"She can't stop thinking about it. And she knows it isn't true. And it still won't stop."
The same worry. The same fear. The same question — on loop. You've answered a hundred times. She knows the hands are clean. She knows she didn't hurt anyone. The thought plays anyway. You are not failing. Her brain is not broken. And there are tools that help.
C-294 | Emotional Regulation | Ages 5–14
Anxiety & OCD Spectrum

ACT I — THE EMOTIONAL ENTRY
You Are Not Alone — The Numbers
Obsessive thoughts are not a character flaw. Not bad parenting. Not a failure of love or reassurance. They are a recognizable, documented, treatable pattern in how the brain processes uncertainty — experienced by children across every country, culture, and background.
1 in 100
Children Have OCD
Global prevalence per WHO data — across every culture and socioeconomic background
80%
ASD + Intrusive Thoughts
Of children with ASD experience intrusive or obsessive thoughts (PRISMA Systematic Review, 2024)
20M+
Pinnacle Sessions
Therapy sessions run by Pinnacle Blooms Network® tracking these exact patterns — 97%+ measured improvement
You are among millions of families navigating this exact challenge. Evidence-based tools exist — from clinic to home — that change the brain's relationship with thoughts. 📞 9100 181 181 — FREE | Talk to a Pinnacle Consortium specialist today

What's Happening in Your Child's Brain
"This is not anxiety about real things. This is the brain's threat-detection system misfiring."
The Neuroscience
The prefrontal cortex and the amygdala are locked in a miscommunication loop. In typical brains: thought arises → amygdala evaluates → prefrontal cortex says "not a real threat" → thought passes.
In obsessive thought patterns: thought arises → amygdala fires alarm → prefrontal cortex attempts to silence it (which makes it louder) → thought intensifies → compulsive response provides brief relief → loop resets and strengthens.
Plain English
The thought isn't true. The child knows it isn't true. But "knowing" doesn't reach the alarm system. The more she tries to push the thought away → the louder it gets. The more you reassure her → the alarm learns to need more reassurance.
This is a wiring pattern, not a character flaw. The brain that learned to loop can learn to let go. That is precisely what these 9 materials help achieve.
Research: Frontiers in Integrative Neuroscience (2020) — Comprehensive framework for evaluating sensory and cognitive processing treatment. DOI: 10.3389/fnint.2020.556660

Where This Sits in Development
Obsessive thoughts are not random. They follow developmental patterns — with known intervention windows. Understanding your child's stage helps you calibrate the right approach.
Ages 2–5
Ritualistic behavior is developmentally normal — serves mastery and predictability. Gentle redirection works well.
Ages 5–8
Transition period. Magical thinking fades. Cognitive awareness of thought content increases. Obsessive patterns begin to crystallize if untreated.
Ages 8–12 ← First Peak
Metacognition develops — the child becomes aware of their own thoughts. If patterns are maladaptive, this awareness amplifies distress significantly.
Ages 12–16 ← Second Peak
Particularly for harm obsessions, perfectionism, and scrupulosity. Children with autism, ADHD, and PANDAS/PANS are at elevated risk.
"The period from pregnancy to age 3 is key — but intervention at any age reshapes developmental trajectories." — WHO Nurturing Care Framework, 2018 | Reference: PMC9978394

The Evidence Behind These Techniques
⭐⭐⭐⭐ Level I — Systematic Review + RCT Evidence
Clinically validated. Home-applicable. Parent-proven.
🔬 CBT with ERP — Gold Standard
The IOCDF classifies Exposure and Response Prevention (ERP) as first-line psychological treatment for pediatric OCD. Multiple RCTs confirm 60–80% response rates.
🔬 Cognitive Defusion (ACT-based)
Acceptance and Commitment Therapy — including thought bubbles, externalization, and mindfulness — shows significant efficacy for pediatric anxiety and obsessive presentations.
🔬 Externalization Techniques
Giving OCD a character name and separating it from the child's identity is a core evidence-based technique across CBT and narrative therapy frameworks.
🔬 Parent-Mediated Intervention
WHO/UNICEF CCD Package confirms family involvement multiplies treatment outcomes across 54 low- and middle-income countries.
Research trail: PMC11506176 | PMC10955541 | PMC9978394 | WHO NCF 2018 | NCAEP 2020 | IOCDF Treatment Guidelines | DOI: 10.1007/s12098-018-2747-4

ACT II — THE KNOWLEDGE TRANSFER
The Technique: What It Is
Formal Name
Obsessive Thought Management — Cognitive Defusion & Externalization Protocol
Parent-Friendly Alias
"Freeing Your Child From Thought Loops"
Technique Code: C-294
Domain C — Emotional Regulation | Ages 5–14 | 10–20 min daily | Frequency: Daily
Definition
Obsessive thoughts are unwanted, intrusive, repetitive mental content that causes distress and is difficult to dismiss — even when the child knows the thoughts aren't true.
Unlike typical worries that respond to reassurance, obsessive thoughts intensify with attempts to suppress or debate them. They follow a cycle: trigger → intrusive thought → anxiety → compulsive ritual → brief relief → loop resets stronger.
This page introduces 9 materials proven to interrupt and weaken this cycle — by changing the child's relationship with thoughts rather than fighting them.

Who Uses These Techniques
"This technique crosses therapy boundaries — because the brain doesn't organize by therapy type."
BCBA / ABA Therapists — Primary Lead
Use ERP (Exposure and Response Prevention), functional analysis of compulsive behaviors, reinforcement of brave responses, and extinction of reassurance-seeking cycles.
Clinical Psychologists / Psychiatrists
Provide OCD diagnosis, CBT with ERP delivery, cognitive restructuring, and medication evaluation (SSRIs as first-line for moderate-severe presentations).
Occupational Therapists
Address sensory processing components that may amplify anxiety, sensory-based grounding techniques, and fine motor aspects of thought-tracking tools.
Speech-Language Pathologists
Work on metacognitive language ("I notice I'm thinking..."), verbal expression of emotional states, and pragmatic language components of social anxiety obsessions.
Special Educators
Support cognitive flexibility, executive function development, school-based accommodation plans, and classroom grounding strategies.
What These Materials Target
Precision targeting — not random activities. A precision system designed to address specific cognitive and behavioral mechanisms.
Target | Observable Behavior | |
Defusion | Child says "That's just OCD" rather than believing the thought | |
Compulsion Resistance | Washes hands once, not seven times | |
Distress Tolerance | Tolerates 2 minutes of uncertainty without reassurance | |
Externalization | Names thought character, talks back to it confidently |
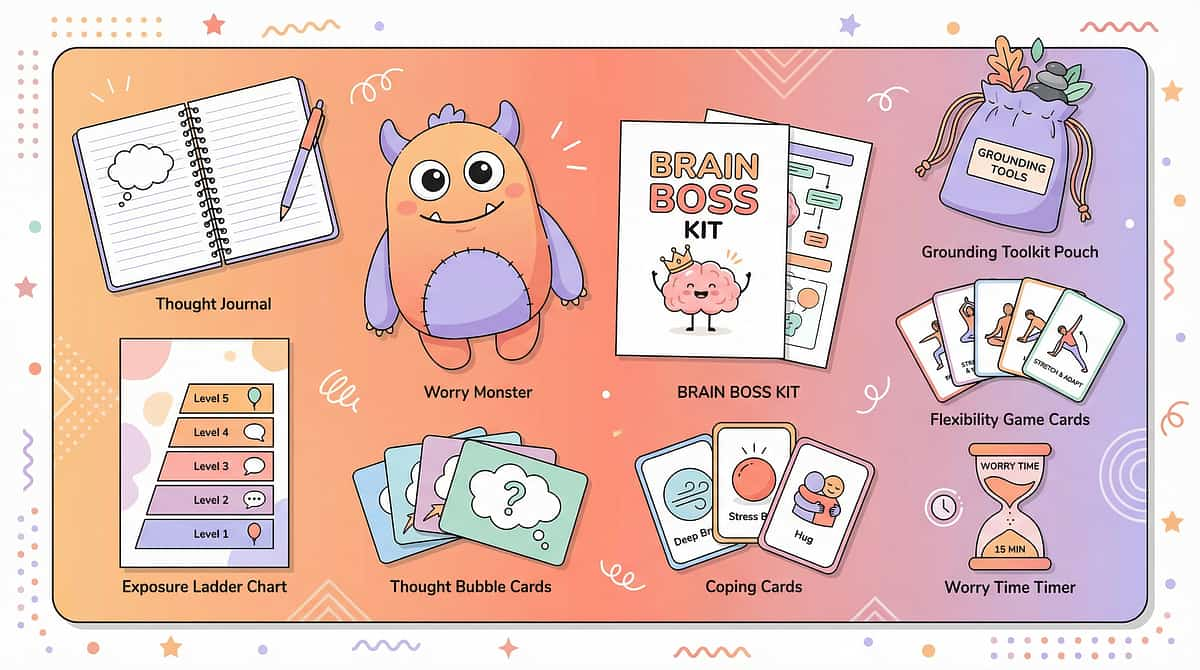
The 9 Primary Materials: What You Need
"9 materials. Each one a different key to the same lock." — Together, these tools address every dimension of the obsessive thought cycle, from externalization to exposure.
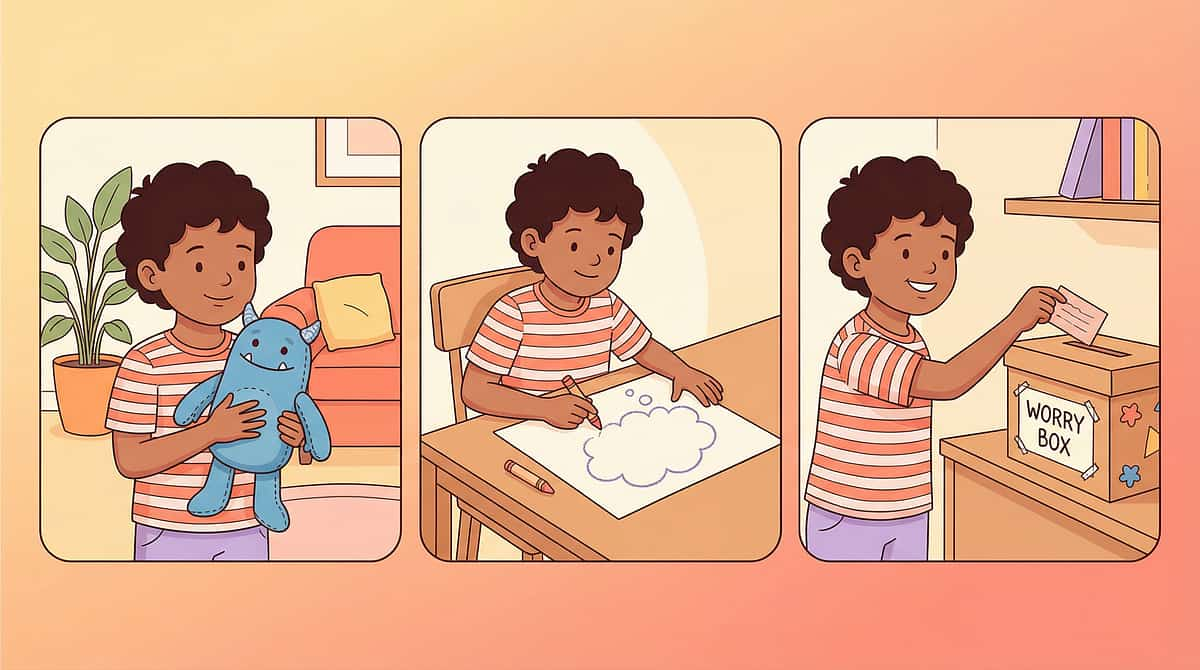
1. Worry Monster
Thought Container — give thoughts a physical home outside the mind
2. Thought Bubbles
Visual Templates — see thoughts as passing events, not facts
3. Brain Boss Kit
Character Externalization — name and boss around the obsessive pattern
4. Flexibility Games
Cognitive Training — build mental set-shifting through structured play
5. Grounding Toolkit
Mindfulness & Sensory — anchor attention to the present moment
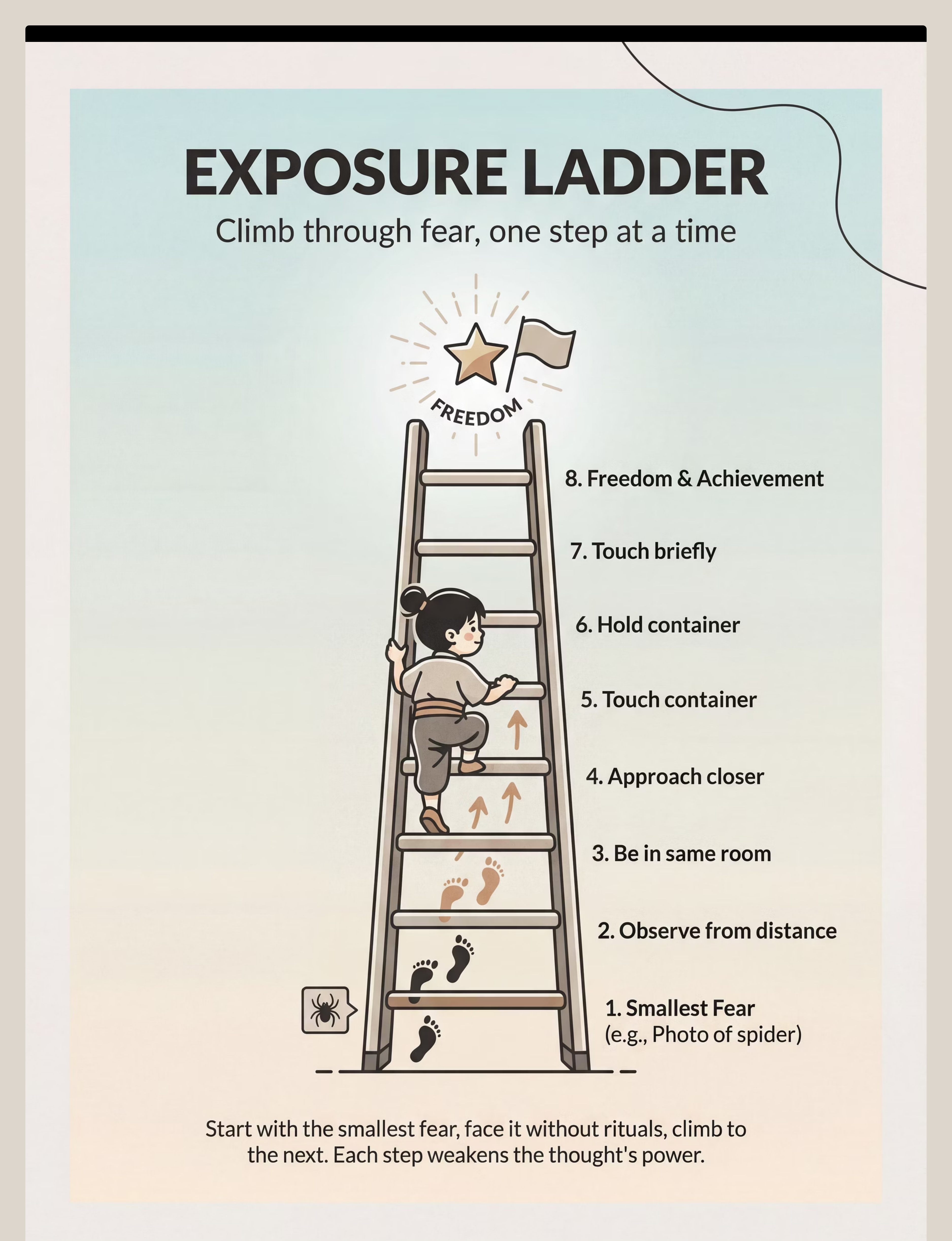
6. Exposure Ladder
ERP Hierarchy — graded exposure to feared thoughts without compulsions
7. Coping Cards
Talking Back Scripts — words to say when thoughts get loud
8. Thought Journal
Pattern Tracking — reveal predictability to reduce surprise-attack power
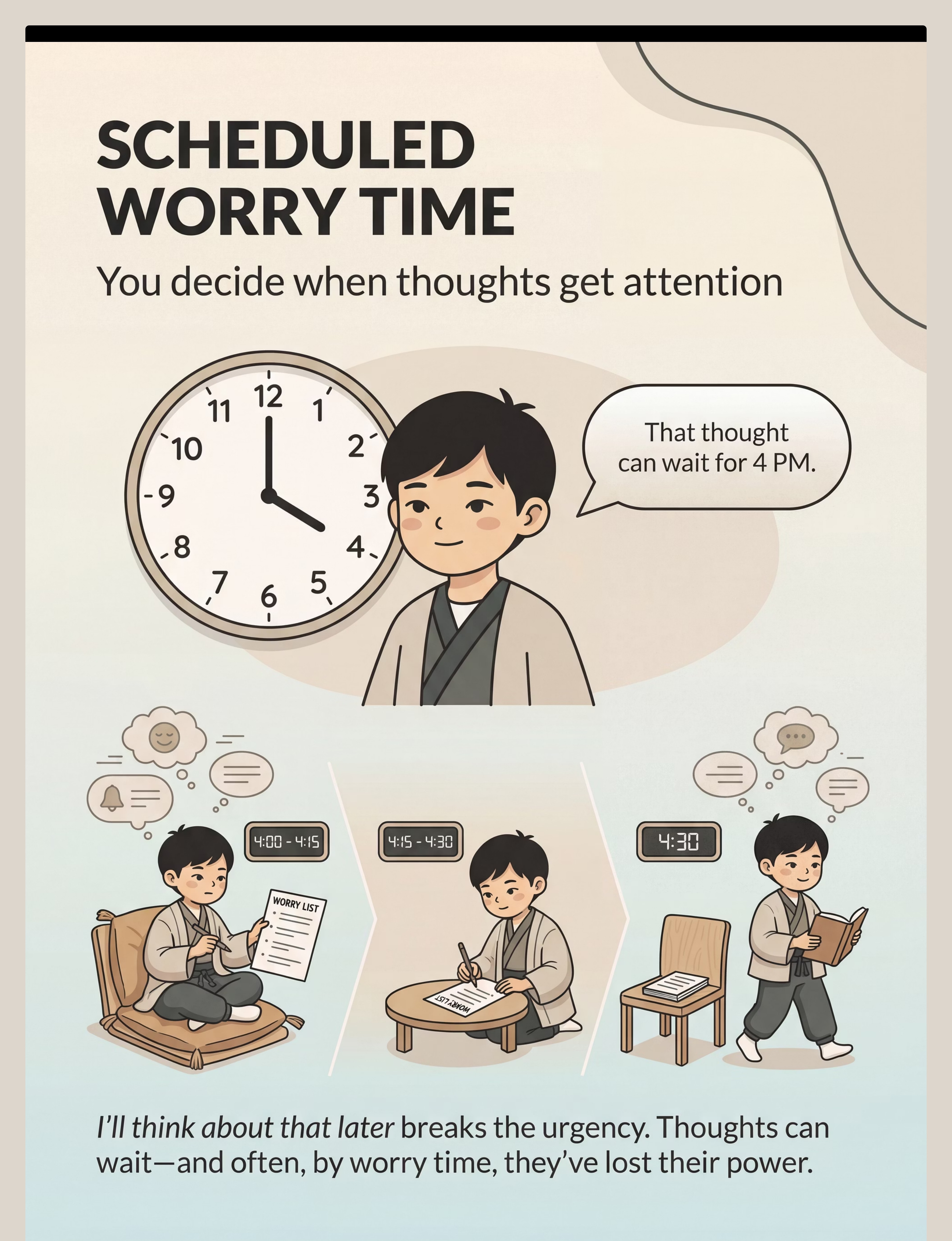
9. Worry Time Kit
Scheduled Containment — thoughts can wait for their appointed window
📞 9100 181 181 — FREE Pinnacle Helpline | Get a personalized materials recommendation call

Materials 1–3: Worry Monster, Thought Bubbles & Brain Boss Kit
Material 1 — Worry Monster / Thought Container
Canon Category: Transition Objects / Comfort Items
- Soft Toy Option: ₹425 | amazon.in/d/022Lj6Fr
- Reward Jar adaptation: ₹589 | amazon.in/d/02C5R9Jn
DIY: Any container + slot cut in lid. Write thought on paper, fold, deposit. The ritual IS the therapy.

Material 2 — Thought Bubble Visual Tools
Canon Category: Problem-Solving Toys / Visual Templates
- Activity Book: ₹199 | amazon.in/d/01KczBmp
- Memory/Visual Game: ₹519 | amazon.in/d/0iwJwOiH
DIY: Draw cloud shapes on paper. Write thought inside. Child physically pops, crumples, or watches "float away."

Material 3 — Brain Boss / Thought Character Kit
Canon Category: Problem-Solving Toys
- Flashcard system: ₹305 | amazon.in/d/07zQavEk
DIY: Blank paper + colored pens. Child draws their OCD character — silly, NOT scary. Name it. Talk to it. "Not now, Worry Brain."

Materials 4–6: Flexibility Games, Grounding Toolkit & Exposure Ladder

Material 4 — Cognitive Flexibility Games
Canon Category: Problem-Solving Toys | Matching Games
- Shut The Box Game: ₹428 | amazon.in/d/0flHweVf
- Memory Game: ₹519 | amazon.in/d/0iwJwOiH
- Rhyming Cards: ₹296 | amazon.in/d/00S726LE
DIY: Simon Says with changing rules. "What else could this be?" with any household object.

Material 5 — Mindfulness & Grounding Toolkit
Canon Category: Transition Objects / Sensory Grounding
- Spike fidget toy: ₹380 | amazon.in/d/01aefj5R
- Focus tracking tool: ₹579 | amazon.in/d/0fpuL3N3
DIY: 5-4-3-2-1 grounding kit from household items: textured fabric, scented item, sour candy, small object. No purchase needed.

Material 6 — Exposure Hierarchy Ladder
Canon Category: Visual Planning Tools
- Sticker rewards for rungs: ₹364 | amazon.in/d/01wrHJWX
DIY: Draw an 8-rung ladder on paper. Child names situations from least to most scary. Track progress up rungs. ₹0 cost.
Materials 7–9: Coping Cards, Thought Journal & Worry Time Kit

Material 7 — Talking Back Scripts / Coping Cards
Canon Category: Reinforcement Menus / Script Cards
- Reward sticker set: ₹364 | amazon.in/d/01wrHJWX
DIY: Write on index cards: "That's a thought, not a fact." / "I hear you, OCD, but I'm in charge." / "Maybe, maybe not — I don't need to solve this." Laminate and carry.

Material 8 — Thought Tracking Journal
Canon Category: Structured Documentation Tools
- Activity sticker book: ₹199 | amazon.in/d/01KczBmp
DIY: Any notebook. Columns: Date | Time | Thought (brief) | Intensity 1–10 | What I Did. Review weekly for patterns.

Material 9 — Scheduled Worry Time Kit
Canon Category: Visual Timer / Transition Objects
- Timer/ritual items: ₹589 | amazon.in/d/02C5R9Jn
DIY: Kitchen timer + cushion from home + any notepad = complete Worry Time setup. ₹0 required. The containment ritual teaches thoughts that they can wait.

Safety First: Before You Begin
"Know before you go. Safety is non-negotiable." Read every zone carefully before initiating any session.
🔴 RED — Do NOT Proceed
- Child has disclosed thoughts of self-harm OR harming others with intent
- Sudden onset of obsessive symptoms (possible PANDAS/PANS — requires medical evaluation)
- Child is in acute crisis or panic state
- Symptoms consuming 3+ hours daily with severe functional impairment
- Previous professional diagnosis of severe OCD with unsuccessful treatment
🟡 AMBER — Proceed With Caution
- Child is currently dysregulated, hungry, or recently had a meltdown → postpone to regulated state
- First attempt at any materials → start with Material 1 or 2 only
- Child with autism comorbidity → modify pace, use more concrete/visual approaches
- Younger child (5–7) → emphasize externalization (Materials 1 & 3), defer coping cards
🟢 GREEN — Proceed
- Child is calm, fed, and in a regulated state
- Thoughts are present but child can engage playfully with materials
- Parent has read this full page and understands the reassurance-avoidance principle
⚠️Critical Parent Alert: Providing reassurance (answering the same question repeatedly) is a compulsion that strengthens the obsessive cycle. Understanding this principle before beginning is essential. Reference: DOI: 10.1007/s12098-018-2747-4 | IOCDF Safety Protocols | 📞 9100 181 181 — FREE | If unsure which zone you're in, call Pinnacle

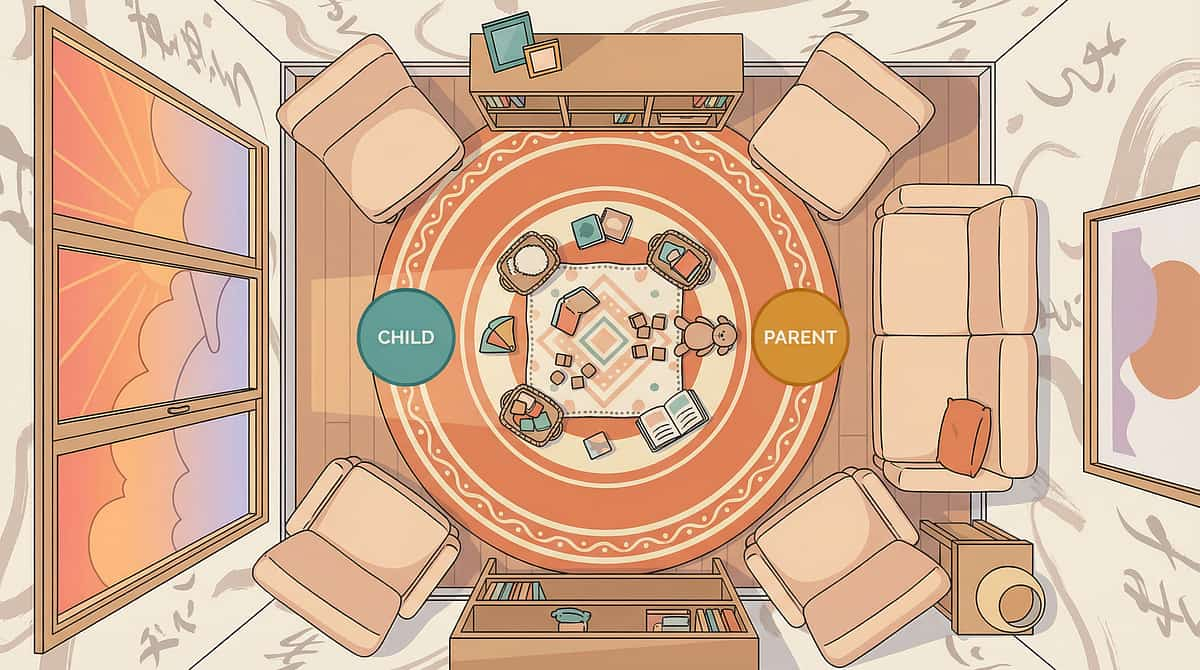
Set Up Your Space
"The space before the session. Spatial preparation prevents 80% of session failures." A well-prepared environment tells the child's nervous system: this is safe, predictable, and good.
Setup Checklist
- Quiet space — TV off, phone silent, siblings elsewhere for 15 min
- Soft, indirect lighting (avoid harsh overhead fluorescents)
- Room temperature comfortable
- All materials laid out before child enters (no setup disruption during session)
- Water and light snack available (blood sugar affects regulation)
- Visual timer visible to child (sets session boundary = reduces anxiety)
- Parent phone face-down (your full presence is the therapeutic container)
- Transition activity ready for after (normalizes ending without abruptness)
What to Remove
- Anything that could become a compulsion trigger during the session
- Other children's toys that may distract
- Reassurance-seeking items (specific objects the child uses to "check")
Room Layout
[Child Position] ← 1 arm's length → [Parent Position]
[Materials Table — all 9 materials laid out visually]
[Exit Route Clear — no blocked corners, no overwhelm]
Validated Setup Protocol — Pinnacle Blooms Consortium 🏆 | Reference: PMC10955541

ACT III — THE EXECUTION
Is Your Child Ready? The 60-Second Readiness Check
"The best session is one that starts right." Run through this check before every session — without exception.
Check | ✅ YES → Continue | NO → Action | |
Fed and hydrated in last 2 hours? | Continue | 🟡 Feed first, wait 20 min | |
Slept adequately last night? | Continue | 🟡 Shorten session, reduce intensity | |
No acute meltdown in last 30 min? | Continue | 🔴 Postpone 60 min minimum | |
Able to make eye contact and respond? | Continue | 🟡 Start with grounding only (Material 5) | |
Not currently in active thought loop? | Continue | 🟡 Use Worry Time container first | |
Child knows what's happening today? | Continue | 🟡 Give 5-min advance notice | |
Parent regulated and calm? | Continue | 🔴 You cannot co-regulate from dysregulation |
✅ All Green
Proceed to Step 1: The Invitation
🟡 1–2 Amber
Modify: start with grounding only (Material 5)
🔴 Any Red
Postpone: reschedule for tomorrow. Skipping a session is data, not failure.
Time: 1–2 minutes
Step 1 of 6 — The Invitation
"Never start with the thought. Always start with the relationship."
"Hey, I've got something I want to show you. It's kind of like a game, kind of like a superpower training. There's no right or wrong — we're just practicing together. And you're totally in charge. Want to see?"
For Younger Children (5–8)
Lead with the physical material. "Look what I found — it's a Worry Monster. Want to know what it eats?" The curiosity pulls them in without any sense of threat.
For Older Children (9–14)
Lead with the science. "I want to show you something actually interesting about how brains work. Including yours. You ready?" Adolescents respond to being treated as intelligent, not managed.
The Principle: Obsessive thoughts have already made the child's world feel threatening. This session must feel safe, playful, and completely optional. Coercion activates the threat system — the opposite of what we need. Reference: ABA antecedent modification principles | PMC11506176
Time: 1–2 minutes
Step 2 of 6 — Establishing Engagement
"Wait for the moment the child leans in. That's your green light."
Engagement Indicators — Look for 2 of These:
Child makes eye contact with the material
Child asks a question about it
Child reaches toward it or picks it up
Child offers information: "I know what that is" or "We do that at school"
Child smiles or shows relaxed body language
If Engagement Is Absent: Try: "Should we start with the game or the monster?" Giving choice creates investment. If still absent: close the materials, do grounding only (5-4-3-2-1, 3 minutes), and try again tomorrow. What You're Building: The child's nervous system needs to learn that the therapy space = safe, predictable, good. The first 10 sessions are about the nervous system, not the technique.
Time: 5–8 minutes
Step 3 of 6 — The Therapeutic Action
"This is the active ingredient. The moment thought becomes object."
With Worry Monster / Container
- Parent narrates: "When you have a thought that won't stop, we're going to give it a home outside your head."
- Child writes or draws the thought on a small slip of paper (non-writers: child speaks, parent writes)
- Child folds the paper
- Child physically deposits it into the container
- Parent says: "It's in there. It's not gone — it's just not inside you anymore. And you're still okay."
- Observe. Don't rush to reassure. Let the moment land.
With Thought Bubbles
- Draw a large thought bubble on paper or whiteboard
- Child writes or dictates the obsessive thought inside
- Child chooses: pop it (tap with finger), let it float away (draw an arrow up), or crumple the paper
- Parent: "That thought happened. And then it went. You're still here, and you're fine."
⚠️ Do NOT say "See? The thought isn't true." This debates the content. The goal is changing the relationship — not winning an argument with the thought. Reference: PMC10955541 | ACT defusion framework
Step 4 of 6 — Repeat & Vary
Target: 3–5 Repetitions
"3 good repetitions are worth more than 10 forced ones."
1
Repetition Targets
3–5 meaningful repetitions per session. Engaged and energized child: up to 7. Signs of satiation (sighing, looking away, body tension): stop immediately — not one more.
2
Variation Options
Swap materials session-to-session. Change thought content (vary to generalize skill). Change physical position (sitting → standing → walking). Add Coping Card (Material 7) as verbal response after depositing.
3
Evidence-Based Dosage
2–3 sessions/week for 8–12 weeks for ERP/defusion. Daily grounding and coping card practice is appropriate. Exposure Ladder: 4–5 times/week once established.
Satiation Indicators: Child is done when flat affect, repeated glancing away, requests to stop, increased body tension, or complete disengagement. Respect these signals immediately. Reference: PMC11506176

Step 5 of 6 — Reinforce & Celebrate
Timing: Within 3 seconds of desired behavior
"Celebrate the attempt, not just the success. Bravery deserves recognition."
Verbal Reinforcement Scripts
- "You just put that thought outside your head. That's real skill."
- "I saw you use your coping card instead of asking me again. That's huge."
- "You didn't check this time. OCD wanted you to, and you didn't. You're the boss."
- "That thought tried to trick you. You didn't let it."
Reinforcement Menu
- 🏆 Reward Jar: ₹589 | amazon.in/d/02C5R9Jn
- 🌟 Reward Sticker Chart: ₹364 | amazon.in/d/01wrHJWX
- Or: 5 extra minutes of screen time, special snack, parent-child game — child chooses from pre-agreed menu
Token Economy
For sustained motivation across weeks: each brave response = 1 token. 10 tokens = agreed reward. This visual chart tracks the weeks-long journey and keeps motivation alive through the hard middle weeks.

Step 6 of 6 — The Cool-Down
Duration: 2–3 minutes
"No session ends abruptly. The transition IS part of the therapy."
2-Minute Warning
"We have two more, and then we're done for today." Predictable endings reduce anxiety about stopping.
Completion Acknowledgment
"We're finished. Good work today." Simple, clear, affirming — no elaboration needed.
Material Ritual
Child helps put materials away. This creates ownership, closure, and respect for the therapeutic boundary.
Grounding Breath
1 round of box breathing together: inhale 4 counts, hold 4, exhale 4, hold 4. Shared regulation signals safety.
Transition Activity Cue
"Let's go do [normal activity]." Name the next thing — this signals a safe, clean exit from the therapeutic space.
⚠️ If child resists ending — don't negotiate. Gently: "We're done for today. The monster will hold the thoughts until tomorrow." Extending sessions when the child protests creates a compulsion pattern around the session itself. 📞 9100 181 181 — FREE | If cool-down regularly fails, call Pinnacle
What If It Didn't Go as Planned?
"Session abandonment is not failure — it's data. Every outcome tells you something useful about your child's nervous system."
"She kept asking for reassurance instead of using the material."
This is exactly the compulsion we're replacing. Don't answer. Say: "That sounds like OCD talking. What can you do instead of asking me?" If she can't, offer the Worry Monster. Expect this pattern for weeks.
"He refused to engage at all — just shut down."
Likely threat-system activation. Today's session is grounding only. Return to the invitation stage (Card 14) next session. Don't push through shutdown — it creates negative associations that set progress back.
"She got more anxious when she tried to externalize."
This is normal initially — externalizing creates awareness before relief. Reduce session duration. Stay in the room. Use grounding (Material 5) immediately after. This phase passes with consistency.
"He 'fed the monster' and immediately asked if the thought was still there."
The checking is the compulsion. Parent script: "The thought is in the container. You don't need to check on it." Do not open the container. Trust the ritual.
"Nothing seems to be working after 3 weeks."
Call 9100 181 181 immediately. Three weeks without measurable progress signals need for professional ERP guidance. This is not a failure — it is exactly when the escalation pathway exists to serve you.
Adapt & Personalize: No Two Children Are Identical
"The technique adapts — you don't force the child to adapt to it." Use the difficulty slider and profile variations to tailor every session.
⬅️ Easier (Bad Days, Early Weeks)
- Use only Material 1 (Worry Monster) — lowest cognitive demand
- Parent does more of the verbal work
- Shorter sessions (7–10 min)
- More reinforcement, lower expectations
➡️ Harder (Good Days, Weeks 6–12)
- Combine Materials 6 + 7 (Exposure + Coping Cards)
- Child takes lead on all steps
- Introduce Worry Time structure (Material 9)
- Reduce reinforcement frequency (shift to variable ratio)
🧩 Autistic Child
- Emphasize visual, concrete materials over verbal scripts
- Avoid metaphors that may be taken literally
- Maintain absolute session structure predictability
- Allow special interest integration (Brain Boss can be their favorite character)
- Slow ERP pace significantly
🧒 Ages 5–7
- Stay in Materials 1 and 3 — purely play-based
- Parent does ALL scripting initially
- Session = 7–10 minutes maximum
👦 Ages 11–14
- Lead with cognitive framework
- Self-designed coping cards (no scripts)
- Digital thought journal (app-based)

ACT IV — THE PROGRESS ARC
Weeks 1–2: What to Expect
Progress: 15% — Foundation Being Built
"Progress in weeks 1–2 is not mastery. It's the first signal that change is possible."
✅ Observable Indicators
- Child engages with at least one material without refusing
- Child tolerates the ritual even if distressed during it
- Parent successfully deflects reassurance-seeking at least once
- Session duration reaches 10 minutes without abandonment
- Child names the thought character OR acknowledges "that's OCD"
What Is NOT Progress Yet (and That's Okay)
- Reduction in frequency or intensity of thoughts — too early for this
- Child spontaneously using coping skills independently
- School improvement or teacher feedback
Parent Emotional Calibration
The hardest moment is weeks 1–2. You're stopping reassurance. Your child is more anxious before they're less anxious. This is correct and expected. You are not making it worse — you are stopping the cycle that was making it worse.

Weeks 3–4: Consolidation Signs
Progress: 40% — Consolidation Underway
"Week 3–4: The brain is rewiring. Watch for these signals."
Child reaches for the Worry Monster spontaneously (without prompting)
Reduction in reassurance requests — even a 10% decrease is real, measurable progress
Child uses the character name unprompted: "Worry Brain is being loud today"
Session intensity decreasing — same material, noticeably less child anxiety during it
First moment of "I know it's just OCD" with some genuine emotional distance from the thought
Neural Pathway Forming — What the Child May Do
- Apply skills to new thought themes (generalization emerging)
- Show less anticipatory anxiety before sessions
- Reference the tools in conversation outside sessions
- Sleep slightly better on nights following sessions
Parent Milestone
You may notice your own anxiety about the sessions is reducing. Your confidence in the protocol is data too — it signals the child is sensing your certainty and calm.

Weeks 5–8: Deepening Mastery
Progress: 70% — Mastery Pathway Emerging
"The 5–8 week window: From managed to mastered."
✅ Mastery Indicators
- Child identifies the thought as OCD/Worry Brain before asking for reassurance
- Uses 2+ materials independently in at least some situations
- Exposure Ladder (Material 6) shows 3+ rungs climbed
- Scheduled Worry Time (Material 9) functioning — containment working outside sessions
- School functioning stabilizing — homework, attendance, peer interaction improving
What Continues to Fluctuate
Setbacks at transitions — new school year, illness, family stress. These are not regressions. They are normal reactivations. Use the materials, not reassurance. Skills resurface faster than they were built.
Introduce Now (If Not Already)
- Cognitive Flexibility Games (Material 4) as daily 10-minute practice
- Thought Tracking Journal (Material 8) — 2-week pattern analysis
- Parent reading: IOCDF Family Guide

Celebrate Every Rung
"These are the moments that matter. Document them." Celebration is not a reward — it is the mechanism by which self-efficacy is built.
First Spontaneous Use
First time child uses a material without prompting from a parent or therapist
First Caught Thought
First time child catches the thought before the compulsion fires — the most critical early milestone
First Good Night
First night of adequate sleep in weeks — a profound sign that anxiety load is genuinely reducing
First Full School Day
First school day where thoughts didn't prevent full participation in learning and social interaction
First Independent Coping Card
First use of coping card independently in a real trigger situation — outside of session, in real life
How to Celebrate: Not with big parties — with specific, named recognition. "You caught Worry Brain before it tricked you. That took real courage." Specificity is the proof that you're paying attention. Every recognized brave moment builds the belief: "I can handle thoughts."📞 9100 181 181 — Share your milestones with our team. We celebrate with you.
Red Flags: When to Escalate
"Progress isn't always linear. Know when home practice needs professional support." These thresholds are clearly defined — use them without hesitation.
🔴 Escalate Immediately
- Thoughts about self-harm (any content, any frequency)
- Sudden dramatic increase in OCD symptoms (possible PANDAS/PANS)
- Child unable to attend school for 3+ consecutive days due to thoughts
- Family accommodation has increased despite this program
🟡 Consult Within 2 Weeks
- No measurable progress after 4 weeks of consistent practice
- Thoughts expanding to new domains faster than skills are developing
- Child's distress increasing rather than decreasing week-over-week
- Parent emotional exhaustion — inability to maintain protocol sustainably
🟢 Normal — Continue
- Single-day regressions after stressful events
- Fluctuating progress week-to-week (non-linear is normal and expected)
- Child resistance on some days
- Slow progress in weeks 1–4 — this often feels flat before the uplift
📞 FREE Escalation Pathway: 9100 181 181 | AbilityScore® Assessment → ERP Therapist → FusionModule™ Plan
Your Progression Pathway
"This technique is one waypoint. Here's the complete journey." Understanding where C-294 sits in the larger therapeutic map helps families and therapists plan intelligently.
Prerequisites
C-292: Understanding Anxiety in Children
C-293: Recognizing OCD Patterns
← You Are Here
C-294: Obsessive Thoughts — Materials & First Tools
Next Level Options
C-295: Compulsive Behaviors — ERP Deep Dive
C-296: Physical Anxiety Symptoms
C-299: Worry Management
Long-Term Trajectory
Anxiety tolerance → Cognitive flexibility → Adaptive daily functioning → Full life participation
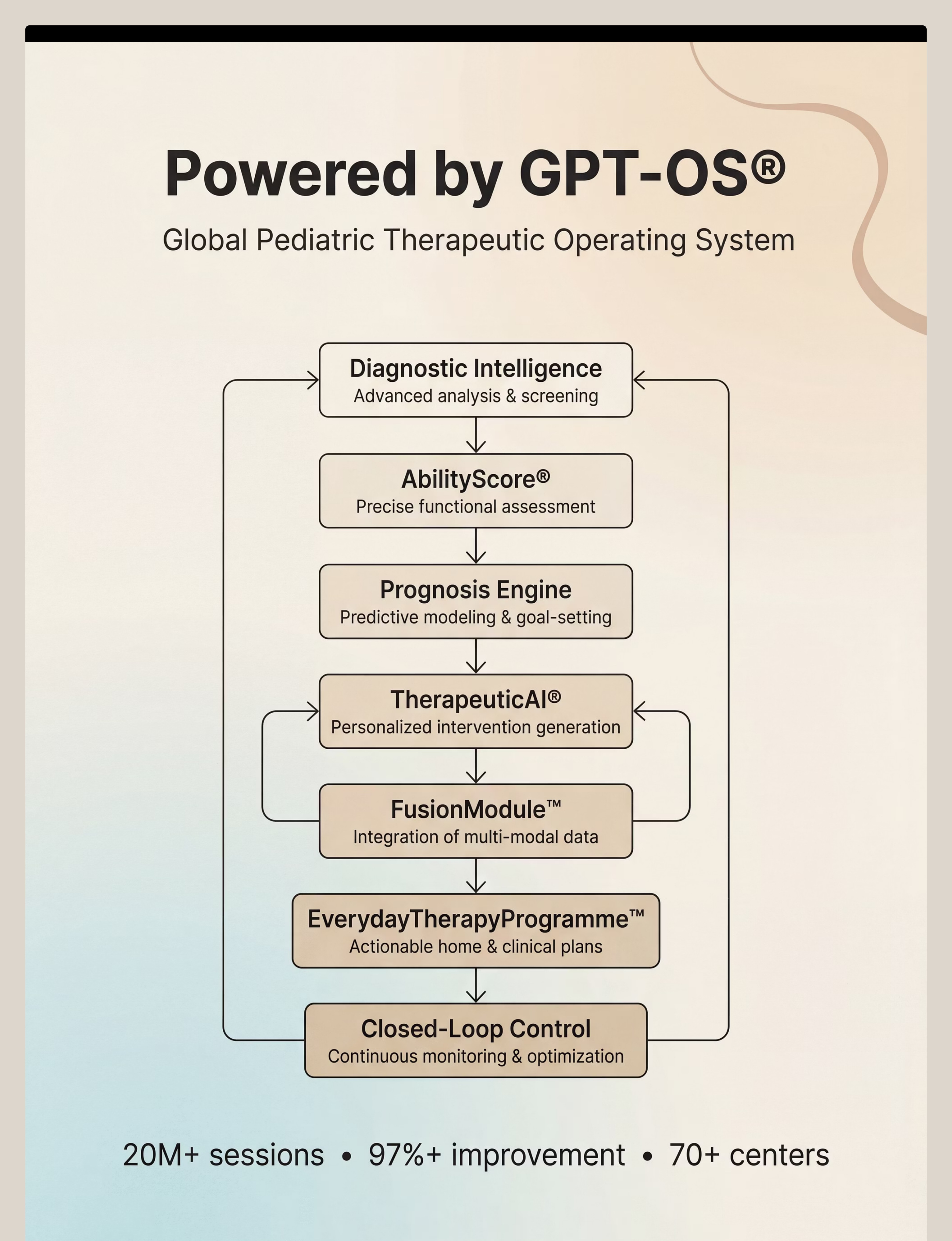
GPT-OS® AbilityScore® tracks your child's position on this trajectory and recommends the precise next technique at the precise right moment. Log sessions → TherapeuticAI® delivers the next intervention to your home → FusionModule™ coordinates across all your therapists.
Related Techniques in This Domain
"More tools in the Anxiety & OCD Spectrum cluster." These techniques share materials and build cumulatively — starting one makes the others easier.
Technique | Domain | Level | Materials Overlap | |
C-292: Understanding Anxiety | Emotional Reg | Intro | Most materials overlap | |
C-293: Recognizing OCD Patterns | Emotional Reg | Intro | Yes — full overlap | |
C-294: Obsessive Thoughts ← YOU | Emotional Reg | Core | — | |
C-295: Compulsive Behaviors | Behavioral | Core | Exposure Ladder carries over | |
C-296: Physical Anxiety Symptoms | Sensory/Reg | Core | Grounding Kit carries over | |
C-298: Building Brave Behaviors | Behavioral | Advanced | Full exposure system carries over |
Browse the full domain: techniques.pinnacleblooms.org/emotional-regulation
Your Child's Full Developmental Map
"Obsessive thought management is one domain. Here's the full picture." GPT-OS® AbilityScore® maps performance across all 12 developmental domains simultaneously.
Domain C — Active Now
This technique advances the C-domain sub-index: Cognitive Flexibility Readiness + Anxiety Management Readiness. Every session logged updates your child's AbilityScore® in real time.
GPT-OS® Integration
Log sessions → TherapeuticAI® identifies which domain to address next → EverydayTherapyProgramme™ delivers the next intervention to your home → FusionModule™ coordinates across all your therapists seamlessly.
📞 9100 181 181 — FREE AbilityScore® consultation
pinnacleblooms.org/ability-score-assessment
pinnacleblooms.org/ability-score-assessment
ACT V — THE COMMUNITY & ECOSYSTEM
Stories From Families Who Have Walked This
"Six months ago, my daughter couldn't leave the house without checking the door lock twelve times. She couldn't eat without me 'guaranteeing' the food was safe. Now she catches herself in the loop. She says, 'That's just OCD being loud' and moves on. She still has the thoughts sometimes, but they don't control her anymore. She named her OCD 'The Worry Gremlin' and she bosses it around. She's not trapped anymore. She's living."— Parent, Pinnacle Network, South India (Illustrative case; outcomes vary by child profile)
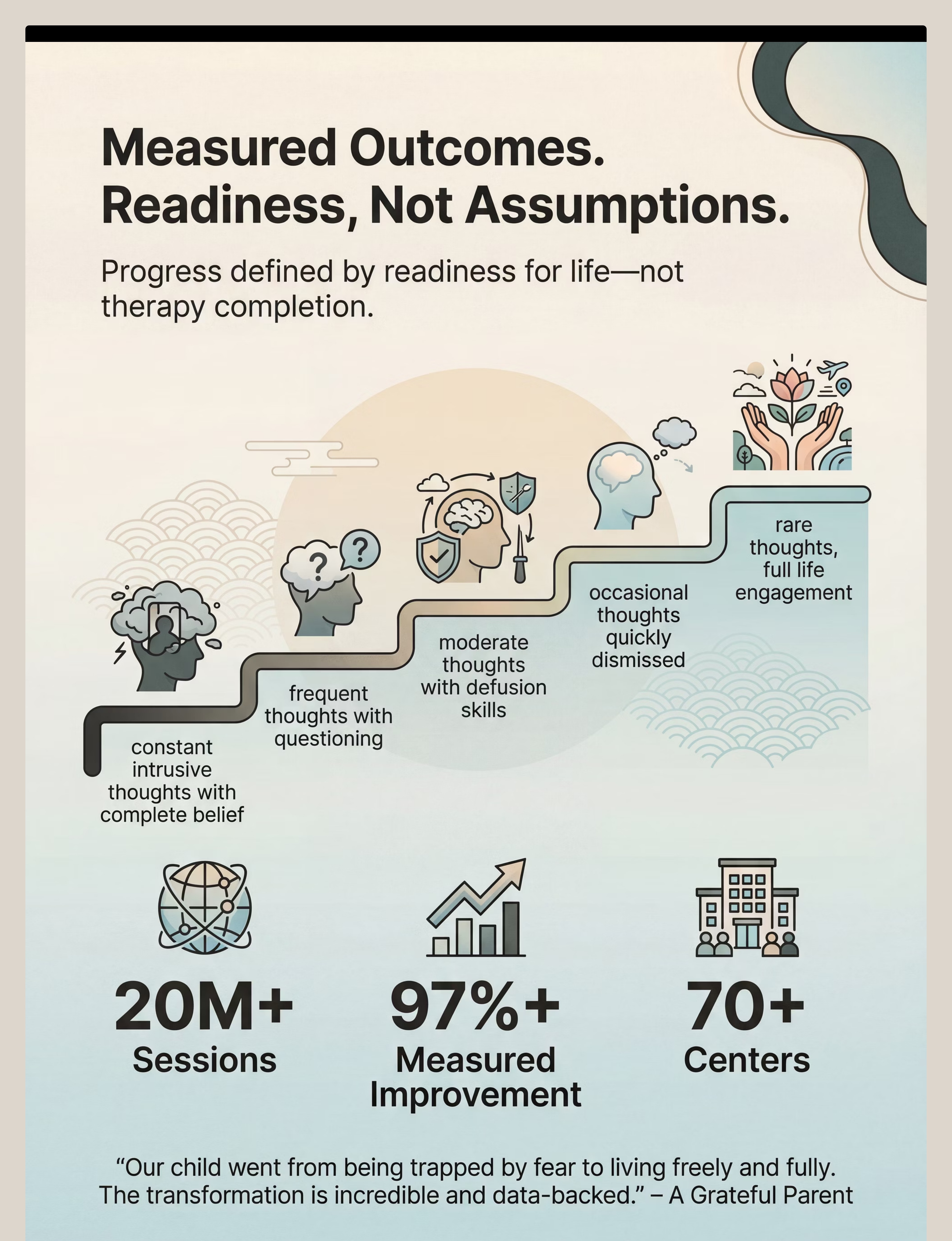
Constant Intrusive Thoughts
Complete belief in thought content, full behavioral control by thoughts
Frequent Thoughts, Questioning
First moments of "is this real?" emerging
Moderate Thoughts With Defusion
Child beginning to name and talk back to thoughts
Occasional Thoughts
Quickly dismissed using learned skills independently
Rare Thoughts, Full Life
Cognitive Flexibility Index: 23 → 71 over 24 weeks
Connect With the Pinnacle Community
"You should not navigate this alone. A community of 70,000+ families has walked this." Every family's experience becomes a resource for the next family facing the same challenge.
Pinnacle Parent Community
pinnacleblooms.org/community — Connect with families navigating the same journey, share strategies, and celebrate milestones together.
WhatsApp Support Groups
Regional, language-specific parent support groups. One parent's "Worry Gremlin" name has helped 50 children through community sharing alone.
Pinnacle Parent Academy
Online courses for OCD support skills. Free Resources Library: pinnacleblooms.org/resources
International Families
IOCDF: iocdf.org | WHO Mental Health: who.int/mental_health | Pinnacle serves 70+ countries through OTT platform and teleconsultation in 16+ languages.
📞 9100 181 181 — FREE | Ask about parent support groups in your language
When to Seek Professional Support
"Home practice is powerful. Professional guidance is essential for moderate-severe presentations." Know this threshold clearly — it protects your child.
Referral Criteria — Seek Evaluation If:
- Thoughts consume 1+ hour daily
- Child cannot attend school regularly
- Family accommodation patterns are entrenched
- Child has disclosed harm thoughts (distinguish from OCD harm obsessions)
- 4+ weeks of home practice without measurable progress
Pinnacle Specialist Pathway
- FREE AbilityScore® Assessment — call 9100 181 181
- OCD/Anxiety evaluation by Pinnacle psychologist
- ERP therapy with trained Pinnacle BCBA/psychologist
- FusionModule™ — coordinated OT + behavioral + family support
- EverydayTherapyProgramme™ — home extension of clinic sessions
Center Locator: pinnacleblooms.org/find-center — 70+ locations across India
International Teleconsultation: 16+ languages | care@pinnacleblooms.org
Reference: IOCDF Treatment Guidelines | NCAEP 2020 | DOI: 10.1007/s12098-018-2747-4
The Research Library
"For the parent who wants to go deeper. The evidence is real and accessible." Every technique in the Pinnacle network is grounded in peer-reviewed research.
PMC11506176 — PRISMA Systematic Review (2024)
Sensory integration and therapeutic intervention evidence base for ASD. pubmed.ncbi.nlm.nih.gov/PMC11506176
PMC10955541 — Meta-Analysis (2024)
World J Clin Cases: Sensory integration therapy — social skills and adaptive behavior outcomes. pubmed.ncbi.nlm.nih.gov/PMC10955541
DOI: 10.1007/s12098-018-2747-4
Padmanabha et al., Indian J Pediatr (2019): Home-based pediatric intervention RCT — significant outcomes confirmed.
NCAEP 2020 + WHO NCF 2018
ERP, cognitive defusion, and visual supports confirmed as evidence-based practices. WHO Nurturing Care Framework: family involvement multiplies outcomes. PMC9978394
Pinnacle Clinical Data: 20M+ sessions | 97%+ measured improvement | pinnacleblooms.org/research

How GPT-OS® Uses Your Data
"Your session data makes this technique smarter for your child — and for every child like yours." The system learns from every session logged across the network.
What GPT-OS® Learns From C-294 Data
- Which material sequence produces fastest defusion learning
- Which thought themes respond fastest to which approaches
- Optimal session duration for different age groups
- Parent protocol fidelity patterns — and where to provide coaching
Privacy Assurance
All data governed under ISO/IEC 27001 Information Security standards. No individual data shared externally. Aggregate anonymized data only in population-level analysis.
Sovereign Positioning
GPT-OS® is India's largest pediatric therapeutic data operating system — purpose-built, clinically governed, and protected by patents filed across 160+ countries.
The 9 Materials — Visual Recap & Video
"See the materials in action." Reel C-294 | Series: Emotional Regulation & Behavioral Support — Episode 294 | Duration: 75–85 seconds | pinnacleblooms.org/reels/C-294
Worry Monster
Give thoughts a physical home outside your head — the ritual IS the therapy
Thought Bubbles
Thoughts are not facts — watch them float, pop, and pass
Brain Boss
Name the bully in your brain — then boss it around
Flexibility Games
Practice shifting your thinking — flexibility is a trainable skill
Grounding Toolkit
Come back to right now — sensory anchoring interrupts the loop
Exposure Ladder
Climb through fear one step at a time — courage builds with each rung
Talking Back Scripts
Words to say when thoughts get loud — scripted bravery becomes real bravery
Thought Tracker
Find the pattern, break the loop — predictability defuses the power of surprise attacks
Scheduled Worry Time
You decide when thoughts get attention — containment teaches thoughts that they can wait
Research confirms video modeling as an evidence-based practice for autism (NCAEP 2020). Watching the Reel before the first session increases parent confidence and child engagement rates significantly. ← C-293: Recognizing OCD Patterns | → C-295: Compulsive Behaviors

ACT VI — THE CLOSE & LOOP
Frequently Asked Questions
"Every question a parent has asked. Answered by the Pinnacle Consortium."
"My child has autism AND obsessive thoughts. Is this safe?"
Yes, with modifications. Autism and OCD co-occur at significantly elevated rates. Use more concrete, visual materials. Slow the ERP pace. Distinguish autism routines (calming, ego-syntonic) from OCD rituals (distressing, ego-dystonic). Call 9100 181 181 for autism-OCD specific guidance.
"How do I stop answering reassurance questions without feeling cruel?"
Agreed script: "I've already answered that, and I know you can handle the uncertainty." This is not cruelty — it is the most loving response. The reassurance you're withholding was fueling the loop. The discomfort is the treatment.
"What if the thoughts are about harming others?"
OCD harm obsessions involve fear of harming — the child is horrified by the thought and does not want to act on it. This is fundamentally different from genuine intent. If any doubt: call 9100 181 181 immediately for clinical triage.
"My child started these suddenly — overnight. Is that OCD?"
Sudden-onset OCD may indicate PANDAS/PANS (infection-triggered). Medical evaluation is essential. Do not start ERP without medical clearance first.
"How long until I see real progress?"
Earliest visible signs: 2–3 weeks. Meaningful functional improvement: 6–12 weeks of consistent practice. Full OCD treatment cycles: typically 12–20 weeks. Early intervention changes outcomes dramatically.
"Can I do this if I haven't done therapy before?"
Materials 1–5 are suitable for informed parent-led practice. Materials 6 and beyond should be guided by a professional for best results. Start here. Build confidence. Escalate if needed.
"Didn't find your answer?"
Ask GPT-OS®: pinnacleblooms.org/ask | Book a teleconsultation: 9100 181 181

Your Next Step: Start Now
"You have read everything. You have the tools. Your child is waiting for freedom."
🟢 Start This Technique Today
Open GPT-OS® EverydayTherapyProgramme™ → C-294 session launcher
pinnacleblooms.org/start/C-294
📞 Book a FREE Consultation
National Helpline: 9100 181 181
24×7 | 16+ Languages | AbilityScore® Assessment | 70+ centers across India
→ Next Technique: C-295
9 Materials That Help With Compulsive Behaviors
techniques.pinnacleblooms.org/emotional-regulation/compulsive-behaviors-c-295
Validated by: OT • BCBA/ABA • SLP • SpEd • NeuroDevelopmental Pediatrics • Mothers & Families | Pinnacle Blooms Consortium — 20M+ sessions | 97%+ improvement | 70+ centers | "From fear to mastery. One technique at a time."
Preview of 9 materials that help with obsessive thoughts Therapy Material
Below is a visual preview of 9 materials that help with obsessive thoughts therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
The Pinnacle Promise
"From fear to mastery. One technique at a time."— Pinnacle Blooms Consortium
Pinnacle Blooms Network®
India's largest autism therapy chain. Built by Mothers. Engineered as a System.
70+ Centers | 70+ Countries Served | 20M+ 1:1 Sessions | 97%+ Measured Improvement
Consortium: OT • SLP • BCBA/ABA • SpEd • NeuroDevelopmental Pediatrics • Clinical Psychologists • Mothers • Fathers • Families • WHO/UNICEF-aligned
📞 FREE National Helpline: 9100 181 181
🌐 pinnacleblooms.org | techniques.pinnacleblooms.org
✉️ care@pinnacleblooms.org
🌐 pinnacleblooms.org | techniques.pinnacleblooms.org
✉️ care@pinnacleblooms.org
⚠️ Medical Disclaimer
This content is educational. It does not replace individualized assessment and treatment by licensed mental health professionals including psychologists, psychiatrists, and specialized therapists. Obsessive thoughts can be symptoms of various conditions requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Always seek professional guidance for moderate-severe presentations.
Navigation
← Return to Card 01 | → Next: C-295 — Compulsive Behaviors
Browse all Domain C: techniques.pinnacleblooms.org/emotional-regulation
© 2025 Pinnacle Blooms Network® | A unit of Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2