
"The sounds won't stop. Everyone's exhausted. Nothing seems to help."
Your child isn't being difficult. Their nervous system is communicating. Here are 9 materials that help — not to silence them, but to regulate them.
🏥 Pinnacle Blooms Consortium®
🧠 OT + SLP + ABA + SpEd + NeuroDev
📍 70+ Centers | 🌍 70+ Countries
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | Available 24×7

You Are Among Millions of Families Navigating This Exact Challenge
30–50%
Vocal Stimming Rate
of autistic children exhibit vocal stimming regularly
80%
Sensory Difficulty
of children with ASD show some sensory processing difficulty
21M+
Therapy Sessions
inform Pinnacle's vocal regulation protocols
Your child's constant sounds — the humming, the squealing, the word repetition that seems to come from nowhere — are not random. They are not defiance. They are the language of a nervous system that processes the world differently. Across India and 70+ countries, families like yours are navigating this same territory. You are not failing. You are asking the right questions.
PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory processing difficulties. Meta-analysis across 24 studies confirms sensory-based interventions effectively promote self-regulation outcomes. — PMC11506176 | PMC10955541
📞9100 181 181 — Speak to a specialist today. FREE.
This Is a Wiring Difference. Not a Behavior Problem.
The Neuroscience
Vocal stimming activates multiple neural systems simultaneously:
- Auditory Cortex — Processes self-generated sounds as rewarding input
- Basal Ganglia — Drives repetitive behavior loops; generates inherent reinforcement
- Vagus Nerve — Vocal vibration activates parasympathetic (calming) pathways
- Limbic System — Regulates emotional arousal through sound production
- Brainstem Reticular Formation — Modulates arousal via auditory self-stimulation
What This Means for Your Child
When your child hums, they may be calming their nervous system. When they squeal, they may be processing excitement their body can't contain otherwise. When they repeat sounds, they may be creating predictable auditory input in an unpredictable world.
The sound IS the therapy — your child's brain found the tool it needed. Our job is to give it better tools that meet the same need.
"Vocal stimming is not meaningless noise. It is a neurological coping strategy. Suppressing it without replacing the need is like removing a smoke alarm — the fire is still there." — Pinnacle Blooms Consortium, OT + NeuroDev Division
Citation: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660
Your Child Is Here. This Is Where We're Heading.
1
Age 18m–3y
Vocal exploration. Normal, universal developmental phase.
2
Age 3–5y ▲
Current Challenge Zone — D-366. Stimming emerges/intensifies; function identified.
3
Age 5–8y
Context awareness develops; regulation strategies introduced.
4
Age 8–12y
Self-regulation with tools; social context mastery.
Common Co-occurrences at This Stage
Sensory Processing Differences
Auditory Hypersensitivity
Anxiety
Communication Differences
Executive Function Differences
Vocal stimming commonly emerges or intensifies between ages 3–7. With the right materials and strategies, most families report significant improvement in regulation and context-awareness within 8–12 weeks. This is not permanent. This is a waypoint.
Citation: PMC9978394 | WHO/UNICEF CCD Package 2023

Clinically Validated. Home-Applicable. Parent-Proven.
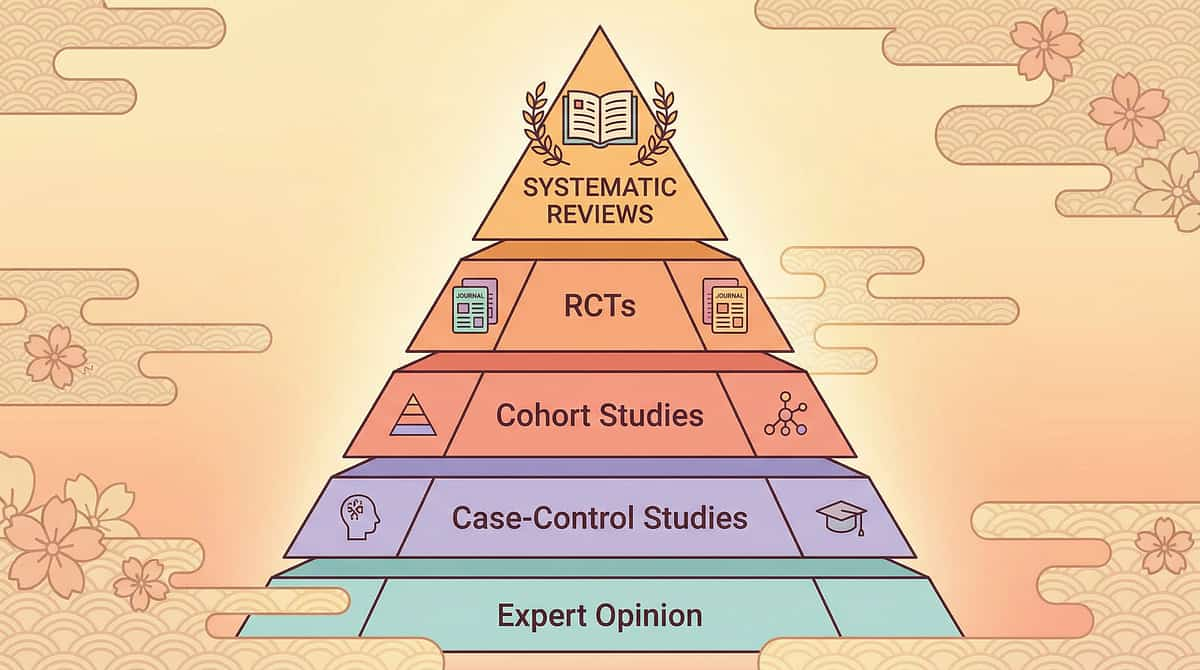
🛡️ LEVEL I — SYSTEMATIC REVIEW + RCT EVIDENCE
Study | Finding | Source | |
PRISMA Systematic Review 2024 | 16 studies confirm sensory integration is evidence-based practice for ASD | PMC11506176 | |
World J Clin Cases Meta-Analysis 2024 | Sensory integration therapy promotes social skills, adaptive behavior, sensory processing across 24 studies | PMC10955541 | |
Indian RCT, Indian J Pediatr 2019 | Home-based sensory intervention shows significant outcomes; safe for parent delivery | DOI: 10.1007/s12098-018-2747-4 | |
WHO/UNICEF CCD Package | Home-based caregiver interventions effective across 54 countries | PMC9978394 | |
NCAEP 2020 | Sensory-based and behavioral regulation strategies classified as evidence-based practice | NCAEP Report 2020 |
82%
Evidence Confidence
Level I — Systematic Review + RCT
"This is not experimental. This is not fringe. This is the global clinical consensus — implemented by Pinnacle's consortium across 20M+ therapy sessions."
📞9100 181 181 — For a personalized assessment, call FREE.

The Technique: Sensory Substitution & Contextual Regulation for Vocal Stimming
Parent Alias: "The Sound Regulation Method"
Vocal stimming (vocal stereotypy / auditory self-stimulation) refers to repetitive vocalizations — humming, squealing, repeating words or sounds, throat noises — that serve sensory and regulatory functions rather than communicative ones. This technique provides alternative sensory inputs that meet the same neurological needs (oral-motor feedback, vibratory input, auditory satisfaction, general nervous system regulation) through materials and structured contexts, reducing functional impairment without harmful suppression. The goal is regulation and context-awareness — not elimination.
🏷️ Domain
D2 — Stimming & Repetitive Behaviours
🏷️ Ages
3–12 years
🏷️ Duration
15–20 min daily sessions + proactive toolkit
🏷️ Frequency
2–3× daily + pre-emptive use in high-stimming contexts
Related techniques: ← D-365 Visual Stimming | → D-367 Hand Flapping | → D-368 Harm-Causing Stimming
Citation: Pinnacle 128 Canon Materials System + 12 Domain Classification. Consortium Lead: OT (Primary) + SLP + ABA
This Technique Crosses Therapy Boundaries Because the Brain Doesn't Organize by Therapy Type
OT — Primary Lead
Sensory integration assessment; sensory diet design; oral-motor and vibration tool selection; weighted product protocols.
SLP
Differentiates vocal stimming from communicative speech/echolalia; oral-motor function; breath control; structured sound activities.
BCBA / ABA
Functional behavior assessment of stimming; context-teaching protocols; reinforcement strategies; data-based decision-making.
SpEd
Classroom accommodation planning; IEP integration; school-based regulation supports; teacher training.
NeuroDev Pediatrics
Rules out medical causes (tics, Tourette's, pain-driven vocalizations); medication review; diagnostic clarity.
A child who hums constantly at school needs their OT's sensory assessment, their SLP's communication differentiation, their BCBA's context-teaching protocol, their SpEd's classroom plan, and their pediatrician's medical clearance — simultaneously. This is why GPT-OS® runs a FusionModule™, not single-discipline siloes.
Citation: DOI: 10.1080/17549507.2022.2141327 (Int J Speech-Lang Pathol, 2022) | UNICEF/WHO NCF for SLPs

This Isn't a Random Activity. It's a Precision Regulatory Tool.
Observable Behavioral Indicators
Reaches for chewable or fidget before stimming escalates
Moves to designated stimming space when prompted or self-initiated
Tolerates headphones as environmental regulation tool
Engages in structured sound activities as acceptable vocal outlet
Demonstrates reduced vocalization in quiet settings over 8-week course
Citation: PMC10955541 (Meta-analysis, World J Clin Cases 2024). Consortium Lead: OT + BCBA
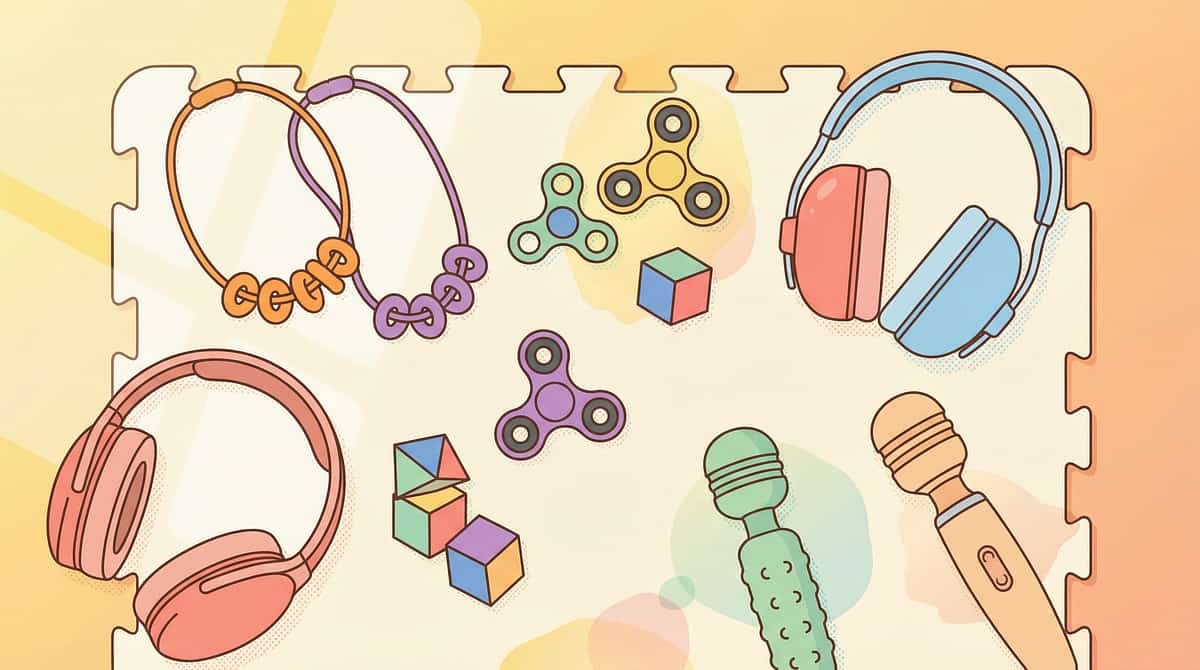
9 Materials. Each Addressing a Different Function of Vocal Stimming.
# | Material | Function | INR Range | Start Here? | |
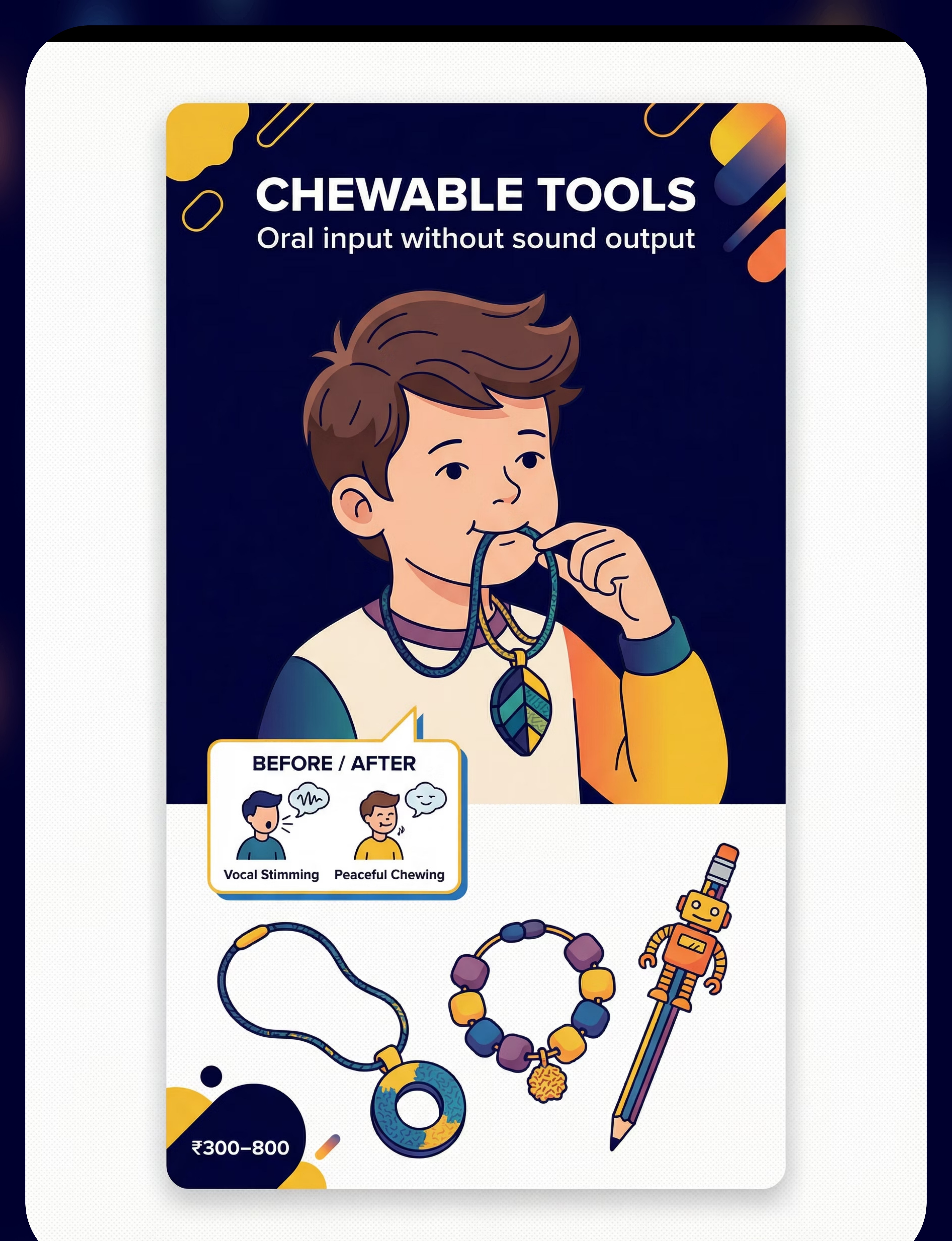
1 | Chewable Jewelry / Oral Sensory Tools | Oral input without sound output | ₹300–800 | 🟢 | |
2 | Noise-Canceling Headphones / Ear Defenders | Control incoming sound, reduce outgoing | ₹1,500–5,000 | 🟢 | |
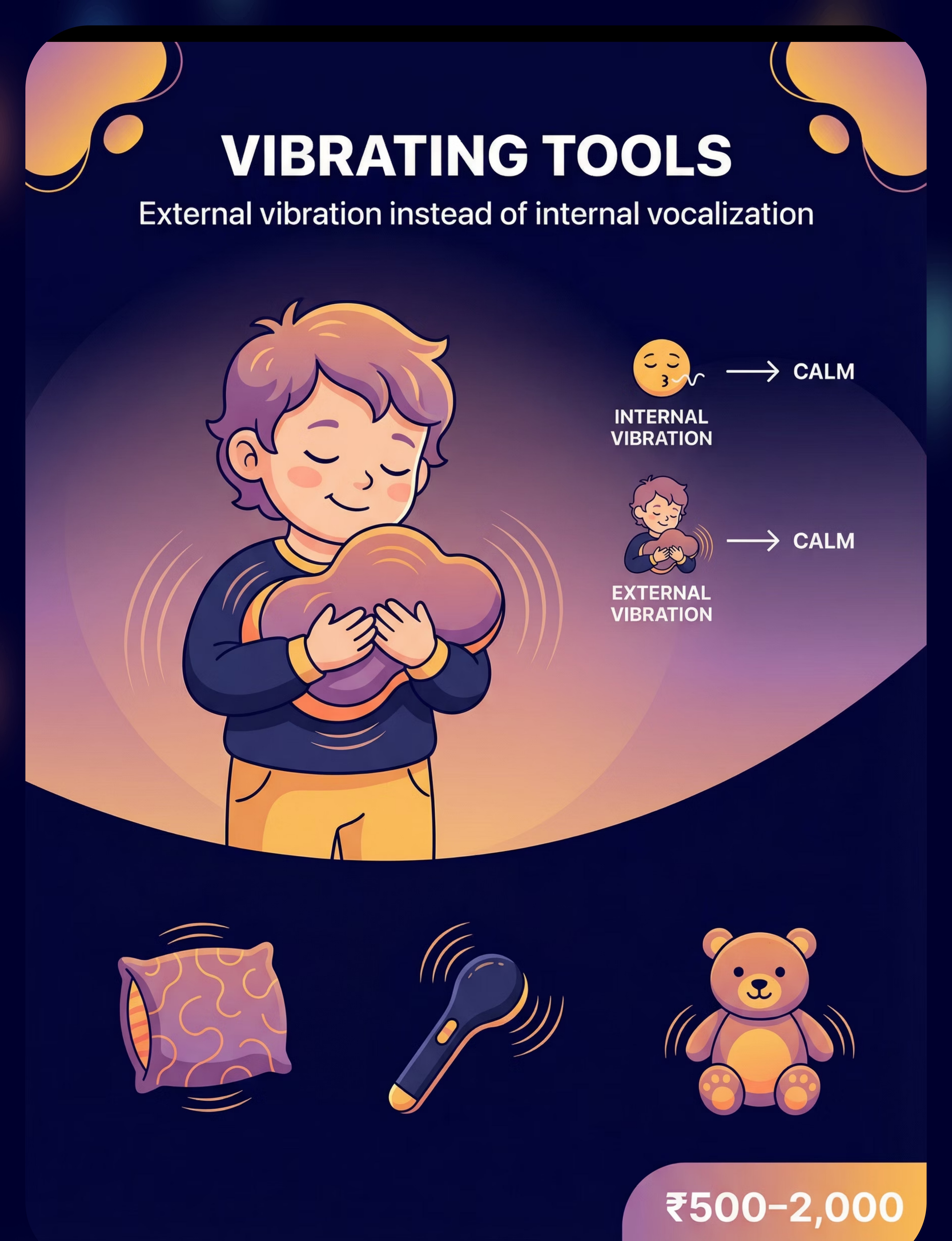
3 | Vibrating Sensory Tools | External vibration instead of internal vocalization | ₹500–2,000 | 🟡 | |
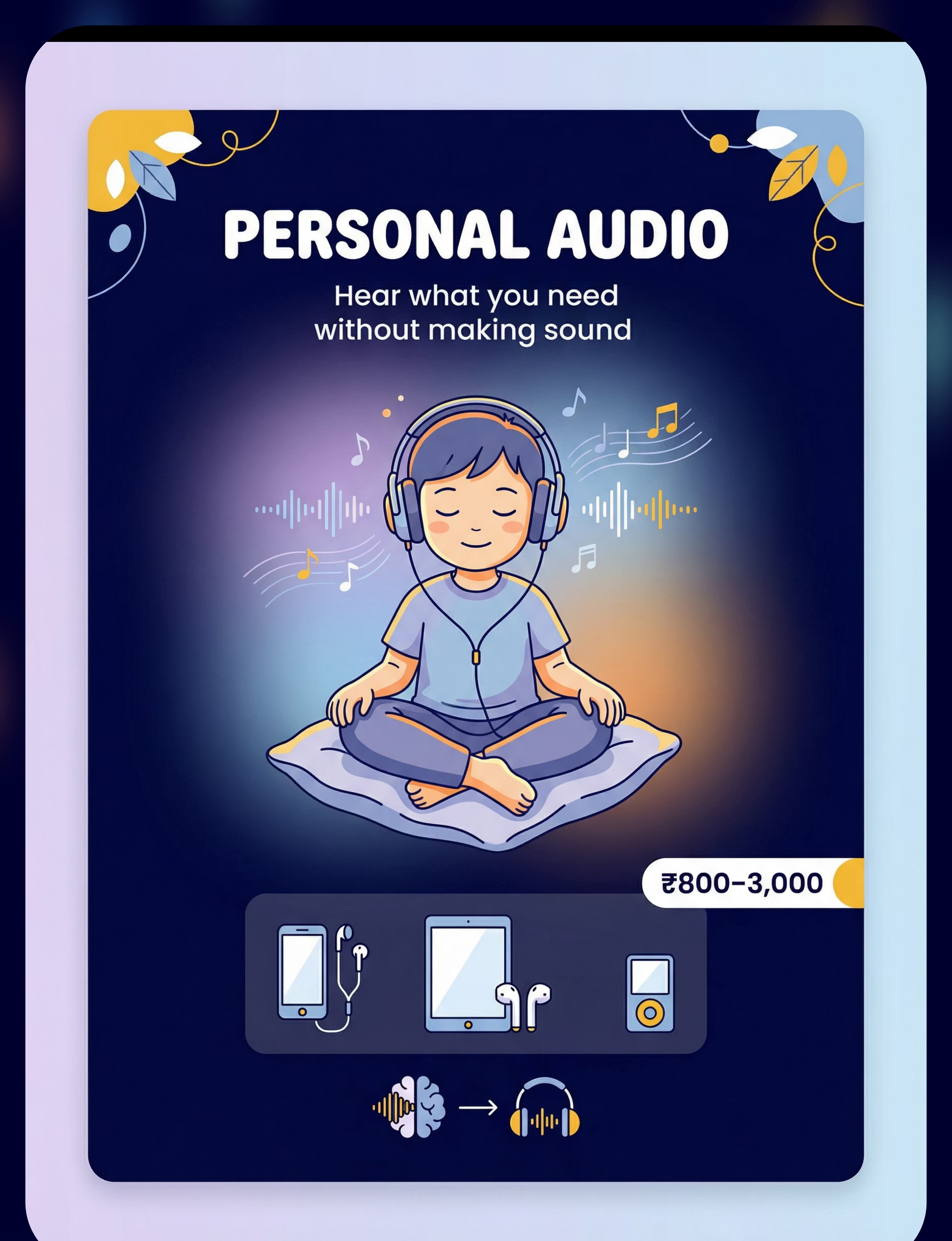
4 | Personal Audio / Headphones with Preferred Music | Hear what you need without making sound | ₹800–3,000 | 🟡 | |
5 | Visual Sensory Alternatives / Light-Up Toys | Capture attention, reduce vocal output | ₹400–1,500 | 🟡 | |
6 | Weighted Lap Pad / Weighted Blanket | Calm the nervous system, quiet the output | ₹1,000–4,000 | 🟡 | |
7 | Designated Stimming Space / Vocal Expression Area | Safe place for full expression | ₹500–3,000 | 🟢 | |
8 | Fidget Tools / Tactile Sensory Toys | Busy hands, quieter mouth | ₹150–600 | 🟢 | |
9 | Structured Sound Activities / Musical Instruments | Acceptable outlet for vocal needs | ₹300–1,500 | 🟡 |
Pinnacle Recommends: Select based on YOUR child's stimming function — not all 9 simultaneously. Start with the material that addresses the primary function (vibration-seeking → vibrating tool; sound-blocking → noise-canceling headphones).
📞9100 181 181 — Ask our OT which material fits your child's profile. FREE. | Full product links: pinnacleblooms.org/therapy-materials

Every Family Can Start Today. Zero Budget Required.
WHO Equity Principle: Not every family can order online. Not every city has next-day delivery. Every technique must have a zero-cost version. This is the WHO/UNICEF inclusion principle in action.
Material | ✅ Buy This | 🔧 Make This (Free) | |
Chewable Tool | Chewable necklace ₹300–800 | Food-grade silicone teether cleaned thoroughly; safe rubber tubing | |
Noise Control | Children's ear defenders ₹1,500+ | Cotton wool earplugs (supervision required); soft foam plugs | |
Vibration Tool | Vibrating sensory pillow ₹500+ | Electric toothbrush (brush head removed) held against sternum | |
Personal Audio | Children's headphones ₹800+ | Phone + earbuds; any audio device with volume control | |
Visual Tool | Light-up spinner ₹400+ | Glitter jar (water + glitter glue in sealed bottle) | |
Weighted Product | Weighted lap pad ₹1,000+ | Rice-filled fabric pouch (~10% body weight; check stitching) | |
Stimming Space | Play tent setup ₹500+ | Corner of room + cushions + fairy lights + blanket "fort" | |
Fidget | Tactile fidget ₹150+ | Dried pulse-filled balloon (seal tightly); textured rubber ball | |
Sound Activity | Kazoo/harmonica ₹300+ | Humming into cupped hands; rhythm clapping games |
"The principle is more powerful than the product. A homemade rice-weight pouch and a cozy corner can begin the journey. Clinical-grade materials accelerate it."
Citation: PMC9978394 | WHO NCF Handbook 2022. Consortium Lead: OT + WHO/UNICEF Equity Framework
Clinical Precision. Parental Safety. Non-Negotiable Gates.
🔴 RED — DO NOT PROCEED IF:
- Child shows self-injurious behavior during stimming (throat-clearing causing damage, head-banging)
- Sudden onset of vocalizations that sound like tics — consult pediatric neurologist
- Vocalizations associated with known medical conditions requiring specialist review
- Child is in acute distress, fever, or illness
- Chewable tools show wear/damage — replace before use
🟡 AMBER — MODIFY APPROACH IF:
- Child resists all offered alternatives — start with observation only; do not force
- Vocal stimming is the child's only functional coping mechanism — introduce alternatives gradually
- Child is in transition period (new school, family change, grief) — increase stimming space time
- Weighted products: ensure child is over age 2 and can remove the weight independently
🟢 GREEN — READY TO PROCEED WHEN:
- Child is fed, rested, and in a baseline-regulated state
- Alternatives introduced during calm times first
- Stimming space is established before redirection is attempted
- All materials checked for age-appropriateness and physical safety
- Family and school aligned on neurodiversity-affirming approach (no shaming, no punishment)
RED LINE — STOP SESSION IMMEDIATELY IF: Throat distress | Vocal cord strain signs | Extreme distress from redirection | Signs of autistic burnout (withdrawal, regression, loss of skills)
📞9100 181 181 — Any concern? Call us FREE before proceeding. | Citation: DOI: 10.1007/s12098-018-2747-4 (Indian J Pediatr, Padmanabha 2019)

Spatial Precision Prevents 80% of Session Failures.
Space Setup Checklist
- Stimming space established and named positively ("your sound room," "free zone")
- Chewables in 3 locations: home, school bag, car
- Noise-canceling headphones accessible before leaving home
- Visual timer available for structured sound time transitions
- All fidget/sensory tools within child's reach — not stored away
- Light-up visual tools in stimming space corner (dim lamp, glitter jar)
- Weighted lap pad at desk/study area
- Music playlist ready on device for personal audio use
Environment Details
Quiet Zone: Study / Meals / Public equivalent — fidget + chewable accessible; headphones available.
Sound Zone: Bedroom corner tent / play area — full vocal expression permitted; cushions, dim light, visual timer.
Lighting: Dim or warm in stimming space — reduce visual overload.
Sound: Reduce background TV and noise at home where possible.
Temperature: Cool to neutral — warmth can increase arousal.
Citation: PMC10955541 (meta-analysis on session structure efficacy). Consortium Lead: OT

The Best Session Is One That Starts Right.
Hunger Check
Child has eaten in last 2 hours. If NO → Feed first. Hunger amplifies stimming.
Regulation Check
No meltdown in last 30 minutes. If NO → Postpone; offer stimming space.
Energy Check
Child is alert, not overtired. If NO → Reschedule to optimal time of day.
Health Check
No signs of illness or pain. If NO → Medical check first.
Materials Check
Materials are available and checked. If NO → Prepare before calling child.
✅ All 5 Ticked → GO
Begin with Material Introduction (Step 1)
⚠️ 3–4 Ticked → MODIFY
Offer stimming space only; no active session
❌ Fewer Than 3 → POSTPONE
Quiet co-regulation; try tomorrow
"You can always try again tomorrow. One skipped session is worth more than one forced session that ends in distress."
Citation: ABA Antecedent Manipulation Principles | PMC11506176. Consortium Lead: BCBA/ABA

Step 1: The Invitation to Engage
You Don't Introduce a Tool During a Storm. You Introduce It in the Calm.
Script A — Verbal Understanding
"Hey, I found something you might really like. Want to try this?" Offer chewable or fidget. No pressure. Let them explore.
Script B — Limited Verbal Processing
Place the material nearby. Model using it yourself briefly. Do not instruct. Let curiosity do the work.
Script C — Introducing Stimming Space
"This is your sound room. You can come here whenever you want to make sounds. Any sounds. This place is just for you."
Key Principle: The tool is offered as a privilege, not a replacement. Never use language that implies stimming is wrong. "This will help you" — not "This will stop that." Morning introductions work better than evening (lower cortisol, higher regulation capacity).
Citation: PMC11506176 | ABA Preference Assessment literature. Consortium Lead: SLP + BCBA

Step 2: Establishing Engagement
Not All Children Engage the Same Way. Follow Their Lead.
🔴 Sensory Seeker
High-intensity vocalizer
Lead with vibrating tools or chewable jewelry — these most directly substitute the physical sensation of vocal stimming. Allow 3–5 minutes of unstructured exploration. Celebrate any engagement with the material.
🟡 Sound-Blocker
Stims in loud environments
Lead with noise-canceling headphones in a moderately noisy situation. Demonstrate how "the sounds go quiet" with headphones. Pair with personal audio playlist.
🟢 Understimulated Vocalizer
Stims in quiet/boring contexts
Lead with personal audio or structured sound activity. Schedule daily "sound time" — child anticipates it and may naturally reduce random stimming.
Engagement Confirmation Signs
Child picks up material voluntarily
Child explores material for more than 30 seconds
Child shows neutral or positive expression during exploration
Child returns to material unprompted
If no engagement in 3 sessions: Rotate to the next material. Not all tools work for all children. Data informs selection.
Citation: PMC11506176 | Sensory preference assessment literature. Consortium Lead: OT + BCBA

Step 3: The Therapeutic Action — Sensory Substitution in Real Time
When vocal stimming begins or is anticipated, observe first — what type of sound? Humming, squealing, or repetition? What is the antecedent — loud environment, boredom, excitement, or stress? Match the function, offer the material quietly, and wait for the child to discover it independently. If context requires quiet, calmly say: "This is a quiet space. You can use your sound room when we're done here." Offer a chewable or fidget as a bridge.
🟢 Ideal Response
Child accepts material; vocalization reduces; continues activity
🟡 Acceptable Response
Child accepts material intermittently; some vocal stimming continues
🔴 Concerning Response
Child becomes distressed by redirection; increase stimming space access immediately
Duration: 10–20 minutes total session; core therapeutic action = 5–8 minutes.
Citation: PMC10955541 (40-minute sessions most effective; 10–20 min home sessions). Consortium Lead: OT (Primary) | Pinnacle Blooms Consortium® OT + SLP + BCBA/ABA + SpEd + NeuroDev Pediatrics

Step 4: Repeat & Vary — 3 Good Interactions › 10 Forced Ones
Daily
Proactive material availability (chewables/fidgets always accessible)
Sessions
2–3 focused interaction opportunities per day
Sound Time
1× daily designated outlet (10–15 minutes)
Course
8–12 weeks for observable pattern shift
Week | Variation Strategy | |
1–2 | Single material exploration; no pressure | |
3–4 | Introduce 2nd material option; begin structured sound time | |
5–6 | Child begins choosing preferred tools; introduce context language ("quiet space" vs "sound room") | |
7–8 | Child initiates material use; begins context-switching with support | |
9–12 | Self-regulation emerging; reduce prompts; build self-advocacy language |
Satiation signs — reduce session: Child turns away | Throws material | Increases vocal stimming (material not meeting the need)
Citation: General SI dosage literature | PMC11506176. Consortium Lead: OT + BCBA

Step 5: Reinforce & Celebrate — The Attempt, Not Just the Success
What to Reinforce
- Any engagement with the alternative material
- Walking toward the stimming space voluntarily
- Tolerating quiet for any duration longer than yesterday
- Any spontaneous self-initiation of regulation strategy
- Requesting a regulation tool verbally or through AAC
Timing
Within 3 seconds of the desired behavior. Timing matters more than magnitude.
Script Examples
"You used your chewable! That's exactly it."
"You went to your sound room — I am so proud of you."
"You used your headphones in the shop today. That was big."
"You asked for your fidget. YES."
❌ What NOT to Do
- Praise for not stimming — this frames stimming as bad
- Withdraw stimming space as consequence — it is never a punishment
- Compare to other children
Citation: BACB Guidelines | ABA reinforcement scheduling literature. Consortium Lead: BCBA/ABA

Step 6: The Cool-Down — Every Transition Is a Regulation Opportunity
Transition Warning
"Two more minutes in your sound room." Show visual timer. "Almost time to put away the vibrating pillow. One more minute."
Cool-Down Activity
Weighted blanket wrap (30 seconds deep pressure) → Slow breathing together ("let's blow out like a candle") → Quiet preferred sensory item.
Put-Away Ritual
Child participates in putting materials away — builds ownership. "You did such a good job. Let's put your chewable here so it's ready for tomorrow."
Transition to Next Activity
Visual schedule cue | Verbal preview | Same routine daily.
If child resists ending: Do NOT pull materials away. Extend by 2 minutes. Use visual timer. Rushing cool-down is the primary cause of post-session dysregulation.
Citation: NCAEP Evidence-Based Practices Report 2020 (Visual Supports). Consortium Lead: OT + SpEd

Capture the Data: 60 Seconds Now = Weeks of Clarity Later
You don't need a complex data system. You need 3 consistent data points collected immediately after each session. That data drives every clinical decision over the next 8 weeks.
Field 1: Stimming Intensity (1–5)
1 = minimal | 2 = mild | 3 = moderate | 4 = high | 5 = very high. Record immediately after session.
Field 2: Material Engaged
Chewable | Headphones | Vibrating tool | Personal audio | Visual tool | Weighted pad | Stimming space | Fidget | Structured sound | None
Field 3: Context Awareness
No awareness | Moved to stimming space when prompted | Self-initiated tool | Self-initiated context switch
📥 Download
D-366 Weekly Tracking Sheet PDF
📱 In-App Tracker
pinnacleblooms.org/track — GPT-OS® Dashboard
📊 Book Review
Bring data to your consultation — our team reviews it with you FREE
📞9100 181 181 — Bring your data to your next consultation. Our team reviews it with you. FREE.
Citation: BACB Data Collection Standards | Cooper, Heron & Heward, Applied Behavior Analysis, 8th ed. Consortium Lead: BCBA/ABA + CRO

Session Abandonment Is Not Failure. It Is Data.
❓ Child refused the chewable
You may have offered during stimming (too late). Offer in a calm moment tomorrow. Try a different texture. Let them explore in their own time.
❓ Vocal stimming increased after session
The material didn't match the function. Reassess: is it vibration-seeking, sound-blocking, or auditory input? Adjust material selection accordingly.
❓ Child became distressed when redirected
Redirection signals were too direct. Increase stimming space access. Reduce all redirection pressure for 1 week. Focus on meeting needs, not restricting behavior.
❓ The stimming space isn't being used
Make it more appealing (add preferred sensory items, adjust lighting). Practice entering/leaving during calm play. Never force.
❓ Headphones were rejected
They may be uncomfortable. Try different styles (over-ear vs. in-ear vs. ear defenders). Some children need days of gradual exposure.
❓ School says they can't implement this
Contact us for school liaison support. Provide the D-366 Family Guide (Card 37). Reference IEP/sensory accommodation rights. Call 9100 181 181.
❓ The stimming is worse this week
Check for stressors: new routine, school change, illness, sensory overload. Increased stimming is always informative data — look for the antecedent.
Citation: ABA functional analysis + OT clinical problem-solving literature. Consortium Lead: OT + BCBA
No Two Children Are Identical. Personalize This Technique.
← Easier | Standard | Harder → | |
Stimming space only — no redirection at all | Proactive tool offering + stimming space | Context-switching practice: "quiet here / sounds there" | |
One material only, always available | 2–3 material rotation | Self-selection from material toolkit | |
No time limits on stimming space | Visual timer for transitions | Child initiates timer | |
Only positive reinforcement | Token economy | Self-monitoring chart |
🔴 Sensory Seeker
Priority: Vibrating tools + chewables. Increase physical sensory input throughout the day (proprioceptive, oral, movement).
🟡 Sound-Blocker
Priority: Noise-canceling headphones. Reduce background noise and acoustic chaos at home and school.
🟢 Anxious Vocalizer
Priority: Weighted products + stimming space. Increase predictability, routine, and prior warning of transitions.
Age variations: Ages 3–5: Simpler tools, longer timelines, more modeling. Ages 6–9: Introduce context language; structured sound activities. Ages 10–12: Self-advocacy language; child designs their own regulation toolkit.
Citation: Clinical practice guidelines OT/ABA/SLP. Consortium Lead: OT + BCBA + SLP
Week 1–2: In the Beginning, Expect Awareness — Not Mastery.
15%
Week 1–2 Progress
Awareness and exploration phase — neural pathways forming
Observable Indicators at This Stage
- Child notices / picks up alternative material at least once
- Any engagement with stimming space, even briefly
- No increase in distress from material availability
- Parent feeling slightly more confident in what the sounds communicate
What Is NOT Progress Yet — And That's Okay
- Spontaneous context-switching
- Reduced overall stimming frequency
- Independent material use without prompt
"If your child touches the chewable and puts it down — that's real progress. If they enter the stimming space for 30 seconds — that's real progress. Do not wait for dramatic change in week 1. The neural pathways haven't formed yet."
Citation: PMC11506176 (8–12 week outcome timeline). Consortium Lead: CRO + OT
Week 3–4: Consolidation Signs Are Emerging
40%
Week 3–4 Progress
Consolidation phase — routines forming, preferences appearing
Child reaches for preferred material without always being prompted
Stimming space used consistently when available and distressed
Some decrease in intensity (not frequency) of vocal stimming
Parent notices what triggers correlate with increased stimming
Child may begin to show preference for a specific material
Neural Pathway Formation: The child anticipates "sound time" and shows reduced anxiety about quiet periods because they know sound time is coming. This anticipation IS the self-regulation skill forming.
Ready to increase? When child spontaneously uses material 3+ times without prompting, introduce context language: "This is a quiet place. You can make sounds in your room when we get home."
Citation: PMC11506176 | Neuroplasticity + pediatric intervention literature. Consortium Lead: OT + BCBA

Week 5–8: Integration Phase — Self-Regulation Is Emerging
70%
Week 5–8 Progress
Integration phase — self-initiation and context-switching developing
Child self-initiates material use (without prompt) in ≥50% of high-stimming situations
Context-switching emerging: can reduce stimming in public/quiet settings with support
Structured sound time engaged in willingly
Vocal stimming frequency reduced in non-designated contexts
Parent reports reduced family stress and exhaustion around the behavior
"You may notice you're more confident too. You know what the sounds mean. You know what to offer. You're no longer helpless — you're a regulation specialist for your child."
Citation: Intervention outcome literature 8-week milestone data. Consortium Lead: OT
Celebrate: This Is What Regulation Looks Like
Stage 1 — Awareness
Child acknowledges own sounds when pointed out
Stage 2 — Tool Acceptance
Child uses ≥1 alternative material regularly
Stage 3 — Context Awareness
Child demonstrates different behavior in stimming space vs. elsewhere
Stage 4 — Self-Initiation
Child requests materials or stimming space without prompting
Stage 5 — Context-Switching
Child navigates quiet environments with available supports
Stage 6 — Integration
Child self-advocates for sensory needs; accepts own stimming without shame
Each stage is measurable. Each stage is celebrated. This is the GPT-OS® Sensory Regulation Readiness Index in action.
📞9100 181 181 — Book an AbilityScore® re-assessment to document your child's progress.

Know When Home Practice Needs Clinical Backup
🔴 Call Your Specialist If:
- Vocal stimming suddenly increases dramatically — may signal pain, medical issue, or major stressor
- Vocalizations begin to sound involuntary, distressing, or tic-like → Pediatric neurology assessment
- Stimming is accompanied by self-injurious behavior
- Signs of autistic burnout: regression, withdrawal, loss of skills, extreme exhaustion
- No improvement after 12 consistent weeks using multiple materials
- Stimming is preventing functional communication entirely
- Family stress is critically high and impacting the child's safety
📞FREE National Autism Helpline: 9100 181 181 — Available 24×7 | 16+ languages | Manned by trained specialists
"Professional support is not a sign of failure. It is the next tier of the same system you've been building."
Citation: Pinnacle Clinical Escalation Protocols. Consortium Lead: NeuroDevelopmental Pediatrics
D-366 Is One Step in a Longer Journey
D-364
Understanding Stimming Functions — Subdomain D2
D-365
Visual Stimming Materials — Subdomain D2
D-366 ← YOU ARE HERE
Vocal Stimming Regulation Materials
D-367
Hand Flapping Materials — Subdomain D2
D-368
Stimming That Causes Harm — Subdomain D2
Next-Level Pathways Based on Child Response
If vibration-seeking is primary → Advanced vibration sensory diet (Sensory Diet series)
If anxiety is driving stimming → Emotional Regulation Domain C series
If school inclusion is the challenge → School Readiness cluster
If communication aspects are significant → SLP Domain B cluster
You Already Have the Foundation. These Are Your Next Steps.
Technique | Code | Difficulty | Canon Materials | |
Understanding Stimming Functions | D-364 | 🟢 Intro | Visual supports | |
Visual Stimming Materials | D-365 | 🟢 Intro | Visual sensory tools | |
Vocal Stimming (You Are Here) | D-366 | 🟡 Core | Oral / Vibration / Audio | |
Hand Flapping Materials | D-367 | 🟡 Core | Tactile / Proprioceptive | |
Stimming That Causes Harm | D-368 | 🔴 Advanced | Safety + Substitution | |
Stress-Increased Stimming | D-380 | 🔴 Advanced | Regulation toolkit |
"You own materials for several of these already." The chewable, fidgets, and weighted pad from D-366 cross-serve D-367 and D-380.
This Technique Is One Piece of a Larger Plan.
The vocal stimming intervention directly supports Domain D (Behavioral) as its primary domain — stimming regulation and context-awareness. It also feeds Domain A (Sensory Processing) through sensory substitution, reduces anxiety through Domain C (Emotional Regulation), and downstream supports Domain B (Social Communication) by reducing acoustic disruption in peer and classroom contexts.
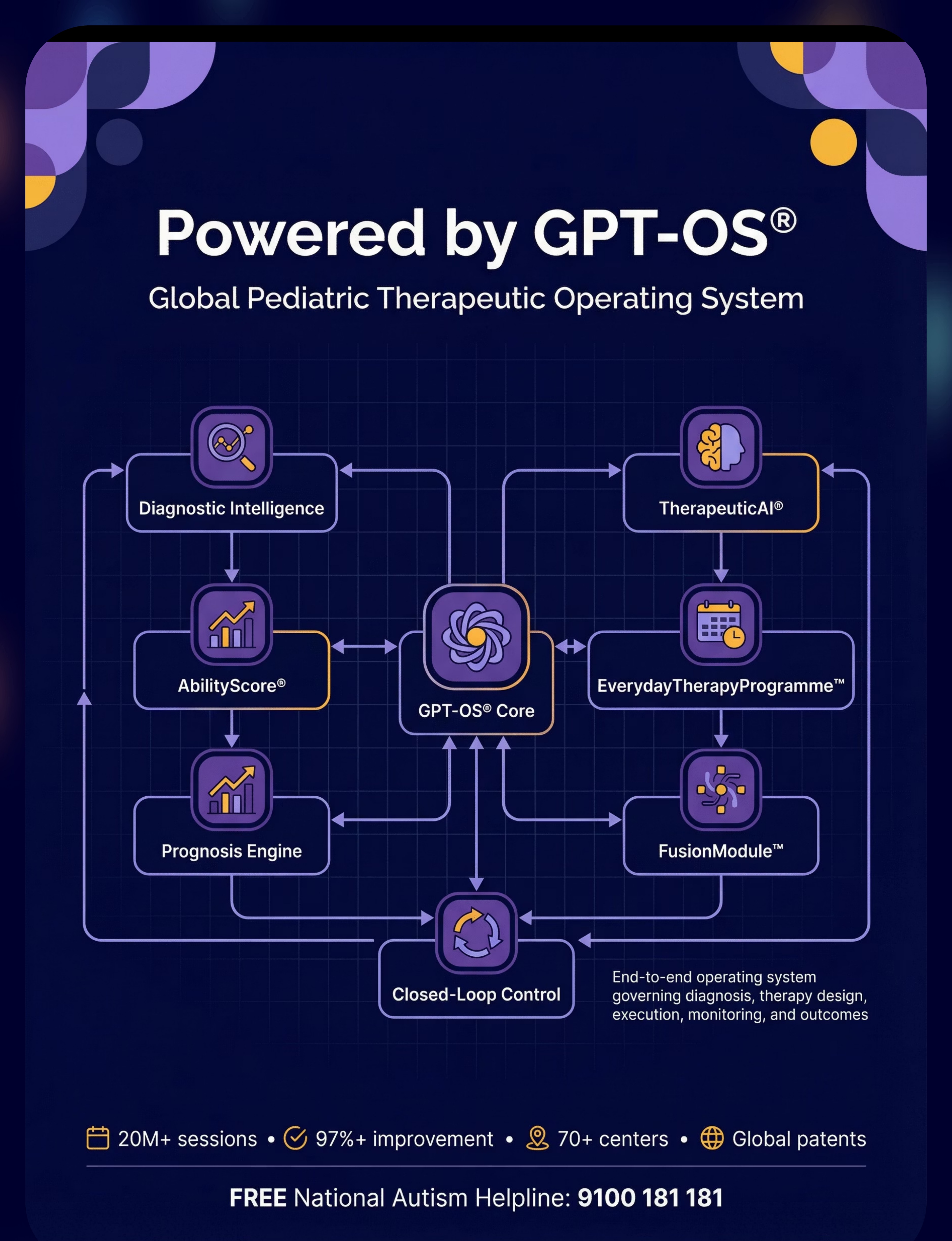
GPT-OS® Integration: Your session data feeds the Sensory Regulation Readiness Index, Self-Regulation Readiness Index, and Social Participation Readiness Index inside GPT-OS®. TherapeuticAI® uses this data to update your child's EverydayTherapyProgramme™ automatically. pinnacleblooms.org/my-child
📞9100 181 181 — Request a full 12-domain AbilityScore® assessment.
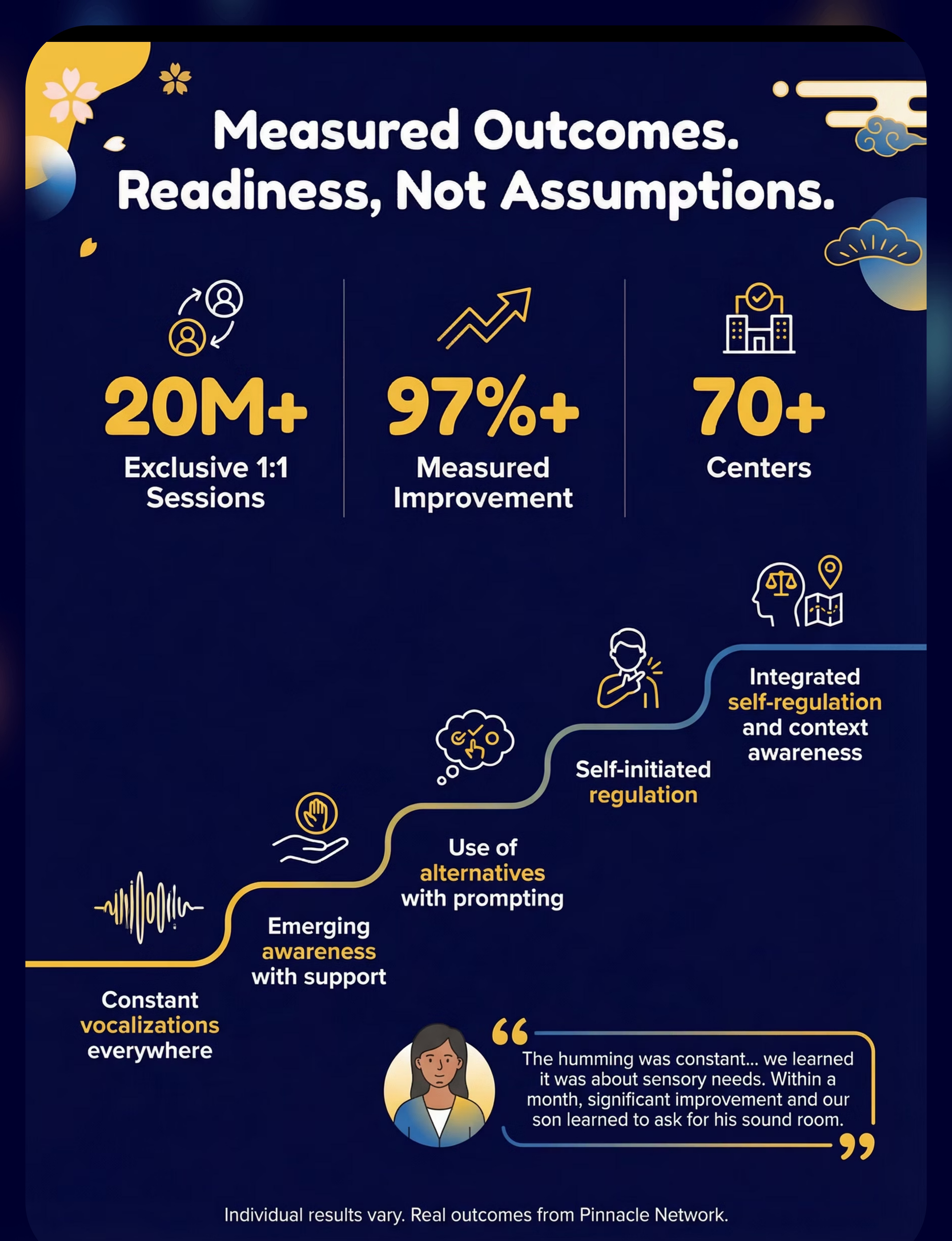
Real Families. Measured Outcomes. Not Assumptions.
"The humming was constant — car, restaurant, school, bedtime. We learned it was about vibration and auditory input. We introduced a vibrating pillow, a chewable necklace, and a corner we called his 'sound room.' Within a month, the constant humming reduced significantly. He still stims, but now he also regulates. He asks for his sound room. That's extraordinary."
— Parent, Pinnacle Hyderabad Centre
"My daughter squealed in every quiet environment — libraries were impossible. The noise-canceling headphones changed everything. She wears them before we enter. She's calmer, we're calmer. Her teacher said she participates in class now."
— Parent, Pinnacle Bangalore Centre
Individual results vary. Real outcomes from Pinnacle Network. See PMC11506176 for systematic evidence base.
📞9100 181 181 — Speak to a parent who has been through this journey. FREE peer support available.

You Don't Have to Figure This Out Alone.
WhatsApp Support Groups
Domain D: Stimming & Sensory Regulation. Join families across India navigating vocal stimming, sensory regulation, and school inclusion. pinnacleblooms.org/community
EverydayTherapyProgramme™
Daily home-based micro-interventions for vocal stimming regulation, delivered through the Pinnacle OTT platform.
GPT-OS® App
Track your child's regulation data, receive personalized daily prompts, and connect with your therapy team in real time.
70+ Centres Across India
In-person OT, SLP, ABA, and SpEd integrated therapy under the GPT-OS® framework. Find your nearest centre today.
"The families who implement these materials consistently report the fastest progress. Consistency requires community."
Clinical-Grade Support Is Closer Than You Think
For vocal stimming, you need an integrated team: an Occupational Therapist for sensory profile assessment and material selection, a BCBA/Behavior Analyst for functional behavior assessment and context-teaching, and a Speech-Language Pathologist to differentiate stimming from communicative echolalia.
Call FREE Helpline
📞9100 181 181 — Trained specialists available 24×7 in 16+ languages
Book AbilityScore® Intake
Comprehensive 12-domain developmental assessment by the Pinnacle Consortium
Receive Your Protocol
Personalized D-366 Sensory Substitution Protocol designed for your child's profile
Begin at Home
Start EverydayTherapyProgramme™ with daily guided micro-interventions
Online / Remote: Available in 16+ languages via teleconsultation. International families: pinnacleblooms.org/international
Deeper Reading for the Curious Parent. Or the Skeptical One.
Study | Key Finding | Link | |
PMC11506176 | PRISMA review: sensory integration is evidence-based for ASD, 16 studies 2013–2023 | pubmed.ncbi.nlm.nih.gov | |
PMC10955541 | Meta-analysis 24 studies: SI therapy improves social, adaptive, sensory, motor domains | pubmed.ncbi.nlm.nih.gov | |
PMC9978394 | WHO/UNICEF CCD: home-based caregiver interventions across 54 LMICs | pubmed.ncbi.nlm.nih.gov | |
DOI: 10.1007/s12098-018-2747-4 | Indian RCT: home-based sensory interventions, significant outcomes | doi.org | |
NCAEP 2020 | Sensory-based + behavioral strategies: evidence-based practice classification | National Clearinghouse on Autism | |
WHO NCF 2018 | Nurturing Care Framework: caregiver-delivered early intervention globally validated |
For professionals and researchers: Full Pinnacle clinical bibliography available at pinnacleblooms.org/research
Your Data Helps Your Child. And Every Child Like Them.
What GPT-OS® Learns from D-366 Data
- Which material types work for which stimming function profiles
- Optimal introduction timing
- Correlation between structured sound time frequency and context-switching emergence
- Weighted product efficacy by child's sensory profile
Privacy Protection
All data is de-identified at source. Individual profiles are protected under DPDP Act (India) and GDPR-equivalent standards. Pinnacle never sells data.
"Your data helps every child like yours. Every session recorded contributes to a smarter system for the next family."
See the Materials in Action — 60 Seconds of Clinical Demonstration
▶ Reel D-366 | Domain D2: Stimming & Repetitive Behaviours
What you'll see in this reel: A child using chewable jewelry, calm and regulated — followed by noise-canceling headphones in a noisy environment, a vibrating sensory tool with a satisfied expression, a weighted lap pad during seated activity, a designated stimming space with free expression, structured sound time with singing and instruments, and a before/after showing dysregulated stimming transitioning to a regulated state with supports.
Presenter
Pinnacle OT + SLP Consortium Specialist
Accessibility
Captions burned-in and timed | WCAG AA compliant
Next in Series
D-367 — 9 Materials That Help With Hand Flapping →
Consistency Across Caregivers Multiplies Impact
WHO research confirms: multi-caregiver consistency is the single most powerful predictor of home-intervention outcomes. Share this resource so grandparents, teachers, and extended family can support the same approach at home, at school, and on the go.
📲 Share on WhatsApp
"I found this resource on vocal stimming regulation — really helped me understand what our child needs. Have a look: techniques.pinnacleblooms.org/domain-d/vocal-stimming-materials-d366"
📄 D-366 Family Guide
Download the 1-page PDF — simple guide for grandparents, teachers, and other caregivers. No clinical background needed.
🏫 School Communication Template
Download the formatted letter requesting sensory accommodations for vocal stimming under school inclusion frameworks.
"Our child makes sounds they can't fully control — it's a brain difference, not misbehavior. We've learned that giving them a safe place to make sounds, and tools like chewable jewelry and headphones, helps them regulate. Please don't tell them to be quiet — offer the chewable instead. It helps." — Explain to Grandparents version
📞9100 181 181 — For caregiver training, call us FREE. | Citation: PMC9978394 (WHO/UNICEF)
Frequently Asked Questions — Answered by the Consortium
Q1: Should I try to stop my child from vocal stimming altogether?
No. Complete suppression is neither realistic nor healthy. Vocal stimming serves real neurological functions. The goal is regulation and context-awareness — teaching "here and now vs. there and later" — not elimination. Suppression without replacement causes anxiety and distress.
Q2: How do I know which material to start with?
Observe what the sounds provide. Humming/throat sounds → vibrating tools or chewables. Stimming in loud places → noise-canceling headphones. Stimming when bored or in quiet → personal audio. When unsure — start with the stimming space. It works for all functions.
Q3: My child's school says they can't accommodate this. What do I do?
Download the Teacher Communication Template (Card 37). Under Right to Education Act provisions, sensory accommodations for neurodevelopmental conditions are a recognized need. Call 9100 181 181 for school liaison support.
Q4: How long will this take to work?
Pattern shift typically emerges across 8–12 weeks with consistent daily use. Week 1–2: material exploration. Week 3–4: consolidation. Week 5–8: self-initiation emerging. Consistent with the systematic review evidence base.
Q5: My child is older (10–12). Is it too late?
No. Materials are adapted for all ages 3–12. Older children can also participate in designing their own regulation toolkit — which increases buy-in significantly. Self-advocacy language becomes central at this age.
Q6: Can I do this without a therapist?
You can begin with materials and the stimming space independently. For functional behavior assessment and a personalized protocol, OT + BCBA guidance is recommended. Call 9100 181 181 for a FREE initial consultation.
Q7: Is vocal stimming always autism?
No. Vocal stimming also occurs in ADHD, anxiety, developmental delay, sensory processing differences, and occasionally in neurotypical children. If unsure, a diagnostic assessment clarifies the profile and informs intervention.
Q8: My child also has echolalia. Is that the same as vocal stimming?
Different but related. Echolalia (repeating heard phrases) often has communicative functions. Vocal stimming is non-communicative. A speech-language pathologist differentiates these — this matters for intervention planning. Call us.

You Now Have Everything You Need to Begin.
20M+
Therapy Sessions
Informing every recommendation
97%+
Measured Improvement
Across Pinnacle Network families
70+
Centers
Across India | 70+ Countries served
🛡️ Validated by the Pinnacle Blooms Consortium®
OT • SLP • BCBA/ABA • SpEd • NeuroDev Pediatrics
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | DPIIT DIPP8651 | CIN U74999TG2016PTC113063
Preview of 9 materials that help with vocal stimming Therapy Material
Below is a visual preview of 9 materials that help with vocal stimming therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

The Pinnacle Promise: From Fear to Mastery. One Technique at a Time.
🛡️ Pinnacle Blooms Consortium®
OT | SLP | BCBA/ABA | SpEd | NeuroDev Pediatrics | CRO | WHO/UNICEF Aligned
"Every parent who reads this page should leave more equipped than when they arrived. Every child whose parent implements these materials deserves to be met with understanding — not commands to be quiet. This is what Pinnacle was built for."
Medical Disclaimer: This content is educational and does not replace individualized assessment and intervention from licensed occupational therapists, behavioral therapists, speech-language pathologists, or medical professionals. Vocal stimming can be associated with medical conditions requiring evaluation. Never punish, shame, or forcibly suppress stimming — this causes harm. Work with qualified professionals to understand function and develop appropriate support strategies. Individual results vary.
Statutory Identifiers
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Copyright
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
techniques.pinnacleblooms.org | 📞9100 181 181 FREE | 24×7 | 16+ Languages