
She hides every time someone new walks in.
Not strangers on the street. Her own teacher. Relatives she's met before. Anyone who isn't her three safe people. Her world is shrinking — and it's happening right in front of you. This isn't shyness. It's not manipulation. It's not defiance. Her nervous system genuinely perceives threat in every unfamiliar face — and she cannot simply choose otherwise. You are not failing. Her nervous system is speaking.
C-279
Social-Emotional Development
Ages 2–10
Episode 279 of 999
🌸Pinnacle Blooms Network® | GPT-OS® Verified | FREE Helpline: 9100 181 181 | Social-Emotional Development Series • Episode 279 • Ages 2–10

Every unfamiliar face. Millions of families.
Stranger anxiety is a normal developmental phase — it peaks at 12–18 months and typically resolves by age 3. But when it persists, intensifies, or shrinks your child's world at age 4, 5, or 7, it is no longer typical development. Research from the National Institute of Mental Health confirms that behavioural inhibition in early childhood is the strongest temperamental predictor of later social anxiety disorder. Early intervention changes this trajectory.
15%
Born Highly Inhibited
Of all children are born with high behavioural inhibition — the temperamental root of fear of new people.
40%
Develop Social Anxiety
Of highly inhibited children develop clinically significant social anxiety without early intervention.
1 in 59
ASD Diagnoses
Children are diagnosed with autism spectrum disorder, for whom fear of new people has neurological depth beyond typical anxiety.
In India, where extended family networks and community interactions are deeply embedded in daily life, fear of new people creates compounding isolation. The family gathering becomes a trauma. The school introduction becomes a crisis. You are among millions of families navigating exactly this.
This is neuroscience. Not behaviour.
When your child sees a new person, their brain responds in a precise, biological sequence — not from choice, but from wiring. Understanding this changes everything about how you respond.
The amygdala fires first
Before any rational thought, the brain's threat-detection system registers "unfamiliar face" as potential danger. This happens in 200 milliseconds — faster than conscious thought. Your child isn't choosing this.
Cortisol floods the body
Heart rate spikes. Stomach tightens. Legs freeze. The body prepares to fight, flee, or freeze. This is a genuine physiological event happening to your child.
The prefrontal cortex gets bypassed
The part of the brain that could say "this person is safe" cannot override the amygdala fast enough — especially in children under 7, whose prefrontal cortex is still developing.
Key Insight: "This is a wiring difference, not a character flaw. The same biology that protects children from genuine danger is being triggered by unfamiliarity. Intervention works by gradually teaching the amygdala that new faces = safe, not threat." — Pinnacle Consortium Neurological Framework
Normal development has a trajectory. Here is where yours is.
1
Birth – 6 months
No fear of new faces. All faces equally novel and welcome.
2
6–18 months
Stranger anxiety emerges and peaks — this is normal, protective development.
3
24–36 months
Wariness decreasing. Warm-up periods begin to shorten with trusted caregiver present.
4
3–5 years
Should tolerate new people with brief warm-up. Gradual resolution typical.
5
5–7 years
Concern zone. Fear persisting, intensifying, or impairing function → intervention recommended.
When concern is warranted: fear persisting beyond age 3 with no decrease; warm-up time extending to hours or never completing; fear responding to people the child has met before; physical symptoms such as vomiting or stomach aches before social situations; school refusal; medical appointment impossibility. Also watch for autism spectrum features, sensory processing differences, selective mutism, and generalised anxiety disorder as co-occurring conditions.

Not hope. Evidence.
Every material in this toolkit is grounded in peer-reviewed research. This is not an experimental approach — it is the clinically validated, gold-standard intervention for fear of new people in children, backed by systematic reviews, randomised controlled trials, and population-level data.
Gradual Exposure
16 controlled studies confirm that systematic, graduated exposure is the gold standard for anxiety reduction in children. Effect sizes: large (d > 0.8) for behavioural outcomes. PMC2697319 | NIMH Behavioural Inhibition Research
Parent-Mediated Intervention
RCT evidence (Indian population, 2019) demonstrates that parent-administered home-based behavioural interventions achieve outcomes equivalent to clinic-delivered sessions when parents receive structured protocols. DOI: 10.1007/s12098-018-2747-4
Visual Supports + Social Stories
NCAEP 2020 classifies social stories and visual supports as evidence-based practices for autism — the population most severely affected by fear of new people. National Clearinghouse on Autism Evidence and Practice
Clinically validated. Home-applicable. Parent-proven. 20M+ sessions of real-world data supporting the GPT-OS® framework that powers this technique.

Technique Code: C-279
Ages 2–10
SOC-ANX
The Fear of New People Toolkit
Formal Name: Materials-Based Social Approach Scaffolding for New People Tolerance. This technique uses nine evidence-based materials and tools to systematically reduce a child's fear response to unfamiliar people. Rather than forcing exposure (which traumatises) or enabling avoidance (which intensifies fear), the approach works on three levels simultaneously:
Preparation
Making the unknown predictable before encounters occur.
Graduated Exposure
Building tolerance one small, achievable step at a time.
In-Moment Regulation
Giving the child tools to manage fear when it rises during encounters.
The result is a child who expands their circle — not from pressure, but from accumulated evidence that new people are safe. This approach is led by Psychology and ABA, with OT, SLP, and Special Education integrated throughout.

Five disciplines. One coordinated approach.
Fear of new people is a whole-brain, whole-body, whole-life challenge. The brain doesn't organise by therapy type — and neither should your child's intervention. Each discipline brings a distinct and essential lens.
Psychology / Child Behaviour Specialists
Primary lead discipline. Conducts comprehensive anxiety assessment, establishes the exposure hierarchy, monitors progress, and coordinates the full intervention protocol using a CBT framework adapted for young children.
Occupational Therapy
Addresses sensory processing components — new people bring unpredictable sensory input (voices, touch, scents). OT ensures the child has sensory regulation strategies and a supportive home environment.
ABA / Behavioural Therapy
Designs reinforcement systems (Brave Bucket protocols), ensures exposure hierarchy is graduated appropriately, tracks behavioural data, and ensures brave behaviour is reinforced — not avoidance.
Speech-Language Pathology
Critical for children with selective mutism. Uses specialised protocols (stimulus fading, sliding-in technique) and builds the child's social script vocabulary for greetings and early interactions.
Special Education
School-context specialist. Ensures the approach generalises to classroom settings — new teachers, classroom transitions, school visitors. Coordinates with educators on preparation protocols.
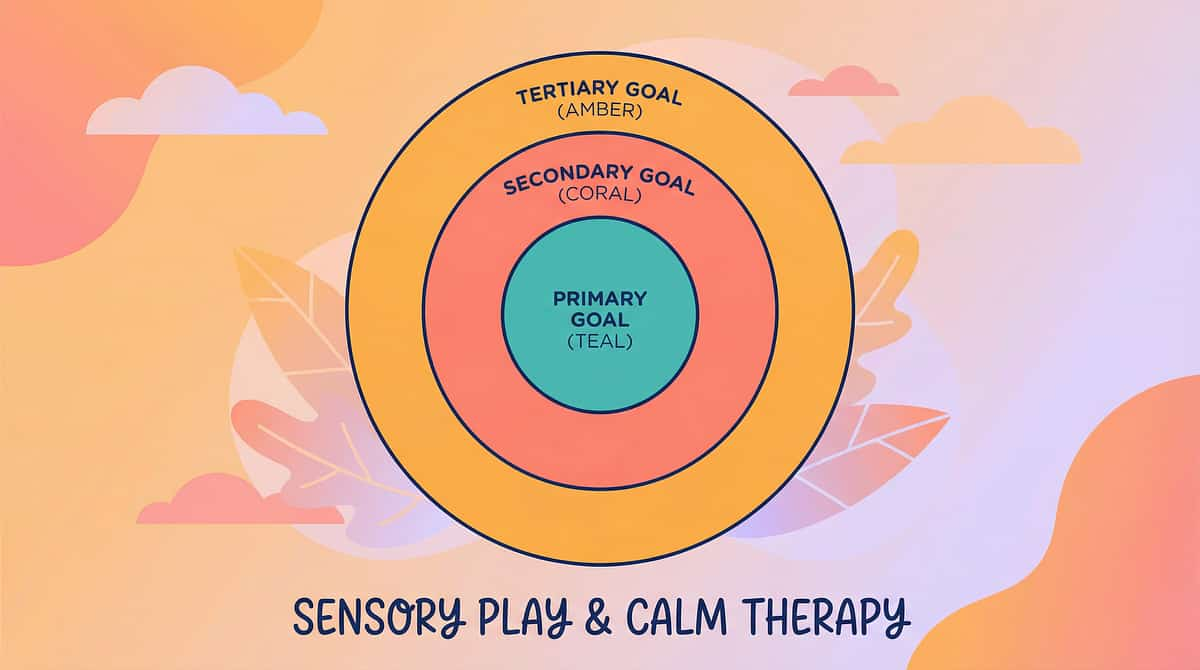
This is a precision toolkit. Here is exactly what it targets.
🎯 Primary Target
Fear of New People Reduction. Decreasing fear thermometer readings. Increasing time before hiding occurs. New people tolerated at distance, then closer proximity.
🔵 Secondary Targets
Emotional regulation, communication, self-efficacy. Spontaneous eye contact emerging. Brief verbal responses beginning. Comfort object use decreasing as confidence grows.
⭕ Tertiary Targets
Peer relationships, academic engagement, community participation. Friend invitations accepted. School transitions managed. Medical appointments less traumatic.
Progress is visible across all three levels. As primary targets improve, secondary and tertiary targets follow — not because you've addressed them separately, but because the child's relationship with unfamiliarity is fundamentally changing at the neural level.
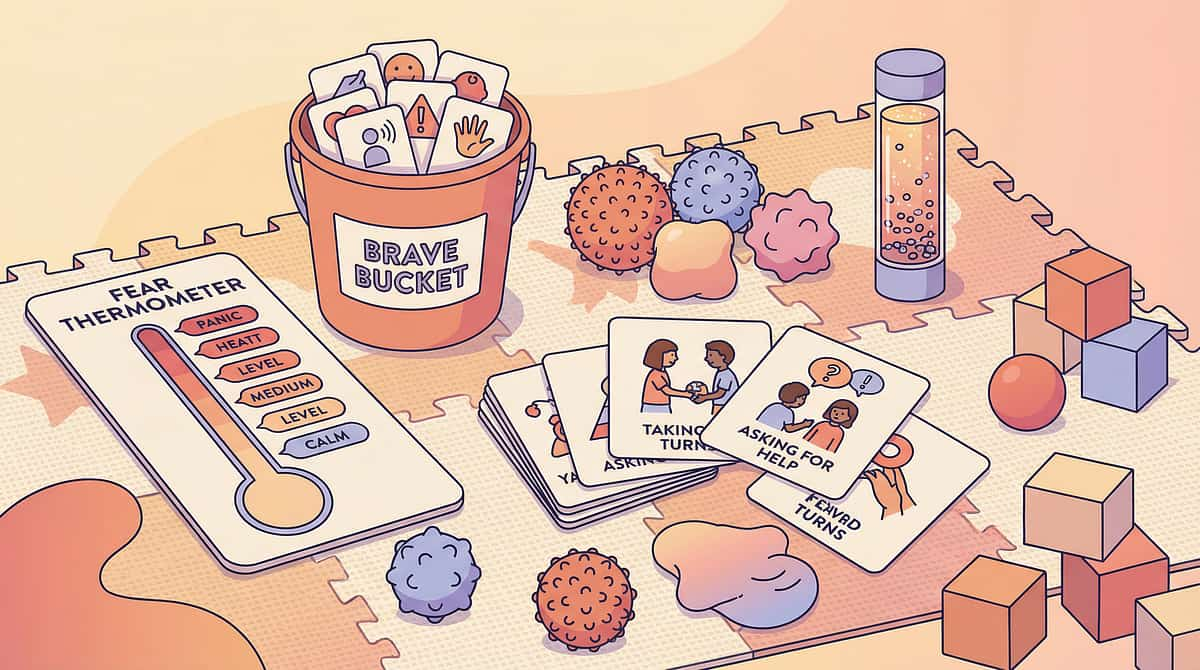
9 materials. A complete toolkit.
Every material below has an evidence base, a clear mechanism, and a ₹0 DIY alternative. Start with whichever feels most accessible. Need help choosing? FREE Helpline: 9100 181 181
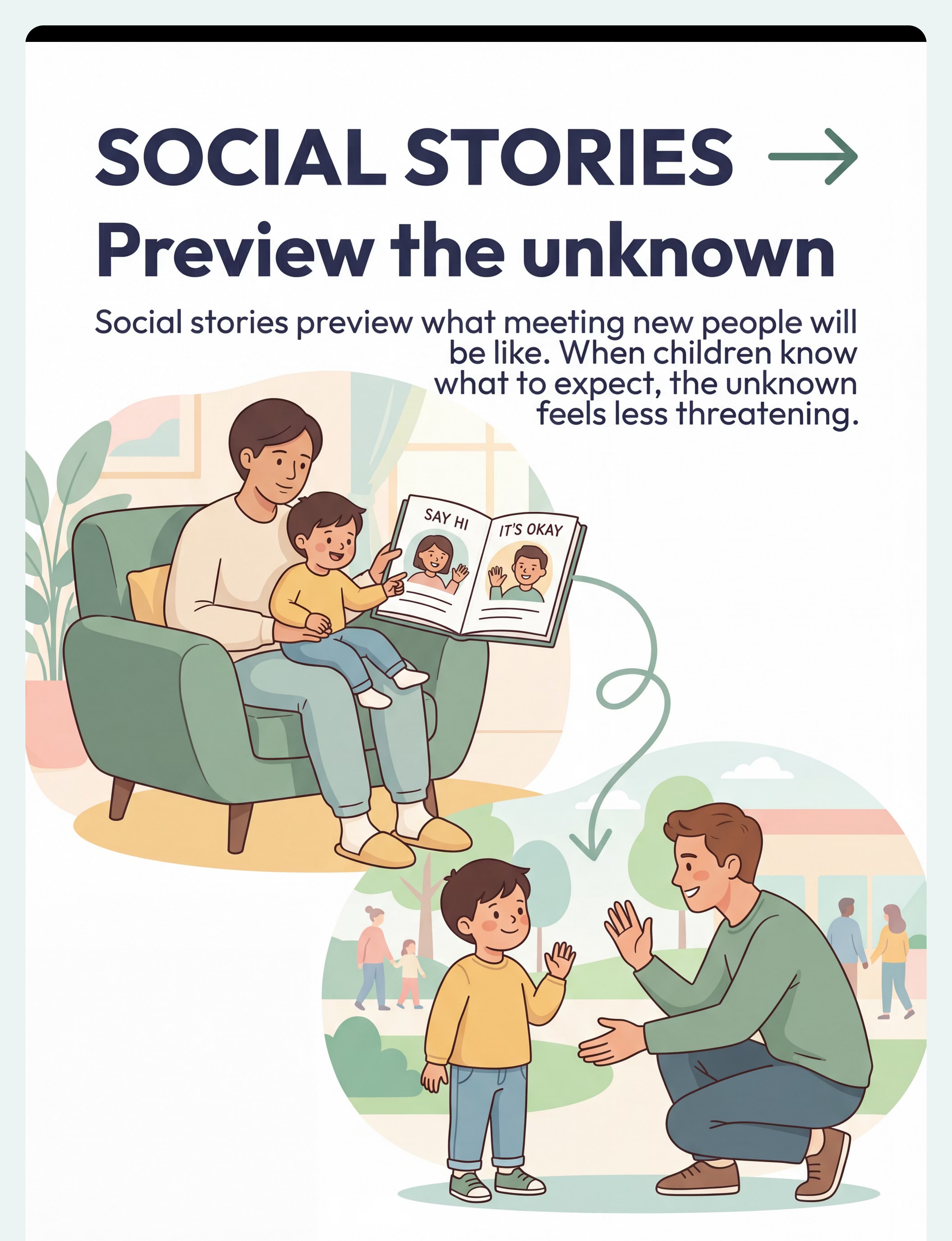
Social Stories About Meeting New People
Custom or pre-made narrative books that preview what meeting new people looks, feels, and sounds like — written from the child's perspective. Fear thrives on the unknown; social stories transform the unknown into a previewed script. ₹200–800 | DIY: ₹0 (handwritten notebook + photos)
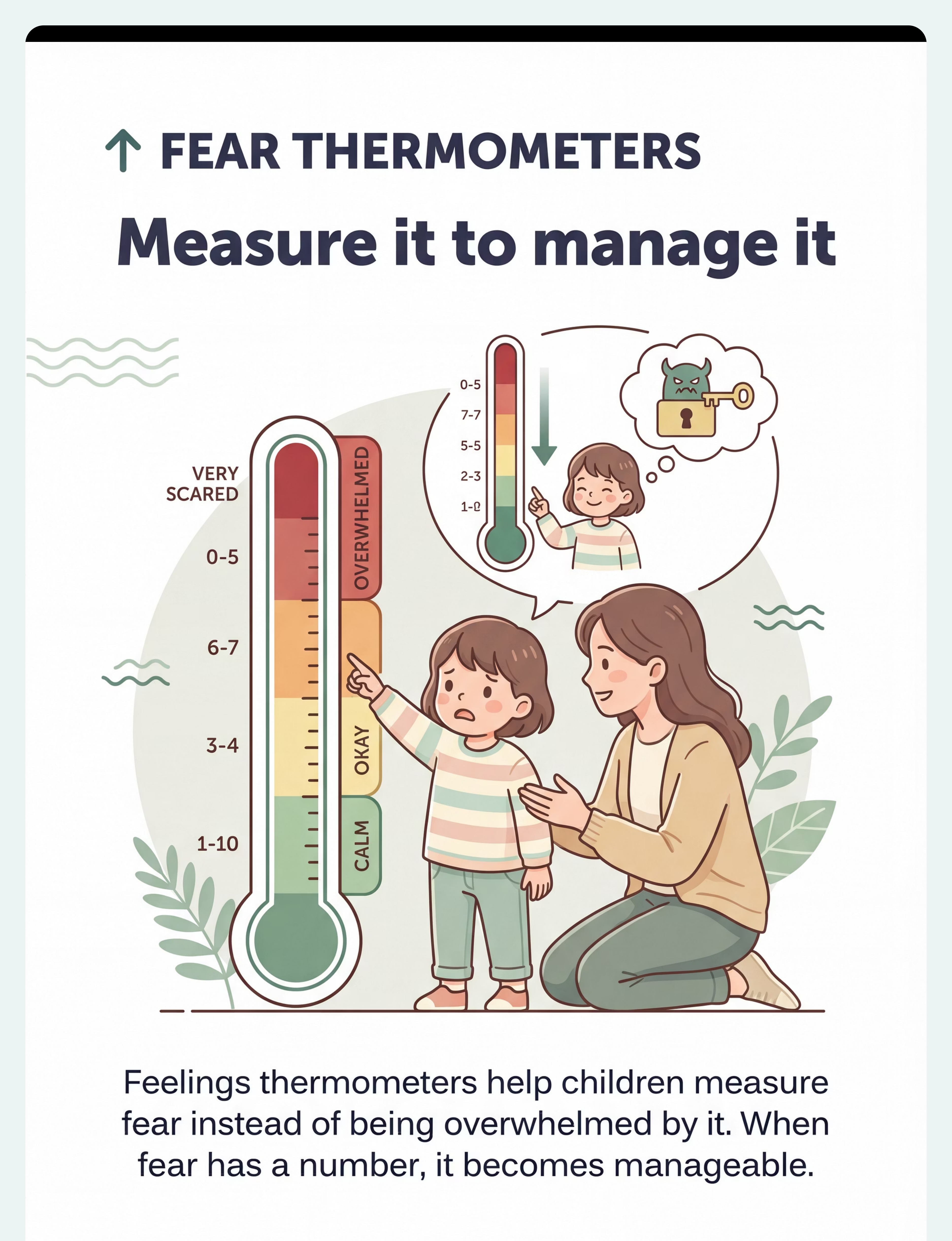
Feelings Thermometers and Fear Scales
1–10 visual scale (colours, faces, thermometer levels) allowing children to name and communicate their fear intensity. Externalises fear — makes it something the child has, not something they are. ₹100–500 | DIY: ₹0 (drawn on paper)
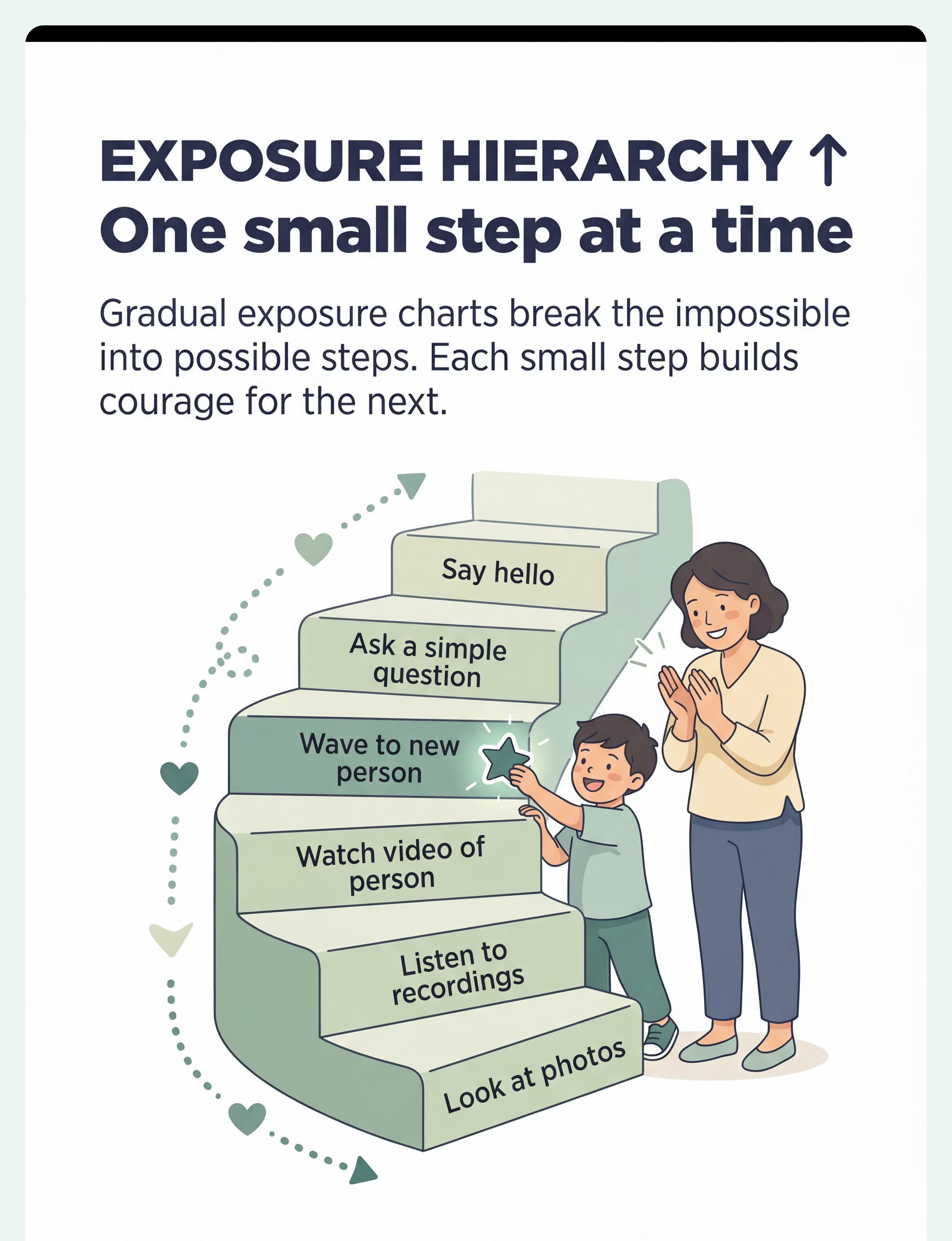
Gradual Exposure Hierarchy Charts
A visual ladder showing graduated steps from least-scary (looking at photos) to most-scary (direct interaction). Child has agency. Progress is visible. Hope is concrete. ₹100–400 | DIY: ₹0 (ladder drawing with stickers)
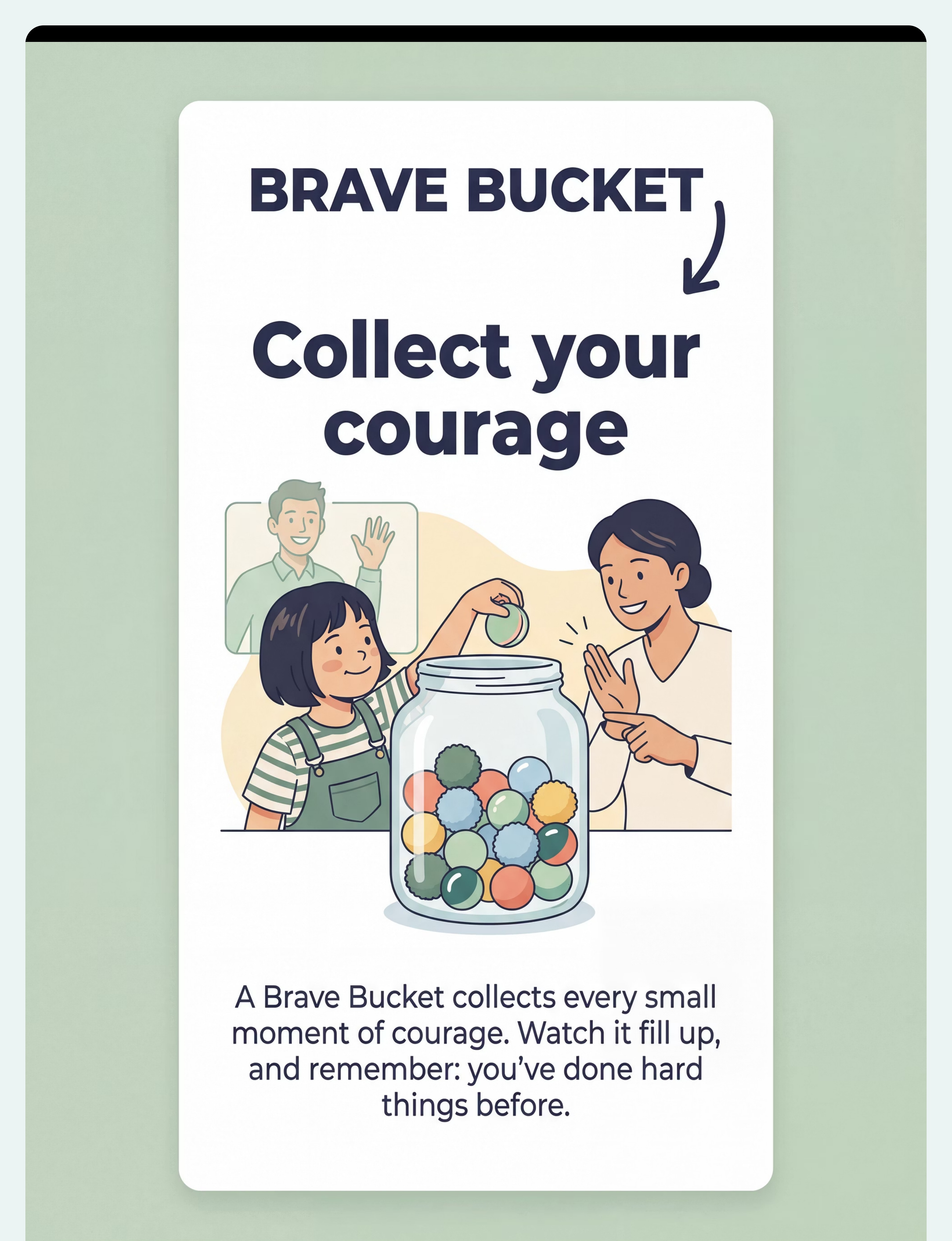
Brave Bucket / Courage Collector
A clear jar + tokens (pom-poms, marbles) that collects every small moment of courage. Reframes identity from "scared child" to "child who is learning to be brave." The full bucket is physical proof. ₹364–589 | DIY: ₹0 (any jar + pom-poms) | Buy the Brave Jar →
Safe Person Introduction Cards
Simple cards (photo + name + 2 facts + "safe person" confirmation) reviewed before meeting specific new people. Transforms complete strangers into "people I know about." ₹50–300 | DIY: ₹0 (index cards)
Transitional Objects and Comfort Items
A beloved stuffed animal or parent's item carried into new-people situations as a portable anchor to safety. Multi-sensory grounding — familiar texture, smell, visual — activates the calm state associated with home. ₹425 | DIY: ₹0 (child's existing comfort item) | Buy Comfort Toy →
Puppets and Persona Dolls for Role-Play
Hand puppets or finger puppets used to rehearse new-people encounters without the pressure of real interaction. One step removed — safer, more controllable. The puppet takes the risk first. ₹200–1,000 | DIY: ₹0 (sock puppets)
Photo Books of Familiar People and Places
Organised photo albums reviewed regularly to prevent familiar faces from becoming strangers between visits. Faces forgotten become strangers again — regular review maintains familiarity. ₹200–800 | DIY: ₹0 (smartphone gallery)
Calm-Down and Coping Strategy Cards
Pocket-sized cards showing coping strategies to use when fear rises during new-people encounters. In acute fear, the brain can only access already-practised skills — the card is the reminder. ₹50–300 | DIY: ₹0 (5 index cards, laminated with tape)
🔆 Need help choosing the right materials for your child's specific profile? FREE National Autism Helpline: 9100 181 181 — 16+ languages, 24×7. Our specialists will guide you to the right starting point.

Every technique on this page can be done for ₹0.
WHO/UNICEF equity principle: therapeutic access must not depend on purchasing power. Every material in this toolkit has an equally effective home-made equivalent. The therapeutic mechanism is in the practice — not the product.
Clinical Version
- Social Story book — ₹200–800
- Printed Fear Thermometer — ₹100–500
- Exposure Hierarchy chart — ₹100–400
- Brave Bucket clear jar — ₹589
- Introduction Cards printed — ₹50–300
- Comfort Toy (dedicated) — ₹425
- Hand Puppets — ₹200–1,000
- Printed Photo Album — ₹200–800
- Coping Cards printed set — ₹50–300
₹0 Home Version
- Handwritten notebook + your child's own photos
- Drawn on paper — 5 circles in green/red/orange
- Ladder drawing on any paper with sticker rungs
- Any jar + pom-poms or coins from home
- Index cards + printed/cut photos
- Your child's existing beloved stuffed animal
- Sock puppets — 5 minutes to make
- Phone photo gallery organised by person
- 5 index cards, one strategy each, tape-laminated
Zero-Cost Starter Kit — You can begin TODAY: A notebook (social story) + paper + crayons (fear thermometer) + a jar + 20 pom-poms (brave bucket) + your child's existing comfort toy. Total cost: ₹0. Therapeutic value: Equal.

Before every session: read this.
🔴 Do Not Proceed If:
- Child is currently in meltdown or acute distress
- Child is ill, feverish, or in pain
- A traumatic incident with a new person occurred in the last 24 hours
- Child has not eaten or is overtired
- You (the parent) are currently anxious or dysregulated — children read our nervous systems
🟡 Modify Approach If:
- Child had a difficult day at school
- New person has previously caused distress
- The encounter is mandatory (doctor's appointment)
- Child is showing early signs of agitation (not yet at meltdown)
🟢 Proceed as Planned If:
- Child is calm, fed, and rested
- You have reviewed the preparation materials
- New person has been briefed on the protocol
- Comfort object is available
- Exit is clearly visible and accessible
🛑 Halt Immediately If:
- Child screams and cannot be redirected for more than 5 minutes
- Child is physically harming self or others
- Child vomits from anxiety
- Child enters complete shutdown (unresponsive)
Never flood. Forcing a child into full interaction before they are ready — even with good intentions — is not exposure therapy. It is traumatisation. It intensifies fear and destroys trust. Gradual hierarchy, at the child's pace, is the only approach with evidence behind it.

The environment is the intervention.
The physical space you create communicates safety before a single word is spoken. A well-set room tells your child's nervous system: you are in control here.
Choose a Familiar Space
Use your home, not a clinic, for first sessions. The child's nervous system should be calibrated to baseline calm before any new-person encounter.
Make the Exit Visible
Door open, child can see it at all times. Knowing they can leave is what allows them to stay. The exit is not an escape hatch — it is a safety anchor.
Set Up Materials Visibly
Fear thermometer on a low table. Brave bucket empty and waiting. Comfort object accessible. Introduction card for today's person already reviewed.
Brief the New Person in Advance
Send them this script: "Please don't approach directly. Don't crouch abruptly. Speak to me first — not to my child. Give it time. Every second they tolerate being near you is enormous progress."
Minimise Sensory Noise
TV off. Lighting warm and natural (not harsh fluorescent). Soft familiar background music at most. New people are already a sensory event — the room should be quiet.
60-second readiness check before every session.
The best session is one that starts right. Use this check as your non-negotiable gate. A session started wrong produces data about why it failed — not therapeutic benefit.
Child State ✅
- Fed within the last 2 hours
- Rested — no sleep deprivation
- No current physical discomfort or illness
- Currently calm or mildly alert (not agitated)
- No major distressing events in the last 30 minutes
Environment State ✅
- Space is set up per Card 12
- New person has been briefed
- Comfort object is available
- Exit is clear and visible
Parent State ✅
- You are calm — your nervous system is your child's signal
- You have reviewed preparation materials
- You have realistic expectations for this session
- You are not pressured by time
Decision Gate
- All green ✅ → GO — proceed to Step 1
- 1–2 amber 🟡 → MODIFY — distance only, no greeting required
- 3+ red 🔴 → POSTPONE — review social story and introduction card only today
Step 1
Begin 24–48 Hours Before
The Preparation — Make the Unknown Known
Fear is always about the unknown. The single most powerful thing you can do before a new-person encounter is to convert the unknown into something partially familiar — through story, image, and conversation.
Script for parents: "Tomorrow we're going to see [Name]. I have a card that tells us about them. Want to look?" [Review introduction card together.] "See? They have a dog named Cookie. Mummy thinks they're really nice. You don't have to talk to them. You can just be near them." [Use fear thermometer.] "That's okay. Nervous is okay. Let's put one brave thought in your head: New people can become familiar people."
Do This
- Review the social story together
- Review the introduction card for this specific person
- Use the fear thermometer to name current anxiety
- Prepare the comfort object: "Your brave buddy is coming"
- Validate and redirect: "Nervous is normal. You have your tools."
Avoid This
- Over-reassuring ("It'll be fine!") — this teaches the child their fear is wrong
- Forcing engagement with the introduction card — normalise resistance
- Raising the planned exposure level if fear thermometer reads 9–10

Step 2
At the Moment of Encounter
The Arrival — Lowest Demand Entry
The arrival moment sets the tone for everything that follows. The protocol for this step is simple: lowest demand, maximum safety, zero pressure. Every second your child remains in the space is the therapy.
2a. Arrival With Anchor
Child enters space with comfort object in hand and parent physically present (child behind or beside parent — never pushed forward). "We're here. You have your brave buddy. I'm right here. You don't have to do anything right now."
2b. First Visual Contact (at Distance)
New person remains minimum 2–3 metres away. No approach. No greeting directed at the child. New person speaks to parent first — this models that they are known and safe to the most trusted person in the child's world.
2c. Fear Thermometer Check
Parent quietly asks: "What number are you at right now?" Child indicates. Parent validates: "Okay, a 6. That's okay. You're here. That's brave already."
Child hiding face or gripping parent? High fear — present. Don't push. Time is the intervention. Child peeking with curiosity? Fear present but curiosity emerging. This is excellent progress. Stay calm and don't over-react to it.
Step 3
Core Therapeutic Action
The Exposure — Time in the Same Space
The single most therapeutic thing that can happen in this session is: the child remains in the same space as the new person, and nothing bad happens. Every second of this is neural rewiring. The amygdala is updating its threat assessment in real time.
Level 1 — First Sessions
Child and new person in same room. No interaction required. New person and parent talk naturally. Child plays, holds comfort object. 5–10 minutes. This is a complete success.
Level 2 — Once Level 1 is Comfortable
New person briefly acknowledges a neutral object: "Your child has a lovely toy." No direct address to child. No expectation of response. 10–15 minutes.
Level 3 — Once Level 2 is Comfortable
New person says something brief and non-demanding toward child's direction: "That's a cute puppy." No expectation of response. Any glance, nod, or ignore is success. 15–20 minutes.
Critical: Do not rush to the next level. Do not prompt the child to respond. Do not apologise for the child's behaviour. Duration beats depth. 10 minutes of presence at Level 1 beats 2 minutes of forced Level 7 every time.

Step 4
The Dosage
Repeat and Vary — How Often, How Much
Consistency is the active ingredient. The nervous system learns through repetition — not intensity. Three good, calm repetitions at the right level produce more lasting change than ten forced, high-stress sessions.
Morning Ritual (3 min daily)
Review the "our people" photo book during breakfast. Name faces. Tell one story about each. Keeps faces familiar and reduces novelty threat before encounters occur.
Brave Bucket Review (2 min, evening)
Count tokens. Celebrate recent bravery specifically: "Remember when you waved to Aunty? That token is for that." The physical counting is as important as the praise.
Social Story Reading (5 min, encounter eve)
Read the social story about meeting new people before sleep on encounter days. Practice the fear thermometer. Review the introduction card for tomorrow's specific person.
Variation by profile: For sensory seekers — add movement (wave hello while jumping). For verbal processors — have child narrate the story back. For play-preference learners — do all preparation through puppet role-play. Watch for satiation: if the child pushes materials away or shows boredom (not anxiety), end the session — 3 good reps beat 10 forced reps.

Catch the courage. Every time.
Reinforce approach behaviour — not outcome. The child doesn't have to speak to the new person. They don't have to enjoy the encounter. They just have to stay, try, or take one small step toward. That earns a token. Every time. Without exception.
Looked at Introduction Card
1 token. Courage starts with willingness to look.
Arrived in the Same Space
2 tokens. Showing up is the hardest part.
Stayed 5+ Minutes
3 tokens. Duration is the therapy.
Waved (Even Tiny)
3 tokens. A wave is a bridge.
Spoke One Word
5 tokens. Language is the final frontier.
Identity-building praise:"You are becoming a person who can do hard things."
Specific affirmation:"You stayed in the room the whole time even though your tummy was nervous. That is exactly what brave people do."
Avoid: "See? That wasn't so bad!" — this dismisses the real fear they just overcame.

End every session with a landing.
The cool-down is not optional — it is the neurological bookend that helps the child's nervous system transition out of heightened state and consolidate the session's learning. Without it, the session lingers unfinished.
2-Minute Warning
"Two more minutes, then we're all done for today." Use a visual timer if your child responds well to them. Predictable endings reduce transition anxiety.
Acknowledgement
"You did something hard today. I'm proud of you." Even if the session was difficult — they showed up. That is always true and always worth naming.
Physical Cool-Down
Child holds comfort object. Parent offers calm physical contact if child accepts. Deep breathing together: "Let's do 3 belly breaths."
Session Closing Ritual
Child drops token in Brave Bucket — the physical act of closure. "Put your brave moment in the bucket. It lives there now." Then name the next activity clearly: "After this, we'll have a snack."
Post-session parent reflection (5 min): What was their fear thermometer reading at arrival vs. end? What level was reached? What worked? What caused escalation? What will I try differently next session?
60 seconds of data now saves hours of guessing later.
Data is not bureaucracy — it is the compass. The child who is tracked is the child who is found. Three data points per session tell you more about progress than a month of impressions.
Arrival Fear Level
Child's fear thermometer reading when new person was first encountered (1–10). This is your baseline. Track whether it decreases over weeks.
Peak Exposure Level Reached
What was the highest hierarchy step reached today? (1=photos only, 3=same room, 5=wave, 7=brief conversation, 10=direct play). Track whether this climbs over time.
Duration of Tolerance
How many minutes did the child spend in the same space as the new person without acute distress? Even 30 seconds more than last week is significant and should be celebrated.
Data entered into the GPT-OS® system tracks your child's Social Engagement Readiness Index progress, adjusts recommended hierarchy steps for the next session, and alerts Pinnacle therapists if a plateau or regression is detected. Download the C-279 Session Tracking PDF →

Sessions don't always go as planned. Here's what to do.
Anxiety doesn't progress linearly. Two steps forward, one step back is not failure — it is the documented, expected pattern of fear reduction. Every difficult session holds data about what to adjust.
"She screamed as soon as the person walked in."
The exposure level was above the child's current tolerance threshold. Return to Level 1 (photos only). Increase preparation time. Brief the new person more explicitly. The hierarchy step was too high — not the child.
"He tolerated the person but completely froze and refused to engage."
Selective mutism response — typical in high-anxiety children. This is not defiance; the child's communication system shut down under anxiety. Remove all expectation of verbal engagement. Presence only. Consider SLP consultation if this persists.
"She did great today but last week was a disaster."
Anxiety doesn't progress linearly. Note what was different today (child state, specific person, environment). Replicate today's conditions. Use today's success data as your guide forward.
"He was fine during the session but had a meltdown 30 minutes after."
Delayed release — the child held it together, then released afterward. This is emotional regulation under pressure, not regression. Plan a calm, low-demand activity for 30–60 minutes after every new-person encounter.
"I'm not seeing any progress after 3 weeks."
Check data for micro-progress: 10 seconds longer tolerance, fear reading lowered by 1 point. 3 weeks may be early for macro-changes. If genuinely flat at 8 weeks, consult a Pinnacle specialist and consider professional assessment. Call 9100 181 181.
Stopping a session when the child is overwhelmed is not failure. It is excellent clinical judgement. You protected your child's trust today.
No two children are identical. Adjust everything.
The protocol is a framework, not a prescription. Your child's age, temperament, sensory profile, and diagnostic picture all shape how you adapt the materials. Here is how to personalise the approach.
For the Sensory-Sensitive Child
Brief new person: no strong perfume, no unexpected touch. Control sound level. Use the quietest, simplest comfort object. Build in sensory breaks during longer encounters. Arrival in a calm, quiet room before others enter.
For the Autistic Child
Use visual supports consistently. Provide explicit, literal scripts: "When they say hello, I can nod my head like this." Social stories with specific photos of this specific person. Longer timeline per hierarchy level — often 2–3 weeks per step.
For the Selectively Mute Child
Never require speech. Sliding-in technique: familiar person present, new person enters gradually, familiar person fades. Reinforce any sound (humming, throat-clearing), not just words. SLP consultation is essential.
For the Very Young Child (Ages 2–4)
Keep hierarchy simple: photo → same room → wave. All materials must be concrete and physical. Brave bucket is especially powerful. Social story very simple: three pages maximum. Parent-led throughout.
For the Older Child (Ages 7–10)
More cognitive involvement — explain the amygdala concept at their level. Let them design their own hierarchy. Let them choose their own coping strategies. Self-monitoring with their own data tracking sheet builds agency and ownership.

Weeks 1–2: You're planting. Not harvesting.
The establishing phase is the hardest phase emotionally for parents — because you are doing significant work without yet seeing visible results. But the neural pathways are forming. The amygdala is receiving new data. Your consistency is the intervention.
What Progress Looks Like
- Child tolerates hearing the new person's name without escalating
- Child will look at the introduction card (even briefly)
- Child arrives in the same space without screaming
- Brave bucket fills with small tokens — document every one
- Fear thermometer readings may be high (8–10) — this is accurate measurement, not failure
What Is Not Expected Yet
- Verbal engagement with the new person
- Reduced fear thermometer readings (these often briefly rise as awareness increases)
- Generalisation to other new people
- You feeling confident — this is also normal at this stage
"If your child tolerates being in the same room as a new person for 30 seconds longer than they could last week — you have two weeks of successful neural rewiring to celebrate."

Weeks 3–4: The brain is updating.
The consolidation phase is when observable micro-changes begin to emerge. These shifts may feel small from the outside — but each one is the measurable signature of the amygdala updating its threat assessment database.
Consolidation Indicators
- Child stops asking "Is anyone new going to be there?" before every outing
- Fear thermometer arrival readings beginning to decrease — even by 1–2 points
- Child initiates getting their comfort object for anticipated new-person situations
- Child looks at introduction card without being asked
- Brave bucket filling visibly — child comments on it spontaneously
- Brief positive associations forming: "The doctor has a dog named Cookie"
Neural Pathway Formation
Each exposure adds a data point to the amygdala's threat-assessment database: "This person was there, and nothing bad happened." Eight to twelve exposures typically begin showing measurable change. You may also notice: you are less anxious going into encounters yourself. Your confidence in the protocol is growing — and your child's nervous system is reading that directly.
When to increase frequency: When fear thermometer readings consistently stay below 6 for an entire session — move to the next exposure level. Do not rush this gate.

Weeks 5–8: The child is becoming.
The mastery phase is when the work becomes visible — not just to you, but in the world. Skills built in the protected space of home begin appearing in contexts you never specifically practised. This is generalisation: the hallmark of genuine learning.
Fear Threshold for Level Mastery
Fear thermometer stays below 4 for 3 consecutive sessions at a level before moving up.
Consecutive Sessions
Three consecutive sessions at threshold confirms mastery — not just one good day.
Generalisation to New People
Behaviour generalises to a second new person without restarting from Level 1.
Photo Mastery
Looks at photos of new people with curiosity, not avoidance.
Presence Mastery
20+ minutes in same space as new person, fear below 4.
Wave Mastery
Initiates a wave to familiar-but-not-daily people without prompting.
Greeting Mastery
Verbal greeting (any form) to new person after brief warm-up.
Conversation Mastery
2–3 turn exchange with new person within 10 minutes of meeting.

You did this. Your child grew because of your commitment.
You showed up for sessions when you were exhausted. You briefed new people awkwardly. You bit your tongue when you wanted to say "just say hi." You filled the brave bucket and counted tokens and read the same social story forty times. And your child — who once couldn't lift their head in the presence of anyone new — is beginning to look up.
From: A child who hid from the entire world beyond three safe people.
To: A child who has an expanding circle — who is learning that new people can become familiar people, and that they have the tools to get there.
The Brave Book
Create a photo book of all the brave moments from this journey — a visual record of courage your child can hold and revisit.
The Brave Person Award
A homemade certificate celebrating the specific achievement — named, dated, and signed. Frame it.
The Before and After Photo
Child at the beginning of this journey, child now — side by side. Visual proof of change.
The New Friend Celebration
Celebrate the first person who moved from "new" to "familiar" — the moment the technique became real.

Even in progress: know when to pause and seek help.
Progress with C-279 is common and measurable — but some presentations require professional clinical support alongside home implementation. Trust your instincts. If something feels wrong beyond what this page describes, that signal is clinical data. Call 9100 181 181.
🔴 Complete Mutism Across All Settings
Child has stopped speaking to anyone outside the immediate family — not just new people. This may indicate selective mutism requiring specialised speech-language intervention. Pause and consult.
🔴 Physical Symptoms Escalating
Vomiting from anxiety before any social encounter, panic attacks, loss of bodily functions. These indicate anxiety severity requiring medical assessment — not a more intensive home protocol.
🔴 Regression After Progress
Child who was at hierarchy Level 5 suddenly cannot tolerate Level 1. Unexplained regression may indicate a traumatic incident, major life change, or clinical anxiety escalation.
🔴 School Refusal Escalating
Fear of new people is now preventing school attendance. Educational impact requires urgent multi-disciplinary intervention — this cannot be managed through home protocol alone.
🔴 No Progress After 8 Weeks
Despite consistent protocol implementation, no measurable change on fear thermometer, hierarchy level, or duration. May indicate clinical social anxiety disorder requiring structured CBT or medication assessment.
📍Find your nearest Pinnacle centre → | FREE Helpline: 9100 181 181 — 24×7, 16+ languages
C-279 is one step on a journey. Here is the full map.
Fear of new people does not exist in isolation. It connects to a broader landscape of social-emotional development — techniques that precede it, run alongside it, and build upon it. Here is where C-279 sits in that journey.
C-277: Understanding Child Anxiety
Prerequisite. The foundation — understanding what anxiety is before you address it.
C-279: Fear of New People
You are here. Materials-Based Social Approach Scaffolding for New People Tolerance.
C-281: Building Social Confidence
Next level. From tolerating new people to actively building friendships.
C-285: Social Skills Development
Advanced. Formal social skills curriculum — entry requires comfort with new people.
→ If your child has mastered C-279
Move to C-281 (Building Social Confidence) — actively building friendships versus reducing fear of new people.
→ If C-279 didn't resonate
Try C-280 (Fear of New Places) using the same graduated exposure framework — children often transfer skills across fear contexts.
Long-Term Developmental Goal
Social Engagement Readiness → Peer Relationship Capacity → Community Participation → School Readiness → Lifelong Social Functioning. C-279 feeds into all of these.

Related techniques in the Social-Emotional Development domain.
Each technique below connects directly to C-279 — either as a foundation, a companion, or the natural next step. Together they form a complete arc from anxiety identification to confident social engagement.
C-277: Understanding Child Anxiety
⬅ PREREQUISITE | Intro Level | The foundation — understanding what anxiety is before you can address it. View Technique →
C-278: Separation Anxiety Basics
⬅ COMPANION | Intro Level | Often co-occurs with fear of new people — address together for faster progress. View Technique →
C-280: Fear of New Places
→ NEXT | Core Level | Same graduated exposure framework applied to places — skills transfer directly. View Technique →
C-281: Building Social Confidence
→ PROGRESSION | Core Level | From tolerating new people to actively building friendships. View Technique →
C-285: Social Skills Development
→ ADVANCED | Advanced Level | The formal social skills curriculum — entry requires comfort with new people. View Technique →
C-286: Fear of Trying New Things
↔ LATERAL | Core Level | Same behavioural inhibition root — often co-presents with fear of new people. View Technique →
C-279 is one piece of a larger developmental picture.
Your child's development spans twelve interconnected domains. Fear of new people sits in Domain C: Social-Emotional Development — but it connects directly to how your child processes sensation, communicates, and manages behaviour. Understanding the full picture accelerates targeted progress.
Domain Connections to C-279
- Domain B (Communication): Language skills needed to navigate new social encounters
- Domain A (Sensory): Sensory processing of new people's unpredictable input
- Domain D (Behaviour): Behavioural flexibility required to approach versus avoid
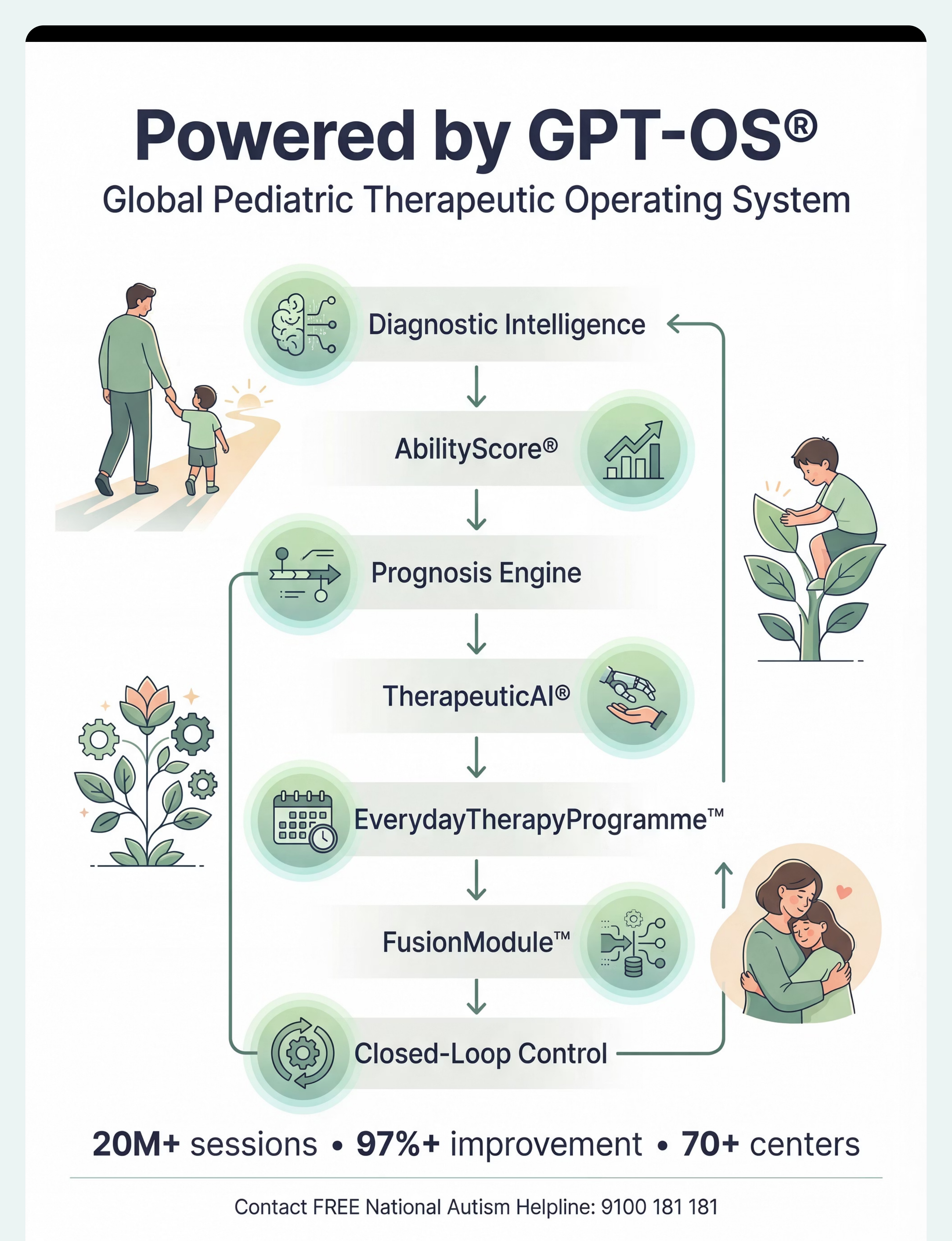
GPT-OS® Full Profile
If your child is in the GPT-OS® system, their AbilityScore® shows all 12 domains simultaneously — identifying which domains are connected to the fear of new people pattern, and which interventions will have cascading positive effects.

Families who started exactly where you are.
The transformation families describe is not dramatic or sudden. It is a thousand small moments: the first time the child didn't hide when the doorbell rang. The first token dropped in the bucket after a wave. Fear of new people doesn't disappear — it becomes manageable. And then background noise. And then a story they tell about who they used to be.
Aditi's Story — Hyderabad, Age 4→5
Before: Aditi screamed at the sound of the doorbell. Every visitor triggered 45-minute meltdowns. Her family had stopped accepting invitations. Her world had shrunk to the apartment.
After 6 months: Aditi attended her cousin's birthday party. She played with three children she had never met. She waved goodbye to the birthday girl's mother. "That was fun," she said in the car.
After 6 months: Aditi attended her cousin's birthday party. She played with three children she had never met. She waved goodbye to the birthday girl's mother. "That was fun," she said in the car.
"She used to be a child who couldn't lift her head. She is becoming a child who can walk into a room." — Aditi's mother, Pinnacle Network, Hyderabad.Outcomes vary. Illustrative case.
Rishi's Story — Bengaluru, Age 6→7
Before: Rishi's paediatrician couldn't examine him without two adults holding him. School had been postponed twice. His parents hadn't had guests in 14 months.
After 8 months: Rishi is in school. He has one friend. His paediatric appointment last month — he allowed the examination, comfort object in hand, fear thermometer reading 4. "Four is okay," he told his mother.
After 8 months: Rishi is in school. He has one friend. His paediatric appointment last month — he allowed the examination, comfort object in hand, fear thermometer reading 4. "Four is okay," he told his mother.
"When he said 'four is okay' I cried in the parking lot. Four is the most okay number I've ever heard." — Rishi's father, Pinnacle Network, Bengaluru.Outcomes vary. Illustrative case.
You are not navigating this alone.
When you connect with other parents on the same journey, your orientation time collapses. Their hard-won knowledge becomes your starting point. And when you share your wins, your experience becomes another parent's hope.
📱 C-Domain Parents WhatsApp Community
Connect with parents working on Social-Emotional Development techniques across India. Real-time support, shared wins, peer guidance. unknown link
💬 Pinnacle Parent Forums
Moderated online community: ask questions, share wins, find parents navigating the same challenge. Searchable by technique code, age, and diagnosis. Join the Forum →
👥 Local Parent Meetups
Pinnacle centres host monthly parent meetups by domain. Find your nearest centre and ask about the Social-Emotional Development parent circle. Find Your Centre →
🤝 Peer Mentoring
Connect with a parent who has completed C-279 and is further along the journey. Their experience is your fastest orientation to what actually works. Request a Mentor Match →
"Over 1,000 individuals from 111 countries contributed to the WHO Nurturing Care Framework — because community knowledge is clinical knowledge." — WHO NCF Community Engagement Principles
Home + clinic = maximum impact.
Research consistently shows that parent-implemented home practice combined with professional clinical guidance achieves outcomes 3–4× better than either alone. This page gives you the home piece. Pinnacle centres give you the clinical piece.
Specialist Matching for C-279
- Exposure hierarchy design → Child Psychologist (all centres)
- Selective mutism protocol → Paediatric SLP (60+ centres)
- Sensory regulation support → Paediatric OT (all centres)
- Behavioural reinforcement design → BCBA (all centres)
- School generalisation → Special Educator (all centres)
- Full integrated plan → FusionModule™ (all centres)
Can't Come to a Centre?
Remote families across India and internationally receive the same protocol via teleconsultation — same specialists, same protocol, same outcomes.
FREE Helpline
🔆9100 181 181 | FREE | 24×7 | 16+ languages
"I don't know where to start" is exactly what we're here for.
"I don't know where to start" is exactly what we're here for.
The science behind what you just learnt.
Every technique on this page is referenced to peer-reviewed, published research. The evidence base spans systematic reviews, randomised controlled trials, cohort studies, and population-level implementation data across India and internationally.
PMC2697319 — Behavioural Inhibition and Social Anxiety
Demonstrates behavioural inhibition in early childhood is the strongest temperamental predictor of social anxiety disorder; early intervention through graduated exposure significantly reduces anxiety development. View on PubMed →
PMC11506176 — Systematic Review of Sensory Integration Interventions (2024)
16 articles confirm sensory integration and related interventions are evidence-based practices for ASD; social engagement and adaptive behaviour are primary outcome domains. View on PubMed →
PMC10955541 — Meta-Analysis, Social-Emotional Outcomes (2024)
24 studies confirm therapy interventions effectively promote social skills, adaptive behaviour, and community participation in paediatric ASD population. View on PubMed →
DOI: 10.1007/s12098-018-2747-4 — Indian RCT (Padmanabha et al., 2019)
Home-based parent-administered interventions in Indian children achieve outcomes equivalent to clinic-delivered sessions when parents receive structured protocols. View Journal →
NCAEP 2020 — Social Stories and Visual Supports
National Clearinghouse on Autism Evidence and Practice classifies social stories and visual supports as evidence-based practices for autism. View Report →
PMC9978394 — WHO Care for Child Development Package
Implementation across 54 countries demonstrates household-material-based intervention efficacy for social-emotional development. View on PubMed →
Your data helps your child — and every child like yours.
The GPT-OS® system uses session data to personalise your child's protocol in real time — and contributes to population-level refinements that improve outcomes for every family using C-279 after you.
What GPT-OS® Learns From C-279 Data
- Which hierarchy levels most children plateau at — and what modifications help
- How fear thermometer trajectories predict long-term social engagement outcomes
- Which material combinations produce fastest progress
- How parent-reported data correlates with clinician-observed outcomes
🔒 Privacy Assurance
All session data is encrypted. No child is individually identifiable in population analysis. Data is never sold or shared with third parties. Governed by India's Digital Personal Data Protection Act 2023.

The reel that brought many families here.
This reel introduces all 9 materials in 60 seconds — each with its key mechanism explained. The reel is the awareness layer; this technique page is the execution layer. Together, they form the complete C-279 parent education experience.
Materials Covered in the Reel
- Social Stories → Preview the unknown
- Fear Thermometers → Measure it to manage it
- Exposure Hierarchy → One small step at a time
- Brave Bucket → Collect your courage
- Introduction Cards → Know them before you meet them
- Comfort Objects → Safety you can hold
- Puppets and Dolls → Practise without pressure
- Photo Books → Keep faces familiar
- Coping Cards → What to do when fear comes
Reel Details
Code: C-279
Title: "9 Materials That Help With Fear of New People"
Series: Social-Emotional Development
Episode: 279 of 999
Domain: C — Social-Emotional Development
Title: "9 Materials That Help With Fear of New People"
Series: Social-Emotional Development
Episode: 279 of 999
Domain: C — Social-Emotional Development
NCAEP 2020: Video modelling is an evidence-based practice for autism. Multi-modal learning improves parent skill acquisition.

Consistency across caregivers multiplies impact.
If only you implement this protocol, your child gets consistent support when they're with you. When grandparents, the school teacher, babysitters, and extended family also understand the approach, your child gets consistent support everywhere. That consistency is the difference between slow progress and fast progress.
Share With Family
Download the one-page Family Guide — non-technical, printable, and written for grandparents and extended family who want to help but don't know how. Download Family Guide PDF →
Explain to Grandparents
"Our child has a very strong fear response to people they don't see often. Their brain treats unfamiliar faces as danger. The most helpful thing you can do is: don't approach directly, let them come to you, don't be offended if they hide, and celebrate any glance or wave as a big victory. Your patience is the most therapeutic thing you can give."
Share With School
The school communication template explains the context, protocol for classroom introductions, how to brief substitute teachers, and what to do if the child freezes at school entry. Download School Template →

Questions parents ask most often about C-279.
My child is 2. Is it too early to start?
No — it is exactly the right time. Behavioural inhibition identified early responds faster to intervention. For 2-year-olds, focus on photo book review, comfort object pairing, and brief same-room exposures. Full hierarchy and coping cards come at 4–5+. Start where your child is.
My child has autism. Does this work differently?
Yes — with adaptations. Use more explicit, literal scripts. Social stories with actual photos of specific people. Longer timeline per hierarchy level (often 2–3 weeks per step). Sensory preparation. SLP consultation for any selective mutism component. The evidence base is strongest for autism populations.
How do I know if my child has selective mutism vs. just fear of new people?
If your child speaks fluently at home but consistently fails to speak in the presence of specific people or settings, selective mutism is possible. Both respond to graduated exposure, but selective mutism requires specialised SLP protocols. Consult Pinnacle SLP if you suspect this. Call 9100 181 181.
My relatives keep insisting she'll "grow out of it." How do I respond?
Use this language: "The paediatric research is clear that fear of new people beyond age 3 that impairs daily function does not automatically resolve. We are using evidence-based intervention — the same approach used by child psychologists."Download Family Explanation Sheet →
Should I stop going to family events until this is resolved?
No — complete avoidance maintains and intensifies fear. Modify events instead: arrive early, use introduction cards in advance, identify a "safe corner," have your exit strategy clear. Every modified exposure is therapeutic. Zero exposure is missed therapy.
The brave bucket worked for a while but now she doesn't care about it.
The reinforcer has lost value — common and expected. Switch the tokens (pom-poms → coins → stamps), change what earns tokens (raise the bar slightly), or add a milestone reward for a full bucket. Reinforcers must be individually meaningful and occasionally refreshed.
At what point should we involve a professional?
Immediately if fear prevents school attendance, causes physical symptoms, includes complete mutism, or doesn't respond to 8 weeks of home protocol. Ideally — professional involvement from the start for moderate-severe presentations. Both together produce the fastest outcomes. FREE consultation: 9100 181 181
My child is terrified of our family doctor. Is there a specific protocol?
Yes. Before the appointment: request a photo of the doctor; review daily for 2 weeks. Write a social story specifically about this doctor. On arrival: parent holds child, narrates every step. After: brave bucket tokens for every tolerating behaviour. Consider scheduling "get to know you" visits with no procedures — just presence.

From hiding to hello. One brave step at a time.
You have the science. You have the materials. You have the protocol. The only next step is: begin. Every moment you act is a moment the amygdala begins to learn. Every token in the brave bucket is a data point toward a child who can walk into a room.
★ Start This Technique Today
Launch your first C-279 session with GPT-OS® guided protocol. pinnacleblooms.org/start/C-279 →
📞 Book a Consultation
Find your nearest Pinnacle centre or book teleconsultation. FREE | 24×7
9100 181 181 →
9100 181 181 →
→ Explore Next Technique
C-280: Fear of New Places — same graduated exposure framework, new context. View C-280 →
🔆FREE National Autism Helpline: 9100 181 181 | Available in Hindi, Telugu, Tamil, Kannada, Malayalam, Bengali, Marathi, Gujarati + 8 more languages | 24 hours × 7 days × 365 days
Preview of 9 materials that help with fear of new people Therapy Material
Below is a visual preview of 9 materials that help with fear of new people therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

From fear to mastery. One technique at a time.
— The Pinnacle Blooms Consortium
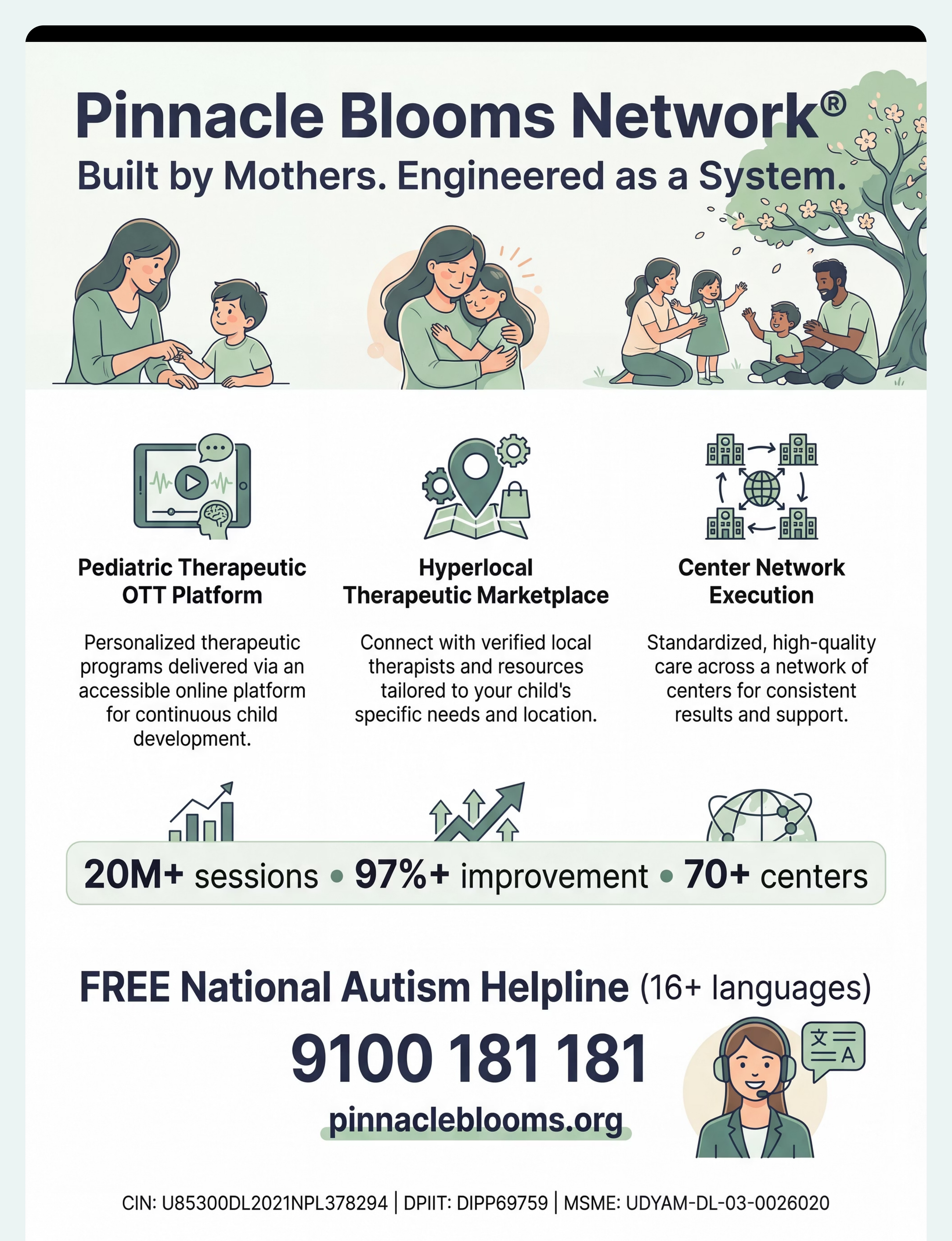
C-279 is one of 70,000+ evidence-linked intervention technique pages being built by the Pinnacle Blooms Consortium — the world's largest multi-disciplinary paediatric therapy consortium. Governed by GPT-OS®, sourced from 20M+ real therapy sessions, referenced to WHO/UNICEF/PubMed research, and designed by parents, for parents.
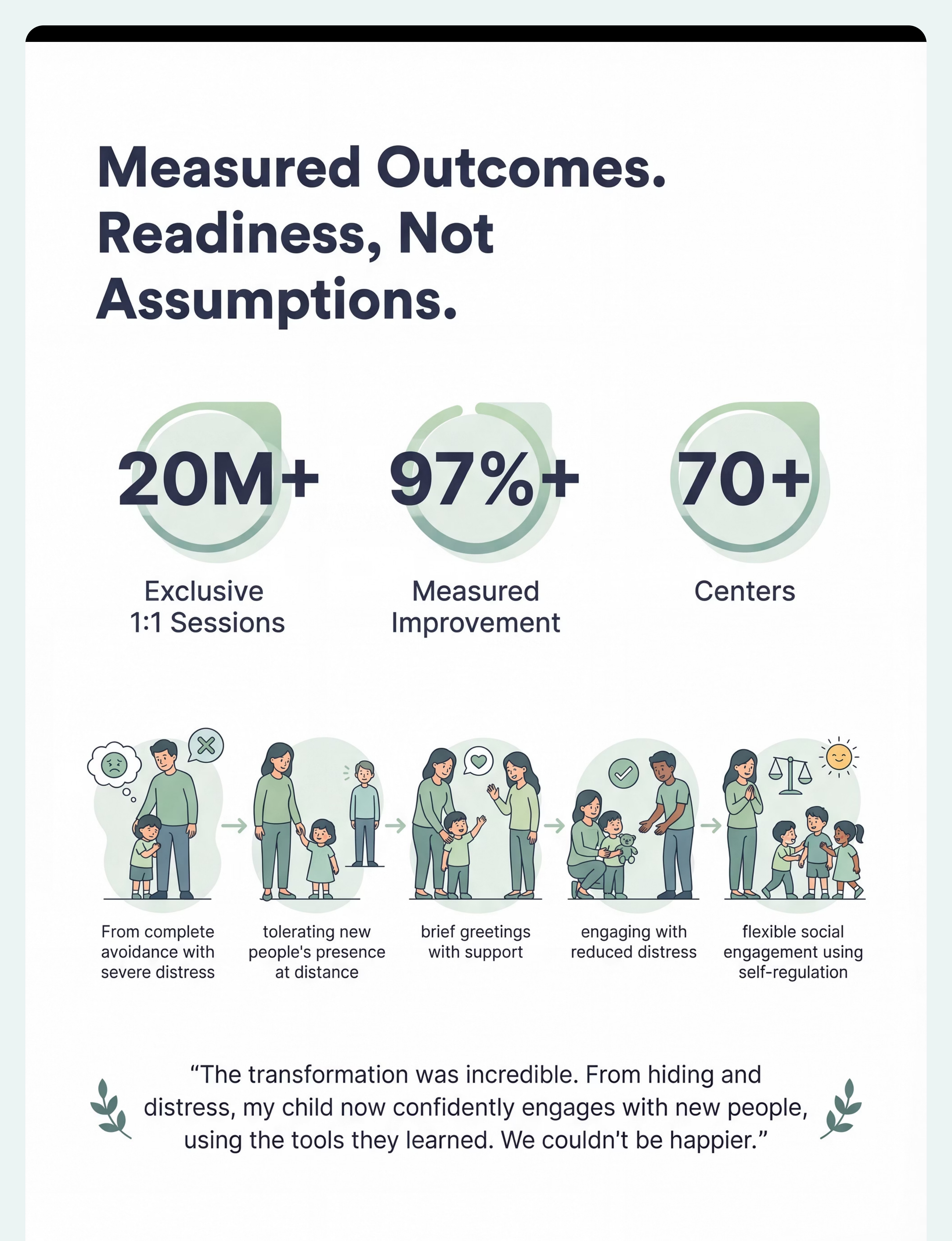
20M+
Sessions Delivered
97%+
Measured Improvement
70+
Centres Nationwide
21M+
Therapy Services
Medical Disclaimer: This content is educational. It does not replace individualised assessment and intervention planning with licensed professionals including psychologists, occupational therapists, and behavioural specialists. Social anxiety causes and interventions vary by individual. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. techniques.pinnacleblooms.org | pinnacleblooms.org
🔆FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | Always free.