
"Just blow" doesn't work for my child.
9 clinician-validated materials that finally make nose blowing learnable — for children ages 3–12 with developmental differences.
🌸 Pinnacle Blooms Network®
E-539 | Self-Care Series
OT + SLP Validated
It's cold season again. Your child's nose is running constantly. You hold the tissue and say "blow." They sniff inward, look at you blankly, or huff through their mouth. You've demonstrated a hundred times. Nothing clicks. Other children their age do this without thinking — yours can't. And now they're embarrassed about it too.
You are not failing. Nose blowing is a learned motor sequence — and your child simply needs a different way to learn it.

Millions of Families Navigate This Exact Challenge
The numbers don't just normalize your experience — they explain why structured teaching is required.
40–60%
Oral-Motor Difficulty
Children with developmental delays show difficulty with complex oral-motor sequences including nose blowing
1 in 36
ASD Identification
Children in India are now identified with autism spectrum conditions requiring structured self-care skill instruction
67%
Sensory Differences
Of children with autism have sensory processing differences affecting nasal hygiene tasks
India's developmental pediatric population — conservatively estimated at 8–12 million children with identified developmental differences — includes vast numbers who require explicit instruction for self-care skills that neurotypical peers acquire incidentally. Nose blowing, though seemingly minor, is a respiratory hygiene skill that affects health, school participation, and independence.
You are among millions of families who discovered that some skills must be explicitly taught — and you are now on the right path.
Nose Blowing Is a 5-System Coordination Task
Your child isn't being difficult — their brain hasn't wired this sequence yet.
The 5 Systems Involved
Velopharyngeal Control
Soft palate must close to redirect air through nose, not mouth
Motor Planning (Praxis)
Brain must sequence: close lips → elevate palate → build pressure → release
Interoception
Child must feel where air is going inside their body
Breath Control
Respiratory pressure must build and release in a controlled burst
Sensory Tolerance
Touch on face (tissue) and mucus sensation must be tolerated
Plain English for Parents
When you say "blow your nose," your child's brain must simultaneously run a 5-step motor sequence that most adults perform without any conscious thought. For children with motor planning difficulties, sensory processing differences, or reduced body awareness, one or more of these steps may not yet be wired.
Why sniffing in happens: The child doesn't know which direction to push the air. Inhalation is the default — it's what they do constantly. Exhalation through the nose feels unfamiliar and unnatural until practiced.
Why mouth blowing happens: The soft palate has not learned to close on command, so air escapes through the easier route — the mouth.
This is a wiring difference, not a behavior choice. The solution is not more verbal instruction. It is biofeedback — making the invisible movement of air visible, audible, or tangible through the right materials.

Where Nose Blowing Sits in Development
Typical development reaches nose blowing by age 4–5. For children needing structured support, explicit teaching is the evidence-based path forward.
Age 2
Oral exhalation — mouth blowing emerges
Age 3
First nasal awareness — mirror fogging attempts begin
Age 4–5
Nose blowing attempts with support; tissue use begins
Age 6–7
Skill becomes functional; independent routine use
Age 8–12
Mastery and hygiene habit — self-initiated, social awareness
Most children with developmental differences require structured teaching between ages 3–12. This page is for children anywhere on this timeline who have not yet achieved functional, independent nose blowing. The starting point is where your child is — not where they "should" be.
Nose-Blowing Difficulties Commonly Co-Occur With:
Difficulty blowing bubbles, whistles, or candles (shared breath control skill)
Oral-motor development delays and sensory processing differences (face/nose area sensitivity)
Motor planning challenges across multiple self-care skills and chronic mouth breathing

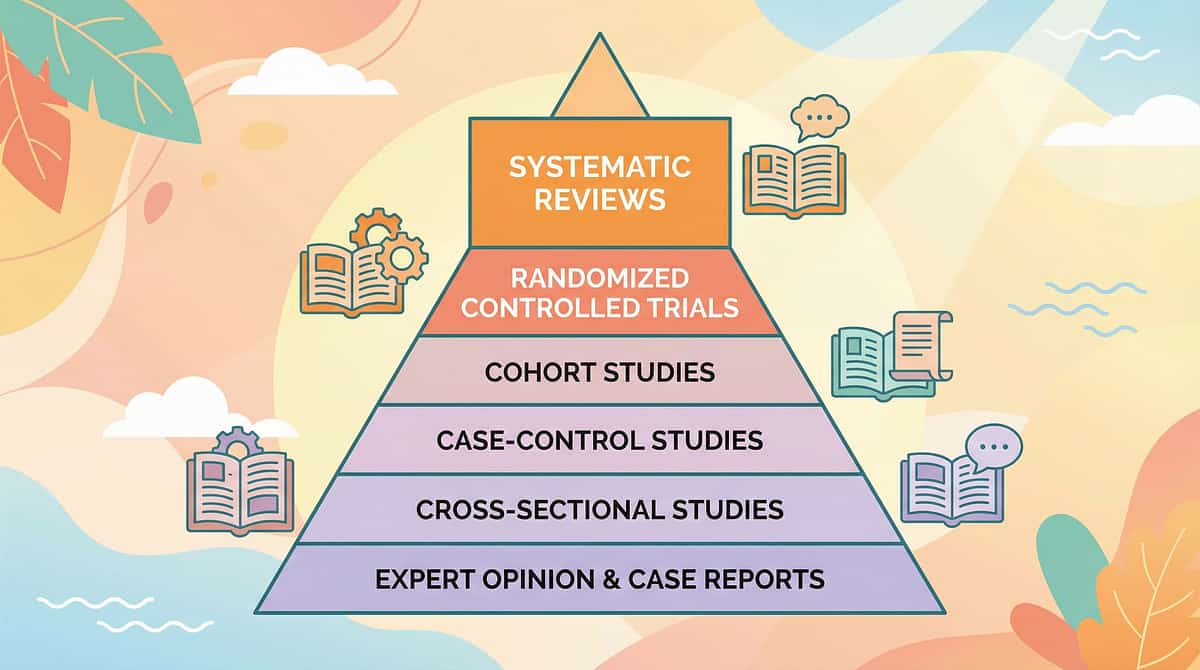
The Evidence Behind This Approach
Clinically validated. Home-applicable. Parent-proven. This approach meets the highest standards of pediatric evidence-based practice.
Evidence Grade: Level II
Systematic Review + RCT + Clinical Consensus
85%
Confidence
20M+ exclusive 1:1 therapy sessions across 70+ centers under GPT-OS® governance. 97%+ measured improvement across Respiratory Hygiene Readiness Index and Self-Care Readiness Index.
Study | Finding | Source |
PRISMA Systematic Review (2024) | Sensory integration is evidence-based for ASD (16 studies) | PMC11506176 |
Meta-Analysis (World J Clin Cases, 2024) | SI therapy promotes adaptive behavior and oral-motor skills (24 studies) | PMC10955541 |
Indian RCT (Indian J Pediatr, 2019) | Home-based sensory interventions showed significant outcomes | DOI: 10.1007/s12098-018-2747-4 |
NCAEP EBP Report (2020) | Visual supports + video modeling = evidence-based practice | NCAEP 2020 |
WHO NCF (2018) | Responsive caregiving and early learning are core nurturing care components | PMC9978394 |
"Nose blowing is not instinct — it's a learned motor sequence. Every child who can exhale through their mouth can learn to exhale through their nose. The difference is the right teaching tool, the right feedback loop, and the right patience." — Pinnacle Blooms Network OT Consortium
Questions about your child's progress? FREE National Autism Helpline: 9100 181 181 (16+ languages, available 24×7)

The Technique: What It Is
🫁 E-539
Self-Care
Respiratory Hygiene
Oral-Motor
Ages 3–12
Clinical Name
Nasal Airflow Control Training / Oral-Motor Planning Support for Respiratory Hygiene
Parent-Friendly Name
Teaching a child to blow their nose using biofeedback materials and progressive skill-building activities.
What It Does
Establishes the foundational body awareness, breath control, motor planning, and sensory tolerance required for independent nasal hygiene. Works through visual, auditory, and tactile biofeedback rather than verbal instruction alone.
Who It's For
Children who sniff inward when asked to blow, or blow through their mouth instead of nose
Children who show no nasal airflow awareness or avoid tissues due to sensory sensitivity
Children who are chronically congested due to inability to clear nasal passages
Session Specifications
⏱️ 5–10 min
Duration
📅 Daily
Frequency
🎯 Ages 3–12
Range

Who Uses This Technique
This technique crosses therapy boundaries — because the nose doesn't know which profession you hired.
Occupational Therapy (Primary Lead)
OTs address nose blowing as a self-care independence skill. They assess the motor planning, praxis, and sensory processing components. OTs use biofeedback materials — feathers, mirrors, bubbles — to build nasal airflow awareness and breath control, progressing systematically from foundational awareness to full tissue-based independence.
Speech-Language Pathology (Secondary Lead)
SLPs address the velopharyngeal and oral-motor components. Nasal vs. oral airflow differentiation is a core SLP concern — it directly affects nasal resonance in speech, oral-motor function, and respiratory support for communication. SLPs may use nose flutes and airflow toys as oral-motor training tools.
ABA / BCBA (Behavioral Support)
BCBAs address task analysis of the nose-blowing sequence, reinforcement schedules, prompting hierarchies (physical → gestural → verbal → independent), and generalization programming across environments and caregivers.
Special Education (Support Layer)
SpEd providers implement visual sequence supports, maintain nose-blowing visual schedules in classrooms, support generalization in school environments, and coordinate with home programs for consistency.
"The brain doesn't organize development by therapy type. Neither should we." — Pinnacle GPT-OS® FusionModule™ Principle

Nine Materials. Five Target Domains. One Cascade of Independence.
Primary Target
Nasal Airflow Control: The child learns to consciously direct exhaled air through the nasal passages rather than the oral cavity. Observable indicator: Can move a feather placed 5cm from nose by exhaling through nose with mouth closed.
Secondary Targets
- Breath Control: Builds respiratory pressure and controlled exhalation — the engine behind effective nose blowing
- Oral-Motor Function: Strengthens velopharyngeal control, lip closure, and coordinated mouth-nose differentiation
- Sensory Tolerance: Reduces aversion to tissue texture, mucus sensation, and facial touch
Tertiary Targets (Long-Term)
Independent respiratory hygiene — no longer requiring adult wiping
Improved nasal breathing, taste, smell, and sleep quality
School participation without embarrassment from visible congestion
Foundation skills for whistles, straws, bubbles, and oral-motor speech tasks

Material 1: Feather / Cotton Ball
🪶 Nasal Airflow Biofeedback
Canon: Biofeedback Instruments
₹20–100

What It Does
Provides immediate visual feedback — when placed on a table 5cm from the nose, it moves when the child successfully exhales through their nose. Teaches the foundational concept: air can come out through the nose on purpose.
Why It Works
Children with motor planning difficulties cannot learn from verbal instruction alone. A moving feather makes invisible nasal airflow suddenly visible, creating the internal body map the child needs.
How to Use
- Place feather/cotton ball on table
- Child closes mouth (gently hold lips together initially)
- Child exhales through nose to move the item
- Start 2cm away; increase distance as control improves
DIY ₹0: Cotton from first aid kit. Tissue paper strip. Small pom-pom from craft box.
Need guidance on which materials to start with for your child's specific profile? FREE: 9100 181 181

Material 2: Nose Flute
🎵 Auditory Feedback Instrument
Canon: Breath Control Materials
₹100–400
What It Does
Makes musical sound only when air flows through the nose. Immediate, unambiguous auditory feedback — if it plays, the child is doing it correctly. The feedback is binary: sound or silence.
Why It Works
Gamifies the skill. Children who cannot grasp "blow through your nose" as an abstract instruction can grasp "make the nose flute play" as a concrete, motivating goal.
How to Use
- Position larger opening over nose, smaller opening near (closed) mouth
- Child exhales through nose to make sound
- Celebrate every successful note
- Individual use only — hygiene essential
DIY ₹0: Straw held at nostril end, other end in cup of water — bubbles = nasal airflow.

Material 3: Small Mirror
🪞 Visual Biofeedback
Canon: Biofeedback Instruments / Visual Supports
₹50–200
What It Does
Fogs when child exhales through nose. Clear mirror = air went through mouth. Fogged mirror = success. Child monitors themselves without adult correction.
Why It Works
Self-monitoring is more powerful than external feedback. The mirror provides immediate, objective, non-judgmental feedback. The child corrects themselves based on fog alone — no adult commentary needed.

How to Use
- Hold mirror under nose (between nose and upper lip)
- Child closes mouth and exhales
- Watch for fogging
- Metal spoon works equally well
DIY ₹0: Metal soup spoon. Tile or glass surface. Safety note: Use unbreakable plastic mirrors with children under 6.

Material 4: Nasal Bubble Set
🫧 Fun Breath Control Practice
Canon: Breath Control Materials
₹50–200

What It Does
Modified bubble-blowing through nose with a tube/straw at nostril entrance. If bubbles form, nasal airflow is active. Breath control practice disguised as play.
Why It Works
Bubble-blowing is universally motivating. The nasal adaptation forces the same motor pattern as nose blowing but removes the social pressure and sensory context of tissue use, making it a low-stakes, high-reward practice.
How to Use
- Position straw/flexible tube at nostril opening (not inside)
- Other end placed in bubble solution
- Child closes mouth and exhales through nose
- Practice single nostril initially
DIY ₹0: Dish soap + water. Straw from kitchen.
Material 5: Pinwheel
🌀 Sustained Airflow Training
Canon: Breath Control Materials
₹30–100
What It Does
Requires sustained nasal exhalation to keep spinning. Builds both the concept of nasal airflow and the breath strength required for effective mucus clearance.
Why It Works
Moving a feather shows airflow exists. Spinning a pinwheel builds the force and duration of airflow — the "dosage" needed for actual nose blowing. Pinwheels create measurable progress: spin time increases as breath strength develops.
How to Use
- Child blows through nose to spin pinwheel
- Start close, increase distance gradually
- Time the spin — creates measurable, motivating progress tracking
DIY ₹0: Paper pinwheel from craft paper (5-minute construction).


Material 6: One-Nostril Trainer
🔧 Task Simplification Tool
Canon: Motor Planning Supports
₹100–400 or ₹0
What It Does
Gently occludes one nostril, directing all airflow through a single passage. Reduces cognitive load and physical complexity — the child focuses on one airway at a time.
Why It Works
Blowing through both nostrils simultaneously doubles the coordination demand. One-nostril training is also how effective adult nose blowing is actually performed. Teaching the correct technique from the start creates the right habit immediately.

How to Use
- Parent's finger gently closes one nostril
- Child closes mouth and blows through open nostril
- Alternate sides
- Teach child to self-occlude progressively over sessions
DIY ₹0: Parent's finger. Teach child to use their own finger — this is the ultimate independence goal anyway.

Material 7: Ultra-Soft / Lotion Tissues
🤍 Sensory Barrier Removal
Canon: Sensory-Friendly Materials
₹100–400

What It Does
Eliminates the sensory aversion to standard tissues that blocks many children from even attempting nose blowing. Soft, lotion-infused, or cloth alternatives remove the tactile barrier so the child can focus entirely on the motor skill.
Why It Works
If the tissue itself is aversive, no amount of technique training succeeds. Sensory profiling the tissue texture is clinical work, not preference indulgence. Alternatives include ultra-soft lotion brands, silk handkerchiefs, or warm damp washcloths.
How to Use
- Trial various textures systematically
- Stock the tolerated type exclusively for practice and daily use
- Never reintroduce a rejected texture during active skill building
DIY ₹0: Warm damp soft washcloth. Silk or satin handkerchief from existing wardrobe.

Material 8: Visual Sequence Cards
📋 Motor Planning Support
Canon: Visual Supports / Communication Boards
₹100–300
What It Does
Breaks nose blowing into 5–7 discrete, illustrated steps. Child references the visual during practice, reducing reliance on verbal instruction and providing consistency across all caregivers.
Why It Works
What appears to be one action — "blow your nose" — is actually 7 sequential steps. Children with motor planning or language processing differences learn sequences through pictures, not words. Visual supports are classified as evidence-based practice by NCAEP (2020).
The 7 Steps Shown on Cards
Take tissue
Hold to nose
Close mouth
Push air out nose
Wipe nose
Dispose tissue
Wash hands
DIY ₹0 (Most Effective Version): Phone photos of your child performing each step, printed and laminated. Free PECS-style visuals also available from AAC resources.
Material 9: Nasal Saline Spray
💧 Congestion Relief + Nasal Awareness
Canon: Medical Supplies / Hygiene Tools
₹100–300
What It Does
Thins thick mucus (making blowing physically possible) and provides nasal sensation that increases body awareness of the nasal passages. Builds confidence through early success experiences.
Why It Works
If mucus is too thick to expel, even perfect technique fails. Thinned mucus enables early successes that build the child's confidence and self-efficacy for the skill — essential for motivation to continue.
How to Use
- Use commercial pediatric saline spray (OTC, no prescription required)
- Apply 2–3 minutes before every practice session
- DIY: ¼ tsp non-iodized salt in 240ml distilled water
DIY ₹0: ¼ tsp salt + 1 cup boiled, cooled distilled water. Use a nasal dropper for application. Always use sterile or boiled water for homemade saline — commercial OTC saline is preferred.

Every Material Has a ₹0 Household Substitute
Every family can start today. This is the WHO/UNICEF inclusion principle in practice — no material should ever be a barrier to your child's development.
Material | Commercial Version | ₹0 Substitute | Same Principle |
Nasal Airflow Feedback | Craft feathers (₹20–100) | Cotton from first aid kit, tissue paper strip | Visual biofeedback of nasal exhalation |
Auditory Feedback | Nose flute (₹100–400) | Straw in cup of water at nostril — bubbles = nasal airflow | Auditory/visual biofeedback |
Visual Biofeedback | Small mirror (₹50–200) | Metal soup spoon, any glass or tile surface | Fog/condensation = nasal airflow |
Breath Bubbles | Bubble set (₹50–200) | Dish soap + water + kitchen straw | Motivating nasal breath feedback |
Breath Strength | Pinwheel (₹30–100) | Paper pinwheel made in 5 minutes | Sustained airflow training |
Nostril Occlusion | Commercial trainer (₹100–400) | Parent's finger → teach child's own finger | Task simplification technique |
Sensory-Friendly Tissue | Lotion tissues (₹100–400) | Warm damp soft washcloth | Sensory barrier reduction |
Visual Sequence | Printed cards (₹100–300) | Phone photos printed at pharmacy | Motor sequence visual support |
Saline | Commercial spray (₹100–300) | ¼ tsp salt in 1 cup boiled cooled water + nasal dropper | Mucus thinning, nasal awareness |
₹0 Version
Cotton from first aid box + metal spoon + damp washcloth → Begin today
₹100 Version
Add craft feathers + bubble solution + pinwheel
Complete Kit
All 9 materials for ₹550–2,000
Safety First: Read Before Starting
Safety is clinical, not optional. Review this traffic light system before every session.
🔴 DO NOT PROCEED IF:
- Child has active nasal infection or sinusitis — seek medical care first
- Ear infection or recent ear surgery — pressure changes affect middle ear
- Child becomes severely distressed, vomits, or shows respiratory distress — stop immediately
- Structural nasal obstruction suspected (chronic mouth breathing, no visible nasal airflow at rest) — medical evaluation first
🟡 MODIFY IF:
- Child is unwell, tired, or dysregulated — shorten to 2–3 minutes maximum
- High sensory sensitivity today — feather on table and mirror only; no tissue contact
- Seasonal allergies during peak season — saline before every session
- Child is congested but not infected — saline first, brief session, stop if distressing
🟢 SAFE TO PROCEED IF:
- Child is well, rested, and in a regulated state
- No active infection or medical contraindication
- Materials are appropriate for age and size (no choking hazards under age 3)
STOP IMMEDIATELY IF CHILD SHOWS: Excessive coughing | Choking | Nosebleed | Severe distress | Facial pain | Signs of ear pain. Emergency guidance: 9100 181 181

Set Up Your Space
The right environment is 50% of the session's success. Spatial precision prevents 80% of session failures before they begin.
Environment Checklist
Quiet space — no TV, no siblings practicing simultaneously
Bright enough to see mirror fogging clearly (natural light or bright LED)
Tissue/waste bin within child's reach — they dispose independently
All materials set out before child arrives — no searching mid-session
Visual sequence card at eye level, 30–45cm from child's natural gaze
Child Position
Seated at table or bathroom counter — head level, not tilted
Parent beside child, not across — side positioning is less confrontational
Feet flat on floor or footrest for postural stability during breath work
Session Duration Guidelines
Weeks 1–2
3–5 minutes per session while tolerance and skill are building
Weeks 3–6
5–10 minutes as child settles into the routine
Ongoing
Daily brief practice always outperforms infrequent long sessions
Remove from Space
- Screens and devices (except for video modeling use)
- Distracting toys not part of the session
- Scented products that may trigger nasal sensitivity
Is Your Child Ready? Pre-Session Readiness Check
60 seconds before you begin. The readiness check that prevents 90% of difficult sessions.
Indicator | ✅ Green — Full Session | 🟡 Modify | 🔴 Postpone |
Has the child eaten recently? | Yes, 2+ hours ago | Snack 15 min ago | Hungry or just ate large meal |
Sleep quality last night? | Rested | Slightly tired | Overtired or sleep-deprived |
Emotional state right now? | Calm and alert | Mildly activated | Distressed or mid-meltdown |
Any current illness? | Well | Mild congestion (good for practice) | Active infection |
Sensory state today? | Regulated | Mild sensitivity | High sensory sensitivity day |
Recent meltdown? | No | 30–60 min ago | Under 30 min ago |
Willingness cue? | Approaches materials | Neutral/uncertain | Active refusal |
5–7 Green
Full session, all materials
3–4 Green + Some Yellow
Shortened 3-minute session, use only preferred materials
Majority Red
Postpone. Offer a preferred calm activity instead.
Postpone Phrase: "Today we're going to do [preferred activity] instead. We'll do our nose practice tomorrow." The best session is one that starts right.
Step 1: The Invitation
Step 01 of 06
Duration: 30–60 seconds
Clinical Purpose
Establish a motivating operation — engage the child's curiosity and willingness before any demand is placed. No tissue visible yet. Do not introduce the nose-blow concept directly.
"Hey, I want to show you something cool. Look at this feather. Want to see if you can make it move without touching it? Just with your breath?"
Body Language Guidance
- Kneel or sit at child's eye level
- Hold material at child's eye height, slightly below nose level
- Demonstrate first — blow through your own mouth to move the item
- Keep expression playful, not clinical
Acceptance Cues (Watch For)
✅ Child reaches toward material or leans forward
✅ Child looks at parent's face with curiosity
✅ Child smiles or vocalizes interest
Resistance Cues and Response
🟡 Child looks away → Move material to their visual field, increase animation
🟡 Child says "no" → "Okay, I'll try and you watch me first"
🔴 Child pushes material away → This is a Postpone signal. Switch to preferred activity.


Step 2: The Engagement
Step 02 of 06
Duration: 1–3 minutes
Introduce nasal airflow concept through the preferred feedback material. First success experience. Deliver verbal praise within 2 seconds of any nasal exhalation.
🪶 With Feather / Cotton Ball
"Now try with just your nose. Close your lips like this. Push air out through your nose." → Child attempt #1: Praise any movement of item, even slight → If no movement: gently hold child's lips together. Try again. → Celebrate each near-success
🪞 With Mirror
"Hold this under your nose. Can you make it foggy? Close your lips and blow out your nose." → Show child your own fog demonstration first → Any fogging = immediate praise
🎵 With Nose Flute
"This is a special nose instrument. It only makes music when you use your nose." → Demonstrate your own nose flute sound → Let child feel vibration before attempting
Response | What It Means | Action |
Moves feather / fogs mirror / produces nose flute sound | Ideal first attempt | Celebrate immediately; proceed to more reps |
Partial movement, intermittent success | Acceptable — skill emerging | Continue; don't adjust method yet |
Complete absence of nasal airflow after 5+ attempts | Needs clinical review | Note for therapist; do not force |

Step 3: The Therapeutic Action
Step 03 of 06
Duration: 3–7 minutes (core of session)
The core skill-building event — progressing from biofeedback awareness to controlled nasal exhalation into a tissue. Use the stage appropriate for your child today.
Stage A — No Awareness Yet
Feather/cotton ball 3cm from nose. Child exhales: feather moves = success. Mirror fogs = success. Repeat 3–5 times. Do NOT rush to tissues. This may be today's entire session.
Stage B — Emerging Awareness
Feather/mirror success achieved consistently. Introduce pinwheel: "Can you keep it spinning?" Introduce nose flute: "Can you make it sing?" 3–5 repetitions of preferred feedback tool.
Stage C — Developing Control
Parent gently closes one nostril. Tissue held by parent at open nostril. Child exhales through open nostril into tissue. Acknowledge any mucus clearance as major success. 2–3 repetitions per nostril.
Stage D — Building Independence
Child holds tissue themselves. Child self-occludes one nostril. Parent provides only verbal prompt: "One nostril, close your mouth, push air out." Fade prompts over successive sessions.
Common Error | Why It Happens | Correction | Tool |
Sniffs inward | Default inhalation reflex | Tap nose, move hand outward: "Push OUT" | Physical cue |
Mouth falls open | Soft palate not closing | Gently press lips together briefly to reset | Lip prompt |
Blows through mouth | Air takes path of least resistance | Nose flute forces nasal-only airflow | Nose flute |
No force/pressure | Insufficient breath pressure | Pinwheel practice to build respiratory strength | Pinwheel |
Step 4: Repeat and Vary
Step 04 of 06
Duration: 3–5 minutes
Core Principle: 3 Good Reps > 10 Forced Reps. A child who successfully exhales through their nose 3 times with genuine engagement has achieved more therapeutic value than one who grudgingly attempts 10.
Target Repetitions by Stage
Stage A
3–5 reps — awareness building
Stage B
5–8 reps — breath control
Stage C
4–6 reps — 2–3 per side
Stage D
2–4 reps — independence, not volume
Variation Options to Maintain Engagement
Variation | When to Use |
Feather → Mirror → Nose Flute rotation | When child starts disengaging with one material |
Blow a feather across a finish line | For children who respond to challenges and competition |
Musical nose flute session | High-resistance days — pure play disguising pure therapy |
Saline + feather sequence | Congested days or discouragement |
Parent competes (and loses) | Anxious, perfectionistic children who fear failure |
Satiation Indicators — Session Is Complete
- Child pushes materials away
- Attention diverts and cannot be redirected
- Quality of attempts deteriorating
- Child asks to stop

Step 5: Reinforce and Celebrate
Step 05 of 06
ABA / BCBA Lead
Timing matters more than magnitude. Reinforcement delivered within 3 seconds of the target behavior is 4× more effective than delayed praise.
For nasal exhalation (any stage)
"YES! That was air through your nose! I saw it move!"
For fog on mirror
"Look at that fog! That's YOUR nose breathing!"
For nose flute sound
"You made music with your nose! That's incredible!"
For Stage D independence
"You did it all yourself. You are a nose-blowing champion."
Celebrate the attempt, not just the success: Even a child who tried and produced no visible result receives: "I saw you try so hard. That trying is how the skill grows. Let's try once more."
Reinforcement Menu
Social Reinforcement
High five, fist bump, enthusiastic praise — primary for most children at all stages
Token Economy
Sticker chart — 5 successful nose breaths = sticker; structured tracking for children who need tangible progress
Natural Consequence
"Now your nose feels clear!" — use after successful mucus clearance for authentic reinforcement
Building a home reinforcement system? Our therapists can help personalize it. FREE: 9100 181 181

Step 6: The Cool-Down
Step 06 of 06
Duration: 2–3 minutes
The Rule: No session ends abruptly. Every session has a cool-down transition. A deliberate cool-down anchors the session as a positive experience the child will want to return to tomorrow.
Cool-Down Scripts
"Two more tries, then we're all done with our nose practice."
"Now let's just take three big slow breaths through your mouth. In...and out. In...and out."
"Great work! Now we're going to [preferred next activity]."
If Child Resists Ending
"I know you want to keep going — that means you did great! We'll do more tomorrow. [Preferred activity] is next." Do not extend session past natural endpoint to "get more reps." Quality over quantity.
Visual Timer Option
A sand timer or visual countdown app placed visibly before the session begins prevents resistance to ending. The child sees time running out — not the parent ending arbitrarily. This is especially powerful for children with transition difficulties.
Why the Material Put-Away Ritual Matters
Child participates in putting materials away — feather in box, pinwheel on shelf, tissues in holder. This is a dignified, self-directed conclusion that builds ownership and routine. It also signals "this is a real skill activity" — not just a game that gets abandoned.
Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Parents who capture even minimal data consistently see the fastest progress — because data capture keeps you engaged, reflective, and consistent.
3 Data Points to Record
1
Nasal Airflow
Did child produce nasal exhalation? (Yes / Partial / No)
2
Stage Reached
A (awareness) / B (breath control) / C (one nostril + tissue) / D (independent)
3
Session Quality
1 (refused) → 3 (mixed success) → 5 (breakthrough moment)
What This Data Does
Feeds into GPT-OS® Respiratory Hygiene Readiness Index and Self-Care Readiness Index
After 14 sessions: algorithm identifies your child's progress pattern and adapts recommendations
After 28 sessions: system projects readiness milestones and next-step guidance
What If It Didn't Go As Planned?
Most sessions won't be perfect. Here's your fix for every common challenge. Session abandonment is not failure — it is data.
Child sniffs inward every time
Why: Inhalation is the unconscious default — the concept of pushing air out through the nose is genuinely novel. Fix: Return to Step 1. Use mouth blowing first (blow feather with mouth). Then block mouth and redirect. Use nose flute — it cannot sound with inhalation.
Child blows entirely through mouth
Why: Soft palate is not closing to redirect air to nasal passage. Fix: Nose flute is the immediate intervention — it physically requires nasal airflow. Also: gently hold child's lips pressed together; the only exit route becomes the nose.
Zero nasal airflow after multiple sessions
Why: Could be structural (adenoids, deviated septum), severe motor planning deficit, or profound sensory aversion. Fix: Clinical referral indicator. Contact Pinnacle OT or SLP. ENT evaluation if structural concern suspected.
Child fogs mirror but refuses tissue
Why: Tissue introduces sensory and social complexity that disrupts the motor skill. Fix: Separate sensory desensitization from motor training. Practice tissue tolerance completely separately. Only combine when both are stable.
Skill regression after initial progress
Why: Normal in neurodevelopmental skill acquisition — often follows illness, stress, or environmental change. Fix: Return to the previous successful stage without expressing frustration. "Your brain is just resting. Let's go back to the fun stuff." Regression does not erase learning.
Session abandoned due to meltdown
Why: Child was not ready — readiness check was missed or overridden. Fix: No recovery attempt same day. Next session: check readiness rigorously, shorten dramatically, start with the most preferred material only.
Adapt and Personalize
No two children are identical. Here is how to make this technique exactly right for yours.
🔴 Sensory Avoider
- Begin with no facial touch — feather on table only
- Introduce mirror only when stable, held by child
- Delay tissue introduction until Stages A and B are fully mastered
- Cotton gloves for child to hold tissue if hand sensitivity co-occurs
🟢 Sensory Seeker
- More intense feedback preferred — pinwheel over feather
- Saline spray first (nasal sensation motivating)
- Faster progression through stages acceptable
- Add challenges: increasing feather distance, longer nose flute songs
🧠 Motor Planning Difficulty
- Heavy use of visual sequence cards at every session
- Hand-over-hand guidance for tissue holding initially
- Explicit narration as each action is performed
- Video model of peer performing nose blowing (NCAEP: evidence-based)
🗣️ Communication Differences
- Replace verbal scripts with visual + gesture cues
- Use PECS symbols if AAC is established communication mode
- "Air out" paired with outward arrow gesture
- Less language during session; more visual + tactile feedback
Age Adaptations
Ages 3–5
Max 3 minutes. One material only. All play-framing.
Ages 6–8
5–7 minutes. Multiple materials. Game framing ("beat your record").
Ages 9–12
7–10 minutes. Adolescent-dignity framing. Full independence focus.

Weeks 1–2: What to Expect
Progress Phase 1 of 4
You Are Here
In Weeks 1–2, here is what real progress looks like. Measure tolerance and attempts, not mastery.
✅ These ARE Progress at Weeks 1–2
Child allows materials near face without immediate refusal
Child attempts nasal exhalation at least once per session, even if unsuccessful
Feather moves slightly OR mirror shows faint fogging on at least 1 attempt
Session length tolerated has increased from Day 1
Child references the activity voluntarily ("Can we do the feather thing?")
❌ NOT Expected Yet (Normal, Not Alarming)
Full nose blowing into tissue — too early
Consistent nasal airflow on every attempt — still developing
Child requesting to blow nose in real situations — weeks away
Parent Calibration: If your child tolerated the feather activity for 3 minutes and produced ONE nasal exhalation — that is Week 1 success. Celebrate it exactly as it is.
Weeks 3–4: Consolidation Signs
Progress Phase 2 of 4
By Weeks 3–4, neural pathways are forming. Watch for these specific signs that the skill is beginning to wire itself in.
✅ Consolidation Indicators
- Child anticipates activity — knows what comes when materials appear
- Nasal exhalation produces feather/cotton ball movement on 50%+ of attempts
- Mirror fogging consistent — child self-monitors with visible satisfaction
- Child begins to self-occlude one nostril when prompted
- Resistance to starting sessions has decreased significantly
- Parent reports child's nose feels clearer after sessions
🧠 Behavioral Signs of Neural Pathway Formation
- Child corrects themselves mid-attempt: "Wait, through my nose"
- Child asks to try the nose flute again after initial success
- Spontaneous nasal exhalation attempts outside of sessions (blowing at dust, cooling food)
These are generalization seeds — celebrate them as the significant milestones they are.
"You may notice you're more confident in the sessions now too. Your timing is better. Your scripts feel natural. Your child's nervous system is not the only one that learned something." — Pinnacle OT Team
When to Increase Intensity: If child is consistently successful at Stage B (feather + mirror + breath control) for 3+ consecutive sessions, begin Stage C (one nostril + tissue).

Weeks 5–8: Mastery Indicators
Progress Phase 3–4 of 4
🏆 Mastery Milestone
97%
Measured Improvement
Across Respiratory Hygiene Readiness Index for children receiving structured instruction
70%
Generalize by Week 8
Children who reach Stage D mastery demonstrate skill in 2+ settings
5+
Settings for Mastery
Confirmed mastery requires independent performance across consecutive days in multiple environments
Mastery Criteria — Specific, Observable, Measurable
✅ Child independently picks up tissue when nose is running (without prompt)
✅ Closes mouth, occludes one nostril, and exhales into tissue
✅ Disposes of tissue and washes hands as an integrated sequence
✅ Performs skill in at least 2 settings (home + school or home + grandparents')
✅ 3 consecutive sessions with Stage D (full independent) performance
Celebrate This Win
You did this. Your child grew because of your commitment.
Your child arrived at this page unable to blow their nose. You spent 5–8 weeks with feathers, mirrors, nose flutes, and tissues. You executed a structured, evidence-based protocol across dozens of sessions. You adapted when it didn't work. You persisted when it felt impossible. And now your child's nose is clear.
What actually happened in those weeks: A motor sequence requiring 5-system neural coordination — velopharyngeal control, motor planning, interoception, breath control, and sensory tolerance — was systematically built from nothing. That is not a small achievement. That is neurodevelopmental engineering performed by a parent.
Create a Champion Card
Make a "Nose Blowing Champion" certificate for your child. Let them choose tonight's dinner. Call the grandparents.
Capture the Moment
Photograph this milestone. "Today [child's name] blew their nose independently for the first time. They looked so proud."
Share Your Story
Your journey helps another family. Share your milestone in the Pinnacle Parent Community — someone else is at Card 1 right now and needs to know it's possible.

Red Flags: When to Pause and Consult
Even in progress, these specific signs mean pause and contact a professional. Trust your instincts — if something feels wrong, not just difficult, pause and ask.
Red Flag | What It Looks Like | Why It Matters | Action |
Zero nasal airflow after 4+ weeks of daily practice | No feather movement, no mirror fogging despite consistent effort | May indicate structural issue (adenoids, deviated septum) | ENT evaluation |
Nosebleeds during or after practice | Blood from nostril during sessions | Thin mucous membranes; practice may be too forceful | Stop practice; consult pediatrician |
Ear pain during sessions | Child holds ear, winces during nose blowing | Eustachian tube pressure changes | ENT evaluation |
Chronic mouth breathing not improving | Child still mouth-breathes 24/7 despite demonstrated nasal capacity | May indicate adenoid enlargement | ENT evaluation |
Repeated respiratory infections | More than 4 respiratory infections per year | Underlying immunological or structural concern | Pediatrician evaluation |
Severe distress at ALL sessions despite extended desensitization | Sessions consistently trigger meltdowns; no adaptation helps | May indicate severe sensory processing disorder requiring specialist | OT sensory specialist |
Escalation Pathway: Concern noted → Teleconsult with Pinnacle OT/SLP (24–48 hrs) → Clinic visit assessment → ENT/Pediatrician referral if needed
PINNACLE HELPLINE: 9100 181 181 — available in 16+ languages, 24×7

The Progression Pathway
Nose blowing mastered. Here is where the journey continues.
Readiness Gate for E-540
Before proceeding to E-540 (General Hygiene Independence): Child must independently blow nose in 3+ different settings across 5+ consecutive days without structured prompting.
Long-Term Goal This Feeds
Self-Care Independence Readiness Index — the cluster of skills enabling a child to manage their own hygiene without adult assistance. A core prerequisite for school inclusion, social confidence, and independent living preparation.

Related Techniques in This Domain
Materials you already gathered for E-539 work for these techniques too — your investment in this kit transfers directly.

E-538: Coughing Into Elbow
🟢 Intro Difficulty | Visual sequence cards overlap directly

E-537: Handkerchief Use
🟢 Intro Difficulty | Soft tissues from E-539 transfer directly

E-520: Oral-Motor Development
🟡 Core Difficulty | All breath control materials overlap

E-545: Breath Control Activities
🟡 Core Difficulty | Feathers and pinwheels transfer directly

Families Who've Been Here
These families started exactly where you are. Both narratives are illustrative composites; individual outcomes vary.
Arjun, Age 8 — Hyderabad Center
Before: "Arjun was 8 and still couldn't blow his nose. Teachers were sending notes. He was embarrassed at school — he could feel that other kids noticed. I had tried everything: videos, demonstrations, games. Nothing worked."
Turning point: "The OT started with a feather on the table. No tissue, no nose, no pressure. Just: 'Can you make this move?' He thought it was a game. Two weeks later — the mirror. Three weeks after that — one nostril and tissue. He started practicing voluntarily."
After: "Four months later, he blows his nose independently whenever he needs to. He carries tissues himself. He looks proud every time. What felt impossible became automatic with the right sequence."
Priya, Age 6 — Bengaluru Center
Before: "My daughter has sensory processing difficulties. Tissues were a complete no — she'd cry if one touched her face. We gave up on nose blowing entirely. Her chronic congestion meant she was mouth-breathing all the time and wasn't sleeping well."
Turning point: "The OT told me not to mix the sensory work with the motor work. Separate problems, separate solutions. Two weeks on tissue textures near her face — zero pressure to blow. Meanwhile, feathers and nose flute for the airflow practice."
After: "When both were stable, we combined them. She has a specific lotion tissue she accepts completely. Nose blowing followed naturally once the sensory barrier was gone."
"The most common reason nose-blowing instruction fails is that parents try to teach the full skill before the foundational awareness is established. You cannot blow your nose if you don't know nasal airflow is something you can control. The feather is not a toy. It is the first lesson." — Pinnacle OT Specialist, 12 years clinical experience

Frequently Asked Questions
Questions every parent asks. Answers from the consortium.
My child is 10. Is it too late to learn nose blowing?
No. Structured teaching successfully establishes the skill at any age through childhood and adolescence. The approach for a 10-year-old emphasizes dignity, autonomy, and framing the skill as a life skill rather than a baby activity. The neural plasticity required is present well into teenage years and beyond.
We've tried everything for months. Is this approach actually different?
Most prior approaches fail because they attempt to teach the final skill (blow into tissue) before the foundational skill (conscious nasal exhalation) is established. Start at Stage A regardless of the child's age — can your child move a feather with nasal airflow? That is your starting point.
How do I know if this is sensory vs. motor planning?
If the child can fog a mirror (nasal airflow present) but refuses tissues → primary sensory barrier. If the child cannot fog a mirror despite trying → primary motor planning/awareness issue. Most children have both components — the approach addresses both in parallel.
My child doesn't understand any instruction. How do I start?
Start entirely non-verbally. Sit beside your child, hold a feather in front of your own nose, exhale to move it — repeat several times. Pass the feather. Use physical guidance to position near their nose. Celebrate any nasal airflow, however accidental. Build from observation and imitation, not verbal instruction.
Can I practice during real congestion or only when nose is clear?
Both, with different purposes. Practice sessions during clear periods build the motor skill without complexity. Real-congestion moments are the generalization targets — use saline first, then the learned skill in context. Both are necessary for full functional independence.
How long until full independence?
Without significant barriers: typically 6–12 weeks of daily practice from Stage A to Stage D mastery. For children with significant developmental differences: 3–6 months is realistic. Progress is non-linear — expect plateaus and mini-regressions as normal parts of the journey.
School isn't cooperating with our home program. What do I do?
Download the school communication template (Card 40). The school's role is minimal: tissues accessible, brief prompt if congested, no wiping unless necessary. The school does not need to run sessions — just not undermine the home program.
Is this safe for children with tube feeds or tracheostomies?
No — do not attempt nose-blowing or nasal pressure training for children with tracheostomies, nasogastric tubes, or significant respiratory conditions without explicit clearance from the treating medical team. Contact a Pinnacle NeuroDev Pediatrician: 9100 181 181.
Preview of 9 materials that help with nose blowing Therapy Material
Below is a visual preview of 9 materials that help with nose blowing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

Your Child Can Learn This Skill. Start Today.
You arrived at this page scared and exhausted, wiping a running nose for the hundredth time. You leave having everything you need to teach your child one of life's foundational independence skills. The feather is waiting. The journey begins now.
🦾 Occupational Therapy
🗣️ Speech-Language Pathology
🧠 ABA / BCBA
📚 Special Education
🩺 NeuroDev Pediatrics
🌸Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. Powered by GPT-OS® Therapy Intelligence. | "From fear to mastery. One technique at a time."
20M+ 1:1 Sessions | 97%+ Measured Improvement | 70+ Centers | Patents Filed Across 160+ Countries | techniques.pinnacleblooms.org
FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | pinnacleblooms.org
20M+ 1:1 Sessions | 97%+ Measured Improvement | 70+ Centers | Patents Filed Across 160+ Countries | techniques.pinnacleblooms.org
FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | pinnacleblooms.org
This content is educational in nature. It does not replace individualized assessment and intervention planning with licensed occupational therapists, speech-language pathologists, and healthcare professionals. Persistent difficulty with nose blowing may indicate underlying developmental, motor, respiratory, or structural conditions requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®. Illustrative narratives are composites; outcomes vary by child profile, underlying needs, and intervention intensity.
© 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Powered by GPT-OS®. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2