"Hand flapping isn't the problem. It's your child's nervous system asking for something it needs."
It's the moment at the dinner table when the food arrives and their hands flutter up beside their ears — rapid, rhythmic, unstoppable. At the playground, the other children stare. You reach over gently and press their hands down, and they look at you like you've just interrupted the most important thing in the world. Because for their nervous system, you have.
You are not failing. You are not missing something obvious. Your child's body is doing exactly what it was built to do — seeking the input it needs to feel organized and safe.
🧠 Domain
Sensory & Self-Regulation | D-362
👶 Age Band
2–12 Years
🏠 Setting
Home + School + Community
⏱️ Episode
362 of 999
9 Materials That Help With Hand Flapping — Understand the need. Expand the options. Transform regulation.
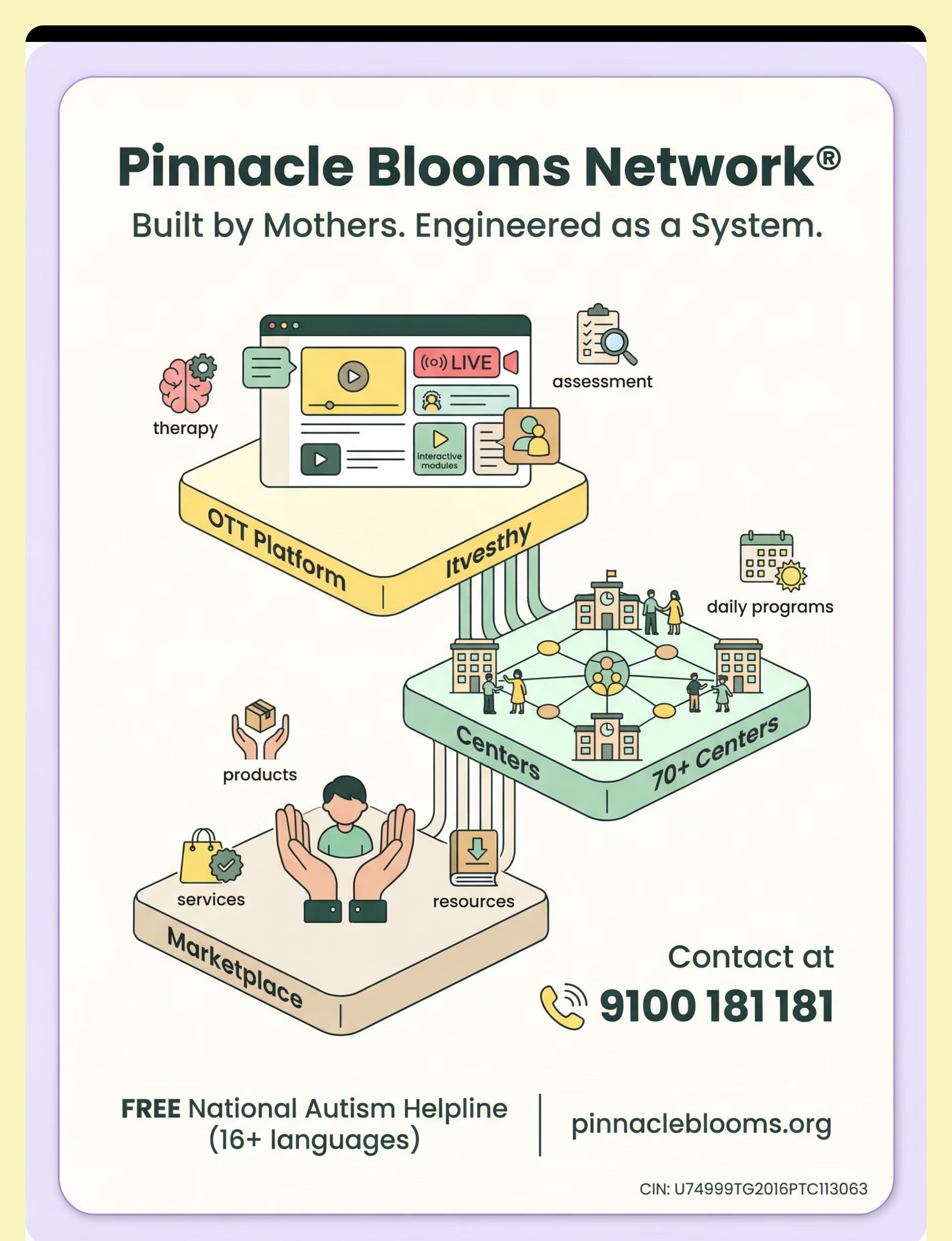
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. OT • SLP • ABA • SpEd • NeuroDev • CRO
📞FREE Helpline: 9100 181 181 | 16+ Languages | 24×7

You Are Among Millions of Families Navigating This Exact Challenge
The numbers behind hand flapping are staggering — and they tell a story of a need that is universal, well-documented, and clinically addressable. You are not an outlier. You are part of a global community of families navigating the same terrain.
60–90%
Motor Stereotypy Prevalence
of children diagnosed with autism display motor stereotypies including hand flapping (Peer-reviewed systematic review literature)
80%
Sensory Processing Differences
of children with ASD show sensory processing difficulties that drive seeking behaviors (PRISMA systematic review, 2024 — PMC11506176)
21M+
Global Children with ASD
children globally living with autism spectrum disorder (WHO Global Autism Prevalence Data)
In India alone, approximately 18 million families are navigating autism-related challenges. Hand flapping is among the most universally reported and misunderstood behaviors in pediatric neurodevelopmental therapy.
"The first time my daughter's teacher called to mention the flapping, I cried in the parking lot. I thought I was the only one. I wasn't. Not even close." — Parent, Pinnacle Network
PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO Global ASD Data (2023)
This Is a Wiring Difference. Not a Behavior Problem.
What Proprioception Actually Is
Proprioception is your body's internal GPS — the system that tells your brain where your body is in space, what pressure your joints feel, and how hard your muscles are working. It's the sixth sense we rarely name but use every moment.
Why Hand Flapping Delivers It
Rapid bilateral hand movement generates intense proprioceptive feedback to the wrist, elbow, and shoulder joints. For a nervous system that processes proprioceptive input differently, this movement is not random — it is precision medicine that the body is administering to itself.
What "Different Wiring" Means
Many children with autism have proprioceptive systems that require more input, different input, or have difficulty modulating what they receive. The flapping isn't excessive — the sensory threshold is higher. The child is not overreacting. The child is calibrating.
When the sensory cortex doesn't receive sufficient proprioceptive feedback, the motor system generates seeking behavior to fill the gap.
Key Insight: The goal was never to stop the flapping. The goal is to understand what the nervous system is asking for — and give it more ways to receive it.
Frontiers in Integrative Neuroscience (2020): Neurological basis for sensory-based interventions in ASD. DOI: 10.3389/fnint.2020.556660 | Ayres Sensory Integration® Theory — foundational framework

Your Child Is Here. Here Is Where We Are Heading.
Understanding where hand flapping sits in your child's developmental timeline transforms how you respond to it. Motor stereotypies are a normal part of early development — and for children with autism, they persist because the sensory need driving them has not yet been met through an alternative channel.
1
Age 6–18 months
Motor stereotypies emerge in all children as normal sensory exploration
2
Age 2–3 years
Typically developing children reduce stereotypies as language and motor skills expand
3
Age 3–7 years (ASD)
Stereotypies persist and intensify — the sensory need is still unmet
4
Current: Your Child
Proprioceptive seeking behavior active — toolkit intervention begins here
5
Weeks 1–8 with Toolkit
Sensory need met through structured alternatives — flapping frequency reduces
You are not trying to stop a behavior. You are trying to meet a need. When the need is met, the behavior changes — because it no longer has to do the job alone.
Motor stereotypy research: Leekam et al. (2011), Autism Research. Developmental trajectory of repetitive behaviors in ASD populations.

Clinically Validated. Home-Applicable. Parent-Proven.
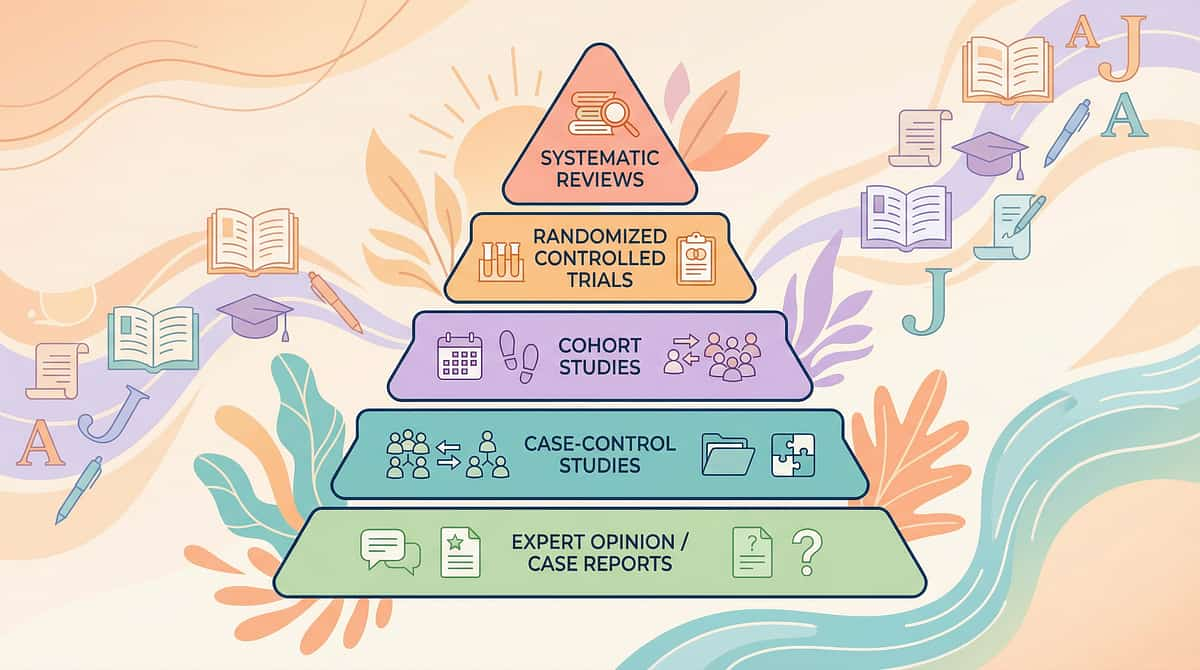
Before you begin building your child's sensory toolkit, you deserve to know that the approach is backed by the highest tier of clinical evidence — systematic reviews, meta-analyses, and real-world trials across global pediatric populations.
PRISMA Systematic Review 2024 (PMC11506176)
16 studies confirm sensory integration intervention is evidence-based practice for ASD. Evidence Level: HIGH
Meta-Analysis World J Clin Cases 2024 (PMC10955541)
24 studies: SI therapy improves sensory processing, motor skills, adaptive behavior. Evidence Level: HIGH
Indian RCT Padmanabha et al. (2019)
Home-based sensory interventions demonstrate significant outcomes in Indian pediatric population. Evidence Level: STRONG
NCAEP Evidence-Based Practices Report (2020)
Sensory-based interventions classified as established EBP for autism. Evidence Level: HIGH
"Sensory integration intervention effectively promotes social skills, adaptive behavior, sensory processing, and motor skills in children with autism spectrum disorder." — World Journal of Clinical Cases, Meta-Analysis, 2024
Evidence Strength
Home Applicability
Parent-Delivered Efficacy

ACT II: THE KNOWLEDGE TRANSFER
Proprioceptive Sensory Input via Therapeutic Materials
Parent-friendly name: "Sensory Toolkit for Hand Flapping"
What it is: A structured approach to meeting the proprioceptive and tactile sensory needs that drive hand flapping — using 9 categories of therapeutic materials that provide equivalent or superior sensory input, expanding the child's regulatory options without eliminating natural coping behaviors.
What it does: Provides hands, arms, and the nervous system with the deep pressure, resistance, vibration, and tactile feedback that flapping seeks — through purposeful, functional, socially flexible alternatives.
Who it's for: Children ages 2–12 with autism, sensory processing differences, motor stereotypies, or any child whose hands seek proprioceptive input for self-regulation.
What it does: Provides hands, arms, and the nervous system with the deep pressure, resistance, vibration, and tactile feedback that flapping seeks — through purposeful, functional, socially flexible alternatives.
Who it's for: Children ages 2–12 with autism, sensory processing differences, motor stereotypies, or any child whose hands seek proprioceptive input for self-regulation.
🎯 Domain
D — Behavior & Self-Regulation
🧩 Sub-Domain
Motor Stereotypy / Proprioceptive Seeking
🏷️ Reel ID
D-362 | Sensory & Self-Regulation — Episode 362
⏱️ Frequency
Daily integration | Embedded throughout day
Pinnacle 128 Canon Materials Taxonomy | GPT-OS® 20 Category Classification System | Domain D: Behavior & Flexibility

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type

🦾 Occupational Therapy (OT) — PRIMARY LEAD
OT is the primary clinical driver. OTs conduct sensory processing assessments, design sensory diets, and prescribe specific materials matched to each child's sensory profile. At Pinnacle, OT leads the proprioceptive input protocol.

🧩 Applied Behavior Analysis (ABA/BCBA)
ABA conducts functional behavior assessments to determine WHY the flapping occurs. ABA also designs reinforcement schedules for toolkit use and builds contextual discrimination: "During class, use your fidget. At home, you can flap freely."

🗣️ Speech-Language Pathology (SLP)
For children with limited verbal communication, SLP integrates sensory regulation tools with AAC systems so the child can communicate their sensory state instead of only expressing it through movement.

🎓 Special Education (SpEd)
Special educators embed sensory diet materials into the classroom — fidgets at desks, compression vests for transitions, heavy work breaks before focused learning tasks. SpEd ensures the toolkit generalizes to the educational setting.
WHO/UNICEF Nurturing Care Framework for Multi-Disciplinary SLPs (2022) | DOI: 10.1080/17549507.2022.2141327 | Pinnacle FusionModule™ integration protocols
This Is Not a Random Activity. It Is a Precision Regulatory Tool.
Target Level | You Will See | Timeline | |
Primary | Child reaches for toolkit material instead of flapping (in some contexts) | Weeks 4–8 | |
Primary | Reduced flapping duration when toolkit is available | Weeks 2–4 | |
Secondary | Child can name or indicate their sensory need | Weeks 6–12 | |
Secondary | Improved attention following sensory input | Weeks 2–6 | |
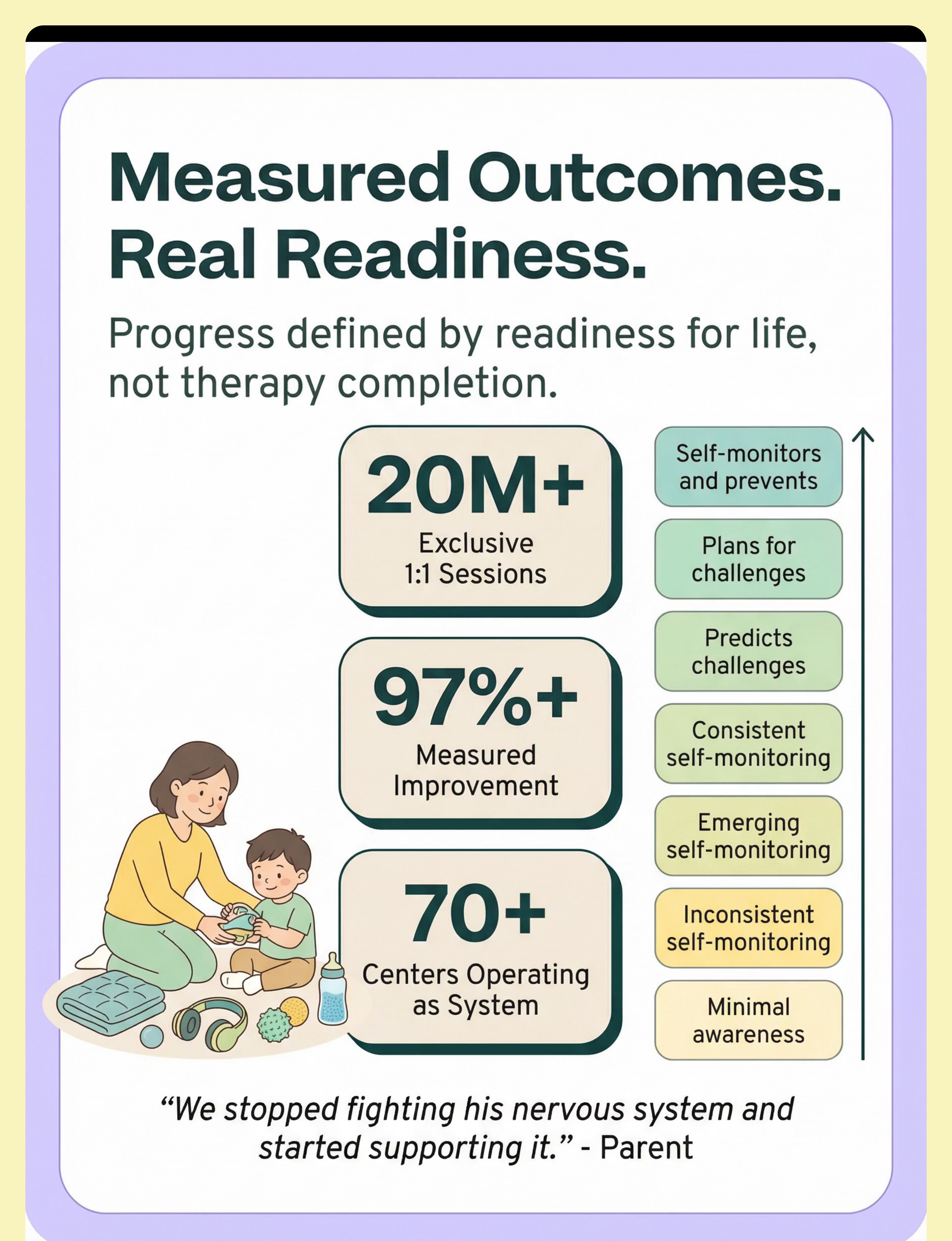
Tertiary | Child self-monitors sensory state and prevents dysregulation | Months 3–6 |
PMC10955541 (Meta-analysis 2024): SI therapy targets confirmed across social, adaptive, sensory, and motor domains | NCAEP 2020 Evidence-Based Practice Standards
9 Materials. One Underlying Principle: Give the Nervous System What It's Seeking.

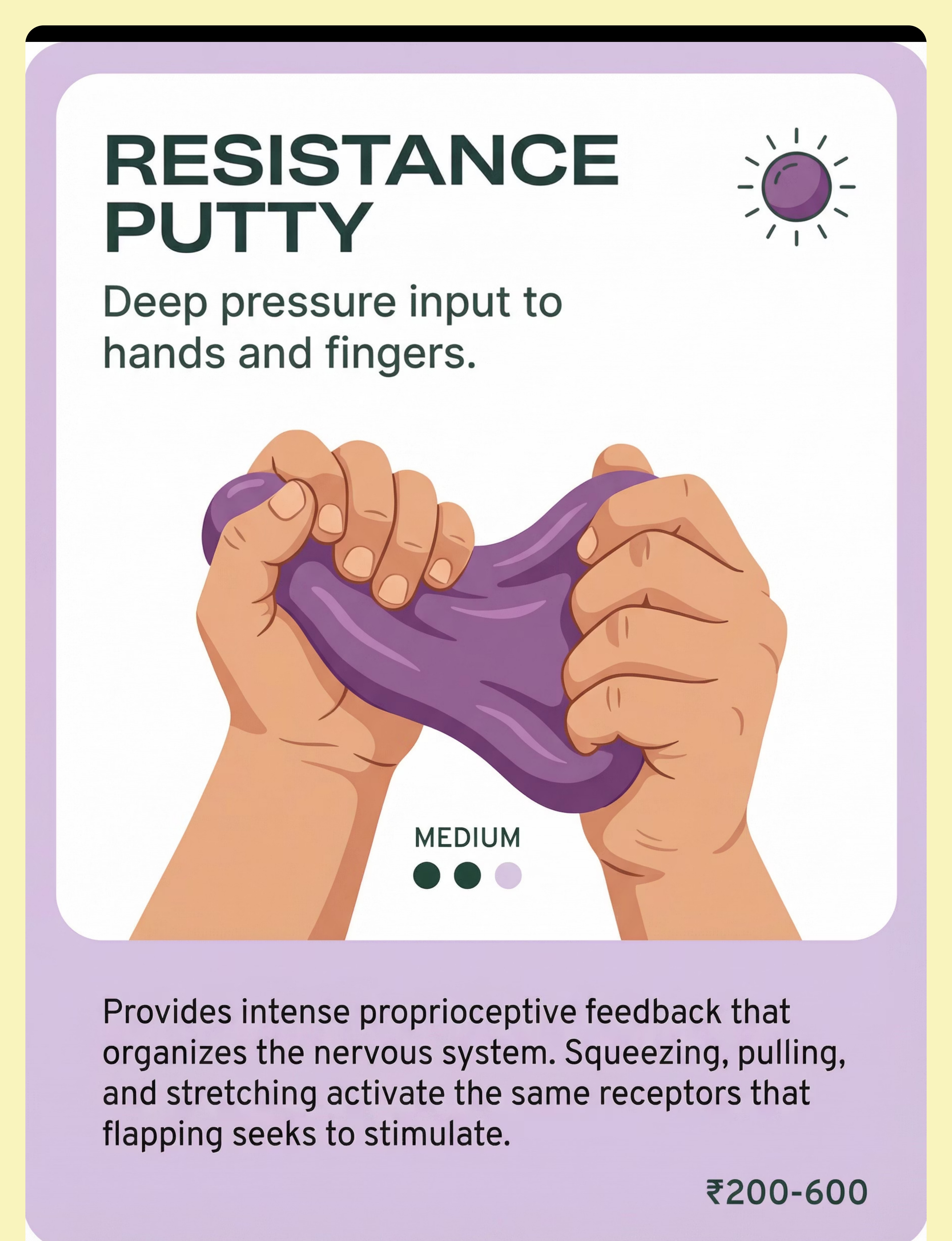
1. Resistance Putty & Therapy Dough
🔵Mechanism: Deep proprioceptive pressure via resistance. Squeezing, pulling, stretching putty activates the same joint and muscle receptors that flapping targets — with greater intensity and control.
💰 ₹200–600 | Search: "therapy putty resistance levels"
💰 ₹200–600 | Search: "therapy putty resistance levels"

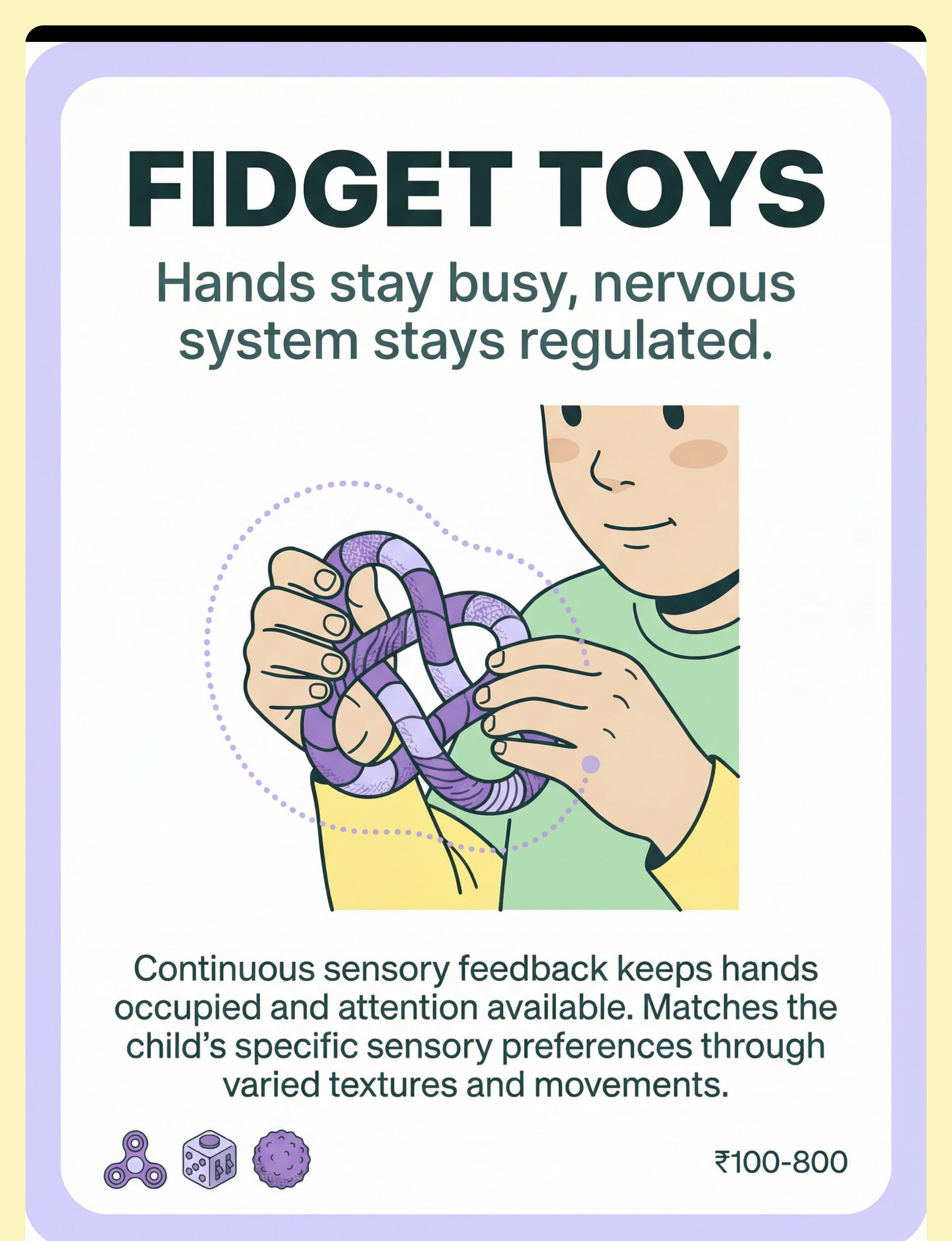
2. Fidget Toys & Hand Manipulatives
🟣Mechanism: Continuous sensory feedback, portable regulation. Spinners, tangles, textured balls, and resistance fidgets keep hands purposefully occupied. Matched to the child's sensory preference — texture, movement, or resistance.
💰 ₹100–800 | Search: "sensory fidget toys autism"
💰 ₹100–800 | Search: "sensory fidget toys autism"

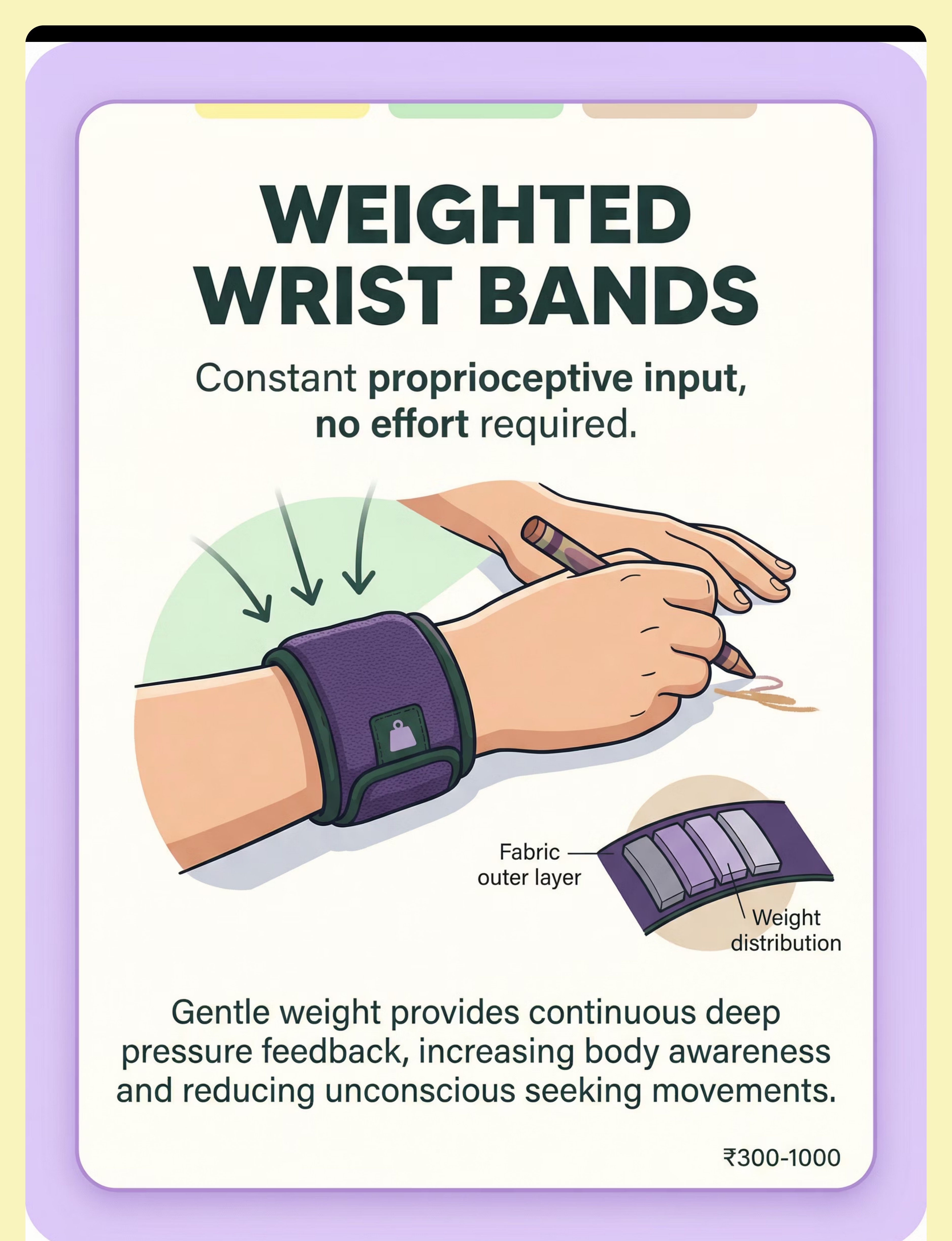
3. Weighted Wrist Bands & Hand Weights
⚫Mechanism: Passive proprioceptive input, continuous. Gentle weight provides constant deep pressure without any action required. Background regulation for the child whose hands seek input throughout the day.
💰 ₹300–1000 | Search: "weighted wrist bands children OT"
💰 ₹300–1000 | Search: "weighted wrist bands children OT"

4. Hand Strengthening Tools & Grip Exercisers
🔴Mechanism: Intense proprioceptive work, builds regulatory capacity. Grip exercisers, therapy balls, and finger resistance tools deliver concentrated proprioceptive feedback. Hard work for the hands = organized signals for the brain.
💰 ₹150–600 | Search: "hand grip exerciser therapy"
💰 ₹150–600 | Search: "hand grip exerciser therapy"

5. Vibrating Massagers & Vibration Tools
🟡Mechanism: Deep penetrating input reaching joint proprioceptors. Vibration delivers proprioceptive and tactile feedback that penetrates deeper than flapping can reach. For intense sensory seekers, vibration is more satisfying than flapping.
💰 ₹300–1500 | Search: "handheld vibrating massager children"
💰 ₹300–1500 | Search: "handheld vibrating massager children"

6. Compression Gloves & Pressure Garments
🟢Mechanism: Passive deep pressure, constant body awareness. Compression creates a continuous proprioceptive "hug" for the hands and arms. Works in the background — the child focuses on other tasks while the garment regulates.
💰 ₹400–1200 | Search: "compression gloves children autism"
💰 ₹400–1200 | Search: "compression gloves children autism"

7. Heavy Work Activities Kit
🟤Mechanism: Full-body proprioceptive loading, proactive regulation. Pushing, pulling, lifting, carrying — natural heavy work meets the sensory need before flapping emerges. Prevention is superior to redirection.
💰 ₹200–1000 | Search: "therapy resistance bands heavy work kit"
💰 ₹200–1000 | Search: "therapy resistance bands heavy work kit"

8. Sensory Bins with Tactile Materials
🔵Mechanism: Rich simultaneous proprioceptive + tactile input. Kinetic sand, rice bins, water beads: hands stay meaningfully engaged with rich sensory input. Hands busy = regulatory need met.
💰 ₹200–800 | Search: "kinetic sand sensory bin"
💰 ₹200–800 | Search: "kinetic sand sensory bin"

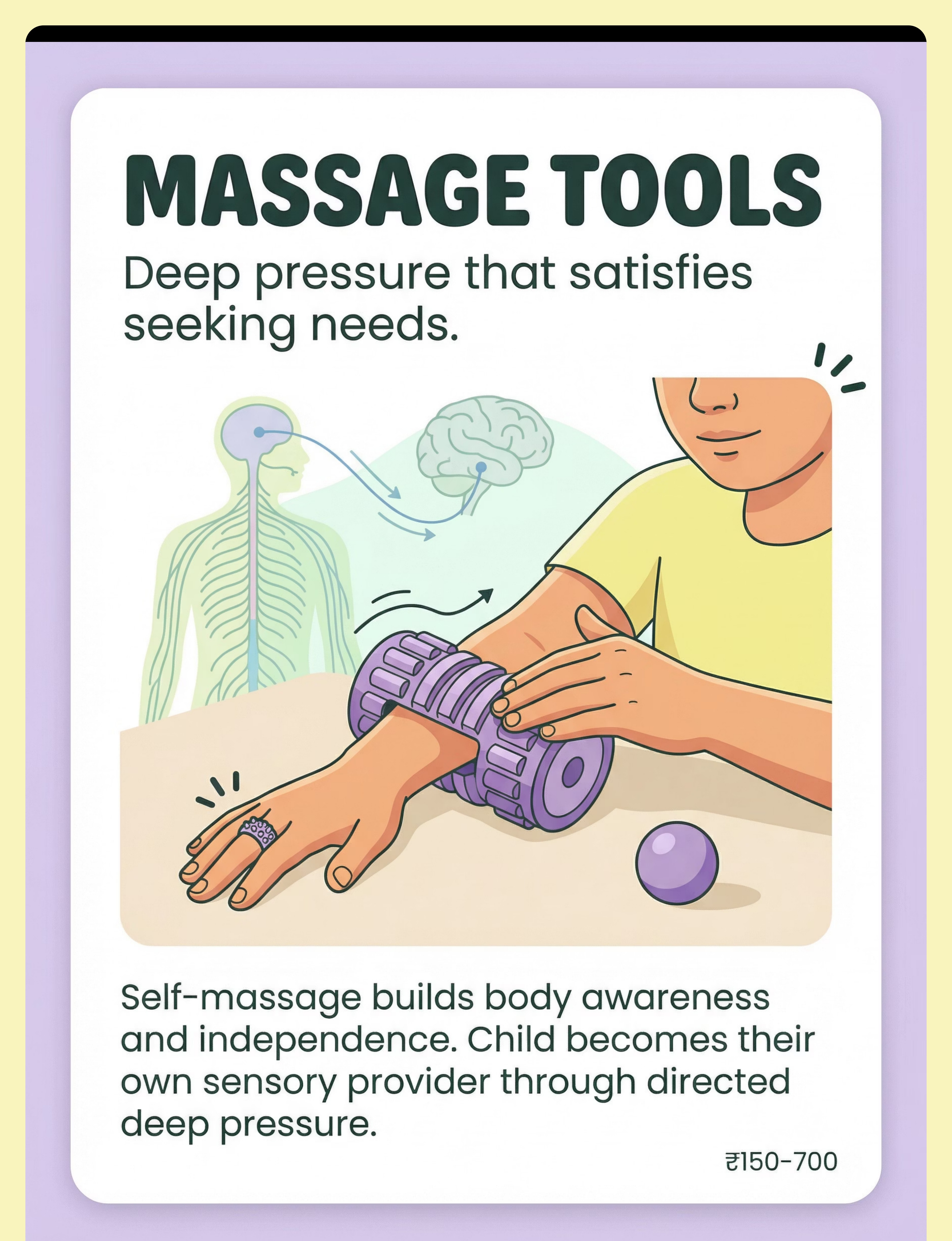
9. Arm & Hand Massage Tools
🟣Mechanism: Targeted deep pressure, builds self-regulation. Massage rollers, acupressure rings, spiky balls deliver directed proprioceptive input. The child becomes their own sensory provider — a core self-regulation skill.
💰 ₹150–700 | Search: "massage roller hand therapy"
💰 ₹150–700 | Search: "massage roller hand therapy"
✅ All 9 materials clinically validated within Pinnacle's OT protocols. Starter Kit: Resistance putty + 1 matched fidget + heavy work activity (₹450–1400 total)

Every Child Deserves Sensory Support — Regardless of What You Can Spend
WHO Nurturing Care Framework Principle: Context-specific, equity-focused interventions. The 9 materials below can all be replicated at home using household items. Zero-cost intervention is valid intervention.
Material | Zero-Cost Substitute | Why It Works | |
Resistance Putty | Homemade dough: 2 cups flour, 1 cup salt, 2 tbsp cream of tartar, 2 tbsp oil, 2 cups water — cook until dough forms; add less water for more resistance | Same proprioceptive resistance principle | |
Fidget Toys | Knotted rope, folded cloth, dried beans in a small bag, rubber band collection | Tactile + mild proprioceptive input | |
Weighted Wrist Bands | Sew fabric tubes, fill with rice or sand, add velcro. Start: 100–200g per wrist | Weight = proprioceptive input regardless of source | |
Hand Strengthening Tools | Clothespins (pinching), spray bottles (squeezing), roll of clay, wet sponges to wring | Resistance = proprioceptive feedback | |
Vibrating Massager | Electric toothbrush handle on hands/arms (brief, supervised) | Receptor response is identical | |
Compression Gloves | Tight bicycle gloves (fingerless), elasticised bandage wrap (light) | Compression principle unchanged | |
Heavy Work Kit | Carry filled backpack, push laundry basket, pull full water bucket, do wall push-ups | Heavy work is activity-based; equipment optional | |
Sensory Bins | Basin of dry rice/lentils + small plastic figures to find, or sand in a tray | Tactile + mild proprioceptive input via digging | |
Massage Tools | Rough cloth or towel for friction massage, tennis ball to roll under palm, fingers for joint compression | Deep pressure doesn't require equipment |
When clinical-grade is non-negotiable: If the child has significant sensory defensiveness, unusual tactile reactions, or medical co-morbidities — consult an OT before DIY substitution. Clinical-grade tools provide standardized, calibrated input that household items cannot always match.
WHO NCF Handbook (2022) | PMC9978394 | CCD Package implemented across 54 LMICs demonstrating household-material intervention efficacy

Read Before You Begin. Every Session.
Safety is not optional — it is the first step of every session. This three-zone system gives you a clear, observable framework for deciding whether to proceed, modify, or postpone. When in doubt, call before you continue.
🔴 STOP — Do Not Proceed
• Child is in active meltdown or severe distress
• Hands/skin show irritation, injury, or infection
• Child is ill, feverish, or significantly sleep-deprived
• Self-injurious behavior during flapping — consult OT/BCBA first
• Sudden onset of new stereotypy patterns — rule out medical cause
• Hands/skin show irritation, injury, or infection
• Child is ill, feverish, or significantly sleep-deprived
• Self-injurious behavior during flapping — consult OT/BCBA first
• Sudden onset of new stereotypy patterns — rule out medical cause
🟡 MODIFY — Proceed with Adjustments
• Child is mildly dysregulated but responsive — 1 material, under 5 minutes
• Child is hungry or fatigued — reduce intensity
• First introduction of any new material — 30-second exposure first
• Allergies: Check wheat/gluten for flour-based putty; latex for rubber-based materials
• Child is hungry or fatigued — reduce intensity
• First introduction of any new material — 30-second exposure first
• Allergies: Check wheat/gluten for flour-based putty; latex for rubber-based materials
🟢 GO — Optimal Conditions
• Child is alert, calm-ish, and recently fed
• Environment is prepared
• You have 10–20 minutes of uninterrupted time
• Child is familiar with at least one toolkit material
• Environment is prepared
• You have 10–20 minutes of uninterrupted time
• Child is familiar with at least one toolkit material
Stop Immediately If: Skin changes: redness, blanching, or numbness during weighted/compression use | Escalating distress in response to any sensory material | Child communicates "no," "stop," or shows avoidance — always honor this
📞9100 181 181 | FREE National Autism Helpline | 16+ Languages | 24×7 — When in doubt, call before you continue.
DOI: 10.1007/s12098-018-2747-4 (Padmanabha et al., Indian J Pediatr, 2019) | AOTA Sensory Integration Safety Guidelines
The Right Environment Multiplies the Effect of Every Material
Setup Checklist
🔇Sound: Soft background music or quiet. No TV or competing demands.
💡Lighting: Natural or soft warm light. No harsh fluorescent.
🌡️Temperature: Comfortable — not hot (increases dysregulation).
📱Screens: All screens off — for the parent too.
🧹Floor Space: 2 square meter clear area if heavy work included.
⏱️Timer: Visual timer visible to child (sand timer or countdown app).
📦Materials: Pre-selected 2–3 options maximum. Choice overload is dysregulating.
💡Lighting: Natural or soft warm light. No harsh fluorescent.
🌡️Temperature: Comfortable — not hot (increases dysregulation).
📱Screens: All screens off — for the parent too.
🧹Floor Space: 2 square meter clear area if heavy work included.
⏱️Timer: Visual timer visible to child (sand timer or countdown app).
📦Materials: Pre-selected 2–3 options maximum. Choice overload is dysregulating.
Parent Positioning
Be at the child's eye level. Sit, don't stand. Close enough to guide — far enough to allow.
What to Remove from the Space
- Other children's toys not in use today
- Strong smells (perfume, candles)
- Any recently distressing objects
- Pets if they cause distraction
Sensory Station Layout
Materials on a low table or floor within the child's reach:
① Putty + fidgets within arm's reach
② Bin / heavy work at the side
③ Massage tools accessible nearby
④ Child on floor or low chair, stable position
⑤ Parent seated at the same level
① Putty + fidgets within arm's reach
② Bin / heavy work at the side
③ Massage tools accessible nearby
④ Child on floor or low chair, stable position
⑤ Parent seated at the same level
Natural window light (not glare) is ideal. Avoid overhead fluorescent lighting which increases sensory load before the session has even begun.
PMC10955541 (Meta-analysis): 1:1 individual treatment sessions in structured environments most effective | Ayres SI: Environmental setup as core principle

ACT III: THE EXECUTION
60 Seconds. 7 Questions. One Decision. The Best Session Is One That Starts Right.
Indicator | ✅ Green | 🔶 Modify | ❌ Postpone | |
Last meal | 1–2 hrs ago | 30 min ago | Hungry/just ate | |
Sleep last night | Good (age-typical) | Slightly tired | Overtired | |
Current arousal | Calm or mildly alert | Slightly elevated | Meltdown/shutdown | |
Response to name | Responds | Delayed response | Not responding | |
Physical state | No illness signs | Mild restlessness | Ill/distressed | |
Flapping intensity | Baseline | Elevated | Continuous, intense | |
Last meltdown | >4 hours ago | 2–4 hours ago | <2 hours ago |
5–7 ✅ Green
Full session. All materials available.
3–4 ✅ Green
Shortened session. 1 familiar material only. 5 minutes max.
Fewer than 3 ✅
Postpone today. Offer calming input: gentle weighted blanket, dim room, quiet.
If Modify — Simplified Version: Bring one piece of familiar putty. Sit together. No demands. Let the child's hands do what they need. Be present. That IS the session today.
ABA Antecedent Manipulation: Setting event conditions determine intervention effectiveness | Pinnacle Clinical Pre-Session Readiness Protocol

Every Protocol Begins with an Invitation. Never a Command.
STEP 1
⏱️ 30–60 seconds
Parent Script
"I have something for your hands. Want to see?"
OR
"Time for hand time. Come sit with me for a minute."
OR (non-verbal): Silently place one piece of putty on the table between you and wait.
OR
"Time for hand time. Come sit with me for a minute."
OR (non-verbal): Silently place one piece of putty on the table between you and wait.
Body Language
• Get to the child's level — sit on the floor if needed
• Relaxed posture, no urgency in expression
• Hold the material casually — explore it yourself first
• Slow movements. No sudden presentation.
• Relaxed posture, no urgency in expression
• Hold the material casually — explore it yourself first
• Slow movements. No sudden presentation.
✅ Acceptance Cues — What to Look For
Child looks at material | Child moves toward material | Child reaches out | Child's body softens | Flapping pauses or changes quality
🔶 Resistance Cues — What to Do
Child turns away: Don't push. Sit quietly 30 more seconds. Try one different material.
Child walks away: Follow (if appropriate) or let them. Today's invitation is for information.
Child becomes distressed: End invitation. No force. Data collected.
Child walks away: Follow (if appropriate) or let them. Today's invitation is for information.
Child becomes distressed: End invitation. No force. Data collected.
ABA Principle: This is pairing — building positive association between the material and the parent's presence before any demand is placed. Rushed pairing = failed sessions later.
ABA Pairing Procedures: Establishing motivating operations before demand placement | OT Just-Right Challenge: Matching task to current capacity
The Child Is Engaged. Now Introduce the Material.
STEP 2
⏱️ 1–3 minutes
The material introduction sequence is the bridge between invitation and engagement. Follow the child's lead at every step — their exploration style is data about their sensory preference.
🟢 Engagement
Child manipulates material, facial expression softens, flapping reduces or stops, child makes eye contact.
🟡 Tolerance
Child holds material without exploring, remains nearby, shows mild interest.
🔴 Avoidance
Child drops material, pushes it away, moves away — honor this, try a different material.
Reinforcement Cue: When you see engagement or tolerance: "Good. Strong hands." — Specific, quiet, immediate. No excessive praise — it can be as dysregulating as criticism.
PMC11506176 (Systematic review): Structured material introduction in sensory integration meets EBP criteria | Reinforcement scheduling from ABA behavioral literature

The Core Therapeutic Event: Meeting the Proprioceptive Need Directly
STEP 3
⏱️ 5–15 minutes (target zone)
Resistance Putty
Guide child through: squeeze → hold 5 seconds → release → roll into ball → pull into snake → tear piece off. Repeat 5–10 times. Encourage strong, deliberate effort.
Fidget Toys
Allow free exploration first. Then suggest: "Can you spin it three times?" Sustained hand engagement — duration matters more than technique.
Weighted Wrist Bands
Simply place on wrists. No action required. Let child engage in regular activity while wearing them. Duration: 20–30 minutes maximum before checking comfort.
Hand Strengthening Tools
Squeeze grip exerciser: 10 repetitions per hand. Rest. Repeat 2–3 sets. Or: hide objects in putty for the child to find by pinching — make it a game.
Vibrating Massager
Apply to back of hands, then forearms, for 1–2 minutes. Let child hold the massager themselves if willing. Observe: relaxation response, vocalization, reduced flapping.
Compression Gloves
Put on, adjust fit. Let child engage in regular activity. Check fingers every 15 minutes (circulation). Remove if child indicates discomfort.
Heavy Work Kit
5 minutes of: wall push-ups (10 reps), carrying filled backpack across room and back (3 trips), pushing heavy basket across floor. Do it WITH the child — make it joint activity.
Sensory Bin
Set bin on floor/table. Place child's hands in. Start with your own hands in the bin — model digging, scooping, burying. Find hidden objects together.
Massage Tools
Parent or child: roll spiky ball across back of hand, up forearm. Apply gentle firm pressure. Teach: hand → fingers → wrist → forearm. Self-massage is the goal.
PMC10955541: 40-minute sessions showed maximum effectiveness. Home sessions 10–20 minutes; core action 40–60% of session time.

3 Good Repetitions Are Worth More Than 10 Forced Ones.
STEP 4
⏱️ 3–5 minutes total
Material | Target Reps | Satiation Signs | Don't Exceed | |
Putty | 5–10 squeeze cycles | Hands slow, interest wanders | 15 min continuous | |
Fidget | 3–5 min continuous | Child puts down unprompted | Child's choice | |
Weighted bands | 20–30 min wear | Child removes or distress | 30 min per session | |
Grip exerciser | 10 reps × 2–3 sets | Fatigue, avoidance | Hand fatigue | |
Vibration | 1–3 min per area | Child pulls away | 5 min per session | |
Compression gloves | Up to 2 hours | Circulation check | Per OT guidance | |
Heavy work | 5–10 min session | Fatigue, refusal | Exhaustion | |
Sensory bin | 5–15 minutes | Interest wanes | Child's choice | |
Massage | 2–5 minutes | Child signals stop | Child's choice |
Change the Material
Putty → Fidget → Bin. Same underlying need, different sensory delivery.
Change the Setting
Floor → Table → Outdoor heavy work. Context variety improves generalization.
Change the Challenge
Easier ← → Harder within the same material. Match the just-right challenge.
Change the Role
Parent-guided → child-led → independent. Build self-regulation capacity over time.
SI dosage research: 2–3 sessions per week, 8–12 weeks typical protocol | Session-level repetition from Pinnacle OT clinical guidelines

Timing Matters More Than Magnitude. Celebrate the Attempt. Not Just the Success.
STEP 5
⏱️ Within 3 seconds of desired behavior
Reinforcement Script
✅"Strong hands! You did it!"
✅"You squeezed! That's what your hands needed!"
✅"Look at you! Hands working hard!"
✅ (Non-verbal): Thumbs up + smile + brief shoulder touch if accepted
✅"You squeezed! That's what your hands needed!"
✅"Look at you! Hands working hard!"
✅ (Non-verbal): Thumbs up + smile + brief shoulder touch if accepted
What NOT to Say
❌"Good boy/girl for not flapping" — never reinforce absence of a natural behavior
❌"I'm so proud you're using this instead of flapping" — frames flapping as wrong
✅"I love how you tried the putty" — reinforce toolkit use, not suppression
❌"I'm so proud you're using this instead of flapping" — frames flapping as wrong
✅"I love how you tried the putty" — reinforce toolkit use, not suppression
🏆 Reinforcement Menu
Tier 1 — Social reinforcement: Verbal praise, smiles, high-fives, celebratory words.
Tier 2 — Token system: Sticker on chart after each successful sensory session (5 stickers = preferred activity).
Tier 3 — Natural consequence: After heavy work → preferred calming activity. After putty → free fidget time.
Tier 2 — Token system: Sticker on chart after each successful sensory session (5 stickers = preferred activity).
Tier 3 — Natural consequence: After heavy work → preferred calming activity. After putty → free fidget time.
Token Economy: Award 1 sticker immediately upon any engagement with a sensory toolkit material — even 10 seconds counts. The reinforcement teaches: "Using the toolkit = good things happen."
ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence | Token economy evidence across autism intervention: multiple systematic reviews | BACB ethical guidelines

No Session Ends Abruptly. The Transition IS Part of the Therapy.
STEP 6
⏱️ 2–3 minutes
Transition Warning Script
"Two more squeezes, then we're all done." → [2 squeezes] → "One more." → [1 squeeze] → "All done. Great job. Hands worked hard today."
Cool-Down Activity (1–2 minutes calming input)
Deep pressure: Cross arms over chest and give yourself a firm hug (teach child to self-apply). Slow breathing: 4 counts in, 4 hold, 4 out (model while doing). Weighted lap pad or blanket if available. Or simply: sit quietly together, no demands, for 60 seconds.
Material Put-Away Ritual
"Help me put the putty back in the jar." | "Can you put the fidget in the box?" Child participation in cleanup = closure ritual + fine motor practice.
Transition to Next Activity
"Now it's time for [next activity]. Your hands feel better?" Bridge the sensory session to what comes next. The regulation effect lasts 2–4 hours.
If Child Resists Ending:"I know. You want more. Five more seconds. [count slowly] All done. We'll do this again [tomorrow/later]." Honor the sensory need even while closing the session.
NCAEP 2020: Visual supports + transition warnings are evidence-based practice for autism | Countdown + warning procedures from ABA transition support literature

60 Seconds of Data Now Saves Hours of Guessing Later.
What to Record (3 data points, maximum)
Duration of session: Minutes (estimate ok). Example: "12 minutes"
Child's engagement level: 1–5 scale (1=rejected, 5=fully engaged). Example: "4 — sustained for 8 min"
Flapping before vs. during: Estimate: more/same/less. Example: "Less during putty, returned after"
Child's engagement level: 1–5 scale (1=rejected, 5=fully engaged). Example: "4 — sustained for 8 min"
Flapping before vs. during: Estimate: more/same/less. Example: "Less during putty, returned after"
📋 Download: D-362 Session Tracker PDF
Direct link to Pinnacle tracking sheet: pinnacleblooms.org/resources/D-362-session-tracker
Why This Matters
After 4 weeks of consistent data, you will see patterns emerge that single-session observation can never reveal:
- "She always rates 4 or 5 with putty but 1 with vibration."
- "He's most regulated on days when we start with heavy work."
- "Engagement doubles when sessions happen before transitions."
This data personalizes your child's sensory diet more precisely than any one-size-fits-all protocol. Your child's nervous system has a fingerprint — and your tracker is how you discover it.
📱GPT-OS® Quick Data Capture: Your anonymized data contributes to the population-level learning database — helping children like yours across 70 countries. Every session counts.
ABA Data Collection Standards: Continuous measurement (frequency, duration) and discontinuous measurement | BACB Guidelines + Cooper, Heron & Heward, Applied Behavior Analysis 8th Ed.

Session Abandonment Is Not Failure. It Is Data.
Every session — good or difficult — teaches you something. The troubleshooting guide below gives you a clear path forward for the seven most common session challenges parents encounter.
Child refused all 9 materials
Why: Sensory profile may not align with these material types, or today's arousal state made any input intolerable.
Next time: Slow down the invitation phase (Card 14). Pre-pair materials over 3–5 days before expecting engagement. Try materials in a different context (bathtime, outdoor play).
Next time: Slow down the invitation phase (Card 14). Pre-pair materials over 3–5 days before expecting engagement. Try materials in a different context (bathtime, outdoor play).
Child engaged briefly then ran away
Why: The sensory input met the need quickly — or the session duration exceeded the child's tolerance window.
Next time: 30-second engagement = success at this stage. Build duration gradually. Keep invitation language completely demand-free.
Next time: 30-second engagement = success at this stage. Build duration gradually. Keep invitation language completely demand-free.
Child flapped more during/after the session
Why: Some highly stimulating materials (vibration, heavy work) can activate before they calm.
Next time: Follow stimulating materials with calming ones. Heavy work → compression or weighted bands. Sequence matters.
Next time: Follow stimulating materials with calming ones. Heavy work → compression or weighted bands. Sequence matters.
Child used the material incorrectly (threw putty, chewed fidget)
Why: The child is exploring through their primary sensory modality — this is information about their sensory profile.
Next time: For oral seekers — consult OT about oral motor tools. For throwers — provide heavier, more resistive materials in a safer context.
Next time: For oral seekers — consult OT about oral motor tools. For throwers — provide heavier, more resistive materials in a safer context.
Parent ran out of patience mid-session
Why: Completely normal. Managing your own regulation while supporting your child's is genuinely hard.
Next time: Shorter sessions (5 minutes) until confidence builds. Tag-team with another caregiver. You cannot pour from an empty cup.
Next time: Shorter sessions (5 minutes) until confidence builds. Tag-team with another caregiver. You cannot pour from an empty cup.
Child used toolkit AND flapped — "it didn't work"
Reframe: Sensory toolkit use and flapping are not mutually exclusive. Co-occurrence is progress. "My child squeezed the putty for 4 minutes AND flapped at the end. That's 4 minutes of new regulatory behavior that didn't exist last week."
Can't tell if it's helping
Why: Short-term effects can be subtle. Without data (Card 20), changes are invisible.
Next time: Implement the tracker for 2 weeks. Patterns emerge that single-session observation cannot reveal.
Next time: Implement the tracker for 2 weeks. Patterns emerge that single-session observation cannot reveal.
ABA Troubleshooting: Functional analysis principles applied to session-level problem solving | Antecedent modification from behavioral literature
No Two Children Are Identical. Neither Are Two Sessions.
Difficulty Slider
EASIER ←──────────→ HARDER
1 material → 3 materials → All 9
Soft putty → Medium → Extra-firm
5 seconds → 2 minutes → 10+ minutes
Parent-guided → Child-led → Independent
Home only → + School → All contexts
1 material → 3 materials → All 9
Soft putty → Medium → Extra-firm
5 seconds → 2 minutes → 10+ minutes
Parent-guided → Child-led → Independent
Home only → + School → All contexts
Age-Based Modifications
Ages 2–3: Sensory bins + soft putty. 3–5 minute sessions. Play-based entirely.
Ages 4–6: Fidgets + putty + heavy work games. 10 minutes. Mix structured and play.
Ages 7–10: Full toolkit. Introduce self-selection and self-monitoring.
Ages 10–12: Child designs own sensory diet. Parent is support, not director.
Ages 4–6: Fidgets + putty + heavy work games. 10 minutes. Mix structured and play.
Ages 7–10: Full toolkit. Introduce self-selection and self-monitoring.
Ages 10–12: Child designs own sensory diet. Parent is support, not director.
Sensory Profile Adaptations
For Proprioceptive Seekers: Start with heaviest work — extra-firm putty + grip exerciser + heavy work. Layer weighted bands for background input.
For Mixed Seekers (proprioceptive + tactile): Open each session with sensory bin (tactile entry), then transition to putty or fidgets. Massage tools to close.
For Sensory Avoiders who incidentally flap: Start with lightest materials: soft putty, compression gloves (passive input), massage tools at low pressure. Never force.
For Non-Verbal Children: Use choice boards — photos of 3 materials → child points to preferred → that's the session material. Builds communication AND sensory self-advocacy simultaneously.
For Mixed Seekers (proprioceptive + tactile): Open each session with sensory bin (tactile entry), then transition to putty or fidgets. Massage tools to close.
For Sensory Avoiders who incidentally flap: Start with lightest materials: soft putty, compression gloves (passive input), massage tools at low pressure. Never force.
For Non-Verbal Children: Use choice boards — photos of 3 materials → child points to preferred → that's the session material. Builds communication AND sensory self-advocacy simultaneously.
Individualized intervention planning: Core principle across OT (sensory profile), ABA (function-based), SLP (communication profile) | Pinnacle clinical adaptation protocols

ACT IV: THE PROGRESS ARC
In Weeks 1–2, You Are Building Trust Between the Toolkit and the Nervous System.
Foundation Phase
Progress is real but subtle in weeks 1–2. Track it.
What Progress Actually Looks Like (Week 1–2)
✅ Child allows material near their body (even without engaging)
✅ Child tolerates one material for 10+ seconds longer than day 1
✅ Child shows curiosity (looks, approaches)
✅ Flapping intensity slightly lower during material exposure
✅ You feel slightly more confident introducing materials
✅ Child tolerates one material for 10+ seconds longer than day 1
✅ Child shows curiosity (looks, approaches)
✅ Flapping intensity slightly lower during material exposure
✅ You feel slightly more confident introducing materials
What Is NOT Progress Yet (and that's fine)
❌ Child preferring toolkit over flapping — too soon
❌ Consistent independent use — not expected
❌ Dramatic flapping reduction — not yet
❌ Generalization to school — not this phase
❌ Consistent independent use — not expected
❌ Dramatic flapping reduction — not yet
❌ Generalization to school — not this phase
Patient Metric:"If your child tolerates a material for 10 seconds longer than last week — that is real, measurable, clinical progress. Track it on your Card 20 sheet. Write it down."
Weeks 1–2 are the hardest. The novelty of the toolkit may provoke resistance. Flapping may temporarily increase because you've introduced change into the sensory environment. This is normal. Stay consistent. You are building the habit before you see the benefits.
PMC11506176: SI intervention outcomes emerge across 8–12 week timelines. Early-phase indicators: tolerance and participation rather than skill mastery

The Brain Is Rewiring. You May Not See It — But It Is Happening.
Neural Pathway Forming
Weeks 3–4: consolidation and preference emerging.
✅ Child Anticipates
May bring the putty or fidget themselves before the session begins.
✅ Preference Emerging
Consistently chooses one material over others — sensory profile becoming clear.
✅ Less Parent Initiation
Child accepts toolkit independently — less prompting required.
✅ Post-Session Calm
Child is noticeably calmer for 1–2 hours after a sensory session.
Signs Most Parents Miss: Child runs fingers over the putty container without being asked (tactile seeking redirected). Child reaches for the fidget before a transition (proactive regulation emerging). Flapping duration shortened without any intervention.
"By Week 4, most parents report that they feel more confident — not just in the toolkit, but in their understanding of their child's sensory system. You may notice you're more confident in explaining the behavior to others."
Neuroplasticity: Synaptic strengthening through repeated structured input follows predictable timelines in pediatric populations. Behavioral consolidation aligns with neural adaptation curves.

Mastery Is Not the Absence of Flapping. It Is the Presence of Choice.
✅ Independent Access
Child accesses sensory toolkit in at least 1–2 contexts without prompting.
✅ Self-Advocacy Emerging
Child can indicate (verbally, gesture, or AAC) when they need sensory input.
✅ Regulatory Flexibility
Child accepts 3+ different materials from the toolkit. Multiple pathways to regulation established.
✅ Generalization
Toolkit use spreading to new settings: grandparents' home, in the car, at school. Child requests a specific material by name or picture.
Mastery Phase
Weeks 5–8: independent use emerging in multiple contexts.
🏆D-362 Mastery Unlocked: Child has used toolkit independently in at least 3 different settings over 2 consecutive weeks.
Next steps:✅ Stay if mastery is emerging but not stable (reinforce 2 more weeks) | ✅ Progress to D-363 Rocking & Swaying | ✅ Deepen with material deep-dive protocols
Next steps:✅ Stay if mastery is emerging but not stable (reinforce 2 more weeks) | ✅ Progress to D-363 Rocking & Swaying | ✅ Deepen with material deep-dive protocols
PMC10955541 (2024): Sensory integration therapy across 24 studies showed effective promotion with measurable outcomes | BACB mastery criteria standards

You Did This. Your Child Grew Because of Your Commitment.
🧠 You Learned the Neuroscience
Why your child flaps — and what their nervous system truly needs.
🧰 You Built the Toolkit
A personalized sensory toolkit from 9 categories of therapeutic materials.
🏠 You Ran a Clinic at Home
A clinical-grade protocol, consistently executed without a clinic.
📊 You Recorded the Journey
Data that now tells a real story of progress, not guesswork.
Your child's nervous system didn't change overnight. But your understanding of it did. And that understanding is the most powerful therapy tool in this entire toolkit.
Mark this milestone in a way your family values. A special meal. A photo of your child with their sensory toolkit. A journal entry. A message in the Pinnacle parent community.
📸Family Photo Prompt: "Take a photo of your child's sensory toolkit. In 6 months, share it with another parent who is where you were at Week 1."

Trust Your Instincts. If Something Feels Wrong — Pause and Ask.
🚩 Self-Injurious Behavior Accompanying Flapping
What it looks like: Child bites their own hands, hits head, bangs wrists during or after flapping.
Why it matters: Self-injury changes the clinical picture entirely — the sensory need may be more intense or the function may be different.
What to do: Stop home protocol. Contact OT/BCBA for functional behavior assessment.
Why it matters: Self-injury changes the clinical picture entirely — the sensory need may be more intense or the function may be different.
What to do: Stop home protocol. Contact OT/BCBA for functional behavior assessment.
🚩 Sudden Onset or Dramatic Change in Stereotypy Pattern
What it looks like: Flapping that was stable suddenly increases, or new body parts involved.
Why it matters: Change can signal medical cause, medication effect, or significant anxiety increase.
What to do: Teleconsult with developmental pediatrician before continuing.
Why it matters: Change can signal medical cause, medication effect, or significant anxiety increase.
What to do: Teleconsult with developmental pediatrician before continuing.
🚩 Flapping Accompanied by Significant Regression
What it looks like: Language loss, loss of previously acquired skills, withdrawal alongside increased stereotypy.
Why it matters: Regression + increased stereotypy = medical evaluation priority.
What to do: Pause all behavioral interventions. Seek urgent developmental pediatrician review.
Why it matters: Regression + increased stereotypy = medical evaluation priority.
What to do: Pause all behavioral interventions. Seek urgent developmental pediatrician review.
🚩 Skin, Circulation, or Pain Response to Materials
What it looks like: Redness, numbness, bruising, or child guarding hands after material use.
What to do: Discontinue that specific material. Teleconsult with OT for material adjustment.
What to do: Discontinue that specific material. Teleconsult with OT for material adjustment.
🚩 Caregiver Unable to Continue
What it looks like: Parent exhaustion, significant anxiety, inability to regulate own emotions during sessions.
Why it matters: Parent regulation is prerequisite for child regulation.
What to do: Pause sessions. Contact helpline for caregiver support resources.
Why it matters: Parent regulation is prerequisite for child regulation.
What to do: Pause sessions. Contact helpline for caregiver support resources.
🚩 No Progress After 8 Weeks of Consistent Protocol
What it looks like: Engagement consistently below 2/5, no behavior change documented.
Why it matters: This material set may not match this child's sensory profile. OT assessment needed.
What to do: Book AbilityScore® assessment. OT sensory processing evaluation.
Why it matters: This material set may not match this child's sensory profile. OT assessment needed.
What to do: Book AbilityScore® assessment. OT sensory processing evaluation.
Escalation Pathway: Self-resolve → 📞 Helpline teleconsult → Pinnacle center clinic visit → Specialist referral
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7
WHO NCF: Primary health care as platform for early identification | Pinnacle clinical escalation protocols | AOTA safety monitoring guidelines
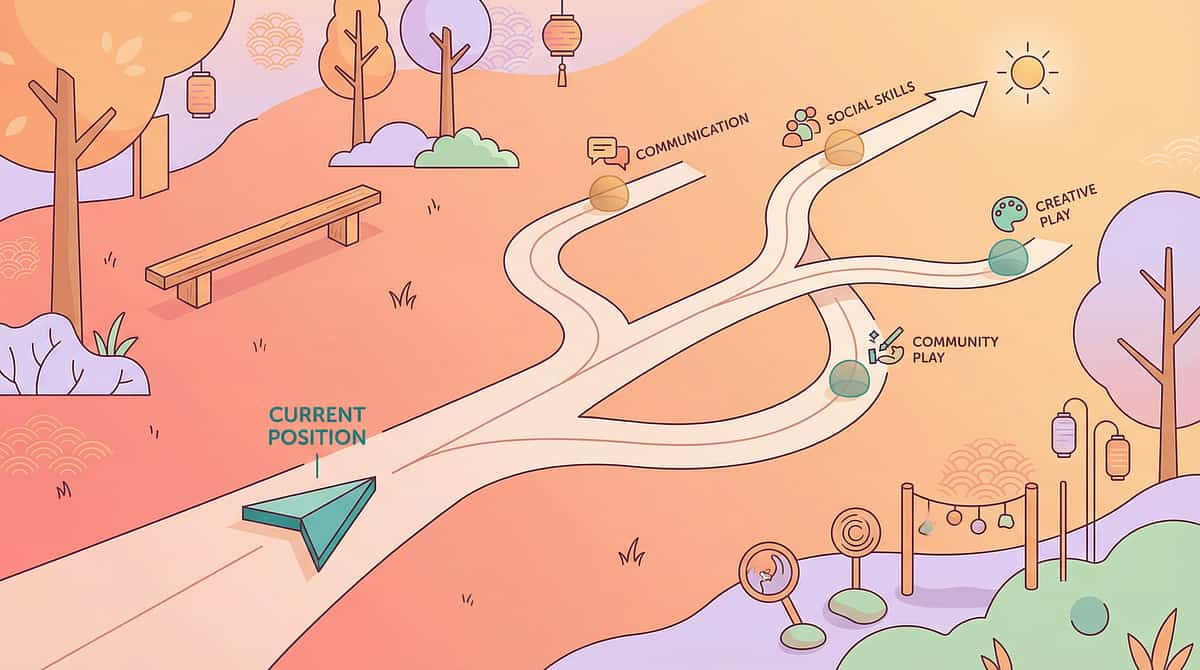
You Are Not Done. You Are On a Journey With a Clear Forward Path.
Completing D-362 doesn't close a chapter — it opens a pathway. Your child's sensory regulation toolkit is now the foundation for the next level of growth.
If flapping is the primary challenge
→ D-363 Rocking and Swaying (similar proprioceptive profile, materials you already own)
If environments are the primary trigger
→ D-364 Sensory Overload Management
If toolkit is working but needs systematizing
→ D-370 Full Sensory Diet Design
If school generalization is the goal
→ D-365 Generalization Across Settings
Long-Term Developmental Goal: This technique feeds into: Sensory Regulation Readiness Index → Body Awareness Readiness Index → Self-Regulation Readiness Index → Environmental Participation Readiness Index
WHO Developmental Milestones Framework + domain-specific sequencing literature | GPT-OS® developmental trajectory mapping
Because Sensory Regulation Is a System — Not a Single Technique
Technique | Code | Difficulty | Materials You Own | |
9 Materials for Rocking & Swaying | D-363 | 🔵 Core | Weighted bands, heavy work kit | |
Sensory Overload Management | D-364 | 🟡 Advanced | Compression gloves, fidgets | |
Transition Preparation Tools | D-360 | 🟢 Intro | Fidgets, visual timers | |
Environmental Structure | D-361 | 🟢 Intro | Sensory bins, calm space setup | |
Sensory Diet Planning | D-370 | 🟡 Advanced | All 9 materials from D-362 | |
Generalization Across Settings | D-365 | 🟡 Advanced | Portable kit from D-362 |
✅ If you have completed the D-362 toolkit — you are 90% equipped for D-363, D-364, and D-370 without any additional purchases.
→ Browse all Domain D: Behavior & Self-Regulation techniques at techniques.pinnacleblooms.org/behavior-regulation
This Technique Is One Piece. Here Is the Whole Picture.
Domain D Encompasses
Motor stereotypy management • Behavioral flexibility • Self-regulation • Sensory diet integration • Transition readiness • Environmental adaptation. D-362 addresses the sensory-seeking dimension of Domain D.
🧠 GPT-OS® AbilityScore® Integration
The GPT-OS® AbilityScore® assessment maps your child across all 12 domains, identifies which 40-card technique pages are most relevant to your child's current developmental needs, and tracks progress across all domains simultaneously.
→ pinnacleblooms.org — Book AbilityScore® Assessment
The 12 domains align with WHO/UNICEF Nurturing Care Framework's five components: health, nutrition, responsive caregiving, security/safety, and early learning.
WHO NCF (2018): Five nurturing care components require holistic monitoring | UNICEF 2025 Country Profiles (42 indicators per country) | PMC9978394
ACT V: THE COMMUNITY & ECOSYSTEM
From the Clinic Notes. Real Families. Real Outcomes.
Vignette 1 — From the Therapist's Notes
Before (Week 0): Arjun, 5 years, flapped his hands continuously — at meals, during car rides, in class, at the grocery store. His parents had tried holding his hands down, offering distractions, and multiple types of redirection over 2 years. His OT at Pinnacle noted: "He's not dysregulated because of the flapping. He's regulated BY the flapping. Our goal is to expand his toolkit, not eliminate his coping mechanism."
After (Week 8): Arjun independently reaches for his resistance putty before school each morning. During excited moments he still flaps — and that is celebrated. During homework and car rides, the putty has become his default. His OT reports: "He uses three toolkit materials independently. We've shifted from 'stop flapping' to 'what does Arjun need right now?' And he's starting to tell us."
(Anonymized case. Identifying details changed. Outcomes vary.)
(Anonymized case. Identifying details changed. Outcomes vary.)
Vignette 2 — Parent Report
Before:"My daughter flapped whenever she was excited. Family gatherings were exhausting — relatives commenting, me constantly apologizing. I felt like I was always managing everyone else's discomfort instead of supporting her."
After (Week 12):"We built a sensory kit for events — a small bag with her fidget, a piece of putty, and compression gloves. She chooses what she needs. She still flaps when she's really excited. But now she also has options. And I've stopped apologizing. Her nervous system is doing exactly what it's supposed to do."
(Parent, Pinnacle Network. Anonymized.)
(Parent, Pinnacle Network. Anonymized.)
"The most common turning point we see: the moment a parent stops asking 'how do I make the flapping stop?' and starts asking 'what does my child need right now?' That shift in question changes everything." — Pinnacle OT Consortium
📞FREE Helpline: 9100 181 181 | 16+ Languages | 24×7
Qualitative research on parent motivation: Peer narratives strongest motivator for home-based intervention adherence | Pinnacle center outcome data, anonymized

Isolation Is the Enemy of Adherence. You Are Not Meant to Navigate This Alone.
💬 Pinnacle Parent WhatsApp Community
Hand Flapping & Sensory Regulation Support Group. Active parents. OT moderation. Real questions, real answers.
→ pinnacleblooms.org/community/sensory-regulation
→ pinnacleblooms.org/community/sensory-regulation
🌐 Online Parent Forum
Pinnacle Blooms Parent Network — Sensory Domain. Share your D-362 progress. Ask questions. Read others' journeys.
→ pinnacleblooms.org/forum/domain-d
→ pinnacleblooms.org/forum/domain-d
📍 Local Parent Meetup
Pinnacle center-organized parent meetups in your city. Monthly meetups at most centers. Ask when you call.
→ pinnacleblooms.org/centers
→ pinnacleblooms.org/centers
🤝 Peer Mentoring
Connect with an experienced parent who has navigated hand flapping. Lived experience paired with clinical support.
→ Request mentor: 9100 181 181
→ Request mentor: 9100 181 181
"Your journey through D-362 will become the map for another parent who is where you were at Week 1. Consider sharing your story."
WHO NCF: Community engagement as core principle | Parent support networks improve intervention outcomes and adherence across all studies reviewed
Home + Clinic = Maximum Impact. The Toolkit Is More Powerful When Designed By a Professional.
🗺️ Find Your Nearest Pinnacle Center
70+ centers across India. Each operating under GPT-OS® clinical standards. All centers offer OT assessment for sensory processing profiles.
→ pinnacleblooms.org/centers
→ pinnacleblooms.org/centers
Therapist Matching — D-362 Relevant
This technique's primary discipline is Occupational Therapy. Request an OT with: Sensory Integration certification + Experience with motor stereotypies.
📞 Book OT consultation: 9100 181 181
📞 Book OT consultation: 9100 181 181
Teleconsultation for Remote Families
Can't reach a center? Our teleconsultation service brings OT guidance to your screen. Available: All states. 16+ languages. GPT-OS® session guided.
→ pinnacleblooms.org/teleconsult
→ pinnacleblooms.org/teleconsult
What a Professional OT Adds to Your Home Protocol
- Standardized sensory processing assessment — not guesswork
- Precise material intensity matching to your child's profile
- Sensory diet design across all 12 hours of your child's waking day
- School consultation and teacher coordination
- AbilityScore® progress tracking across all 12 domains
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7
No appointment needed for the helpline. Call to discuss, then book.
No appointment needed for the helpline. Call to discuss, then book.
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies | Primary health care as key platform for reaching all families
Deeper Reading for the Curious Parent. Every Material on This Page Has a Study Behind It.
PRISMA Systematic Review (2024) — PMC11506176
16 studies (2013–2023) confirm sensory integration meets evidence-based practice criteria for ASD. Population: Children 2–12 with autism. Evidence Level: I
Meta-Analysis, World J Clin Cases (2024) — PMC10955541
Effective promotion of social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. Evidence Level: I
Indian RCT, Padmanabha et al. (2019)
Significant sensory and behavioral outcomes in home-delivered protocol in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4 (Indian J Pediatr). Evidence Level: II
NCAEP Evidence-Based Practices Report (2020)
Sensory-based interventions classified as established EBP for autism spectrum disorder. ncaep.fpg.unc.edu. Evidence Level: Consensus
Frontiers in Integrative Neuroscience (2020)
Neurological basis for sensory-based interventions established with measurement framework. DOI: 10.3389/fnint.2020.556660. Evidence Level: II
All citations above + WHO NCF (2018) + UNICEF CCD Package (2023) + PMC9978394 + OCEBM Levels of Evidence applied throughout this page
Your Data Helps Every Child Like Yours. Here Is Exactly How.
🔒 Privacy Assurances
• All session data anonymized before entering population analytics
• Individual child data never shared with third parties
• DPIIT-registered data practices: DIPP8651 (Govt. of India)
• Compliant with IT Act 2000 and Digital Personal Data Protection Act 2023
• Individual child data never shared with third parties
• DPIIT-registered data practices: DIPP8651 (Govt. of India)
• Compliant with IT Act 2000 and Digital Personal Data Protection Act 2023
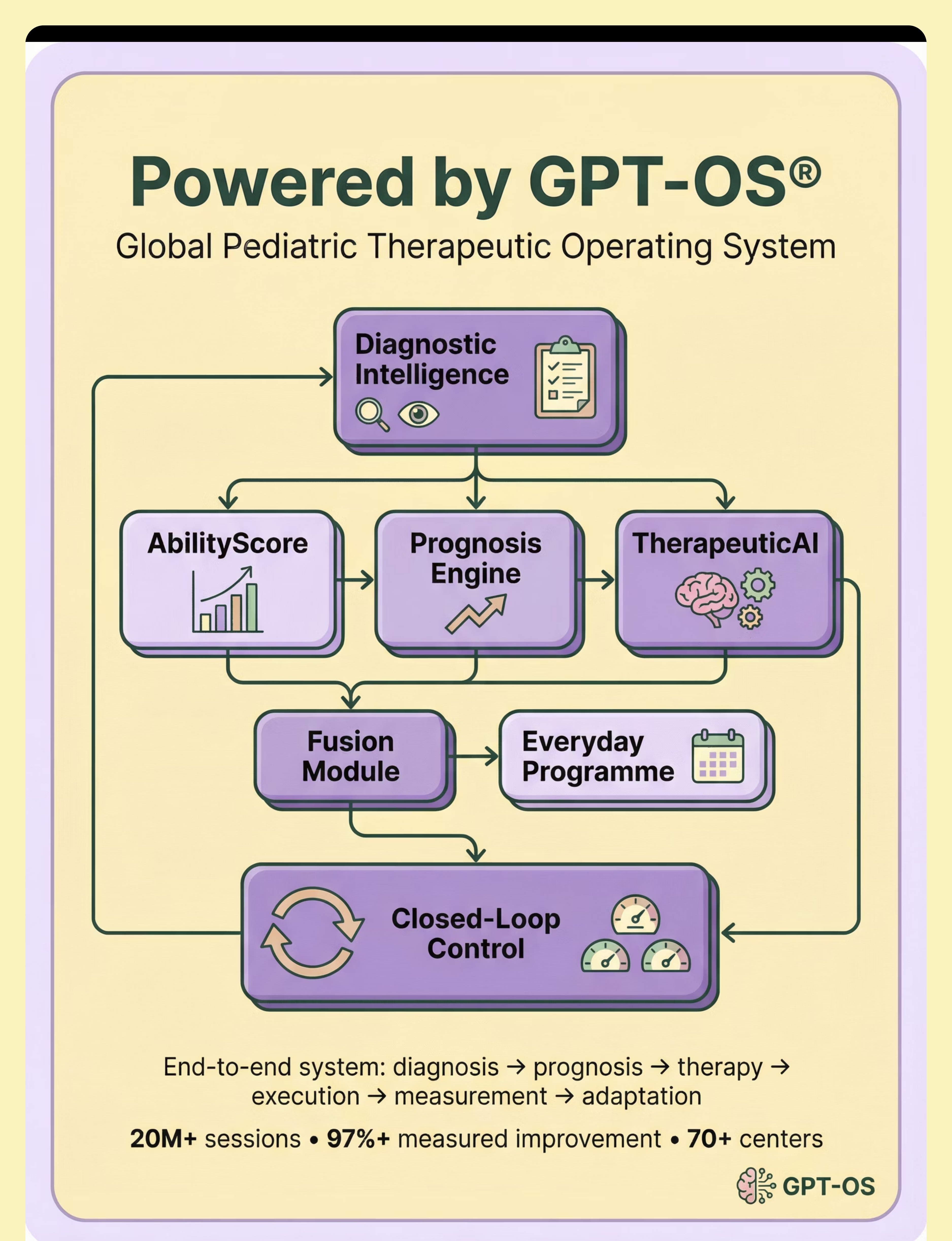
GPT-OS® Stack Involved in D-362
- Diagnostic Intelligence: Sensory processing profile identification
- TherapeuticAI®: Material-to-profile matching algorithms
- EverydayTherapyProgramme™: Daily sensory diet embedding
- Prognosis Engine: 8-week outcome trajectory based on response data
- Closed-Loop Control: Session data → plan → re-measure → adapt
Digital health ASD RCTs (2024): 21 RCTs, 1,050 participants | Gamified digital health interventions for ASD show measurable promise | Pinnacle 20M+ session data infrastructure
D-362 — Watch the Reel That Started This Journey
📹 Reel ID: D-362
9 Materials That Help With Hand Flapping
📚 Series
Sensory & Self-Regulation Support — Episode 362
⏱️ Duration
75–85 seconds | Captions in 16 languages
🎯 Domain
D — Behavior & Self-Regulation
Presented by the Pinnacle Blooms OT Consortium. This Reel was designed, reviewed, and validated by: Pediatric Occupational Therapists (Sensory Integration Specialists) • Board Certified Behavior Analysts (Motor Stereotypy Focus) • Child Developmental Pediatricians • Special Educators (Classroom implementation specialists) • Parents and Caregivers (Content validation panel).
This web page is the deep-dive companion to the 75-second Reel. Everything the Reel shows — this page explains, evidences, and operationalizes into a protocol you can execute at home. Watch at: pinnacleblooms.org/reel/D-362
NCAEP 2020: Video modeling is evidence-based practice for autism | Multi-modal learning (visual + text + demonstration) improves parent skill acquisition

Consistency Across Caregivers Multiplies Impact. One Parent Implementing Is Good. A Whole Family Is Transformative.
Share This Page
📱WhatsApp — Share this page with your support network
📧Email — Send to school teacher, grandparents, doctor
🔗Copy Link — techniques.pinnacleblooms.org/behavior-regulation/hand-flapping-materials-D-362
📧Email — Send to school teacher, grandparents, doctor
🔗Copy Link — techniques.pinnacleblooms.org/behavior-regulation/hand-flapping-materials-D-362
📄 D-362 Family Guide (1-page PDF)
The complete sensory toolkit for hand flapping in 1 page — for grandparents, teachers, and all caregivers.
→ pinnacleblooms.org/resources/D-362-family-guide
→ pinnacleblooms.org/resources/D-362-family-guide
"Explain to Grandparents" Version
"[Child's name] sometimes flaps their hands when excited or overwhelmed. This is their nervous system asking for sensory input — not misbehavior. When you see it, please don't hold their hands down. Instead, offer them their sensory putty or fidget toy from the bag I've packed. These materials give their brain what it needs. We're building their ability to self-regulate. Your support makes this work."
Teacher/School Communication Template
"Dear [Teacher name], [Child's name] has been working with our OT on a sensory diet that includes 9 specific materials for proprioceptive regulation. Hand flapping is a sensory-seeking behavior, not a behavioral challenge. I'd like to schedule a 15-minute consultation to discuss classroom accommodations — fidgets at the desk, compression gloves during focused work, and heavy work breaks before demanding tasks."
WHO CCD Package: Multi-caregiver training critical for intervention generalization and maintenance | PMC9978394
ACT VI: THE CLOSE & LOOP
Every Question a Parent Has Asked — Answered.
Q: My child's hand flapping is constant. Is that too severe for home intervention?
High-frequency flapping indicates high sensory need — not that home intervention is inappropriate. It means the sensory diet needs to be comprehensive and consistent. Start with the 3-item starter kit (putty, fidget, heavy work) and contact our helpline for OT guidance. 📞9100 181 181
Q: Should I try to stop the flapping entirely?
The neurodiversity-affirming and clinically supported answer is no. The goal is not elimination — it is expanding options. Many children who have a robust sensory toolkit continue to flap when excited or overwhelmed, and that is healthy. The difference is that flapping is no longer their only tool.
Q: My child is 10. Is it too late to build a sensory toolkit?
Not at all. Sensory needs don't have an expiry date. Older children can actually benefit more — they can participate in choosing their own materials, understanding their sensory state, and developing self-advocacy language.
Q: The school won't allow fidgets in the classroom. What do I do?
Compression gloves and weighted wrist bands are invisible — they provide proprioceptive input without any visible "fidgeting." Both are clinically appropriate classroom accommodations. Use the teacher communication template in Card 37 to initiate a school consultation.
Q: My child chews or mouths the materials. Is that safe?
Do not use putty or small fidgets if mouthing is a concern — switch to oral motor tools designed for this purpose. Contact an OT to assess whether oral-seeking is part of your child's profile and which materials are safe and appropriate.
Q: How long before I see results?
Weeks 1–2: tolerance and early engagement. Weeks 3–4: consolidation and preference. Weeks 5–8: independent use in some contexts. Consistent data tracking (Card 20) is the most reliable way to see actual progress rather than relying on impression.
Q: Hand flapping increased after I started the toolkit. Did I do something wrong?
A temporary increase in flapping after introducing new sensory materials is common. Change to the sensory environment — even positive change — can initially increase arousal. Stay consistent for 2 more weeks and track the data. If the increase continues beyond 3 weeks, contact an OT. See Card 21 for session-level troubleshooting.
Q: Can my child use the sensory toolkit at school without an OT's sign-off?
For most of the 9 materials (fidgets, sensory bins, massage tools) — yes, parental discretion applies. For weighted materials — OT guidance on weight and duration is recommended. When in doubt, call the helpline before introducing weighted items. 📞9100 181 181
FAQ content derived from Pinnacle clinical FAQ database, parent community queries at 70+ centers, and OT consortium clinical notes

You Have Everything You Need to Begin. The Only Step Left Is the First One.
🚀 Start D-362 Today
GPT-OS® Session Launcher — guided step by step through your first sensory toolkit session.
📞 Book Free OT Consultation
9100 181 181 | FREE National Autism Helpline. Get a personalized sensory profile assessment. 16+ Languages • 24×7 • FREE
→ Explore D-363 Next
9 Materials That Help With Rocking & Swaying. You already own most of the materials. One click away.
📞9100 181 181 | FREE National Autism Helpline
Available in: Telugu, Hindi, Tamil, Kannada, Malayalam, Bengali, Marathi, Gujarati, Punjabi, Odia, Assamese, Urdu, English + 3 more. No registration. No appointment. Just call.
Available in: Telugu, Hindi, Tamil, Kannada, Malayalam, Bengali, Marathi, Gujarati, Punjabi, Odia, Assamese, Urdu, English + 3 more. No registration. No appointment. Just call.
Pinnacle Blooms Consortium — Validated by Expert Consortium | OT • SLP • ABA • SpEd • NeuroDev • CRO • WHO/UNICEF Aligned | 20M+ Sessions • 97%+ Improvement
Preview of 9 materials that help with hand flapping Therapy Material
Below is a visual preview of 9 materials that help with hand flapping therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

From Fear to Mastery. One Technique at a Time. — The Pinnacle Blooms Consortium
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, personalized, multi-disciplinary pediatric therapy environment — accessible to every family, regardless of geography or income, through the power of the GPT-OS® Global Pediatric Therapeutic Operating System.
🔄 Return to Top
Begin again with Card 01 — recognition grounds every visit.
➡️ Next: D-363
9 Materials That Help With Rocking & Swaying — your toolkit is already 90% ready.
🏠 Browse All Techniques
techniques.pinnacleblooms.org — 999 evidence-based technique pages
📞 Get Help Now
9100 181 181 | FREE | 16+ Languages | 24×7
Medical Disclaimer: This content is educational and does not replace individualized assessment with licensed occupational therapists, behavior analysts, or developmental specialists. Hand flapping and motor stereotypies can be associated with various conditions; professional evaluation is recommended. The goal is not elimination of all stereotypy but supporting regulation and expanding options. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Always consult qualified healthcare professionals before implementing therapeutic protocols.
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 (Govt. of India — Startup India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network® | A unit of Bharath Healthcare Laboratories Pvt. Ltd. | Content developed under GPT-OS® Content Engine | Technique Code: D-362 | Published: techniques.pinnacleblooms.org/behavior-regulation/hand-flapping-materials-D-362
← D-361: Environmental Structure | → D-363: 9 Materials That Help With Rocking & Swaying
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7