
When your whole family walks on eggshells to keep things exactly the same.
Insistence on sameness isn't stubbornness. It's a nervous system that genuinely perceives change as danger.
"My child has to have everything exactly the same, every single time. The same route to school — if I take a different turn, complete meltdown. The same cup for milk — if it's in the dishwasher, crisis. The same bedtime routine — skip one step, an hour of screaming. We can't travel. We can't have people over. We walk on eggshells trying to keep everything exactly the same to avoid the next explosion. But we can't keep the world the same forever."
Pinnacle Blooms Consortium
Ages 2–12
Behavioral Flexibility Series — Episode D-373
📞 FREE National Autism Helpline: 9100 181 181 | Available 24×7 in 16+ languages

You Are Among Millions of Families Navigating This
These behaviors are not a parenting failure. They are not defiance. They are a documented neurological difference in how the brain processes uncertainty — confirmed across 160+ countries in Pinnacle's own 20M+ session dataset.
1/36
Children with ASD
Diagnosed globally (CDC 2023) — with insistence on sameness as a core diagnostic feature
80%
Show Repetitive Behaviors
Of children with ASD show significant restrictive/repetitive behaviors including sameness insistence (PMC11506176, 2024 PRISMA review)
47M
Children Worldwide
Live with autism spectrum disorder — and rigid routine dependence affects all of them to varying degrees
Research: PMC11506176 (PRISMA Systematic Review, 2024) | PMC10955541 (Meta-analysis, 2024) | WHO/UNICEF CCD Package (2023)

This Is a Wiring Difference. Not a Behavior Choice.
The Neuroscience
Prefrontal Cortex: Governs cognitive flexibility and set-shifting. In sameness insistence, this region shows reduced activation during transitions, making shifting between mental sets genuinely difficult.
Amygdala Hyperactivation: Unpredictable events trigger the threat-detection system — the same response as physical danger. The child is not overreacting. Their brain is registering a genuine alarm.
Intolerance of Uncertainty (IU): The brain treats uncertainty itself as aversive — driving the need for sameness as a regulatory mechanism.
Weak Central Coherence: Difficulty seeing the "big picture" means individual details feel critically important — any deviation from expected details reads as crisis.
What This Means for You
"When your child melts down because you took a different route to school, they are not being dramatic. Their amygdala fired a genuine distress signal. The brain said 'threat.' They responded the way any of us respond to a threat — with fight, flight, or freeze."
The path forward is not demanding they "get over it." It is teaching the brain that change can be survived — through graduated, supported, visually scaffolded exposure.
Research: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660
Your Child Is Here. Here's Where We're Heading.
Some routine preference is developmentally healthy. The goal is not eliminating your child's need for predictability — it is expanding what counts as "predictable." With the right materials, that window can grow significantly.
Age 18 months
Typical routine preference emerges
Ages 3–6
Insistence on sameness peaks in ASD — most responsive to intervention
Ages 5–8
With support, tolerance window expands meaningfully
Ages 8–12
Functional flexibility for school and community settings
Adolescence
Navigating daily life changes with increasing independence
Comorbidities to be aware of: Anxiety disorders (co-occurs in 40–60% of children with ASD) · OCD (requires distinct clinical pathway) · Sensory Processing Disorder · ADHD (rigidity as compensation for internal executive chaos)
Research: WHO CCD Package (2023) | PMC9978394 | Padmanabha et al., Indian J Pediatr 2019
Evidence Grade: LEVEL I–II
Clinically Validated. Home-Applicable. Parent-Proven.
These are not informal suggestions. They are clinically validated tools deployed across 70+ Pinnacle centers and 20M+ therapy sessions.
Study | Key Finding | |
NCAEP 2020 Report | Visual supports classified as Evidence-Based Practice for ASD | |
PMC11506176 (2024 PRISMA) | Visual schedule interventions show significant reduction in transition-related behavior across 16 studies | |
PMC10955541 (Meta-analysis, 2024) | Sensory regulation interventions improve behavioral flexibility across 24 studies | |
Padmanabha et al., 2019 | Home-based interventions demonstrate equivalent outcomes to clinic-based when parent-trained | |
WHO/UNICEF CCD Package | Multi-caregiver, structured visual intervention across 54 LMICs confirms generalizability |
83%
Evidence Confidence
Level I–II (Systematic Reviews + RCTs)
97%
Measured Improvement
Across Pinnacle's 20M+ therapy sessions
📞 FREE National Autism Helpline: 9100 181 181

Insistence on Sameness — Multi-Material Flexibility Building Protocol
Also known as: "The Predictability Toolkit"
Insistence on Sameness (IS) is the intense need for routines, rituals, and environmental consistency — with significant distress when changes occur. It is a core feature of Autism Spectrum Disorder and also presents in anxiety disorders, OCD, and developmental conditions.
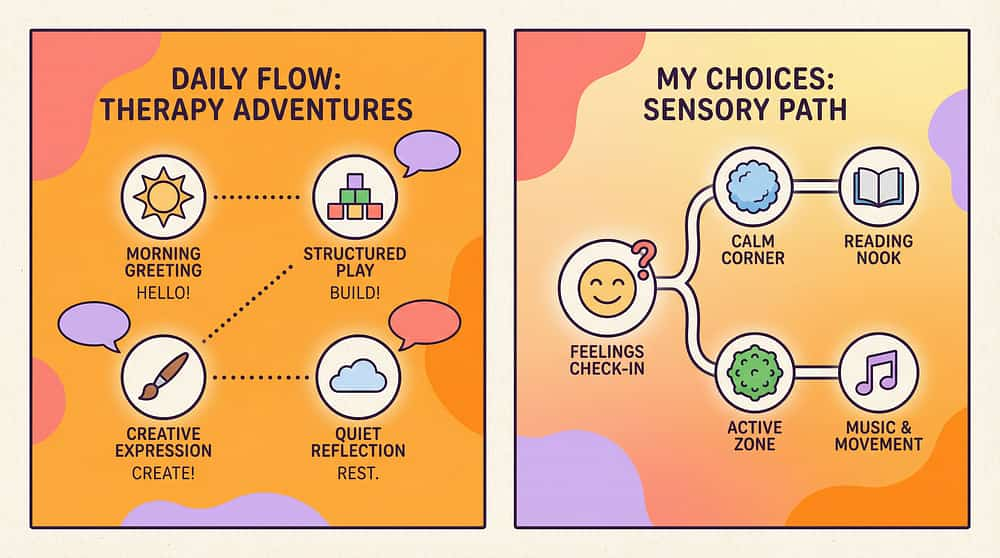
The Predictability Toolkit is a structured, materials-based home intervention that simultaneously provides the predictability children need AND gradually expands their tolerance for variation — using 9 evidence-based materials across 5 categories: visual systems, cognitive scaffolding, sensory regulation, transition support, and portable comfort.
🧠 Behavioral Development
🔄 Cognitive Flexibility
💜 Emotional Regulation
🔬 Autism Spectrum Features
😰 Anxiety Management
Age Range | 2–12 years | |
Setting | Home + School + Community | |
Frequency | Daily integration (not discrete sessions) | |
Duration | Long-term — 6–18 months for significant flexibility gains |

Five Disciplines. One Integrated Protocol. Zero Gaps.
Your child's brain doesn't organize itself by therapy type. Flexibility is built through regulation (OT), language (SLP), behavior (ABA), education (SpEd), and medical clarity (NeuroDev) — simultaneously.
BCBA / ABA
Designs reinforcement system for flexibility; functional behavior assessment to identify sameness drivers; graduated exposure planning
Occupational Therapist
Sensory profile assessment; calming toolkit design; visual schedule setup; sensory-driven sameness differentiation
Special Educator
Visual schedule implementation at school; predictability cards for classroom; school-teacher communication
Speech-Language Pathologist
Social stories design; language scaffolding for change narratives; communication supports during transitions
NeuroDev Pediatrician
Rules out OCD requiring distinct pathway; medication considerations for anxiety; developmental context
Validated by Pinnacle Blooms Multi-Disciplinary Consortium | 📞9100 181 181

Precision Tools for Precisely Defined Targets
This protocol targets behavioral flexibility across three levels — from immediate observable change to long-term developmental gains.
🎯 Primary Targets
- Tolerance for announced changes (showing change card without meltdown)
- Transition smoothness between activities (using timers without resistance)
- Coping strategy initiation during distress (independently reaching for toolkit)
🎯 Secondary Targets
- Reduction in meltdown intensity and duration
- Reduction in family avoidance behaviors ("walking on eggshells" index)
- Increased parental confidence in introducing variation
- Generalization of flexibility to school and community settings
🎯 Tertiary Developmental Gains
- Interoceptive awareness (recognizing own regulation state)
- Executive function development (set-shifting, cognitive flexibility)
- Anxiety management capacity (generalizable beyond sameness contexts)
- Social participation (events, visitors, travel)
Observable Behavioral Indicators
Can look at change card without immediate shutdown
Asks "what will happen?" rather than refusing to hear about change
Transition from preferred activity takes <5 minutes (vs. 30+)
Uses comfort object independently when entering new environments
References coping strategy during distress

The 9 Materials. Clinically Mapped. Ready to Use.
Pinnacle Recommends ✓
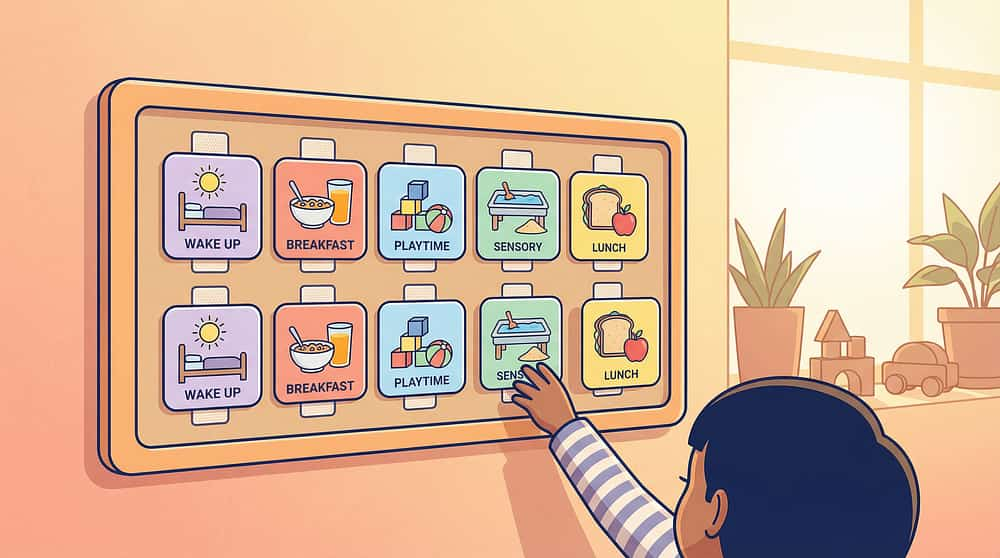
1. Visual Schedule Board
Externalizes routine into visible, changeable format. DIY: paper strips + velcro + phone photos. ₹500–₹2,000

2. Comfort Object / Transitional Toy
Portable sameness anchor for all environments. Animal Soft Toys. ₹425 — Amazon.in

3. Sensory Calming Toolkit
Stress ball, textured fidgets, weighted lap pad, noise-canceling headphones. ₹800–₹3,000

4. Visual Timer
Time Timer, sand timer, or countdown strip — makes time visible and tangible. ₹400–₹1,500
5. Social Story Books
Custom printed or DIY social stories about change and coping. ₹300–₹1,500 or free DIY
6. First-Then Board
Shows the path through change to something desired. Two-panel visual contingency map. ₹300–₹1,000
7. Worry Box + Journal
Externalizes anxiety — child places worries inside the box to give them a place to go. ₹200–₹800

8. Predictability / Sequence Cards
Step-by-step visual narratives for new experiences. Index cards or printed photos. ₹300–₹1,000

9. Flexibility Games
Low-stakes playful change practice. SHINETOY Shut The Box Game. ₹428 — Amazon.in
Zero-Cost Access. Every Parent. Every Budget. Every Postal Code.
Every one of the 9 materials can be made at home with zero budget. The neuroscience works regardless of the price of the tool.
Buy This
Visual Schedule Board — ₹500–₹2,000
Calming Toolkit — ₹800–₹3,000
Visual Timer — ₹400–₹1,500
Social Story Book — ₹300–₹1,500
First-Then Board — ₹300–₹1,000
Worry Box — ₹200–₹800
Comfort Object — ₹425
Predictability Cards — ₹300–₹1,000
Flexibility Games — ₹428
Make This (Free)
A4 paper strips laminated + phone photos + velcro dots (₹50)
Ziplock bag: rice (tactile) + rubber band (proprioceptive) + cotton ball with lavender + earphones
Countdown drawn on paper; phone timer with screen visible; sand in a bottle
Typed A4 pages with child's photo + simple drawings, laminated
Two A4 papers labeled "FIRST" and "THEN" with drawn/printed pictures
Any cardboard box + child decorates with crayons; slot cut in lid
Child's existing favourite item (often already owned)
Index cards + real photos printed on phone + staple/ring binder
"Opposite Day" or "Story Twist" — no materials needed
"These strategies must work for families in Nagpur and in New York, in a village with no Amazon delivery and in a city with same-day shipping. The neuroscience works regardless of the price of the tool." — WHO/UNICEF Equity Principle
Read Before You Begin. Every Time.
Before using any of these 9 materials, run through this safety checklist. The environment and state of your child determine whether today is a go, a modify, or a postpone day.
🔴 DO NOT PROCEED IF:
- Child is currently in meltdown or severely dysregulated
- Child has not eaten or is sleep-deprived
- Child shows signs of illness (sensory sensitivity heightens)
- Rigidity appears to be OCD-driven (compulsive rituals, washing, checking) — requires specialist pathway
- Any flexibility intervention causes self-injurious behavior or aggression
🟡 PROCEED WITH MODIFICATION IF:
- Child had a difficult morning (use simplified version; skip flexibility games today)
- Sibling conflict or household stress is elevated (maintain core routines; postpone flexibility practice)
- New medications recently started (monitor for behavioral changes before introducing new materials)
🟢 GOOD TO PROCEED:
- Child is fed, rested, regulated
- No recent major disruptions (illness, move, school change)
- Core routine is established and predictable (do not introduce flexibility before the routine feels safe)
- Comfort object is accessible throughout
Safety Non-Negotiables
- Never introduce new materials during a meltdown
- Never remove comfort object as "motivation" for flexibility
- Never flood the child with multiple changes simultaneously
- Never punish rigidity — it escalates anxiety and rigidity
- Seek professional evaluation if rigidity causes harm to safety/health/nutrition
If you are unsure whether to proceed — 📞9100 181 181 — our consortium specialists will guide you. FREE. 24×7.

The Right Environment Is Half the Intervention.
The environment IS part of the therapy. Visual schedules on walls, timers on tables, toolkits on shelves — these communicate safety before a single word is spoken.
Room Setup Checklist
- ☐ Visual schedule mounted at child's eye level
- ☐ Comfort object within child's reach at all times
- ☐ Calming toolkit bag accessible (not hidden away)
- ☐ Timer visible to child
- ☐ First-Then board ready with current activity pictures
- ☐ Worry box within reach for anticipated changes
- ☐ Screens OFF during flexibility practice sessions
- ☐ Predictability cards prepared for any known upcoming changes
- ☐ Quiet, low-sensory environment (reduce ambient noise/light if possible)
- ☐ YOU are calm — your regulation co-regulates theirs
Key Positions
Quiet corner — no TV/screen distractions
Visual schedule — mounted at child's eye level on wall
Calm space — soft mat + comfort object + calming toolkit bag nearby
Timer — placed where child can see it clearly
First-Then board — accessible, moveable
Parent position — within arm's reach but not hovering

60-Second Pre-Flight Checklist
Before every flexibility practice session, run this 60-second check. The best flexibility session is one the child is ready for — pushing through an unready child builds the association: change = distress.
Fed in the last 2 hours?
Slept adequately last night?
No fever, illness, or pain?
Core routine was followed today?
Not currently in sensory overload?
No major disruption in last 30 minutes?
Comfort object accessible?
7/7 ✅ → GO
Proceed with full flexibility practice session
5–6/7 ✅ → MODIFY
Use only regulation tools today; postpone flexibility games
4 or fewer ✅ → POSTPONE
Maintain complete sameness today; connection over correction
"Patience now multiplies gains later."

Step 1 of 6
Safety First. The Foundation Before Flexibility.
PROTOCOL STEP 1 — Establish Baseline Predictability (Days 1–14)
Before introducing ANY flexibility, the child must feel genuinely safe and anchored in their routine. Do not rush past this phase — it is the foundation everything else is built on.
1
Visual Schedule — Trust First
Child must understand and rely on the schedule before change cards are introduced. Run the same routine visually for 7–14 days.
2
Comfort Object — Everywhere
Begin bringing it everywhere — this is the portable sameness anchor across all environments.
3
Calming Toolkit — During Calm Only
Assemble the toolkit and practice during calm times only — at least 5 sessions of calm toolkit use before first use during distress.
4
Timer — One Low-Demand Transition
Introduce for one low-demand transition (e.g., ending puzzles). Build the habit of visible timing with neutral stakes.
5
Social Story — Daily Calm Reading
One social story about "changes happen" is read daily — not during distress, at a calm time like bedtime.
Parent Role: Follow the routine reliably. Narrate the schedule ("First breakfast, now we can see it on the board"). Validate without shaming: "You like knowing what happens next. That makes sense."
Step 2 of 6
Make Change Visible Before It Happens.
PROTOCOL STEP 2 — The Change Card System (Week 3–4)
Once the visual schedule is trusted, introduce the change card — a distinctive, visually prominent card that announces variation before it occurs. The first change card experience should always lead to something good.
1
Create Change Cards
3–4 cards in a distinctive color (orange or red). Use a star, question mark, or "change" symbol.
2
Introduce During Calm
No actual change yet — explain: "Sometimes something different happens. When it does, I'll show you first."
3
First Use — Positive Change
Park visit added, favorite activity added. The first change card experience must lead to something GOOD.
4
Build to Neutral Changes
Slightly different cup, slightly different order. Always pair with a predictability sequence showing what WILL happen.
The Change Card Ritual
📞 9100 181 181 | Research: PMC11506176 | NCAEP 2020
Step 3 of 6
You Cannot Flex a Brain That's in Panic Mode.
PROTOCOL STEP 3 — Regulation-First Protocol (Weeks 3–8, ongoing)
The sequence is always: Regulation → Acknowledgment → Flexibility request. Most parents make the mistake of announcing the change first, then offering calming tools. Reverse this order — always.
Before announcing the change
Hand child the calming toolkit / ensure comfort object is in hand
Announce with visual
Show change card on the schedule — make it visible and concrete
Name the feeling
"This is different from usual. It's okay to feel worried."
Wait for partial regulation
Not full calm — just reduced arousal before moving forward
Activate First-Then Board
Show the path THROUGH the change to something desired
Debrief after
"That was different. You got through it. What helped?"
Common Mistake: Announcing the change first, THEN offering calming tools. Reverse this order. Regulation → then information.
Step 4 of 6
Practice Change When the Stakes Are Low.
PROTOCOL STEP 4 — Daily Flexibility Games (Week 4 onward, 10–15 min/day)
Flexibility is a skill. Like reading or cycling, it improves with practice — but ONLY when the brain is safe. Daily playful flexibility practice builds the neural pathways without triggering the threat system.
Game | What Changes | Stakes | |
Opposite Day | One small thing reversed (different chair, different cup) | Zero — it's playful | |
Story Twist | Change the ending of a familiar story | Low — fiction | |
Role Reversal | Child plays parent for 5 minutes | Low — fun | |
Surprise Box | Pick from a box of silly tasks (make an animal sound, wear glasses) | Low — silly | |
Game Rule Change | Take existing game, change one rule | Low — child can decide |
"You just did something different! That's what flexible thinkers do!"
CRITICAL: Do NOT use games as disguised demands about real-life triggers. Games must be genuinely playful. If distress appears, stop and regulate. Return next day. The Flexibility Point Chart rewards flexibility — not compliance.

Step 5 of 6
Give the Worry a Place to Go.
PROTOCOL STEP 5 — Worry Processing Daily Ritual
Every worry that lives inside your child's nervous system without expression becomes anxiety fuel. The worry box and change journal give that energy somewhere to go — outside the body, on paper, in a box.
☀️ Morning Routine (5 minutes)
- Review today's visual schedule together
- Name any changes on the schedule
- "Is there anything you're worried about today?" → child draws or writes it → places in worry box
- Review change journal: "Look how many changes you've already survived!"
- Pack calming toolkit if going out
🌙 Evening Routine (5 minutes)
- Review what happened today
- Note any changes encountered and how child coped
- Add to change journal: Date | What changed | How I felt | What helped | What happened
- Celebration: "That was different from usual. You handled it."
- Read social story if tomorrow has a known change
"Every entry is evidence. The journal proves — to your child and to their nervous system — that changes have been survived before. This is your child's personal scientific dataset of flexibility."
Step 6 of 6
Make the Unknown Known Before You Get There.
PROTOCOL STEP 6 — Predictability Mapping for New Experiences
For ANY anticipated new experience — doctor visit, party, new restaurant, school event — build a card sequence that makes the unknown completely visible. Review daily for 3–5 days before. Bring cards to the actual event.
Research the Environment
Visit in advance if possible; look up photos; note sights, sounds, smells at each step
Build the Card Sequence
Step-by-step visual narrative including potential discomfort honestly ("It might smell like medicine") and coping steps
Review Daily
3–5 days before the experience — familiarity before arrival
Bring Cards to the Event
Child can reference during the actual experience for real-time anchoring
Debrief After
Add to change journal — each new entry is evidence of survival and flexibility
Example — Doctor Visit Sequence: Drive to clinic → Park and walk to door → Waiting room (blue chairs, might be noisy) → Nurse calls our name → Doctor's room (bright light) → Doctor checks ears and throat → We're done! Sticker from nurse → Ice cream on the way home. 📞 9100 181 181

What Gets Measured, Gets Better.
Without data, you're guessing. With data, you see the trend that isn't visible day to day. Parents who track consistently report 3× more confidence in the process — because they can see the progress that feels invisible in the daily struggle.
Daily Tracking (2 minutes)
- Change card shown today? (Y/N)
- Child's distress level during change: 1 (none) → 5 (severe meltdown)
- Calming toolkit used? (Y/N)
- Flexibility game played today? (Y/N)
- One flexibility win today (free text)
- Worry box used today? (Y/N)
- Predictability card used today? (Y/N)
AbilityScore® Integration
These data points flow directly into GPT-OS® and update your child's Behavioral Flexibility Readiness Index — a real-time measure of progress on the 0–1000 AbilityScore® scale.
The EverydayTherapyProgramme™ tracker uses this data to personalize the next day's session and coordinate OT/ABA/SLP inputs through FusionModule™.

The 7 Most Common Obstacles — Solved.
If your materials aren't working as expected, one of these seven patterns is almost certainly the cause. Each has a clear clinical solution.