




Study | Finding | Grade | |
PRISMA Systematic Review (2024) — 16 studies | Sensory-based feeding interventions classified as evidence-based practice for ASD | Level I | |
Meta-analysis, World J Clin Cases (2024) — 24 studies | Sensory/motor interventions effectively promote adaptive behavior and self-care | Level II | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based interventions demonstrate significant outcomes in Indian pediatric populations | Level II | |
ASHA/AOTA Clinical Practice Guidelines | Graduated cup training with oral motor support is standard feeding therapy protocol | Consensus | |
NCAEP EBP Report (2020) | Visual supports and structured task instruction evidence-based for ASD populations | Level I |

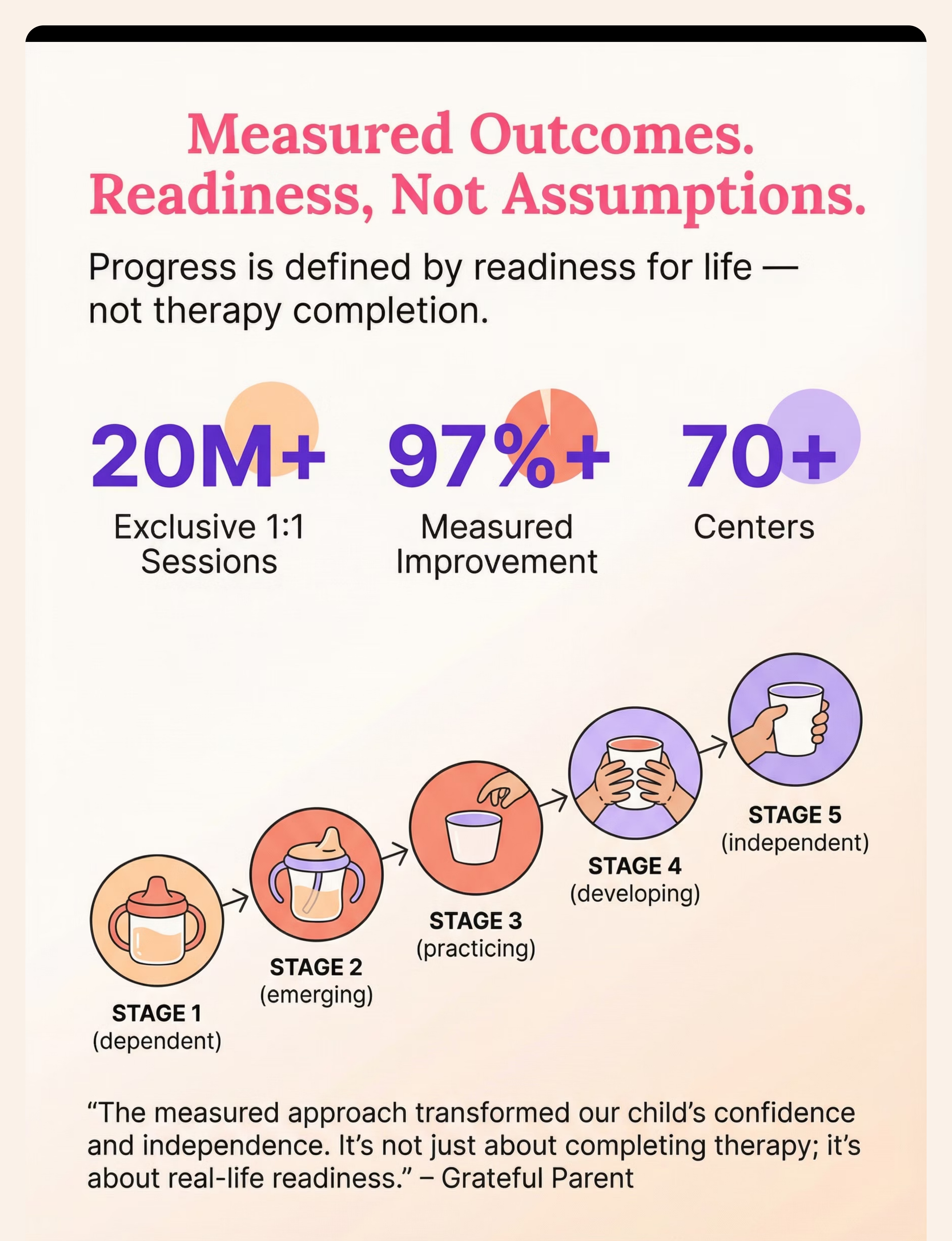
Target | Child can do this when mastered | |
Lip closure | Drinks without liquid leaking from sides of mouth | |
Jaw grading | Does not flood or bite rim; opens appropriate amount | |
Flow anticipation | Stops tipping as liquid approaches; no flooding | |
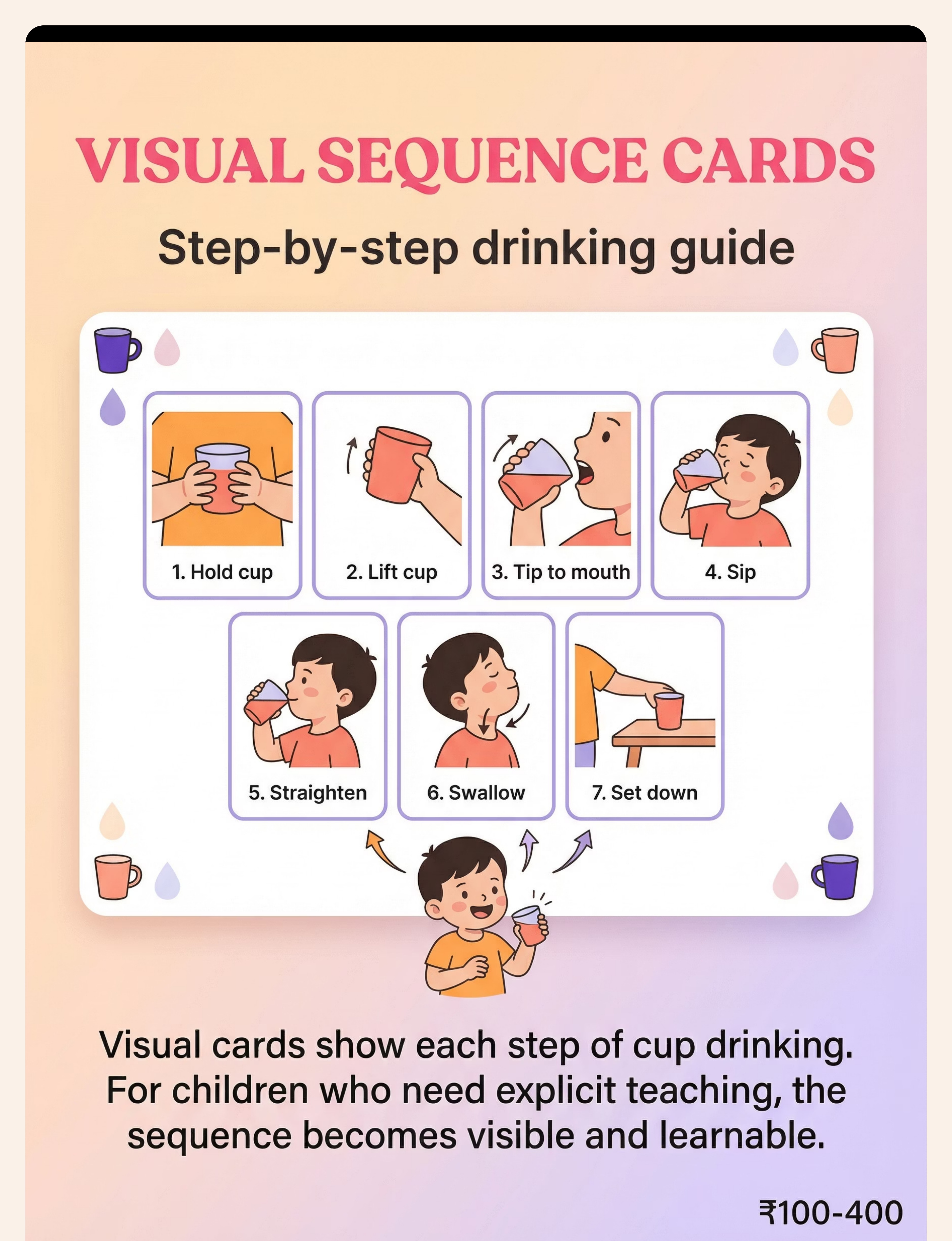
Motor planning | Completes all 7 steps in sequence without reminders | |
Coordination | No coughing or choking during drinking | |
Independence | Drinks from open cup across home, school, restaurants |





Every Family, Every Budget: DIY & Substitute Options
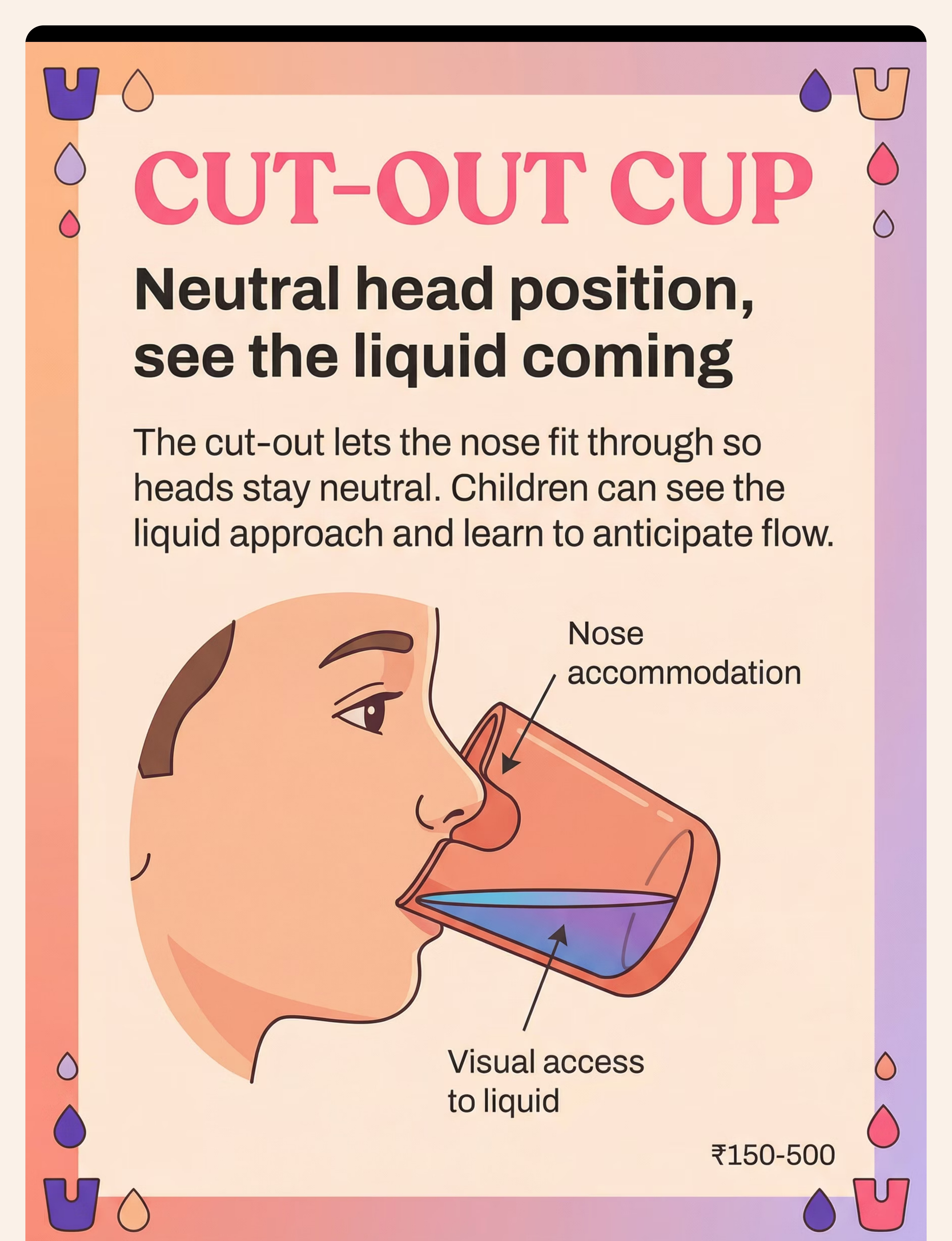
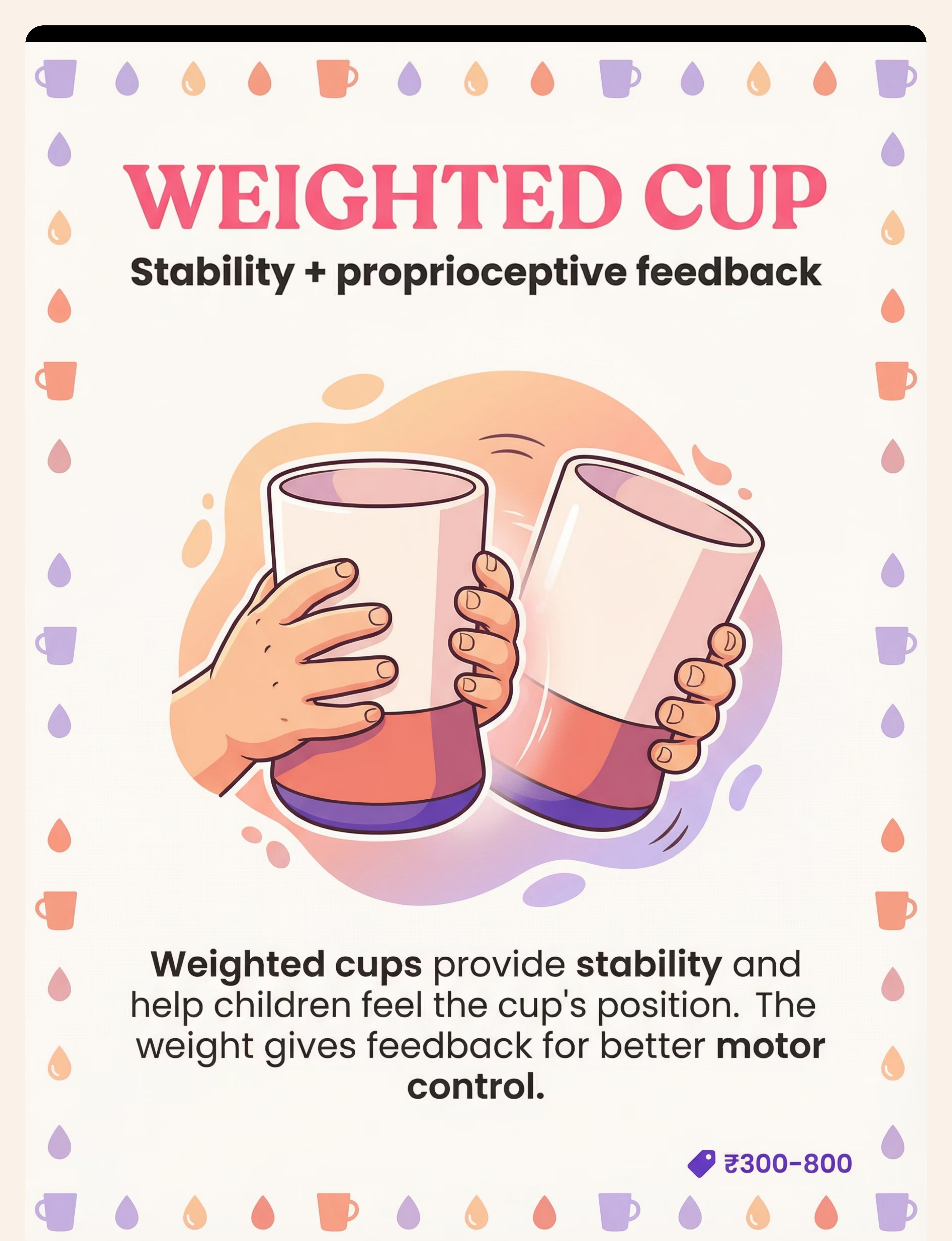
"Context-specific, equity-focused interventions ensure every family can participate regardless of economic access." — WHO NCF 2018 Material Commercial Option DIY / Substitute Why It Works Cut-out cup Nosey/flexi cup ₹150–500 Cut a U-shape notch from a disposable plastic cup — smooth edges carefully Same nose-accommodation principle Small open cup Shot glass plastic ₹50 Medicine dispensing cups, steel katori, shot-glass-sized dabbas Proportionally appropriate vessel Weighted cup Commercial ₹300+ Fill a regular cup 30–40% with sand at base, sealed with waterproof tape Adds proprioceptive weight-feedback Visual sequence cards Printed laminated ₹100–400 Print 7 photos of the steps — laminate with contact paper Brain processes real photos effectively Oral motor warm-up Chewy tube ₹200+ Chewy granola bars; blowing bubbles for lip activation; licking peanut butter from spoon Same oral motor activation principle Zero-Cost Version: Use any small plastic cup from the kitchen. Fill with 1–2 tablespoons of water. Sit child upright. Follow 7-step sequence (draw it on paper). Warm up with 2 minutes of lip exercises first.

• Structural differences (cleft palate, tongue tie, severe hypotonia) → Medical clearance required
• Coughing or wet-gurgling voice occurs consistently → Stop and seek professional assessment
• Severe food/liquid aversion → Desensitization programme required first
• Child just had a meltdown → Postpone to next scheduled practice
• Child is very hungry → Feed first; practice works best when slightly thirsty
• Significant resistance (crying, pushing away) → Use visual schedule; do not force
• Child is mildly thirsty (preferred liquid ready)
• Good posture support is in place (feet flat, hips at 90°)
• 10–15 minutes of uninterrupted practice time available
• Small towel ready for spills — normalize, not shame

Check | ✅ GO | ⚠️ MODIFY | ❌ POSTPONE | |
Emotional state | Calm, smiling, responsive | Quiet but neutral | Crying, agitated, melting | |
Physical state | Alert, well-rested | Slightly tired | Sick, very tired, post-meltdown | |
Hunger/thirst | Slightly thirsty | Just ate | Ravenous or just had full meal | |
Engagement | Eye contact, engaged | Looking around | Actively avoiding/withdrawing | |
Body posture | Upright, stable | Some fidgeting | Slumped, resistant to sitting |

"Hey! Look what we have today. This is our special cup. Let's just see it — you don't have to drink yet."
Walks away → Allow it; try in 5 minutes
Ignores → Pair with a preferred activity nearby

"Your lips are ready! This cup is going to help you drink like a champion. See the special design?"


Variation | How | Why | |
Liquid variety | Change from water to diluted juice mid-session | Sensory novelty maintains motivation | |
Cup progression | Start with Material 2; attempt 1 rep with Material 4 | Graduated challenge builds confidence | |
Color change | Use coloured water (food colouring) | Visual novelty for flow anticipation practice | |
Temperature | Slightly chilled liquid | Increases sensory awareness of liquid in mouth | |
Volume | Begin with 1 tbsp; increase to 2 tbsp if successful | Graduated volume builds confidence |



# | What to record | How | Example | |
1 | Sip attempts today | Tally | 3 | |
2 | Spills per attempt | Rating: 0=none, 1=small, 2=significant | 1, 0, 1 | |
3 | Child's engagement level | 1=resistant, 2=tolerant, 3=engaged, 4=enthusiastic | 3 |
E-463 Cup Practice [date] | Attempts: 3 | Spills: small, none, small | Mood: 3/4 | Cup used: Recessed lid | Notes: Needed hand guidance on steps 1–3

What If It Didn't Go As Planned? Troubleshooting Guide
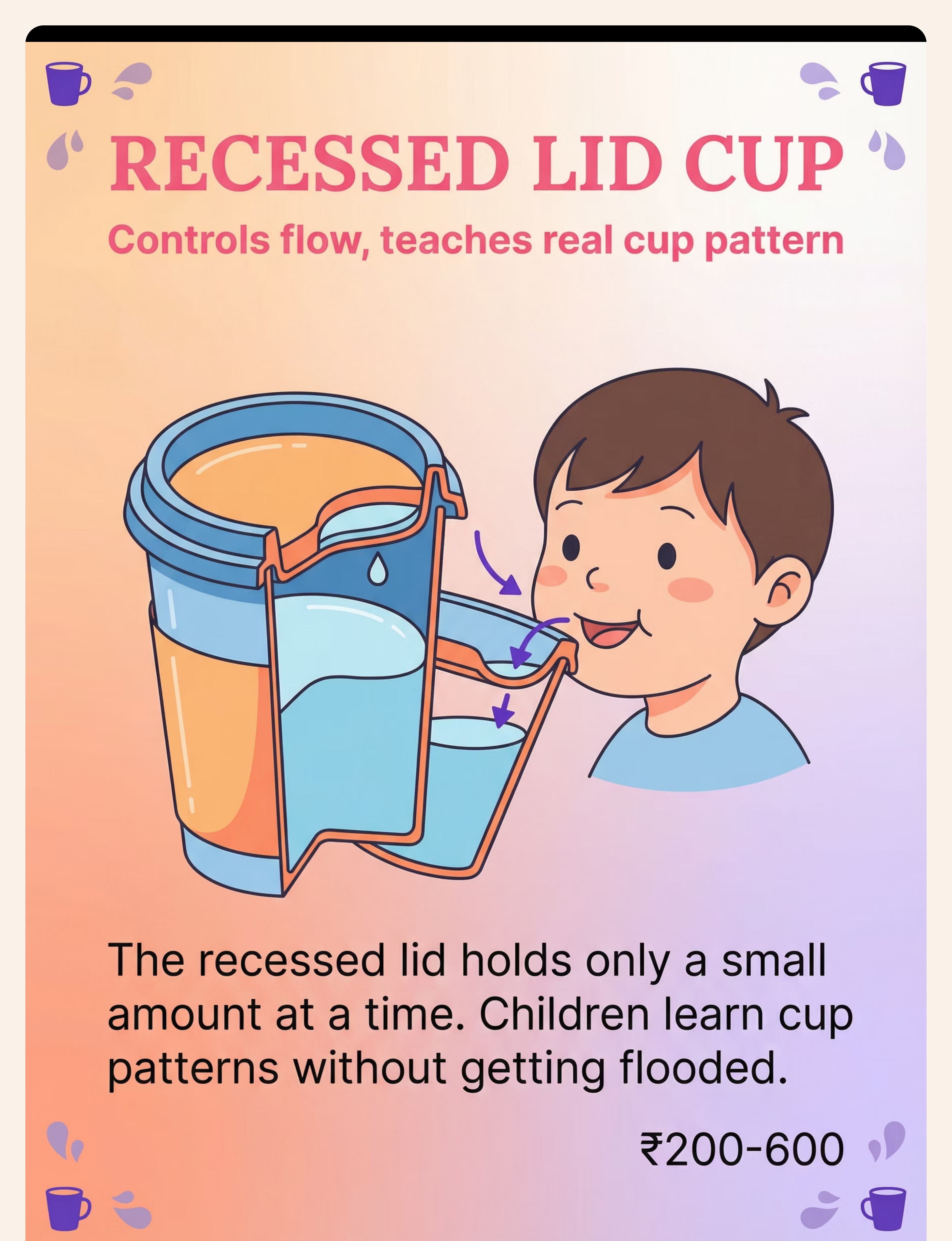
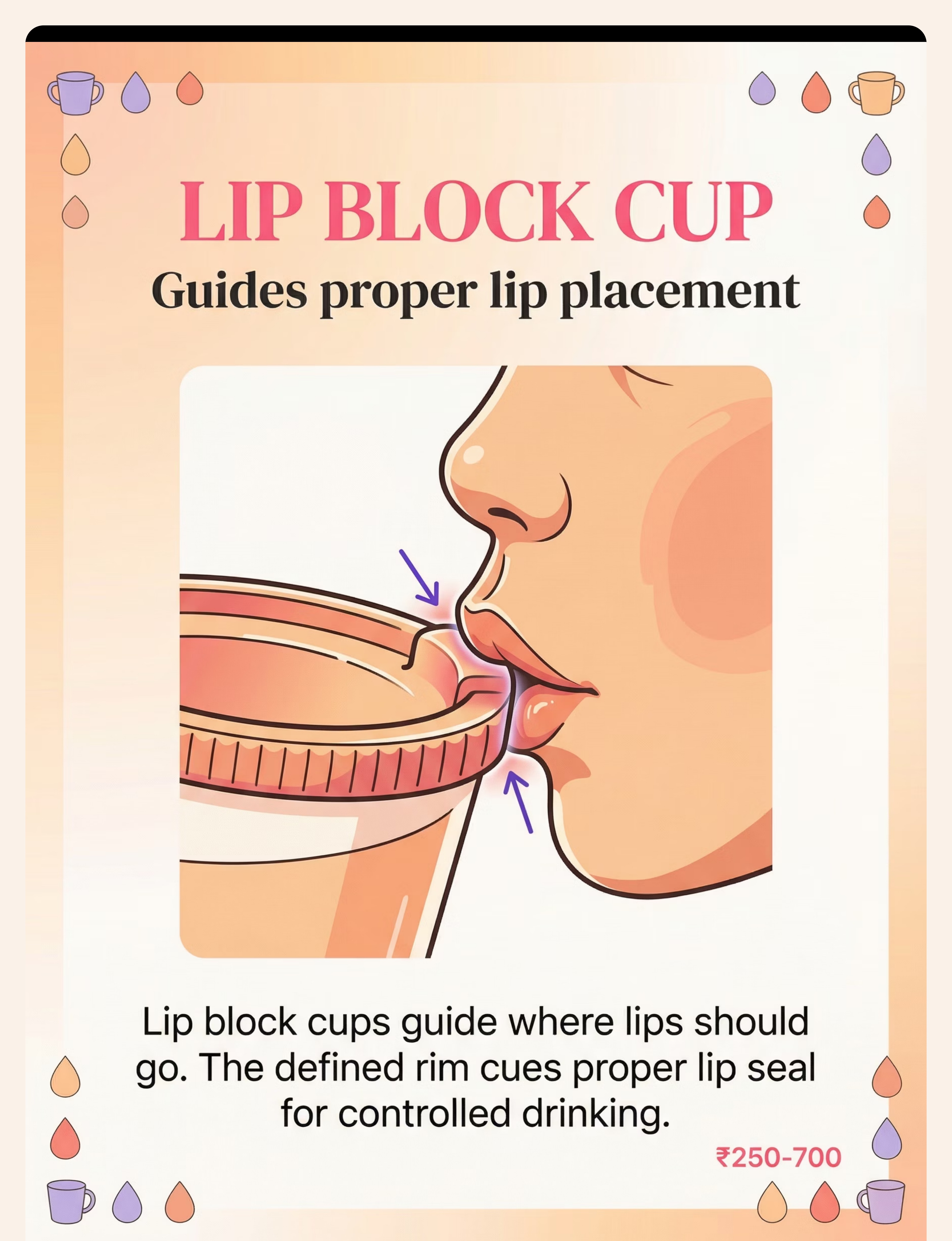
"Session abandonment is not failure — it's data. Modify and return." — Pinnacle Protocol Most sessions don't go perfectly. Every problem has a specific clinical explanation and a targeted fix. Use this guide before concluding that the protocol isn't working. 🌊 Child flooded — coughed Why: Tipped too far; no flow anticipation.Fix: Switch to recessed lid cup (Material 2). Reduce to 1 tablespoon. Practice "slow tip" with hand guidance. 🚫 Refused to touch the cup Why: Sensory aversion; negative association; demand threshold exceeded.Fix: Return to material phase — explore cup without drinking for 2–3 sessions. Use "just hold it" prompt only. 💧 Liquid leaks from sides consistently Why: Lip closure deficit — orbicularis oris weakness.Fix: Add 5 min lip exercises before session. Switch to lip block cup (Material 5). Add straw training daily. Refer for SLP if no improvement in 4 weeks. 😬 Child bites the rim Why: Jaw grading difficulty; oral sensory seeking.Fix: Offer chewy tube before session. Use cup with smaller rim. Consult OT about jaw grading exercises. 🏫 Perfect at home, refuses at school Why: Generalization failure — skill is context-specific.Fix: Send preferred training cup to school. Share visual sequence cards with teacher. Practice in varied home environments first. 📉 No improvement after 4 weeks Why: Possible structural issue, significant hypotonia, sensory barrier, or aspiration concern.Fix: Book professional assessment. Call 9100 181 181 — free teleconsultation. Request SLP + OT feeding evaluation.

• Same cup every session for 2 weeks
• Gradual exposure: hold → smell → taste from spoon → sip (weeks 1–3)
• Minimal sensory preparation — avoid overwhelming
• Weighted cup for more feedback
• Chewy items before session
• Faster progression through materials
• Weighted cup for proprioceptive input
• Postural support critical
• Smaller volumes; rest periods between reps
• Same cup, position, liquid for weeks 1–4
• Hand-over-hand for full sequence
• Self-talk strategy: child narrates steps aloud
Age | Modification | |
12–24 months | Adult-supported throughout; two-handled cup; minimal liquid; model drinking on yourself | |
2–4 years | Graduated independence; token rewards; choice between 2 cups | |
5–7 years | Self-monitoring: child rates own performance; peer modeling helpful | |
8–10 years | Social motivation: "Let's practice so you can drink at your friend's birthday" |

"You may notice you're more confident too. Your reading of their cues has improved. You know when to push, when to wait, when to stop. That is the parent-therapist emerging in you." — Pinnacle Parent Training Principle

Mastery Criteria | Observable Behaviour | ✅/❌ | |
Independent sequence | Completes all 7 steps without verbal prompt | __ | |
Lip closure | Drinks without liquid leaking from sides | __ | |
Flow control | Rarely floods; good tip-sip-straighten coordination | __ | |
Appropriate volume | Adjusts tipping to appropriate sip size | __ | |
Generalization | Drinks from 2+ different cup types | __ | |
Setting transfer | Drinks successfully in 2+ different environments | __ | |
Choking-free | No coughing during typical cup drinking practice | __ |
Next: E-464 Straw Drinking | Drinking from water fountains | Different cup shapes across environments

"The first time my child drank from a cup without a lid was ________. We felt ________. This mattered because ________."

Technique | Code | Difficulty | Lead Discipline | Canon Material | |
Straw Drinking | E-464 | ⭐⭐ Core | SLP + OT | Straw Training Systems | |
Oral Sensory & Feeding | E-465 | ⭐⭐⭐ Advanced | OT + SLP | Oral Motor Tools | |
Slow Eating | E-462 | ⭐ Intro | OT + SpEd | Visual Timers | |
Food Texture Sensitivity | E-461 | ⭐⭐ Core | OT + SLP | Textured Feeding Tools | |
Bottle Weaning | E-466 | ⭐⭐ Core | SLP + ABA | Adaptive Cups | |
Oral Motor Weakness | E-467 | ⭐⭐⭐ Advanced | SLP | Oral Motor Tools |
✅ You own visual supports from E-463 → directly applicable to E-462

Your Child's Full 12-Domain Developmental Map
Cup drinking is one piece of a 12-domain developmental journey. Feeding independence is not just a mealtime skill — it feeds directly into school participation, self-care ADL independence, executive function and sequencing, and social communication at mealtimes.




Your Child's Cup-Drinking Independence Starts With One Session Today.
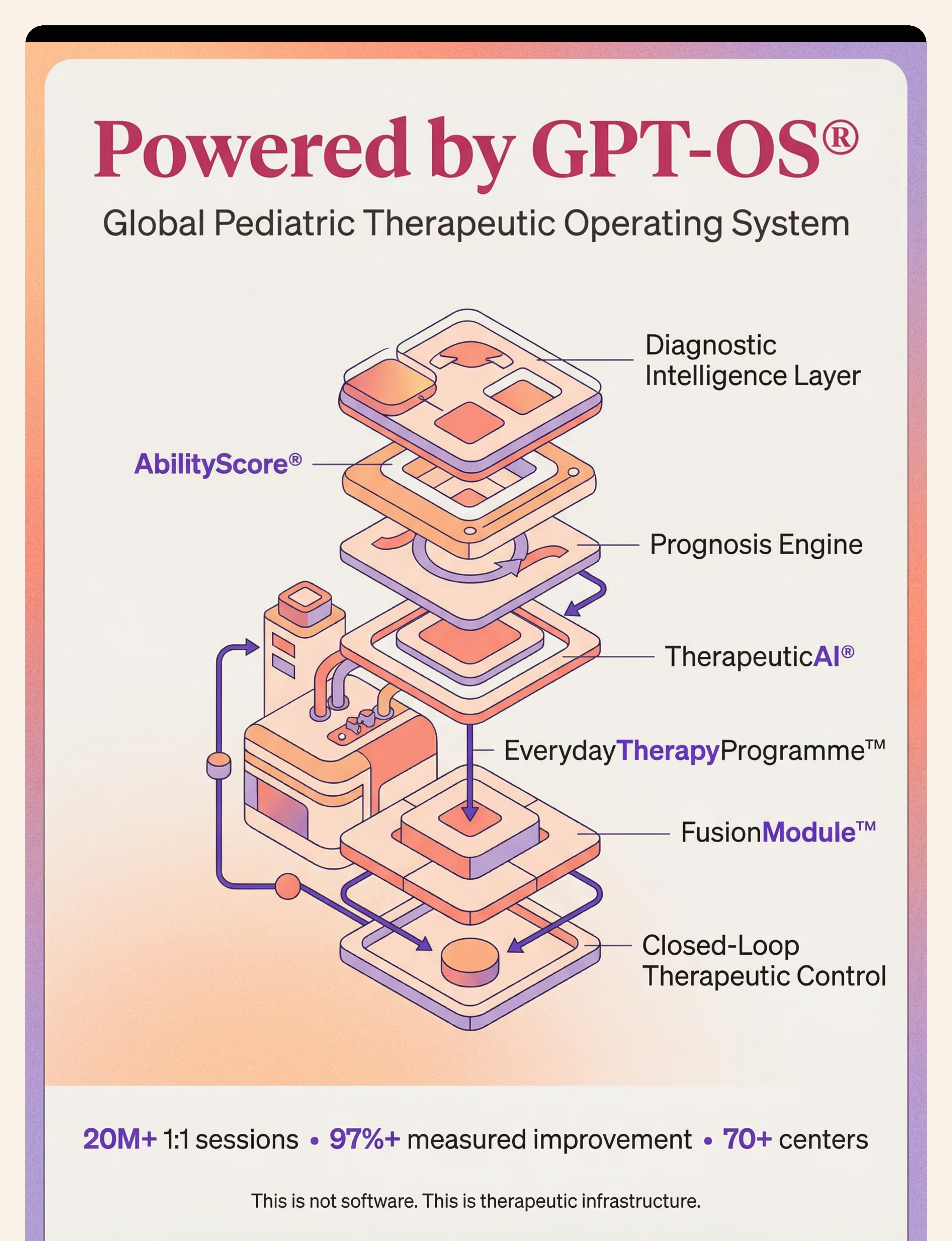
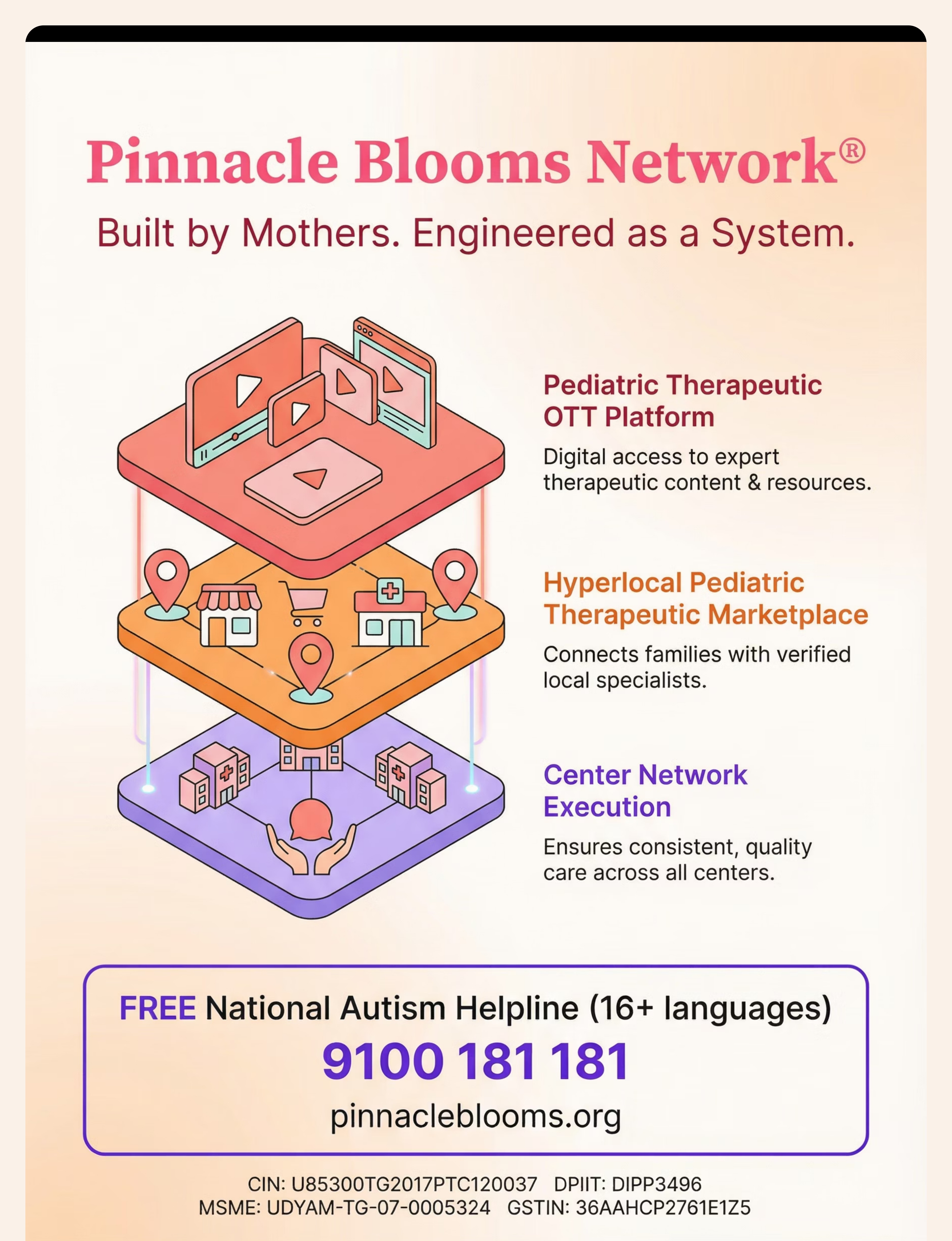
Every family who has walked this path started exactly where you are right now — with a wet shirt, a patient child, and a decision to try systematically. The materials are within reach. The protocol is in your hands. The next session is today. 🏆 Pinnacle Blooms Consortium — Validated Clinical Technique OT • SLP • ABA • SpEd • NeuroDev | 20M+ Sessions | 97%+ Improvement | 70+ Centers Across India ▶ Start This Technique Today — GPT-OS® Session Launcher 📞 Book a Free Consultation — 9100 181 181 → Explore Next Technique: E-464 Straw Drinking "This technique is part of the GPT-OS® EverydayTherapyProgramme™ — the world's most comprehensive home-based paediatric therapy system, built from 20 million clinical sessions."
Preview of 9 materials that help with cup drinking Therapy Material
Below is a visual preview of 9 materials that help with cup drinking therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








"From fear to mastery. One technique at a time."