
"He Knows How to Play — But He Just Stands There"
You've watched it a hundred times. The toys are there. The other children are playing. Your child has the skills — you've seen them. But they won't start. They wait. They watch. They stand at the edge of everything and need you to push them in. You're not imagining this. And it's not laziness. It's not defiance. It's a neurological difficulty called initiation deficit — and it has a name, a science, and a solution.
"He knows how to play but just stands there waiting. He has the words but won't speak first. The skill is there — the starting isn't." — Parent, Pinnacle Blooms Network
Validated by Pinnacle Blooms Expert Consortium: SLP • OT • BCBA • SpEd • NeuroDev Pediatricians

This Is More Common Than You Think
Initiation difficulty is one of the most frequently reported executive function challenges in pediatric autism, ADHD, and developmental conditions. Research consistently shows that 60–80% of children on the autism spectrum demonstrate measurable difficulties with task initiation — the ability to independently begin an action without external prompting.
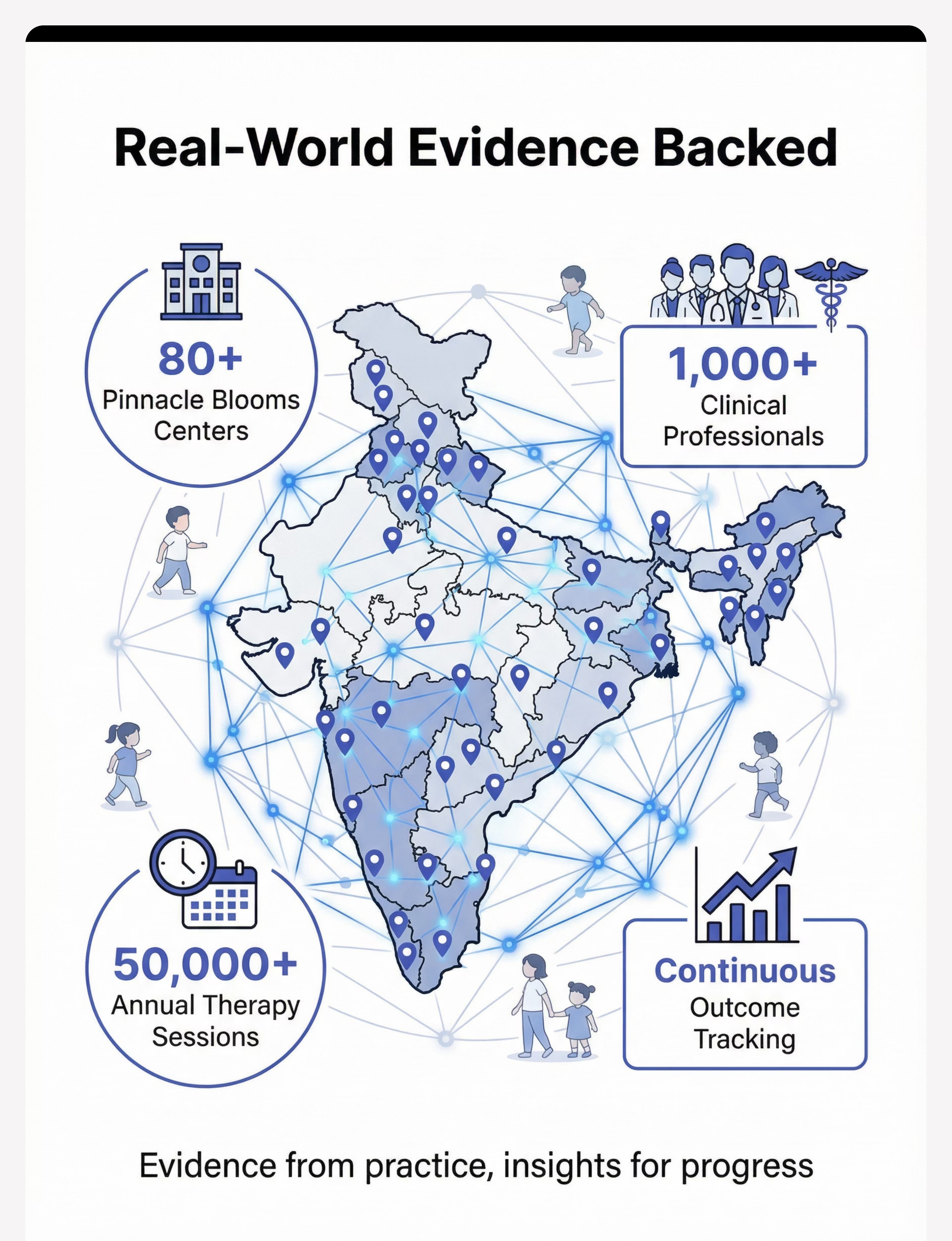
At Pinnacle Blooms Network, across 20M+ exclusive 1:1 therapy sessions delivered through 80+ centers, initiation deficit ranks among the top 5 concerns parents report at first assessment. This is not a rare problem. This is not your child being difficult. This is one of the most well-documented executive function challenges in pediatric neurodevelopment — and one of the most treatable.
60–80%
ASD Initiation Difficulty
of children with ASD show measurable initiation difficulties (Ozonoff et al., 1991; Barkley, 2012)
20M+
Therapy Sessions
delivered by Pinnacle Blooms Network tracking initiation progress
97%+
Measured Improvement
across one or more developmental readiness indexes
9
Validated Materials
that build the bridge from waiting to starting
"Every parent in our network has described this exact moment — watching their capable child wait while the world moves around them. You are not alone in this. And your child is not choosing to stand still."
Why Starting Is Harder Than Doing
Clinical Explanation
Initiation is governed by the prefrontal cortex — particularly the dorsolateral prefrontal cortex (DLPFC) and the anterior cingulate cortex (ACC). These regions generate the internal "go signal" that translates intention into action. In children with autism, ADHD, and related conditions, neuroimaging studies show reduced activation in these areas during task-switching and self-initiated behavior. The supplementary motor area (SMA) also shows atypical activation — meaning the child literally struggles to generate the neural command that begins an action, even when all downstream systems are fully functional.
What This Means for Your Child
Think of it like this: Your child's brain has the entire engine — the knowledge, the motor skills, the language, the desire. But the ignition switch doesn't fire reliably. They need someone else to turn the key. The 9 materials on this page are designed to be external ignition systems — ways to get that engine started from outside until the brain's own starter motor strengthens.
Brain regions involved: Prefrontal Cortex (planning/initiation) • Anterior Cingulate Cortex (motivation/drive) • Supplementary Motor Area (action sequencing) • Basal Ganglia (movement initiation)
"This is a wiring difference, not a behavior choice. Your child is not being lazy, defiant, or stubborn. Their brain genuinely struggles to generate the internal start signal that neurotypical children activate automatically."

Initiation Across the Developmental Timeline
The WHO Care for Child Development (CCD) Package and UNICEF MICS developmental monitoring indicators map initiation as an emerging skill from 12 months onward — beginning with simple motor initiation and progressing through social, task, and cognitive initiation.
12–18 Months
Motor initiation — reaching for objects, pointing to communicate wants
18–24 Months
Play initiation — beginning simple play sequences independently
2–3 Years
Social initiation — approaching peers, offering toys, greeting familiar people
3–4 Years
Communication initiation — spontaneous commenting, asking questions, sharing experiences
4–6 Years
Task initiation — beginning assigned activities with minimal prompting
6–12 Years
Cognitive initiation — generating ideas, planning projects, self-starting complex sequences
Your child is here — capable of the skill, but struggling with the starting. The 9 materials on this page target this specific gap.
Initiation difficulties commonly co-occur with: ADHD (activation/motivation pathway) • Anxiety (fear-based initiation blocking) • Motor Planning Disorders (sequencing the first step) • Language Disorders (communication initiation specifically) • Autism Spectrum Conditions (across all initiation types)
Clinically Validated. Home-Applicable. Parent-Proven.
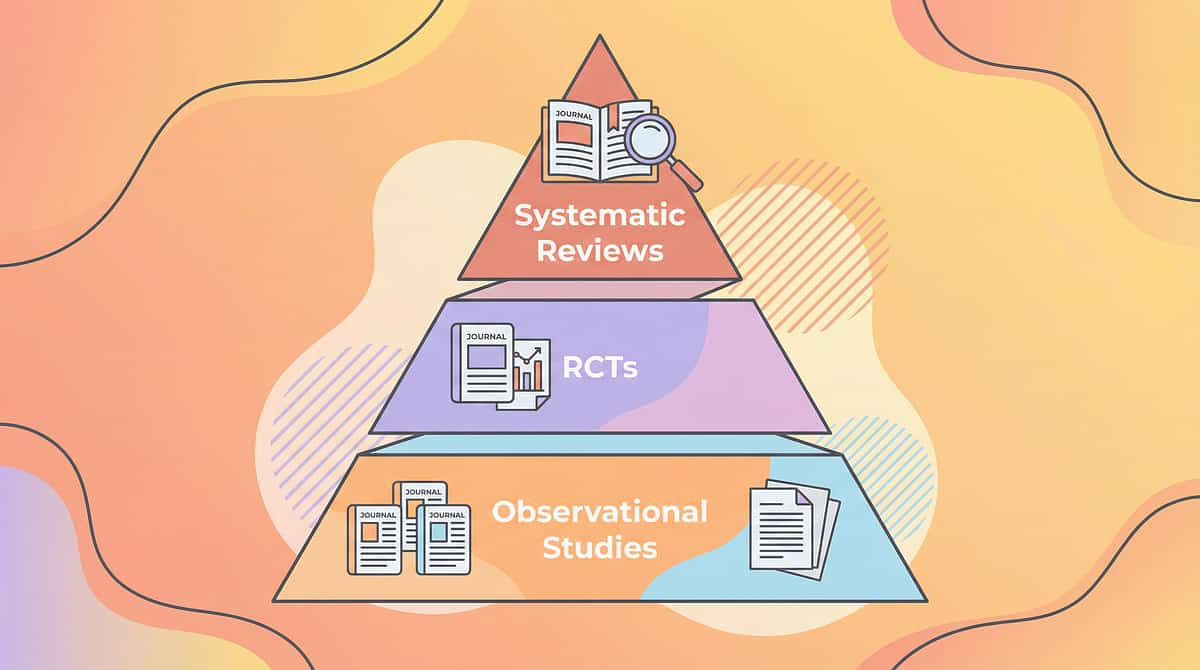
Level II Evidence — Systematic Reviews, Multiple Controlled Studies & Clinical Consensus
The materials presented on this page are drawn from three converging evidence streams: (1) Applied Behavior Analysis (ABA) research on antecedent interventions and motivating operations; (2) Speech-Language Pathology evidence on communication temptation and mand training; and (3) Occupational Therapy research on visual supports, environmental structuring, and executive function scaffolding.
Koegel LK et al. (2016)
Pivotal Response Treatment for ASD — evidence-based approaches to increasing initiation across communication and play domains
NCAEP Report (2020)
Visual supports, antecedent interventions, and self-monitoring classified as evidence-based practices for autism
PRISMA Review (2024)
16 articles from 2013–2023 confirm structured intervention meets evidence-based criteria for children with ASD (PMC11506176)
Meta-Analysis (2024)
Across 24 studies, structured intervention effectively promoted social skills, adaptive behavior, and functional independence (PMC10955541)
Across 20M+ exclusive 1:1 therapy sessions, the Pinnacle Blooms Network has tracked initiation progression through the GPT-OS® Daily Living & Independence Index, documenting systematic improvement from prompted initiation → cued initiation → self-cued initiation → independent initiation → generalized self-starting.
Confidence Level: 80% — Strong evidence with multiple evidence streams converging (PMC11506176 | PMC10955541 | PMC9978394 | Koegel LK et al., 2016 | NCAEP 2020)

Material-Based Initiation Scaffolding: Building External Start Signals
Clinical Definition:Initiation deficit / Task initiation difficulty / Self-starting impairment — A specific executive function difficulty where children struggle to independently begin actions, conversations, tasks, or play — even when they possess the skills to complete the activity once started.
This technique uses 9 categories of physical materials and environmental setups to create external starting cues for children who lack reliable internal "go signals." The approach is based on a fundamental principle: if the brain's internal start signal is weak, we build external start signals that the child can see, hear, touch, and follow. Over time, the child internalizes these cues and begins to self-start without them.
These children are responders rather than initiators — able to follow, continue, and complete, but unable to begin without external prompting. The materials systematically address five categories of initiation: task initiation, social initiation, communication initiation, play initiation, and problem-solving initiation.
External Cueing Systems
Visual schedules, timers, choice boards that show the child WHAT and WHEN to start
Motivation-Based Initiation
Mand training and sabotage setups that leverage DESIRE to spark starting
Social Scripting
Conversation starters and play scripts that provide the WORDS and STEPS to begin
Metacognitive Tools
Self-monitoring checklists that build AWARENESS of the starting process itself

This Technique Crosses Therapy Boundaries
Because the brain doesn't organize by therapy type, initiation difficulty requires a converged, multi-disciplinary approach. Every major pediatric therapy discipline contributes uniquely to building initiation capacity.
Applied Behavior Analysis (ABA) — Lead Discipline
ABA provides the foundational science of antecedent interventions, motivating operations, and systematic prompt fading. Mand training (Material 5) and sabotage/communication temptation (Material 6) are pure ABA interventions.
Speech-Language Pathology (SLP) — Co-Lead
SLP addresses communication initiation specifically — the child who has words but won't use them first. Conversation starter cards (Material 2), mand training (Material 5), and social scripts (Material 7) draw directly from SLP evidence.
Occupational Therapy (OT)
OT contributes visual supports, environmental structuring, and the sensory-motor interface of initiation — helping children who struggle with the motor planning component of starting. Timer tools (Material 4) address occupational performance.
Special Education (SpEd)
SpEd provides task analysis, self-monitoring frameworks (Material 8), and academic initiation strategies. The progression from external to self-monitoring originates from SpEd research on metacognition and self-regulation.
NeuroDevelopmental Pediatrics
Pediatric neurology provides the neurological framework — understanding which brain regions are involved, monitoring medication effects on initiation, and identifying when assessment is needed.
"At Pinnacle Blooms, the FusionModule™ within GPT-OS® coordinates all five disciplines into a single converged pathway — because initiation difficulty doesn't belong to one therapy room. It crosses all of them."

Precision Targets — This Isn't a Random Activity
Every material on this page is mapped to specific, measurable initiation targets. Understanding what you're building toward helps you recognize progress when it happens.
Child checks visual schedule independently
→ begins first task without prompt
Child selects conversation starter card
→ approaches peer unprompted
Child points to choice board
→ engages in selected activity immediately
Child marks own self-monitoring checklist
→ demonstrates metacognitive awareness of own starting behavior
9 Materials That Build the Bridge From Waiting to Starting
Each of these 9 materials has been selected from the Pinnacle Blooms 128 Canon Materials database and mapped against 687 clinically verified products. Together they address every type of initiation difficulty across all learning modalities.
# | Material | Purpose | Price Range | DIY? | |
1 | Visual Schedule Cards & First-Then Boards | Externalizes the "what to start" cue | ₹150–500 | ✅ | |
2 | Conversation Starter Cards | Ready-made opening phrases for social initiation | ₹100–400 | ✅ | |
3 | Choice Boards & Option Selection Materials | Transforms initiation into simple selection | ₹100–350 | ✅ | |
4 | Timer & Visual Countdown Tools | Creates unambiguous external start signals | ₹300–800 | ✅ | |
5 | Request/Mand Training Materials | Leverages motivation to drive initiation | ₹200–600 | Partial | |
6 | Sabotage & Incomplete Activity Setups | Creates naturalistic need for initiation | ₹0–200 | ✅ | |
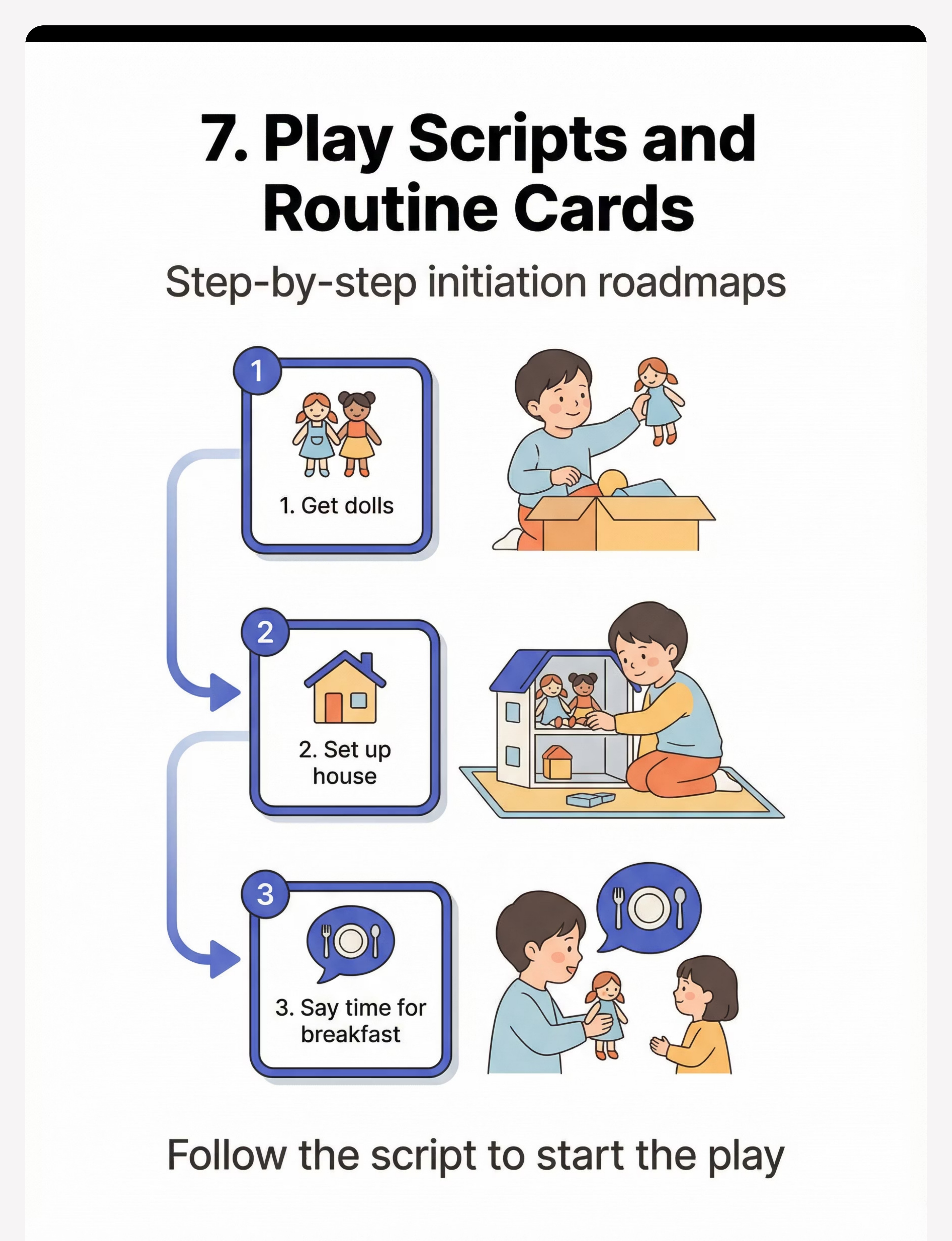
7 | Play Scripts & Initiation Routine Cards | Step-by-step starting sequences | ₹150–400 | ✅ | |
8 | Self-Monitoring Checklists | Builds metacognitive awareness of starting | ₹50–200 | ✅ | |
9 | Cause-Effect Toys & Action-Response Materials | Teaches "when I start, something happens" | ₹300–1,000 | Partial |
Total Investment: ₹1,350–4,450 for comprehensive setup | Essential Starters: Materials 1, 2, 3 (₹350–1,250) | 7 of 9 materials can be created at zero cost using household items

Zero-Cost Alternatives — Because Every Family Deserves Access
"The Pinnacle Blooms Consortium believes that evidence-based intervention should never be gated by budget. Every material on this page has a zero-cost DIY alternative that maintains therapeutic efficacy. The science is in the strategy, not the price tag."
Visual Schedule Cards
Print pictures from free image banks (ARASAAC, OpenSymbols). Arrange on a cardboard strip with tape or Velcro. Draw simple pictures if no printer is available.
Conversation Starter Cards
Write opening phrases on index cards: "Want to play?" "What are you doing?" "Can I join?" "Look at this!" Practice in safe situations first.
Choice Boards
Cut pictures from magazines or draw 2–4 activity options on cardboard. Teach: "Pick one." Accept any selection method — point, touch, gaze.
Timer Tools
Use phone timer, sand timer (₹50–100), or count down aloud: "5… 4… 3… 2… 1… GO!" Establish routine: countdown ends = action begins.
Mand Training Setup
Identify 3–5 powerful motivators your child loves. Place them visible but out of reach (high shelf, closed clear container). Wait for ANY initiation attempt. Immediately reinforce.
Sabotage Setups
Give puzzle with one piece missing. Put paint out with lid still on. Serve snack in an unopenable container. The "problem" creates a need for the child to initiate communication.
Play Scripts
Write 3–5 step scripts on paper: "1. Get dolls 2. Set up house 3. Say 'time for breakfast.'" Use pictures for non-readers. Tape near play area for reference.
Self-Monitoring Checklists
Create a chart: "Things I Started Myself Today" with checkbox rows. Celebrate every check mark. Count progress over time.
Cause-Effect Learning
Any toy that responds to action works: light switches, water play (pour → splash), ball ramp (push → roll → crash). The principle is what matters.

Safety First — The Clinical Guardrails
✅ DO
- Distinguish "can't start" from "won't start" — initiation deficit is neurological, not defiance
- Start with the child's strongest modality (visual learner → visual schedules first)
- Celebrate ALL initiation attempts, even partial ones
- Fade supports gradually — never remove all cues suddenly
- Maintain the child's dignity — never shame for not starting
- Ensure the child always has at least one way to communicate needs
- Keep tracking positive — celebrate progress, not perfection
❌ DON'T
- Don't punish lack of initiation — it increases anxiety and worsens the deficit
- Don't withhold basic needs during mand training — only use non-essential motivators
- Don't overwhelm with too many choices — start with 2–3 options maximum
- Don't force initiation during high-stress moments — read the child's state first
- Don't compare to neurotypical peers — each child's timeline is their own
- Don't create complete dependence on any single support — vary approaches
- Don't use timers punitively — they should signal opportunity, not threat
🔴 Red Flags — Seek Professional Help If: Complete inability to start anything without physical prompting • Initiation difficulties combined with significant skill regression • Extreme anxiety or distress when any initiation is expected • No response to any initiation supports after 4+ weeks of consistent use • Initiation difficulty significantly worsening over time
FREE National Autism Helpline:📞9100 181 181 — 18+ languages, 24×7

Preparing Your Home Initiation Station
The Initiation Zone
Designate one clear, uncluttered space with defined boundaries (specific table, corner, or mat). Visual schedule posted at child's eye level. Choice board accessible and within reach. Timer visible within child's sight line. 2–3 motivating items positioned strategically — visible but requiring initiation to access.
Reduce Competing Stimuli
Turn off background TV/music during initiation practice. Remove toys/items not part of the current session. Ensure other family members understand "initiation practice time." Minimize transitions — the child stays in one space.
Position Yourself
Sit at child's level, to the side (not across). Be close enough to respond instantly to any initiation attempt. Have reinforcers ready within YOUR reach (not the child's). Phone on silent — your response timing matters.
Session Duration
Total: 10–20 minutes maximum. Active initiation practice: 5–10 minutes. Start with 3–5 initiation opportunities per session. Increase gradually based on success, not calendar.

Before You Begin — Is Your Child Ready Right Now?
Readiness Check
Before beginning any initiation session, run through this quick readiness check. A session that starts right is worth ten sessions that start wrong.
✅ Readiness Indicators — Check All That Apply
- Child is calm and regulated (not in meltdown, not drowsy, not ill)
- Child has had basic needs met (fed, rested, comfortable)
- Child shows some environmental awareness (looking around, not fully zoned out)
- No major transitions happened in the last 15 minutes
- Preferred motivators are identified and accessible to you
- Your own emotional state is calm and patient (your regulation matters)
- Time buffer exists — no rushing to the next appointment
5+ Checks = GO ✅
Proceed to Step 1: The Invitation
3–4 Checks = MODIFY ⚠️
Use simplified version — one material, 2–3 initiation opportunities, heavy scaffolding
0–2 Checks = POSTPONE ⏸️
Offer calming activity instead. Try again when conditions improve. A postponed session is better than a failed one.

Step 1 — The Invitation (30–60 seconds)
ACT III: Execution
"Hey [child's name], look what I have! Want to see something fun?" — Place one motivating item in view, within child's sight but slightly out of reach. Sit at their level. Smile. Wait.
Body Language Guidance
- Relaxed, open posture — no crossed arms, no hovering
- Eye contact available but not demanded
- Animated facial expression — model the energy of "starting"
- Hands visible — show the materials playfully
What Acceptance Looks Like
- Child looks at the materials
- Child moves toward you or the materials
- Child reaches, points, or vocalizes
- Child makes any movement that breaks the passive stance
What Resistance Looks Like
- Child turns away, closes eyes, or moves further → MODIFY: reduce demand, offer simpler choice
- Child becomes distressed → POSTPONE: this is not the right moment
Timing: 30–60 seconds. If no response, gently reposition the motivating item or try a different one. Two invitation attempts maximum before moving to modified approach.

Step 2 — The Engagement (1–3 minutes)
The child has shown interest. Now introduce the first material. Choose ONE of the 9 materials based on your child's strongest modality and today's goal.
Path A — Visual Schedule
For task initiation: Place the visual schedule in front of the child. Point to the FIRST item. Say: "Look — first [activity]. Let's start!" Wait 5 seconds for the child to initiate.
Path B — Conversation Starters
For social initiation: Fan out 3 conversation starter cards face up. Say: "Pick one to say!" Wait for selection. Model if needed: pick up a card and read it aloud, then hand the deck back.
Path C — Choice Board
For any initiation type: Present board with 2–3 options. Say: "What do you want to do? Point to one." Accept ANY selection method — finger point, eye gaze, reaching, vocalizing.
Path D — Timer
For task initiation: Set timer for 10 seconds. Say: "When the timer goes — we start!" Count down together. Celebrate the start moment.
Path E — Mand Training
For communication initiation: Place preferred item in sight, in closed container. Wait. Look at the child expectantly. Count silently to 10. Reinforce ANY initiation attempt.
Engagement ✅
Child interacts with material → proceed to Step 3
Tolerance ⏳
Child watches but doesn't act → provide one model, wait again
Avoidance ↩️
Child turns away → try different material or postpone

Step 3 — The Initiation Moment (3–5 minutes)
The Core Principle: This is where the child INITIATES. Your job is to create the opportunity, then WAIT. The hardest part for parents is the waiting. Count silently. Give 5–10 seconds of pure wait time. Resist the urge to help, prompt, or fill the silence.
What Counts as Initiation — Accept ALL of These
- Reaching for materials
- Looking at the visual schedule
- Pointing to a choice
- Vocalizing (even non-words)
- Moving toward the activity
- Picking up a conversation card
- Pressing the timer start button
- Making any request gesture (sign, PECS, AAC)
Common Parent Errors
- ❌ Prompting before the wait time is up
- ❌ Completing the initiation step for the child
- ❌ Accepting only "perfect" initiation (verbal, specific, full sentence)
- ❌ Showing frustration during the wait
- ✅ CORRECT: Wait, watch, accept any attempt, celebrate immediately

Step 4 — Repeat & Vary (3–5 minutes)
Target Repetitions: 3–5 initiation opportunities per session (quality over quantity)
1
Same material, different activity
Visual schedule → different first task
2
Different material, same goal
Switch from choice board to conversation cards
3
Same principle, natural context
Practiced initiation → now at snack time
Satiation Indicators — When to Stop: Child's response time increasing significantly • Child becoming restless, looking away, stimming more • Engagement quality dropping (mechanical responses vs. genuine initiation) • 5 initiation opportunities completed successfully
"3 genuine initiations are worth more than 10 prompted ones. Stop while it's still working."
Step 5 — Reinforce & Celebrate (Ongoing)
Reinforcement Timing: Within 3 seconds of initiation attempt. Speed matters more than magnitude.
"You STARTED that! You did it all by yourself!"
"Look at you — you began without anyone telling you!"
"That was YOUR idea to start. I love that!"
Natural Reinforcement
The activity itself is the reward — child initiated play → play happens
Social Reinforcement
High-five, hug, specific verbal praise naming the behavior
Token Economy
Sticker/star chart leading to preferred activity
Tangible
Preferred snack item (especially for early stages of training)
"Celebrate the ATTEMPT, not just the SUCCESS. A child who reaches toward the materials but doesn't quite complete the initiation has done the hardest part — they've begun to fire that internal start signal. That attempt deserves the same celebration as a complete initiation."
Step 6 — The Cool-Down (1–2 minutes)
Cool-Down Activity
- Child helps put materials away (this IS an initiation opportunity!)
- 1 minute of preferred calming activity (music, quiet play, movement break)
- Simple sensory regulation activity (deep breaths, hand squeeze, gentle rocking)
Transition to Next Activity
- Preview what comes next: "Now we're going to have snack. What do you want?" (another embedded initiation opportunity)
- Use visual schedule if available to show transition
If Child Resists Ending
- Validate: "I know, this was fun! We'll do it again tomorrow."
- Use timer: set 1-minute visual timer for transition
- Offer choice: "Do you want to clean up toys first or put away cards first?" (initiation through choice)

Record It Now — Within 60 Seconds
Data captured within 60 seconds of a session is 10× more accurate than data recalled at bedtime. Your quick tally today builds the evidence base that drives your child's therapy plan tomorrow.
Initiation Attempts Today
Total opportunities presented during the session
Successful Initiations
Any attempt that began without prompting — count all forms
Best Moment
One sentence — what worked? What did you see? What surprised you?
📱 GPT-OS® In-App Tracker
pinnacleblooms.org/tracker — feeds directly into Daily Living & Independence Index
📄 Downloadable PDF
Weekly Initiation Tracker — print and keep on the fridge
📝 Simple Notebook
Date + number of unprompted starts + one line of notes
When you track through the Pinnacle system, your data feeds directly into your child's Daily Living & Independence Index, enabling the TherapeuticAI® to adjust intervention recommendations in real-time.

When It's Not Working — Troubleshoot Before You Quit
"My child won't even look at the materials."
The materials aren't motivating enough. Find what your child LOVES (specific character, food, sensory experience) and use THAT as the initiation target. The material is the vehicle — motivation is the fuel.
"My child waits 10 seconds and then I give in."
Your child has learned your pattern. Vary your wait time (7, 12, 5, 15 seconds). Commit: no prompting until the wait time is up, even if it's uncomfortable.
"It works at home but not at school."
Generalization takes time. Share your initiation materials with teachers/therapists. Use the same visual schedule format across settings. Consistency across caregivers multiplies impact.
"My child initiates with me but not with peers."
Peer initiation is harder — it has more uncertainty. Practice conversation starter cards with siblings or familiar children first. Role-play peer approaches at home before real situations.
"We've been doing this for 3 weeks with no progress."
Check: Are you waiting long enough? Are motivators truly motivating? Is the demand matched to ability? Consider a different material type. If no progress after 6 weeks of consistent daily practice, consult your Pinnacle therapist.
"My child only initiates for food/preferred items."
This is EXPECTED and GOOD at early stages. Motivation-based initiation (mand training) is the entry point. Once reliable initiation for preferred items is established, you systematically expand to less preferred activities.
One Technique, Many Children — Adapt to Yours

🟢 Ages 2–4 / Pre-verbal / Early Learners
- Start with Material 9 (cause-effect toys) — the most concrete initiation form
- Use Material 3 (choice boards) with only 2 options using real objects, not pictures
- Accept ANY initiation form: reach, point, gaze, vocalization, body movement
- Sessions: 5 minutes maximum, 2–3 initiation opportunities

🔵 Ages 4–7 / Emerging Language
- Start with Material 1 (visual schedules) + Material 5 (mand training)
- Add Material 2 (conversation starters) when 1-word initiations are consistent
- Begin Material 8 (self-monitoring) with adult support for checkbox marking
- Sessions: 10 minutes, 3–5 initiation opportunities

🟣 Ages 7–12 / Verbal / School-Age
- Full range of all 9 materials available
- Emphasize Materials 7 (play scripts) + 8 (self-monitoring) for metacognitive development
- Add Material 6 (sabotage) for naturalistic practice
- Sessions: 15–20 minutes, 5–7 initiation opportunities
Sensory Profile Adjustments: Sensory-seeking child → cause-effect toys with strong sensory feedback (lights, sounds, vibration) • Sensory-avoiding child → quiet choice boards and conversation cards, minimize sensory load • Mixed profile → alternate between high-stimulation and low-stimulation materials within session
ACT IV: The Progress Arc
Weeks 1–2: The Foundations
The first two weeks are about building the pattern — establishing routine, building trust with the materials, and capturing those first precious unprompted moments. Progress may feel slow, but neural pathways are being laid.
Child begins to tolerate materials in their environment
First unprompted reaches, glances, or movements toward materials appear
Pattern recognition begins
Child starts to anticipate the routine — their nervous system is learning what comes next
Realistic Milestones
✅ Child looks at visual schedule when placed in view (even briefly) ✅ Child touches or manipulates materials offered ✅ At least 1 unprompted initiation per session by end of Week 2 ✅ Child tolerates the 5–10 second wait without significant distress
Parent Milestone: "You may notice you're getting better at waiting. Your comfort with the silence is growing. That's YOUR neural pathway strengthening too." — Progress: 25% 🟧🟧🟧🟧░░░░░░░░░░░░

Weeks 3–4: Momentum Is Building
Initiation attempts are becoming more frequent and faster. You may notice your child beginning to use materials with less setup from you. This is consolidation in action — the neural pathway is strengthening and becoming more automatic.
✅ Realistic Milestones
- 2–3 unprompted initiations per session consistently
- Child begins checking visual schedule without being directed to it
- Response time shortening — less wait time needed before action
- At least 1 initiation outside of structured practice (mealtime, play, sibling interaction)
📊 Behavioral Consolidation Markers
- Child approaches materials independently before session begins
- Child uses conversation starters with familiar adults beyond parent
- Self-monitoring checklist generating genuine pride reactions
About Week 3 Plateaus: A plateau around Week 3 is consolidation, not failure. The brain is integrating. Keep going.
Parent Milestone: "You may notice you're prompting less in daily life too. Your instinct to 'help them start' is being replaced with confidence that they CAN start." — Progress: 50% 🟧🟧🟧🟧🟧🟧🟧🟧░░░░░░░░

Weeks 5–8: The Shift to Self-Starting
This is the phase where the shift becomes visible to others — teachers comment, grandparents notice, therapists document. The child is no longer just responding to your setups; they're generating their own starts.
5+
Daily Initiations
without structured practice sessions
2+
Settings
initiation occurring across home, school, and community
3+
Strategies
different initiation strategies used independently by child
Generalization Indicators
Initiation appearing in novel situations (new playground, new people) • Child beginning to show initiative in non-trained contexts • Requesting help when stuck (problem-solving initiation)
Mastery Badge Criteria
When 4 of 6 mastery criteria are met consistently for 2+ weeks → MASTERY UNLOCKED. Your child is ready for multi-step task initiation, group social initiation, and independent problem-solving.
Progress: 75% 🟧🟧🟧🟧🟧🟧🟧🟧🟧🟧🟧🟧░░░░

You Did This. Your Child Grew Because of Your Commitment.
Five to eight weeks ago, you watched your child stand at the edge of everything — waiting, watching, capable but motionless. You chose to understand why. You learned the brain science. You gathered the materials. You sat on the floor and waited in those long, uncomfortable silences. You celebrated reaches that other parents wouldn't even notice. You tracked data when you were exhausted.
And now — your child starts things. Not every time. Not perfectly. But they START. They check the schedule. They pick up a card. They point to a choice. They reach for what they want. They say the first word. That is not a small thing. That is the ignition switch firing. That is a neural pathway that didn't exist eight weeks ago, built by your hands, your patience, and your refusal to accept that your child couldn't learn to begin.
Celebration Suggestion: Let your child choose a special activity today — and let THEM start it. Watch them initiate. Take a photo. Write the date. This is the day you'll look back on.
🏆 "Independent Initiation — Mastery Achieved" | Date: ___________
Even in Progress — Know When to Pause and Ask
⚠️ Safety Alert
🔴 Complete Regression
Child who was initiating stops entirely and returns to baseline passivity. May mean: Medical issue, sleep disruption, environmental stressor, medication change. Do: Pause practice, address underlying factors, consult therapist if persists more than 1 week.
🔴 Initiation Paired with Extreme Anxiety
Child initiates but shows panic signs (hyperventilation, crying, freezing immediately after). May mean: Anxiety disorder may be driving the difficulty, not just executive function. Do: Reduce all demand. Consult mental health professional. Do NOT push through anxiety.
🔴 Physical Symptoms
Headaches, stomach aches, or sleep disruption coinciding with increased initiation demands. May mean: Somatic stress response — the intervention may be too intensive. Do: Reduce session frequency and duration. Add calming activities before practice.
🔴 No Progress After 6+ Weeks
Consistent daily practice with no observable increase in initiation attempts. May mean: Underlying condition requiring different approach or professional assessment. Do: Book assessment — Call 9100 181 181.
🔴 Aggressive Behavior
Child becomes physically aggressive when initiation is expected. May mean: Demand exceeds current capacity; frustration tolerance is overloaded. Do: Immediately reduce all demand. Return to cause-effect toys (simplest initiation form). Consult BCBA.
Escalation Pathway: Self-resolve (adjust approach) → Teleconsult with Pinnacle therapist → In-center assessment
"If something feels wrong, pause and ask. Your parental intuition is a clinical instrument."
Where You Are — And Where You're Going
⬅ Prerequisite Techniques
- B-197: Grammar and Plurals (language foundations)
- B-195: Difficulty Retelling Stories (narrative initiation)
★ Current: B-198
9 Materials That Help When Child Can't Initiate
➡ Next-Level Options
- B-199: Child Can't Respond
- B-200: Difficulty with Transitions
- B-201: Task Completion Problems
- B-220: Social Approach Difficulties
↔ Lateral Alternatives
- K-940: Building Independence at Home
- K-955: Executive Function Strategies for Parents

More Executive Function Techniques Available
If you've assembled the 9 materials on this page, you already have the tools for B-199, B-200, and B-201. Each technique builds on the last — your investment compounds.

B-195: Difficulty Retelling Stories
Level: Intro | Visual supports for narrative initiation and story sequencing
B-196: Word Order Difficulty
Level: Core | Language cards for syntax and sentence formation

B-199: Child Can't Respond
Level: Core | Timer tools and response-building strategies — the complement to initiation
B-200: Difficulty with Transitions
Level: Core | Schedule boards and transition support materials

B-201: Task Completion Problems
Level: Advanced | Self-monitoring and task persistence strategies

B-220: Social Approach Difficulties
Level: Advanced | Social scripts and peer approach specialization

This Technique Is One Piece of a Larger Plan
Executive Function — the domain containing initiation — sits at the intersection of Communication, Social Skills, Adaptive Behavior, and Academic Readiness. When you build initiation, you build across all four of these domains simultaneously.
GPT-OS® Integration: "Connect with GPT-OS® to see your child's full profile across all 12 domains. Your AbilityScore® assessment maps exactly where your child stands — and where they're heading."
ACT V: Community & Ecosystem
From Other Parents Who Walked This Path
"He used to wait for everything. Wait for me to tell him to eat. Wait for me to say 'go play.' After three weeks with the visual schedule and timer, he walked to the breakfast table and sat down before I said a word. I cried. It seems so small, but it was everything."
— Parent, Pinnacle Blooms Network (Illustrative case; outcomes vary by child profile.)
"The conversation starter cards changed playground time completely. My daughter used to stand at the fence watching other children. Now she walks up holding a card that says 'Want to play?' She doesn't need the card anymore — but she carries it in her pocket like a lucky charm."
— Parent, Pinnacle Blooms Network (Illustrative case; outcomes vary by child profile.)
"He raised his hand in class for the first time. His teacher called me. We both cried."
— Parent, Pinnacle Blooms Network (Illustrative case; outcomes vary by child profile.)

You Don't Do This Alone
Pinnacle Parent Community
- 📱 WhatsApp Support Groups by region and language
- 🌐 Online Parent Forums: pinnacleblooms.org/community
- 📅 Monthly Parent Webinars on Executive Function Strategies
- 👨👩👧 Family Support Programs: K-881 (Parents After Diagnosis)
Free Downloadable Resources
- 📄 Initiation Tracker PDF — weekly session log
- 📘 Family Guide — Explaining Initiation to Caregivers
- 🎥 Parent Training Video Series
Get Support Now
📞FREE National Autism Helpline: 9100 181 181
18+ languages • Available 24×7
18+ languages • Available 24×7

80+ Pinnacle Blooms Centers Across India
Whether you need a comprehensive assessment, weekly therapy sessions, or a single consultation to get your home practice on track — Pinnacle Blooms has a center near you. Our 80+ centers are staffed by the same consortium of specialists who validated every technique on this page.
AbilityScore® Assessment
Comprehensive developmental baseline across all 12 domains — including initiation severity scoring and personalized intervention mapping
Behavioral Therapy (ABA)
Initiation protocols, mand training, antecedent interventions delivered by certified BCBAs
Speech Therapy
Communication initiation, conversation starter training, AAC integration for non-verbal children
Occupational Therapy
Task initiation, environmental structuring, sensory-motor interface for initiation difficulty
Parent Training
Home implementation coaching through the EverydayTherapyProgramme™ — your daily practice guided by clinicians
Special Education
Academic initiation, self-monitoring, school-based strategies and teacher consultation
The Science Behind Every Material on This Page
Research Library
Every recommendation on this page is anchored in peer-reviewed research and clinical consensus. Below are the primary citations that form the evidence foundation for these 9 materials.
Barkley RA (2012)
Executive Functions: What They Are, How They Work, and Why They Evolved. Guilford Press. Foundational framework establishing task initiation as a discrete, trainable executive function.
Ozonoff S et al. (1991)
Executive function deficits in high-functioning autistic individuals. Journal of Child Psychology and Psychiatry. Seminal research documenting initiation difficulties specific to autism.
Koegel LK et al. (2016)
Pivotal Response Treatment for Autism Spectrum Disorders. Paul H. Brookes Publishing. Evidence-based approaches to increasing initiation through motivation and natural reinforcement.
NCAEP Evidence-Based Practices Report (2020)
National Clearinghouse on Autism Evidence and Practice. Visual supports, antecedent interventions, and self-monitoring classified as evidence-based practices. PubMed: PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Across 24 studies, structured intervention effectively promotes social skills, adaptive behavior, and functional independence. PubMed: PMC10955541
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm structured intervention meets evidence-based criteria for children with ASD. PubMed: PMC11506176
WHO/UNICEF CCD Package (2023)
Care for Child Development. Age-specific evidence-based recommendations for caregivers implemented in 54+ countries. PubMed: PMC9978394
Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022)
Multi-disciplinary contributions to nurturing care. DOI: 10.1080/17549507.2022.2141327
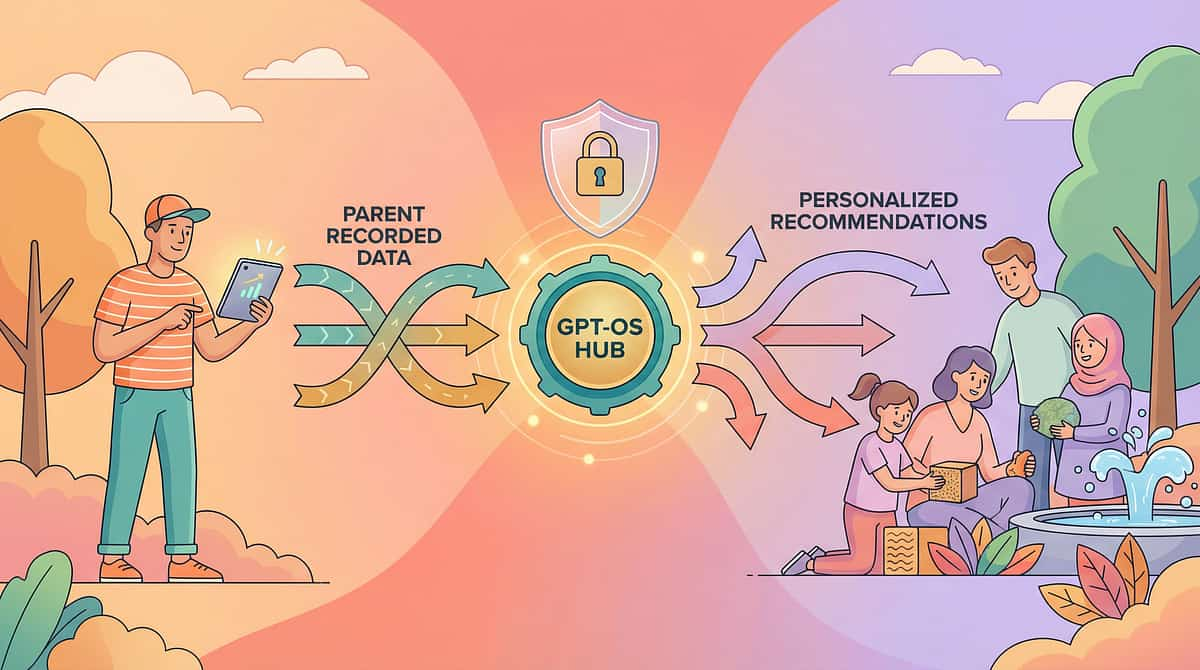
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
This technique page is one of 70,000+ intervention techniques within the GPT-OS® ecosystem — the end-to-end operating system governing diagnosis, prognosis, therapy design, execution, monitoring, and readiness outcomes in child development as one closed, accountable system.
Diagnostic Intelligence Layer
591+ structured observations across 349 skills and 79 developmental abilities
AbilityScore®
Patented universal developmental score (0–1000) — baseline, severity, longitudinal change
TherapeuticAI®
Therapy focus, intensity, sequencing, and escalation — under licensed human clinical authority
FusionModule™
Speech + OT + ABA + SpEd + Medical converged into a single therapeutic pathway
EverydayTherapyProgramme™
Clinical plans translated into daily home-executable micro-interventions
Closed-Loop Control
Observation → Score → Plan → Execute → Re-measure → Adapt
20M+
1:1 Sessions
97%+
Measured Improvement
80+
Centers
160+
Countries (Patents Filed)
"This is not software. This is therapeutic infrastructure."

Watch: 9 Materials That Help When Child Can't Initiate
Reel B-198
Executive Function Series — Episode 198
75 seconds
Meet our therapist demonstrating each of the 9 materials in action — watch how simple environmental setups can spark independent initiation in children who usually wait. This reel captures real initiation moments: the reach, the point, the first unprompted word.
Connected Reel: "9 Materials That Help When Child Can't Initiate" — from the 999 Reels Master Library | Pinnacle Blooms Network | Domain: Executive Function & Independence | Evidence base: NCAEP (2020) — Video modeling as evidence-based practice for autism

Consistency Across Caregivers Multiplies Impact
"If only one caregiver implements these strategies, progress is limited to one setting. When the whole family understands initiation support, the child's world opens up." (PMC9978394 — WHO CCD Package: Multi-caregiver training as critical for generalization)
Share on WhatsApp
Pre-formatted message with page link — techniques.pinnacleblooms.org/executive-function/child-cant-initiate-materials
Send via Email
Subject: "Something that will help [child's name] start things independently" — ready-to-send template included
Copy Link
techniques.pinnacleblooms.org/executive-function/child-cant-initiate-materials
📄 Family Guide (1-page PDF)
Simplified version for grandparents, aunts/uncles, school staff — core principles, no jargon
👵 "Explain to Grandparents" Version
Key principles in simple language. What initiation deficit is. How to wait. How to celebrate. How not to accidentally prompt.
👩🏫 Teacher Communication Template
Letter to school explaining initiation strategies with classroom adaptation suggestions — ready to personalize and send
Your Questions, Answered
ACT VI: The Close
Is initiation difficulty the same as laziness?
No. Initiation deficit is a neurological executive function challenge — not a character flaw, not defiance, not laziness. The child's prefrontal cortex struggles to generate the internal signal that begins action. They want to start but genuinely cannot activate the "go" pathway without external support.
How long until I see results?
Most families see initial signs of improved initiation within 2–3 weeks of consistent daily practice. Meaningful, generalized improvement typically emerges by weeks 5–8. Every child's timeline is different — progress depends on severity, consistency, and the match between materials and learning style.
Do I need all 9 materials?
No. Start with 2–3 that match your child's strongest modality. We recommend beginning with Visual Schedule Cards (Material 1), Conversation Starters (Material 2), and Choice Boards (Material 3) — available for ₹350–1,250 or zero cost as DIY.
Will my child become dependent on these supports?
The goal is systematic fading. External cues are the training wheels — they're meant to come off. As the child's internal initiation pathways strengthen, you gradually reduce external supports. This fading process is built into the protocol.
Can this be done alongside professional therapy?
Absolutely — and it should be. These materials are designed to EXTEND what happens in therapy sessions into daily home life. Share this page with your child's therapist to ensure alignment between home and clinic strategies.
My child initiates negative behaviors but not positive ones. Why?
Negative behaviors often have built-in motivation and immediate reinforcement — they get results fast. Positive initiation requires more cognitive effort with less immediate payoff. The materials on this page are designed to make positive initiation as motivating and immediately reinforcing as possible.
Is this appropriate for non-verbal children?
Yes. Visual schedules, choice boards, cause-effect toys, and mand training work without spoken language — using pictures, gestures, sign language, or AAC devices. Initiation doesn't require words — it requires action.
What if my child has both initiation AND response difficulties?
This is common. Work on initiation first (this page) — then move to B-199 (Child Can't Respond). Initiation is the more foundational skill because it activates the child's agency in the interaction.
Didn't find your answer?🤖 Ask GPT-OS® for AI-powered therapeutic guidance, or 📞Call 9100 181 181 — FREE National Autism Helpline, 18+ languages, 24×7

The First Step Is Yours
🟠 Start This Technique Today
GPT-OS® Guided Session Launcher — Begin with a personalized initiation protocol matched to your child's AbilityScore® profile. The system walks you through setup, session pacing, and data capture.
🔵 Book a Consultation
Schedule a comprehensive executive function assessment at your nearest Pinnacle Blooms center. Includes AbilityScore® baseline, initiation severity scoring, and personalized 12-week intervention plan.
⬜ Explore Next Technique
B-199: Child Can't Respond — Ready for the next step? Move to response initiation, the complement to self-starting. Your current materials already support this transition.
Validated by the Pinnacle Blooms Expert Consortium: OT • SLP • BCBA • SpEd • NeuroDev
Preview of 9 materials that help when child cant initiate Therapy Material
Below is a visual preview of 9 materials that help when child cant initiate therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!
The Pinnacle Promise
Pinnacle Blooms Network® — Expert Consortium
SLP • OT • BCBA • SpEd • NeuroDev Pediatrics • Clinical Research
"From fear to mastery. One technique at a time."
You arrived on this page watching your child stand at the edge. You leave knowing why — and knowing what to do about it. This is one technique in a library of 70,000+ interventions, each backed by evidence, validated by consortium, and built for your home. Your child's first step is the hardest — and the most beautiful. You have the tools now. Start today.
Medical Disclaimer: This content is educational and does not replace assessment by a licensed professional. Initiation difficulties may reflect various underlying conditions requiring comprehensive assessment. Intervention should be individualized based on the specific nature of initiation challenges. Individual results vary based on child profile, consistency of implementation, and underlying conditions. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Consult qualified professionals for personalized guidance.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All Rights Reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | GSTIN: 36AAGCB9722P1Z2 | ISO 13485: Medical Device QMS | ISO/IEC 27001: Information Security
Site: techniques.pinnacleblooms.org | Helpline: 9100 181 181 | Web: pinnacleblooms.org