Musical Statues — every freeze game IS safety training. The red hand signal (visual STOP) is paired with the verbal command for noisy environments and distance use.
⚠️ STOP must NEVER be followed by punishment. If "STOP" leads to scolding, the child learns to AVOID responding to STOP. Every successful stop → immediate praise, treat, or high-five.

E-552: Your Home Protocol — Stop and Wait
Daily Protocol
- 10 STOP practices per day — random timing during play, walking, running
- Reinforce EVERY successful stop immediately
- Red Light/Green Light: 5 minutes daily
- Community: "STOP" at every crossing, parking lot, gate
Mastery Criteria
Freezes within 2 seconds in 9/10 trials, across 3 settings, with 3 different people.
Until mastery is confirmed and maintained: CONSTANT supervision near any danger zone. No exceptions.

E-553 · Street Safety
E-552: Street Safety
⚠️ Traffic: #2 Cause of Death in Children with ASD (after drowning)
Indian roads present a uniquely dangerous environment: no sidewalks at most crossings, auto-rickshaws weaving unpredictably, bikes on footpaths, trucks without indicators, cattle crossing, and constant construction diversions. This is the most dangerous environment your child enters daily — and it demands explicit, repeated, graduated safety training.
Level I Evidence — Road safety skills with in-vivo practice. NCAEP 2020 | NAA
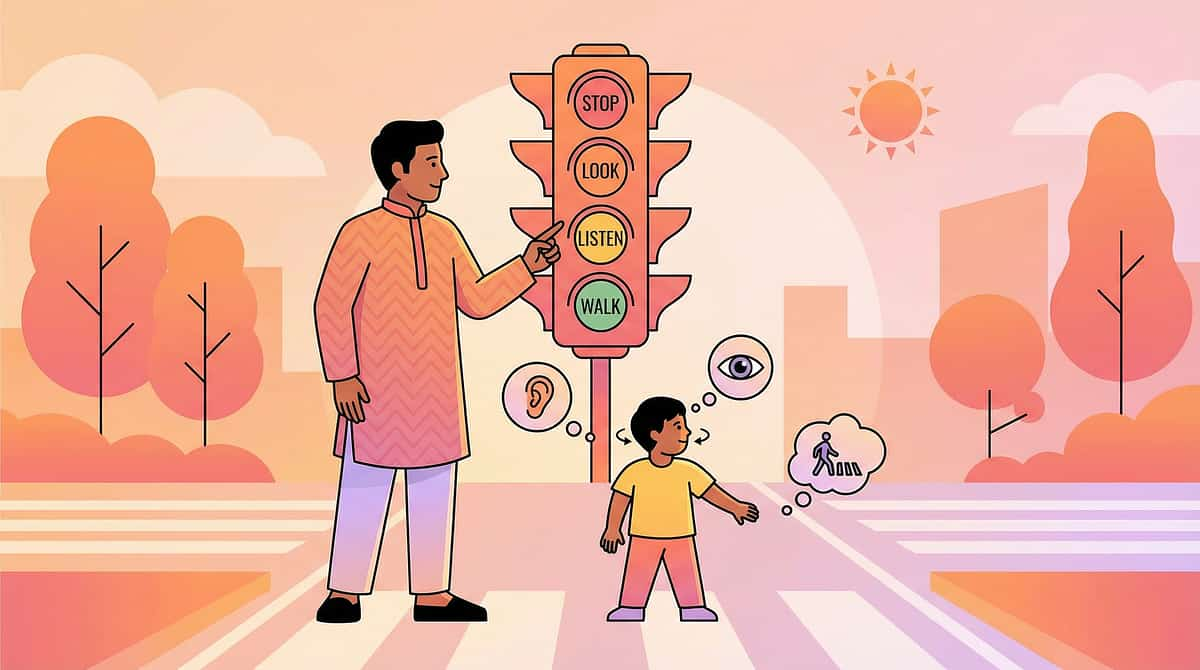
E-553: Street Safety — Intervention Strategy
Street safety is a five-component skill: visual scanning, auditory processing, speed-distance estimation, impulse inhibition, and sustained vigilance across the entire crossing — not just at the start. The four-step protocol provides a procedural anchor for all five.
Indian road-specific additions: crossing without zebra lines, auto-rickshaw approach awareness, two-wheeler speed awareness, open drain avoidance near road edges. GPS tracker and ID on child at all times (linked to E-416 elopement protocol).
⚠️ Requires 1,000+ trials before any consideration of independent crossing. Until mastery is firmly established: CONSTANT hand-holding at every road edge.

E-553: Your Home Protocol — Street Safety
Every single walk is a practice opportunity. Road safety training is not a separate lesson — it is woven into every community outing until the protocol becomes second nature.
01
Level 1
Parent holds hand. Parent checks for vehicles. Child observes and listens.
02
Level 2
Parent holds hand. Child checks WITH parent guidance and narrates what they see.
03
Level 3
Parent beside child. Child checks independently. Parent confirms.
04
Level 4
Parent two steps behind. Child leads the check and crossing sequence.
05
Level 5
Child crosses within parent's sight. Level 5 requires months of consistent Level 1–4 mastery across varied conditions.

E-554 · Water Safety
E-554: Water Safety
⚠️ Drowning Is the #1 Cause of Death in Children with ASD Under 14
Children with ASD are 160 times more likely to drown than their neurotypical peers. Many are actively attracted to water — drawn by visual fascination, tactile seeking, and vestibular input — while simultaneously lacking fear, being unable to call for help, and being unable to swim. The combination is lethal without active intervention.
Level I Evidence — Water safety is a life-saving clinical priority. NCAEP 2020 | NAA | ASD Drowning Research Data

E-554: Water Safety — The Neuroscience of Water Attraction
Water presents a paradox: the same sensory properties that make it rewarding to the ASD brain are what make unsupervised access so dangerous. Understanding this helps parents recognize why "he just knows to stay away" is never a safe assumption.
Visual Fascination
Light on water, movement, reflections — powerful visual stimuli that draw the child toward the source with strong approach motivation.
Tactile Seeking
Deep pressure of immersion and the sensation of water on skin provide intense sensory input that many ASD children actively seek out.
Vestibular Input
Floating and buoyancy provide vestibular regulation — the same system targeted in swings and movement therapy. Water is profoundly regulating.
Safety System Failure
While reward systems draw the child TO water, hazard recognition, fear response, and impulse control all simultaneously fail to prevent entry. Elopement toward water is the most dangerous elopement pattern.

E-554: Water Safety — Intervention Strategy
Rule #1 — Non-Negotiable
NEVER unsupervised near ANY water. Not for 30 seconds. Drowning takes 20 seconds and is completely silent. This rule has no exceptions.
Environmental Barriers First
Pool fencing (4-sided, self-closing gate), bathroom door locks, buckets and tubs drained immediately after use, well and tank covers — every open water source secured.
Survival Swim Lessons
NOT recreational swimming — survival: roll to back, float, reach edge. ASD-adapted instruction with a trained therapist. Swim skill alone does not equal water safety.
Indian Water Hazards
Temple tanks, construction pits (monsoon fills), open wells, river ghats, monsoon flooding, and BUCKET DROWNING — large vessels with water are lethal for young children and must be emptied immediately after use.
If Child Is Missing
Search WATER FIRST. Any pool, pond, ditch, tank, river, bucket within a 5-minute walking radius. Search water before calling anyone. Every second counts.

E-555 · Fire Safety
E-555: Fire Safety
The Moment
Fascinated by flames. Reaching for the gas stove. Standing too close to the diya. Fire presents a sensory-danger paradox: the visual system finds fire deeply rewarding — flickering light is a natural visual stim — while the danger is completely abstract. "Pretty things can hurt" requires PFC reasoning that may be delayed or unavailable in the moment of attraction.
Level I Evidence — Fire safety teaching with environmental protection. NCAEP 2020

E-555: Fire Safety — Intervention Strategy
"HOT" as Emergency Word
Visual (red flame symbol) + controlled tactile experience (warm surface → "THIS is warm. HOTTER = DANGER"). Build the sensation-word link.
Fire Identification
Candle, stove, matchstick, lighter, iron, hot water, hot oil — photo cards paired with "DANGER — HOT." Discrimination training across 50+ trials.
Distance Rule
"Stand BACK from fire" — arm's length minimum. Practice physically with visual floor markers near the kitchen entrance.
STOP — DROP — ROLL
Practice physically and make it a game. Weekly repetition. "If your clothes catch fire — STOP, DROP, ROLL." Fun practice = retained procedure.
Indian Fire Hazards: Gas stove (open flame), agarbatti/diya during puja, Diwali crackers, kerosene stove, kitchen oil fires. Environmental barriers: stove guards, locked lighters/matches, child-proof kitchen gate.

Section 2: Personal Safety
E-556 · What to Do If Lost
E-556: What to Do If Lost
The Moment
The market. The temple. The mall. One moment beside you — the next, swallowed by the crowd. A lost child with ASD presents a compound emergency: they may not ask for help (communication barriers), may not appear distressed (atypical expression), may not respond to their name (auditory processing), and may ELOPE further away as anxiety escalates. Being lost is not a momentary problem — it can become a catastrophic one within minutes.
Level I Evidence — Safety skills and identification strategies. NCAEP 2020 | NAA

E-556: What to Do If Lost — Intervention Strategy
The "STAY" rule reduces the search area exponentially. Every strategy below supports the primary goal: keep the child in one place until a trusted adult finds them.
STAY Rule
Lost → STOP MOVING. Stay where you are. This single instruction dramatically reduces the search area and is the most important survival behavior to teach first.
ID Always On Child
Laminated card or bracelet — full name, parent phone (Hindi + English), diagnosis statement: "I have autism — I may not respond or look scared." Waterproof, worn at all times.
Teaching "I'm Lost"
Verbal phrase, card to show, or AAC button — practiced until automatic. Pair with "Show this to someone in uniform" (visual of police, security, shop staff).
Technology Layer
GPS tracker (smartwatch/pendant — ₹2,000–5,000), phone tracking app, photo shared in advance with local shopkeepers, neighbors, and school staff.

E-556: If Your Child Is Missing — Emergency Protocol
1
Search Water First
Before anything else — check ALL water within walking distance. Pool, pond, ditch, tank, river, bucket. (E-554 protocol.)
2
Alert Security Immediately
Notify mall/temple/market security and police simultaneously. Show recent photo. Do not wait.
3
Show Photo to Everyone
Actively approach all nearby adults and staff. Do not wait for people to come to you. Cover ground systematically.
4
Check Sensory Magnets
Water features, escalators, toy shops, food stalls, music sources — favourite stimuli locations are the most likely places to find the child.
5
Call 100 or 112
Police emergency or India's unified emergency number. Have child's photo, ID card details, and GPS tracker access ready to share.

E-557 · Body Safety
E-557: Body Safety
⚠️ Children with Disabilities Are 3–4× More Likely to Experience Abuse
ASD amplifies vulnerability across every dimension: reduced ability to recognize inappropriate behavior, compliance training (taught to follow adults — predators exploit this directly), communication deficits that prevent reporting, sensory-seeking that may blur appropriate/inappropriate touch boundaries, and social naivety that produces indiscriminate trust. Body safety education is not optional — it is a clinical imperative for every child with ASD.
Level I Evidence — Body safety education essential for ALL children with ASD. NCAEP 2020 | WHO Violence Prevention Research
E-557: Body Safety — Intervention Strategy
Body Ownership
"MY body belongs to ME. No one touches without MY permission." This foundational concept must be explicitly taught and regularly reinforced — it does not develop implicitly.
Safe vs. Unsafe Touch
Safe: hug from parent, doctor WITH parent present, high-five. Unsafe: touching private areas, touch that feels bad, SECRET touch. Visual discrimination training with role-play.
NO — GO — TELL
Three-step response: say NO (even to adults), GO away from the situation, TELL a trusted person. Practiced until automatic — this is a motor chain, not a deliberation.
Trusted Person List
3–5 specific people the child can tell, shown on a visual card with photos: "These people will believe me." Review quarterly to keep current.
Secrets vs. Surprises
"Surprises are HAPPY and everyone finds out soon. Bad secrets are NOT okay — always tell." This distinction is critical and requires direct, repeated teaching.
Indian context: Cultural elder respect can directly conflict with "say no to adults." Children MUST learn that the body safety rule supersedes deference norms. Review compliance training to ensure body autonomy is explicitly preserved.
E-557: Your Home Protocol — Body Safety
Ongoing Teaching
- Body safety conversation: monthly, age-appropriate, calm, matter-of-fact
- "NO — GO — TELL" role-play: regular practice with trusted adults
- Trusted persons list: review quarterly with photos
- Vulnerability audit: who has unsupervised access to your child? Minimise.
- BELIEVE your child: if they disclose anything — believe first, investigate second. Always.
Red Flags — Act Immediately
Sudden behavior change · New fear of specific person or place · Unexplained regression · Increase in self-harm · Sexualised behavior · Sleep disturbance · Reluctance to be alone with a specific person
Any of these may indicate abuse. Consult a child protection professional immediately — do not wait, investigate, or confront the suspected person yourself.
E-558 · Private Parts Education
E-558: Private Parts Education
The Moment
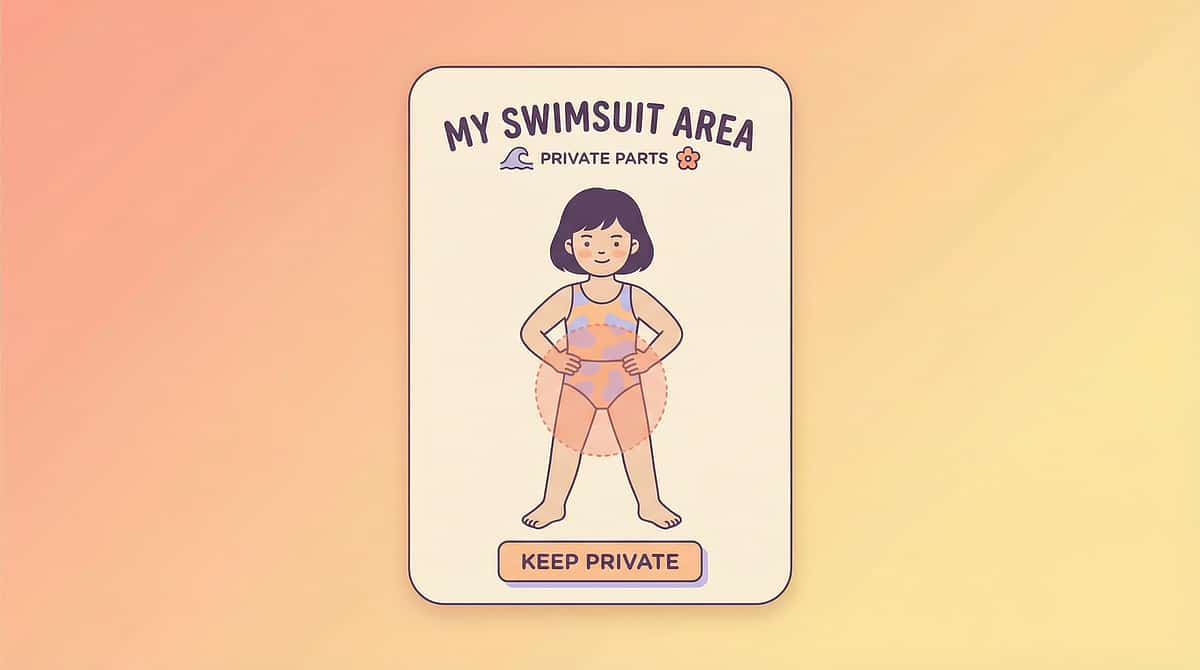
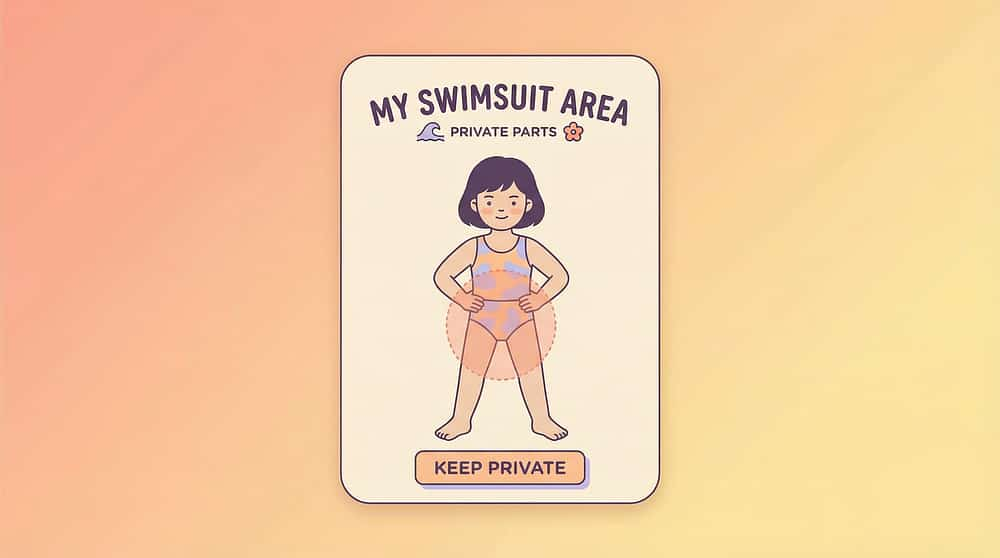
The practical teaching companion to E-557. Private parts education covers: identifying private body areas, understanding the bathing suit rule, and knowing that private parts are private — no one sees, no one touches except for medical or hygiene reasons with a trusted caregiver present. This teaching simultaneously protects against exploitation AND addresses public undressing and public touch behaviors that are common in ASD.
Level I Evidence — Explicit private parts education. NCAEP 2020 | Body Safety Curricula Research
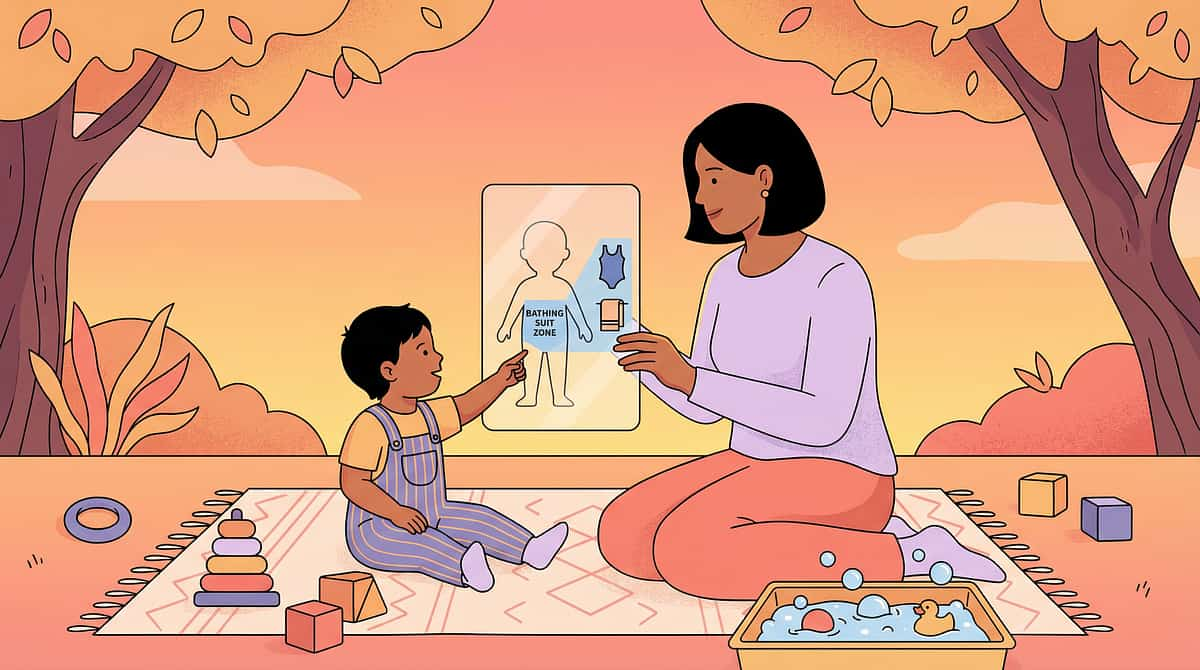
E-558: Private Parts Education — The Teaching Challenge
Understanding "private" requires abstract social-category thinking: the SAME body part is acceptable to touch in the bathroom but NOT in the living room. Context-dependent rules are among the most challenging concepts for the ASD brain, which processes best with absolute rules. The teaching must therefore be structured as absolute: "Private areas = ALWAYS covered in public. ONLY you touch them. ONLY in private places."
The Bathing Suit Rule
Parts covered by your bathing suit = PRIVATE. Visual body outline with bathing suit marked — laminated, reviewed monthly. Simple, concrete, memorable.
Correct Anatomical Names
Use accurate terms — children who know correct names are more likely to disclose inappropriate contact and more likely to be believed. Reduces vulnerability significantly.
Who Can See/Touch
ONLY the child, parents during hygiene help, and doctors WITH parent present. NO ONE ELSE. No exceptions. This is taught as an absolute rule — no grey area.
Age Progression
Ages 3–5: bathing suit rule + correct names. Ages 6–9: consent concept + public/private distinction. Ages 10+: puberty, relationship boundaries, online safety, POCSO awareness.
E-559 · Emergency Calling
E-559: Emergency Calling
The Moment
Fire. Medical emergency. A parent collapses. An intruder. The child is the ONLY person who can get help. Can they call? Do they know how? Do they know WHEN? Emergency calling is one of the hardest skills to teach in ASD because it demands situational judgment, communication under maximum stress, and device operation — simultaneously, in a moment of crisis, often with reduced adult support.
Level I Evidence — Emergency skills training with intensive, varied practice. NCAEP 2020

E-559: Emergency Calling — The Four-Step Challenge
Each step is independently compromised in ASD. Under stress, prefrontal cortex function drops — making every step harder precisely when it matters most. Teaching must build automaticity at each stage independently before chaining them together.
For nonverbal children: SOS button on phone/watch, pre-programmed emergency text, medical alert device with GPS. The goal is GETTING HELP — the method must match the child's communication profile.

E-559: Emergency Calling — Intervention Strategy
Teach ONE Number: 112
India's unified emergency number — simplest to remember, routes to police, fire, and ambulance. Teach 112 exclusively to avoid confusion under stress.
Scripted Response
"My name is [name]. I need help. I am at [address]." Practiced until completely automatic — set to rhythm if needed. No improvisation required in the emergency moment.
Emergency Recognition Card
Visual card showing EMERGENCY situations (fire, someone hurt, someone sick on floor, stranger in house) vs. non-emergencies. "When you see THESE → call 112."
Monthly Role-Play Practice
"Mama fell down and isn't waking up — what do you do?" Practice on actual phone in airplane mode. Practice under mild anxiety, not just when calm, to simulate stress conditions.
Indian context: 112 is not yet widely known — explicitly teach it as the single emergency number. Arrange a community awareness visit to the local police station to build familiarity with police as helpers.

E-560 · Personal Information
E-560: Personal Information — The Capstone Safety Skill
The Moment
"What is your name?" "Where do you live?" "What is your parent's phone number?" If a child is lost, found by a stranger, in an emergency, or at a hospital — can they provide the information that brings them home? Personal information is the critical link between a lost or endangered child and rescue. It is the capstone of the entire E4 subdomain — and it must be automatic, not effortful.
Level I Evidence — Personal information teaching as a core safety skill. NCAEP 2020 | NAA Safety Research
E-560: Personal Information — Intervention Strategy
Five essential items. Each must be stored in long-term procedural memory (basal ganglia encoding) so they can be retrieved even when the prefrontal cortex is offline during extreme stress. Rote rehearsal — like times tables — is the teaching method of choice.
Full Name
Daily morning Q&A: "What is your name?" → Full name, immediately. Practice with multiple people asking.
Parent Phone Number
Taught as a SONG or RHYTHM — musical memory is often a strength in ASD and dramatically improves recall under stress. India's mobile-first context: parent's mobile number is the priority.
Home Address
Simplified to essential components: city + area + landmark. Full address if the child can manage it — landmark-based if not. Visual backup card always carried.
School Name
Useful for police and emergency services to triangulate location and contact additional known adults. Practice as part of the five-question daily routine.
Caregiver Name
Parent/caregiver full name — not just "Mama" or "Papa." Emergency responders need a searchable name to make contact.
Safe disclosure teaching: Share personal information with police, uniformed persons, or teachers — NOT with random strangers who approach and ask. This distinction must be explicitly taught alongside the information itself.
E-560: Your Home Protocol — Personal Information
Daily Practice (Until Automatic)
- "What is your name?" → Full name (every morning)
- "What is Mama/Papa's phone number?" → Number set to song
- "Where do you live?" → Address or area + landmark
- "What school do you go to?" → School name
- "What is Mama/Papa's name?" → Full caregiver name
Backup Systems
- ID card on child always (laminated, waterproof)
- Medical alert bracelet (₹500–2,000)
- QR code tag linking to full contact information
- Phone emergency contact screen visible without unlock
- School ID with parent's mobile number
Mastery Criteria
All 5 questions answered, with 3 different people asking, in 3 different settings, within 5 seconds per answer. Available under stress.

The E4 Safety Skills Message
Safety skills are not one lesson — they are a lifetime practice. Every technique in this subdomain must be maintained, practised, generalised, and updated as the child grows.
Layer 1: Environment
Physical barriers always come first. Lock gates. Fence pools. Guard stoves. No teaching replaces a locked door.
Layer 2: Teaching
Explicit, systematic instruction across all 10 techniques. Thousands of repetitions. Multiple people. Multiple settings.
Layer 3: Supervision
Active, close supervision at all times until mastery criteria are met and maintained across months of consistent performance.
Layer 4: Independence
Comes only with demonstrated, maintained mastery — never assumed, never rushed. Each child sets their own timeline.

All 10 Techniques — E4: Safety Skills
Each technique includes three structured cards, 9 canon therapy materials, and a full 40-card deep-dive page. Use the links below to explore any technique in depth.
Code | Technique | URL | Section | |
E-551 | Danger Awareness | Environmental | ||
E-552 | Stop and Wait | Environmental | ||
E-553 | Street Safety | Environmental | ||
E-554 | Water Safety | Environmental | ||
E-555 | Fire Safety | Environmental | ||
E-556 | What to Do If Lost | Personal | ||
E-557 | Body Safety | Personal | ||
E-558 | Private Parts Education | Personal | ||
E-559 | Emergency Calling | Personal | ||
E-560 | Personal Information | Personal |
9 Canon Therapy Materials — All E4 Techniques
Every technique in Subdomain E4 is supported by the same nine evidence-based therapy materials. These are not optional supplements — they are the scaffolding that makes explicit safety teaching possible for children with ASD across communication profiles and learning styles.

Sequences safety routines into predictable, visual steps the child can follow independently.

Narrative-based teaching that makes abstract safety rules concrete and personally relevant.

Enables nonverbal and minimally verbal children to communicate in safety situations.
Visual demonstration of correct safety responses — viewed, paused, discussed, and practiced.
Structures safety practice with clear, motivating contingency: practice FIRST, reward THEN.
Sustains motivation through thousands of necessary safety repetitions with consistent reinforcement.
Domain E: Daily Living — Complete Subdomain Map
Safety Skills (E4) is the fourth and final subdomain in Domain E. Together, all four subdomains cover 110 evidence-based techniques across 120 structured cards — the most comprehensive daily living skills resource for children with ASD in the Indian context.
40
E1: Feeding & Eating
E-451 to E-490 · Complete ✅
30
E2: Toileting
E-491 to E-520 · Complete ✅
30
E3: Dressing & Grooming
E-521 to E-550 · Complete ✅
10
E4: Safety Skills
E-551 to E-560 · Complete ✅
Total Domain E: 110 techniques · 120 structured cards · E-451 to E-560 · ✅ Complete

Who Leads Safety Skills Intervention?
Safety skills teaching is a multi-disciplinary effort. No single professional owns the full scope — effective safety outcomes require coordinated input across disciplines, with families as the primary implementers in daily life.
ABA Therapist (BCBA)
Leads behavioral safety skills programming — task analysis, repetition protocols, generalization planning, data-driven mastery criteria across all 10 techniques.
Psychologist / Special Educator
Addresses cognitive and emotional components — fear calibration, risk comprehension, social safety concepts, body safety curriculum, and personal information recall.
Occupational Therapist
Supports sensory processing, interoceptive awareness, fine motor device operation (phone use), and environmental modification recommendations.
SLP / AAC Specialist
Develops communication supports for safety vocabulary, emergency scripts, AAC emergency buttons, and disclosure language for nonverbal children.
Safety Skills Are Never "Done"
Unlike many therapy goals, safety is not a milestone to check off — it is a practice to maintain across the child's entire life. As the child grows, their access to the world expands: new environments, new technologies, new social contexts, and new risks emerge at every developmental stage.
Ages 2–4
Danger vocabulary, environmental barriers, STOP reflex, basic water rules, body ownership concept.
Ages 5–7
Street safety protocol, "I'm lost" response, fire safety, NO-GO-TELL, bathing suit rule, basic personal information.
Ages 8–11
Emergency calling, full personal information recall, consent concepts, public/private behavior, community independence preparation.
Ages 12+
Puberty safety, online safety, POCSO awareness, relationship boundaries, increasing independence with maintained safety skills monitoring.
Every skill must be revisited, updated, and generalized as the child's world expands. The three-layer system — environment → teaching → supervision — adjusts at each stage, but never disappears entirely.
Preview of safety skills Therapy Material
Below is a visual preview of safety skills therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!
Start With Pinnacle Blooms Network®
Subdomain E4 Safety Skills is part of the most comprehensive evidence-based intervention resource for children with autism in the Indian context. With 21M+ therapy sessions and a full GPT-OS® clinical intelligence system, Pinnacle Blooms supports families, therapists, and program leads with the tools they need to save lives — one practiced repetition at a time.
For Parents
Step-by-step home protocols, daily practice guides, and material links for every technique. Start with E-551 Danger Awareness.
For Therapists
Evidence-based technique cards with neuroscience foundations, mastery criteria, and 9 therapy materials per technique. GPT-OS® clinical support available.
For Program Leads
Population-level safety curriculum across 10 techniques, 30 structured cards, and full domain architecture. Integrate into existing therapy programs.
📋Domain E: Daily Living · ← E3: Dressing & Grooming · Subdomain E4: Safety Skills | Pinnacle Blooms Network® | 9100 181 181