
When the dark becomes the enemy.
And bedtime becomes a two-hour war you didn't ask for.
It's 11 PM. You've checked under the bed four times. You've shown her the empty closet. You've left two nightlights on and the hallway light blazing. But she's still at your bedroom door — shivering. Not from cold. From fear. You found her there at 3 AM last week too, having slept on the floor rather than call for you, too scared to stay in her room and too small to ask for help.
You are not failing. Your child's nervous system is doing exactly what it was designed to do — it just needs the right tools to feel safe.
C-284
Ages 2–10
Emotional Regulation & Anxiety Support — Episode 284

This Is Not Rare. This Is Not Your Fault.
Fear of the dark (nyctophobia) is one of the most common childhood fears globally. It typically emerges between ages 2–6 when symbolic thinking develops — the same cognitive leap that enables language, play, and creativity. The brain can now imagine monsters. It cannot yet reliably prove they don't exist. You are among tens of millions of families navigating this exact challenge tonight.
43%
Children Affected
of children aged 3–8 experience fear of the dark significant enough to affect sleep
73M
Children in India
children aged 2–10 in India — the primary age window when fear of the dark emerges and peaks
2–6
Peak Age Window
years old — when imagination develops faster than the ability to distinguish imagined threats from real ones
"The imagination that creates monsters in the dark is the same imagination that will one day create stories, solve problems, and build worlds. It's a feature, not a bug — it just needs time and support." — Pinnacle Blooms Consortium, Behavioral Psychology Lead

What's Happening in Your Child's Brain
The Neuroscience of Darkness Fear
What the amygdala does
The amygdala is the brain's alarm system. When lights go off, it receives an ambiguous signal: no visual confirmation of safety. For young children, whose prefrontal cortex is still 15–20 years from full development, the alarm fires: DANGER. THREAT. PANIC.
Why logic doesn't work
The amygdala's fear response bypasses the rational prefrontal cortex. "There are no monsters" is processed in a different brain region from where the fear lives. Showing your child an empty closet doesn't stop the fear — reassurance and fear are having different conversations in different rooms of the brain.
The Developmental Mismatch
Imagination (vivid, fear-capable): Develops from ages 2–4 ✓
Reality-testing (fear-override): Develops fully by ages 8–10 ⏳
The gap years: Ages 4–8 are when fear of the dark is most intense.
Reality-testing (fear-override): Develops fully by ages 8–10 ⏳
The gap years: Ages 4–8 are when fear of the dark is most intense.
What Helps
Evidence-based tools work by reducing amygdala activation (environmental control, sensory anchors) and building prefrontal regulation capacity (graduated exposure, cognitive tools). They work with the developing brain — not against it.
Research: Frontiers in Integrative Neuroscience (2020), DOI 10.3389/fnint.2020.556660

Where This Sits in Development
Your child's fear of the dark isn't a behavior problem. It's a predictable consequence of healthy cognitive growth — and it has a natural developmental arc.
0–24 months
Separation anxiety begins; imagination starts; first imaginative fears possible
⚡ Ages 2–4
Fear of dark emerges — symbolic thinking develops; monsters become imaginable; dark = unsafe
🔥 Ages 4–6
Peak intensity — imagination vivid; reality-testing limited; fear most intense and most common
Ages 6–8
Cognitive tools developing; fear begins responding to reason; graduated exposure most effective
Ages 8–10+
Reality-testing matures; fear naturally diminishes; persistence past age 10 warrants clinical support
Where Your Child Is: This is developmentally normal. Fear of the dark at ages 2–10 is not a pathology — it's a predictable consequence of healthy cognitive development. The goal is not to rush the brain to maturity. The goal is to build coping capacity to bridge the gap while the brain matures naturally.
The Science Supporting These 9 Materials
Level II–III Evidence
Systematic Reviews · RCTs · Clinical Consensus
These materials aren't guesswork. Every element of the Dark Safety Toolkit is grounded in peer-reviewed research and clinical validation across thousands of pediatric cases. Here's the evidence behind the approach.
PMC3018839
Childhood Phobias & Evidence-Based Treatments
Graduated exposure is the most effective evidence-based treatment for specific phobias in children, including fear of the dark. Strong outcomes in ages 3–12.
Graduated exposure is the most effective evidence-based treatment for specific phobias in children, including fear of the dark. Strong outcomes in ages 3–12.
PMC11506176
PRISMA Systematic Review (2024)
Multimodal interventions show superior outcomes vs. single-modality approaches. 16 studies reviewed, 2013–2023.
Multimodal interventions show superior outcomes vs. single-modality approaches. 16 studies reviewed, 2013–2023.
PMC10955541
Meta-Analysis (2024)
24 studies, 1,050+ participants. Combined sensory-behavioral interventions effectively promote adaptive behavior and anxiety management.
24 studies, 1,050+ participants. Combined sensory-behavioral interventions effectively promote adaptive behavior and anxiety management.
AAP Guidelines
Healthy Sleep Guidelines
Environmental modifications are first-line recommendations for childhood bedtime anxiety. Graduated independence is preferred over eliminating all supports.
Environmental modifications are first-line recommendations for childhood bedtime anxiety. Graduated independence is preferred over eliminating all supports.
NCAEP 2020
Evidence-Based Practices Report
Behavioral reinforcement strategies (bravery charts, token economies) classified as evidence-based practice for pediatric anxiety.
Behavioral reinforcement strategies (bravery charts, token economies) classified as evidence-based practice for pediatric anxiety.

The Technique — What It Is
🌙 Materials-Based Fear Desensitisation for Nyctophobia
"The Dark Safety Toolkit"
A multi-material, graduated intervention approach for childhood fear of the dark that works by: (1) modifying the environment to provide appropriate sensory anchors, (2) externalising fear through play-based tools, (3) building progressive tolerance through graduated exposure, and (4) reinforcing brave behaviour through systematic tracking. This is not one technique — it is a coordinated ecosystem of 9 evidence-anchored materials that parents deploy in sequence, matching each tool to the child's current fear level and developmental stage.
Domain
Emotional Regulation & Anxiety
Age Range
2–10 years
Duration
20–45 min nightly bedtime routine
Frequency
Every bedtime — consistency is the treatment
Who It's For: Children aged 2–10 with fear of the dark or bedtime anxiety ranging from mild reluctance to severe nyctophobia, including children with autism, anxiety disorders, sensory sensitivities, or developmental differences.

This Technique Crosses Therapy Boundaries
"Your child's brain doesn't organise itself by therapy type. Neither do these materials."
Behavioral Psychologist / ABA Therapist
Primary Lead. Applies graduated exposure protocols, designs the exposure hierarchy, trains parents in reinforcement procedures, monitors anxiety response data, and determines pacing for each step.
Occupational Therapist (OT)
Sensory Environment Lead. Selects appropriate nightlight color temperatures and brightness levels based on sensory profile, addresses sensory sensitivities, and optimises the bedroom sensory environment — critical for children with ASD.
Special Education Therapist
Visual Supports Lead. Creates visual schedules for the bedtime routine, designs concrete fear ladders appropriate to cognitive level, develops social stories, and ensures all tools are accessible for children with communication differences.
Neuro-Developmental Pediatrician
Medical Context Lead. Rules out medical contributors, assesses for co-occurring anxiety disorders, evaluates whether fear of the dark is part of a broader clinical profile, and coordinates escalation pathways.
"I thought I needed to see a different specialist for each thing — the OT for the sensory stuff, the psychologist for the anxiety, the developmental doctor for the autism. Pinnacle showed me these all feed into the same bedtime problem from different angles." — Parent, Pinnacle Network
Precision Targets — Not a Random Activity
Every material in the toolkit aims at specific, observable outcomes. Here's exactly what you're working toward — from immediate sleep wins to long-term resilience.
Observable success indicators: ✅ Child kisses goodnight without crying or negotiating ✅ Child stays in bed when they wake at night ✅ Child enters dark hallways without requiring adult escort ✅ Child uses coping tools spontaneously ✅ Anticipatory anxiety disappears — child doesn't dread sunset

The 9 Materials — Your Complete Dark Safety Toolkit
Every material below has been selected, tested, and validated by the Pinnacle Blooms Consortium. All are available in India. Most cost less than a single therapy session. All can be implemented tonight.
🌟 Adjustable Nightlight with Dimmer
Role: Environmental control — graduated light reduction over weeks
Price: ₹500–2,500 | Dimmable LED · Smart bulb · Red/amber spectrum
Price: ₹500–2,500 | Dimmable LED · Smart bulb · Red/amber spectrum
👾 Worry Monster / Fear Eater Toy
Role: Fear externalisation — child feeds written/drawn fears into the monster's mouth
Price: ₹400–1,500 | Commercial zippered toy · DIY worry box · Worry dolls
Price: ₹400–1,500 | Commercial zippered toy · DIY worry box · Worry dolls
⭐ Glow-in-the-Dark Stars (Ceiling Stickers)
Role: Visual transformation — turns dark ceiling from threat to beautiful sky
Price: ₹200–1,000 | Stick-on stars · Glow projector · Glow-in-dark paint
Price: ₹200–1,000 | Stick-on stars · Glow projector · Glow-in-dark paint
📖 Therapeutic Storybooks (Fear of Dark theme)
Role: Bibliotherapy — child sees characters like them overcome the same fear
Price: ₹200–800 | "The Dark" (Snicket) · "Can't You Sleep, Little Bear?" · "The Owl Who Was Afraid of the Dark"
Price: ₹200–800 | "The Dark" (Snicket) · "Can't You Sleep, Little Bear?" · "The Owl Who Was Afraid of the Dark"
🧸 Comfort Object / Security Item
Role: Transitional security — brave companion that stays with child through the night
Price: ₹200–1,500 | Stuffed animal · Weighted comfort toy · Parent-scented item
Price: ₹200–1,500 | Stuffed animal · Weighted comfort toy · Parent-scented item
🔦 Child-Safe Flashlight / Tap Light
Role: Agency restoration — "I can make light whenever I need it"
Price: ₹100–600 | Child-friendly flashlight · Tap light · Squeeze-activated light
Price: ₹100–600 | Child-friendly flashlight · Tap light · Squeeze-activated light
🎵 White Noise / Calming Audio Device
Role: Auditory safety — fills the silence that fear loves to inhabit
Price: ₹300–2,000 | White noise machine · Nature sounds · Bluetooth speaker + Moshi / Calm app
Price: ₹300–2,000 | White noise machine · Nature sounds · Bluetooth speaker + Moshi / Calm app
🌟 Bravery Chart / Sticker Reward System
Role: Progress visibility — makes invisible courage visible and celebrated
Price: ₹100–500 | Sticker chart · Token board · Reward jar
Price: ₹100–500 | Sticker chart · Token board · Reward jar
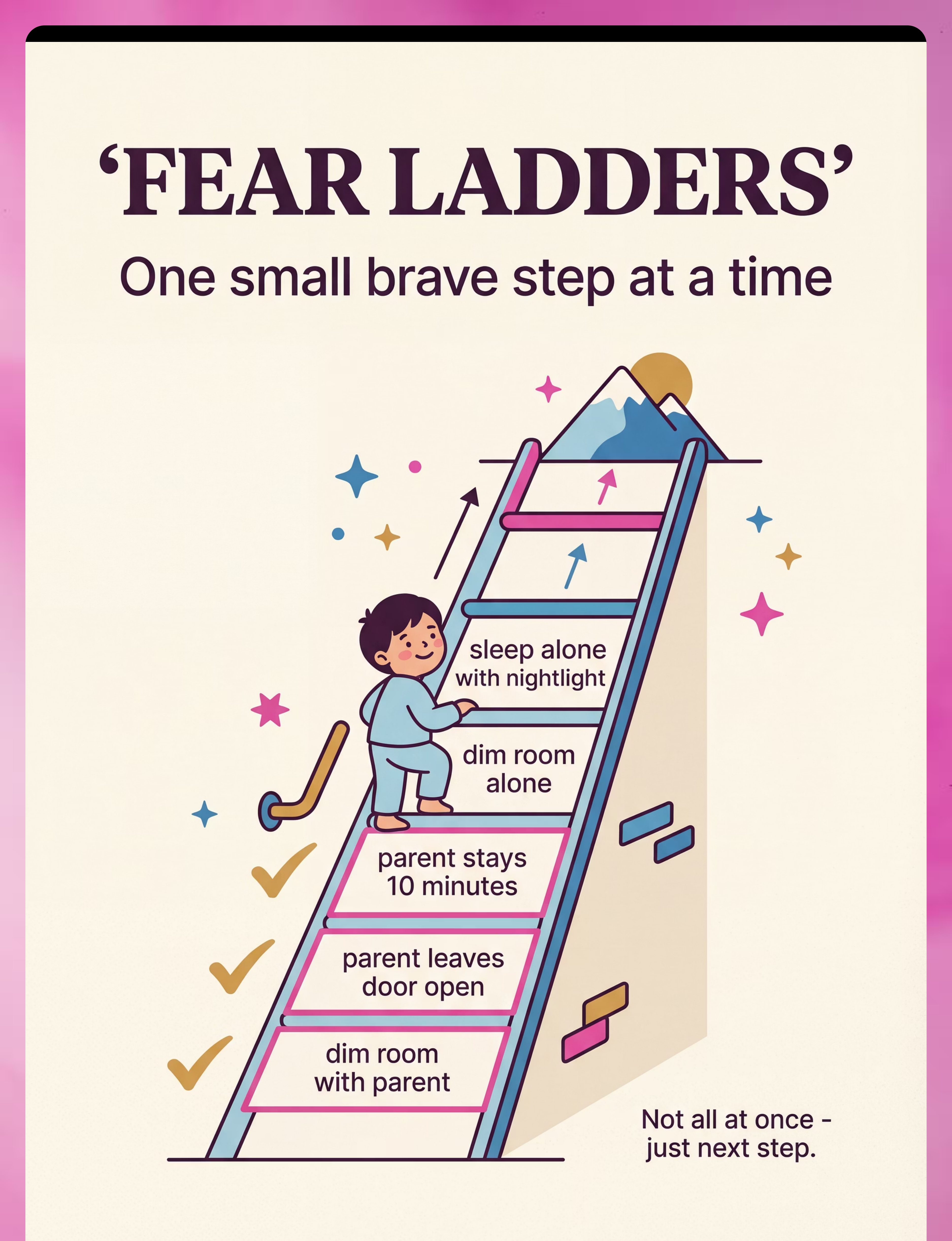
🪜 Fear Ladder / Graduated Exposure Worksheet
Role: Structured desensitisation — one small brave step at a time
Price: ₹100–400 | Fear ladder worksheet · Visual hierarchy chart · Brave challenge cards
Price: ₹100–400 | Fear ladder worksheet · Visual hierarchy chart · Brave challenge cards
Total Starter Kit Estimate: ₹1,400–8,700 for all 9 materials. Essential 4-Item Starter Kit: Adjustable nightlight + comfort object + one storybook + bravery chart = ₹1,000–5,300. Pinnacle Recommends badges indicate clinically validated products reviewed by our Consortium.
Zero-Cost Versions — Because Every Family Deserves Access
WHO/UNICEF Equity Principle: Evidence-based intervention should not be gatekept by cost. Every material in this toolkit has a zero-cost or near-zero-cost alternative that works on the same therapeutic principle.
Buy: Adjustable Nightlight (₹500–2,500)
Make: Any lamp + app-controlled smart bulb (₹200 bulb). Or layer multiple low-watt bulbs. Or red/orange cellophane over a regular bulb. The mechanism is graduated dimming, not the product brand.
Buy: Worry Monster (₹400–1,500)
Make: Old pillowcase + needle/thread + 10 minutes = personalised worry monster. Or a decorated shoebox. Or a plain envelope with child's drawing on the front. The ritual of externalising fear matters more than the product.
Buy: Glow Stars (₹200–1,000)
Make: Glow-in-dark paint (₹150 tube) applied in star patterns with child's paintbrush. Special ritual: Charge the glow together with a torch before lights-out. Build this into the routine.
Buy: Therapeutic Storybook (₹200–800)
Make: Create a personalised story featuring YOUR child as the brave character — with photos of their actual room, bed, and toys. 4–8 pages. Free templates at pinnacleblooms.org/resources. Child sees themselves, not a fictional character, overcoming the fear.
Buy: Comfort Object (₹200–1,500)
Make: The comfort object often chooses itself. Observe what your child already gravitates toward and formalise it. Give an existing beloved toy a "bravery upgrade" through a special story. The ritual of naming the role is free.
Buy: Flashlight (₹100–600)
Make: Any household torch works. For very young children who struggle with buttons: a small glow stick is perfect — no mechanism needed, pure ambient glow. Cost: ₹20–50.
Buy: Calming Audio (₹300–2,000)
Make: A standard household fan provides excellent white noise at zero cost. Or free YouTube/Spotify nature sounds. Or record a parent's voice reading a calming script — personalised guided relaxation your child can play independently.
Buy: Bravery Chart (₹100–500)
Make: A piece of paper + coloured markers + sticker stars (₹30 pack) = fully functional bravery chart. Draw the child's name in big letters, draw 30 squares. Each brave night = one sticker. Zero manufacturing required.
Buy: Fear Ladder (₹100–400)
Make: Hand-draw a ladder on paper with your child. Each rung is one step. Child colours in the rung when they master it. Free download at pinnacleblooms.org/fear-ladder-template.
When is the clinical-grade material non-negotiable? For children with autism, sensory processing disorder, or co-occurring anxiety requiring precise sensory input calibration — nightlight colour temperature and brightness level may require OT guidance. For typical developmental fear of the dark, the DIY versions are clinically equivalent.

Safety Gate — Read Before Starting Any Protocol
Read This First
🔴 STOP — Seek Professional Consultation
These signs indicate the fear may require clinical assessment:
• Fear emerged suddenly after a traumatic event (accident, loss, abuse disclosure)
• Child is experiencing severe panic attacks (hyperventilation, vomiting, loss of bladder control)
• Fear is spreading to ALL dark environments AND also enclosed spaces, crowds, or alone time
• Child has expressed fear of a specific person or thing in their room (potential safeguarding concern)
• Significant regression in other developmental areas simultaneously
• Child is over age 10 and fear is intensifying
Call Pinnacle FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages)
• Fear emerged suddenly after a traumatic event (accident, loss, abuse disclosure)
• Child is experiencing severe panic attacks (hyperventilation, vomiting, loss of bladder control)
• Fear is spreading to ALL dark environments AND also enclosed spaces, crowds, or alone time
• Child has expressed fear of a specific person or thing in their room (potential safeguarding concern)
• Significant regression in other developmental areas simultaneously
• Child is over age 10 and fear is intensifying
Call Pinnacle FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages)
🟡 AMBER — Modify and Consider Professional Support
• Child has co-occurring autism, ADHD, or sensory processing differences → Follow ASD-specific guidance
• Child has generalized anxiety disorder → Slower pacing; professional guidance recommended
• Fear has been present 6+ months without any improvement → Professional functional assessment
• Parents severely sleep-deprived and struggling with consistent implementation → Seek respite support
• Child has generalized anxiety disorder → Slower pacing; professional guidance recommended
• Fear has been present 6+ months without any improvement → Professional functional assessment
• Parents severely sleep-deprived and struggling with consistent implementation → Seek respite support
🟢 GREEN — Safe to Proceed
Environmental safety checklist:
☐ Nightlights positioned safely (no direct eye shine; stable)
☐ Electrical cords managed safely
☐ Comfort objects age-appropriate (AAP safe sleep guidelines)
☐ Flashlight tested; child practises using it during the day
☐ White noise at low volume (child can still hear parent)
☐ Fear ladder steps are child-appropriate
☐ Bravery chart goals are achievable
☐ Nightlights positioned safely (no direct eye shine; stable)
☐ Electrical cords managed safely
☐ Comfort objects age-appropriate (AAP safe sleep guidelines)
☐ Flashlight tested; child practises using it during the day
☐ White noise at low volume (child can still hear parent)
☐ Fear ladder steps are child-appropriate
☐ Bravery chart goals are achievable
STOP IMMEDIATELY if child becomes severely distressed at any point — shaking, vomiting, inability to breathe, prolonged inconsolable crying. Session abandonment is not failure. It is data. Pause, comfort, return to an easier step.

Set Up Your Space — The Optimal Dark Safety Bedroom
Set this up before bedtime, every night. The physical environment IS part of the intervention.
Adjustable Nightlight — Floor level, near the door
Warm amber/red spectrum. Set at current tolerable brightness. NOT pointed at child's eyes. Timer set to dim 30 minutes after expected sleep time if using smart controls.
Flashlight / Tap Light — On the nightstand
Within easy reach of child's hand without needing to sit up. Child has practised finding it in the day. It is THEIR light. They control it. They know where it is.
White Noise Device — On a shelf or dresser, not beside the head
Set to low consistent volume — background, not foreground. Nature sounds or plain white noise preferred. No spoken content at sleep onset.
Comfort Object — On the pillow beside the child
Introduced during the bedtime story as the "brave companion." Child places it themselves as part of the ritual.
Worry Monster — On the nightstand, "on guard"
Child has already fed it their fears during the pre-sleep ritual. It is now guarding the room. Its job is done; the child's fears are contained.
Glow Stars — Above the bed on the ceiling
"Charged" with torch during the bedtime ritual. After lights out, child looks up at the sky their room becomes.
Fear Ladder + Bravery Chart — Visible from the bed
Child can see their progress from where they sleep. Tomorrow morning they add the sticker.
Remove before bedtime: Screens · Toys that create noise/light unexpectedly · Items that cast ambiguous shadows · Anything the child has previously identified as scary. Lighting tip: Begin dimming household lights 30–60 minutes before bedtime. Melatonin production requires absence of blue-spectrum light.

Pre-Flight Check — Is Your Child Ready?
The best session is one that starts right. A child who is overtired, dysregulated, or hungry cannot engage with coping tools. 60 seconds of assessment prevents 2 hours of battle.
Fed?
Child has had a light snack if needed; not hungry, not overfull
Regulated?
No active meltdown in the last 20 minutes; baseline calm. Not past point of extreme overtiredness.
Screened?
No scary content (TV, stories, conversations) in the last hour
Prepared?
Child given 15-minute warning that bedtime is approaching
Connected?
Parent has had 5 minutes of warm, calm, positive interaction with child today
🟢 GO — 4–5 checked
Proceed with full nightly protocol. This is your best opportunity for progress.
🟡 MODIFY — 3–4 checked
Simplified version tonight. Focus on comfort and routine. "Tonight is a cozy night. No brave challenges. Just rest."
🔴 POSTPONE Graduated Work — fewer than 3 checked
Basic bedtime routine only. No exposure steps. Comfort, safety, warm parental presence. Record the triggering factor in your data log. Tomorrow is another opportunity.
Note: Postpone is NOT failure. It is good clinical judgment. The child learns nothing positive from pushed sessions.
Step 1 of 6 — The Invitation
⏱ Timing: 5–10 minutes before lights-out
The Principle: Every protocol begins with an invitation, not a command. The child enters the therapeutic space through warmth, play, and low-demand engagement. Tonight's brave work begins here — not with fear, but with connection.
"Okay, [child's name], it's almost time for our special night routine. You know what we're going to do tonight? We're going to feed [Worry Monster's name] all the scary thoughts from today, and then we're going to charge up the stars. Do you want to come and do that with me?"
Why "special night routine" works
Frames bedtime as a ritual, not a punishment. Positive anticipation is built before fear is activated.
Why question form ("Do you want to?") works
Child agency — invitation, not command. Reduces power struggle and activates intrinsic motivation.
If child resists
Lower demand: "Okay, bring [comfort object] and just come sit with me for a minute. You don't have to do anything." If crying: Reduce demands to comfort-only tonight (Modify mode).

Step 2 of 6 — The Engagement Rituals
⏱ Timing: 10–15 minutes — the active pre-sleep ritual
The Principle: This step activates three pre-sleep tools — worry externalisation, environmental transformation, and comfort anchoring. Each mini-ritual serves a clinical function AND feels like play.
1
Ritual A — The Worry Monster Feeding
"[Monster's name] is hungry for worries. What scary thoughts have you had today? Can we write/draw/whisper them and feed them to [Monster]?"
After feeding: "[Monster] has eaten all those worries. They're HIS now, not yours. He'll keep them safe all night." Place monster on nightstand: "[Monster] is on guard."
After feeding: "[Monster] has eaten all those worries. They're HIS now, not yours. He'll keep them safe all night." Place monster on nightstand: "[Monster] is on guard."
2
Ritual B — Charging the Stars
"Time to charge the stars! Ready? Point the light right at them…"
After charging: "When I turn off the light in a minute, watch what happens. Your room turns into a galaxy."
This reframe is clinically significant: "my room at night" becomes a positive identity.
After charging: "When I turn off the light in a minute, watch what happens. Your room turns into a galaxy."
This reframe is clinically significant: "my room at night" becomes a positive identity.
3
Ritual C — The Comfort Companion
"[Bear/Bunny] is ready for night duty. Do you want to tell [Bear] what brave thing you're doing tonight?"
Give the object agency: "[Bear] is very brave. He's going to watch out for you."
Give the object agency: "[Bear] is very brave. He's going to watch out for you."
Research: Externalisation therapy (fear projection to object) | ABA reinforcement scheduling | Attachment object research (Winnicott, transitional objects)

Step 3 of 6 — The Therapeutic Action
⏱ Timing: 10–15 minutes — the therapeutic centrepiece
The Principle: Two components — the storybook (bibliotherapy and fear modelling) and the brave step check-in (advancing one rung on the fear ladder). This is where progress is made.
Component A — The Therapeutic Storybook
Choose one book from the reading list (Material 4). When the character encounters fear:
• Pause: "Does [character] feel scared? Does that look familiar?"
• Connect: "You feel scared at night too sometimes. Like [character]."
• Model: "Look what [character] does when scared. Do you think that could work for us?"
• Pause: "Does [character] feel scared? Does that look familiar?"
• Connect: "You feel scared at night too sometimes. Like [character]."
• Model: "Look what [character] does when scared. Do you think that could work for us?"
Close: "You know what? [Character] was scared, just like you. And look — they made it through. You make it through too. Every single night."
Component B — The Fear Ladder Check-In
Both look at the fear ladder from the bed. Confirm tonight's target step:
"Tonight we're doing [current step]. Remember: [exact description of tonight's brave challenge]."
Child confirms. Adjust only if child expresses extreme distress (drop back one rung).
Execution Notes
✅ Ideal: child settles within 15 minutes with manageable anxiety
⚠️ Acceptable: settles within 30 minutes with significant but contained anxiety
🔴 Concerning: escalates beyond manageable → Modify protocol
⚠️ Acceptable: settles within 30 minutes with significant but contained anxiety
🔴 Concerning: escalates beyond manageable → Modify protocol
Research: Bibliotherapy for childhood anxiety (strong evidence base) | PMC11506176 | Graduated exposure dosage research | Meta-analysis 40-minute optimal session time (PMC10955541)

Ongoing — spans days and weeks, not a single session
Step 4 of 6 — Repeat & Vary — The Weekly Rhythm
The Principle: Therapeutic dosage. Fear of the dark is overcome through repeated, graduated exposure — not a single heroic night. The protocol runs every night. But within that consistency, there is intelligent variation.
Nightly Repetition
The same ritual structure (Worry Monster → Stars → Story → Fear Ladder step) runs every night. Consistency is the treatment. Variation in the structure itself undermines the safety signal the routine provides.
When to Advance the Ladder
After 3–5 nights of successful completion of a fear ladder step, advance to the next rung. Only advance if: child completed step on 3+ consecutive nights AND anxiety was manageable (not zero — tolerable) AND distress was self-resolving.
The "3 Good Repetitions" Principle
"3 successful nights at a step are worth more than 10 pushed nights." If your child has a bad night, return to the previous step. This is not failure — it is responsible pacing.
Week | Fear Ladder Step | Nightlight Level | Door Position | |
Weeks 1–2 | Parent sits in room until asleep | Full brightness | Open | |
Weeks 3–4 | Parent in hallway; checks every 5 mins | Full brightness | Open | |
Weeks 5–6 | Parent says goodnight; 1 check only | Full brightness | Cracked | |
Weeks 7–8 | Parent says goodnight; no return | Dimmed 20% | Cracked | |
Weeks 9–10 | Full independence | Dimmed 40% | Closed |
This is a sample — your child's ladder may have more or fewer rungs. Research: SI therapy dosage | Graduated exposure pacing literature | BACB mastery criteria

Step 5 of 6 — Reinforce & Celebrate
⏱ Window A: At bedtime goodnight · Window B: Next morning
The Principle: ABA reinforcement — immediate, specific, enthusiastic. The celebration of brave behaviour strengthens the behaviour. Two reinforcement windows: the moment of brave commitment (goodnight) and the morning after success.
Window A — The Bedtime Goodbye
"You are SO brave. You know what you're doing tonight? You're being a courage warrior. [Bear] knows it. I know it. And tomorrow morning, we're going to put a star on the chart. Goodnight, my brave one. I love you. Sleep well."
Parent leaves per the agreed fear ladder step. No additional returns unless child is in genuine distress (not negotiating distress — true distress, per Card 11 RED criteria).
Window B — The Morning Celebration
"YOU DID IT! You stayed in your room all night! You were so brave! Come — let's put your star on the chart RIGHT NOW."
Child places the sticker on the bravery chart themselves. This is their victory. Their physical act of claiming it matters.
"Look at all these brave nights. Look how many. You are building such strong courage."
✅ Reinforcement Menu
Verbal praise (warm, specific, enthusiastic — always) · Sticker on bravery chart (every successful night) · Token accumulation toward small preferred reward (every 5–7 brave nights) · Certificate of Bravery for major milestones
❌ What NOT to Do
Don't bribe before bedtime · Don't over-explain or over-reassure during the goodnight · Don't punish bad nights — remove sticker opportunities, not earned stickers

Step 6 of 6 — The Cool-Down
⏱ The 5 minutes DURING which parent transitions out
The Principle: No session ends abruptly. The cool-down IS the transition — from parental presence to independent sleep. Done well, it is not a loss (parent leaving) but a completion (ritual fulfilled).
"Everything is ready. [Monster] is on guard. The stars are charged. [Bear] is here. And you are brave. I'll see you in the morning. Goodnight."
Variation: "Sleep tight. I love you. The night is safe."
After 2–3 weeks of hearing the same close, the child's nervous system begins associating these words with the transition to sleep. The words become a sensory anchor — a signal to the brain that the safe sequence is complete and sleep is appropriate.
If Child Calls Out (non-emergency)
After 3–5 minutes only: brief, calm, low-stimulation return.
"You're okay. [Monster] has the worries. [Bear] is here. Back to sleep now."
One brief reassurance, then parent exits again. Do not stay. Do not negotiate.
"You're okay. [Monster] has the worries. [Bear] is here. Back to sleep now."
One brief reassurance, then parent exits again. Do not stay. Do not negotiate.
If Child Resists the Ending
"5 more minutes?" → "We've done our ritual. It's complete. 1 more quiet minute, then I go."
"Don't go" → Warm, firm: "I love you and I'm going. You have everything you need. Goodnight."
Escalating distress → Return to current fear ladder step; do not advance. The resistance is data.
"Don't go" → Warm, firm: "I love you and I'm going. You have everything you need. Goodnight."
Escalating distress → Return to current fear ladder step; do not advance. The resistance is data.

Capture the Data — Right Now
Record this before you make tea. Before you decompress. Immediately after you leave the room. 60 seconds of data now saves hours of guessing later.
Data Point 1 — Fear Ladder Step
Tonight's step number: [ ] / Total steps: [ ]
Did child complete the step? ☐ Yes ☐ Partial ☐ No
Did child complete the step? ☐ Yes ☐ Partial ☐ No
Data Point 2 — Settling Time
How long from goodnight to quiet? [ ] minutes
Was there significant distress? ☐ None ☐ Mild ☐ Moderate ☐ Significant
Was there significant distress? ☐ None ☐ Mild ☐ Moderate ☐ Significant
Data Point 3 — Night Summary
Night wakings requiring parental intervention: [ ]
Child came to parents' room? ☐ Yes ☐ No
Morning mood: ☐ Positive ☐ Neutral ☐ Dysregulated
Child came to parents' room? ☐ Yes ☐ No
Morning mood: ☐ Positive ☐ Neutral ☐ Dysregulated
GPT-OS® App (Recommended)
Log in at pinnacleblooms.org/app — aggregates data across 20M+ sessions, identifies patterns, refines recommendations, generates personalised next-step guidance.
Downloadable PDF Tracker
Free Fear of Dark Progress Tracker — download at pinnacleblooms.org/dark-toolkit. Paper log also entirely valid — use the 3 data points above in any notebook.
After 2 weeks: which steps are solid vs. stalling. After 4 weeks: overall trend. After 8 weeks: readiness for professional review or progression to maintenance.

Reality Check — What If It Didn't Go As Planned?
"Session abandonment is not failure — it is data. The technique needs adjustment, not the parent."
Problem 1: "My child screamed for 45 minutes and never settled."
Why: The current fear ladder step is too challenging. Do: Return to the previous step. Spend 5–7 more nights there before advancing. Reduce the step change increments. If this happens 3+ times, consider professional consultation to review the ladder design.
Problem 2: "My child used every tool correctly but still couldn't sleep for 2 hours."
Why: Residual hyperarousal, or bedtime is past the optimal sleep window. Do: Move bedtime 30 minutes earlier. Extend calm-down period. Review evening screen use. Reduce pre-bed stimulating activities.
Problem 3: "My child fed the worry monster but then said 'what if Monster drops my worries?'"
Why: Child's imagination is working the tool — this is therapeutic engagement, not failure. Do: Expand the story. "Monster has a VERY strong zip." Let the child make the monster stronger — paint it, give it powers.
Problem 4: "After 3 great weeks, my child fully regressed."
Why: Setbacks follow illness, scary events, routine changes, or the natural non-linearity of anxiety treatment. Do: Return to the most recent successful fear ladder step without shame. Do NOT start from scratch. Regression is temporary — the capacity built is real and retrievable.
Problem 5: "The flashlight 'doesn't work' — child still scared with light on."
Why: The flashlight provides agency, not immediate elimination of fear. Do: Reframe: "Being scared AND having a light is better than being scared without one. The flashlight is your power — you have it even when you're scared."
Problem 6: "My child refuses to participate at all."
Why: Anxiety may be severe enough that even low-demand ritual engagement is overwhelming, or there is a trauma/clinical component. Do: Return to zero-exposure: lights fully on, all tools present but not required, parent presence throughout. Call 9100 181 181.
Problem 7: "After 6 weeks, there's no progress at all."
Why: Steps may be too large, reinforcement isn't motivating, or a co-occurring condition requires clinical-level oversight. Do: Book a consultation. 6 weeks of consistent, correct implementation without progress is a signal to escalate to clinical support.
Adapt & Personalise — No Two Children Are Identical
⬅ EASIER — For Severe Fear / First Weeks / ASD Profiles
• Parent remains in room until asleep (every night; this is the starting point)
• All lights on (nightlight at maximum)
• Door open fully
• Fear ladder not yet introduced (comfort rituals only for first 1–2 weeks)
• Morning data only; no in-session pressure
• All lights on (nightlight at maximum)
• Door open fully
• Fear ladder not yet introduced (comfort rituals only for first 1–2 weeks)
• Morning data only; no in-session pressure
➡ HARDER — For Advancing Children / Maintenance Phase
• Parent says goodnight at door (no room entry)
• Nightlight at 10% brightness or off
• Door closed
• Fear ladder: advanced rungs (handling dark hallway alone; sleeping over at relative's house)
• Child initiates own bedtime ritual without prompting
• Nightlight at 10% brightness or off
• Door closed
• Fear ladder: advanced rungs (handling dark hallway alone; sleeping over at relative's house)
• Child initiates own bedtime ritual without prompting
ASD-Specific Adaptations
Children with autism may experience:
• Sensory sensitivity to light wavelengths → OT-assessed nightlight; red/amber spectrum preferred
• Difficulty with abstract concepts → Use concrete, visual language; literal social stories
• Stronger attachment to comfort objects → Leverage these fully; do NOT remove as "graduation" pressure
• Rigid insistence on door positions → Make door position part of the visual schedule; changes must be pre-announced
• More gradual pacing needed → Allow 3–5× longer at each step vs. neurotypical timelines
• Sensory sensitivity to light wavelengths → OT-assessed nightlight; red/amber spectrum preferred
• Difficulty with abstract concepts → Use concrete, visual language; literal social stories
• Stronger attachment to comfort objects → Leverage these fully; do NOT remove as "graduation" pressure
• Rigid insistence on door positions → Make door position part of the visual schedule; changes must be pre-announced
• More gradual pacing needed → Allow 3–5× longer at each step vs. neurotypical timelines
Age-Based Modifications
Ages 2–4: Story-only; skip abstract fear ladder; focus on environmental modification and comfort objects.
Ages 5–7: Full protocol. Fear ladder highly effective. Child can help design steps.
Ages 8–10: More cognitive engagement. Motivation may shift from stickers to pride and independence.
Ages 5–7: Full protocol. Fear ladder highly effective. Child can help design steps.
Ages 8–10: More cognitive engagement. Motivation may shift from stickers to pride and independence.
GPT-OS® ASD-specific fear of dark protocol available at pinnacleblooms.org/autism-bedtime. We strongly recommend professional OT/ABA guidance alongside the home protocol for children with ASD.
Weeks 1–2: The Establishment Phase
Progress: ~15%
Not mastery. Not independence. Not a fear-free child. You're building the infrastructure of safety. This is the most important phase — it sets the foundation for everything that follows.
Signs of Progress in Weeks 1–2
Child participates in ritual without full meltdown · Engages with at least one tool with some interest · Settling time occasionally shorter · Does not come to parents' room EVERY night · Any reduction in daytime anticipatory anxiety
Expected — Not Yet Progress
Child still distressed at bedtime (normal) · Night wakings continue (night waking lags daytime progress by weeks) · Child still demands parent presence · Setbacks on Days 4–5 (very common — the brain tests the new pattern before accepting it)
Parent Emotional Preparation
Weeks 1–2 are the hardest. Expect: extinction burst (behaviour briefly worsens before improving) · Your own guilt and doubt (normal — validate it, keep going) · Exhaustion (recruit your partner or family member into the protocol)
Extinction burst: When you change a well-established pattern, the brain first tries harder to maintain the old pattern — so things often seem worse in Week 1 before they improve. This is a sign the intervention is working, not failing.

Weeks 3–4: The Consolidation Phase
Progress: ~40%
If the protocol has been consistent, weeks 3–4 bring observable neural consolidation — the new pathways are forming. You'll see this in four distinct ways.
Indicator 1: Child Anticipates the Ritual Positively
"Is it time to feed [Monster]?" asked before you initiate = the ritual has become safety, not threat. This is a profound shift.
Indicator 2: Settling Time Drops Below 30 Minutes
The child's nervous system is accepting the new pattern. This is the most reliable indicator of real progress.
Indicator 3: Spontaneous Use of Coping Language
Child says "I was scared but then I looked at my stars" — unprompted. This is self-regulation beginning to internalise.
Indicator 4: First Full Independent Night
This may happen for the first time in weeks 3–4. It may be one night in a row. That is a major milestone. Celebrate it fully.
Parent Milestone: You may notice YOU are more confident too. The nightly dread you felt approaching bedtime is reducing. This parental calm communicates to your child: bedtime is safe now. Your nervous system's improvement is part of their treatment.

Weeks 5–8: The Mastery Phase
Progress: ~75%
A child has reached mastery for this technique when they demonstrate ALL of the following criteria. Mastery doesn't mean perfection — it means consistent, independent, manageable.
☐ Completes bedtime routine without parental presence beyond goodnight
With standard supports: nightlight, comfort object, white noise
☐ Settles to sleep within 15–20 minutes on most nights
Night wakings do not require parental intervention on most nights
☐ Uses at least one coping tool independently when fear arises
Daytime anticipatory anxiety about bedtime has significantly reduced or resolved
☐ Fear has not generalised
Child can navigate dark hallways/bathrooms with manageable anxiety. Can teach a younger sibling what to do when scared. Teaching = deepest mastery.
Maintenance Check: After reaching mastery, reduce protocol intensity gradually: Weeks 9–10: remove one ritual element (child decides which). Weeks 11–12: shift to abbreviated check-in routine. Month 4+: organic bedtime; tools available but not structured.
You Did This.
Your child grew because of your commitment.
Eight weeks ago, your child shivered on the hallway floor at 3 AM. Tonight, they kissed you goodnight and you walked away. They stayed. They slept. They were brave. And so were you.
Built a Personalised Toolkit
A set of coping strategies that belong to your child — that they chose, named, and made their own.
Mastered Graduated Darkness Tolerance
Step by step, rung by rung, they proved to themselves that they could face something scary and survive it.
Developed Self-Regulation Skills
Skills that will serve them far beyond bedtime — in school, friendships, and every future challenge they face.
📸Photo/Journal Prompt: Take a photo tonight of your child's bravery chart — full of stickers. Or a photo of them in their bed, asleep, alone, safe. In 5 years you will show this to them and say: "You did this at age 6."

Clinical Guardrails — Even in the Celebration Zone
Red Flags — When to Pause
"Trust your instincts. If something feels wrong, pause and ask."
🚩 Red Flag 1: Fear returns suddenly and intensely after significant improvement
May indicate a new triggering event (school transition, family stress, something witnessed). Do: Pause exposure steps. Return to comfort-only bedtime. Have a gentle conversation: "Is there something new that's feeling scary?" Consider professional assessment if cause is unclear.
🚩 Red Flag 2: New fears appear alongside the improving fear of dark
May indicate underlying generalised anxiety requiring clinical-level treatment. Do: Book a teleconsultation. Note the specific new fears in your data log. Do not assume the home protocol addresses co-occurring anxiety disorders.
🚩 Red Flag 3: Sleep disturbance is affecting daytime functioning significantly
Falling asleep at school, unable to concentrate, mood severely impacted — these have medical and developmental consequences. Do: Pediatric consultation. Combine with anxiety treatment, not instead.
🚩 Red Flag 4: Fear accompanied by disproportionate physical symptoms
Regular vomiting at bedtime, uncontrolled hyperventilation, severe gastrointestinal distress every night. Do: Pediatric consultation first; anxiety treatment proceeds concurrently.
🚩 Red Flag 5: Child discloses something specific during the fear ritual
During worry monster feeding or storybook discussion, child makes a disclosure suggesting something real has happened. This is a safeguarding situation, not an anxiety situation. Do: Take seriously. Consult a trained professional immediately.
Escalation Pathway: Self-manage → Teleconsultation (pinnacleblooms.org/book) → Clinic visit → Emergency pathway. FREE Helpline: 9100 181 181 | 24x7 | 16+ languages
Your Developmental GPS — Where This Leads
⭐ YOU ARE HERE: C-284
Mastering the Dark Safety Toolkit is one milestone on a larger developmental journey. Here's what came before, and where three clear paths lead next.
Path 1 — Next Anxiety Technique
→ C-285: Separation Anxiety — 9 Materials That Help
Use when: Child's nighttime fear has resolved but separation anxiety in other contexts persists
Use when: Child's nighttime fear has resolved but separation anxiety in other contexts persists
Path 2 — Sleep Independence Deepening
→ C-290: Bedtime Routine Challenges — Building Reliable Sleep Architecture
Use when: Fear of dark is resolved but bedtime resistance continues from other causes
Use when: Fear of dark is resolved but bedtime resistance continues from other causes
Path 3 — Generalisation
→ C-286: Social Anxiety in Children — Early Signals and Supports
Use when: Child's anxiety is expanding into social domains as fear of dark resolves
Use when: Child's anxiety is expanding into social domains as fear of dark resolves
More Techniques in Emotional Regulation & Anxiety
Explore the full Domain C library. Many use materials you already own.

🟡 C-282 — Understanding Childhood Anxiety
The Parent's Foundation Guide · Difficulty: Intro · Materials: Knowledge-only

🟡 C-283 — Recognising Anxiety Signs in Children
The Observation Toolkit · Difficulty: Intro · Materials: Observation-based

🟠 C-285 — Separation Anxiety — 9 Materials That Help
Difficulty: Core · Materials you own: ✓ Comfort objects, bravery charts

🟠 C-286 — Social Anxiety in Children — Early Signals and Supports
Difficulty: Core · Materials you own: ✓ Storybooks, bravery systems

🟠 C-290 — Bedtime Routine Challenges
Building Reliable Sleep Architecture · Difficulty: Core · Materials you own: ✓ White noise, nightlight, routine visuals
🔴 C-295 — Panic Management for Children
Graduated Body-Based Techniques · Difficulty: Advanced · Materials: Breathing tools, calming audio
This Technique Is One Piece of a Larger Plan
Your child's development spans 12 domains. The Dark Safety Toolkit addresses one critical node — and connects to everything else.
Domain C Progress — Where You Are
C-282 ✓ → C-283 ✓ → C-284 ✓ → C-285 → C-286 → ... → C-300
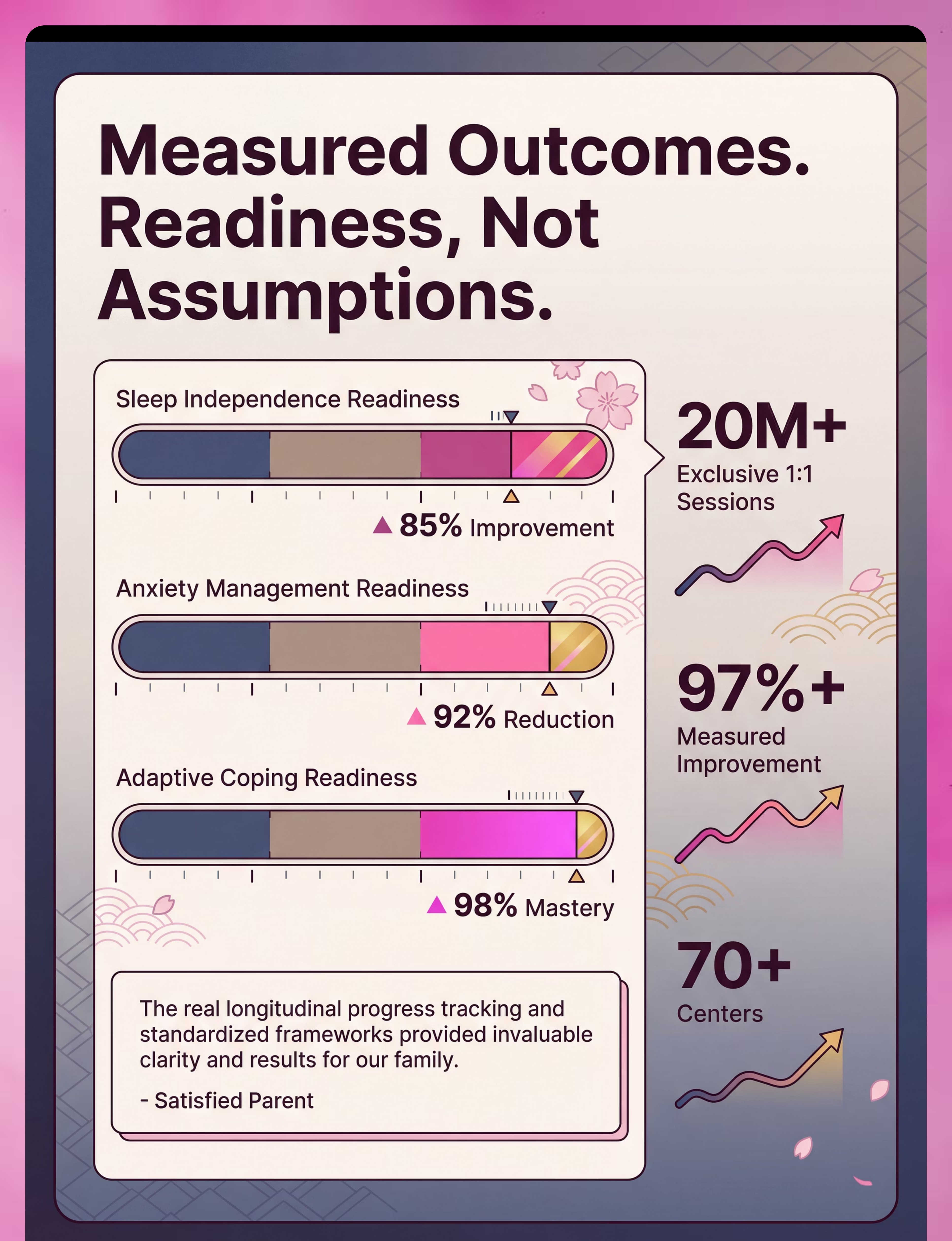
This technique contributes to your child's Sleep Independence Readiness Index and Anxiety Management Readiness Index within GPT-OS®.
WHO/UNICEF Framework Alignment
WHO Nurturing Care Framework 5 components: Health · Nutrition · Responsive Caregiving · Security & Safety · Early Learning.
This technique directly addresses Security & Safety + Responsive Caregiving, with downstream benefits to Early Learning through improved sleep quality.
Real Families. Real Progress.
Anonymised clinical narratives from the Pinnacle Network. Individual outcomes vary.
Arjun, 5 years — Hyderabad
Before: Two-hour bedtime battle every night. Arjun would not let his mother leave the room. Once a week they'd find him on the floor outside their room at 2 AM. "I was sleeping on his floor just to get through the night. I was beyond exhausted. I felt like I was failing him."
After (8 weeks):"The first night he stayed in his room alone, I stood outside his door for 10 minutes not believing it was real. In the morning he ran to his bravery chart and put the sticker on himself. He told me: 'Mama, Nanu kept all my worries.' Something changed in him that night. He knew he was brave."
Therapist Note:"Arjun's case illustrates the classic pattern: ritual + graduated exposure + reinforcement. The sticker chart made his progress visible to him — which mattered as much as the progress itself."
Priya, 7 years, ASD — Chennai
Before: Priya was hypersensitive to light. Standard nightlights caused sensory distress; she needed dark but was terrified of it. A painful paradox. Bedtime had become a 3-hour ordeal.
After (12 weeks, ASD pacing): OT recommended a red-spectrum nightlight at a specific brightness threshold. Glow stars in Priya's preferred yellow-green wavelength. Week 12: Priya self-initiates her bedtime routine, uses her stars as her primary visual anchor, and sleeps through on most nights. "Nobody had ever told us the light spectrum mattered. One conversation with the OT changed everything."
Kabir, 4 years — Mumbai (Early Intervention)
Before: Fear appeared suddenly after a power cut. Within two weeks, Kabir couldn't be in any room with lights off. Was this trauma?
After (6 weeks): A social story specifically referencing the power-cut event processed the trigger. Fear ladder started at actual capability. "The social story was the key. He needed to process the event. Once he did, the fear dissolved quickly."

You Are Not Alone — And Neither Are They
Isolation is the enemy of adherence. Find your community. When parents share strategies, celebrate milestones, and support each other through hard nights — progress accelerates for everyone.
Pinnacle Parents WhatsApp Community
Join thousands of Indian parents navigating childhood anxiety and bedtime challenges. Real conversations. Real strategies. Peer support from parents who've completed this exact protocol.
Online Parent Forum
Discussion threads, Q&A with Pinnacle therapists, shared data insights. "What worked for us" posts from across the network. pinnacleblooms.org/community
Local Pinnacle Parent Meetups
Monthly parent support sessions at 70+ Pinnacle centers across India. Share journeys. Meet therapists. See other families who've been where you are. Find your nearest center
Become a Peer Mentor
Has your child completed this protocol? Your experience — your hard evenings, your self-doubt, your breakthrough — is the most powerful resource for a parent in Week 1. pinnacleblooms.org/mentor
Home + Clinic = Maximum Impact
These materials work best when supported by professional guidance. Pinnacle's 70+ center network exists for exactly this — to give your home protocol clinical backing and personalised adjustment.
Find Your Nearest Center
70+ centers across India | Hyderabad · Bengaluru · Chennai · Mumbai · Delhi NCR · and more
Book Teleconsultation
Video consultation with a Pinnacle-credentialed therapist from anywhere in India or internationally.
FREE National Helpline
📞9100 181 181 | 24x7 | 16+ languages | Free of charge
What to Expect from a Pinnacle Consultation:
- AbilityScore® baseline assessment (20–30 minutes)
- Functional analysis of the specific fear presentation
- Personalised fear ladder design with therapist
- Parent coaching on protocol execution
- GPT-OS® data integration for ongoing monitoring
The Evidence Base — For the Curious Parent
Deeper reading for the curious parent
Level I — PMC3018839
Journal of Child Psychology and Psychiatry (2011)
Graduated exposure therapy is the most effective treatment for specific phobias in children, including fear of the dark. CBT approaches adapted for developmental level show strong outcomes. Read on PubMed
Graduated exposure therapy is the most effective treatment for specific phobias in children, including fear of the dark. CBT approaches adapted for developmental level show strong outcomes. Read on PubMed
Level I — PMC11506176
PRISMA Systematic Review, Children (2024)
Multimodal interventions (environmental + cognitive + behavioral) demonstrate superior outcomes. 16 studies reviewed, 2013–2023. Read on PubMed
Multimodal interventions (environmental + cognitive + behavioral) demonstrate superior outcomes. 16 studies reviewed, 2013–2023. Read on PubMed
Level I — PMC10955541
World Journal of Clinical Cases (2024)
24 studies; 1,050+ participants. Combined sensory-behavioral interventions effectively promote adaptive behaviour and anxiety management. Read on PubMed
24 studies; 1,050+ participants. Combined sensory-behavioral interventions effectively promote adaptive behaviour and anxiety management. Read on PubMed
Level II — PMC9978394
WHO/UNICEF Care for Child Development (CCD) Package
Caregiver-administered interventions using structured materials show significant outcomes across diverse populations in 54 LMICs. Read on PubMed
Caregiver-administered interventions using structured materials show significant outcomes across diverse populations in 54 LMICs. Read on PubMed
Level II — Padmanabha et al. (2019)
Indian Journal of Pediatrics | DOI: 10.1007/s12098-018-2747-4
Home-based behavioral interventions administered by trained Indian parents show significant outcomes — demonstrating that the Pinnacle home-based protocol has specific Indian evidence support.
Home-based behavioral interventions administered by trained Indian parents show significant outcomes — demonstrating that the Pinnacle home-based protocol has specific Indian evidence support.
Additional authorities: AAP Healthy Sleep Guidelines | NCAEP Evidence-Based Practices Report (2020) | WHO Nurturing Care Framework (2018)

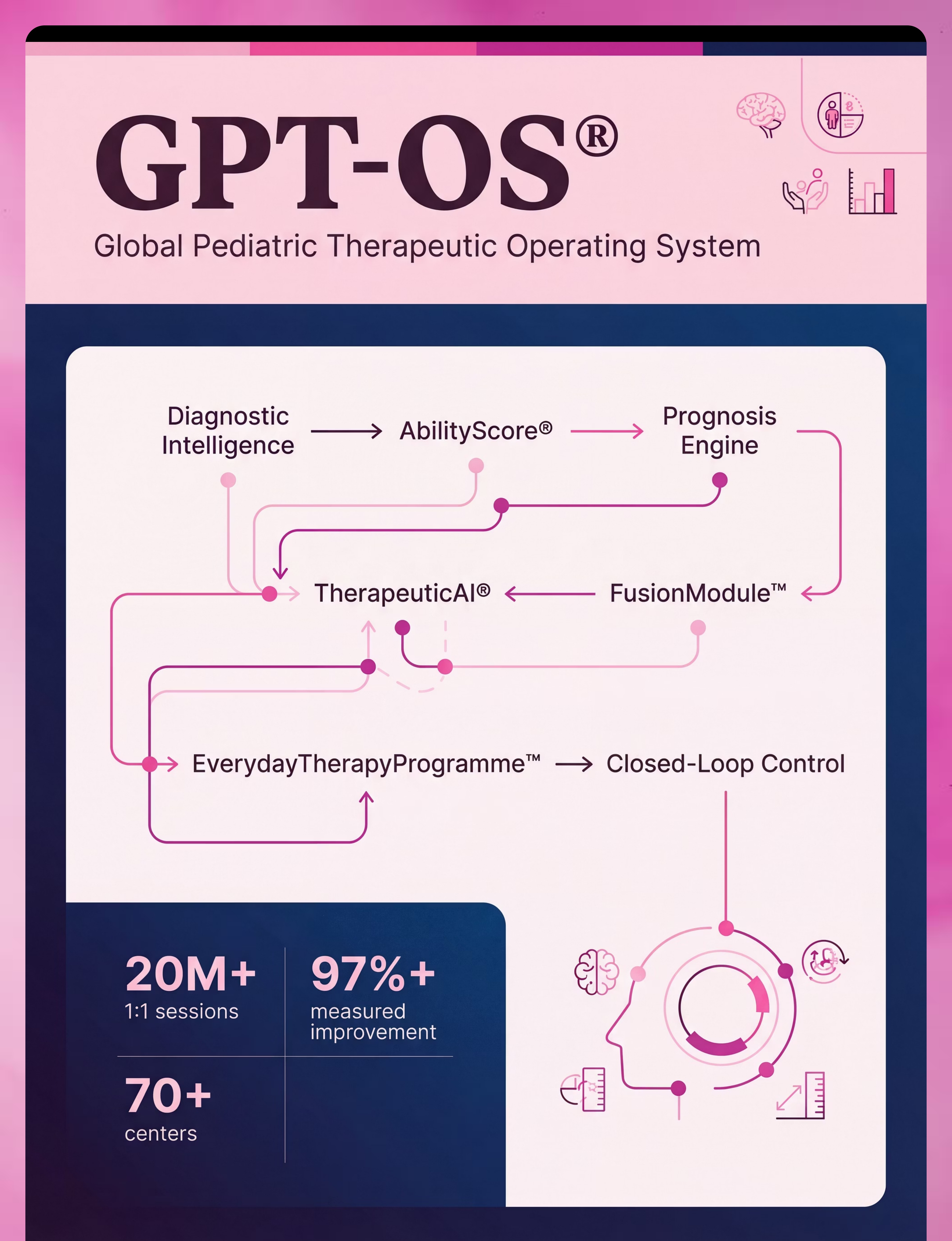
Your Data. Your Child. Your Progress. Powered by 20M+ Sessions.
GPT-OS® Technology
GPT-OS® is the world's only closed-loop pediatric therapeutic operating system. Here's how it works — and how your nightly data powers it.
Diagnostic Intelligence Layer
Your child's fear profile (severity, triggers, response patterns) is captured through 591+ structured observations across 349 skills — replacing fragmented, subjective assessment with standardised diagnostic clarity.
AbilityScore®
A standardised developmental score (0–1000) that establishes baseline and tracks longitudinal change, including the Sleep Independence Readiness Index and Anxiety Management Readiness Index relevant to this technique.
TherapeuticAI®
Determines which fear ladder step to advance to next, what reinforcement schedule is optimal for your child's profile, and when to recommend professional escalation — based on your nightly data input.
EverydayTherapyProgramme™
Translates clinical plans into daily home-executable micro-interventions. Your nightly bedtime protocol IS the ETP — personalised, sequenced, monitored.
FusionModule™
Coordinates OT, ABA, behavioral psychology, and special education inputs into ONE integrated bedtime plan. Closed-loop: you observe → GPT-OS® scores → plan adapts → you execute → re-measure → adapt again.
Privacy Assurance: All data is encrypted, anonymised for population analysis, and subject to India DPDP Act compliance + ISO/IEC 27001 standards. Individual family data is never shared without explicit consent. Your child's brave nights help children across India and 70+ countries.

Watch the Reel That Started This
🎬 Reel C-284 | 75–85 seconds | Emotional Regulation & Anxiety Support — Episode 284
This web page is the deep-dive behind the Reel. The Reel introduced the 9 materials. This page shows you exactly how to use them, in sequence, with clinical precision.
"Fear of the dark is one of the most common childhood fears — and one of the most treatable. These children aren't being dramatic or manipulative; they're experiencing genuine fear that their developing brains can't yet regulate. These materials help bridge the gap — providing control, externalising fear, building gradual tolerance, and celebrating brave steps." — Pinnacle Blooms Consortium, Behavioral Psychology Lead
<
← C-283 — Watch First
Recognising Anxiety Signs in Children
▶ C-284 — You Are Here
9 Materials That Help With Fear of the Dark
→ C-285 — Watch Next
9 Materials That Help With Separation Anxiety
NCAEP (2020): Video modelling is an evidence-based practice for autism and pediatric behavioral intervention. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition.
Consistency Across Caregivers Multiplies Impact
If only one parent uses this toolkit, results are limited. When everyone in the child's life knows the approach — and uses it consistently — progress accelerates dramatically.
📱 Share on WhatsApp
"My child has been struggling with fear of the dark at bedtime. I found this amazing resource from Pinnacle Blooms Network that explains exactly what to do — 9 materials + a step-by-step protocol. Sharing with you so we can all use the same approach."
📄 Family Guide (1-page PDF)
One page. Plain language. The 5 key things every caregiver needs to know. Designed for grandparents, relatives, and part-time caregivers.
📝 Teacher Communication Letter
Informs school staff that child is undergoing a structured bedtime anxiety program; requests understanding of possible tiredness during early weeks.
"Explain to Grandparents" Summary: "We're using a gentle, step-by-step method to help [child's name] feel safe at night. Key things: (1) Don't turn all lights on when they cry — follow the nightlight plan. (2) The worry monster is their tool — please respect it. (3) The bravery chart is theirs — please celebrate it. (4) Consistent goodnight script every night. (5) Call [parent name] if anything feels concerning."
Questions Parents Actually Ask
Generated from real parent queries at Pinnacle centers and the online community.
Q1: How long will this take? When will I see a difference?
Most families see the first observable change within 1–2 weeks. Significant improvement by weeks 3–4. Sleep independence for most children by weeks 6–10. Children with ASD or co-occurring anxiety may take 2–3× longer. There is no race. Progress is the goal, not speed.
Q2: Should I just let them cry it out?
No. Cry-it-out is not recommended for fear-based sleep resistance. Fear of the dark is an anxiety condition — forcing exposure without graduated support and coping tools can worsen the fear and damage trust. Graduated exposure is the evidence-based approach.
Q3: My child only sleeps with lights fully on. Is that okay for now?
Yes — for now. Full lights on = the first rung of the fear ladder. You will gradually dim from here. There is no timeline pressure for the first 1–2 weeks. Meeting the child where they are is the starting point, not a permanent position.
Q4: We tried the worry monster but my child refuses. What now?
The mechanism (externalisation) matters; the vessel is flexible. Alternatives: a designated "worry jar" with sealed written fears; a piece of paper torn up and thrown in the bin; whispering fears into a pillow. Same clinical function, different form.
Q5: My child has ASD. Will this work differently?
Yes — with adaptations. Core principles are identical; pacing, language, and sensory calibration must be personalised. Key adaptations: concrete language (not metaphors), visual schedule for the ritual, OT-assessed nightlight wavelength, slower fear ladder pacing. Guide at pinnacleblooms.org/autism-bedtime.
Q6: My partner wants to be firm. What do we do?
Share Cards 03 (neuroscience) and 05 (evidence base). Fear of the dark is an anxiety condition, not a behavioral problem. Being firm and providing tools are not mutually exclusive. This protocol is firm AND supportive. Consistency between caregivers is critical.
Q7: What if this doesn't work after 8 weeks?
Book a consultation. 8 weeks of consistent, correct implementation without meaningful progress warrants professional clinical assessment. There may be a co-occurring condition requiring clinical-level treatment alongside the home protocol. Call 9100 181 181.
Q8: Fear appeared suddenly — my child used to sleep independently.
Sudden-onset fear is often triggered by a specific event — a nightmare, a power cut, something heard or seen. It typically responds very well to targeted intervention (particularly social stories addressing the specific trigger) and often resolves faster than gradual developmental fear.

Enough Reading. Your Child Needs This Tonight.
You now have everything you need — the neuroscience, the materials, the step-by-step protocol, the safety guardrails, and the evidence base. The only thing left is to begin.
🌙 Start This Protocol Tonight
Download the complete Dark Safety Toolkit Quick-Start Guide (PDF). Includes: Fear ladder template, bravery chart, bedtime script card, worry monster instructions.
📞 Book a Consultation
Speak with a Pinnacle-credentialed therapist who specialises in childhood anxiety. Available online (teleconsultation) and at 70+ centers across India.
→ Next Technique: C-285
Separation Anxiety — 9 Materials That Help. The journey continues at techniques.pinnacleblooms.org
📞FREE National Autism Helpline: 9100 181 181 | 24x7 | 16+ languages | Free of charge
Validated by the Pinnacle Blooms Consortium · OT · SLP · ABA · Special Education · Neuro-Developmental Pediatrics · CRO
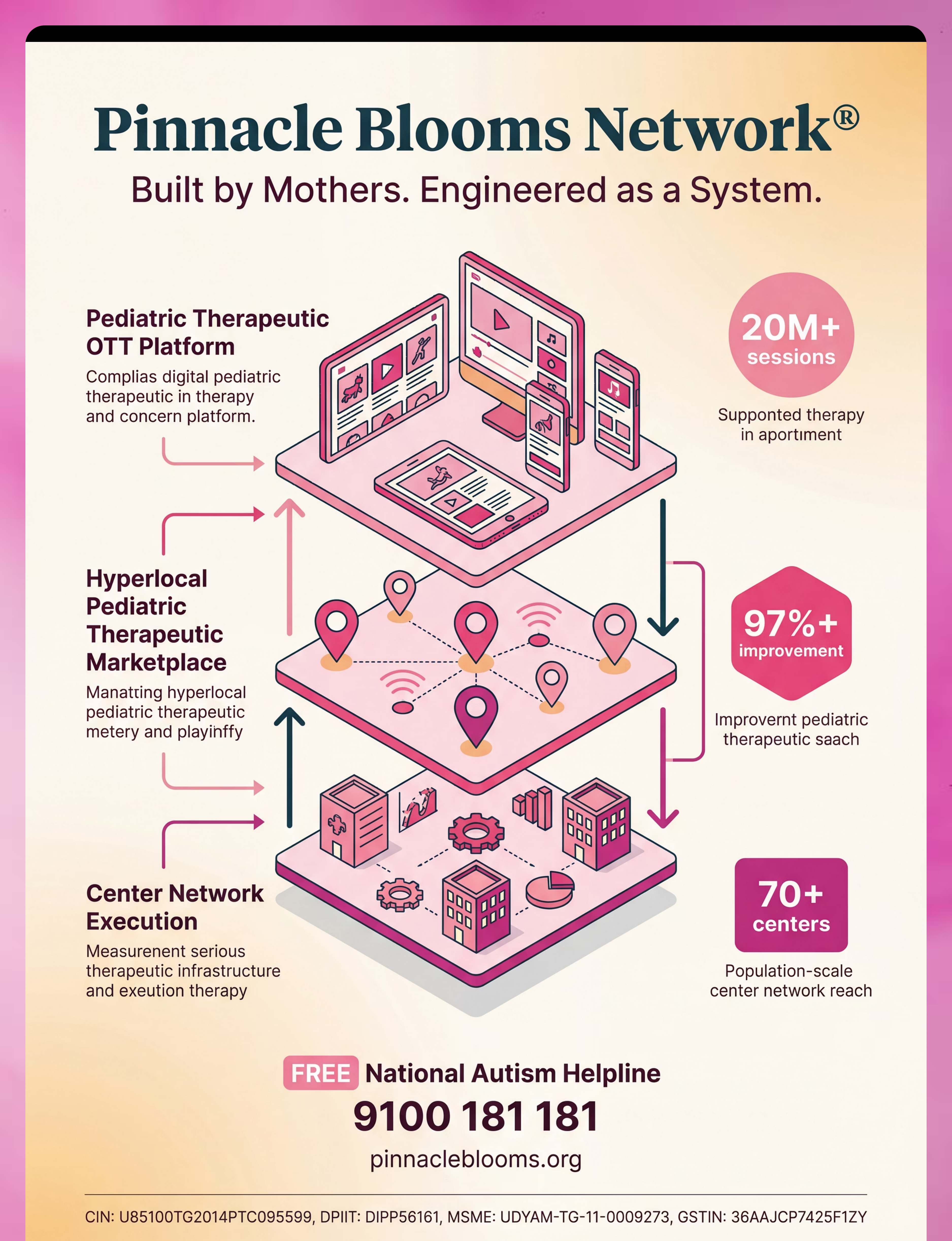
Built by Mothers. Engineered as a System. Trusted by 21 Million sessions.
Validated by the Pinnacle Blooms Consortium · OT · SLP · ABA · Special Education · Neuro-Developmental Pediatrics · CRO
Built by Mothers. Engineered as a System. Trusted by 21 Million sessions.
Preview of 9 materials that help with fear of the dark Therapy Material
Below is a visual preview of 9 materials that help with fear of the dark therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

The Pinnacle Promise
Pinnacle Blooms Network®
A consortium of: Pediatric OT · SLP · ABA · Special Education · Neuro-Developmental Pediatrics · Clinical Research · Regulatory Expertise · Mothers + Fathers + Families
A consortium of: Pediatric OT · SLP · ABA · Special Education · Neuro-Developmental Pediatrics · Clinical Research · Regulatory Expertise · Mothers + Fathers + Families
"From fear to mastery. One technique at a time."
Built across 70+ centers. Validated across 20 million sessions. Trusted by families in 70+ countries. Powered by GPT-OS® — the world's only closed-loop pediatric therapeutic operating system.
A parent arrived on Card 01
Scared, exhausted, and out of ideas. Standing at the bedroom door at 3 AM, not knowing what to do next.
By Card 40
Their child is sleeping. Their child is brave. They have the tools, the evidence, the community, and the professional support to keep going.
And so are they.
— The Pinnacle Blooms Consortium
Medical Disclaimer: This content is educational. It does not replace individualised assessment and intervention planning with licensed professionals including psychologists, behavioral therapists, and pediatricians. Fear intensity and appropriate interventions vary by individual child. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U85100TG2014PTC095599 | DPIIT: DIPP56161 | MSME: UDYAM-TG-11-0009273 | GSTIN: 36AAJCP7425F1ZY | ISO 13485 | ISO/IEC 27001
CIN: U85100TG2014PTC095599 | DPIIT: DIPP56161 | MSME: UDYAM-TG-11-0009273 | GSTIN: 36AAJCP7425F1ZY | ISO 13485 | ISO/IEC 27001