
Major Life Events — 30 Evidence-Based Interventions for Children with Autism
Houses move. Babies arrive. People die. Festivals happen. Hospitals are visited. Life doesn't pause for anyone — including children with autism. This subdomain equips caregivers, therapists, and educators with 30 structured, evidence-based interventions across the most significant life events children face.
Subdomain I2
Domain I: Transitions & Change
Pinnacle Blooms Network®
Why Major Life Events Hit Differently for Autistic Children
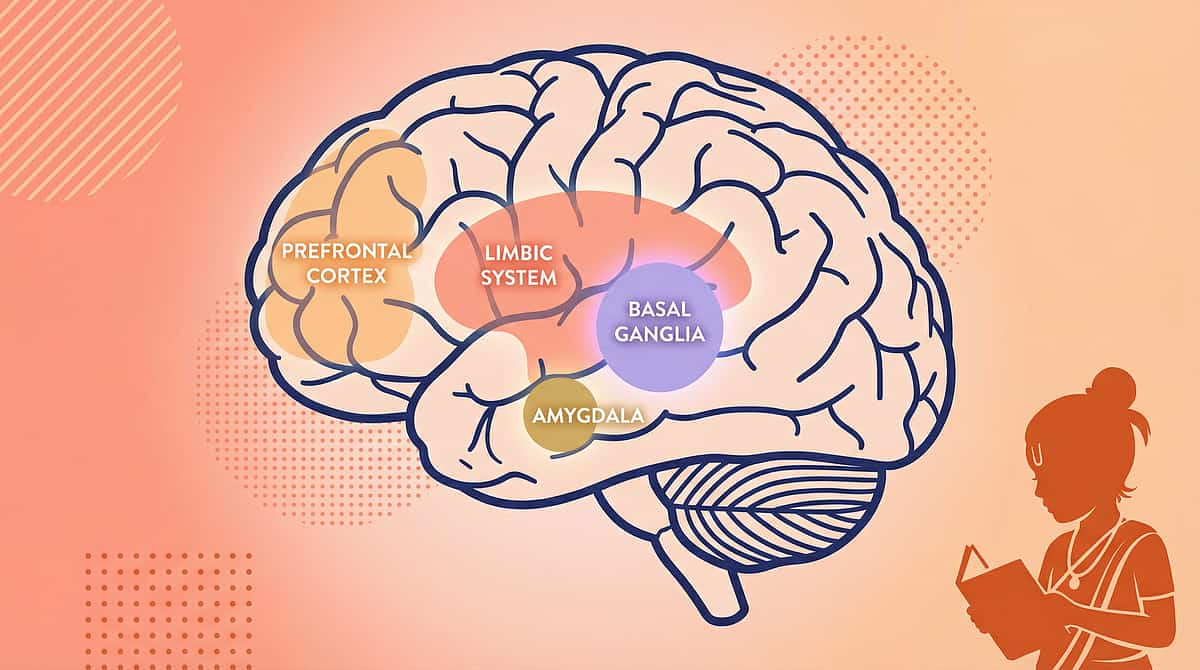
Major life events for children with ASD aren't simply "harder" — they are neurologically distinct experiences. While daily transitions disrupt one routine, a major life event can invalidate an entire system of routines simultaneously. Understanding the neuroscience behind this helps caregivers respond with precision and compassion.
🧠 Basal Ganglia
Major events erase the brain's entire automated routine library at once — every familiar path, object location, and sequence invalidated simultaneously.
⚡ Amygdala
Extended uncertainty over days or weeks sustains amygdala activation — producing chronic anxiety, sleep disruption, behaviour escalation, and skill regression.
💭 Prefrontal Cortex
Abstract concepts like permanence, causality, and temporality — central to death, divorce, and moving — must be made concrete for the ASD brain to process.
🌊 Limbic System
Intense emotions — grief, fear, excitement — may exceed regulation capacity and emerge through behaviour, sleep changes, eating shifts, or regression rather than words.

I-811 · House Moving
9 Materials That Help With House Moving
Moving house is the largest routine disruption possible — every room, every object, every sensory detail changes simultaneously. The child's entire spatial map must be rebuilt from zero. The hippocampus, which builds a detailed map of the home, is forced to start over while the basal ganglia's entire automated programme library is invalidated at once.
The 3-Month Timeline
- Show photos and videos of new house weeks before
- Visit the new home multiple times — explore each room
- Pack child's room LAST, unpack FIRST
- Bring familiar items immediately: bed, blanket, visual schedule, favourite toys
- Maintain same bedtime and schedule — routine is portable
Indian Context
Include the child in the pooja (housewarming ritual) — a culturally meaningful transition marker that gives the move a defined beginning and sacred anchor. For joint family moves, coordinate across all caregivers. Rented vs. owned transitions carry different emotional weights for families.
📊 Evidence Level I
NCAEP 2020 | Environmental transition research | PMC10955541

I-812 · New Baby Coming
9 Materials That Help With New Baby Coming
A sibling's arrival splits parental attention, increases household noise, disrupts routines with new feeding and sleep schedules, and fundamentally changes the child's position in the family. For an ASD child, baby crying — high-frequency, unpredictable auditory input — can be the most distressing sensory element of all.
Prepare Months Before
Use a social story about the new baby. Visit families with babies. Use dolls as practice. Describe what babies realistically do — cry, sleep, eat — not an idealised picture.
Protect the Child's Routine
Where possible, the baby adapts to the family routine — not the other way around. Schedule protected 1:1 parent time that remains consistent regardless of infant demands.
Noise Desensitisation
Record baby crying sounds and play at low volume, gradually increasing. This systematic desensitisation reduces the auditory shock when the baby arrives.

I-813 · Pet Death
I-814 · Family Member Death
Pet Death & Family Member Death
For many children with ASD, pets often represent their safest relationships—unconditional, non-verbal, predictable, and sensory-rich. Their death can be a child's first experience of loss and permanence. The death of a family member is an even more significant life event, simultaneously confronting the child with abstract concepts of death, grief they may lack vocabulary to express, and severe disruptions to their routines.
Pet Death
What to Say: Use concrete, honest language: "[Pet name] has died. Their body stopped working. They won't come back." Avoid euphemisms — "went to sleep" confuses sleep with death; "went away" implies return. Clarity is kindness.
Supporting Grief: Allow all forms of expression — crying, withdrawal, anger. Create a memorial: drawing, photo album, or planting a plant in the pet's memory. A weighted lap pad or soft toy with similar texture can provide sensory comfort.
Don't rush getting a new pet — allow time to grieve first.
Family Member Death
Telling the Child: "Thatha has died. His body stopped working. He cannot come back." Keep it simple. Repeat as often as needed.
What to Expect: Confusion, regression, behaviour changes, sleep disruption, repetitive questions. Grief may be delayed — appearing weeks or months after the death.
Indian Cultural Context: Prepare the child for cremation and funeral rituals — incense, crying adults, fire, crowds. The 13-day mourning period requires specific sensory and social preparation.

I-815 · Explaining Death
I-816 · Grief Processing
Explaining Death & Grief Processing
Explaining death to a child with ASD requires concrete language and consistent repetition across four abstract concepts (irreversibility, universality, nonfunctionality, causality). Grief in ASD looks different — the child may not cry, may continue playing, may seem unaffected — but is processing through behaviour and sensory channels.
EXPLAINING DEATH
Language to USE
- "Died"
- "Body stopped working"
- "Won't come back"
- "Not alive anymore"
Language to AVOID
- "Went to sleep" — creates fear of sleep
- "Lost" — implies they can be found
- "Went away" — implies possible return
- "God took them" — potentially frightening
For repetitive questions, answer the same way each time — consistency reduces anxiety.
In families with reincarnation beliefs: "Will Thatha come back as someone else?" needs a thoughtful, honest answer.
GRIEF PROCESSING
- Recognise ASD Grief: Look for behaviour changes — regression, increased stimming, sleep disruption, appetite changes, withdrawal — rather than waiting for tears.
- Support Through Routine: Maintaining the child's daily routine is the single most stabilising action during grief.
- Memory Preservation: Create a photo book, memory box, or regular "remembering" time.
- When to Seek Help: Seek professional support if grief interferes with daily functioning for 3+ months, if self-harm appears, or if regression is extreme.
I-817 · Divorce
9 Materials That Help With Divorce
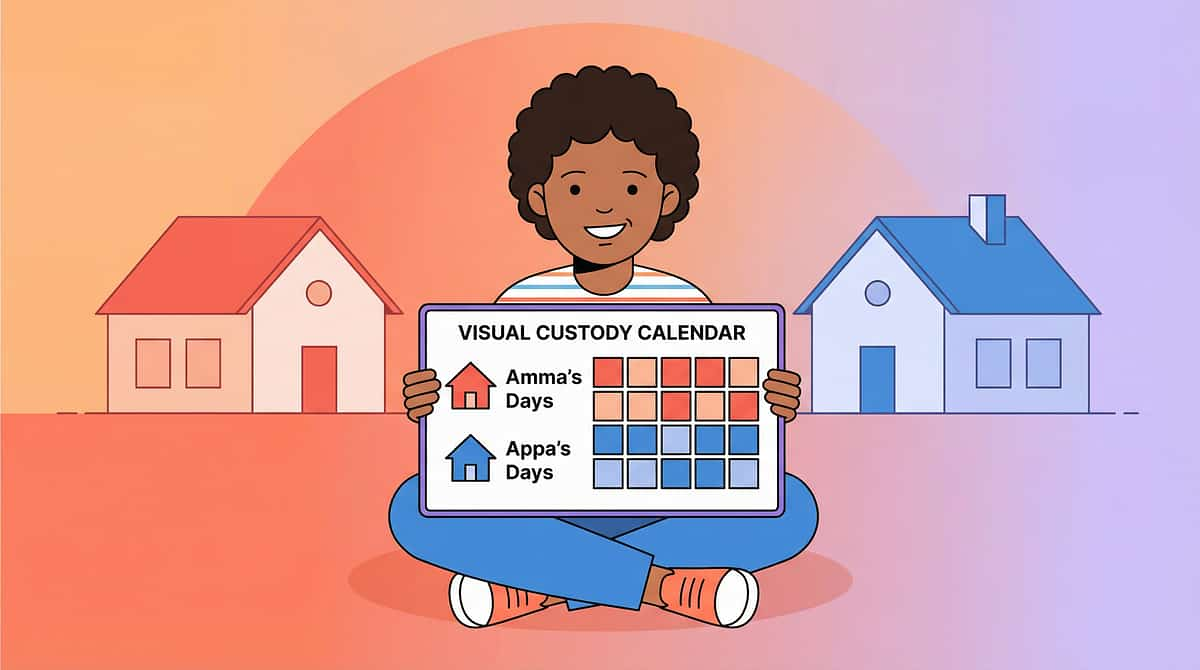
Parents separating creates disruption through every channel: two homes with different rules, custody schedules, emotionally compromised adults, and the abstract confusion of "Why? Is it my fault?" For a child with ASD, the most destabilising element is routine fragmentation — the when and where of daily life fundamentally changes.
What to Say
Use concrete, simple, repeated language: "Amma and Appa will live in different houses. You will live with Amma on [days] and Appa on [days]. We both love you. This is NOT your fault." A visual custody calendar showing which days with which parent is essential.
Consistency Between Homes
The greatest gift separated parents can give their child: the same visual schedule format, the same behaviour approach, and the same bedtime routine across both homes. Consistency of strategy matters more than consistency of location.
Indian Context
Navigate divorce stigma and joint family involvement sensitively. Ensure therapy continuity across both homes and custody arrangements. Never involve the child in adult conflict — their emotional safety is paramount.

I-818 · Parent Illness
9 Materials That Help With Parent Illness
When the primary caregiver is ill, the child loses their anchor. Young children with ASD depend on parental co-regulation — borrowing the parent's calm nervous system to regulate their own. When that system is compromised, dysregulation escalates at precisely the moment when the household can least manage it.
Concrete Explanation
"Amma is sick. Her body needs rest to get better. [Other caregiver] will help you today." Simple, honest, and reassuring.
The Backup Plan
Identify a secondary caregiver in advance who knows the child's full routine, strategies, and triggers — trained BEFORE illness strikes, not during it.
Written Routine
A detailed daily schedule that any caregiver can follow independently. Written, visual, and always accessible — not stored only in the primary caregiver's memory.
Child's Role
Give the child a simple, concrete task: "You can bring Amma water." Active participation reduces helplessness and maintains a sense of competence and connection.
I-819 · Family Hospitalization
I-825 · Hospital Preparation
Family Hospitalization & Hospital Preparation
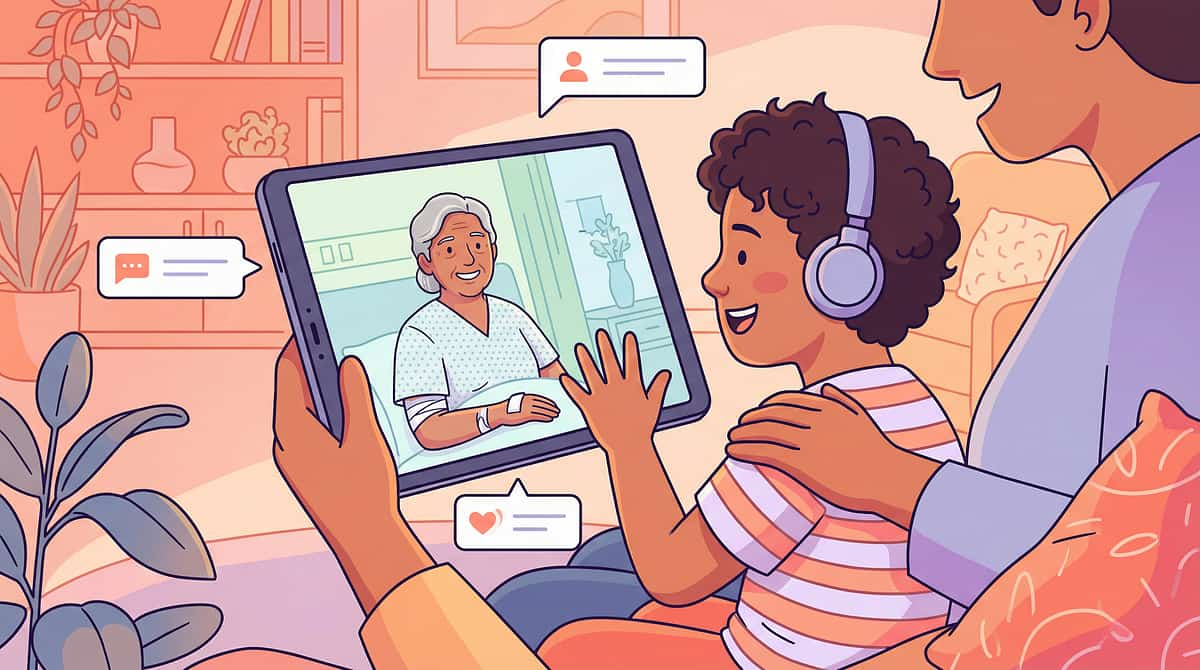
Hospital events hit children with ASD from two angles — when a family member is hospitalized (dual disruption: person absent + adults emotionally compromised), and when the child themselves must attend hospital (sensory nightmare: bright lights, antiseptic smells, alarming sounds, strangers touching the body, long waits).
FAMILY HOSPITALIZATION
- Concrete Explanation: "[Person] is in the hospital. Doctors are helping them. They will come home when they are better." Repeat as needed.
- Routine is the Priority: The child's routine continues regardless of the hospitalization — the single most stabilising action.
- Hospital Visits: Prepare with a social story. Keep visits short. Prepare for antiseptic smell, monitoring equipment sounds, IV lines. A video call can maintain connection without the sensory burden.
- Indian Hospital Context: Crowded government hospitals, family members as primary caregivers, varying private hospital rules all require specific preparation.
HOSPITAL PREPARATION
- Pre-Visit Preparation: Social story about the hospital visit. Photos of the specific hospital. Age-appropriate video of the procedure. Play-acting with a toy medical kit. Describe what it will smell, look, and feel like before arrival.
- Comfort Kit: Headphones, fidget tool, comfort toy, preferred snack, visual schedule of the visit. Tell medical staff: "My child has ASD. Please show rather than just tell. They may need extra time to process."

I-820 · Natural Disasters
9 Materials That Help With Natural Disasters
Earthquake. Flood. Cyclone. Extended power outage. Natural disasters are the ultimate unexpected transition — zero preparation time, maximum environmental disruption, extreme sensory input, and sustained uncertainty. Every safety signal the child depends on may be disrupted simultaneously.
01
Prepare in Advance
Build an emergency bag with the child's essentials: medication, sensory tools, comfort item, visual schedule, snacks, headphones, and favourite toy. Pre-teach a social story: "Sometimes Emergencies Happen."
02
During the Event
Stay calm — your regulation IS the child's regulation. Provide sensory comfort. Maintain as much routine structure as possible. Explain simply: "There is a storm. We are safe here."
03
After the Disaster
Rebuild routine FIRST before addressing anything else. Expect regression — it is a normal nervous system response. Seek professional support if trauma symptoms persist beyond two weeks.
I-821 · Emergency Situations
9 Materials That Help With Emergency Situations
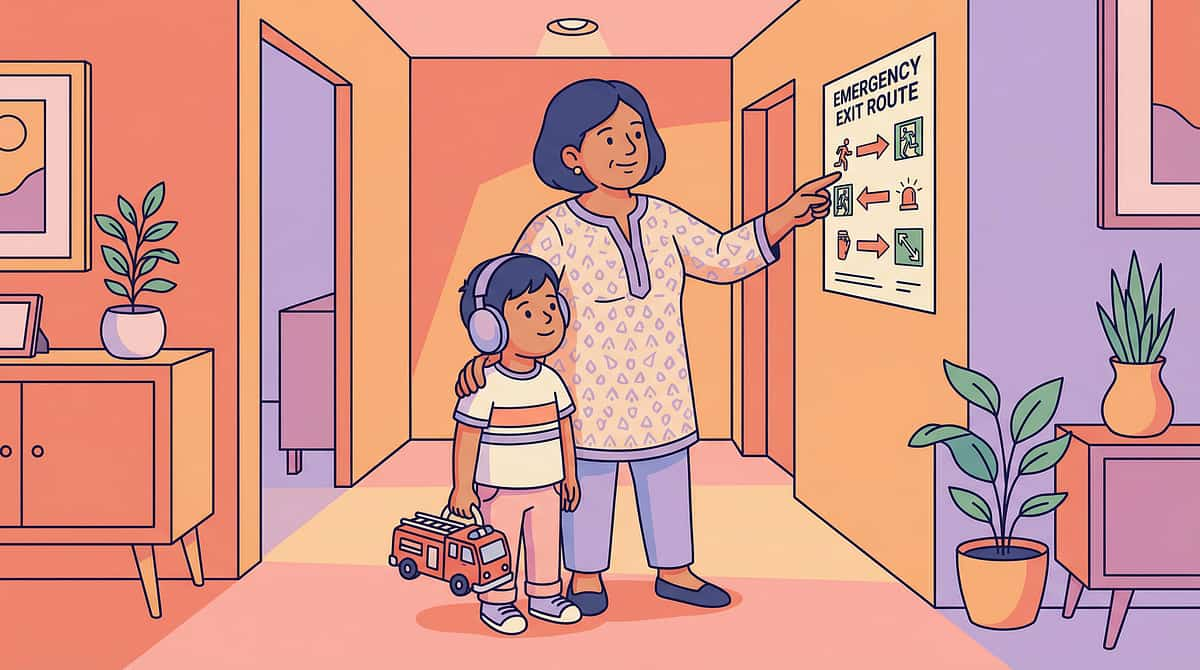
Fire alarm. Medical emergency. Accident. Police siren. Emergencies demand immediate action — but children with ASD may freeze, bolt, meltdown, or fail to understand the urgency. In ASD, the amygdala's fight-flight-freeze response may produce atypical reactions. Emergency response must be practised like any other skill — not assumed to be instinctive.
Monthly Fire Drill
Practice at home until the evacuation route becomes automatic. Basal ganglia automation means the body knows what to do even when the PFC is overwhelmed by fear.
Emergency ID
The child carries identification at all times: name, diagnosis, parent phone number, address. Medical ID bracelet or laminated card in pocket — always.
Emergency Script
Rehearse a minimal-word, maximum-clarity verbal cue: "FIRE. We go OUTSIDE. NOW." Simple, consistent, repeated until automatic.
School Emergency Plan
Inform school of the child's likely emergency response (freeze, bolt, or meltdown). Identify an aide or buddy for drills. Don't wait for an actual emergency to discover gaps.

I-822 · Sudden Routine Loss
9 Materials That Help With Sudden Routine Loss
COVID lockdown. School closure. Therapist resignation. Extended power cut. Domestic help leaving suddenly. When the schedule a child depends on disappears without warning, the basal ganglia's entire programme library is invalidated — not one routine disrupted, but all routines simultaneously. The COVID pandemic demonstrated this at global scale for ASD families.
Immediate Action (24 Hours)
Create a NEW temporary routine within 24 hours of the disruption. Structure matters more than perfection at this stage. Even a rough schedule — wake → breakfast → activity → snack → activity → lunch → rest → activity → dinner → bed — provides the scaffolding the nervous system needs.
Anchor Points
Maintain consistent wake time, bedtime, and mealtimes even when everything between them changes. These three daily anchors are the skeleton of any emergency routine. Communicate the change visually: "Things are different right now. Here is our new plan."
Indian Context
Families who had emergency routine protocols in place during COVID recovered faster. Festival schedule disruptions, bandh closures, and strike days are opportunities to practise emergency routine activation before a true crisis arrives.

I-823 · Building Resilience
9 Materials That Help Building Resilience
Resilience is not the absence of distress — it is the capacity to return to baseline after distress. It is a neural capacity: PFC recovery speed, amygdala habituation, and vagal tone. Resilience builds through supported exposure to manageable stress, successful recovery experiences, and the security of a safe attachment base.
Secure Relationship
A safe base — a trusted adult who provides co-regulation and unconditional support — is the foundation of all resilience. Without it, no other strategy builds effectively.
Coping Toolkit
Regulation strategies from Domain C, always accessible. The calm-down kit, the breathing script, the sensory tool — practised in calm moments so they're available in hard ones.
Success History
A portfolio of challenges survived. Explicitly reference past resilience: "Remember when the power went out and you used your calm-down kit? You handled it." Evidence of past success builds confidence for future challenges.
Resilience ≠ not being upset. Resilience = being upset AND recovering. Honour the distress while building the return.

I-824 · Preparing for the Unexpected
9 Materials That Help Preparing for the Unexpected
The paradox: preparing for what you can't prepare for. You cannot predict which unexpected event will arrive — but you can build general preparedness: flexible thinking, change tolerance, emotional regulation toolkit, and a "change happens" acceptance framework. This is meta-preparation: not for specific events, but for the capacity to handle any event.
🎒 "Change Happens" Toolkit
Calm-down kit (always accessible), change card (visual signal that the plan is different), social story library pre-made for common unexpected events, and a rehearsed coping script: "This is different. I can handle different. I'll use my tools."
🎲 Weekly Surprise Practice
Introduce planned surprises at low stakes — different breakfast, new route to the park, unexpected activity. Build the cognitive flexibility muscle in safe, manageable doses so it's available when life demands it.
🧳 Emergency Essentials Bag
Always packed: sensory tools, comfort item, medication, ID, visual schedule template. Ready to go at any moment — because unexpected events don't provide packing time.
I-826 · Surgery Preparation
I-827 · Travel Preparation
Surgery Preparation & Travel Preparation
Surgery is the highest-anxiety medical event — anaesthesia, unfamiliar operating room, separation from parents, post-operative pain. Travel combines extended sensory confinement, schedule disruption, a new destination, and an unfamiliar bed. Both require systematic graded preparation weeks in advance.
1
SURGERY PREPARATION
Graded Exposure (start 2–4 weeks before):
- Look at pictures of hospital
- Visit waiting room
- Sit in exam chair
- Open mouth for inspection
- Allow instruments to touch
- Brief procedure
- Full appointment
Day-Of Plan:
- Visual schedule for the entire day.
- Comfort item through to pre-op.
- Request parent presence until anaesthesia is administered.
Post-Operative Recovery:
- Pain management is critical — child may not communicate pain verbally.
- Use a visual pain scale.
- Return to routine as quickly as medically possible.
- Watch for signs of medical PTSD.
2
TRAVEL PREPARATION
Before Travel:
- Social story
- Photos and video of destination
- Visual schedule for travel day
- Pack sensory and comfort kit
- Build activity rotation bag
At Airport/Station:
- Pre-visit if possible.
- Arrive early — never rush.
- Prepare for crowd, announcements, and security queue specifically.
During Journey:
- 10-minute activity rotation cycles.
- Snacks as regulation anchors.
- Headphones for noise management.
On Arrival:
- Explore the new space before any demands are placed.
- Set up familiar items first.
I-828 · Vacation Adjustment
I-829 · Holiday Preparation
Vacation Adjustment & Holiday Preparation
The vacation paradox — the event designed for family joy can be the child's most stressful sensory-routine experience. School holidays remove 6–8 hours of daily structured time. For children with ASD, school IS the routine — remove it and the day becomes unstructured, unpredictable, and endless. Both require proactive structure.
1
VACATION ADJUSTMENT
The Portable Routine
The visual schedule travels with the family. Mealtimes and bedtime are maintained. A vacation visual schedule is created for each day — even on holiday, knowing what comes next is essential for regulation. Schedule daily downtime: no wall-to-wall activities.
Destination Matching
Choose destination based on the child's current tolerance: quiet over chaotic, familiar over exotic, short over long. Hill stations, trusted relative homes, and familiar domestic locations are excellent starting points. Day 1 and 2 are always the hardest — expect difficulty and stay the course.
2
HOLIDAY PREPARATION
Holiday Visual Schedule
Structured but relaxed: wake → breakfast → activity → snack → outing → lunch → rest → activity → free time → dinner → bedtime. Visual, posted, consistent.
Anchor Points
Same wake time (±30 minutes), same bedtime, same mealtimes. These three anchors hold the structure even when everything between them changes.
Holiday Activities
Continue therapy where possible. Graded outings, skill-building (cooking, swimming), structured play dates, and dedicated special interest time.
Screen Management
Set holiday screen time limits BEFORE the holiday begins — not reactively during it. A written agreement posted on the visual schedule works far better than verbal limits during boredom.

I-830 · Festival Overwhelm
9 Materials That Help With Festival Overwhelm
India's festivals are sensory spectacles — and for a child with ASD, they can be magical or traumatic depending on preparation. Festival overwhelm occurs when disrupted routine, extreme sensory input, social demands, late nights, and emotional intensity combine to exceed the child's processing capacity. Multi-day festivals compound: each day starts from a higher baseline of exhaustion than the last.
Prepare Specifically
Create a social story for each individual festival — Diwali preparation differs entirely from Holi preparation. Describe what it will look, sound, smell, and feel like. Provide a visual schedule for the festival day and identify the escape plan before arriving.
Participation Grading
Watch from distance → brief participation → extended participation → full participation. Never force full participation as the starting point. Let the child determine their comfort level and expand from there.
Recovery Day
The day after a major festival is a low-demand day — always. Recovery time is not optional; it is part of the festival preparation plan itself.

I-831 · Diwali Preparation
9 Materials That Help With Diwali Preparation
Diwali is THE festival event for Indian families — and the most sensory intense. Firecrackers (sudden, unpredictable, 80–120 dB), diyas and lights (flickering visual load), sweets distribution (social interaction and food novelty), new clothes (tactile change), visitors (social demand), and late nights (routine disruption). It requires the most specific and detailed preparation of any festival.
Firecracker Strategy
Begin desensitisation weeks before using recorded firecracker sounds at gradually increasing volume. Noise-cancelling headphones are mandatory on Diwali night. An indoor celebration option must always be available.
Joyful Participation
Rangoli (tactile and creative — many ASD children love this), diya lighting with supervision, and sweet distribution as structured social practice. Let the child lead their level of engagement.
Clothing Preparation
Try on new clothes multiple times in the weeks before Diwali. Choose comfortable, familiar fabrics. The sensory surprise of new clothing on an already overwhelming night can be the tipping point into meltdown.
Family Communication
"Our child needs headphones and may go inside during crackers. Please don't force participation." Advocate clearly, warmly, and in advance — not in the moment of crisis.

I-832 · Holi Preparation
9 Materials That Help With Holi Preparation
Holi presents unpredictable tactile contact — colour thrown, water splashed, people approaching to smear colour — all without consent. For a tactile-defensive child, Holi may be the most aversive day of the year. For a tactile-seeking child, it may be a sensory paradise. Knowing your child's sensory profile completely determines the approach.
Tactile-Defensive Child
- Stay indoors during community Holi celebrations
- Family-only celebration with full consent from the child
- Organic or herbal colours only — gentler on sensitive skin
- One trusted person applies colour if the child agrees
- Immediate wash option always available
Tactile-Seeking Child
- Supervised participation with organic colours
- Set a clear time limit before starting
- Establish a wash routine for after play
- Practice the "No thank you" phrase for declining colour from strangers
Family Advocacy
When family says "Let them play!" — respond: "Forced sensory input is harmful, not fun. We celebrate in the way that works for our child."

I-833 · Birthday Parties
9 Materials That Help With Birthday Parties
Birthday parties are the social-sensory endurance event: loud music, unpredictably popping balloons, a crowd of children, structured games with complex rules, food anxiety, the expectation to appear joyful, and — if it's the child's own birthday — being the centre of unwanted attention for hours at a time.
Own Birthday: Child-Led
Small guest list the child approves. Preferred activity as the party format. Familiar, sensory-friendly venue. Visual schedule for the party. An identified escape space available. The child's comfort defines the party — not social expectation.
Others' Birthday: Prepared Entry
Preparation includes who, where, when, and what activities. Arrive early before the crowd builds. Parent stays throughout. Headphones available. Clear exit plan: "If it's too much, we leave — no shame, no negotiation."
Balloon Phobia
Balloon phobia is common in ASD — the unpredictable POP triggers extreme startle responses. Warn in advance, avoid seating near balloons, or choose balloon-free venues where possible.

I-834 · Wedding Attendance
9 Materials That Help With Wedding Attendance
Indian weddings are multi-day sensory marathons: mehndi, sangeet, ceremony, and reception — each event hours long, with 100+ dB music, hundreds of guests, new clothes every day, late nights, and continuous social demands. Cumulative overload compounds daily, with each day starting from a higher baseline of exhaustion than the last.
Selective Attendance
Don't attend everything. Choose 1–2 events — ceremony plus reception, skipping sangeet if it is too loud. Arrive late and leave early: attend the core moments, skip the extended waiting.
Sensory Kit in the Bag
Headphones, fidget tool, comfort item, preferred snack. Identify a quiet space in advance — the car, a corridor, a side room — before the event begins, not during a meltdown.
Clothing Strategy
Comfort over tradition: familiar fabric, tried-on multiple times before the event. One greeting phrase rehearsed: "Namaste aunty/uncle." That is sufficient and valid social participation.
Family Advocacy
When family pressure to attend everything arrives: "We'll come for the ceremony for one hour. That's what works for our child." Clear, warm, non-negotiable.

I-835 · Family Gatherings
9 Materials That Help With Family Gatherings
Festival dinners, Sunday family lunches, relative visits. Family gatherings combine social demands (conversation, affection expectations, questions about the child), variable sensory loads (cooking smells, noise, crowd), and the most anxiety-producing element of all: uncertain duration. "When are we leaving?" "Soon" — the most unhelpful answer a child with ASD can receive.
Before Arriving
Use photos to preview who will be there. Confirm the location. Provide a concrete timeline: "We'll stay for lunch and leave after — about two hours." This single piece of information can transform the entire experience for the child.
The Child's Space
Identify a quiet room or corner at the gathering location before entering. The child knows: "When I need a break, I go here." This exit option reduces anxiety for the entire visit.
Family Education Script
"He may not make eye contact or hug. Please don't force it. He says hello in his own way." Brief, warm, clear. Delivered to key relatives in advance — not reactively during the gathering.
The Exit Signal
An agreed signal between parent and child: "Show me the red card and we leave in ten minutes." The child has agency; the parent has warning. Both feel safer.

I-836 · Restaurant Visits
I-837 · Mall Visits
Restaurant Visits & Mall Visits
Community outings — restaurants and malls — combine auditory load, olfactory challenge, crowd density, visual overload, and social expectations simultaneously. Both require the same core strategy: off-peak timing, sensory preparation, a clear purpose, and a planned exit.
Restaurant Visits
Off-Peak Timing
Visit during quiet hours — weekday mornings or early lunch. Sit in a corner or booth, away from the kitchen and speaker system.
Activity Bag for Waiting
Waiting is the hardest part. Prepare a dedicated activity bag: fidget tools, a small colouring book, a preferred tablet game. Order the moment you sit down.
Food Strategy
Start with familiar restaurants. Bring preferred food to supplement menu items if needed. South Indian restaurants and familiar chains are excellent starting points in India.
Mall Visits
Quiet Hours Strategy
Weekday mornings are a different environment from weekend afternoons. Go with a specific purpose — "We're going to buy shoes" — not open-ended browsing. Set a 30-minute time limit initially and extend as tolerance builds.
What to Avoid First
The food court is the most overwhelming section. Avoid during sale season. Peak hours on weekends require full sensory protection before entry.
Sensory Breaks
Identify a quiet bench or corner in advance. Schedule sit-down breaks every 15 minutes initially. Headphones for noise management throughout the visit.

I-838 · Temple Visits
9 Materials That Help With Temple Visits
Temple, mosque, gurudwara, and church visits are deeply important in the daily and weekly life of many Indian families. Each religious space carries a unique and intense sensory profile: incense and camphor (olfactory), bells and chanting echoing in enclosed stone spaces (auditory), crowd contact and floor sitting (tactile and proprioceptive), and specific ritual sequences of behaviours expected from the child.
Temple Sensory Profile
- Olfactory: Incense, camphor, flowers — among the most intense smells in any environment
- Auditory: Bells, chanting, crowd — amplified by stone architecture
- Tactile: Crowd contact, bare feet on stone, water at the entrance
- Behavioural: Folding hands, accepting prasad, sitting, standing — specific ritual expectations
Preparation Strategy
Social story: "When We Go to the Temple." Visit during early morning on weekdays — the quietest times. Start with darshan and leave (brief, purposeful) before extending duration. Practice ritual gestures at home before the visit. Stand at the back or side to reduce crowd contact.
Respect + Accommodation
Modified participation is full participation. "We worship in our way" — the child's presence and engagement, however it looks, is valid and meaningful.
I-839 · Doctor Appointments
9 Materials That Help With Doctor Appointments
Regular doctor visits involve a waiting room (long, crowded, unpredictable), an examination by a stranger touching the body (stethoscope cold against skin, blood pressure cuff squeezing, tongue depressor triggering gag reflex), and the fundamental unpredictability of what the doctor might do next. Anticipatory anxiety activates the amygdala before the visit has even begun.
Before the Visit
Social story about the doctor visit. Play with a toy medical kit at home — practise being the patient and the doctor. Show a photo of the specific doctor if possible. Early morning appointments mean the shortest wait times.
During the Examination
Parent holds the child throughout. Explain every step immediately before it happens: "Doctor will listen to your chest with this. It will feel cold." Allow the child to touch each instrument first. Never surprise.
Communication to the Doctor
"My child has ASD. Please explain before touching. They may need extra time and may not follow verbal instructions. Please show rather than just tell." Most doctors respond positively to clear, specific guidance.

I-840 · Dental Appointments
9 Materials That Help With Dental Appointments
Dental visits are the most feared medical appointment for ASD families — and neurologically, this makes complete sense. The mouth is the most sensory-dense region of the body. Dental work assaults oral, auditory, visual, tactile, proprioceptive, and vestibular channels simultaneously. The drill's high-pitched, unpredictable sound is the single most-reported dental fear trigger for children with ASD.
Begin this programme six months before the first dental visit. Each step is mastered and feels comfortable before advancing to the next. Rushing the hierarchy to meet appointment schedules undermines the entire approach.
Finding the Right Dentist
Seek a paediatric dentist with specific SEN (Special Educational Needs) experience. Ask directly: "Do you have experience with autistic children?" A dentist who understands ASD will adjust pace, explanation, and sensory accommodation automatically. Pinnacle Blooms can recommend ASD-friendly dental networks across India.
Sedation Options
For essential procedures where desensitisation isn't yet complete or sufficient, discuss sedation options with your dentist and paediatrician. Sedation is a valid and compassionate clinical choice — not a failure. Pain-free dental experiences in childhood build a lifetime of dental health cooperation.
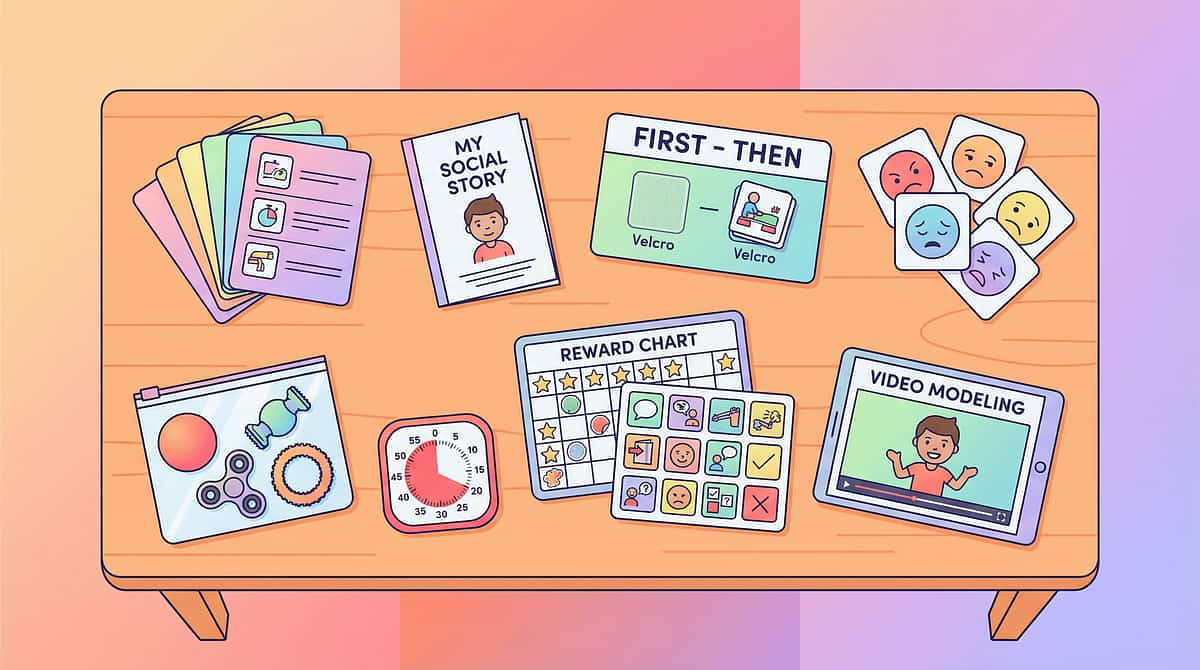
The 9 Canon Materials — Supporting Every Technique
Every intervention in Subdomain I2 draws from the same nine foundational materials. These are the core tools that make abstract events concrete, unpredictable moments structured, and overwhelming experiences manageable. Build your toolkit once — deploy it across every life event.
Visual Schedule
The portable routine that travels to every event
Social Stories
Narrative preparation for every major life event
First-Then Board
Contingency visuals that make sequences predictable
Emotion Cards
Feelings vocabulary for experiences that exceed words
Calm-Down Kit
The always-accessible self-regulation toolkit
Visual Timer
Time made concrete for transitions and durations
Reward Charts
Motivation and acknowledgment across all events
Communication Board
Low-tech AAC for environments that overwhelm verbal output
Video Modeling
Preview of unfamiliar environments and situations
The Subdomain I2 Map — All 30 Techniques
Every technique in this subdomain is linked to a dedicated 40-card page with full intervention protocols, downloadable materials, and session-ready resources for therapists, educators, and families.
# | Code | Technique | Section | |
01 | I-811 | House Moving | Family Changes | |
02 | I-812 | New Baby Coming | Family Changes | |
03 | I-813 | Pet Death | Family Changes | |
04 | I-814 | Family Member Death | Family Changes | |
05 | I-815 | Explaining Death | Family Changes | |
06 | I-816 | Grief Processing | Family Changes | |
07 | I-817 | Divorce | Family Changes | |
08 | I-818 | Parent Illness | Family Changes | |
09 | I-819 | Family Hospitalization | Crisis & Resilience | |
10 | I-820 | Natural Disasters | Crisis & Resilience | |
11 | I-821 | Emergency Situations | Crisis & Resilience | |
12 | I-822 | Sudden Routine Loss | Crisis & Resilience | |
13 | I-823 | Building Resilience | Crisis & Resilience | |
14 | I-824 | Preparing for Unexpected | Crisis & Resilience | |
15 | I-825 | Hospital Preparation | Medical & Travel | |
16 | I-826 | Surgery Preparation | Medical & Travel | |
17 | I-827 | Travel Preparation | Medical & Travel | |
18 | I-828 | Vacation Adjustment | Medical & Travel | |
19 | I-829 | Holiday Preparation | Medical & Travel | |
20 | I-830 | Festival Overwhelm | Medical & Travel | |
21 | I-831 | Diwali Preparation | Cultural Events | |
22 | I-832 | Holi Preparation | Cultural Events | |
23 | I-833 | Birthday Parties | Cultural Events | |
24 | I-834 | Wedding Attendance | Cultural Events | |
25 | I-835 | Family Gatherings | Cultural Events | |
26 | I-836 | Restaurant Visits | Community Outings | |
27 | I-837 | Mall Visits | Community Outings | |
28 | I-838 | Temple Visits | Community Outings | |
29 | I-839 | Doctor Appointments | Community Outings | |
30 | I-840 | Dental Appointments | Community Outings |

Evidence Base & Research Foundations
Every intervention in Subdomain I2 is grounded in peer-reviewed research and evidence-based practice frameworks. The following sources underpin the clinical rationale across all 30 techniques.
NCAEP 2020
National Clearinghouse on Autism Evidence and Practice — the primary evidence classification framework used across all 30 techniques. All interventions rated Level I.
PMC10955541
Peer-reviewed environmental transition research supporting the neurological basis for major life event disruption in ASD populations.
Bereavement in ASD
Specialist research on grief processing, bereavement responses, and death comprehension in children with autism spectrum disorder.
Trauma-Informed Care
WHO NCF 2018 trauma-informed frameworks applied to medical preparation, emergency response, and crisis intervention for neurodivergent children.
📊 All 30 Techniques: Evidence Level I
21M+ Sessions
GPT-OS® Powered
Preview of major life events Therapy Material
Below is a visual preview of major life events therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.
Link copied!
Life Is Coming. Here's How We Face It Together.
Major life events don't wait for readiness. Houses move, babies arrive, people die, festivals happen, teeth need cleaning. The child cannot be shielded from life — they must be prepared for it.
Every social story, every sensory kit, every visual schedule in this subdomain is a tool that says: "Life is coming. Here's how we face it together." A child who can transition can go to school, visit family, celebrate festivals, survive loss, travel the world, and grow into an adult who handles what life brings. That's the gift of transition support: not just smoother days — but a bigger life.
30
Techniques
One for every major life event
9
Materials Per Technique
Canon toolkit, always accessible
21M+
Sessions
Across the Pinnacle Blooms Network®
60
Domain I Techniques
I1 Daily Transitions + I2 Major Life Events