
When Every Dog Becomes a Threat
Your child isn't just cautious — they're terrified. The fear makes them freeze, scream, or bolt. Logic doesn't help. Avoidance makes it worse. Forced exposure backfires. There is a better way.
Ages 3–12
Evidence-Based
Domain C — Emotional Regulation

"She saw a small, leashed puppy across the street — a golden retriever puppy, wagging its tail — and she had a full panic attack. Hyperventilating. Crying. Shaking. She's seven. Her world is shrinking every day. And I don't know what to do." — Parent navigating animal phobia, Pinnacle Network
You are not failing. Your child's fear system is doing exactly what fear systems do — they just need a different path through. This page will show you that path, step by step.
🏥 Pinnacle Blooms Consortium®
Clinical-grade, multi-disciplinary framework
📋 Domain C — Emotional Regulation
Technique C-283 — Animal Fears
👶 Ages 3–12 Years
Adapted for all developmental profiles
🔬 Evidence-Based Protocol
Level I systematic review + RCT evidence

Millions of Families Are Navigating This Exact Challenge
Animal phobias are among the most common — and most treatable — challenges in child psychology. Your child is not alone. And neither are you.
1 in 10
Children affected
Develop a clinically significant specific phobia at some point in childhood
Ages 5–9
Peak emergence window
When fear most commonly becomes phobic rather than simply developmental
80%
Begin before age 10
Of specific phobias start early — and often persist untreated into adulthood
🇮🇳Indian Context: With 280 million+ children under 14 in India, animal phobias represent one of the most prevalent yet undertreated childhood anxiety conditions. Street dogs, birds, and insects are omnipresent — making avoidance strategies impossible to sustain across urban and semi-urban environments.
Sources: PMC3018970 (CBT + Exposure Meta-analysis) | AACAP Practice Parameters | WHO Child Development Data
This Is a Wiring Difference, Not a Behaviour Choice
Understanding what's happening in your child's brain is the first step to helping them heal.
The Amygdala Alarm System
When your child sees a dog, their amygdala (the brain's threat-detection centre) fires an immediate alarm signal — before the thinking brain (prefrontal cortex) even has a chance to evaluate the situation. The body enters fight-or-flight: heart racing, breathing shallow, muscles tensed for escape. In a child with phobia, this fires with the same intensity for a leashed puppy as it would for a genuine predator.
What This Means for You
Your child is not being dramatic
They cannot "just calm down" on command
Reasoning doesn't work — the thinking brain goes offline during the alarm
Forcing exposure makes the alarm louder, not quieter
The path through is gradual, child-controlled exposure — rewiring the alarm safely
"Fear generalization occurs when the amygdala extends its threat response from specific to broader stimulus categories. This is neurologically predictable — and neurologically reversible with the right intervention." — Pinnacle Consortium Neurodevelopmental Team
Research: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660
Where This Sits in Your Child's Development
Not all animal fear is the same. Understanding where your child sits on the developmental timeline helps calibrate when to watch, when to act, and when to celebrate progress.
Age 2–4
🟢 NORMAL wariness — resolves naturally in most children
Age 4–6
🟢 NORMAL — watch if fear isn't reducing with positive experiences
Age 5–9
⚠️ PEAK PHOBIA WINDOW — intervention most effective here
Age 8–12
✅ INTERVENTION WINDOW — excellent outcomes with structured approach
12+
✅ FREEDOM possible at any age with right therapeutic support
⚠️Children at higher risk for persistent animal phobias: Anxious temperament | Sensory sensitivities | Autism spectrum traits | Prior negative experiences with animals | Behavioral inhibition. Children with these profiles benefit most from structured, GPT-OS® guided intervention.
WHO Care for Child Development (CCD) Package — implemented across 54 low- and middle-income countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)

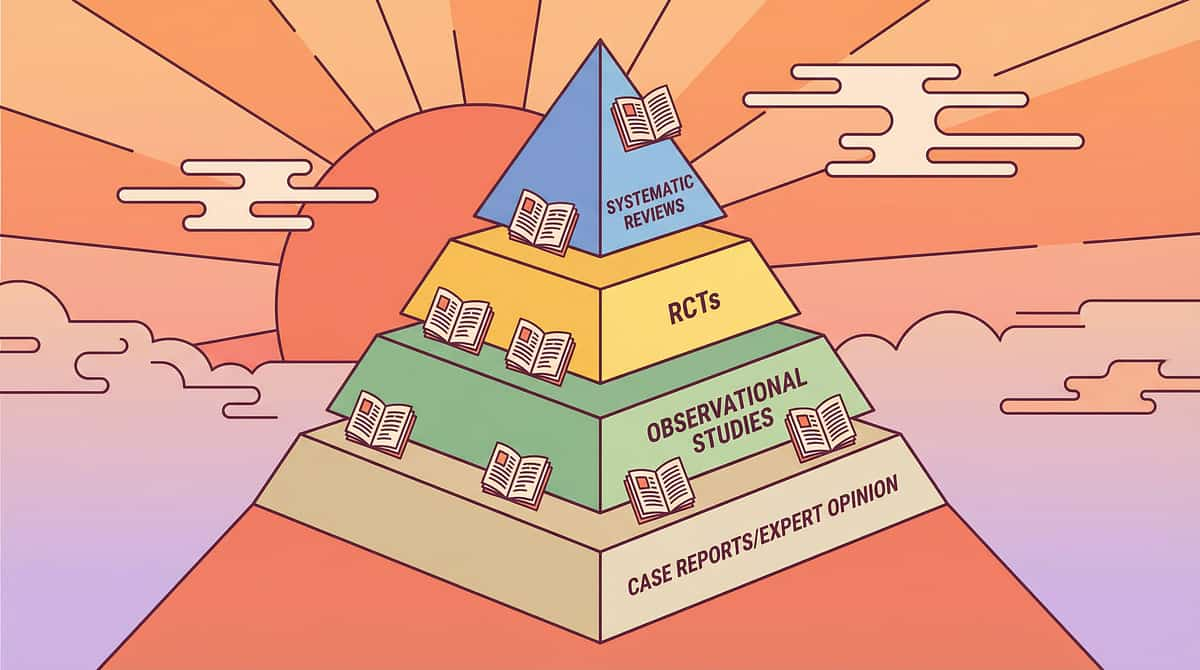
The Evidence Behind This Technique
Clinically validated. Home-applicable. Parent-proven. This is not guesswork — it is the highest tier of clinical evidence applied to your living room.
🛡 LEVEL I — Systematic Review + RCT Evidence
Study | Finding | Source | |
CBT + Graduated Exposure Meta-Analysis | Gold-standard treatment for specific phobias in children. Systematic desensitization significantly reduces fear and avoidance. | PMC3018970 | |
AACAP Practice Parameters | Exposure-based CBT is the recommended first-line treatment for childhood specific phobias including animal type. | AACAP 2007/2020 | |
ADAA Exposure Guidelines | Graduated, child-paced approaches produce durable fear reduction with low relapse rates. | ADAA Clinical Guidelines | |
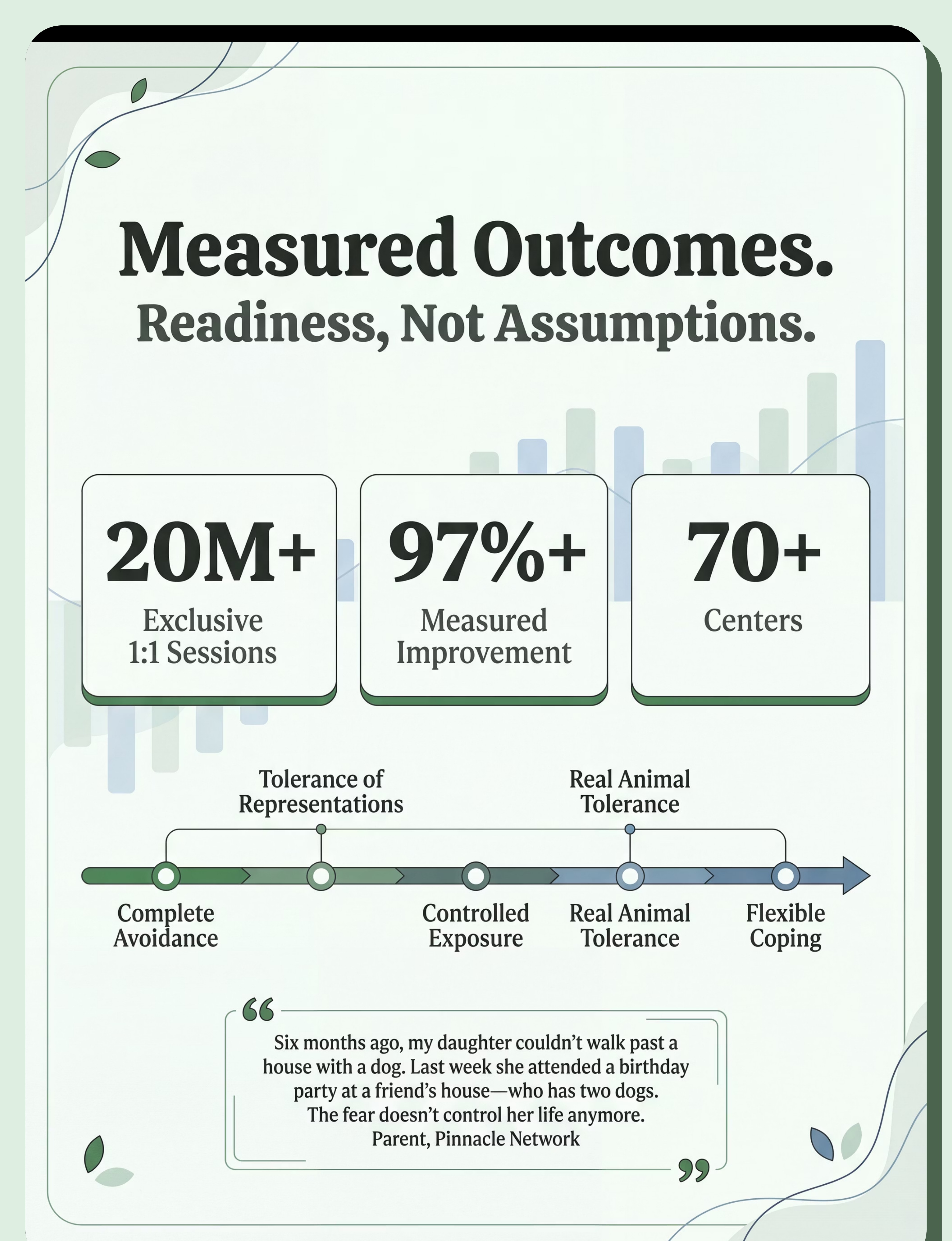
Pinnacle GPT-OS® Network Data | 97%+ measured improvement across Anxiety Readiness Index and Community Participation Readiness Index across 20M+ sessions. | Pinnacle Network RWE | |
Indian J Pediatr RCT (Padmanabha, 2019) | Home-based structured interventions demonstrate significant outcomes in Indian pediatric populations. | DOI: 10.1007/s12098-018-2747-4 |
"The brain needs experiential evidence, not just verbal reassurance. Graduated exposure provides the corrective experience that rewires threat responses — something no amount of reasoning can achieve." — Pinnacle Consortium Clinical Psychology + ABA Team

The Technique: What It Is
Technique C-283
The Fear Ladder Approach
Graduated Exposure Therapy for Animal Fears
A structured, child-paced system of gradually increasing exposure to feared animals — moving from the least scary representations (cartoon images) through progressively more realistic contact (stuffed animals, videos, real animals at distance) until the child can tolerate normal animal encounters with manageable anxiety and effective coping.
What it does: Rewires the brain's threat-assessment system. Each successful encounter teaches the amygdala: "This is not actually dangerous. I survived. I can handle more."
Who It's For
Children ages 3–12 with specific phobia (animal type) — including cynophobia (dogs), fear of birds, cats, insects, or generalised animal anxiety. Particularly valuable for children with autism spectrum traits, sensory sensitivities, and high anxiety temperament.
📁 Domain
Emotional Regulation / Anxiety
👶 Ages
3–12 Years
⏱ Duration
10–20 min/session, 3–5x/week
📅 Programme
8–12 weeks for measurable outcomes
Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organise by therapy type. C-283 is a multi-disciplinary protocol, and each profession brings something irreplaceable.
Clinical Psychology / Psychologist
Primary discipline. Designs the full exposure hierarchy, manages cognitive restructuring, oversees parent coaching. Leads severe phobia cases requiring professional CBT.
Occupational Therapist (OT)
Addresses sensory components. For children with sensory sensitivities, the textures, sounds, and unpredictable movements of animals are additional triggers. OT desensitises these alongside fear.
BCBA / ABA Therapist
Structures the reinforcement system (Brave Points), designs antecedent management, and ensures consistent protocol fidelity. The operant framework makes courage visible and measurable.
Special Educator
Generalises progress to school settings. Creates accommodation plans, communicates with teachers, ensures school environments don't inadvertently trigger or maintain the phobia.
Neurodevelopmental Paediatrician
Rules out medical contributors, guides families on medication options if anxiety is severe, and coordinates with mental health team for co-occurring conditions.
GPT-OS® FusionModule™ coordinates all discipline inputs into a single converged therapeutic pathway — so Psychology, OT, ABA, and Special Education are working in alignment, not in parallel silos.

What This Targets
This isn't a random activity. It's a precision intervention with layered goals — from eliminating panic to building lifelong resilience.
✅ Child can look at pictures of feared animals
✅ Can tolerate stuffed version
✅ Watches calm animal videos
✅ Observes real animal at distance
✅ Attends events where animals are present
✅ Flexible coping with unexpected encounters
Research: Meta-analysis (World J Clin Cases, 2024): Exposure-based CBT promotes adaptive behaviour (primary), social participation (secondary), and community functioning (tertiary). PMC10955541

Nine Materials. One Mission: Freedom From Fear.
Clinically sequenced. Home-executable. INR-priced. Zero-cost DIY alternatives for every item.
🪜 Material 01
Fear Ladder / Exposure Hierarchy Visual — Makes the impossible look achievable, step by step
Canon: Calm-Down Kit / Visual Supports | ₹100–400
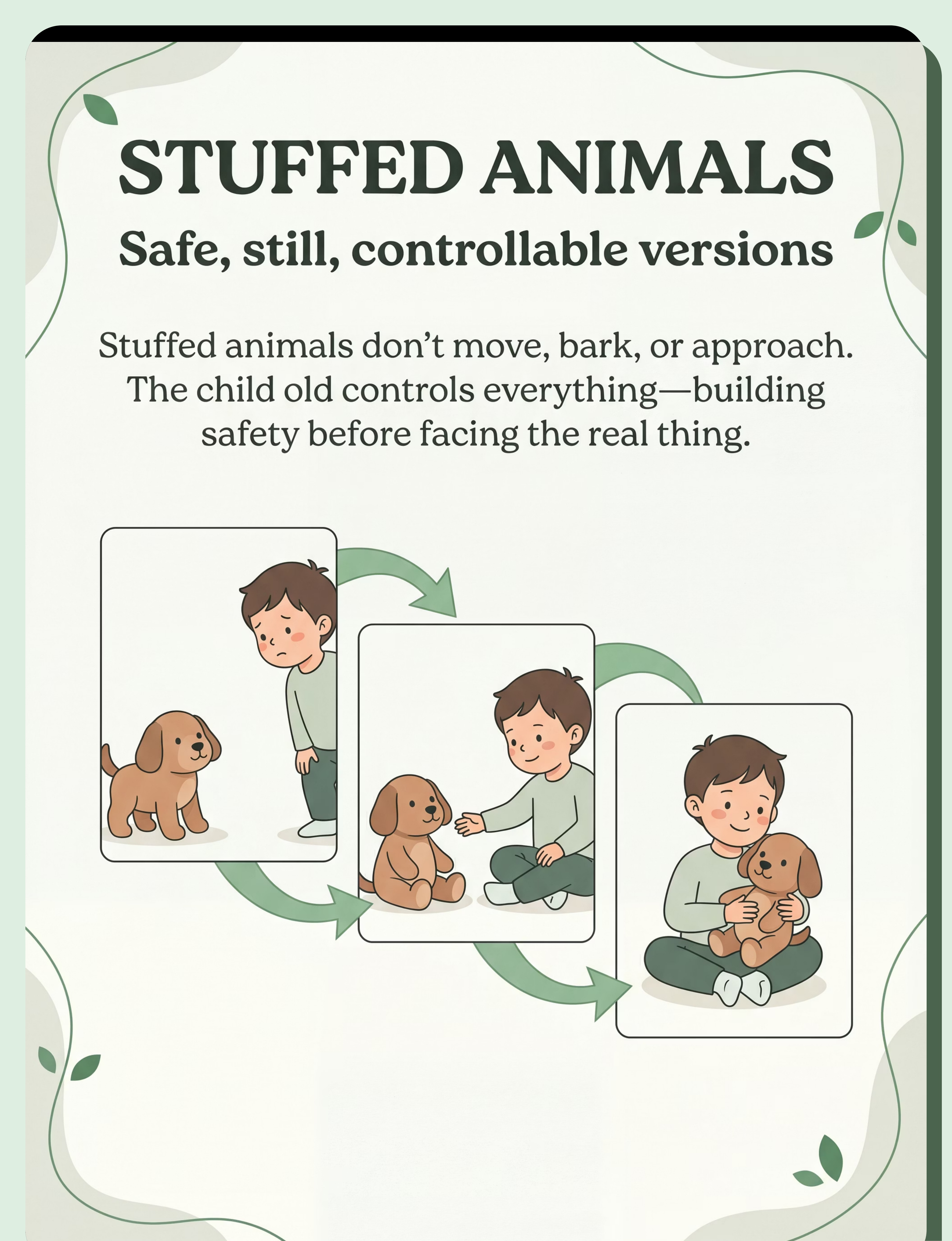
🧸 Material 02
Stuffed Animals (Plush of Feared Species) — Safe, still, completely controllable version of the feared animal
Canon: Transition Objects | ₹200–1,500
📚 Material 03
Books About Animals and Overcoming Fear — Knowledge defeats fear; stories build hope and model courage
Canon: Social Stories / Narrative Supports | ₹150–600
📱 Material 04
Video Content with Gradual Animal Exposure — Real animal movement, complete parental control — pause and stop always available
Canon: Parent Education Resources | ₹0 (free streaming)
🌬 Material 05
Relaxation and Coping Strategy Tools — Calm the body, calm the fear: breathing, squeeze tools, calm-down cards
Canon: Breathing / Relaxation Tools | ₹100–600
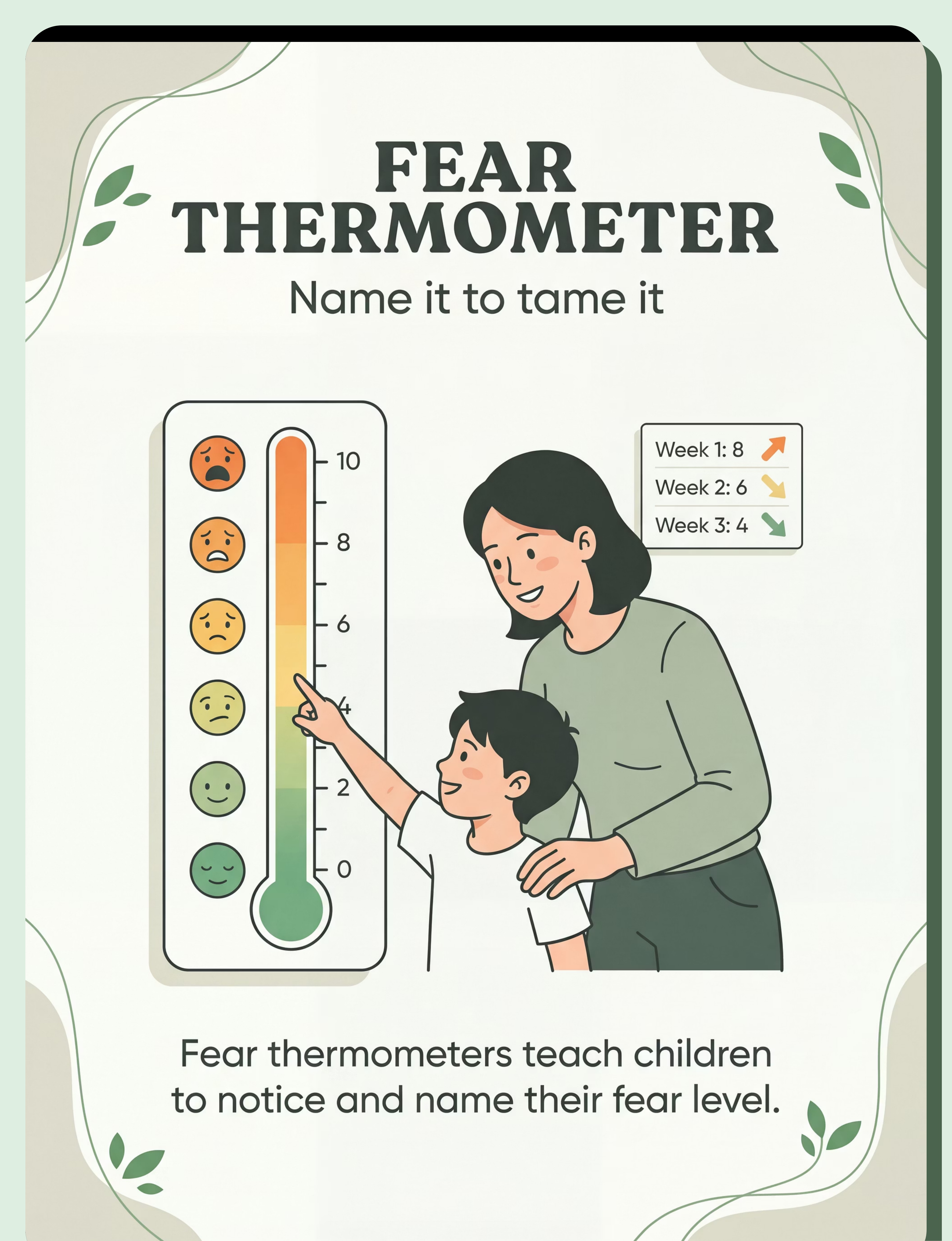
🌡 Material 06
Brave Thermometer / Fear Rating Scale — Name it to tame it: turns invisible fear into trackable numbers
Canon: Behavior / Feelings Thermometer | ₹50–250
⭐ Material 07
Reward Charts and Brave Points Systems — Courage deserves recognition; rewards effort, not the absence of fear
Canon: Reinforcement Menus | ₹100–400
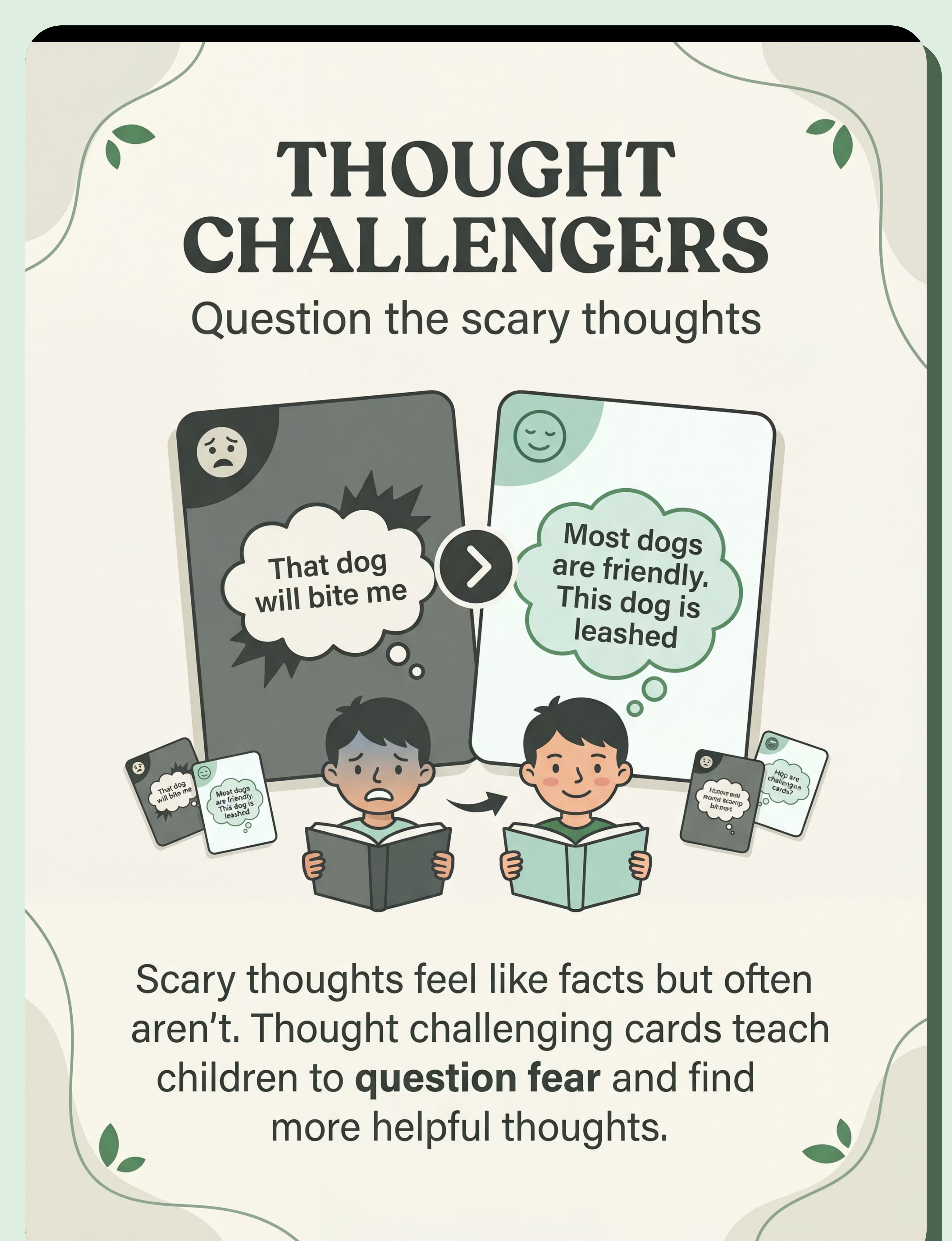
🃏 Material 08
Thought Challenging Cards / Worry Busters — Question the scary thoughts: cognitive restructuring made child-friendly
Canon: Emotion Cards / Feelings Faces | ₹100–400
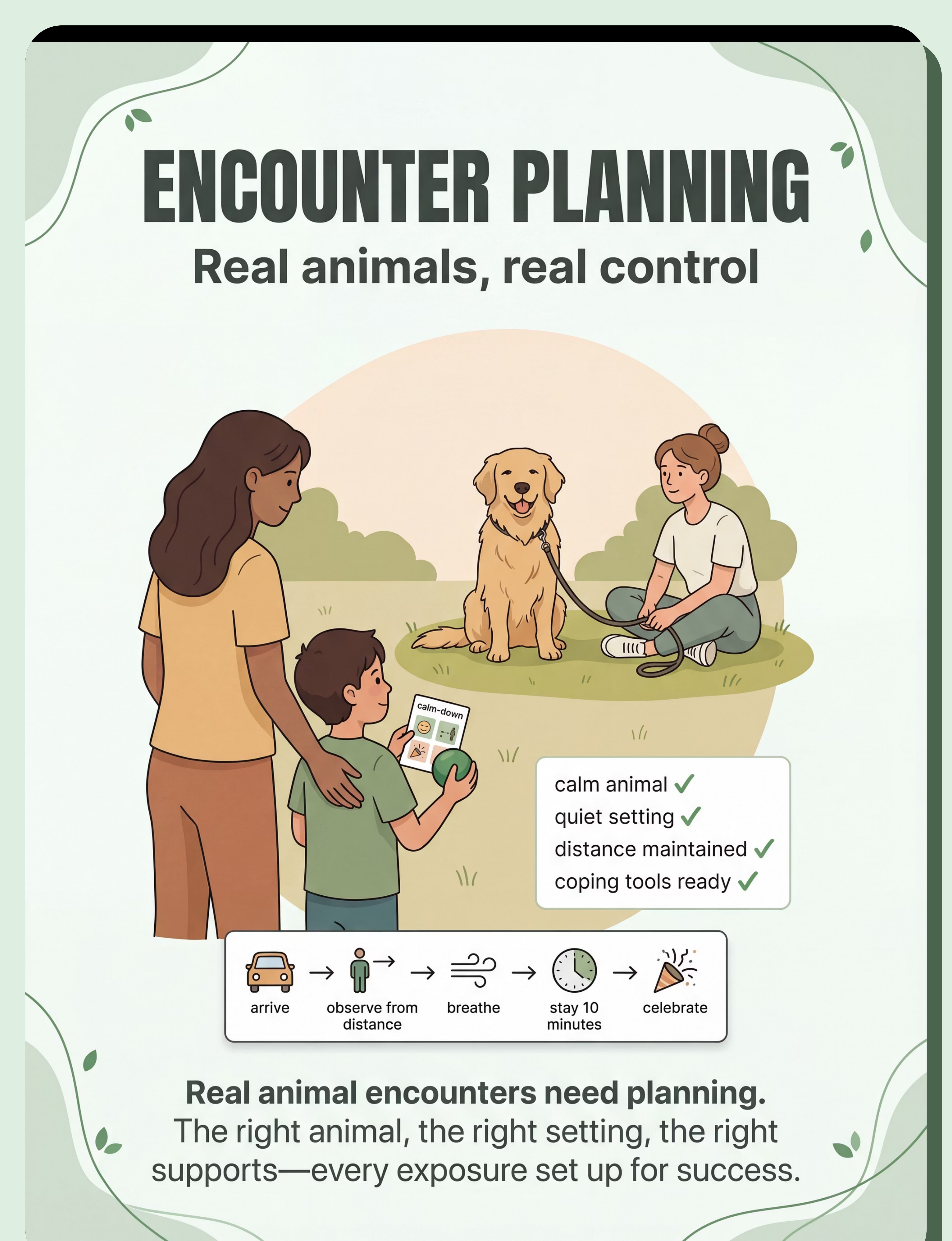
📋 Material 09
Safe Animal Encounter Planning Kit — Real animals, real control: every real encounter planned for success
Canon: Visual Schedule System | ₹50–200
All prices INR. Products linked to materials.pinnacleblooms.org Canon database. DIY alternatives available for every material — see next card.
Every Family Can Start Today — Regardless of Budget
The therapeutic mechanism is not in the product — it's in the structured, predictable exposure process. A hand-drawn fear ladder is therapeutically equivalent to a printed one. Here is how to make every material yourself at zero cost.
Material | Zero-Cost DIY Version | |
Fear Ladder | Poster board + markers + stickers. Draw 10 steps, involve child in writing each one. Laminate for durability. Post on bedroom wall. | |
Stuffed Animal | Use any stuffed animal the child already owns. Or borrow one. Start with the least realistic. | |
Animal Books | Library — free. Print and bind a simple homemade book with Google Images progressing from cartoon → realistic animals. | |
Videos | YouTube is free. Curate a playlist: cartoon animals → calm real animals → children with animals. Save to "Watch Later" list. | |
Relaxation Tools | Teach belly breathing using a stuffed animal on tummy (watch it rise and fall). Use a small squeeze ball from the kitchen. | |
Fear Thermometer | Draw a thermometer on paper, add 0–10 scale with emoji faces. Laminate. | |
Brave Points Chart | Paper + pen + any stickers. Define what earns points. Set milestone rewards from things you already have. | |
Thought Cards | Index cards: scary thought on one side, brave thought on the other. Child helps create them. | |
Encounter Planning | Create a simple checklist: Is the animal calm? Is it controlled? Do I have my tools? Have I practiced my breathing? |
Why DIY works: The parent's consistent, calm, child-paced presence is the most powerful tool in this entire kit. A hand-drawn fear ladder is therapeutically equivalent to a printed one. WHO Nurturing Care Framework (2018): Context-specific, equity-focused interventions. PMC9978394
Safety First: Read This Before Every Session
Before you open a single material, run through this safety gate. Starting a session in the wrong conditions can set back progress significantly. This takes 60 seconds and protects months of work.
🔴 DO NOT PROCEED if:
• Child had a frightening animal encounter within 24 hours
• Child is in active meltdown, panic, or severe dysregulation
• Child is unwell, feverish, overtired, or hungry
• You are planning to force any level of exposure the child has refused
• You are using flooding (direct, unprepared real-animal contact)
• The animal to be encountered is unfamiliar or uncontrolled
• Child is in active meltdown, panic, or severe dysregulation
• Child is unwell, feverish, overtired, or hungry
• You are planning to force any level of exposure the child has refused
• You are using flooding (direct, unprepared real-animal contact)
• The animal to be encountered is unfamiliar or uncontrolled
🟡 MODIFY the session if:
• Child is mildly dysregulated but able to engage with support
• Child wants to skip steps in the hierarchy
• Session environment has unexpected distractions or noise
• Child is not in their usual regulated window but not in crisis
• Child wants to skip steps in the hierarchy
• Session environment has unexpected distractions or noise
• Child is not in their usual regulated window but not in crisis
🟢 PROCEED when:
• Child is calm, fed, rested, and in a regulated state
• Environment is set up as planned
• Parent is calm and not anxious about the session
• Materials are prepared and available
• Child knows what will happen — no surprises
• Environment is set up as planned
• Parent is calm and not anxious about the session
• Materials are prepared and available
• Child knows what will happen — no surprises
⛔ABSOLUTE SAFETY RULE: Never rush a fear ladder step. Never skip steps. Never force. The child sets the pace — always. A session that ends early because the child wasn't ready is a successful session, not a failure.
If the child has experienced a genuine traumatic animal encounter (severe bite, attack), home practice should be supervised by a licensed clinical psychologist. FREE helpline: 📞9100 181 181
If the child has experienced a genuine traumatic animal encounter (severe bite, attack), home practice should be supervised by a licensed clinical psychologist. FREE helpline: 📞9100 181 181

Set Up Your Space
Spatial precision prevents 80% of session failures. A prepared environment signals safety to a child's nervous system before the session even begins. Spend five minutes setting this up correctly every time.
Location & Comfort
✅ Quiet room, no unexpected noise (TV off, fans low)
✅ Child seated comfortably — cushion on floor, low chair, or sofa
✅ Warm, moderate lighting — not harsh overhead fluorescent
✅ Comfortable temperature
✅ Child seated comfortably — cushion on floor, low chair, or sofa
✅ Warm, moderate lighting — not harsh overhead fluorescent
✅ Comfortable temperature
Materials & Visibility
✅ All materials prepared before child enters the space
✅ Fear Ladder visible on wall or tabletop
✅ Brave Points Chart visible and ready
✅ Fear Thermometer within child's reach
✅ Coping tools (breathing or squeeze item) within child's reach
✅ Fear Ladder visible on wall or tabletop
✅ Brave Points Chart visible and ready
✅ Fear Thermometer within child's reach
✅ Coping tools (breathing or squeeze item) within child's reach
Safety & Clarity
✅ Exit path clear — child knows they can signal to stop at any time
✅ No surprises — child knows exactly what material is planned today
✅ Parent position: side-by-side (not behind — this signals surveillance, not support)
✅ No surprises — child knows exactly what material is planned today
✅ Parent position: side-by-side (not behind — this signals surveillance, not support)
🏠Indian Home Adaptation: In joint-family settings, ensure other family members are briefed not to interrupt or comment during the session. Assign a specific corner of any room — the space doesn't need to be dedicated. Consistency of the space matters more than perfection.

Is Your Child Ready? The 60-Second Readiness Check
The best session is one that starts right. Run this quick assessment before every session. Two minutes of readiness checking saves two weeks of regression.
Check | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Is child fed? | Full meal 1–2 hrs ago | Slightly hungry — offer snack first | Hasn't eaten, very hungry | |
Is child rested? | Normal sleep last night | Slightly tired but manageable | Overtired or sleep-deprived | |
Regulatory state? | Calm, engaged, responsive | Mildly elevated but coachable | Active meltdown or crisis | |
Animal exposure today? | No encounters today | Brief distant sighting, recovered | Direct frightening encounter today | |
Child's stated readiness? | "Yes" or neutral | "Maybe" | Clear refusal |
3+ GREEN = GO
Proceed to Step 1: The Invitation
Any AMBER = MODIFY
Use easier fear ladder step or briefer session
Any RED = POSTPONE
Use calming activity; reschedule session
Postpone Activity Option: If postponing, spend 5 minutes doing a favourite calm activity with the child — this preserves the parent-child connection and keeps therapy feeling positive rather than punitive.

STEP 1 of 5
The Invitation
Duration: 30–60 seconds
"Hey, I have something fun for us to do together. You don't have to do anything you don't want to — you're completely in charge. Want to check out what we have today?"
Body Language Guide
- 😊 Relaxed face — not tense, not falsely cheerful
- 👐 Open posture — no arms crossed
- 👁️ Eye contact at child's level — sit or crouch down
- 📐 Side by side — not face to face (which can feel confrontational)
Reading Your Child's Response
Acceptance Cues (GO): Moves toward materials | Makes eye contact | Nods or says yes | Asks a question about the activity
Resistance Cues (MODIFY): Backs away | Says "I don't want to" | Goes quiet and tenses up | Diverts attention elsewhere
If Resistance: "Okay, what if we just look at the picture from over here? We don't have to go closer." Always give the child a modified version that still counts as brave.

STEP 2 of 5
The Engagement
Duration: 1–3 minutes — Introduce today's Fear Ladder step
Early Stage — Looking at Pictures
"Look at this picture of a dog. He looks pretty sleepy, doesn't he? What do you notice about him?"
Narrate calmly. Point out non-threatening features. "Look how small his ears are."
Narrate calmly. Point out non-threatening features. "Look how small his ears are."
Middle Stage — Stuffed Animal
"This is Buddy. He's a stuffed dog. He can't move, can't bark, can't come near you unless you want him to. Should we just look at him first?"
Place stuffed animal 3 metres away. Let child observe. No pressure to touch.
Place stuffed animal 3 metres away. Let child observe. No pressure to touch.
Video Stage
"I found a video of a really sleepy golden retriever. Want to watch it with me? You hold the tablet — you can pause it any time."
Hand control to child. Watch together. Narrate calmly.
Hand control to child. Watch together. Narrate calmly.
✅ Engaged
Leaning in, asking questions, pointing
⚠️ Tolerating
Still, neutral, not approaching but not fleeing
🛑 Avoidance
Turning away, requesting to leave, escalating anxiety — check fear thermometer
Reinforcement Cue: At the first sign of engagement or tolerance — immediate verbal praise: "That was really brave. You looked right at it."
STEP 3 of 5
The Therapeutic Action
Duration: 3–10 minutes — The core of the session
Remain at the current fear ladder step long enough for anxiety to begin to decrease naturally. This is called habituation — the brain learns through experience that the feared stimulus is not actually dangerous. Stay until the child's self-reported fear rating drops at least 2 points, or until 5–10 minutes have elapsed with stable or decreasing anxiety.
Fear Thermometer Check every 2–3 minutes: "Quick check — what number are you at right now on the fear thermometer?" Record the number. A decreasing number = neurological progress happening.
Fear Rating | Meaning | Action | |
8–10 | Overwhelming — too much | Step back to easier step, use coping tools | |
5–7 | Target zone — hard but manageable | Hold here, support, don't advance or retreat | |
2–4 | Mild anxiety — good progress | Stay a bit longer, then advance next session | |
0–1 | Mastered this step | Advance to next step in the next session |
The Golden Rule: Stay in the target zone (5–7). Don't advance when it's too scary. Don't retreat when it's just uncomfortable. The discomfort IS the therapy.

STEP 4 of 5
Repeat & Vary
Duration: 2–5 minutes | Dosage principle: 3 good repetitions beat 10 forced ones.
Repetition Guidance
- Within session: Aim for 3–5 successful contacts with the current fear ladder step
- Across sessions: Return to the same step until fear rating consistently reaches 2–3 before advancing
- Across weeks: Aim for 3–5 sessions per week. Fear that is faced regularly shrinks. Fear that is avoided weekly grows.
Variation Options
Different angle: View the feared stimulus from a slightly different position
Different distance: Inch 30cm closer than last time
Different context: Same material but during a favourite activity
Dual task: Use coping strategy simultaneously (breathing while viewing)
Satiation Indicators (time to wrap up the step): Child begins fidgeting or requesting to do something else | Focus decreasing, engagement dropping | Fear rating has been at 1–2 for multiple checks

STEP 5 of 5
Reinforce & Celebrate
Duration: 1–2 minutes — Award Brave Points immediately at the moment the session ends or when a specific brave moment occurs.
What Earns Brave Points
- Attempted any fear ladder step (even if scary)
- Used a coping strategy (breathing, squeeze toy, thought card)
- Stayed at a scary step for the agreed time
- Completed the whole session
- Used the fear thermometer and communicated their level
- Said "I'm scared but I'll try"
Praise Scripts — Use These Exact Words
"You were scared, and you did it anyway. That is what brave looks like."
"I saw your fear thermometer go from an 8 to a 5. Your brain is learning that dogs aren't as dangerous as it thought. That's real progress."
What NOT to Say
- ❌ "See? That wasn't scary at all!" — Dismisses their real experience
- ❌ "You're fine!" — Tells them not to trust their feelings
- ❌ "Good job not being scared!" — Fear is not something to be ashamed of

Cool-Down & Data Capture
The session ends. The learning consolidates. After each exposure session, the child needs a transition activity to signal the work is done and the nervous system can fully relax. Data capture takes two minutes and is the foundation of measurable progress.
Cool-Down Ritual (3–5 minutes)
🎨 5 minutes of favourite drawing or colouring
📖 1 chapter of a non-animal-related favourite book
🧩 Brief puzzle or building activity
🥤 Snack + chat: "Tell me one thing you noticed today"
🎮 Short favourite game
Session Log — C-283 Data Capture
Date: ___________
Fear Ladder Step Attempted: ___________
Starting Fear Rating: ___ / 10
Ending Fear Rating: ___ / 10
Duration at Step: ___ minutes
Brave Points Earned: ___
Parent Observations: ___________
Notes for Next Session: ___________
Fear Ladder Step Attempted: ___________
Starting Fear Rating: ___ / 10
Ending Fear Rating: ___ / 10
Duration at Step: ___ minutes
Brave Points Earned: ___
Parent Observations: ___________
Notes for Next Session: ___________
📊GPT-OS® Integration: Connect your session data to GPT-OS® via your centre's EverydayTherapyProgramme™ portal. Your TherapeuticAI® engine uses real session data to adjust the fear hierarchy, recommend next steps, and track progress against the Anxiety Readiness Index.

Troubleshoot: When Things Go Wrong
Every family hits these walls. Here's how to break through. Setbacks are not failures — they are data points that guide the next step.
🔴 "My child refuses to start any session"
Drop to a lower fear ladder step. Or try a non-session approach: watch an animal cartoon together without labelling it as therapy. Build positive association first.
🔴 "My child was doing well but suddenly regressed"
Regression after illness, stress, or a scary encounter is normal and temporary. Return to 2–3 steps below current mastery level. Rebuild from solid ground. Setbacks don't erase progress.
🔴 "I panic when animals are near — am I making it worse?"
Possibly. Model active coping out loud: "I feel a bit nervous too, but I'm going to take a deep breath and notice that this dog is calm and leashed."
🔴 "My child's fear is spreading to more animals now"
Fear generalisation is neurologically predictable. Expand the fear hierarchy to address the new fears. Consider whether professional CBT support is needed for the scope of the phobia.
🔴 "We had a bad real encounter and now we're back to zero"
You're not at zero — you're at a setback. The neural pathways you've built don't erase. Return to representations (pictures, stuffed animals). Rebuilding will happen faster than the first time.
🔴 "My child says they're ready to pet a real dog but I'm not sure"
Use the encounter planning kit (Material 09) to set up the most controlled possible encounter. Use a calm, trained, handler-controlled dog. Let the child approach voluntarily, at their pace. Never rush.
📞 If home practice has not produced measurable improvement in 6 weeks, or if fear is causing significant school/social impairment, call 9100 181 181 for a guided GPT-OS® assessment.
Adapt the Technique: One Fear, Many Paths
Find the version that fits your child. The same destination — freedom from fear — is reachable by many routes. Let your child's profile guide the path.
1
← EASIER
For bad days, regression, sensory-sensitive children: cartoon/drawing only, stuffed animal in box, muted video, full calming tools throughout every session
2
STANDARD
Photos → stuffed animal at distance → full video → real animal at distance → guided encounter with known calm animal
3
→ HARDER
For good days, approaching mastery: real animal sounds in video, closer stuffed animal play, pet store visit, friend's calm leashed dog visible at distance
🧩 Autistic Children
Extra visual supports. More predictability — same sequence every time. Smaller step increments. Sensory desensitisation (textures, sounds) alongside fear exposure. May need longer at each step.
😰 Highly Anxious (GAD)
Address overall anxiety alongside specific phobia. Ensure relaxation skills are robust before beginning exposure. May need CBT for GAD before animal phobia work.
👶 Very Young (Ages 3–5)
Focus on behavioural exposure with minimal cognitive work. Shorter sessions (5–8 minutes). More play-based. Parent modelling is very important. Keep it joyful.
Your Child's Personalised Version
Your child's fear ladder. Your family's version. Personalisation is not optional — it is what makes this evidence-based approach work in your specific home, with your specific child.
Build the Hierarchy With Your Child
8–12 steps, using child's own fear ratings. Starting step rated 2–3/10 — just slightly uncomfortable, not overwhelming.
Select Your Materials
Preferred stuffed animal selected | Brave points milestones agreed with child | Coping strategy selected and practised together
Agree the Structure
Cool-down activity agreed | Session frequency set (target: 3–5x/week) | Data capture system in place
Connect to GPT-OS®
Your personalised programme lives inside EverydayTherapyProgramme™ — continuously adapting with your home session data + therapist clinical inputs + TherapeuticAI® recommendations.
✅Pinnacle Consortium Seal: This technique is validated by the Pinnacle Blooms Consortium: Clinical Psychology • Occupational Therapy • ABA • Special Education • Neurodevelopmental Paediatrics.

Week 1–2
Building the Foundation
What to Expect in Weeks 1–2
Progress is in the infrastructure, not the fear level. You are building the tools, the language, the trust, and the process. The fear changes later — after the infrastructure is solid.
✅ What Progress Looks Like
- Child tolerates looking at cartoon/drawn version of feared animal for 30+ seconds
- Child can name and rate their fear (even if it's still high)
- Child knows the coping strategies by name
- Parent and child have completed at least 3 sessions
- Fear thermometer ratings are being recorded
🔄 What Is NOT Progress Yet — And That's Okay
- Fear around real animals is unchanged — this is expected
- Child still avoids and seeks reassurance — this is expected
- Some sessions ended early — this is expected and normal
In weeks 1–2, you are building the infrastructure. The fear changes later. Be patient — the foundation is everything.
Research: PMC11506176 — Systematic review (Children, 2024): Early-phase indicators focus on tolerance and participation, not skill mastery.

Week 3–4
Consolidation — 40%
Week 3–4: Consolidation Signs
Synaptic pathways are forming. The amygdala is receiving corrective information. Your child's brain is literally restructuring its threat-assessment response. This is real neuroscience happening in your living room.
Child references the fear ladder independently
"I'm on step 4!" — Self-initiated engagement is a powerful consolidation indicator.
Fear thermometer ratings decreasing for practised steps
The numbers are the evidence. A step that was a 7 last week is now a 5 — that is measurable neurological change.
Child uses a coping strategy without being prompted
Spontaneous use of breathing or a squeeze tool means the skill is truly internalised.
Child begins making distinctions
"That dog is small — maybe a 3." Nuanced fear assessment means the threat system is differentiating, not generalising.
First spontaneous approach toward a feared representation
The child moves toward the material without being asked. This is the first signal of self-directed bravery.

Week 5–8
Breakthrough — 65%
Week 5–8: Breakthrough Indicators
At around week 5–6, most children experience a notable shift — the fear feels different. It's still uncomfortable, but it's no longer overwhelming. The child begins to believe "I can handle this." That shift in self-efficacy changes everything.
Fear Hierarchy Progression
Child is moving up the ladder at their own pace — each step mastered before the next begins
Manageable Real Encounters
Real animal sightings at distance producing 4–5 rather than 9–10 on the fear thermometer
Talking About Animals
Child discussing feared animals in conversation without immediate distress — huge cognitive progress
Planned Real-Animal Encounter
Child has completed at least one planned real-animal encounter, even briefly at distance
Attempting Previously Avoided Activities
Parent reports child trying parks, neighbours' homes, or outdoor activities that were previously off-limits
"The fear doesn't control her life anymore." — Parent, Pinnacle Network (Illustrative case; individual results vary.)
Celebrating Mastery
Your child is brave. That deserves to be seen — not just by you, but by the whole family. Celebrating milestones is not indulgence; it is evidence-based reinforcement that consolidates neurological change.
First Thermometer Drop Below 3
The first time a previously overwhelming step rates below 3 — the amygdala has officially updated its threat assessment.
First Real Animal Observed
Watching a real animal from a distance without panic — the bridge from representation to reality, crossed.
First Event With Animals Present
Attended a birthday party, park visit, or neighbourhood outing where animals were present. Life participation restored.
Child's First Words: "I'm Still Scared But It's Okay"
This sentence is the finish line. Not the absence of fear — the presence of courage alongside it.
🎉 Celebration Ideas
Special meal or outing chosen by child | "Brave Story" narrated as a family | Brave certificate printed and framed | Video call to grandparents to share achievement | Bravery Milestone added to brave points chart in a special colour
Red Flags & When to Escalate
Home practice has limits. Knowing when to call for professional support is not a sign of failure — it is expert parenting. These red flags indicate the need for clinical supervision immediately.
🔴 Seek Professional Support If:
• Panic attacks (hyperventilation, chest pain, loss of consciousness)
• Fear spreading rapidly to all animals and broader phobia categories
• Child refusing school, meals, or sleep due to fear
• Home exposure attempts are consistently traumatising
• No improvement after 8 weeks of consistent home practice
• Co-occurring depression, other phobias, or self-harm
• Fear stems from a genuine traumatic animal encounter (attack, bite)
• Fear spreading rapidly to all animals and broader phobia categories
• Child refusing school, meals, or sleep due to fear
• Home exposure attempts are consistently traumatising
• No improvement after 8 weeks of consistent home practice
• Co-occurring depression, other phobias, or self-harm
• Fear stems from a genuine traumatic animal encounter (attack, bite)
Escalation Pathway
01
FREE Helpline
📞9100 181 181 — 16+ languages, 24×7
02
AbilityScore® Assessment
Full functional evaluation across all domains
03
GPT-OS® Guided Programme
Professional CBT under clinical supervision
04
FusionModule™ Coordination
Psychology + OT + ABA + NeuroDev converged
05
Pinnacle Centre Near You
70+ centres across India for in-person care
Progression Pathway: The Broader Journey
Animal fears don't exist in isolation. C-283 sits within a complete emotional regulation curriculum. Understanding the full C-series helps caregivers and clinicians see where this technique fits — and what comes next.
1
C-281
Understanding Childhood Fears vs. Phobias
2
C-282
Recognising Anxiety in Children
3
C-283
ANIMAL FEARS — THIS PAGE
4
C-284
Medical Procedure Anxiety
5
C-285
Separation Anxiety
6
C-286
Social Anxiety in Children
Foundational Techniques Supporting C-283
- C-231: Meltdown Management — regulate first, expose second
- Domain A Sensory Techniques — for children with sensory-driven fear components
- B-198: Emotional Communication — building the language to describe fear
Techniques That Build On C-283
Related Techniques
C-283 connects laterally to a broad network of evidence-based techniques across multiple domains. These interconnects help clinicians and parents build comprehensive, co-occurring support plans.
Technique | Domain | Why Related | |
Emotional Reg | Build the diagnostic vocabulary first — know what you're treating before you treat it | ||
Emotional Reg | Common co-occurrence — children with animal phobia frequently present with separation anxiety | ||
Sensory | Animal sounds (barking, birds) are often the primary trigger — addresses the auditory component | ||
ABA | Understanding fear-maintained avoidance at a functional level guides hierarchy design | ||
Social Comm | Language for fear expression enables fear thermometer use and self-advocacy |
The Full Therapeutic Map
C-283 is one technique in a complete therapeutic universe — 999 techniques across 12 domains, unified by GPT-OS®. Every technique is interconnected, every domain informs every other.
Domain | Focus | Techniques | |
A | Sensory Processing | Tactile, Auditory, Visual, Vestibular, Proprioceptive | |
B | Social Communication | Prelinguistic, Joint Attention, Language Building | |
C ← YOU ARE HERE | Emotional Regulation | Anxiety, Phobias, Meltdown, Self-Regulation | |
D | Behaviour / ABA | Stimming, Repetitive Behaviour, Skill Acquisition | |
E | Cognitive Development | Attention, Memory, Executive Function | |
F | Fine Motor | Handwriting, Scissors, Manipulation | |
G | Gross Motor | Balance, Coordination, Locomotion | |
H | Speech & Language | Articulation, Fluency, Voice | |
I | Feeding & Oral Motor | Texture, Chewing, Swallowing | |
J | Daily Living Skills | Dressing, Toileting, Self-Care | |
K | Family & Caregiver | Parent Training, Sibling Support | |
L | School Readiness | Pre-Academic, Social School Skills |

Family Stories From the Journey
Parents who have walked this path — and what they found on the other side. These stories are what evidence-based practice looks like in real families, in real homes.
"For two years, we couldn't go to the park, visit my in-laws (who have a dog), or go to any birthday party. My son's world was shrinking and so was ours. The fear ladder felt impossibly slow at first. Cartoon pictures for a week? Really? But by week 4, he was watching dog videos and laughing. By month 3, he stood 10 metres from my brother's dog and gave me a thumbs up. That thumbs up is the moment I carry with me." — Parent, Chennai | Pinnacle Network (Illustrative; individual outcomes vary.)
"It wasn't just dogs. Birds terrified her. Pigeons, sparrows, even a butterfly startled her. Our OT called it fear generalisation. The hierarchy we built started with toy birds — very small, very still. It took 12 weeks of patient, consistent work. Now she feeds pigeons at the park. Every single pigeon in India is her friend." — Parent, Hyderabad | Pinnacle Network (Illustrative; individual outcomes vary.)
📊 GPT-OS® tracks fear generalisation patterns across the network. Families whose children showed fear generalisation still showed 97%+ measured improvement with extended, structured exposure protocols.
Connect With the Pinnacle Community
You don't have to figure this out alone. Thousands of parents across India and the world are navigating the same journey — and the Pinnacle community exists to walk alongside you.
Pinnacle Parent Community
Join thousands of parents navigating similar journeys — forums, peer support, and shared experience
WhatsApp Support Group
Real-time peer support, available via 9100 181 181 — connect with a community that understands
pinnacleblooms.org/community
Forums, resources, and parent webinars — searchable, multilingual, clinician-moderated
care@pinnacleblooms.org
Clinical questions answered within 24 hours by the Pinnacle team — care@pinnacleblooms.org
International Resources
ADAA — Anxiety and Depression Association of America — Parent resources on childhood phobias
AACAP — American Academy of Child & Adolescent Psychiatry
WHO Nurturing Care Framework
AACAP — American Academy of Child & Adolescent Psychiatry
WHO Nurturing Care Framework
📞FREE National Autism & Child Development Helpline: 9100 181 181
16+ languages | 24×7 | India-wide | DPIIT Recognised
16+ languages | 24×7 | India-wide | DPIIT Recognised
Find Your Nearest Pinnacle Centre
70+ centres across India. One converged system. Whether you need a full clinical team or a single specialist, Pinnacle's network delivers the same evidence-based GPT-OS® framework wherever you are.
🏥 Full-Service Therapy Centre
OT + SLP + ABA + Psychology + Special Education — complete multi-disciplinary team under one roof
🧠 Anxiety & Phobia Specialist Clinic
Dedicated clinical psychology and CBT services for specific phobia intervention including C-283
🏠 Home Visit Programme
Selected cities — the therapist comes to your home, within the child's own environment
📱 Teleconsultation
India-wide + 70 countries — GPT-OS® guided sessions from anywhere, anytime
Services Relevant to C-283
- Child Psychology — CBT for specific phobias
- Occupational Therapy — Sensory-integrated fear desensitisation
- ABA — Functional analysis and exposure hierarchy design
- Parent Training — Guided home programme coaching
📞9100 181 181 — Call to be connected with your nearest centre or book a teleconsultation today
The Research Library
Read the science behind these 9 materials. Every element of C-283 is grounded in the highest tier of clinical evidence — from systematic reviews to real-world data across 20M+ sessions.
Study | Summary | Link | |
CBT + Graduated Exposure Meta-Analysis | Gold-standard treatment for specific phobias in children. Systematic desensitisation significantly reduces fear and avoidance. | ||
AACAP Practice Parameters (2007/2020) | Exposure-based CBT is first-line for childhood specific phobias. | ||
ADAA Exposure Guidelines | Graduated, child-paced approaches produce durable fear reduction with low relapse rates. | ||
WHO Nurturing Care Framework (2018) | Global standard for early childhood emotional development and caregiver-delivered interventions. | ||
Padmanabha et al., Indian J Pediatr (2019) | Home-based interventions demonstrate significant outcomes in Indian paediatric populations. | DOI: 10.1007/s12098-018-2747-4 | |
PMC10955541 — World J Clin Cases (2024) | Sensory integration + exposure therapy promotes adaptive behaviour, social skills, participation. | ||
PMC11506176 — Children Systematic Review (2024) | 16 articles confirming sensory integration as evidence-based practice for ASD + anxiety. |

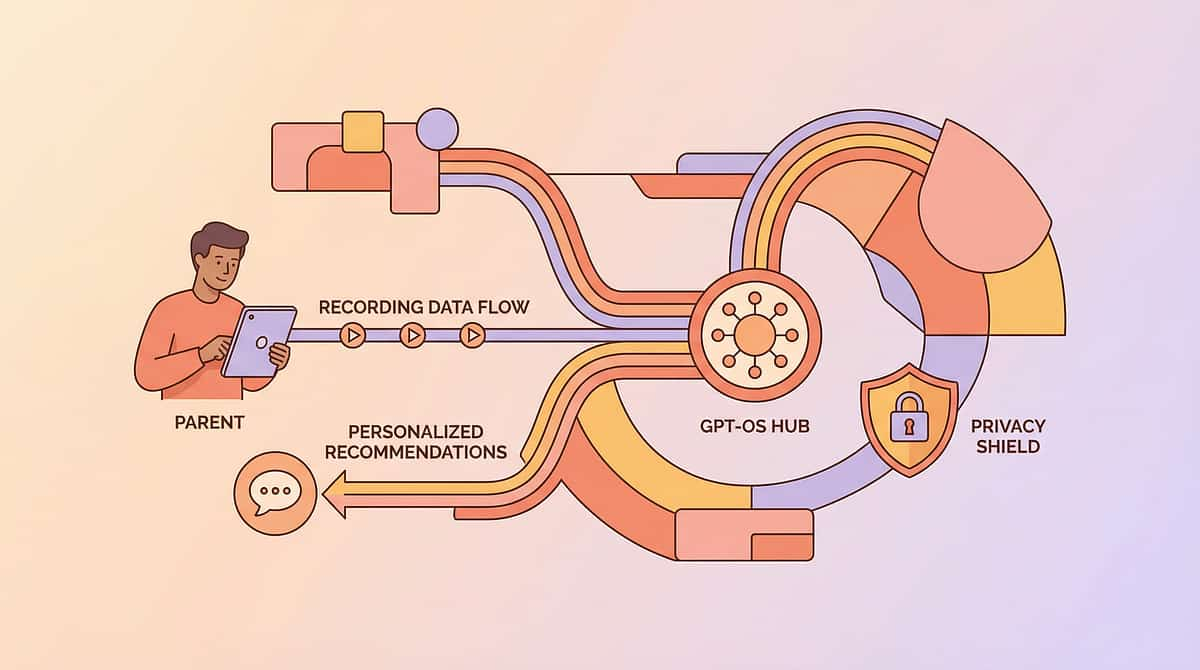
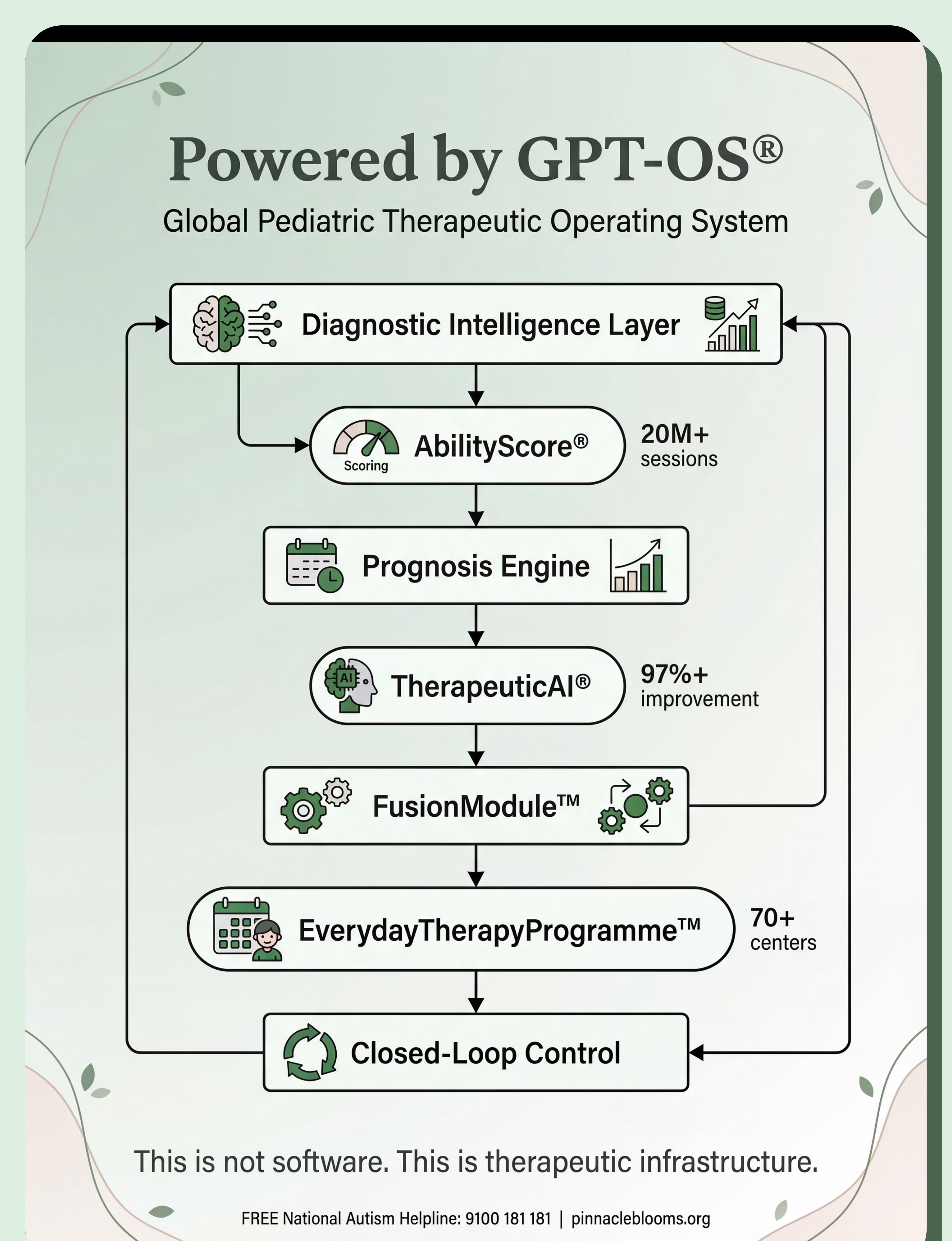
How GPT-OS® Uses Your Data
This is not software. This is therapeutic infrastructure. GPT-OS® is the Global Pediatric Therapeutic Operating System — a closed-loop AI engine that transforms your home session data into a continuously optimised, personalised intervention plan.
GPT-OS® specifically learns from C-283 data: speed of habituation at each fear ladder step | which materials produce fastest fear reduction | optimal session length and frequency for this child profile | predictors of relapse and how to prevent them | how animal phobia outcomes correlate with sensory profile across the population.
🔒 Privacy Assurance
All data is DPDPA (India) compliant. Your child's data is never sold. Population-level anonymised insights improve recommendations for all families. "Your data helps every child like yours."
📊 System Stats
20M+ sessions | 97%+ improvement | 70+ centres | Patents filed 160+ countries
Watch the Reel: C-283
Multi-modal learning — visual demonstration combined with text and clinical guidance — significantly improves parent skill acquisition and technique fidelity. Reel C-283 shows you exactly what this looks like in practice.
Reel C-283 Details
Title: 9 Materials That Help With Animal Fears
Series: Emotional Regulation & Anxiety Management
Domain: Domain C — Emotional Regulation / Anxiety
Duration: 75–85 seconds
Series: Emotional Regulation & Anxiety Management
Domain: Domain C — Emotional Regulation / Anxiety
Duration: 75–85 seconds
What You'll See
- 🎬 Child engaging with fear ladder, marking completed steps
- 🎬 Gradual stuffed animal engagement sequence
- 🎬 Parent and child reading animal book together
- 🎬 Child watching calm animal video with control over playback
- 🎬 Using breathing tools and fear thermometer
- 🎬 Brave points celebration moment
- 🎬 Planned animal encounter from comfortable distance
"Animal fears are among the most treatable childhood conditions when approached correctly. The key is graduated exposure: small steps that build tolerance without traumatising. These materials support that process at home — making the therapeutic middle path accessible to every family." — Therapist Voiceover, Reel C-283
Video modelling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning improves parent skill acquisition. → Browse all 999 Reels at Pinnacle Platform
Share With Your Family
Consistency across caregivers multiplies therapeutic impact. When grandparents, teachers, and other family members understand the approach, the child receives a unified, reinforcing environment across all contexts.
"Explain to Grandparents" Simplified Version
"[Child's name] is working on getting braver around [dogs/birds/animals]. The therapist says the way to help is NOT to say 'don't be scared' or force her near the animal. Instead, we're taking very small steps — from looking at pictures all the way to being near a calm animal. Her brave chart is on the wall. Please give her a brave point if she tries anything scary. Call us if you have questions."
Teacher Communication Template
"Dear [Teacher], [Child] is participating in a structured anxiety programme for animal-related fears. Please avoid discussing animals unexpectedly / let [child] use the coping card in class / avoid letting classroom animals approach without warning. We'd appreciate consistency with home strategies. Happy to discuss at our next meeting."
Research: WHO CCD Package emphasises multi-caregiver training as critical for intervention generalisation and maintenance. PMC9978394

Frequently Asked Questions
Your questions, answered by the Pinnacle Consortium. These are the questions every family asks — and the answers that the evidence actually supports.
"My child's fear seems irrational. Do I need to treat it as real?"
Yes, absolutely. The fear response is completely real — physiologically and neurologically — even if the danger is objectively low. Treating the fear as real while gently building tolerance is the only approach that works. Dismissing it as irrational makes it worse.
"How long will this take?"
Most children show meaningful progress within 8–12 weeks of consistent, structured practice. Speed depends on severity, consistency, child's age and temperament, and co-occurring conditions. Some show dramatic change in 4–6 weeks; others take 4–6 months. Progress is real even when it's slow.
"My spouse thinks we should just force the child near the dog. What do I say?"
Flooding (forced exposure) is not graduated exposure therapy. Research shows flooding without child-controlled pacing typically increases fear and can be traumatising. Graduated exposure has the highest evidence base for lasting results. Share Card 5 (Evidence Card) with your spouse.
"Can we start this if my child hasn't been formally diagnosed?"
Yes. These materials are helpful for any child with significant animal fears, regardless of diagnosis. If there is a formal diagnosis (autism, anxiety disorder), the programme should ideally be supervised by a clinician. Call 9100 181 181 for guidance.
"What if my child's fear is only of one specific animal (like just dogs)?"
Single-animal fears often respond faster than generalised animal fears. Build your hierarchy specifically around dogs (or the specific feared animal). The same materials and process apply — and outcomes are typically excellent.
"Is this the same as what a psychologist would use?"
This programme is based on the same evidence-based CBT + graduated exposure principles used by clinical psychologists — adapted for home delivery within the GPT-OS® framework. For severe phobias, a licensed psychologist should supervise or lead treatment.
"Can I use these materials for fear of insects or snakes?"
Yes. The graduated exposure framework applies to any animal phobia. Build the hierarchy specific to the feared animal. Be especially careful with snakes — real-animal encounters require absolute control. Insects are often effectively addressed with photos, videos, and observation from distance.
"My child with autism has extreme animal fear. Is this approach safe?"
Yes, with adaptations. Autistic children may need smaller hierarchy steps, more predictability, additional sensory supports, and longer time at each step. Professional guidance is recommended. See the Adapt card for autism-specific modifications. Call 9100 181 181 for personalised guidance.
Preview of 9 materials that help with animal fears Therapy Material
Below is a visual preview of 9 materials that help with animal fears therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

Your Next Step: Start Now
You have everything you need. Your child is ready to be free. Start with one step. One material. One session. That's how fear ladders are climbed — and that's how worlds stop shrinking and start expanding again.
✅Validated by the Pinnacle Blooms Consortium®
Clinical Psychology • Occupational Therapy • ABA • Special Education • Neurodevelopmental Paediatrics
20M+ sessions | 97%+ improvement | 70+ centres | 70+ countries served
Clinical Psychology • Occupational Therapy • ABA • Special Education • Neurodevelopmental Paediatrics
20M+ sessions | 97%+ improvement | 70+ centres | 70+ countries served
From Terror to Tolerance. One Technique at a Time.
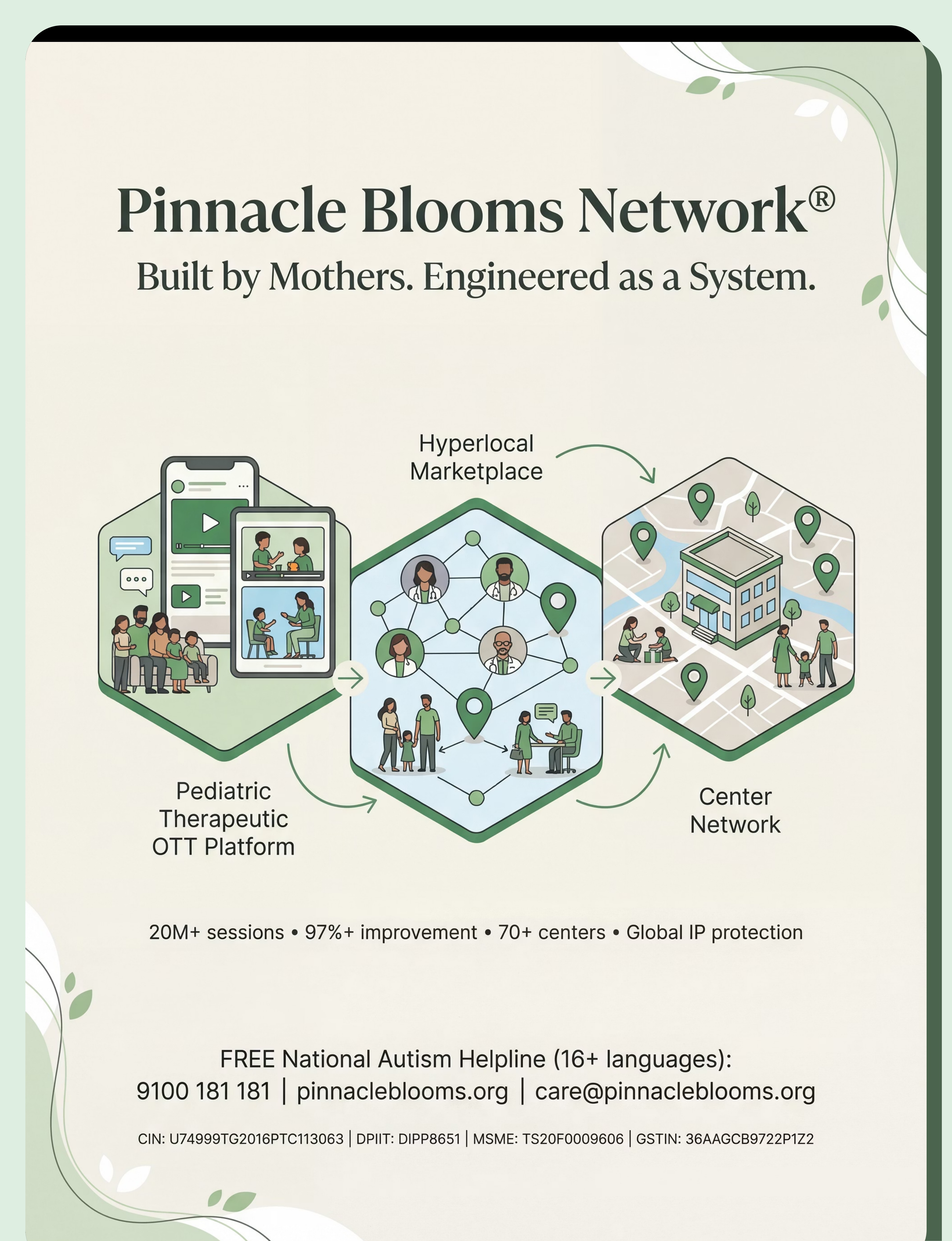
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7, personalised, multi-sensory, multi-disciplinary, integrated therapeutic environment — powered by GPT-OS® and the collective expertise of the world's most comprehensive paediatric therapy consortium.
⚕️Medical Disclaimer: This content is educational. It does not replace individualised assessment and intervention planning with licensed mental health professionals. Severe phobias may require professional cognitive-behavioural therapy with trained specialists. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
📞 FREE National Autism Helpline (16+ languages): 9100 181 181 | 🌐pinnacleblooms.org | 📧care@pinnacleblooms.org
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Built by Mothers. Engineered as a System.
"This is not software. This is therapeutic infrastructure." — GPT-OS® | Global Pediatric Therapeutic Operating System