
9 Materials That Help With Toothbrushing
Evidence-based tools to transform twice-daily trauma into twice-daily routine — for children with oral sensory sensitivity, ages 2–12.
Series E-532
Toileting & Self-Care Independence
Age 2–12 Years

When Brushing Feels Like a Battlefield
It is 7:45 AM. School starts in 20 minutes. You pick up the toothbrush and your child's entire body goes rigid. Before the bristles touch their teeth, they're gagging, crying, clamping their mouth shut with everything they have. You stand there — again — wondering how a two-minute task can feel like a war zone, every single morning, and every single night.
You are not failing. Your child's nervous system is speaking.
The mouth is one of the most densely innervated regions of the human body. For children with oral sensory processing differences, what feels neutral to you may feel genuinely painful, nauseating, or intolerable to them. This is neurology — not defiance.
🏅 Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev Pediatrics

You Are Among Millions of Families Navigating This Exact Challenge
Toothbrushing resistance due to oral sensory over-responsivity is not rare, not unusual, and not your child being difficult. It is a documented neurological phenomenon with documented solutions.
80%
Oral Sensory Difficulty
of children diagnosed with autism display sensory processing difficulties — including oral sensory over-responsivity. Source: PRISMA Systematic Review, 2024 — PMC11506176
1 in 36
ASD Prevalence
children in the US are diagnosed with ASD (CDC, 2023). In India, prevalence studies suggest 1–2% of the pediatric population — approximately 5–10 million families navigating similar challenges.
97%+
Measured Improvement
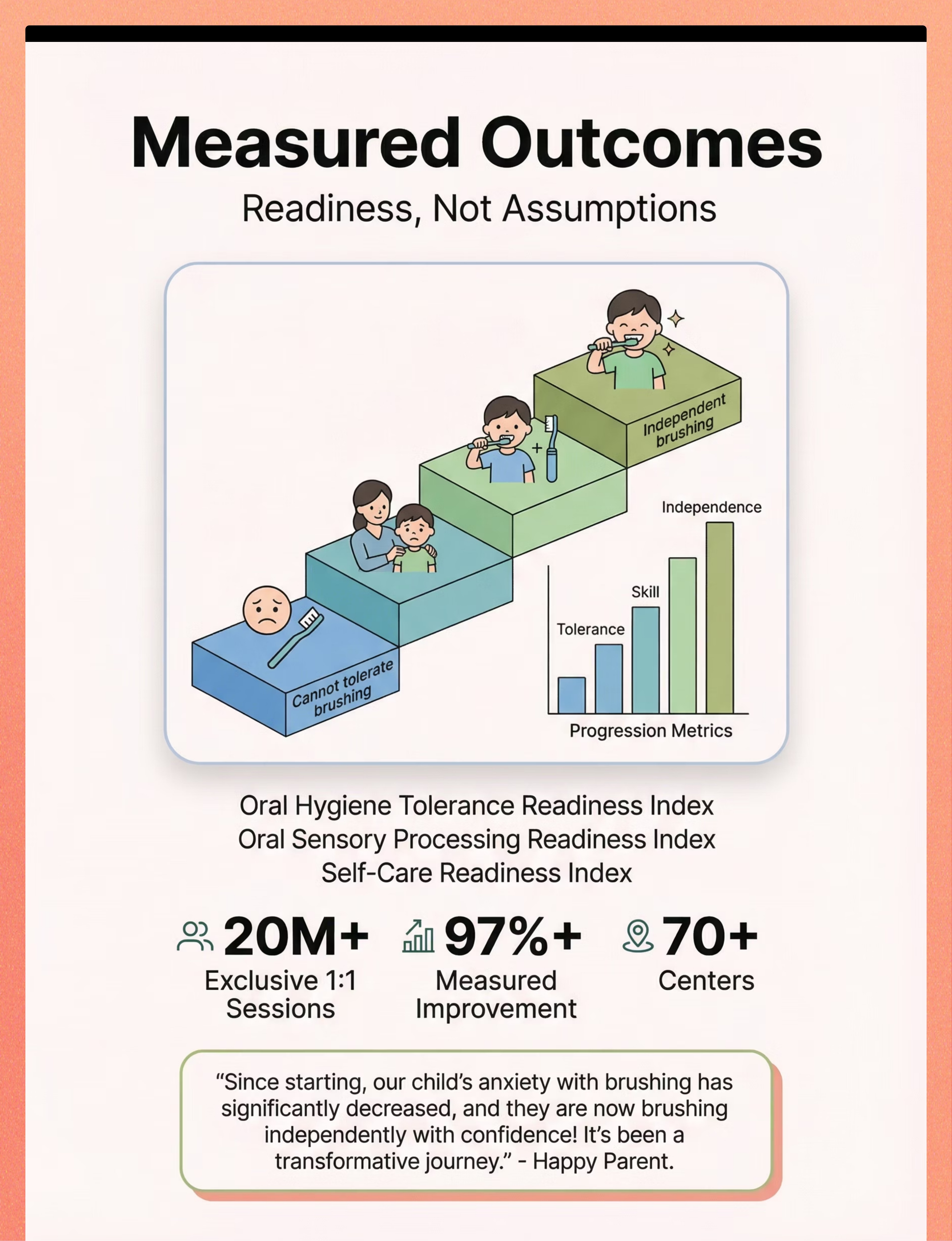
of children in Pinnacle Blooms Network® show measured improvement across readiness indexes — including Oral Hygiene Tolerance Readiness Index. Source: GPT-OS® Real-World Evidence Database | 20M+ sessions
"The gagging, the crying, the fighting — this is the most common oral hygiene challenge reported by families at our 70+ centers across India." — Pinnacle Blooms Consortium Clinical Note

The Neurological Truth About Oral Sensory Defensiveness
The somatosensory cortex processes tactile input from every part of the body. The mouth has an extraordinarily dense concentration of nerve endings — more per square centimeter than almost any other body region. In children with oral sensory over-responsivity, the nervous system amplifies this input, interpreting neutral or mild sensations as threatening or painful.
This is a wiring difference. Not a behavior choice.
The gag reflex — designed to protect against choking — can become hypersensitive, triggering inappropriately from toothbrushing that would not trigger it in a neurotypical child. This processing pattern is particularly common in children with Autism Spectrum Disorder, Sensory Processing Disorder, feeding difficulties, and anxiety disorders.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration treatment in ASD, establishing the neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660

Your Child's Developmental Waypoint — Not a Dead End
WHO/UNICEF developmental context establishes oral hygiene as a progressive skill domain. Many sensory-sensitive children need structured scaffolding through the critical zone between ages 2 and 12.
Commonly co-occurring challenges in children struggling with toothbrushing include feeding texture aversions, hair brushing or nail trimming resistance, dental visit difficulty, speech and articulation differences, and general sensory over-responsivity. Your child is at a waypoint — not a destination. The right materials and gradual desensitization create forward movement.

Clinically Validated. Home-Applicable. Parent-Proven.
🏆 Evidence Grade: Level I–II
Systematic Review + Multiple RCTs + Clinical Consensus
Every material and technique in this guide rests on a multi-study evidence foundation — not clinical opinion alone. The research spans systematic reviews, randomized controlled trials, international health frameworks, and real-world outcome data from 20 million+ Pinnacle therapy interactions.
Study | Finding | Reference | |
PRISMA Systematic Review (2024) — 16 studies | Sensory integration intervention meets evidence-based practice criteria for ASD | PMC11506176 | |
Meta-analysis, World J Clin Cases (2024) — 24 studies | Sensory integration therapy effectively promotes adaptive behavior, sensory processing, motor skills | PMC10955541 | |
WHO Care for Child Development Package (2023) | Home-implemented caregiver strategies improve developmental outcomes across 54 LMICs | PMC9978394 | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory interventions showed significant outcomes in Indian pediatric population | DOI: 10.1007/s12098-018-2747-4 | |
NCAEP Evidence-Based Practices Report (2020) | Visual supports, video modeling classified as evidence-based practices for autism | NCAEP 2020 |
The clinical principle underlying all 9 materials: Reducing oral sensory input intensity + building predictability + providing preparatory proprioceptive input = measurable reduction in oral defensiveness and toothbrushing resistance.
📞FREE Autism Helpline: 9100 181 181 | pinnacleblooms.org

9 Materials That Help With Toothbrushing — Your Complete Toolkit
Multi-Modal Oral Sensory Desensitization Material Protocol
A precisely curated set of 9 therapy-grade materials that address the multiple sensory barriers preventing children with oral sensory over-responsivity from tolerating toothbrushing. Each material targets a specific sensory pathway — tactile, gustatory, proprioceptive, predictability, or motor control — to make toothbrushing a calm, achievable routine rather than a twice-daily crisis.
Oral Motor Tools
Extra-soft brush, silicone bristle brush, three-sided brush, finger brush, oral vibration tool — addressing tactile and motor barriers directly.
Sensory Regulation Materials
Chewy tubes, oral motor chews, Z-Vibe — preparing the nervous system before brushing begins through proprioceptive and vibratory input.
Visual Supports
Visual timers, child-safe mirrors, social stories — building predictability and control so the child's nervous system feels safe to engage.
Reinforcement Menus
Token economies, praise systems, tangible rewards — the behavioral architecture that makes consistency motivating and sustainable for child and family.
Who It's For
Children aged 2–12 with oral sensory defensiveness, oral tactile over-responsivity, ASD-related oral sensitivity, feeding-related texture aversion, or any child for whom toothbrushing is currently distressing.
Session Parameters
Duration: 5–10 minutes total | Frequency: Twice daily | Setting: Home bathroom (primary), School, Clinic | Age Range: 2–12 years

The Consortium Disciplines Behind These 9 Materials
This technique crosses professional boundaries because the oral sensory system doesn't organize itself by therapy type. Four disciplines converge on a single coordinated protocol.
🧑⚕️ Occupational Therapist — Primary Lead
The OT designs the oral desensitization protocol: which tools, in what sequence, with what preparatory inputs. OTs assess the child's full sensory profile using tools like the Sensory Profile, select the correct brush texture, design the chewy tube warm-up sequence, and train the parent in technique.
🗣️ Speech-Language Pathologist — Co-Lead
The SLP brings oral motor expertise — understanding the relationship between oral sensory processing, oral motor control, and the gag reflex. The SLP assesses oral motor function, contributes to the desensitization protocol from a feeding and communication lens, and may lead the Z-Vibe/vibration component.
📊 Behavior Analyst / BCBA — Behavioral Architecture
The ABA specialist structures the reinforcement system around toothbrushing tolerance. Visual timers, token economy, reinforcement menus, and the behavioral shaping sequence — from tolerating brush proximity to accepting brief contact to full brushing — are ABA contributions.
🩺 NeuroDevelopmental Pediatrician — Medical Oversight
Rules out contributing medical factors (dental pain, oral infections, medication side effects). Coordinates with the dental team, guides parents on fluoride decisions when toothpaste is temporarily not possible, and monitors overall oral health trajectory.
"This brain doesn't organize by therapy type. The Pinnacle FusionModule™ ensures all four disciplines contribute to one converged protocol — so your child receives coordinated, not fragmented, care." — Pinnacle Blooms Consortium

What These 9 Materials Are Working to Achieve
The primary target is clear: the child tolerates toothbrushing for a dentally adequate duration (2 minutes) without severe distress, gagging, or physical resistance. Secondary targets include oral sensory desensitization, self-care independence, and reduced anticipatory anxiety. Tertiary gains — including feeding expansion, dental health, and family wellbeing — frequently emerge as the oral sensory system adapts. Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promoted adaptive behavior, sensory processing, and motor skills across 24 studies. PMC10955541

Material 1 — Extra-Soft or Silicone Bristle Toothbrush
🪥 Canon Category: Oral Motor Tools
🏅 Pinnacle Recommends
The first line of change. Standard bristles feel scratchy or painful on sensitive gums. Extra-soft bristles reduce tactile intensity dramatically. Silicone bristle brushes — soft rubber nubs instead of bristles — feel entirely different from any conventional toothbrush. For many children, this single substitution makes the difference between a session that is possible and one that is not.
Why It Works
Bristle texture is the most common tactile trigger for oral defensiveness. Silicone nubs provide contact pressure without the sharp, individual bristle sensation that amplifies the oral threat response.
How to Get It
Price Range: ₹100–400
Search on Amazon.in: "silicone bristle toothbrush child" or "extra soft toothbrush sensitive child India"
DIY Alternative: Soak existing toothbrush in warm water to soften bristles. Ask dentist for sample soft brushes.
Search on Amazon.in: "silicone bristle toothbrush child" or "extra soft toothbrush sensitive child India"
DIY Alternative: Soak existing toothbrush in warm water to soften bristles. Ask dentist for sample soft brushes.

Material 2 — Unflavored or Training Toothpaste
🧴 Canon Category: Oral Motor Tools
🏅 Pinnacle Recommends
Mint "burns." Fruit flavors are "too strong." Even mild children's toothpastes have flavors and sweeteners that can overwhelm a sensitive palate. Unflavored toothpaste removes the taste barrier entirely. Training toothpaste — safe to swallow — is ideal for children who cannot yet spit. This is not pampering; it is addressing a genuine gustatory sensory barrier with a precise, clinical solution.
Why It Works
Gustatory over-responsivity means flavor intensity is genuinely aversive — not a preference. Eliminating the taste trigger allows the child's nervous system to focus on tolerating bristle contact rather than managing two simultaneous sensory assaults.
How to Get It
Price Range: ₹150–500
Search on Amazon.in: "unflavored toothpaste India" or "training toothpaste fluoride free child"
DIY Alternative: Tiny amount of baking soda + water, or brush with plain water temporarily — check with your dentist.
Search on Amazon.in: "unflavored toothpaste India" or "training toothpaste fluoride free child"
DIY Alternative: Tiny amount of baking soda + water, or brush with plain water temporarily — check with your dentist.

Material 3 — Oral Vibration Tool (Z-Vibe or Similar)
📳 Canon Category: Oral Motor Tools / Sensory Regulation
🏅 Pinnacle Recommends | OT/SLP Supervised Use
The desensitization pre-tool. Vibration input to lips, cheeks, and gums before brushing organizes the nervous system and reduces oral defensiveness. The Z-Vibe is the OT/SLP gold standard for oral sensory preparation. Used for 1–2 minutes before brushing sessions as a preparatory activity, it literally changes the nervous system's readiness state before any brush contact occurs. This is clinical preparation — not preamble.
Why It Works
Vibration input provides deep pressure proprioception to the oral structures, calming the oral sensory system's threat response before the toothbrush is introduced. It is the clinical equivalent of warming up muscles before exercise.
How to Get It
Price Range: ₹800–2,000
Search on Amazon.in: "Z-Vibe oral motor tool India" or "oral vibration therapy tool child autism"
DIY Alternative: Electric toothbrush held to cheek — not inside mouth yet — provides similar preparatory vibration input.
Search on Amazon.in: "Z-Vibe oral motor tool India" or "oral vibration therapy tool child autism"
DIY Alternative: Electric toothbrush held to cheek — not inside mouth yet — provides similar preparatory vibration input.
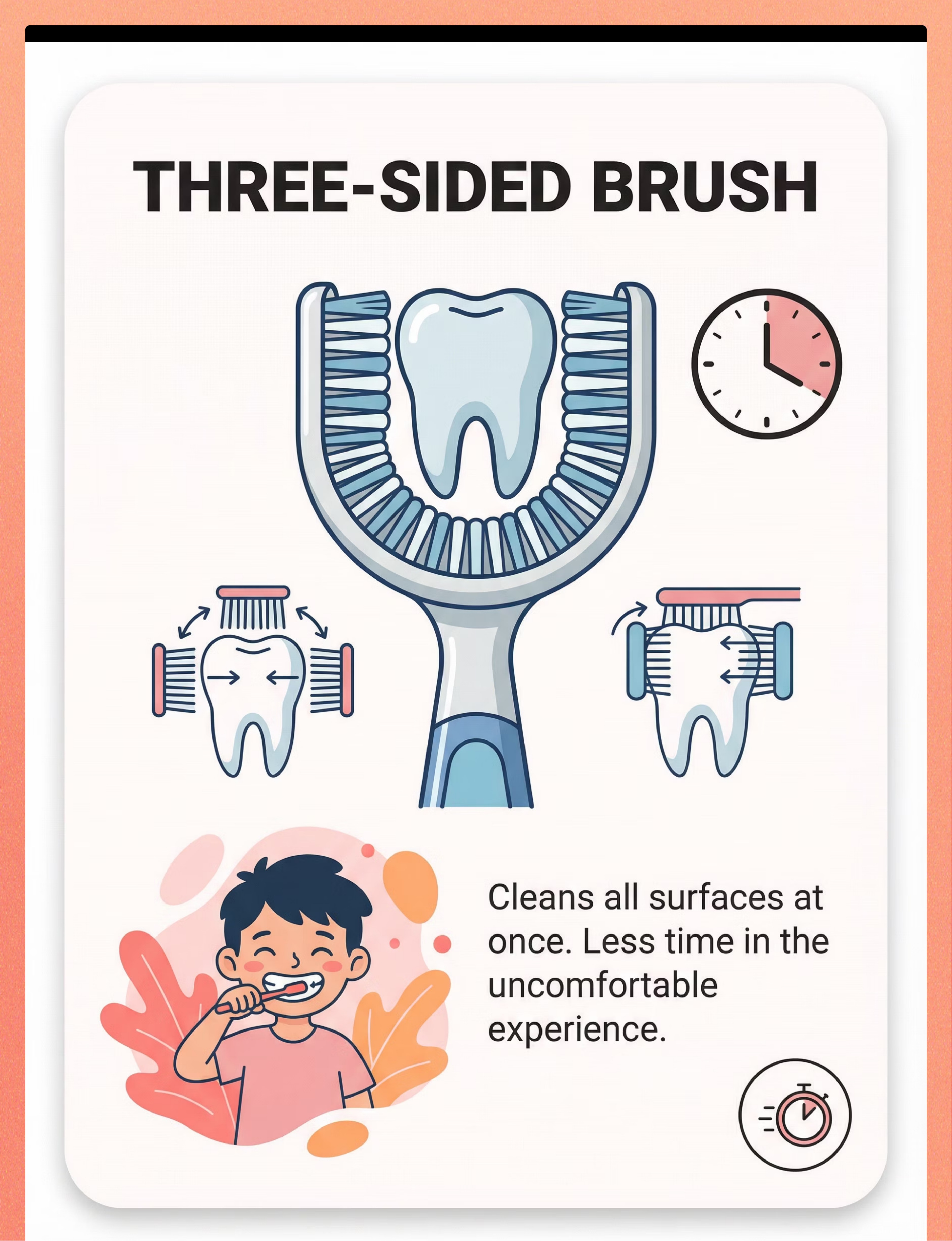
Material 4 — Three-Sided Toothbrush
🦷 Canon Category: Oral Motor Tools
Cleans all tooth surfaces simultaneously — front, back, and chewing surface in a single motion. Faster brushing means less time in an uncomfortable sensation. The simplified forward-back motion along the tooth row also reduces motor demands on the child, making self-brushing attempts more achievable. Worth trialing for any child who can only tolerate brief brushing windows.
Why It Works
Duration is the primary sensory challenge — every second in an uncomfortable sensation feels longer to a dysregulated nervous system. Simultaneous three-surface coverage cuts effective brushing time significantly without compromising dental hygiene outcomes.
How to Get It
Price Range: ₹300–800
Search on Amazon.in: "3 sided toothbrush child U shaped" or "surround toothbrush autism India"
DIY Alternative: Standard soft brush, brushing faster with simpler strokes — the duration-reduction strategy still applies.
Search on Amazon.in: "3 sided toothbrush child U shaped" or "surround toothbrush autism India"
DIY Alternative: Standard soft brush, brushing faster with simpler strokes — the duration-reduction strategy still applies.

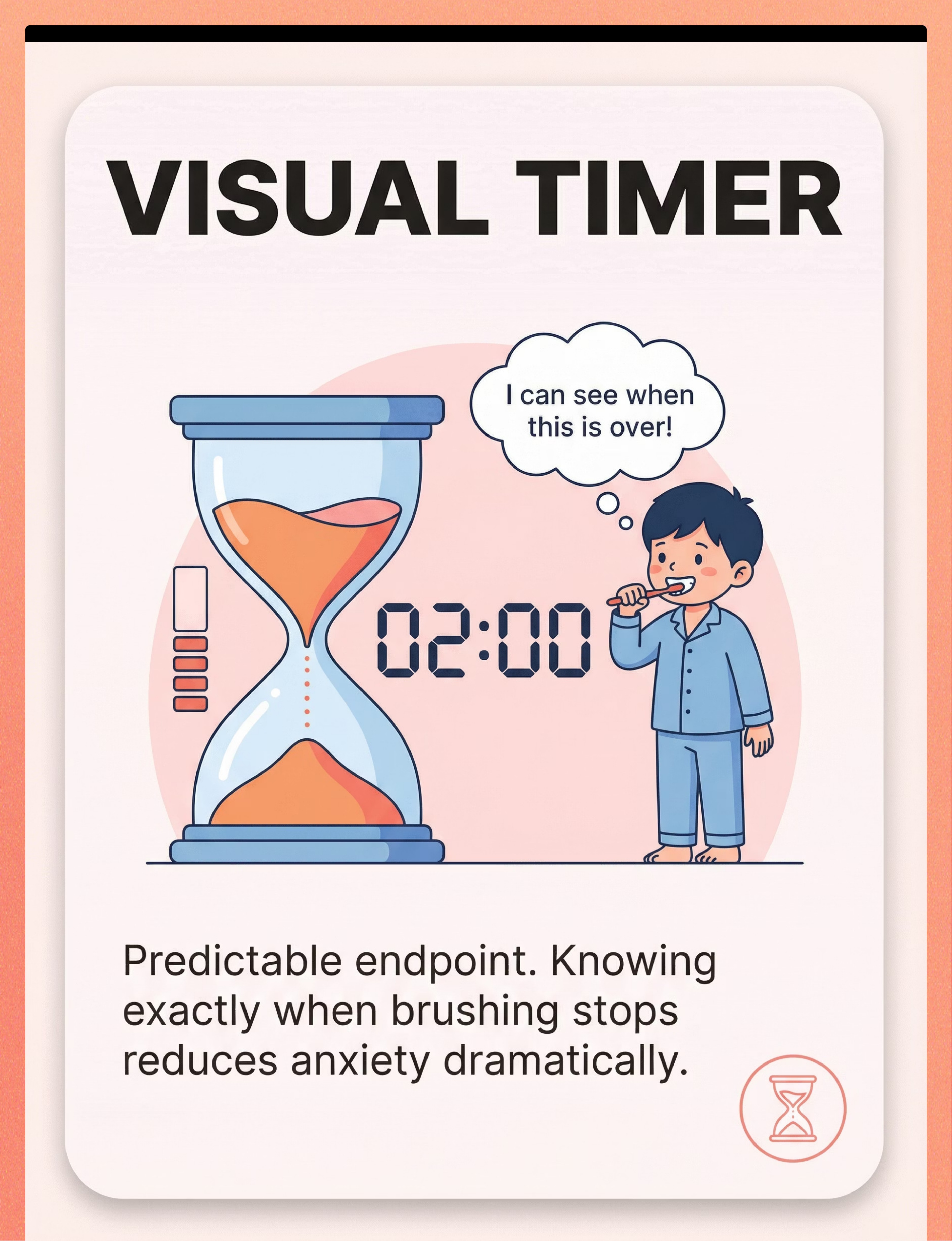
Material 5 — Visual Timer (Sand Timer or App)
⏱️ Canon Category: Visual Supports | Predictability Tools
🏅 Pinnacle Recommends
Unpredictability amplifies sensory distress. A visual timer gives the child visible, concrete evidence that brushing has a defined end. "When the sand runs out, we're done." That single visible endpoint transforms the experience from "endless torture" to "I can do this for 30 seconds." Start short. Honor the timer absolutely. Build duration gradually. The timer's power comes entirely from its trustworthiness.
Why It Works
Predictability is a clinical tool, not a comfort measure. A child who can see the end of a difficult experience has fundamentally different neurological engagement than one who cannot. Visual timers reduce the cognitive load of tolerating discomfort by providing temporal certainty.
How to Get It
Price Range: ₹0–500
Search on Amazon.in: "sand timer 2 minute visual timer child"
Free Apps: Brush DJ or Star Chart
DIY: Phone timer facing the child. Any visible countdown works — the visual is the clinical requirement.
Search on Amazon.in: "sand timer 2 minute visual timer child"
Free Apps: Brush DJ or Star Chart
DIY: Phone timer facing the child. Any visible countdown works — the visual is the clinical requirement.

Material 6 — Finger Toothbrush or Oral Wipes
👆 Canon Category: Oral Motor Tools / Gentler Alternatives
When no toothbrush is tolerable — these maintain oral hygiene. The finger brush fits over the parent's finger: the child feels a familiar touch rather than a foreign object. Oral wipes — dental-grade textured wipes — clean surfaces with minimal intrusion. These are clinically valid stepping stones toward brush tolerance. Something is always better than nothing, and these materials preserve the habit of oral hygiene even when full brushing is temporarily not achievable.
Why It Works
The parent's finger is a familiar sensory experience. Replacing an alien foreign object (toothbrush) with a known tactile input (parent's finger) dramatically reduces the oral threat response — even when the cleaning outcome is similar.
How to Get It
Price Range: ₹100–400
Search on Amazon.in: "silicone finger toothbrush baby" or "dental wipes oral wipes child India"
DIY Alternative: Wet soft washcloth wrapped around index finger, wiping tooth surfaces gently — same finger pressure, similar sensation, immediately available.
Search on Amazon.in: "silicone finger toothbrush baby" or "dental wipes oral wipes child India"
DIY Alternative: Wet soft washcloth wrapped around index finger, wiping tooth surfaces gently — same finger pressure, similar sensation, immediately available.

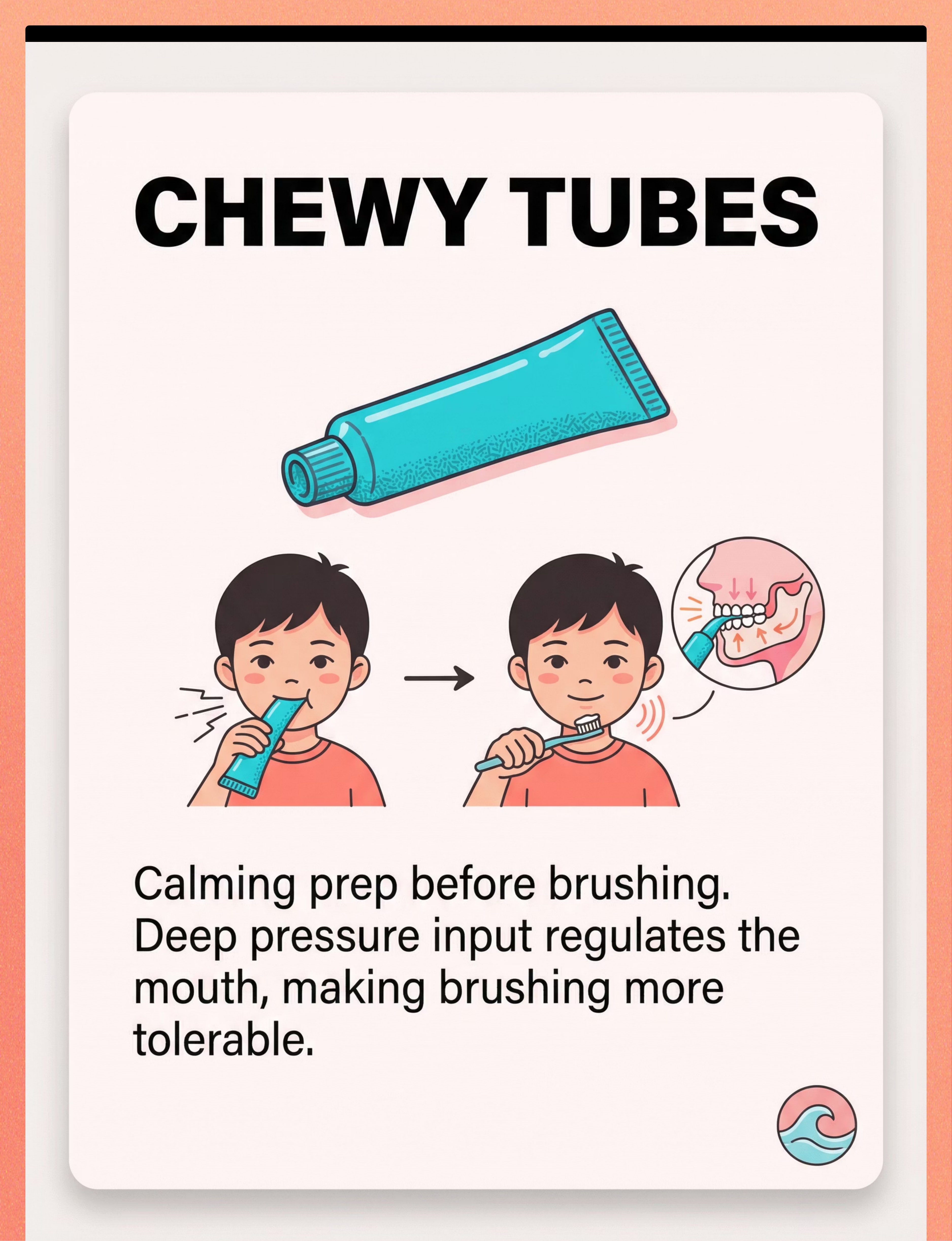
Material 7 — Chewy Tubes / Oral Motor Chews
🦷 Canon Category: Oral Motor Tools / Sensory Regulation
🏅 Pinnacle Recommends
Chewing before brushing provides deep pressure proprioceptive input to the jaw — calming and organizing the oral sensory system before the toothbrush arrives. Children who find chewing pleasurable (sensory seekers) benefit most. One to two minutes of pre-brush chewing genuinely changes the nervous system's readiness state — not as a distraction, but as direct neurological preparation. This is clinical medicine delivered through a preferred sensory activity.
Why It Works
The jaw muscles have a high concentration of proprioceptors. Rhythmic, sustained chewing activates these receptors and sends calming, organizing signals through the somatosensory pathway — the same pathway that processes toothbrush contact. Pre-loading this pathway with positive input reduces the threat signal from brushing.
How to Get It
Price Range: ₹200–600
Search on Amazon.in: "chewy tube oral motor child autism" or "sensory chew necklace pediatric India"
DIY Alternative: Chewing firm food (carrot stick, apple) before brushing activates the same jaw proprioceptive pathway.
Search on Amazon.in: "chewy tube oral motor child autism" or "sensory chew necklace pediatric India"
DIY Alternative: Chewing firm food (carrot stick, apple) before brushing activates the same jaw proprioceptive pathway.
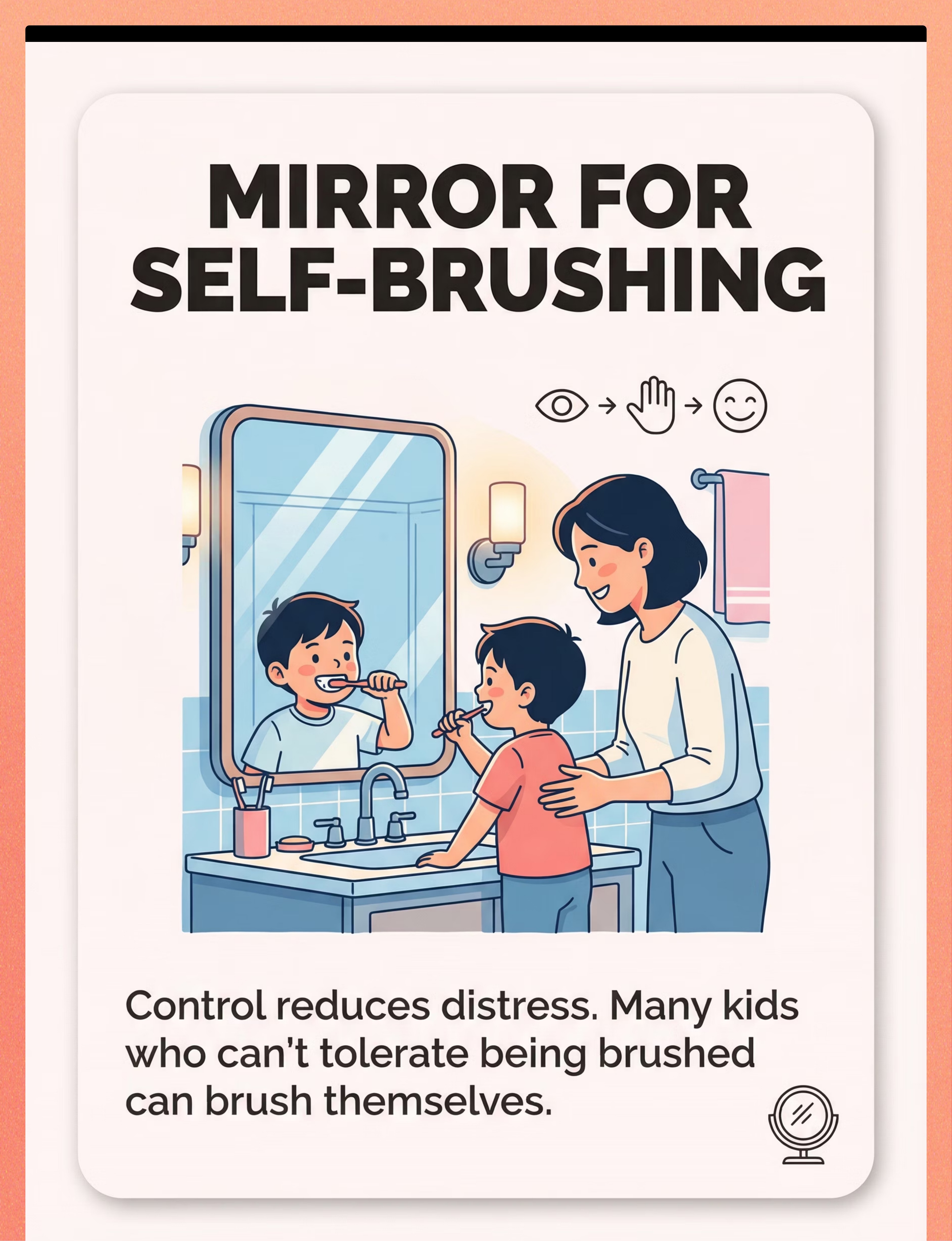
Material 8 — Child-Safe Mirror for Self-Brushing
🪞 Canon Category: Visual Supports / Independence Tools
Control reduces distress. A mirror lets the child see what is happening in their mouth — transforming "something done to me" into "something I can watch and participate in." Many children who cannot tolerate a parent brushing their teeth can tolerate brushing their own teeth with a mirror. Builds agency, independence, and eventually full self-brushing capability. This material addresses the autonomy barrier — one of the most clinically underestimated drivers of toothbrushing resistance.
Why It Works
Visual input of their own mouth gives the child real-time control and prediction. When a child can see what is happening and what is coming next, the threat response is modulated — the limbic system receives "I can see it, I can manage it" rather than "unknown sensation incoming."
How to Get It
Price Range: ₹200–800
Search on Amazon.in: "child safe shatterproof mirror bathroom"
Already have it? Use your existing bathroom mirror today — position at child's eye level using a step stool if needed. Handheld mirrors also work.
Search on Amazon.in: "child safe shatterproof mirror bathroom"
Already have it? Use your existing bathroom mirror today — position at child's eye level using a step stool if needed. Handheld mirrors also work.

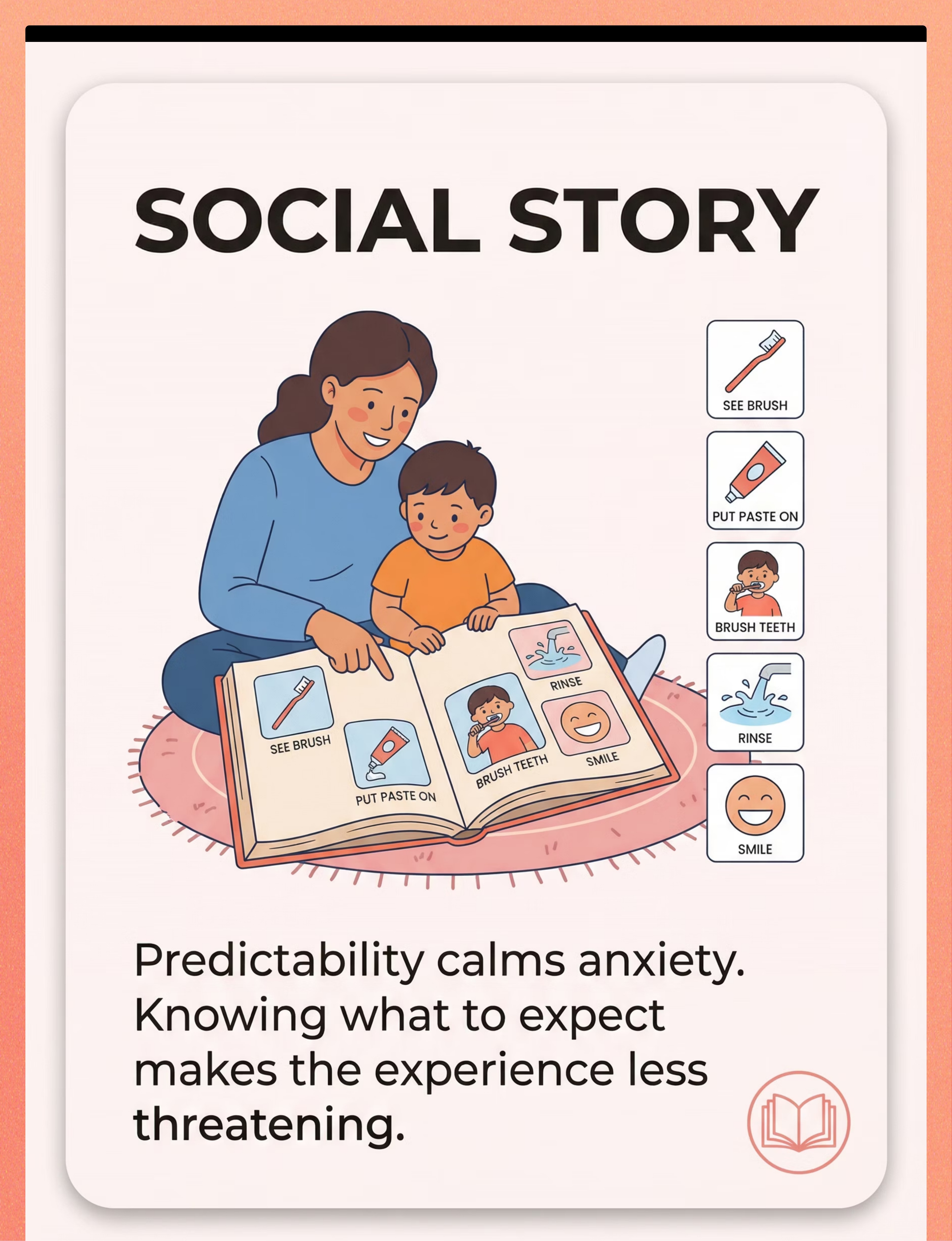
Material 9 — Social Story for Toothbrushing
📖 Canon Category: Visual Supports / Behavioral Supports
🏅 Pinnacle Recommends
Predictability is a clinical tool. A social story — illustrated, step-by-step, showing exactly what will happen, in what order, with coping language — is classified as an evidence-based practice for autism (NCAEP 2020). Read before brushing. Reduces anticipatory anxiety. "First we get the brush. Then a little paste. Then we brush. Then we rinse. Then we're done. My teeth stay healthy." The story's power is in its specificity and in the parent's commitment to match it exactly, every session.
Why It Works
Anticipatory anxiety — the distress that begins before brushing even starts — is often the largest barrier. The social story neutralizes this by making every step of the routine cognitively visible and emotionally manageable before any sensory challenge begins.
How to Get It
Price Range: ₹100–500 or free
Search on Amazon.in: "social story toothbrushing autism visual"
DIY (often MORE effective): Photograph your child's actual bathroom, brush, and toothpaste. Print 5 pictures. Sequence them. Tape to the bathroom wall. Real photos of real context outperform generic printed versions.
Search on Amazon.in: "social story toothbrushing autism visual"
DIY (often MORE effective): Photograph your child's actual bathroom, brush, and toothpaste. Print 5 pictures. Sequence them. Tape to the bathroom wall. Real photos of real context outperform generic printed versions.
📞Need guidance selecting materials? FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7

Every Material Has a Zero-Cost Alternative
WHO/UNICEF Equity Principle
Every family, regardless of income, can begin today
Access to therapeutic materials should never be a barrier to beginning. Every one of the 9 materials has a functional substitute — some of which are actually more effective than commercial versions because they use familiar, available items from your child's own environment.
Material | Buy This | DIY / Free Alternative | Why It Works | |
Extra-Soft Brush | ₹100–400 silicone bristle brush | Soak existing brush in warm water. Ask dentist for sample soft brushes. | Softened bristles reduce tactile intensity — same mechanism | |
Unflavored Toothpaste | ₹150–500 online | Tiny amount of baking soda + water; or plain water temporarily | Mechanical cleaning still occurs. Taste barrier removed. | |
Oral Vibration Tool | ₹800–2,000 Z-Vibe | Electric toothbrush held to cheek (not inside mouth) before brushing | Vibration provides similar preparatory desensitization | |
Three-Sided Brush | ₹300–800 online | Standard soft brush, faster with simpler strokes | Duration-reduction strategy via technique | |
Visual Timer | ₹200–500 sand timer | Free phone timer facing child. Free apps: Brush DJ, Clock apps | Any visible countdown meets the clinical requirement | |
Finger Brush | ₹100–300 silicone | Wet soft washcloth wrapped around index finger | Same finger pressure; readily available | |
Chewy Tubes | ₹200–600 therapeutic | Firm food (carrot, apple) before brushing; gum if age-appropriate | Jaw proprioceptive input — food chewing activates same pathway | |
Child Mirror | ₹200–800 | Existing bathroom mirror; step stool if needed | Vision of own mouth provides control and engagement | |
Social Story | ₹100–500 | Photograph child's actual bathroom, brush, toothpaste. Print. Sequence. Tape to wall. | Real photos of real context are MORE effective than generic versions |
When is commercial-grade non-negotiable? The oral vibration tool (Z-Vibe) is the one material where clinical-grade equipment has clear advantages — frequency, intensity, and tip variety are calibrated. For severe oral defensiveness, consult your OT before substituting.
The Pre-Session Safety Gate
🔴 Safety First
Read Before Every Session Until It Becomes Second Nature
🔴 DO NOT PROCEED if:
- Child has a dental infection, oral sores, or visible mouth pain — see dentist first
- Child is acutely ill (fever, vomiting, significant distress unrelated to brushing)
- Child has had a severe emotional meltdown within the last 30 minutes — wait for full regulation
- You are feeling frustrated, exhausted, or emotionally activated — your state transfers to your child
- Child has had a recent traumatic oral procedure — consult OT before resuming
🟡 MODIFY if:
- Child is tired but not dysregulated — use shorter duration, praise-heavy approach
- Child seems anxious but not distressed — extra social story reading, slower pace
- You skipped yesterday — child may need re-priming; start with chewy tube or vibration tool
- New environment (travelling, school) — familiar materials matter more in unfamiliar spaces
🟢 PROCEED if:
- Child is fed, rested, and in a calm-alert state
- Parent is calm and has 5–10 minutes without interruption
- All materials are assembled at the sink before you invite the child
- Visual timer is visible and set
STOP IMMEDIATELY if: Child shows signs of genuine distress escalating (not just protest — actual panic) | Gagging progresses to vomiting | Child bites down on finger brush hard enough to cause pain — remove calmly, try again tomorrow | You feel you are forcing — stop. Forced sessions create trauma and worsen long-term tolerance.
📞Concern? Uncertainty? FREE Helpline: 9100 181 181
📞Concern? Uncertainty? FREE Helpline: 9100 181 181

The Bathroom Setup That Changes Everything
Spatial preparation prevents 80% of session failures
Set up before inviting the child
The environment is a clinical variable — not a backdrop. An organized, predictable bathroom setup reduces sensory load before your child takes a single step toward the sink. Assemble everything before the invitation.
Remove / Minimize
- Sibling interference — close door if possible
- Phone and screen distractions (yours and theirs)
- Other bathroom noise — fans, running water not yet needed
- Clutter on sink counter — minimal sensory input in the space
The 30-Second Pre-Launch Check
✅ Timer set and visible?
✅ Brush with paste already prepared?
✅ Chewy tube / Z-Vibe ready if using?
✅ Mirror at child's eye level?
✅ You are calm and unhurried?
→ Ready. Now invite your child.
✅ Brush with paste already prepared?
✅ Chewy tube / Z-Vibe ready if using?
✅ Mirror at child's eye level?
✅ You are calm and unhurried?
→ Ready. Now invite your child.
The 60-Second Pre-Session Assessment — Is Your Child Ready?
The best session is one that starts right. Observe your child right now before proceeding.
Readiness Indicator | ✅ Go | 🟡 Modify | ❌ Postpone | |
State of arousal | Calm-alert, engaged | Slightly tired but responsive | Dysregulated, crying, melting down | |
Last meal timing | 30+ minutes ago | Recently fed, content | Hungry or nauseous | |
Recent activities | Calm play or routine | Active play, winding down | Just came from high-stimulation activity or struggle | |
Response to approach | Makes eye contact, receptive | Slightly avoidant but redirectable | Turning away, pushing you away, saying no | |
Body cues | Relaxed posture, normal breathing | Some tension but not rigid | Stiff, rigid, shallow breathing |
🟢 3+ Green → GO
Proceed to full protocol — Step 1: The Invitation
🟡 Mixed → MODIFY
Shortened version: chewy tube prep only, timer for 30 seconds, just front teeth, extra praise, end immediately on success
🔴 2+ Red → POSTPONE
Do oral wipes as hygiene maintenance. Note time of day and plan for when child is typically most regulated.
What time of day works best? Most families find the morning session harder (rushed, transition stress) and the bedtime session easier. If mornings are consistently failing — try after morning snack instead of before school. Timing flexibility is yours; the dentally required frequency (twice daily) is not.
Step 1 — The Invitation
Duration: 30–60 seconds
ABA Pairing Principle + OT Just-Right Challenge
The session begins with an invitation — never a command. The child's nervous system must feel safe to approach. Safety before sensation.
✅ What to Say — The Invitation Script
"Hey [child's name] — it's toothbrush time. Want to come see your timer? We're doing [X] seconds today."
For a child who needs more preparation:
"Remember our toothbrushing story? Let's go look at the timer together."
For a child who needs more preparation:
"Remember our toothbrushing story? Let's go look at the timer together."
❌ What NOT to Say
"Come brush your teeth RIGHT NOW." — Directive. No choice. No preparation. Increases resistance before the session begins.
Your Body Language
Get to child's level — crouch down or sit. Offer your hand, don't lead by the shoulder. Relaxed posture — your nervous system regulation is visible to your child. Neutral-warm tone — not anxious, not punitive, not performatively cheerful.
When Child Resists
Child runs away → follow calmly, re-invite once, then move to modified version.
Child says "no" → "I know. We do 30 seconds. You can hold the timer."
Child covers mouth → "That's okay. We'll use the chewy tube first."
Child says "no" → "I know. We do 30 seconds. You can hold the timer."
Child covers mouth → "That's okay. We'll use the chewy tube first."

Step 2 — The Engagement
Duration: 1–3 minutes
Material Introduction + Preparatory Input
Child is at the sink. Now: prepare the oral system before the brush touches teeth. This preparation phase is not optional — it is the clinical ingredient that makes brushing possible.
Chewy Tube (recommended)
"First, let's do some chewing. Pick your chewy." Allow 1–2 minutes of chewing. This proprioceptive input begins calming the oral nervous system before any brush contact.
Oral Vibration Tool (Z-Vibe / Electric Brush)
Begin on hands: "First on your hand — feel that?" Progress to cheek → lips → inside mouth only if child willingly opens. Never force. 30–60 seconds maximum.
Introduce the Visual Timer
"Look — [X] seconds on the timer. When it's done, we're done. I promise." Start the timer only when brushing begins — not during preparation.
Show the Toothbrush
Let child examine the extra-soft/silicone brush. Let them touch the bristles with their finger if willing. "Feel how soft these are? They feel different from the other brush."
Systematic review (Children, 2024): Sensory integration with structured material introduction meets evidence-based practice criteria. PMC11506176

Step 3 — The Therapeutic Action: Brushing Begins
Duration: 30 seconds (build to 2 minutes)
The Active Ingredient
START THE TIMER. NOW the session is running.
Start Front Teeth Only (first 2 weeks)
The further back in the mouth, the higher the gag reflex sensitivity. Begin at the front incisors. Build backward only as tolerance increases: Front → Side → Back molars. This is a clinical progression, not a shortcut.
Apply Minimal Pressure
The therapeutic requirement is the opposite of instinct. Gentle, circular or soft back-and-forth motion. Cleaning happens at any pressure with a quality brush. Intensity is the enemy of tolerance.
Narrate While Brushing
"Brushing the bottom front teeth... see in the mirror?... now the top... good... almost there... timer is at [X]..." Narration keeps the child's cortex engaged, provides temporal information, and maintains calm co-regulation.
Honor the Timer Absolutely
When the timer ends, brushing ends. No "just a few more seconds." Trust is the therapeutic currency. Break it once and the timer loses its power completely.
Child's Response Spectrum: Ideal — tolerates, watches in mirror, shows minimal distress ✅ | Acceptable — makes protest sounds but does not physically fight; timer is visible ✅ | Concerning — gags, vomits, physically tries to escape — STOP, soothe, end with dignity. This is not failure. It is data.
Step 4 — Repeat and Vary
Build Across Days and Weeks
Therapeutic Dosage Protocol
Within a single session, do not repeat brushing multiple times. The therapeutic unit for toothbrushing is the session itself — one entry, one brushing, one exit. Repetition happens across days, not within a session.
Week | Timer Duration | Coverage | Toothpaste | Preparation | |
Week 1–2 | 30 seconds | Front teeth only | None or water | Chewy tube / Z-Vibe every time | |
Week 3–4 | 45–60 seconds | Front + sides | Tiny amount unflavored | Chewy tube or Z-Vibe | |
Week 5–6 | 60–90 seconds | Most teeth | Small amount unflavored | 50% of sessions need prep | |
Week 7–8 | 90–120 seconds | All teeth | Unflavored, appropriate amount | As needed | |
Week 9+ | 2 minutes | Full brushing | Child's choice of mild paste | Child determines if prep needed |
Introduce variation to maintain engagement: Alternate who holds the brush (child vs. parent) | Change order (child chooses) | Change timer style | Let child pick their chewy tube | Allow child to put toothpaste on the brush themselves.
"3 good, calm seconds beats 30 forced seconds, every single time."

Step 5 — Reinforce and Celebrate
Timing: Within 3 Seconds of Timer Ending
ABA Reinforcement Principles
The most important rule: Reinforce the ATTEMPT, not just perfect completion.
"[Child's name]! You did it! You brushed for [X] seconds! That was so calm! High five!"
Social Reinforcement
Hug, high five, verbal praise, dance together. Most powerful for most children. Costs nothing. Available immediately.
Activity Reinforcement
5 minutes of preferred screen time, favourite game. Immediate access is the key — delayed reinforcement loses its clinical power.
Token Economy
Star on chart → reward after 7 stars. Pinnacle Reinforcement Menu Set ₹364 | Premium Set ₹589
Tangible
Small preferred item, sticker, special snack. Use consistently; phase out toward social praise over time as brushing becomes routine.
What NOT to do: Do not withdraw reinforcement if the session was less than perfect — even 10 seconds of tolerated brushing deserves celebration. Do not use toothbrushing as a condition for other necessities. Do not express disappointment if child didn't tolerate what they did yesterday — sensory tolerance fluctuates, and fluctuation is neurological, not behavioral.
📞Questions about reinforcement strategy? FREE Helpline: 9100 181 181

Step 6 — The Cool-Down
Duration: 1–2 minutes
No Session Ends Abruptly
The cool-down is a clinical requirement, not a courtesy. Abrupt session endings cause post-session dysregulation — the child's nervous system needs a deliberate, predictable transition out of the therapeutic activity.
Warning (while timer ends)
"Timer's almost done... one more second... DONE! All finished!"
Immediate Positive Closure
Reinforcement delivered. Then: "Okay — all done with brushing. Let's rinse and you can put the brush away."
Child Participates in Put-Away
Child places brush in holder if able. This ritual signals "session complete" neurologically. Participation builds ownership of the routine.
Rinse Ritual
Water rinse from cup or tap. Secondary oral desensitization effect — water in the mouth after brushing extends intraoral tolerance in a pleasant, child-controlled way.
Transition Cue to Next Activity
"After rinsing, we're going to [breakfast / story / outdoor play]." The child knows what comes next. Predictability extends throughout the routine, not just during brushing. Pinnacle Transition Objects / Comfort Items ₹425 for children who need physical comfort during transition.

Capture the Data — Right Now
60 Seconds of Data
Complete Within 60 Seconds of Session End While It's Fresh
Data tracking is not bureaucracy — it is the mechanism that makes progress visible. Sensory tolerance gains are often sub-threshold and invisible to the parent who lives them daily. Data reveals what the naked eye misses.
Duration Tolerated
Record seconds/minutes on timer. Your single most important metric — watch this number trend upward across weeks.
Distress Level
1–5 scale (1=calm, 5=severe distress). Tracks quality alongside duration — a child can tolerate 2 minutes at distress level 4 or 30 seconds at level 1; both data points matter differently.
Coverage
Front only / Most teeth / All teeth. Tracks brushing completeness and clinical progression through the front-to-back protocol.
What Helped Today
Chewy tube / Z-Vibe / Timer / Mirror / None needed. Identifies which materials are driving success for your specific child's profile.
Quick Daily Tracking Format:
DATE: _______ | TIME: _______ | SESSION: AM / PM
Duration: _____ seconds | Distress (1–5): _____ | Coverage: Front / Most / All
Preparation used: _____________ | Notes: _________________________________
GPT-OS® In-App Tracker: Log this session in your GPT-OS® dashboard for AI-powered pattern analysis → pinnacleblooms.org/gpt-os
DATE: _______ | TIME: _______ | SESSION: AM / PM
Duration: _____ seconds | Distress (1–5): _____ | Coverage: Front / Most / All
Preparation used: _____________ | Notes: _________________________________
GPT-OS® In-App Tracker: Log this session in your GPT-OS® dashboard for AI-powered pattern analysis → pinnacleblooms.org/gpt-os
What If It Didn't Go as Planned?
The Reality Card
"Session abandonment is not failure. It is data."
Most sessions are not perfect. Most weeks contain hard days. Here is specific guidance for the most common challenges — because vague reassurance is not clinical support.
Child gagged or vomited during brushing
Why: Gag reflex hypersensitive today — fatigue, illness onset, brush too far back, or baseline sensitivity. Next time: Stay to front teeth only. More chewy tube / Z-Vibe preparation. Try oral wipes instead for today's hygiene.
Child refused to open mouth at all
Why: Previous sessions may have been traumatic; or today's state makes any oral invasion intolerable. Next time: Social story and timer review without brushing. Offer chewy tube only. No brushing today — rebuild trust before advancing.
Timer ran out but teeth aren't clean enough
Why: You are correctly prioritizing tolerance over hygiene in early stages. Next time: Add a second short timed session at a different point in the day for teeth not covered. Incomplete hygiene temporarily is clinically appropriate in the early protocol.
Yesterday was great, today was terrible
Why: Sensory tolerance is not linear — it fluctuates with sleep quality, immune activation, stress, schedule disruption. What to do: This is expected. Do not reset your progress assessment. "Bad days" are neurological events, not behavioral regression. Use modified approach today. Continue tomorrow.
3 weeks in and nothing has changed
Why: Progress at this level is often sub-threshold — too small to see without data tracking. What to do: Review your data log. If genuinely flat across 3 weeks of consistent, calm sessions — this is the signal for professional OT/SLP assessment. Call 9100 181 181.

Adapt and Personalize — No Two Children Are Identical
Calibrate to Your Child's Current State
The protocol is a framework, not a script. The most effective implementation is one that meets your child where they are today — not where they were last week or where you want them to be next month.
For Sensory Avoiders
Oral defensiveness is the primary profile — these children need maximum preparation and minimum surprise.
- More preparation time (chewy tube + Z-Vibe before every session)
- Start shorter (15–20 seconds) and build more slowly
- Unflavored toothpaste is non-negotiable
- Mirror and narration essential — give maximum control
- Sessions at most regulated time of day only
For Sensory Seekers
Crave oral input, chew everything — but still resist brushing for complex reasons.
- May enjoy chewy tube too much to transition — use a fixed timer for chewing too
- May respond better to electric toothbrush vibration than manual
- Can often move faster on the duration scale — test and build
- May prefer stronger but controlled sensation; firm bristle pressure sometimes preferred
For Younger Children (2–4 years)
- Parent brushes first; child's mirror holding is the "participation"
- Shorter sessions (15–30 seconds maximum)
- Social story in 3 pictures, not 5
- Finger brush often more tolerable than any toothbrush at this age
For Older Children (8–12 years)
- Self-brushing goal is primary — independence, not parent-brushed compliance
- Give full control of timer, toothpaste amount, brushing order
- Age-appropriate reinforcement (screen time, privileges rather than stickers)
- Oral hygiene connected to social self-awareness may become motivating
Weeks 1–2 — The Calibration Phase
Progress: ~15%
Do NOT Expect Mastery. Expect Calibration.
Week 1–2 Progress
You are here — the calibration phase. Consistency of environment is more important than any single outcome at this stage.
What You WILL Likely See
- Child accepting chewy tube or vibration preparation without resistance — this alone is progress
- Session duration increasing from 10 to 20 to 30 seconds across two weeks
- Gagging reducing (not eliminating) — the gag threshold is being raised
- "Fight" replaced by "reluctant compliance" — significant progress even when it doesn't feel like it
- Visual timer becoming familiar — child starting to check the timer during brushing
What You Will NOT See Yet
- Child asking to brush teeth independently
- Calm, willing opening of mouth at first approach
- Full 2-minute brushing
- No distress at all
Parent milestone for Week 1–2: "I established a consistent routine at the same time each day, with the same materials, in the same sequence." The nervous system is learning predictability — and predictability is the foundation everything else is built on.
📞FREE Helpline: 9100 181 181 | "How is Week 1 going? Our OTs can guide you."

Weeks 3–4 — The Neural Pathway Forms
Progress: ~40%
Watch for These Signs — the Nervous System Is Adapting
Week 3–4 Progress
Consolidation indicators are emerging. Go back to your data log — the improvement is often invisible to the parent who lives it daily, but measurable in the numbers.
Consolidation Indicators — What to Look For:
Walks to bathroom with less protest
Anticipatory anxiety is reducing — the nervous system is beginning to predict "manageable" rather than "threatening."
Reaches for chewy tube or vibration tool before you offer it
Child is self-initiating the preparation sequence — profound progress in self-regulation capacity.
Looks in the mirror during brushing
Engagement is replacing avoidance — the child is participating rather than enduring.
Duration consistently 30–45 seconds without escalation
The tolerance window is stable — the foundation for building further duration.
Asks "when will the timer be done?" (not "I don't want to")
Timer is working as a regulator — the child trusts the endpoint exists.
When to increase duration: When the child completes the current timer duration with distress score of 2 or lower for 3 consecutive sessions — increase by 10–15 seconds. Not before. Consistency at each level builds the neural pathway that supports the next level.

Weeks 5–8 — Approaching Mastery
Progress: ~75%
🏆 Oral Hygiene Tolerance — Mastery Unlocking
Week 5–8 Progress
Mastery criteria are within reach. Generalization to other contexts is the gold standard of neurological change.
Mastery Criteria — What "Mastery" Actually Looks Like:
✅ Duration + Distress
Child tolerates 60–120 seconds of brushing with distress score ≤ 2 (mild protest only). Gagging reduced to rare or absent within the brushing tolerance zone.
✅ Approach Behavior
Child approaches bathroom without severe anticipatory distress. At least partial self-brushing: child holds brush and brushes front teeth independently.
✅ Generalization
Progress appears in OTHER contexts: grandparents' house, the dentist, food texture tolerance. Generalization is the gold standard of neurological change — not just behavior compliance at home.
Meta-analysis (World J Clin Cases, 2024): Effective promotion of skills with measurable outcomes across 24 studies. Mastery criteria derived from behavioral measurement standards. PMC10955541 | BACB Mastery Criteria Standards

You Did This. Your Child Grew Because of Your Commitment.
This did not happen easily. You navigated the mornings when you wanted to give up. You stayed calm when your child was screaming. You prepared the space, assembled the materials, honored the timer, and showed up again the next day when the previous session went badly.
This is what therapeutic parenting looks like. It is quiet, consistent commitment — morning and evening, for weeks.
What Your Child Has Learned
- My mouth is something I can manage, not just endure
- The timer is trustworthy — it always ends when it says it will
- My parent is safe — they don't force past the boundary
- I can brush some of my own teeth
What YOU Have Learned
- Your child's sensory system responds to gradual, positive exposure
- Preparation (chewy tube, Z-Vibe) is clinical medicine, not preamble
- Data tracking shows progress that the naked eye misses
- A good enough session (30 calm seconds) beats a thorough traumatic one every time
Family celebration suggestion: Let your child choose tonight's bedtime story. Tell them specifically: "You were so brave with brushing this week. I'm proud of you." Document this milestone — a photo of your child smiling after a calm brushing session. Caption: "Week [X] — we did it."

Clinical Guardrails — When to Pause and Seek Guidance
🚨 Red Flags
Specific Thresholds — Not Vague Concerns
🔴 Red Flag 1: Gagging progresses to vomiting in majority of sessions
What it means: Gag reflex hypersensitivity is severe; protocol modification insufficient. Requires OT oral desensitization assessment.
Action: Oral wipes only for hygiene. Book OT evaluation. Call 9100 181 181.
Action: Oral wipes only for hygiene. Book OT evaluation. Call 9100 181 181.
🔴 Red Flag 2: No improvement in distress score across 4 consecutive weeks
What it means: Underlying oral sensory processing may require clinical-grade desensitization beyond parent implementation.
Action: OT referral for standardized sensory profile assessment. GPT-OS® TherapeuticAI® protocol upgrade.
Action: OT referral for standardized sensory profile assessment. GPT-OS® TherapeuticAI® protocol upgrade.
🔴 Red Flag 3: Oral sensitivity significantly impacts eating — texture aversions worsening
What it means: Oral sensory issues are broader than hygiene; feeding is affected. SLP feeding evaluation needed.
Action: Simultaneous OT + SLP evaluation. Do not allow dental health to deteriorate while investigating.
Action: Simultaneous OT + SLP evaluation. Do not allow dental health to deteriorate while investigating.
🔴 Red Flag 4: Child shows signs of NEW oral pain during brushing
What it means: Dental decay, mouth sore, or oral infection may be present. New acute pain should be evaluated before continuing.
Action: Dental examination before continuing brushing protocol.
Action: Dental examination before continuing brushing protocol.
🔴 Red Flag 5: Overall sensory over-responsivity worsening across multiple domains
What it means: Possible regression requiring developmental pediatrician evaluation. Can indicate immune activation, neurological change, or unaddressed anxiety.
Action: Developmental pediatrician or NeuroDev consultation via Pinnacle.
Action: Developmental pediatrician or NeuroDev consultation via Pinnacle.
Escalation pathway: Self-modify → Teleconsult (9100 181 181) → Center visit → Specialist referral
📞FREE Helpline: 9100 181 181 | Book teleconsultation: pinnacleblooms.org

Your Developmental GPS — Where You Are, Where You're Going
📍 You Are Here: E-532 Toothbrushing Tolerance
Every technique in the Pinnacle Self-Care Series builds on what came before and creates the foundation for what comes next. Understanding the full pathway helps you see today's work in its developmental context.
Path B — Deeper Oral Sensory Work
If progress is slower than expected:
→ E-532-DD-01: Oral Desensitization Protocol with Z-Vibe — Deep Dive
→ E-532-DD-02: Sensory-Friendly Toothbrush Selection Guide
→ E-532-DD-01: Oral Desensitization Protocol with Z-Vibe — Deep Dive
→ E-532-DD-02: Sensory-Friendly Toothbrush Selection Guide
Path C — Feeding Overlap
If oral sensitivity affects eating:
→ Connect with SLP feeding pathway
→ FusionModule™ assessment: OT + SLP combined protocol for oral sensory + feeding
→ Connect with SLP feeding pathway
→ FusionModule™ assessment: OT + SLP combined protocol for oral sensory + feeding
Long-term developmental goal: Self-Care Readiness Index — Full Independence. Child performs complete oral hygiene routine independently, with appropriate technique, without distress. This directly impacts social participation, health outcomes, and transition-to-school readiness.

From Real Families — Real Outcomes
Anonymized narratives from Pinnacle's 70+ centers. Individual outcomes vary.
Family Story 1 — 4-year-old with ASD, Hyderabad
Before: "Our morning routine was destroyed for 20 minutes every single day. He would scream the moment he saw the toothbrush. His dentist found 3 cavities."
Change: Silicone bristle brush + unflavored toothpaste + chewy tube pre-session + 30-second timer.
After (6 weeks): "He chews his tube, picks up the soft brush, watches himself in the mirror, and we're done in a minute. The dentist visit last month was the calmest we've ever had."
Change: Silicone bristle brush + unflavored toothpaste + chewy tube pre-session + 30-second timer.
After (6 weeks): "He chews his tube, picks up the soft brush, watches himself in the mirror, and we're done in a minute. The dentist visit last month was the calmest we've ever had."
Family Story 2 — 7-year-old, Chennai, SPD without ASD
Before: "She'd been saying toothpaste 'burns' for years. Every dentist told us she was fine and we should just be more consistent. She wasn't fine."
Change: Unflavored toothpaste + Z-Vibe pre-session for 6 weeks + social story before every session.
After (8 weeks): "She brushes her own teeth. Uses unflavored toothpaste because she prefers it — not because she can't handle flavor. The Z-Vibe is in the drawer now; she doesn't need it most days."
Change: Unflavored toothpaste + Z-Vibe pre-session for 6 weeks + social story before every session.
After (8 weeks): "She brushes her own teeth. Uses unflavored toothpaste because she prefers it — not because she can't handle flavor. The Z-Vibe is in the drawer now; she doesn't need it most days."
Family Story 3 — 3-year-old, Bengaluru, feeding difficulties + oral defensiveness
Before: "We were doing oral wipes only because no brush was tolerated. Pediatric dentist said we needed to do more. We didn't know how."
Change: Finger brush → silicone brush progression over 3 months, combined with feeding therapy.
After (12 weeks): "We're at a soft toothbrush with 45-second timer. For a child who screamed at the sight of anything approaching her mouth — 45 seconds of calm brushing is our miracle."
Change: Finger brush → silicone brush progression over 3 months, combined with feeding therapy.
After (12 weeks): "We're at a soft toothbrush with 45-second timer. For a child who screamed at the sight of anything approaching her mouth — 45 seconds of calm brushing is our miracle."
Frequently Asked Questions — Toothbrushing Sensitivity
Is this sensory sensitivity real, or is my child just being difficult?
It is real. The mouth has one of the highest concentrations of sensory nerve endings in the human body. Gagging is a real reflexive response — not theater. The clinical term is oral tactile over-responsivity. It has a neurological basis and a documented intervention pathway.
Will my child outgrow this on their own?
Some children do. Many do not — particularly children with ASD or broader sensory processing challenges. Waiting without intervention allows dental problems to develop and allows the negative behavioral pattern to become more entrenched. Begin now, not later.
My dentist says to just make them do it. Is forcing the answer?
No. Forcing a child through oral distress builds trauma association, not tolerance. A child who is forced through severe distress has higher resistance at the next session. The clinical evidence is clear: graduated exposure with sensory modification and positive reinforcement is the effective pathway.
How long until I see real improvement?
With consistent implementation: most families see meaningful distress reduction within 3–4 weeks. Duration increases typically emerge within 6–8 weeks. Full 2-minute calm brushing: typically 8–12 weeks for moderate oral sensitivity. Severe oral defensiveness may require 3–6 months of clinical OT support.
Do I need ALL 9 materials, or can I start with just some?
Start with the 3-material starter kit: Extra-soft brush + Unflavored toothpaste + Visual timer. These three address the most common barriers. Add materials based on which barriers remain. The Z-Vibe and chewy tubes are for children with more significant oral defensiveness.
Can we brush without toothpaste at all?
Temporarily yes. Mechanical brushing removes plaque even without toothpaste. If your child truly cannot tolerate any toothpaste, prioritize getting the brushing motion established with water only. Introduce toothpaste once brushing motion is tolerated — inform your dentist.
My child is 10 and still can't brush. Is it too late?
No. Oral sensory processing can improve at any age with appropriate intervention. Older children often respond faster once they understand the "why" and have agency in the process. Give full control to the child, connect oral hygiene to self-image, and work with an OT who specializes in adolescent sensory challenges.
Didn't find your answer? → Ask GPT-OS®: pinnacleblooms.org/gpt-os | Book teleconsultation: pinnacleblooms.org/teleconsult
📞Urgent? FREE Helpline: 9100 181 181 | 24×7
📞Urgent? FREE Helpline: 9100 181 181 | 24×7
Preview of 9 materials that help with toothbrushing Therapy Material
Below is a visual preview of 9 materials that help with toothbrushing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

From Fear to Mastery. One Technique at a Time.
🏛️ Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev • CRO • WHO/UNICEF-Aligned Research
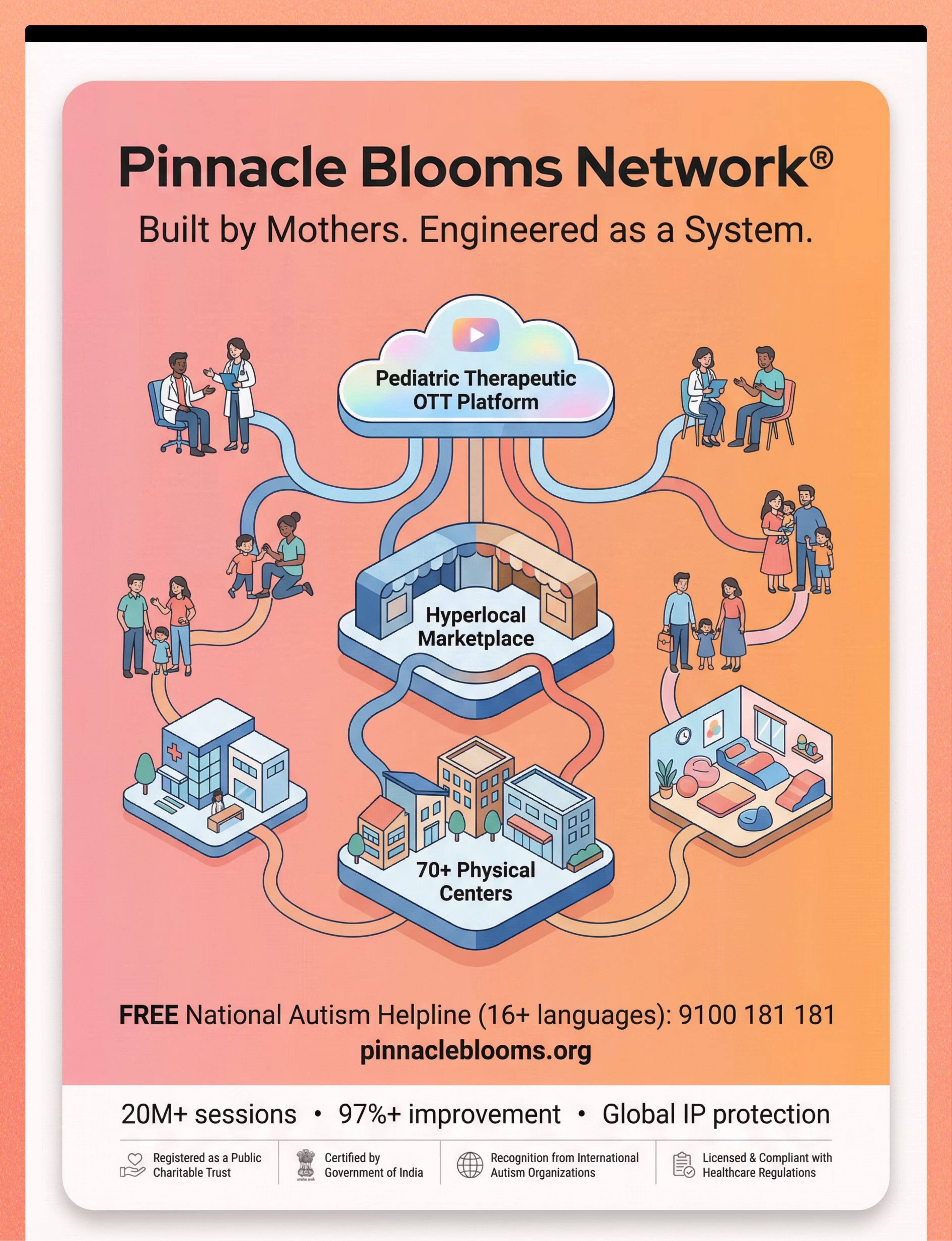
This technique page was built by a consortium of practicing pediatric therapists, developmental scientists, regulatory experts, and — most importantly — parents and families who have lived these challenges. It is part of the largest structured pediatric intervention knowledge base on Earth: 70,000+ technique pages, each evidence-linked, parent-accessible, and connected to the GPT-OS® system that has governed 20 million+ therapy interactions.
Your child's potential is not limited by their diagnosis. It is expanded by what you know, and by what you do with what you know — consistently, gently, and with evidence on your side.
🚀 Start This Technique Today
Launch your GPT-OS® guided toothbrushing protocol — personalized to your child's profile → pinnacleblooms.org/start/E-532
📋 Book a Professional Consultation
OT + SLP assessment | 70+ centers | Teleconsultation available across India and 70+ countries → pinnacleblooms.org/book
→ Next Technique: Bath Time Sensory Issues — E-533
You already own materials for this technique → techniques.pinnacleblooms.org
📞FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | India's only free, multi-lingual pediatric therapy helpline
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention planning with licensed occupational therapists, speech-language pathologists, dentists, and healthcare professionals. Persistent oral sensory sensitivities affecting oral hygiene may indicate underlying sensory processing or developmental conditions requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®. This is not medical advice.
© 2025 Pinnacle Blooms Network® | Unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | pinnacleblooms.org | Helpline: 9100 181 181 | GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are proprietary marks of Pinnacle Blooms Network®. All rights reserved.