

"You are not failing. Your child is not broken. The environment is missing the right scaffolding. These 9 materials are that scaffolding." — Pinnacle Blooms Consortium, Community Access Division
- Sensory overload isn't "being difficult." It's the nervous system reaching maximum capacity and triggering a protective response.
- Meltdowns in public aren't manipulation. They are the system crashing — exactly as any computer crashes when processing capacity is exceeded.
- Social withdrawal at gatherings isn't rudeness. It's the child's only available regulation strategy when no other tools exist.
- The good news: The brain is extraordinarily plastic. With the right supports, neural pathways for community participation can be built, strengthened, and made automatic over time.
"This is a wiring difference, not a behavior choice. Your child isn't resisting — they're surviving." — Pinnacle NeuroDev & OT Consortium

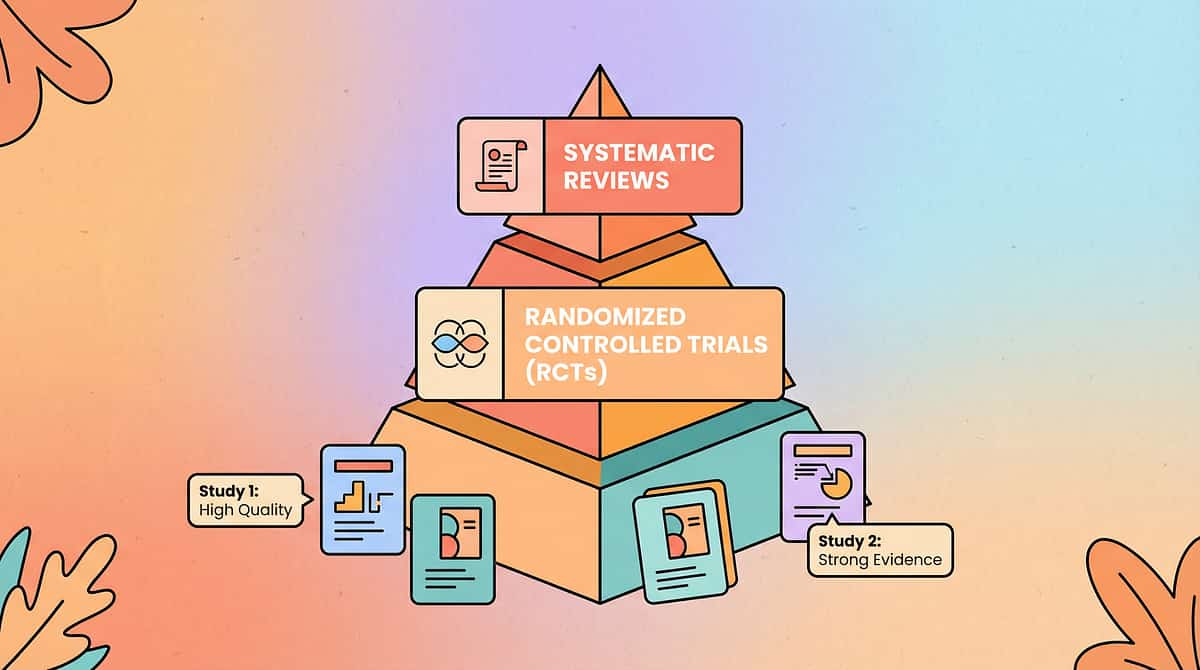
Study | Finding | Source | |
NCAEP Systematic Review (2020) | Social stories, visual supports, and sensory regulation tools are classified as evidence-based practices for autism community participation | NCAEP 2020 | |
Meta-analysis (World J Clin Cases, 2024) | Sensory integration + social skills training effectively promotes community adaptive behavior across 24 studies | PMC10955541 | |
Indian RCT (Padmanabha et al., 2019) | Home-based, parent-implemented sensory and social interventions show significant community participation outcomes in Indian pediatric populations | DOI: 10.1007/s12098-018-2747-4 | |
PRISMA Review (Children, 2024) | 16 studies (2013–2023) confirm sensory-social interventions meet evidence-based practice criteria for ASD | PMC11506176 | |
UN CRPD Article 30 | International legal framework mandating community participation rights for all persons with disabilities — including children | UN, 2006 |
Evidence Grade: A — Systematic Review + Multiple RCTs
"Community inclusion is clinically validated, internationally mandated, and systematically achievable — with the right materials and protocols."


- Ability to access and participate in community environments without meltdown
- Functional communication in community settings (shops, parks, gatherings)
- Sensory regulation in unpredictable multi-sensory public environments
- Social initiation with peers and community members
- Reduced family isolation and increased family community participation
- Anxiety reduction associated with unpredictable environments
- Social rule understanding (unwritten community codes)
- Independence and self-advocacy in public settings
- Long-term quality of life and community belonging
- Peer friendship formation through community exposure
- Cultural participation (religious ceremonies, family events)
- Civic identity and sense of belonging to a broader community
Target Domain | Observable Evidence of Progress | |
Community access | Child tolerates 15-minute park visit without meltdown | |
Communication | Child successfully orders at a shop counter using cards or speech | |
Sensory regulation | Child uses regulation tools proactively in overwhelming environments | |
Social initiation | Child greets a familiar shopkeeper or neighbor independently | |
Reduced anxiety | Child enters a community setting with reduced pre-departure distress |









Material | ₹ Purchased | ₹0 DIY Version | Why It Works the Same | |
Social Stories | Printed books ₹200–800 | Handwritten pages with photos from your phone, stapled into a booklet | The preparation and narrative structure is the active ingredient — not the printing quality | |
Sensory Travel Kit | ₹1,500–5,000 complete | Ziplock bag: cotton balls for ears, ₹50 sunglasses, smooth garden stone, chewy food item, water bottle | Same sensory input principles; the regulation system doesn't grade materials by price | |
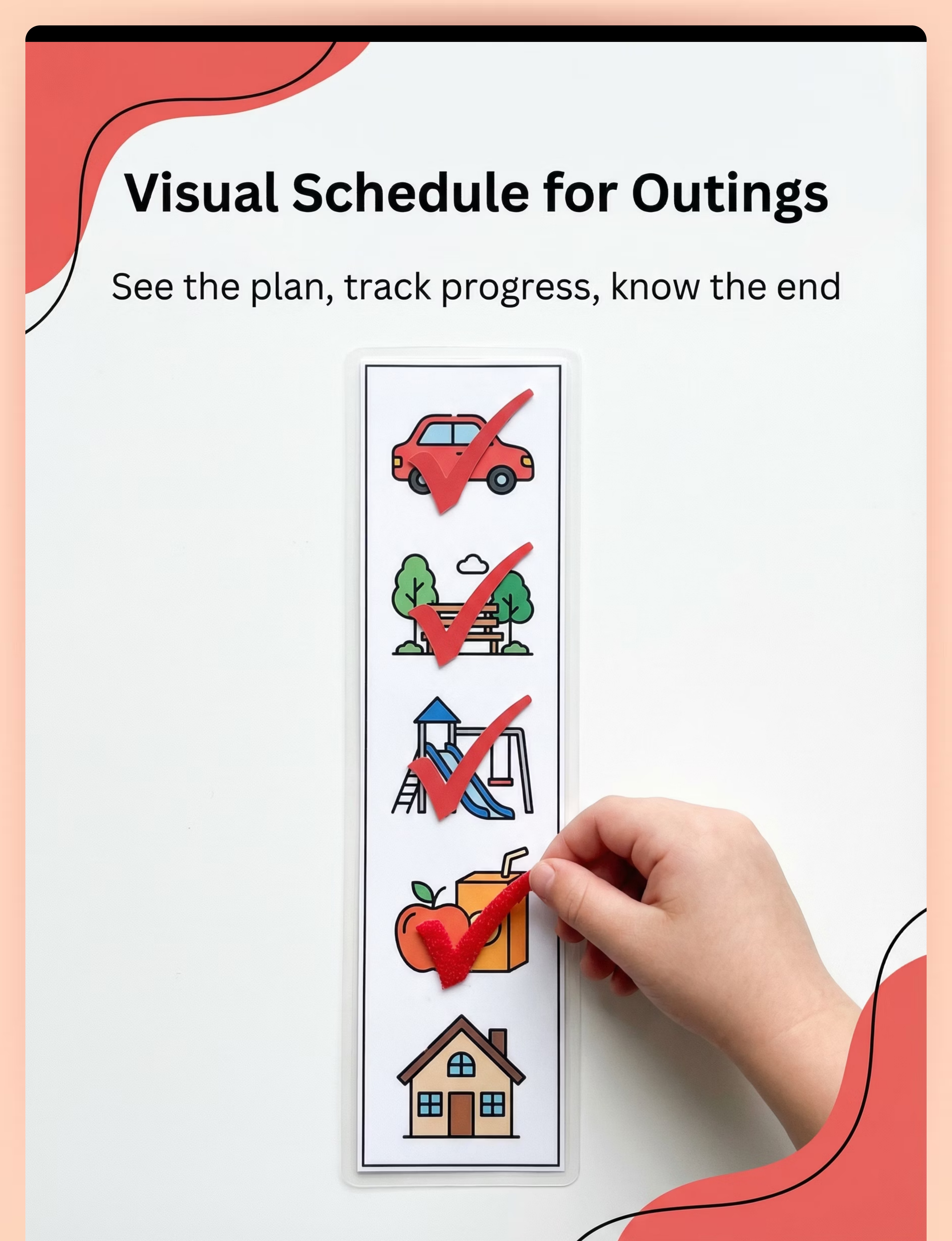
Visual Schedule | Laminated strip ₹100–500 | Index cards with drawn icons in a rubber-banded stack; check off each with a pen | Visibility + sequence + predictability = the mechanism. Paper works. | |
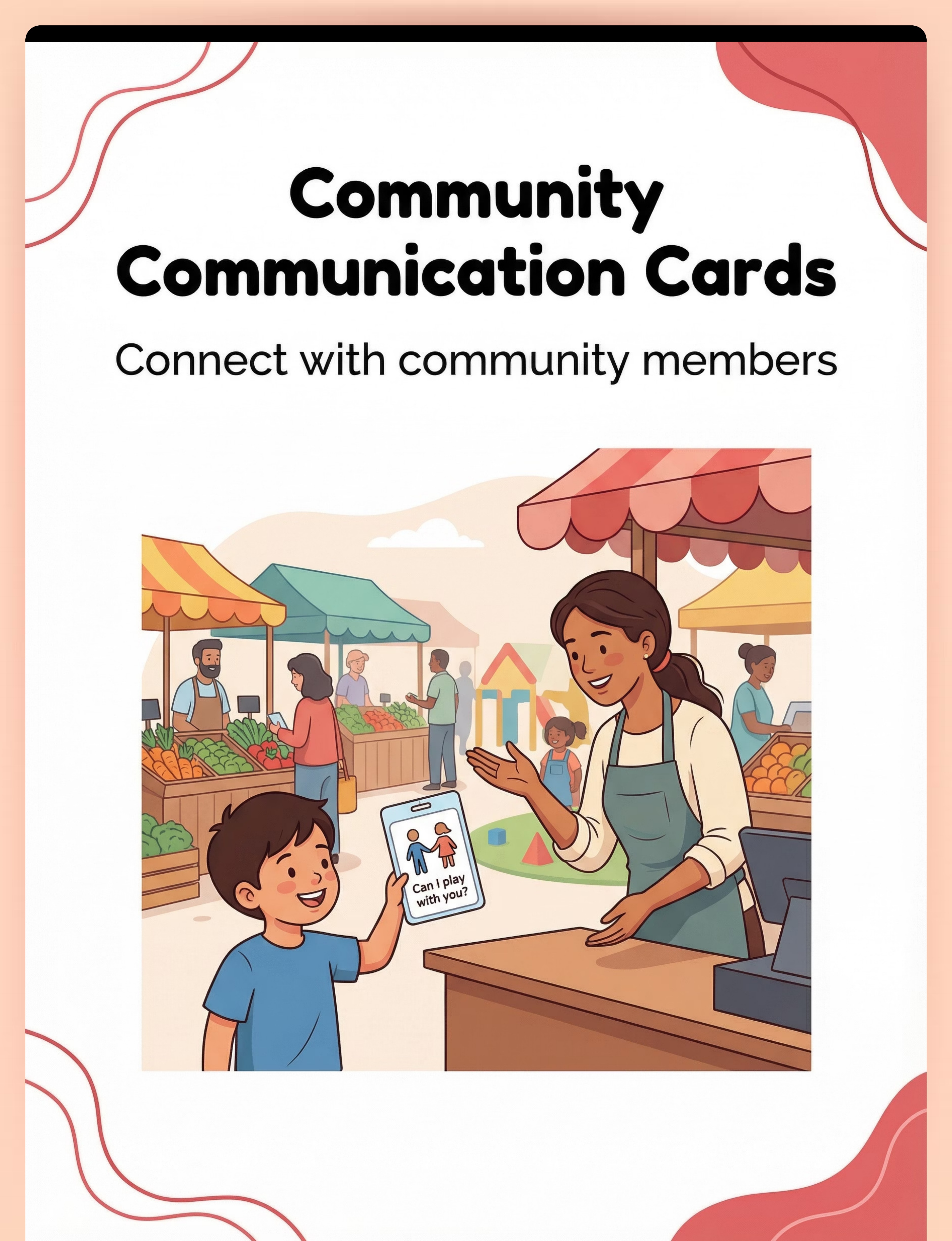
Communication Cards | Printed keyring ₹100–400 | Paper strips in a small notebook; draw pictures + write words | Communication content is the tool; format is secondary | |
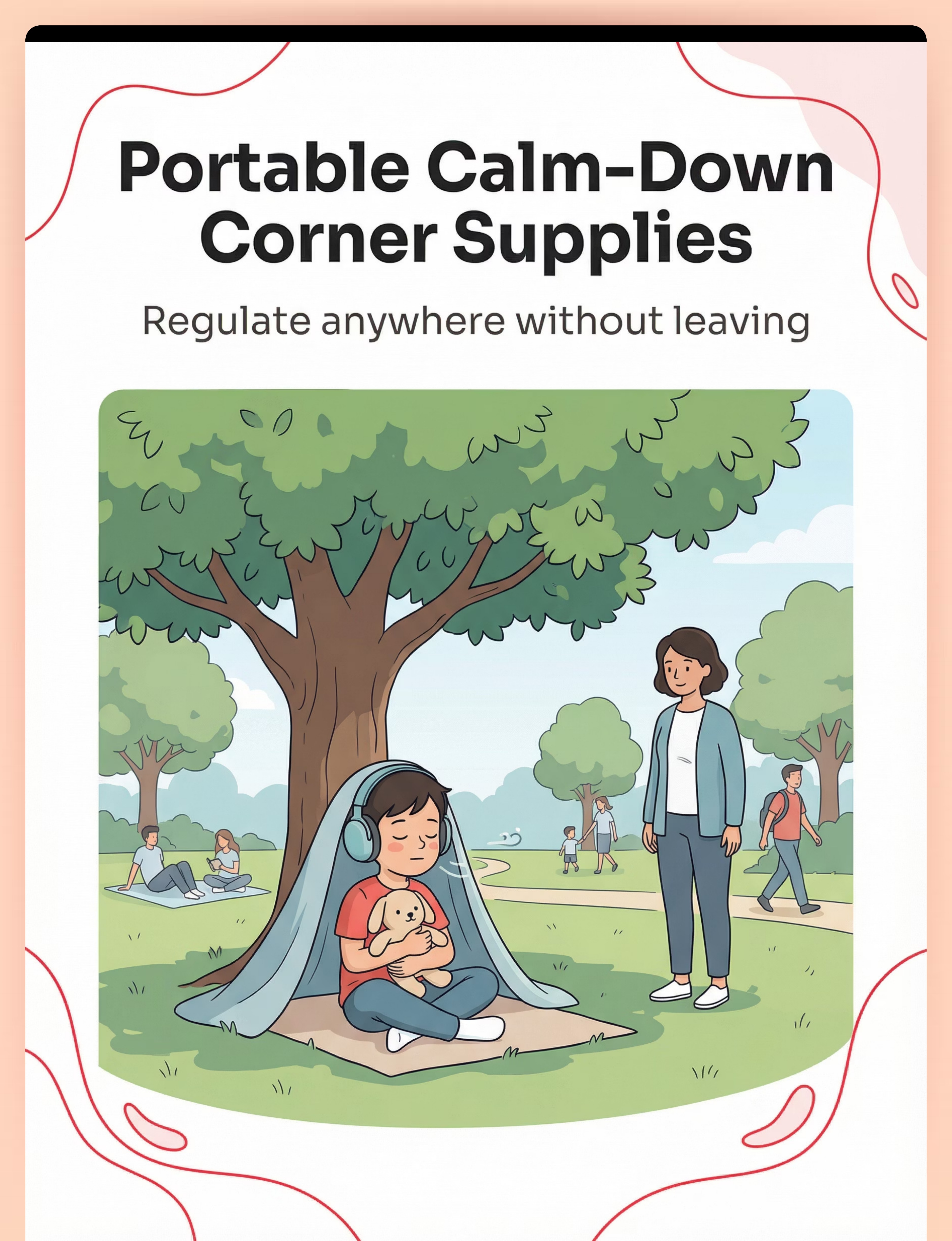
Calm-Down Supplies | ₹500–2,000 kit | Old dupatta/scarf as privacy barrier; household stuffed animal; printed breathing card | Privacy + sensory comfort + regulation cues work regardless of product category | |
Social Scripts | Cards ₹100–300 | Write on paper strips; practice daily | The memorized language is the tool — no purchase required | |
Ally Cards | ₹50–300 printed | Write on plain paper; laminate if possible, or use as-is | The information is the tool; the format matters less than giving it | |
Participation Log | ₹50–200 notebook | Any notebook; a few lines after each outing | Tracking is the tool |

- Child has been unwell in the past 48 hours (illness increases sensory sensitivity significantly)
- Child experienced a severe meltdown or emotional crisis within the last 24 hours
- The planned setting has a known extreme trigger not yet addressed therapeutically
- Child is showing pre-meltdown indicators before departure
- You are not in a regulated state yourself — your anxiety is contagious
- Child is showing mild irritability — shorten, lower demands, bring full sensory kit
- The setting is more crowded than usual — consider off-peak timing
- Child has not slept well — briefer outing, remove optional demands
- New or unfamiliar setting — re-read social story, add extra preparation time
- Child is regulated, fed, rested
- Social story reviewed in the last 24 hours
- Sensory kit is packed and checked
- Visual schedule is prepared
- You have an exit plan that doesn't feel like failure
- All sensory items must be age-appropriate (no small choking-risk items for children under 3)
- Chewy tubes must be food-grade silicone, not generic plastics
- Noise-reducing headphones must be properly fitted — too tight causes discomfort, defeating their purpose
- Communication cards should include emergency contact information on reverse
Indicator | ✅ Go | ⚠️ Modify | 🔴 Postpone | |
Physical state | Rested, fed, no illness | Slightly tired but regulated | Unwell, hungry, dysregulated | |
Emotional state | Calm, neutral, or positive | Mildly irritable but manageable | Distressed, crying, significantly stimming | |
Social story | Reviewed in last 24h | Can be reviewed now in 5 min | Not reviewed; child is anxious | |
Sensory kit | Packed and accessible | Can be quickly assembled | Not available | |
Recent history | No meltdowns in 48h | Mild episode yesterday, recovered | Severe episode in last 24h | |
Your state | Regulated, patient, prepared | Slightly stressed — take 5 min first | Highly dysregulated — don't go today |

"[Name], today we're going to [location]. You remember — we read the story about it! Let me show you our plan for today. See — we'll go to [X], then [Y], and then we come home. Your kit is ready. Let's go!"
- Kneel to child's level during the invitation
- Calm, matter-of-fact tone — not excited (excitement can be dysregulating)
- Point to the visual schedule as you speak — visual anchoring
- Give the child a moment to orient before expecting movement

"We're here! This is [location]. Let's see — [point to visual schedule] — first we [first activity]. See the [specific feature from social story]? Exactly like our story. You can put on your headphones if you want."


Week | Duration | Key Focus | Success Marker | |
Week 1 | 5–10 min | Presence and regulation | Child is present without meltdown | |
Week 2 | 10–15 min | Active engagement with environment | Child interacts with one element of setting | |
Weeks 3–4 | 15–25 min | Social proximity | Child tolerates other people in shared space | |
Weeks 5–6 | 20–30 min | Brief social interactions | One communication card used with a real community member | |
Weeks 7–8 | 30–45 min | Functional community participation | Child completes a community role (buying, ordering, asking) |
- Vary the time of day (morning vs. afternoon)
- Vary the specific entry point to the setting
- Vary the community role assigned to the child
- Introduce a new but related community setting once the first is accessible
"3 successful 15-minute outings > 1 attempted 90-minute outing that ends in meltdown. Frequency and success rate matter more than duration."

Achievement | Exact Praise Script | |
Entered the community setting | "You walked right in! That was brave and I'm so proud of you!" | |
Used communication card with a stranger | "You showed your card to the shopkeeper! That was amazing communication!" | |
Tolerated 10 minutes at the park | "Ten whole minutes at the park! You regulated so well today!" | |
Greeted a neighbour using script | "You said hello to Uncle! That is exactly the kind of community member you are becoming!" | |
Returned to outing after a calm-down break | "You took a break AND came back. That is the strongest thing you can do." |
- Immediate verbal praise + physical affirmation (high five, hug if welcomed)
- Preferred snack at the end of the outing (natural reinforcer)
- Token for the reward jar
- Preferred activity when home (30 minutes of chosen screen time, favourite game)
- Community celebration: "You went to the market! Let's call Grandma and tell her!"
"Celebrate the attempt, not just the success. A child who walked to the park entrance and back deserves the same celebration as one who stayed for 30 minutes. Every boundary pushed is a victory."
- Date, Setting, Duration, Overall Success Rating (1–5)
- What worked today
- What was challenging
- What to try differently next time
- Any regulation tools used — which ones helped?
- Any social interaction (even brief)?
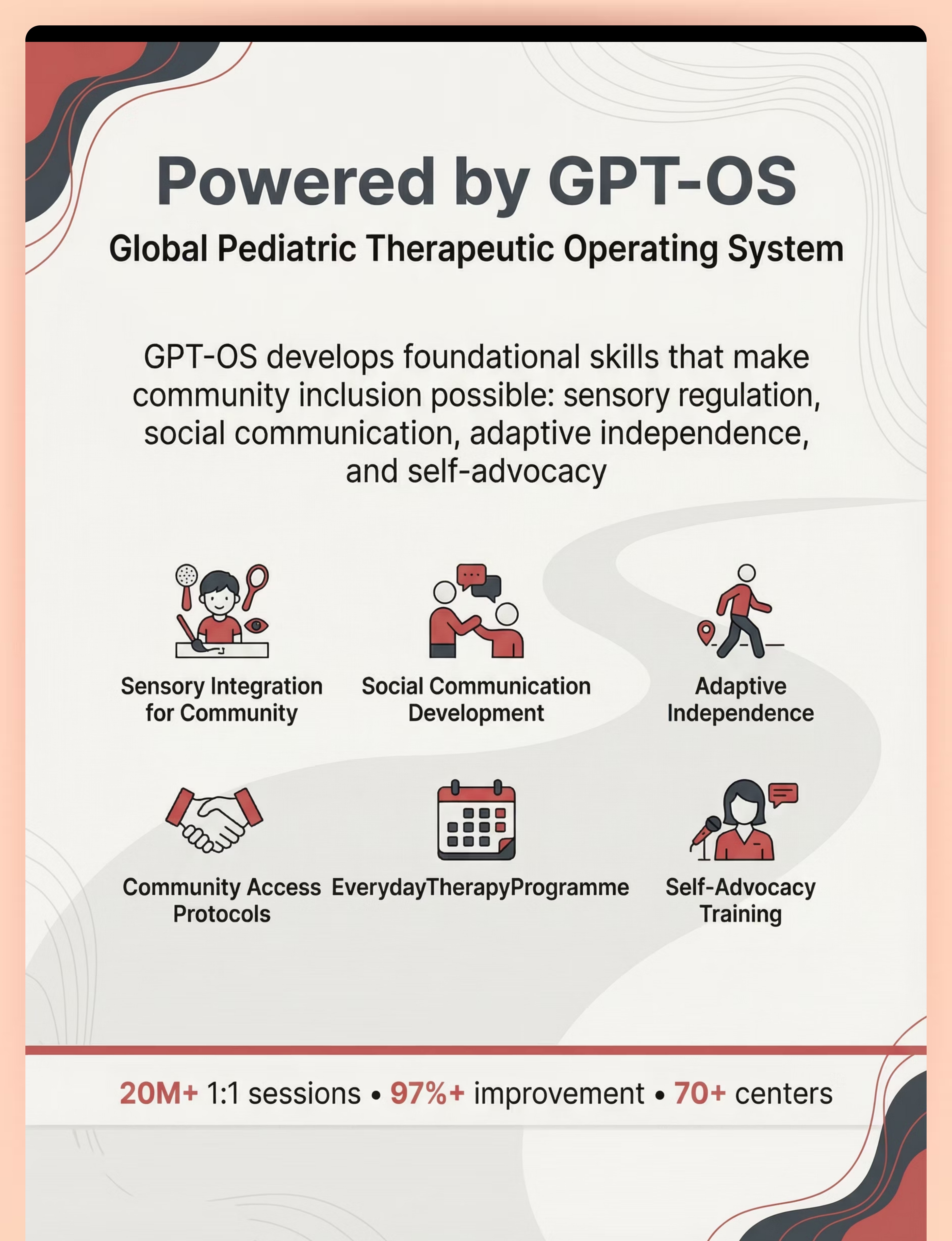
- Download the Community Outing Log PDF via GPT-OS®
- Track digitally in GPT-OS® App at pinnacleblooms.org/gpt-os
- Use Material 9 notebook for paper tracking
- Complete within 60 minutes while memory is fresh

- Provide proprioceptive input BEFORE outing
- Choose settings with natural heavy work (carrying bags, park climbing)
- Movement breaks during outing are energizing, not calming
- May seek more community contact than you expected
- Schedule sensory input during outing via kit — not before
- Choose sensory-light versions of settings (early morning, uncrowded)
- Movement breaks should be to quiet, low-stimulation areas
- May need longer at each stage before expanding

- Child tolerates being in a community setting for the planned duration
- Sensory kit is accepted and used without resistance
- Visual schedule provides some reassurance (child references it)
- One or two moments of genuine environmental engagement
- Reduced pre-departure meltdown compared to previous attempts
- Independent social initiation with peers or community members
- Consistent use of communication cards with strangers
- Complete absence of regulation challenges
- Spontaneous requests to return to community settings
"If your child tolerated the park for 8 minutes this week, and last week they refused to get in the car — that is not a small win. That is everything. The nervous system is being rewired, visit by visit."

- Child anticipates the outing routine — they recognise the kit being packed
- Pre-departure anxiety is reducing (shorter warm-up time needed)
- In-setting regulation tool use is becoming more automatic (child reaches for headphones proactively)
- Child begins referencing the visual schedule independently, without being prompted
- Child begins to show preference for specific elements of the setting
- Duration of comfortable participation is extending without increased regulation challenges
- Brief social acknowledgement of community members (eye contact, nodding, half-smile to familiar shopkeeper)
"By week 3–4, you may notice that you are planning outings with anticipation rather than dread. Your own regulation around community access is consolidating too. This is important data."
- Child mentions the outing setting spontaneously at home
- Child spontaneously uses a community social script in a new setting
- Child asks to return to a community setting they've accessed
- Child's in-clinic social and sensory performance is also improving (skills transfer bidirectionally)
"Our world has expanded from the walls of our home to the entire community. This is what inclusion looks like." — Father, Pinnacle Network
Technique | Domain | Difficulty | Materials You Already Have | |
J-877: Neighbourhood Navigation | Community Access | 🟢 Intro | Social stories, visual schedule | |
J-878: Public Transportation | Community Access | 🟡 Core | Visual schedule, sensory kit | |
J-880: Independent Travel | Community Access | 🔴 Advanced | Communication cards, scripts | |
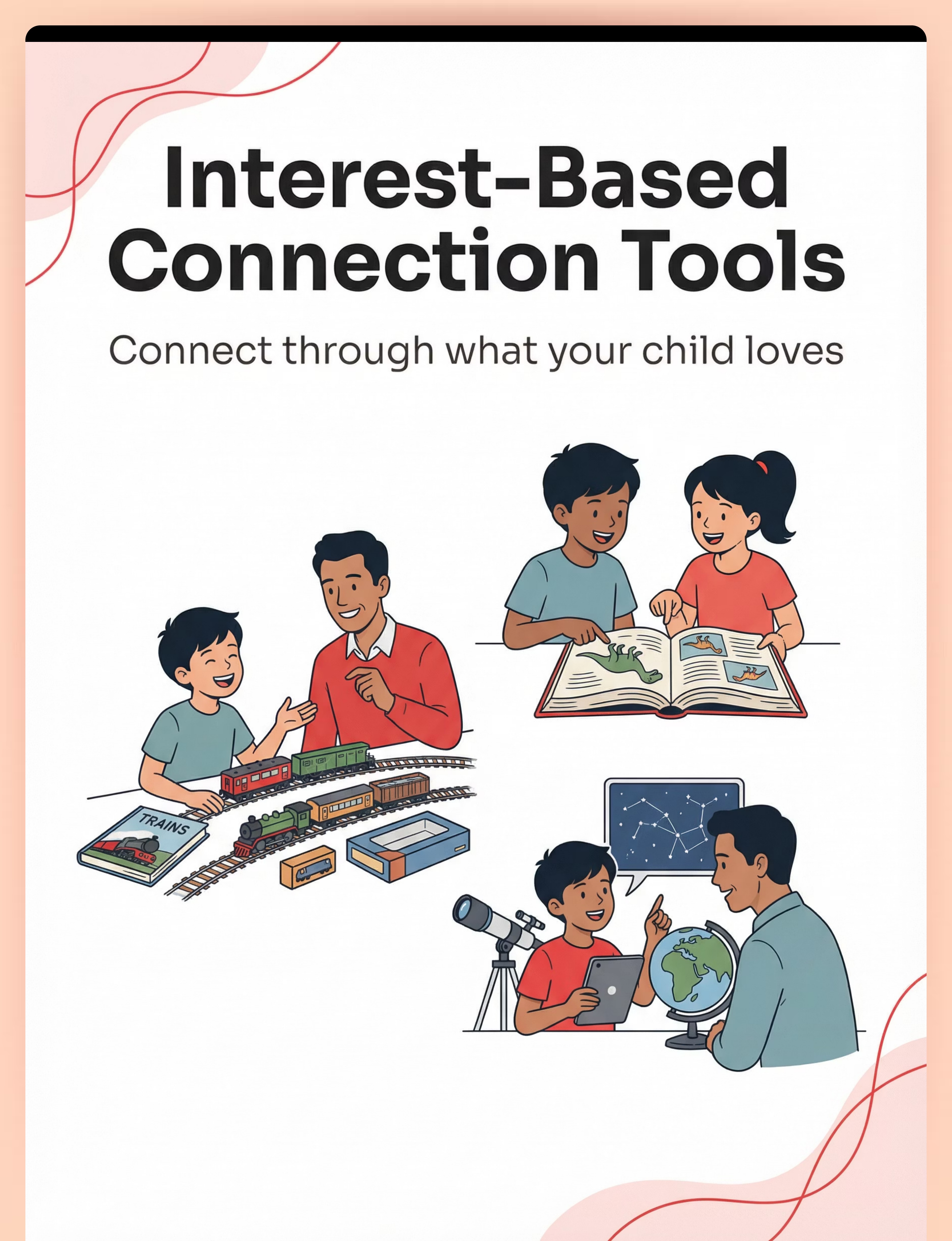
J-881: Recreational Activities | Community Access | 🟡 Core | Interest tools, sensory kit | |
J-882: Religious & Cultural Participation | Community Access | 🟡 Core | Social stories, ally cards | |
F-501: Peer Interaction Skills | Social Participation | 🟢 Intro | Social scripts, interest tools |


Home + Clinic = Maximum Community Access Impact
Home practice and professional guidance are not alternatives. They are multipliers. The families with best community access outcomes do both. Your Child's Primary Challenge Book With Sensory overwhelm in community Occupational Therapist — Sensory Integration specialist Communication barriers in community Speech-Language Pathologist — Community communication specialist Behavioral challenges during outings BCBA / ABA Therapist — Community access behavioral specialist Social interaction deficits Special Education + Social Skills specialist Anxiety about community environments NeuroDev Pediatrician + Clinical Psychologist 🌐 Find Your Center pinnacleblooms.org/centers | 70+ Centers Across India | Serving 70+ Countries 📞 FREE Helpline 9100 181 181 | 16+ Languages | 24x7 | Multilingual support for all families 💻 Teleconsultation 45-minute video session with a Pinnacle community access specialist. pinnacleblooms.org/teleconsult Find Nearest Center → Book Teleconsultation

Study | Finding | Reference | |
PRISMA Systematic Review, Children (2024) | 16 studies (2013–2023) confirm sensory integration intervention is evidence-based practice for community social participation in ASD | ||
Meta-analysis, World J Clin Cases (2024) | Across 24 studies, sensory integration therapy effectively promotes social skills, adaptive behavior, and community participation | ||
Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory + social interventions in Indian pediatric populations demonstrate significant community participation outcomes | ||
WHO Care for Child Development (2023) | Community participation embedded as developmental imperative across 54 low-middle income countries | ||
NCAEP Evidence-Based Practices (2020) | Social stories, visual supports, and video modeling classified as evidence-based practices for autism community participation | ||
UN CRPD Article 30 (2006) | International legal right to community, cultural, and recreational participation for all persons with disabilities |
- Your child's community tolerance ceiling across settings
- Most effective regulation tools by setting type
- Social script success rates by community interaction type
- Optimal community access frequency and timing for your child's profile
- All individual data is encrypted and owned by you
- Population-level learning uses fully anonymized aggregate data only
- GDPR and Indian Data Protection Bill compliant
- You can delete your data at any time

Preview of 9 materials that help with community inclusion Therapy Material
Below is a visual preview of 9 materials that help with community inclusion therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
📞 9100 181 181 | 🌐 pinnacleblooms.org | 📧care@pinnacleblooms.org
techniques.pinnacleblooms.org | J-879 | Community Access Domain