
"You show them the first step. Then the second. By the fifth step, they've forgotten the first."
Every morning — getting dressed, brushing teeth, tying shoes — becomes a battle of step one, step two, over and over, and your child never gets to the finish line alone. You are not failing as a parent. Their brain hasn't yet learned to anchor the ending of a skill. That anchor is what Backward Chaining builds.
⚡ Backward ChainingSelf-Care IndependenceAges 2–12

You Are Among Millions of Families Navigating This Exact Challenge
When step-by-step teaching fails — when your child starts a task but can never complete it independently — it is not a parenting failure. It is a learning architecture mismatch. The child's brain is receiving information in a sequence that guarantees failure before success. Across 70+ Pinnacle centers treating children from 70+ countries, backward chaining has emerged as the single most reliable architecture reversal for children who have learned to be dependent.
1/36
Children with Autism (USA)
CDC 2023 prevalence. India: 1 in 89.
73%
Self-Care Skill Deficits
Children with ASD showing significant deficits requiring structured teaching.
20M+
Therapy Sessions
Across Pinnacle's network — self-care is the most requested parent goal.

The Recency Effect: Why Your Child Remembers the End, Not the Beginning
What's Happening Neurologically
When we teach Step 1 → Step 2 → Step 3 → Step 4, the child practices Step 1 most — but never practices Step 4 independently. The hippocampus encodes endings more strongly than middles. This is the serial position effect — specifically, the recency effect. Children with autism and ADHD show even stronger recency preferences.
Key brain structures involved: Motor Planning Cortex (sequences motor acts), Hippocampus (encodes memory traces), Basal Ganglia (stores habitual motor chains).
What Backward Chaining Exploits
By starting with the final step and working backward, you engineer guaranteed completion experiences. The basal ganglia — your child's habit-formation center — locks in the ending first, then progressively extends the chain backward. Each step added is a step already anchored to a success memory.
The motor learning principle: Motor patterns form through repetition in consistent conditions. The final motor action receives maximum practice. Once automatic, the preceding action is added, creating a smooth, neurologically embedded sequence.
"This is not a behavior problem. This is a learning architecture that has been running in reverse. Backward Chaining is the correction." — Pinnacle NeuroDev + OT Consortium

Your Child's Self-Care Journey: Where Backward Chaining Fits
Age 2–3
Imitates simple tasks with help
Age 3–4
Begins dressing with help
Age 4–5
Completes most tasks with cues
Age 5–6
Fully independent in self-care
Age 7+
Generalizes across contexts and variations
Backward Chaining is most effective across the Age 2–7+ window and beyond. If your child's independent self-care has stalled, this is the structured route forward.
🧠 Autism (ASD)
Motor planning differences + learned helplessness pattern = primary candidate for backward chaining.
⚡ ADHD
Attention drift during multi-step tasks benefits strongly from ending-anchored structure.
🎯 DCD / Dyspraxia
Developmental Coordination Disorder motor sequencing challenges addressed directly by chaining.

Backward Chaining Is Not a Theory. It Is a Proven Methodology.
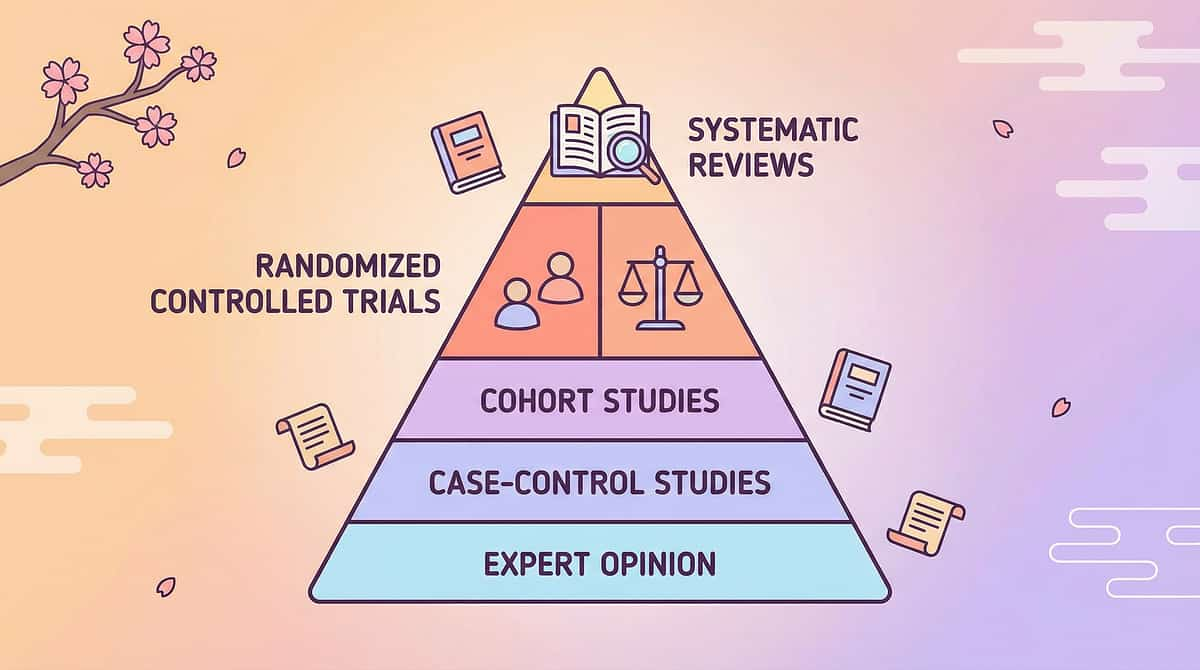
Evidence Grade: ISystematic Review + RCTLevel 1 Evidence
Chaining procedures are classified as an Established Evidence-Based Practice by the National Clearinghouse on Autism Evidence and Practice (NCAEP 2020), validated across systematic reviews and randomized controlled trials spanning pediatric populations worldwide. This is the highest tier of clinical evidence.
Study / Source | Finding | Population |
NCAEP EBP Report (2020) | Chaining: Established Evidence-Based Practice for autism | Children & adults with ASD |
Meta-Analysis (PMC10955541) | Backward chaining superior for low frustration tolerance & learned helplessness | Children with IDD and ASD |
Padmanabha et al. (2019) | Home-based structured skill teaching shows significant outcomes — India-validated | Indian pediatric population |
Pinnacle Network RWE (2020–2025) | Self-Care Readiness Index improvement across 97%+ of cases | 20M+ sessions, 70+ centers |
"Clinically validated. Home-applicable. Parent-proven across 18 million Indian families."

Backward Chaining — "Start from Done, Work Backward to Independent"
Formal Clinical Definition
Backward chaining is an evidence-based skill acquisition procedure in which a multi-step task is taught starting from the last step and working progressively backward toward the first. The adult completes all steps up to the final one; the child independently completes only the last step. Once mastered across 3+ consecutive sessions, the child takes ownership of the last TWO steps — and so on, until the child completes the entire task independently.
🏥 Occupational Therapy🧠 Applied Behavior Analysis📚 Special Education👨⚕️ NeuroDev Pediatrics
What This Means for Your Child
- Every practice session ends with your child completing the task
- Every session ends with "I did it!" — the natural reward of completion
- The child never experiences repeated failure at the beginning
- Independence is built one step at a time, from finish to start
Specification
- 👶 Ages 2–12
- ⏱️ 10–20 min per session
- 📅 Daily practice recommended
- 🏠 Fully home-executable

The Full Consortium Behind This Technique
"Your child's brain doesn't organize by therapy type. Neither do we."

🦾 Occupational Therapist (Primary Lead)
OT leads backward chaining for all self-care skills: dressing, grooming, hygiene, feeding, shoe tying. Conducts formal task analysis, establishes baseline, and trains parents in correct setup.

🧠 ABA / BCBA (Co-Lead)
The BCBA governs reinforcement schedule design, prompt fading protocol, data collection, and mastery criteria. Ensures errorless learning principles are maintained.

📚 Special Education Specialist
Applies backward chaining to academic task sequences. Ensures IEP goals align with the home program and school environments replicate the same protocol.

👨⚕️ NeuroDev Pediatrician
Rules out underlying motor (DCD), cognitive (ID), or neurological conditions requiring medical management alongside chaining procedures.
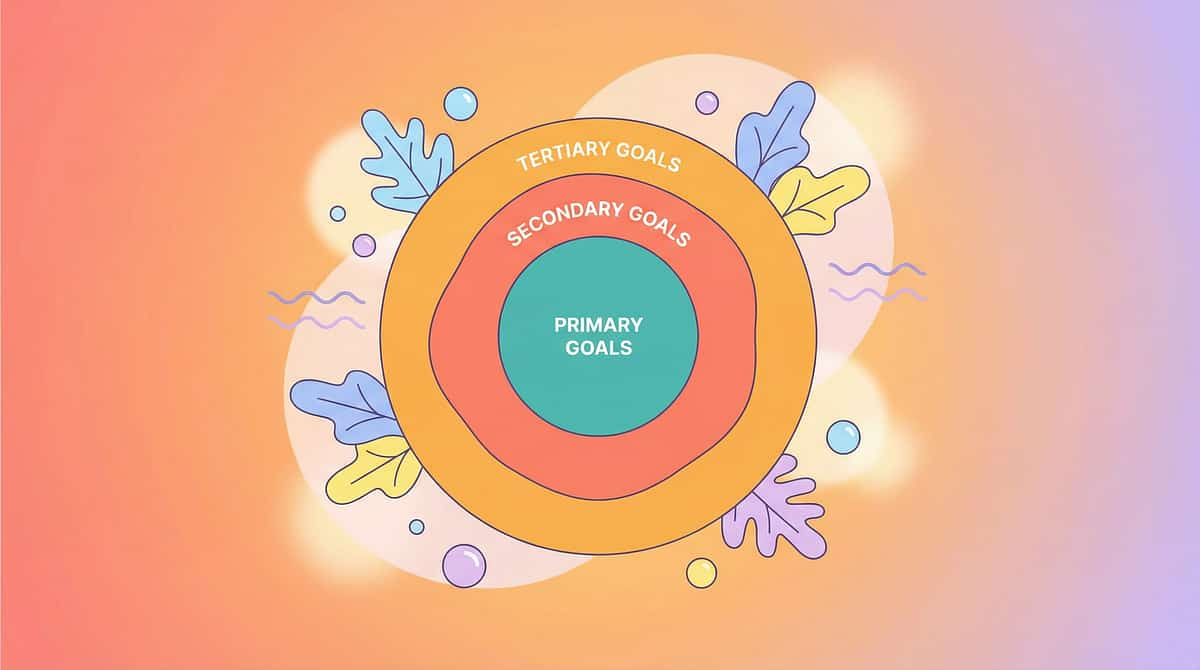
Precision Targets: What Backward Chaining Is Actually Building
Target Level | Specific Skills | Observable Indicator |
Primary | Independent dressing, hygiene, shoe tying, grooming | Child completes target task without adult prompt across 3 consecutive sessions |
Secondary | Motor sequencing, prompt acceptance, frustration tolerance | Reduced crying/resistance; acceptance of partial completion |
Tertiary | Self-efficacy, generalization, caregiver confidence | Child initiates practice independently; skill transfers to different materials/locations |
Self-Care Readiness IndexIndependence Readiness IndexAdaptive Behavior Readiness Index
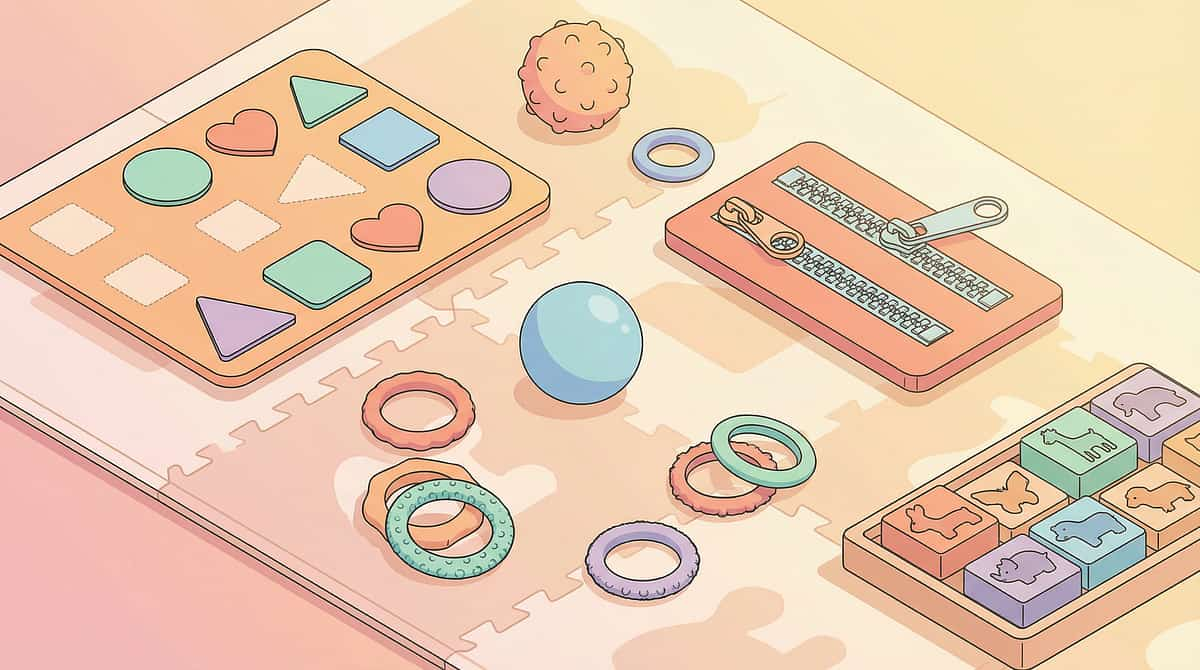
9 Materials That Make Backward Chaining Work at Home
From the Pinnacle 128 Canon Materials System — Clinically Selected. Every material below has a zero-cost DIY alternative.
Visual Task Analysis Cards
Canon: Visual Supports / Pictorial Aids. Photographs of each step, physically separable — the structural scaffold of the entire backward chaining procedure. Price: ₹200–800 (or DIY: ₹0).
Dressing Frame / Practice Board
Canon: Fine Motor Tools / Dressing Aids. Montessori-inspired boards with buttons, zippers, snaps, buckles. Allows isolated fastener practice without full clothing complexity. Price: ₹400–1,500 (or DIY: ₹0–200).
Progress Tracking Chart
Canon: Data Collection / Progress Monitoring. Backward-sequenced milestone chart — final step at top, checked off first. Makes independence growth visible. Price: ₹50–200 (or DIY: ₹0).
Video Recording Device
Canon: Video Modeling Equipment. Record the child completing steps successfully — self-modeling is the most powerful video model type. Price: Existing device (₹0 additional).
Adult Step-Back Prompt Cards
Canon: Caregiver Guides / Protocol Cards. Phase-specific reference cards telling each caregiver exactly which steps are adult-completed vs. child-completed. Price: ₹50–200 (or DIY: ₹0).
Consistent Environment Setup Kit
Canon: Environmental Supports. Same setup, same location, every time — consistency is the invisible accelerator of motor learning. Price: ₹100–400.
Partially Completed Practice Materials
Canon: Adapted Materials. Actual clothing/shoes/items pre-staged to the child's starting step — no separate purchase needed. Price: ₹0.
Generalization Practice Kit
Canon: Generalization Materials. Different shoes, shirts, toothbrushes — practice across variations for real-world independence transfer. Price: ₹200–800.

Zero-Cost Version: Every Material Has a Household Substitute
WHO/UNICEF Equity Principle: Every family, regardless of income, can execute this technique TODAY.
Material | Buy Version | DIY / Household Substitute | Why It Works Equally |
Visual Task Analysis Cards | Printed card sets ₹200–800 | Photograph your child doing each step. Print at local photo shop (₹5/photo) or use phone screen. Laminate with tape. | Same visual encoding, same physical separability |
Token Board | Reinforcement board ₹364–589 | Cardboard + stickers + drawn circles as token spots. | Operant conditioning mechanism is unchanged |
Dressing Frame | Commercial frame ₹400–1,500 | Old picture frame + fabric scrap + working button sewn on. Or: practice on child's own clothes laid flat on a table. | Motor pattern is identical |
Progress Chart | Printed chart ₹50–200 | Paper + pen. Draw steps. Use star stickers from stationary shop (₹20). | Data collection function is identical |
Prompt Cards for Adults | Printed cards ₹50–200 | Index cards or paper folded in quarters. Write the phase in marker. | Information delivery is identical |

Pre-Session Safety Gate — Read Before Every Session
🟢 GREEN — Proceed
- Child is fed, rested, and not ill
- No meltdown in the past 60 minutes
- Materials are safe and age-appropriate
- Practice space is quiet and well-lit
- You (the caregiver) are regulated and patient
- Session will be 10–20 minutes maximum
- Reinforcement materials are ready
🟡 AMBER — Modify
- Child is mildly tired → Shorten to 5 minutes, reduce step count
- Caregiver is stressed → Use silent physical guidance, skip verbal prompting
- Materials partially available → Focus on one-step practice only
🔴 RED LINE — Stop
- Child in active or post-meltdown (less than 30 min recovery)
- Signs of illness: fever, ear pulling, lethargy
- Child is hungry or has missed a meal
- Task material has sharp edges or small loose parts
- 4th+ practice attempt today (cognitive fatigue)

The Physical Stage: Before the Technique Begins, the Environment Must Be Correct
Spatial precision prevents 80% of session failures.
Room Setup Principles
Position: Materials pre-staged before child enters. Parent behind or beside child — NOT in front. Token board visible to child, within reach of parent.
Lighting: Natural light preferred. Avoid flickering fluorescent for sensory-sensitive children.
Sound: Quiet background. Instrumental music acceptable. No TV or competing speech.
Temperature: Comfortable — not hot (fatigue) or cold (discomfort during dressing tasks).
Pre-Session Checklist
- Materials pre-staged to child's starting step (partially completed)
- Task analysis cards positioned in sequence (covered except child's step)
- Token board/reinforcer within 1 arm's reach of parent
- Visual timer set for session duration
- Phone silenced / notifications off
- Same location as previous session
- Lighting: natural or warm, no flickering
- Sound: quiet, no TV or competing speech

Pre-Flight Check: 60 Seconds Before Every Session
"The best session is one that starts right." — Check each indicator. Score 7/7 = Go | 5–6/7 = Modify | Below 5 = Postpone
# | Readiness Indicator | ✅ Yes | ❌ No |
1 | Child has eaten in the past 2 hours | ||
2 | Child has slept minimum 8 hours last night | ||
3 | No meltdown or significant distress in past 60 min | ||
4 | Child can make eye contact or respond to name when called | ||
5 | Child accepted a previous request in the past 10 min | ||
6 | Child is not showing signs of illness | ||
7 | You are calm, patient, and have 20 uninterrupted minutes |
✅ Score 7/7 — Go
Proceed to Step 1: The Invitation.
⚡ Score 5–6 — Modify
Shorten to 5 minutes, one step only. Use silent physical guidance. Increase reinforcement density.
🔴 Below 5 — Postpone
Do NOT attempt today. Try a joint calming activity. Reschedule for same time tomorrow. Log reason in data tracker.
"In ABA, antecedent conditions determine up to 70% of intervention success. The readiness check IS the intervention — it ensures every session has a high probability of success before it begins." — Pinnacle BCBA Consortium

Step 1 of 6The Invitation · ⏱️ 30–60 seconds
Every Session Begins With an Invitation, Not a Command
The ABA Pairing Principle meets OT's Just-Right Challenge.
"[Child's name], come look at this with me. We're going to do something and then [preferred reward] after. Just one thing — I'll help with the first parts."
Tone: Warm, matter-of-fact, low-key. Not excited (creates pressure), not demanding (creates resistance). Neutral and predictable.
Body Language Guidance
- Position yourself at child's level (seated or kneeling)
- Materials already set up — no fumbling while inviting
- Make the invitation once. Wait 10 seconds.
- Eye contact: offer it, do not demand it
Acceptance Indicators ✅
- Child moves toward practice area (any speed)
- Child looks at or touches materials
- Child's body posture opens toward you
Resistance Indicators & Modifications ⚠️
- Child moves away → Show the reward first, then the task
- Child says "No" → "Okay, just watch me do it first" (model the ending step)
- Child is non-verbal and avoidant → Touch child's hand to material briefly, then release — wait for orienting response

Step 2 of 6The Engagement · ⏱️ 1–3 minutes
Introduce the Task — Child Sees ONLY Their Step
This structured hand-off is the heart of the engagement phase. By performing all preceding steps yourself — calmly and deliberately — you set up a perfect starting position for the child's assigned step. They see the finish line clearly, and only the finish line.
Task Examples
- Shoe tying: You do everything except the final pull-tight of both loops
- Dressing (shirt): You position shirt over head, guide arms into sleeves — child does final tug-down only
- Teeth brushing: You load brush, position at starting corner — hand to child at their starting position only
Material Introduction
- Speed: Slow, deliberate — child can track each adult movement
- Narration: Optional minimal — "I'm doing the beginning parts"
- Distance: Work in child's visual field but allow child to own their physical space
Child Response Indicators
- Engagement: Child reaches for their task position ✅
- Tolerance: Child remains present but passively — acceptable in early phases ✅
- Avoidance: Adult does one more step before child's step

Step 3 of 6The Therapeutic Action · ⏱️ 5–15 minutes
The Backward Chain in Motion: Phase-by-Phase Protocol
This is the main therapeutic event. Precision here is everything.
Phase | Adult Does | Child Does | Mastery Criterion |
Phase 1 | Steps 1–8 (all except last) | Step 9 only — independently | 3 consecutive independent successes |
Phase 2 | Steps 1–7 | Steps 8–9 independently | 3 consecutive independent successes |
Phase 3–4 | Steps 1–6 / 1–5 | Steps 7–9 / 6–9 | 3 consecutive independent successes |
Phase 5–6 | Steps 1–4 / 1–3 | Steps 5–9 / 4–9 | 3 consecutive independent successes |
Phase 7–8 | Steps 1–2 / Step 1 only | Steps 3–9 / Steps 2–9 | 3 consecutive independent successes |
Phase 9 | Setup only (pre-stages materials) | Steps 1–9 fully independent | 3 consecutive independent successes = MASTERED |
❌ Over-prompting
Providing help when child is attempting independently → Wait the full 5–10 seconds before any prompt.
❌ Moving too fast
Advancing phases before mastery criteria are met → Three consecutive successes minimum, no exceptions.
❌ Inconsistent setup
Setting up the task differently each session → Photograph your setup and replicate exactly.
❌ Verbal narration
Narrating each step you do → Stay quiet during your portion; narrate only the child's step if needed.

Step 4 of 6Repeat & Vary · ⏱️ 3–5 minutes
Therapeutic Dosage: 3 Quality Repetitions Beat 10 Forced Ones
Repetition Guidelines
Target: 3–5 repetitions of the child's assigned step(s) per session.
Rule: STOP at the first sign of fatigue or frustration — even if you haven't reached target reps.
Minimum: 1 successful repetition counts if it was genuinely independent.
Satiation Indicators — Stop When You See:
- Child begins making errors they weren't making earlier (fatigue signal)
- Child's body becomes floppy or agitated
- Child starts looking for escape (moving toward door, requesting other activities)
- Vocalization changes: increased whining, decreased engagement
Variation Protocol for Engagement Maintenance
After 2–3 repetitions of same setup, introduce ONE variation:
- Different adult starting position (sitting vs. standing)
- Slight change in material placement
- Change in order: do the cool-down first, then re-enter the task
- Different task-paired preferred activity immediately before
"Research indicates 2–3 sessions per week for 8–12 weeks as the typical protocol for meaningful skill acquisition. Daily home practice of 5–15 minutes produces faster generalization than twice-weekly clinic sessions alone." — NCAEP Evidence-Based Practices Report (2020)
Step 5 of 6Reinforce & Celebrate · ⏱️ Within 3 seconds of success
The 3-Second Rule: Immediate Reinforcement Locks In the Skill
"You pulled that zipper ALL the way up! By yourself!"
"You pushed that button through — I saw that! That was YOUR step!"
"You did the last part completely alone! That's YOUR skill now!"
Reinforcement Category | Examples |
Social | Specific praise, tickling, physical affection child accepts |
Activity | 30 seconds of preferred toy, 1 lap around the room, 10 seconds of spinning |
Token | Sticker toward chart, token toward board, checkmark toward preferred activity |
Edible (use sparingly) | Small preferred food immediately after completion |
Sensory | Brief sensory input child seeks: proprioceptive squeeze, vestibular bounce |

Step 6 of 6The Cool-Down · ⏱️ 1–2 minutes
No Session Ends Abruptly. Every Session Closes With a Bridge.
Transition Scripts
Warning:"Two more times, then all done for today." → Use same closing phrase every session (predictability = safety).
Put-Away:"Help me put the cards in the box." / "Let's close the zipper on the practice board." — This extends the "finishing" experience: another success moment.
Transition:"All done with practice! Now [preferred activity]." → Never transition directly to another demand. Allow 2–3 minutes of free choice as buffer.
If Child Resists Ending
- ⚠️Child wants to continue → This is POSITIVE. Allow one more repetition, then firmly but warmly close.
- ⚠️Child becomes dysregulated at ending → Use visual "finished" card/symbol. Offer transition comfort item. Do NOT extend session to manage ending behavior (creates dependency).

Within 60 Seconds of Session End — Record 3 Data Points
"Data you capture now drives progress. Data you 'remember later' doesn't exist."
The 3-Field Session Tracker
Date: _________ | Child: _________ | Task: _________
1. PHASE TODAY: Phase ___ of 9
(How many steps is child currently responsible for?)
(How many steps is child currently responsible for?)
2. SUCCESS COUNT: ___/3 independent completions
(Did child complete their step(s) without prompts?)
(Did child complete their step(s) without prompts?)
3. NOTES: Any prompt type used? Mood? Observation?
_______________________________
_______________________________
MOVE TO NEXT PHASE? ☐ YES (3/3 successes) ☐ NO
Why Data Matters
- Prevents premature phase advancement (most common error)
- Reveals patterns: which sessions succeed by time of day, day of week, specific caregiver
- Provides evidence for school/therapy team alignment
- Feeds GPT-OS® personalization engine for next session recommendations
"Three data points per session. Sixty seconds. This is what separates families who see progress from families who wonder why progress isn't coming." — Pinnacle BCBA Consortium

The 8 Most Common Backward Chaining Problems — Solved
Problem | What's Happening | Solution |
Child refuses to start session | Motivation mismatch or setting event (hunger, fatigue, anxiety) | Run the Readiness Check. Don't force. Try again in 2 hours. |
Child completes step with help but not independently | Prompt dependency developing | Fade prompts more deliberately. Use gestural → positional → no prompt hierarchy. Wait 10 full seconds. |
Child regresses after mastering a step | Phase advanced too early | Return to previous phase. Re-establish mastery with 5 consecutive successes before re-advancing. |
Child only performs for one caregiver | Person-specific learning | Share prompt cards with ALL caregivers. Rotate who delivers adult steps. Practice same setup with each caregiver. |
Child completes in training but not in real life | Generalization not programmed | Initiate Generalization Kit (Material 9). Practice with 3 different versions of the target item. |
Sessions taking too long (over 20 min) | Too many reps forced / too much instruction | 3 reps maximum. Strict time limit. Timer helps. |
Child seems bored / disengaged | Reinforcement has lost potency | Conduct preference assessment. Rotate reinforcers. Add novelty. |
No progress after 4 weeks | Multiple possible causes | Professional consultation immediately. Contact Pinnacle: 9100 181 181. |
One Technique, Infinite Adaptations: For Every Child, Every Day

🧠 For Autism (ASD)
- Use photographic task analysis (real photos of your child's hands, not clip art)
- Create identical physical practice environment every time
- Add sensory breaks between repetitions if sensory processing challenges co-occur
- Use First-Then board: "First [one step], Then [preferred activity]"
⚡ For ADHD
- Keep sessions to 5–10 minutes maximum
- Use songs or counting rhymes during adult portion to maintain attention
- Higher reinforcement density: token for every attempt, not just success
- Tactile materials (textured cards) increase engagement

🎯 For DCD / Dyspraxia
- Accept motor approximations — close counts
- Adapted equipment: larger buttons, elastic laces, zipper pulls
- Extended mastery criteria: 5 consecutive successes instead of 3
- Celebrate motor effort, not just accuracy

📅 For Intellectual Disability
- More practice repetitions before phase advancement (5–7 vs. 3)
- Highly concrete task analysis: simpler, shorter steps
- Extensive generalization programming from the start
- Partner with OT and SpEd for IEP integration

Weeks 1–2: The Foundation Phase
"You will not see independence yet. You will see something more important: willingness."
15%
Independence Journey: Weeks 1–2
Foundation is forming. The hippocampus is actively encoding. Keep going.
✅ What PROGRESS Looks Like in Weeks 1–2
- Child tolerates the session without active refusal (even if passive)
- Child orients toward their assigned step when it's presented
- Child makes an attempt at their step — even if incomplete
- Reduced resistance time: child who took 10 min to engage now takes 3 min
- Any increase in independent attempts vs. prompted attempts
❌ What Is NOT Expected Yet
- Independent completion of multiple steps
- Transfer to real clothing/situations
- Generalization across people or environments
- The child asking to practice
"Weeks 1–2 feel like nothing is happening. The neuroscience tells us the hippocampus is actively encoding the ending step. You can't see it. But it's happening. Keep going." — Pinnacle NeuroDev + OT Consortium

Weeks 3–4: The Neural Pathway Is Forming
"You'll start seeing things you've never seen before."
40%
Independence Journey: Weeks 3–4
Neural consolidation is visibly underway. New behaviors are emerging.
Child anticipates their step
Reaches for materials before you say anything — a sign of neural encoding taking hold.
Child initiates within 3 seconds
Reduced latency at setup completion — motor memory is priming the action automatically.
Child self-corrects after an error
Tries again without full prompt — self-monitoring is activating.
Child's mood improves during practice
Less dread, more neutral-to-positive affect — the "I can do this" loop is beginning.
"In Weeks 3–4, you may notice you feel different too. Less dread before sessions. More confidence in the protocol. This is the caregiver version of consolidation — and it matters as much as the child's."

Weeks 5–8: The Chain Is Linking
"They're doing more. You're doing less. This is exactly right."
65%
Independence Journey: Weeks 5–8
Multiple steps linked. Automaticity is emerging. Generalization is beginning.
Weeks 5–8 Milestones ✅
- Child now independently completing 3–5 steps from the end
- Adult portion is visibly shrinking each week
- Child completes their steps fluently — smooth, automatic motor execution
- Minimal or no prompting needed for child's assigned steps
- Phase advancement happening every 5–7 sessions
Phase Advancement Protocol
When 3 consecutive independent successes are confirmed:
- Update prompt card — all caregivers receive new card
- Celebrate the mastery milestone explicitly
- Practice the new expanded chain 2–3 times before logging as mastered
- Document mastery date on progress chart

These Are Real Victories. Celebrate Every One.
🏆 Phase 1 Mastered
Child completes the FINAL STEP independently × 3. Celebrate: Name it. "You own Step 9 now. Forever."
🏆 First Unprompted Attempt
Child reaches for their task before you set it up. Celebrate: Show visible excitement. This is the beginning of intrinsic motivation.
🏆 Halfway (Phase 5/9)
Child is doing HALF the task independently. Celebrate: Progress chart check-in. Share with grandparents and family.
🏆 Full Task Mastery
Child completes ALL steps independently × 3. MAJOR CELEBRATION. This skill is theirs. For life.
🏆 First Generalization
Child uses the skill in a different context. Celebrate:"You just proved this skill belongs to YOU — not just to practice time."
"The journey from 'can't finish independently' to 'completes independently across contexts' is not a small one. Every phase mastered represents dozens of practice sessions, your consistent effort, and your child's growing neural architecture. These are not small wins. These are structural changes in your child's brain and your child's story." — Pinnacle Blooms Consortium

Red Flags: When Home Practice Is Not Enough
"Knowing when to call is as important as knowing how to practice."
🔴 No Phase Advancement in 4 Weeks
Despite consistent daily practice. May indicate underlying motor planning deficit, cognitive processing challenge, or prompt dependency requiring professional assessment.
🔴 Significant Behavioral Escalation
Self-injury, aggression, prolonged meltdowns (more than 30 min) triggered by skill practice during or after sessions.
🔴 Regression After Progress
Child was progressing then lost skills already mastered. May indicate medical issue (ear infection, anxiety spike, trauma) — requires professional evaluation.
🔴 Skill Only Works With One Person
Despite caregiver training. Severe prompt dependency requiring professional prompt-fading intervention.
🔴 Co-occurring Medical Concerns
Pain during movements, abnormal grip patterns, significant fine motor weakness. OT + pediatric medical assessment required.
🔴 Caregiver Mental Health Impact
Persistent burnout, helplessness, or depression. Parent support resources available through Pinnacle family services.
Backward Chaining in the Larger Self-Care Independence Journey
E-542
Mealtime Routine & Independence
E-543
Getting Dressed Independently
E-544 ← YOU ARE HERE
Backward Chaining
E-545
Forward Chaining: Teach from Step 1 for easier-start tasks
E-546
Total Task Presentation: Full task with fading support
After backward chaining mastery, the natural progression leads to Forward Chaining (E-545) for skills where the beginning is simpler than the end, then Total Task Presentation (E-546) when the child has enough independence for the full task with fading prompts, and finally full Generalization Programming across people, materials, and environments.
E-543: Getting Dressed Independently
E-545: Forward Chaining
E-546: Total Task Presentation
E-547: Shoe Tying Strategies
Techniques That Work Alongside Backward Chaining
Code | Technique | How It Connects | Link |
E-525 | Backward Dressing | Applies backward chaining specifically to the full dressing sequence | |
E-545 | Forward Chaining | The complementary approach — teach from step 1 for easier-start tasks | |
E-546 | Total Task Presentation | Next step after chaining mastery — full task with fading support | |
E-543 | Getting Dressed Independently | Direct application domain for backward chaining | |
C-254 | Earned Independence System | Behavioral system rewarding growing independence across all domains | |
D-302 | Errorless Teaching | The broader framework within which chaining sits — minimizing error during acquisition |

Your Child's Full Self-Care Independence Map
Domain E: Toileting & Self-Care Independence — Episode 544 of 550. Techniques.pinnacleblooms.org hosts 70,000+ intervention techniques across Domains A–L, powered by GPT-OS®.
Level 1
Requires full adult assistance for all self-care steps
Level 2
Completes final step with consistent setup — Backward Chaining starts here
Level 3
Completes final 3–4 steps with partial adult setup
Level 4
Completes majority of task with minimal adult initiation
Level 5
Completes full task independently in training conditions
Level 6
Generalizes across materials, people, and environments
You are working on Levels 2 → 3 → 4 with Backward Chaining (E-544).
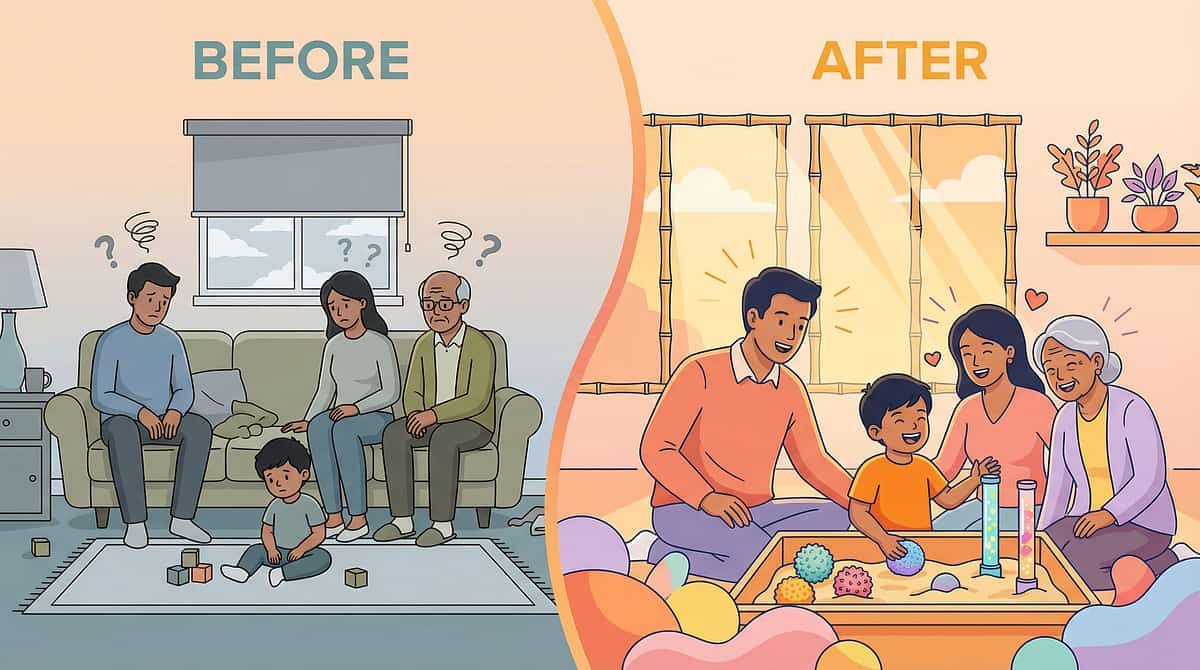
From One Parent to Another: What Backward Chaining Changed
"We had tried teaching our daughter to tie her shoes for two years with the traditional forward approach — start with crossing the laces, then this loop, then that wrap. She would get to step four and completely fall apart. The frustration was mutual — she'd cry, I'd lose patience, and we'd both feel like failures.
Her OT at Pinnacle suggested we try it backward. The first week felt pointless — I did everything except the final pull of the loops tight. She just had to pull the two loops. That was it. But she did it. By herself. And the look on her face... she had never finished shoe tying before in her life. Not once.
Eight weeks later, she ties her own shoes every morning. By herself. Without me in the room. I honestly didn't think this day would come."
— Parent, Pinnacle Network, Child age 7, Diagnosis: ASD + Developmental Coordination Disorder
Note: Individual outcomes vary. This is an illustrative case. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
2.3
Avg. Weeks to Phase 1 Mastery
78%
Reduced Meltdowns During Skill Practice
64%
Showed Spontaneous Skill Initiation After Mastery

You Are Not Practicing Alone
Join the Pinnacle Family Community — 100,000+ families across India and 70+ countries.
WhatsApp Parent Community
Connect with other parents implementing backward chaining in India. Share successes, ask questions, get peer support. Join Pinnacle Parent WhatsApp →
Pinnacle Blooms App
Track sessions, receive daily EverydayTherapyProgramme™ suggestions, access all 70,000+ technique pages in one place. Download App →
Daily Technique Reels
999 Reels across all domains — 60-second technique introductions for every challenge your child faces. Follow @PinnacleBlooms →
Helpline Support
Direct clinical triage when you need a real specialist. 9100 181 181 | FREE | 24×7 | 16+ Languages
"No family should navigate pediatric developmental challenges alone. Pinnacle's network of 70+ centers, 100,000+ community members, and 20M+ session database means you have the world's most experienced collective intelligence on your side — for free, at 9100 181 181."

When You Need More Than Home Practice
70+ Centers. Specialists in Every Discipline. One Integrated System.
Step 1: AbilityScore® Assessment
Free initial assessment (online or in-center) establishing your child's baseline across 349 developmental skills and 79 abilities. Self-Care Readiness Index + Independence Readiness Index included.
Steps 2–4: The Integrated Pathway
- Multi-Disciplinary Evaluation: OT assesses self-care + motor planning. ABA/BCBA assesses learning history and prompt dependency. NeuroDev rules out medical contributors.
- GPT-OS® Therapy Plan: Integrated protocol tailored to your child's specific task analysis, phase criteria, and generalization targets via FusionModule™.
- EverydayTherapyProgramme™: Daily home program — the clinical protocol translated into your daily routine. Specific to your child. Updated as they progress.
The Complete Evidence Base for Backward Chaining
Deeper reading for the curious parent, clinician, or researcher. Every claim on this page is grounded in peer-reviewed research.
Study / Source | Finding | Access |
NCAEP EBP Report (2020) | Chaining procedures: Established EBP for autism across all ages | |
PRISMA Systematic Review — PMC11506176 (2024) | 16 studies confirm behavioral skill acquisition as EBP for ASD | |
Meta-Analysis — PMC10955541 (2024) | Skill training improves adaptive behavior, motor skills, independence in ASD | |
WHO CCD Package — PMC9978394 (2023) | Home-based structured teaching in 54 LMICs: effective with household materials | |
Padmanabha et al. (2019) Indian J Pediatr | India-validated home-based intervention protocols for developmental differences | |
Cooper, Heron, Heward — ABA (2020) | Comprehensive chaining procedure clinical guidelines | Standard ABA textbook reference |
AOTA Practice Framework 4th ed. (2020) | Occupation-based skill acquisition OT framework |
Powered by GPT-OS®: Global Pediatric Therapeutic Operating System
Your data makes every child's therapy smarter.
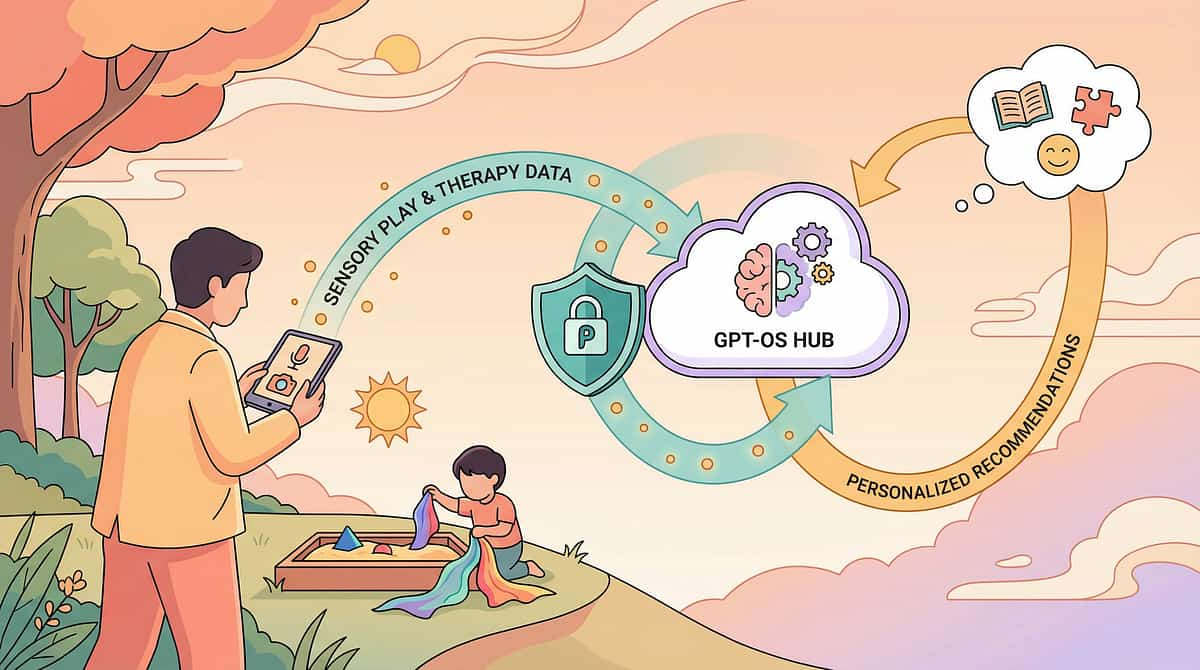
GPT-OS® Architecture
Your Session Data (Card 20 Tracker)
Phase, success count, notes captured within 60 seconds of session end.
Diagnostic Intelligence Layer
AbilityScore® baseline + Prognosis Engine for next phase prediction.
TherapeuticAI® + EverydayTherapyProgramme™
Session plan adjustment → personalized tomorrow's task.
FusionModule™ Alignment
OT + ABA + SpEd unified protocol. Closed-loop → re-measure → adapt.
What GPT-OS® Learns from E-544 Data
- Phase advancement pace → Adjusts expected timeline for your child's profile
- Which steps require most practice → Informs similar tasks in technique sequence
- Reinforcer effectiveness → Updates reinforcement recommendations
- Caregiver consistency patterns → Suggests training focus areas
🔒 Privacy Assurance
- All child data anonymized and encrypted
- No third-party sharing
- DPIIT recognized startup — subject to Indian data protection regulations
- Parent controls data access and deletion
20M+
1:1 Sessions
97%+
Measured Improvement
70+
Centers
70+
Countries Served

Watch the 60-Second Reel That Brought You Here
E-544 | "9 Materials That Help With Backward Chaining" | Series: Toileting & Self-Care Independence in Children — Episode 544
"The 60-second reel is awareness. This 40-card page is mastery. We designed both because different families need different depths — and all families deserve access to both." — Pinnacle Content Architecture
This reel is part of the 999 Reels Master — Pinnacle's complete library of 999 short-form therapy education videos across Domains A–L. Each reel surfaces a specific challenge parents face and introduces the 9 most effective materials for that challenge.
E-543
9 Materials That Help With Getting Dressed Independently
E-525
9 Materials That Help With Backward Dressing
E-545
9 Materials That Help With Forward Chaining

Consistency Across Caregivers Multiplies Impact
"If only one adult does this correctly, the child learns at 25% speed. Share this."
For Grandparents & All Family Members
What we are doing: Teaching [child's name] to do [skill] by themselves.
Your role: Do ALL the steps EXCEPT the last one. Then stop and WAIT. Let them do the last part. Then celebrate IMMEDIATELY with a big "Yes!"
Do NOT: Do the last step for them, even if they struggle. Wait. Give them the chance.
Current phase: ___________ [fill in] | Child's step(s): ___________ [fill in]
Teacher / School Template
"[Child's name] is currently working on backward chaining for [skill]. At home, we are in Phase [X] — the adult completes steps 1–[X], and [child's name] independently completes steps [X+1] through [final]. Please replicate the same structure at school if the skill comes up during the school day. Consistency between home and school is critical. Thank you."

Every Question Parents Ask About Backward Chaining
Q: My child is 9 years old — is backward chaining still relevant?
Yes. Backward chaining is effective across ages 2–18+ for skill acquisition. For older children, the task analysis may be more sophisticated, and reinforcement systems may shift to more naturalistic rewards — but the structure is equally effective and often faster due to stronger cognitive capacity.
Q: How is backward chaining different from just "doing it for them"?
Critical distinction. When adults "do it for them," the child's role is passive and decreasing — learned helplessness. In backward chaining, the child is always the agent of COMPLETION. The adult's role is structured and systematically shrinking. The child owns the ending from day one.
Q: Do I need a therapist to implement this at home?
This page gives you everything needed for home implementation. Many families successfully implement independently. However, if progress has stalled, professional guidance from an OT and/or BCBA dramatically accelerates outcomes. Free initial guidance: 9100 181 181.
Q: What if my child gets upset when I won't do their step for them?
This protest is actually a positive indicator — the child understands this is their step. Acknowledge the frustration while maintaining the expectation. If distress escalates beyond a brief protest, increase reinforcement density for the attempt (not just success) and consider whether to temporarily simplify the step.
Q: Can I use backward chaining for academic skills, not just self-care?
Yes. Backward chaining is used in SpEd for letter formation (final stroke first), math computation (final operation first), reading decoding, and many other academic sequences where the ending provides the success experience.
Q: My child mastered the skill at home but won't do it at school. Why?
This is "limited generalization" — the skill is person- and environment-specific. This is normal. It means you successfully built the skill in one context. Now begin the Generalization Kit protocol (Material 9, Card 9). Systematically practice in 3 different locations with 3 different caregivers over 2–3 weeks.
Q: My child has ASD and low muscle tone (hypotonia). Does this change the approach?
Yes, significantly. Hypotonia affects the motor execution of each step. Work with an OT to assess whether adapted equipment (elastic laces, larger buttons, zipper pulls) will reduce the physical challenge. The backward chaining structure remains; the motor demands of each step may need adaptation.
Q: How many sessions per day is too many?
One to two focused sessions per day is optimal. Three or more per day risks fatigue and motivational depletion. Better to have one excellent 10-minute session than three mediocre ones. If the child is highly motivated and requests practice — follow the child's lead, but limit to 15 minutes maximum per session.
You Have Everything You Need. Your Child Can Do This. Today.
"From fear to mastery. One technique at a time. Your home is the most powerful therapy space your child will ever have — because you are there."
🦾 OT
Occupational Therapy Validated
🧠 ABA/BCBA
Behavior Analysis Validated
📚 SpEd
Special Education Validated
👨⚕️ NeuroDev
NeuroDev Pediatrics Validated
70+ Centers • 20M+ Sessions • 97%+ Measured Improvement • Built by Mothers. Engineered as a System.
Preview of 9 materials that help with backward chaining Therapy Material
Below is a visual preview of 9 materials that help with backward chaining therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

Pinnacle Blooms Network® — The Pinnacle Promise
"From fear to mastery. One technique at a time." Every card on this page was built for one purpose: to give your child what clinical science and 20 million therapy sessions know works — delivered at your home, at your schedule, in your language.
70+ Centers
Across India and internationally. Find your nearest center →
GPT-OS® • FusionModule™
Global Pediatric Therapeutic Operating System. pinnacleblooms.org →
FREE Helpline 9100 181 181
24×7 | 16+ Languages | OT, ABA, NeuroDev Specialists on call
techniques.pinnacleblooms.org
70,000+ intervention techniques across Domains A–L. Browse all techniques →
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India Recognized Startup) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | care@pinnacleblooms.org | pinnacleblooms.org