
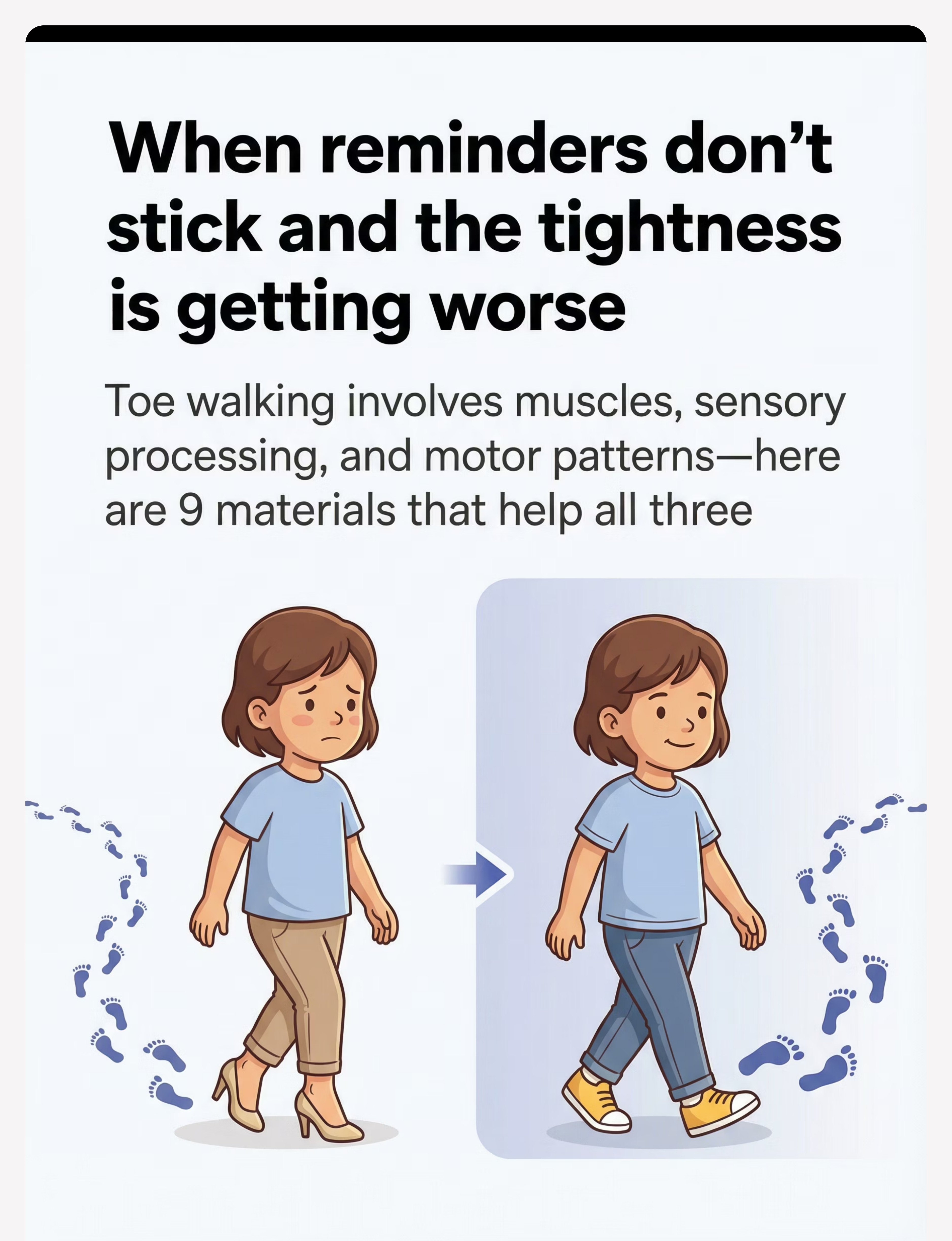
When reminders don't stick and the tightness is getting worse
Toe walking involves muscles, sensory processing, and motor patterns — here are 9 materials that help all three.
"My child is 4 and still walks on their toes most of the time. I thought they'd grow out of it, but now their calves are getting really tight. They can put their heels down if I remind them, but the moment they forget, they're back up on their toes. I'm worried about their muscles getting permanently tight. What actually helps toe walking? What can we use at home?" — Parent, Pinnacle Network
🏥 Pinnacle Blooms Consortium
👶 Ages 2–10
📺 Motor Development Series – Episode 367
FREE National Autism Helpline: 9100 181 181 | Available 24×7 in 16+ languages
You are among millions of families navigating this exact challenge
Toe walking is the second most common gait variation in early childhood. It is seen across typically developing children, children with autism, sensory processing differences, and developmental coordination disorder. You are not failing. Your child's nervous system is speaking — and now we have a vocabulary to respond.
~20%
ASD & Toe Walking
Children with ASD who exhibit toe walking
5%
Persistent Past Age 3
Children who persist in toe walking past age 3
80%
Respond to Intervention
Toe walkers who respond to early comprehensive intervention
Across 70+ Pinnacle centers, toe walking is among the top 5 gross motor concerns brought to developmental pediatricians and OTs. Most families wait 1–3 years before seeking structured intervention.
Sources: PMC11506176 (PRISMA Review, 2024) | PMC10955541 (Meta-analysis, World J Clin Cases, 2024)
This is not a habit to scold out of them. Here's the science.
🦵 The Muscle Story
The calf muscles (gastrocnemius + soleus) attach via the Achilles tendon to the heel. When these shorten, achieving full heel contact becomes physically uncomfortable — the body defaults to toes.
🧠 The Sensory Story
Proprioceptors in the feet send signals about body position. Some children seek intense input through toe-walking (sensory seekers) or avoid heel contact because surfaces feel overwhelming (sensory avoiders).
⚙️ The Motor Pattern Story
Once a gait pattern is established, the brain automates it. The child isn't choosing to toe walk — their motor cortex has encoded it as "normal walking."
"This is a wiring difference and a physical pattern — not a behavioral choice. Reminders alone cannot change shortened muscles or sensory processing differences."
Understanding the three-part mechanism — muscle, sensory, and motor pattern — is the foundation of every effective intervention. Addressing only one component while ignoring the others explains why well-meaning reminders and brief stretches so rarely produce lasting change.
Source: Frontiers in Integrative Neuroscience (2020): Comprehensive neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660

Your child is at a waypoint — not at the end of the road
Understanding where toe walking fits in typical development helps calibrate expectations and urgency. Preventing muscle shortening is always easier than reversing it — but improvement is documented at every age.
🟢 12–18 Months
Toe walking normal as new walker finds balance
🟢 18–24 Months
Gradual transition to heel-toe gait begins
🟡 24–36 Months
Most children complete transition; some persist
🟠 3 Years
Persistent toe walking warrants professional evaluation
🔴 3–5 Years
Progressive calf tightening risk if unaddressed
⭐ Any Age
With the right intervention, normalization is achievable
What commonly co-occurs: #ASD (20%) | #SensoryProcessing | #DevelopmentalCoordinationDisorder | #ADHD | #LowMuscleTone | #BalanceDifficulties
Source: WHO Care for Child Development (CCD) Package — age-specific evidence-based recommendations implemented across 54 low- and middle-income countries. | PMC9978394
🏥 Pinnacle Blooms Consortium
OT • PT • NeuroDev • Pediatrics
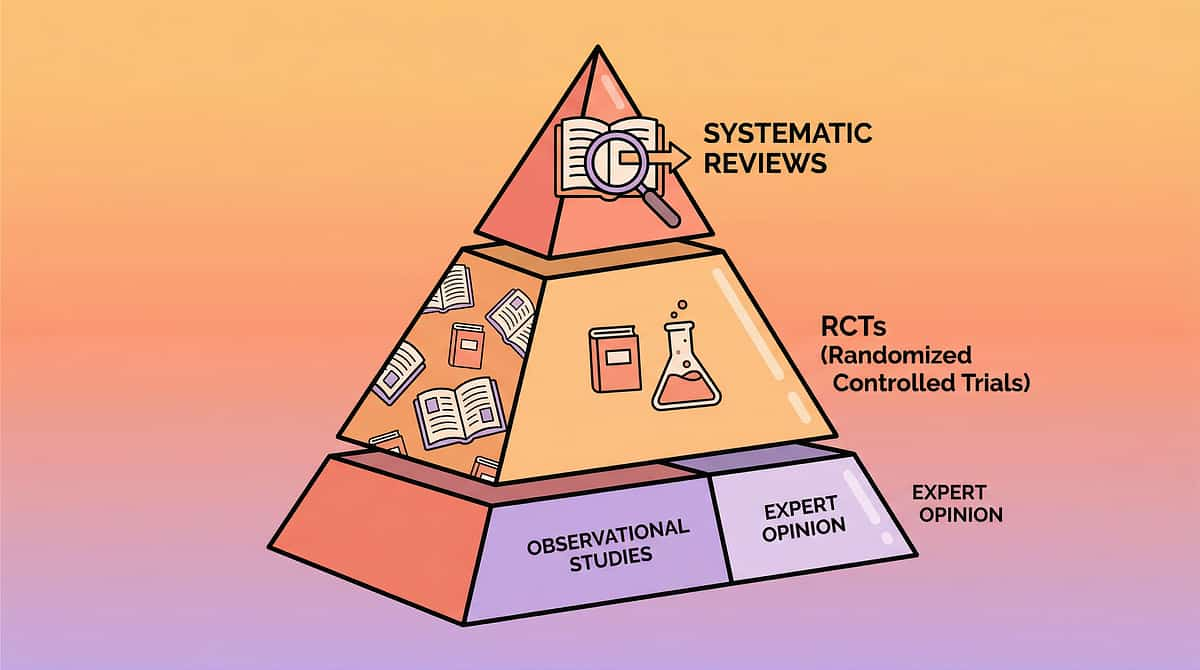
The Evidence Behind This Approach
⚕️ Evidence Grade: Level I–II
Systematic Review + Meta-Analysis
📊 PRISMA Systematic Review (2024)
16 studies, 2013–2023. Sensory integration intervention confirmed evidence-based practice for children with ASD. Multi-modal approach (sensory + motor + stretching) outperforms single-modality.
PMC11506176
📊 Meta-analysis, 24 Studies (2024)
World J Clin Cases: Sensory-motor intervention significantly improves gross motor skills, adaptive behavior, and sensory processing in pediatric populations.
PMC10955541
📊 Indian RCT — Home-Based Intervention
Home-administered sensory-motor programs demonstrate significant outcomes equivalent to clinic delivery when caregiver-trained.
DOI: 10.1007/s12098-018-2747-4 (Padmanabha et al., Indian J Pediatr, 2019)
"Clinically validated. Home-applicable. Parent-proven."
FREE National Autism Helpline: 9100 181 181 — for a structured assessment

Multi-Modal Gait Normalisation Intervention
Parent Alias: "The Heel-Down Programme"
What It Is
A structured home-based intervention combining sustained calf stretching, sensory integration, proprioceptive input, muscle strengthening, and motor pattern retraining to normalize heel-toe gait in children who persistently walk on their toes.
Effective across idiopathic, sensory-based, and habitually-driven toe walking patterns.
Programme Details
- 🏷️ Domain: D — Motor Development / Gait Patterns
- 🏷️ Ages: 2–10 years
- 🏷️ Frequency: Daily, embedded in routine
- 🏷️ Duration: 15–30 min total/day (distributed)
- 🏷️ Materials Required: 9 (commercial + DIY options)
Why This Approach Works — In 3 Words
Muscles + Sensory + Pattern

This technique crosses therapy boundaries — because the brain doesn't organize by therapy type
🟦 Occupational Therapist (Lead)
Addresses sensory processing, proprioceptive intervention, tactile desensitization, weighted gear protocols, sensory diet design.
🟩 Physical Therapist
Ankle range-of-motion assessment, stretching protocols, orthotic recommendations, gait retraining, strengthening programs.
🟧 BCBA / ABA Therapist
Behavioral reinforcement for consistent heel walking, shaping programs, environmental setup, data collection on gait patterns.
🟪 NeuroDev Pediatrician
Rules out neurological causes, monitors for contracture progression, coordinates orthotics and specialist referrals.
"Toe walking is one of the few gait challenges where OT, PT, and ABA must operate in concert from day one. The sensory system won't change without sensory input; the muscle won't lengthen without sustained stretch; and the pattern won't transfer without behavioral shaping." — Pinnacle Consortium Clinical Lead
NCAEP 2020 | DOI: 10.1080/17549507.2022.2141327
This isn't a random activity. It's a precision intervention.
Observable indicators of progress: ✅ Heel visibly contacts ground during walking ✅ Even shoe wear (not just toe area) ✅ Can squat with heels flat on floor ✅ Maintains heel contact without verbal reminders ✅ Able to run without full toe-strike pattern
PMC10955541

9 Materials That Help With Toe Walking
Addressing muscles, sensory system, and motor patterns — simultaneously
1. Incline Board
🦵 Sustained calf stretch | ₹800–2,500
2. Orthotics (AFOs/SMOs)
🦶 Mechanical repositioning | ₹1,500–15,000+
3. Textured Sensory Mats
👣 Sensory heel input | ₹500–3,000
4. Weighted Vest/Ankle Weights
🧠 Proprioceptive grounding | ₹1,000–4,000
5. Resistance Bands
💪 Dorsiflexor strengthening | ₹300–800
6. Therapeutic Shoes
👟 Every-step guidance | ₹1,500–5,000
7. Proprioceptive Equipment
⚡ Satisfy the input need | ₹2,000–10,000
8. Gait Training Mirror
👁️ See it, change it | ₹500–3,000
9. Backward/Heel Walking Kit
↩️ Practice the opposite | ₹300–1,500
🔵 Muscle Length (1, 2, 6) — Stretch and reposition | 🟢 Sensory-Motor (3, 4, 7) — Feed the nervous system | 🟡 Pattern Retraining (5, 8, 9) — Build new motor programs
Not sure where to start? FREE Helpline: 9100 181 181

Material 1 of 9
🦵 Muscle Length
INCLINE BOARD
Sustained stretch while standing — muscles lengthen over time
10–15 minutes daily during TV or play provides the stretch duration that brief exercises can't match. Brief stretches (30 seconds) have minimal lasting effect. 10+ minutes of sustained low-load stretch changes tissue length permanently.
The Science
The gastrocnemius and soleus connect via the Achilles to the heel. In toe walkers, these shorten until heel contact becomes uncomfortable. An incline board forces ankle dorsiflexion under body weight — the optimal condition for connective tissue lengthening.
How-To Guide
- Start at 15° angle — increase as flexibility improves
- Heels MUST stay flat on board (if they hover, reduce angle)
- Position board in front of TV/play table
- Barefoot is better — true ankle positioning + sensory input
- Straight knees (gastrocnemius) → Bent knees (soleus) — do both
- Aim: 10–15 min, 2–3 times daily during preferred activities
💡 DIY Option (₹0): Use any sturdy wooden board propped at an angle against a wall. Secure with non-slip mat. Test stability before child stands on it.
⚠️ Safety: Ensure board is non-slip and stable. Never force a stretch that causes pain. Supervise initially. | Price: ₹800–2,500

Material 2 of 9
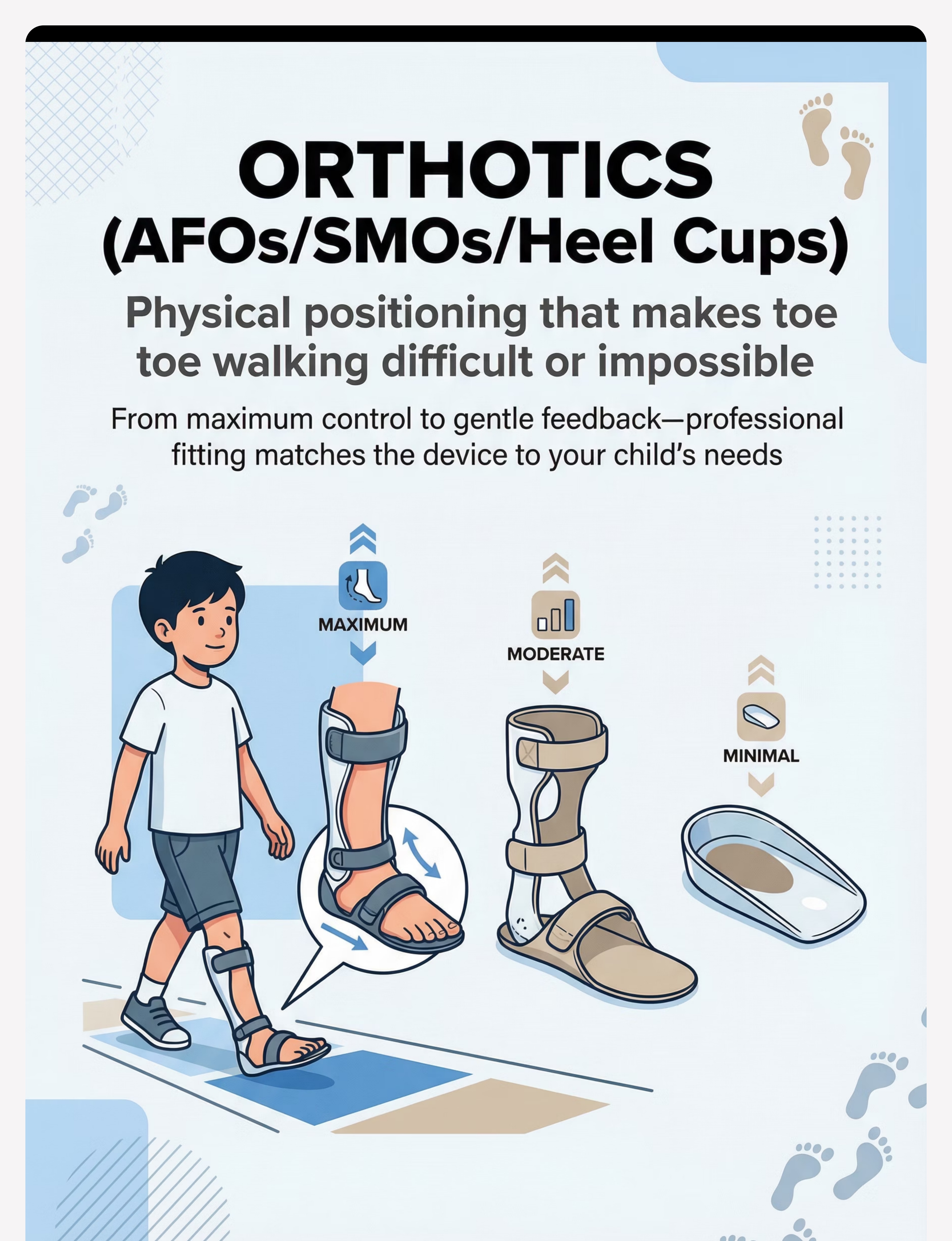
🦶 Mechanical Positioning
ORTHOTICS (AFOs / SMOs / HEEL CUPS)
Physical positioning that makes toe walking difficult or impossible
🟡 Heel Cups / Heel Wedges
Proprioceptive feedback to heels. Best for sensory-based walkers. Inserts into existing shoes. Minimal intervention, maximum compliance.
🟢 SMOs (Supramalleolar Orthoses)
Foot + ankle positioning with more movement freedom. Mild-moderate cases. Available custom or prefabricated.
🔵 AFOs (Ankle Foot Orthoses)
Full ankle control. Prescribed for significant tightness or neurological causes. Custom-molded. Worn most waking hours for maximum benefit.
Orthotics work 24/7 — that's hundreds of hours of positioning that therapy sessions alone cannot provide. ⚠️ Custom orthotics REQUIRE professional fitting. Improper fit causes skin breakdown and joint problems. Never use another child's orthotics.
Shoe checklist when wearing AFOs: Removable insoles + extra depth | Velcro closure | Wide toe box | Rigid heel counter
Price: ₹1,500–15,000+ (custom vs. prefabricated) | FREE guidance: 9100 181 181

Material 3 of 9
👣 Sensory Processing
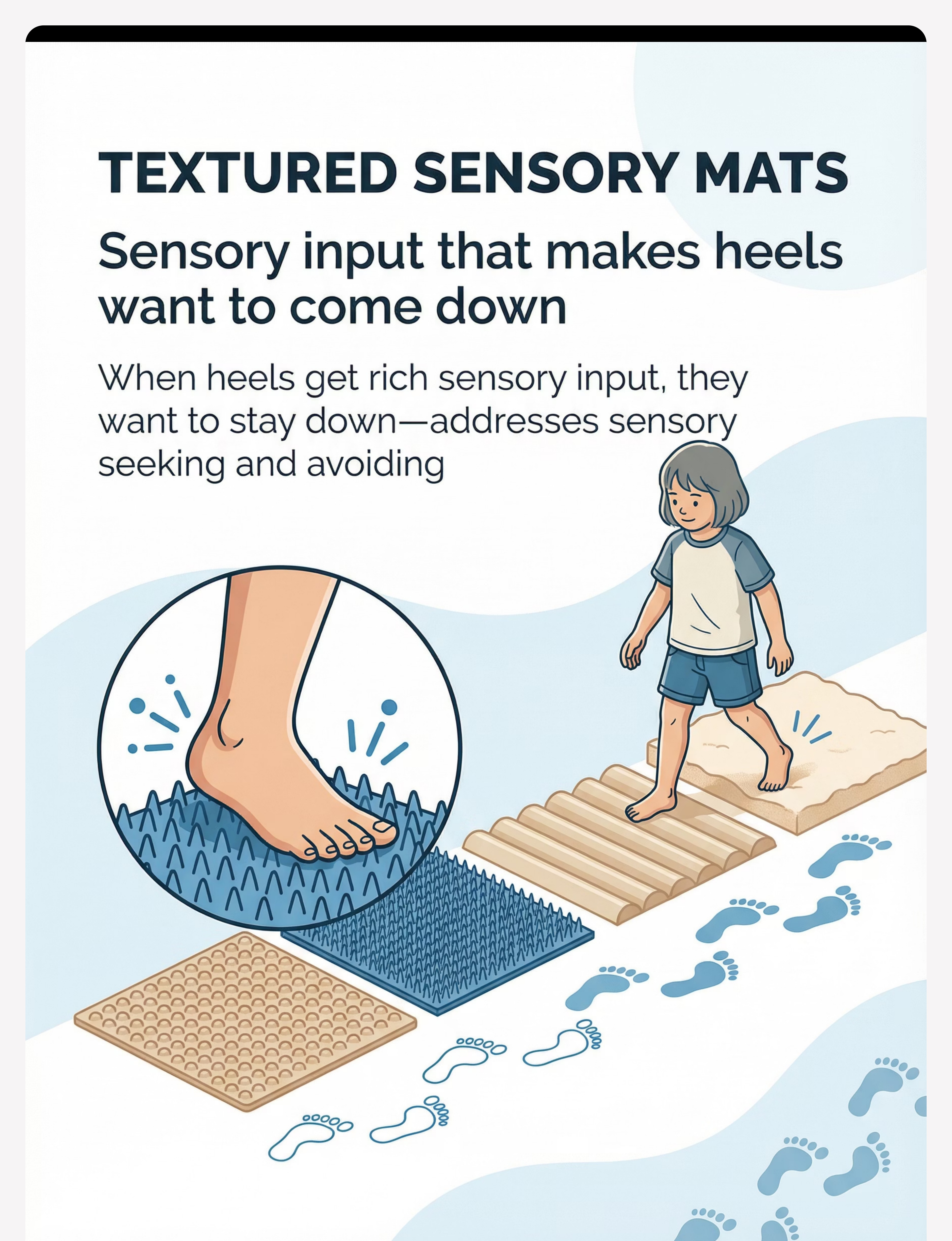
TEXTURED SENSORY MATS
Sensory input that makes heels want to come down
For Sensory SEEKERS
Highly textured surfaces deliver the intense proprioceptive input the child craves — through the ENTIRE foot. When the input need is met, the drive to toe walk decreases naturally.
For Sensory AVOIDERS
Graduated texture exposure desensitizes the soles. Starting with soft textures and progressing to more challenging ones, the nervous system learns that heels-down is safe.
DIY Walking Path Ideas
🟫 Door mats (vary texture) | 🟩 Artificial grass | 🪨 Smooth river rocks in tray | 💦 Rubber bath mats | 🧶 Carpet samples | 🫧 Bubble wrap (taped down)
OT-Guided Setup
- Place path in frequently traveled areas (hallway → bathroom → play area)
- Always BAREFOOT — socks eliminate the input
- Make it a game: "Walk the path to breakfast!" "Find the treasure at the end!"
- For avoiders: never force — graduated approach only
- Cue heels: "Press your heels into the bumps — feel how different that is!"
Toe walking is often sensory BEFORE it's structural. Address the sensory need and the structural pattern often resolves faster. | Price: ₹500–3,000

Material 4 of 9
🧠 Proprioceptive Input
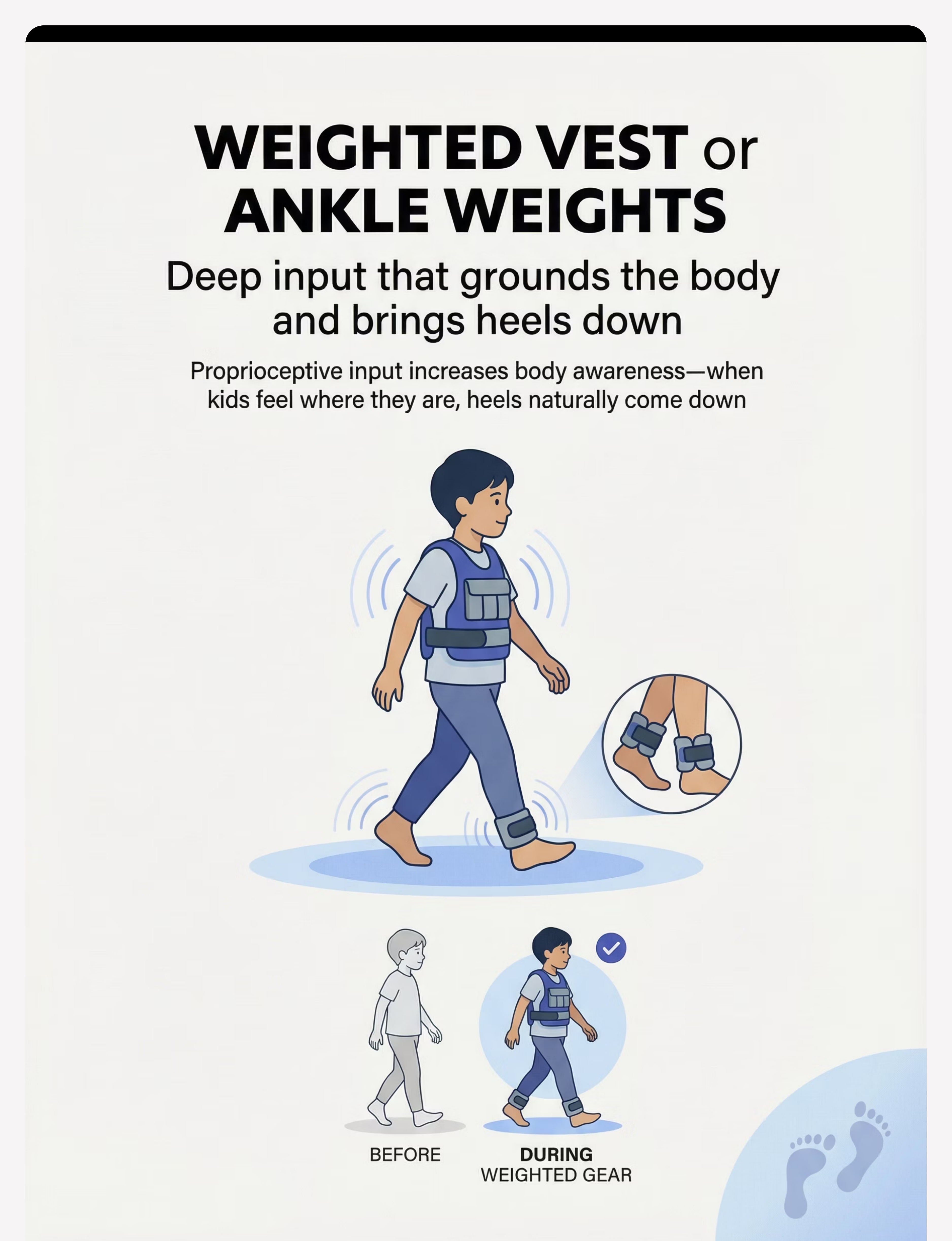
WEIGHTED VEST or ANKLE WEIGHTS
Deep input that grounds the body and brings heels down
The Mechanism
Weighted gear provides deep proprioceptive input — the sensory information from muscles and joints about body position. Children who toe walk often have reduced proprioceptive awareness: they literally don't clearly feel where their feet are in space.
Weighted vest → whole-body awareness → calms nervous system → heels come down naturally
Ankle weights → loads lower limbs → makes toe walking more effortful → body prefers efficient heel-toe
Usage Protocol
- Weight: 5–10% of child's body weight (vest)
- Duration: 15–30 minute intervals during active movement
- Timing: Before activities where heel contact is needed
- NOT for: All-day wear, running activities, or children with cardiac/respiratory conditions
DIY Vest Option
Rice or sand in sewn pockets of a snug compression shirt. Ensure weight is evenly distributed and secured.
⚠️ Never exceed 10% body weight. Remove if child shows fatigue or distress. Consult OT for child-specific recommendation. | Price: ₹1,000–4,000 | FREE Helpline: 9100 181 181

Material 5 of 9
💪 Muscle Strengthening
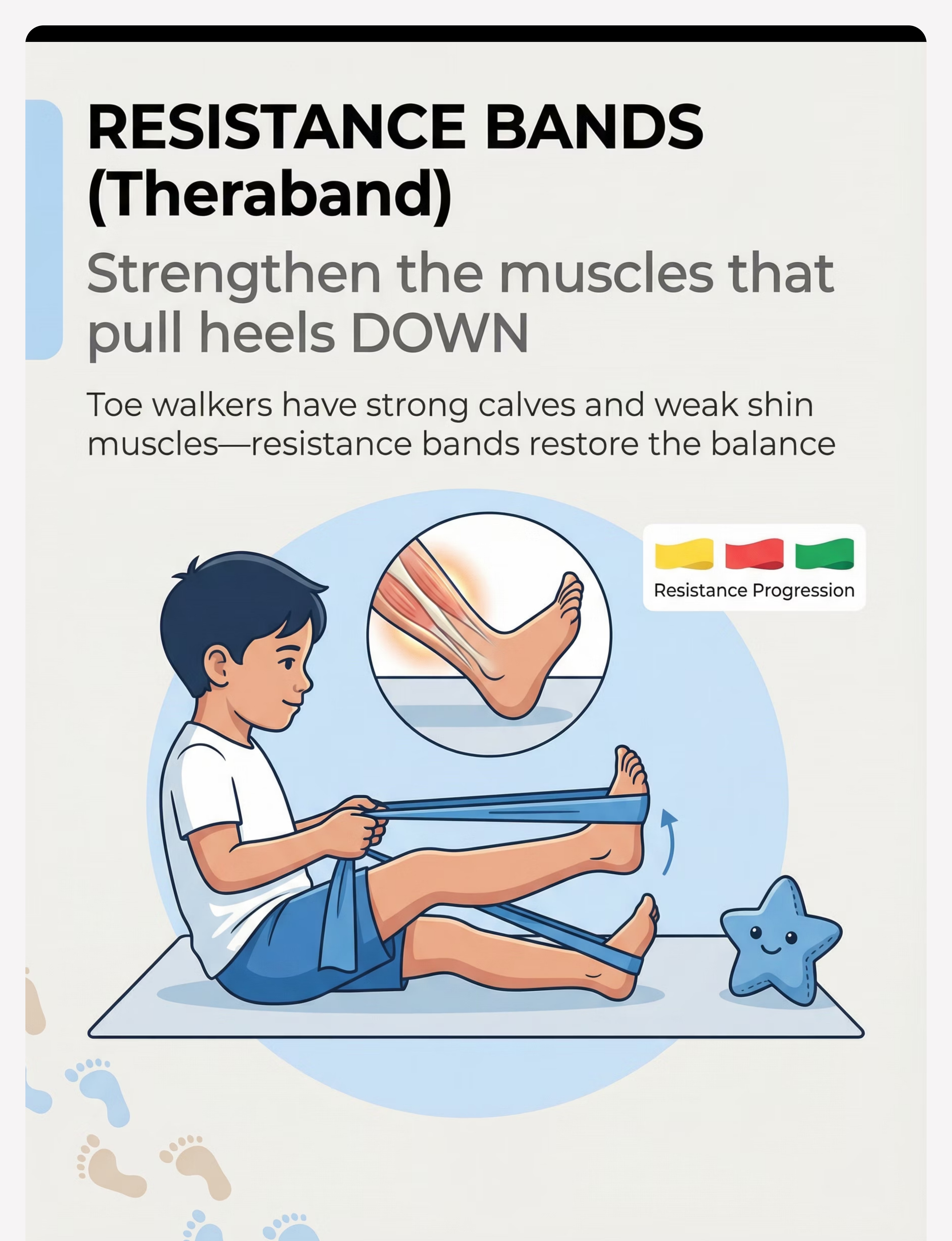
RESISTANCE BANDS (Theraband)
Strengthen the muscles that pull heels DOWN
Toe walkers have STRONG calf muscles and WEAK shin muscles (tibialis anterior — the dorsiflexors). This muscular imbalance maintains the pattern. Resistance bands rebuild the opposition.
Resistance Progression
🟡 Yellow (lightest) → Start here | 🔴 Red (light) → After 2 weeks | 🟢 Green (medium) → After 4–6 weeks
1. Ankle Alphabet (Seated)
Band around foot — "write" A–Z in the air with foot. Works all ankle movements simultaneously.
2. Dorsiflexion Pulls (Seated)
Band around ball of foot, anchored to chair leg. Pull foot UP toward shin. 10–15 reps × 2–3 sets.
3. Eccentric Lowering
Pull up, then SLOWLY lower — both strengthens and lengthens simultaneously. Progress to standing.
Make it a game: Pull foot to ring a bell | Knock down a tower | Hit a target | "Ankle tug of war" with stuffed animal
⚠️ Inspect band before use for cracks. Stop at any pain. Latex allergy — use latex-free bands. | Price: ₹300–800

Material 6 of 9
👟 Every-Step Guidance
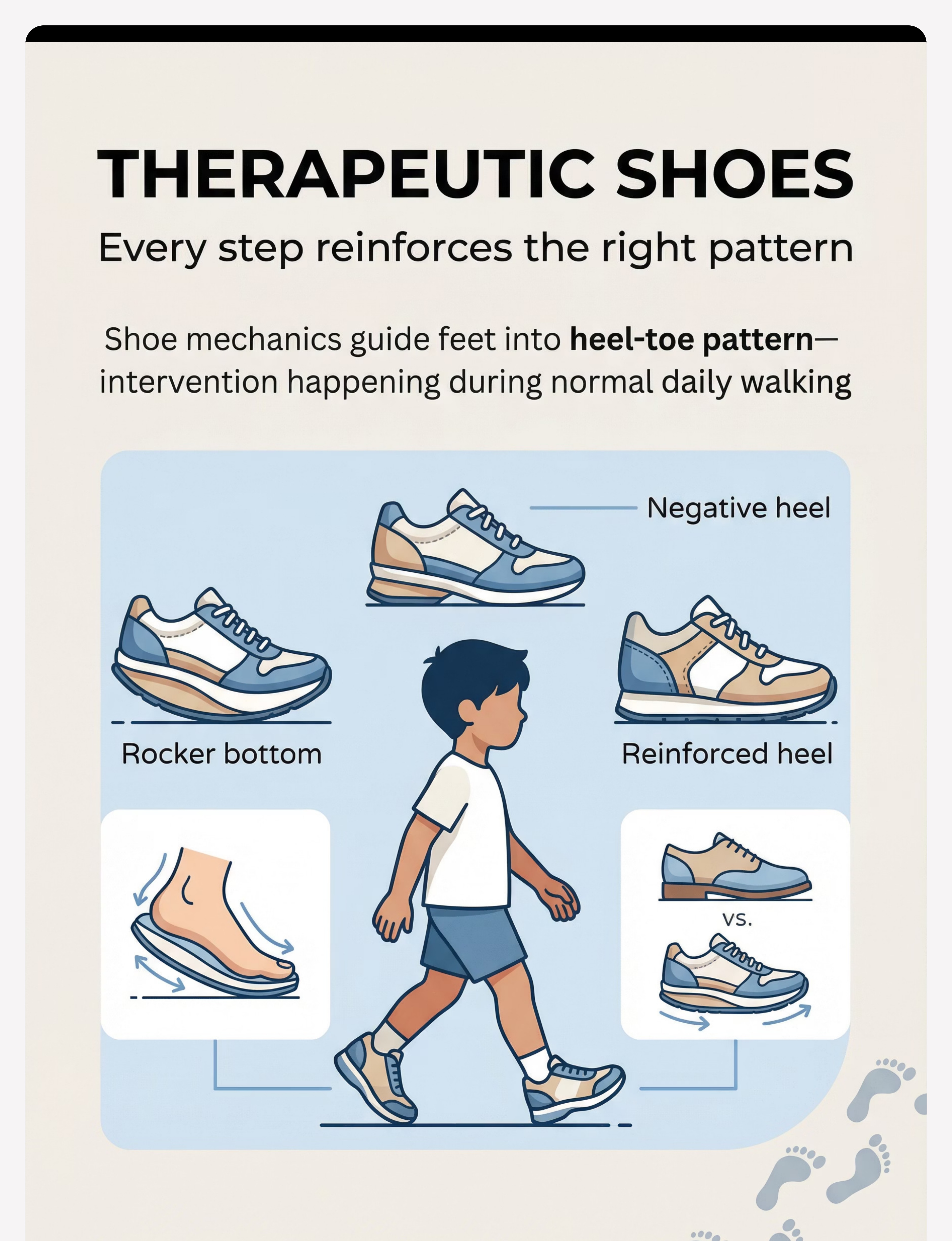
THERAPEUTIC SHOES
Every step reinforces the right pattern — without a reminder
Shoes are worn for 8–12 hours daily. That's therapeutic intervention happening during normal life — hundreds of corrective inputs that no therapy session can replicate.
🟦 Rocker Bottom Sole
Curved sole from heel to toe promotes natural heel-to-toe gait progression. Good for habitual toe walkers. Shoe shape does the mechanical reminding.
🟩 Negative Heel
Heel slightly lower than toes — constant gentle stretch similar to incline board, during walking. Combines stretch with mechanical guidance.
🟧 Reinforced/Elevated Heel
High heel counter provides proprioceptive feedback. Prevents foot from slipping back into toe-only position.
Shoe Selector Guide
Habitual toe walking → Rocker bottom | Muscle tightness → Negative heel | Poor heel awareness → Reinforced heel counter | Orthotic required → Extra-depth shoe with removable insole
Fit checklist:☑️ Snug heel | ☑️ Rigid toe box | ☑️ Velcro or lace closure | ☑️ Non-slip sole | Price: ₹1,500–5,000

Material 7 of 9
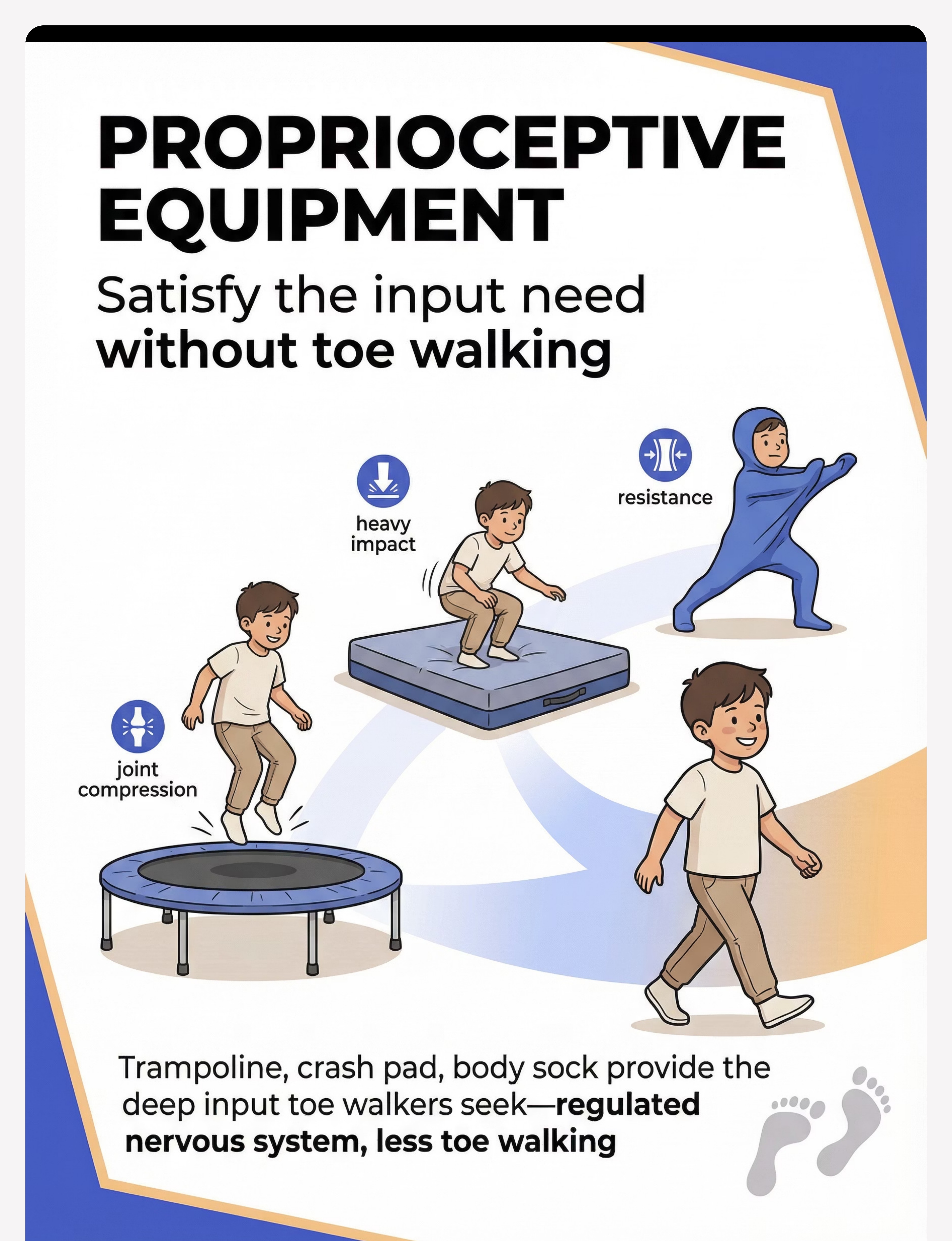
⚡ Proprioceptive Regulation
PROPRIOCEPTIVE EQUIPMENT
Satisfy the input need — without toe walking
Some children toe walk to GET proprioceptive input. Their nervous system sends a "need more information about where my body is" signal. Provide the input another way, and the toe walking loses its purpose.
🎪 Mini Trampoline (Indoor)
Rhythmic joint compression through jumping. 10–15 min provides lasting regulation. Cue heel contact during landing — "Can you feel your heels on the bounce?" Price: ₹2,000–6,000
🛏️ Crash Pad / Bean Bag
Heavy impact input through jumping/falling. Satisfies sensory seeking safely. DIY: stack couch cushions with non-slip base. Price: ₹1,500–4,000
🧤 Body Sock
Stretchy fabric provides resistance + whole-body proprioception. Walking and stretching inside body sock is profoundly regulating. 5–10 min sessions. Price: ₹1,200–2,500
Use BEFORE activities where heel contact is needed. Regulation effect typically lasts 30–60 minutes. Think of it as a daily proprioceptive "diet" — multiple short doses throughout the day.
FREE National Autism Helpline: 9100 181 181

Material 8 of 9
👁️ Visual Awareness
VISUAL FEEDBACK SYSTEM (Mirror / Video)
See your walking, change your walking
The Mechanism
Children often don't know they're toe walking — they can't see themselves. Visual feedback makes the invisible pattern visible. When children SEE their gait, they can actively modify it.
This bridges the gap between: "Can put heels down when reminded" → "Automatically walks with heel contact"
Setup Guide
- 📐 Full-length mirror at end of hallway (securely wall-mounted)
- 📱 Phone slow-mo video — record from side angle (best for seeing heel contact)
- 📊 Monthly progress videos — child sees their own improvement
Video Protocol
- Record walking (side view) — review together
- Pause at heel strike: "Look! Your heel touched!"
- "How many steps can you count where heels touch?"
- Celebrate: "You're getting it!"
ALWAYS positive framing: "I see your heels!" — not "You're toe walking again." | Price: ₹500–3,000 (mirror) | Phone/tablet you already have | NCAEP 2020: Video modeling is an evidence-based practice for autism.

Material 9 of 9
↩️ Motor Pattern Retraining
BACKWARD WALKING & HEEL WALKING PRACTICE
Practice the opposite — change the pattern
"Walking backward requires a toe-to-heel pattern — the exact opposite of toe walking. It's nearly IMPOSSIBLE to walk backward on toes. Meanwhile, heel walking directly strengthens the dorsiflexors and provides intense proprioceptive feedback to the heels." — Pinnacle Consortium PT
Backward Walking
- Start with hand-held for safety — progress to independent
- Walk hallway backward: 10–20 laps daily
- Game: "Can you walk backward to the door without looking?"
Heel Walking
- Walk on heels with toes lifted
- Short distances first (5–10 steps) — build to full hallway
- Balance beam heel walking adds proprioceptive challenge
Progress milestones: Week 1–2: 5 consecutive heel steps | Week 3–4: Full hallway | Week 6–8: Spontaneous heel contact in daily walking
Equipment (low-cost):🏷️ Masking tape ₹50–100 | 🏷️ Low balance beam ₹300–800 | 🏷️ Cones/targets ₹200–500
⚠️ Clear path for backward walking — child can't see behind. Non-slip surface essential.

60 Seconds Before You Begin — Check This
Pre-Session Readiness Checklist
☑️ Child has eaten in the last 2 hours
☑️ No signs of illness (fever, pain, fatigue)
☑️ No significant meltdown in the last 30 minutes
☑️ Child is in an alert/calm state
☑️ Materials are set up and ready before involving child
☑️ You have 15–20 uninterrupted minutes
☑️ Preferred reinforcer is identified and available
🟢 GO (5–7 checks)
Proceed with full session
🟡 MODIFY (3–4 checks)
Do shorter, simpler version — 5 min incline board + 5 min mirror
🔴 POSTPONE (under 3)
Offer calming activity instead; try again in 1–2 hours. Try: 5 min proprioceptive input → rest → re-assess
"The best session is one that starts right. A 5-minute excellent session builds more than a 20-minute forced session that ends in distress." — Pinnacle Consortium

Step 1
Every session begins with an invitation — not a command
"Hey [child name], want to do our special feet time? It's the one where you stand on the cool board / walk on the bumpy mats / do the bouncing. We've got [preferred item] ready for you."
Body Language Cues
- Get physically level with child (crouch down)
- Offer choice: "Do you want to start with the board or the bouncy path today?"
- Hold preferred item toward child to activate motivation
- Wait 10–15 seconds for child to orient and accept
Reading the Response
✅Acceptance: Child moves toward materials | Eye contact + approach | Verbal "yes" or pointing
⚠️Resistance: Child moves away | Verbal "no" | Head-turning → Give 30-second break, re-offer once with different preferred item. If still resistant → Postpone (see Card 19).
Timing: 30–60 seconds | ABA citation: Pairing procedures — establishing motivating operations before demand placement.
Step 2
Introduce the material playfully — the child's response tells you everything
For Incline Board Sessions
"Let's stand on the tilty board while you watch [show/game]. Heels stay down, like this — watch me first." (parent demonstrates first)
For Sensory Mat Sessions
"Walk along the bumpy path with me. Let's count the different textures!" (walk alongside, not behind)
For Proprioceptive Sessions
"Jump time! Can you do 20 big jumps? Let's count together." (trampoline / body sock)
🟢 Engaged
Participating, tolerating, exploring → continue. Reinforce positively.
🟡 Tolerating
Passive participation, not seeking → reinforce positively and continue
🔴 Avoiding
Pulling away, distress → reduce demand, simplify, or postpone
Reinforcement begins here. Every approach toward material, every heel contact, every tolerance — praise it specifically: "I see your heels touching! That's exactly it!" | Timing: 1–3 minutes introduction
The Active Therapeutic Window — 10–15 Minutes of Purposeful Practice
Steps 3–5
Step 3 — The Therapeutic Action (5–10 min)
Stretching: Child stands on board, heels flat, doing preferred activity. Knees straight (3–5 min) → slightly bent (3–5 min). Sensory-motor: Child navigates path / jumps / moves in body sock. Cue heel contact at natural moments. Gait training: 5 min mirror practice + 5 min backward/heel walk games.
Step 4 — Repeat & Vary (2–3 Sets)
Incline board: alternate positions | Sensory path: change direction, add stations | Gait training: vary speed, targets, path length. "3 great reps beat 10 forced reps."
Step 5 — Reinforce & Celebrate
Within 3 seconds of every heel contact: "YES! I saw your heel touch! That's exactly what we're building!" Choose one: 🌟 Verbal praise | 🎫 Sticker token | 🎮 Extra preferred activity time | 🤗 High-five
ABA citation: Immediate, specific reinforcement increases behavior occurrence. | BACB ethical guidelines.

Step 6
No session ends abruptly — the transition IS part of the therapy
The 2-minute cool-down sequence prevents abrupt endings that can spike distress and undermine future session willingness. Use a visual timer for the last 2 minutes so ending is predicted, not sudden — visual supports are an NCAEP 2020 evidence-based practice.
If child resists ending: "One more turn — then we're all done." (pre-commit language) Never abruptly remove access. | NCAEP 2020 — Visual supports are evidence-based practice.

60 Seconds. Right Now. Before You Forget.
Capture the Data — Immediately Post-Session
📅 Date + Time | Record today's date and time of session | |
⏱️ Session Duration | ___ minutes total | |
👣 Heel Contact Rating | 0–10 (0 = no contact, 10 = consistent contact throughout) | |
💬 Child Response | 😊 Cooperative / 😐 Neutral / 😣 Resistant | |
🔔 Notable Change | Free text — 1 sentence describing any new observation |
Why This Matters
Data captured now becomes the progress chart that motivates you through the hard weeks. A heel contact rating going from 2 → 5 → 8 over 8 weeks tells you the intervention is working — even when daily progress is hard to see.
GPT-OS® Integration
Log this in your EverydayTherapyProgramme™ dashboard to automatically generate progress charts and TherapeuticAI® session recommendations.
PMC11506176: Outcomes emerge across 8–12 week timelines. Weekly data reveals early indicators. | Questions about tracking? FREE: 9100 181 181
Every family hits obstacles. Here's what to do.
Troubleshooting: When Things Don't Go As Planned
🔴 Child refuses incline board entirely
Start with just 30 seconds while holding parent's hands. Place favorite toy/screen at eye level ON the board. Increase by 30s each day. Use preferred item ON the board surface.
🔴 Toe walking increases when excited/running
This is normal. Pattern breakdown under arousal is expected. Focus stretching + weighted gear BEFORE high-arousal activities. Count baseline vs. calm walking, not excited walking.
🔴 Orthotics cause skin redness
Stop wearing immediately. Contact prescribing PT/orthotist. Do NOT continue through skin breakdown. This is a fitting issue requiring professional adjustment.
🔴 No visible improvement after 4 weeks
First: assess consistency (minimum 15 min stretch + 5 min gait practice daily?). Second: consider OT assessment to identify if approach needs rebalancing. Call 9100 181 181 for guidance.
🔴 Child is toe walking MORE after starting
Possible: sensory system is being aroused before it's regulated. Prioritize proprioceptive input (trampoline/weighted gear) as first step. Let nervous system regulate before stretching.
🔴 Family members are undermining progress
Use Card 33 (Share with Family) to create a consistent household approach. Inconsistency across caregivers is one of the biggest saboteurs of gait programs.
If challenges persist beyond 6 weeks of consistent intervention, a formal physiotherapy or OT assessment is recommended. Toe walking with neurological signs requires specialist evaluation at any point.
Not all toe walkers need the same intervention. Here's how to calibrate.
Personalise: Adapting for Your Child
PRIMARY = Muscle Tightness
↑ Increase: Incline board time | Orthotic consideration | Negative-heel shoes
↓ Secondary: Gait training (once range improves)
↓ Secondary: Gait training (once range improves)
PRIMARY = Sensory Seeking
↑ Prioritize: Trampoline | Body sock | Weighted gear | Textured mats
↓ Reduce: Stretching emphasis until sensory needs are met
↓ Reduce: Stretching emphasis until sensory needs are met
PRIMARY = Sensory Avoiding
↑ Prioritize: Graduated textured mat exposure | Desensitization | Heel cup
↓ Avoid: Forcing bare foot on intense textures
↓ Avoid: Forcing bare foot on intense textures
PRIMARY = Habitual / Motor Pattern
↑ Prioritize: Mirror gait training | Backward walking | Visual feedback | Heel walking
↓ Reduce: Heavy sensory focus unless secondary profile confirmed
↓ Reduce: Heavy sensory focus unless secondary profile confirmed
Easier Version (Bad Days)
5 min incline board only | Mirror walk to bathroom
Full Circuit (Breakthrough Days)
Incline board → textured path → trampoline → mirror walking → backward walking
Age-Based Adaptation
Ages 2–4: Shorter sessions (5–8 min), more play-based, weighted gear minimized | Ages 5–7: Full protocol with game-based framing | Ages 8–10: Child actively participates in data tracking and self-monitoring

Weeks 1–2
Building the Foundation
Progress in weeks 1–2 looks nothing like the finish line
✅ What You WILL See
Child tolerates incline board for increasing durations (even 3 seconds more = real progress) | Reduced resistance to material introduction | Occasional spontaneous heel contact | Child begins recognizing "feet time" as a routine
⏳ What You Will NOT See Yet (and that's OK)
Consistent heel contact during free walking | Spontaneous correction without cues | Observable gait change to others
"If your child tolerates the incline board for 30 seconds longer than last week — that IS significant progress."
Week 1–2 feel the hardest because you're doing all the work with minimal visible return. This is when most parents give up. Please don't. You are laying neural and physical infrastructure. | PMC11506176: Sensory integration outcomes emerge across 8–12 week timelines. Early phase = tolerance and participation, not mastery.
Weeks 3–4
Consolidation — 40%
The neural pathways are starting to form — look for these signs
Child anticipates "feet time"
Starts moving toward materials without being called — routine has formed
2–5 spontaneous heel contacts during daily walking (unprompted)
Improved tolerance to foot touch and textured surfaces
Incline board duration increased to 5+ minutes with less resistance
Can heel-walk 8–10 consecutive steps
Gait data chart showing upward trend in heel contact rating
Most parents report that their own anxiety about toe walking decreases significantly by week 4. You've built a routine. You've seen the first signs. The system is working.
When to increase intensity: If child is consistently at or above planned session goals for 5 days — increase incline board time by 2–3 min, increase resistance band difficulty (next color), add a gait training mirror session.
Neuroplasticity evidence: Synaptic strengthening through repeated structured input follows predictable timelines in pediatric populations.
Weeks 5–8
Emerging Mastery — 70%
The work you did in weeks 1–4 is now showing up in real walking
Mastery Indicators
- Heel contact present in familiar environments without reminders
- Child self-corrects when they notice toe walking (mirror training transferring!)
- Ankle range of motion measurably improved — child can squat heels-down
- Shoe wear pattern normalizing — heel wear visible, not just toes
- Heel walking: 20+ consecutive steps easily
- Sessions no longer feel like a battle — routine is fully established
Generalization Phase — Extend to New Environments
- Practice heel contact at school (teacher briefed)
- Practice in shoes (not just barefoot)
- Practice at various speeds (not just slow, deliberate walking)
- Practice outdoors (different surfaces)
🔴 Red Flags — If These Persist Past Week 8
- Zero heel contact even during deliberate practice → seek PT assessment
- Ankle range not improving despite consistent stretching → orthopaedic review
- Regression in other skills simultaneously → NeuroDev Pediatrics review

🏆 Mark Every Victory. Every One.
Milestone | Date Achieved | |
First session completed without resistance | ___ | |
First spontaneous heel contact (unprompted) | ___ | |
5 consecutive heel steps — heel walking | ___ | |
Heel contact rating reached 5/10 | ___ | |
Incline board for 10+ minutes without protest | ___ | |
20 consecutive heel steps — heel walking | ___ | |
Someone else noticed the improvement | ___ | |
Heel contact in shoes (not just barefoot) | ___ | |
Heel contact outdoors | ___ | |
Consistent heel-toe in familiar settings | ___ |
"We were told to wait and see for two years. By the time we started, my 5-year-old had significant calf tightness. With incline board stretching, textured mats, and daily backward walking practice, within four months heel contact went from 0% to about 70%. By eight months, she walks normally most of the time without any reminders." — Parent, Pinnacle Network
Your child's journey: Constant Toe Walking → With Reminders → Spontaneous Sometimes → Consistent in Familiar Environments → Generalized Automatic Heel-Toe Gait ✅
Share your milestone: 9100 181 181 | pinnacleblooms.org

These signs require professional evaluation — not more home practice
🔴 IMMEDIATE: See Your Doctor
- Toe walking appeared suddenly in a child who previously walked normally
- Toe walking on ONE side only (asymmetric)
- Child cannot put heels down even when trying very hard
- Toe walking with muscle weakness (falls frequently, trouble climbing)
- Any neurological symptoms (coordination loss, tremor, regression)
- Rapid onset + deterioration of other skills simultaneously
🟡 WITHIN 4–6 WEEKS: Seek PT/OT Assessment
- No improvement in heel contact after 6+ weeks of consistent intervention
- Ankle range not improving despite daily incline board use
- Child's toe walking is causing daily pain or leg fatigue
- Unsure whether approach is correctly matched to your child's cause profile
🟢 ROUTINE: Schedule When Possible
- First-time toe walking beyond age 3 — confirm cause type with PT
- Considering custom orthotics — requires professional fitting
- Child has ASD, DCD, or other condition affecting motor development
Toe walking in Cerebral Palsy is a MEDICAL matter requiring specialist management (physiatrist, orthopaedic, neurologist). This page provides home support for idiopathic, sensory, and habitual toe walking. CP requires supervised specialist intervention.
FREE National Autism Helpline: 9100 181 181 — our clinical team will help you navigate next steps.

Toe walking is one waypoint in your child's gross motor journey
Your Developmental Pathway Map
What Comes Next
- D-368: In-Toeing and Out-Toeing — gait pattern variations
- D-369: Running Development — heel-toe transfer to running
- K-900: Understanding Physical Therapy for Your Child
What Came Before
- D-366: Walking Balance — prerequisite postural stability
- D-365: Visual Stimming — if sensory processing component identified
GPT-OS® AbilityScore® tracks your child's full 12-domain developmental profile. See your child's complete map at pinnacleblooms.org/gpt-os
🏥 Pinnacle Blooms Consortium
OT • PT • ABA • NeuroDev
You are not the first family on this path. Here's what others found.
Story 1 — ASD + Sensory-Based
Before: "Our son (6 years, ASD) was a constant toe walker — every surface, always on toes. We'd been told it was 'just autism' and nothing could be done. His calves were tight and he started refusing to walk outdoors."
Intervention: Sensory OT assessment revealed proprioceptive seeker profile. Started trampoline input twice daily, body sock for regulation, textured path in hallway. Added incline board when calf tightness confirmed.
After (12 weeks): "Heel contact went from zero to around 60%. He actually asks for the body sock now. His PT says his ankle range improved by 15 degrees." — Parent, Pinnacle Hyderabad Center
Story 2 — Habitual/Idiopathic
Before: "My 5-year-old had idiopathic toe walking. Muscle tightness confirmed by PT. Calves tight, couldn't squat heels-down. We'd been doing 30-second stretches with no result."
Intervention: Incline board 15 min twice daily (during TV), resistance band exercises, backward walking games before school.
After (8 weeks): "First time she squatted heels-down at the park. I cried. She didn't even notice she did it." — Parent, Pinnacle Bengaluru Center
"When a child who has toe-walked for years makes heel contact automatically — even once — it proves the pattern is not fixed. That moment is when we know the programme is working." — Pinnacle Occupational Therapist
Isolation is the enemy of consistency. Your community awaits.
📱 Toe Walking & Gait Support — Pinnacle Parent Community
WhatsApp group for parents addressing gait differences. Share updates, ask questions, receive peer support. Join via pinnacleblooms.org/community
💻 Pinnacle Parent Forum — Motor Development Section
Searchable Q&A, technique discussions, therapist-moderated conversations. Visit pinnacleblooms.org/forum
🏢 Local Pinnacle Center Parent Meetups
Monthly parent meetups at 70+ centers across India. Find your nearest center at pinnacleblooms.org/centers
🤝 Peer Mentoring
Connect with an experienced parent who has completed the toe walking programme. Request via 9100 181 181
"Community engagement is a core principle of the Nurturing Care Framework — over 1,000 individuals from 111 countries contributed." — WHO NCF
FREE National Autism Helpline: 9100 181 181 | Available 24×7
70+ centers. India's largest integrated pediatric therapy network. One near you.
🟦 Occupational Therapy
Sensory processing, weighted gear, sensory diet design, tactile desensitization
🟩 Physical Therapy
Stretching, gait training, orthotic fitting and management, strengthening
🟧 NeuroDev Pediatrics
Cause identification, contracture monitoring, specialist coordination
🟪 ABA / BCBA
Behavioral shaping for consistent heel contact, data collection, reinforcement design
What to Ask For at Your First Appointment
AbilityScore® Assessment | Ankle Range-of-Motion Measurement | Sensory Processing Profile (OT) | Gait Analysis (video gait assessment if available)
Teleconsultation available. Can't reach a center? Book via 📞9100 181 181 (FREE) or 🌐 pinnacleblooms.org/teleconsultation | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2

This page is backed by peer-reviewed science. Here's where to explore deeper.
📚 PMC11506176 — PRISMA Systematic Review (2024)
16 studies confirming sensory integration as evidence-based practice for ASD. Key finding: multi-modal approaches outperform single-modality intervention.
📚 PMC10955541 — Meta-analysis (World J Clin Cases, 2024)
24 studies. Sensory-motor intervention significantly improves gross motor skills, adaptive behavior, and sensory processing in pediatric populations.
📚 PMC9978394 — WHO Care for Child Development Package
Age-specific evidence-based recommendations for caregivers across 54 LMICs. Validates home-based caregiver-administered intervention.
📚 DOI: 10.1007/s12098-018-2747-4 — Indian RCT
Padmanabha et al., Indian J Pediatr (2019). Home-based sensory interventions for Indian pediatric population — outcomes equivalent to clinical delivery.
📚 NCAEP Evidence-Based Practices Report (2020)
Confirms video modeling, visual supports, and sensory integration as evidence-based practices for autism. Direct relevance to gait training protocol.
📚 DOI: 10.3389/fnint.2020.556660 — Frontiers in Integrative Neuroscience
Neurological basis for sensory-based interventions. Comprehensive review relevant to the sensory component of toe walking intervention.
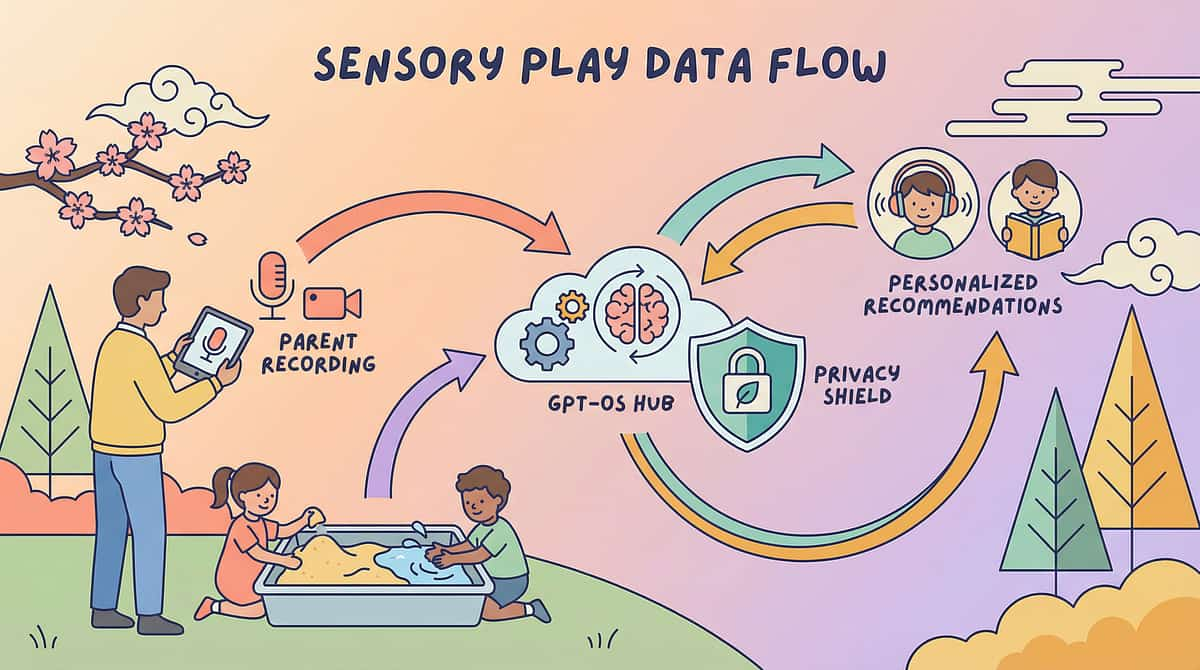
Your home sessions feed the world's largest pediatric therapeutic intelligence system
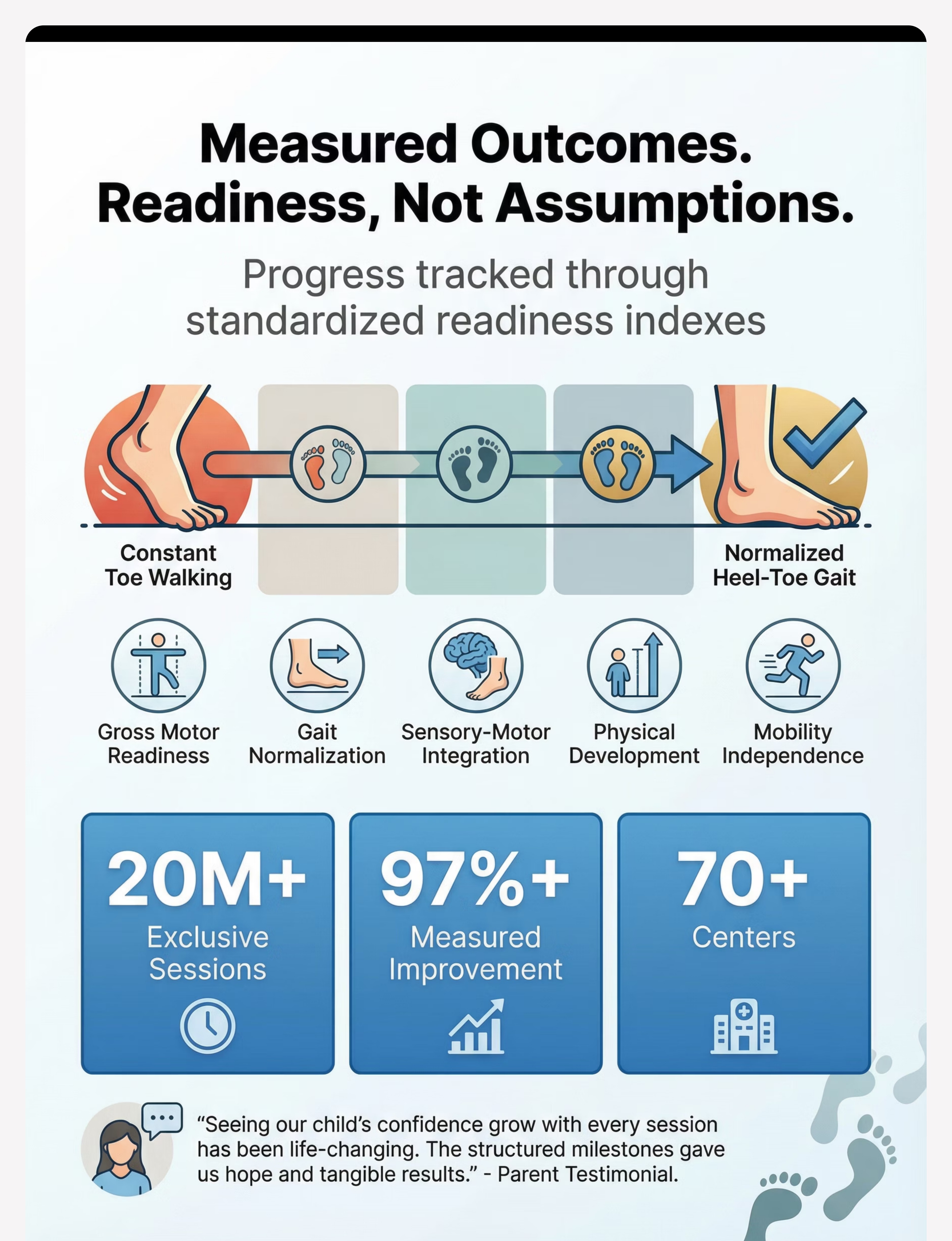
GPT-OS® Data Flow
Gross Motor Readiness Index
Gait Normalization Index
Ankle Mobility Progress
Sensory-Motor Integration Index
Heel Strike Pattern Consistency
"This is not software. This is therapeutic infrastructure." — 20M+ sessions | 97%+ measured improvement | 70+ centers | Patents filed across 160+ countries

Watch the 9 Materials — demonstrated by our therapy team
Pinnacle Reel D-367 | Motor Development Series — Episode 367
This 75-second reel shows all 9 materials in action with therapist voice-over. Real child demonstrations, actual Pinnacle therapy settings, parent-friendly narration. Part of the 999-reel Motor Development educational series. Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning — visual + text + demonstration — improves parent skill acquisition.
◀️ D-366
9 Materials That Help With Vocal Stimming
📌 D-367
9 Materials That Help With Toe Walking (You Are Here)
▶️ D-368
9 Materials That Help When Stimming Causes Harm
📌 D-380
9 Materials That Help With Jumping Skills

Consistency across caregivers multiplies impact — share this with everyone who walks with your child
Pre-filled WhatsApp message: "This page has everything we need for [child]'s heel walking programme. Please read Cards 19–23 before doing any sessions."
For Grandparents
"When [child] walks on toes, we don't say 'put your heels down.' We encourage them to stand on the board, walk the mat path, or do their jumping practice. Then we wait. Consistent home practice is building new muscle and brain patterns."
For Teachers & Schools
A ready-to-use school communication template explains the intervention, requests consistent verbal cues, and provides contact for therapist consultation.
WHO CCD Package: Multi-caregiver training is critical for intervention generalization and maintenance. | FREE: 9100 181 181 | pinnacleblooms.org
Preview of 9 materials that help with toe walking Therapy Material
Below is a visual preview of 9 materials that help with toe walking therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

Questions parents ask most often
Q1: My child is 3 — is it too early to start intervention?
No. Age 3 is actually the ideal time. Toe walking is developmentally expected until age 2–3. If it persists at 3+, beginning intervention NOW prevents the progressive calf tightening that makes later intervention harder. Earlier is always better for musculoskeletal prevention.
Q2: My child has ASD — how does that change the approach?
ASD-related toe walking is most commonly sensory-based (seeking proprioceptive input). Start with sensory-first approach: trampoline, weighted gear, textured mats. Address the sensory need BEFORE focusing on mechanical stretching. Then add incline board if ankle range is limited.
Q3: We've been doing incline board for 3 weeks with no change. What's wrong?
Check: Is the child actually keeping heels ON the board (not hovering)? Is duration 10+ minutes? Is angle appropriate? Also consider: if this is sensory-based toe walking, stretching alone won't change it. Add sensory-motor approach (Cards 12–16) in parallel.
Q4: Can toe walking cause permanent damage?
Prolonged untreated toe walking can cause progressive Achilles tendon and calf muscle shortening (contracture), joint changes in ankles and knees, and gait compensations. This is why early intervention matters. However, at any age, significant improvement is achievable with consistent intervention.
Q5: Do we need orthotics?
Not necessarily for all toe walkers. Orthotics are recommended when: (a) significant muscle tightness with limited ankle range, (b) neurological component present, (c) other interventions not maintaining gains. A physiotherapist should assess whether orthotics are indicated for your child.
Q6: How long until we see heel contact in normal daily walking?
Typical timeline: 8–12 weeks of consistent daily intervention for first spontaneous heel contact in familiar settings. Full generalization often takes 4–6 months. Progress varies by underlying cause and consistency.
Q7: Can we do this at home without a therapist?
The materials on this page can be started at home independently. However, a professional assessment is recommended to: confirm cause type, measure ankle range, determine if orthotics are needed, and create a personalized protocol. Call FREE: 9100 181 181
Q8: My child has tight calves but no ASD. Does this page apply?
Yes. Most materials are equally applicable for idiopathic toe walking, habitual toe walking, and toe walking in typically developing children. The mechanical approach (incline board, orthotics) is more primary in pure muscle-tightness cases; sensory-first is emphasized when ASD or sensory processing differences are present.
FREE National Autism Helpline: 9100 181 181 | Available 24×7 | 16+ Languages
Your child's heel-toe gait is achievable. Start today. Every day of consistent practice is one day closer to normalized gait. The materials exist. The science supports it. Your child is ready.
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
🏥 Pinnacle Blooms Consortium
OT • PT • ABA/BCBA • SpEd • NeuroDev • CRO
This content is educational. It does not replace individualized assessment from licensed physical therapists, orthopedists, or developmental pediatricians. Persistent toe walking requires professional evaluation to determine cause. Never force stretches or exercises that cause pain. Individual results vary. Statistics represent aggregate outcomes across Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
🆘 FREE National Autism Helpline: 9100 181 181 | pinnacleblooms.org | care@pinnacleblooms.org