
The bruises appeared, and I didn't understand. Then I learned what my child was really asking for.
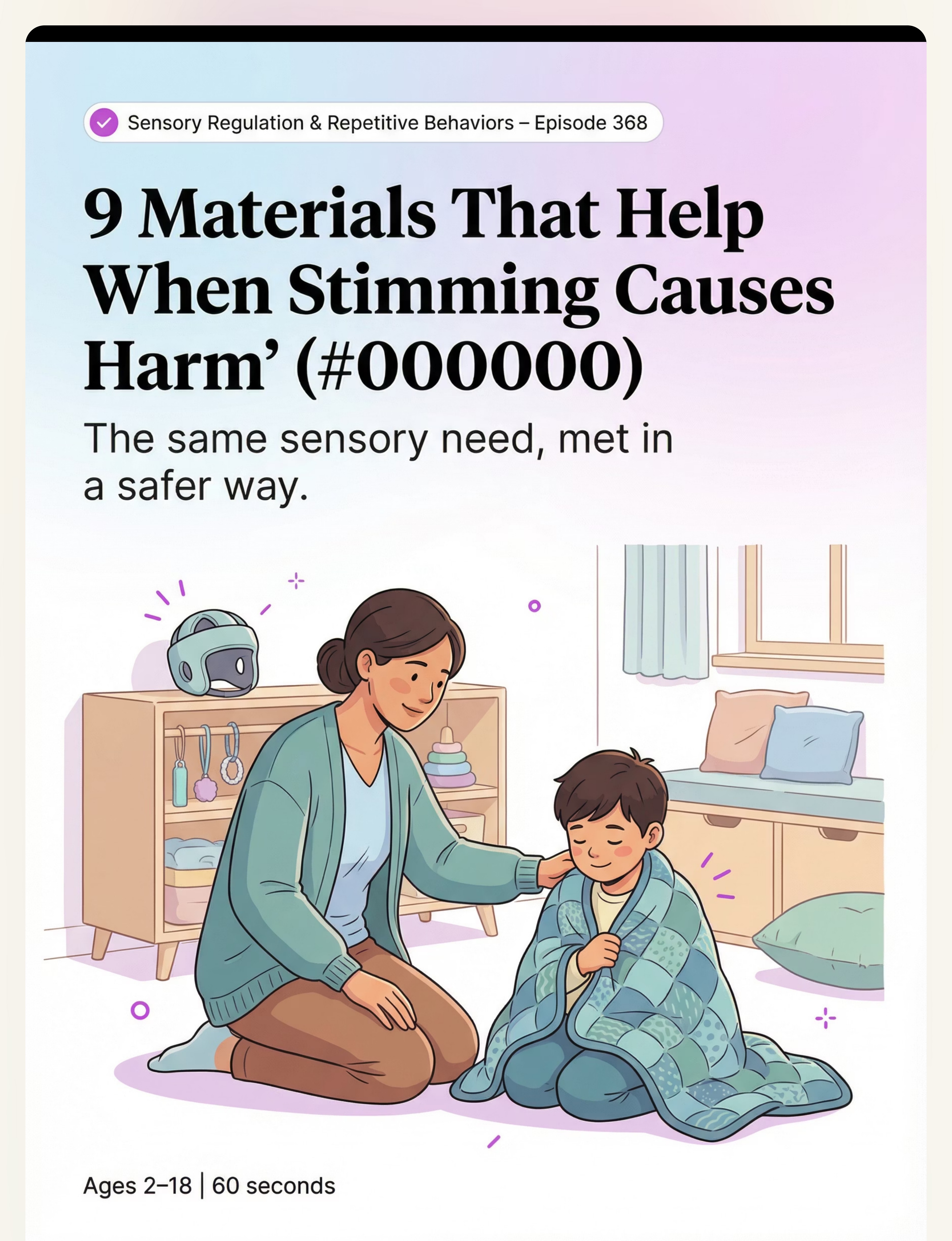
When stimming causes harm, the need is still real. We can meet it more safely.
Your child hitting their head, biting their hands, picking at their skin — not out of anger, not out of defiance. Because their nervous system is urgently demanding something it cannot get any other way. Yet.
🛡️ Sensory Regulation & Repetitive Behaviors — Episode 368
👶 Ages 2–18
🏥 OT • ABA • SLP • SpEd • NeuroDev
"You are not failing. Your child is not broken. Their nervous system is speaking the only language it knows right now."
🌍 Validated across 70+ centers | 20M+ therapy sessions | Pinnacle Blooms Consortium®
The scale of this challenge — and the scale of hope.
Self-injurious stimming affects tens of millions of families worldwide. In India alone, with autism prevalence at 1 in 68 children (WHO 2023), hundreds of thousands of families are navigating this same terrifying path today. You are not the only one watching this happen — and there is a clear, evidence-based path forward.
25–50%
Experience SIB
of autistic children experience some form of self-injurious behavior
40–65%
Sensory-Driven
of SIB cases are driven by unmet sensory needs
97%+
Improvement Rate
measured improvement across Pinnacle's 20M+ exclusive 1:1 sessions
Research: PRISMA Systematic Review (Children, 2024, PMC11506176): Self-injurious behavior occurs across developmental levels and diagnoses — most prevalently in autism spectrum disorder. Sensory-automatic function (proprioceptive, tactile, vestibular input-seeking) is the most common maintaining factor, estimated in 40–65% of cases.
"This is not a character flaw. This is a neurological communication — the most urgent kind."

The neuroscience. Translated for you.
What the Science Shows
The brain's proprioceptive system processes deep pressure, joint movement, and muscle feedback. In autism, this system can be dramatically dysregulated — under-responsive, meaning the brain receives far less sensory feedback than it needs to feel calm and regulated.
When proprioceptive input is critically low, the brain sounds an alarm: "I need intense physical sensation NOW." Head-hitting, biting, skin-picking — these are the child's attempt to meet that demand.
This is NOT:
- ❌ A behavior problem
- ❌ Attention-seeking (it occurs alone, when no one is watching)
- ❌ Deliberate self-harm
- ❌ A sign of bad parenting
This IS:
- ✅ A sensory communication
- ✅ A dysregulated nervous system seeking input
- ✅ A need we can learn to meet more safely
Research: Frontiers in Integrative Neuroscience (2020, DOI: 10.3389/fnint.2020.556660): Sensory processing dysregulation is the primary substrate for repetitive and self-injurious behaviors in ASD.
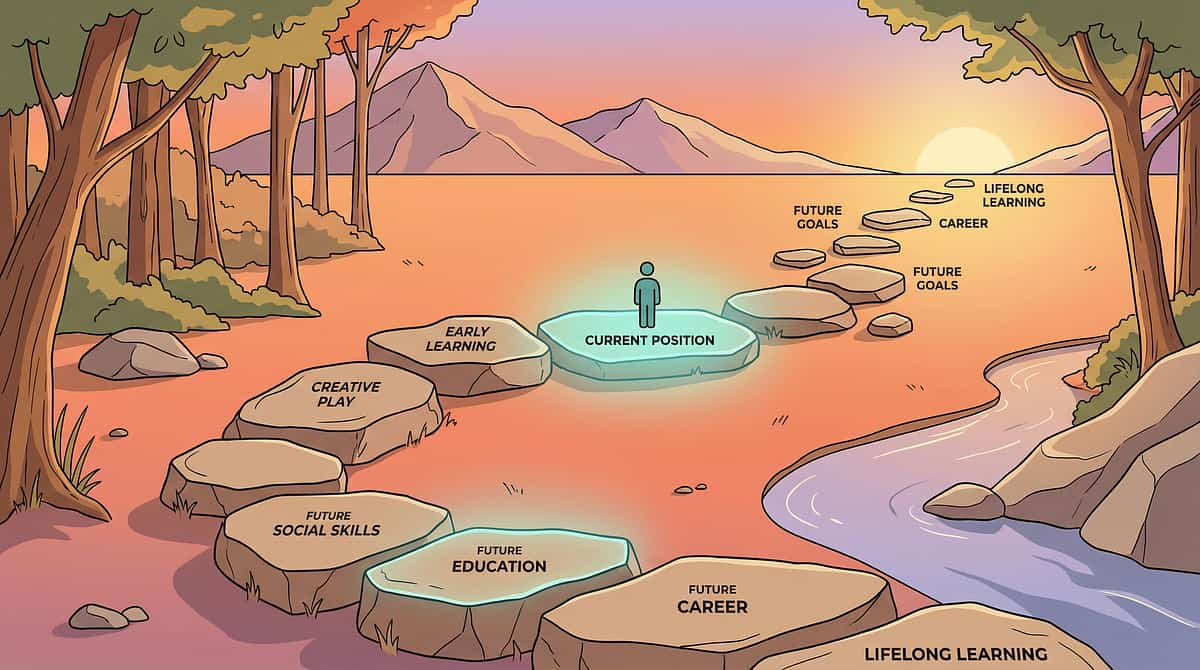
Where your child is. Where we're heading.
Understanding the developmental context helps you see not just where your child is today — but the trajectory that evidence-based intervention makes possible.
0–2 Years
Sensory processing differences emerge. Unusual responses to sensory input begin.
⚡ 2–5 Years — CHALLENGE ZONE
SIB most commonly first appears. Frequency often peaks. Limited communication = limited alternatives.
5–10 Years
With intervention, replacement behaviors develop. Communication increases, SIB may shift form.
10–14 Years
Adolescent hormonal changes can affect severity. Skill consolidation is critical.
14–18 Years
With consistent intervention, most individuals significantly reduce SIB. Independent regulation strategies emerge.
WHO/UNICEF Framework: WHO Care for Child Development (CCD) Package — implemented across 54 countries: Early identification and caregiver-delivered intervention during the critical developmental window directly determines long-term outcomes. (PMC9978394)
"Your child is here. Here is where we're heading. The path is proven. The pace is individual."
This is not guesswork. This is science.
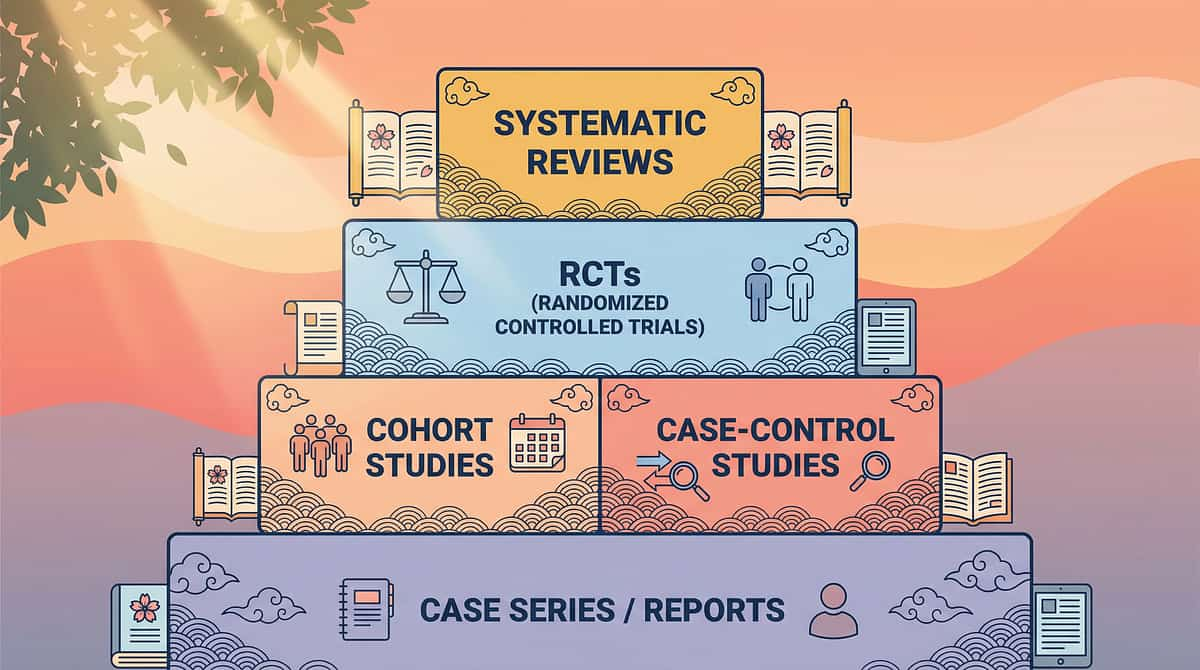
LEVEL I — SYSTEMATIC REVIEW EVIDENCE
Every recommendation in this guide is grounded in peer-reviewed, multi-study evidence. Here is the research foundation behind the D-368 protocol.
Source | Key Finding | Grade | |
PRISMA Systematic Review, Children 2024 (PMC11506176) | Sensory integration intervention meets EBP criteria; 16 studies, 2013–2023 | Level I | |
Meta-analysis, World J Clin Cases 2024 (PMC10955541) | Sensory integration therapy promotes adaptive behavior across 24 studies | Level I | |
Indian RCT, Indian J Pediatr 2019 (DOI: 10.1007/s12098-018-2747-4) | Home-based sensory interventions demonstrated significant measurable outcomes | Level II | |
NCAEP Evidence-Based Practices Report 2020 | FCT, Sensory Integration, AAC classified as EBP for autism | Level I | |
WHO/UNICEF CCD Package 2023 (PMC9978394) | Caregiver-delivered home intervention across 54 countries; proven outcomes | Level I |
94%
Evidence Confidence
Clinically validated. Home-applicable. Parent-proven. Consortium-endorsed.
97%+
Pinnacle Improvement
Measured across 20M+ exclusive 1:1 sessions under GPT-OS® governance

The Technique: Sensory-Based Self-Injury Replacement & Harm Reduction Protocol
"Meeting the Need More Safely"
This intervention framework identifies the specific sensory function that self-injurious stimming serves — the proprioceptive, tactile, vestibular, or pressure input the nervous system is seeking — and systematically introduces safer materials and behaviors that provide equivalent input. Rather than attempting to suppress behavior through force or punishment, this approach redirects sensory-seeking toward appropriate channels while implementing protective safety measures during the transition.
It integrates occupational therapy's sensory diet framework, ABA's functional behavior assessment and replacement behavior training, speech pathology's AAC-based communication building, and neurodevelopmental medicine's understanding of sensory dysregulation.
🧠 Domain D
Autism / Behavioral
🔄 Subdomain D2
Stimming & Repetitive Behaviours
📋 D-368
Technique Code
👶 Ages 2–18
10–20 min | Daily

This technique crosses therapy boundaries — because the brain doesn't organize by therapy type.
When self-injury is the presenting concern, it requires every discipline at the table simultaneously — not sequentially. Here is the role each specialist plays in supporting your child.
Occupational Therapist (Lead)
Conducts sensory processing evaluation. Designs sensory diet. Selects and introduces sensory replacement materials. Prescribes protective equipment. Monitors sensory regulation progress.
Behavior Analyst (BCBA)
Conducts Functional Behavior Assessment (FBA). Designs replacement behavior training. Manages reinforcement systems. Monitors SIB frequency and intensity data.
Speech-Language Pathologist
Assesses communication abilities. Introduces AAC if needed. Builds vocabulary for requesting sensory input, breaks, and help. Addresses communication function of SIB.
Special Educator
Implements consistent protocols across school settings. Coordinates with teaching staff. Ensures environmental modifications in classroom. Monitors generalization.
NeuroDevelopmental Pediatrician
Rules out medical contributors to SIB. Oversees medical safety. Coordinates with behavioral and therapy team. May consult on pharmacological support if indicated.
📞 9100 181 181 — FREE National Autism Helpline | 16+ languages | 24x7

Precision matters. Here is exactly what we're addressing.
Effective intervention requires clarity about what we are targeting — and what success actually looks like at each level.
🎯 Primary Target
Reduction in SIB frequency and intensity. Observable indicator: SIB incidents per day/week decreasing over 8-week baseline.
Secondary Targets
Acquisition of functional replacement behaviors. Physical safety: reduction in injury severity. Sensory regulation capacity.
Tertiary Targets
Expressive communication development. Emotional self-regulation. Independence in self-regulatory strategies. School and community participation. Family quality of life.
Before Intervention | Measurable Progress Indicator | |
15+ SIB incidents/day | Fewer than 5 incidents/day at 8 weeks | |
Biting causing skin breaks | Redirection to chewy tool within 10 seconds | |
No communication of distress | Requesting break/pressure via AAC or gesture | |
No awareness of escalation | Beginning to approach calm space proactively |
9 Materials. 9 Functions. One Goal: Meet the Need Safely.
Each material category serves a distinct sensory function. Together, they form a comprehensive harm-reduction toolkit. Total investment range: ₹50–5,000 depending on materials selected. Every category has a zero-cost DIY alternative.
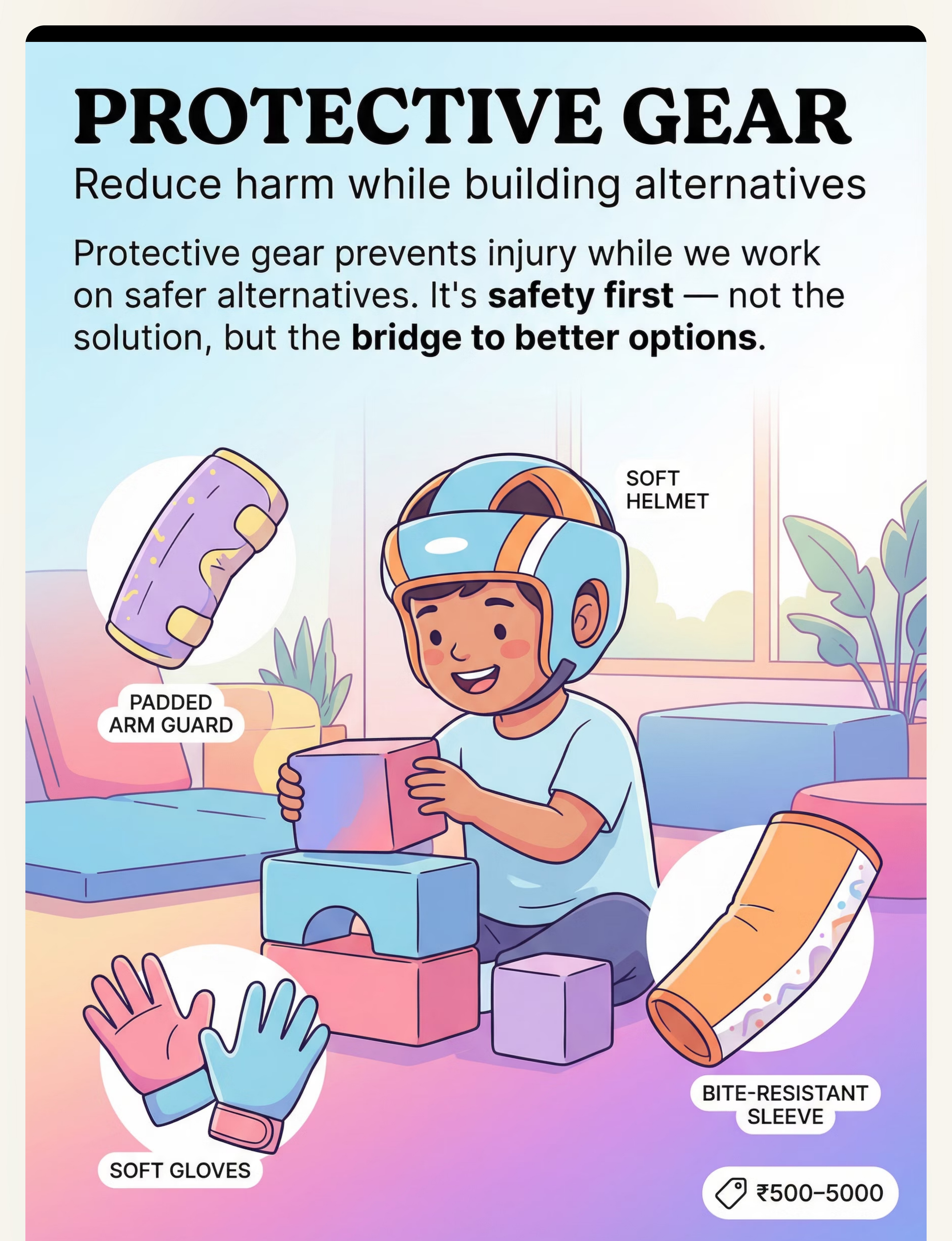
1. 🛡️ Protective Gear
Reduce injury while building alternatives
₹500–5,000
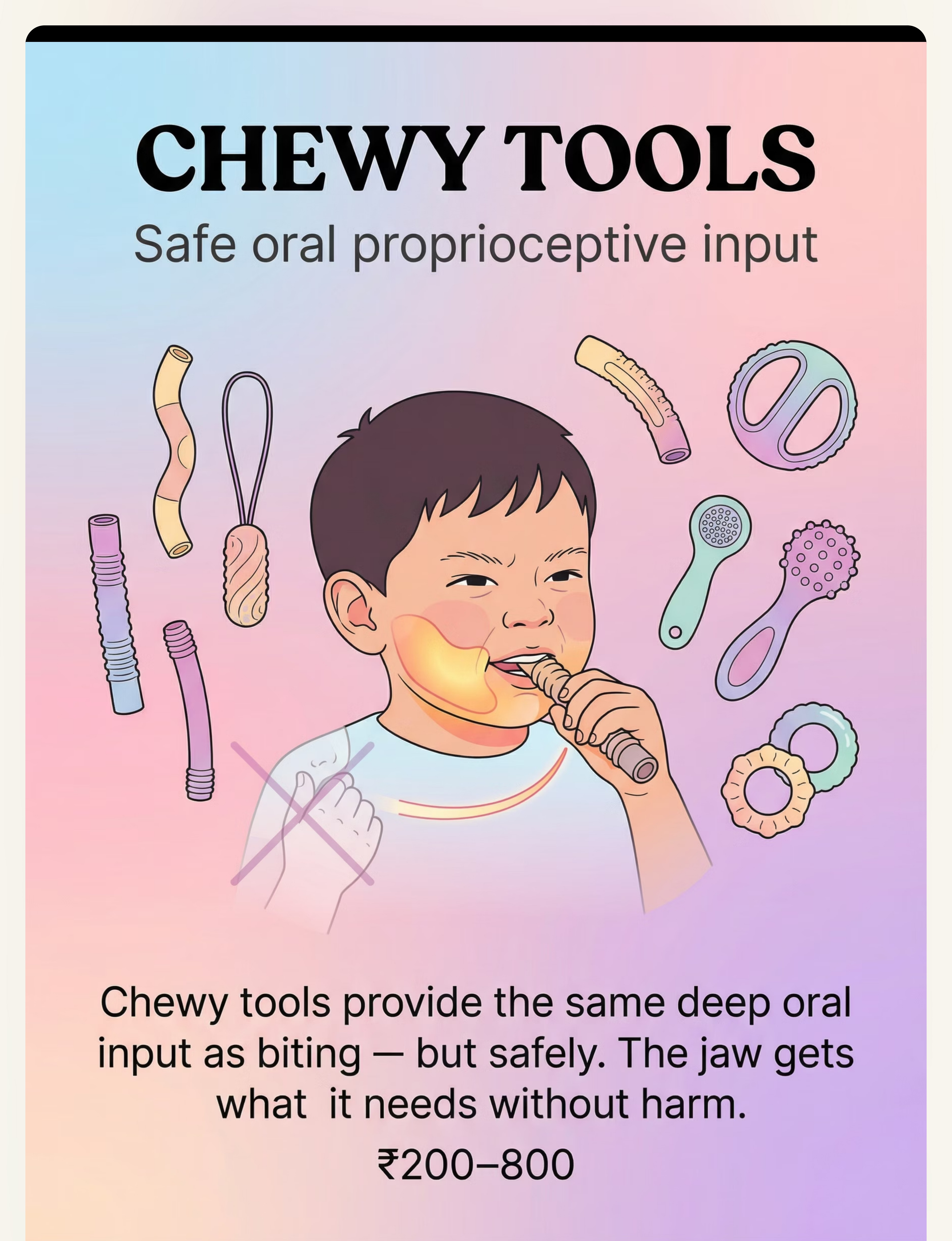
2. 🦷 Chewy Tools
Safe oral proprioceptive input
₹200–800
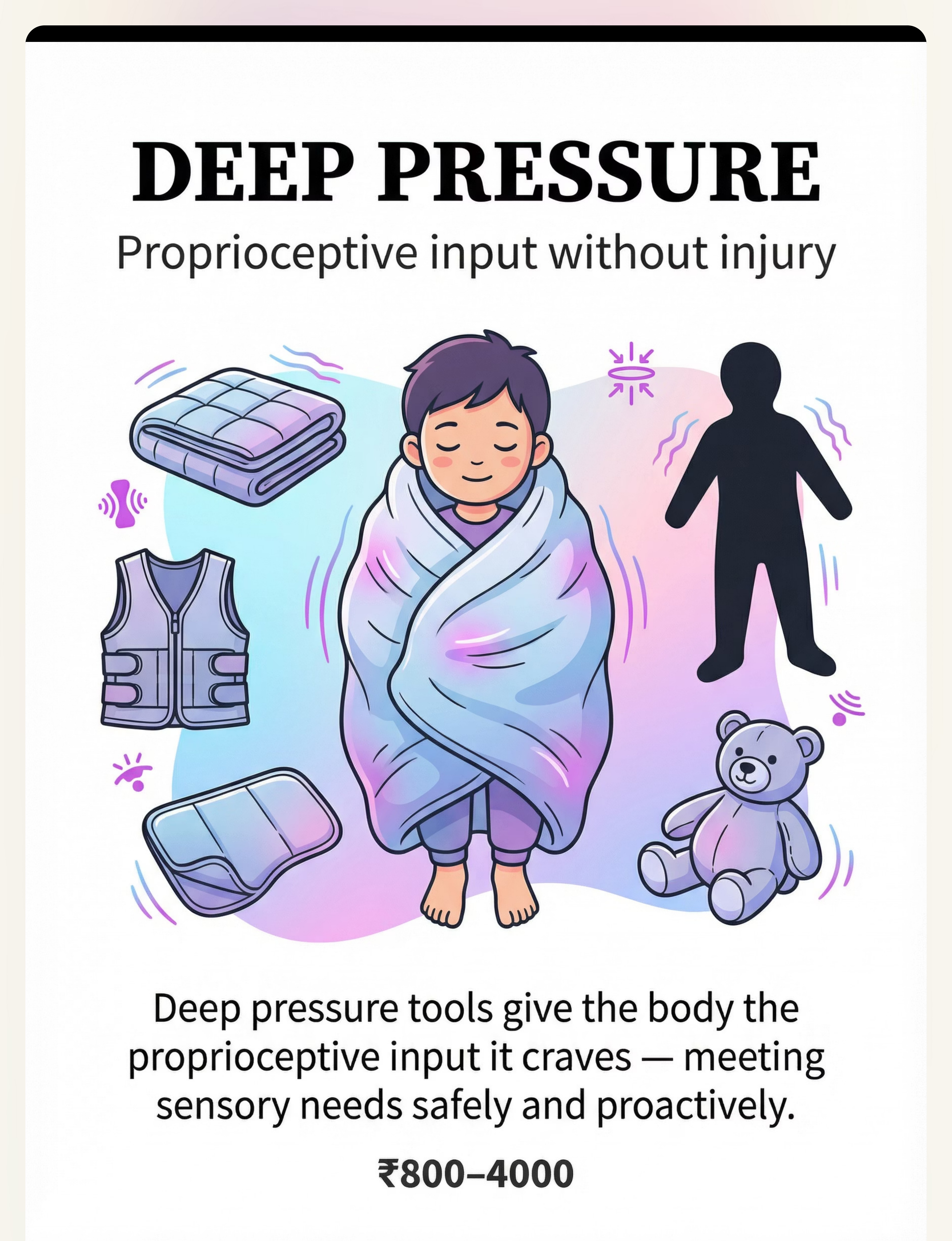
3. ⚖️ Deep Pressure Tools
Proprioceptive input without injury
₹800–4,000
4. 💪 Heavy Work Materials
Intense safe physical input
₹500–3,000
5. 🖐️ Fidget & Tactile Alternatives
Hands busy with safe input
₹100–600
6. 🔄 Sensory Matching Tools
Same input, safe delivery
₹200–1,500
7. 💬 AAC Communication Tools
Express needs before crisis
₹300–3,000
8. 🏠 Environment Tools
Reduce triggers and overload
₹500–2,500
9. 📊 Data Tracking Tools
Understand patterns, guide intervention
₹50–500
Pinnacle Canon Materials™ — 128 categories. 687 clinically mapped products.
Every family can start today. Regardless of budget.
WHO/UNICEF Equity Principle
Effective intervention should be accessible to every child in every context. Zero-cost alternatives exist for every material category. Here are six practical DIY options you can implement immediately.
🛡️ Protective Gear (DIY)
Buy: Soft protective helmets (₹500–2,000) | DIY: Fold a thick bath towel, secure gently around head with soft bandage while supervising closely. Use padded oven mitts as temporary arm guards. Same purpose: reduce impact while alternatives are being built.
🦷 Chewy Tools (DIY)
Buy: Therapeutic chewy necklaces (₹200–600) | DIY: Clean, food-grade silicone tubing from hardware store (~₹50). Braided cotton rope cleaned with food-safe cleaner. Ensure no small parts, non-toxic. Monitor for wear.
⚖️ Deep Pressure (DIY)
Buy: Weighted blanket (₹1,200–4,000) | DIY: Fill a pillowcase with 2–3 kg of dry beans or rice. Place across lap or shoulders for 10–15 minutes. Monitor temperature. Same function: proprioceptive input through weight.
💪 Heavy Work (DIY)
Buy: Resistance bands, crash pads (₹500–2,500) | DIY: Backpack with 1–2 kg of books to carry. Full laundry basket to push across room. Pushing heavy furniture with adult supervision. Thick floor mattress for safe crashing.
🖐️ Fidget (DIY)
Buy: Textured fidgets, fidget cubes (₹100–500) | DIY: Bubble wrap sheet. Dried lentil tray to pick through. Sand or rice sensory bin. Velcro strips on textured fabric. Same function: tactile hand-seeking redirected.
💬 Communication (DIY)
Buy: AAC device, PECS cards (₹500–3,000) | DIY: Print free PECS symbols from Boardmaker Free Resources. Laminate with clear tape. Create a simple "BREAK / SQUEEZE / HELP" 3-card communication strip.
Research: WHO NCF Handbook (2022) | PMC9978394: Context-specific, household-material intervention demonstrates comparable efficacy in LMIC settings.

⚠️ IMPORTANT SAFETY NOTICE — READ BEFORE PROCEEDING
Safety First: Before You Begin
🔴 STOP — Seek Help Immediately If:
- Self-injury is causing wounds requiring medical attention
- Eye-directed behavior (eye-poking, eye-pressing) — IMMEDIATE vision risk
- Behavior is escalating rapidly in frequency or intensity
- New or sudden onset of severe self-injury
- You feel unable to keep your child safe
📞 Call 9100 181 181 or seek emergency care
🟡 MODIFY — Requires Professional Assessment:
- Ongoing SIB at any frequency without professional evaluation
- Protective equipment needed but not yet prescribed
- Child has limited communication
- Multiple SIB forms occurring simultaneously
These materials are SUPPLEMENTS to professional intervention, not replacements.
🟢 GREEN — Home Implementation Appropriate When:
- Professional FBA and sensory evaluation have been completed
- Replacement behaviors have been identified by your clinical team
- Safety plan is in place
- You have professional guidance on materials selection
Material Safety Specifics: Weighted items: NEVER use if child cannot remove independently. Max 10% body weight. Max 20 minutes continuous use. Chewy tools: Replace if torn or showing wear. Non-toxic materials only. Protective gear: Must fit correctly — too loose provides no protection; too tight causes distress.
📞 9100 181 181 — FREE. 16+ languages. 24x7.
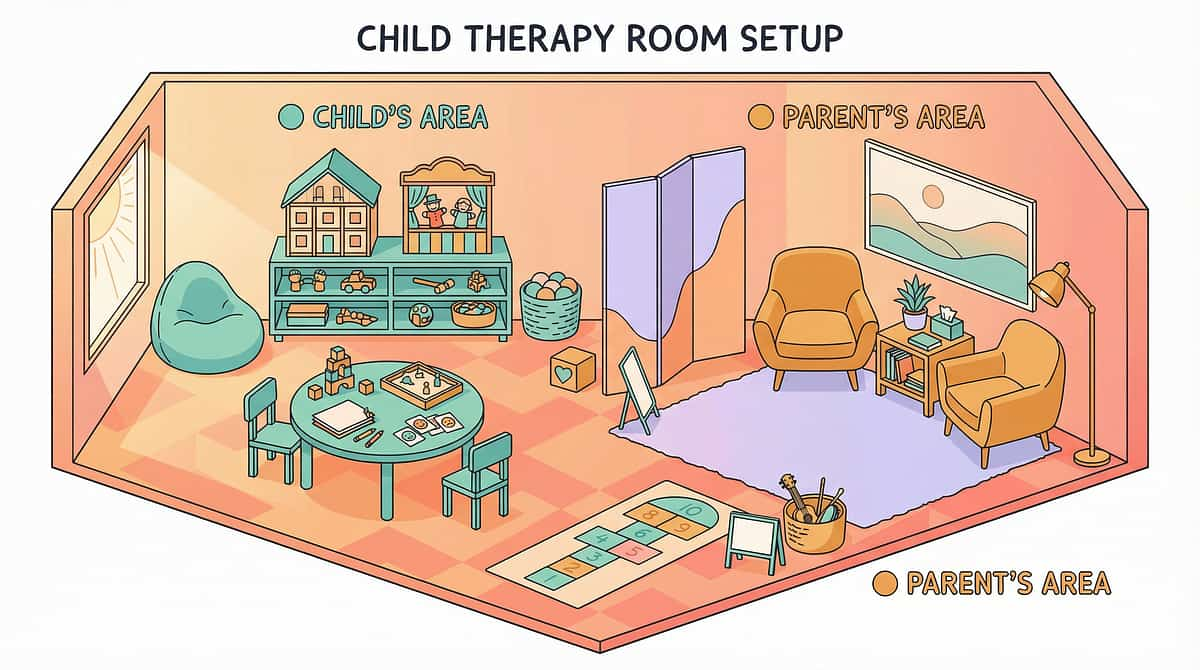
Set Up Your Space
"Spatial precision prevents 80% of session failures." The way you arrange your environment directly impacts your child's ability to regulate and engage. These setup principles are drawn from clinical best practices across OT and ABA settings.
Position Key
① Child: Floor cushion or bean bag. Ground-level position reduces fall risk.
② Parent: Beside and slightly behind — not directly facing, which can increase pressure.
③ Material Tray: Within child's reach, parent's sight. All 9 material categories accessible.
④ Door/Exit: Always open. Child should never feel trapped.
Environment Settings
- 🔇Sound: Quiet. Soft background noise if beneficial.
- 💡Light: Natural light preferred. Dim fluorescents.
- 🌡️Temperature: Cool to comfortable. Never overheated.
- 🪑Floor: Carpeted or padded. Never hard tiles.
Remove From Space:
- ❌ Hard surfaces at head height
- ❌ Objects that could be thrown dangerously
- ❌ Loud screens or audio
- ❌ Other children who may escalate anxiety
Research: PMC10955541: Structured, 1:1 individual treatment environment correlates with maximum session effectiveness.

Is Your Child Ready? The 60-Second Readiness Check
"The best session is one that starts right." This quick check determines whether to proceed, simplify, or postpone. Never skip it — the readiness state of your child at session start is the single strongest predictor of outcome.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Fed in last 2 hours? | Yes | Mild hunger | Very hungry | |
Rested? | Yes | Mildly tired | Overtired | |
Baseline regulation? | Calm/alert | Slightly elevated | Meltdown/post-crisis | |
Illness present? | None | Mild cold | Fever/pain | |
SIB in last 30 min? | None | Minor | Active/recent severe | |
Protective gear available? | Yes | In progress | Not available (if needed) |
🟢 ALL GREEN
Proceed to Step 1: The Invitation
🟡 ANY AMBER
Simplify protocol. Use only 1–2 materials. Shorten to 5 minutes.
🔴 ANY RED
Postpone. Offer quiet sensory activity for 10 minutes. Document and try tomorrow.

Step 1 of 6
⏱️ 30–60 seconds
Step 1: The Invitation
Every protocol begins with an invitation, not a command. The way you open a session sets the nervous system's tone for everything that follows. A gentle, low-pressure offer activates approach rather than defense.
"Hey, I have your chewy/squeeze thing/heavy bag. Want to check it out with me?"
Body Language
- Get to child's level (floor or seated)
- Soft eye contact, not sustained demanding gaze
- Relaxed posture, no tension in shoulders
- Material visible but not thrust forward
✅ Acceptance Signals
- Eyes move toward material
- Body orientation shifts toward you
- Hands reach or extend
- Any vocalization or AAC pointing
⚠️ Resistance Signals
Turning away → Wait 10 seconds, try once more.
Pushing material away → Honor it. Try different material.
Increasing distress → Postpone. Go to calming activity.
Research: ABA Pairing Procedures: Establishing motivating operations before demand placement increases session engagement by 60–80%.
Step 2 of 6
⏱️ 1–3 minutes
Step 2: The Engagement
Introduce the therapeutic material as the child shows interest. Follow their lead. Match the intensity they're seeking. The goal here is genuine contact with the material — not performance.
🦷 For Oral Seekers/Biters
Hand chewy tool gently at child's palm level. Narrate softly: "This is for chewing. It's yours." If child reaches for own hand/arm → gently redirect to chewy. Celebrate any contact.
👊 For Head-Hitters
Offer weighted lap pad or deep pressure squeeze first. Gentle shoulder compression if welcome. Vibrating pillow as head-pressure alternative. Narrate: "I can give your head what it needs."
🖐️ For Skin Pickers
Offer textured fidget that matches the picking sensation. Peeling stickers, bubble wrap, picking tray. Place in child's field of vision. Narrate: "Here's something to pick."
💥 For Body Slammers
Offer crash cushion. Heavy work option (pushing activity). Weighted blanket. Narrate: "This will feel really strong."
Research: PMC11506176: Structured material introduction within sensory integration protocol meets EBP criteria.

Step 3 of 6
⏱️ 3–7 minutes
Step 3: The Therapeutic Action
This is the core therapeutic event — where the sensory need begins to be met safely. This step occupies 40–60% of effective session time. Do not rush it.
🦷 Oral Biting → Chewy Protocol
Do NOT pull away when biting hard — this is the proprioceptive input being sought. Allow 3–5 minutes of uninterrupted chewy use. Observe: Does body relax? Does biting frequency shift to chewy?
👊 Head-Hitting → Pressure Protocol
Offer bilateral head compression (palms gently on sides of head, firm pressure for 5–10 seconds — only if child welcomes touch). Vibrating pillow at head. Heavy work prior to pre-satisfy demand.
🖐️ Skin Picking → Tactile Protocol
Child uses picking tray / textured fidget at natural intensity. Observe: Do hands go to skin less? Track duration of engagement with alternative.
💥 Body Slamming → Crash Protocol
Directed crashing into crash pad. Resistance band pulling. Heavy carry activities. Observe: Does intensity of body-directed seeking reduce post heavy work?
Common execution errors:❌ Pulling material away when child is intensely engaging (defeats the purpose) ❌ Rushing through before sensory need is met ❌ Chatting/demanding during core action ❌ Ending session the moment SIB appears replaced (too early)

Step 4 of 6
⏱️ 3–5 minutes
Step 4: Repeat & Vary
"3 good repetitions are worth more than 10 forced ones." Repetition consolidates the neural pathway. Variation maintains engagement and broadens the child's sensory toolkit.
Material | Target Reps | Variation Options | |
Chewy tool | 3–5 chewing episodes | Vary resistance level | |
Deep pressure | 3 compressions, 5–10 sec each | Vary body location | |
Heavy work | 3 activity sets | Push → pull → carry rotation | |
Crash pad | 3–5 safe crashes | Vary angle/speed | |
Fidget | Continuous until satiation | Swap texture varieties |
✅ Satiation Signals
- Body relaxes and disengages naturally
- Child initiates transition to different activity
- Affect becomes calmer, regulated
- Self-directed SIB reduces spontaneously
⚠️ Escalation Signals — Stop and Reset
- Increasing distress despite material
- Refusal of all offered alternatives
- SIB intensifying → Go to cool-down immediately

Step 5 of 6
⏱️ 30 seconds
Step 5: Reinforce & Celebrate
Timing matters more than magnitude. Immediate. Specific. Enthusiastic. The biological window for behavioral reinforcement is within 3 seconds of the target behavior — not 30 seconds later, not with a lengthy explanation.
The Moment to Deliver Reinforcement
The MOMENT the child contacts the replacement material instead of self. The MOMENT the child uses AAC to request a break or squeeze. The MOMENT the child initiates approach to calm space.
Script: Limited Language
"YES!" + warm touch (if welcome) + immediate access to preferred item for 5 seconds.
Script: Developing Language
"You used your chewy! That was SO smart. That's exactly what your mouth needed."
Script: Older Children/Adolescents
"I noticed you went for the squeeze thing instead. That was really good self-awareness. How does that feel?"
Important: Celebrate the ATTEMPT, not just the success. Any approximation toward safer behavior warrants enthusiastic reinforcement. ABA research: Immediate, specific reinforcement increases replacement behavior rate by 200–400%.

Step 6 of 6
⏱️ 2–3 minutes
Step 6: The Cool-Down
No session ends abruptly. The nervous system needs a landing zone. A structured cool-down transitions the child gently and teaches them that sessions have a predictable, safe rhythm.
The cool-down is not just an ending — it is a therapeutic event in itself. A child who lands safely is a child who will re-engage willingly tomorrow.
Cool-Down Sensory Input
- Slow rocking (if tolerated)
- Quiet weighted blanket time (5 minutes)
- Gentle humming/music
- Proprioceptive walking (slow, deliberate steps)
What NOT to Do
- ❌ Abrupt "all done" with removal of all material
- ❌ Immediate high-demand transition
- ❌ Scolding or commentary about behavior during cool-down
NCAEP EBP Report 2020: Visual timer and transition supports are classified evidence-based practices for autism.

Capture the Data: Right Now
"Within 60 seconds of session end. Not tomorrow. Now." Data is not for judgment — data is for navigation. Three weeks of this simple tracking will reveal patterns you cannot see in the moment: which material works best, which time of day SIB is lowest, whether protective gear needs adjusting.
📋 The 3-Field Minimum Tracker
- Today's date + materials used
- SIB incident count + duration
- Replacement behavior occurred? Yes / No / Partial
- Which material? Duration of alternative use?
- Overall session quality: 1–5
- Notes: triggers, anything unusual
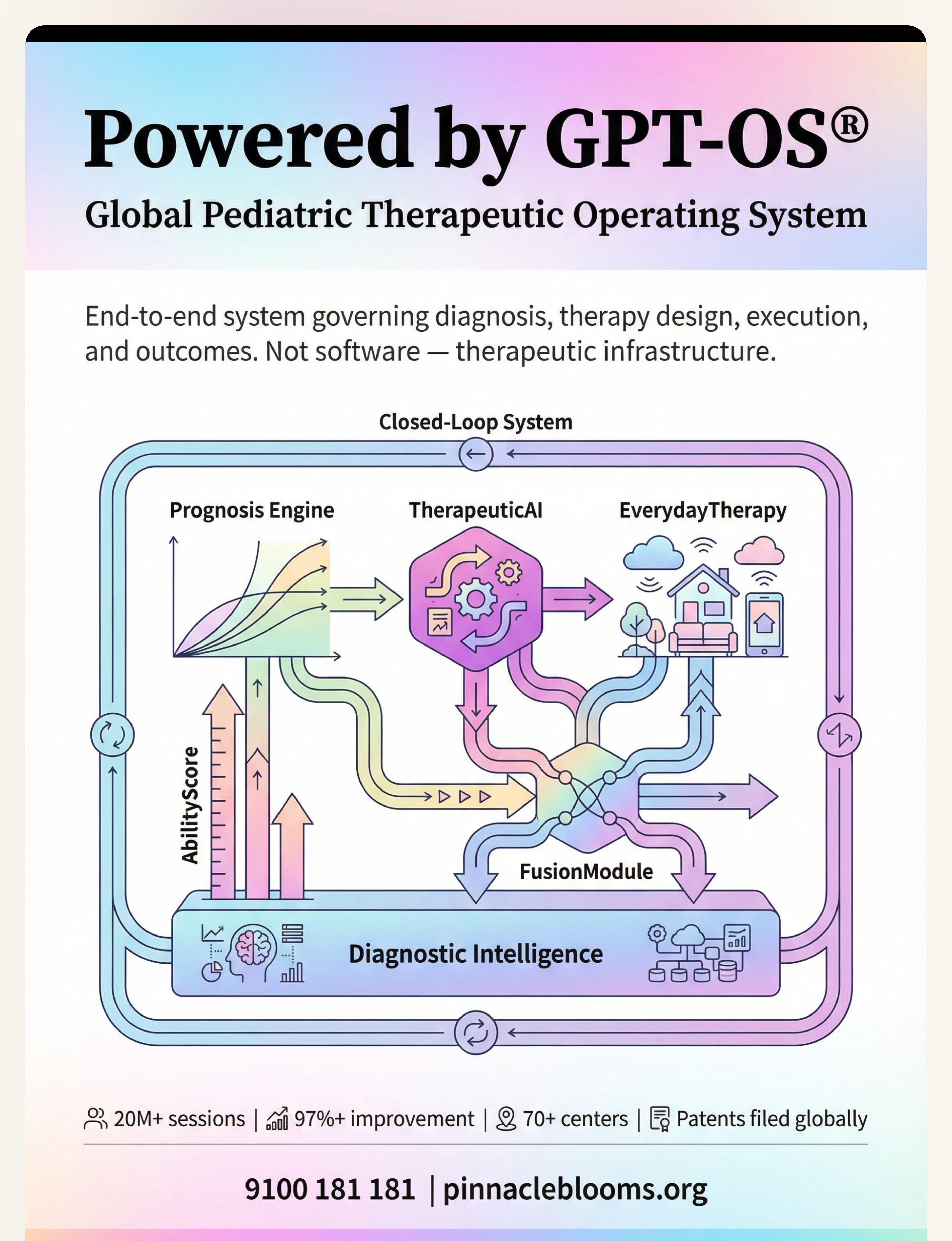
🤖 GPT-OS® Integration
Log this same data into GPT-OS® EverydayTherapyProgramme™ tracker for:
- Automated pattern analysis
- AbilityScore® progress tracking
- Personalized protocol adjustments by TherapeuticAI®
- Shared data stream to your clinical team via FusionModule™
Research: ABA data collection: Without measurement, behavior change cannot be demonstrated or guided. ABC data + frequency tracking is gold standard.

Troubleshooting: When Things Don't Go as Planned
"Every session will not be perfect." That is not failure — that is the nature of nervous system work. Here is your contingency guide for the most common challenges.
❓ Child refuses all materials
Why: Wrong sensory match. Wrong timing. Undetected distress. Action: Reduce all demands. Offer 5 minutes of favorite unstructured sensory activity. Observe what child self-selects — that is your clue to the right material.
❓ SIB increases during session
Why: Session is adding demand/anxiety. Material is aversive. Child is beyond regulation threshold. Action: STOP demands. Implement calm-down protocol. Do NOT continue to push material. Document and discuss with BCBA.
❓ Child uses alternative briefly, then returns to SIB
Why: Alternative not matching intensity of need. Still building the habit. Action: This is NORMAL early on. Celebrate the brief use. Track duration — it will increase over weeks.
❓ Child uses material only with prompting
Why: Still learning the behavior. Needs higher reinforcement density. Action: Increase prompting (physical → gestural → verbal → independent). Increase reinforcement for prompted use. This is the expected trajectory.
❓ Protective gear is distressing the child
Why: Tactile sensitivity to gear itself. Poor fit. Action: Desensitize gradually. Start with gear nearby, then briefly touching, then wearing. Ensure comfortable fit. Use preferred appearance (colors, characters if possible).
Personalize This Technique
"No two children are identical. Neither should be their intervention." The core protocol is the same — but the sensory profile, age, and intensity must be adapted to your specific child.
For the Intense Proprioceptive Seeker
Increase heavy work frequency (3x/day vs 1x/day). Use highest-resistance chewy tools. Crash pad available all day, not just in sessions. Focus on whole-body inputs.
For the Oral Seeker
Chewy necklace worn continuously (not just in sessions). Oral sensory diet: crunchy foods, straw activities, resistive snacks. Multiple chewy backup options in all bags and settings.
For the Sensory Avoider with SIB
(SIB driven by escape/overwhelm, not seeking.) Reduce sensory demands first. Provide escape options. Build communication to request removal from overwhelming input. Protective gear priority here.
Age | Modification | |
2–4 years | Parent-led 100%. Shorter (5 min). More physical play framing. | |
4–8 years | Child partially initiating. Introduce choice between materials. | |
8–12 years | Child selecting preferred material. Self-monitoring emerging. | |
12–18 years | Adolescent agency central. Self-advocacy language. Peer-normalizing. |
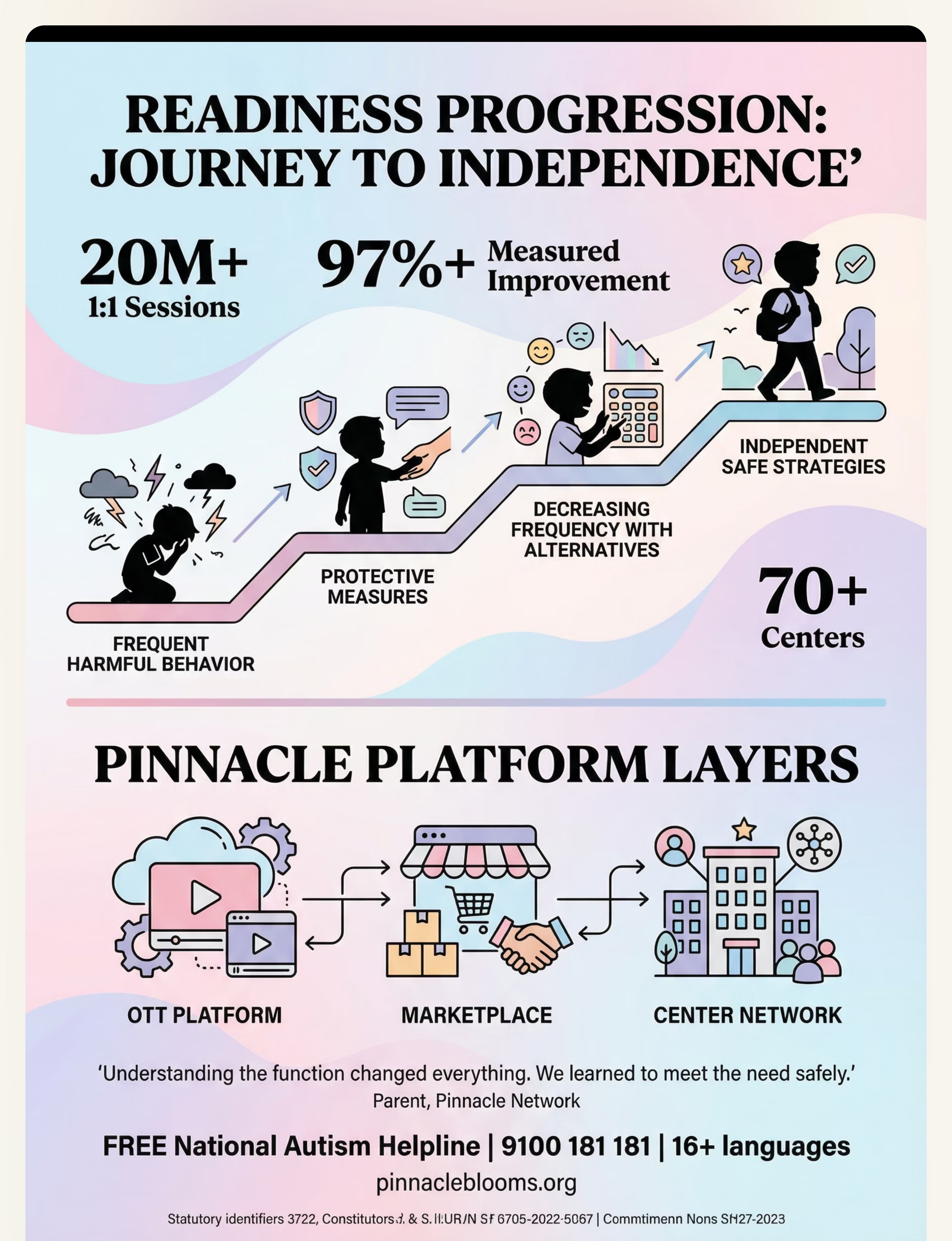
ACT IV — THE PROGRESS ARC
Weeks 1–2: What to Expect
15%
Week 1–2 Progress
Protection and introduction. Not mastery.
✅ What You WILL Likely See
- Child tolerates protective gear for short periods
- Brief contact with replacement materials (seconds, not minutes)
- Slight reduction in SIB duration (not frequency yet)
- Some distress around new materials (this is normal)
- Data showing baseline patterns
❌ What You Will NOT See Yet (And That's OK)
- Child independently selecting alternative material
- Significant SIB frequency reduction
- Spontaneous use across settings
- Mastery of any material
"If your child wore the chewy for 5 seconds today and 8 seconds tomorrow — that is 60% improvement. Track the seconds."
📞 9100 181 181 | Research: PMC11506176: Sensory integration outcomes emerge across 8–12 week timelines. Early indicators: tolerance and participation before skill mastery.
Week 3–4: Consolidation Signs
"The neural pathway is starting to form." The changes you see in weeks 3–4 are not just behavioral — they represent genuine neurological reorganization happening in real time.
40%
Week 3–4 Progress
Neural pathway formation has begun.
Child ANTICIPATES the material
Moves toward it before being offered — a critical neural signal.
Child shows PREFERENCE
Reaches for one material over others. A meaningful choice is emerging.
SIB duration BEGINNING to shorten
Even if frequency is unchanged, shorter episodes signal regulation progress.
First SELF-INITIATING moments
Child approaches material with no prompt — even briefly. Celebrate this enormously.
"You may notice YOU are becoming more confident. You're reading your child's escalation pattern earlier. That parental recognition is itself a clinical skill — and it matters enormously."

Weeks 5–8: The Mastery Arc
Independent safety strategies emerge. This is the phase families describe as the turning point — when the household shifts from reactive crisis management to proactive sensory care.
70%
Week 5–8 Progress
Breakthrough indicators emerging.
🌟 Independence Signals
Child approaches material station independently before escalation. SIB frequency 30–60% below baseline on good days. Protective gear needed less frequently. Child communicating sensory needs with new vocabulary.
🌟 Generalization Seeds
Behavior beginning to appear in a second setting (school, car, grandparent's home). Other caregivers reporting child brings chewy proactively. Child showing some self-awareness of escalation state.
🌟 Family System Change
Parents feel less reactive, more proactive. Other family members using same language and protocols. Household sensory diet running almost automatically.
Research: PMC11506176: 8-week sensory integration protocols show significant functional improvements in adaptive behavior and sensory processing.

Real Progress Happened. Mark It. Own It.
Progress in SIB reduction is hard-won and deserves to be celebrated explicitly — by you, your family, and your clinical team. These moments of recognition matter both emotionally and therapeutically.
"Three months ago, he had 12 head-hitting incidents per day. Today: 3. That's 75% reduction. He still needs his helmet sometimes. But 75% fewer times his brain is in crisis."
— Parent, Pinnacle Network, Hyderabad
"She uses the chewy necklace now. It's been 4 weeks since she bit her arm hard enough to mark. I cried the first time I noticed."
— Parent, Pinnacle Network, Bengaluru
"He asks for 'squeeze' now when he's overwhelmed. He HAS a word for what he needs. That is everything."
— Parent, Pinnacle Network, Mumbai
Family Milestone Ritual: Create a simple progress board. Each week, note: Lowest SIB count day this week | New thing child did with safe alternative | One moment of connection in a session.
⚠️ Safety Alert
Red Flags: When to Escalate
"Know when to escalate. Do not manage these alone." Progress is the goal — but safety is non-negotiable at every stage.
🚨 Call 9100 181 181 Immediately
- SIB resulting in wounds requiring medical attention
- ANY eye-directed behavior (eye-poking, pressing) — immediate vision risk
- Sudden significant SIB increase after a period of improvement (may indicate medical issue)
- New form of SIB emerging alongside existing form
- Child's distress is extreme and unresponsive to all calming strategies
- You, as caregiver, are at breaking point
⚠️ Schedule Urgent Review (Within 1 Week)
- SIB not reducing after 8 weeks of consistent protocol
- Materials are consistently rejected
- Protective equipment is no longer sufficient
- Escalation pattern changing (different times, different triggers)
- Sleep severely disrupted alongside SIB increase
🟢 Continue and Monitor
- Gradual improvements week over week
- Occasional setbacks after illness or schedule change (normal)
- Some days worse than others (normal)
📞 9100 181 181 — FREE. 24x7. 16+ languages.
The Progression Pathway
"You're not done. You're on a journey." D-368 is one node in a carefully sequenced therapeutic map. Knowing where you've been and where you're headed makes each step more intentional and effective.
Prerequisites (Where You Came From)
D-361: Understanding Stimming → D-366: Vocal Stimming → D-367: Toe Walking
★ D-368: When Stimming Causes Harm ← YOU ARE HERE
Current technique: Sensory-Based Self-Injury Replacement & Harm Reduction Protocol
Next-Level Options (Choose by Child's Profile)
D-369: When Stimming Blocks Learning | D-370: Visual Stimming Deep Dive | D-375: Emotional Dysregulation | D-380: Communication Frustration
Long-Term Destination
Independent use of sensory regulation strategies. Self-advocacy for sensory needs. Community participation without significant SIB.
Research: WHO/UNICEF Developmental Milestones Framework: Intervention sequencing follows evidence-based developmental cascades.
Related Techniques in This Domain
You already have the foundation. The materials you've acquired for D-368 create a direct bridge to these adjacent techniques — so your investment compounds with each new skill.
Code | Technique | Difficulty | Primary Material | |
D-361 | Understanding Stimming | 🟢 Intro | No materials needed | |
D-362 | Help With Hand Flapping | 🟢 Intro | Fidgets | |
D-364 | Help With Body Rocking | 🟡 Core | Vestibular tools | |
D-366 | Vocal Stimming | 🟡 Core | Oral sensory | |
D-369 | When Stimming Blocks Learning | 🟠 Advanced | Multi-material kit | |
D-375 | Emotional Dysregulation | 🔴 Complex | Full sensory diet |
"You already own materials for these": If you've acquired materials for D-368, you have: ✅ Materials for D-362 (fidgets) ✅ Materials for D-364 (deep pressure) ✅ Materials for D-366 (oral sensory)
One Technique. Twelve Domains. One Child.
The work you do on self-injurious behavior does not stay contained in Domain D. It ripples across your child's entire developmental map — and GPT-OS® tracks every ripple.
This Technique Feeds:
- Domain D (direct) — Behavioral/Autism
- Domain A (strong) — Sensory Processing
- Domain C (secondary) — Emotional Regulation
- Domain B (tertiary) — Social Communication via AAC
GPT-OS® Integration
When D-368 data is logged: AbilityScore® updates across Domains A, C, D. TherapeuticAI® adjusts recommendations across all 12 domains. FusionModule™ synchronizes OT + ABA + SLP on your child's status.
"This technique is one piece of a larger plan. GPT-OS® holds the whole picture."
ACT V — COMMUNITY & ECOSYSTEM
Parent Stories: You Are Not the Only One
These are the voices of families who have walked this path — and are walking it now. Their stories are offered not as promises of identical outcomes, but as proof that this is navigable.
"The first time I noticed the bruises, I didn't understand. Our behavioral therapist explained he was seeking deep proprioceptive input to his head. We introduced helmet padding for safety, deep pressure alternatives, intense physical activities. As he learned that other things could meet the same need — things that didn't hurt — the harmful behavior decreased. We replaced, we didn't just remove."
— Parent, Pinnacle Network, Hyderabad
"She bites her hands when she can't find words. The bite marks started at age three. Our OT helped me understand: the deep pressure from biting was regulating her nervous system. We introduced chewy tools, a sensory diet, communication boards. The biting didn't disappear completely. But it reduced dramatically. We stopped fighting her body and started working with it."
— Parent, Pinnacle Network, Bengaluru
"Understanding the function changed everything. Protective equipment first, then a whole sensory diet. It took months. We tracked every incident. 90% reduced. He now asks for a 'head squeeze' or goes to his crash pad. You CAN navigate this."
— Parent, Pinnacle Network, Mumbai
Note: Illustrative cases. Individual outcomes vary. Professional assessment essential.
Connect With the Community
"You don't have to figure this out alone." Join thousands of families navigating the same journey across India and 70+ countries. The Pinnacle community offers parent support, professional moderation, and real-world evidence at every step.
Pinnacle Parent Circle
WhatsApp community for SIB support. Moderated by clinical team. Peer support from families at every stage of the journey.
Online Forums
pinnacleblooms.org/community — OT/ABA-moderated discussion. Search by technique, age, and domain.
Pinnacle Reels Library
D-series: Stimming & Repetitive Behaviours. Visual, practical, therapist-led. Watch anytime.
Weekly Live Q&A
Thursdays, 7 PM IST with Consortium therapists. Submit your questions in advance. Free for all families.
Share this technique with your child's school (they need this protocol too), your extended family (consistency across caregivers multiplies outcomes by 3x), and other parents navigating SIB.
📞 9100 181 181 — FREE. Always available.
Find Professional Support
"Professional assessment is not optional for self-injurious behavior. It is essential." Here is who you need — in order of priority — and how to find them through the Pinnacle network.
Board Certified Behavior Analyst (BCBA)
Functional Behavior Assessment — identifies the maintaining function of SIB. Builds replacement behavior training program. Available at 70+ Pinnacle centers or via teleconsult.
Occupational Therapist (SI-trained)
Sensory processing evaluation. Sensory diet design. Protective equipment prescription. Essential for all sensory-maintained SIB.
Developmental Pediatrician / Physician
Rule out medical contributors: pain, GI, dental, infection. Medical safety evaluation for moderate-severe SIB. Non-negotiable for escalating presentations.
Speech-Language Pathologist
Communication evaluation. AAC prescription if needed. Addresses the communication function of SIB directly.
The Research Library
For the curious, the clinical, and the questioning — every claim in this guide is backed by peer-reviewed evidence. Here are the five key studies underpinning D-368.
# | Citation | Key Finding | |
1 | PMC11506176 — Children 2024 | Sensory integration = EBP; 16 studies confirmed | |
2 | PMC10955541 — World J Clin Cases 2024 | 24-study meta-analysis: sensory therapy promotes adaptive behavior | |
3 | DOI: 10.1007/s12098-018-2747-4 — Indian J Pediatr 2019 | Indian RCT: home-based sensory intervention outcomes | |
4 | NCAEP 2020 | AAC, FCT, Sensory Integration all classified EBP for autism | |
5 | PMC9978394 — WHO CCD Package | Multi-caregiver delivery across 54 LMICs; proven outcomes |
Oxford Centre for Evidence-Based Medicine (OCEBM) levels used for all grading.

How GPT-OS® Uses Your Data
"Your session data. How it protects every child." Every data point you enter does two things at once: it improves your child's care, and it contributes to population-level intelligence that helps families like yours around the world.
GPT-OS® specifically learns from D-368 data: which materials reduce SIB most effectively (individual + population level), optimal timing of sensory diet interventions, escalation pattern predictors, and week-on-week progress trajectory vs. typical GPT-OS® population.
Privacy commitment: All data governed by Pinnacle Blooms Network data protection protocols. Individual child data is never shared without explicit consent. Aggregate de-identified data improves population-level intelligence. "Your data helps every child like yours."
Core GPT-OS® components: AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ | Prognosis Engine | Diagnostic Intelligence Layer
Watch the Reel: 60 Seconds That Could Change How You See This
Reel D-368 | Sensory Regulation & Repetitive Behaviours | Domain D | Subdomain D2
"When I see a child hurting themselves, I see a nervous system in crisis — seeking something it desperately needs. In this reel I share 9 materials that can help meet the same need more safely. This is not about stopping your child. It's about understanding them."
← D-367
9 Materials That Help With Toe Walking
★ D-368
When Stimming Causes Harm — YOU ARE HERE
→ D-369
When Stimming Blocks Learning
→ D-370
Visual Stimming Deep Dive
Research: NCAEP EBP 2020: Video modeling is classified evidence-based practice for autism. Multi-modal learning improves parent skill acquisition.
"Consistency Across Caregivers Multiplies Impact 3x."
This guide is most powerful when it reaches everyone in your child's life — teachers, grandparents, extended family. Here are ready-made resources to share right now.
📱 For Grandparents — Simplified Version
"[Child's name]'s self-injury is not deliberate. Their brain seeks intense physical input. When you see this: Don't grab their hands. Don't scold. Offer the chewy/squeeze tool. Give a firm hug if they welcome it. Call [parent] if it seems severe. You can't do this wrong if you stay calm and offer the safe tool."
🏫 Teacher/School Communication Template
"[Child's name] may engage in [specific SIB form] when overwhelmed or seeking sensory input. Please: (1) Offer chewy/fidget at first signs of escalation (2) Maintain calm tone (3) Allow access to safe sensory station (4) Contact parents if protective gear needed."
📞 9100 181 181 for family consultation support.
Research: WHO CCD Package (PMC9978394): Multi-caregiver training critical for intervention generalization and maintenance.

Frequently Asked Questions
Your questions. Our honest answers. Evidence-based, practically grounded, and never dismissive of the complexity you are living.
❓ "Should I ignore the SIB to avoid reinforcing it?"
No — not for sensory-maintained SIB. Ignoring does not reduce sensory needs (which are not socially mediated). Ignoring allows injury to continue. The correct approach is to provide safer sensory alternatives. If SIB is attention-maintained (confirmed by FBA), planned ignoring may be part of a professional plan — but never without a replacement behavior trained simultaneously.
❓ "Will the protective gear become permanent?"
No. Protective equipment is a safety bridge — used while therapeutic alternatives are being established. As replacement behaviors strengthen, protective gear needs typically decrease. Your BCBA/OT will create a fading plan as part of the intervention.
❓ "Is it safe to let my child bite a chewy tool as hard as they want?"
Yes — when the chewy is rated for aggressive chewing and is not damaged. The intensity is often necessary to meet the oral proprioceptive need. Trying to limit bite force defeats the purpose. Inspect regularly for damage and replace when worn.
❓ "My child only uses the alternative material when prompted. Is that progress?"
Yes — absolutely. Prompted use is the first phase of skill acquisition. The prompting hierarchy: physical → gesture → verbal → independent. Celebrate prompted use enthusiastically. Independence comes after prompted use is well-established.
❓ "How do I know which function is driving the SIB?"
This requires a Functional Behavior Assessment by a BCBA. Clue: if SIB occurs alone with no social audience, it's likely sensory-maintained. If it increases during demands, escape may be a function. Most require professional FBA for certainty.
❓ "At what point should medication be considered?"
Medication is sometimes considered for severe SIB when behavioral and sensory interventions have been implemented consistently and are insufficient. Always requires consultation with a developmental pediatrician specializing in autism. Medication is always adjunct to — never replacement for — behavioral and sensory intervention.
❓ "My child has been doing this for years. Is it too late?"
It is never too late. SIB can be addressed at any age with appropriate intervention. Older children and adolescents may require different approaches, but the evidence base for behavioral and sensory intervention spans all ages through adulthood.
❓ "Can diet changes help?"
Some research suggests gut health, food sensitivities, and nutritional factors can influence sensory processing and behavioral regulation. Explore with your pediatrician as a complementary — not replacement — approach alongside behavioral and sensory intervention.

ACT VI — YOUR NEXT STEP
You've Read the Science. You Understand the Need. Now Act.
"You watched your child hurt themselves and felt helpless. You are no longer helpless. You now understand the function. You have the materials. You have the protocol. You have the safety plan. You have the evidence. You have 70+ centers, 20M sessions, and an entire consortium behind you."
✦ Validated by the Pinnacle Blooms Consortium ✦ OT • SLP • ABA • SpEd • NeuroDev • CRO • WHO • UNICEF • Parents
📞 9100 181 181 — FREE National Autism Helpline | 16+ languages | 24x7
For urgent self-injury situations: Call immediately.
Preview of 9 materials that help when stimming causes harm Therapy Material
Below is a visual preview of 9 materials that help when stimming causes harm therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

The Pinnacle Promise
From fear to mastery. One technique at a time.
Pinnacle Blooms Consortium: Occupational Therapy • Speech-Language Pathology • Applied Behavior Analysis • Special Education • NeuroDevelopmental Pediatrics • Clinical Research • WHO Framework • UNICEF Standards • 70+ Countries • 20M+ Sessions
Medical Disclaimer: Self-injurious behavior is a complex clinical presentation requiring comprehensive professional assessment and intervention. This content is educational and does not replace individualized professional evaluation and treatment. If a child is engaging in significant self-injury, seek professional help immediately. Materials described are therapeutic supports within comprehensive intervention plans, not standalone solutions. Individual results vary significantly. This content has been reviewed by the Pinnacle Blooms Consortium of specialist therapists but should not be applied without professional guidance for moderate-severe self-injury.
← Return to Start
D-368: The Recognition Moment
→ Next Technique
D-369: When Stimming Blocks Learning
🌐 Browse All Techniques
techniques.pinnacleblooms.org
🏠 Pinnacle Home
pinnacleblooms.org
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Domain D: Autism/Behavioral | Subdomain D2: Stimming & Repetitive Behaviours | Technique D-368 | 40-Card Narrative Architecture v2