

"My son has to touch every doorknob three times before he can walk through. He washes his hands until they're raw and bleeding, and still doesn't feel clean. He asks me the same question forty times a day, and my answer never satisfies him. The rituals eat hours of his day. They're getting worse, not better. And when I try to stop them — the panic in his eyes is so real, so desperate, that I feel like I'm torturing him. I don't understand what's happening inside him. I just know that something has taken hold of my child, and it won't let go."
You are not failing. This is not a discipline problem. Your child's brain is trapped in an anxiety loop — and there is a treatment that works.

of all children develop clinically significant OCD — that's millions of families worldwide
of children with autism show OCD-spectrum compulsive behaviors — often underdiagnosed and undertreated
response rate with properly implemented ERP therapy — the most evidence-supported treatment in child psychiatry
Compulsive behaviors are not a parenting failure. They emerge from a neurological anxiety cycle that gains power each time a ritual is performed. Across every culture and every family, millions of children are trapped in the same loop. And the same treatment works: systematic, graduated, courageous exposure. You are among the families for whom the evidence is clearest — this gets better with the right tools.
TRIGGER → Thought, image, impulse, or situation
↓ OBSESSION → Intrusive thought generates overwhelming anxiety
↓ COMPULSION → Ritual performed to reduce distress
↓ BRIEF RELIEF → Anxiety decreases temporarily
↓ REINFORCEMENT → Brain learns: "the ritual saved you"
↓ ESCALATION → Next time, more ritual required
Brain regions: Orbitofrontal Cortex + Caudate Nucleus + Thalamus — a hyperactive "error detection" circuit treating ordinary events as emergencies.
Think of your child's brain as having an overly sensitive alarm system. The alarm goes off for everyday situations — touching a surface, leaving a room, writing a letter imperfectly. The ritual is your child's attempt to silence the alarm. It works briefly. But each time it works, the alarm becomes more sensitive, more demanding.
This is not a choice. The anxiety is real. The urge is overwhelming. The only way to reset the alarm is to face the situation without performing the ritual — and discover that nothing terrible happens.
Rigid bedtime routines, insistence on sameness — normal developmental phase. Alert if: causing >30 min disruption daily.
Lucky objects, avoiding cracks, counting games — typically transient. Alert if: preventing normal daily function.
Peak emergence of clinically significant OCD — average onset 9.6 years. Alert if: consuming >1 hour/day or causing marked distress.
Complex mental rituals, covert compulsions emerge. Alert if: interfering with school, friendships, or family life.

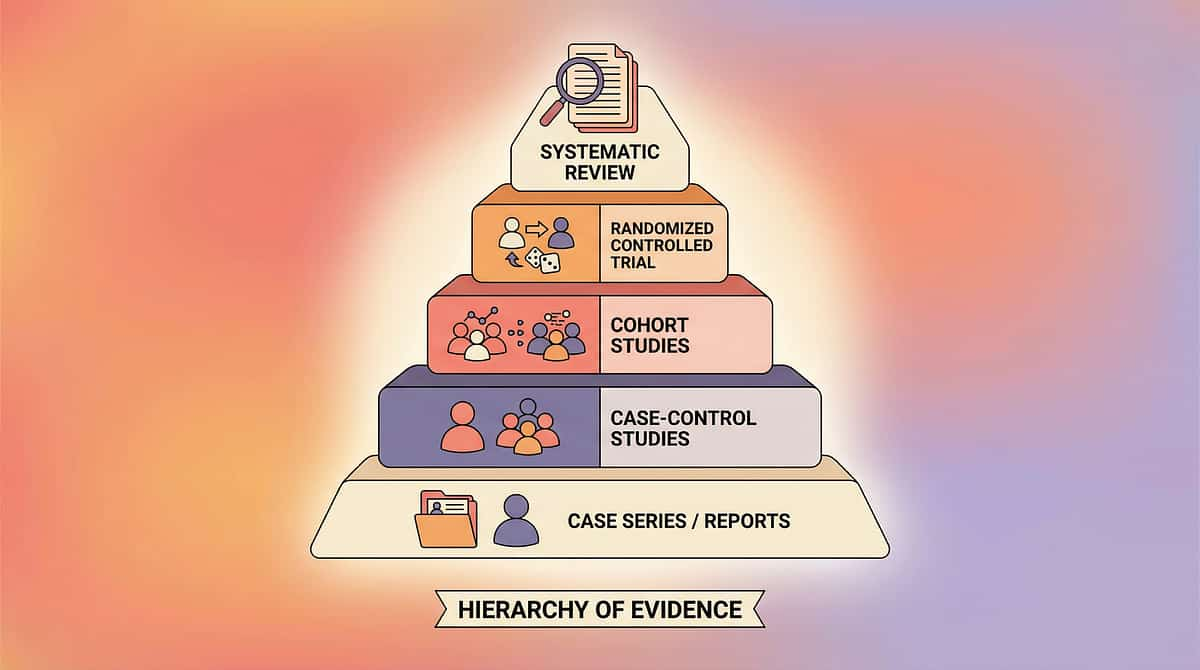
Systematic Review + Multiple Randomized Controlled Trials
Gold Standard Treatment Classification
C-295 ERP evidence sits at the top of the evidence pyramid — Systematic Reviews and RCTs confirm ERP as the most effective psychological treatment for pediatric OCD.
- March & Mulle RCT (1998): ERP produced significant symptom reduction in 87% of pediatric OCD cases — landmark trial establishing ERP as first-line treatment
- POTS Study (2004): Multi-site RCT — combined ERP + medication superior to either alone; ERP alone significantly superior to medication alone
- Meta-analysis (2021): 16 RCTs confirm ERP as most effective psychological treatment, with large effect sizes (d > 1.0)
- Pinnacle Real-World Evidence: 20M+ therapy sessions | 97%+ measured improvement in Behavioral Flexibility Readiness Index
Citations: PMC2797569 | DOI: 10.1007/s12098-018-2747-4 | NCAEP 2020 | WHO NCF 2018

Formal Name: Compulsive Behavior Intervention via Exposure and Response Prevention (ERP) Materials System | Parent-Friendly Alias: "The OCD Freedom Toolkit"
This technique introduces a curated set of 9 therapeutic materials used within Exposure and Response Prevention (ERP) therapy — the globally validated, first-line psychological treatment for compulsive behaviors and OCD in children. Each material serves a specific function in the treatment chain, forming a complete home-applicable therapeutic toolkit that supports professional ERP therapy and extends treatment into the child's daily environment.
Session Duration
3–5 formal sessions/week
With profile adaptations
Home, therapy, school, community
Habit Reversal Training / ABA
Designs and supervises the ERP protocol. Develops the fear hierarchy. Guides graduated exposures. The ERP-trained psychologist is the clinical cornerstone.
Addresses sensory components fueling compulsions. Designs competing responses based on motor patterns. Particularly valuable when OCD co-occurs with autism.
Designs reinforcement systems and victory trackers. Conducts functional analysis. Implements token economy for exposure completion.
Implements school-based accommodations. Supports exposure practice in educational settings. Manages academic impact of compulsive behaviors.
Differential diagnosis — OCD vs. autism vs. tic disorders vs. PANDAS/PANS. Medication evaluation referrals and comorbidity management.

ERP targets compulsive behavior at every level — from the immediate ritual in the moment, to the child's lifelong capacity to tolerate discomfort and live flexibly. Measurable outcomes include: morning routine under 30 minutes, ability to wait 5 minutes before ritual, spontaneous use of externalization language, and reduced sibling disruption. Reference: PMC10955541 — meta-analysis confirming multi-domain improvement via ERP.

Every material below serves a precise function in the ERP treatment chain — from measuring anxiety to celebrating victory. All are available at low cost or free as DIY alternatives.
# | Material | Canon Category | Price Range | DIY? |
1 | Anxiety / SUDS Thermometers | Behavior/Feelings Thermometer | ₹150–500 | ✅ Free |
2 | Externalization Tools (OCD Monster Kit) | Emotion Cards / Social Stories | ₹100–400 | ✅ Free |
3 | Fear Ladders & Exposure Hierarchies | Visual Supports | ₹100–400 | ✅ Free |
4 | Response Delay Timers | Visual Timer | ₹300–800 | ✅ Phone timer |
5 | Thought Challenging Cards | Cognitive Tools | ₹200–600 | ✅ DIY cards |
6 | Competing Response Tools | Fidget Tool Set / Therapy Putty | ₹200–700 | ✅ Stress ball |
7 | Exposure Practice Kits | Therapy/Sensory Materials | ₹100–600 | ✅ Household items |
8 | Calming Strategy Toolkit | Calm-Down Kit | ₹300–900 | ✅ DIY kit |
9 | Victory Trackers | Reinforcement Menus | ₹150–500 | ✅ Paper chart |

A visual 0–10 scale where 0 = completely calm and 10 = worst anxiety imaginable. SUDS = Subjective Units of Distress Scale. Children point to, circle, or mark their current anxiety level — making the invisible monster visible and measurable.
- Before every exposure session
- During the wait period
- After the urge passes
- To track progress across weeks
- Home, therapy room, classroom (discreet pocket version)
Compulsions feel like emergencies. But not all anxiety is a 10. When children learn to quantify distress — "I'm at a 7, not a 10" — they begin to see that anxiety is survivable. When they track their SUDS during exposure exercises and watch it drop from 7 → 5 → 3, they gain irrefutable evidence that anxiety is temporary. "Last week, not checking the lock was a 9. This week it's a 6." Progress is visible.
- Draw or print thermometer with 0–10 scale
- Create personal anchors in the child's own words
- Practice rating during calm times (not just anxiety)
- Use during every exposure — rate before, during, after
- Graph the decrease — show child their own habituation curve
Price: ₹150–500 | DIY: ₹0 (pencil + paper) | PMC2797569 — habituation measurement in ERP studies
What It Is: Materials for separating the child's identity from the OCD — giving the compulsion a name, a face, a character that the child can talk back to and defeat. The OCD becomes "Mr. Worry," "The Checking Monster," "Brain Bully" — something external that pushes the child around but is NOT the child.
Compulsions feel like they ARE the child — "I AM a worrier, I AM broken, I CAN'T stop." Externalization fundamentally reframes this: "There's a bully in your brain giving you bad information. You are not your OCD. Let's fight it together." The shame dissolves. The fight becomes empowering.
- "Nice try, OCD, but I'm not doing your ritual today."
- "I hear you, Brain Bully. I'm not listening."
- "That's just my OCD lying to me. I know the truth."
- "Boring! I already know that trick."
- Drawing paper + markers — ₹0–200
- "Worry Monster" figurine — ₹200–500
- Externalization storybooks (Huebner's What to Do When Your Brain Gets Stuck) — ₹400–800
- "Boss Back Journal" — ₹100–300
Have child draw their OCD as a character. Name it. Write what it says. Write what the child says BACK. Role-play with a puppet.
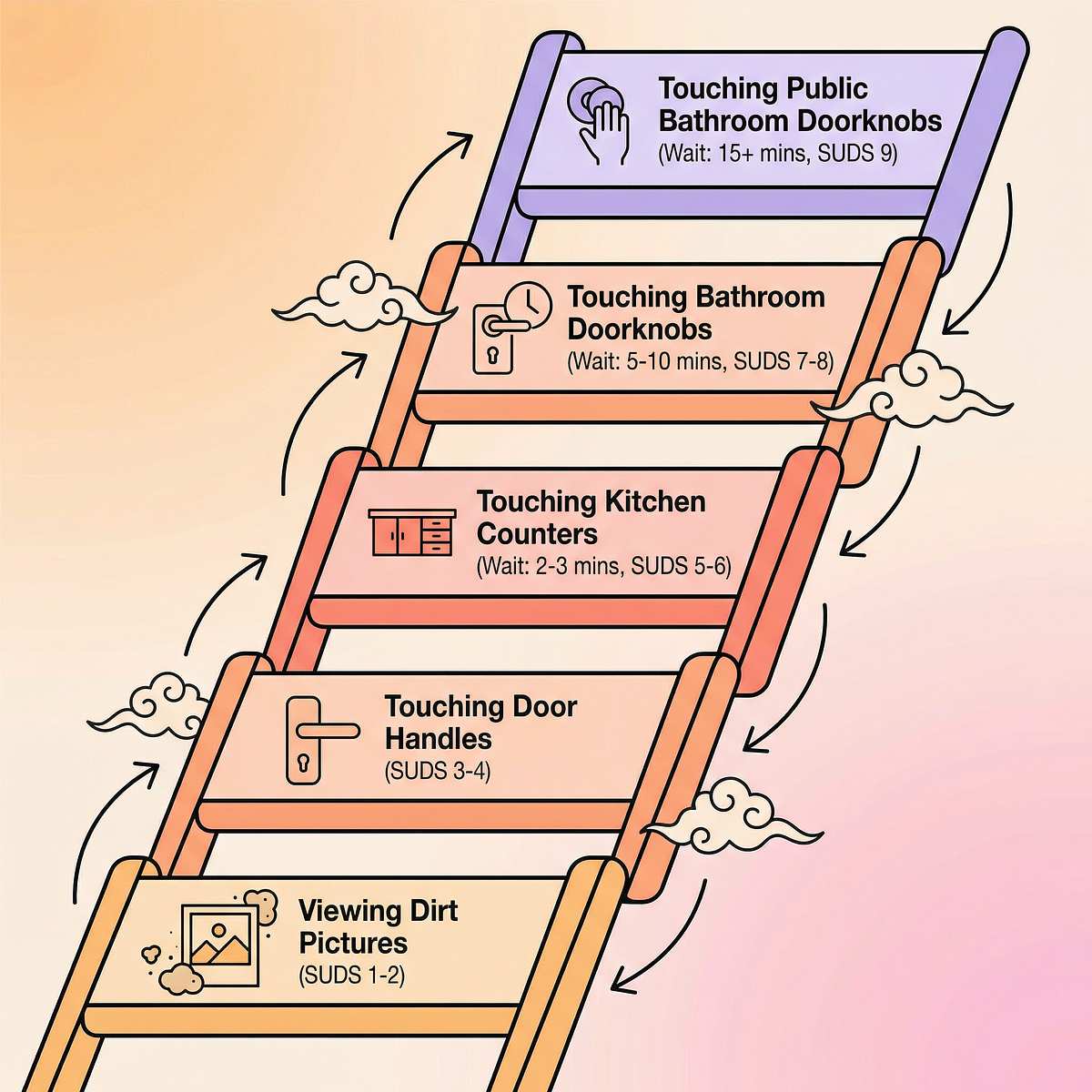
What It Is: A ranked list of feared situations arranged from least anxiety-provoking (bottom rung) to most (top rung), each with a SUDS rating. Treatment climbs the ladder one step at a time, mastering each level before moving to the next.
Jumping straight to the scariest trigger overwhelms and backfires. Fear ladders make the impossible feel possible. Each step mastered provides irrefutable evidence: "I did step 4. The anxiety peaked at 7 and dropped to 2. Nothing bad happened. Maybe I can try step 5." This is inhibitory learning — the brain builds new associations that compete with fear.
- Fear ladder template (printable) — ₹0 DIY
- Visual step chart poster — ₹100–300
- Progress tracking stickers — ₹50–200
- "Brave Ladder" goal-setting worksheets — ₹100–300

Before beginning any ERP session, run through this readiness gate. A session with poor readiness produces zero therapeutic benefit — and may set back progress. The best session is one that starts right.
- Child has eaten in the last 2 hours
- Child is not currently in meltdown
- No significant illness today
- No triggering event in last 30 minutes
- At least 20 minutes available
- Materials are ready and organized
- Parent is calm and patient
Proceed with planned session.
Use simplified version, shorter duration, lower rung on the fear ladder. Don't push for a full session — a partial win still counts.
Skip today. Do a calming activity instead. Tomorrow is also a session day. Postponing is not failure.
Children with OCD already live with anxiety all day. A session announcement that feels like a threat increases resistance. The invitation reduces anxiety and increases buy-in through agency, warmth, and connection to past victories.
- "Hey, want to do 10 minutes of bossing back [child's OCD name]? I'll be right here."
- "It's brave time. Should we pick an easy step or a medium one today?"
- "Remember how you got [OCD name] down to a 5 last week? Want to try for a 4 today?"
- Refer to the victory tracker: "Look how many wins you already have"
- Let child choose today's rung — agency increases compliance
- Remind child of the specific, immediate reward waiting
- ❌ "You have to do this" — creates power struggle
- ❌ "It's for your own good" — dismissive of real distress
- ❌ Starting during high anxiety — wait for regulated state

Why This Matters: Pre-exposure rating establishes a baseline and activates the child's "scientist brain" — they're not just suffering through anxiety, they're measuring it. This cognitive shift reduces emotional flooding. The child becomes an observer of their own anxiety, not just a victim of it. Prediction practice builds tolerance for uncertainty, a core ERP skill.
"Before we start, let's check your thermometer. What number are you at right now? What number do you think you'll reach when we start the exposure? Let's see if your prediction is right."
Materials Needed: SUDS thermometer | Fear ladder | Timer | Reference: Inhibitory learning model — PMC2797569

Leave the house after checking the lock once. Parent covers the lock with a cloth so it can't be re-checked. Stay out for 10 minutes.
Child touches "mildly contaminated" surface (per fear ladder rung). Parent is present but does NOT permit handwashing for the designated wait period.
Intentionally move one object slightly out of arrangement. Child sits with discomfort for 5 minutes without fixing it.
Parent script: "I know you're anxious. I love you. I'm not going to answer that question because answering feeds the OCD. I'm right here with you."
Duration: 10–45 minutes depending on rung difficulty. Critical: No partial rituals. No substitution rituals. No reassurance. Complete response prevention is essential. | PMC10955541 — 40-minute sessions showed maximum effectiveness

The Dosage Principle: ERP research indicates 2–3 sessions per week for 8–12 weeks as standard protocol. Within each session, the same rung may be practiced 2–4 times. Repetition is what produces habituation — each repeat shows a faster peak and faster drop in SUDS. "3 good, complete exposures beat 10 partial, rushed ones every time."
Checking the lock at home, then at grandparents' house — generalizing the learning.
Morning exposure, then evening repeat — building consistency across the day.
If today's rung feels easy, try the next rung for the last repetition — capitalizing on momentum.

The ABA Reinforcement Principle: Reinforcement must be immediate (within 3 seconds), specific (name exactly what was brave), and enthusiastic (OCD's voice is loud — your celebration must be louder). Reward the effort, not just the outcome.
"You sat with anxiety at a 7 and didn't wash your hands. That is INCREDIBLE. You just proved OCD wrong."
"Remember last week when that was an 8? Today it was a 5. You're getting stronger than OCD."
"You bossed back [OCD name] twice today. That earns [specific reward]."
- Breathing card (deep breathing visual prompt)
- Stress ball / fidget tool for hands
- Comfort item (soft toy, weighted blanket)
- Transition object — signals "therapy is done, free time now"
"I hear you. The brave part is done. Your brain worked hard today. Time to rest it."
The cool-down ritual re-establishes the child's sense of control and predictability — a critical support for children with OCD, who thrive on consistent structure. Visual timers and transition supports are classified as evidence-based practices by NCAEP 2020.

Recording just three data points after each session builds a powerful picture of your child's progress — and feeds TherapeuticAI® personalization for more precise recommendations.
Which fear ladder step was practiced?
What was the highest anxiety rating during the exposure?
What was the anxiety rating when the session ended?
Why: Anxiety too high, wrong time of day, insufficient motivation. Fix: Step down to an easier rung. Revisit the invitation approach. Confirm readiness check was complete.
Why: Response prevention wasn't enforced or rung was too difficult. Fix: Revisit response prevention strategy with therapist. Consider one rung down.
Why: Exposure too brief, or subtle avoidance (mental rituals, post-session reassurance-seeking). Fix: Review with therapist. Longer exposure or identification of hidden compulsions.
Why: Natural parental instinct when child is distressed. Fix: Prepare scripts in advance. Note it, don't repeat it. Progress isn't destroyed by one slip.
Why: Rung too difficult, child wasn't ready, or exposure too long. Fix: Step down 2 rungs next session. More calming preparation. More motivation setup.

- Play-based exposure framing
- Parent leads more actively
- Shorter sessions: 5–10 min
- Heavier emphasis on reward and externalization
- Simpler SUDS: 3-point scale (okay / worried / very worried)
- More visual supports throughout
- More gradual hierarchy steps
- Additional sensory calming supports
- More session structure and predictability
- Distinguish OCD-driven vs. autism-driven behaviors with therapist

- Start with imaginal exposures before in-vivo
- More preparation time per rung
- More calming toolkit between repetitions
- Consider intensive outpatient for severe OCD
- Psychiatric evaluation for medication if needed
Consortium Note: Adaptations are not shortcuts. They are precision — matching the intervention to the child's profile, not the other way around.
Child understands the SUDS scale and can use it. OCD has been named and externalized. Fear ladder completed with therapist. First 2–3 fear ladder rungs attempted. Child has completed at least 3 exposures with parent support. Child can say "that's my OCD" at least once.
Complete elimination of rituals (not expected until weeks 8+). Child voluntarily choosing exposures without prompting. No anxiety during exposures — anxiety is the point, it must be tolerated. Don't measure success by symptom absence at this stage.
This phase is hard. Your child is in real distress during exposures. You will want to rescue them. Know that every moment of tolerated anxiety is building new neural pathways. The distress during ERP is the medicine.
"If your child's SUDS dropped from 8 to 5 during one exposure — that's genuine neurological progress. Celebrate it." | Reference: PMC11506176 — early-phase ERP indicators

Same-rung repetitions show lower peaks (e.g., rung 3 was 7 → now peaks at 4). Habituation is happening faster within sessions.
Child occasionally uses externalization language spontaneously — without being prompted. This is a meaningful clinical milestone.
Morning routine slightly faster than week 1. Child beginning to anticipate that anxiety will pass — not just believe it intellectually.
At least one instance of child initiating response prevention without parental prompt. A landmark moment in treatment.
The synaptic changes happening right now are real and measurable. Repeated exposure without ritual is literally building new associative pathways: "That surface is just a surface, not a threat." Each completed exposure strengthens these pathways; each avoided exposure weakens them. Parent Milestone: You may notice you feel more confident too. Your tolerance for sitting with your child's anxiety — without rescuing — is itself a clinical skill you've developed. | PMC11506176 — neuroplasticity timelines

Multiple lower fear ladder rungs now feel "boring" or easy — the gold standard of ERP success at this stage.
First instances of ritual reduction without formal exposure session. Child approaching real-life triggers with learned tools — this is generalization.
School reports fewer disruptions. Child expressing pride: "I beat OCD today." SUDS baseline measurably lower than week 1.

Completed first exposure without ritual — "I did it once"
Fear ladder rung drops below SUDS 3 — "I conquered that step"
Real-life trigger handled without ritual — "OCD tried, I won"
Full morning routine completed in under 30 minutes — "My day is mine again"
"Six months ago, mornings took two hours. Last week, he got ready for school in twenty minutes. He checked the lock once, said 'nice try, OCD,' and walked to the car. He looked at me and said, 'Mom, I'm stronger than it now.' I cried all the way to school. Happy tears." — Parent, Pinnacle Network (Illustrative case; outcomes vary by child profile)
Pinnacle Data: 20M+ sessions | 97%+ measured improvement | 70+ centers. 📞9100 181 181
- Child expressing thoughts of self-harm or suicidal ideation
- Complete inability to function — can't leave home, eat, or attend school
- Rapid symptom escalation — new rituals appearing daily
- Sudden onset after infection (possible PANDAS/PANS — requires medical evaluation)
- Child in acute panic with no de-escalation possible
- Parent feeling unsafe or overwhelmed
- No SUDS decrease after 4+ consecutive sessions on same rung
- Family accommodation increasing rather than decreasing
- Child refusing all ERP engagement for 2+ weeks
- Covert mental rituals identified
- New OCD themes emerging while treating original ones
- SUDS fluctuates day to day — expected
- Some sessions better than others — normal
- Setbacks after illness or school exams — expected, not regression
- Progress slower than hoped — 8–12 weeks is standard
Each technique in the Behavioral Regulation Series builds on the skills developed in the previous one. If you have the C-295 toolkit, you already own materials for C-293, C-294, C-296, and C-297. Log your session data in GPT-OS® to have TherapeuticAI® map your child's exact next technique. WHO developmental milestones framework + domain-specific sequencing | PMC9978394

These related techniques share materials, principles, and the same therapeutic foundation as C-295. Many families work on these in parallel or sequential order.
Technique | Title | Difficulty | Primary Material |
C-293 | Anxiety & Worry Management | 🟢 Intro | Feelings thermometer |
C-294 | Rigid Routines & Change | 🟡 Core | Visual schedule |
C-296 | Rigid Thinking Patterns | 🟡 Core | Thought cards |
C-297 | Perfectionism in Children | 🟡 Core | Progress journals |
C-300 | Reassurance-Seeking | 🔴 Advanced | Scripts + boundaries |
D-361 | Stimming & Repetitive Behaviors | 🟡 Core | Sensory kit |

Emotional Regulation encompasses anxiety management, compulsive behaviors, emotional identification, frustration tolerance, sensory-emotional integration, behavioral flexibility, self-regulation, and coping strategies. C-295 addresses the Compulsive Behaviors subdomain — one of 8 areas within Domain C. See your child's full AbilityScore® profile across all 12 domains at pinnacleblooms.org/gpt-os. WHO/UNICEF Nurturing Care Framework — PMC9978394
"We didn't know what ERP was when our daughter's OCD started. We thought stricter parenting was the answer. We tried — it made everything worse. When we finally found a system that extended therapy into our home, everything changed. She's 11 now and she catches herself before rituals. She calls the OCD 'the lying brain' and she bosses it back. We're not done, but we're not prisoners anymore." — Mother, Hyderabad, Pinnacle Network
"My 9-year-old had checking compulsions so severe he couldn't leave the house. We had canceled family holidays, birthday parties, everything. The fear ladder felt impossibly hard at first. The first exposure took 40 minutes and was brutal. But it worked. Six months later he's at step 8 and counting. The victory tracker on his wall is covered in stickers. He's proud." — Father, Chennai, Pinnacle Network

Connect with families managing pediatric compulsive behaviors across India. Shared experience, practical tips, and emotional support. pinnacleblooms.org/community
Track your child's progress, receive personalized technique recommendations, connect with your therapy team — one integrated platform. pinnacleblooms.org/gpt-os
9100 181 181 | 24×7 | 16+ Languages | Not just for autism — for all pediatric behavioral health questions. Free guidance, triage, and referral.
Pinnacle centers run parent education workshops, family groups, and OCD-specific support sessions. Contact 9100 181 181 to join your city's family support group.
International Resource: International OCD Foundation (IOCDF) — iocdf.org — global resource for families navigating OCD. WHO CCD Package — multi-caregiver support as evidence-based principle | PMC9978394
- Compulsive behaviors consume >1 hour/day
- Family life revolving around accommodating rituals
- Child cannot function at school due to compulsions
- Home ERP attempts not producing progress after 3–4 weeks
- Any red flags from the escalation card
- FREE Helpline call: 9100 181 181 — first-level guidance and center referral
- AbilityScore® Assessment: Comprehensive developmental baseline
- OCD/Anxiety Specialist Assessment: Differential diagnosis, ERP-specific planning
- FusionModule™ Therapy Plan: Psychology + OT + BCBA + NeuroDev coordinated
Hyderabad • Chennai • Bangalore • Mumbai • Delhi + 65 more cities
pinnacleblooms.org/find-center
Can't reach a center? Book online teleconsultation.
care@pinnacleblooms.org | pinnacleblooms.org/teleconsult
Psychology (OCD/ERP) | Psychiatry (if medication indicated) | OT (sensory + motor) | BCBA (reinforcement + data) | Parent Coaching (accommodation reduction)
PMC2797569 — Exposure and Response Prevention for Pediatric OCD: comprehensive systematic review confirming ERP as gold-standard treatment with large effect sizes. Read on PubMed →
POTS Study (2004) — Pediatric OCD Treatment Study: multi-site RCT confirming ERP superiority over medication alone. Access DOI →
PMC10955541 — Meta-analysis (World J Clin Cases, 2024): 24 studies confirming multi-domain improvement via behavioral intervention. Read on PubMed →
WHO Mental Health Action Plan 2013–2030 | WHO NCF 2018 | WHO/UNICEF CCD Package — PMC9978394 | NCAEP 2020 Evidence-Based Practices Report | DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al., Indian Journal of Pediatrics (2019)

GPT-OS® learns from every C-295 session: rate of habituation, optimal session length, which compulsion types respond fastest, when to step up vs. step down the hierarchy, and family accommodation patterns. All data is encrypted and DPDP Act 2023 compliant. "Your data helps every child like yours."
"Your grandchild has OCD — a brain condition where anxiety feels like a real emergency. The family is working with therapists on a treatment called ERP. The most important thing you can do: don't answer reassurance questions repeatedly — it actually makes things worse. Instead say: 'I know you're worried. I love you. The worry will pass.' That's your job. You can do it."
OCD heals in proportion to the consistency of the environment around it. One family member accommodating rituals that others are carefully not accommodating undermines treatment. This page is the shared family reference.
- 📲WhatsApp: Share C-295 page with family members
- 📧Email: Send to spouse, grandparents, teachers, school counselor
- 🔗Copy Link: techniques.pinnacleblooms.org/emotional-regulation/compulsive-behaviors-c295
- 📄Family Guide (1-page PDF): "What Our Child Is Working On and How to Help"
- 📄Teacher Communication Template: Supporting a student managing compulsive behaviors
- 📄Accommodation Reduction Guide: "How to Stop Feeding OCD (Gradually)"

Key difference: OCD rituals feel ego-dystonic (the child doesn't want to do them, feels compelled by anxiety). Autism repetitive behaviors are typically ego-syntonic (comforting, wanted, enjoyable). Some children have both. Diagnosis requires specialist assessment. Contact 9100 181 181 for evaluation guidance.
Exposure practice at home with parent support is part of treatment — but the fear hierarchy MUST be designed by a trained ERP therapist. Poorly designed exposures can worsen symptoms. Professional oversight is not optional for OCD treatment.
When properly implemented — graduated, paced to the child, with full response prevention, within a supportive therapeutic relationship — ERP does not traumatize. It liberates. Flooding is NOT ERP. Graduated ERP is the standard and has a strong safety record.
They do help — briefly. That brief relief is exactly why compulsions persist. Each ritual teaches the brain "the anxiety was dangerous and the ritual saved me." Over time, rituals must grow more elaborate. ERP breaks this cycle by showing the brain: "I tolerated the anxiety. The ritual was never necessary."
Typically 8–12 weeks for significant improvement. Predictors of faster progress: early intervention, higher motivation, strong family support, consistent practice, and professional guidance. Some children show meaningful change earlier; complex cases may take longer.
Didn't find your answer? Ask GPT-OS® at pinnacleblooms.org/ask | Book a teleconsultation at care@pinnacleblooms.org | 📞9100 181 181 — 24×7 FREE

The rituals are not going to stop themselves. ERP works. These materials make it actionable. Start today.
Occupational Therapy
ERP Clinical Lead
Behavioral Analysis
Special Education
Pediatric Neurodevelopment
Preview of 9 materials that help with compulsive behaviors Therapy Material
Below is a visual preview of 9 materials that help with compulsive behaviors therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





















"From the ritual that holds all the power — to the child who holds their own power back. From fear to mastery. One technique at a time."
Built by Mothers. Engineered as a System.
OT | Psychology | BCBA/ABA | SpEd | NeuroDevelopmental Pediatrics
21M+ Therapy Services | 97%+ Outcomes
70+ Centers | 70+ Countries Served
📞9100 181 181 — FREE | 16+ Languages | 24×7
🌐 pinnacleblooms.org
✉ care@pinnacleblooms.org
This content is educational. It does not replace individualized assessment and treatment with qualified mental health professionals specializing in OCD and anxiety disorders. Outcomes vary by individual. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are trademarks of Pinnacle Blooms Network®. Patents filed in 160+ countries.
These materials support the path to freedom. Technique C-295 — Compulsive Behaviors | Pinnacle Blooms Network®