

System | What It Does | What Happens When Delayed | |
Postural Control | Trunk & core stability that frees the arms | Child slumps, uses arms for balance instead of feeding | |
Shoulder Stability | Proximal platform for distal hand precision | Arm fatigue, difficulty lifting utensil to mouth | |
Fine Motor Grasp | Grip patterns on utensil handles | Utensil slips, drops, or cannot be held at all | |
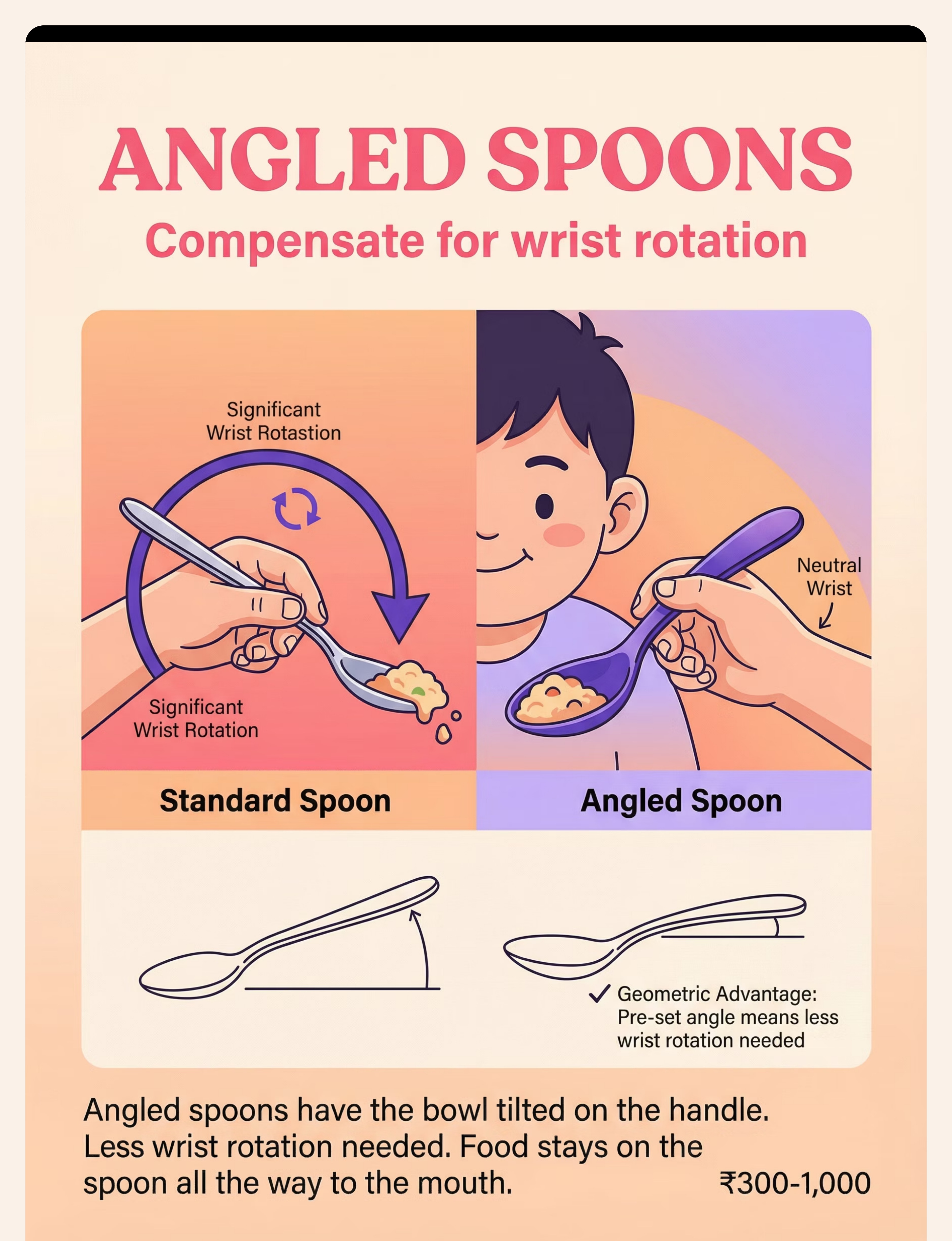
Wrist Rotation | Angles spoon to scoop and deliver | Food falls off before reaching mouth | |
Motor Planning | Sequences the scoop → lift → transport → deliver chain | Can do each step separately but cannot combine them | |
Hand-Eye Coordination | Guides utensil accurately to mouth | Misses, overshoots, inaccurate food delivery | |
Oral Motor Readiness | Receives food cleanly from the utensil | Struggles to clear food from spoon once delivered |
"This is not stubbornness. This is motor architecture. When any link breaks, the whole chain fails — and adapted tools rebuild the chain, one link at a time." — Pinnacle Blooms Occupational Therapy Consortium

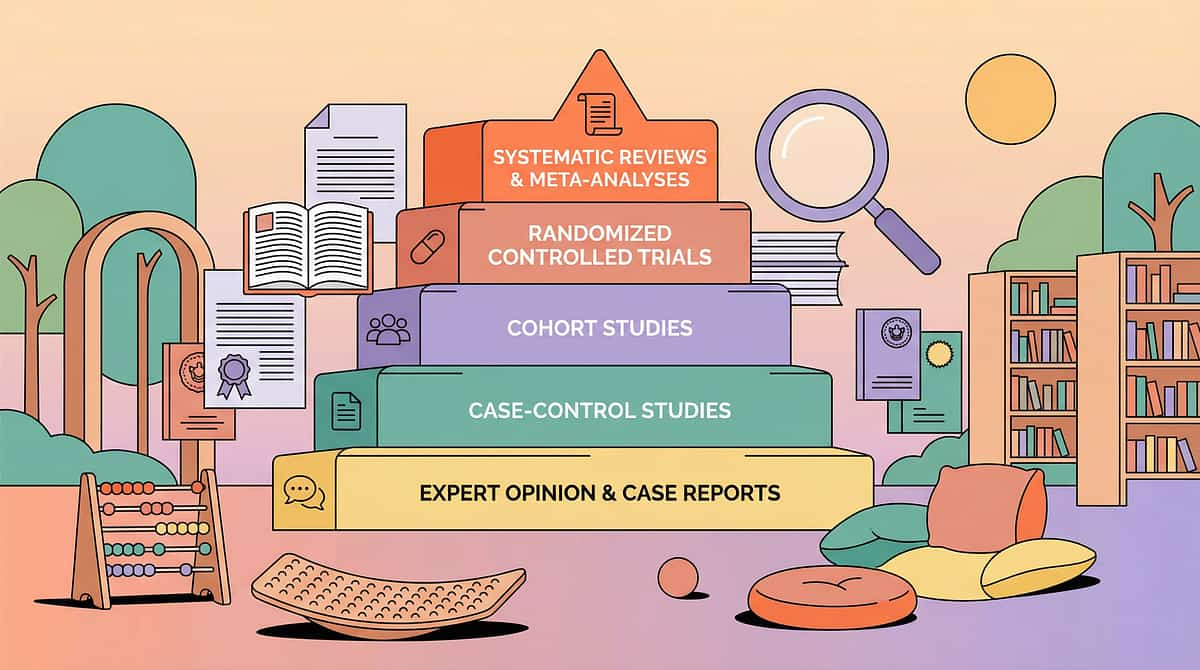
Source | Finding | |
AOTA Practice Guidelines | Adaptive equipment for self-feeding is Tier 1 OT intervention for pediatric ADL deficits | |
PRISMA Review (Children, 2024) PMC11506176 | Structured home-based interventions show significant outcomes across ASD and developmental delay populations | |
Pinnacle Blooms GPT-OS® | 97%+ measured improvement across ADL readiness indexes in 20M+ sessions | |
Padmanabha et al. (2019) | Home-based OT interventions demonstrated significant outcomes in Indian pediatric population | |
WHO NCF (2018) | Early ADL intervention during sensitive developmental windows produces compounding benefits |


"Self-feeding is not a mealtime problem. It is an independence, dignity, and neurodevelopmental milestone. The Pinnacle Blooms Consortium brings 5 disciplines to every feeding case — because the brain doesn't organize by therapy type."

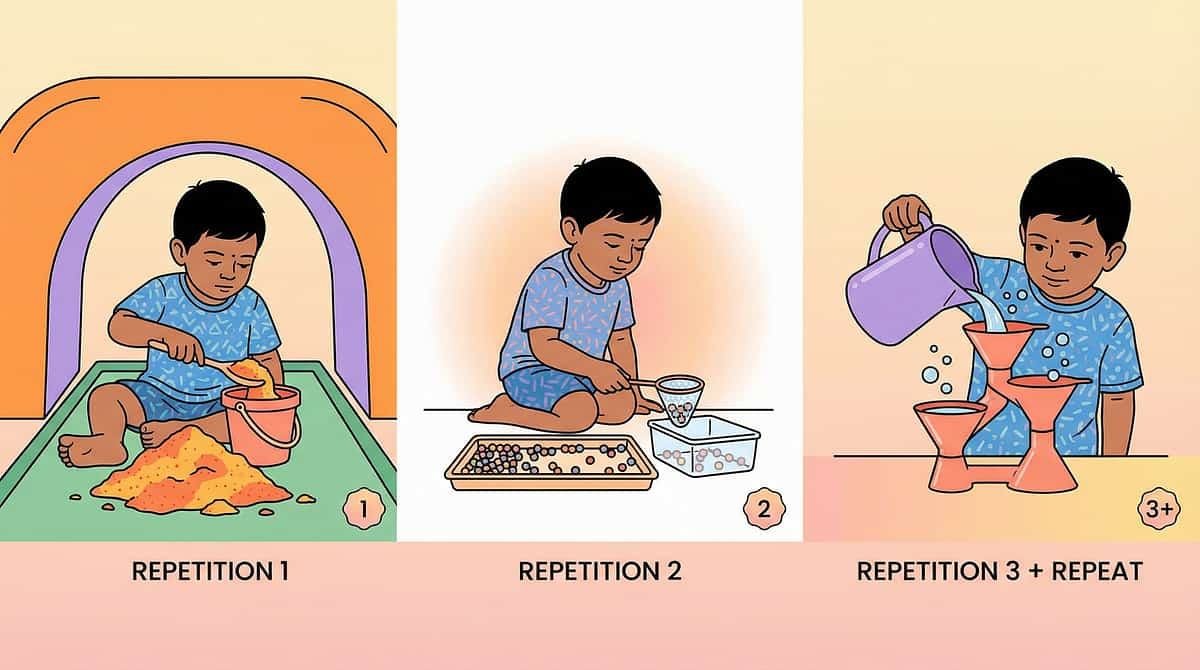
Precision targeting across 3 levels.
Each of the 9 materials targets specific points in the self-feeding chain. Progress moves through three distinct layers — primary indicators emerge first, secondary skills consolidate over weeks, and tertiary outcomes define long-term independence. Primary — What You'll See First (Weeks 1–4) Child holds spoon without dropping it for more than 5 seconds Food stays on utensil for at least 50% of transport Child initiates bringing food toward mouth independently Secondary — Weeks 3–8 Scooping success rate increases above 3 attempts per meal Bilateral coordination improves — dish steadied while scooping Child resists being fed, preferring independence PMC10955541 (Meta-analysis, World J Clin Cases, 2024) | AOTA Practice Guidelines, Feeding and Eating | GPT-OS® Self-Feeding Readiness Index







Material | Buy | DIY Alternative (Cost ₹0–80) | |
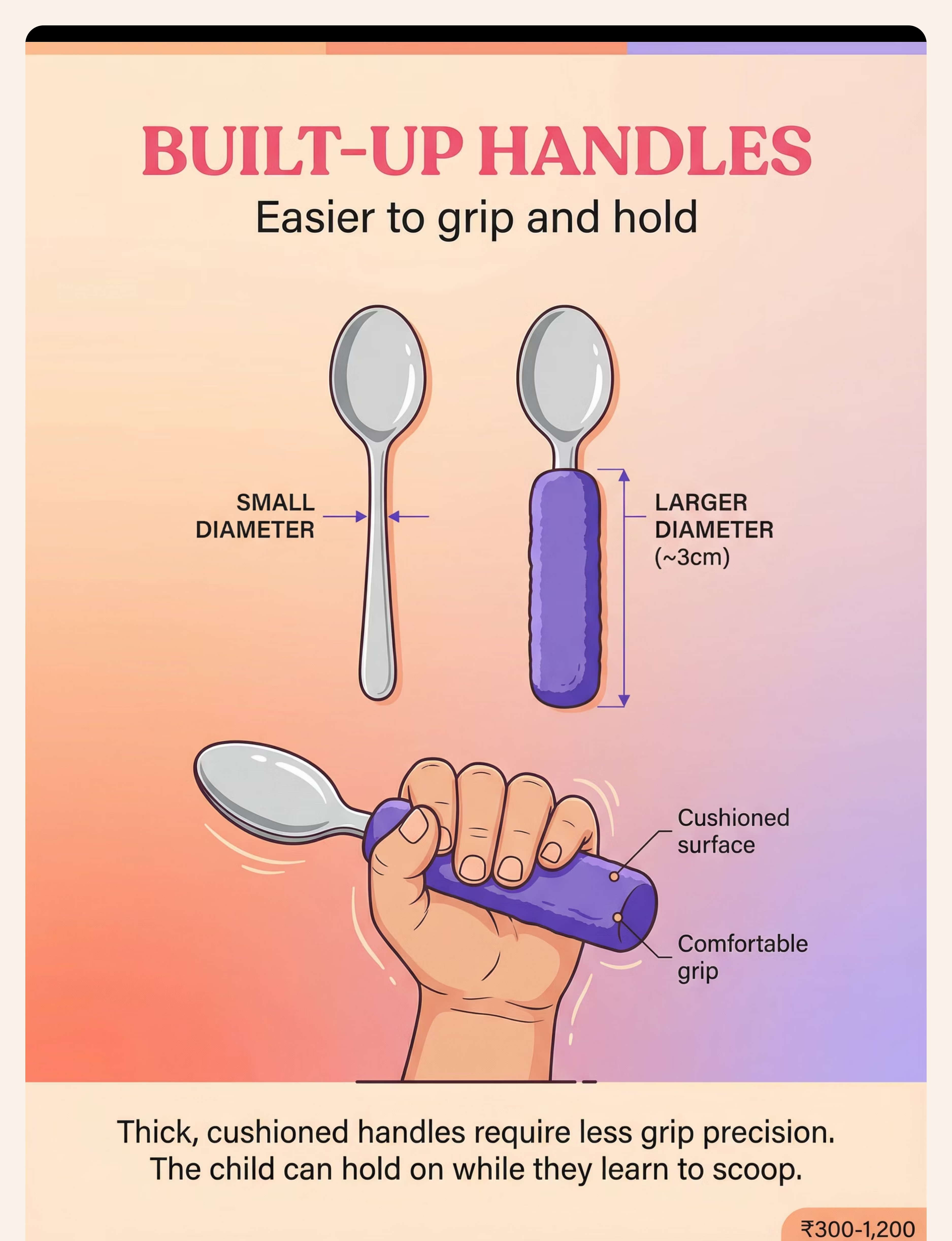
Built-Up Handles | ₹300–1,200 | Wrap handle with foam pipe insulation or yoga mat strips (food-safe tape). Target ~3cm diameter. | |
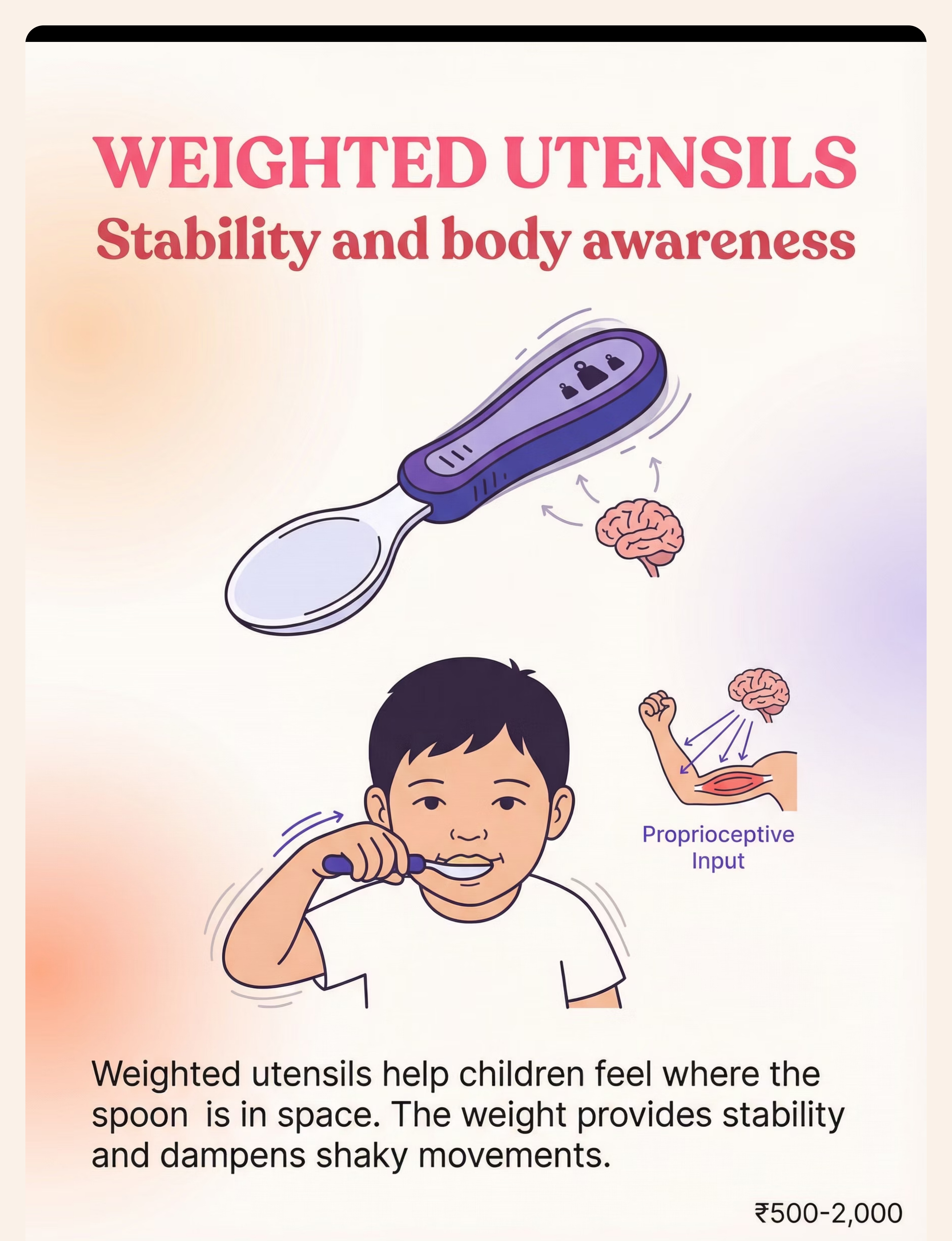
Weighted Utensils | ₹500–2,000 | Attach metal washers to standard spoon handle using rubber bands or moldable putty. Weight in handle only. | |
Angled Spoons | ₹300–1,000 | Bend a sturdy metal spoon to required angle with pliers (test for safety). Rubber grip tape on handle. | |
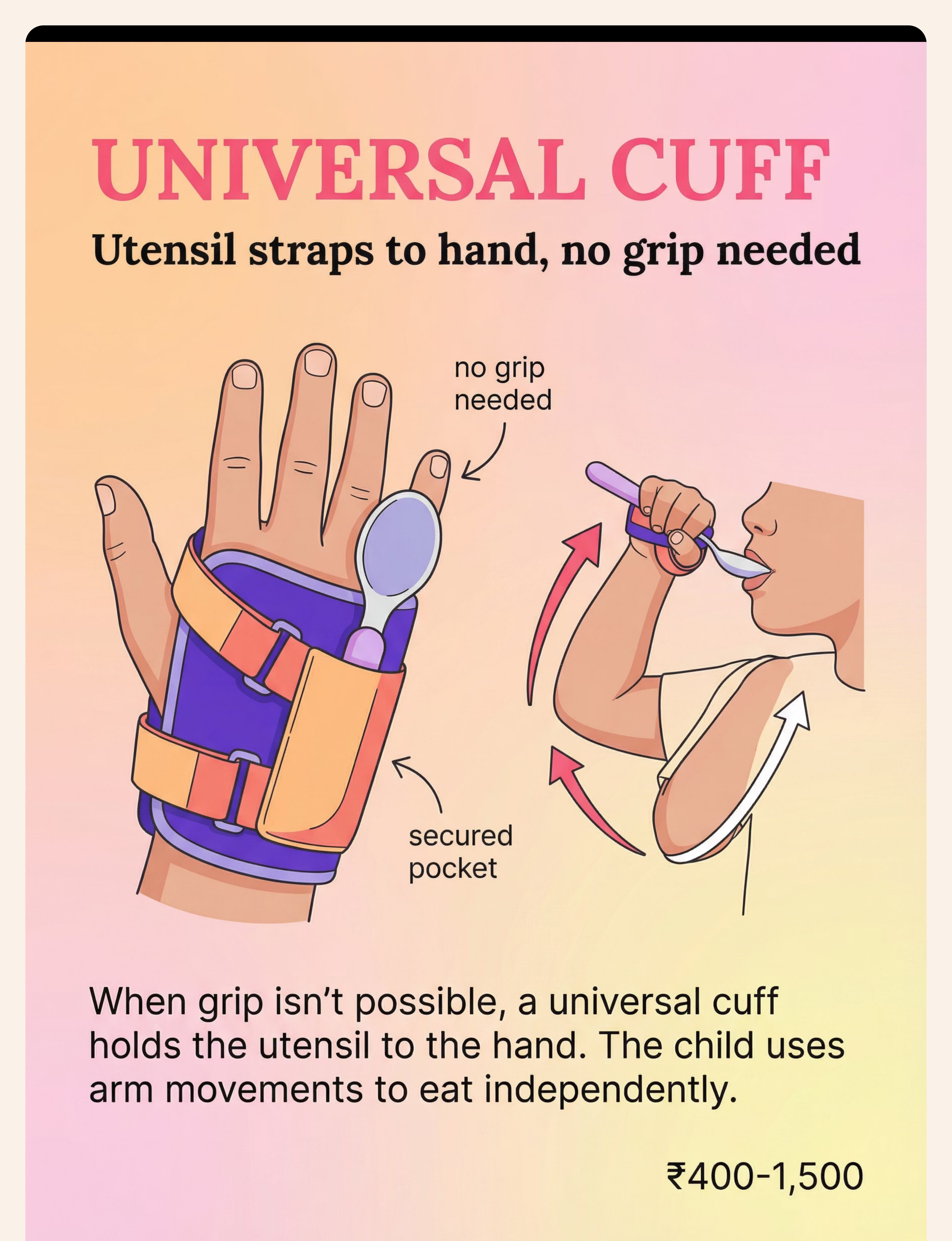
Universal Cuff | ₹400–1,500 | Velcro strap through a loop — create pocket from thick elastic band secured around palm. Thread spoon handle through. | |
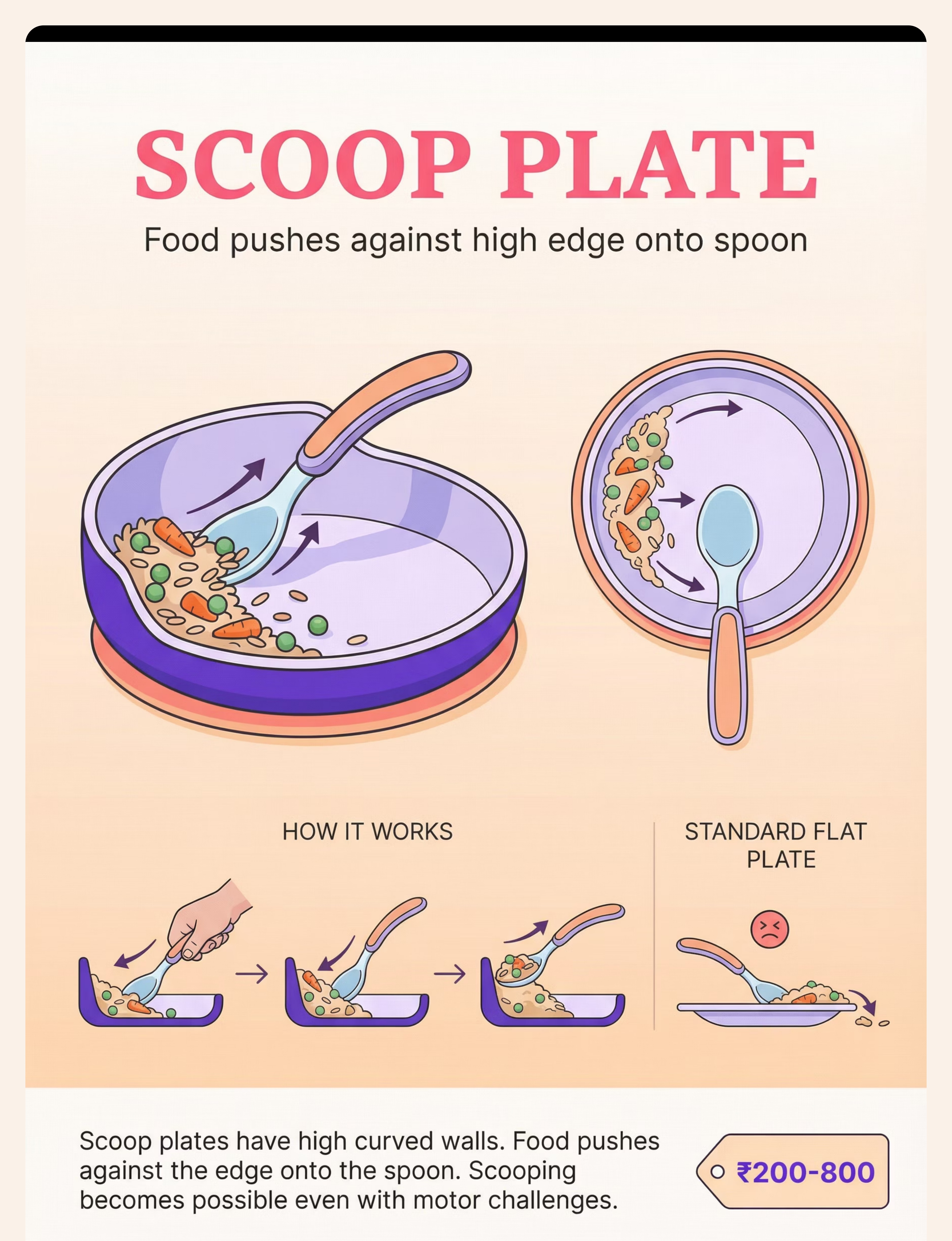
Scoop Plate | ₹200–800 | Use any bowl with sloped sides. Or attach folded cardboard guard to flat plate edge. | |
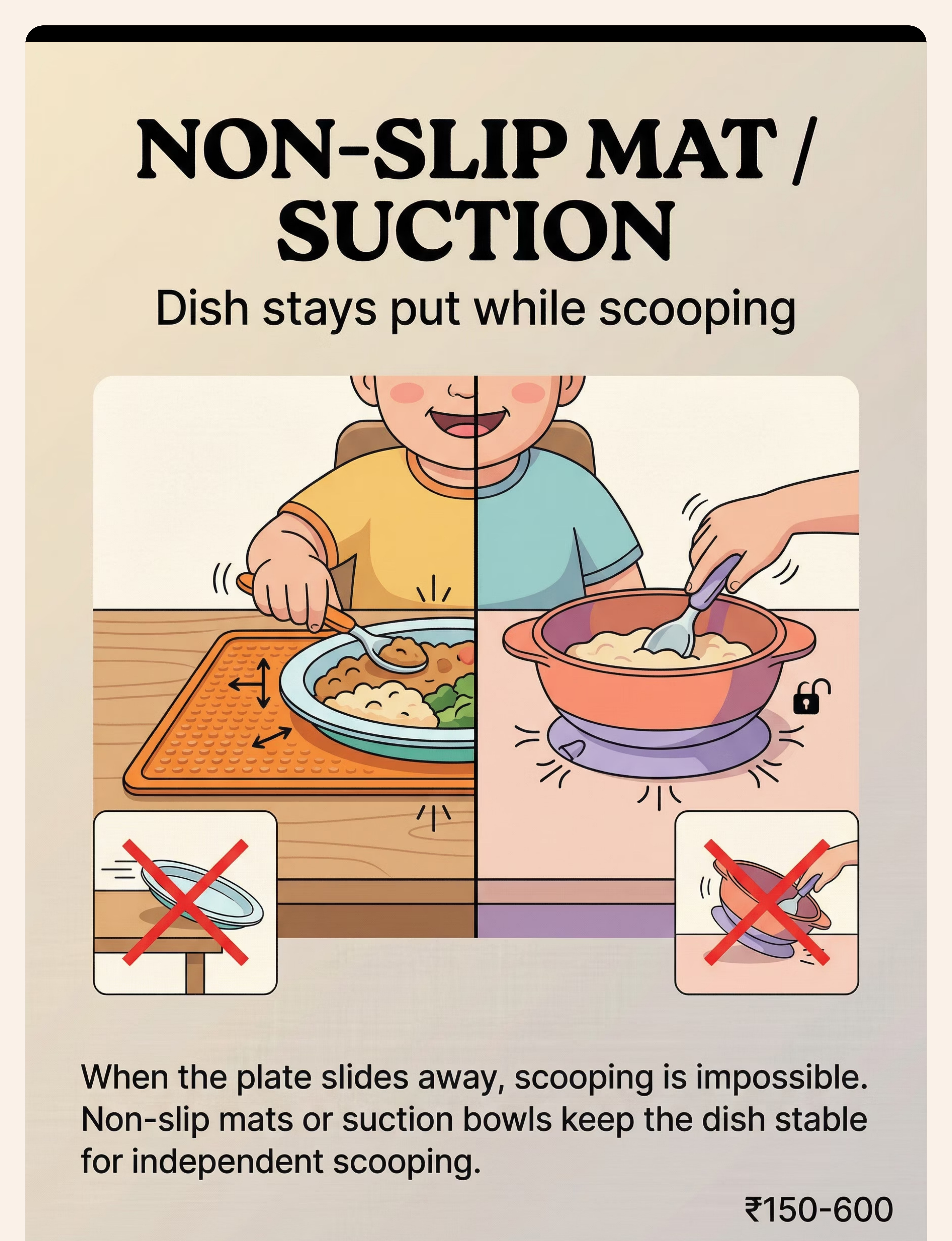
Non-Slip Mat | ₹150–600 | Rubber shelf liner, silicone oven mitt flattened, or wet cloth under plate. | |
Finger Food Feeders | ₹150–500 | Secure soft food inside clean muslin cloth tied at neck for baby. Straw inserted through soft food piece as gripper. | |
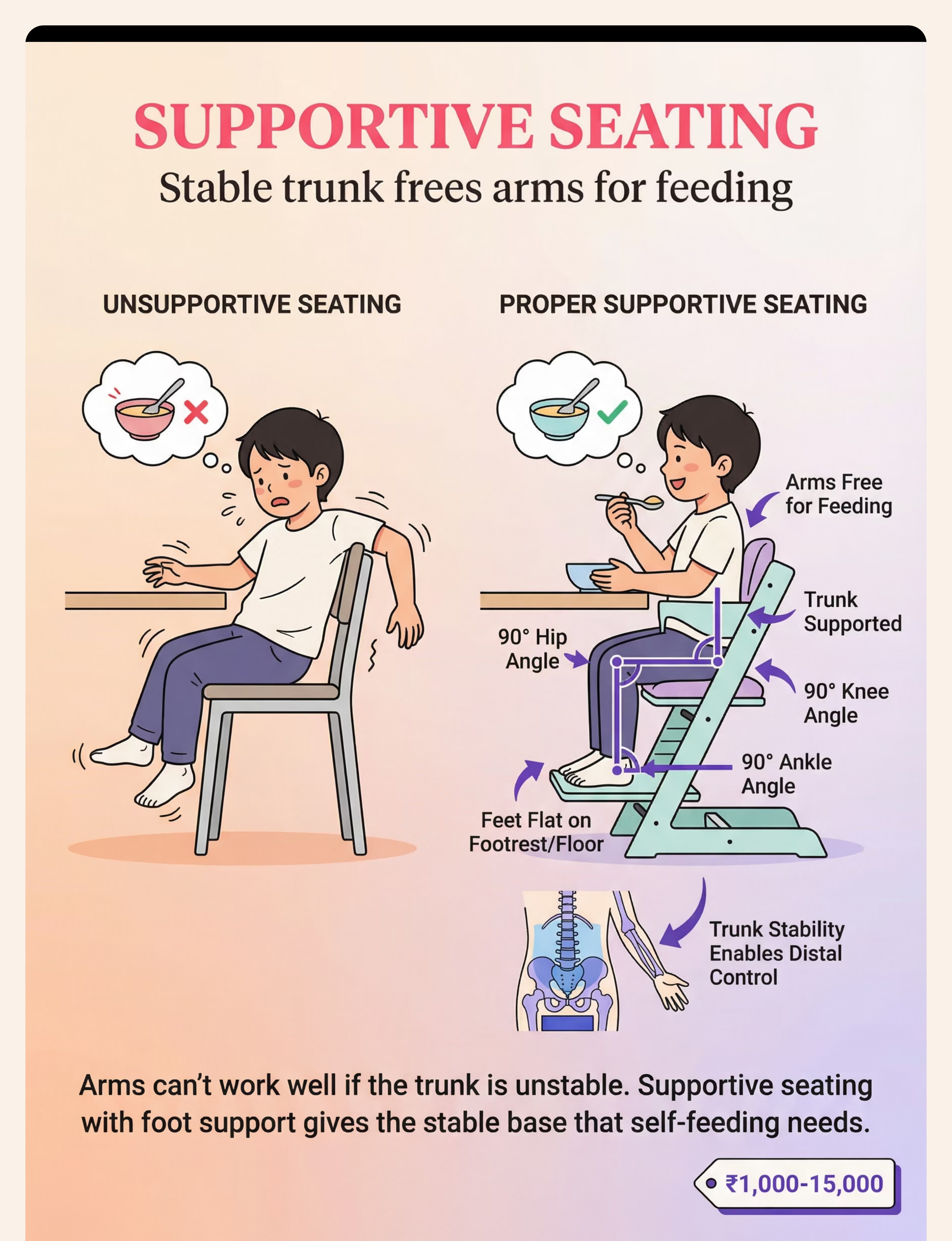
Supportive Seating | ₹1,000–15,000 | Rolled towels for lateral trunk support + stool/books as footrest + phone book on chair to raise height. 90-90-90 rule. | |
Pre-Loaded Practice | ₹200–800 | Any spoon holder (clay dough block with spoon rested in it, adult-loaded). Child practices transport only. |

- Child has active vomiting, nausea, or is unwell
- Signs of oral motor swallowing difficulty (gagging, coughing with thin liquids)
- Child is in acute distress, meltdown, or highly dysregulated
- Any DIY material has sharp edges, loose parts, or non-food-safe materials
- Suction bowl suction fails mid-meal — risk of hot food spill
- Child is fatigued — reduce session length, increase adult assistance
- Child is rejecting specific material — try alternative from DIY card
- Seating is not optimal — improvise support before proceeding
- First-time introduction — use hand-over-hand guidance for session 1
- Child is calm, alert, and has appropriate hunger (not famished, not full)
- All materials are age-appropriate, securely constructed, food-safe
- Seating provides 90-90-90 positioning with foot support
- Adult is present and engaged — not distracted by phone or other activities

Check | GO ✅ | MODIFY ⚠️ | POSTPONE 🛑 | |
Hunger level | Mild-moderate hunger | Very hungry (rushed) | Just ate, no interest | |
Regulation state | Calm, alert, present | Slightly fussy (use preferred food) | Active meltdown | |
Physical state | Well, no fever | Tired (reduce expectations) | Sick or vomiting | |
Sensory load | Normal | High (simplify setup) | Just came from intensive sensory context | |
Equipment | All items in place | One item missing (improvise) | No adaptive equipment available | |
Seating | 90-90-90, feet flat | Footrest missing (use books now) | No seat support at all | |
Your energy | Present, patient | Rushed (set 15-min timer) | Highly stressed yourself |
"No session today is not failure. A postponed session that starts right tomorrow builds more skill than a forced session that ends in tears today."

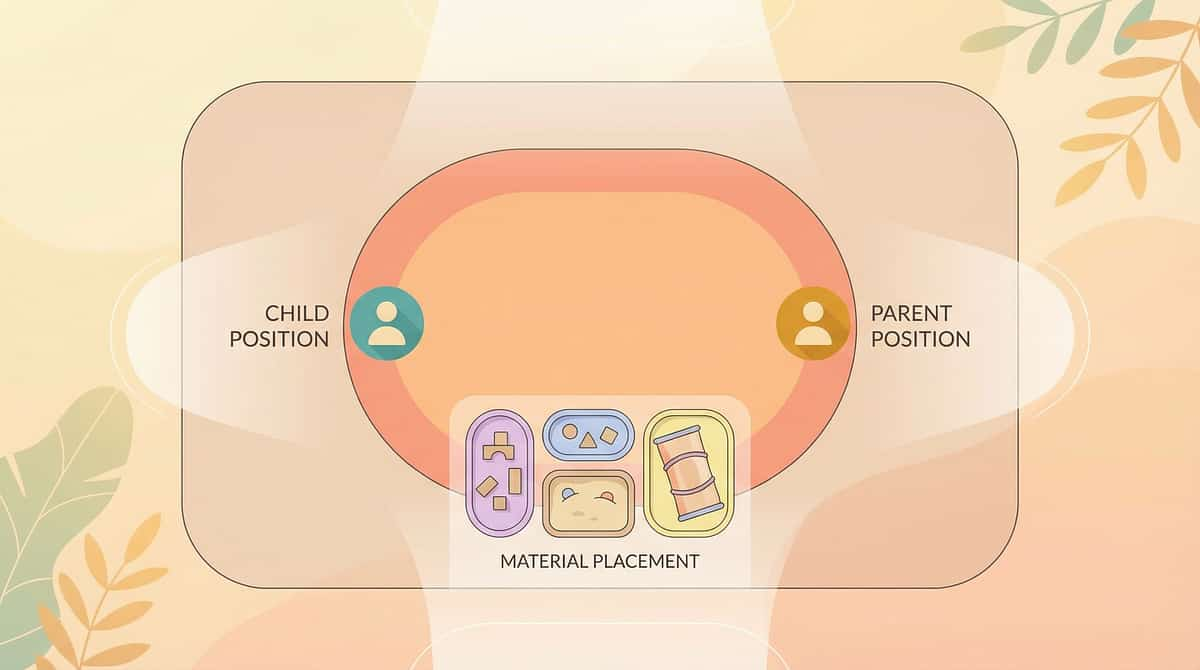
"Look what we have today! [Place adapted utensil near child's hand.] Do you want to try? Let's see what your hands can do."
- Place the adapted utensil near (not in) the child's dominant hand. Let them choose to pick it up.
- Sit slightly to the side — not looming over. Open, relaxed posture and calm voice.
- Get to child's eye level. This is a shared experience, not a lesson.
- Pre-load the first spoon and place it at the child's position. The first ask is only: "pick it up."
- Give 10–15 seconds of silence after invitation. Do NOT prompt again immediately.
- Reaches toward utensil
- Looks at food with interest
- Leans forward toward table
- Opens mouth slightly
- Child ignores → wait 15 seconds, then offer preferred food as motivation
- Child pushes away → offer finger food version instead
- Child cries → POSTPONE signal — return to readiness check

9 materials. 9 therapeutic pathways. Choose the one that matches your child's challenge.
Step 3 of 6 Built-Up Handle Utensils Action: Child grasps thick-handled spoon with full hand (cylindrical grasp). Scoop food toward curved wall of scoop plate. Lift and guide to mouth. Larger diameter = whole-hand grip, no pincer required. Ideal for: Grip weakness, low muscle tone, immature grasp patterns. Weighted Utensils Action: Child lifts weighted spoon — weight provides proprioceptive feedback, telling the brain where the hand is. Reduces tremor. Arm-to-mouth path becomes more controlled. Ideal for: Tremor, motor control issues, proprioceptive processing differences. Angled / Bent Spoons Action: Child holds spoon in neutral wrist position. The pre-set angle means the bowl faces up toward mouth without wrist rotation required. Removes the most common "food falls off" failure point. Ideal for: Wrist rotation difficulty, limited forearm supination, motor planning issues. Universal Cuff Action: Secure cuff around palm. Insert utensil into pocket. Child uses shoulder + elbow flexion to scoop and bring food to mouth. No grip required. Bypasses hand function entirely. Ideal for: Significant grip impairment, cerebral palsy, very low tone, hand differences. Scoop Plate / Plate Guard Action: Child pushes food toward the high curved wall with spoon. Food loads onto spoon bowl against the wall. Position plate so high wall faces away from child. The wall does the stabilizing. Ideal for: Scooping difficulty, motor planning, bilateral coordination challenges. Non-Slip Mat / Suction Bowl Action: Place dish on non-slip mat or use suction bowl. Child scoops without dish sliding. Full focus goes to the utensil. Eliminates one degree of freedom from the task. Ideal for: ALL children beginning self-feeding. Use universally as baseline. Finger Food Feeders / Grippers Action: Load mesh feeder with soft food. Child grasps the handle (not the food). Brings feeder to mouth. Handle is easier to grasp and less aversive than slippery food. Ideal for: Pre-utensil stage (under 18 months), sensory aversion to food touch. Supportive Seating — The Foundation Action: Set seating to 90-90-90 (hips, knees, ankles). Feet FLAT on footrest or floor. Trunk supported. Tray at elbow height. THEN introduce any other material. Never skip this. Ideal for: ALL children with self-feeding delays. Non-negotiable baseline. Pre-Loaded Spoon Practice Action: Adult loads spoon. Places it in holder at child's position. Child grasps, lifts, transports to mouth. Scooping is NOT required. Component isolation — master transport before combining with scoop. Ideal for: Motor planning difficulties, children who can grasp but lose food in transport.
Phase | Reps/Meal | Meal Time | Assistance Level | Progress Signal | |
Week 1–2 (Emerging) | 3–5 bites with help | 15–20 min | Hand-over-hand → elbow guide | Tolerates material | |
Week 3–4 (Developing) | 5–10 bites, light prompts | 15–20 min | Verbal prompts only | Initiates independently | |
Week 5–8 (Advancing) | 10–20 bites independently | 20–25 min | Standby only | Corrects own errors | |
Week 8+ (Mastery) | Full meal independently | Age-appropriate | Setup only | Generalizes to new settings |

"Celebrate the attempt, not just the success. A child who attempts 10 times and fails 10 times is working harder than a child who succeeds twice without trying. Reinforce both." — ABA Principle, adapted for home self-feeding


- Confirms the right material is being used
- Guides difficulty adjustment — harder or easier
- Demonstrates measurable progress to school, insurance, and developmental team
- Predicts trajectory to full independence
- Feeds into GPT-OS® Self-Feeding Readiness Index — your real-time progress dashboard

Profile | Likely Challenge | Best Adaptation | |
Sensory Avoider | Won't touch food, finger feeding impossible | Finger food feeder → Adapted utensil fast track | |
Sensory Seeker | Plays with food, overloads mouth | Divided scoop plate (portion control), pre-loaded practice | |
Low Proprioception | Loose grip, food drops, overshooting | Weighted utensils (primary), thick handles (secondary) | |
Low Tone (Hypotonic) | Trunk instability, arm fatigue | Seating FIRST. Lightest equipment. Frequent breaks. | |
Motor Planning (Dyspraxia) | Can do steps separately, not sequenced | Pre-loaded practice → Component training → Combination |

- Child tolerates adapted utensil being placed near hand (previously refused)
- Child attempts to pick up utensil 1–2 times per meal — any attempt counts
- Food reaches mouth at least once per meal with adapted equipment
- Mealtime meltdown frequency begins to reduce
- Child looks at food with increased interest
- Consistent independent bites across the full meal (this comes later)
- Clean eating — mess is still high at this stage and expected
- Requesting the adapted utensil themselves — this is a Week 4+ behavior
"If your child holds the adapted spoon for 3 seconds longer than last week — that is real progress. Synaptic pathways take weeks to consolidate. You are doing the biology. Keep going."
- Child reaches for adapted utensil independently before adult places it
- 3–5 successful independent bites per meal without hand-over-hand
- Child shows frustration when self-feeding fails — this is POSITIVE (means they want to do it)
- Food-to-mouth accuracy improving — less spillage per attempt
- Child starting to show preference for adapted vs. standard utensil
- Child is achieving 5+ bites independently for 3 consecutive meals
- Child is requesting the adapted utensil unprompted
- Child is attempting scooping (not just transport)

You showed up to every mealtime. You set up the adaptive equipment when it would have been easier to just feed them. You held your patience when the food went everywhere. You celebrated 3 bites like they were the Olympics. You are the therapist your child needed most.
- Coughing, gagging, or respiratory distress during meals
- Blue color around lips during eating
- Food or liquid consistently going "down the wrong way"
- Sudden regression after illness — possible swallowing change
- No improvement across any indicator after 4 weeks of consistent technique
- Child showing increased mealtime anxiety or expanding food refusal
- Significant weight loss or dehydration signs
- Grip has weakened — possible neurological change requiring evaluation
- Self-feeding delay beyond 18 months with no utensil interest
- Cannot finger-feed independently by 12 months
- All 9 adapted materials tried without any measurable progress
- Co-occurring concerns: oral hypersensitivity, food selectivity, swallowing issues






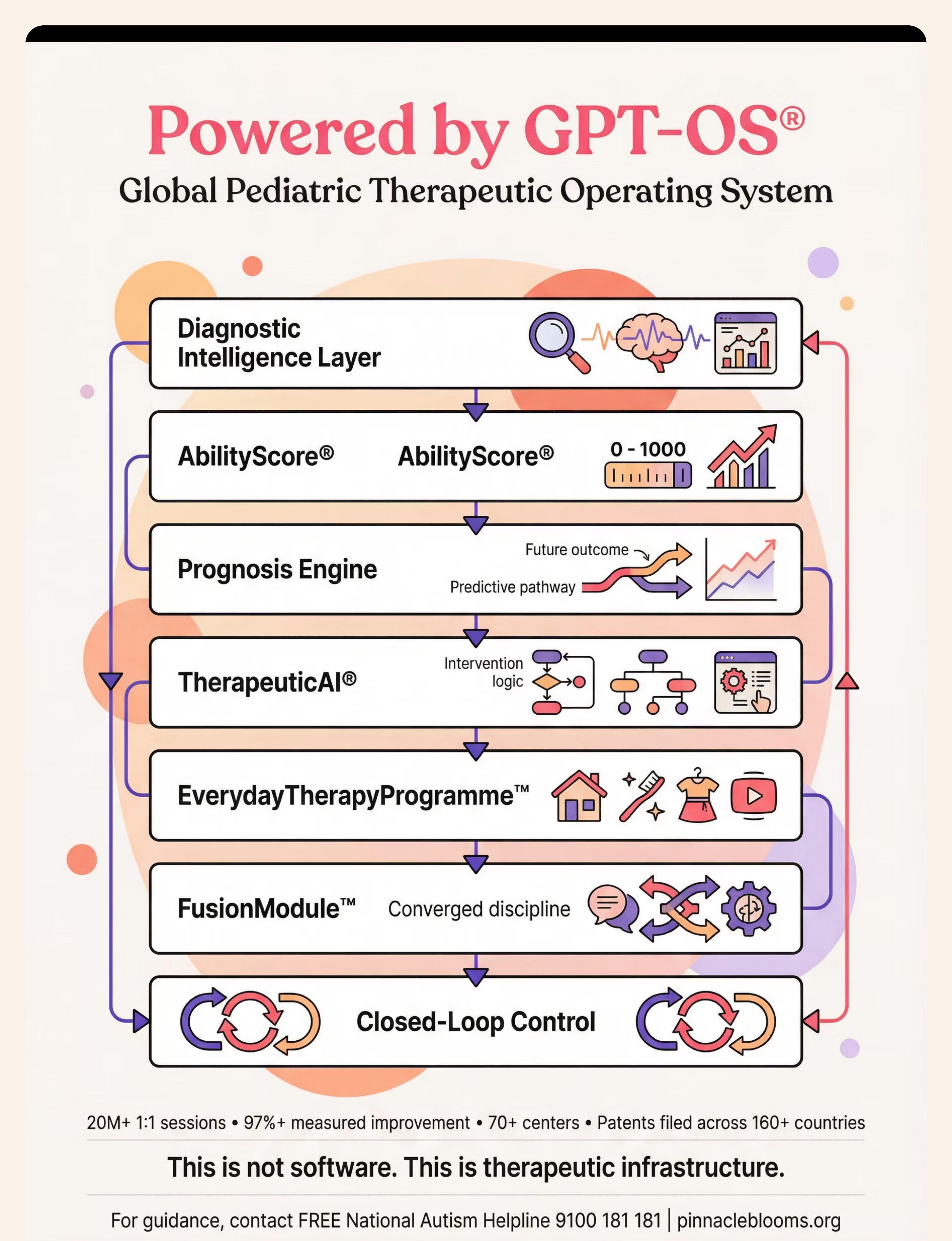
E-465 lives within the Global Pediatric Therapeutic Operating System (GPT-OS®). Here is where.
Domain E Location: E-465 → Feeding & Mealtime Independence cluster (E-451 to E-490) → within Daily Living Skills (E-451 to E-560) → GPT-OS® Domain E of 12. Domain E also contains Dressing (E-491–520), Hygiene (E-521–545), and Home ADL (E-546–560). Browse All Domain E Techniques All 70,000+ Techniques

"Consistency across caregivers multiplies impact." — WHO CCD Package. Sharing this technique with your child's teachers, grandparents, and daycare providers is not optional — it is therapeutic. Consistency across all settings is where independence generalizes.



- Always use the thick-handled spoon — not regular spoons
- Make sure the plate/bowl doesn't slide — use the mat
- Don't feed them if they're trying — even if it's slow and messy
- Praise every attempt: "Good job trying!"


Preview of 9 materials that help with self feeding Therapy Material
Below is a visual preview of 9 materials that help with self feeding therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










"Built by Mothers. Engineered as a System." — "From fear to mastery. One technique at a time." You arrived on this page carrying a challenge. You leave with 9 tools, a protocol, a community, and the clinical backing of India's largest multi-disciplinary pediatric therapy consortium. 21 million therapy services. 97%+ measured improvement. 70+ centers. 70+ countries. One mission: Every child, independent.