
"The same 5 foods. Every single day. And the fear in their eyes when something new appears — that's real."
You've tried shapes. Hiding vegetables. Rewards. Waiting it out. Other parents say their children grew out of it. Yours haven't. This is different. And you're exhausted.
You are not failing. Your child's nervous system is telling you something important — and there are 9 evidence-based tools that can help.
🌸 Pinnacle Blooms Consortium
Feeding & Nutrition Series — Episode E-451

Millions of Families Are Navigating Exactly This
Extreme picky eating — when a child's food repertoire is severely limited, when they gag or cry at new textures, when they would rather go hungry than try something unfamiliar — is not rare. It's estimated to affect 1–5% of children in clinical ranges (ARFID), with sensory-based feeding difficulties in up to 90% of children with ASD.
1 in 3
Picky Eating
Children experience some degree of picky eating in early childhood
90%
ASD & Feeding
Children with ASD have significant feeding difficulties
5–20
ARFID Foods
Average food repertoire in ARFID — vs. 30+ in typical development
In India alone, if 2 million children are on the autism spectrum and 80–90% have feeding difficulties — that's 1.6–1.8 million children and families needing exactly what you're reading right now. You are among hundreds of thousands of Indian families, and millions globally, navigating this exact challenge.
This Is Not a Behavior Problem. This Is a Wiring Difference.
The Neuroscience
When a child with sensory-based feeding difficulties encounters an unfamiliar food, their brain's threat-detection pathways (amygdala and insular cortex) fire as if the food represents genuine danger. Their taste, texture, and olfactory receptors process ordinary food properties — a slightly different brand, a new texture, a changed color — as genuinely aversive sensory input. The body enters fight-or-flight before a single bite is taken.
What Parents See
The gagging is real — not performed. The refusal is not stubbornness — it's self-protection. The specific brand requirement is not manipulation — it's pattern recognition as a safety mechanism. Your child's nervous system is doing exactly what it was built to do. It has a different calibration. That's what therapy addresses.
Sensory Processing
Hyper-sensitivity to taste, texture, smell, temperature
Oral Motor
Difficulty chewing or swallowing certain textures
Anxiety
Fear responses from past negative food experiences
Medical
GI issues, reflux, allergies creating pain associations
Developmental
ASD/ADHD profiles with rigidity and sensory needs

Typical Picky Eating Resolves. This Is Different — and It Has a Clear Therapeutic Pathway.
Age 2–4
Typical picky phase — normal developmental stage
Age 4–6
Typical resolving — most picky eating improves naturally
Age 6–8
⚠ Red Flag — if still fewer than 20 foods, seek evaluation
Age 8–12
⚠ Red Flag — unchanged patterns require professional intervention
Adolescent
⚠ Escalation risk — social impact and nutritional consequences increase
Your Child Is Here: If your child is eating fewer than 20 foods, avoiding entire food groups, showing genuine fear or distress at mealtimes, or not improving with standard strategies — this page was built for them.
Common co-occurring conditions: Autism Spectrum Disorder (70–90% have feeding difficulties), ADHD, Sensory Processing Disorder, Anxiety Disorders, and Gastrointestinal conditions where pain creates negative food associations.

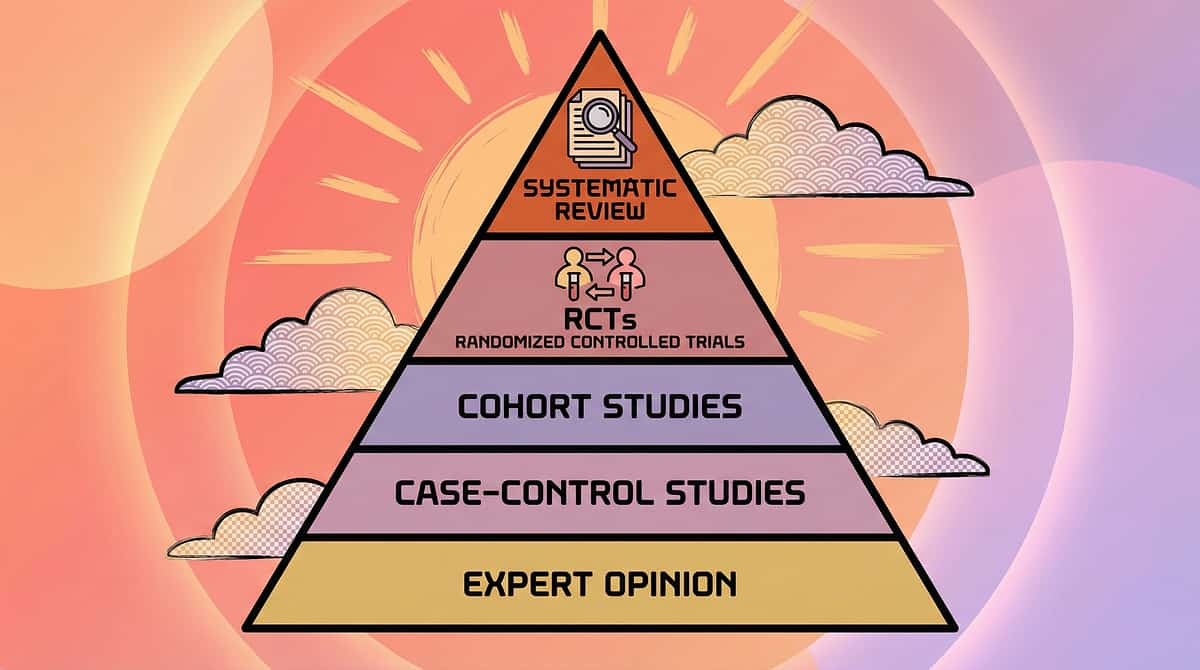
This Approach Is Backed by International Research. Not Guesswork.
🛡️ Level I–II Evidence
Systematic Reviews + RCTs
Study | Key Finding | Source | |
PRISMA Systematic Review, 2024 | Sensory integration therapy is evidence-based practice for ASD across 16 studies (2013–2023) | PMC11506176 | |
Indian RCT (Padmanabha et al., 2019) | Home-based sensory interventions show significant functional outcomes | DOI: 10.1007/s12098-018-2747-4 | |
Meta-analysis, World J Clin Cases, 2024 | SIT promotes social skills, adaptive behavior, sensory processing across 24 studies | PMC10955541 | |
NCAEP Report, 2020 | Visual supports classified as evidence-based practice for autism | ncaep.fpg.unc.edu | |
Fraker et al. Food Chaining | Systematic diet expansion evidence base established | Food Chaining, 2007 |
80%
Evidence Confidence
Strong evidence base with ongoing research across multiple disciplines
Clinically Validated. Home-Applicable. Parent-Proven. Every material in this guide has been reviewed and consortium-validated by OT, SLP, ABA, and NeuroDevelopmental specialists at Pinnacle Blooms Network®.

What This Technique Is: The Calm Food Journey Toolkit
Formal Name: Sensory-Based Feeding Intervention — Graduated Exposure Protocol with Environmental and Material Support System
"Eating is the final step in a long journey. We start at Step 1 — tolerating food in the room — and work forward from there."
A structured, multi-disciplinary approach to expanding the food repertoire of children with extreme picky eating by addressing underlying sensory, oral motor, anxiety, and behavioral factors. Rather than pressuring children to eat, this approach builds comfort with food through gradual, non-threatening exposure — starting where the child is.
Step 1–3: Tolerance
Food in room → on table → on plate
Step 4–5: Interaction
Touching → Interacting with tools
Step 6–7: Sensory
Smelling → Lips and tongue contact
Steps 8–9: Tasting
Tastes → Eats ✓ (the final goal)
🏷️ Domain E
Feeding & Nutrition
👶 Age Range
18 months – 12 years
⏱️ Session
10–20 min | 2–3x per week
📊 Approach
SOS + Food Chaining + Sensory Integration

This Approach Crosses Therapy Boundaries — Because Your Child's Feeding Difficulty Crosses Them Too.
🔵 Occupational Therapist (Lead)
Primary discipline. Assesses sensory processing, oral sensory defensiveness, environmental factors. Designs sensory desensitization program. Selects and sequences materials. Leads the home program.
🟢 Speech-Language Pathologist (Co-Lead)
Assesses oral motor function, swallowing safety, jaw/lip/tongue coordination. Addresses texture progression. Leads oral motor therapy. Supports food exploration toolkit work.
🔴 BCBA / ABA Therapist
Applies behavioral principles — positive reinforcement for food exploration, systematic exposure ladders, anxiety desensitization protocols. Data collection and progress measurement.
🟡 Special Educator / Dev. Pediatrician
Adapts mealtime structures for developmental profile. Coordinates school mealtime supports. Rules out medical contributing factors. Monitors growth and nutritional status.
"Your child's OT looks at how their nervous system processes food. Their SLP looks at whether their mouth can handle it. Their ABA therapist builds the approach ladder. In the Pinnacle Consortium, all four look at the same child together — via FusionModule™." 🌸
These 9 Materials Are Precision Tools, Not Random Activities.
Each of the 9 materials maps precisely to one or more of these targets. Understanding the target tells you which material to use, when to use it, and how to measure whether it is working.
Observable Indicator 1
Child tolerates new food on divided plate without meltdown
Observable Indicator 2
Child engages with food exploration toolkit without avoidance
Observable Indicator 3
Food repertoire increases by 1+ new food per month with consistent approach
Material 1 of 9
🍽️ Divided Plates
Divided Plates — Keep Foods Separate, Eliminate Contamination Anxiety
The Science (OT Lead)
When a child's preferred food is "contaminated" by touching a non-preferred food, the entire plate may be rejected. This is a real sensory or anxiety response — the brain registers food contact as a threat to the "safe" item. Divided plates keep foods completely separated, removing this major source of mealtime distress. They allow new foods to be present in the child's visual field — on their own plate, in their own section — without threatening preferred foods. This is the first step toward visual tolerance of unfamiliar foods.
How To Use
- Place preferred/safe food in the largest compartment
- Place new/exploration food in the smallest compartment (even 1 piece)
- Set the expectation: "Your safe food is here. The new food has its own space."
- Do not comment on whether the new food is eaten
- Gradually, over weeks, increase new food presence
💰 Price Range: ₹200–800 | BPA-free, microwave and dishwasher safe
DIY Alternative (Zero Cost): Use 3–4 separate small bowls or steel katoris. The principle is identical — food separation.
⚠️ Safety Note: Ensure plates are stable and appropriate for child's age. BPA-free materials are preferred for microwave use.
Material 2 of 9
🔧 Food Exploration Toolkit
Food Exploration Toolkit — Before Eating Comes Exploring
The Science (OT + SLP): The Steps to Eating hierarchy — from the internationally validated SOS Approach to Feeding — makes a radical point: eating is Step 9 out of 9. The food exploration toolkit enables Steps 4–6 in a playful, zero-pressure context. Familiarity builds through repeated interaction — not through eating.
Tool | Purpose | Step Enabled | |
Kid-safe crinkle cutter / plastic knife | Cutting food = controlled interaction | Step 5 | |
Toothpicks / food picks | Poking, picking up without direct touch | Step 5 | |
Cookie cutters | Shaping soft foods — play without eating | Step 5 | |
Small tongs / tweezers | Picking up food without skin contact | Step 4–5 | |
Small pastry brush | "Painting" with sauces — sensory exploration | Step 5–6 | |
Magnifying glass | Examining food texture/color closely | Step 3–4 |
Script to use: "Let's see what's inside this carrot!" — Cut, poke, examine. Adult does it too, on their own food. No expectation of eating. "You don't have to eat it. We're just exploring."
💰 Price Range: ₹300–1,000 | DIY Alternative: Your kitchen has all of this — plastic cutlery, toothpicks, a child's fork as a probe, a small brush from a baking set.

Material 3 of 9
🔗 Food Chaining
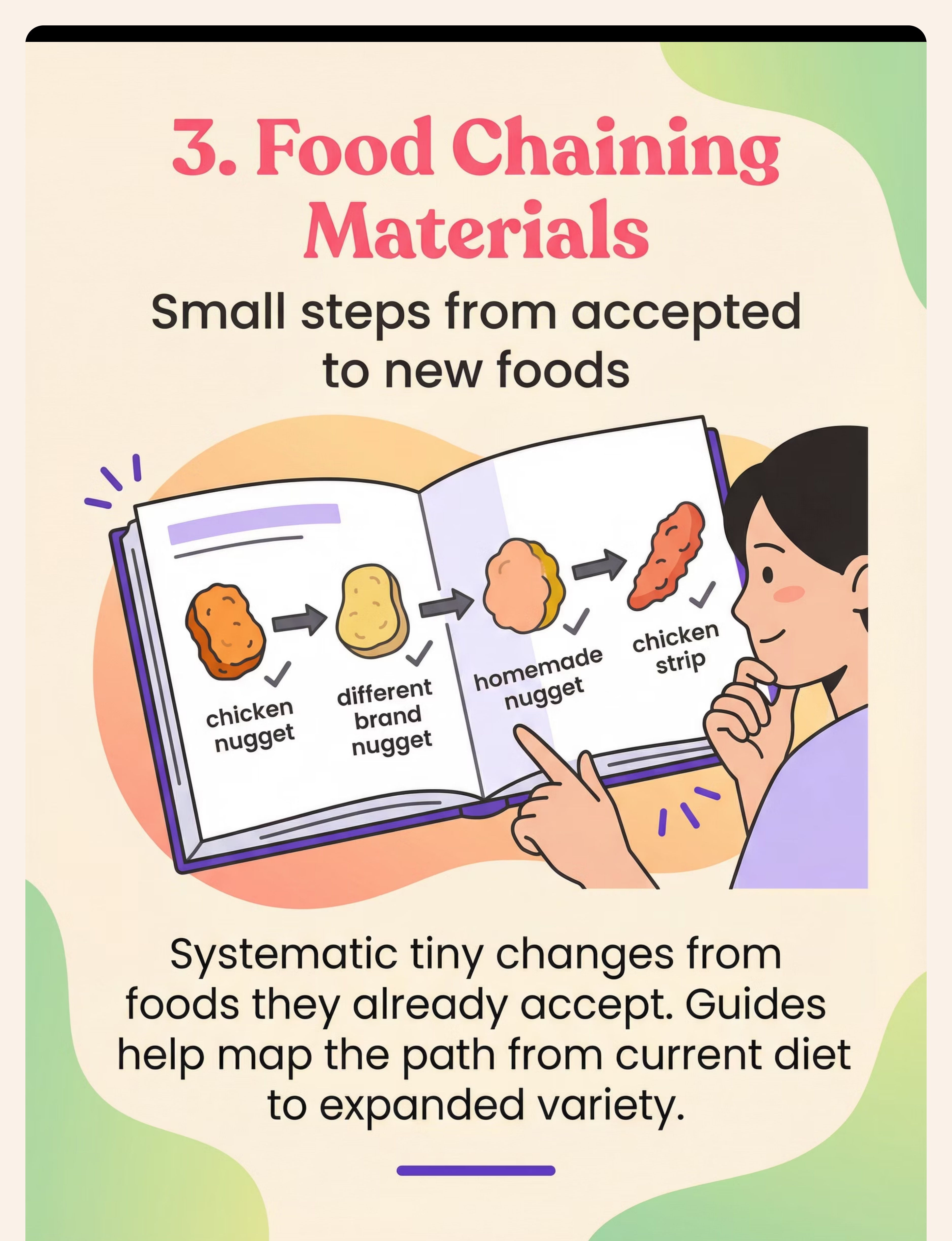
Food Chaining — The Science of Tiny Steps from Accepted to New Foods
The Science (SLP + OT): Random new food offers almost always fail for children with extreme selectivity. Food chaining — developed by Fraker, Fishbein and colleagues — works because it starts from neurological safety. Each change is so small the child's threat-detection system doesn't fire. Success at each step builds before moving to the next.
How To Create Your Own Chain
- List all currently accepted foods
- Pick one — your "anchor food"
- Identify its key properties: brand, texture, shape, preparation, color
- Change ONE property minimally
- Present the new version without comment or pressure
- Wait for acceptance (days to weeks) before the next step
💰 Price Range: ₹500–2,000 (books and printed guides) | DIY Alternative (Free): Download food chaining worksheets free at ASHA (asha.org) or create your own using the framework above.

Material 4 of 9
🎨 Sensory Food Play
Sensory Food Play — Desensitize Through Play, Not Eating
The Science (OT Lead): When a child finger-paints with yogurt, stamps with vegetables, or builds with crackers — they are accumulating sensory exposure in a positive emotional context. This rewires the brain's threat-response to those food properties. Tolerance in play precedes tolerance in eating. The rule is absolute: no eating is expected or requested during sensory play.
Activity | Food Used | Sensory Properties Targeted | |
Finger painting | Yogurt, pudding, pureed mango | Wet texture, color, smell | |
Vegetable stamping | Cut bell peppers, broccoli | Firm texture, shape, smell | |
Dry sensory bin | Uncooked pasta, rice, lentils | Dry texture, temperature | |
Building structures | Crackers, pretzel sticks | Crunchy texture, shape | |
Edible playdough | Peanut butter + oats | Malleable texture, smell |
If child brings food to their mouth during play — positive, let it happen naturally. Never prompt eating during a sensory play session.
💰 Price Range: ₹200–500 | DIY Alternative: 100% DIY — everything comes from your kitchen. No purchase needed whatsoever.

Material 5 of 9
📋 Visual Mealtime Supports
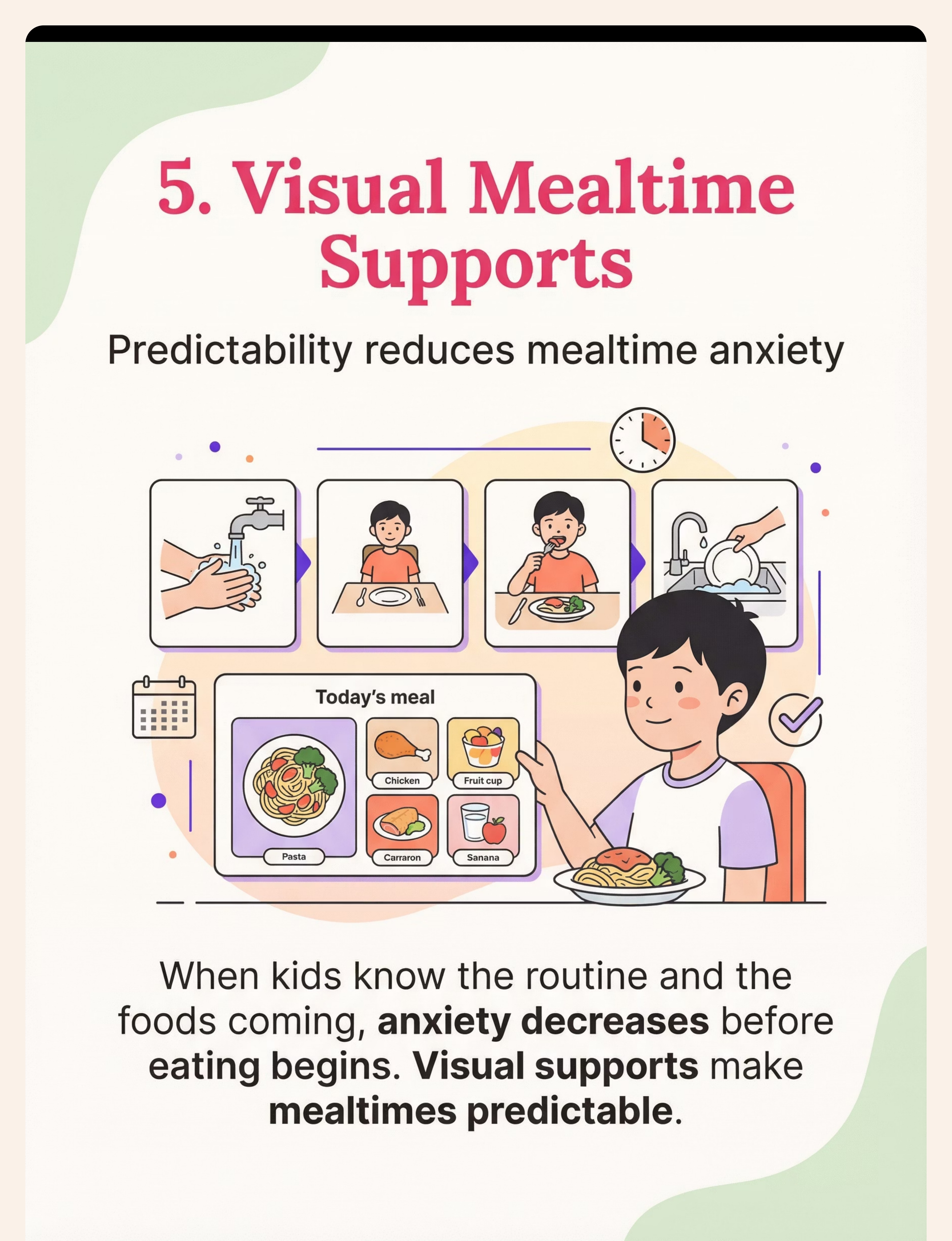
Visual Mealtime Supports — Predictability Dissolves Anxiety Before It Starts
The Science (SpEd + ABA): Anxiety doesn't start at the table — it starts hours before the meal. When a child knows the routine sequence, the foods being served, their choices, and that they won't be forced to eat the new food — their nervous system begins to regulate before they sit down. Visual supports are classified as evidence-based practice by NCAEP (2020).
📅 Mealtime Sequence Cards
Visual schedule showing routine — wash hands, sit at table, see what's on menu, eat, put plate away. Reviewed 5 minutes before meal.
📸 Visual Menu
Photographs of the actual foods being served today. Posted on fridge or at table place. No surprises = no pre-meal panic.
✅ Choice Board
Visuals showing which items child can choose. Control = reduced anxiety. Even small choices matter significantly.
🔍 Exploration Step Card
"Today at dinner we are: LOOKING at broccoli. That's all." Makes clear that no eating is required today.
💰 Price Range: ₹200–600 | DIY Alternative (Free): Photograph your actual foods on your phone. Print and laminate at any stationery shop (₹5–10/sheet).

Material 6 of 9
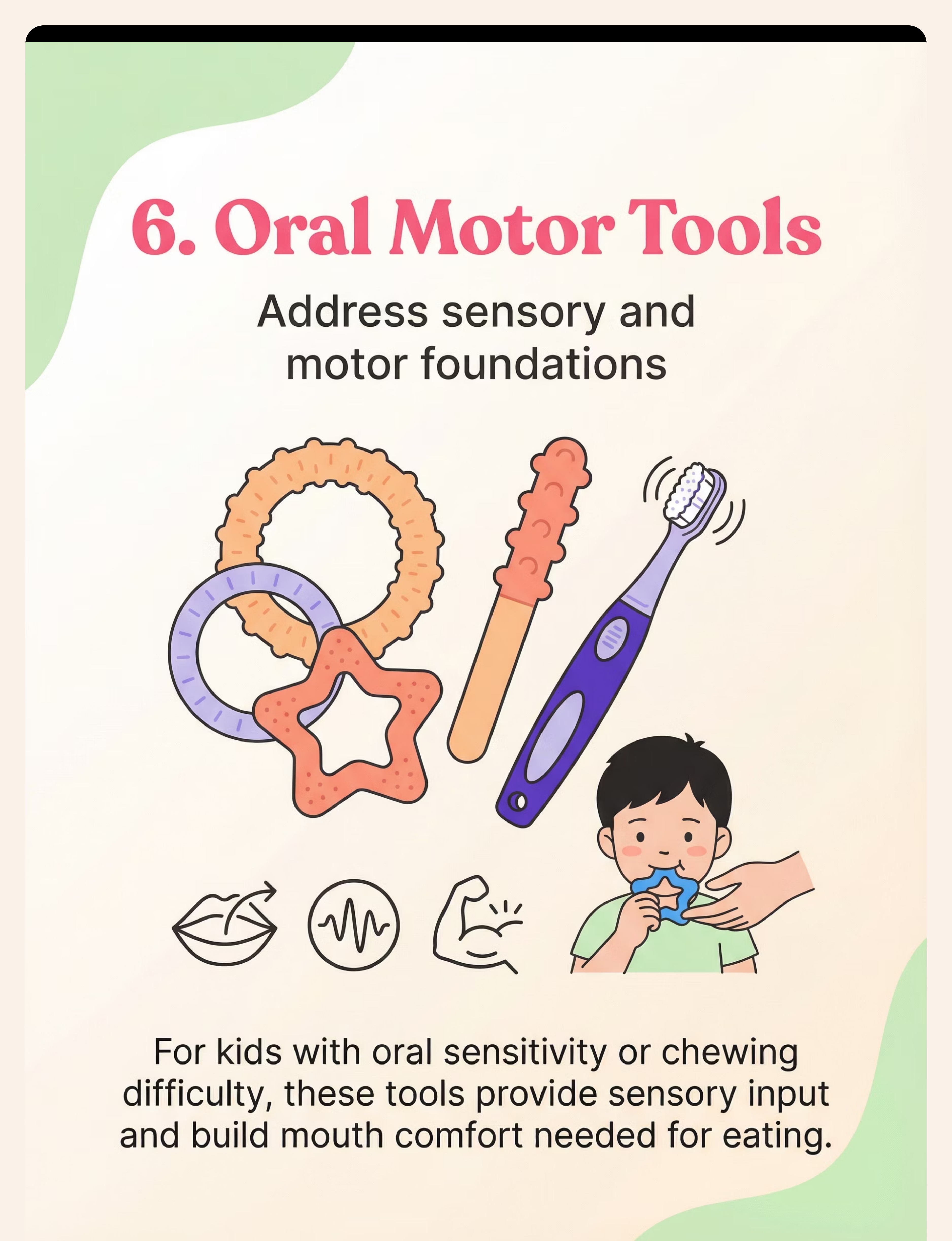
🦷 Oral Motor Chewy Tools
Oral Motor Tools — Address the Physical Foundations That Make Eating Possible
The Science (SLP Lead): Many children with extreme picky eating have underlying oral sensory processing differences or oral motor challenges never identified because the presenting problem looks behavioral. Oral motor chewy tools provide controlled, organizing sensory input to the mouth, reducing hypersensitivity. This is foundational, not supplementary.
🟢 Chewy Tools
Safe silicone chewys in multiple textures/resistances — reduce oral hypersensitivity, support regulation
🔵 Vibrating Toothbrush
Desensitizes gums, cheeks, tongue — graduated introduction to tactile input in the mouth
🟡 Oral Motor Exercises
Horns, whistles, straws (varying diameters) — build lip, jaw, and tongue strength for chewing
🔴 Textured Spoons
Introduces texture gradually in a familiar, non-food context before mealtime
💰 Price Range: ₹300–1,500 | Search "ARK Therapeutic chewy tools" or "oral motor tools children" on Amazon.in
⚠️ Safety Note: Chewy tools must be age/chewing-strength appropriate. Inspect regularly for wear. Consult OT/SLP for children with significant oral motor challenges. 📞 Oral motor evaluation referral: 9100 181 181

Material 7 of 9
🥄 Tiny Tasting Dishes
Tiny Tasting Dishes — Start Impossibly Small. That's Not Giving Up. That's Strategy.
The Science (OT + ABA)
A full serving of a feared food on a plate activates the child's threat response proportionally. One pea in a tiny cup? The threat level is minimal. The ABA principle of antecedent manipulation says: control what you can to maximize success. Portion control dishes engineer success by making the amount of new food so small the child's nervous system can tolerate it. The message from a tiny cup is: "This is so small it cannot hurt you."
How To Use
- New food goes in tiny dish — 1 piece or 1 teaspoon maximum
- "This tiny cup has one piece of carrot to look at." (Not eat — look at.)
- Tiny dish sits beside the main plate — it is decorative, not demanded
- No comment on whether it was eaten
- Over weeks: "to look at" → "to touch" → "to smell" → "to taste if you want"
Your Collection
Condiment cups, small dipping bowls (₹10–20 each), silicone cupcake molds, small ramekins, decorative shot glasses for older children
DIY Alternative (Free)
Use bottle caps, small ceramic katoris, or any tiny container you have at home. The size is what matters, not the material.
💰 Price Range: ₹100–400 for a full set of varied sizes

Material 8 of 9
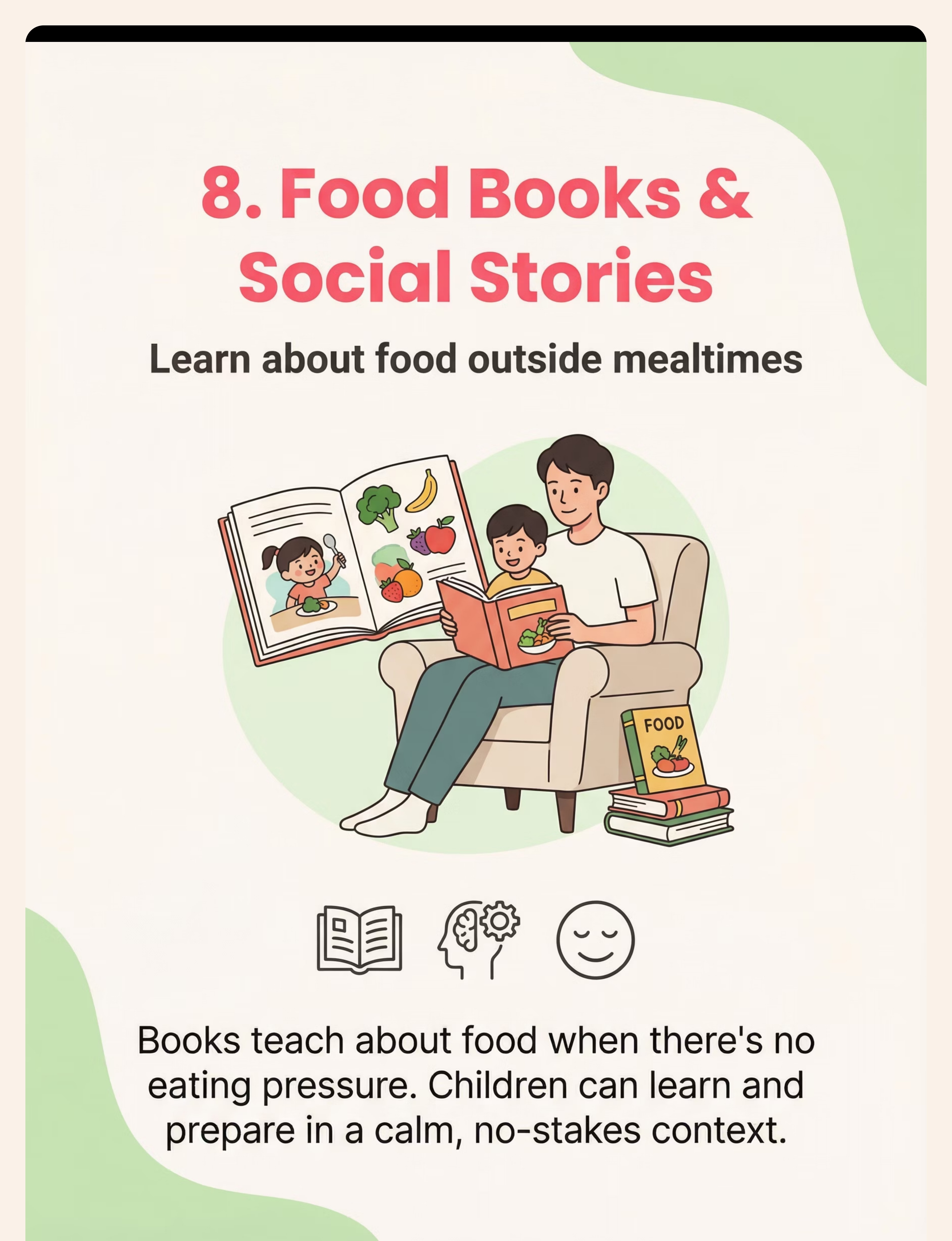
📚 Food Books & Social Stories
Food Books & Social Stories — Prepare the Mind When There's No Pressure to Eat
The Science (SpEd + SLP): Cognitive preparation happens best when there is no immediate demand. Picture books and social stories allow children to think about, discuss, and process food-related experiences in a completely calm, pressure-free context. A child who has read a story about a character bravely sniffing an orange has cognitive scaffolding for that encounter.
📖 Picture Books About Food
- Books showing characters exploring new foods with realistic hesitation — not instant liking
- Books explaining why different foods help bodies grow
- Books about being brave with new things
- Read together at bedtime — never just before meals
📝 Personalized Social Stories
Written specifically for YOUR child, about THEIR mealtime:
"Tonight at dinner there will be rice, dal, and one small piece of capsicum in a tiny cup. The capsicum will not touch my rice. I don't have to eat the capsicum. I can look at it or touch it if I want. My safe foods will be there. Dinner will end. Then I can play."
⚠️ Avoid books where characters instantly love new foods — realistic hesitation is more therapeutically accurate and relatable for children.
💰 Price Range: ₹300–1,500 (books) | ₹0 (personalized social stories — written by you, free)
Material 9 of 9
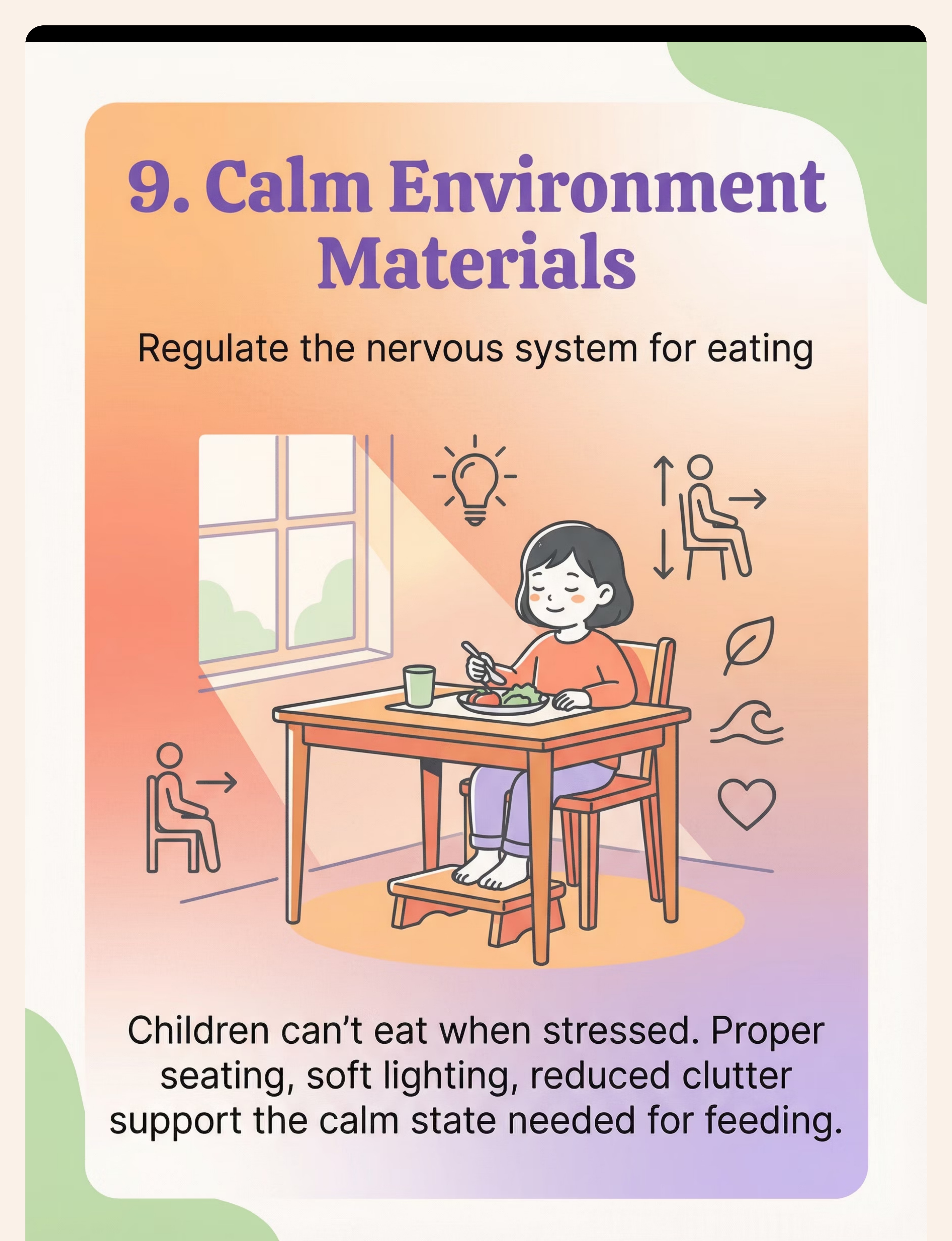
🏠 Calm Mealtime Environment
Calm Mealtime Environment — You Cannot Eat Under Siege. Neither Can Your Child.
The Science (OT + NeuroDev Pediatrician): The autonomic nervous system governs whether a child can eat. In a calm, predictable environment, the parasympathetic nervous system is active — digestion works, sensory thresholds are higher, flexibility increases. In a stressful environment, the sympathetic nervous system activates, digestion slows, and the child's threat response to food intensifies. Environmental modification is not "giving in." It is creating the neurological conditions under which eating is physically possible.
🪑 Seating
Child's feet flat on a surface | Hips at 90° | Table at elbow height | Use footrests, boosters, or appropriate chair
💡 Lighting
Soft, warm light preferred | Avoid harsh fluorescents | Natural light if possible
🔇 Sound
Reduce background noise | TV off during meals | Soft background music if helpful for the child
📵 Screens
Remove ALL screens. Screen distraction prevents eating awareness building — this is non-negotiable.
💰 Price Range: ₹500–3,000 (seating supports, lighting) | Many environmental modifications are completely free — rearrange, reduce clutter, change a lightbulb.

Every Single Material Has a Zero-Cost DIY Version. The Therapy Works Either Way.
WHO/UNICEF Equity Principle: "Effective intervention should never depend on purchasing power. The therapeutic principle is what heals — not the brand."
# | Material | Buy Option | Price | Free DIY | |
1 | Divided Plates | Amazon.in | ₹200–800 | 3 separate katoris from your kitchen | |
2 | Exploration Toolkit | Amazon.in | ₹300–1,000 | Toothpicks + plastic cutter + fork | |
3 | Food Chaining Guide | Books + worksheets | ₹500–2,000 | Chain chart in a notebook | |
4 | Sensory Food Play | Art supply kits | ₹200–500 | Kitchen ingredients + newspaper | |
5 | Visual Supports | Printed laminated cards | ₹200–600 | Phone photos + stationery shop laminate | |
6 | Oral Motor Tools | Amazon.in | ₹300–1,500 | Consult SLP; some exercises need no tools | |
7 | Tiny Tasting Dishes | Kitchen store | ₹100–400 | Bottle caps, steel katoris, small cups | |
8 | Food Books | Bookstore | ₹300–1,500 | Write personalized social stories — free | |
9 | Calm Environment | Seating supports | ₹500–3,000 | Rearrange, reduce clutter, change light |
Starter Kit (₹700 total): Divided plate + 3 tiny bowls + printed visual schedule + food exploration kit (items from home) = Complete foundation to start TODAY.

⚠️ Read This Before Your First Session.
🔴 STOP — Do Not Proceed If:
Child has a history of choking, aspiration, or unsafe swallowing | Child has identified food allergies — all materials must be allergy-screened | Signs of failure to thrive or nutritional deficiency | Child has active illness or high distress state today | Chewy tools show visible wear or damage
🟡 Modify — Proceed With Caution If:
Child is currently under stress (school exam, recent change) | This is the first session — use only one material to start | Child has a history of very strong gag reflex — go slower with oral materials | Environmental setup is not yet complete
🟢 Green Light — Proceed When:
Child is calm, fed (not hungry), and regulated | Environment is set up correctly | You have reviewed the approach with child's current therapist | You have ONE material ready, not all nine at once
"The best feeding session is one that starts right. One good step forward beats five forced steps that cause regression."
If your child has fewer than 10–15 foods, significant gagging, any nutritional concerns, or fear that seems like panic — professional feeding evaluation is not optional. It is the starting point.

Your Mealtime Setup: A Bird's-Eye View
Getting the physical setup right before your first session dramatically increases the likelihood of a calm, productive mealtime. Use this checklist before every session — consistency in setup reduces your child's anticipatory anxiety.
Child's Seating
Feet supported, hips stable, appropriate height — use footrest or booster if needed
Divided Plate
Safe food in large section, new food in small section — physical separation is essential
Tiny Dishes
1–2 exploration items in separate small containers beside the main plate
Visual Menu
Photos of tonight's foods posted at table — reviewed before sitting down
Lighting & Sound
TV off, soft warm light, optional quiet background music — no screens at all
Your Mindset
No agenda. Beside child, not directly across. If one new food is tolerated on plate — that is success.
📊 Track your setup consistency over 8 weeks using the Pinnacle E-451 Session Data Tracker. Consistent setup is the single strongest predictor of early progress.

60-Second Readiness Check — Before Every Session
Running this check before each session takes less than a minute and dramatically reduces failed sessions. A session that starts wrong rarely recovers.
Check | ✅ Go | 🟡 Modify | ❌ Postpone | |
Hunger level | Slightly hungry (best) | Just ate (full) | Ravenous (too dysregulated) | |
Emotional state | Calm, regulated | Mildly elevated | Meltdown, panic, illness | |
Recent events | Stable day | Minor stress | Major upset, transition, illness | |
Child's signal | Comes to table willingly | Needs prompting | Actively refuses |
✅ GO
4–5 green lights → Proceed with full session
🟡 MODIFY
2–3 green lights → 1 material only, reduce duration and new food presence
❌ POSTPONE
Fewer than 2 green lights → Skip today. Do a preferred activity. Reset tomorrow.
"Postponing a session when the child isn't ready is therapeutic wisdom, not failure."

Step 1 of 6
⏱️ 30–60 seconds
The Invitation — Invite, Don't Command
"Hey, are you ready? I've got your [safe food name] and something for us to explore together. No pressure. Come when you're ready."
Body Language Guidance
- Sit down yourself first — let the child approach
- No direct eye contact on food (glancing, not staring)
- Relaxed posture — no tension the child can read
- Have your own plate in front of you too — model eating your own food
Resistance Responses
- "I don't want to eat that" → "You don't have to eat anything. We're just exploring."
- Stands up and leaves → Allow it. Try again tomorrow. Do NOT follow or pressure.
- Covers eyes or turns away → Use this as information: today is a Modify day.
Child sits (even reluctantly) → ✅ Green light. Child looks at their plate → ✅ Green light.
Step 2 of 6
⏱️ 1–3 minutes
The Engagement — The Therapeutic Work Starts the Moment They Sit
"Look, your [safe food] is here. And I have this tiny cup with [new food name] — we're just going to see what it looks like today. You have your [exploration tool] if you want to poke at it."
Presentation of New Food: Place tiny dish with new food to the side — not in their space. Distance from child: 30–40 cm initially — you can move it closer as the session progresses. Never place new food on child's preferred food plate.
Child Response | Meaning | Your Action | |
Ignores new food completely | Normal at this stage | Continue eating your own meal. No comment. | |
Looks at new food | Step 3 achieved! | Note it internally. Small smile. No fanfare. | |
Pokes new food with tool | Step 5 achieved! | Celebrate warmly: "Look at you exploring!" | |
Pushes new food away | Tolerance boundary | Move dish slightly further. No pressure. | |
Gags at sight | High sensitivity | Modify: reduce new food's visibility today. |
Reinforcement Cue: When child engages positively — even looking — acknowledge warmly within 3 seconds: "Nice exploring." Simple. Specific. Immediate.

Step 3 of 6
⏱️ 3–7 minutes
The Therapeutic Action — This Is Where Change Happens
Using the appropriate material(s) from the 9 (based on the child's current Step on the Eating Hierarchy), execute the planned therapeutic engagement for this session. Each session focuses on one specific Step.
If child is at Step... | This session's action | Material used | |
1–2 (room/table tolerance) | New food in room, child not at table | Divided plate at distance | |
3 (plate tolerance) | New food in tiny dish on their side of table | Tiny tasting dish + divided plate | |
4 (touching) | Use exploration tool to touch new food | Food exploration toolkit | |
5 (interacting) | Cut, poke, build with new food | Toolkit + sensory play | |
6 (smelling) | Bring food to nose on a tool — "What does it smell like?" | Toolkit + social story | |
7–9 (lips/taste/eat) | Tiny taste opportunity offered — never required | Tiny dish + calm environment |
❌ Common Execution Errors
Jumping ahead to eating when child is at Step 4 → Causes rejection and regression. Commenting on what or how much was eaten → Increases pressure. Showing visible disappointment → Child reads it; anxiety increases.
✅ The Golden Rule
Meet the child EXACTLY where they are. Celebrate the current step. Nothing more. Every step forward — however small — is genuine neurological progress.
Step 4 of 6
⏱️ 3–5 minutes
Repeat & Vary — 3 Good Repetitions Beat 10 Forced Ones. Always.
Target Repetitions
2–4 repetitions of the core therapeutic action per session
Vary Each Rep
Different tool, slightly closer, or different food from same chain
Honor Satiation
When child signals "done" — stop immediately. Trust their signal.
For Exploration Toolkit Sessions
- Rep 1: Child uses tongs to pick up new food
- Rep 2: Child uses brush to paint new food on paper
- Rep 3: Child uses cutter to cut new food in half
For Food Chaining Sessions
- Rep 1: Present current chain step alongside accepted food
- Rep 2: Compare the two visually — "Same shape? Different color?"
- Rep 3: Child interacts with chain-step food using tool of choice
For Sensory Play Sessions
- Rep 1: Adult models activity with new food
- Rep 2: Child joins with tool (indirect contact)
- Rep 3: Child makes direct contact if comfortable
The Satiation Rule: A session that ends on the child's initiative builds trust for next session. One that ends on your insistence damages it.
Step 5 of 6
⏱️ 30 seconds per reinforcement event
Reinforce & Celebrate — Celebrate the Attempt, Not Just the Success
The Reinforcement Science (ABA): Immediate, specific, enthusiastic reinforcement within 3 seconds of desired behavior. What you reinforce is what repeats.
Child sat with new food present
"Great sitting with something new there!"
Child looked at new food
"You looked right at it!"
Child used tool to touch new food
"Wow — you touched it! That's huge!"
Child brought food to lips
"You brought it right up close — that's brave!"
🎯 Social
Specific verbal praise (most powerful)
🎯 Physical
High-five, fist bump, hug if child accepts
🎯 Token
1 sticker per step achieved → reward jar
🎯 Activity
5 minutes preferred activity post-meal
Do NOT reinforce eating itself with big celebrations (creates pressure). Do NOT use food as a reward (complicates food relationship). Do NOT compare to siblings or previous sessions.

Step 6 of 6
⏱️ 2–3 minutes
The Cool-Down — No Session Ends Abruptly. The Cool-Down Is Therapeutic.
Why This Matters: Predictable endings teach the child that mealtimes have boundaries — that they end, and that safety is restored after the meal. This reduces anticipatory anxiety for the NEXT session. Consistent endings are as therapeutic as consistent beginnings.
If child wants to continue eating preferred food
Allow 2 more minutes, then firm close. Consistent end times must be maintained.
If child is upset at new food being removed
Acknowledge the feeling + close the session. Never allow a session to drag hoping child will try new food.

Capture the Data — Within 60 Seconds of Session End
What gets measured gets improved. 8 weeks of session data reveals patterns invisible in the moment — which days work best, which materials have the most impact, whether the child is progressing.
📅 Date & Session #
Today's date + running session count
Example: 15 Jan 2025, Session #7
Example: 15 Jan 2025, Session #7
🎯 Steps Achieved
Which Steps on hierarchy were reached for which food
Example: Broccoli — reached Step 4 (touched with tool)
Example: Broccoli — reached Step 4 (touched with tool)
📊 Child's State
Overall regulation: 1 (very dysregulated) to 5 (calm)
Example: 4/5 — mild initial resistance, settled well
Example: 4/5 — mild initial resistance, settled well
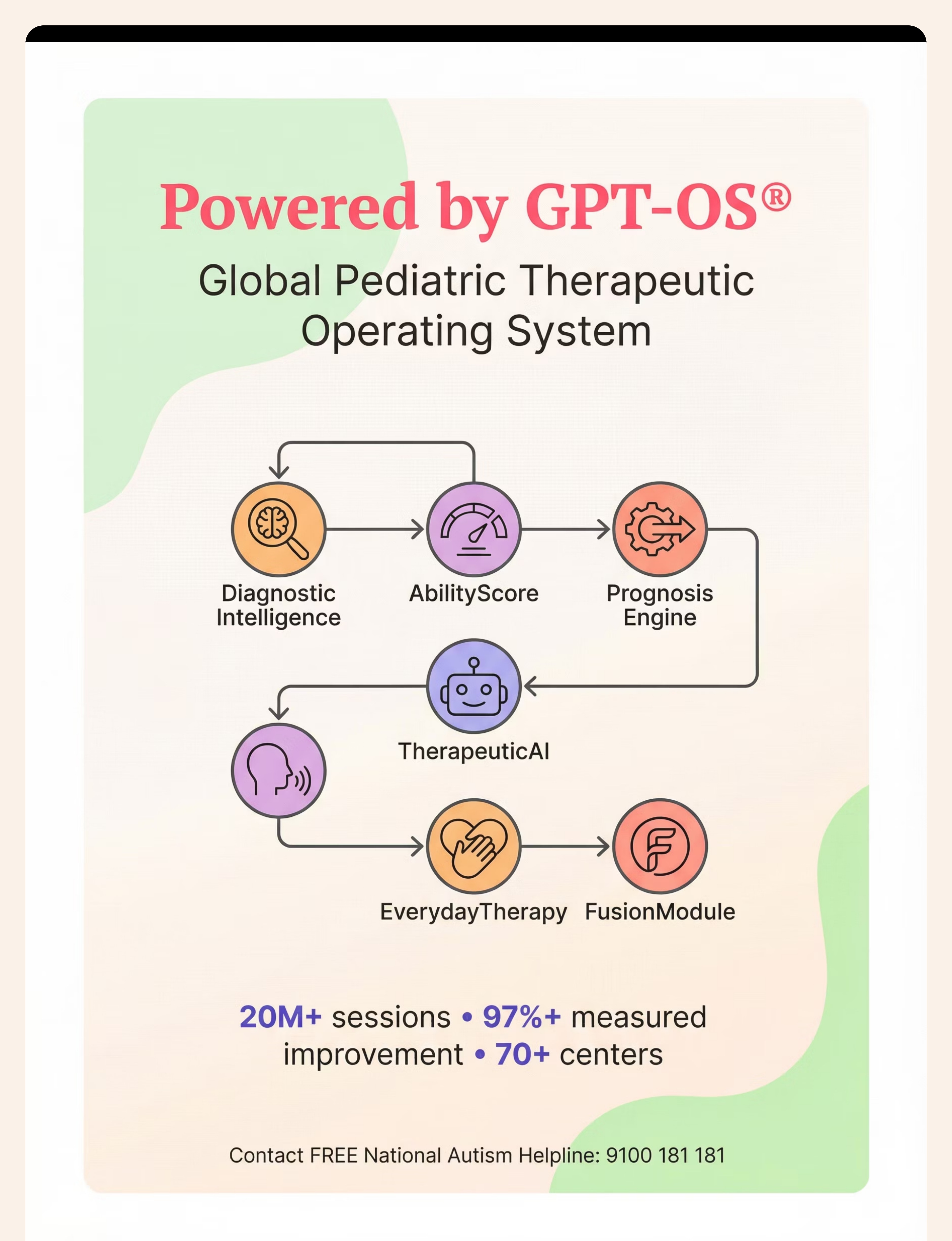
GPT-OS® Integration: Data recorded feeds → AbilityScore® → TherapeuticAI® → Updated EverydayTherapyProgramme™ → FusionModule™ coordination across OT, SLP, ABA, and Dietitian teams.
Optional fields: New food exposure today (yes/no + food name) | Duration of session (minutes) | Materials used | Parent notes. All data feeds the Pinnacle Prognosis Engine to improve recommendations for every family.
Troubleshooting — When It's Not Working
This is hard. Here are the 6 most common challenges — and what the evidence says to do about each one.
❌ Challenge | ✅ Evidence-Based Response | |
Child refuses to sit at table | Go back one step: food at distance. Child not required to sit yet. | |
New food on plate triggers meltdown | Remove new food. Divided plate only with safe foods. Start with food in room, not on plate. | |
Child making progress then regression | Regression is normal after illness, vacation, or stress. Restart from where they were comfortable. | |
Sibling eats easily and child compares | Never compare. Each child's nervous system is different. Focus only on this child's Steps. | |
Parents disagreeing on approach | Consistency matters more than perfection. Choose ONE approach. Pressure from either parent amplifies anxiety. | |
No progress after 8 weeks | Professional feeding evaluation is indicated. This is not failure — it is time for clinical assessment. |
"Pressure makes extreme picky eating worse, not better. If you catch yourself bribing, forcing, negotiating, or showing frustration — stop. Reset. The therapeutic approach requires adult regulation first."
🔴 Professional Indicators: Fewer than 10 foods | Growth concerns | Gagging/choking | Fear that looks like panic | Nutritional deficiency signs

One Approach. Infinite Personalizations. Your Child Is Not a Textbook Case.
🔵 The Sensory Avoider (Hypersensitive)
Overwhelmed by even small amounts of new foods. Texture aversion is primary. Adapt: Start much further back on hierarchy. More sensory play, more distance, smaller portions. Oral motor work first.
🟢 The Anxious Eater (Anxiety-Primary)
Fear of new foods, anticipatory anxiety, rigid routines. Less sensory, more psychological. Adapt: Maximum predictability. Social stories. Visual supports. Gradual exposure with explicit reassurance that eating is never required.
🔴 The Oral Motor Struggler (Motor-Primary)
Avoids foods hard to chew. Pocketing, choking, spitting out. Adapt: Oral motor therapy first, then food chaining focused on texture progression. SLP assessment essential.
18 mo–3 yrs
Keep entirely in play/sensory mode. No tasting pressure whatsoever.
3–6 years
Steps hierarchy, visual supports, food play prominent in every session.
6–12 years
Add cognitive preparation. Child can understand and co-create the approach.

Progress Arc
Week 1–2
Weeks 1–2: You're Laying Foundation, Not Harvesting Results.
15%
Progress Stage
Week 1–2 foundation building
✅ What Progress Looks Like Now
- Child sits at table without pre-meal meltdown (even if reluctant)
- New food on divided plate tolerated for duration of meal (even ignored)
- Child uses exploration tool at least once
- Mealtime ends without incident at least 3 out of 5 times
- Parent has executed 3+ sessions with consistent approach
❌ Not Expected Yet (And That's Fine)
- Eating the new food → Not expected until Weeks 6–12+
- Child showing interest in new food → May come in Weeks 3–4
- No more meltdowns → Stability comes with repetition
Parent Metric: If mealtime is 5% less stressful than before — that is measurable progress. If your child sat for 3 seconds longer — that is measurable progress. Precision over drama.

Progress Arc
Weeks 3–4
Weeks 3–4: The Neural Pathways Are Forming. You May Not See It Yet. It's Happening.
40%
Progress Stage
Weeks 3–4 consolidation
Child anticipates session
Brings themselves to table without reminder — intrinsic motivation emerging
Increased exploration confidence
More confident manipulation of new food with the exploration toolkit
Visual supports reviewed independently
Child references the visual menu or schedule before you prompt them
Mealtime duration stabilizing
Sessions settling into consistent 20–25 minute windows
What the Brain Is Doing: Repeated, structured input at the same level causes synaptic strengthening. The neural pathway from "new food → threat" is being retrained toward "new food → familiar situation." This is neuroplasticity in action. It is invisible. Trust the process.
Parent Milestone: You may notice you are more confident. Your own regulation at mealtimes has improved. This is real — and it matters, because children eat better when the adults around them are calm.
Progress Arc
Weeks 5–8
Weeks 5–8: The Breakthroughs Begin. Watch for These Specific Indicators.
70%
Progress Stage
Weeks 5–8 mastery indicators
First New Food Tolerated
New food on plate without distress → This is a breakthrough. Celebrate warmly.
Unprompted Tool Use
Child reaches for exploration tool without being asked — intrinsic motivation has arrived
Step 7 Reached
Child brings food to lips (even if not tasting) — extraordinary and significant progress
Repertoire Expands
Food repertoire increases by 1 food — even a small variation on a safe food counts as a new food
If you're at Week 8 and haven't reached these indicators — a comprehensive feeding evaluation with a Pinnacle OT/SLP feeding specialist is the next step. Not a failure — an upgrade. 📞 9100 181 181
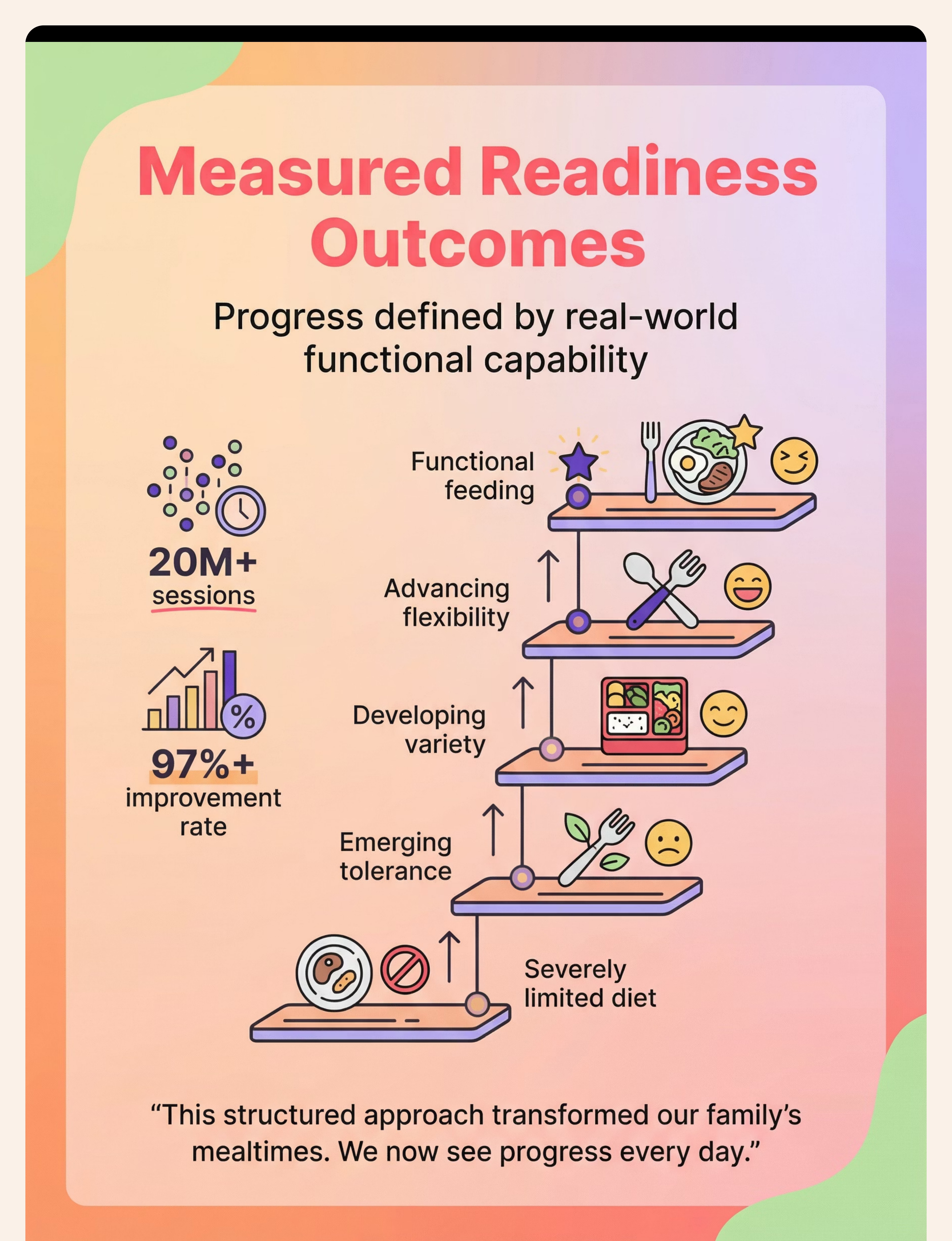
Every Step on This Ladder Is Worth Celebrating. Loudly.
Starting Point
Severely limited diet + mealtime distress
Emerging Tolerance
First new food tolerated on plate
Developing Variety
Repertoire slowly expanding with support
Advancing Flexibility
New foods with support, varied contexts
Functional Feeding ✓
Adequate variety + positive mealtimes
"Our son was down to 7 foods. After 8 months of systematic feeding therapy using gradual exposure and food chaining, he eats 35 foods now — including some vegetables. More importantly, he's no longer terrified at mealtimes. We can go to restaurants. He's still selective, but it's manageable." — Parent, Pinnacle Network
🌸 Pinnacle Blooms Network®
97%+ Measured Improvement | 20M+ Sessions

Red Flags — These Signs Mean It's Time for Professional Feeding Evaluation. Don't Wait.
🔴 Act Within 2 Weeks
Fewer than 10–15 foods across all categories | Entire food groups absent | Gagging or choking — swallowing safety concern | Panic response (not just reluctance) to new foods | Growth concerns, weight plateau, underweight | Feeding tube history or failure-to-thrive | Child is getting worse over 8 weeks of structured approach
🟡 Consult Within 1 Month
No progress after 8 weeks of consistent home approach | Severe mealtime anxiety generalized to all food contexts | Child missing school or social events because of feeding challenges | Significant family stress affecting multiple members
Referral Path
- 📞 Call 9100 181 181 (FREE — 16 languages — 24x7)
- Request: Comprehensive Feeding Evaluation + Oral Motor Assessment
- Specialists involved: Feeding OT + Feeding SLP + Dietitian
- Assessment: Feeding history + Sensory processing + Oral motor + Nutritional analysis
E-451 Is One Technique in a Comprehensive Feeding Therapy Journey.
E-449
Oral Motor Foundations for Feeding — Foundational prerequisite
E-450
Sensory Processing + Eating — Foundational prerequisite
📍 E-451
You Are Here: Extreme Picky Eating — Core technique
E-452
Mealtime Behavior Challenges — Core next step
E-453+
Transition to Family Meals → Self-Feeding → School Eating Refusal
Domain A — Sensory
Sensory processing techniques — foundational connections to feeding progress
Domain B — Communication
Oral motor techniques for feeding — SLP-led lateral domain
Domain C — Emotional Regulation
Mealtime anxiety management — critical co-domain for feeding work
Domain D — Behavioral
Positive reinforcement for feeding — ABA-led lateral domain

Extreme Picky Eating Is One Node in Your Child's Full Developmental Journey.
A: Sensory
B: Social Comm
C: Emotional Reg
D: Behavioral
E: FEEDING ← You
F–L: More Domains
You're working on Domain E — Feeding & Nutrition — Technique E-451. This domain connects to Domain A (Sensory Processing), Domain C (Emotional Regulation), and Domain D (Behavioral). Progress in feeding often accelerates when these adjacent domains are addressed simultaneously.
GPT-OS® Personalization: Your child's AbilityScore® integrates feeding progress with all 12 domains to generate a converged developmental profile — showing not just feeding readiness but overall developmental trajectory and priority intervention sequence.

Families Who've Walked This Path — In Their Own Words.
"My daughter ate 6 foods. The same 6. For three years. Our feeding therapist introduced divided plates and tiny tasting dishes and said 'we're not going to ask her to eat anything new for three months.' Month 4, my daughter tasted watermelon. She's now at 28 foods. I cried for an hour."
— Mother of a 7-year-old, Chennai | Outcome: 6 → 28 food repertoire over 11 months
"The food chaining approach changed everything. We started with his one safe brand of cracker. Three months later he eats four different types of crackers, plain rice cakes, and we're working toward toast. It sounds small. For us it's miraculous."
— Father of a 5-year-old with ASD, Hyderabad | Outcome: Food repertoire expanding via systematic chaining
"What nobody told me was that stopping pressure makes things better. The feeding therapist said 'put the food in front of him and walk away.' The change in his mealtime anxiety was immediate. Now we actually have peaceful dinners."
— Parent, Bangalore | Outcome: Mealtime anxiety reduced within 2 weeks of pressure removal
Illustrative cases. Individual outcomes vary by child profile, underlying factors, and intervention consistency.
🌸 Pinnacle Blooms Network®
97%+ Measured Improvement | 20M+ Sessions

You Don't Have to Figure This Out Alone.
🟢 FREE National Autism Helpline
9100 181 181 | 16+ languages | 24x7 | Talk to a feeding specialist today
🔵 Pinnacle Parent Community
pinnacleblooms.org/community | 70,000+ families | India's largest autism parent support network
🟡 WhatsApp Feeding Support Group
Daily Q&A with feeding therapists | Recipe swap for selective eaters | "First new food" celebration thread
🔴 Monthly Live Q&A
"Feeding Fridays" with Pinnacle OT + SLP feeding specialists | Free for registered families
For Therapists: Refer your client families to techniques.pinnacleblooms.org | Professional portal: pinnacleblooms.org/professionals
Preview of 9 materials that help with extreme picky eating Therapy Material
Below is a visual preview of 9 materials that help with extreme picky eating therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

When Home Programs Are Not Enough — Professional Feeding Therapy Is the Path.
When to Seek Professional Evaluation
- Fewer than 15–20 foods total
- Any growth or nutritional concern
- Gagging, choking, or swallowing difficulty
- Fear or panic response to foods
- Not improving after 8 weeks of structured home approach
- Significant family mealtime distress
Your Feeding Therapy Team
- 🔵Feeding OT — Sensory processing, oral sensory defensiveness, environmental modification
- 🟢Feeding SLP — Oral motor function, swallowing safety, texture progression
- 🟡Pediatric Dietitian — Nutritional assessment, supplement guidance, meal planning
- 🔴Dev. Pediatrician — Medical rule-outs, growth monitoring, diagnostic clarity
- 🟣Child Psychologist — Anxiety component, food phobia, family dynamics
Referral Path
- Call 9100 181 181 (FREE, 16 languages)
- Request: Feeding & Nutrition Assessment — Domain E
- First appointment: AbilityScore® + Feeding Screening
- Full evaluation: Comprehensive Feeding Evaluation + Oral Motor + Nutritional
Pinnacle operates 70+ centers across India with Feeding OT + Feeding SLP specialists.
🌸Consortium Seal: Validated by the Pinnacle Blooms Consortium — OT • SLP • ABA • SpEd • NeuroDev Pediatrics | 20M+ Sessions | 97%+ Measured Improvement | 70+ Centers | 70+ Countries Served
This content is educational. It does not replace individualized feeding evaluation and intervention from licensed feeding therapists, dietitians, and pediatricians. Children with growth concerns, nutritional deficiencies, or significant feeding difficulties need comprehensive evaluation by qualified professionals.
© 2025 Pinnacle Blooms Network® | Unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2