

"You are not failing. Your child's nervous system is speaking."




- Sensory regulation during eating (body calm enough to focus on food)
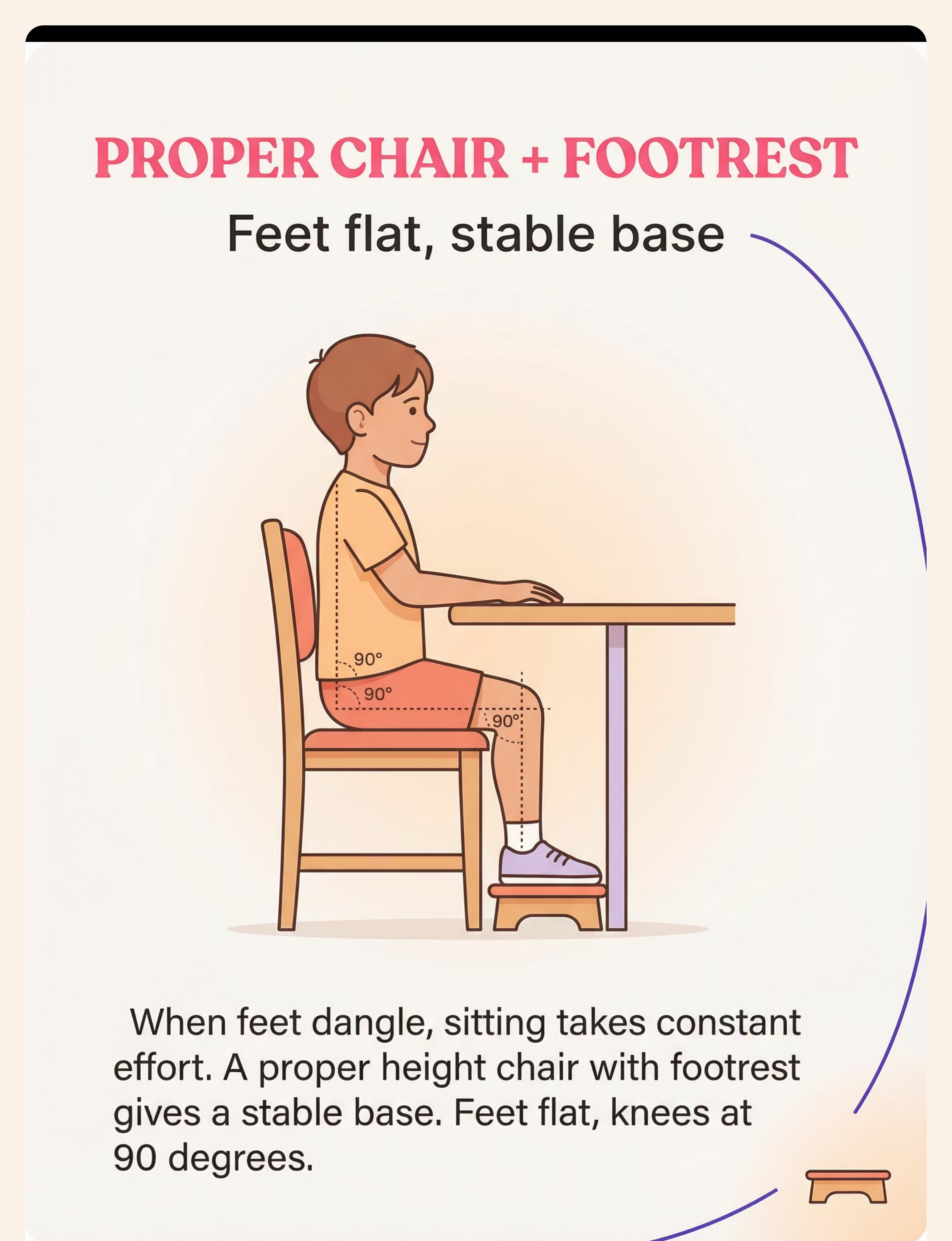
- Postural stability improvement via supported positioning
- Mealtime food intake naturally improves when sitting is supported
- Reduction in mealtime conflict and caregiver distress
- Self-regulation skills generalize across seated tasks
- Family mealtime participation and social-communicative benefits
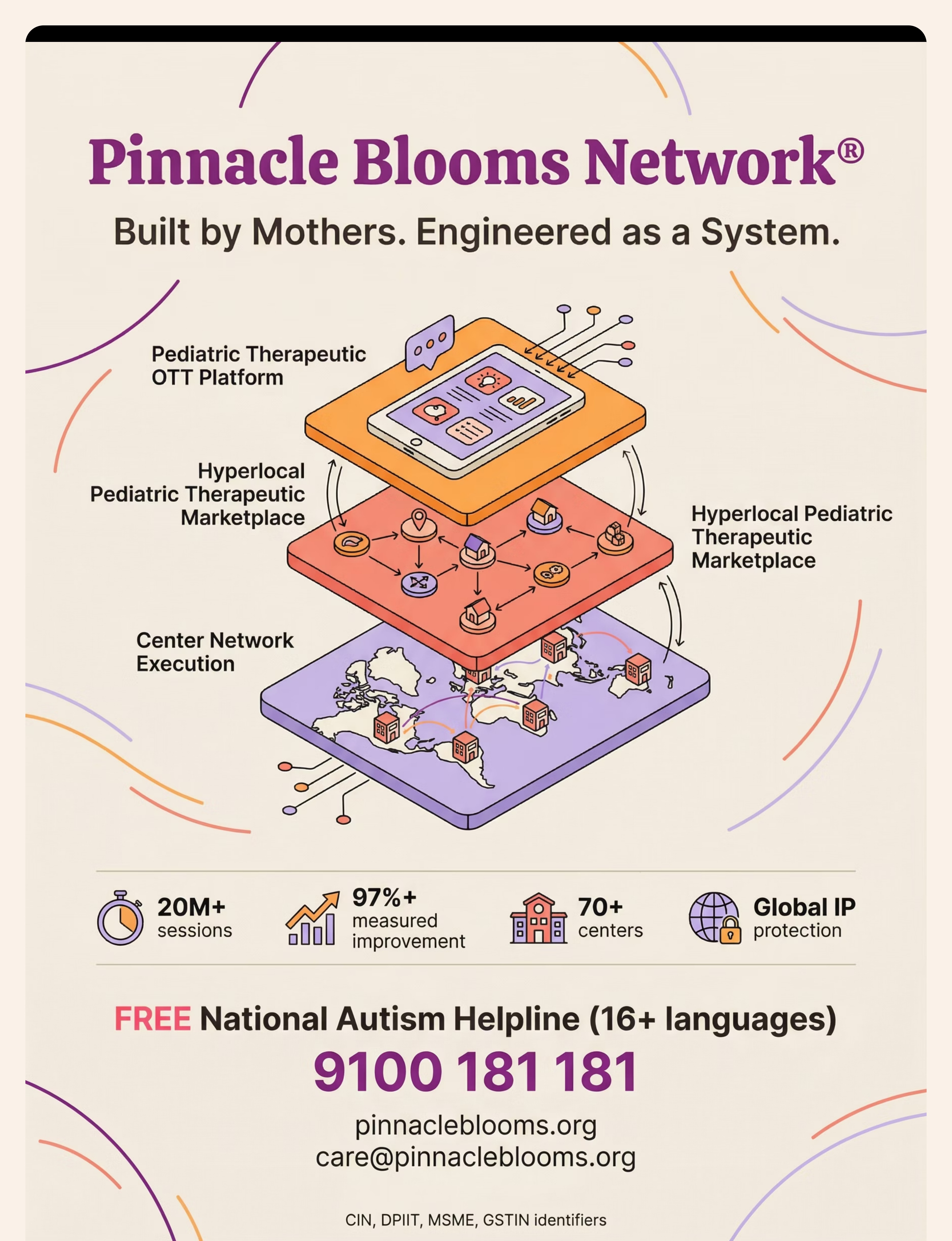
- AbilityScore® growth across Mealtime Independence + Postural Control Indexes
- Foundation for independent eating, table manners, and restaurant readiness
Indicator | Early Progress | Mastery | |
Duration in seat | +30 sec/week | Full meal consistently | |
Position changes/meal | Reducing weekly | Within normal range | |
Adult redirections | Decreasing | Occasional reminder only | |
Independent meal completion | Partial with breaks | Complete with minimal support |

9 Materials. One for Every Root Cause.
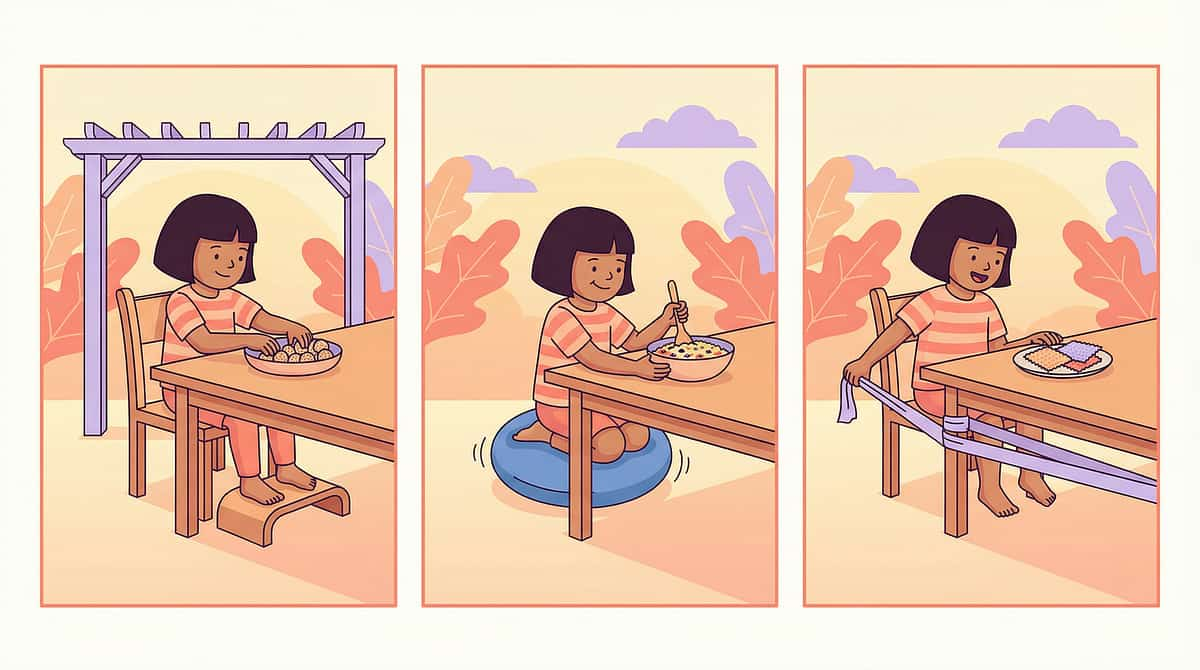
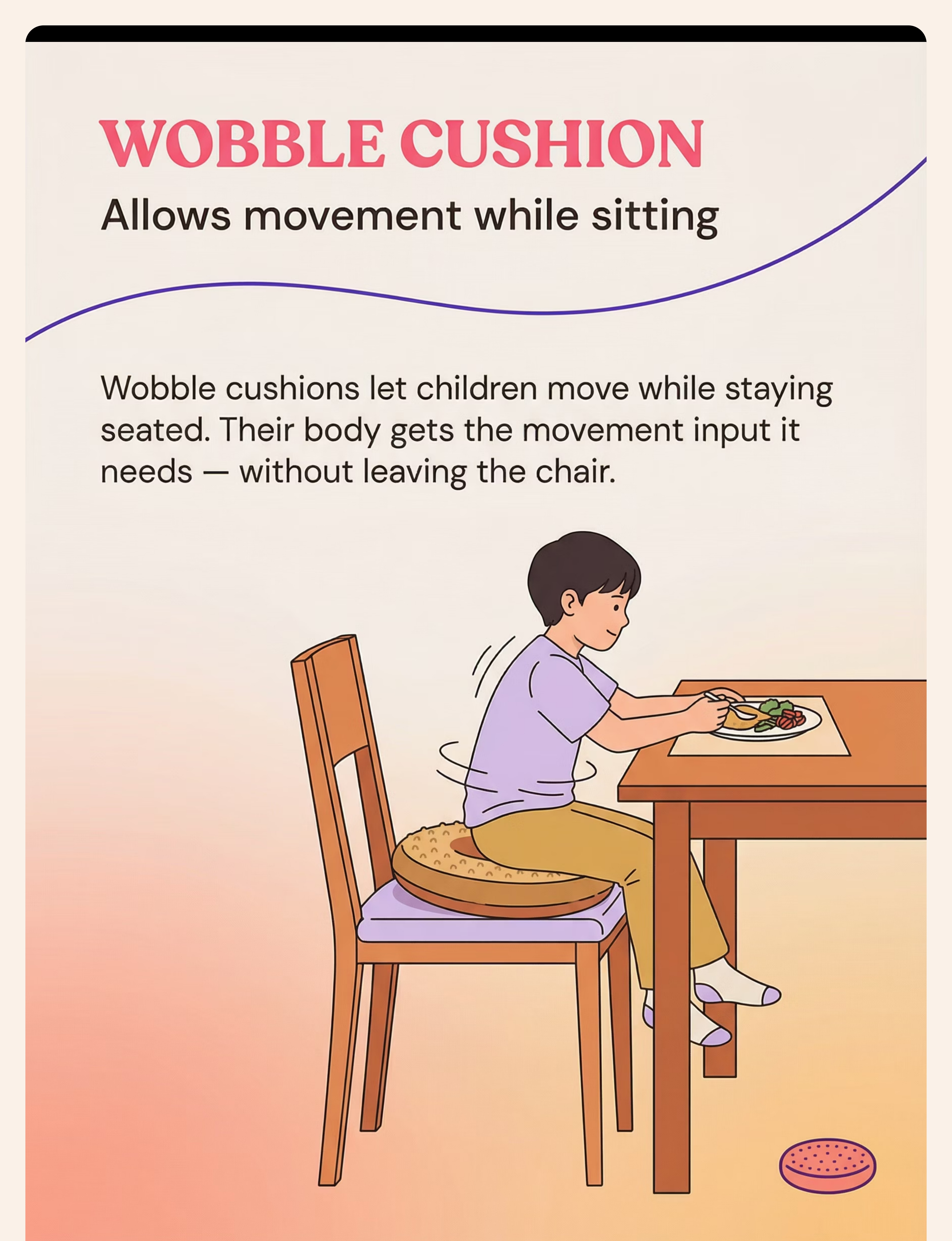
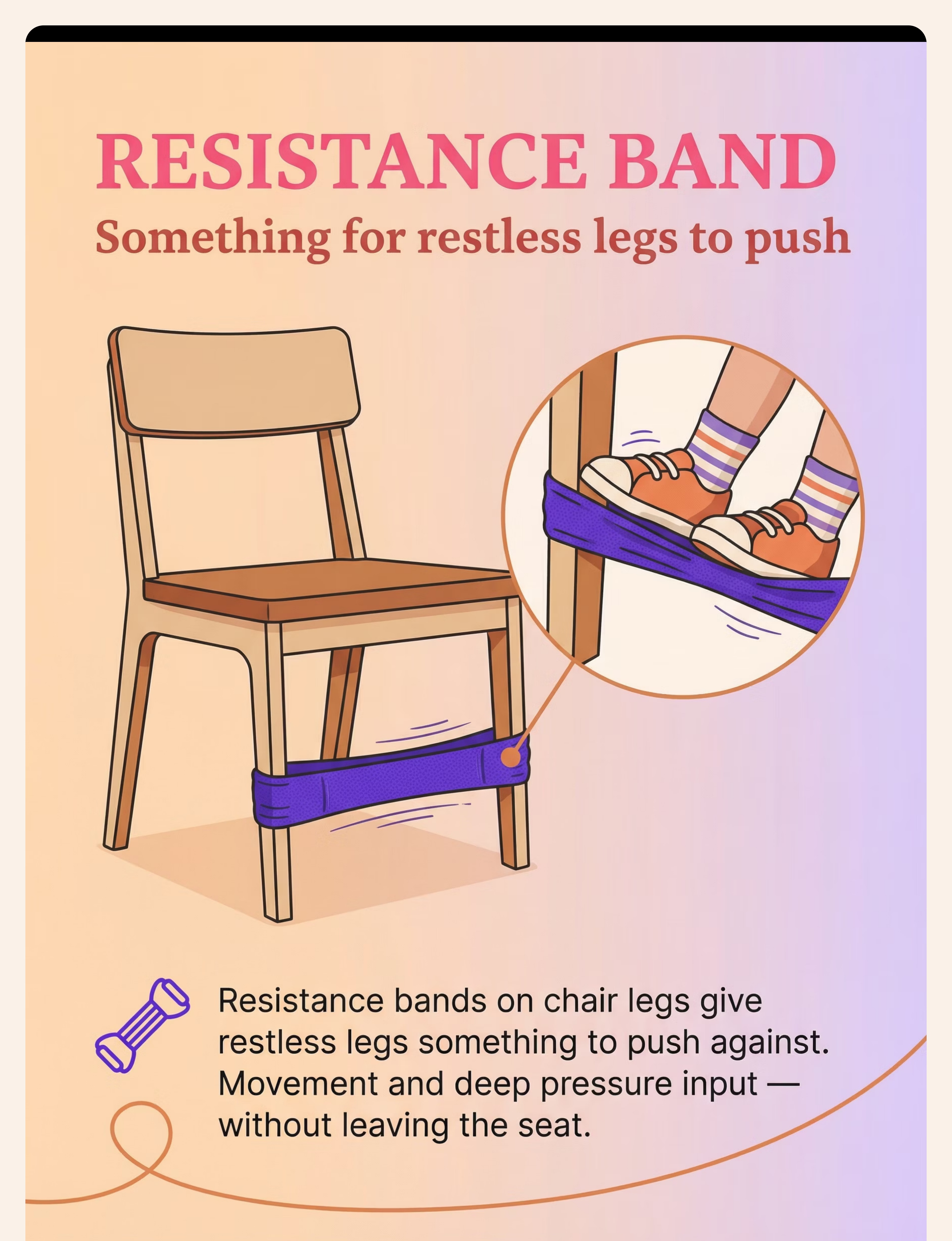
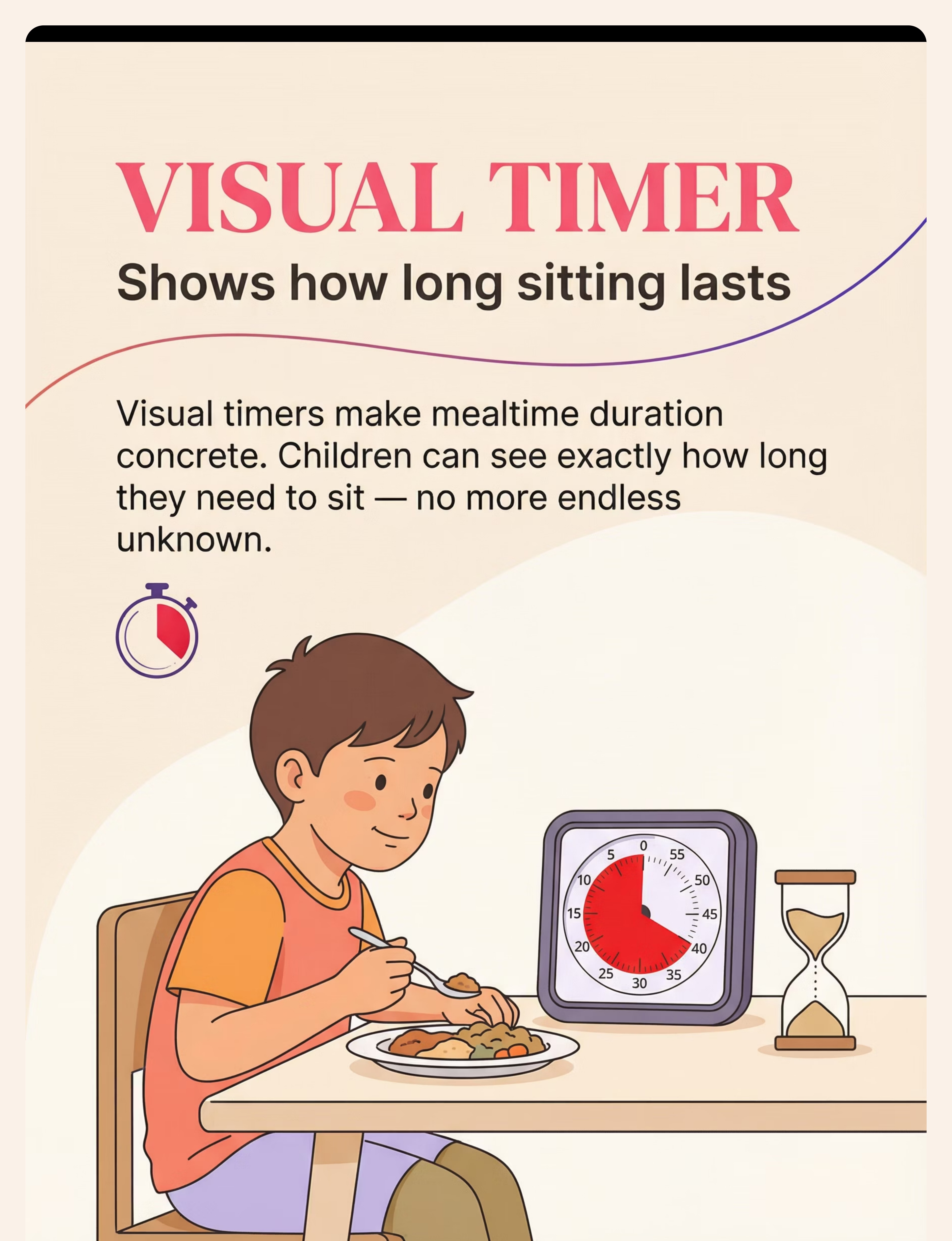
Use the right material for your child's specific profile. Each of the nine materials below targets a different underlying driver of mealtime sitting difficulty. You don't need all nine at once — identify your child's primary root cause and start there. 1. Proper Height Chair + Footrest 🪑 The most impactful single change. Feet flat. Knees at 90°. Hips at 90°. ₹500–5,000 2. Wobble Cushion ⭕ Allows micro-movement while seated. Meets sensory needs without leaving the chair. ₹300–1,200 3. Resistance Band on Chair Legs 🔵 Gives restless legs something to push. Deep pressure input without leaving the seat. ₹100–400 4. Visual Timer ⏱️ Makes mealtime duration concrete and visible. Transforms "forever" into "until this." ₹200–1,000 5. Weighted Lap Pad ⚖️ Grounding deep pressure across the thighs. Calms the drive to move. Anchors in the seat. ₹500–2,000 6. Structured Movement Break System 🔄 Planned breaks — not escape. Brief movement → return to seat. Prevents dysregulation. ₹100–400 7. Pre-Meal Heavy Work 💪 Load the sensory system BEFORE sitting. 5–10 minutes of proprioceptive input = easier meal. ₹0–500 8. Visual Seating Reminder Card 🃏 Silent, constant cue. No nagging needed. The expectation is always visible at their spot. ₹50–200 9. Engaging Mealtime Conversation 💬 Bored children move. Engaged children sit. Give attention something to anchor to. ₹0 For personalized material guidance: FREE Helpline: 9100 181 181

Material | Buy It | Make It (₹0 version) | Why It Works | |
Footrest | Adjustable stool ₹500–2,000 | Sturdy cardboard box, thick book stack, wooden step | Same principle: feet flat, stable base | |
Wobble Cushion | Balance disc ₹300–1,200 | Partially deflated bicycle inner tube under chair cushion | Same micro-movement provision | |
Resistance Band | Therapy band ₹100–400 | Old trouser elastic tied between chair legs | Same proprioceptive input | |
Visual Timer | Time Timer ₹500–1,000 | Sand timer ₹50, or phone countdown with visible display | Same duration visibility | |
Weighted Lap Pad | Commercial ₹500–2,000 | Small bag of uncooked rice sewn into cloth pouch (1–2 kg) | Same deep pressure mechanism | |
Movement Break Timer | Timer ₹100 | Verbal countdown + visual schedule drawn on paper | Same structured predictability | |
Pre-Meal Heavy Work | None needed | Carrying grocery bags, pushing laundry basket, wall push-ups | Same proprioceptive loading | |
Visual Reminder Card | Printed card ₹50 | Hand-drawn picture card, laminated with packing tape | Same visual cueing function | |
Mealtime Engagement | None needed | Family conversation starters prepared in advance | Same attention anchoring |

- Child is ill, feverish, or showing signs of respiratory distress
- Weighted materials on any child with cardiac, respiratory, or circulatory conditions without OT sign-off
- Resistance bands showing cracks, tears, or degradation — replace immediately
- Footrest that rocks or slides — must be completely stable before use
- Forcing a child to sit when in full meltdown — address dysregulation first
- Any seating modification the child cannot exit independently in an emergency
- First introduction of weighted lap pad: start with 10-minute maximum, observe response
- Wobble cushion for very poor trunk stability: start partially inflated
- Pre-meal heavy work: end 2–3 minutes before meal to allow nervous system to settle
- Movement breaks: keep bounded (30–60 sec) — open-ended breaks are hard to end
- Visual timer increasing anxiety: pause use, reassess framing
- Child is fed, rested, and not in post-meltdown recovery
- Materials are tested and stable before child sits
- Parent/caregiver is calm and ready to follow the structure
- Space is prepared with a backup plan ready if child cannot complete

- Lighting: Warm, not harsh overhead fluorescent
- Sound: Background music optional (calming, no lyrics)
- Temperature: Comfortable, not hot
- Smells: Avoid strong fragrances during meals for sensory-sensitive children
- Chair height checked — hips, knees, ankles at 90° with footrest
- Wobble cushion placed and inflation level appropriate
- Resistance band tied securely at foot level
- Visual timer set to starting duration (child's current tolerance)
- Weighted lap pad within reach
- Visual reminder card at child's spot
- Plate ready before child sits (reduce waiting time)
- Distractions removed: TV off, screens away
- Pre-meal heavy work completed 2–5 minutes ago
- Parent emotional state: calm, patient, ready for the plan — not the battle

Indicator | Green ✅ | Amber ⚠️ | Red 🔴 | |
Child's mood | Calm/neutral/playful | Slightly irritable | Post-meltdown / upset | |
Hunger level | Not starving (snack 20 min ago if needed) | Mildly hungry | Extremely hungry | |
Fatigue | Alert and present | Slightly tired | Exhausted / overtired | |
Recent meltdown | None in past 2 hours | 1–2 hours ago | Less than 1 hour ago | |
Pre-meal heavy work | Completed 2–5 min ago | Skipped today | Never been introduced | |
Space ready | All Card 12 setup complete | Most items ready | Not set up |

- Warm, relaxed tone — not tense or braced for battle
- Crouch to child's eye level for the invitation
- Move to your own seat calmly once child is positioned
- No hovering directly over the child


Questions? FREE Helpline: 9100 181 181

Phase | Sitting Goal | Movement Breaks | Sessions/Day | Week Target | |
Week 1–2 | Current tolerance + 1 min | As needed | 3 (all meals) | Consistent execution | |
Week 3–4 | +2–3 additional min | Reduce by 1 break | 3 | Stable tolerance at new duration | |
Week 5–8 | Building toward age-appropriate | Only if needed | 3 | Self-regulation emerging | |
Week 9+ | Fade supports one at a time | Planned, not reactive | 3 | Independence building |

Reinforce & Celebrate
STEP 5 of 6 Timing: Within 3 seconds of desired behavior. Every time. "I noticed you kept your feet on the footrest that whole time. That's your body doing the work!" "The timer finished and you were still in your chair — that's a huge deal!" "Yesterday you managed 3 minutes. Today it was 4. That's your brain building." 🌟 Verbal Specific, enthusiastic, immediate praise — name exactly what they did right 🎫 Token Sticker on chart → earns preferred activity or item after the meal 🎮 Activity 5 minutes of preferred activity post-meal as earned reinforcer DO NOT: Withhold meal as punishment for not sitting (creates food anxiety) · Only reward perfect sitting (shape behavior gradually) · Praise so effusively that it feels artificial

- Gentle joint compression on shoulders
- "High-fives" (provides proprioceptive input)
- Deep breath "blowing out candles"
- Move to a preferred sensory activity
AbilityScore® Assessment: pinnacleblooms.org/abilityscore

Easier Version (start here if struggling) | Standard | Harder Version (when mastering) | |
3-minute timer goal | Age-appropriate duration | Full meal without timer | |
1-2 materials, fading others | 3-4 materials | All materials deployed simultaneously | |
Meal served in 2-minute portions | Standard plate | Full plate at once | |
Parent at table entire time | Parent nearby | Child eating with family independently |

- Child is tolerating the footrest without removing it (even if they fidget)
- Timer is visible and child glances at it (awareness, not yet compliance)
- Movement breaks are happening as planned, not as escape
- Adult redirect count starting to reduce from Day 1 baseline
- Pre-meal heavy work routine is established (child anticipates it)
- One material (even just footrest) is showing clear positive effect
- Full meal sitting duration is not achieved yet
- Child is still squirming, just slightly less
- Some meals are still difficult
- Timer doesn't fully hold attention yet
"If your child sat for 3 minutes today and last week they sat for 2 — that is a 50% improvement. That is real, measurable, neurological progress."
PMC11506176 — Systematic review: Early-phase indicators are tolerance and participation, not yet skill mastery.

"You may find yourself more confident at meals. You've stopped dreading the chair conversation. You have a plan and it's working. That confidence translates to the child — they read your calm."

- Child is sitting for 70–80% of age-appropriate duration without prompting
- Movement breaks are optional, not required, at most meals
- Weighted lap pad or wobble cushion may no longer be needed at every meal
- Child is engaged in mealtime conversation independently
- Other caregivers (grandparents, school) are reporting improved sitting
Stop. Look Back. Your Child Has Come So Far.
You have delivered therapeutic support at every meal, every day, often when you were exhausted, frustrated, and unsure it was working. You are not a bystander to your child's progress — you are its primary architect. 🥉 Bronze First 5-minute meal seated. Neurological growth — real and measurable. 🥈 Silver First meal without a movement break. Their sensory system regulated without leaving. 🥇 Gold First age-appropriate duration meal completed. Once unimaginable. Now real. 🏆 Platinum Consistent sitting across 5+ consecutive meals. Mastery is not one good day. It's a pattern. "Remember when you couldn't stay in your chair at all? Look at you now." Specific, past-referenced praise creates identity: "I am a person who can sit for meals." This identity becomes the child's own motivation — more powerful than any external reward over time.
- Sitting difficulty severe enough that child is not eating sufficient nutrition
- Postural issues worsening (increasing slouching, W-sitting, frequent falls)
- Challenges pervasive across ALL contexts — classroom, car, everywhere
- Home strategies consistently applied for 6+ weeks with no measurable improvement
- Signs of suspected ADHD, autism, or developmental delay not yet professionally evaluated
- Mealtime creating significant family distress across multiple family members
- Inconsistent response to materials — works some days, not others, no clear pattern
- Only one material is helping and it's reaching its limit of effectiveness
- Child's sitting tolerance has plateaued for 4+ weeks at a suboptimal level
- School is reporting significant sitting challenges in classroom setting







→ Request link: care@pinnacleblooms.org | Or call 9100 181 181
→ pinnacleblooms.org/find-center — Center locator map
→ Call 9100 181 181 | pinnacleblooms.org
Response within 24 hours for clinical queries.
Deeper Reading for the Curious Parent and the Referring Clinician.
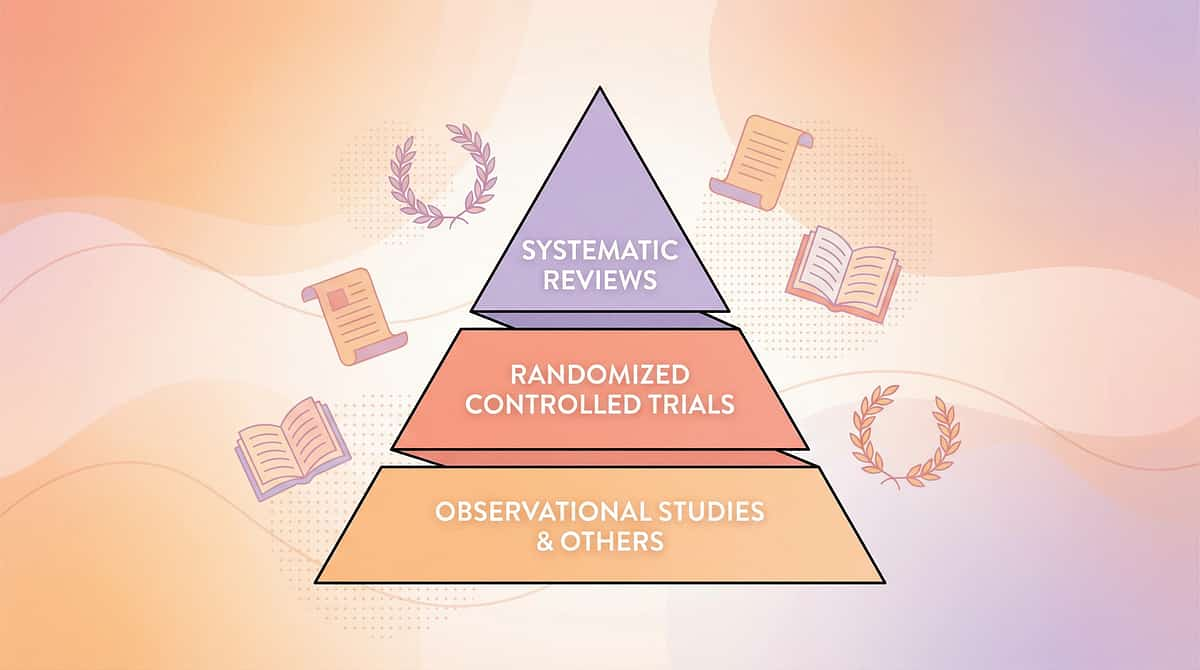
Evidence Pyramid Systematic Reviews (Highest) RCTs Cohort Studies Case Studies (Lowest) Key Studies PRISMA Systematic Review (2024) 16 articles, 2013–2023. Sensory integration intervention confirmed as evidence-based practice for ASD. → PMC11506176 Meta-Analysis — World J Clin Cases (2024) 24 studies. Sensory integration therapy improves adaptive behavior, sensory processing, gross/fine motor skills. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 Indian RCT — Indian J Pediatr (2019) Padmanabha et al. Home-based sensory interventions: significant outcomes in Indian pediatric population. → DOI: 10.1007/s12098-018-2747-4 WHO Care for Child Development Package (2023) Age-specific evidence-based caregiver guidance. Implemented across 54 LMICs. → PMC9978394 NCAEP Evidence-Based Practices Report (2020) Visual supports, sensory-based interventions, and reinforcement classified as evidence-based for autism. Frontiers in Integrative Neuroscience (2020) Neurological framework for sensory integration/processing treatment in ASD. → DOI: 10.3389/fnint.2020.556660

When [name] gets up from the table at mealtimes, it is NOT rudeness and NOT that they're not hungry. Their body physically cannot stay still for long periods yet. We are working on it with specific supports: a footrest (feet need to be flat), a cushion on the chair, and a timer so they know how long they need to stay.

Questions Parents Ask Most at Pinnacle Centers About Mealtime Sitting.
Q: My child is 7, not 2. Is it too late for these strategies to work? Neuroplasticity remains high through childhood. The strategies in E-467 work across ages 2–10 and beyond. Older children may respond faster because they can understand the purpose of the materials. It is never too late. The starting point is wherever your child is now. Q: Should I use ALL 9 materials at once? No. Identify your child's primary root cause first (postural? sensory? attention?) and deploy the most relevant 2–3 materials. Layer others as tolerance builds. Too many changes simultaneously makes it harder to identify what's working. Q: My child has ADHD, not autism. Does this still apply? Yes. Mealtime sitting difficulty in ADHD is driven primarily by attention and impulse regulation challenges. The visual timer, structured movement breaks, and engaging conversation strategies are particularly powerful for ADHD profiles. The footrest is universally helpful. Q: How long before I should see improvement? Most families see measurable improvement (even if modest) within 2 weeks of consistent application. The key word is consistent — every meal, every day. If after 6 weeks of consistent daily application there is no measurable improvement, professional assessment is recommended. Q: Is the wobble cushion safe? Will it make my child more unstable? The wobble cushion is designed to allow micro-movement, not destabilize. For children with very poor trunk stability, start with less inflation. If it makes sitting harder, use a firm textured cushion instead and refer to OT for seated postural assessment. Q: Can I use screens to help my child sit for meals? Screens increase sitting duration but do not build the underlying regulation skill — and they interfere with the social and communicative benefits of family mealtimes. We recommend mealtime engagement strategies (Material 9) that build genuine attention regulation rather than bypassing it. Q: My child was sitting well and then suddenly stopped. Why? Regression can indicate: illness (check first), a developmental phase change, environmental change, or plateau of a material's effectiveness. Return to baseline materials, shorten the timer target temporarily, and rebuild. Regression is part of the trajectory, not failure. Q: When does a mealtime sitting problem become an autism red flag? Mealtime sitting difficulty alone is not diagnostic of autism. However, if it co-occurs with: limited eye contact, delayed speech, rigid routines, significant sensory sensitivities, social communication differences — a formal developmental evaluation is warranted. FREE: 9100 181 181. Didn't find your answer? → Ask GPT-OS®: pinnacleblooms.org/gpt-os | Book teleconsultation: pinnacleblooms.org/consult
Preview of 9 materials that help sitting for meals Therapy Material
Below is a visual preview of 9 materials that help sitting for meals therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










🌐pinnacleblooms.org | care@pinnacleblooms.org | Find nearest center: pinnacleblooms.org/find-center