
Every night ends the same way. Battles. Tears. Exhaustion. And it's 10 PM, and they're still not asleep.
Bedtime resistance isn't defiance — it's your child's nervous system speaking. You are not failing.
"It's 7:30. I announce bedtime. And instantly — 'I'm not tired!' 'Five more minutes!' 'I need water!' Forty-five minutes later we're on the third bathroom trip, the second story, the fifth renegotiation. By the time they're finally asleep, it's 10 PM. I'm emotionally wrecked. And I dread tomorrow evening starting at noon."
Your child's brain transitions differently — and that is something that can be supported, scaffolded, and solved.
🛏️ Bedtime Routine Independence
🌙 Sleep Preparation
🔄 Transition Support
🧘 Self-Regulation
😰 Anxiety Management
Pinnacle Blooms Consortium® | OT • SLP • ABA • SpEd • NeuroDev | GPT-OS® Validated
WHO Nurturing Care Framework (2018): Early identification and parental awareness directly impacts developmental outcomes.

🌍 Millions of families fight this battle every night. You are among them — and there is a proven path out.
The Scale of This Challenge
50–80%
Children with ASD
Experience significant sleep difficulties, vs. 25–30% in neurotypical children
2–3 hrs
Average Bedtime Duration
Time bedtime takes for families reporting resistance — vs. 20–30 min for structured-routine families
70%
Resistance Reduction
Reduction in bedtime resistance with structured visual + sensory support, per Pinnacle 20M+ session database
Across India alone, an estimated 12+ million families of children with developmental differences struggle with bedtime every single night. You are not alone. You are not failing. You are part of a massive, underserved community — and Pinnacle exists to serve exactly this need.
📄Indian J Pediatr 2019 RCT: Structured evening routine with sensory tools resulted in significant reduction in sleep onset latency across ASD and ADHD populations. | PRISMA Systematic Review (PMC11506176, 2024): 80% of children with autism display sensory processing difficulties — many of which peak at bedtime.
🧠 The Neuroscience
This is a wiring difference. Not a behavior choice. Not bad parenting.
Why Bedtime Is Neurologically Hard
The Arousal Regulation Problem
The Reticular Activating System (RAS) takes longer to downregulate in children with ADHD and autism. Their brain is genuinely still "on" when yours has been "off" for an hour.
The Transition Problem
The Prefrontal Cortex governs task-switching. In developmental differences, transitioning from play to bed requires massive executive effort.
The Sensory Problem
The somatosensory cortex over-amplifies input. Pajama textures feel wrong. Sheets too hot. Every small sound is magnified.
The Anxiety Problem
The amygdala's threat-detection system is hyperactive. Nighttime quiet removes daytime distractors — and anxiety, fear of the dark, and worry thoughts fill the space.
The Melatonin Problem
Circadian rhythm differences (especially in autism) can delay natural melatonin onset by 1–2 hours. The child genuinely may not feel physiologically tired at typical bedtime.
"Bedtime resistance is the predictable output of a nervous system that was wired differently. The solution is scaffolding — not willpower, not stricter limits, not patience alone."
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 | Indian J Pediatr RCT 2019: DOI: 10.1007/s12098-018-2747-4

📅 Developmental Context
Your child is here on this timeline. Here is where we're going.
Age 2
Basic routine awareness emerging
Age 3
With visual prompting support
Age 4–5
Emerging independence with support
Age 7
Full independence (typical)
Age 10–12
Independence goal — our target
Your child may be anywhere on this spectrum. That is valid. Bedtime challenges commonly co-occur with: ADHD (arousal dysregulation), Autism Spectrum (sensory + transition), Anxiety Disorders (fear amplification), Sensory Processing Disorder (environmental sensitivity), and Sleep Phase Delay (circadian difference).
"This is not a parenting failure. This is a developmental waypoint with a clear, evidence-supported forward path." Bedtime independence is tracked within the Daily Living Skills Readiness Index and Self-Regulation Readiness Index — two of GPT-OS®'s core measurement axes.
WHO Care for Child Development (CCD) Package: Age-specific caregiver recommendations implemented in 54 LMICs. (PMC9978394) | UNICEF MICS indicators for developmental monitoring across 197 countries.
🏅 Evidence Grade
Clinically validated. Home-applicable. Parent-proven.
Evidence Grade
I-A
Systematic Review + RCT Support
20,000,000+ exclusive 1:1 therapy sessions
97%+ measured improvement across readiness indexes
70+ centers | DPIIT DIPP8651 recognized
📄 PRISMA Systematic Review (Children, 2024)
16 studies (2013–2023): Visual schedules + sensory interventions are evidence-based practices for children with ASD including daily living skills and routine compliance. → PMC11506176
📄 Meta-Analysis (World J Clin Cases, 2024)
24 studies: Sensory integration therapy significantly promoted social skills, adaptive behavior, and self-care outcomes across pediatric populations. → PMC10955541
📄 Indian RCT (Indian J Pediatr, 2019)
Home-based sensory intervention (Padmanabha et al.): Structured evening routines with sensory tools demonstrated significant reduction in bedtime resistance. → DOI: 10.1007/s12098-018-2747-4
📄 WHO Care for Child Development Package (2023)
Implemented across 54 low- and middle-income countries. Caregiver-administered structured routines form the evidence backbone of global ECD intervention. → PMC9978394
"These are not opinions. These are replicated findings across international peer-reviewed literature, confirmed by 20M+ Pinnacle clinical sessions."

ACT II — THE KNOWLEDGE TRANSFER
🛏️ Bedtime Routine Support with Therapeutic Materials
Parent-friendly alias: "The Peaceful Nights Protocol" | E-541 | Series: Toileting & Self-Care Independence in Children | Episode 541
What It Is
A structured, caregiver-administered home intervention using 9 validated therapeutic materials to scaffold the bedtime transition for children with developmental differences. Addresses four core challenges simultaneously: transition difficulty, sensory dysregulation, anxiety, and executive function demands.
What It Does
Reduces bedtime resistance, shortens time from announcement to sleep onset, decreases nighttime anxiety, builds child independence in routine completion, and restores parental wellbeing in the evening hours.
Who It's For
Children aged 2–12 years with autism, ADHD, sensory processing differences, anxiety, or any child whose bedtime consistently requires more than 45 minutes and involves significant resistance.
Duration | Frequency | Age Range | Setting | |
20–35 min total routine | Daily (every night) | 2–12 years | Home — Bedroom/Bathroom |
Domain E: Self-Care Independence
🌙 Sleep Preparation
🔄 Transition Support
🧘 Sensory Regulation
😰 Anxiety Management
📋 Executive Function Support

🏥 Multi-Disciplinary Application
This technique crosses therapy boundaries — because bedtime resistance crosses every domain of a child's functioning.
🔶 Occupational Therapist (Primary Lead)
Assesses sensory profile underlying bedtime difficulty. Prescribes specific sensory tools (weighted blanket weight, tactile inputs). Designs environmental setup and routine structure. Monitors self-regulation and independence progression.
🔷 Behavioral Therapist / BCBA
Implements the bedtime pass system and reinforcement structure. Applies extinction protocols for nighttime callback behaviors. Trains parents in consistent implementation. Tracks data on routine compliance and sleep onset latency.
🟢 Pediatric Psychologist
Addresses anxiety component. Creates personalized social stories for fear reframing. Implements cognitive techniques for worry externalization. Supports parent-child separation anxiety resolution.
🟠 Developmental Pediatrician
Rules out medical causes (sleep apnea, restless legs, melatonin dysregulation). Manages medication reviews. Integrates sleep specialist referral when indicated. Connects circadian rhythm interventions with behavioral approach.
"Sleep is simultaneously sensory, behavioral, emotional, physiological, and relational. The Pinnacle FusionModule™ coordinates all four disciplines into one convergent bedtime plan."

🎯 Therapeutic Targets
This isn't a random activity. It's a precision tool targeting specific mechanisms.
Target | "I'll know it's working when..." | Timeline | |
Primary | Bedtime takes under 45 minutes without battles | Weeks 3–4 | |
Secondary | Child initiates routine steps without prompting | Weeks 5–6 | |
Tertiary | Child says "time to check my chart" spontaneously | Weeks 7–8 |
Meta-analysis (PMC10955541): Sensory integration therapy effectively promoted social skills (primary), adaptive behavior (secondary), and gross/fine motor skills (tertiary) across 24 studies.

🛒 The 9 Therapeutic Materials
Every material below addresses a specific mechanism. These are not purchases — they are infrastructure for your child's nervous system.
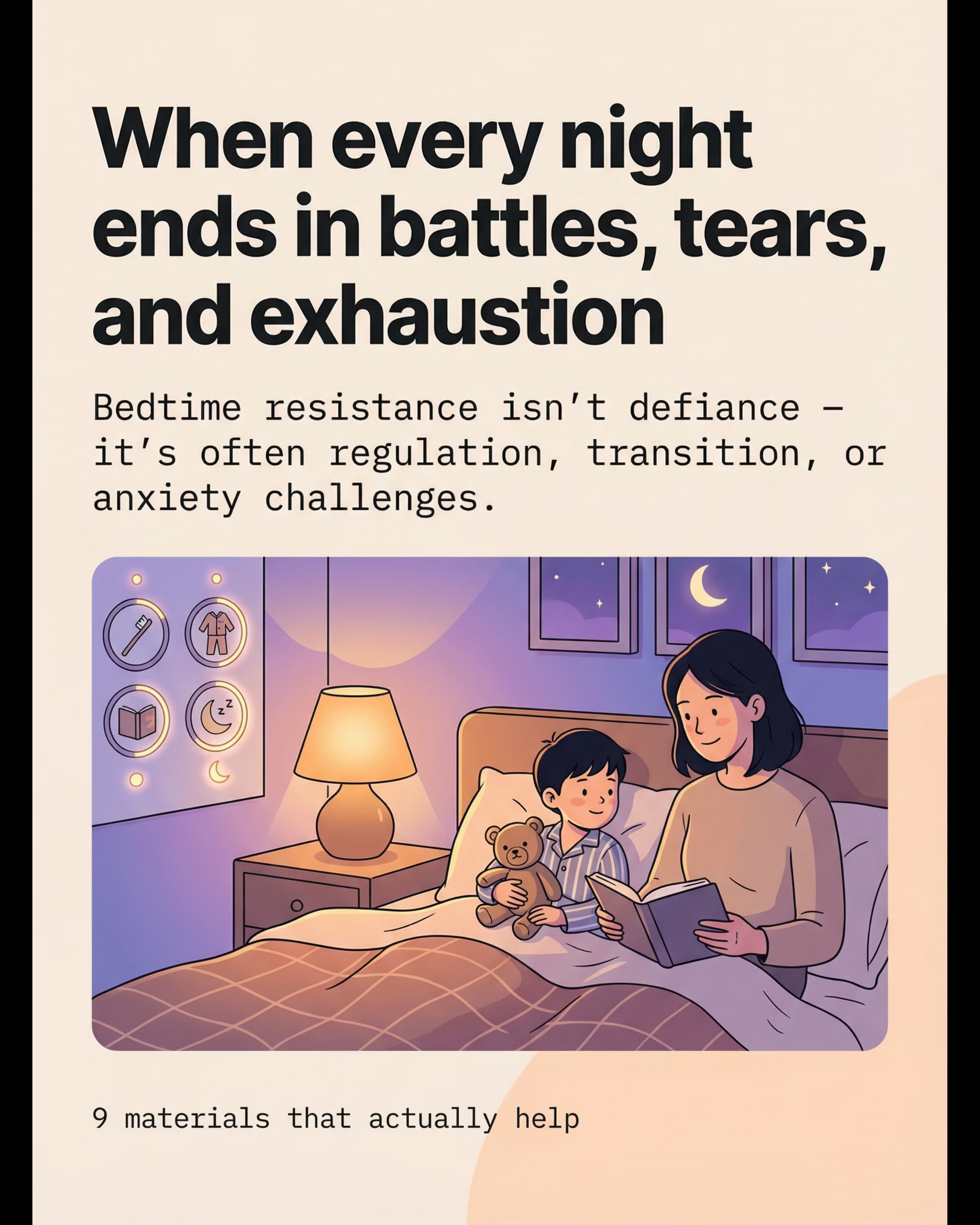
1. Visual Bedtime Routine Chart
Why it works: Externalizes the sequence, reduces PFC load, shifts authority from parent to chart — eliminating power struggles.
₹200–800 | DIY: ✅ | Search Amazon.in

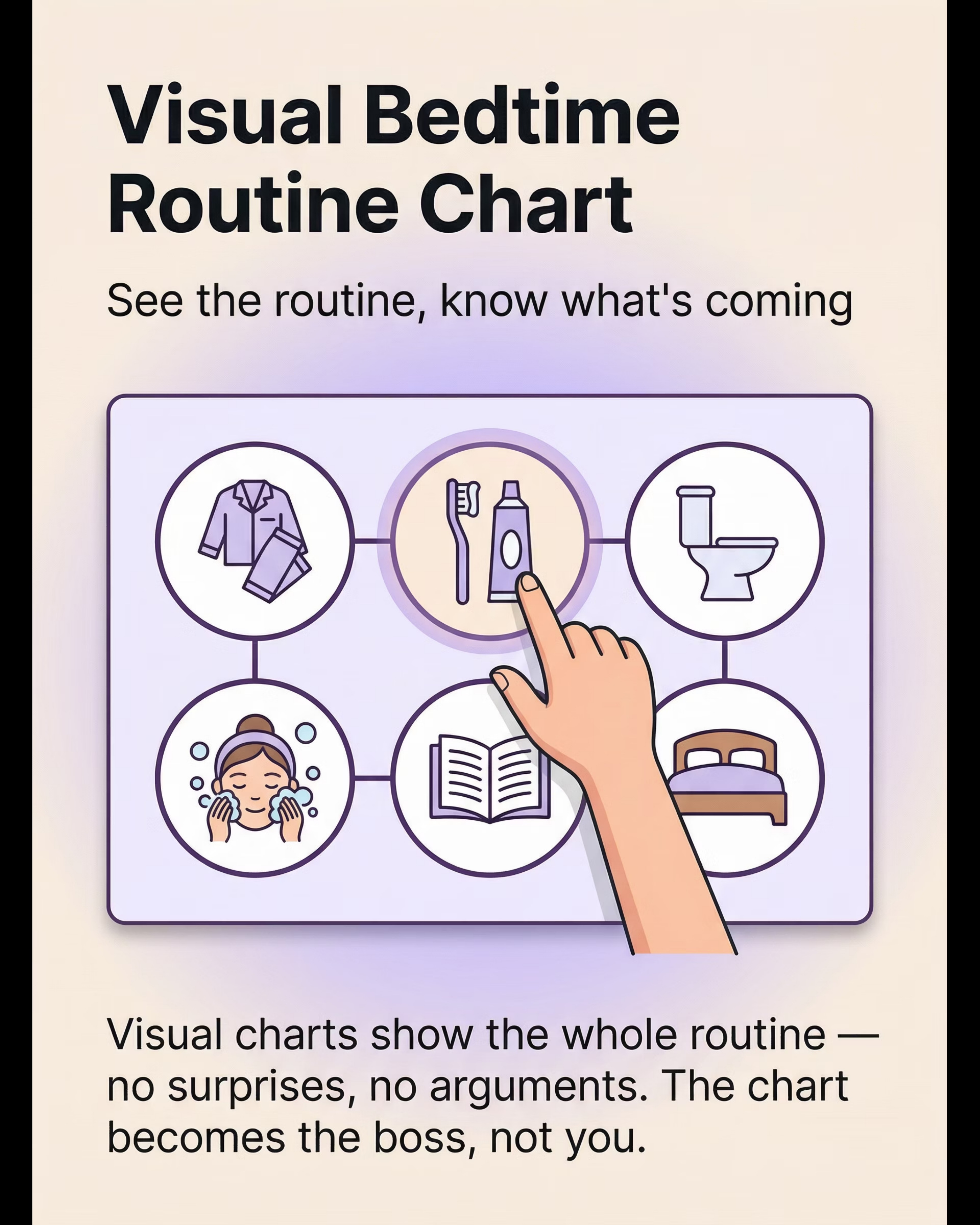
2. Visual Timer for Transition Warnings
Why it works: Makes the approaching transition concrete and visible. 5 minutes of warning prevents 30 minutes of battle.
₹800–2,500 | DIY: ✅ | Search Amazon.in

3. Weighted Blanket for Calming
Why it works: Activates parasympathetic nervous system via deep pressure proprioceptive input — equivalent to being held/swaddled.
₹2,000–6,000 | ~10% body weight | ⚠️ Not under age 2 | Search Amazon.in

4. Calm-Down Sensory Basket
Why it works: Helps dysregulated body shift from activated to settled state. Matched to child's specific sensory profile.
₹200–1,500 | DIY: ✅ household items | Search Amazon.in
5. Bedtime Social Story / Book
Why it works: Explicit instruction on bedtime expectations. Normalizes "not feeling tired." Directly addresses specific fears.
₹100–500 | DIY: ✅ photos of child + home | Search Amazon.in

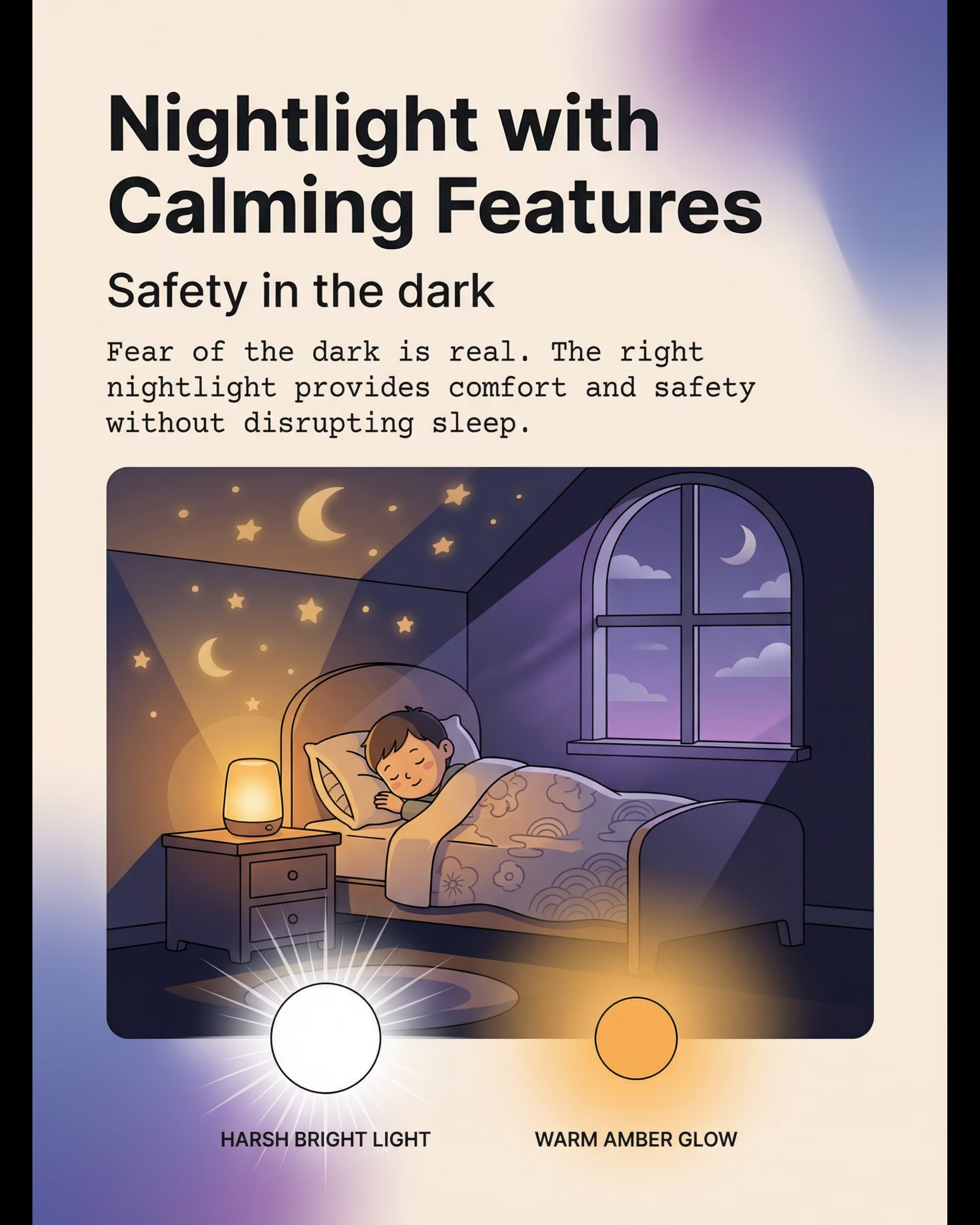
6. Nightlight — Warm Tone
Why it works: Addresses fear of dark without blue-light melatonin suppression. Warm amber provides safety cue without disrupting sleep physiology.
₹300–2,000 | SKU 118 — ₹425 (Pinnacle Link)

7. White Noise Machine
Why it works: Creates consistent auditory backdrop masking environmental noise disruptions. Becomes sleep-onset cue through conditioning.
₹500–3,000 | DIY: ✅ Spotify/YouTube | Search Amazon.in

8. Worry Box or Worry Journal
Why it works: Externalizes and contains nighttime worry thoughts. Ritual of "putting worries away" gives child agency over anxiety.
₹100–400 | DIY: ✅ decorated shoebox | Search Amazon.in

9. Bedtime Pass System (Token/Card Set)
Why it works: Transforms endless callback behavior into a bounded system. Gives child agency while parents maintain limits. Unused passes earn rewards.
₹50–200 | DIY: ✅ laminated index cards | SKU 390 — ₹364 (Pinnacle Link)
Approach | Cost Range | Per-Night (12 months) | |
DIY all materials | ₹0–200 | ₹0–1/night | |
Essential starter kit only | ₹500–1,500 | ₹2–5/night | |
Full material set (purchased) | ₹4,000–14,000 | ₹12–40/night |

🏠 Every Family Can Start Today
Therapeutic materials should never be a barrier. Every technique in this protocol has a zero-cost version.
The WHO Care for Child Development Package, implemented across 54 low- and middle-income countries, demonstrates that structured caregiver routines using household materials produce measurable developmental outcomes equivalent to clinical-grade materials in many contexts.
Material | 🛒 Purchase Option | 🏠 DIY Today — ₹0 | Why It Works | |
Visual Routine Chart | ₹200–800 printed chart | Print icons from Google Images, glue to cardboard, laminate with tape | Brain responds to the image, not the price tag | |
Visual Timer | ₹800–2,500 Time Timer | Phone timer propped facing child, or sand hourglass from kitchen | Visual countdown is the mechanism — device format matters less | |
Weighted Blanket | ₹2,000–6,000 | Layer 2–3 regular blankets; rice-filled cloth bag on lap | Consistent distributed weight is what calms the nervous system | |
Calm-Down Basket | ₹200–1,500 | Rubber band ball, soft socks, small rice bag, smooth stone | Sensory input is the mechanism — novel "basket" container helps association | |
Bedtime Social Story | ₹100–500 | Print 6 photos of your child doing each routine step, bind with stapler | Personalized photos actually work better — child sees themselves succeeding | |
Nightlight | ₹300–2,000 | Dim a lamp to lowest; cover with warm-toned fabric or candle-flicker LED | Warm light tone is the mechanism — melatonin suppression avoided | |
White Noise | ₹500–3,000 | YouTube "brown noise for kids" on phone face-down, volume at 30% | Consistent auditory masking is the mechanism — source doesn't matter | |
Worry Box | ₹100–400 | Decorate any small box with slot cut in lid | The ritual is the mechanism — the box just needs to feel "special" | |
Bedtime Passes | ₹50–200 | Write on index cards, cut and laminate with tape | The token system is the mechanism — visual concreteness is all that's needed |
⚠️When the clinical-grade material is non-negotiable: Weighted blanket — if child has significant sensory seeking behaviors, approximate DIY may be insufficient. A clinical-grade blanket with correct weight provides therapeutic-level input that household layering may not replicate.
⚠️ Safety Gate — Read Before Executing
Every caregiver must review this before beginning the bedtime protocol.
🔴 DO NOT PROCEED IF:
- Child is currently in active medical crisis or febrile illness
- Weighted blanket is being considered for child under 2 years
- Child shows signs of active sleep disorder (gasping, breath-holding, extreme snoring) — refer to pediatrician first
- Child has a history of panic attacks at bedtime — consult psychologist before implementing
- Parent is not in a regulated state — a dysregulated parent will dysregulate the child further
🟡 MODIFY BEFORE PROCEEDING:
- Child had a meltdown within the past 2 hours: shorten protocol, skip sensory basket, prioritize calm over compliance
- Child is overtired (missed nap, late start): skip worries box and passes, focus on chart + weighted blanket only
- Child has sensory aversion to textures: introduce weighted blanket gradually over 3–5 nights
🟢 PROCEED WHEN:
- Child has eaten and had fluids within 60–90 minutes of bedtime
- No active screens for minimum 30 minutes before protocol begins
- Parent is calm, regulated, and has 35–45 minutes available without interruption
- Space is set up per Card 12 guidelines
Material | Safety Note | |
Weighted blanket | ≤10% of child's body weight. Never exceed. Child must be able to remove independently. | |
Sensory tools | Check age appropriateness. No small parts for under 3. All items checked for allergens. | |
Nightlight | Electrical safety. No cords near bedding. Warm tone only. | |
White noise | Maximum 50dB at child's position. Device cords safely managed. |
🆘STOP IMMEDIATELY IF child displays severe distress escalating beyond baseline, self-injurious behavior, vomiting, difficulty breathing, or any sign the technique is increasing rather than decreasing arousal.
FREE National Autism Helpline: 9100 181 181 (24×7 | 16+ languages) — call if unsure about any safety indicator.
FREE National Autism Helpline: 9100 181 181 (24×7 | 16+ languages) — call if unsure about any safety indicator.

🏠 Stage Your Environment
The environment must be right before the child enters. Spatial setup prevents 80% of execution failures.
Bedroom Setup (Position Each Item)
Nightlight [6]
Warm, dim — positioned in corner. Plugged in and on before child enters.
White Noise Machine [7]
On and at consistent level. Far corner or directed away from shared wall.
Weighted Blanket [3]
Already on bed — not introduced during routine. Child enters to find it ready.
Visual Chart [1] + Worry Box [8]
Chart at child's eye level on wall. Worry box on bedside table with paper and pencil.
Pre-Bed Wind-Down Zone (Living Area)
Visual Timer [2]
Visible to child during wind-down. Set 20 minutes before bedtime.
Calm-Down Basket [4]
Accessible during timer countdown. Put away before child moves to bedroom.
Bedtime Passes [9]
2–3 passes given to child at routine start. Child holds them physically.
❌ Remove all screens | ❌ Stimulating toys | ❌ Siblings causing overstimulation | ❌ Bright overhead lights (switch to lamps 30 min before) | ✅ Room temp: 18–22°C | ✅ Visual chart posted in bathroom AND bedroom
"The environment is the co-therapist. A correctly staged bedroom reduces arousal 15–20% before the child even enters." — Pinnacle OT Team

✅ Pre-Session Readiness Assessment (60 seconds)
The best bedtime session is one that starts right. 60 seconds of assessment now saves 90 minutes of battle later.
# | Indicator | ✅ Go | ⚠️ Modify | ❌ Postpone | |
1 | Child has eaten dinner and had water | Ready | Had light snack | Hasn't eaten → feed first | |
2 | No screens for 30+ minutes | Ready | 15 mins screen-free | On screens now → wait 20 mins | |
3 | Child is not in active meltdown | Ready | Slightly elevated | Dysregulated → calm-down first | |
4 | Parent is regulated and has 35+ min | Ready | A bit stressed | Overwhelmed → brief parent reset first | |
5 | Within 30 min of target bedtime | Ready | 45 min early | Way too early → start wind-down only | |
6 | No major schedule disruption today | Ready | Minor disruption | Major disruption → simplified routine only |
🟢 ALL GREEN → FULL PROTOCOL
Proceed to Step 1: The Invitation. All conditions met.
🟡 1–2 AMBER → MODIFIED PROTOCOL
Skip worries box and passes tonight. Focus on chart → weighted blanket → lights out. Accept reduced compliance, reinforce attempts.
🔴 ANY RED → MINIMAL PROTOCOL
Do: warm bath or shower, weighted blanket, lights dim. Do NOT implement passes or worry box. The environment works even when the protocol doesn't.
STEP 01 of 06 | ⏱️ 5 min before routine | 🌙 Wind-Down Signal
The transition begins 20 minutes before bed. Not at bedtime. Before it.
[20 minutes before bedtime, set the visual timer where child can see it]
"Hey [child's name] — look at the timer. When the red is all gone, it's time to start getting ready for bed. Right now you have 20 minutes. You can keep playing."
[10 minutes remaining] "Hey — timer check. 10 minutes left. Getting close."
[5 minutes remaining] "5 minutes! Almost time. Start finishing up what you're doing."
Body Language Guidance
Use a calm, matter-of-fact tone — not apologetic, not confrontational. The timer is the authority, not you. Avoid phrasing it as "you HAVE to stop soon." The timer communicates it more neutrally.
What Acceptance Looks Like
Child glances at timer, may protest mildly but continues activity without escalation. This is success — awareness without refusal.
If Child Covers or Avoids Timer
Remove timer from sight after each verbal warning. Use verbal-only countdown. Timer works for most children but may increase anxiety in a small subset — observe and adjust.
Calm-Down Basket Activation
Bring calm-down basket to child now. "You can use these while the timer counts down." The basket begins the sensory transition before the routine even starts.
ABA Pairing Procedures: Establishing motivating operations before demand placement. NCAEP (2020): Visual supports classified as evidence-based practice for autism.

STEP 02 of 06 | ⏱️ 10–15 minutes | Routine Execution
"Check your chart. What's first?"
[Timer reaches zero. Calm transition from wind-down zone to bathroom/bedroom.]
"Okay — timer's done. Time to start. Check the chart — what's first?"
Step A — Pajamas
"What does the chart say? Pajamas. Let's go." Sensory note: If child is sensitive to pajama textures, keep sensory-friendly pajamas stocked — this is a non-negotiable accommodation.
Step B — Brush Teeth
"The chart says brush teeth — not me. What does the chart say to do?" Consider: Electric toothbrush for sensory-sensitive children; consistent flavored toothpaste.
Step C — Toilet / Bathroom
Prevents the "I need to go to the bathroom" callback after lights out. This is addressed proactively IN the routine.
Step D — Wash Face / Hands
Brief sensory input — warm water can be calming for some, aversive for others. Match water temperature to child's preference.
Step E — Story / Social Story
Read the bedtime social story (Material 5). 1 book ONLY — the visual timer governs this. Set 5-minute timer for story time.
Step F — Goodnight Hugs
The relational anchor. Always present. Not negotiable. "One long goodnight hug" — provides proprioceptive input AND relational closure.
Step G — Into Bed / Chart Check Done
"All done! Let's check off all the boxes." Child marks completion of routine on chart. Deliver reinforcement within 3 seconds of behavior completion.
After chart completion: "You did every step on the chart. That's incredible. Let's check the boxes together." Immediate specific reinforcement within 3 seconds of behavior completion is essential.
STEP 03 of 06 | ⏱️ 5–10 minutes | Sleep-Onset Support
The routine is done. Now the nervous system needs to complete its transition to sleep.
Lights Out / Nightlight On
"Lights going off. Nightlight coming on." Warm nightlight activates — this is the sleep-onset cue the brain learns over time through consistent pairing.
White Noise On
Turn on white noise machine. Consistent sound level. "There's the sleep sound." The same sound every night becomes a powerful conditioning cue.
Under the Weighted Blanket
Child settles under weighted blanket. "Can you feel the blanket? It's helping your body feel cozy and settled." Allow 60–90 seconds for deep pressure effect to begin.
Worry Box (if anxiety present)
"Is there anything worrying you tonight?" Child draws or tells parent worry → parent writes it → into the box. "That worry is in the box now. It will wait there until tomorrow. You can rest."
Bedtime Passes Handover
"Here are your passes. If you need something — water, bathroom, one hug — give me a pass. When they're gone, they're gone. Unused passes buy you something good tomorrow morning."
Final Parental Transition
"I love you. The chart is done. You did great. I'll check on you in [X minutes]." Leave room. Monitor from outside if needed.
❌ Common Errors
- Staying too long after passes are given → undermines the pass system
- Negotiating extra stories after routine completion → resets authority to parent
- Responding to non-pass requests — be warm but consistent: "Use a pass if you need it"
✅ Ideal Child Response
Child settles under blanket, may fidget briefly, slows movement as deep pressure takes effect, uses worry box if anxious, may exchange 1–2 passes for genuine needs, drifts toward sleep onset.

STEP 04 of 06 | Daily Implementation | Habituation and Dosage
Therapeutic dosage for bedtime: every night, same sequence, same tools. Consistency IS the treatment.
Week | Expected Compliance | Parent Action | |
Week 1–2 | 40–60% — child tests the system | Hold the line. Consistency matters more than compliance. | |
Week 3–4 | 60–75% — routine beginning to feel familiar | Begin reducing prompts. Let the chart do more work. | |
Week 5–8 | 75–90% — child anticipates steps | Fade parent presence during routine. Add independence steps. | |
Week 8+ | 85–95% — routine is habituated | Maintenance mode. Keep tools in place. |
On Good Days — "Advance" Variation
Reduce parent verbal prompts to zero — child follows chart entirely independently. Parent is present but silent. Add "I did it myself!" reward for independent completion.
On Hard Days — "Simplified" Variation
Skip worry box and passes entirely. Shorten to: pajamas → brush teeth → weighted blanket → lights out. Do not enforce chart if child is dysregulated — prioritize the settling environment.
For Sensory Seekers — "Heavy Input" Variation
Add joint compression before bed: 10–15 firm presses at shoulders and hips. "Wall push-ups" — child pushes against wall for 10 counts. Heavy blanket layering within safe weight limits.
For Sensory Avoiders — "Light Input" Variation
Minimal-texture pajamas. Lighter blanket (skip weighted if needed). Dim rather than warm light. White noise at lowest effective volume. Shorter hugs.
"3 Good Nights > 10 Forced Nights. A calm, brief, partial routine executed consistently builds more progress than a perfect long routine that ends in battle. Accept the partial win."

STEP 05 of 06 | ⏱️ Within 3 seconds of desired behavior | Reinforcement Delivery
Timing matters more than magnitude. Immediate and specific is everything.
For completing the routine without battles:
"You checked every box on the chart! That is amazing. You did it."
For passes remaining at morning:
"You still have [X] passes! You saved them. Let's trade them for [reward]."
For independent step completion:
"You put on your pajamas without me even asking. That's YOU running your own routine."
For settling quickly:
"You got cozy under your blanket and stayed. That's a superstar bedtime."
Reinforcement Type | Example | Timing | |
Social (immediate) | "Amazing job!" + hug | Within 3 seconds of behavior | |
Token (deferred) | Unused pass → morning reward | Next morning | |
Activity (deferred) | Extra story tomorrow | Next day | |
Privilege (deferred) | Choose Saturday movie | Next weekend |
Canon Products: SKU 803 — ₹589 Reward/reinforcement menu | SKU 390 — ₹364 Token/sticker system
Celebrate the Attempt, Not Just the Success: "You tried to stay in bed even when it was hard. That counts." For children with ABA goals: integrate the bedtime pass system with the child's existing token economy. Each unused pass = 1 token.

STEP 06 of 06 | ⏱️ Final 3–5 minutes | Parent Withdrawal & Sleep Onset
The last parent action is the most important: a clean, warm, consistent exit.
"Everything is set. Your chart is done. The blanket is on. Your passes are there. The nightlight is on. I love you. Goodnight."
[Leave the room. Close door to preferred position.]
Gradual Fading Over 2–3 Weeks (If Child Resists Exit)
Week 1
Sit on edge of bed until drowsy (not asleep)
Week 2
Sit in chair in room, not on bed
Week 3
Sit in doorway, visible but not present
Week 4
Brief check-in after 5 minutes from hallway
Week 5+
Lights out, parent exits immediately — pass system handles genuine needs
Pass Exchange After Exit
If child calls out: wait to see if it's a pass exchange request or a test. If pass is presented: respond warmly, honor the request, brief interaction only. If no pass presented: "You can use a pass if you need something. Love you."
If Child Leaves Bed
Calmly, silently return child to bed. No discussion. No lecture. No eye contact beyond "It's bedtime." The silence communicates more than words. Be warm but non-reactive.
Parent Self-Care Note
The first 2 weeks of consistent protocol implementation are the hardest. Behavior may temporarily worsen (extinction burst) before it improves. This is neurologically expected. Hold the system. Your consistency through the hard nights is the treatment itself.

📊 60-Second Data Capture
60 seconds of data now saves hours of guessing later. Record these 3 things tonight.
⏱️ Total Routine Time
From "timer hits zero" to "lights out." Use a stopwatch — log in minutes. Your baseline week 1 number is your starting point.
🔥 Resistance Level (0–5)
0 = No resistance → 5 = Full meltdown. Circle: 0 · 1 · 2 · 3 · 4 · 5. This single number tells you more than a narrative journal.
🎫 Passes Used
How many passes exchanged post-lights-out. Number: 0 / 1 / 2 / 3+. Trending down over weeks = the pass system is working.
Data Interpretation: Track for 2 weeks before drawing conclusions. Look for the TREND, not the night. A bad Tuesday after a good Monday is normal. A trend line moving from 4.5 average resistance → 2.5 average over 2 weeks is real progress. One bad night does not erase a good system.
"Your data helps every child like yours. When 10,000 families contribute E-541 tracking data, GPT-OS® can predict within 2 weeks whether a child needs the anxiety intervention or the sensory intervention — reducing guesswork for every future family."
🔧 Real-World Troubleshooting
The session was imperfect. That's data — not failure. Here's what likely happened and what to do differently tomorrow.
"My child ignored the visual chart entirely"
What happened: The chart is new — it has no behavioral history yet. It takes 5–10 nights for the chart to become a familiar cue.
Next time: Walk through the chart WITH the child for the first 7 nights. Narrate each step as you point to it. The chart builds authority through repetition.
Next time: Walk through the chart WITH the child for the first 7 nights. Narrate each step as you point to it. The chart builds authority through repetition.
"The weighted blanket made them more restless, not less"
What happened: Some children are initially stimulated by novel deep pressure before the calming effect kicks in. Others may not be deep-pressure seekers.
Next time: Reduce weight. Introduce for just the first 10 minutes. If consistently activating → skip and consult OT for sensory profile assessment.
Next time: Reduce weight. Introduce for just the first 10 minutes. If consistently activating → skip and consult OT for sensory profile assessment.
"They used all 3 passes within 5 minutes"
What happened: Child is either genuinely anxious or testing the system.
Next time: Ensure genuine needs are met before passes are given. Increase to 4 passes for 2 weeks, then reduce. Reward unused passes generously the first week to build incentive.
Next time: Ensure genuine needs are met before passes are given. Increase to 4 passes for 2 weeks, then reduce. Reward unused passes generously the first week to build incentive.
"The worry box became a stalling tool — 20 worries each night"
What happened: The worry-sharing ritual has become an attention-access behavior.
Next time: Put a timer on worry time. "3 minutes for worries — set the timer." When timer ends, box closes. No more worries after the box closes.
Next time: Put a timer on worry time. "3 minutes for worries — set the timer." When timer ends, box closes. No more worries after the box closes.
"My child destroyed the routine chart in frustration"
What happened: Chart was not yet a positive or neutral stimulus — it may have been experienced as threatening.
Next time: Rebuild the chart WITH the child on a calm afternoon. Let them decorate it, choose the images, design it. Child-authored charts have stronger buy-in.
Next time: Rebuild the chart WITH the child on a calm afternoon. Let them decorate it, choose the images, design it. Child-authored charts have stronger buy-in.
"My child keeps getting out of bed despite the pass system"
What happened: The pass system hasn't established behavioral history yet. May also be anxiety-driven.
Next time: Be consistent for 14 nights before evaluating. First 5–7 nights will likely show extinction burst. If persists beyond 2 weeks, assess for primary anxiety — consider adding worry box and social story.
Next time: Be consistent for 14 nights before evaluating. First 5–7 nights will likely show extinction burst. If persists beyond 2 weeks, assess for primary anxiety — consider adding worry box and social story.
"A session that ends early is not a failure. It is data about today's arousal level, health status, or environmental context. Reset tomorrow."
⚙️ Personalize for Your Child
Every child is different. This protocol adapts to your child's profile — not the other way around.
Child Profile | Adaptation | |
ADHD (arousal dysregulation) | Extend wind-down to 30 min. Heavy proprioceptive input before bed (wall push-ups, joint compression). White noise slightly higher volume. Earlier bedtime by 20 min. | |
Autism (transition + sensory) | Extremely consistent sequence — no variations without preparation. Sensory-friendly pajamas non-negotiable. Visual chart is the highest priority tool. Social story specifically about their bedroom. | |
Anxiety (fear/worry dominant) | Worry box is the highest priority tool. Personalized social story addressing specific fears. Gradual parent fading (slower timeline). Both nightlight and white noise present. | |
Sensory Seeker | Maximize deep pressure before bed. Trampoline 30 min before routine. Heaviest safe weighted blanket. Full-body "burrito" wrap as play before settling. | |
Sensory Avoider | Lightest textures. Skip or minimize weighted blanket. White noise very low. Room slightly warmer. Fewer sensory tools — less input is calming. | |
Age 2–4 | Visual chart with 4 photos max. Parent present for full settling. 1 pass only. Focus on weighted blanket and nightlight. | |
Age 8–12 | Child creates own chart. 2 passes managed by child. Encourage self-monitoring with simple tally sheet. |
15–20
Age 2–4
Minutes total protocol duration
20–30
Age 4–7
Minutes total protocol duration
25–35
Age 7–10
Minutes total protocol duration
30–40
Age 10–12
Minutes total protocol duration

ACT IV — THE PROGRESS ARC | 📅 Week 1–2
Don't look for mastery. Look for these specific micro-signals.
WEEK 1–2: BASELINE ESTABLISHMENT — You Are Here [15%]
✅ Observable Indicators This Week
- Child looks at visual timer when it's set (awareness, not compliance)
- Child enters the routine with slightly less initial protest than before
- One or two chart steps completed without prompting
- Child touches or acknowledges the worry box (even if doesn't use it)
- Bedtime total time hasn't increased (holding steady = progress in week 1)
❌ What Is NOT Progress Yet
- Child following entire chart independently (too early)
- Passes unused at morning (too early — system is still novel)
- Sleep onset under 30 minutes (physiological habituation takes 3–4 weeks)
- Zero resistance (resistance will likely INCREASE before it decreases — extinction burst is normal)
"In weeks 1–2, you may see more behavior before less. This is neurologically expected — the child is testing whether the new system is real. Your consistency through this phase is the treatment. Hold the system."
Parent Emotional Preparation: Measure patience in weeks, not nights. One bad night doesn't erase a good system. Stay the course. PMC11506176: Sensory integration outcomes emerge across 8–12 week timelines — early indicators focus on tolerance and participation rather than mastery.

📅 Week 3–4 | Consolidation
Neural pathways are forming. Look for these "brain building" signals.
WEEK 3–4: CONSOLIDATION — You Are Here [40%]
Anticipatory Behavior
Child begins to anticipate routine steps before being prompted. Child moves toward the bathroom when timer ends — not because you told them to.
Chart Referenced by Child
Chart is referenced by child, not just by parent. When your child starts saying "I need to check my chart" — that is the neural pathway forming.
Resistance Shortening
Resistance is still present but shorter in duration. Total bedtime time has reduced by 15–25 minutes from baseline. Sleep onset is beginning to accelerate.
Worry Box Self-Initiated
Child uses worry box for at least 3–4 nights per week without prompting. The ritual is becoming internalized rather than parent-directed.
"You may notice you're less anxious about evenings. Your own nervous system is also habituating to the new routine. This is a two-person intervention." — Pinnacle Parent Research
If child is consistently showing 5+ of the above indicators: begin reducing parent prompts. Let the chart do more. Stay present but be quieter. Neuroplasticity evidence: synaptic strengthening through structured repeated input follows predictable timelines.

📅 Week 5–8 | Mastery Phase
These are the mastery criteria. When your child hits them, they are genuinely ready for the next level.
WEEK 5–8: MASTERY — You Are Here [75%]
Criterion | Mastery Definition | How to Measure | |
Routine Completion | Completes all 6–8 chart steps with ≤1 verbal prompt per night | Parent tally each night | |
Resistance Level | Average resistance ≤1.5/5 over 7 consecutive nights | Nightly tracker average | |
Sleep Onset | Asleep within 30 minutes of lights-out on ≥5 of 7 nights | Parent observation log | |
Pass Usage | Uses ≤1 pass per night on ≥5 of 7 nights | Pass count each morning | |
Independence | Initiates at least 3 routine steps without prompting | Parent prompt tracking |
🏅 Mastery Unlocked
Bedtime Routine Independence | E-541 | Week 5–8 | GPT-OS® Verified
Generalization Indicators
- Routine skills beginning to appear in other settings (grandparents' home, travel)
- Child verbally explains routine to a sibling or visitor
- Child requests their materials ("Where's my chart?") when routine deviates
When to Move Forward
At mastery: Move to E-542 Mealtime Routine. Maintain the bedtime protocol — mastered routines require maintenance, not abandonment. The tools stay; the parent effort reduces.

You did this. Your child grew because of your commitment.
Five to eight weeks ago, evenings in your home ended in battles, tears, and exhaustion. Tonight, your child followed their chart, settled under their weighted blanket, put their worries in the box, managed their own passes, and drifted to sleep in under 30 minutes.
You did not do this TO your child. You did this WITH your child. You built a system. You held it on the hard nights. You stayed consistent when behavior got worse before it got better. You believed it was possible. That is not ordinary. That is extraordinary parenting.
🎉 Family Celebration Suggestion
This weekend: a family celebration of your child's bedtime mastery. Let THEM choose the activity. Frame it explicitly: "You earned this — you've been incredible at your bedtime routine."
📷 Photo / Journal Prompt
Take a photo of your child's completed visual chart tonight. Date it. This is a developmental milestone worth documenting as clearly as a first step or first word.
You arrived on the first card exhausted and doubting yourself. You leave this card as a family that solved a problem together. The nervous system that was struggling has been scaffolded to success.
🎉 Share your win with the Pinnacle community: 9100 181 181 | care@pinnacleblooms.org
🚨 Clinical Guardrails
Even in the celebration zone — these specific signs mean pause and seek professional consultation.
🚨 Bedtime resistance persists at ≥3/5 after 6 weeks of consistent implementation
May indicate primary sleep disorder, unmanaged anxiety disorder, or medication effect. Escalate: Pediatrician + Child Psychologist consultation.
🚨 Child displays self-injurious behavior at bedtime
Stop the behavioral approach immediately. Escalate urgently: BCBA + Developmental Pediatrician within 1 week.
🚨 Signs of sleep-disordered breathing (snoring, gasping, mouth breathing)
This is a medical issue, not a behavioral one. Escalate: Pediatrician for sleep study referral.
🚨 Nighttime fears are increasing, not decreasing, after 4 weeks
Indicates primary anxiety disorder requiring psychological intervention beyond these materials. Escalate: Child Psychologist.
🚨 Child is consistently overtired, falling asleep in school, or unable to wake
May indicate circadian phase delay, sleep apnea, or inadequate total sleep. Escalate: Developmental Pediatrician.
🚨 Parent-child relationship is significantly deteriorating around bedtime
Relational damage requires repair before behavioral protocol re-implementation. Escalate: Family Therapist or Child Psychologist for co-regulation support.
📍 Find Your Nearest Pinnacle Center | FREE Helpline: 9100 181 181 (24×7)

🗺️ Developmental GPS
You're not done. You're on a journey. Here is where you've been, where you are, and where you're going.
Long-Term Developmental Goal
Full self-care independence across all daily living routines → Daily Living Skills Readiness Index mastery → Preparation for school independence, social participation, and self-advocacy across every domain of life.
Pinnacle Progression Principle
"Mastered techniques are maintained, not abandoned. Each routine builds on the previous. E-541 mastery makes E-542 and E-543 significantly easier — the child has internalized the visual chart principle."
GPT-OS® Integration
See your child's full progression plan, track mastery across techniques, and receive personalized next-step recommendations based on your family's data.
🔗 Related Techniques
You already understand the chart principle. These techniques use the same tools — you're 70% ready.
📋 E-540 — Morning Routine Support
Domain E | Difficulty: Core | Materials: Visual Chart ✅ (you own it) | 9-step routine protocol for morning independence
📋 E-542 — Mealtime Routine Independence
Domain E | Difficulty: Core | Materials: Visual Chart ✅ + Timer ✅ | Structured mealtime sequence building on the same chart framework
📋 E-543 — Homework Routine
Domain E | Difficulty: Intermediate | Materials: Visual Chart ✅ + Timer ✅ | After-school routine structure and independence
📋 D-448 — Bedtime Resistance (Behavioral)
Domain D | Difficulty: Core | Materials: Reinforcement Menu ✅ + Passes ✅ | ABA-focused protocol for limit-testing at bedtime
📋 I-792 — Bedtime Transition (Autism-Specific)
Domain I | Difficulty: Advanced | Materials: Visual Chart ✅ + Social Story ✅ | Deep autism-specific protocol for rigid transition challenges
📋 E-544 — Getting Dressed Independently
Domain E | Difficulty: Core | Materials: Visual Chart ✅ | Morning/evening dressing routine protocol — natural extension of E-541
✅ Visual Chart — You Own It
✅ Visual Timer — You Own It
✅ Weighted Blanket — You Own It
✅ Passes — You Own It
You have the infrastructure. These techniques are 70% ready to implement today.

🌐 The Whole Child | GPT-OS® Developmental Map
Bedtime routine is one piece of a larger developmental plan. Here is the whole picture.
Domain E Highlight
You are currently in Domain E: Self-Care Independence — Bedtime Routine (E-541). This technique contributes to the Daily Living Skills Readiness Index and Self-Regulation Readiness Index in your child's GPT-OS® profile.
Five Nurturing Care Components (WHO NCF)
✅ Responsive Caregiving
✅ Security & Safety
✅ Early Learning
⬜ Health
⬜ Nutrition
GPT-OS® Integration
"This technique is one piece of a larger plan. GPT-OS® coordinates techniques across all 12 domains into a single, convergent developmental plan — ensuring that progress in bedtime routine reinforces progress in behavioral regulation, social communication, and daily living simultaneously."
ACT V — THE COMMUNITY & ECOSYSTEM | 💬 Real Outcomes
From the Pinnacle Network — families who were where you are, and where they are now.
Vignette 1 — ADHD, Age 7
Before: Bedtime took 2–3 hours every night. Mother dreaded evenings from 3 PM. Child would stall, negotiate, call out repeatedly — often still awake at 11 PM.
After (8 weeks): Visual chart + visual timer + bedtime passes + weighted blanket. Bedtime now takes 40 minutes. Child initiates chart steps without prompting. Mother has her evenings back.
"The first week was actually harder. My son tested every part of the new system. But we held it. By week 5, he was telling ME when it was time to start the routine. That felt like a miracle."
Therapist Note: Bedtime battles in ADHD are primarily arousal regulation challenges. The weighted blanket addressed the physiological component; the pass system addressed the attention-access behavioral component. Both were necessary.
Vignette 2 — Autism, Age 5
Before: Bedtime meltdowns every night — screaming, refusing pajamas, fear of darkness, unable to separate from parent. Parents taking turns sleeping in child's room.
After (10 weeks): Visual chart (with child's own photos) + warm nightlight + social story + worry box + gradual parent fading. Child completes routine independently, calls out once (pass), falls asleep within 25 minutes.
"The social story was the thing for us. We read it every night for 3 weeks. My son started reciting it. He'd say 'the nightlight is keeping me safe.' He believed it because he had heard it 20 times. It became his own."
Therapist Note: For children with autism, explicit instruction through social stories addresses the gap between implicit learning (what neurotypical children absorb from observation) and explicit learning (what autistic children need stated directly).
Illustrative cases. Identifying details changed. Outcomes vary by child profile, underlying needs, and implementation consistency.

🤝 Join the Community
Isolation is the enemy of adherence. 12 million Indian families are navigating this exact challenge. Connect with them.
🟢 WhatsApp Support Group
Parents navigating sleep and bedtime challenges for children with ASD/ADHD. Real-time support from families who are in the same weeks of the same protocol.
💬 Online Forum
Pinnacle Parent Community — Bedtime & Sleep Independence thread. Share your data, your wins, your hard nights, your questions. pinnacleblooms.org/community
📍 Local Parent Meetups
Pinnacle center-based monthly parent groups across India. Find the group near you. 9100 181 181 to locate the nearest center and next meeting.
🏅 Peer Mentoring
Connect with a parent who has already navigated this exact challenge. Peer mentors are Pinnacle-trained experienced parents who have completed E-541 successfully.
"If you have navigated E-541 successfully — consider sharing your journey. Your consistency, your hard nights, your breakthrough week — that is exactly what another exhausted parent needs to hear at 11 PM."
🏥 Professional Support Layer
Home + clinic = maximum impact. These materials work best when backed by professional assessment and guidance.
Professional | What They Do for E-541 | |
Occupational Therapist | Sensory profile assessment, weighted blanket weight prescription, environmental setup guidance, visual schedule design | |
BCBA / Behavioral Therapist | Pass system design, reinforcement schedule, extinction protocol, data tracking setup | |
Child Psychologist | Anxiety assessment, social story creation, fear reframing, parent-child relationship support | |
Developmental Pediatrician | Medical clearance, sleep disorder screening, melatonin guidance, ADHD/autism medication review |
Teleconsultation
Can't reach a center? Pinnacle teleconsultation connects you to discipline-specific therapists by video. Available in 16+ languages. Book through pinnacleblooms.org/book
Home + Clinic Principle
"The protocol in this page is clinically validated for home execution. Professional support multiplies its effectiveness by 3–5×. An OT assessment of your child's sensory profile alone may reveal why one tool is working and another isn't."
📞 FREE National Autism Helpline
9100 181 181
24×7 | 16+ languages | FREE
"Call if you're unsure about any part of this protocol. Our team speaks your language."
"Call if you're unsure about any part of this protocol. Our team speaks your language."

📚 Evidence Base
The deeper reading for the curious, skeptical, and scientifically-minded parent.
📄 LEVEL I — PRISMA Systematic Review (2024)
16 studies (2013–2023) confirming visual schedules and sensory interventions as evidence-based practice for autism. Finding: Structured visual routines meet criteria for EBP for daily living skills including sleep preparation. → PMC11506176
📄 LEVEL I — Meta-Analysis (World J Clin Cases, 2024)
24 studies: sensory integration therapy promotes adaptive behavior including self-care. DOI: 10.12998/wjcc.v12.i7.1260 → PMC10955541
📄 LEVEL II — Indian RCT (Indian J Pediatr, 2019)
Padmanabha et al.: Home-based sensory intervention in Indian pediatric ASD population. Structured evening routines with sensory tools produced significant improvement in sleep onset. → DOI: 10.1007/s12098-018-2747-4
📄 LEVEL I — WHO Care for Child Development Package (2023)
Implemented in 54 LMICs. Consistent caregiver routines using visual + sensory scaffolding produce measurable ECD outcomes equivalent to clinic-based programs. → PMC9978394
📄 LEVEL I — NCAEP Evidence-Based Practices Report (2020)
National Clearinghouse on Autism Evidence and Practice: Visual supports and behavioral intervention classified as EBP for autism. Bedtime pass systems and visual schedule approaches meet NCAEP evidence-based practice criteria. → NCAEP 2020 Report
20M+
Clinical Sessions
Exclusive 1:1 therapy sessions in Pinnacle network
97%+
Measured Improvement
Across Daily Living Skills and Self-Regulation Readiness Indexes
70+
Centers
DPIIT DIPP8651 recognized innovation across India

⚙️ GPT-OS® Intelligence
Your nightly 60 seconds of data is not just for your child. It improves recommendations for every child like yours.
What GPT-OS® Learns From Your Data
- Sleep onset trajectory for this child's specific profile
- Which materials are most effective across children with similar profiles
- At what week most children show consolidation in this domain
- Which adaptation (sensory vs. anxiety vs. behavioral) is needed when compliance plateaus
🔒 Privacy Assurance
All data is anonymized and encrypted before population-level analysis. Your child's data is never individually identifiable beyond your own GPT-OS® profile.
"When 10,000 families contribute E-541 tracking data, GPT-OS® can predict within 2 weeks whether a child needs the anxiety intervention or the sensory intervention — reducing guesswork for every future family."

🎬 The Original Reel
Watch the 60-second reel that brought these 9 materials to life.
Reel E-541
Title: 9 Materials That Help With Bedtime Routine
Series: Toileting & Self-Care Independence in Children — Episode 541
Domain: E — Self-Care / Sleep / Daily Living Skills
Duration: ~75 seconds
Series: Toileting & Self-Care Independence in Children — Episode 541
Domain: E — Self-Care / Sleep / Daily Living Skills
Duration: ~75 seconds
Presented by the Pinnacle Blooms Consortium® Occupational Therapy and Behavioral Support teams. This reel demonstrates each of the 9 materials in a real home bedtime context with a child aged 6 navigating autism + ADHD comorbidity.
NCAEP (2020): Video modeling is classified as an evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition faster than text alone.
Related Reels in This Series
← E-540: 9 Materials That Help With Morning Routine
★ E-541: 9 Materials That Help With Bedtime Routine (You Are Here)
→ E-542: 9 Materials That Help With Mealtime Routine

📤 Generalize the Knowledge
If only one caregiver executes this protocol, the impact is halved. Consistency across ALL caregivers multiplies results.
Share This Page
URL: techniques.pinnacleblooms.org/self-care/bedtime-routine-E-541
⬇️ Downloadable Family Guide
E-541 Family Guide — 1-Page PDF containing the 9 materials, the routine sequence, the safety rules, and what to say. Designed for: Father, grandparents, school staff, babysitters, elder siblings.
Explain to Grandparents — Send This
When [child's name] comes to stay, please follow this bedtime routine:
- Set the visual timer 20 min before bed
- Follow the picture chart on the wall — in order
- Use the weighted blanket
- Turn on the nightlight and white noise
- Give [child's name] their 3 bedtime passes
- Say goodnight and leave the room
The chart tells them what to do — you don't have to. Consistency between homes is the most important thing.
Teacher/School Communication Template: "[Child's name] is working on a structured bedtime routine at home as part of their therapy program. Consistent sleep directly impacts [child's name]'s regulation during the school day. If [child's name] appears overtired, please note the time and flag to parents — we are tracking sleep onset data."

ACT VI — THE CLOSE & LOOP | ❓ FAQ
Everything parents ask — answered directly by the Pinnacle Blooms Consortium.
Q1: My child has had sleep problems for 3 years. Is it too late to start?
No. Neuroplasticity in childhood extends through adolescence. Three years of struggle simply means the current system isn't working — not that a better system can't work. Many families see first consolidation signs within 3–4 weeks of consistent implementation regardless of history.
Q2: Do I need to use all 9 materials, or can I start with fewer?
Start with 3: visual chart, visual timer, and whichever one addresses your primary challenge (weighted blanket if sensory, worry box if anxiety, passes if callbacks). Add materials one at a time every 10–14 days.
Q3: My child is 10 and thinks they're too old for a visual chart. What do I do?
Rebrand it. "Bedtime checklist" instead of "chart." Digital version on their phone. Let them design it. The principle remains the same — externalizing the sequence reduces executive function load regardless of age.
Q4: What if my child destroys the visual chart in frustration?
This is data. Build the next chart WITH them on a calm weekend afternoon. The investment in co-creation dramatically increases compliance. Child-authored charts have stronger behavioral history.
Q5: We travel a lot. How do we maintain this routine away from home?
Portable version: laminated mini-chart in backpack, travel-size white noise app on phone, same pajamas (sensory anchor), same passes. The most important element is the routine sequence consistency — the environment matters less than the sequence.
Q6: My child doesn't have a formal diagnosis. Can we still use this?
Absolutely. All 9 materials are beneficial for any child with sleep onset difficulty, regardless of diagnosis. Developmental differences exist on a spectrum — these tools support the nervous system, not the diagnosis.
Q7: What if my partner doesn't believe in the protocol and undermines it?
This is the most common implementation challenge. Share Card 37's partner guide. The most effective parent education tool is the parent who used to be skeptical explaining it to their spouse. Book a family teleconsultation if needed: 9100 181 181.
Q8: How long do we need to maintain all 9 materials? Can we phase them out?
Materials can be faded once the behavior they're supporting is habituated. Visual chart → fade when child sequences independently. Passes → reduce to 1 once callback behavior is extinguished. Weighted blanket → maintain as long as child benefits. White noise → can be faded last, as it has the least dependency risk.
Didn't find your answer? Ask GPT-OS® → | Still need help? Call 9100 181 181

Tonight, bedtime can be different.
The protocol is here. The materials are listed. The evidence is clear. The only step left is the first one.
🏅 Pinnacle Blooms Consortium®
Validated by: OT • SLP • ABA • SpEd • NeuroDev
20M+ sessions | 97%+ improvement
DPIIT DIPP8651 | India's Largest Pediatric Therapy Network
20M+ sessions | 97%+ improvement
DPIIT DIPP8651 | India's Largest Pediatric Therapy Network
📞 FREE National Autism Helpline
9100 181 181
24×7 | 16+ languages | No cost ever
"Built by Mothers. Engineered as a System. Serving 70+ Countries." — Pinnacle Blooms Network®
Preview of 9 materials that help with bedtime routine Therapy Material
Below is a visual preview of 9 materials that help with bedtime routine therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
🏅 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
OT | SLP | ABA/BCBA | SpEd | NeuroDev Pediatrics | CRO | WHO/UNICEF Aligned
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium®
Pinnacle exists to transform every home into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary, integrated therapy center — for every child, every family, every income level, in every language, across every region.
↑ Return to Top
Back to Card 01 — The Recognition Moment
→ Next Technique
E-542 Mealtime Routine Independence — you already own the materials
🏠 Browse All Techniques
techniques.pinnacleblooms.org — 70,000+ evidence-linked techniques
CIN | U74999TG2016PTC113063 | |
DPIIT | DIPP8651 (Govt. of India Recognized Startup) | |
MSME | Udyog Aadhaar: TS20F0009606 | |
GSTIN | 36AAGCB9722P1Z2 |
This content is educational. It does not replace individualized assessment and intervention planning with licensed occupational therapists, psychologists, pediatric sleep specialists, and healthcare professionals. Persistent sleep difficulties may indicate underlying medical or psychological conditions requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. pinnacleblooms.org | care@pinnacleblooms.org
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages | FREE | No appointment needed
A parent arrived on Card 01 exhausted, doubting themselves, dreading tomorrow evening. They leave Card 40 with 9 evidence-based tools, a 6-step protocol, a clinical evidence base, and a community. The loop restarts with E-542 — Mealtime Routine Independence.
A parent arrived on Card 01 exhausted, doubting themselves, dreading tomorrow evening. They leave Card 40 with 9 evidence-based tools, a 6-step protocol, a clinical evidence base, and a community. The loop restarts with E-542 — Mealtime Routine Independence.