
"Stop doing that." "Don't hit." "No, stop throwing things."
You've said these words a hundred times today. And it isn't working. D-360: Teaching What TO Do — the behavioral shift that replaces "stop" with skill.

Every Family Navigating This Is Part of a Global Reality
You are among millions of families navigating this exact challenge — across India, across 70+ countries. The question is not whether your child can learn alternatives. The research says they can. The question is which materials help them learn fastest.
1 in 36
Children with Autism (USA)
CDC, 2023. Replacement behavior teaching is core to every ABA protocol.
70–80%
Respond to Replacement Teaching
Meta-analysis, Journal of Positive Behavior Interventions. Challenging behaviors reduced through functional replacement teaching.
21M+
Sessions Delivered by Pinnacle
97%+ measured improvement. GPT-OS® Real-World Evidence Database.
Across Pinnacle's 70+ centers, teaching "what TO do" is the #1 behavioral intervention request from families in every city, every income level, every diagnosis profile. BACB Standards: Functional Communication Training has the strongest evidence base of any behavioral intervention for reducing challenging behaviors in autism. | bacb.com
Your Child Isn't Choosing the Problem Behavior. They're Using the Only Tool They Have.
The Neuroscience
All behavior serves a function. The prefrontal cortex — the brain's "what should I do?" decision center — requires explicit learning to generate socially appropriate alternatives. Children with autism frequently show differences in:
- Prefrontal-limbic connectivity — the pathway linking impulse to alternative selection
- Working memory load — under stress, the brain cannot retrieve abstract verbal rules
- Inhibitory control — the neurological "brake" that requires practiced alternatives to engage
The behavioral vacuum principle: When a behavior is suppressed without a replacement, the same neurological need simply finds a new behavior. The "whack-a-mole" effect parents describe is real neurological evidence of an unmet function.
Plain English for Parents
Your child hits because hitting works — it ends conflict, gets attention, or escapes a demand. Their brain has learned: "This behavior produces the outcome I need."
You cannot simply remove that tool. You must install a better one.
When you teach an alternative that works just as well — or faster — the brain naturally shifts. Not because the child is "choosing to behave." Because the new pathway is more efficient.
Clinical Term: Functional Replacement Behavior Teaching | Differential Reinforcement of Alternative Behavior (DRA) — Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660

This Is a Developmental Skill Gap — Not a Character Problem
Many children with ASD are operating 18–36 months behind typical developmental norms in replacement behavior acquisition. This is not delay — this is the target. Below is the WHO developmental timeline for replacement behavior skills.
Age 2
Simple requests emerging — "More," "Help," basic gestures
Age 3
Turn-taking foundations | Waiting 30–60 seconds
Age 4
Basic problem-solving language | "I can ask"
Age 5
Multi-step alternative behaviors | Ask → Wait → Receive
Ages 6–8
Self-regulation with verbal mediation | Internal scripts
Ages 9–12
Generalized alternatives across all contexts
Comorbidity Awareness
Replacement behavior deficits commonly co-occur with: limited functional communication (expressive language gaps), sensory dysregulation, executive function differences, and anxiety. Your child is here. The 9 materials on this page help build the bridge to where they're going.
WHO Care for Child Development (CCD) Package: Age-specific evidence-based recommendations for caregivers — implemented in 54 low- and middle-income countries, including India. | PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
🏛️ Level I Evidence — Systematic Review + RCT-Supported
This is not an experimental approach. Teaching what TO do instead of what NOT to do is the most researched, most replicated, most endorsed intervention in pediatric behavior science. The 9 materials on this page are the delivery vehicles for that evidence.
Source | Finding | |
NCAEP Evidence-Based Practices (2020) | Functional Communication Training classified as an evidence-based practice for autism across all age groups | |
BACB Professional Standards | Differential Reinforcement of Alternative Behavior (DRA) — foundational behavioral intervention with decades of RCT support | |
Journal of Positive Behavior Interventions | 70–80% reduction in challenging behaviors when replacement behaviors are systematically taught | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based behavioral skill teaching shows significant outcomes in Indian pediatric population |
Evidence Badge: NCAEP 2020 | BACB Standards | WHO Aligned | PMC11506176 | PMC10955541 | PMC9978394 | DOI: 10.1007/s12098-018-2747-4

Technique D-360 | Behavior Support & Skill Building
What Is D-360: Teaching What TO Do?
Technique Identity
Formal Name: Replacement Behavior Teaching / Functional Communication Training
Parent-Friendly Alias: Teaching What TO Do
Code: D-360
Domain: Applied Behavior Analysis / Positive Behavior Support
Age Range: 2–12 years
Session Duration: Integrated throughout the day
Frequency: Continuous — every time the target situation arises
Parent-Friendly Alias: Teaching What TO Do
Code: D-360
Domain: Applied Behavior Analysis / Positive Behavior Support
Age Range: 2–12 years
Session Duration: Integrated throughout the day
Frequency: Continuous — every time the target situation arises
Definition
Teaching What TO Do is the proactive, science-backed practice of explicitly teaching children an appropriate alternative behavior that serves the same function as their challenging behavior. Rather than suppressing behavior through punishment or extinction alone, this approach identifies what the child is trying to achieve — attention, escape, access to something desired, or sensory input — and teaches a socially acceptable behavior that achieves the same outcome.
Canon Materials: Reinforcement Menus | Visual Supports | Communication Cards | Social Stories
Discipline Lead: BCBA/ABA Primary | SLP Co-lead | OT Supporting
Discipline Lead: BCBA/ABA Primary | SLP Co-lead | OT Supporting
The Entire Consortium Uses This — For Different Reasons
🔵 BCBA / ABA Therapist — Primary Lead
Conducts functional behavior assessment (FBA) to identify the function of challenging behavior. Designs the replacement behavior protocol. Trains parents in reinforcement delivery. Tracks data on replacement behavior acquisition and problem behavior reduction.
🟢 Speech-Language Pathologist — Co-Lead
Designs the communicative alternative. For children with limited verbal language: AAC device programming, PECS implementation, picture card vocabulary. Ensures the replacement behavior is communicatively accessible — not just behaviorally correct.
🟡 Occupational Therapist — Supporting
Addresses sensory and motor barriers to using the alternative behavior. If a child hits because of tactile defensiveness, the OT resolves the sensory trigger while the BCBA installs the communicative alternative. Designs calm-down kit components.
🟠 Special Educator — Generalization Lead
Ensures replacement behaviors taught in therapy transfer to school. Creates classroom versions of prompt cards, Instead Of charts, and reinforcement systems. Coordinates with teachers on consistent implementation.
🔴 NeuroDev Pediatrician — Clinical Oversight
Rules out medical factors contributing to challenging behavior (pain, sleep, medication effects). Provides diagnostic clarity on comorbid conditions affecting replacement behavior learning. Supervises clinical escalation decisions.
"The brain doesn't organize by therapy type. A child who hits because they can't communicate needs their SLP to give them a voice and their BCBA to make that voice more rewarding than the fist." — Pinnacle Blooms Consortium Clinical Lead

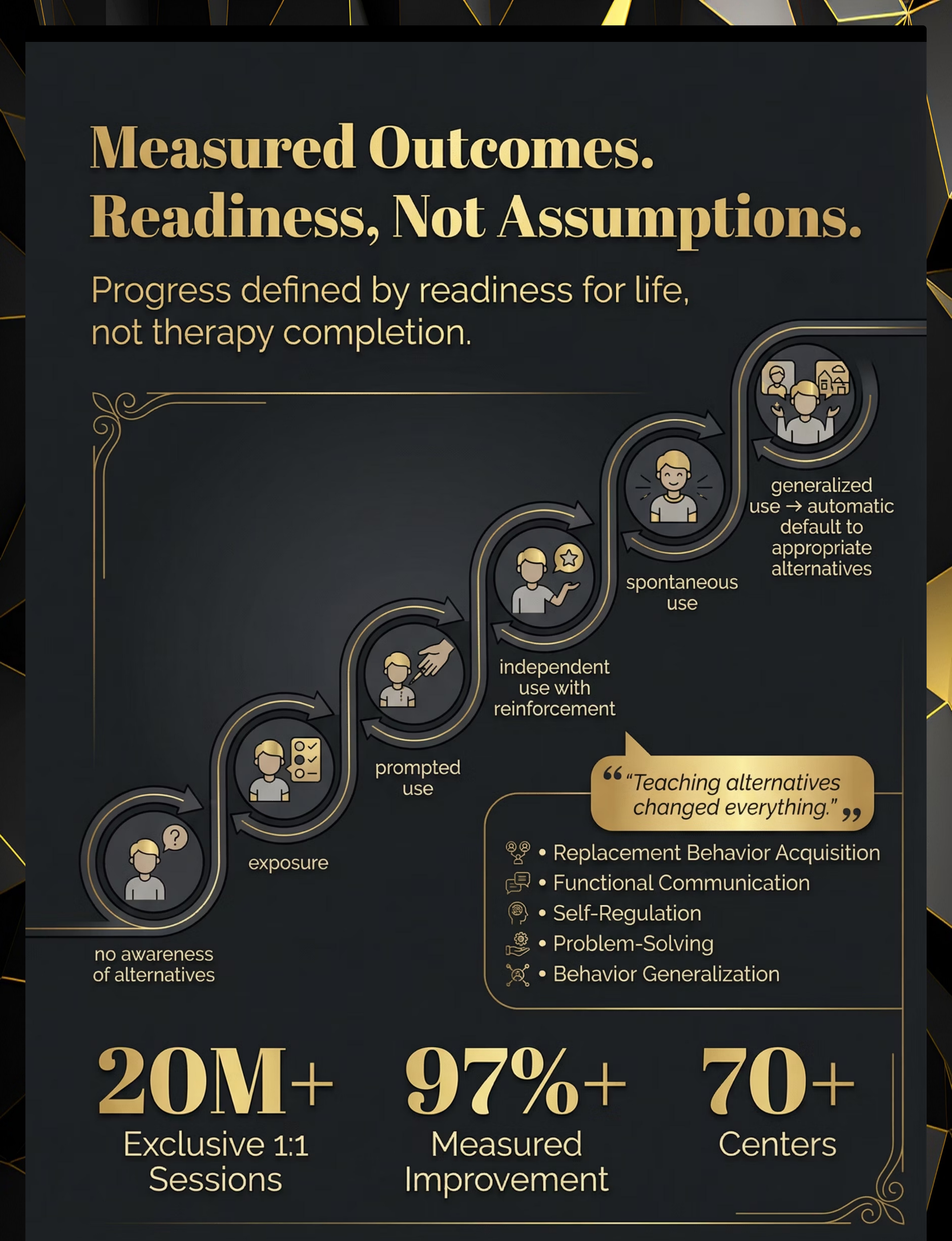
Precision Tool. Not a Random Activity.
D-360 is designed to hit specific developmental targets — from the immediate goal of replacement behavior acquisition all the way through to long-term independence and social inclusion.
Observable indicator of success: Child uses the alternative behavior — even once — in the same context where the problem behavior previously occurred. GPT-OS® Readiness Indexes track all five domains: Replacement Behavior Acquisition, Functional Communication, Self-Regulation, Problem-Solving, and Behavior Generalization. | PMC10955541

9 Materials. Clinically Chosen. Home-Ready.
These 9 materials span three functional categories — visual alternatives (Cards, Charts), practice tools (Puppets, Video), and reinforcement systems (Tokens, Rewards). A starter kit of ₹500–800 covers the essentials for most families.
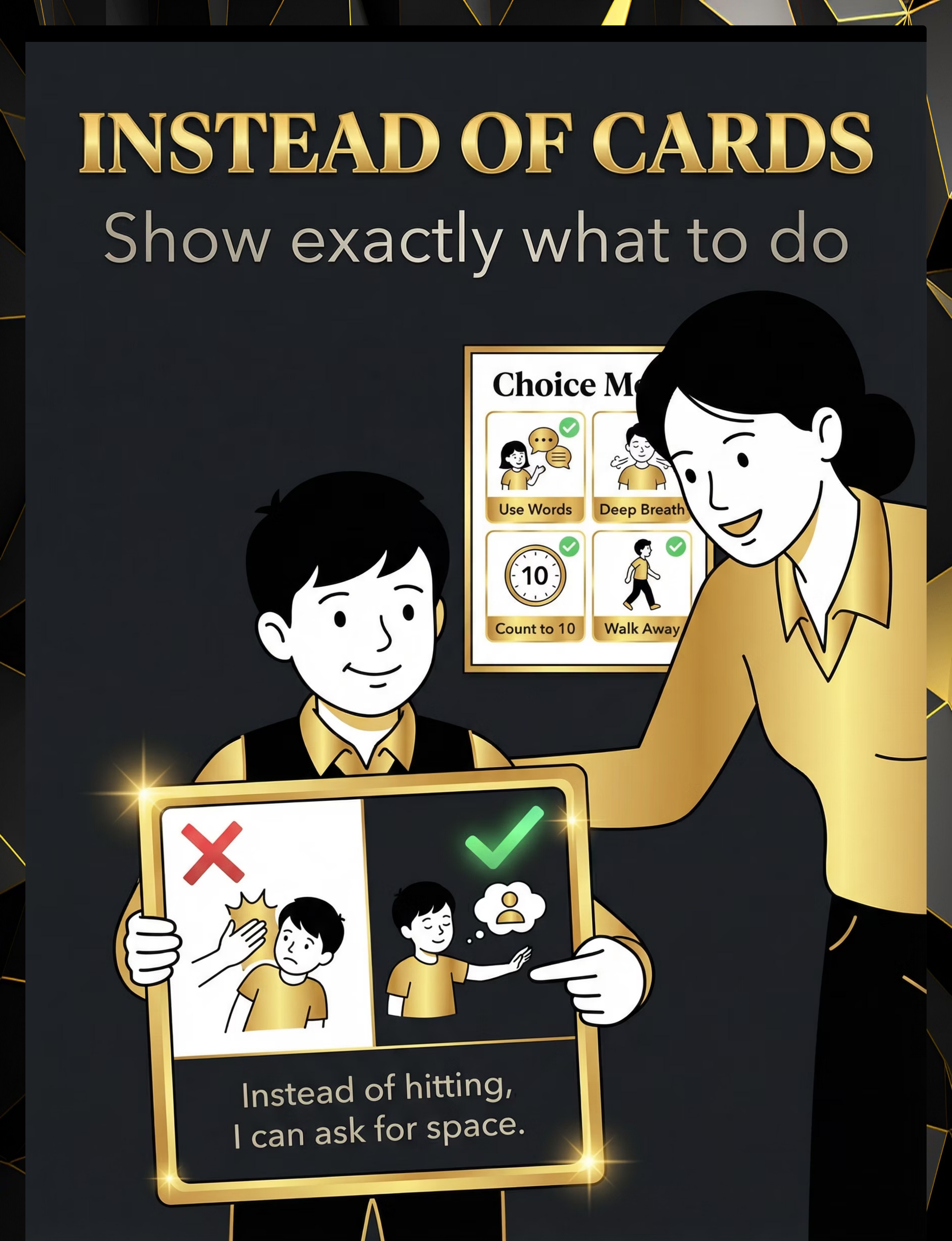
Instead Of Cards / Choice Board
Visual Supports — shows child what to do instead of the problem behavior. 🔍 Search Amazon.in

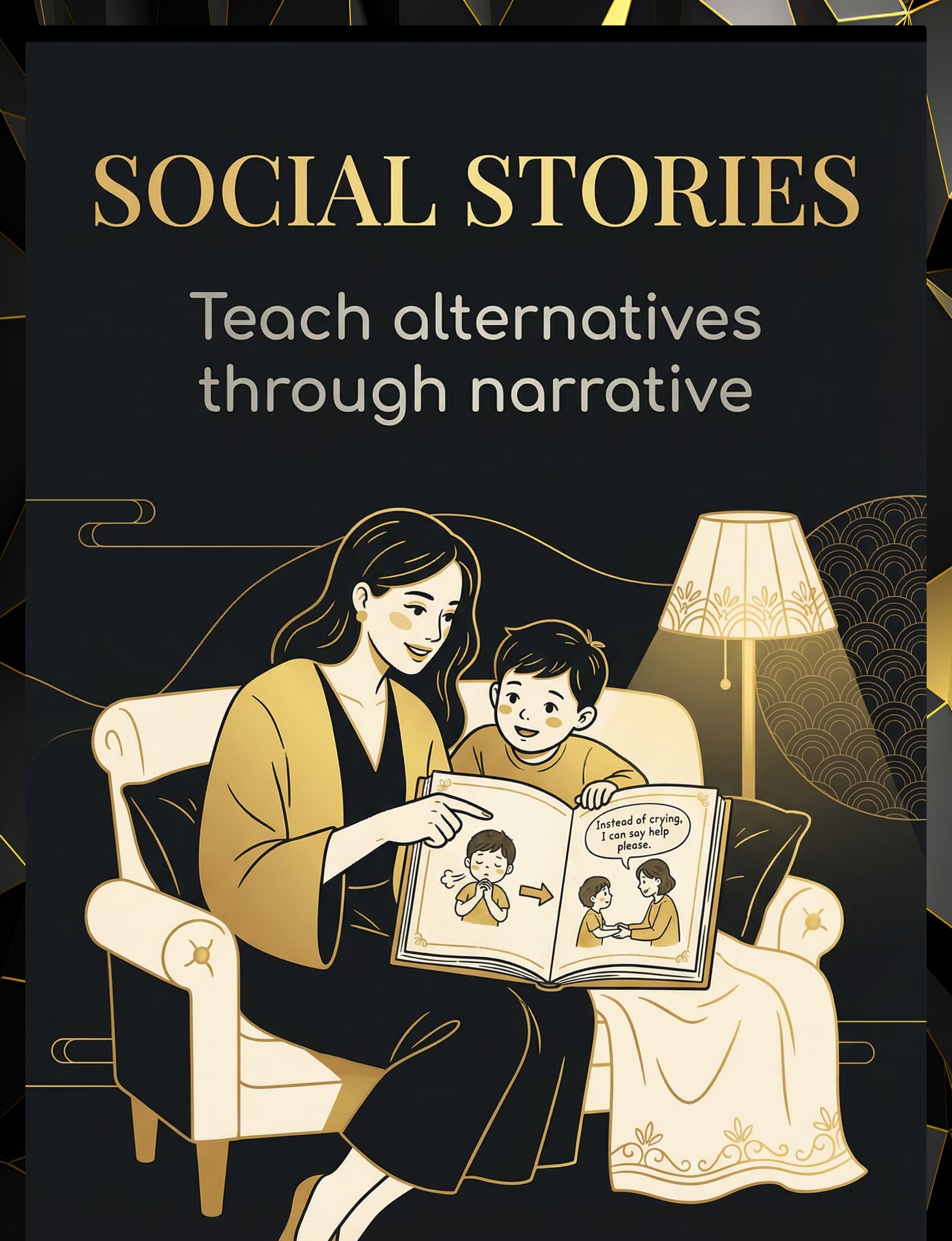
Social Story Books
Social Narratives — teaches behavior through relatable stories. 🔍 Search Amazon.in
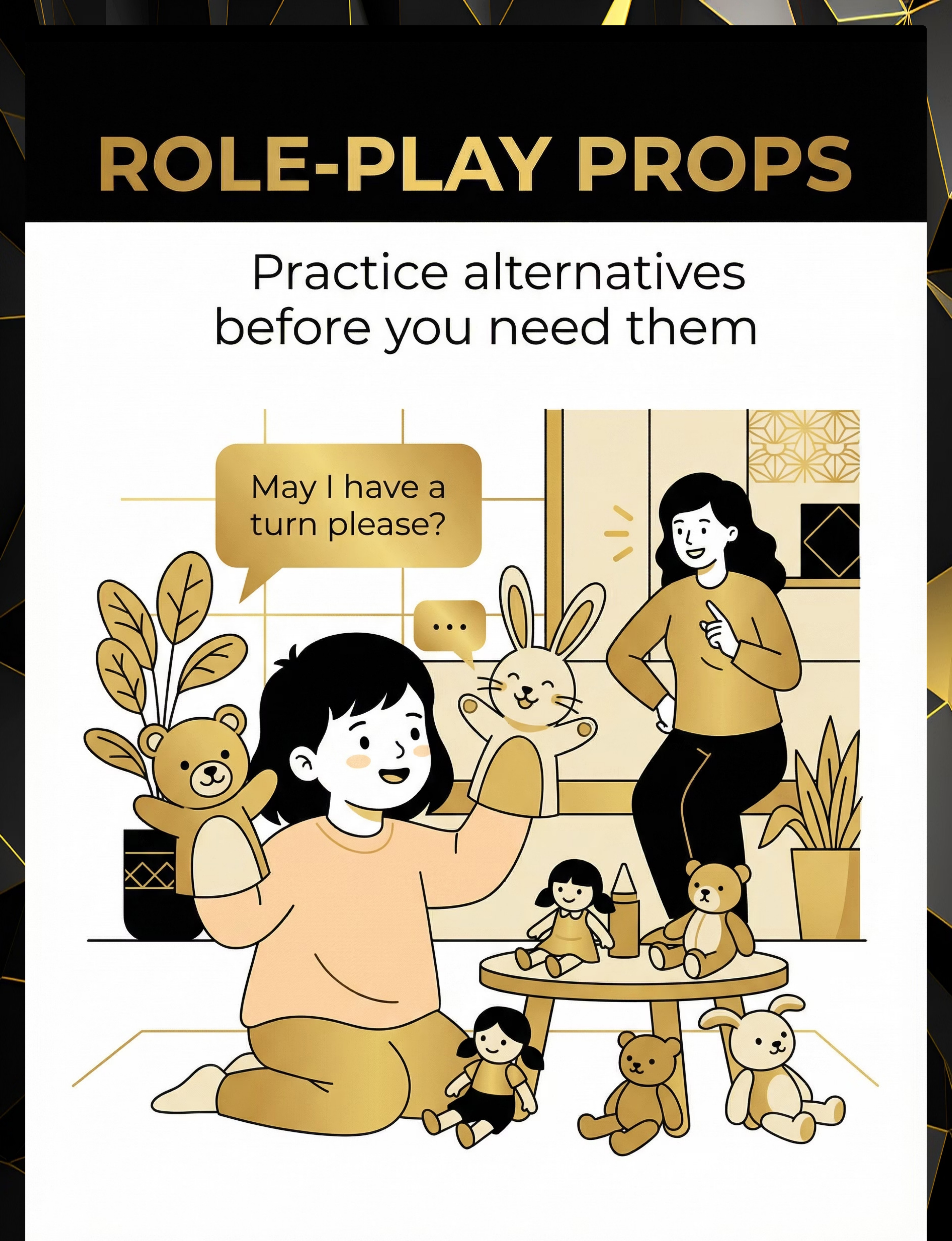
Hand Puppets / Role-Play Props
Role-Play Materials — safe practice of alternative behaviors. 🔍 Search Amazon.in

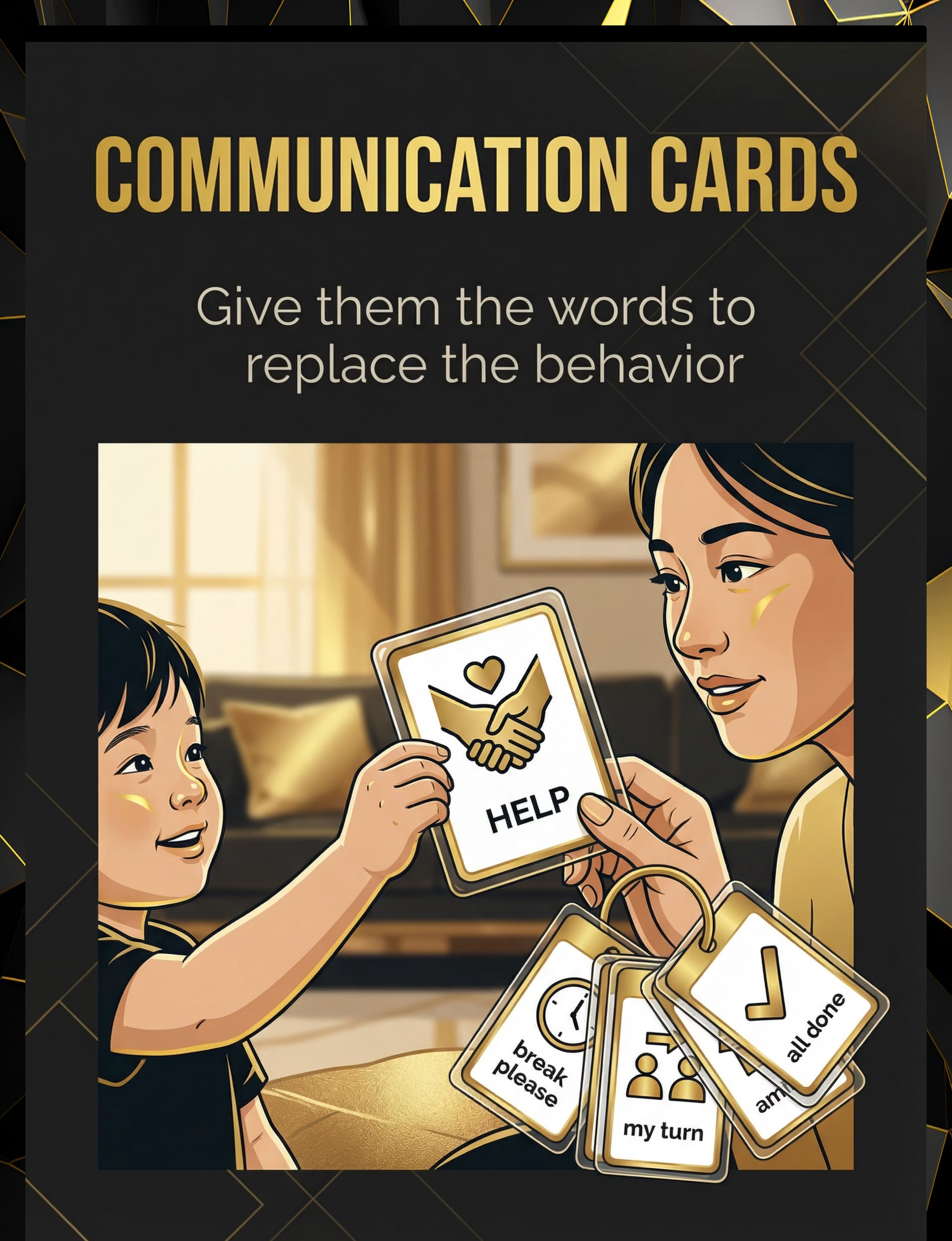
Communication Cards / PECS System
AAC Supports — gives children without verbal language a functional voice. 🔍 Search Amazon.in

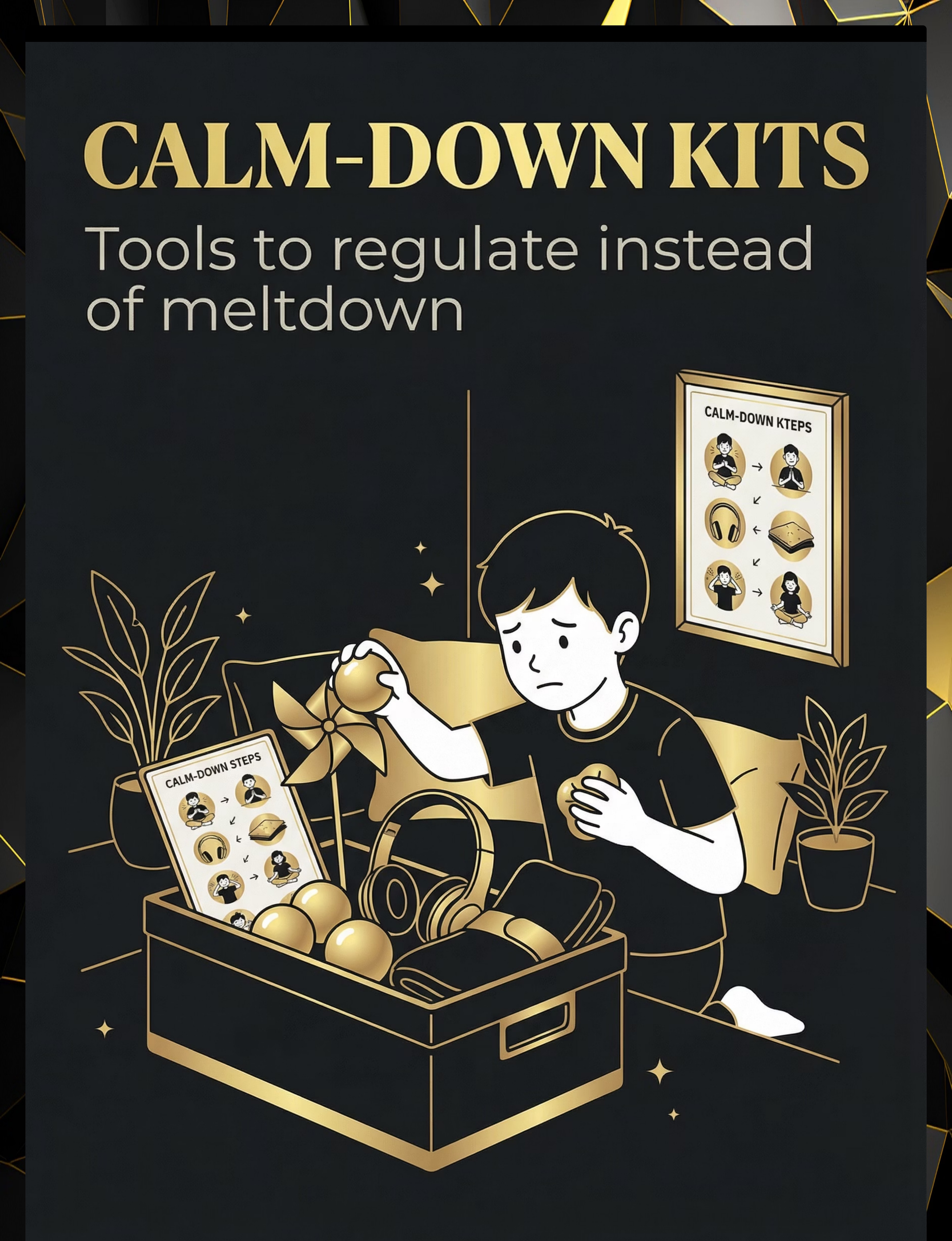
Stress Balls / Calm-Down Kit
Sensory Regulation Tools — provides sensory alternative to problem behavior. 🔍 Search Amazon.in

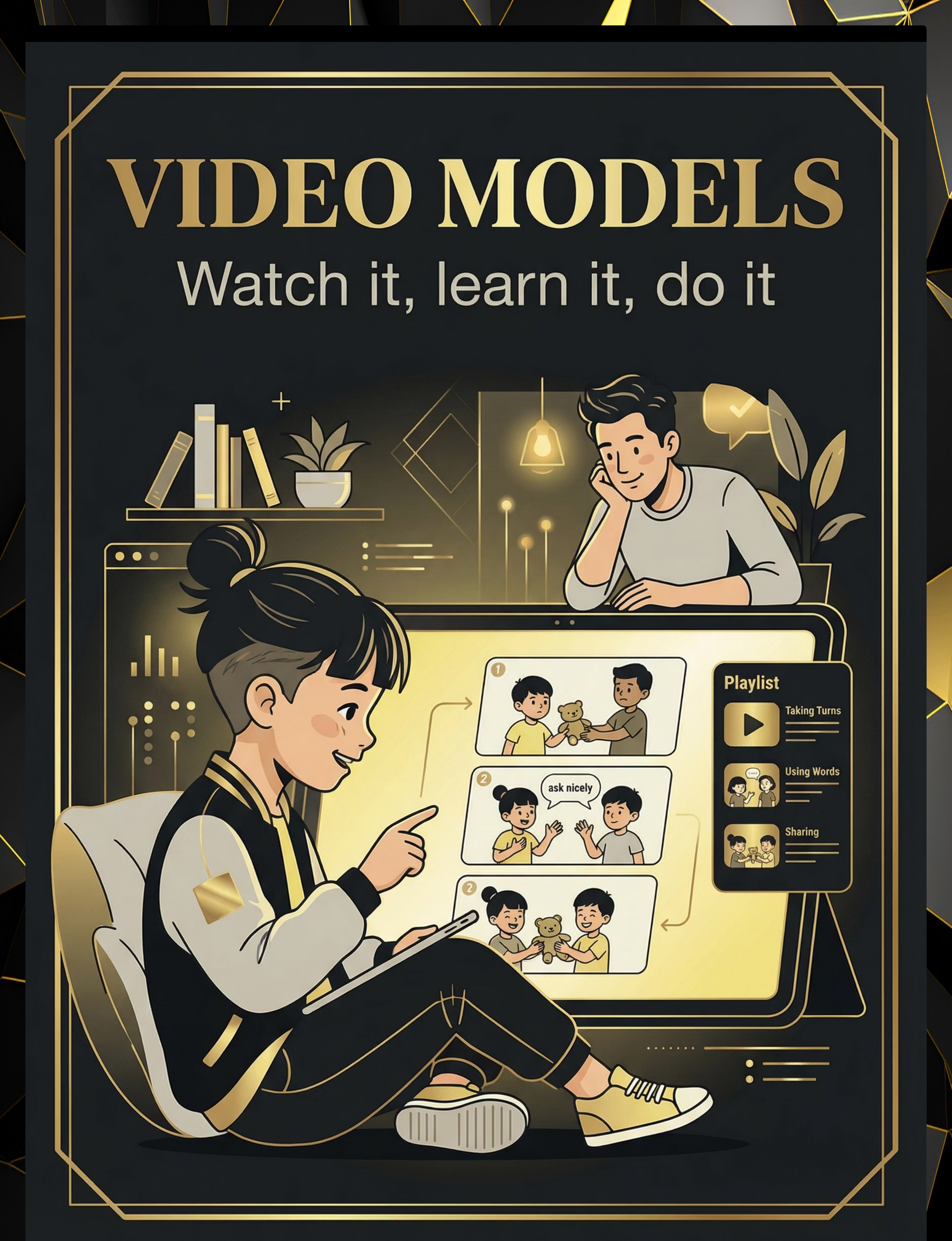
Video Model on Tablet
Video Modeling — evidence-based visual demonstration of the alternative behavior. NCAEP 2020 classified.

Every Child Deserves This. Regardless of Budget.
WHO/UNICEF Equity Principle: Household-material interventions are equally effective when the therapeutic principle is maintained. The therapeutic value is in the function, not the material.
Buy This
- Printed Instead Of Cards (laminated)
- Social Story Book
- Hand Puppets
- Communication Card Ring
- Calm-Down Kit Box
- Video Model on Tablet
- Problem-Solving Chart (printed)
- Prompt Cards (laminated)
- Token Board (purchased)
Make This (₹0)
- Cut paper, draw or print pictures, slip into ziplock bag
- 5 sheets of A4 paper folded and stapled; draw scenes or print photos
- Two socks from the drawer
- Sticky notes on the fridge
- Shoebox + soft cloth, rice bag, paper pinwheel
- Phone recording of child or parent demonstrating the alternative
- Draw on a whiteboard or cardboard with marker
- Index cards with handwritten reminders
- Sticker chart on paper
Zero-Cost Starter Kit: (1) Draw 3 "Instead Of" cards for your child's most common behaviors. (2) Write a 5-sentence social story tonight. (3) Use two socks for your first role-play session tomorrow morning. | PMC9978394

Read This Before You Begin. Every Time.
🔴 RED — Do Not Proceed If:
- Child is in active meltdown or severe distress — wait minimum 30 minutes after calm
- Child is ill, in pain, or has not slept
- Target behavior involves self-injury or aggression posing immediate safety risk — call 9100 181 181 first
- You are unable to respond consistently for the next 15–30 minutes
🟡 AMBER — Modify Your Approach If:
- Child is tired but not dysregulated — shorten practice to 1 role-play only
- You are emotionally activated — ground yourself first; your nervous system regulates theirs
- There has been a recent behavioral incident — allow 60-minute recovery period before teaching
🟢 GREEN — Safe to Proceed When:
- Child is regulated, fed, and rested
- You have 10–30 minutes of consistent availability
- Materials are prepared and accessible before the session begins
- You have reviewed the target alternative behavior for today's session
RED LINE — Stop Immediately If: The child becomes aggressive, self-injurious, or escalates beyond what you can safely manage. Session abandonment is not failure. It is data. Document what happened and call your Pinnacle therapist.
FREE National Helpline: 9100 181 181 (Available 24x7, 16+ languages) | DOI: 10.1007/s12098-018-2747-4
FREE National Helpline: 9100 181 181 (Available 24x7, 16+ languages) | DOI: 10.1007/s12098-018-2747-4

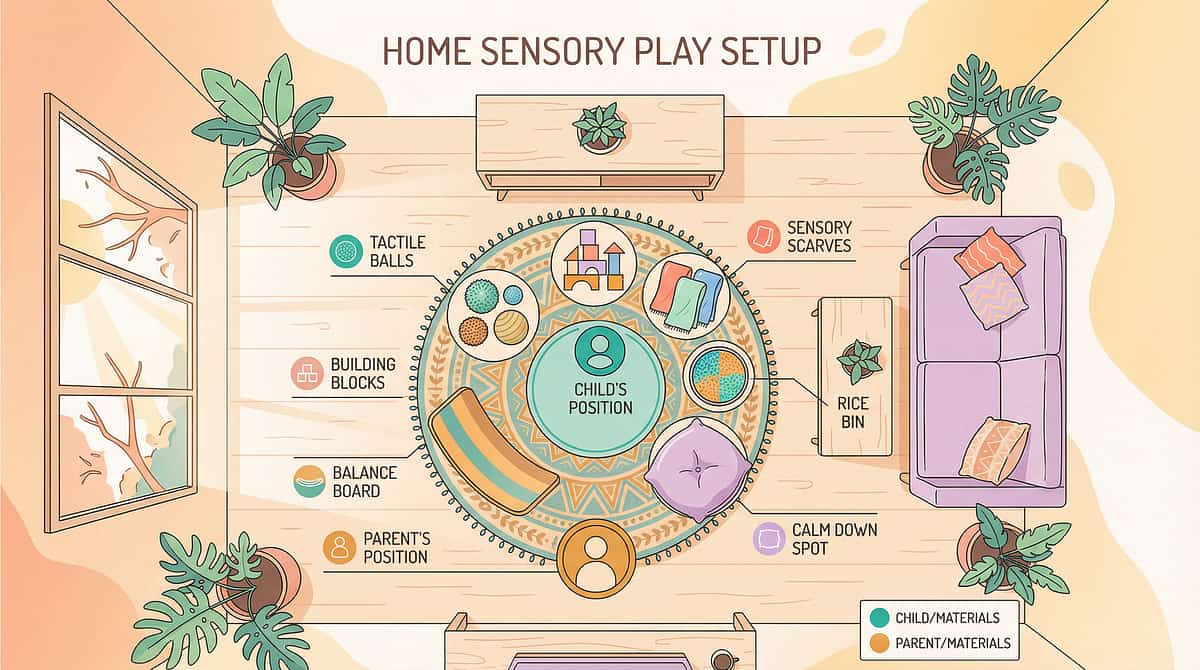
The Right Environment Multiplies Your Results
Setup Checklist
- Instead Of cards — posted at child's eye level on a nearby wall
- Calm-down kit — accessible in the corner, not hidden
- Communication cards — on a ring, within arm's reach of child
- Token board — visible to child throughout the session
- Distraction removal — TV off, tablets face-down, siblings in another room if possible
- Your phone — on silent but accessible for data capture
Environmental Settings
- Lighting: Natural light preferred; avoid harsh fluorescent
- Sound: Background noise below 50 dB; avoid competing audio
- Temperature: Comfortable; sensory comfort is a prerequisite for learning
- Space: Enough room for the child to move if they need motor breaks
Best Time-of-Day Windows
- 60–90 minutes after waking (alert but not overstimulated)
- After a preferred activity (motivation is high)
- NOT immediately before meals or sleep

60-Second Readiness Assessment
Before every session, run through this quick assessment. The best session is one that starts right. A 5-minute session on a green day outperforms a 30-minute session on a red day.
Indicator | ✅ GO | ⚠️ MODIFY | ❌ POSTPONE | |
Regulated state | Calm, engaged | Slightly unsettled | Crying, melting down | |
Fed and hydrated | Meal within 2 hours | Snacked but not full meal | Hungry | |
Rested | Normal sleep | Slightly tired | Sleep-deprived | |
No recent incident | 60+ min since behavior | 30–60 min since incident | Within 30 min | |
Open to interaction | Eye contact, approaching | Tolerating presence | Actively avoiding | |
Your readiness | Calm and focused | Slightly stressed | Overwhelmed |
✅ 5–6 Greens → GO
Proceed to Step 1: The Invitation
⚠️ 3–4 Greens → MODIFY
Run a 5-minute simplified practice only — one role-play, one card review
❌ 2 or Fewer → POSTPONE
Offer a preferred activity; document in your tracker

Step 1 of 6
Step 1: The Invitation — Begin With Invitation, Not Instruction
⏱ 30–60 seconds | Get to the child's eye level. Open posture — no crossed arms, no tension. Voice: warm and genuinely curious, not directive. Physical distance: 60–90 cm — close enough for connection, far enough for autonomy.
"Hey [child's name], I have something really cool to show you. Can I show you something?"
or
"We're going to practice something — and you get to use the puppet / the cards / the kit. Ready?"
or
"We're going to practice something — and you get to use the puppet / the cards / the kit. Ready?"
What Acceptance Looks Like
- Child orients toward you
- Child makes eye contact (even briefly)
- Child moves toward or touches the material
- Child vocalizes or gestures toward the activity
Resistance → Modification
- Turns away: Bring material to their field of vision; reduce demand
- Says "no": Offer choice: "Puppet or cards — which one first?"
- Continues current activity: Join them briefly, then introduce
- No response: Wait 10 seconds, offer once more, then postpone
ABA Pairing Procedures: Establishing motivating operations before demand placement reduces avoidance and increases engagement rate. | OT "Just-Right Challenge" principle
Step 2 of 6
Step 2: The Engagement — Introduce the Material, Let the Child Explore First
⏱ 1–3 minutes | Present the material with low demand first. The goal is contact before instruction.
For Instead Of Cards
"Look at this card — see this picture? This shows what to do when you feel angry." [Child explores card] → [Parent narrates without demanding]
For Puppets / Role-Play Props
"This is Tommy Puppet. Tommy has a problem — he wants the toy but his friend has it. What do we think Tommy should do?" [Child engages with puppet] → [Parent builds narrative around the alternative]
For Communication Cards
"This card says HELP. Whenever you want help, you can hand me this card. Let's try — can you hand me the HELP card?" [Child hands card] → [Parent immediately responds: "Oh, you need help! I'm coming!"]
Reinforcement Cue — First Appearance
The moment the child successfully makes contact with the material or demonstrates the alternative behavior even once: deliver immediate specific praise: "YES! You used the card! That's exactly right!" Then deliver the natural consequence: give what they asked for, provide the break they requested.
🟢 Engagement
Actively participates, explores, attempts the alternative
🟡 Tolerance
Passively allows interaction, watches
🔴 Avoidance
Moves away; reduce demand, go to simpler version

Step 3 of 6
Step 3: The Therapeutic Action — The Alternative Behavior in Action
⏱ 5–15 minutes | Explicitly demonstrate the replacement behavior in the exact context where the problem behavior occurs. This is not general teaching — it is situated practice of a specific alternative for a specific function.
Any attempt at the alternative — even imperfect — earns immediate reinforcement. Prompt hierarchy: physical prompt → gestural prompt → verbal prompt → full model.
Target Behavior | Function | Replacement | Protocol | |
Hitting when wanting something | Access | "Can I have a turn?" / hand card | Model → prompt → reinforce | |
Screaming when frustrated | Escape / attention | Break card / "I need a break" | Model card use → honor immediately | |
Running away from demand | Escape | "I need help" / raise hand | Teach break request → deliver break | |
Grabbing toys | Access | "May I have?" / exchange card | Model exchange → give item → praise | |
Throwing objects | Sensory / escape | Squeeze stress ball / ask for break | Calm-down kit + communication card |
Meta-analysis (World J Clin Cases, 2024): Structured therapeutic action — explicitly teaching functional alternatives — produced the strongest effect sizes across 24 reviewed studies. | PMC10955541
Step 4 of 6
Step 4: Repeat & Vary — Repetition Builds Neural Pathways. Variation Prevents Rigidity.
⏱ 3–5 minutes | Target: 3–8 practice trials per session. "3 excellent, reinforced, joyful repetitions outperform 20 forced, reluctant ones."
Trials 1–3: Minimum Target
Same scenario, full support. Build the pathway. Reinforce every attempt.
Trials 4–6: Consolidation Zone
Begin to vary the partner or location. Introduce slight changes to confirm learning is generalizing.
Trials 7–8: Strength Zone
Change emotional intensity or material prop. Building robust, flexible behavior.
Variation Protocol
After 2–3 successful trials with the same scenario: change the communication partner (other parent, sibling) | change the physical location (kitchen → bedroom) | change the emotional intensity (mild → higher frustration) | change the material prop (card → words → gesture).
The 3 Good Reps Rule: If you get 3 successful, independent, reinforced trials — stop. Let the child end on success. The nervous system consolidates during rest, not during exhaustion. Stop if child seeks another activity, stops looking at materials, or reinforcer effectiveness drops.
Step 5 of 6
Step 5: Reinforce & Celebrate — Timing Matters More Than Magnitude.
⏱ Immediate — within 3 seconds of behavior. Celebrate the attempt, not just the perfect execution. You are building the behavior, not auditing it.
Verbal Praise — Always
"YES! You asked for help — that is exactly what we do!"
"BRILLIANT! You used your break card instead of running!"
"I saw you choose to ask instead of hit. That's YOUR new superpower."
"BRILLIANT! You used your break card instead of running!"
"I saw you choose to ask instead of hit. That's YOUR new superpower."
Natural Consequence — Always
Give the item they asked for; grant the break they requested. This teaches: "The alternative WORKS. It gets me what I need."
Token Economy
1 token = used alternative behavior. 3 tokens = 5-min preferred activity. 5 tokens = choice from reinforcement menu. Token Board ₹364 | Premium ₹589
Social Celebration
High five, hug (if tolerated), thumbs up. A child who tries to hand the card but doesn't quite manage it yet deserves a "good try!" + guided completion + full reinforcement.
FREE National Autism Helpline: 9100 181 181 | pinnacleblooms.org | ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence. | BACB Ethical Guidelines

Step 6 of 6
Step 6: The Cool-Down — No Session Ends Abruptly.
⏱ 1–2 minutes | The cool-down is not optional — it is part of the protocol. A structured ending prevents post-session dysregulation and sets the child up for the next session's success.
"Two more times, and then we're all done for today." [After 2 trials:] "All done! Great work today."
Cool-Down Activity Options (choose one)
- Child-led play for 3–5 minutes
- Preferred sensory activity (swing, squeeze, brush)
- Snack or hydration
- Quiet book time
- Outdoor movement
If Child Resists Ending
- Do not force an abrupt ending
- Offer 1 more choice: "One more or all done?"
- Use a visual timer if the child responds to it
- Deliver a preferred item upon successful transition
Material Put-Away Ritual
"Can you put the cards in the box? Thank you." This creates a behavioral boundary: materials away = session over.
NCAEP Evidence-Based Practices (2020): Visual supports and transition cuing are classified as evidence-based practice for autism. Preventing post-session dysregulation through structured cool-down maintains session efficacy.
60 Seconds of Data Now Saves Hours of Guessing Later
Record immediately after each session. If alternative behavior ↑ and problem behavior ↓ over 2 weeks — the technique is working.
📋 Full Session Log
Date | Session Duration | Target Behavior | Material Used Today | Number of Practice Trials | Times Child Used Alternative Independently | Times Child Needed Prompting | Child's Engagement Level (1–5) | Problem Behavior Occurrences | Notes (anything unusual)
✅ Simple Tally (Busy Days)
☑ Session happened
Alternative used: ___ times (any prompt level)
Problem behavior: ___ times
Today's mood: 😐😊😄
Alternative used: ___ times (any prompt level)
Problem behavior: ___ times
Today's mood: 😐😊😄
📈 Track These 3 Weekly Numbers
- Frequency of alternative behavior use per day
- Frequency of problem behavior per day
- Prompt level needed — full model → gesture → verbal → independent
BACB Data Collection Standards: Continuous behavioral measurement (frequency, duration, prompt level) is the standard for tracking replacement behavior acquisition. | Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.) | FREE National Autism Helpline: 9100 181 181

Most Sessions Are Imperfect. That's Data, Not Failure.
Every challenge you encounter is diagnostic information about what needs to be adjusted. Here are the seven most common obstacles and exactly what to do next.
Child Refused to Participate
Why: Motivation levels fluctuate; the material may not be paired with enough value yet. Fix: Pair the material with a preferred item for 2–3 days before teaching. Let child play with the puppet freely before using it for role-play.
Used Alternative Once, Then Returned to Problem Behavior
Why: The alternative isn't stronger than the problem behavior yet. Fix: Reinforce the alternative 5x more heavily. Make the problem behavior less rewarding by not delivering its outcome.
Alternative Works in Practice but Not in Real Life
Why: Classic generalization gap — the brain treats different contexts as different events. Fix: Practice in the actual location where the problem occurs. Practice with the actual trigger present.
The Alternative I Chose Isn't Working
Why: The replacement may not match the function of the problem behavior. Fix: Re-identify the function. Consult your BCBA. Call 9100 181 181 for guidance.
Child Became Aggressive During Practice
Why: The teaching context itself activated the problem behavior. Fix: Stop immediately. Deliver cool-down (Step 6). Next day: lower demand substantially and increase reward dramatically.
Inconsistency Across Caregivers
Why: Inconsistency across environments is the #1 reason replacement behaviors fail to generalize. Fix: Share this page with all caregivers today. Everyone must respond identically.
No Improvement After 4 Weeks
Why: May indicate skill vs. performance deficit mismatch, unidentified function, or insufficient reinforcement intensity. Fix:Call 9100 181 181. Request a BCBA consultation. This requires professional eyes.
No Two Children Are Identical. Your Protocol Shouldn't Be Either.
Individualized intervention planning is a core principle across OT, ABA, and SLP clinical practice guidelines. Adapt the protocol to your child's profile, communication level, and sensory needs.
Limited Verbal Language
- Use picture exchange (PECS) or AAC device as the replacement
- One symbol = one function (HELP picture = request for help)
- Accept any approximation: pointing, reaching, vocalizing toward the card
High Verbal Ability
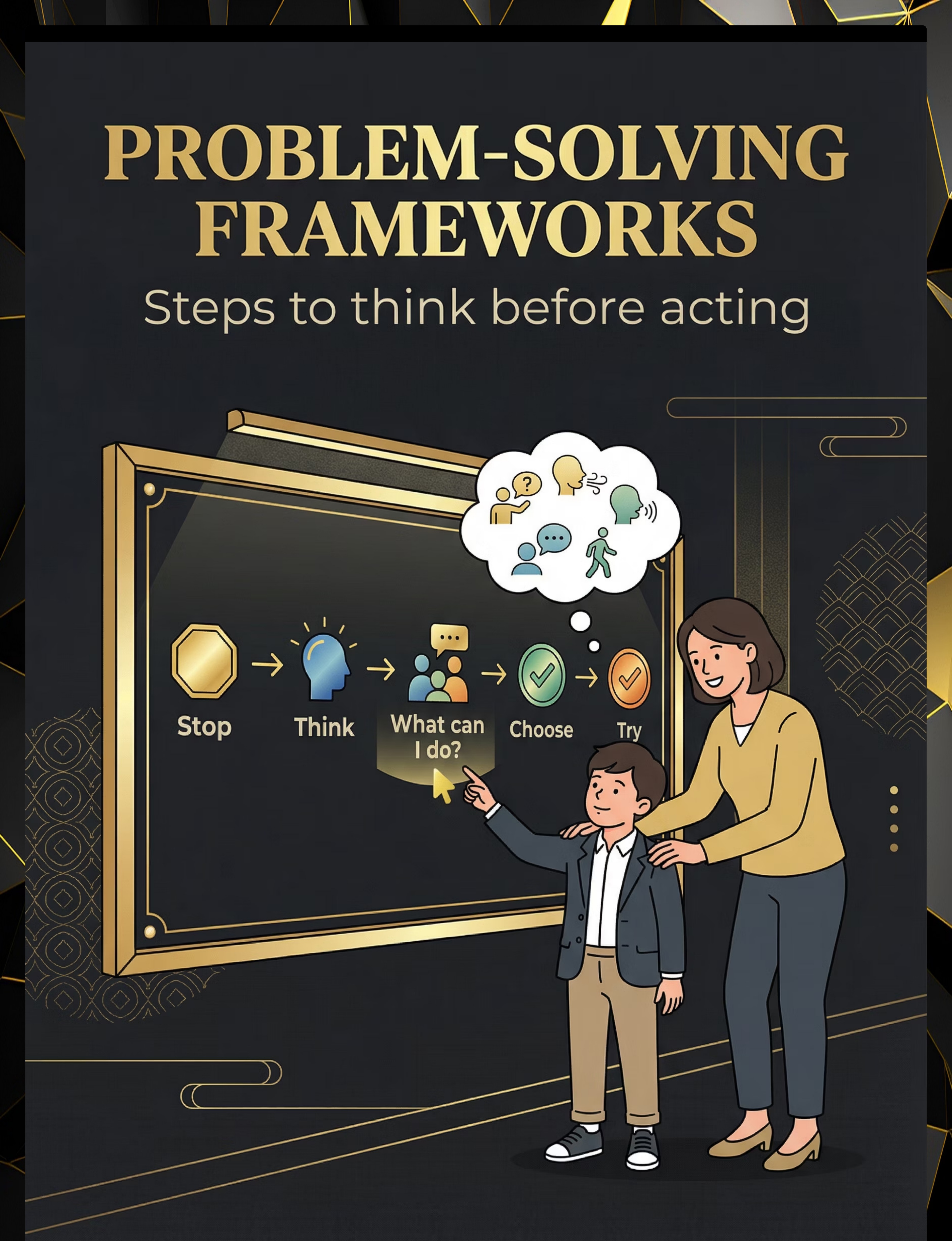
- Move to verbal problem-solving scripts: "What can I do when...?"
- Introduce the problem-solving framework
- Practice in abstract scenarios, not just lived situations
Sensory Seekers
- Calm-down alternatives must provide EQUIVALENT sensory input
- If child hits for proprioceptive input: replace with heavy work (push-ups, carrying, wall push)
Sensory Avoiders
- Reduce the intensity of the practice scenario — high arousal blocks alternatives
- Run practice in neutral emotional context, never when escalated
Age Modifications & Bad Day Protocol
- Ages 2–4: Single picture, single word or gesture. Maximum 1 alternative per session.
- Ages 5–7: 2–3 word phrase + picture. 2–3 scenarios per session.
- Ages 8–12: Verbal scripts, problem-solving frameworks. Self-monitoring tools.
Bad Day Version (3-minute protocol): (1) Show one Instead Of card. (2) Child names or points to the alternative. (3) Deliver reinforcement. (4) Done. That counts.
Progress in Weeks 1–2 Looks Nothing Like Mastery — And That's Exactly Right
✅ What You WILL See
- Child notices the Instead Of card or material when you present it
- One or two unprompted attempts at the alternative (even imperfect)
- Slight reduction in intensity (not necessarily frequency) of problem behavior
- Increased tolerance for the teaching session itself
⏳ What You Will NOT See Yet
- Spontaneous use of the alternative without prompting
- Complete cessation of the problem behavior
- Generalization to other settings or caregivers
"If your child tolerates the role-play for 90 seconds longer than last week — that is real, measurable neural progress. The brain is beginning to register a new option."
Parent Milestone — Week 2: You have delivered this consistently. That alone is the intervention. Most parents experience hope mixed with doubt at this stage. Keep the data. The data will reassure you when your feelings can't. | PMC11506176
Progress Arc — Week 3–4
The Neural Pathway Is Forming. Watch for These Signals.
These are the "tells" that the alternative is becoming a real behavioral option — not just trained compliance. Watch for these signs that the brain is genuinely reorganizing.
Spontaneous Reach
Child reaches for the communication card BEFORE you prompt it
Visual Check-In
Child looks toward the Instead Of chart during a moment of conflict
Behavior Drop
Problem behavior frequency measurably lower on days with practice
Verbal Fragment
Child begins to verbalize the alternative — even a fragment: "break... I need..."
Positive Anticipation
Child anticipates the teaching session with positive affect
Self-Correction
Child starts the problem behavior, then stops and uses the alternative
Parent Milestone — Week 4: You may be noticing YOUR behavior changing too. That is also therapeutic. The parent who responds differently is part of the treatment. If consolidation signs are clear by Week 4, increase daily practice opportunities from 2–3 to 4–5 per day. The neural window is open — maximize it.

Progress Arc — Week 5–8
Mastery Is Not Perfection. Mastery Is Reliable Generalization.
Your child demonstrates mastery when they can use the alternative behavior reliably — not just in the practice room, but in the messy, variable, emotionally loaded situations of real life.
Uses alternative WITHOUT prompt in trained context
Uses alternative in at least ONE untrained setting
(home → school, or home → community)
Problem behavior reduced 50%+ from baseline
Uses alternative with at least ONE untrained partner
(teacher, grandparent)
No regression despite two or more "bad days"
🏆 Mastery Badge Criteria: Child demonstrates 3 of 5 criteria above for 5 consecutive days.
All 5 Met → D-361
Move to Environmental Structure | techniques.pinnacleblooms.org/behavior/environmental-structure-D-361
3–4 Met → Continue
Stay with D-360 protocols, increase generalization practice
Fewer than 3 → Call
9100 181 181 — professional support layer recommended

You Did This. Not the Therapy Room. Not the Clinic. You.
You spent weeks watching your child struggle with behaviors that seemed impossible to change. You learned the science. You gathered the materials. You practiced when you were tired, when sessions didn't go perfectly, when you doubted whether anything was working.
And then it worked.
Your child reached for the card instead of hitting. Your child said "I need a break" instead of running. Your child handed you the HELP card and waited.
That is not a small thing. That is a new neural architecture. That is your child's future — and you built it.
Family Celebration Suggestion: Tonight, tell your child: "I am so proud of how you're learning new ways. You did something really hard." Then document this moment. Take a photo. Write in a journal. Post in your parent community. This milestone belongs to your family's story.
Journal Prompt: "On [date], my child used [alternative behavior] instead of [problem behavior] in [context]. We started this journey on [date]. This is what I want to remember about this journey: ___"

Even in Progress, Stay Alert. These Signs Require Professional Consultation.
🚨 Flag 1: Behavior Escalating in Intensity
Problem behavior happens less frequently but more intensely when it does occur. May indicate the function has changed or an unidentified trigger is compounding. Consult your BCBA.
🚨 Flag 2: New Problem Behaviors Emerging
Hitting reduces, but self-injurious behavior begins. The function is being met through a more dangerous replacement. Requires immediate BCBA assessment.
🚨 Flag 3: Alternative Used Only to Avoid Demands
Child uses break card 20+ times per day to escape every task. The alternative has become a problem behavior. Requires protocol adjustment with BCBA supervision.
🚨 Flag 4: Sleep, Appetite, or Sensory Sensitivity Worsening
Child is regressing in regulation, sleep, or eating while behavioral demands increase. May indicate a medical, sensory, or developmental factor overwhelming the system.
🚨 Flag 5: You Are Not Coping
You are consistently unable to deliver reinforcement without frustration; you are burning out. Parental wellbeing is a therapeutic variable. A burnt-out parent cannot run an effective protocol.
Escalation Pathway: Minor Concern → Troubleshooting (Card 21) → Moderate → Teleconsultation → Serious → In-clinic BCBA Assessment → Emergency → 9100 181 181 immediately. Available 24x7 | 16+ languages.

You Are Here. Here Is Where You're Going.
D-360 sits in a sequenced developmental pathway. Based on your child's response to this technique, the next step is intentional — not arbitrary.
Alternative Firmly Established →
D-361 Environmental Structure — Proactively modify the environment to prevent the problem behavior from occurring at all
Communication Is the Primary Barrier →
D-375 Functional Communication Training — Deepen the communicative alternative with full FCT protocol
Self-Regulation Is Lagging →
← D-358 Self-Regulation Skills — The body must be regulated before alternatives can be accessed under stress
More Tools in Your Behavior Support Arsenal
The materials you've already gathered for D-360 — Calm-Down Kit, Token Board, Communication Cards, Instead Of Charts — cover four of the six related techniques below. Your investment compounds.
Technique | Code | Difficulty | Materials You Already Have | |
Self-Regulation Skills | D-358 | 🟡 Core | Calm-Down Kit ✓ | |
Consistent Responses | D-359 | 🟢 Intro | Token Board ✓ | |
Environmental Structure | D-361 | 🟡 Core | Prompt Cards ✓ | |
Antecedent Interventions | D-362 | 🟡 Core | Visual Schedules | |
Functional Communication Training | D-375 | 🔴 Advanced | Communication Cards ✓ | |
Token Economy Systems | D-380 | 🟡 Core | Token Board ✓ |
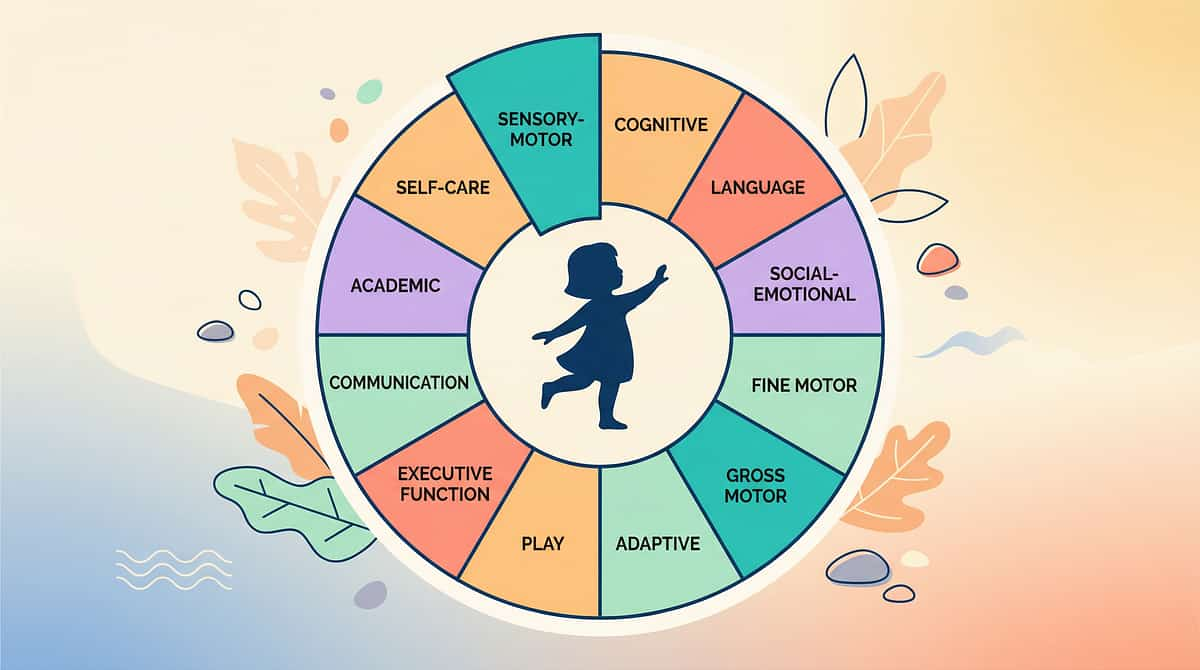
D-360 Is One Piece of a Larger Plan. Here Is the Full Picture.
Domain D is not isolated. When you teach What TO Do, three other domains grow simultaneously — Social Communication, Emotional Regulation, and Play Skills all benefit directly from the work you're doing right now.
Your child's AbilityScore® across all 12 domains, updated as you deliver sessions and enter data, is available through your Pinnacle center or the GPT-OS® platform. → View Your Child's Full AbilityScore® Profile | WHO/UNICEF Nurturing Care Framework (2018) | FREE National Autism Helpline: 9100 181 181
From the Families Who Walked This Path Before You
Arjun, Age 5 — Hyderabad
Before: He hit his sister every time she had a toy he wanted. Timeout, ignoring, reward charts for not hitting — nothing lasted more than a week.
The Shift: His BCBA did a functional assessment. The function was access — he wanted the toy. We taught him to say "my turn please" using a picture card. Reinforced every attempt. Immediately. Within 3 weeks, hitting dropped 70%.
After: By week 6, Arjun was using "my turn please" spontaneously — at home, at school, at his cousin's house. His BCBA called it generalization. We called it a miracle.
— Parent, Pinnacle Hyderabad | Illustrative case; outcomes vary
The Shift: His BCBA did a functional assessment. The function was access — he wanted the toy. We taught him to say "my turn please" using a picture card. Reinforced every attempt. Immediately. Within 3 weeks, hitting dropped 70%.
After: By week 6, Arjun was using "my turn please" spontaneously — at home, at school, at his cousin's house. His BCBA called it generalization. We called it a miracle.
— Parent, Pinnacle Hyderabad | Illustrative case; outcomes vary
Meera, Age 7 — Bengaluru
Before: She screamed every time we said homework. Two years of dreading every evening.
The Shift: The scream was an escape behavior. We taught her to raise her hand and say "I need help please" or hand us a break card. Gave the break immediately, every time, without negotiation.
After: Eight weeks later, she raises her hand when she's stuck. The screaming occurs maybe once every two weeks on very difficult days. But the skill is real.
— Parent, Pinnacle Bengaluru | Classic FCT protocol response
The Shift: The scream was an escape behavior. We taught her to raise her hand and say "I need help please" or hand us a break card. Gave the break immediately, every time, without negotiation.
After: Eight weeks later, she raises her hand when she's stuck. The screaming occurs maybe once every two weeks on very difficult days. But the skill is real.
— Parent, Pinnacle Bengaluru | Classic FCT protocol response
"The families who see the fastest results are the ones who stop focusing on the problem behavior and start obsessing over the alternative. The child isn't choosing to be better — they're choosing the better deal." — BCBA, Pinnacle Blooms Network

You Are Not Doing This Alone. There Is a Community Waiting.
📱 WhatsApp — Teaching What TO Do Strategies
Parents specifically working on replacement behavior teaching. Share wins, troubleshoot failures, and ask questions in real time. Join WhatsApp Group →
💬 Pinnacle Online Parent Forum
Longer discussions, resource sharing, therapist Q&A threads, weekly live sessions with Pinnacle BCBAs. Join Forum →
📍 Local Pinnacle Parent Meetups
Monthly in-person meetups at 70+ Pinnacle centers across India. Find your city. Find Nearest Meetup →
🤝 Peer Mentoring
Parents who have completed D-360 and are 6+ months into the journey. Real experience, no clinical distance. Request a Peer Mentor →
"If this page helped you, your story could be the one that helps the next family find the courage to start. Consider sharing your journey." | WHO NCF: Community engagement is a core principle. Parent support networks improve intervention adherence and outcomes. | FREE National Autism Helpline: 9100 181 181

Home + Clinic = Maximum Impact. Find Your Team.
"What you practice at home, we reinforce at clinic. What we teach at clinic, you maintain at home. The loop is the intervention."
Need | Specialist | How to Access | |
Functional Behavior Assessment | BCBA / ABA Therapist | In-clinic or teleconsultation | |
AAC / Communication Card Setup | Speech-Language Pathologist | In-clinic or home visit | |
Sensory-based alternatives | Occupational Therapist | In-clinic | |
School generalization plan | Special Educator | Home/school coordination | |
Medical evaluation (if needed) | NeuroDev Pediatrician | In-clinic |
🏥 In-Clinic Assessment
Full AbilityScore® evaluation + individualized D-360 protocol. Book In-Clinic →
💻 Teleconsultation
30-minute BCBA consultation for protocol review and troubleshooting. Book Teleconsult →
📞 FREE Helpline — 24x7
Immediate guidance in 16+ languages. 9100 181 181 | Available any time, any day.
The Science Behind D-360 — For the Curious Parent
You don't need to read every study to use this technique effectively. But knowing the research exists — and is robust — can be the confidence anchor that keeps you consistent on hard days.
Study | Finding | Link | |
NCAEP Evidence-Based Practices (2020) | FCT is an evidence-based practice for autism across all ages | ncaep.fpg.unc.edu | |
World J Clin Cases (2024), 24 studies | Alternative skill teaching showed significant improvement in problem behavior, communication, and social participation | ||
Children (2024), 16 articles | Behavioral interventions meet EBP criteria for ASD across 2013-2023 | PMC11506176 | |
Indian J Pediatr (2019) | Home-based behavioral skill teaching with parent training: significant outcomes in Indian pediatric population | DOI: 10.1007/s12098-018-2747-4 | |
WHO CCD Package (2023) | Home-based caregiver-delivered interventions effective across 54 low- and middle-income countries | PMC9978394 |
Every Data Point You Enter Makes Every Child's Outcomes Better
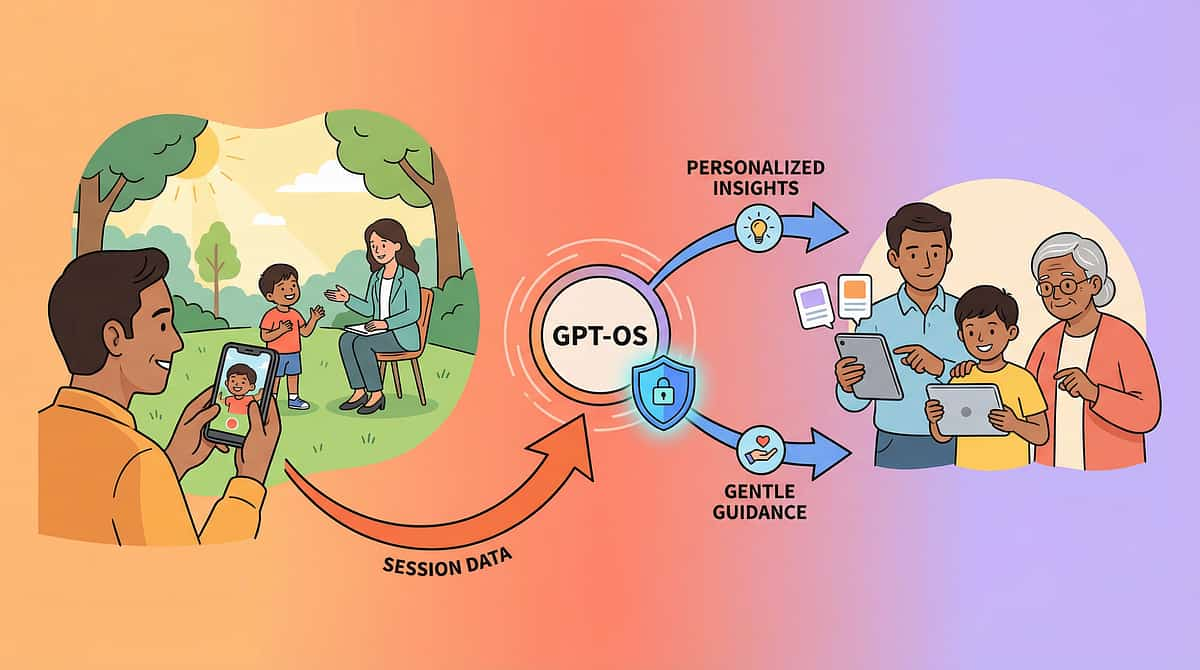
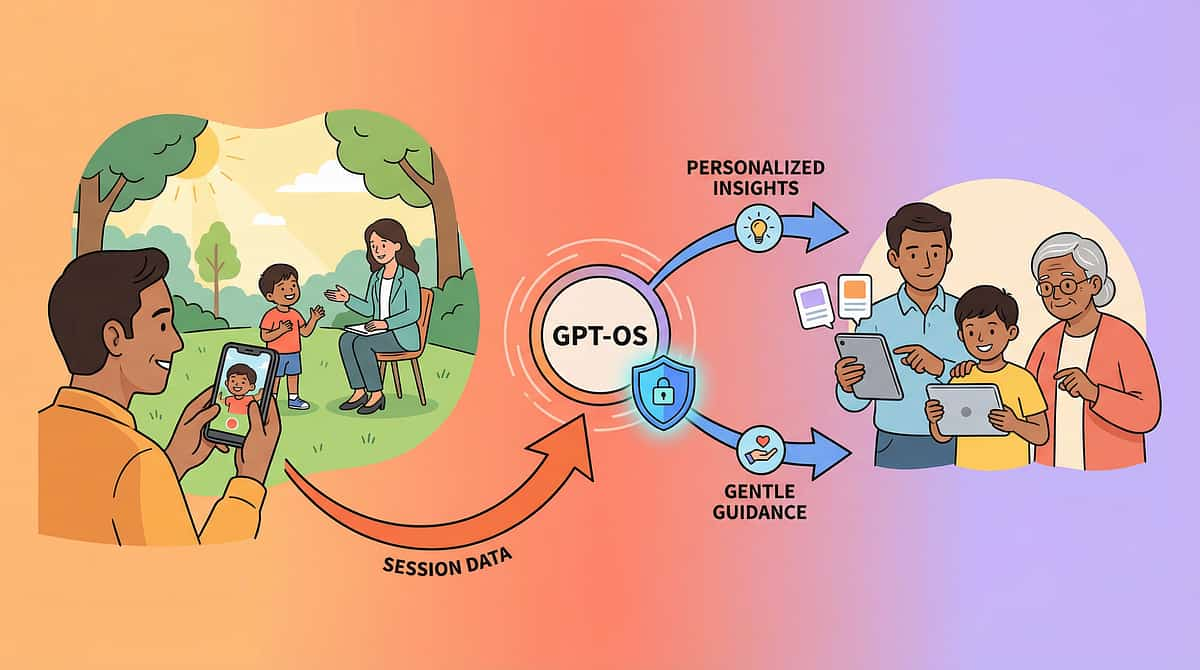
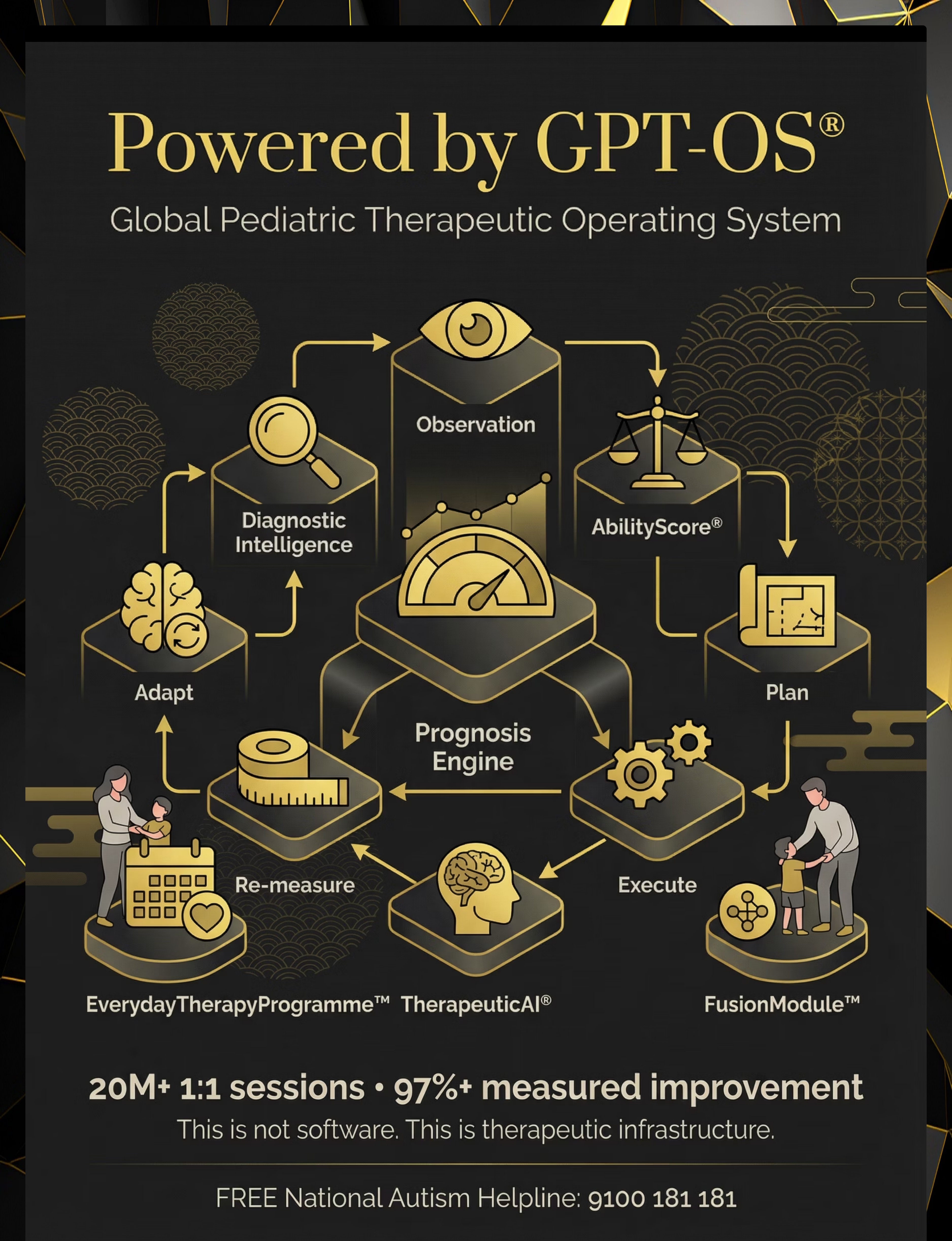
How GPT-OS® Uses Your Session Data
Your session data (frequency, prompt level, behavior counts) flows through the GPT-OS® TherapeuticAI® layer for pattern recognition and progression prediction. This generates personalized recommendations for you — and contributes to population-level intelligence about what works for children with similar profiles globally.
What GPT-OS® Learns from D-360 Data
- Which of the 9 materials produces fastest replacement behavior acquisition for this child's profile
- Optimal reinforcement schedule for this child's reinforcer preferences
- Generalization trajectory — when to introduce the next environment
- Red flag detection — early identification of stalled progress requiring professional review
Privacy Assurances
- All data is encrypted at rest and in transit
- Individual child data is never shared without consent
- Aggregate (anonymized) patterns improve all 70,000+ technique recommendations
- DPDPA (India) compliant | GDPR aligned for international families
"Your data helps every child like yours. When 20 million sessions converge, the intelligence becomes sovereign-grade — capable of predicting, preventing, and accelerating outcomes no single clinic could see."
See the 9 Materials Demonstrated by the Pinnacle Team
Reel ID: D-360 | Series: Behavior Support & Skill Building — Episode 360 | Duration: ~75–85 seconds | Presenter: Pinnacle BCBA / Behavior Specialist
Instead Of Cards
Demonstrated with a child in a real conflict moment
Social Story
Being read at bedtime — warm, natural setting
Role-Play with Puppets
Child practicing "asking nicely" — joyful, engaged
Communication Card
Child handing card to parent instead of melting down
Calm-Down Kit
Stress ball → regulated state — before and after
Video Model on Tablet
Child watching peer demonstrate the alternative behavior
Problem-Solving Chart
Parent and child reviewing together before a transition
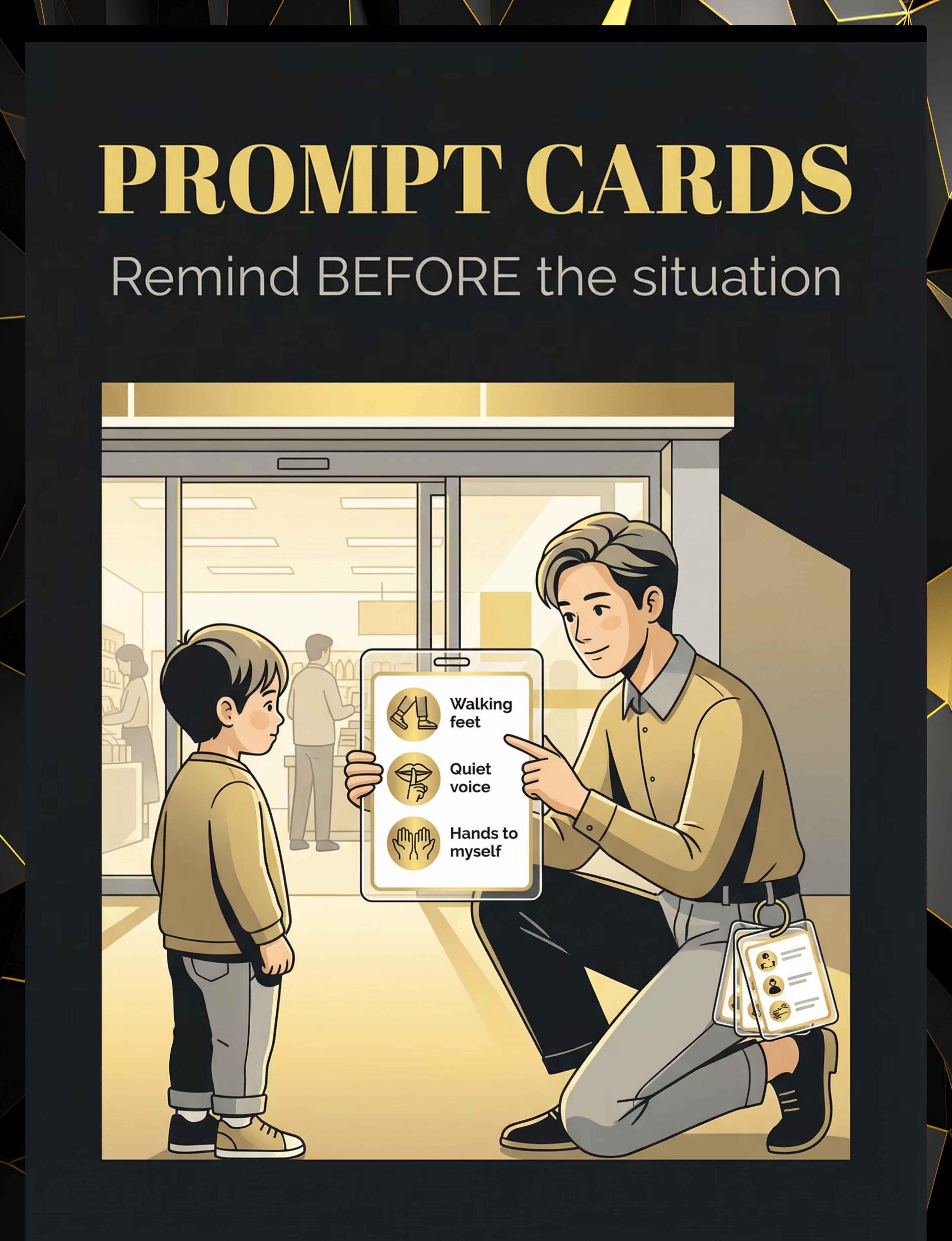
Prompt Card
Reviewed before entering a challenging store environment
Token Board
Child receives token for using alternative — visible celebration
"The most important shift in behavior support is moving from 'stop doing that' to 'do this instead.' Every challenging behavior is a child's attempt to meet a need. Your job isn't to take away their tool. It's to give them a better one." — Pinnacle Behavior Specialist
Consistency Across Caregivers Multiplies Impact. Share This Page Now.
Inconsistency across environments is the #1 reason replacement behaviors fail to generalize. Every caregiver in your child's life must respond identically to the alternative behavior and the problem behavior.
WhatsApp-Ready Summary for Family:
"We're using D-360 — Teaching What TO Do. Instead of 'don't hit/don't scream/don't grab,' we're teaching [child's name] what to do INSTEAD.
• Wanting something → hand HELP card or say "may I have a turn"
• Frustrated → squeeze stress ball or say "I need a break"
• Needs something → point to the picture card
EVERY TIME they use the alternative: praise immediately + give what they asked for. DON'T give attention/items after the problem behavior. Consistency is the medicine."
"We're using D-360 — Teaching What TO Do. Instead of 'don't hit/don't scream/don't grab,' we're teaching [child's name] what to do INSTEAD.
• Wanting something → hand HELP card or say "may I have a turn"
• Frustrated → squeeze stress ball or say "I need a break"
• Needs something → point to the picture card
EVERY TIME they use the alternative: praise immediately + give what they asked for. DON'T give attention/items after the problem behavior. Consistency is the medicine."
Explain to Grandparents
"We've learned that [child's name] doesn't know how to ask for things yet in the right way. So instead of saying 'no, don't do that,' we're showing them what TO do. When they use the right way — praise them immediately and give them what they asked for. This is the science. Please follow it consistently."
School Communication
A pre-written letter with D-360 protocol summary for the class teacher is available as a download — ensuring what your child learns at home transfers to school.
WHO CCD Package: Multi-caregiver training is critical for intervention generalization and maintenance. | PMC9978394 | FREE National Autism Helpline: 9100 181 181

Questions Every Parent Asks — Answered by the Consortium
How long before I see results?
Most families see initial signs of alternative behavior use within 2–3 weeks of consistent daily practice. Significant reduction in problem behavior typically occurs by weeks 5–8. Children with more severe profiles or significant communication delays may require 12–16 weeks. The key variable is consistency of reinforcement delivery, not the child's motivation.
My child uses the alternative at home but not at school. Normal?
Yes. This is a generalization gap — extremely common. The brain treats different environments as different contexts. Explicitly practice in the school environment. Share the protocol with the class teacher using Card 37's template.
Do I need to address the problem behavior directly?
Ideally both. Teach the alternative AND ensure the problem behavior no longer produces the outcome it used to. If hitting used to get the toy, hitting must no longer get it while the alternative always does. This is called differential reinforcement.
My child has no verbal language. Can this still work?
Yes. This is where communication cards, AAC systems, and PECS become the alternative behavior. A child who points to a picture of HELP instead of screaming is using a functional alternative. Start with the most physically accessible response — even a gaze shift toward the card.
Should I never say "no" or "don't"?
No, that's not the message. "Don't" is fine as a real-time response. The issue is using it as the primary teaching strategy. The teaching happens during calm practice — role-play, social stories, video models — not in the heat of the moment.
Child uses the alternative to avoid everything — 30+ break requests per day?
The alternative needs to be shaped. Gradually require more before the break is granted: "Finish 2 more problems, then break." This is called a communication-based delay. A BCBA should supervise this step. Call 9100 181 181.
Is this appropriate for my child's age?
Yes — with adaptations. Ages 2–4: single gesture or picture. Ages 4–7: 1–3 word phrase + card. Ages 8–12: verbal scripts and problem-solving frameworks. See the Adapt & Personalize section for full age-specific modifications.

You Have Everything You Need. Start Today.
Every day of consistent practice is a day the neural pathway gets stronger. You don't need perfect conditions. You need today's 10 minutes, today's materials, and today's willingness to try.
🚀 Start This Technique Today
Launch a GPT-OS® guided D-360 session — personalized to your child's profile and today's readiness level.
📅 Book a BCBA Consultation
Professional protocol setup and troubleshooting in 30 minutes. In-clinic or teleconsultation available.
→ Explore Next: D-361
Environmental Structure — the next technique in the Domain D pathway. Proactively design your home to prevent problem behaviors before they start.
✓ Validated by BCBA • SLP • OT • SpEd • NeuroDev Pediatrics | ✓ Evidence-Grade: Level I | NCAEP 2020 | BACB Standards | ✓ 20M+ Sessions | 97%+ Measured Improvement | 70+ Centers | FREE National Autism Helpline: 9100 181 181 | Available 24x7 | 16+ languages
Preview of 9 materials that help teaching what to do Therapy Material
Below is a visual preview of 9 materials that help teaching what to do therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
From Fear to Mastery. One Technique at a Time.
We exist to transform every home into a proven, scientific, 24x7, personalized, multi-sensory, multi-disciplinary, integrated pediatric therapy environment — for every family, in every economic condition, in every geography. No child should have their potential limited by access to clinical expertise. GPT-OS® is our answer. — Pinnacle Blooms Network®
OT • SLP • ABA/BCBA
Primary clinical leads for D-360 — occupational therapy, speech-language pathology, and applied behavior analysis working in integrated concert.
SpEd • NeuroDev • CRO
Special education, neurodevelopmental pediatrics, and clinical research oversight — the full Pinnacle Blooms Consortium seal of validation.
Continue Your Journey
Medical Disclaimer: This content is educational and informational. It does not replace individualized assessment, diagnosis, or intervention with licensed behavior analysts, psychologists, speech-language pathologists, occupational therapists, or developmental pediatricians. Complex behavioral presentations, safety concerns, aggression, self-injury, or limited progress with home strategies require professional evaluation and support. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content generated under GPT-OS® Content Engine. Technique D-360. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
FREE National Autism Helpline: 9100 181 181 | care@pinnacleblooms.org | pinnacleblooms.org