
When they can't let you out of sight.
These materials help children learn that alone doesn't mean abandoned — one small step at a time.
Emotional Regulation · Series C-288 · Ages 3–12

ACT I — THE EMOTIONAL ENTRY
You can't go to the bathroom alone.
There are tiny fingers under the door and a small, panicked voice: "Mama? Mama? Are you still there?" Your child — who is seven years old, who is sweet and smart and funny — hasn't been in a room by herself for more than thirty seconds in two years.
This isn't manipulation. This is terror. Real, consuming, primal terror. And you're exhausted in a way that goes beyond tired.
You are not failing. Your child's nervous system is trying to protect her — and you can show it a different way.
Not a behavior choice
This fear is neurological — not a parenting failure or a child's defiance.
Real physiological fear
The stress response is as genuine as seeing a fire. The brain needs proof, not promises.
Solvable with the right tools
Evidence-based materials can systematically build independence, one brave moment at a time.
YOU ARE NOT ALONE
You are among millions of families navigating this exact challenge.
1 in 3
Children affected
Experience clinically significant separation anxiety at some point in childhood.
40–60%
Children with ASD
Show heightened separation anxiety and fear of being alone.
20M+
Therapy sessions
Delivered by Pinnacle — including anxiety and independence interventions.
Fear of being alone is one of the most common yet most isolating challenges parents face. You feel like you're the only family where the parent hasn't used the bathroom in privacy for two years. You're not. Millions of families globally are trapped in the same exhausting cycle — a child who cannot bear separation, a parent who has lost all privacy, a marriage suffering under the weight of constant surveillance.
The WHO's Nurturing Care Framework identifies emotional security and attachment as foundational to all child development. This is not a parenting failure. It is a nervous system that hasn't yet learned the most important developmental truth: absent does not mean gone forever.
THE NEUROSCIENCE
This is a wiring difference — not a behavior choice.
The Science
Your child's amygdala — the brain's threat-detection center — fires an emergency alarm the moment you step out of view. The hypothalamic-pituitary-adrenal (HPA) axis floods her body with cortisol. Her heart races. Her stomach hurts. Her muscles tighten.
This is a genuine physiological stress response — as real as if she saw a fire. Not because you've disappeared, but because her nervous system has mapped your absence as equivalent to danger.
Plain English
Her brain isn't being dramatic. It genuinely believes something terrible might happen when you're gone. The rational part — the prefrontal cortex — hasn't yet learned to override this alarm. She hasn't built the neural pathway that says: "Parent went to the kitchen. Parent always comes back. I am safe."
That pathway is built through experience. Through hundreds of times of you leaving and returning. Through proof, not promises.
"Verbal reassurance alone doesn't change the implicit fear system. The brain needs experiential evidence — repeated, successful experiences of being alone and surviving — to rewire the fear response." — Pinnacle Clinical Consortium

DEVELOPMENTAL CONTEXT
Your child is here. Here is where we're heading.
6–8 months
Object permanence develops. Separation anxiety begins — this is completely normal.
14–18 months
Separation anxiety peaks — child understands absence but not return. Normal.
2–3 years
Most children resolve with secure attachment experiences. Normal window.
4–7 years ⚠️
Flag Zone: Persistent or worsening fear of being alone signals unresolved anxiety needing support.
7–12 years 🎯
C-288 Target: School-age children need age-appropriate alone tolerance for full social and academic functioning.
The developmental window for natural separation tolerance resolution is 2–4 years old. When fear of being alone persists or intensifies beyond this window, the normal developmental resolution process has been disrupted. This is not the child's fault. It is not the parent's fault. It is a nervous system that needs systematic, supported help to build what other children built through ordinary developmental experiences.
LEVEL I EVIDENCE
Clinically validated. Home-applicable. Parent-proven.
This technique page synthesizes evidence from systematic review, randomized controlled trial, and 20 million real therapy sessions across 70+ centers — drafted by the Pinnacle Blooms Consortium of Pediatric OTs, SLPs, ABA Specialists, Special Educators, and NeuroDevelopmental Pediatricians.
PMC2565992 — Separation Anxiety RCT
Graduated exposure reduces separation anxiety in 87% of treated children.
NCAEP 2020
Social stories, visual supports, and reinforcement systems are classified as evidence-based for autism.
Bowlby / Ainsworth Research
Transitional objects serve a regulatory function as portable attachment figure representations.
Pinnacle Clinical Data
97%+ measured improvement across Independence Readiness Index + Anxiety Management Readiness Index.
Gold Standard Finding: Graduated exposure — systematic, stepwise increases in separation duration with successful coping — is the gold standard treatment for fear of being alone in children.

ACT II — KNOWLEDGE TRANSFER
The Alone-Time Safety Programme
Formal name: Graduated Exposure with Supportive Materials for Separation Anxiety and Fear of Being Alone
This technique cluster uses nine specific materials to systematically build a child's capacity to tolerate being alone — progressing from near-constant parental presence to age-appropriate, distress-free independent time. The approach combines graduated exposure (systematic, stepwise increases in separation) with attachment bridging (materials that maintain connection during separation) and self-regulation building (tools that teach the child to manage their own anxiety).
Age Range
3–12 years
Daily Practice
10–20 minutes, multiple short sessions per day during intensive phase
Timeline
Observable improvement in 4–8 weeks with consistent daily practice
Evidence Grade
Level I (RCT + Systematic Review)
Emotional Regulation
Anxiety Management
Independence Building
Secure Attachment
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type.
NeuroDevelopmental Pediatrician
Diagnoses anxiety disorders, ASD, and attachment disruptions. Determines whether pharmacological support is indicated alongside behavioral intervention. Supervises medical safety of graduated exposure.
Pediatric Occupational Therapist
Addresses sensory processing components that amplify alone-fear. Designs sensory-regulatory elements of calming kits and selects and sequences appropriate materials.
Pediatric Speech-Language Pathologist
Crafts social stories with appropriate language complexity. Teaches emotion vocabulary via feelings scales. Ensures communication about the fear is possible and precise.
Pediatric ABA Specialist / BCBA
Designs the graduated exposure hierarchy (separation ladder). Determines reinforcement schedules. Monitors behavior data across sessions and applies behavioral shaping.
Pediatric Special Educator
Extends separation tolerance skills to school environments. Coordinates teacher communication templates. Addresses learning impact of chronic anxiety.
The Pinnacle FusionModule™ coordinates all five disciplines into a single converged therapeutic pathway — eliminating siloed care and ensuring no discipline's gains are undermined by another's approach.

Nine barriers to alone-time tolerance — nine materials to address them.
Barrier | What's Missing | Material | |
Physical absence feels absolute | Attachment bridge | Transitional Object | |
Duration unknown → feels endless | Concrete time structure | Visual Timer | |
No voice = complete loss | Auditory connection | Walkie-Talkie | |
Narrative: "alone is danger" | Story rewriting | Social Story | |
Progress invisible | Visual progress map | Separation Ladder | |
Fear monopolizes attention | Competing engagement | Busy Box | |
Fear unnamed → unmanageable | Emotional vocabulary | Feelings Scale | |
Courage unrecognized | Motivational identity | Brave Badge | |
Anxiety has no exit strategy | Self-regulation tools | Calming Kit |
No single material addresses all dimensions of the fear. The power of this approach is the simultaneous multi-system intervention: physical connection is bridged, time is made visible, voice is maintained, narrative is rewritten, progress is mapped, attention is captured, fear is named, courage is celebrated, and anxiety management is taught.
9 MATERIALS OVERVIEW
9 Materials That Help With Fear of Being Alone
Evidence-based · Home-applicable · Zero-to-low cost options for every material
🧸 Transitional Objects
Carry your parent with you · ₹100–800 · DIY: ₹0
⏱️ Visual Timers
See the end coming · ₹300–1,500 · DIY: free apps
📻 Walkie-Talkies
Hear me when you can't see me · ₹500–2,000 · DIY: intercom app
📖 Social Stories
Rewrite the fear narrative · ₹0–600 · Fully DIY
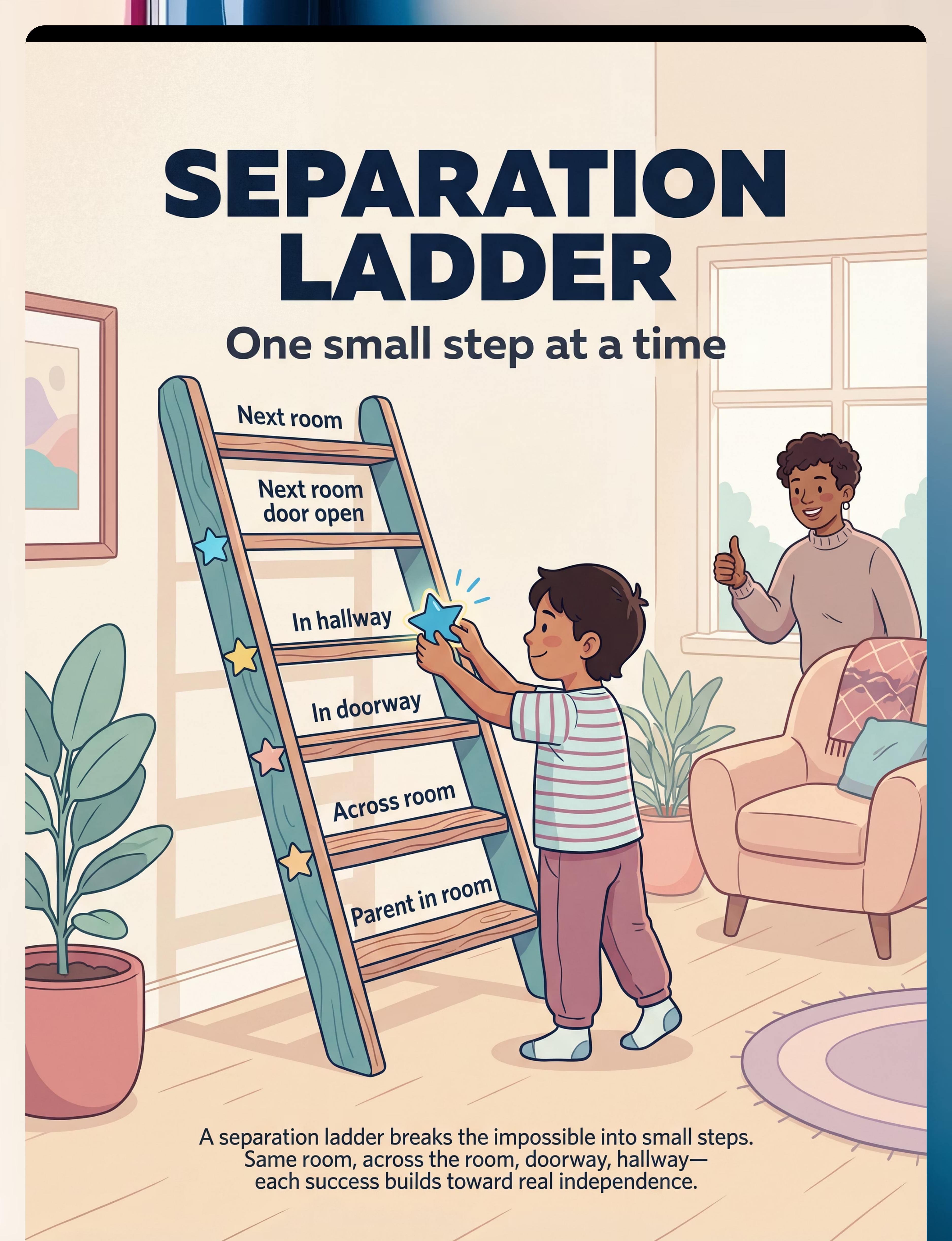
🪜 Separation Ladder
One small step at a time · ₹0–400 · Fully DIY
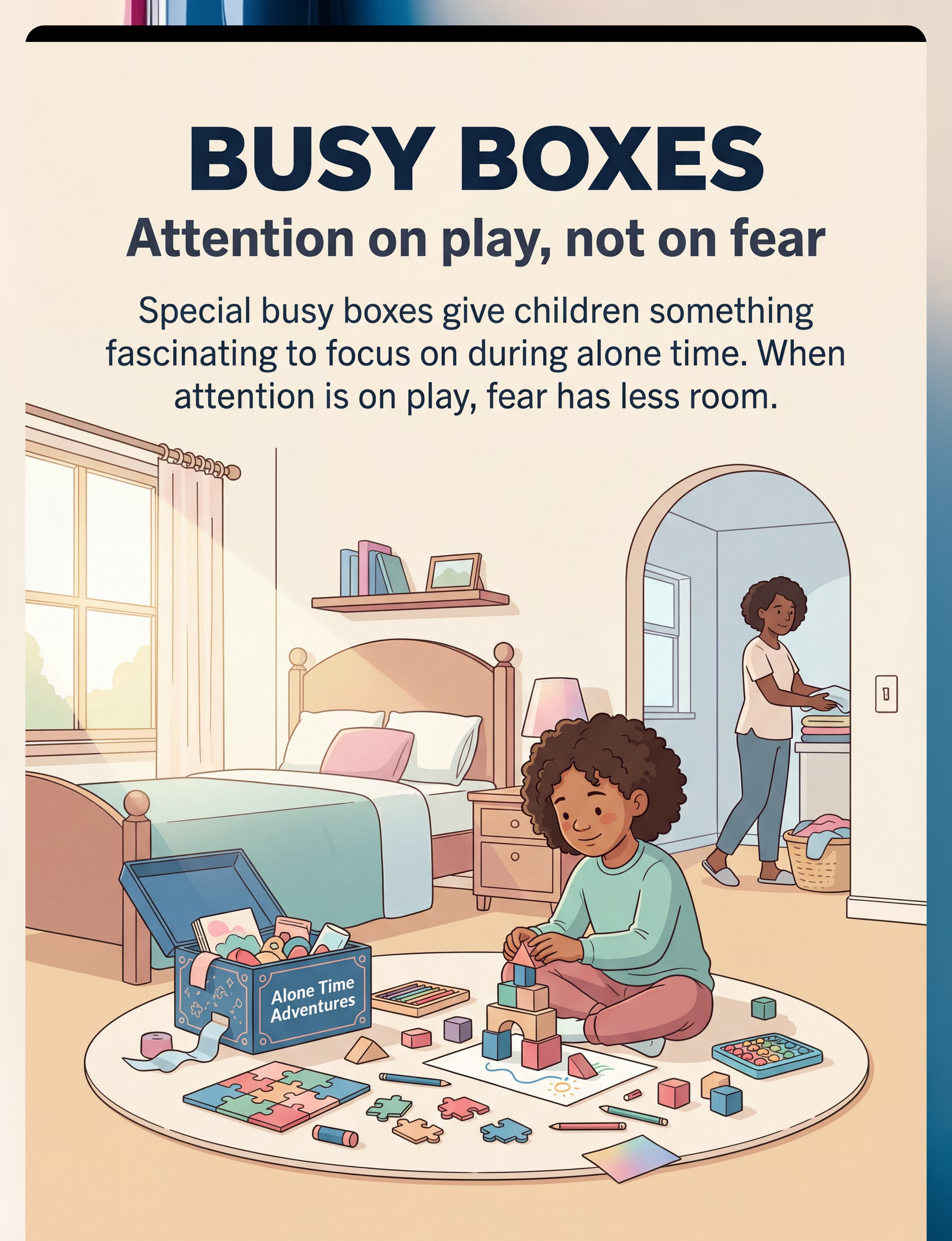
📦 Busy Boxes
Attention on play, not fear · ₹300–1,500 · DIY: ₹0
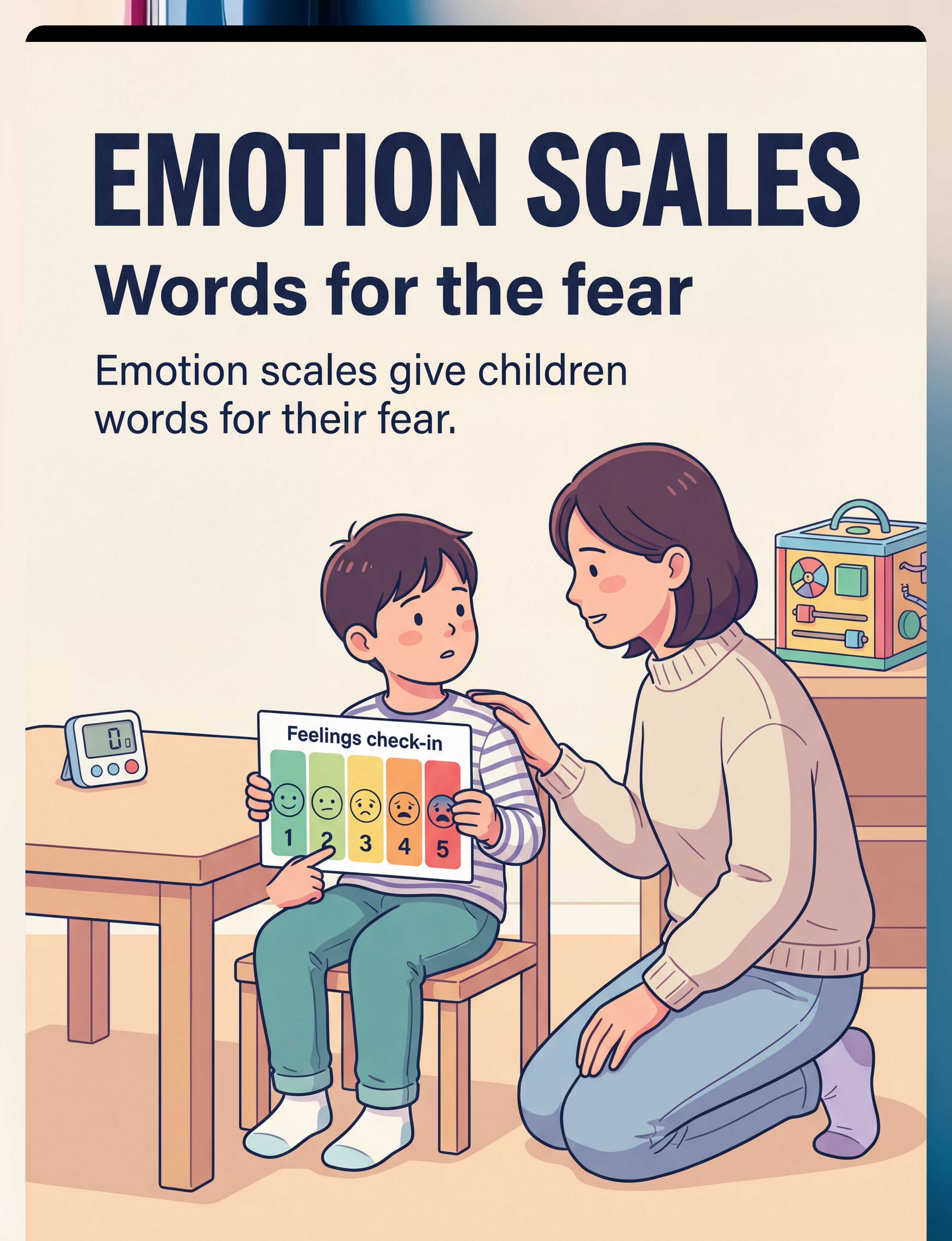
🌡️ Emotion Scales
Words for the fear · ₹0–500 · Fully DIY
🏅 Brave Badges
Celebrate every step · ₹0–500 · Fully DIY
🧘 Calming Kits
Tools to manage the fear · ₹300–1,000 · DIY: ₹100–300
Starter Kit Recommendation: For families beginning today — the essential four: Transitional Object + Visual Timer + Reward Chart + One Highly Engaging Busy Box. Total cost: ₹500–2,500 or ₹0 with DIY options.
MATERIAL 1 of 9
🧸 Transitional Objects
Carry Your Parent With You · ₹100–800 · DIY: ₹0
Transitional objects serve as portable representations of the attachment figure — physical bridges between "with parent" and "without parent." When a child holds something that carries the parent's presence — a shirt that smells like Mama, a special object the parent has blessed, a framed photo, a recorded voice message — the child is not truly alone. The amygdala's threat alarm quiets because the nervous system's attachment signal is satisfied by proxy.
This is not a crutch. This is a stepping stone. Over time, the child internalizes the security the object represents and needs it less. But in early stages, it is a crucial bridge between dependence and independence.
Scent-charge the object
Sleep with a small stuffed animal or fabric square for 3 nights — it absorbs your scent.
Present with ceremony
"This is your Mama Bear. I put my love into it. When you hold it, I'm with you."
Practice with it
Hold Mama Bear for 30 seconds while parent stands in the doorway. Gradually extend.
Refresh weekly
Sleep with the item again each week. A faded-scent item loses its power. Always have a backup.
The child isn't fully alone when holding something that represents you. This makes the first steps possible.
MATERIAL 2 of 9
⏱️ Visual Timers
See the End Coming · ₹300–1,500 · DIY: Free apps
Fear of being alone is partly fear of the unknown. "How long will this last? Will it ever end?" The child cannot see time. "I'll be back soon" means nothing to a frightened nervous system — because "soon" could be forever. Visual timers transform abstract time into a concrete, visible, shrinking entity. The child watches the red section shrink. Time is passing. The end is approaching. And when the timer ends — and parent returns exactly when promised — the child receives the most powerful medicine there is: proof that separations end, and parents return.
Begin with 30-second timer — guarantee success
Say: "I'm going to the kitchen. Watch the timer. When the red is all gone, I'll be back."
Return at exactly 30 seconds — or slightly before
Celebrate: "You did it! The timer worked!"
Progress after 3 successes at each level
45 seconds → 1 minute → 2 minutes. Never rush the ladder.
Absolute Rule: Always return when timer ends. Never late. This is non-negotiable. The timer is a promise — and keeping it builds everything.
Unknown duration feels endless. Known, visible duration feels survivable.
Unknown duration feels endless. Known, visible duration feels survivable.

MATERIAL 3 of 9
📻 Walkie-Talkies
Hear Me When You Can't See Me · ₹500–2,000 · DIY: Baby monitor or intercom app
The terror of being alone often centers on the complete absence of the attachment figure — no sight, no sound, no confirmation they still exist. Walkie-talkies or audio monitors maintain an auditory tether even when visual connection is broken. The child can hear the parent moving in the kitchen, humming, or can press a button and hear immediate response: "I'm here. I hear you. I love you."
This is a critical intermediate step: more separation than being in the same room, less than complete absence. It teaches: I can be in a different room and still be connected. Over time, the child calls less frequently, then not at all — but in early stages, this auditory bridge makes the impossible possible.
What to use
- Child-friendly walkie-talkies (bright colors, simple buttons) — ₹800–2,000
- Two-way baby monitors — ₹800–1,500
- Intercom apps on old smartphones/tablets — ₹0
- Simple speakerphone call between two phones
DIY Protocol
- Practice first with door open and parent visible
- Show child: "Press this button when you want to talk. I'll always answer."
- Respond to every call within 5 seconds initially
- Gradually allow 10-second, then 30-second delays
- As confidence builds, calls become naturally less frequent
Auditory connection is a bridge between togetherness and true separation. Use it as a stepping stone — not a permanent endpoint.

MATERIAL 4 of 9
📖 Social Stories
Rewrite the Fear Narrative · ₹0–600 · Fully DIY
Children with fear of being alone carry a catastrophic internal narrative: "If I'm alone, something terrible will happen. If I can't see Mama, she might disappear. Alone means abandoned." This narrative lives in language and story — and language and story can change it. Social stories, developed by Carol Gray and validated across thousands of anxiety studies, directly address catastrophic beliefs by walking through what actually happens during separations.
Read repeatedly — daily, especially before practice sessions — this rewires the narrative from alone = danger to alone = temporary and safe.
My name is [Child's Name]. Sometimes Mama goes to the kitchen. When Mama goes to the kitchen, she is still in the house. She can hear me. She always comes back. Nothing bad has happened to me when Mama was in the kitchen. I am safe in the living room. I can play with my toys. When the timer goes, Mama comes back. I am brave. I can do this.
Write with real names and real rooms
Use the child's actual name and actual rooms in your home — specificity is key.
Print, laminate, add real photos
Include photos of child in room, parent in kitchen, and happy reunion.
Read together 2x daily
Once in the morning, once just before a practice session.
Update as child progresses
Revise the story to reflect new separation milestones as they're achieved.

MATERIAL 5 of 9
🪜 The Separation Ladder
One Small Step at a Time · ₹0–400 · Fully DIY
Fear of being alone often presents as all-or-nothing: either parent is here, or parent is gone. A graduated separation ladder breaks this binary into 10–12 small, named steps, each building on the last. The child can see the full map, see exactly where they are, see that the next step is small — and see how far they've come. This is systematic desensitization made visible.
Rung 1–2: Parent in room
Parent doing own activity (30 sec) → Parent with back to child (1 min)
Rung 3–4: Parent at threshold
Parent in doorway (1 min) → Parent in hallway, voice audible (1 min)
Rung 5–7: Adjacent room
Hallway silent (2 min) → Adjacent room, door open (2 min) → Door mostly closed (3 min)
Rung 8–10: Full separation
Elsewhere in house, known location (5–10 min) → Child in own room, door closed (10–15 min)
Big fears are beaten by small steps. Each rung builds the neural pathway that says: "I survived this. I can survive the next one."
Never skip rungs. Going back is okay. The ladder never judges.
Never skip rungs. Going back is okay. The ladder never judges.

MATERIAL 6 of 9
📦 Busy Boxes
Attention on Play, Not on Fear · ₹300–1,500 · DIY: ₹0 using existing toys
Fear flourishes when attention has nowhere else to go. A child alone with nothing to do is a child alone with their fear. Busy boxes are specially curated containers of activities reserved exclusively for alone-time practice — novel, captivating, irresistible. This does three things simultaneously: it gives anxiety's spotlight-stealing something to compete with; it creates a positive association with alone time ("alone time = my special box"); and it generates absorbed, focused states in which minutes pass unnoticed.
What goes in the box
- Art supplies — only for alone time (special markers, washi tape, sticker sheets)
- Building sets partially pre-assembled for immediate engagement
- Kinetic sand or sensory materials
- Special puzzle at just-right difficulty
- Favourite book series with bookmark
- Small world play setups (animals, vehicles, figures)
The Reframe
The rule is simple: "This box ONLY comes out during Brave Alone Time."
Restricted access increases its appeal dramatically. Before practice, ask: "Which activity are you choosing from your special box today?" This shifts the frame from "I have to be alone" to "I get to open my box."
MATERIAL 7 of 9
🌡️ Emotion Scales
Words for the Fear · ₹0–500 · Fully DIY
Children often cannot articulate the nuances of their fear. "I'm scared" describes both mild nervousness and full-blown panic — and these require very different responses. Feelings cards and emotion scales give children precision in the language of fear. A 1–5 scale allows the child to communicate their internal state exactly — and proves to them that their internal states are visible, valid, and heard.
Level | Face | Feeling | What to Do | |
1 | 😊 | Totally okay | Great time to practice! | |
2 | 🙂 | A little nervous | Can practice with supports | |
3 | 😐 | Nervous | Short practice with all tools | |
4 | 😟 | Really scared | Shorter practice, more support | |
5 | 😰 | Can't do it | Not today — do calming first |
Before each practice: "What number are you at?" After: "What number were you at while I was in the kitchen?" This builds meta-awareness — the beginning of self-regulation. Building emotional literacy is a foundational skill of knowing what one feels.
What's measurable is manageable. "I'm at a 3" gives everyone a shared language for responding appropriately.

MATERIAL 8 of 9
🏅 Brave Badges
Celebrate Every Step · ₹0–500 · Fully DIY
Overcoming fear of being alone is genuinely hard work. The child who sits in the living room for two minutes while Mama is in the kitchen has just done something her nervous system told her was equivalent to surviving a disaster. She deserves recognition proportional to that effort. Brave badges, sticker charts, and token systems serve multiple evidence-based functions: they motivate continued effort, create visible success records, build identity, and shift the framing from punishment-of-fear to celebration-of-courage.
Define clear, achievable criteria
"Stay in the living room while Mama goes to the kitchen for 2 minutes."
Award immediately after success
Within 3 seconds of the target behavior — the most powerful reinforcement window.
Specific, enthusiastic praise
"You were SO brave. You sat with your nervous feeling and you stayed. That's amazing."
Mark the milestone chart
5 stars = choose dinner · 10 stars = special outing · 20 stars = biggest celebration
"You're a Brave Alone-Time Champion. Look at all your stars. Every single one means you were brave when it was hard."
Safety Note: Rewards are for genuine effort. Never withdraw reward as punishment for failing to separate. Never make the child feel shame for fear.

MATERIAL 9 of 9
🧘 Calming Kits
Tools to Manage the Fear · ₹300–1,000 · DIY: ₹100–300
When anxiety rises during alone time, children need accessible, self-deployable strategies — because the parent is, by definition, not immediately present. A calming kit transforms the child from a passive victim of their fear into an active manager of their nervous system. This is the pivotal therapeutic shift: from "I need you to make the fear stop" to "I have tools to handle my fear myself."
🌸 Breathing Card
"Smell the flower — blow the candle." 4 counts in, hold 2, out 6. Activates the parasympathetic nervous system within 60–90 seconds.
🤜 Fidget / Stress Ball
Proprioceptive and tactile input provides immediate sensory regulation when anxiety spikes.
📸 Parent Photo + Scent Object
A photo of parent and child together + something carrying the parent's scent. Visual and olfactory attachment anchors.
🔊 Recorded Voice Message
"I love you. I'm in the [room]. I'll be back when the timer goes. You're safe. You can do this."
📋 Coping Statement Cards
"I am safe." / "Mama is in the house." / "She always comes back." / "I am brave."
Teach EACH tool at calm times — make it playful. Before separation practice: "Your Brave Box is right here. Everything you need is in it." After successful use: "You used your tools! You managed your own nervous feeling. That's HUGE."

ACT III — THE EXECUTION
The best session is one that starts right.
Before any practice session, run through this quick readiness check. Pushing a session when the child is already dysregulated doesn't build confidence — it risks retraumatizing. The goal is challenging-but-manageable experiences, not overwhelming ones.
✅ Check These First
- Child is fed — not hungry
- Child has slept adequately — not overtired
- No major transitions or stressors in the last hour
- Child is in baseline calm — not already elevated
- Materials are prepared and accessible
- Parent is calm, patient, and has 20+ minutes
🟢 GO — Full Practice
5–6 checkmarks + emotion scale Level 1–2. Proceed at current ladder rung with all materials.
🟡 MODIFY — Adjust Today
3–4 checkmarks + emotion scale Level 3. Shorter duration, more tools, one rung lower on the ladder.
🔴 POSTPONE — Not Today
0–2 checkmarks + emotion scale Level 4–5. Do calming activities first. Practice tomorrow instead.
A postponed session is not a failure. Pushing through Level 4–5 distress doesn't build confidence — it retraumatizes. The goal is challenging but manageable — not overwhelming.

STEP 1 of 6 · 30–60 SECONDS
The Invitation
"[Child's name], we're going to do our Brave Alone Time practice. I'm going to [kitchen/hallway/other room] for [timer duration]. You have your [transitional object], your timer, your [walkie-talkie if using], and your Brave Box. When the timer goes, I'll come right back. What number are you at?"
What to do
- Get eye level with child before leaving
- Show the timer, show the duration ("This much red")
- Hand over transitional object and walkie-talkie
- Maintain calm, confident energy — not apologetic, not tense
- Wait for child to acknowledge before leaving
Reading the signals
🟢 Green light to proceed: Child nods or says okay, emotion scale 1–3, no physical blocking.
🔴 Modify instead: Child grabs parent, cries before parent moves, emotion scale 4–5.
If resistance: "Okay, I'll just go to the doorway for 30 seconds. I'll be able to see you the whole time. Ready?"
STEPS 2–4 · THE PRACTICE + RETURN + COOL-DOWN
The Practice, the Return, and the Cool-Down
1
Step 2: The Separation
Go to the agreed location and stay there. Return at or slightly before the timer ends — never late. If using walkie-talkie, respond promptly to every call. If the child shows escalating distress, return early without shame: "You did so well to try."
2
Step 3: The Return & Reinforce
"You did it! You stayed so brave! How was that? What number are you at now? Look — you just proved that alone time is okay and I always come back. Let's put your star on the chart!" Award the brave badge within 3 seconds. Acknowledge: "You were nervous AND you stayed — that's amazing."
3
Step 4: The Cool-Down
Allow child-led transition back to normal activity. Brief debrief: "What helped today? What should we try next time?" Physical reconnection — a hug, sit together. Then normalise it: "That was great practice. What are we having for lunch?"
Child's response spectrum during separation: Ideal = engaged with busy box, regulated. Acceptable = slightly anxious but staying. Concerning = crying intensely, escalating. If concerning: return early, reduce the rung next session, never push through full panic.
DATA CAPTURE
Within 60 seconds of session end — record these three things.
Data captured now becomes the evidence that drives progress. Three weeks of tracking gives you and your therapist a picture no single session observation can provide — showing which materials work best, what times of day yield best results, and exactly how far your child has come.
📅 | Date | Today's date | |
🪜 | Ladder Rung | Which step you practiced | |
⏱️ | Duration | How many minutes/seconds | |
🌡️ | Before Level | Child's emotion scale rating before | |
🌡️ | After Level | Child's emotion scale rating after | |
✅ | Success? | Full / Partial / Postponed | |
📝 | Notes | What worked, what didn't, what to try next |
GPT-OS® Integration: Track via the EverydayTherapyProgramme™ — your therapist sees your home practice data in real time, adapts the programme accordingly, and celebrates your child's progress with you.

ACT IV — THE PROGRESS ARC · WEEKS 1–2
Week 1–2: What to Expect
15%
Progress
You are here. The foundation is being built.
✅ What you will see
- Child participates in practice without catastrophic meltdown — even if distressed, this is progress
- Timer is accepted as a structure — child watches, anticipates return
- Transitional object is held and used during brief separations
- Walkie-talkie calls decrease slightly across the week
- Emotion scale ratings decrease slightly post-practice vs. pre-practice
⏳ Not progress yet
- Spontaneous independent play without practice
- Comfortable bedtime routine
- Parent going to bathroom without distress
If your child tolerates 30 seconds longer than last week — that is real progress. Neural pathways are forming. Evidence is accumulating. The brain is learning.
Parent emotional preparation: This week is the hardest. Stay consistent. The return-when-promised is the foundation of everything.
PROGRESS ARC · WEEKS 3–4
Week 3–4: Consolidation
40%
Progress
The neural pathway is forming. The prefrontal cortex is beginning to override the alarm.
Child anticipates practice
Begins preparing their busy box without prompting. The routine is taking hold.
Timer is referenced spontaneously
"How much red is left?" — the child is engaging with time as a concrete, manageable structure.
Walkie-talkie calls reduce significantly
Child may go 3–5 minutes without calling. Each silent minute is a win.
Emotion scale levels dropping
Pre-practice levels shifting from 3–4 down to 2–3 on average.
Genuine engagement with busy box
First moments of truly absorbed play — not just distraction, but real independent focus.
Child shows chart proudly
May reference progress to another family member. Identity as a "brave child" is beginning to form.

PROGRESS ARC · WEEKS 5–8
Week 5–8: Emerging Independence
70%
Progress
Emerging independence. Synaptic strengthening through repeated structured input.
5–10 min alone
Completing sessions with low distress and all materials in place.
Spontaneous play begins
Independent play starting without being prompted by practice sessions.
Brave chart filling up
Child is proud. Identity as a "Brave Alone-Time Champion" is real now.
Bedtime improving
Falling asleep with parent nearby but not necessarily in the room — a major milestone.
What's happening neurologically: The "alone is safe" pathway is now strong enough to be accessed reliably. The amygdala no longer fires immediately — it waits for more evidence before alarming. The prefrontal cortex is winning.
CELEBRATE
You did this. Your child grew because of your commitment.
From "I can't go to the bathroom alone" → to "My child played in her room for 20 minutes while I folded laundry."
From "She follows me like a shadow" → to "She said 'I'm going to read in my room for a while.'"
From "I haven't had a private moment in two years" → to "She's not afraid anymore."
You stayed patient when it was exhausting. You returned every single time when you said you would. You celebrated courage, not just success. You gave your child the evidence her nervous system needed. You built the neural pathway, one brave moment at a time.
Family Celebration Suggestion: Hold a "Brave Alone-Time Graduation." Frame the filled sticker chart. Take a photo. Let the child explain to grandparents: "I learned to be brave about being alone." This moment matters.
Parent Wellbeing Note: Your exhaustion was valid. Your need for privacy was valid. Building your child's independence was right for both of you.
Parent Wellbeing Note: Your exhaustion was valid. Your need for privacy was valid. Building your child's independence was right for both of you.

SAFETY
Trust your instincts. If something feels wrong, pause and ask.
Most children make steady progress with consistent home strategies. But some presentations require professional assessment. Use these red flags as a checklist — if one or more applies, reach out before continuing the programme independently.
No improvement after 6–8 weeks
Consistent daily practice with zero measurable change signals a need for professional assessment.
Panic attacks with physical symptoms
Heart racing, vomiting, hyperventilating, or fainting during separation attempts.
Intrusive thoughts about harm
Fear accompanied by thoughts about harm to parent or self requires immediate professional evaluation.
Sudden regression after progress
A potential triggering event may need to be identified and addressed clinically.
Refusal of food, school, or major functions
Significant functional impairment across multiple domains requires specialist involvement.
Escalation Pathway: Self-resolve → Pinnacle Helpline consultation → Teleconsult with Pinnacle therapist → In-center assessment → Specialist referral
THE PROGRESSION PATHWAY
This technique is a waypoint — not a destination.
C-288 sits within a carefully sequenced clinical pathway. Progress here directly enables progress in related domains. The long-term developmental goal is a child who can spend time alone and deeply enjoy togetherness — not trapped in fear of either state.
Child's Response Pattern | Next Technique | |
Alone at home resolved → general anxiety remains | C-286: Understanding Child Anxiety | |
Alone at home resolved → nighttime still challenging | C-290: Nighttime Fears and Sleep Anxiety | |
Home independence achieved → school separation remains | C-295: School Separation Anxiety | |
Progress stalled at medium ladder rung | C-287: Fear of New Experiences (parallel work) |
RELATED TECHNIQUES
Explore the Full Emotional Regulation Domain
The foundation for all anxiety work — understanding the nervous system, the fear cycle, and how to break it.
Parallel work for children who struggle with novelty alongside separation — highly complementary to C-288.
Building environmental confidence — the natural next step after home independence is established.
Extending alone-time tolerance into the night — the hardest frontier for many families.
Translating home independence gains into school functioning — a critical developmental milestone.
Parent Support Resources
K-1800: Supporting an Anxious Child · K-1805: Parent Self-Care · K-1810: When Reassurance Doesn't Work
Domain C: Emotional Regulation — 128 Canon Materials · 70+ Intervention Techniques · 12 Subdomains. C-288 sits in Subdomain C3: Anxiety & Fear Management alongside 29 related techniques spanning understanding anxiety, specific fears, generalized anxiety, social anxiety, and performance anxiety.

ACT V — COMMUNITY & ECOSYSTEM
Stories from the Pinnacle Network
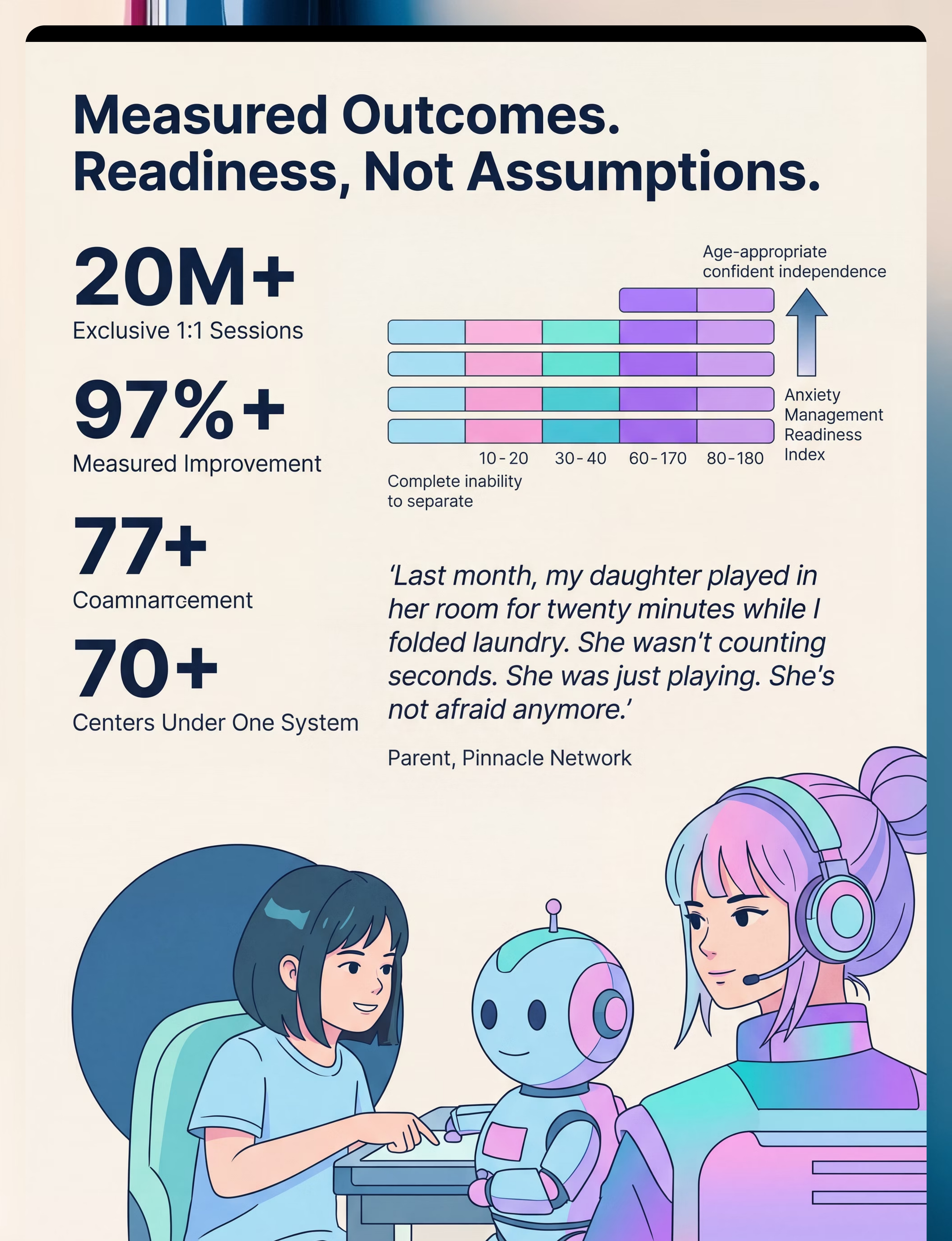
"Last month, my daughter played in her room for twenty minutes while I folded laundry. Twenty minutes. Alone. No walkie-talkie, no timer. When I came to check on her, she looked up and said 'Hi Mama!' and went back to her toys. Two years ago, she couldn't let me walk to the bathroom. Last night, she said 'I'm going to read in my room for a while.' I sat on the couch and cried. Happy tears. She's not afraid anymore."
— Parent, Pinnacle Network(Illustrative case; outcomes vary)
"We tried everything — reassurance, firmness, rewards, nothing worked. Our son was 9 and still couldn't be in a room alone for 60 seconds. Three months after starting the separation ladder with our Pinnacle therapist, he's playing independently for 30 minutes while I cook dinner. He uses his calm box when he feels nervous. He moves his star up the ladder himself. He's proud of himself. That's the part that gets me — he's proud."
— Parent, Pinnacle Center, Hyderabad(Illustrative case)
You don't have to figure this out alone.
WhatsApp Community
Families supporting anxious children, sharing strategies in real time. A warm, moderated community of parents who truly understand.
Pinnacle Parent Forums
Parent forums, Q&A with therapists, technique discussions. Visit pinnacleblooms.org/community or email care@pinnacleblooms.org.
Find a Pinnacle Center
70+ locations across India. In-person assessment, therapy, and FusionModule™ coordinated care. pinnacleblooms.org/find-a-center
FREE National Autism Helpline
📞9100 181 181 — 24x7, 16+ languages. Free screening conversations, referrals, and caregiver support.

PROFESSIONAL SUPPORT
When you're ready for structured, expert-led intervention.
AbilityScore® Assessment
Establish baseline across Independence Readiness Index + Anxiety Management Readiness Index. Patented 0–1000 developmental score.
Psychology + Behavioral Services
Anxiety assessment, attachment evaluation, CBT-based intervention, and BCBA-designed graduated exposure with systematic data collection.
OT + Family Therapy
Sensory profile assessment, regulatory support, and systemic family therapy for the whole unit — not just the child.
EverydayTherapyProgramme™
Clinical plans translated into daily home-executable micro-interventions. Your therapist sees your home data in real time.
FusionModule™ Coordinated Plan
OT + SLP + ABA + SpEd + Medical → single converged pathway. No siloed care. No conflicting approaches.
RESEARCH LIBRARY
The evidence base behind this technique page.
Randomized controlled trial: graduated exposure for separation anxiety disorder in children. 87% symptom reduction.
Social stories, visual supports, reinforcement: evidence-based for autism. Cross-discipline validated practices.
Emotional security as foundational to all developmental domains. Implemented in 54+ countries.
Implementation evidence from global scale deployment of CCD package across low-resource settings.
Sensory integration and intervention evidence-base, comprehensive review of 2024 literature.
Bowlby (1969/1982) — Attachment and Loss
Foundation of transitional object theory and graduated exposure rationale. The seminal attachment research.
Pinnacle Blooms Network Clinical Data
20M+ sessions, 97%+ measured improvement across 70+ centers. Largest pediatric therapy dataset in India.
Disclaimer: This page synthesizes published research. Individual results vary. Always consult a licensed professional for individualized assessment and intervention planning.
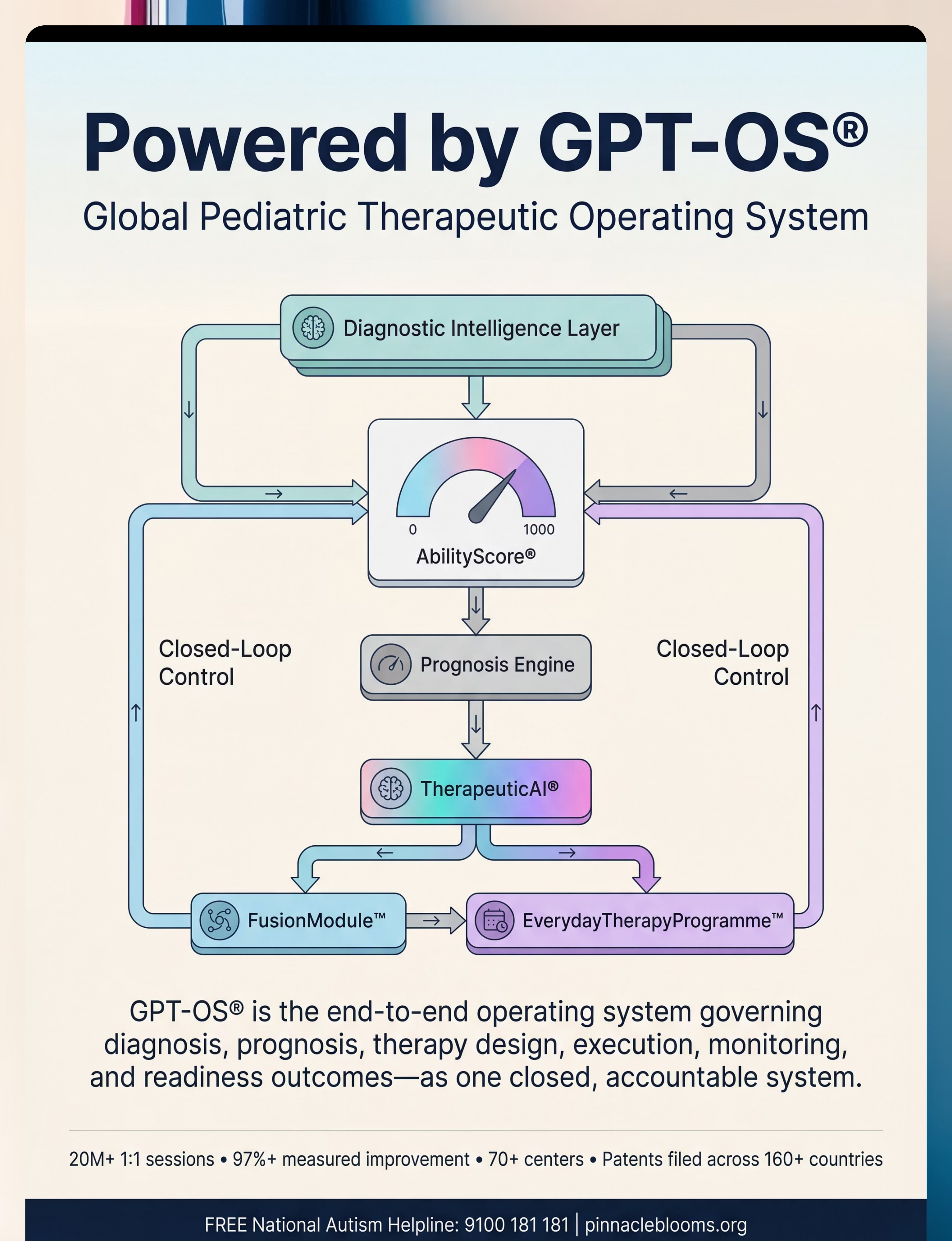
POWERED BY GPT-OS®
Global Pediatric Therapeutic Operating System
This is not software. This is therapeutic infrastructure.
Layer | Function | |
Diagnostic Intelligence Layer | 591+ structured observations → standardized diagnostic clarity | |
AbilityScore® | Patented 0–1000 universal developmental score | |
Prognosis Engine | Trajectory prediction from 20M+ session patterns | |
TherapeuticAI® | Therapy focus, sequencing, escalation — under licensed human authority | |
FusionModule™ | OT + SLP + ABA + SpEd + Medical → single converged pathway | |
EverydayTherapyProgramme™ | Clinical plans → daily home-executable micro-interventions | |
Closed-Loop Control | Observe → Score → Plan → Execute → Remeasure → Adapt |
20M+
1:1 Sessions
97%+
Measured Improvement
70+
Centers
160+
Countries Patented
WATCH IT IN ACTION
Reel C-288: 9 Materials That Help With Fear of Being Alone
Series: Emotional Regulation & Anxiety Support | Episode: 288 | Domain: ANX-SEP
"Fear of being alone is not manipulation. It's genuine terror. A child's nervous system telling them that separation means danger. These nine materials build the evidence — the real, lived, experiential proof — that alone is safe, that parents who leave always return, and that independence can be learned one small step at a time."
— Pinnacle Blooms Therapist, Reel C-288
📽️Embed C-288 Reel — 75–85 seconds
Preview coming soon — follow @pinnacleblooms for release notification.
Preview coming soon — follow @pinnacleblooms for release notification.
Related Reels in this Series:
C-286
Understanding Child Anxiety
C-287
Fear of New Experiences
C-289
Fear of New Places
C-290
Nighttime Fears
Consistency across caregivers multiplies impact.
If only one caregiver executes the technique, impact is limited. When the separation ladder, the timer system, and the brave badge protocol are consistent across Mama, Papa, grandparents, and school — the child's nervous system receives consistent evidence from every environment. Consistency multiplies impact.
For Grandparents
"Our child is learning that being alone is safe. We're practicing with special materials: a comfort toy, a timer, and a special activity box. When [child's name] is practicing, please don't rush to help or comfort unless she's in distress. Let the timer run. Trust the process. She's being brave."
For Teachers / School
"Our child is working on separation tolerance with a Pinnacle Blooms therapist. Strategies that help at home include visual timers, transitional objects, and calm-down tools. We're happy to share her Separation Ladder progress with you. Please contact us to discuss school-specific modifications."
ACT VI — THE CLOSE
Frequently Asked Questions
How long before I see real improvement?
Most families see meaningful progress within 4–6 weeks of daily practice. In weeks 1–2, progress looks like less screaming and the timer being accepted. In weeks 5–8: 10–15 minutes of independent play with low distress. Full age-appropriate independence typically requires 3–6 months of consistent practice.
Should I push through screaming and crying every session?
No. Pushing through Level 4–5 distress doesn't build confidence — it may retraumatize. If every session involves full-blown panic, go further back on the separation ladder (shorter duration, smaller steps) or seek professional guidance. The therapeutic zone is challenging but manageable — not overwhelming.
Is this separation anxiety or something more serious?
Fear of being alone exists on a spectrum. Developmentally typical separation anxiety resolves by age 3–4. Persistent, severe, functionally impairing fear — especially in children over 6 — warrants professional evaluation. Call our FREE Helpline (9100 181 181) for a screening conversation.
My child has autism — does this approach still work?
Yes, with adaptations. Children with ASD may need more explicit visual supports, slower ladder progression, and more sensory components in the calming kit. Social stories may need to be more literal and detailed. Pinnacle OT and ABA specialists are trained in exactly these adaptations.
We've tried everything. Nothing works. What next?
If consistent home strategies for 6–8 weeks have shown no improvement, seek professional assessment. Some cases of fear of being alone are rooted in trauma, attachment disruption, or anxiety disorders that require specialized intervention. Book an AbilityScore® assessment: 9100 181 181.
Can I do this without a therapist?
Many families make significant progress with home strategies alone — this page is designed to be parent-executable. However, for children with ASD, trauma history, or severe/functionally impairing fear, therapist guidance accelerates progress and prevents common mistakes.
My child regressed after several good weeks. What happened?
Regression after progress is normal. Common triggers: illness, transition (new school year, new sibling, family stress), or the non-linear nature of learning. Return to the last rung your child mastered successfully and rebuild from there. Regression is not failure — it's information.
My partner isn't consistent with this approach. What do I do?
Caregiver consistency is critical. Share this page with your partner. The research section contains the evidence base. The Family Guide PDF (downloadable above) provides a simplified explanation. A Pinnacle family therapist session to align all caregivers around the approach can be invaluable.

Your child can learn that alone is safe.
The first step is 30 seconds. A transitional object. A timer. A return when you said you would. That is the entire programme in its essence — proof, repeated until the nervous system believes it.
🚀 Start Today — Free
Download the Brave Alone Time Starter Kit. Everything you need to begin in the next 30 minutes.
📅 Book an Assessment
AbilityScore® Assessment + Anxiety Evaluation. Expert-led, data-driven, home-extended care.
📖 Explore Next Technique
C-289: Fear of New Places — the natural next step once home independence is established.
✦ Validated by the Pinnacle Blooms Therapeutic Consortium
OT · SLP · ABA · SpEd · NeuroDev Pediatrics · 20M+ sessions · 97%+ measured improvement · 70+ centers · Built by Mothers. Engineered as a System.
OT · SLP · ABA · SpEd · NeuroDev Pediatrics · 20M+ sessions · 97%+ measured improvement · 70+ centers · Built by Mothers. Engineered as a System.
Preview of 9 materials that help with fear of being alone Therapy Material
Below is a visual preview of 9 materials that help with fear of being alone therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

PINNACLE BLOOMS NETWORK®
From fear to mastery. One technique at a time.
Pinnacle Blooms Network® content is drafted by an integrated consortium of: Certified Pediatric Occupational Therapists · Pediatric Speech-Language Pathologists · Board-Certified Behavior Analysts · Pediatric Special Educators · NeuroDevelopmental Pediatricians · Regulatory Scientists · WHO/UNICEF-aligned Implementation Experts · And the most important experts of all — Mothers, Fathers, and Caregivers who have navigated this journey.
Contact & Support
📞 FREE National Autism Helpline: 9100 181 181 (24x7 · 16+ languages) · 🌐pinnacleblooms.org · 📧care@pinnacleblooms.org
Medical Disclaimer
This content is educational. It does not replace individualized assessment and intervention planning with licensed professionals. Fear and anxiety presentations vary by individual and may indicate conditions requiring professional treatment. Individual results may vary.
Statutory Identifiers
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 (Govt. of India) · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
Copyright
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique code C-288. Version 1.0. Last reviewed 2025-12-27. · techniques.pinnacleblooms.org