
When the bathroom is the scariest room in the house.
Your child knows when they need to go. They're physically ready. They understand perfectly. But the moment you mention the toilet — their body goes rigid, their eyes fill with tears, and no reward in the world feels worth facing that fear.
Toilet Fear Intervention — C-289
Adaptive Behavior · Self-Care · Anxiety Management
This is not a training problem. This is not stubbornness. This is not manipulation. This is genuine, visceral, real terror — and it needs to be treated as terror, not defiance. You are not failing. Your child's nervous system is speaking. And today, we're going to listen.
🏛️Pinnacle Blooms Consortium — Validated by Pediatric OT • ABA • Clinical Psychology • Special Education • NeuroDev | WHO Nurturing Care Framework (2018): Early identification and caregiver-led intervention directly shapes developmental trajectories.

25% of children experience toileting difficulties. You are among millions of families navigating this exact challenge.
25%
Toileting Anxiety
of typically developing children experience some degree of toileting anxiety or resistance (Benninga et al., Journal of Pediatrics)
80%
ASD + Sensory
of children with ASD experience sensory processing differences that directly affect toileting comfort (PMC11506176 — Systematic Review, 2024)
4+
Months Typical
is the typical resolution duration with appropriate graduated intervention — not days, not weeks (Clinical consensus, Pediatric OT + Psychology literature)
Globally, pediatricians see toilet fear as one of the most underdiagnosed, over-dismissed challenges in early childhood. In India alone, with 27 million children aged 0–5 with developmental differences, toilet-related anxiety is widespread — and frequently met with harmful advice: "Just push through it." The Pinnacle Blooms Consortium — spanning 70+ centers, 20M+ therapy sessions — affirms: toilet fear is real, it is neurological, and it responds to the right tools.
PMC11506176 | PMC10955541 | WHO NCF 2018 | Padmanabha et al., Indian J Pediatr (2019) | NCBI PMC5346795
This is a wiring difference, not a behavior choice.
The Neuroscience
When a child with sensory processing differences approaches the toilet, multiple neurological systems activate simultaneously:
- Auditory cortex — pre-activates in anticipation of the 75–85 dB flush, triggering startle and threat response
- Vestibular system — registers genuine physical instability: dangling legs, large seat opening, no hand holds
- Interoceptive cortex — processes unfamiliar body sensations of elimination as potentially threatening
- Amygdala — classifies the entire bathroom as a threat environment, triggering fight/flight/freeze
- Prefrontal cortex — in children 2–8, not yet developed enough to override the amygdala's fear signal
What This Means for Your Child
Your child's brain is not broken. It is doing exactly what brains are designed to do: protect the body from perceived danger.
The terror they experience is not proportionate to the actual danger — but it is proportionate to what their nervous system perceives as danger. No reward, no punishment, no reasoning can override a live amygdala threat response.
What works: changing the input so the brain stops reading the bathroom as dangerous.
Frontiers in Integrative Neuroscience (2020): Environmental and sensory-based interventions have established neurobiological basis. DOI: 10.3389/fnint.2020.556660
Your child is here. Here is where we're heading.
1
Age 18m–2y
Physical readiness emerging
2
Age 2–3y
Typical toilet training window
3
Age 3–4y
Daytime dryness achieved (most)
4
Age 4–6y
Full independence developing
5
Age 6–8y
Generalization to public toilets
Highlighted Zone: Toilet fear can emerge at any point in this timeline and makes chronological progress irrelevant until the fear is addressed.
WHO/UNICEF developmental milestones set the typical window for toileting at 18 months–4 years — but these are built on neurotypical populations. For children with ASD, sensory processing disorder, anxiety disorders, or constipation history, the timeline looks meaningfully different — and that is entirely appropriate for this population.
Toilet fear frequently co-occurs with sleep resistance, meltdown patterns, food rigidity, and separation anxiety — all governed by the same threat-detection systems. Addressing toilet fear often creates positive ripple effects across all these domains. Approximately 40%+ of children with ASD referred to the Pinnacle Blooms Network present with toilet-related anxiety.
WHO Care for Child Development Package (2023) | PMC9978394 | UNICEF MICS Developmental Indicators

The Evidence Behind This Approach
🛡️ LEVEL II — STRONG EVIDENCE
Systematic Reviews + Multiple RCTs + Clinical Consensus
Graduated Exposure
Cochrane-reviewed gold standard for childhood phobia. Multiple RCTs: 80–90% resolution rates when conducted at child-paced, child-controlled pace. CBT/Exposure therapy systematic reviews (2022–2024)
Sensory-Based Modification
PRISMA systematic review (Children, 2024): 16 studies confirm sensory integration meets criteria for evidence-based practice in ASD — including environmental modifications. PMC11506176
ABA-Informed Reinforcement
NCAEP (2020): Reinforcement-based procedures are evidence-based for adaptive self-care skill acquisition in ASD populations. NCAEP EBP Report (2020)
Materials-Based Intervention
Meta-analysis (World J Clin Cases, 2024): Structured sensory integration using specific materials promoted adaptive behavior across 24 studies. Effect size: moderate-large. PMC10955541
"Clinically validated. Home-applicable. Parent-proven. Evidence reviewed by the Pinnacle Blooms Consortium across OT, ABA, Psychology, and NeuroDev disciplines."

Toilet Fear Desensitisation — Materials-Based Graduated Exposure Protocol
Parent-Friendly Name: "The Bathroom Bravery Programme"
A structured, multi-material intervention framework that systematically reduces toilet-related fear and avoidance in children aged 2–8 years by (1) modifying the sensory and physical environment to eliminate genuine threat triggers, (2) providing sensory comfort and body security during toileting, (3) building toilet familiarity through narrative and play, and (4) reinforcing approach behaviors through child-controlled graduated exposure at a pace set by the child.
This is NOT a toilet training programme for children who lack readiness. This IS a fear-resolution protocol for children who are physically and cognitively ready but whose nervous systems classify the toilet as dangerous.
🧠 Domain
Adaptive Behavior · Anxiety Management · Sensory Processing · ABA Graduated Exposure
👶 Age Range
2–8 years (adaptable for older children with developmental delays)
⏱️ Session
5–30 minutes · Daily or near-daily · Consistency is essential
📅 Timeline
4–16 weeks to full resolution (varies by fear severity)

This technique crosses therapy boundaries because fear doesn't organize itself by discipline.
Pediatric OT (Primary Lead)
Addresses the sensory architecture of toilet fear: proprioceptive insecurity, auditory sensitivity, vestibular instability, tactile aversion. The OT designs what materials change the sensory experience from threatening to tolerable.
BCBA / ABA Analyst (Co-Lead)
Designs the graduated exposure hierarchy (the Fear Ladder), the reinforcement schedule, and the data collection system. ABA provides the behavioral architecture that the OT's sensory modifications sit within.
Pediatric SLP
Addresses the social story and narrative component — building the child's understanding, giving language to the experience, and building the verbal self-regulation script: "My body is sending me a message. I know what to do."
Special Educator
Adapts materials for children with cognitive differences, ensures visual supports are at the right comprehension level, and builds the routine-based structure that makes graduated exposure predictable and safe.
NeuroDev Paediatrician
Rules out medical contributors (constipation, UTI, anatomical factors), considers pharmacological anxiety support, and provides the developmental context that guides timeline expectations.
This isn't a random activity. It's a precision intervention.
Observable Outcome Indicators
- Child enters bathroom without distress within 2 weeks
- Child sits on toilet (clothed) without panic within 4 weeks
- First successful elimination on toilet within 6–10 weeks
- Independent home toileting within 12–16 weeks
Why This Matters Beyond Toileting
Toilet independence is a prerequisite for mainstream school entry. It removes a major barrier to peer social inclusion and is one of the highest-impact self-care milestones a family can achieve together.
PMC11506176 | PMC10955541 | NCAEP EBP Report (2020)
9 materials. Each one removes a specific fear trigger.
Every material below targets a distinct layer of toilet fear — sensory, physical, emotional, or behavioral. Together, they form a comprehensive desensitization toolkit that transforms the bathroom from a threat environment into a safe one.
Toilet Seat Insert with Handles & Foot Support
Canon: Toileting Visuals / Supports · ₹800–2,500
Why it works: Eliminates the #1 fear — falling in. Child-sized opening, grip handles, firm foot support = genuine physical security.
Why it works: Eliminates the #1 fear — falling in. Child-sized opening, grip handles, firm foot support = genuine physical security.
Noise-Reducing Headphones / Ear Defenders
Canon: Noise-Reducing Headphones / Ear Defenders · ₹300–2,000
Why it works: Flush averages 75–85 dB. Ear defenders cut this to safe levels, removing the most common fear trigger.
Why it works: Flush averages 75–85 dB. Ear defenders cut this to safe levels, removing the most common fear trigger.
Social Stories & Toilet Preparation Books
Canon: Social Stories / Narrative Supports · ₹200–800
Why it works: Fear thrives in the unknown. When children understand what happens and why it's safe, imagination stops filling gaps with monsters.
Why it works: Fear thrives in the unknown. When children understand what happens and why it's safe, imagination stops filling gaps with monsters.
Bathroom Environment Modification Kit
Canon: Calm-Down Kit / Self-Regulation Toolbox · ₹500–3,000
Why it works: The bathroom itself triggers dysregulation before the child reaches the toilet. Environment modifications address this pre-toilet fear layer.
Why it works: The bathroom itself triggers dysregulation before the child reaches the toilet. Environment modifications address this pre-toilet fear layer.

9 Materials — Continued
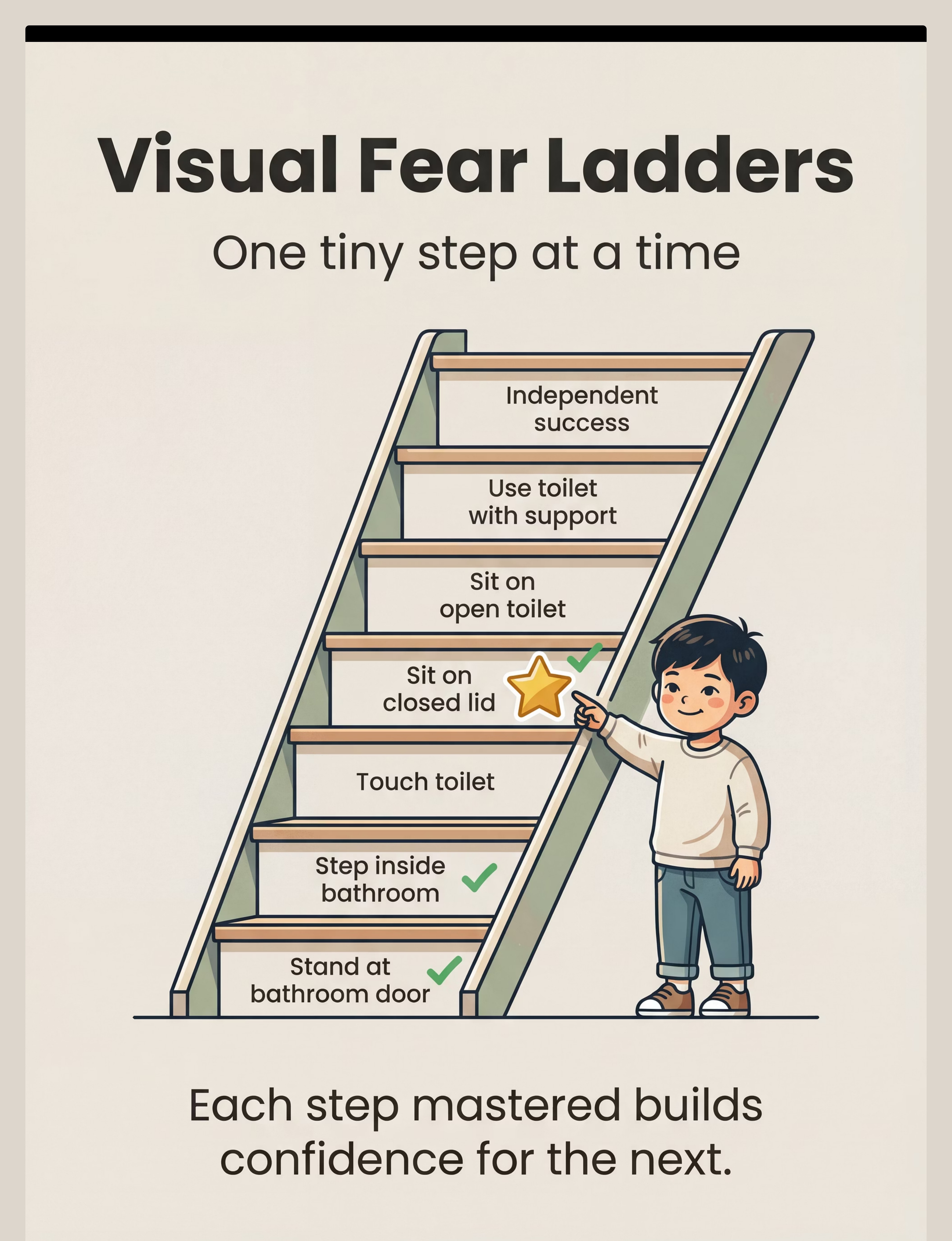
Visual Fear Ladder (Graduated Exposure Cards)
Canon: Visual Schedule System / Sequencing Cards · ₹100–500 or free DIY
Why it works: Graduated exposure is the clinical gold standard for childhood phobia. Visual ladders make progress concrete and child-controlled.
Why it works: Graduated exposure is the clinical gold standard for childhood phobia. Visual ladders make progress concrete and child-controlled.
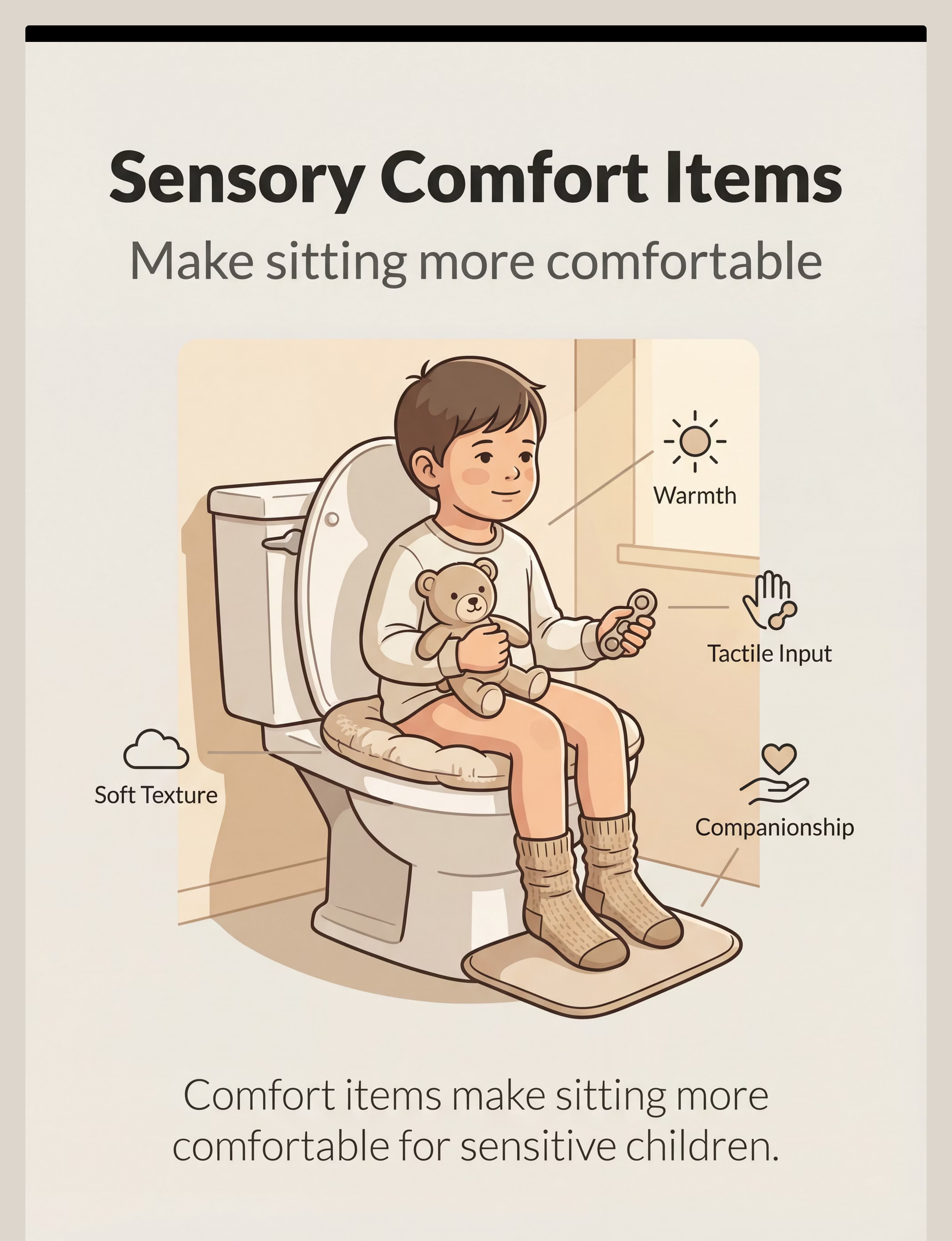
Sensory Comfort Items (Transition Objects)
Canon: Transition Objects / Comfort Items · ₹300–1,500
Why it works: The toilet is a sensorially vulnerable experience. A comfort companion and tactile input reduce sensory overwhelm and provide co-regulation.
Why it works: The toilet is a sensorially vulnerable experience. A comfort companion and tactile input reduce sensory overwhelm and provide co-regulation.
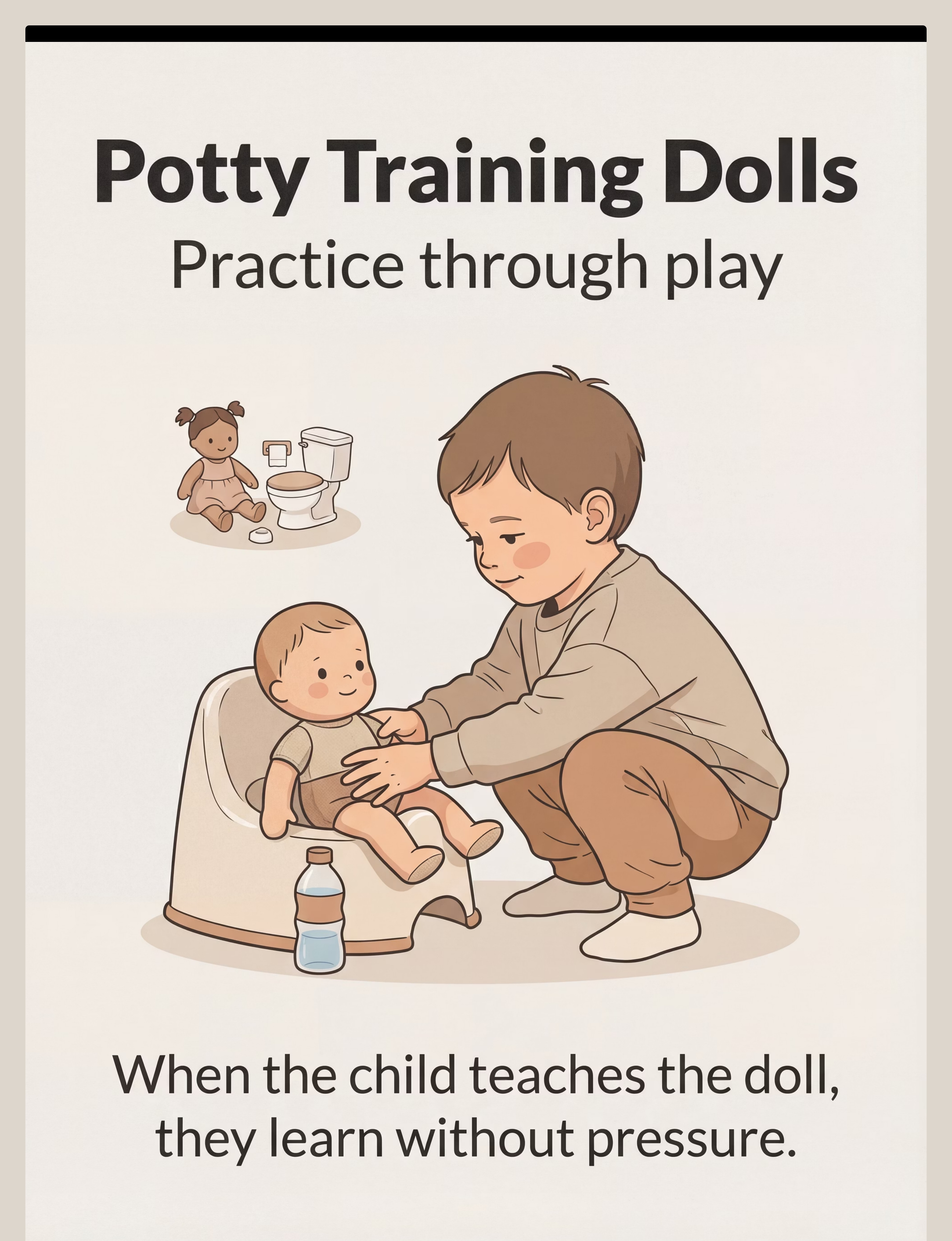
Potty Training Dolls & Role-Play Props
Canon: Role-Play / Pretend Play Props · ₹600–2,000
Why it works: Children learn through teaching. When the child "trains" the doll, they process their own fears through play — without pressure.
Why it works: Children learn through teaching. When the child "trains" the doll, they process their own fears through play — without pressure.
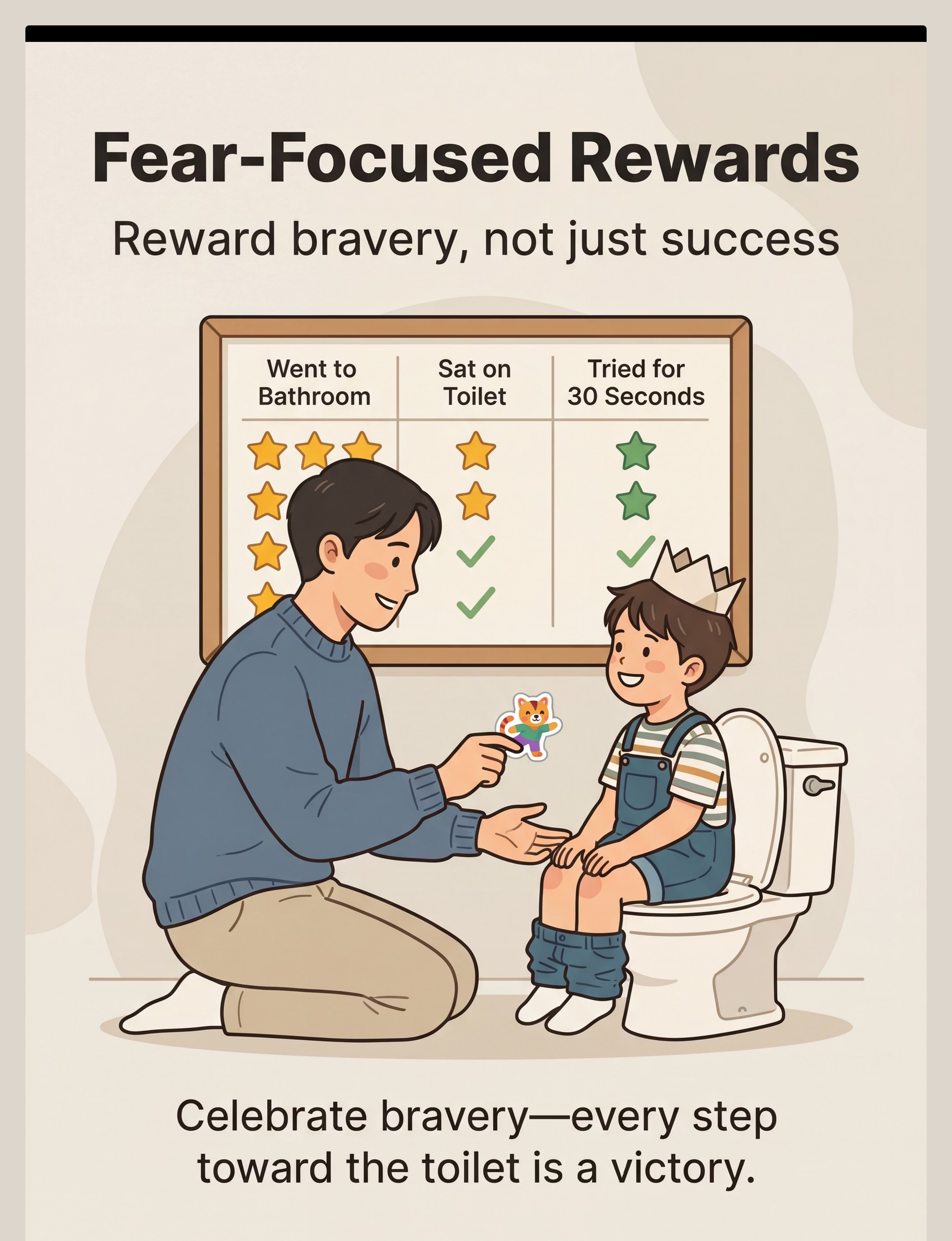
Fear-Focused Reward System
Canon: Reinforcement Menus · ₹100–589
Why it works: Standard rewards fail for fear because they reward the end result the child cannot reach. Fear-focused rewards celebrate every brave approach step.
Why it works: Standard rewards fail for fear because they reward the end result the child cannot reach. Fear-focused rewards celebrate every brave approach step.
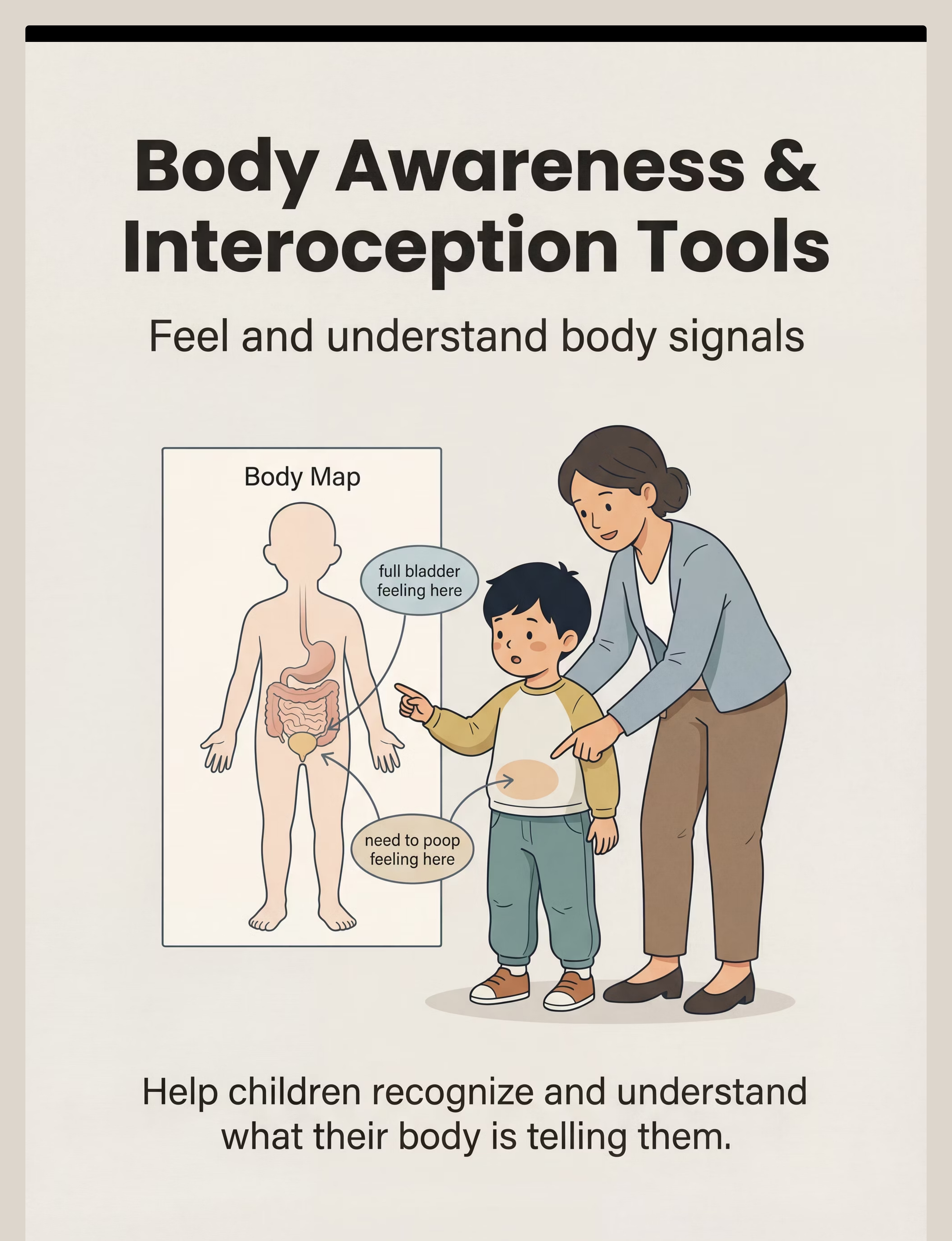
Body Awareness & Interoception Tools
Canon: Social Stories / Narrative Supports + Visual Schedule System · ₹200–800
Why it works: Some children can't feel elimination signals until urgent. Others find body sensations frightening. These tools build the interoceptive foundation toileting requires.
Why it works: Some children can't feel elimination signals until urgent. Others find body sensations frightening. These tools build the interoceptive foundation toileting requires.
Every parent can start today. No budget required.
WHO/UNICEF Equity Principle
Every intervention in the Pinnacle system has a zero-cost version. Access to therapy tools should not depend on ability to purchase.
Material | Clinical Grade | Zero-Cost DIY | |
Toilet seat security | Commercial insert with handles ₹800+ | Stable stool for feet + child holds parent's hands | |
Noise protection | Ear defenders ₹300+ | Parent's hands gently cupping ears; bathroom music during flush | |
Social story | Commercial book ₹200+ | Hand-written story with YOUR bathroom photos on paper | |
Environment modification | Commercial rugs/lighting ₹500+ | Bath towel as rug; dim main light + use phone torch | |
Fear ladder | Printed cards ₹100+ | Hand-drawn ladder on paper, star stickers for steps | |
Comfort companion | Commercial soft toy ₹300+ | Any beloved existing toy designated as "bathroom buddy" | |
Role-play | Commercial potty doll | Any doll + small container as pretend potty | |
Reward system | Commercial reward jar ₹589 | Handmade sticker chart on A4 paper | |
Body awareness | Commercial body map | Draw a simple body outline together on paper |
Consortium Guidance: For severe toilet phobia, the OT-grade toilet seat insert with handles and calibrated ear defenders deliver meaningfully better outcomes. When budget permits, Material 1 and Material 2 are the highest-priority clinical-grade purchases.

Read this card before any session. Every time.
🔴 RED — Do NOT Proceed
- Chronic constipation (3+ days without bowel movement regularly) — medical treatment MUST come first
- Recent painful elimination event (anal fissure, UTI, hard stool) — resolve physical pain before fear work
- Signs of encopresis (involuntary soiling) — requires medical management
- Child is acutely unwell, feverish, or post-meltdown
- Urinary withholding causing abdominal distension or pain
🟡 AMBER — Modify the Session
- Child had a difficult night or is over-tired → maintain last successful step only
- Upcoming stressful event → hold at current level, no new steps
- Parent is significantly stressed → brief your nervous system first
- Child showed regression in the last 48 hours → two steps back, one step forward
🟢 GREEN — Proceed
- Child is fed, rested, in baseline regulated state
- No recent painful elimination events
- Medical factors ruled out or managed
- Parent is calm with 20–30 uninterrupted minutes
- Today's fear ladder step has been pre-decided
STOP IMMEDIATELY IF: Child shows signs of extreme panic (hyperventilating, dissociation, vomiting from distress), child is hurting themselves trying to escape, or any sign of physical pain during elimination. This educational content does not replace assessment by a licensed OT or pediatric psychologist.

The bathroom needs to feel safe before the toilet can feel safe.
① Temperature
Warm the bathroom to 24–26°C before the session. Cold environments amplify sensory discomfort.
② Lighting
Replace harsh overhead fluorescent with a soft lamp or nightlight at child height. Harsh lighting increases vigilance and arousal.
③ Sound Absorption
Place a soft bath mat on the floor. Hard tile surfaces echo and amplify all sounds including the flush.
④ Comfort Items
Position the "bathroom buddy" (comfort toy) in a visible, accessible spot. It belongs here now.
⑤ Ear Defenders
Pre-positioned and easily accessible, associated with "bathroom brave gear."
⑥ Toilet Setup
Insert mounted securely. Foot stool positioned. ZERO wobble. Grip handles within easy reach.
⑦–⑩ Final Checks
- Visual ladder — mounted at child eye height, today's step visible
- Reward system — ready and visible from inside bathroom
- Door — can be left ajar; never lock
- Distractions removed — no audience, no siblings, no phones
Parent Positioning
Sit or kneel to child height. Physical proximity but not blocking the exit. Your body language communicates: "There is no threat here. I am calm. You are safe."

The best session is one that starts right.
60-Second Readiness Assessment
Child has eaten within the last 2 hours
Hunger amplifies dysregulation and lowers the fear threshold.
Child has slept adequately
Fatigue reduces regulatory capacity — a tired child cannot access their window of tolerance.
Child is at baseline regulation
Not mid-meltdown or immediately post-meltdown. The nervous system needs a calm starting point.
No recent painful elimination event
Within the last 24 hours. Pain creates rational avoidance that cannot be addressed by behavioral intervention alone.
You are regulated
Your nervous system is your child's first co-regulator. Your calm is their calm.
✅ All 7 Green
GO — Proceed to Step 1: The Invitation
⚠️ 1–2 Amber
MODIFY — Stay at last mastered step; no advancement today
🛑 3+ or Any Red
POSTPONE — Read the toilet social story together instead. Progress doesn't require a bathroom every session.

STEP 1 of 6
The Invitation
Core Principle: Every session begins with an invitation, not a command. The child must choose to approach. Choice is the antidote to forced exposure trauma.
"I have your Brave Kit ready in the bathroom. Your [comfort animal] is already there. Would you like to come do your bathroom brave work with me today?"
Why This Wording Works
- "Brave Kit" reframes tools as the child's equipment — they are the agent
- Announcing the comfort animal first reduces the approach cost
- "Would you like to" gives genuine choice — child must say yes for exposure to be therapeutic
If Child Resists
If child says no: "That's okay. Let's read [toilet book] together then." Do NOT force. Reschedule for later.
If child hesitates: "Let's just go look at your brave chart — we don't have to do anything you're not ready for."
Timing: 30–60 seconds. Do not extend this phase. Parent Body Language: Kneel to child height. Relaxed face. No urgency in posture. A smile that says "this is fine either way."
STEP 2 of 6
The Engagement — Approaching the Bathroom
What's Happening: The child has accepted the invitation. Now: the approach. This step is entirely about making the journey to the bathroom safe and predictable. The bathroom is not the goal yet — approaching it is.
"Look at your brave chart — what step are we at today? [Point to visual ladder.] That's where you are. You've already done all of these. Today we're going to [describe today's specific step]."
The Fear Ladder — Sample Sequence (adapt to child)
Stand at bathroom door (outside)
Step into bathroom, stay 10 seconds, leave
Touch the toilet (lid closed)
Sit on closed toilet lid (fully clothed, 10 seconds)
Sit on open toilet with clothes on
Sit on toilet with clothes lowered (no elimination required)
Sit on toilet during likely elimination time (with support)
First successful elimination (celebrated enormously)
Today's Step Principle: Only advance one step when the child shows ZERO distress at the current step on 3 consecutive sessions. Distress-free mastery is the only gate — not time elapsed. Timing: 2–5 minutes. Approach + arrival only.

STEP 3 of 6
The Therapeutic Action
This is the active ingredient — the specific exposure the child is ready for today, executed with full sensory modification support. The therapeutic action is not "use the toilet." The therapeutic action is "tolerate today's step without distress."
If Today's Step Involves the Toilet Seat
Insert is mounted and checked for zero wobble. Child places both feet firmly on step stool. Child grips handles. Parent says: "You can feel how it won't let you fall. Your hands are holding on. Your feet are on the floor." Ear defenders ON if flush is anywhere near.
If Today's Step Involves Sound Desensitization
Ear defenders on. Child controls when to flush — "You press it when you're ready. You can leave if you need to." Practice flushing from outside bathroom first. Then doorway. Then inside.
If Today's Step Involves Sitting
Comfort animal on lap. Fidget toy in hand. Visual timer: "Just [30 seconds / 1 minute] — then we're done." Parent sits at child height beside them — not watching, but present.
✅ Ideal
Calm, engaged, body relaxed
✅ Acceptable
Mild anxiety, manageable, staying at the step
🛑 Concerning
Crying, rigidity, panic — return to last mastered step immediately
ABA Graduated Exposure Protocols | OT Sensory Modification Literature | NCAEP EBP (2020)

STEP 4 of 6
Repeat & Vary
Therapeutic Dosage
- Repetitions per session: 1–3 approaches to the same fear ladder step
- Session frequency: Daily or near-daily — consistency builds the neural path faster than intensity
- Step advancement: Only after 3 consecutive distress-free sessions at current step
3 calm, successful repetitions are worth more than 10 pressured attempts.
Variation Options
Variation A — Bring the Doll: Have the child "teach the doll" to do today's step. Role reversal externalizes the fear and gives the child agency.
Variation B — Story Time in the Bathroom: No toileting agenda — just read the toilet social story while sitting (clothed) on the bathroom floor. Rewires its emotional valence.
Variation C — Bathroom "Explorer" Mode: For very young or severely avoidant children: explore the bathroom as scientists. "What does the tap sound like? Touch the rug. How soft is it?" Curiosity is incompatible with fear.
Satiation Indicators (when child has had enough): Interest in comfort object drops · Increased fidgeting or restlessness (not fear, just boredom) · Child says "done" or equivalent. Timing: 3–8 minutes total for this phase.

STEP 5 of 6
Reinforce & Celebrate
The ABA Principle Applied to Fear: For toilet fear, the target behavior is approach — not elimination. The child who walks to the bathroom door today deserves exactly as much celebration as the child who sits on the toilet.
"You were SO brave. You [did today's specific step]. That was hard, and you did it anyway. I am so proud of you."
Why Specificity Matters: "Good job" is vague. "You stood at the bathroom door for 10 whole seconds even when your tummy felt scared — THAT is brave" creates a specific, retrievable memory of success that the brain returns to.
Token/Sticker System
Star on fear ladder for today's step. Rosette Reward Jar (₹589) or 1800+ Reward Stickers (₹364)
Social Celebration
High five, special dance, parent cheering — for children motivated by social approval
Token Economy
Tokens accumulate toward a preferred activity or small item
Immediate Tangible
Small preferred item immediately after the step — for children needing high motivation
Critical Rule: Never remove previously earned rewards due to regression. Regression is a normal part of fear recovery — not a behavior to punish.

STEP 6 of 6
The Cool-Down
The Principle: No session ends abruptly. The cool-down prevents post-session dysregulation and closes the loop on a positive, predictable note. "Done and proud" — not "done and uncertain."
Transition Warning
30–60 seconds before ending: "We have time for one more. Then we're all done with brave work for today."
If child resists ending: This is positive — the child is comfortable and engaged. Offer one more brief continuation, then close with the same ritual.
Post-Session
Within 60 seconds of session ending → go to the Data Capture step while memory is fresh. Capturing data immediately after the session is part of the protocol, not optional.
NCAEP EBP (2020) — Visual supports and transition procedures as evidence-based practices for ASD

60 seconds of data now saves hours of guessing later.
Today's Step
Which fear ladder step did you attempt? Record the specific step number and description while it's fresh.
Distress Level (0–5)
0 = Completely calm | 3 = Manageable anxiety | 5 = Panic/session ended early. Record today's score.
Duration
How long did the child tolerate today's step? Record in seconds or minutes.
Weekly Tracking Pattern
- Distress score decreasing over 3+ sessions = ready to advance
- Distress score stable or increasing = step is too advanced; modify
- Sudden regression after previous progress = check for environmental stressors or medical factors
GPT-OS® Data Integration
This data feeds directly into your child's AbilityScore® — Self-Care Skills Readiness Index and Anxiety Management Readiness Index. Each session captured improves the TherapeuticAI® recommendation engine for your child specifically.
Session abandonment is not failure — it's data.
Problem: Child refused to enter the bathroom at all
What happened: Fear is activated from a distance. Today's ladder step is too far ahead of current tolerance.
Next time: Back off to last comfortable step — even standing at the hallway looking toward the bathroom counts as progress.
Next time: Back off to last comfortable step — even standing at the hallway looking toward the bathroom counts as progress.
Problem: Child had a panic attack / extreme distress
What happened: The session attempted a step beyond the child's current window of tolerance.
Next time: Return to a step 2–3 rungs below where the panic occurred. Rebuild trust before advancing again. If panic attacks are frequent, professional psychological support is warranted.
Next time: Return to a step 2–3 rungs below where the panic occurred. Rebuild trust before advancing again. If panic attacks are frequent, professional psychological support is warranted.
Problem: Child used to be fine at this step but now refuses
What happened: Regression — normal and expected in fear work. Common triggers: illness, travel, new sibling, school change.
Next time: Treat regression as returning to an earlier chapter, not starting over. Previous neural pathways are not erased — they need reactivation.
Next time: Treat regression as returning to an earlier chapter, not starting over. Previous neural pathways are not erased — they need reactivation.
Problem: Rewards aren't working — child doesn't care about stickers
What happened: The reinforcer is not potent enough or not individualized.
Next time: Conduct a preference assessment — what does the child actually want? Electronics time? A specific food? A preferred activity? The reinforcer must be genuinely motivating.
Next time: Conduct a preference assessment — what does the child actually want? Electronics time? A specific food? A preferred activity? The reinforcer must be genuinely motivating.
Problem: Child is fine at home but panics in school/public bathrooms
What happened: Generalization hasn't occurred yet — automatic flushes, strange smells, different sounds, no familiar materials.
Next time: This is Phase 4 of the exposure sequence. It comes AFTER home mastery. Do not attempt school bathroom work while still establishing home mastery.
Next time: This is Phase 4 of the exposure sequence. It comes AFTER home mastery. Do not attempt school bathroom work while still establishing home mastery.
Problem: Other family members are undoing the progress
What happened: Inconsistent approach across caregivers.
Next time: Share the Family Guide with all caregivers. Consistency across all people is essential for fear extinction.
Next time: Share the Family Guide with all caregivers. Consistency across all people is essential for fear extinction.

No two children have the same fear. No two protocols should be identical.
⬇️ Easier
Stay outside the bathroom for first 5+ sessions · Role-play with doll as primary fear exposure · Read toilet books as sole "bathroom work" for 1–2 weeks · Bathroom play with NO toilet expectations
Standard
Core protocol as described in Steps 1–6 · Full fear ladder with daily sessions · Sensory modifications fully deployed · 4–16 week timeline
⬆️ Harder
Introduce elimination timing to toilet sits · Practice at a second bathroom in the home · Visit familiar locations for generalization · Introduce public bathroom visits with ear defenders (family/accessible bathroom first)
Sensory Profile Adaptations
Auditory-sensitive: Focus 60% of protocol on flush desensitization. Child controls all flushing. White noise machine to reduce bathroom echo.
Proprioceptive/vestibular: Extended time on physical security work. Let the child test the security themselves: "Try to fall. You can't. Show me."
Interoceptive: Dedicate extra time to body awareness work. Practice naming body sensations throughout the day in ALL contexts — not just bathroom.
Age Adaptations
2–3 years: All work through play and doll. Fear ladder maximum 5 steps. Sessions maximum 10 minutes.
4–6 years: Full protocol as described. Engage child in making the ladder.
7–8 years: Child co-designs the protocol. More language-based processing. Can explain "what would help?"
Week 1–2
Progress: 15%
If your child entered the bathroom doorway without screaming — that IS progress.
✅ What Progress Looks Like
- Willingness to look at toilet books without distress
- Walking toward (not into) the bathroom when asked
- Reduced anticipatory anxiety when bathroom is mentioned
- First distress-free step on the fear ladder
❌ Not Expected Yet
- Sitting on the toilet
- Any elimination on the toilet
- Reduced distress at higher fear ladder steps
- Generalization to other bathrooms
"You may feel impatient. The world has opinions. The school is calling. Family members are questioning. This is the hardest phase — when you're doing everything right and seeing small changes that look like nothing to anyone else. Trust the data on your tracking sheet. If distress scores are decreasing — even by 1 point — the nervous system is learning safety. That is the work."
PMC11506176 — 8–12 week outcome timeline evidence | Clinical milestone literature

Week 3–4
Progress: 40%
The brain is forming new pathways. Watch for these consolidation signs.
Child asks about the fear ladder spontaneously
Self-initiated engagement with the protocol is a strong indicator of internal motivation developing.
Distress is reducing predictably session-to-session
Watch for consistent downward trends in your distress scores — even small reductions are neurologically significant.
Child starts to show pride in their progress
Pointing to completed ladder steps, telling other family members — this is the prefrontal cortex beginning to create a "brave" identity.
Less overall household tension around bathroom time
The nervous system shift in the child is measurable at the family level. When the bathroom stops being a battleground, co-regulation improves for everyone.
Child starts testing materials independently
Putting on ear defenders, sitting on the toilet seat insert without being asked — this is the most powerful consolidation signal.
Neural Pathway Formation: What you are observing in weeks 3–4 is neurological change — repeated safe bathroom experiences are literally building new synaptic connections in the prefrontal cortex that can begin to modulate the amygdala's threat signal. This cannot be rushed. But it is happening. Parent Milestone: You may notice you are less anxious about bathroom time too. That is your own nervous system recalibrating.

Week 5–8
Progress: 75%
You're approaching the moment that will change your family's daily life.
75%
Progress Achieved
Approaching full mastery of home toileting
3/3
Mastery Gate
3 consecutive distress-free sessions at all home bathroom steps
0–1
Target Distress
Distress scores consistently at 0–1 at all home bathroom steps
Mastery Criteria — What It Looks Like
Child approaches bathroom without prompting for elimination needs
Child sits on toilet comfortably (with insert/supports) without significant distress
First successful elimination on toilet with parent support — celebrated enormously
Consistent daily eliminations on toilet with decreasing support needs
Mastery Confirmation: Does progress persist if you skip the formal reward system for 2 days? Does the child self-initiate bathroom visits when at baseline regulation? Can sessions reduce from daily to every-other-day without regression? If yes to all three: mastery is confirmed.
You did this. Your child grew because of your commitment.
Your child told fear: not today. They did it scared. They did it uncertain. They did it even when every instinct in their nervous system screamed "danger." And they did it because you created safety, consistency, and a path they could walk at their own pace.
"You understood that toilet fear is real, not willful. You refused to force, shame, or rush. You built a fear ladder and let your child climb it. You celebrated bravery — not just success. You gave your child their first experience of conquering a fear they chose to face. This is not a small thing."
🏆 Family Celebration
Create a "Brave Work Complete" certificate with your child. Let them design it. Frame it. This is a real achievement that deserves a real marker.
📓 Journal Prompt
"Today my child [describe what felt impossible 8 weeks ago]. What I was feeling when we started. What I'm feeling now. What my child said about the toilet today."
📤 Share This Moment
Share in the Pinnacle Parent Community — your story is the hope another family needs right now.
Trust your instincts — if something feels wrong, pause and ask.
🔴 Chronic Constipation Returning
If stool withholding is causing physical distension, abdominal pain, or 3+ days without bowel movement: pause behavioral work, seek medical evaluation immediately.
🔴 Encopresis
Involuntary overflow soiling requires medical management before behavioral work can resume.
🔴 Panic Attacks Generalizing
If toilet fear anxiety is spreading to other situations — refusing to leave home, extreme anxiety about other bodily functions: refer to pediatric psychologist.
🔴 No Progress After 8 Weeks
Professional OT + psychology assessment is warranted if there is genuinely no measurable progress after 8 weeks of consistent, well-executed work.
Escalation Pathway
- Teleconsultation with Pinnacle OT or Psychologist
- In-center assessment at nearest Pinnacle Blooms Network center
- If medical factors: Pediatric Gastroenterologist referral
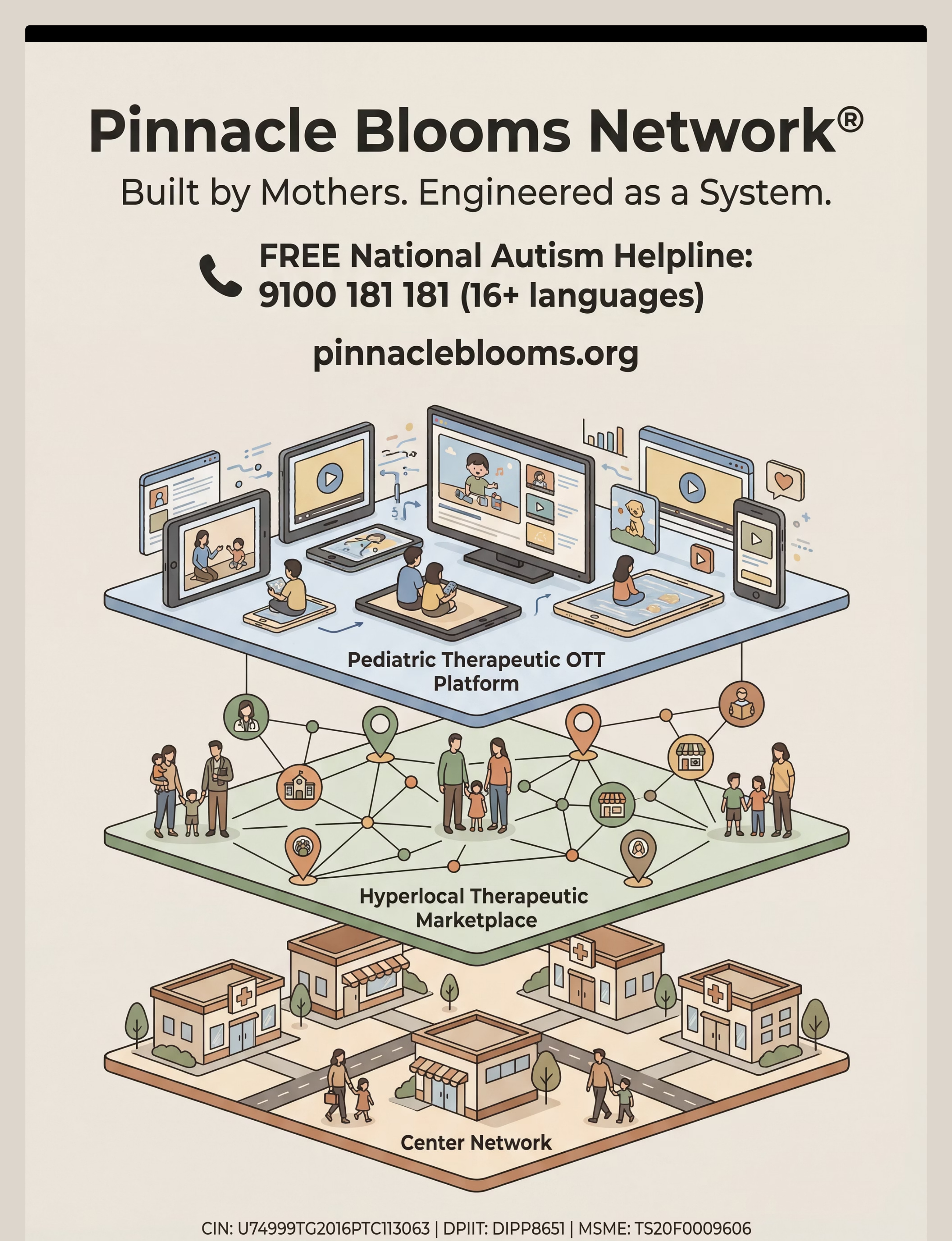
Free Support — Right Now
FREE National Autism Helpline: 9100 181 181
Available 24x7 | 16+ languages
For professional guidance and center referral
Available 24x7 | 16+ languages
For professional guidance and center referral
Toilet fear resolution is one waypoint. Here's the full journey.
📍 YOU ARE HERE: C-289 Toilet Fears
Path A — Autism/ASD Deepening → C-290
For children with ASD requiring more systematic approach with visual schedules and ABA-structured sessions
Path B — Nighttime Training → C-291
Once daytime toileting is established, address nocturnal enuresis with targeted nighttime strategies
Path C — Public Bathroom Generalization → C-292
For children who have mastered home toileting but panic at school or public bathrooms
Path D — Medical Factors → C-295
If constipation remains a contributing factor after behavioral resolution is achieved
Long-Term Developmental Goal: Full adaptive independence in self-care skills → school inclusion readiness → peer social participation → reduced caregiver burden → improved family wellbeing.
You already own materials for some of these.
Technique | Difficulty | Canon Materials You Already Have | |
C-287: Toilet Readiness Assessment | 🟢 Intro | Visual Supports | |
C-290: Autism-Specific Toilet Training | 🟡 Core | Social Stories + Reinforcement | |
C-291: Nighttime Dryness | 🟡 Core | Visual Timer + Comfort Items | |
C-295: Constipation Management | 🟡 Core | Body Awareness Tools | |
C-298: School Bathroom Preparation | 🟡 Core | Ear Defenders + Fear Ladder | |
C-156: Sensory Sensitivity Management | 🟢 Intro | Fidget Kit + Noise Headphones |
You already own: Ear Defenders + Comfort Items + Reinforcement Menus (purchased for C-289) → directly usable in C-290, C-156, and C-291. Your investment in this technique continues to pay forward.
Toilet fear resolution is one piece of a larger plan.
Toilet fear does not exist in isolation. It connects to sensory processing (Domain A), anxiety management (Domain C), and self-care independence (Domain E). Children who overcome toilet fear frequently show improvements across all three domains simultaneously — because the graduated exposure skills, body awareness tools, and sensory modification strategies transfer broadly.
The GPT-OS® FusionModule™ coordinates this cross-domain data so your child's full therapeutic profile is always being optimized — not just one domain at a time.
WHO/UNICEF Nurturing Care Framework (2018) — 5 nurturing care components require holistic developmental monitoring.
They started exactly where you are.
Family 1 — Hyderabad, Child aged 5
Before: Complete toilet avoidance since age 3. School enrollment delayed by 6 months.
After (14 weeks): Child uses home toilet independently and school bathroom with ear defenders.
After (14 weeks): Child uses home toilet independently and school bathroom with ear defenders.
"The fear ladder was the turning point. She made it herself. When she crossed off Step 3 — just sitting on the closed lid for 30 seconds — she ran to tell her grandmother. That's when I knew we were going to be okay."
Family 2 — Bengaluru, Child aged 4, ASD
Before: Auditory sensitivity to flush was primary trigger — even neighbors' toilets triggered full meltdowns.
After (8 weeks): Child wears ear defenders, controls timing himself.
After (8 weeks): Child wears ear defenders, controls timing himself.
"The moment I stopped trying to get him to flush without covering his ears — and just gave him complete control over when and how it happened — the whole thing shifted in one week."
Family 3 — Delhi, Child aged 6, SPD
Before: Triple sensory trigger. Parents had tried 11 different approaches over 2 years.
After (16 weeks): Full toilet independence at home.
After (16 weeks): Full toilet independence at home.
"We wish someone had told us earlier: this is NOT a willpower problem. There is no amount of pushing that fixes sensory fear. When we understood that, we stopped fighting her and started building with her."
Isolation is the enemy of adherence. You need a community.
WhatsApp Parent Group
Toilet Training & Bathroom Fears Parent Group. Real parents, real progress, real-time support. Moderated by Pinnacle clinical staff.
Pinnacle Online Forum
Evidence-based discussion, technique sharing, milestone celebration, peer mentoring at pinnacleblooms.org/community
Local Parent Meetups
Organized monthly at 70+ center locations. Real families, guided by clinical staff. Find your nearest meetup via center locator.
Peer Mentoring Programme
Connect with a parent who has successfully navigated toilet fear with their child. One conversation can change everything.
A Note on Joint Family Contexts: In Indian households, grandparents and family members often have strong opinions about toilet training. The Pinnacle Parent Network includes specific guidance on navigating family pressure while maintaining the evidence-based approach. You are not alone in this.
Home + clinic = maximum impact.
When to Bring in Professionals
- Fear is severe and not reducing after 3 weeks of consistent home work
- Child has ASD with complex sensory profile requiring full OT assessment
- Medical constipation requiring Pediatric GI support
- Anxiety extending beyond toileting
- Family under significant stress impacting the home protocol
Pinnacle Blooms Network — Clinical Support
🏥70+ Centers across India — Pediatric OT, ABA/BCBA, SLP, Special Education, NeuroDev under one roof, one GPT-OS® protocol
💻Teleconsultation — Remote OT and psychology sessions for families in non-center locations
📊AbilityScore® Assessment — Maps Self-Care Skills Readiness Index, Sensory Profile, and Anxiety Management profile, providing a clinical baseline and personalized therapeutic plan
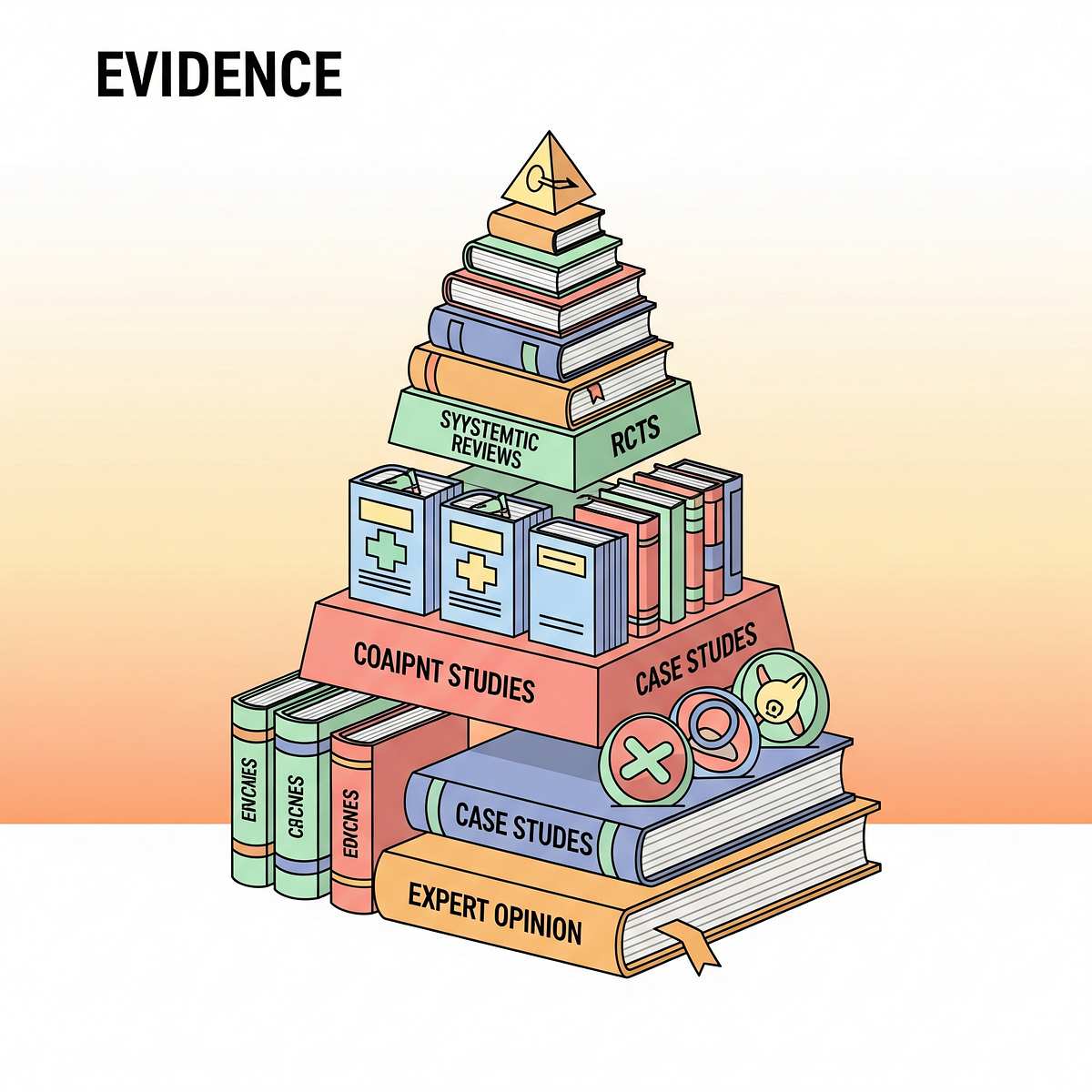
Deeper reading for the curious parent. Evidence pyramid included.
Systematic Review — Children, 2024
Sensory integration intervention meets criteria as evidence-based practice for children with ASD across 16 studies (2013–2023). Evidence Grade: Level I. PMC11506176
Meta-Analysis — World J Clin Cases, 2024
Sensory integration therapy effectively promotes adaptive behavior and social participation across 24 studies. Effect size: moderate-large. PMC10955541
India-Specific — Indian J Pediatr, 2019
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric populations when parent-administered with structured guidance. Padmanabha et al.
Toileting Resistance — Journal of Pediatrics
~25% of children experience toileting difficulties; graduated exposure approaches are effective for fear-based toileting resistance. NCBI PMC5346795
WHO Nurturing Care Framework, 2018
Evidence-based caregiver-led interventions in home environments drive the strongest long-term developmental outcomes in early childhood. nurturing-care.org
NCAEP EBP Report, 2020
Reinforcement procedures, visual supports, and graduated exposure classified as evidence-based practices for ASD — applicable to adaptive skill development including toileting.
Your data helps every child like yours.
What GPT-OS® Learns from C-289 Data
- Rate of fear reduction (distress score trajectory)
- Which specific materials are most effective for which fear profiles
- Optimal step progression pace by age, diagnosis, and sensory profile
- Which children benefit from additional professional support at which points
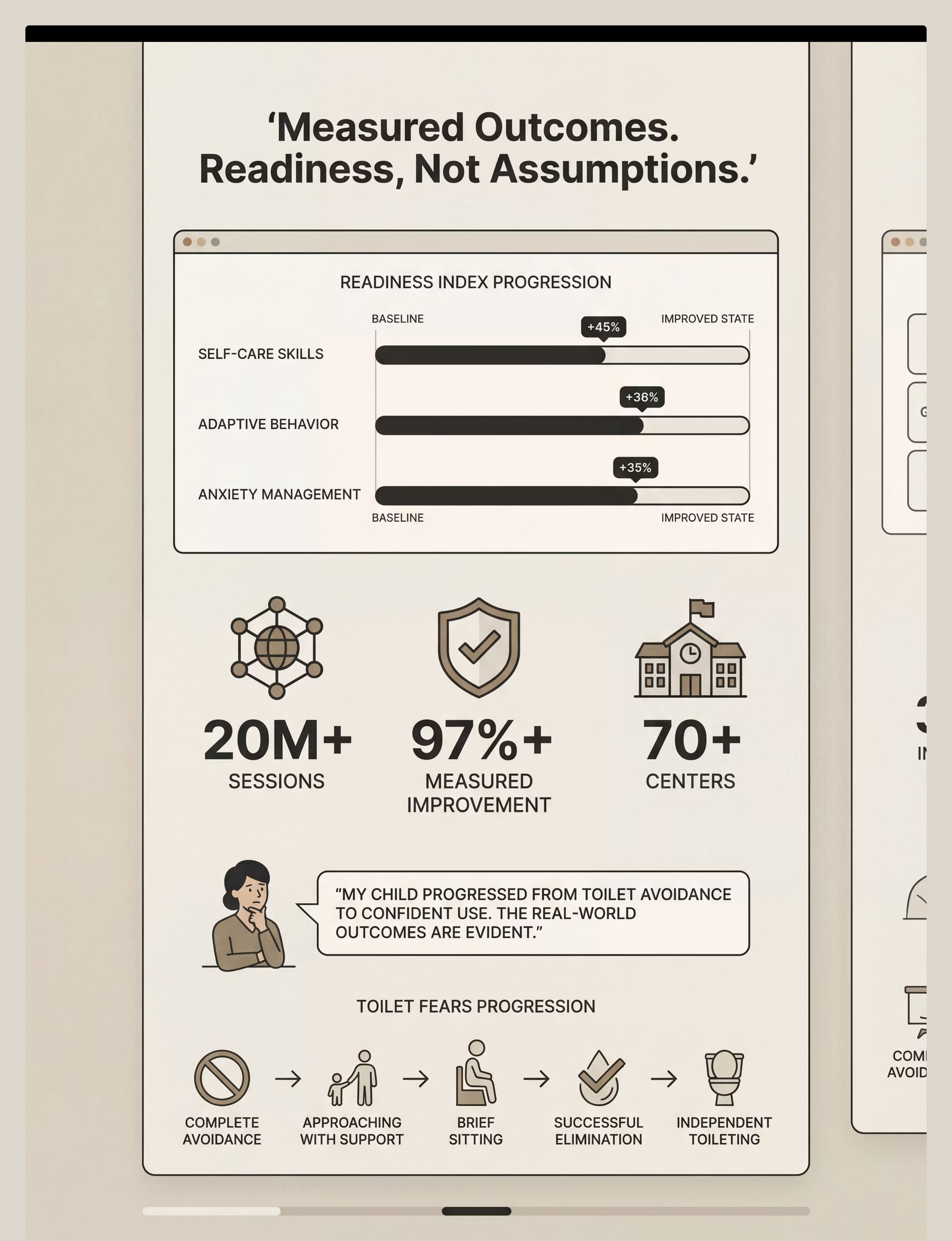
20M+ sessions across 70+ centers creates population-level patterns that no individual clinician could see. Your child's data improves recommendations for all families navigating toilet fear — across India and 70+ countries.
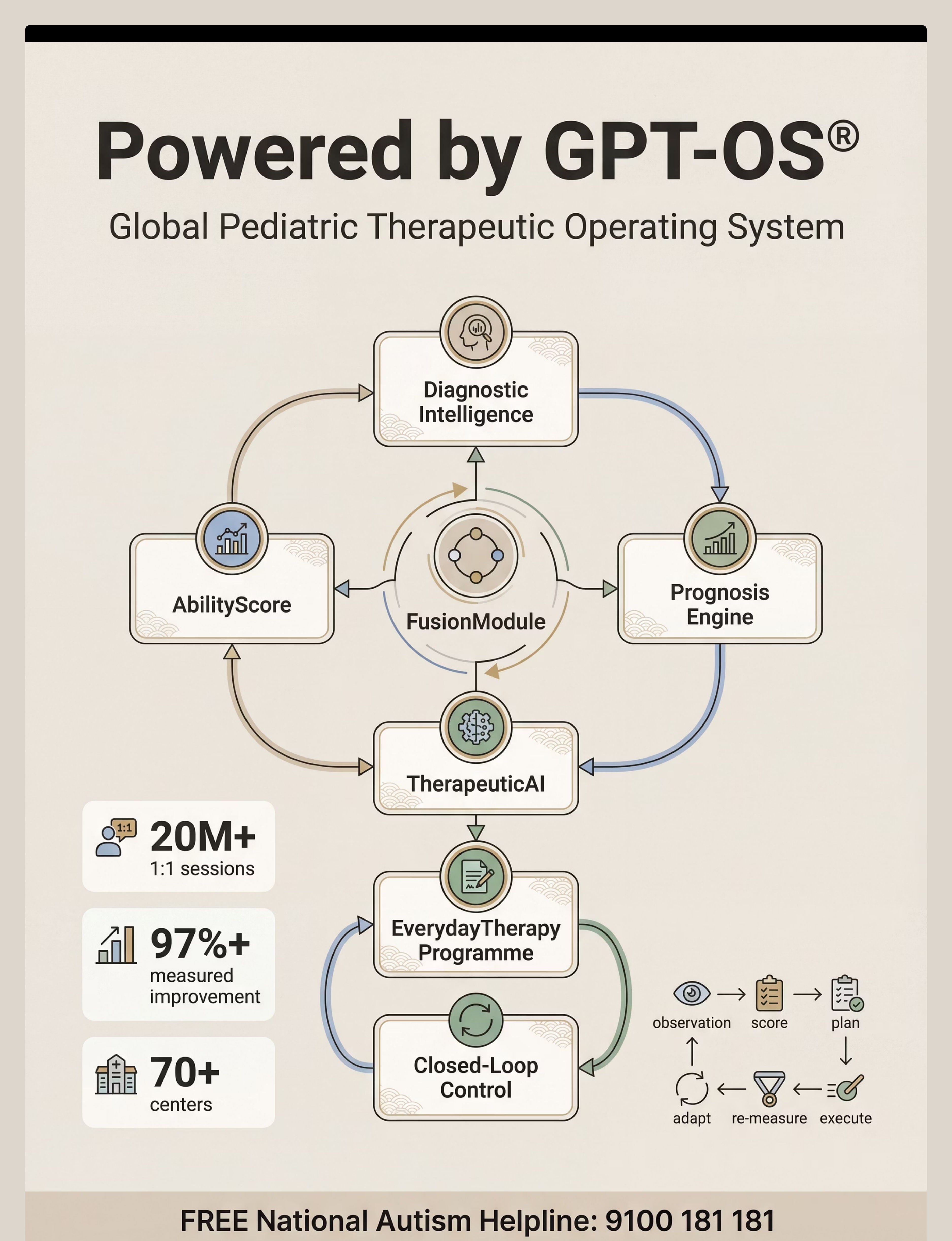
The GPT-OS® Stack
- AbilityScore® — Universal developmental score (0–1000) tracking your child longitudinally
- TherapeuticAI® — Therapy decisions always under licensed human clinical authority
- FusionModule™ — OT + ABA + SLP + SpEd + Medical coordination in one pathway
- EverydayTherapyProgramme™ — Daily home micro-interventions between clinic sessions
- Prognosis Engine — Trajectory prediction from 20M+ session patterns
Your Privacy: All data within GPT-OS® is de-identified, encrypted, and governed by India's DPDP Act 2023. Your child's individual data never leaves GPT-OS® without your explicit consent.

The Reel that brought you here — and the therapist who explains it.
🎬 Reel Details
Title: 9 Materials That Help With Toilet Fears
Reel ID: C-289 | Series: Self-Care & Adaptive Skills Series — Episode 289
Domain: ADL-TOI | Adaptive Behavior / Toilet Training / Anxiety Management
Reel ID: C-289 | Series: Self-Care & Adaptive Skills Series — Episode 289
Domain: ADL-TOI | Adaptive Behavior / Toilet Training / Anxiety Management
🎭 Therapist Introduction
Presented by the Pinnacle Blooms Consortium — Pediatric OT and BCBA/ABA Specialist team. The reel demonstrates all 9 materials in a real bathroom setting, showing a child progressively moving through the fear ladder from complete avoidance to comfortable toilet use.
📽️ Video Modeling Note
Video modeling is classified as an evidence-based practice for ASD (NCAEP, 2020). Watching a child successfully navigate each material reduces the parent's anticipatory anxiety and provides a concrete model for home execution.
Related Reels
C-287
Understanding Toilet Training Readiness
C-288
Common Toilet Training Challenges
C-290
Toilet Training for Children with Autism
A-089
Managing Auditory Sensitivity in Children
Consistency across caregivers multiplies impact. One parent can't do this alone.
For Grandparents / Extended Family
"[Child's name] has toilet fears — this is real, not stubbornness. We are working with therapists on a plan. Here is what helps:"
- ✅ Don't mention the toilet unless necessary
- ✅ If [child] needs to go, calmly say: "[child], your body is sending you a message. Your brave kit is ready."
- ✅ Celebrate any step toward the bathroom — even walking past it
- ✅ Never force, shame, or compare to other children
- ✅ If you're not sure, ask us first
"This is medical, not behavioral. Your patience and consistency are part of the treatment."
For the School / Teacher (Email Template)
"[Child's name] is currently working with a pediatric OT and behavioral specialist on toilet anxiety — a recognized therapeutic challenge, not behavioral defiance. [Child] uses ear defenders during flushing and a specific toilet seat insert. We would appreciate if the school bathroom could accommodate these supports. We are happy to share the clinical protocol with the school's support team."
Frequently Asked Questions
Q: How long will this take?
Fear resolution timelines vary. Mild toilet fear in a neurotypical child: 4–8 weeks. Moderate fear: 8–12 weeks. Severe toilet phobia in children with ASD or constipation history: 12–24 weeks. Consistency and pace are more important than speed. Children who progress slowly but steadily maintain gains better than those rushed through steps.
Q: My child is 7 and still in diapers. Is this too late?
No. Toilet fear resolution has been achieved in children as old as 12–14 years with appropriate support. The protocol adapts for age and cognitive level. Older children benefit from increased involvement in designing their own fear ladder. The same neurological principles apply at any age.
Q: The pediatrician says to "just stop using diapers cold turkey." Should I?
For fear-based toilet resistance, cold turkey approaches typically increase fear, worsen withholding, and damage the parent-child relationship without producing the desired outcome. The evidence supports graduated approaches for fear. If your pediatrician is unfamiliar with toilet phobia as a clinical entity, a referral to a pediatric OT or psychologist is appropriate.
Q: We've been doing this for 6 weeks with no progress. What's wrong?
Check: (1) Is constipation present and medically managed? (2) Is the fear ladder advancing too fast — is the child experiencing distress rather than mastery? (3) Is there inconsistency across caregivers? If all three are ruled out and there is genuinely no progress after 8 weeks of consistent work, professional assessment is indicated.
Q: My child screams "no bathroom" constantly. Do I ignore this?
The verbal "no bathroom" in a child with toilet fear is communication — it means "I'm scared." Respond to the fear, not the behavior: "I hear that you're scared. Your brave kit is ready when you want to try." Never override the "no" with force. The goal is to make the "yes" more appealing through safety-building, not to overpower the "no" through pressure.
Q: What about automatic-flush toilets at school?
Practical solutions: (1) Pack sticky notes — covering the flush sensor prevents automatic flushing. (2) Use ear defenders for all public bathroom visits. (3) Request accessible/family bathroom access at school. (4) Phase 4 (generalization to school) comes AFTER Phase 3 (home mastery) — do not attempt school bathroom work while still establishing home mastery.
Q: Is this just for autism? My child doesn't have a diagnosis?
No. Toilet fear occurs across the neurodevelopmental spectrum and in neurotypical children. The materials and protocol here are effective regardless of diagnosis. The underlying mechanism — graduated exposure, sensory modification, reinforcing approach behaviors — is evidence-based for childhood fears generally.
Q: How do I talk to my child about their fear without making it worse?
Key principles: (1) Validate: "The toilet feels scary to your body. That feeling is real." (2) Separate child from fear: "That's the scared feeling talking. You're braver than that feeling." (3) Focus on progress: "Remember last week when you couldn't stand at the door?" (4) Never minimize: "It's just a toilet" increases shame without reducing fear. (5) Never compare to other children.
Preview of 9 materials that help with toilet fears Therapy Material
Below is a visual preview of 9 materials that help with toilet fears therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

You've read the science. You have the materials. You know the steps.
Your child is waiting for a parent who believes they can do this.
🏛️ Pinnacle Promise
✅ Evidence-linked · ✅ Consortium-validated · ✅ Parent-executable · ✅ Equity-accessible · ✅ Child-first
📞 FREE Helpline
9100 181 181
24x7 · 16+ languages
pinnacleblooms.org
24x7 · 16+ languages
pinnacleblooms.org
🔍 Explore Next
C-290: Autism Toilet Training
C-291: Nighttime Dryness
C-292: Public Bathrooms
C-291: Nighttime Dryness
C-292: Public Bathrooms
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. · CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2 · Technique C-289
This content is educational and does not replace individualized assessment by licensed occupational therapists, pediatric psychologists, or behavioral specialists. Individual results may vary. care@pinnacleblooms.org · pinnacleblooms.org