

"You are not failing. Your child's language is developing in its own profound order." — Pinnacle Blooms Consortium, SLP Division
- Broca's Area — stores language as holistic gestalt units rather than isolated morphemes
- Hippocampus — strong episodic-contextual memory encoding (movie quotes stored with vivid emotional anchors)
- Mirror Neuron System — advanced imitation of complex vocal patterns precedes generative language formation
- Prefrontal Cortex — working memory for novel sentence construction is still building its scaffolding

Stage | Typical Age | With Support | |
Stage 1–2 | 12–24 months | Any age (starting point) | |
Stage 3–4 | 24–36 months | 2–4 years with intervention | |
Stage 5–6 | 36–48 months | 3–6 years with structured support |
"Your child is not stuck at Stage 1. Every child Pinnacle has worked with who received appropriate gestalt-aware support made measurable progress through the stages. The trajectory is forward. Always forward."
- Prizant & Wetherby (1987) — Established echolalia as functional, communicative behavior, not noise
- Blanc (2012) — Natural Language Acquisition (NLA) framework: gestalt-first language development pathway
- Frontiers in Integrative Neuroscience (2020) — Neurological basis for gestalt-first acquisition. DOI: 10.3389/fnint.2020.556660
- PMC Meta-analysis (PMC10955541) — Individual structured sessions in prepared environments showed strongest language outcomes across 24 studies
- Skinner (1957) / Cooper, Heron & Heward — Verbal behavior framework underpinning script modification and reinforcement protocols
"The scripts are not the problem. The scripts are the solution — in their current form. Our job is to help them evolve." — Pinnacle Clinical Framework, B-193

💡FusionModule™ Principle: At Pinnacle, these four disciplines deliver a converged plan — not four separate therapy streams. The SLP, ABA, OT, and SpEd specialists share one GPT-OS® child profile and one language progression target. This is the difference between siloed care and therapeutic infrastructure.








# | Material | Primary Target | Stage Fit | |
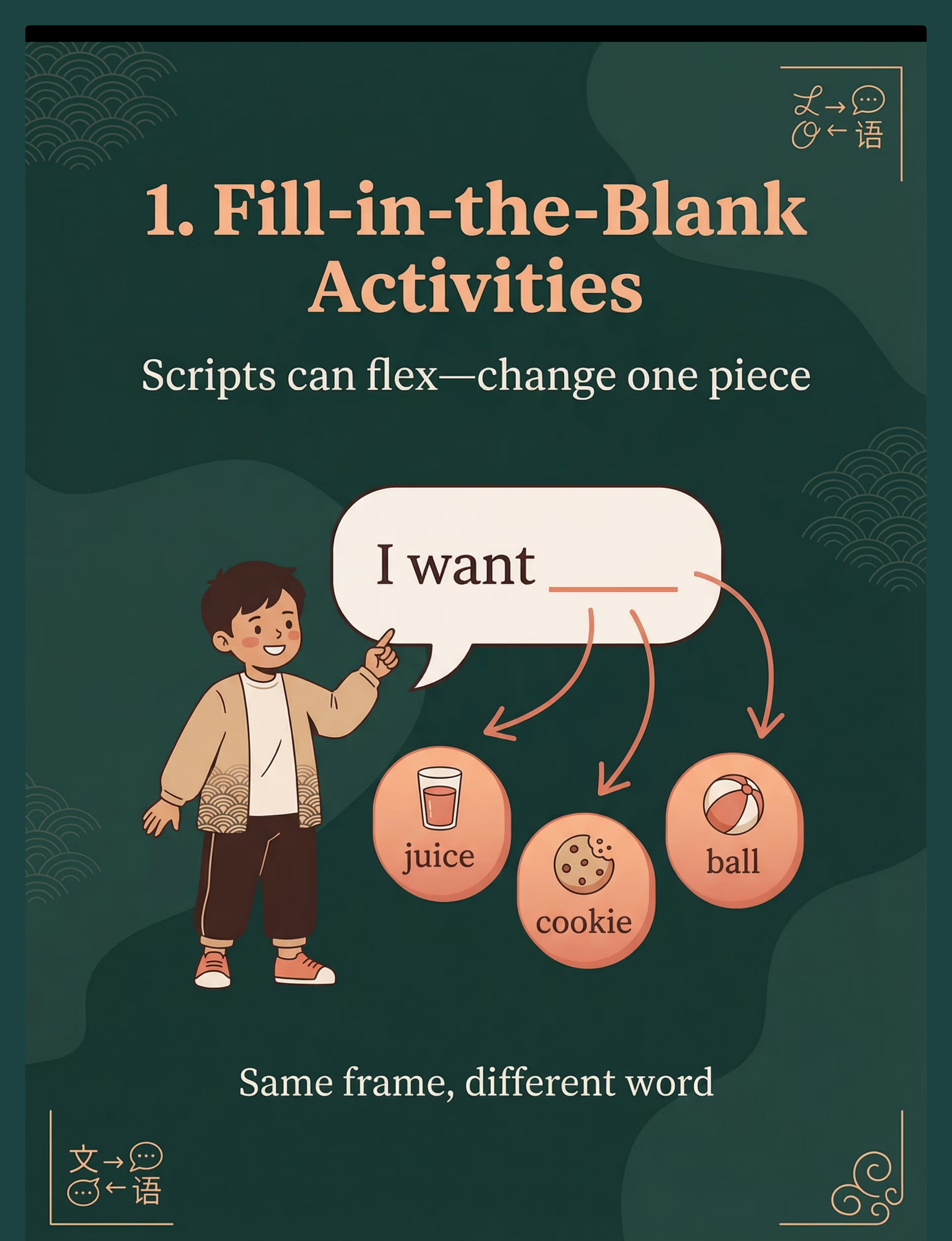
1 | Fill-in-the-Blank / Cloze | Script flexibility — one word at a time | Stage 1–3 | |
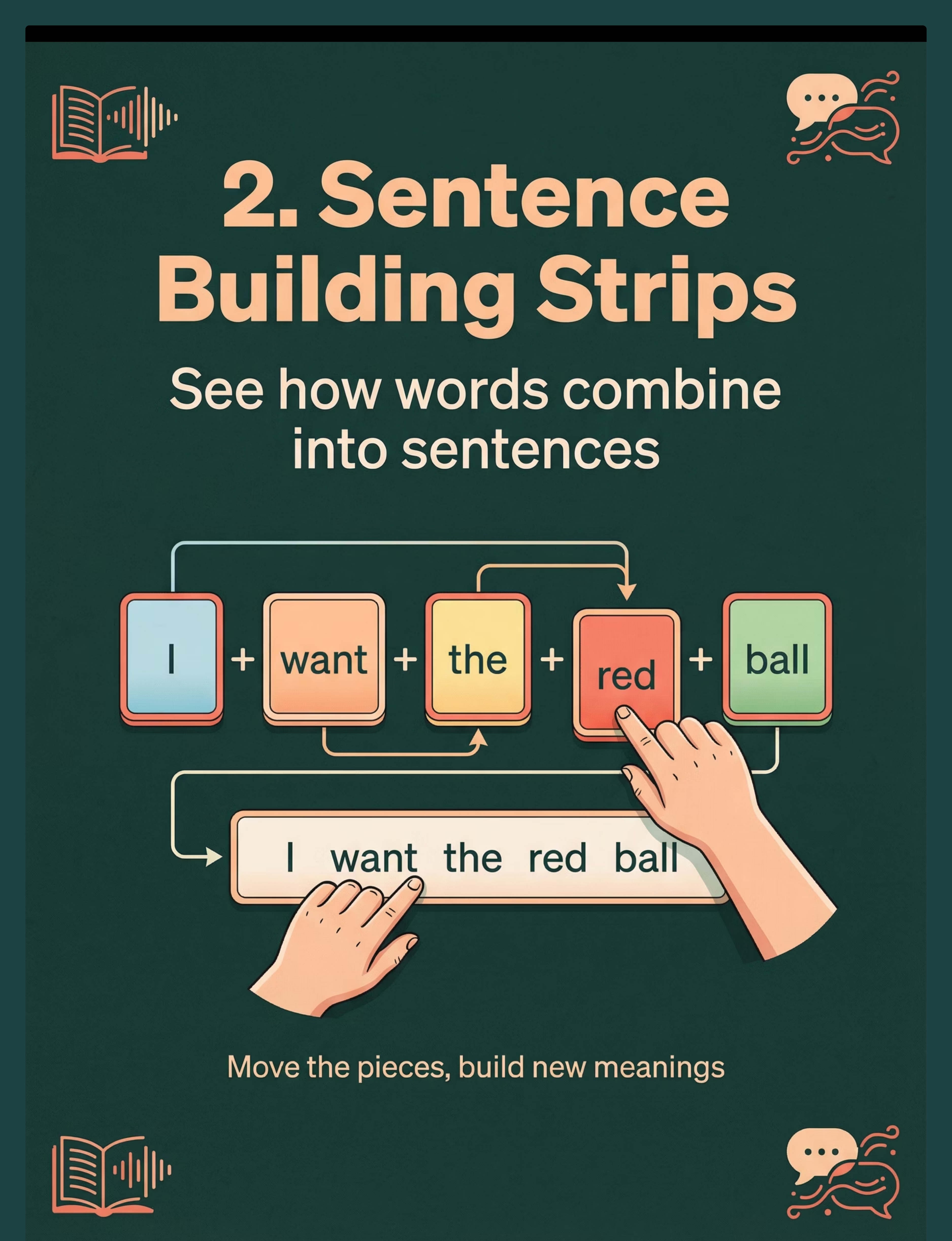
2 | Sentence Building Strips | Language structure visibility | Stage 2–4 | |
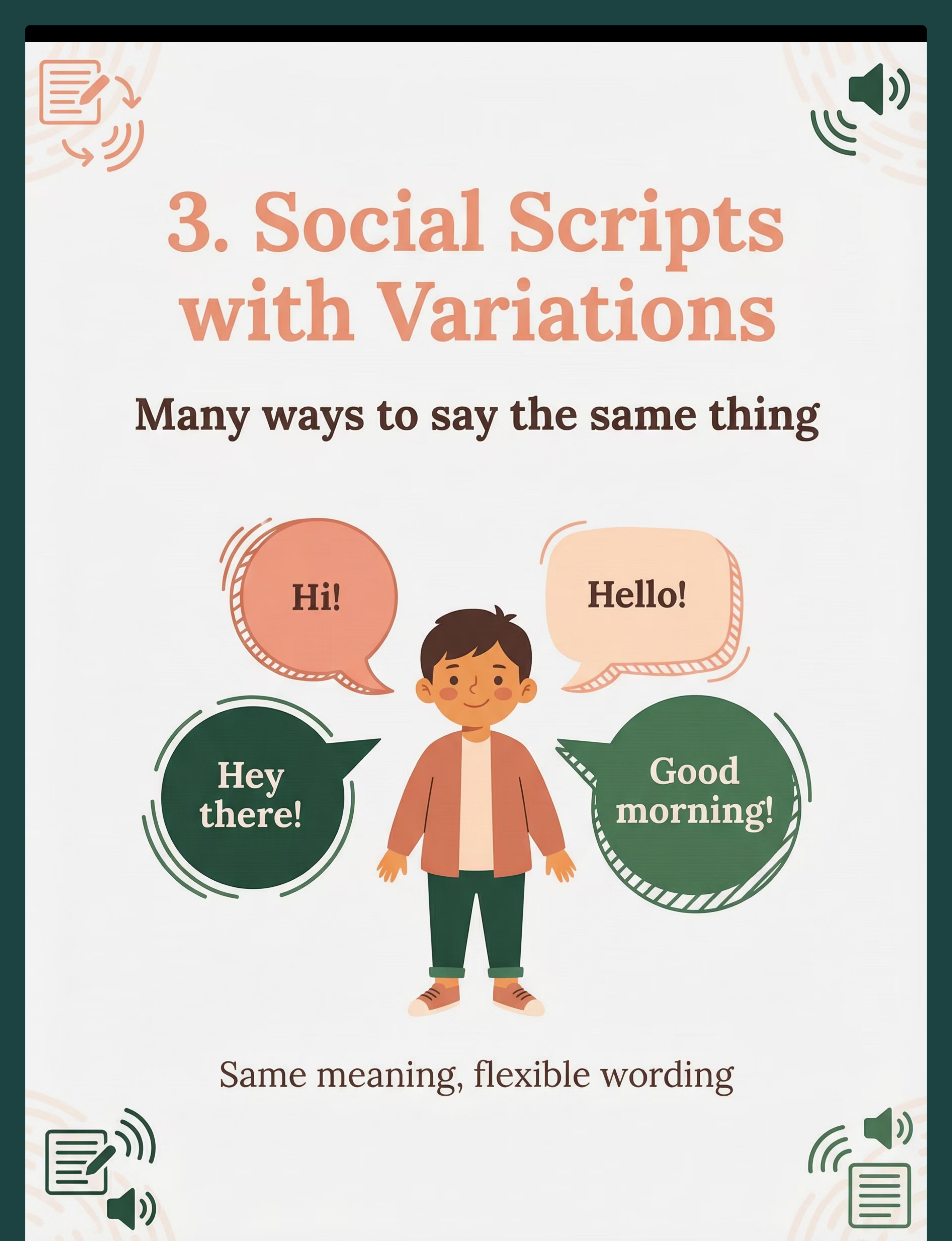
3 | Social Scripts with Variations | Flexible scripts for social moments | Stage 1–3 | |
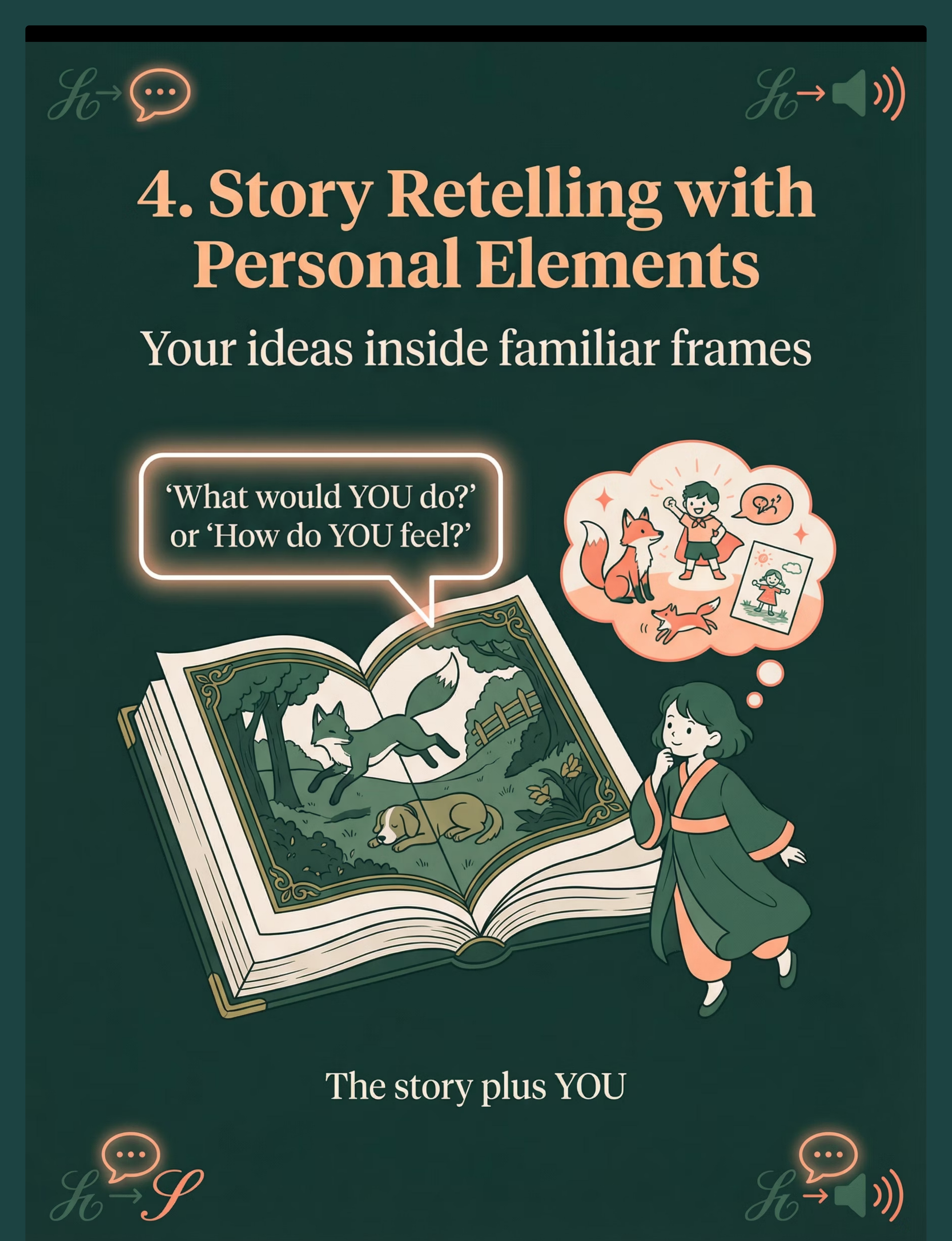
4 | Story Retelling + Personal Elements | First-person perspective language | Stage 2–4 | |
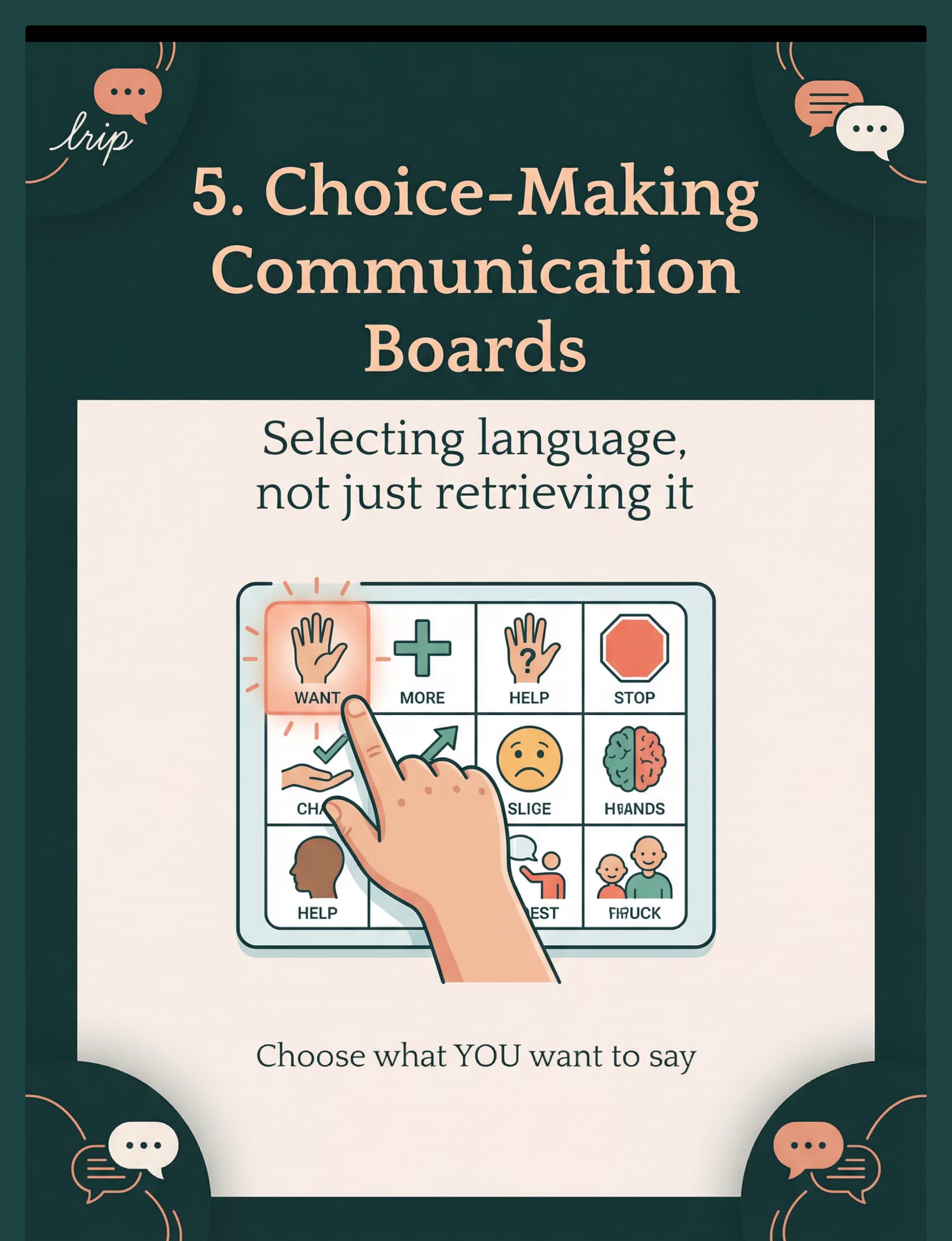
5 | Choice-Making Communication Boards | Active communicative agency | Stage 1–4 | |
6 | Open-Ended Question Prompts | Novel language generation | Stage 3–5 | |
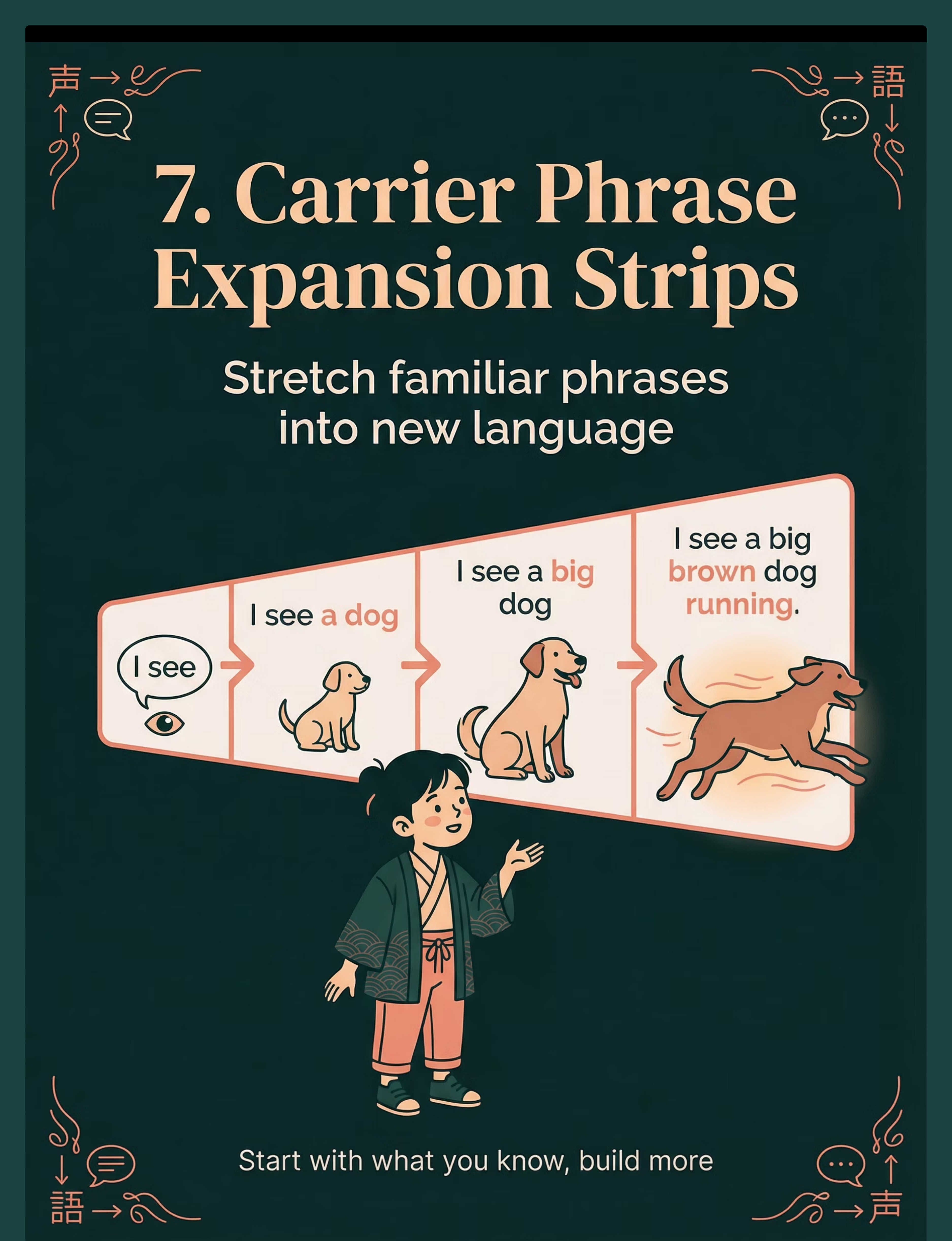
7 | Carrier Phrase Expansion Strips | Script elongation and complexity | Stage 2–4 | |
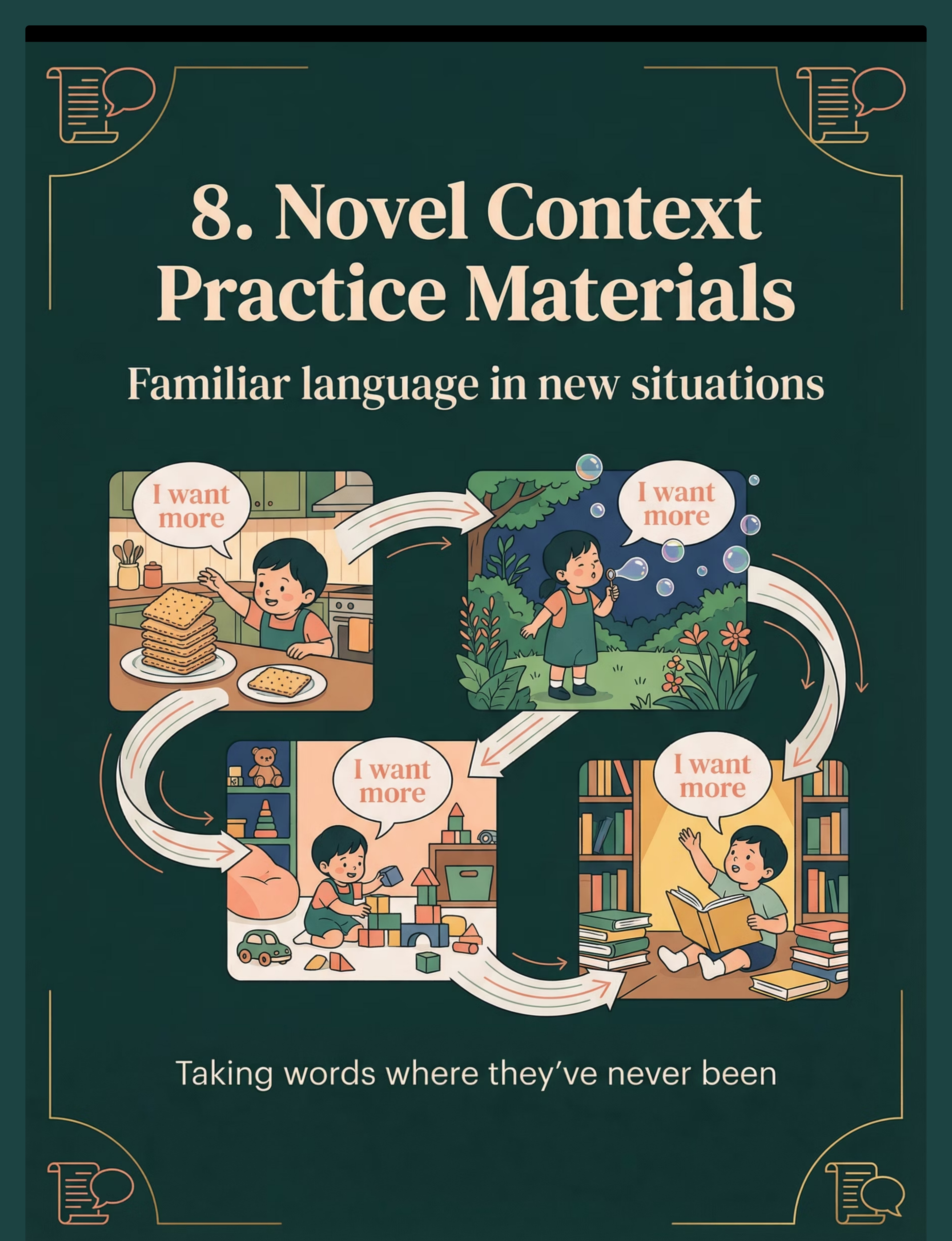
8 | Novel Context Practice Materials | Generalization across settings | Stage 3–5 | |
9 | Thought Bubble & Inner Voice | Metacognitive self-expression | Stage 3–6 |

Material | Buy (₹) | Make at Home (₹0) | |
Fill-in-Blank Cards | ₹150–400 | Write child's scripts on paper. Leave one word blank. Draw 3 picture options below. | |
Sentence Building Strips | ₹200–500 | Cut paper strips. Write one word per strip. Arrange, swap, rebuild on the floor. | |
Social Script Variation Cards | ₹200–450 | Fold paper into cards. Write 4 ways to say "hello" — one per card. Practice daily. | |
Story Retelling Materials | ₹250–500 | Use any favorite book. Add sticky note questions: "What would YOU do?" | |
Choice Boards | ₹200–600 | Draw 4 boxes on cardboard. Paste magazine pictures or draw options. Laminate with tape. | |
Open-Ended Question Cards | ₹150–350 | Write questions on index cards. Keep in your pocket for meals, car rides, bedtime. | |
Expansion Strips | ₹150–400 | Cut A4 paper into long strips. Write expanding sentences. Add one segment per session. | |
Novel Context Practice | ₹200–450 | Create a simple picture book of the same phrase in 4 settings. Phone photos + paper = done. | |
Thought Bubble Activities | ₹100–300 | Draw a cloud shape on paper. Ask child to fill it with "your own ideas." |
- Child is in an active meltdown or severely dysregulated state
- Child has a fever, illness, or significant physical discomfort
- Child has had no sleep the previous night
- You as the caregiver are in a heightened emotional state
- Less than 30 minutes after a high-stimulation activity
- Child has explicitly communicated unwillingness (any modality)
- Recent significant trauma or environmental disruption (same day)
- Child is mildly tired → Reduce session to 5 minutes, 1 material only
- Child ate recently (within 30 min) → Allow settling time first
- Child is visibly distracted → Remove one environmental distractor first
- Child is in "scripting mode" → Join the script first (match + expand, don't interrupt)
- Child is fed, rested, and in a regulated calm-alert state
- Environment is quiet with minimal visual distractions
- Parent is patient, unhurried, and in a positive emotional state
- 10–20 minutes of uninterrupted time available
- Materials are prepared before inviting child to the activity
- Quiet room with door closed or background noise minimized
- Seating at child's eye level (floor mat OR low table + chairs)
- Materials laid out and accessible before child enters
- 30–45 minutes since last meal
- TV/screens off
- Other toys not being used today — out of sight
- Siblings or additional people (unless part of the activity)
- Anything the child will fixate on non-productively
- One preferred comfort item nearby (for child security)
- Timer (visual hourglass or phone) — child sees session has an end
- Reinforcement menu within your reach (not child's)
- Water for child
- Natural light preferred
- Avoid harsh overhead fluorescents if child has light sensitivity
- No flickering lights
- Child: seated comfortably, facing parent
- Parent: eye-level with child, not behind or above
- Materials: to child's left, within easy reach (30cm)

- Lower yourself to child's eye level or below
- Relaxed face — no urgency, no performance anxiety
- Material held casually, not thrust toward child
- Slow, warm movements
- If child makes eye contact → smile, mirror expression
- Moves toward you or the material
- Points at or touches the material
- Produces any sound or script fragment related to the material
- Settles physically near you
- Makes sustained eye contact (even briefly)



These are communication signals. Honor them immediately. When the child has had enough, the therapeutic work for today is done. A clean ending preserves willingness for tomorrow's session.
- Child puts one piece away = "Thank you!"
- Name each item as it goes back — generalizes material vocabulary
- Builds routine predictability for next session
- Free: Phone timer shown to child
- Budget: Sand hourglass (₹150–300)
- Clinical: Time Timer visual clock (₹400–600)
- Do not extend the session — this reinforces resistance
- Use distraction: "Let's go see [preferred thing]"
- Give 30 seconds of preferred activity as the ending bridge
- Stay calm. Consistent endings train cooperative endings.
- Document resistance pattern for therapist review

○ Passive tolerance (present but not responsive)
○ Active engagement (interacted with material)
○ Communicative attempt (used material to communicate)
○ Novel language produced — circle one word child said: ___
0 / 1 / 2 / 3 / 4 / 5+
😟 Difficult — Need help | 😐 Neutral — OK | 😊 Good — Made progress | 🌟 Excellent — Breakthrough moment

Next Time: Invite 30 minutes later. Reduce to just ONE material. Start with only the invitation step — even brief engagement IS success. Consider earlier in-day session timing.
Next Time: Switch to choice board or fill-in-blank. Model new content 3 times before inviting child. Reduce the demand: "Tell me with 1 word" not "Make a sentence."
Next Time: NEVER change a script the child is using for regulation in that moment. Match script first: say it WITH them 3 times. Then offer a CHOICE: "Or can we try...?"
Next Time: Celebrate the script use as communication. Introduce mitigated gestalts. Document which scripts are functional — these are the building blocks.
Next Time: Use Novel Context Practice (Material 8) specifically. Practice the word in 3 different contexts this week. Celebrate every use — context accuracy comes with practice.
Response: Short sessions are valid. 5 good minutes beats 20 forced minutes. Try splitting into 2×8 min sessions across the day.
Response: There is no "wrong" in a safety-met session. If child was safe and you stayed calm — the session was successful. Call 9100 181 181 for a 20-minute parent coaching session.

Parameter | Easier | Harder | |
Session Duration | 5 min | 20 min | |
Materials per Session | 1 only | 3 materials | |
Demand Level | No demand | Structured trial | |
Response Required | Gesture OK | Specific word | |
Repetitions | 1 rep | 5 reps |



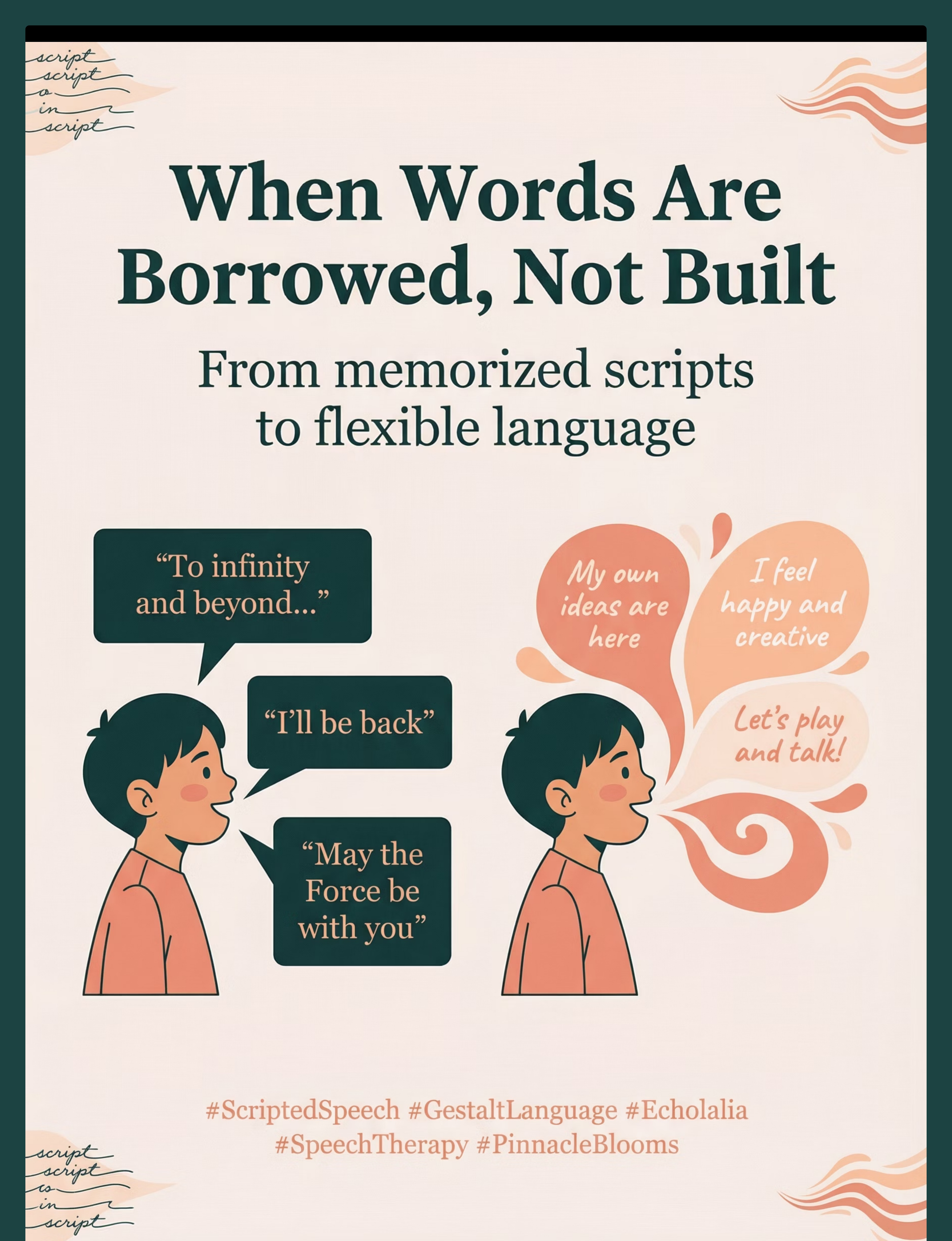
Your child said something that was entirely their own. Not a movie quote. Not a TV line. Not a borrowed phrase. Theirs. And that happened because you showed up, session after session, with patience that most people will never understand.

Share This with Your Family
ACT V — GENERALIZATION This technique works best when everyone in your child's world knows it. Consistency across caregivers multiplies impact. Multi-caregiver training is critical for intervention generalization and maintenance. (PMC9978394, CCD Package) 📱 Share on WhatsApp "I found something important about how [child's name] communicates. Please read this — it's changed how I understand scripted speech." [Link: techniques.pinnacleblooms.org/speech/scripted-only-speech-B-193] 📥 Family Guide — 1-Page PDF Simple, visual guide for spouse/partner, grandparents, aunts/uncles, and anyone who spends regular time with your child. pinnacleblooms.org/B-193-family-guide 📥 Teacher Communication Template Ready-to-send letter explaining scripted speech to your child's school teacher. Includes: what scripted speech is, how to respond, what NOT to do, and how to support in the classroom. pinnacleblooms.org/B-193-teacher-template For Grandparents & Extended Family [Child's name] learns language differently. Instead of building sentences word by word, they memorize whole phrases first — like movie quotes. This is NOT a behavior problem. This is a brain difference that responds to specific support techniques.When they quote a movie: → DON'T correct them or say "that makes no sense" → DO respond as if it's real communication → DO match their phrase, then add ONE new word.The therapy is working. Your job is consistency. When everyone responds the same way, [child's name] learns faster.

"You now know more about your child's language than most parents ever will. The science is in your hands. The materials are in your reach. The only question is: will you begin tonight?"
Preview of 9 materials that help with scripted only speech Therapy Material
Below is a visual preview of 9 materials that help with scripted only speech therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






FROM FEAR TO MASTERY. ONE TECHNIQUE AT A TIME.
Pinnacle Blooms Network® exists to transform the home of every family raising a neurodiverse child into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy center. Not as a replacement for clinical care. As an extension of it.
A parent who is informed, consistent, and empowered is the most powerful therapeutic force in any child's life. We build that parent. One technique, one evidence base, one session at a time. For 70+ countries. For every family. For every child.