
Sensory Regulation Series — D-370
Ages 2–12 | Occupational Therapy Lead
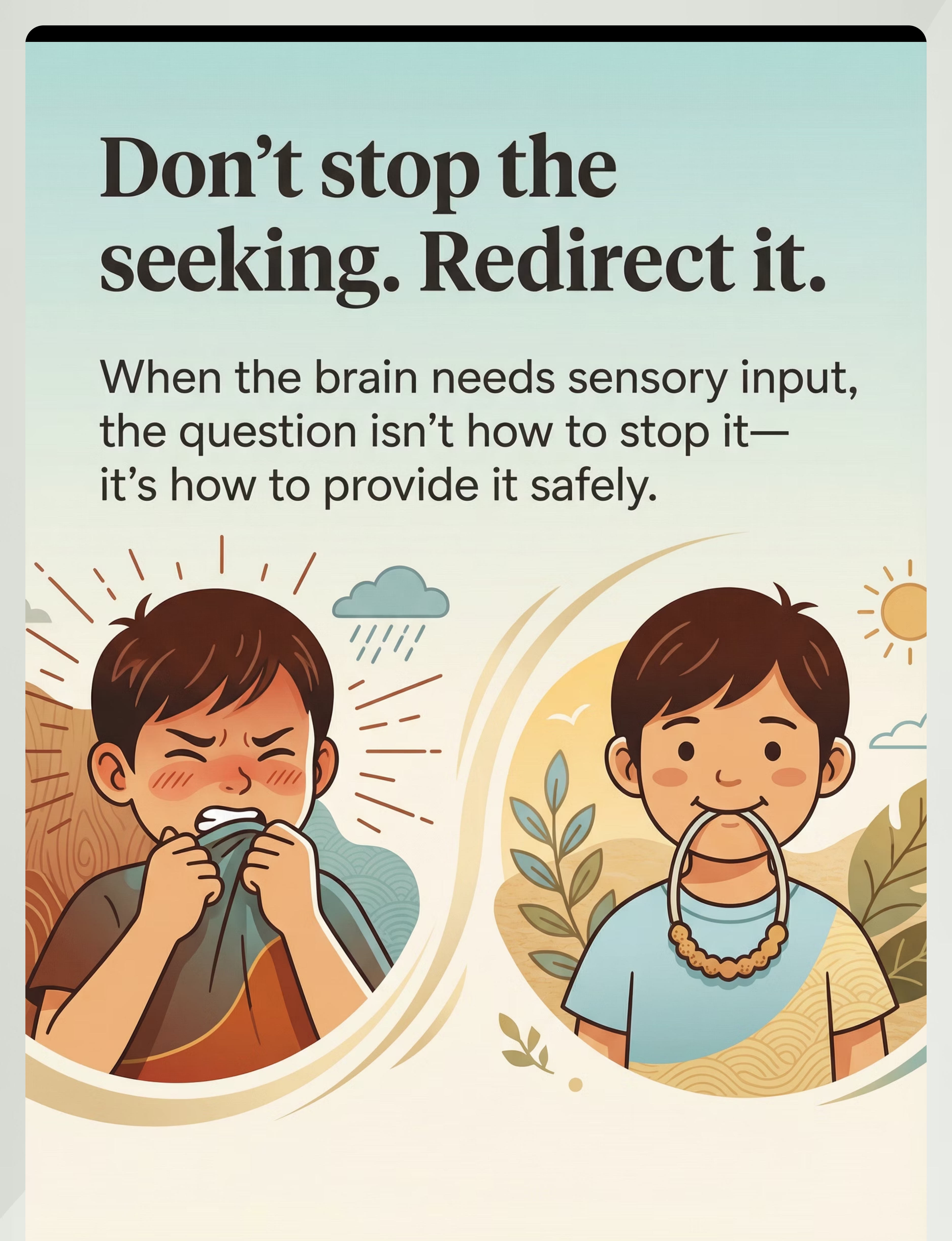
"Don't Stop the Seeking. Redirect It."
Your child's brain isn't misbehaving — it's searching for the input it needs. This page will teach you how to listen, understand, and respond with 9 science-backed sensory alternatives used by 70+ Pinnacle therapy centers.

9 in 10 Families Navigating This Have Never Been Shown This Approach
80%
Sensory Differences
of children with autism display sensory processing differences that drive seeking behaviors
1:36
ASD Diagnosis Rate
children in the US diagnosed with ASD; India estimates at 1:40 in the pediatric population
62M
Children in India
under 15 with neurodevelopmental support needs — sensory differences present in the majority
When your child seeks sensory input through chewing, crashing, spinning, or constant touching — you are among millions of families worldwide navigating the same neurological reality. Sensory seeking is not defiance. It is not a parenting failure. It is a wiring difference that science fully understands — and that evidence-based intervention can redirect safely and effectively. "You are among millions of families facing this. You are not alone. And you now have a roadmap."

The Brain That Seeks Is Not Broken — It's Searching
The Neuroscience (Plain English)
Your child's brain is like a GPS that needs satellites. Different brains need different types of sensory "signal" to feel organized, calm, and ready to learn. Some brains need more deep-pressure signal (proprioception). Some need more movement signal (vestibular). Some need more touch signal (tactile).
When the brain isn't getting enough of its preferred signal, it drives behavior designed to get more — chewing, crashing, spinning, touching everything. This is not misbehavior. This is biology.
The solution is not to stop the seeking. It's to provide better pathways to get the signal the brain needs.
Four Sensory Pathways
Proprioceptive System
Joint and muscle receptors drive chewing (jaw proprioception), crashing (joint compression), and heavy work when input is insufficient.
Vestibular System
Inner ear → cerebellum integration. Under-responsive systems drive spinning, rocking, swinging, and constant movement-seeking.
Tactile System
Skin mechanoreceptors drive touching, mouthing, and texture-seeking when tactile needs go unmet.
Oral Proprioceptive
Periodontal ligament and jaw mechanoreceptors provide the most direct proprioceptive input available — why oral seeking is so persistent.
"Sensory needs are neurobiological, not behavioral choices. You cannot punish or reason them away. But you can redirect them to safe, appropriate, and effective alternatives." — Pinnacle Blooms Consortium, Occupational Therapy Division
Sensory Seeking Across the Developmental Timeline
Ages 2–4
Peak sensory seeking. Brain is rapidly building sensory maps. Seeking behaviors are most intense and visible. This is the prime intervention window.
Ages 5–7
School entry creates friction. Sensory needs collide with classroom demands. Alternative sensory input strategies become critical for inclusion.
Ages 8–12
Entrenchment risk. If unaddressed, seeking behaviors become more conspicuous. Intervention remains highly effective; emphasis shifts to self-monitoring.
Adolescence
Self-management strategies become the focus. Adult adaptive functioning and independence are the long-term goals of early intervention.
Sensory processing differences commonly co-occur with: Autism Spectrum Disorder (80%+ prevalence) | ADHD (sensory modulation component) | Developmental Coordination Disorder | Anxiety disorders (sensory avoidance pattern). "Your child is here. The intervention window is open. The path leads from seeking without alternatives → to seeking with appropriate tools → to self-monitoring sensory needs with independence."

Clinically Validated. Home-Applicable. Parent-Proven.
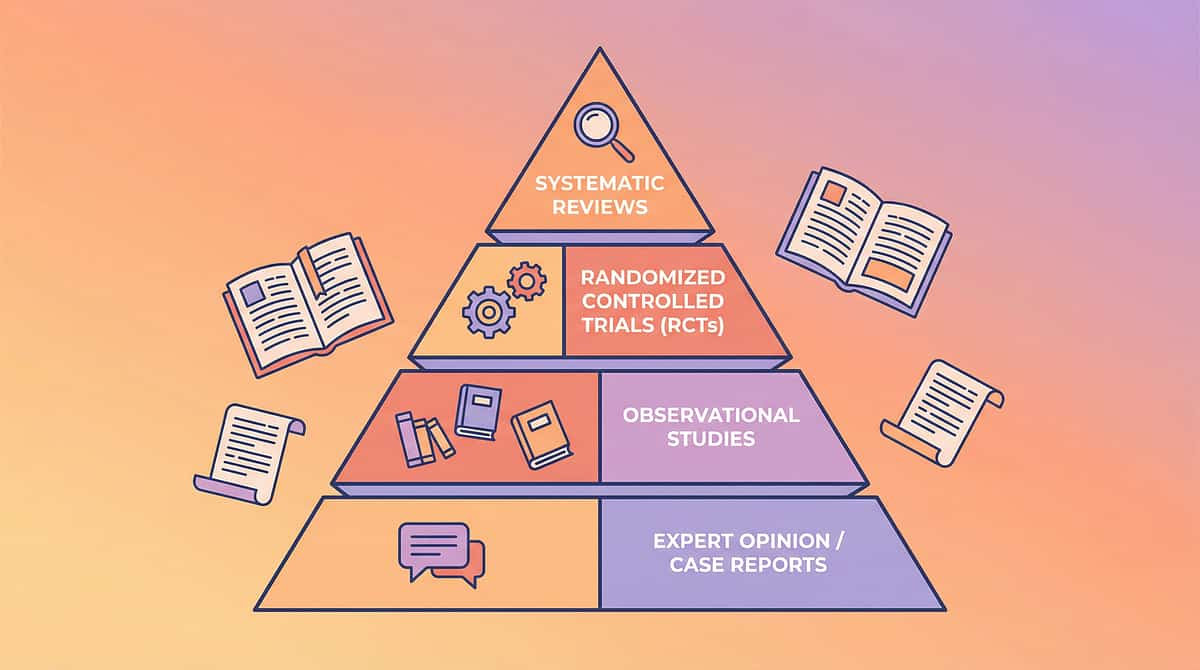
Level I–II Evidence
Systematic Review + Meta-Analysis + RCT Support
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria as evidence-based practice for children with ASD. Outcomes include sensory regulation, motor skills, adaptive behavior, and social participation. PMC11506176
Meta-Analysis, World J Clin Cases (2024)
24 studies demonstrate sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills across diverse populations. PMC10955541
Indian RCT, Indian J Pediatrics (2019)
Home-based sensory interventions by trained parents demonstrated significant developmental outcomes in Indian pediatric populations with ASD. Padmanabha et al. DOI: 10.1007/s12098-018-2747-4
WHO/UNICEF CCD Package
Implemented in 54 low- and middle-income countries. Household-material-based interventions demonstrate efficacy equivalent to clinic-based approaches when caregiver training is provided. PMC9978394
"The science is clear. The evidence is strong. The question is not whether sensory alternatives work. It's whether your child has access to them starting today."

Alternative Sensory Input — The Technique Defined
Domain D: Autism/Behavioral
D2: Stimming & Repetitive Behaviours
Ages 2–12
Daily Integration
Alternative Sensory Input refers to the practice of providing safe, appropriate, and effective ways to meet the same sensory needs that problematic or unsafe behaviors are attempting to address. When a child's nervous system seeks a specific type of sensory signal — proprioceptive, vestibular, oral, tactile, auditory, or visual — attempting to eliminate the seeking behavior without providing an alternative consistently fails. The brain's need doesn't disappear; it finds another outlet, often equally or more problematic. Sensory substitution identifies precisely what input the brain is seeking and provides appropriate tools that satisfy the same neurological need through safe, dignified, socially acceptable pathways.
Also known as: Sensory Substitution | Replacement Behavior Strategies | Sensory Diet Implementation
Oral Motor Chews
Compression Vest
Wobble Board
Fidget Tool Set
Therapy Swing
Noise-Reducing Headphones

The Pinnacle Blooms Consortium Speaks With One Voice on This
🔵 Occupational Therapy — PRIMARY LEAD
OTs design the full sensory diet, assess sensory processing profiles (SPD subtypes), prescribe appropriate tools by sensory system, and train parents in sensory substitution protocols.
🟢 ABA / BCBA — BEHAVIORAL LAYER
BCBAs provide functional behavior assessment to confirm sensory function of behaviors, design reinforcement for appropriate tool use, and collect data on behavior reduction.
🟡 Speech-Language Pathology — ORAL MOTOR LAYER
SLPs address oral sensory seeking specifically — chewing, mouthing, oral motor sensitivity — using specialized oral motor tools as part of the sensory diet.
🔴 NeuroDev Pediatrics — CLINICAL OVERSIGHT
Provide diagnostic clarity, rule out medical causes, and align sensory intervention with the broader therapeutic plan.
This technique crosses therapy boundaries because the brain doesn't organize by therapy type. Sensory needs are addressed through the convergence of OT, ABA, SLP, and medical expertise — not in isolation. Special Education addresses classroom sensory accommodations; WHO/UNICEF CCD Framework ensures equity-focused adaptation for all resource settings.
Pinnacle Blooms Consortium™ — OT • ABA • SLP • SpEd • NeuroDev
Precision Targeting: What This Intervention Actually Changes
Primary Targets (Observable)
- Reduction in chewing on inappropriate objects (shirts, pencils, non-food items)
- Reduction in unsafe crashing and body-slamming
- Reduction in disruptive fidgeting and inability to remain seated
- Child independently uses appropriate sensory tools
Secondary & Tertiary Gains
- Improved emotional regulation and reduced meltdown frequency
- Improved attention and on-task behavior
- Reduced family and caregiver stress
- Self-awareness and self-monitoring of sensory needs
- Academic engagement and social participation

The 9 Materials That Redirect the Seeking Brain
Each material below maps to a specific sensory system. Your OT will help identify which systems your child most needs support with. Every material has a DIY household alternative — no family is priced out of this approach.
Chewable Jewelry & Oral Motor Tools
Oral Proprioceptive | ₹200–800 | Amazon.in
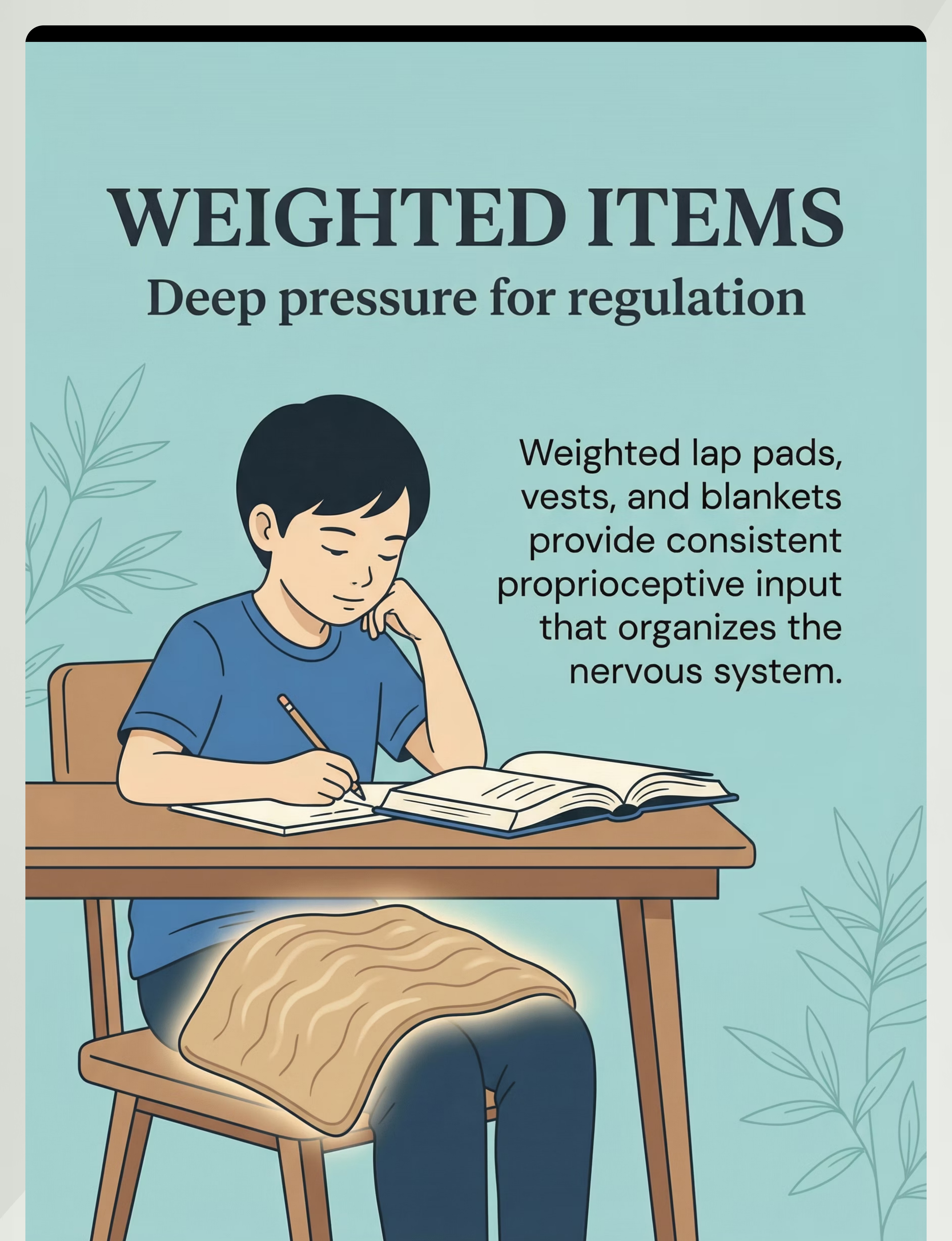
Weighted Items — Lap Pads, Vests, Blankets
Deep Pressure / Proprioceptive | ₹500–3000 | Amazon.in
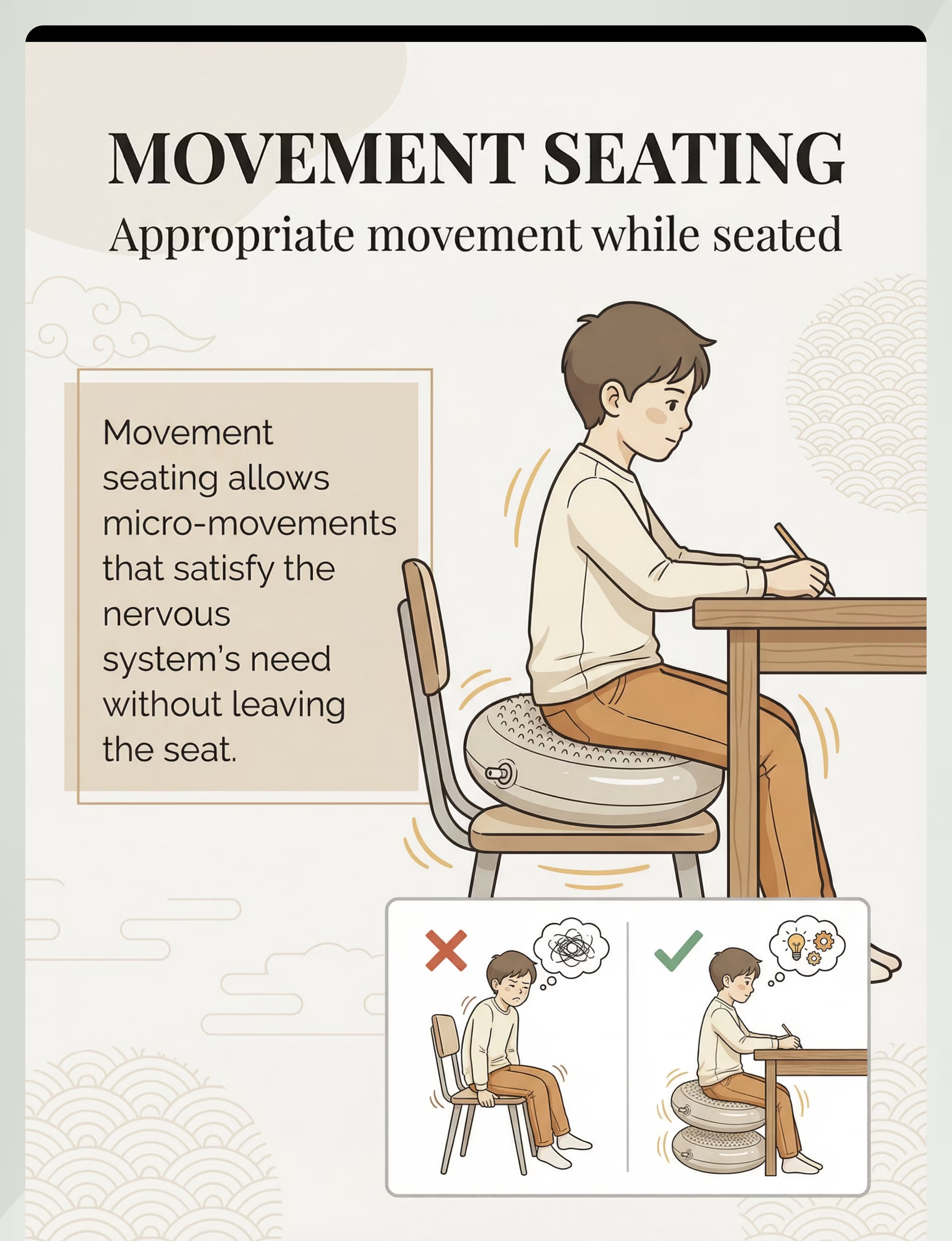
Wobble Cushions, Ball Chairs, Movement Seating
Vestibular / Movement | ₹400–2500 | Amazon.in
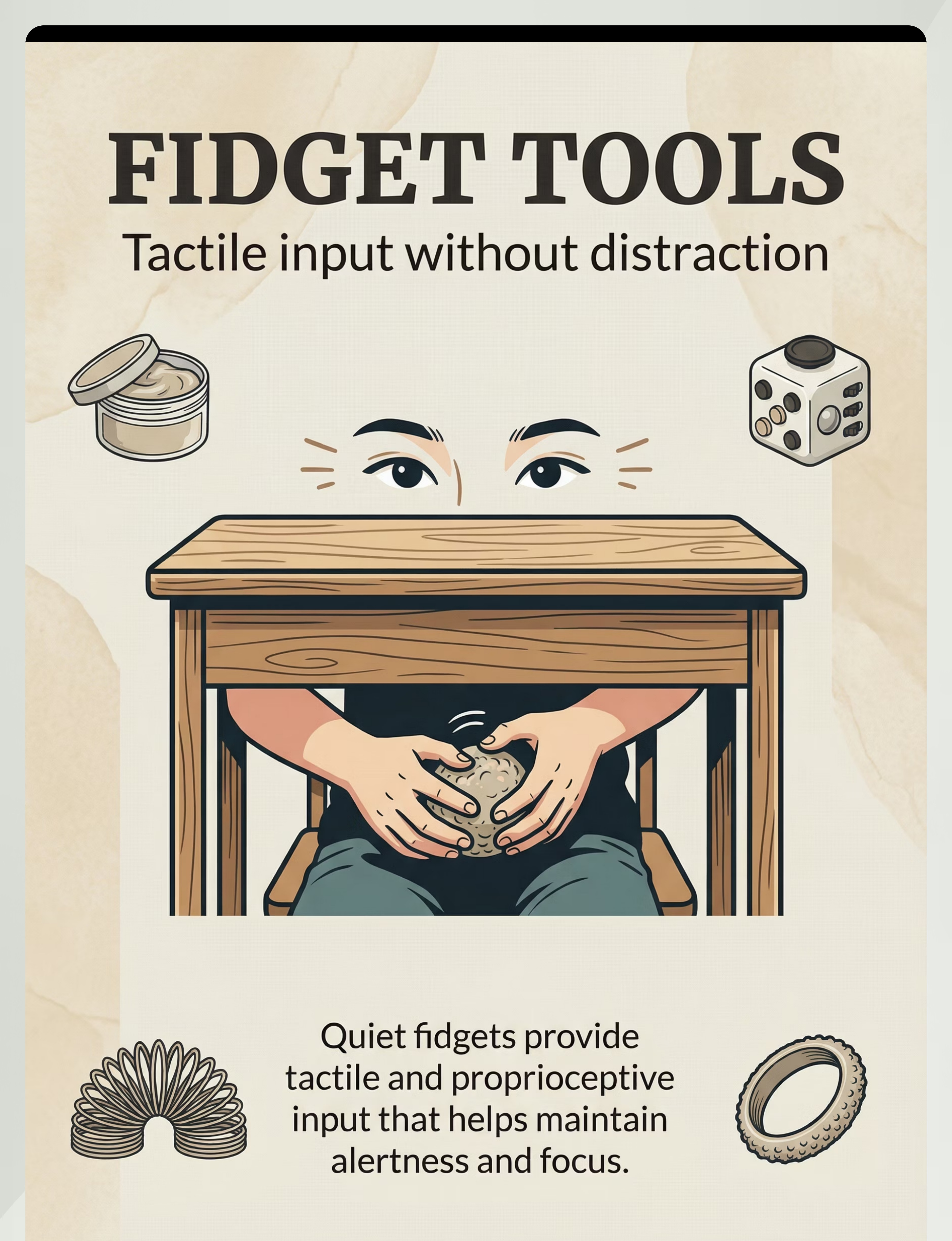
Fidget Tools — Quiet, Purposeful Options
Tactile / Proprioceptive | ₹50–500 | Amazon.in
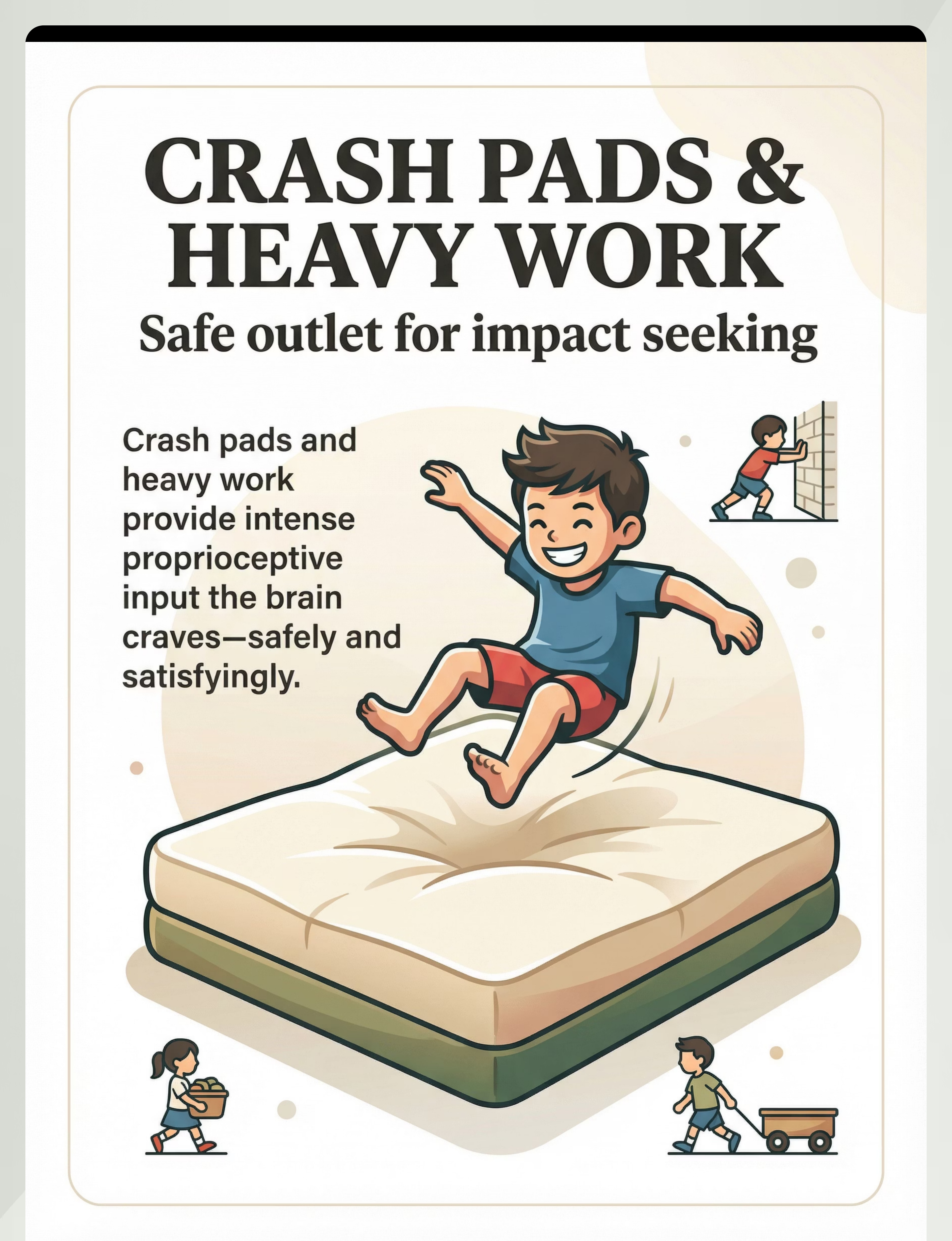
Crash Pads & Heavy Work Materials
Impact / Proprioceptive | ₹1000–5000 | Amazon.in
Noise-Canceling Headphones & White Noise
Auditory | ₹500–3000 | Amazon.in
Sensory Bins & Tactile Exploration Materials
Tactile Exploration | ₹300–1500 | Amazon.in
Therapy Swings, Spin Seats, Rocking Equipment
Vestibular | ₹1000–8000 | Amazon.in
Visual Alternatives — Light Panels, Calming Visuals
Visual | ₹500–3000 | Amazon.in
📞FREE National Autism Helpline: 9100 181 181 — Ask a Pinnacle OT which materials to start with | 16 Languages | 24×7
Material 1: Chewable Jewelry & Oral Motor Tools
Oral Proprioceptive
Most Common Starting Point
Why This Works
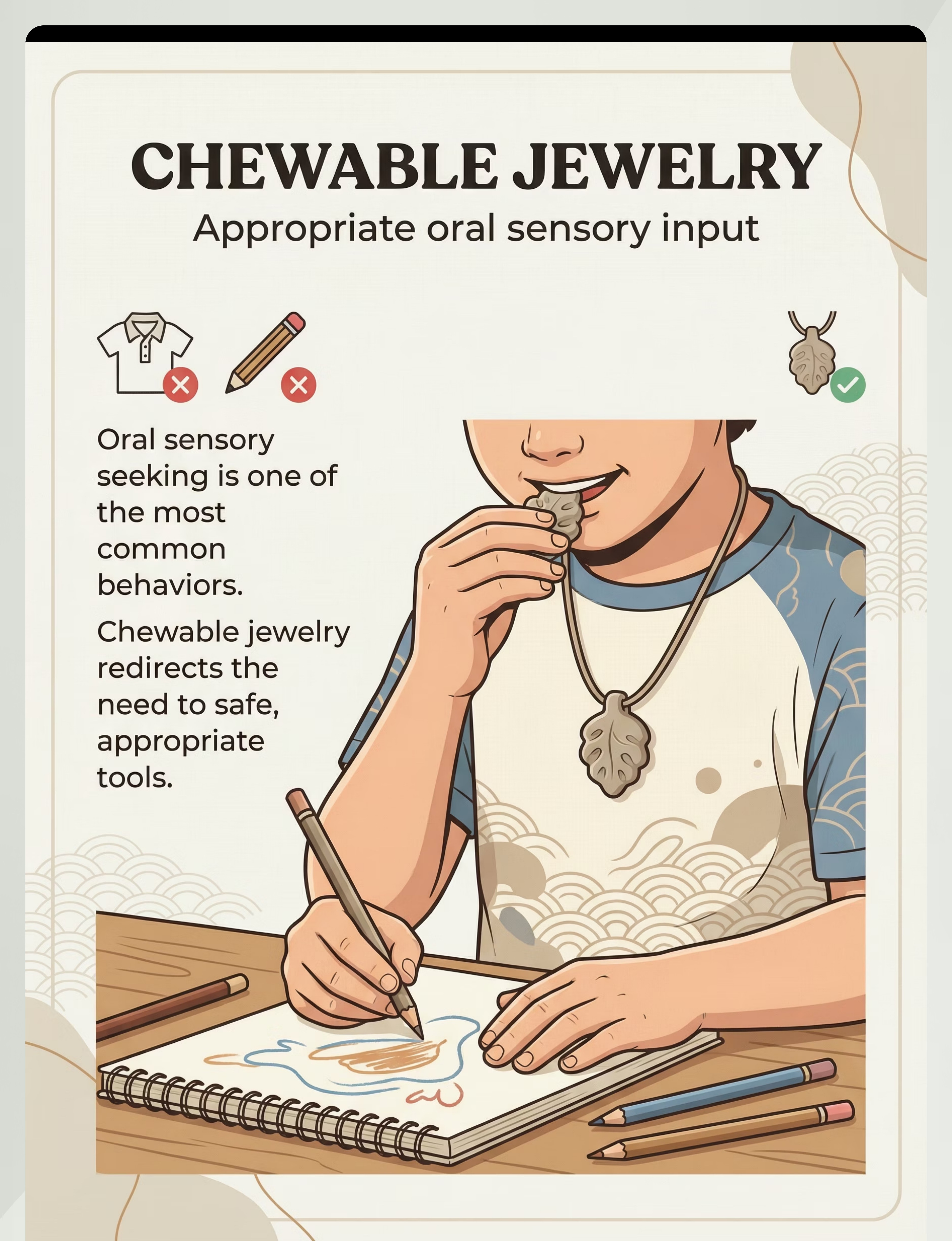
Oral proprioception from jaw movement is one of the most regulating sensory inputs available to the human nervous system. The jaw is rich in mechanoreceptors that send calming proprioceptive signals directly to the brain's regulatory centers.
When a child chews their shirt collar or pencil eraser, they are getting this exact input through an unsafe, socially inappropriate pathway. A chewable necklace delivers the identical neurological signal through a safe, dignified alternative.
Product: 3 Styles Speech Therapy Tools, Oral Kit, Tongue Cleaner
Price: ₹200–800 | Amazon.in
Price: ₹200–800 | Amazon.in
How to Introduce It
- Place around child's neck or in their hand
- Say: "When you feel like chewing, this is the safe thing to chew."
- Do not force into mouth — allow child to explore
- Rotate firmness levels and shapes to maintain engagement
🏠 Zero-Cost DIY Alternative
Food-grade silicone tubing; folded thick fabric strip hemmed at edges; commercial straw cut to necklace length with cord.
⚠️ Safety Note
Check for bites and tears after each use. Replace immediately if damaged — risk of material ingestion. Aggressive chewers require clinical-grade materials; consult an OT.

Material 2: Weighted Items — Lap Pads, Vests & Blankets
Deep Pressure / Proprioceptive
Why This Works
Consistent proprioceptive deep-pressure input organizes the nervous system and reduces the neurological drive to seek heavy pressure through crashing or body-slamming. The gentle, sustained weight tells the brain: "You are here. You are grounded. You are safe."
Product: Mediexchange Compression Vest (2-pair pack)
Price: ₹500–3000 | Amazon.in
Price: ₹500–3000 | Amazon.in
Clinical Guideline
Weighted items should be approximately 10% of the child's body weight. A 20kg child would use a 2kg lap pad. Use 20-minute on/off cycles. Never cover the child's face. Never exceed 15% body weight without OT guidance.
🏠 Zero-Cost DIY Alternative
Pillowcase filled with dried lentils or rice (~10% of body weight); old jeans folded and placed on lap; heavy book covered in soft fabric.
How to Introduce It
- Place on your own lap first, then offer to child's lap
- Say: "This is your heavy blanket. See how heavy? It feels good."
- Allow child to accept or reject; never force placement
- Begin with shorter wear periods and extend as tolerated
⚠️ Safety Note
Watch for pressure marks on skin. Child must be able to remove it independently or request removal. Never use during sleep without OT guidance.
Material 3: Wobble Cushions, Ball Chairs & Movement Seating
Vestibular / Movement Seating
Why This Works
Wobble cushions and movement seating allow continuous micro-movements while seated — satisfying the vestibular system's need for movement input without the child leaving their chair. Research consistently shows that children attend better and stay on-task longer when this movement need is met rather than suppressed.
Product: Wobble Balance Board
Price: ₹400–2500 | Amazon.in
Price: ₹400–2500 | Amazon.in
Introduction & DIY
How to Introduce It
- Place on chair and sit on it yourself first — make it look fun
- Child will naturally want to try it when they see you use it
- Start with slightly deflated for a gentler wobble
- Pair with seated tasks the child enjoys for positive association
🏠 Zero-Cost DIY Alternative
Slightly deflated air-filled cushion or small pillow; folded blanket layer on chair; sitting on a low stool with slightly uneven surface.

Material 4: Fidget Tools — Quiet, Purposeful Options
Tactile / Proprioceptive
Why This Works
Fidget tools provide combined tactile and proprioceptive input through the hands, maintaining alertness and focus while keeping hands productively and appropriately occupied. When hands have something purposeful to do, they are less likely to seek input by touching inappropriate objects, picking at skin, or disrupting others.
Product: ANAB GI Fidget Cube — Stress & Anxiety Pressure Relief
Price: ₹50–500 | Amazon.in
Price: ₹50–500 | Amazon.in
How to Introduce It
- Give to child's hands with no instruction — let them explore freely
- Name what they're doing: "You're squeezing it! That feels good."
- Rotate 3–4 different textures and resistances weekly to maintain engagement
- Avoid fidgets with small parts for children who mouth objects
🏠 Zero-Cost DIY Alternative
Dried lentils in a sealed zip-lock bag (tactile); tightly wound rubber band ball; smooth stone from garden; kneadable dough made from flour + salt.

Material 5: Crash Pads & Heavy Work Materials
Impact / Proprioceptive
Why This Works
Crash pads provide a safe, designated outlet for impact-seeking — the neurological drive that causes children to body-slam furniture, walls, and people. Heavy work (carrying, pushing, pulling, climbing) provides intense proprioceptive joint-compression input that the "crashing brain" craves.
When this input is proactively provided before high-demand situations, unsafe crashing decreases dramatically. Therapy putty and resistive hand tools also provide this deep proprioceptive input in a portable, discreet format.
Product: Therapy Putty (resistive hand tools)
Price: ₹1000–5000 | Amazon.in
Price: ₹1000–5000 | Amazon.in
How to Use It
- Jump or fall on the crash pad yourself first with big positive affect — make it the most appealing object in the room
- Redirect: "Let's crash HERE." and guide child to crash pad
- Build "heavy work breaks" proactively into the daily schedule
- Heavy work before high-demand tasks dramatically improves regulation
🏠 Zero-Cost DIY Alternative
3–4 old mattresses stacked; large bean bag made from old pillows in a zippered cover; soft landing area with folded quilts; carrying grocery bags, pushing laundry basket, climbing stairs.

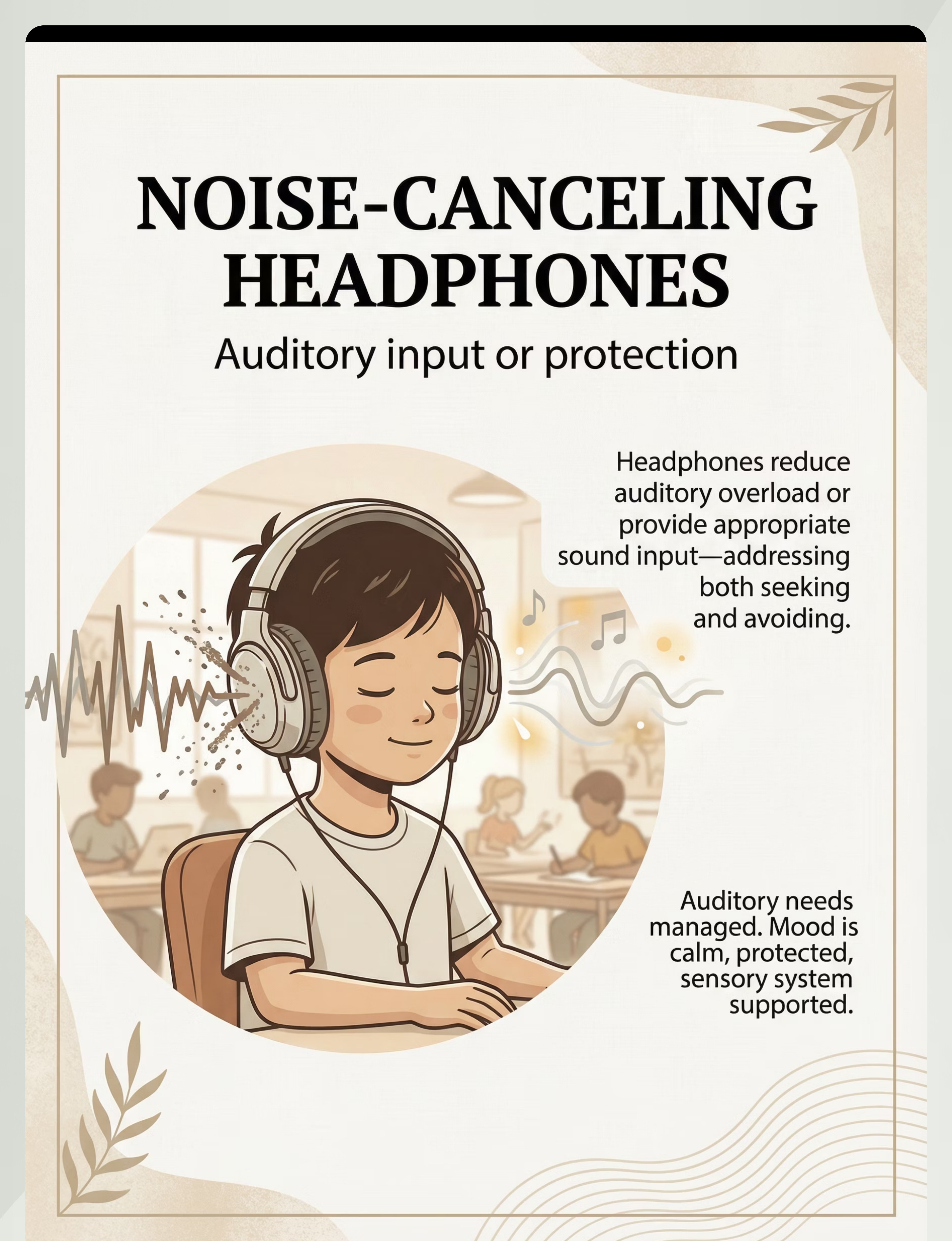
Material 6: Noise-Canceling Headphones & White Noise
Auditory System
Why This Works
Auditory sensory differences manifest in two primary ways: seeking quiet (auditory overwhelm — the child covers ears, hums loudly, or shuts down in noisy environments) and seeking controlled sound (the child makes constant noise, seeks specific sounds, or uses sound to self-regulate).
Noise-reducing headphones address the first by creating a controlled auditory environment. White noise machines address the second by providing consistent, non-triggering background sound that satisfies the auditory system without overload.
Products: SNOWIE SOFT Noise Cancellation Ear Muffs (₹500–3000) + Babelio White Noise Machine (₹800–2000) | Amazon.in
How to Introduce It
- Wear headphones yourself first and describe the experience positively
- Let child touch and handle the headphones before wearing
- Start with very short wearing periods in low-demand situations
- Monitor volume on any audio-producing devices
⚠️ Safety Note
Child must still be able to hear safety-relevant sounds (fire alarm, parent calling urgently). Do not use in settings where the child needs to hear instructions or warnings.
🏠 Zero-Cost DIY Alternative
Cotton ear plugs; soft ear muffs for winter; folded fabric over ears for temporary attenuation; consistent low-volume background music.

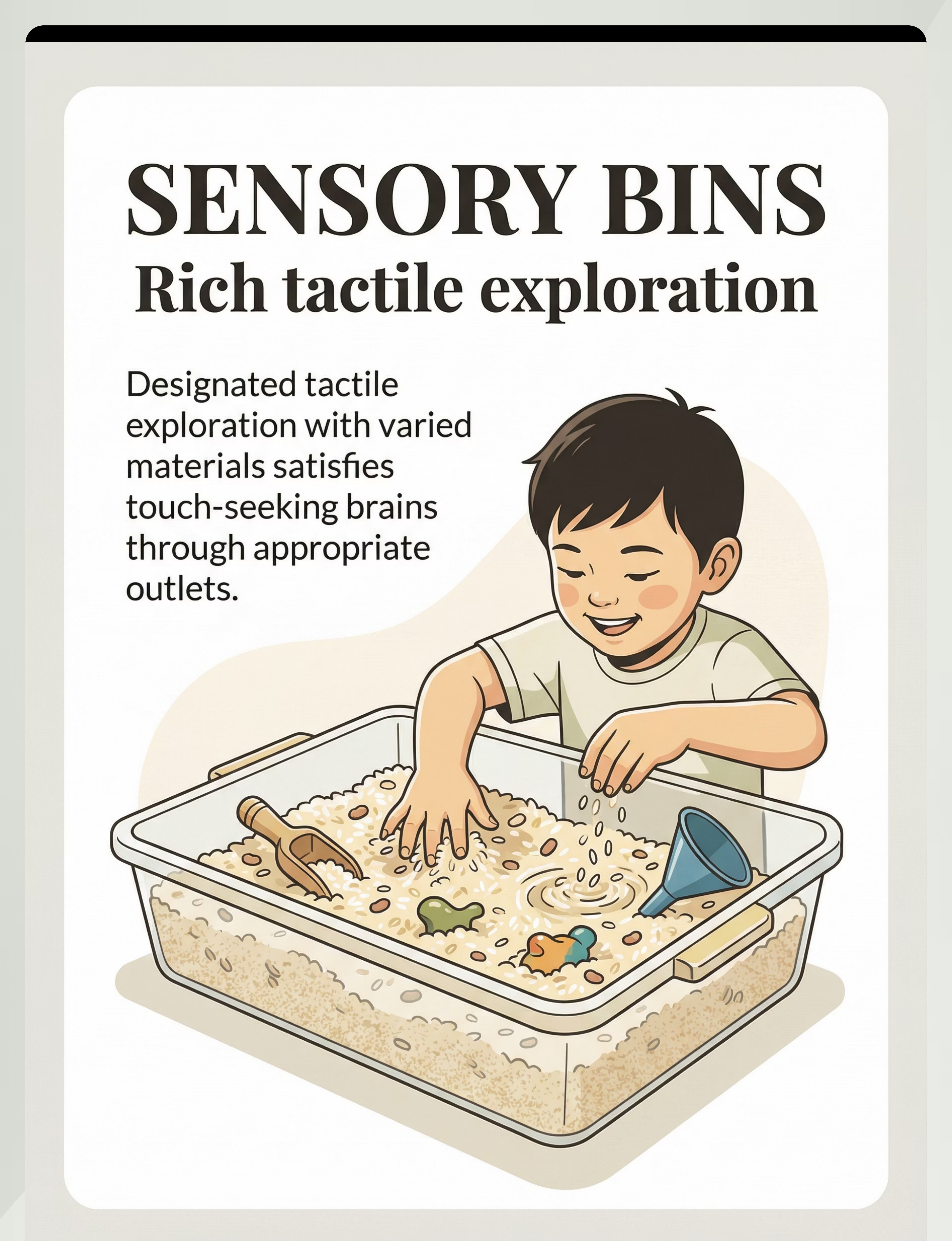
Material 7: Sensory Bins & Tactile Exploration Materials
Tactile Exploration
Why This Works
A sensory bin provides a designated, rich environment for tactile exploration — reducing the neurological drive to touch inappropriate objects throughout the rest of the day. When the tactile system gets its fill in the right place and at the right time, it is less insistent everywhere else.
Products: Littleok Textured Sensory Mat (7 types) + CRAZINOS Kinetic Sand Bucket
Price: ₹300–1500 | Amazon.in
Price: ₹300–1500 | Amazon.in
Rotation Schedule & DIY
Weekly Rotation (maintains engagement)
- Week 1: Uncooked rice
- Week 2: Dried lentils or beans
- Week 3: Kinetic sand
- Week 4: Water beads or dried pasta
🏠 Zero-Cost DIY Alternative
Plastic storage tub + uncooked rice; lentils; sand from local play area; dried pasta; used cooking salt. Rotate weekly to maintain novelty and engagement.
⚠️ Safety Note
Supervise closely with young children. Check for allergens (wheat pasta, nut shells). No mouthing of small items. Keep away from young siblings.

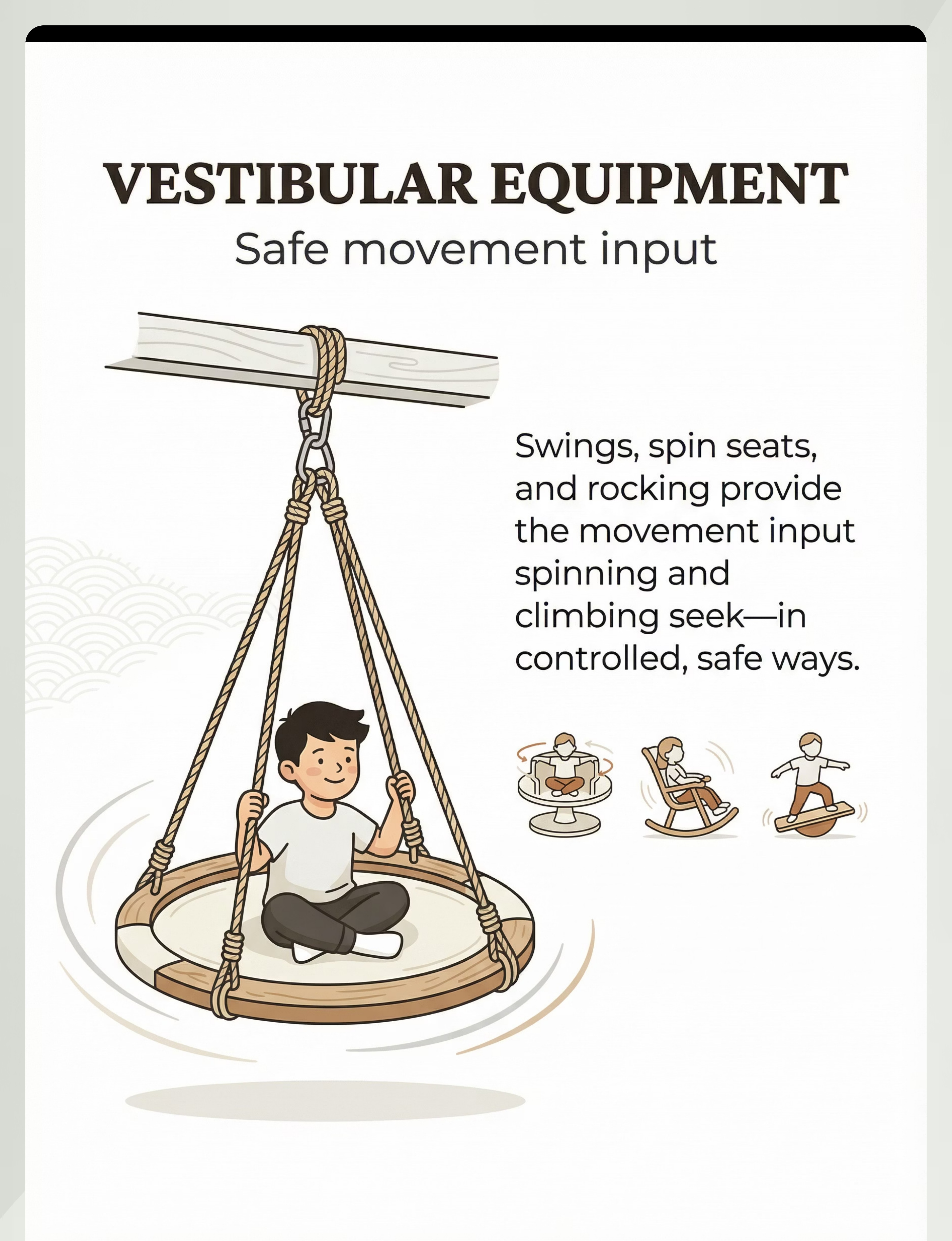
Material 8: Therapy Swings, Spin Seats & Rocking Equipment
Vestibular System
Why This Works
For children whose vestibular system is under-responsive, the drive to spin, swing, rock, and climb is as compelling as hunger. Vestibular input through the inner ear communicates directly with the cerebellum and brainstem — the brain's core regulatory centers.
Therapy swings, spin seats, and rocking equipment provide safe, controlled vestibular input that satisfies this seeking appropriately — without the danger of spinning in traffic, climbing unstable furniture, or rocking in a classroom chair.
Products: Kids Swing Seat + Trampoline with Handle
Price: ₹1000–8000 | Amazon.in
Price: ₹1000–8000 | Amazon.in
How to Use It Safely
- Start with slow, linear movements before rotational input
- Watch for flushed face, glazed eyes, or nausea — stop immediately
- Allow 30–60 seconds of vestibular input, then pause and observe
- Vary swing type: linear vs. rotational for different regulatory effects
- Provide vestibular input BEFORE high-demand situations proactively
🏠 Zero-Cost DIY Alternative
Hammock from old bedsheets between two strong hooks; rocking on a large pillow; seated on a towel that someone gently rocks side-to-side; garden swing.

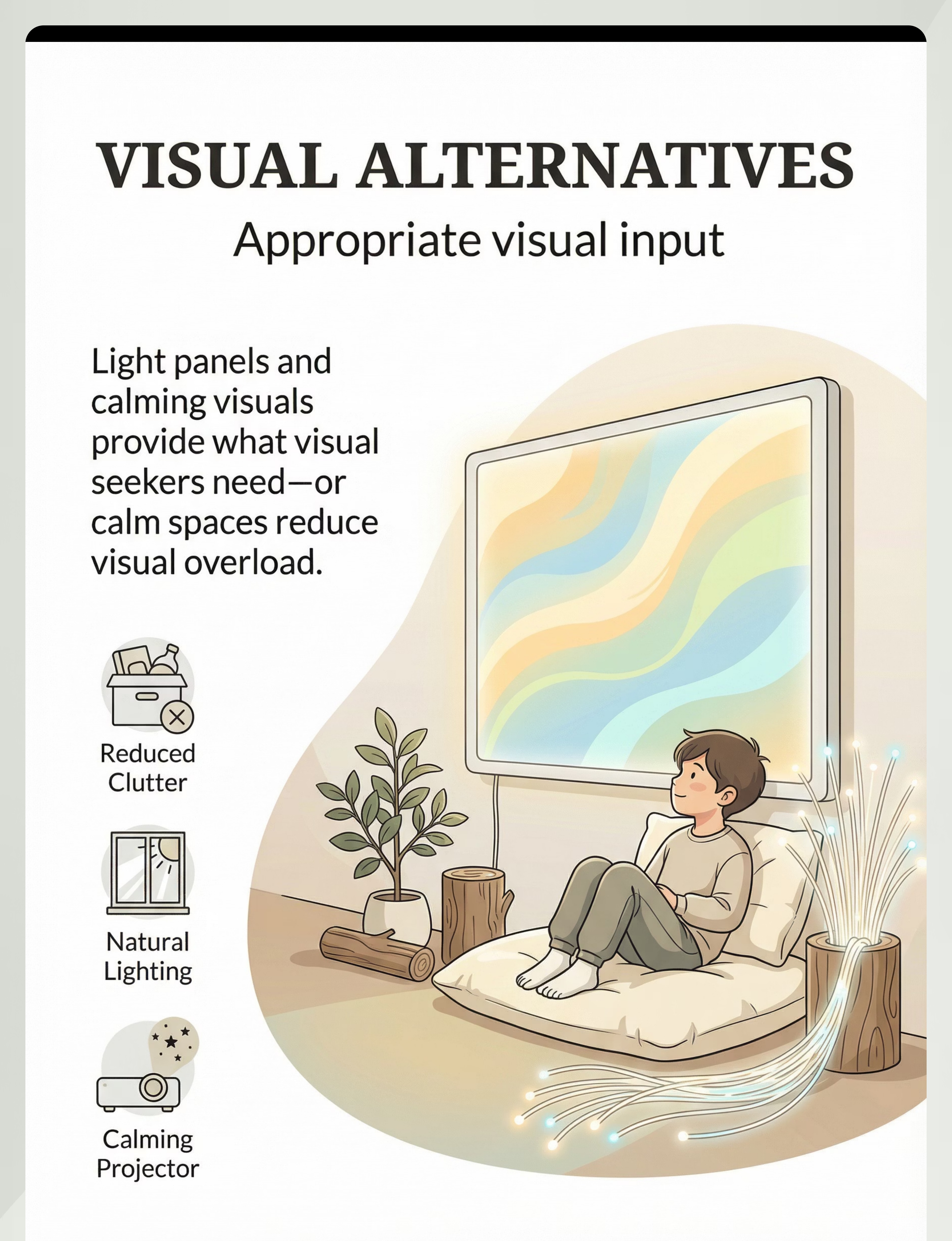
Material 9: Visual Alternatives — Light Panels, Calming Visuals & Vibrating Tools
Visual System
Why This Works
Visual sensory seeking manifests as staring at lights, seeking visual stimulation, tracking moving objects, or being overwhelmed by visual clutter. Visual alternatives provide controlled, calming visual input that satisfies the seeking without overwhelm.
Tinted lenses reduce visual overwhelm for light-sensitive children. Vibrating tools add a tactile + proprioceptive dimension that pairs powerfully with visual regulation strategies.
Products: HANNEA 10-Piece Lens Cover + PIPALIYA Mini Vibrating Massage Tool
Price: ₹500–3000 | Amazon.in
Price: ₹500–3000 | Amazon.in
Practical Application
- Light panels: Use in a dim corner; set to slow color transitions
- Tinted lenses: Trial different tints with OT guidance; start in high-stimulation environments
- Vibrating tools: Apply to hands, arms, or back — follow child's preference
- Reduce visual clutter in the home environment to lower the baseline demand on the visual system
🏠 Zero-Cost DIY Alternative
Dark cloth over one lamp for dim lighting; plain colored paper on walls to reduce visual clutter; bubble-wrap pressing as visual + tactile stimulation; slow-moving fish tank or candle (supervised).
⚠️ Safety Note
No prolonged staring at bright light sources. Consult neurologist before using visual stimulation tools if child has a seizure history.

Every Family Can Start Today — Zero-Cost Options Available
WHO equity principle: Effective sensory alternatives do not require expensive equipment. Every strategy below has a household equivalent.
🛒 Commercial Option | 🏠 Zero-Cost DIY Alternative | |
Chewable Jewelry (₹200–800) | Food-grade silicone tubing; folded thick fabric strip hemmed at edges; commercial straw on cord | |
Weighted Lap Pad (₹500–2000) | Pillowcase filled with dried lentils/rice (~10% body weight); heavy book in soft fabric cover | |
Wobble Cushion (₹400–1500) | Slightly deflated air cushion or small pillow; folded blanket on chair seat | |
Fidget Tools (₹50–500) | Lentils in sealed zip-lock bag; rubber band ball; smooth garden stone; flour-salt dough | |
Crash Pad (₹1000–3000) | Stacked old mattresses; bean bag from old pillows; folded quilts soft landing zone | |
Headphones (₹500–3000) | Cotton ear plugs; soft winter ear muffs; folded fabric over ears | |
Sensory Bin (₹300–1000) | Plastic tub + uncooked rice, lentils, or dried pasta; sand from local play area | |
Swing / Rocking (₹1000+) | Hammock from old bedsheets; rocking on a large pillow; towel rocking with caregiver | |
Visual Alternatives | Dim lamp with dark cloth; plain paper on walls; supervised bubble-wrap pressing |
"The sensory principle works with household items because the brain doesn't know what the material cost. It knows what input it received. A rice-filled pillowcase provides proprioceptive weight input identically to a purchased weighted lap pad. Start with what you have." — Pinnacle Blooms OT + Parent Advisory Panel

Read This Before You Begin — Clinical Safety Gate
🔴 RED — DO NOT PROCEED IF:
- Child is in a meltdown, distressed state, or sensory overload episode
- Child shows signs of illness (fever, ear infection, respiratory distress)
- Chewable material has been bitten through or shows tears
- Child has a known latex allergy (check all materials)
- Weighted item exceeds 10% of body weight without OT guidance
- Child has seizure history and you are introducing visual stimulation tools
🟡 AMBER — MODIFY BEFORE PROCEEDING:
- Child has eaten in the last 30 minutes (reduce vestibular intensity; no inversion)
- Child is tired or post-nap groggy (gentle sensory input only)
- New environment (introduce one tool at a time)
- Child has expressed dislike of a specific tool previously (try a different tool first)
🟢 GREEN — PROCEED:
- Child is in a calm-alert or slightly under-aroused state
- Familiar environment with established routine
- Tools have been checked for safety and condition
- Parent/caregiver is calm and available for the full session
🛑STOP IMMEDIATELY if you observe: self-injury, extreme distress, vomiting (vestibular), loss of consciousness, or allergic reaction. Call 9100 181 181 or your local emergency number.

The Sensory Environment Is Half the Intervention
Remove From the Space
- Screen devices (TV, tablet — visual distraction)
- Excess toys not involved in this session
- Food (unless crunchy snacks are part of oral sensory diet)
- Other children or pets (initial sessions)
Prepare the Space
- Soft mat or carpet on floor (for crash pad safety)
- Natural or warm lighting (not harsh fluorescents)
- Moderate temperature (not too hot — affects regulation)
- Low background sound (or deliberate white noise)
- All materials accessible but not overwhelming — introduce 1–2 initially
Parent Preparation Checklist
- Phone on silent
- 20–30 minutes of uninterrupted time set aside
- Calm emotional state — your regulation influences theirs
- Tracking sheet or GPT-OS® app ready
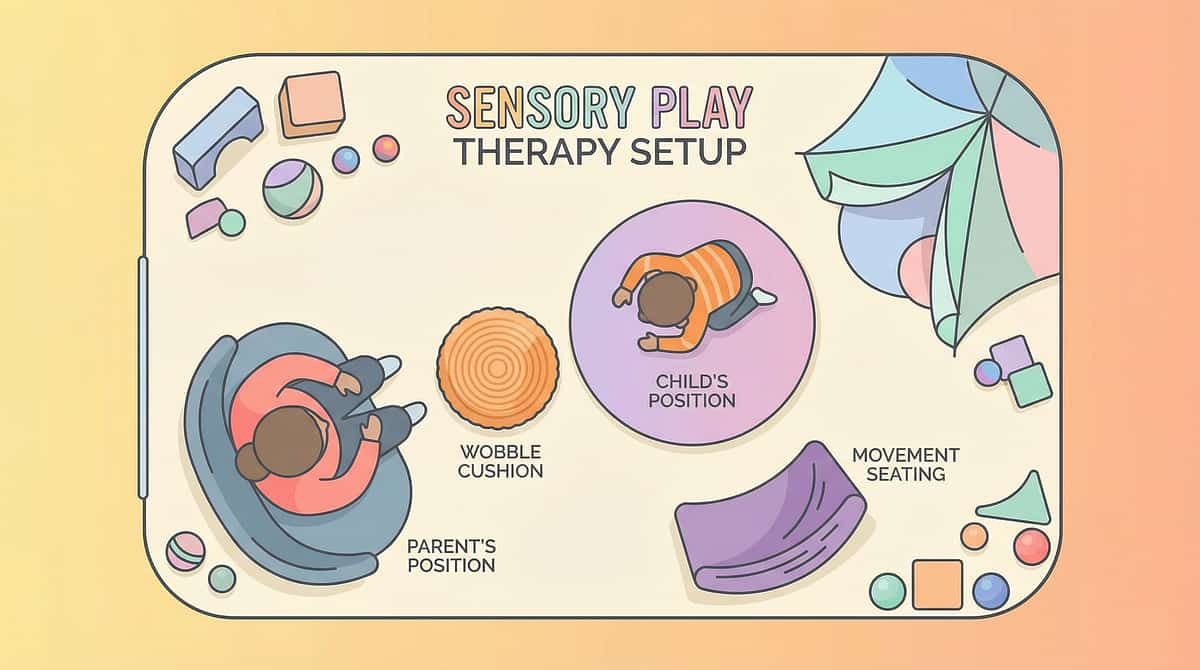
Space Layout Principle
- Crash pad zone: 3m × 2m clear soft surface
- Visual corner: light panel or calming projector
- Child seated on wobble cushion or standing at activity
- Sensory bin within arm's reach to one side
- Material tray: all tools within reach
- Clear exit/transition pathway visible
"Environment is the third therapist. A well-prepared sensory space removes 80% of session failures before they begin."
60-Second Readiness Assessment — Before Every Session
Run this quick check before every session. The best session is one that starts right. A session started when the child isn't ready produces negative associations that take days to undo.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Arousal state | Calm-alert | Slightly under/over | Meltdown/shutdown | |
Last meal | 30+ min ago | 15–30 min ago | Just finished | |
Sleep last night | Typical | Slightly short | Very disrupted | |
Recent stressor | None | Mild event | Major transition | |
Physical health | Well | Slightly tired | Fever/pain/illness | |
Response to you | Engaging | Neutral | Actively avoiding |
All ✅ → Full Session
Proceed with standard 20-minute protocol using all planned materials.
1–2 ⚠️ → Modified Session
10 minutes only. Use only the child's most preferred sensory tool. No new tools today. Follow child's lead entirely.
Any 🛑 → Postpone
"Today we're going to rest. Let's do [calming activity]. We'll try our sensory tools tomorrow."
Step 1 of 6
Invite, Never Command
"Hey, I've got something I want to show you. Look what I found... I wonder what this does... want to try it with me?"
You are pairing yourself with the sensory tool before any demand is placed. The child must associate YOU and the TOOL with positive experience before any therapeutic use begins. This is ABA's pairing procedure applied to sensory substitution. Present the material with curiosity, not instruction.
Body Language
- Get on the child's level (sit or kneel)
- Face slightly away — non-threatening approach
- Use a calm, curious voice — not performative excitement
- Have the tool visible but not pressing it toward the child
Cues to Watch
✅ Acceptance Cues (proceed to Step 2):
- Child reaches toward the tool
- Child makes eye contact with the tool or you
- Child's body posture relaxes or orients toward you
🛑 Resistance Cues (stay at Step 1 longer):
- Child moves away or pushes tool away
- Child cries, screams, or goes rigid
- → Put the tool nearby, continue a preferred activity, let child approach on their own timeline

Step 2 of 6
Introduce the Material — Let the Brain Experience It
"This is your chewing necklace. It's yours. You can use it whenever you need it."
Chewable Jewelry
Place around child's neck or in their hand. Say: "When you feel like chewing, this is the safe thing to chew." Do not force into mouth.
Weighted Lap Pad
Place on your own lap first, then offer to child's lap. Say: "This is your heavy blanket. See how heavy? It feels good."
Wobble Cushion
Place on chair, sit on it yourself first, make it look fun. Child sits naturally when ready.
Fidget Tool
Give to child's hands with no instruction. Let them explore. Name what they're doing: "You're squeezing it! That feels good."
Crash Pad
Jump or fall on it yourself first with big positive affect. Make it the most appealing object in the room.
When child touches or engages with the tool — deliver immediate, specific, warm praise: "Yes! You're using your chew necklace!" Timing window: 1–3 minutes at this stage.

Step 3 of 6
The Core Substitution — Brain Meets Better Pathway
When the child demonstrates their typical seeking behavior, redirect them — calmly, without frustration — to the appropriate alternative tool. This is the moment of substitution.
Seeking Behavior | Redirect Script | Alternative Tool | |
Chewing shirt/pencil | "Shirt is not for chewing. Here is your necklace." | Chewable jewelry | |
Crashing into couch/wall | "Let's crash HERE." [guide to crash pad] | Crash pad + heavy work | |
Can't sit still, rocking | "Here's your moving cushion — you can move while you sit." | Wobble cushion | |
Constant touching/picking | "Hands need something to do — here." | Fidget tool | |
Spinning dangerously | "Spinning time — on the spin seat." | Therapy swing | |
Humming/vocalizing | "Let's put on your music." | Noise-canceling headphones | |
Hands in mouth | "Hands in the bin." | Sensory bin |
Match the sensory system
Redirect chewing to oral tools, not fidgets. The match must be neurologically precise.
Match the intensity
Aggressive chewers need firm chewables. Soft ones don't satisfy the neurological need.
No emotional loading
Redirect matter-of-factly, without frustration or shame. Calm redirects work. Emotional ones don't.
Immediate reinforcement
When child uses the alternative, celebrate immediately — within 3 seconds.

Step 4 of 6
Build the New Neural Habit — Consistency Creates Pathways
The alternative sensory tool only becomes the child's preferred pathway through repeated, reinforced exposure over days and weeks. Each successful redirect creates a slight strengthening of the "appropriate alternative" neural pathway. This accumulates.
Week | Frequency | Expected Child Response | |
Weeks 1–2 | Redirect every time seeking behavior occurs | Compliance with prompting; may revert quickly | |
Weeks 3–4 | Child begins reaching for alternative before seeking escalates | Beginning of self-initiation | |
Weeks 5–8 | Child independently accesses alternative when sensing input need | Independence emerging |
Variation Options (maintain engagement)
Chewables
Rotate firmness levels, shapes, and flavors (if applicable) weekly.
Weighted Items
Vary weight slightly; alternate lap pad / vest / blanket across days.
Fidgets
Rotate 3–4 different textures and resistances weekly.
Sensory Bins
Change fill material weekly: rice → beans → kinetic sand → water beads.
"3 successful redirects with genuine alternative use > 10 prompted uses where the child is merely complying. Quality of sensory input matters more than quantity."

Step 5 of 6
Celebrate Every Correct Choice — Timing Is Everything
Within 3 seconds of the child choosing the appropriate alternative — deliver reinforcement. The brain's reward circuit requires temporal proximity between behavior and consequence to form associations. Three seconds is the window.
Reinforcement Scripts (vary to prevent habituation)
- "YES! You used your necklace! That's exactly right!"
- "I saw you go to your crash pad — I'm so proud of you."
- "Look at you! You knew what your body needed and you got it."
- "That's it! Your body needed chewing and you used the right thing."
Reinforce the Attempt, Not Just Success
When a child reaches for their chewable instead of their shirt — even if they touch the shirt first — reinforce: "You remembered your necklace!"
Reinforcement Menu
- Verbal praise (specific to the behavior)
- Physical affection (if child accepts — brief, celebratory)
- Access to preferred activity for 2–3 minutes
- Token/sticker toward a reward chart
- First-Then visual: "First sensory tool, then [preferred activity]"
Graduated Reinforcement
As the child uses the alternative consistently, gradually shift from every-correct-choice reinforcement toward intermittent reinforcement — which actually maintains behavior more durably (ABA variable ratio schedule).
Step 6 of 6
Close the Session — Transitions Are Therapeutic Events
"We have two more [crashes/chews/wiggles], then we're going to put the tools away."
Use a visual timer countdown starting 2–3 minutes before the end. Allow one final complete use of the primary sensory tool. Have the child participate in putting tools away — this develops ownership and respect for the tools. Bridge with: "We'll get your [chew necklace / fidget / wobble cushion] back out next time."
If child resists ending: Avoid power struggles — stay calm and matter-of-fact. Add one more brief use, then transition. Never abruptly remove access to a sensory tool without transition — this creates negative associations that undo progress. Use "first-then" language: "First we put this away, then we do [preferred activity]."
60 Seconds of Data Now = Months of Therapeutic Intelligence
Behavior Frequency
How many times did the seeking behavior occur today (total)?
- 0–2 times
- 3–5 times
- 6–10 times
- 10+ times
Alternative Use Rate
When seeking behavior occurred, did child use the alternative?
- Never (0%)
- Sometimes (25–50%)
- Often (50–75%)
- Almost always (75%+)
Session Response
Child's overall response to sensory alternative tools today:
- Refused / distressed
- Tolerated
- Accepted willingly
- Sought out independently
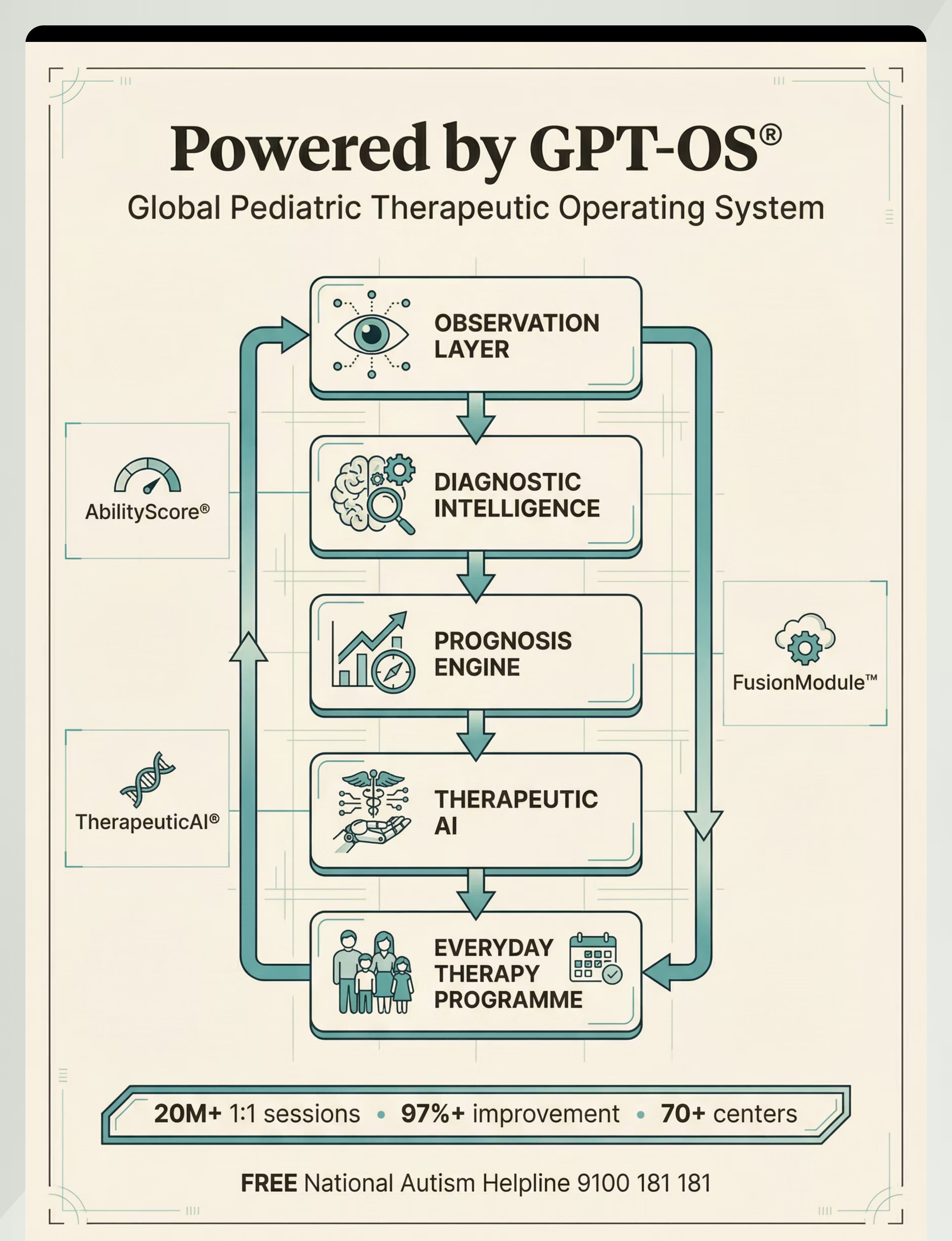
Your daily data points feed directly into GPT-OS® TherapeuticAI®, which tracks behavior reduction trends across weeks, alerts your therapist when alternative use rate crosses 50% (the consolidation milestone), generates AbilityScore® delta for the Sensory Regulation Readiness Index, and adjusts the EverydayTherapyProgramme™ based on your child's specific response.
Every Imperfect Session Is Data. Not Failure.
"My child refused the alternative completely."
What happened: The alternative hasn't been paired with enough positive experience yet. The tool is new; the brain prefers known pathways, even inefficient ones.
Next time: Increase the pairing phase (Step 1). Make the tool available during preferred activities with NO therapeutic demands. Let the child observe you using it.
Next time: Increase the pairing phase (Step 1). Make the tool available during preferred activities with NO therapeutic demands. Let the child observe you using it.
"My child used the alternative once, then went back to the seeking behavior."
What happened: This is a success. Once is a start. The alternative pathway is new and weak; the original pathway is deeply worn.
Next time: Celebrate that one use extravagantly. Lower expectations to "one successful redirect per session" for weeks 1–2.
Next time: Celebrate that one use extravagantly. Lower expectations to "one successful redirect per session" for weeks 1–2.
"My child threw or destroyed the sensory tool."
What happened: The child was likely over-aroused, or the tool provided the wrong type of input.
Next time: Check readiness first. Consider whether the tool matches the sensory need. Try a different material from the 9.
Next time: Check readiness first. Consider whether the tool matches the sensory need. Try a different material from the 9.
"The behavior seems worse since we started."
Why this sometimes happens: Extinction burst — when seeking behavior is redirected, intensity temporarily increases. This is a sign the intervention is working. Stay consistent. This phase typically passes in 3–7 days. Call 9100 181 181 if concerned.
"My child uses the alternative at home but not at school."
What happened: Generalization hasn't occurred yet — this is normal.
Next time: Request a school meeting. Send a spare set of tools to school. Brief the teacher using the Family Guide. Your Pinnacle OT can write a formal school letter.
Next time: Request a school meeting. Send a spare set of tools to school. Brief the teacher using the Family Guide. Your Pinnacle OT can write a formal school letter.
📞9100 181 181 — Troubleshooting support available 24×7 in 16 languages

No Two Nervous Systems Are Identical — Personalize Relentlessly
Child Profile | Adaptation | |
High-intensity seeker (crashes hard, chews aggressively) | Provide more intense alternatives — firm chewables, heavy crash pads, resistive fidgets | |
Low-intensity seeker (subtle seeking, gentle mouthing) | Softer alternatives — light chewable, standard fidget, slight wobble cushion | |
Sensory avoider (overwhelmed by input) | Reduce intensity of environment first; offer tools as escape, not input | |
Mixed seeker/avoider (seeks some inputs, avoids others) | Map each sensory system individually — use OT assessment |
Age Modifications
Ages 2–4
Focus on 1–2 tools only. Make all alternatives playful and parent-led. Expect 60% parent-directed use.
Ages 5–8
Introduce self-monitoring language: "What does your body need right now?" 2–4 tools. School integration is critical.
Ages 9–12
Self-selection from a personal sensory toolkit. Independent use in public. Social dignity is prioritized in tool selection.
Your session data (Step 6: Data Capture) automatically informs GPT-OS® TherapeuticAI® which modifications are needed. The EverydayTherapyProgramme™ updates weekly based on your child's specific response trajectory.

Weeks 1–2: Tolerance Is Progress. Don't Miss It.
Progress Arc
~15% of Journey
15%
Progress Milestone
Weeks 1–2 progress level. Tolerance and pairing are the primary goals at this stage.
✅ What You WILL Likely See
- Child tolerates sensory tool being in the space without distress
- Child occasionally uses alternative when heavily prompted
- Seeking behavior frequency unchanged or slightly increased (extinction burst — this is normal and expected)
- Parent becomes more confident identifying when seeking behavior is starting
⚠️ What You Will NOT See Yet (and That's OK)
- Independent tool use without prompting
- Significant reduction in seeking behavior frequency
- Generalization to school or other environments
- Child self-identifying their sensory needs
The Milestone Parents Miss
If your child chews their shirt 8 times today vs. 10 times last week — that is measurable progress. If they tolerated the chew necklace being around their neck for 5 minutes — that is neural pathway formation. Track these micro-progresses in your GPT-OS® data.
"If your child tolerates the sensory tool for 3 seconds longer this week than last week — that is real neurological progress. Celebrate it."

Weeks 3–4: The Brain Is Forming New Habits — Watch Carefully
Progress Arc
~40% of Journey
40%
Consolidation Phase
Alternative use rate should be crossing from below 25% toward 25–50% in your GPT-OS® tracker.
🧠 Neural Pathway Signals
- Child reaches for sensory tool BEFORE the seeking behavior escalates
- Child begins bringing their sensory tool to different spaces in the home
- Parent reports "they just picked it up on their own" — this is the consolidation moment
- Seeking behavior intensity is decreasing, even if frequency is unchanged
🌱 Generalization Seeds (encourage these)
- Child uses fidget at mealtime (new context from original)
- Child asks for weighted lap pad when doing homework (self-identified need)
- Child uses chewable in the car without prompting
📊 When to Intensify
When alternative use rate exceeds 50% over 5 consecutive sessions, or child independently seeks the alternative 2+ times per day — signal to your Pinnacle OT: time to add a second sensory tool.
"You may notice you're more confident too. You're reading your child's sensory signals earlier, redirecting before escalation, and feeling less like you're fighting a losing battle. That's your parallel neurological adaptation — parent learning is real."
Weeks 5–8: Mastery Is When the Child Owns Their Sensory Strategy
Progress Arc
~75% of Journey
75%
Mastery Phase
Child is independently selecting and using sensory alternatives in familiar environments.
🏅 Mastery Indicator 1 — Tool Independence
Child independently selects and uses sensory alternative in familiar environments without prompting, at least 75% of incidents of seeking behavior.
🏅 Mastery Indicator 2 — Self-Identification
Child can communicate or signal their sensory need before behavior escalates: points to tool, verbalizes "I need my necklace," or independently retrieves their kit.
🏅 Mastery Indicator 3 — Generalization
Alternative use is observed in at least two different environments (home + school, or home + grandparent's house).
🏅 Mastery Indicator 4 — Maintenance
Seeking behavior frequency is measured at less than 50% of baseline after 3 consecutive weeks.
If not at mastery by Week 8: This is not a failure. Complex sensory profiles, comorbidities, or inconsistent implementation across caregivers may extend the timeline. Call 9100 181 181 for a consultation. The GPT-OS® mastery unlock automatically generates the next technique recommendation when criteria are met.

You Did This. Your Child Grew Because of Your Commitment.
"Five to eight weeks ago, your child chewed their shirts, crashed into walls, and couldn't sit still — and you had no tools. You learned the science. You prepared the space. You stayed consistent through the extinction burst. You redirected a hundred times without giving up. And now your child reaches for their sensory tool. That is you. That is your work. That is your child's new neural pathway — built by your hands." — Pinnacle Blooms Consortium
✅ What Your Child Achieved
- Learned to meet a neurobiological need through a safe pathway
- Developed awareness of their own sensory system
- Built a skill that will serve them for life — in classrooms, workplaces, and relationships
🎉 Family Celebration Ideas
- Create a "sensory warrior" certificate for your child
- Take a photo of your child calmly using their sensory tool
- Write a one-paragraph journal entry about this journey
- Share your story (anonymously if preferred) with the Pinnacle community

Even in Progress — Know When to Pause and Seek Professional Guidance
🚨 Behavioral Red Flags — Call 9100 181 181
- Seeking behavior is escalating in intensity (not just frequency) over 2+ consecutive weeks
- New self-injurious behaviors emerging that were not present before
- Child is using sensory tools compulsively — cannot be separated from them without severe distress
- New sensory avoidances emerging alongside the seeking (mixed profile shift)
🚨 Physical Red Flags — Call 9100 181 181
- Chewable jewelry is being bitten through repeatedly — risk of material fragment ingestion
- Signs of injury from crashing: bruising, limping, wincing on movement
- Vestibular equipment use resulting in vomiting, headache, or extreme pallor
- Weight items leaving pressure marks or child refusing to have them removed
🚨 Emotional/Relational Red Flags — Call 9100 181 181
- Parent exhaustion and inconsistency increasing rather than decreasing at week 4+
- Family conflict around sensory accommodations escalating
- Child's anxiety increasing even as sensory behavior is redirected
"If something feels wrong — even if you can't name it — pause and ask. Your instinct as a parent is clinical data." — Pinnacle Blooms Consortium
You Are Here on the Sensory Regulation Map — Here's What Comes Next
D-368
Sensory Processing Patterns — Prerequisite baseline assessment
D-369
Sensory Diet Basics — Foundational structured dietary approach
D-370 ← YOU ARE HERE
Alternative Sensory Input — The 9 materials and substitution approach
D-371
Sensory Overwhelm Management — Next technique in the progression
D-372
Sensory Breaks Protocol — Structured regulation breaks
D-375
Self-Regulation Challenges — Advanced independent self-management
This technique simultaneously supports: Domain A (Sensory Processing) | Domain C (Emotional Regulation) | Domain E (Executive Function — attention component) | Domain J (Daily Living — independence). The long-term developmental goal is independent self-monitoring and self-management of sensory needs across all environments, supporting classroom participation, social inclusion, and adaptive functioning in adulthood.

These Families Started Exactly Where You Are
Family Vignette 1 — Hyderabad
Before (Week 0): "Our 5-year-old son chewed through 3 school shirts every week. His teachers were calling. We'd spent months saying 'stop chewing' — it never worked once. I felt like a failure."
After (Week 8): "He wears his chew necklace to school every day now. His teacher told us last week that he reaches for it on his own before getting dysregulated. The chewing still happens — but on the necklace, not the shirt. He's calmer. He can focus. We cried when we saw his first clean shirt come home from school."
"We didn't stop his need to chew. We gave his brain a better answer. That was everything."
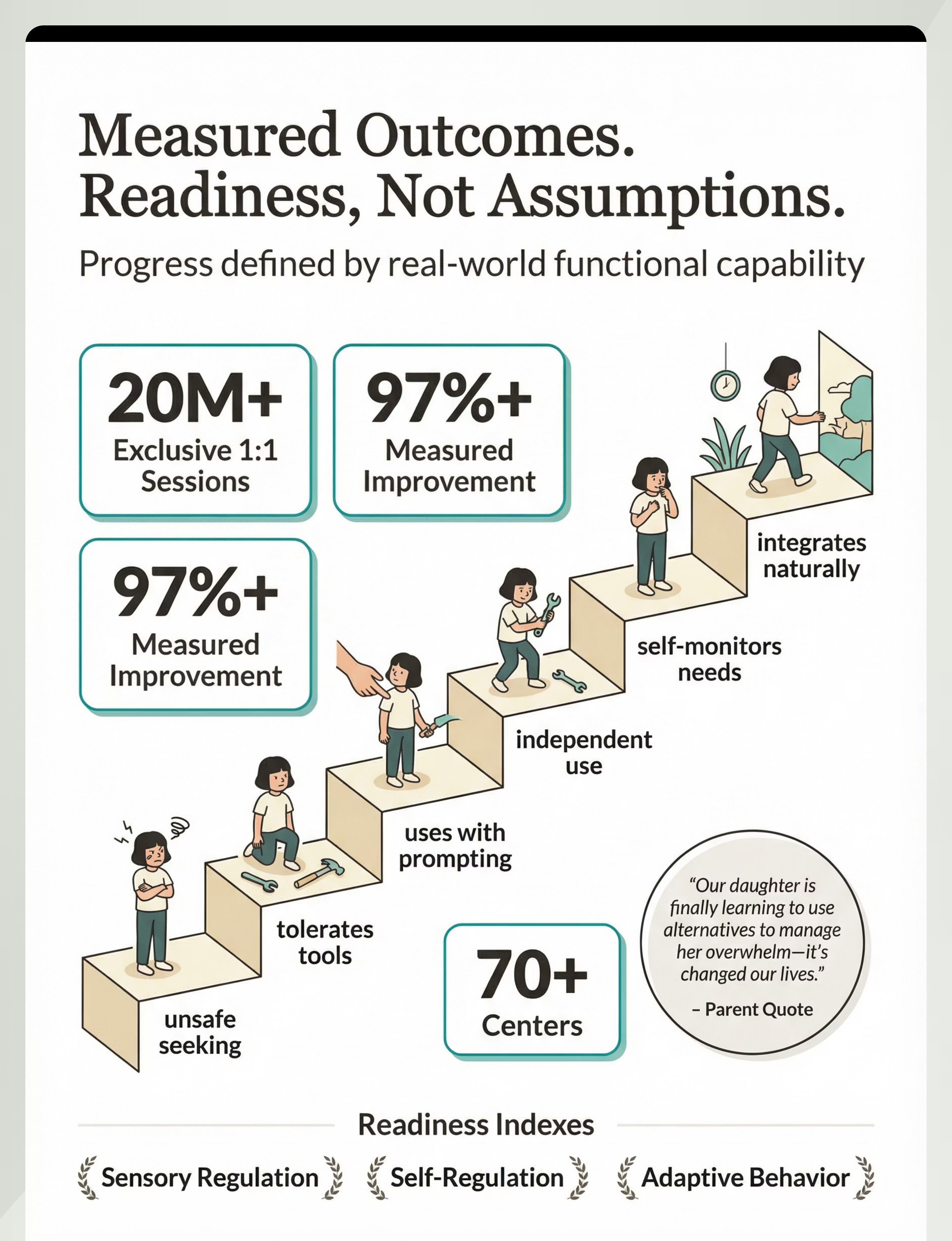
The child's Sensory Regulation Readiness Index moved from Level 1 (unsafe seeking) to Level 4 (independent tool use) across 9 weeks. Parent consistency was the primary determinant of outcome.
Family Vignette 2 — Bengaluru
Before (Week 0): "Our 7-year-old daughter crashed into everything. Walls, furniture, people. We couldn't take her anywhere. She fell down constantly — not by accident. She was seeking the impact. We had no idea that was what she was doing."
After (Week 10): "She has a crash pad in her room now. Before we go out, she gets '5 crash pad crashes' as part of her routine. She's regulated for 2 hours after that. We take her everywhere. She's in a mainstream classroom. She still needs the input — but now she knows where to get it."
"The crash pad didn't fix her. It gave her an answer. Now she can manage the world."
Heavy work + crash pad combination reduced unsafe impact-seeking by 78% across 10 weeks. Proactive sensory diet scheduling — input provided BEFORE high-demand situations — was critical.
Vignettes are illustrative narratives based on aggregate clinical patterns. Individual results vary. Statistics represent outcomes across the Pinnacle Network.

You Are Not Navigating This Alone — Join 70,000+ Families
WhatsApp Support Group
Sensory Seeking & Alternatives — challenge-specific parent group moderated by Pinnacle OTs. Available in Hindi, Telugu, Tamil, Kannada, Marathi, Bengali, English + 10 more languages.
Online Community Forum
pinnacleblooms.org/community — parent Q&A, technique sharing, material recommendations, and progress celebrations from families across 70+ countries.
Local Parent Meetups
Your nearest Pinnacle center hosts monthly parent meetups organized by challenge area. Find sensory regulation meetups near you at pinnacleblooms.org.
Peer Mentoring Program
Connect with a parent who has already completed this technique journey. Request a mentor at pinnacleblooms.org. Your journey helps other families — consider sharing when you're ready.
WHO evidence confirms: parent support networks improve intervention outcomes, reduce parental isolation, and increase implementation consistency. You are more likely to maintain the approach for 6+ weeks if you are connected to community. 📞9100 181 181 | care@pinnacleblooms.org
Preview of 9 materials that help with alternative sensory input Therapy Material
Below is a visual preview of 9 materials that help with alternative sensory input therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Home + Clinic = Maximum Impact
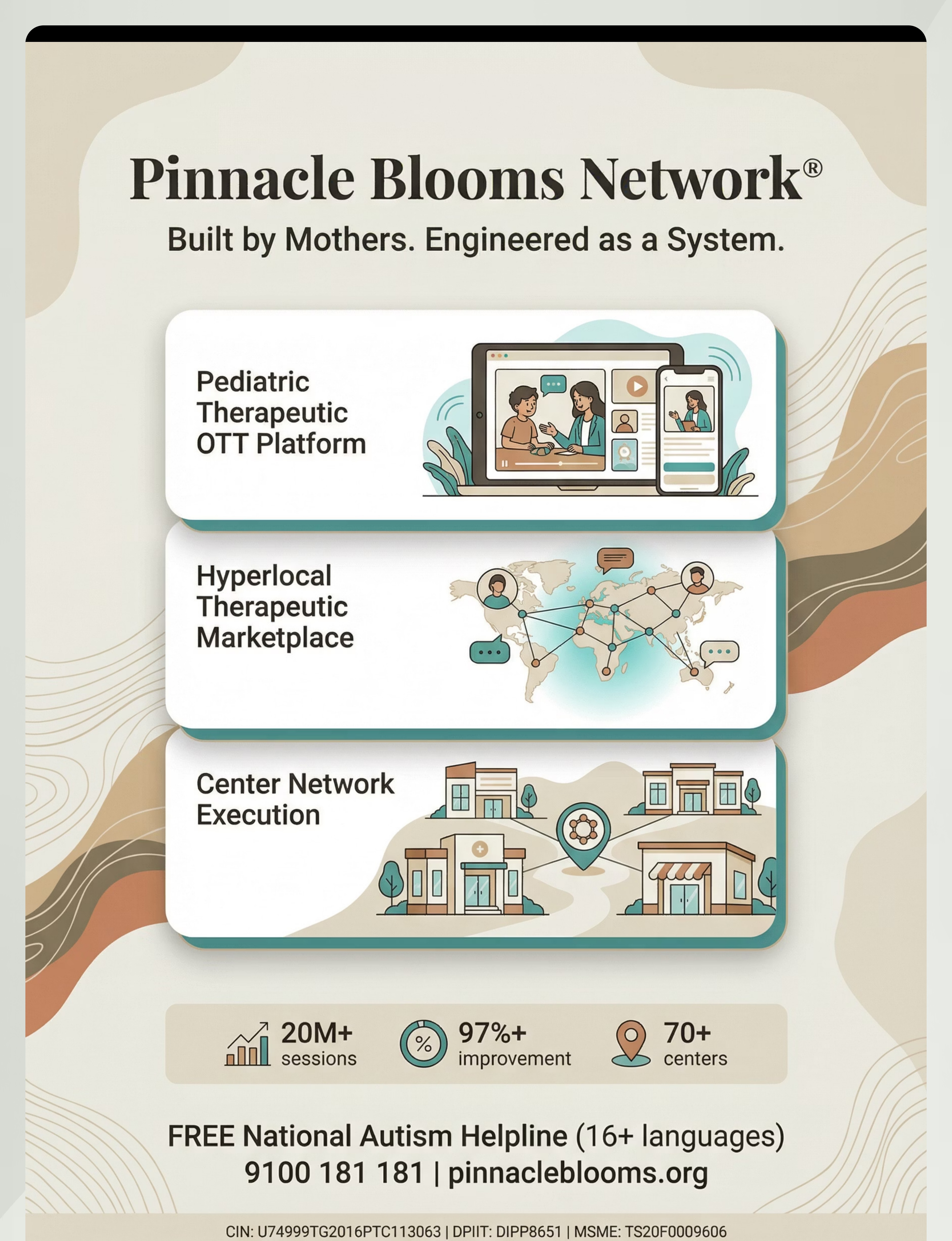
📍 70+ Pinnacle Centers Across India
Every center operates under GPT-OS® clinical standards. Every OT is trained in sensory integration and alternative sensory input protocols.
🔵 OT Specialization
Comprehensive Sensory Profile Assessment | Sensory Integration Therapy | Individualized Sensory Diet Design
🟢 ABA Specialization
Functional Behavior Assessment | Data-driven alternative use training | School behavior support
🟡 SLP Specialization
Oral motor assessment | Oral sensory seeking specific intervention | Feeding/mouthing differentiation
🆓 FREE Assessment Path
- Call 9100 181 181 — FREE National Autism Helpline
- Schedule FREE initial consultation
- AbilityScore® Assessment + Sensory Processing Evaluation
- Personalized GPT-OS® therapy plan
📱 Teleconsultation — Available Everywhere
Can't reach a center? Pinnacle OTs provide teleconsultation across 70+ countries in 16 languages. Professional OT assessment identifies your child's specific sensory profile (hyper/hypo-responsive by system), selects the precise tools needed, designs an individualized sensory diet, and monitors progress with clinical precision.
Home implementation is the delivery system. Professional guidance is the design system.
Your Child's Brain Is Seeking.
You Now Know How to Answer.
This content is educational and does not replace individualized assessment by licensed occupational therapists, behavior analysts, or developmental specialists. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Pinnacle Blooms Consortium™
OT • ABA • SLP • SpEd • NeuroDev
WHO/UNICEF Aligned | NCAEP 2020