
"We stopped going to restaurants. Every single time ended in disaster."
You are watching your child struggle — not misbehave. A restaurant tests every skill at once: waiting, sitting, sensory tolerance, unfamiliar food, social rules — all simultaneously, in public, under judgment. That is not a behavior problem. That is an impossible ask without the right support.
Community Participation Series • Episode J-845
9 Materials That Help With Restaurant Behaviour
You are not failing as a parent. Your child's nervous system is speaking loudly in an environment built for neurotypical adults. Today, that changes.
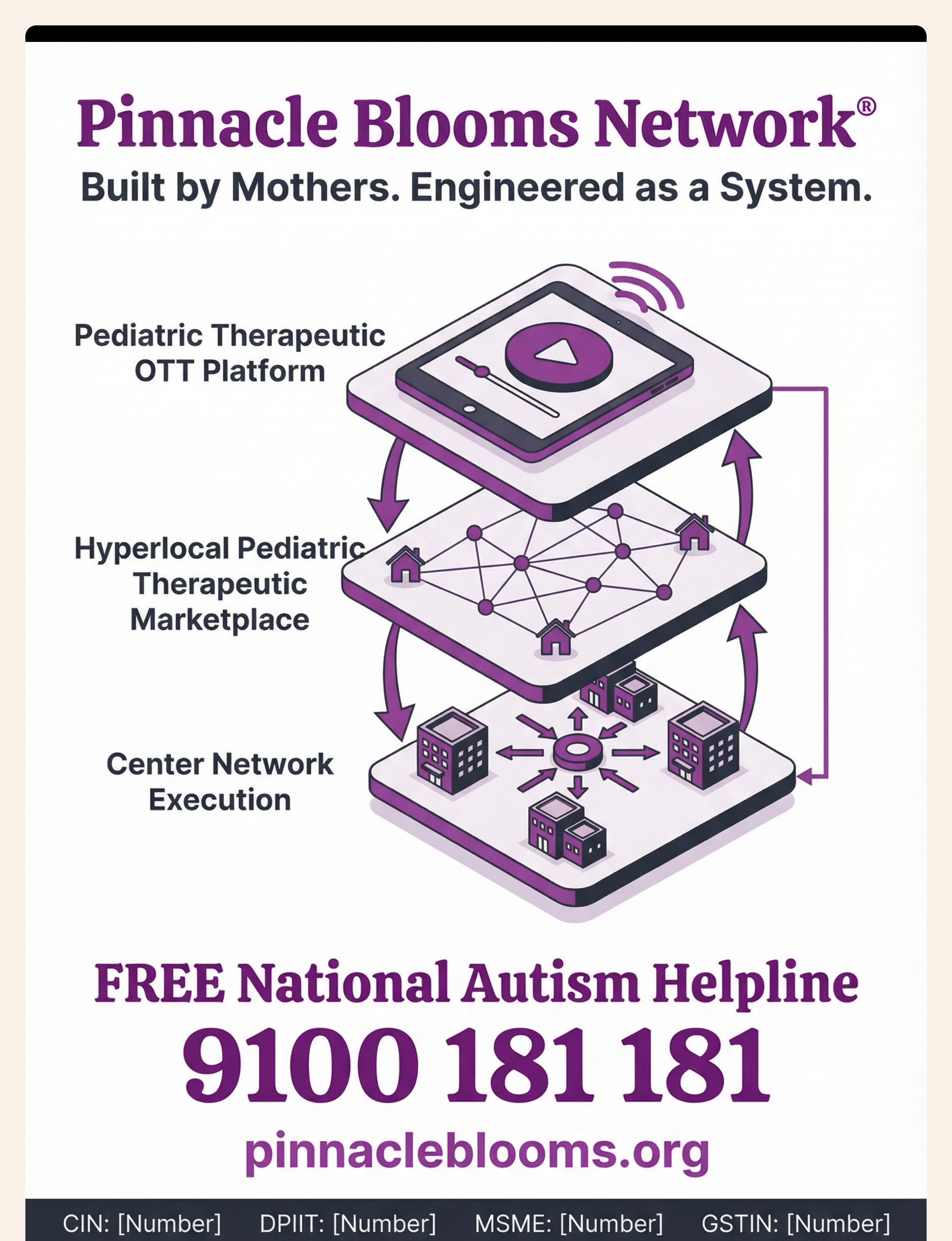
🏅Pinnacle Blooms Consortium | OT • SLP • ABA • SpEd • NeuroDev • Pediatrics — GPT-OS® Technique Library | techniques.pinnacleblooms.org

You Are Among Millions of Families Navigating This Exact Challenge
1 in 36
Children with ASD
Children in the US are diagnosed with Autism Spectrum Disorder (CDC Autism Prevalence Report 2023)
80%
Sensory Difficulties
Of children with ASD experience sensory processing difficulties that make public environments overwhelming (PMC11506176 — PRISMA Systematic Review, 2024)
70%
Avoid Public Outings
Of families with autistic children report avoiding public outings due to behaviour challenges (Pinnacle Network Survey Data, 2024)
Restaurant avoidance is not a parenting failure — it is the predictable outcome of placing a child with sensory processing differences into an environment that simultaneously overwhelms every sensory system while demanding maximum self-regulation. The stares from other diners are not seeing a poorly-behaved child. They are witnessing a nervous system under assault.
🌏In India: An estimated 18 million children are on the autism spectrum (Mathur & Bhargava, NIMHANS). Fewer than 3% access structured intervention. The materials in this series serve families in all 28 states, 8 union territories, and 70+ countries where Pinnacle operates.
PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | Padmanabha et al., Indian J Pediatr, 2019

This Is a Wiring Difference. Not a Behaviour Choice.
What Is Happening Neurologically
A restaurant activates EVERY sensory channel simultaneously — auditory (noise, music, clatter), visual (movement, lights, screens), olfactory (cooking smells, cleaning products), tactile (unfamiliar seating, utensils), proprioceptive (unfamiliar body positioning in booth or chair).
In children with Sensory Processing Differences (SPD) — common in autism, ADHD, and anxiety — the somatosensory cortex and auditory processing pathways over-amplify incoming signals. What feels like manageable background noise to a neurotypical adult feels like standing next to a jet engine to a sensory-sensitive child.
The Prefrontal Cortex Factor
The prefrontal cortex — responsible for impulse control, patience, and self-regulation — is still developing until age 25. For children with ADHD, this development is 30% slower than peers. Asking a 7-year-old with ADHD to sit still for 45 minutes is neurologically equivalent to asking a 4-year-old without ADHD to do the same.
The result: The nervous system floods. The amygdala triggers fight-or-flight. What looks like "misbehaviour" is dysregulation — a biological response, not a moral failure.
"Behaviour is communication. When words fail, the body speaks." — Pinnacle Blooms Consortium Clinical Team
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 — Sensory integration neurological basis for sensory-based interventions in ASD.

Your Child Is Here. Here Is Where We Are Heading.
Children with autism, ADHD, or sensory processing differences frequently show a functional gap between chronological age and restaurant tolerance age. A 10-year-old with autism may have the restaurant tolerance of a 3-year-old — not because they are less capable, but because the prerequisite skills have not yet been built with appropriate scaffolding.
Age 2–3
Brief visits 10–15 min with constant support
Age 4–5
30–45 min with heavy supports deployed
Age 6–8
Full meals with full support, some tools remaining
Age 9–12
Moderate independence with parental care
Age 13+
Age-appropriate independence
This is not permanent. These skills can be built systematically — at any age — with the right materials and approach.
Restaurant challenges are common in: Autism Spectrum Disorder • ADHD • Sensory Processing Disorder • Anxiety Disorders • Developmental Delays • PDA Profile • Hyperlexia
WHO Care for Child Development (CCD) Package — implemented in 54 low- and middle-income countries. UNICEF MICS developmental monitoring indicators. PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
🛡️ LEVEL I — SYSTEMATIC REVIEW + META-ANALYSIS
Supported by 24+ controlled studies across 3 continents
✅ PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm sensory integration and visual support interventions meet evidence-based practice criteria for children with ASD. (PMC11506176)
✅ Meta-analysis, World J Clin Cases (2024)
Sensory integration therapy effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills across 24 studies. (PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260)
✅ NCAEP Evidence-Based Practices Report (2020)
Visual supports, first-then boards, and behavioural support systems classified as evidence-based practices for autism.
✅ Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions demonstrated significant measurable outcomes in Indian paediatric populations. (DOI: 10.1007/s12098-018-2747-4, Indian J Pediatr)
✅ Social Stories Research (Gray, 1994 — ongoing)
Social story methodology demonstrates effectiveness across community settings for autism and ADHD.
"The 9 materials presented in this series are not opinions. They are distilled from the largest structured evidence base in paediatric community participation intervention." — Pinnacle Blooms Research & CRO Division
J-845 | 9 Materials That Help With Restaurant Behaviour
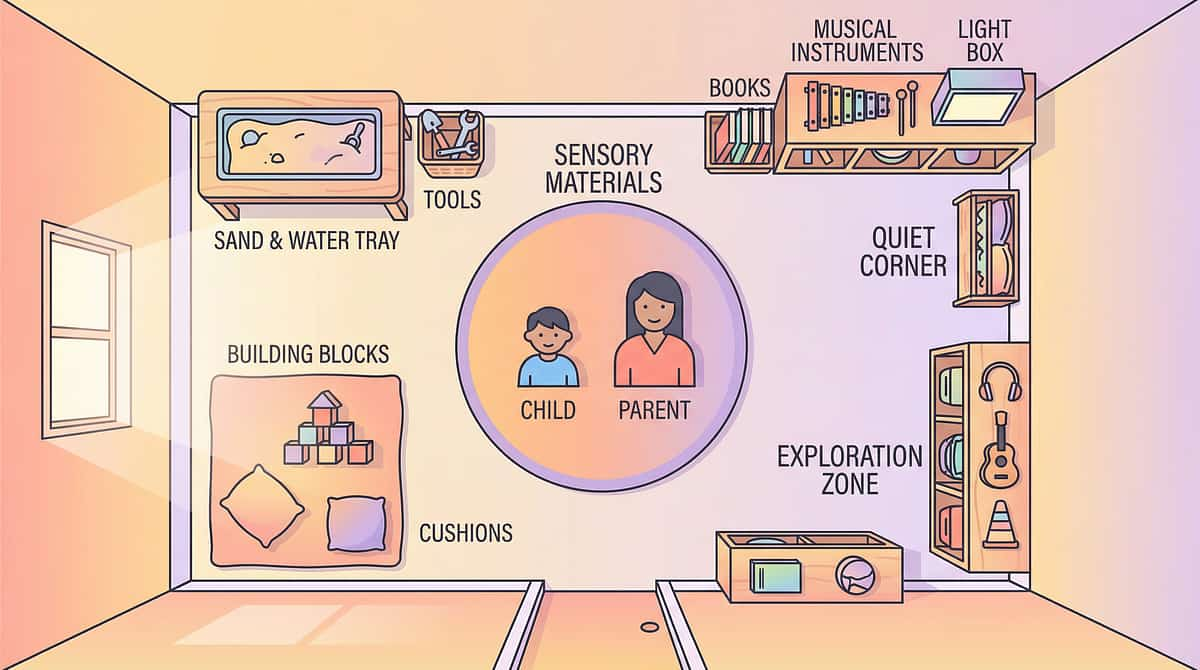
🍽️ The Restaurant Success Kit
Definition: Restaurant Behaviour Support is a multi-material intervention framework that equips children with autism, ADHD, sensory processing differences, and anxiety disorders with the preparation, environmental scaffolding, sensory management tools, and behavioural supports needed to successfully participate in public dining experiences. Rather than a single technique, this framework addresses restaurant dining as a complex adaptive challenge requiring simultaneous support across multiple developmental domains.
🟠 Domain Badges
Community Participation | Public Behaviour | Sensory Regulation | Waiting Skills | Daily Living Skills | Social Skills | Adaptive Behaviour
📦 Canon Materials
Social Stories | Visual Timers | Sensory Toolkits | First-Then Boards | Reinforcement Menus | Visual Schedules | Behaviour Checklists
🔧 Technical Details
👶 Age Range: 3–14 years | ⏱ Session: Full restaurant visit (30–90 min) | 📅 Frequency: Every outing | 🏠 Setting: Community + Home Preparation
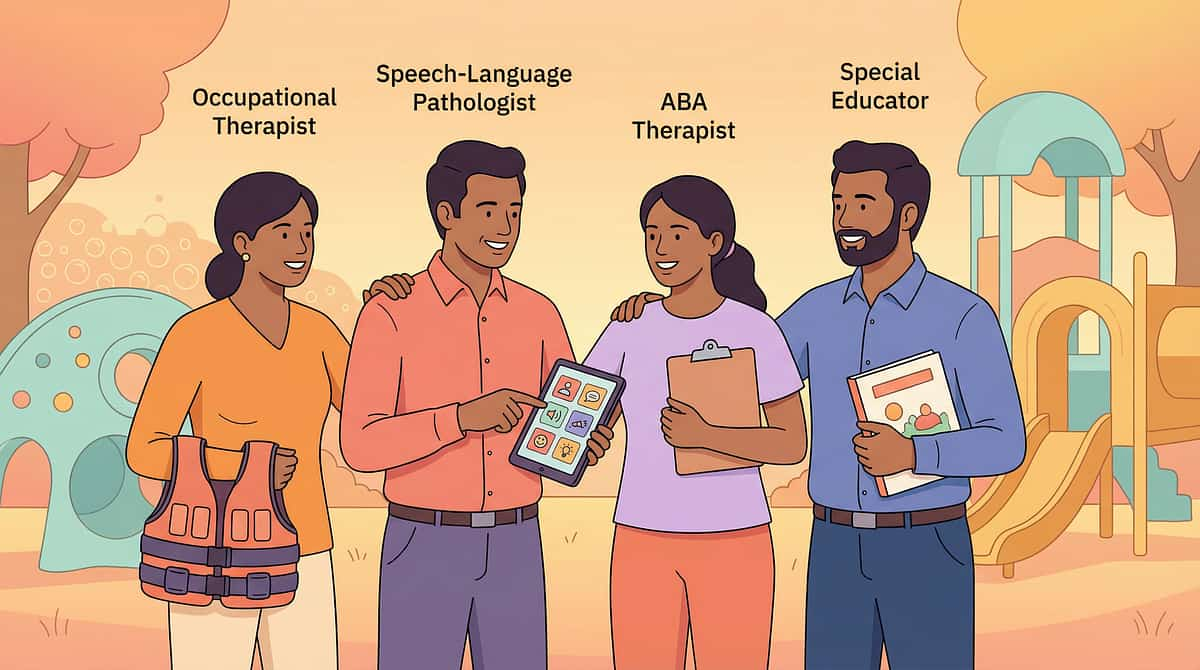
This Technique Crosses Therapy Boundaries — Because Your Child Doesn't Organise Their Brain by Therapy Type
Occupational Therapy (Lead)
OTs design the sensory toolkit (headphones, fidgets, seat cushions), analyse the restaurant's sensory environment, and grade the graduated exposure progression. OT leads the sensory integration component of every restaurant outing.
Applied Behaviour Analysis (ABA/BCBA)
BCBAs design the behaviour checklist, reinforcement systems, and first-then boards. ABA provides the antecedent strategies (social story preview) and consequence strategies (reward menus) that shape restaurant behaviour.
Speech-Language Pathology (SLP)
SLPs address the communication component: how to request a break, how to order food, how to use the break card. For AAC users, the restaurant presents unique communication demands addressed in SLP sessions.
Special Education (SpEd)
SpEd specialists design the visual schedules, social stories, and first-then boards that scaffold the restaurant sequence for children who need explicit instruction in social routines.
NeuroDev Paediatrics
NeuroDev paediatricians provide the diagnostic context (ASD, ADHD, SPD, anxiety) that informs which materials are prioritised. Medical management of sensory processing and anxiety supports the behavioural intervention.
"When OT, ABA, SLP, and SpEd work from the same case formulation — as they do under GPT-OS®'s FusionModule™ — restaurant success becomes a measurable, achievable clinical target rather than a hopeful wish." — Pinnacle Blooms Consortium FusionModule™ Team
Precision Tools. Specific Targets. Measurable Outcomes.
Target | Observable Behaviour Indicator | |
Participation tolerance | Stays at table for 30+ minutes without elopement | |
Sensory regulation | Tolerates restaurant environment with sensory tools in place | |
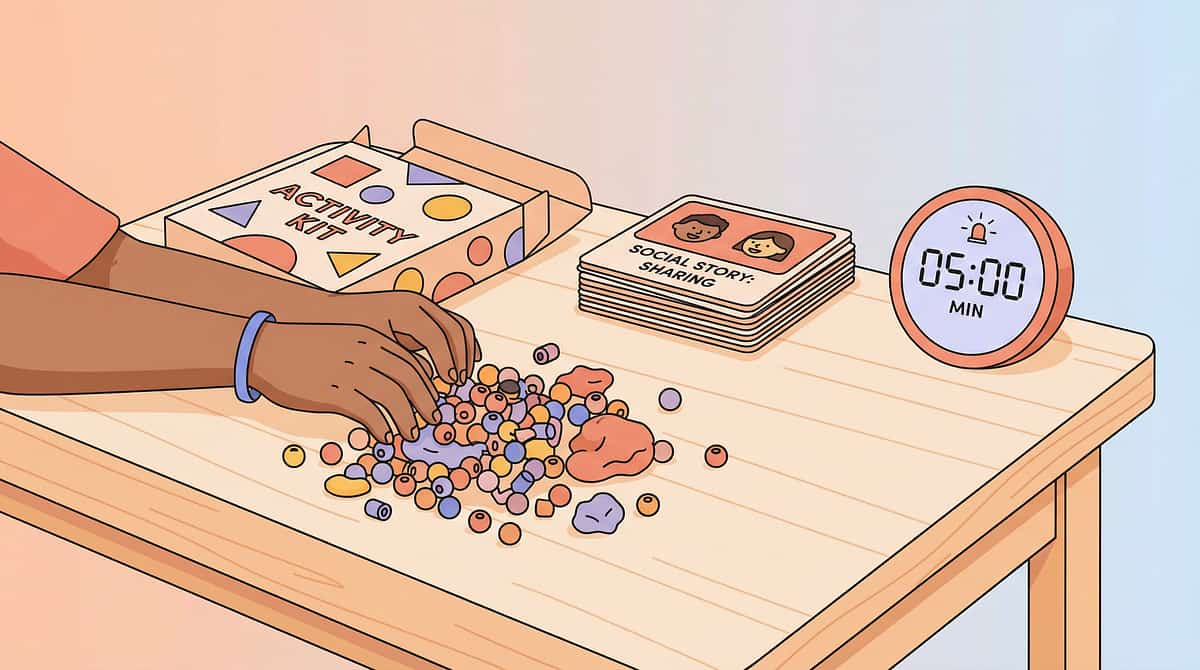
Waiting skills | Remains engaged with activity kit for 15+ minute wait | |
Food flexibility | Attempts familiar food backup without distress | |
Spatial awareness | Keeps hands in own space; drink stays on table |
PMC10955541 — Meta-analysis confirms sensory integration effectively promotes social skills (primary), adaptive behaviour (secondary), and motor skills (tertiary).

9 Materials. One Kit. A Restaurant Experience Transformed.
Each of the 9 materials addresses a specific failure point in the restaurant experience. Together, they form a complete system of preparation, engagement, sensory support, and regulation that gives your child — and your family — a genuine chance at success.
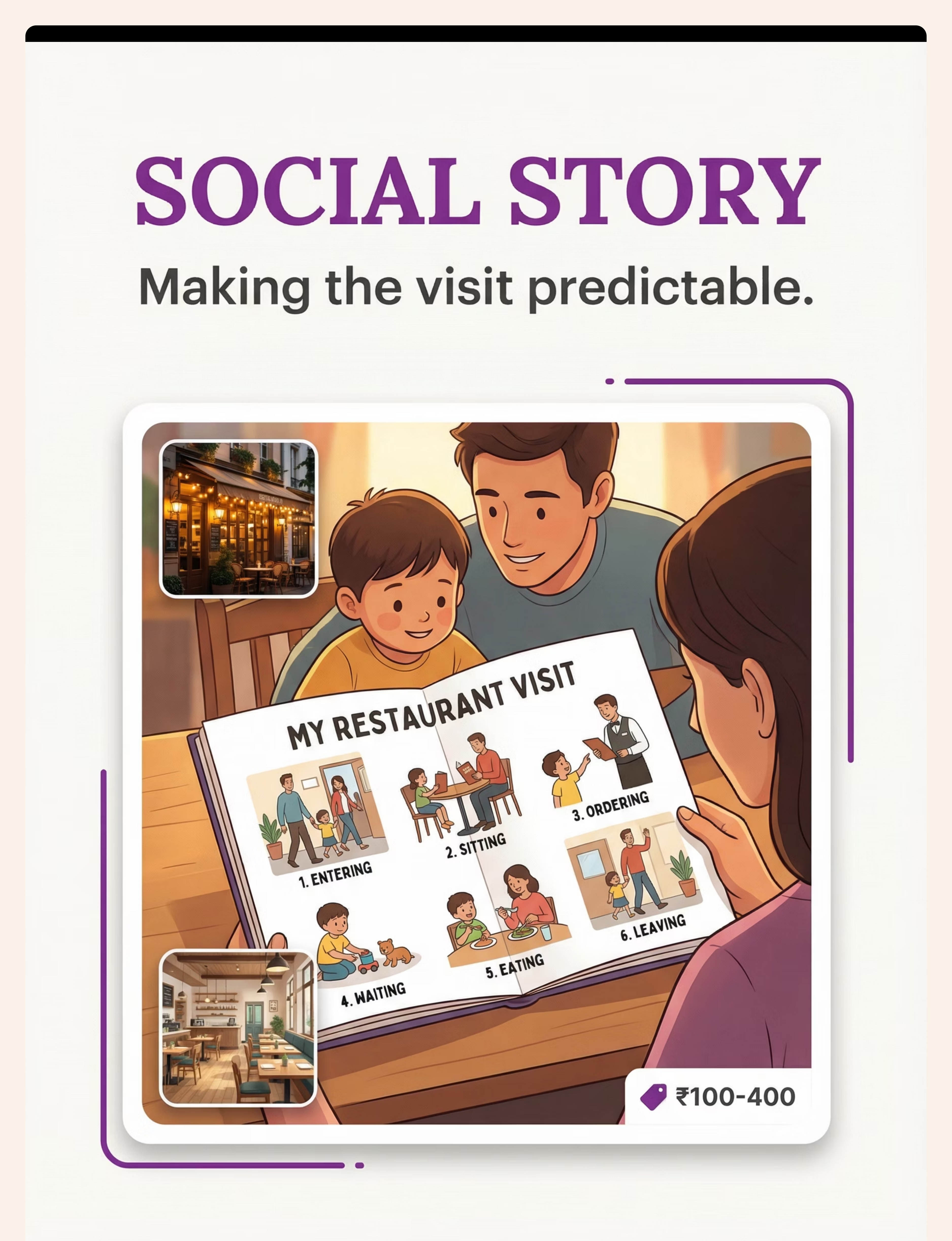
1. Social Story & Visual Preview
Makes the visit predictable before it begins | ₹100–400 (mostly DIY)
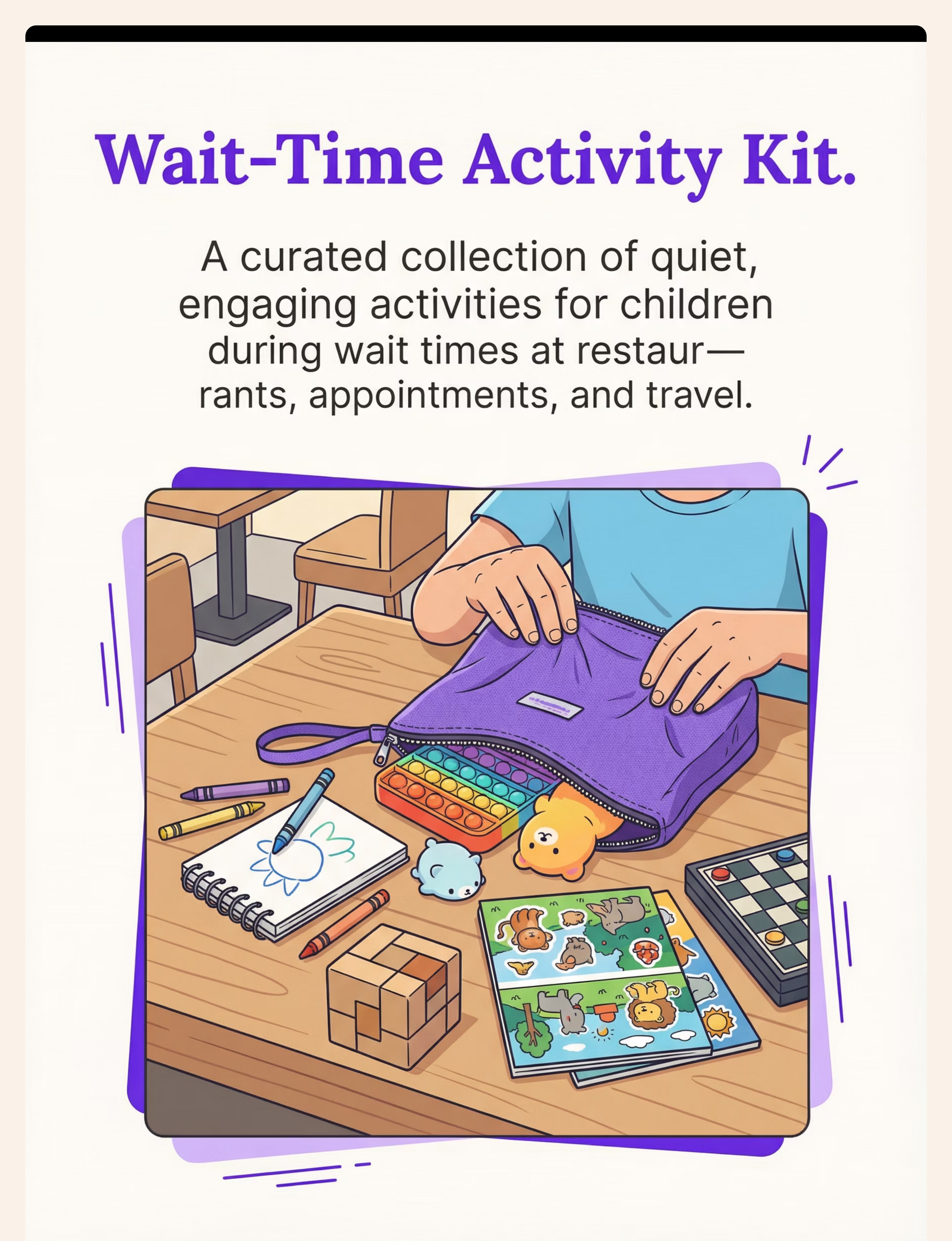
2. Wait-Time Activity Kit
Structured engagement during the hardest 20 minutes | ₹300–1,000
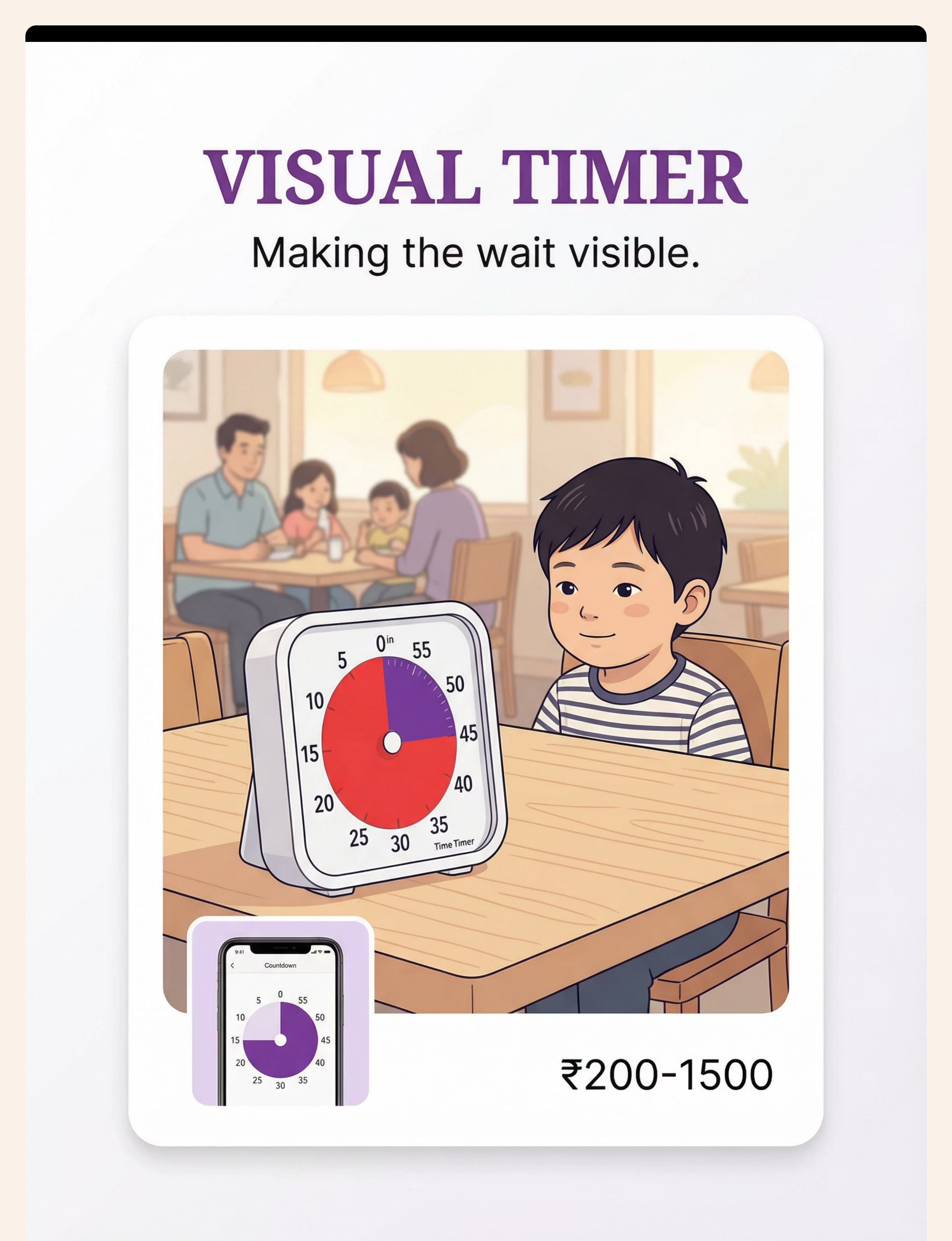
3. Visual Timer
Makes invisible time visible and countable | ₹200–1,500
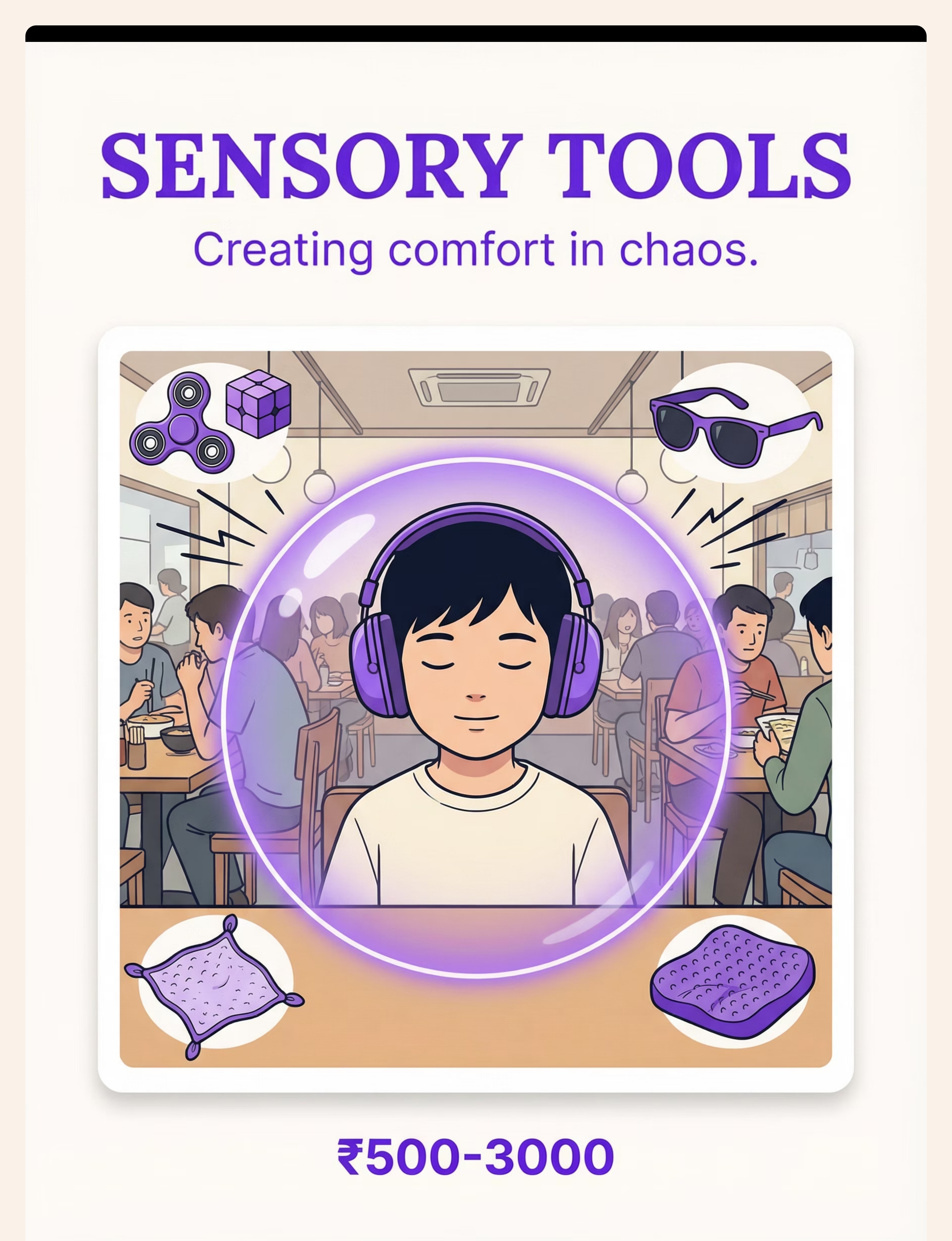
4. Sensory Support Toolkit
Creates a personal sensory bubble in a chaotic environment | ₹500–3,000
5. Portable Placemat System
Defines personal space; prevents spills; reduces nagging | ₹300–800
6. First-Then Board
Shows what comes next; makes the abstract concrete | ₹100–400
7. Familiar Food Container
Ensures the child can eat something; removes one layer of crisis | ₹50–200
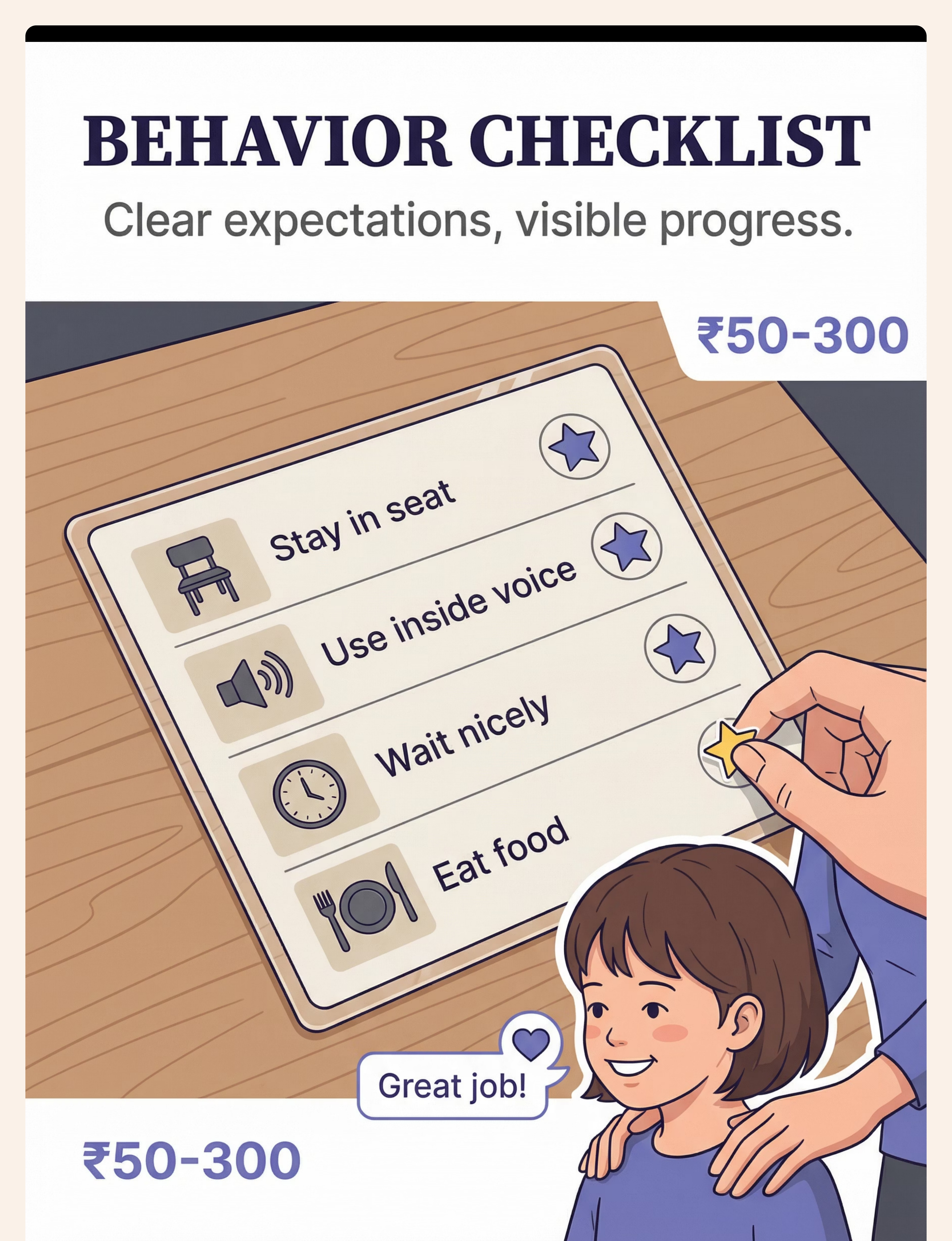
8. Behaviour Checklist with Reinforcement
Externalises expectations; tracks visible progress; motivates | ₹50–300
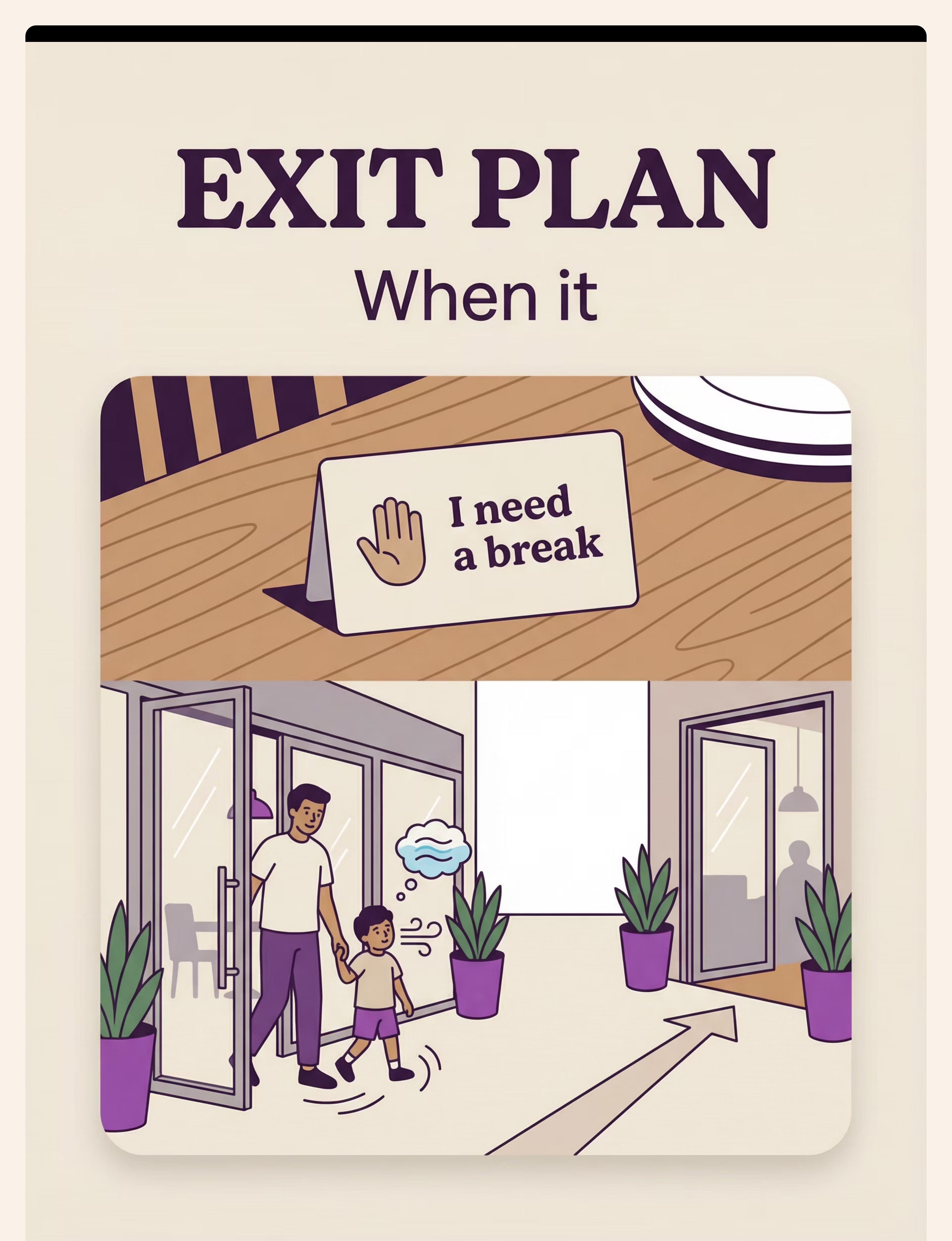
9. Exit Strategy & Calm-Down Plan
Pre-planned response that prevents catastrophe and enables re-entry | ₹0–200
💰Total Kit Cost Range: ₹1,300–6,800 for all 9 materials | ✅ Budget option available for every material (₹0 DIY alternatives)
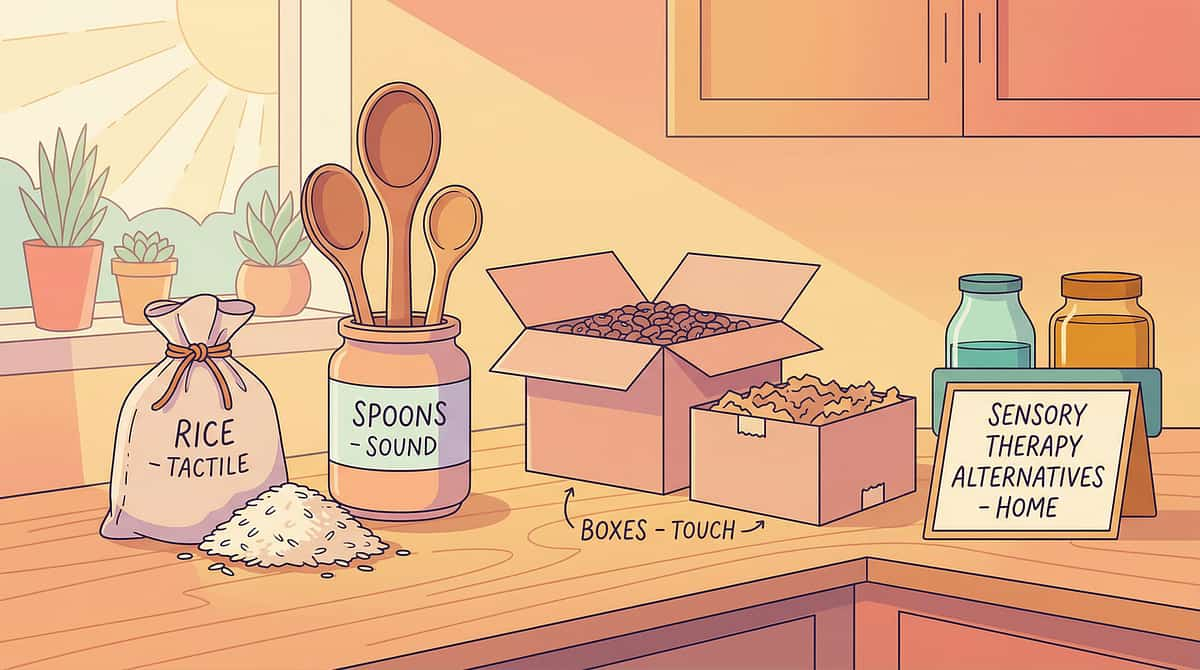
Every Material Has a ₹0 Version. Your Income Does Not Determine Your Child's Access.
The WHO Nurturing Care Framework and UNICEF's equity principles require that evidence-based interventions be accessible regardless of economic status. Every material in this series has a household-based alternative. These alternatives work because they activate the same neurological and behavioural mechanisms as the commercial versions.
Material | Buy (₹) | Make (₹0) — Why It Works | |
Social Story | 100–400 | Paper + pencil + Google images — Same predictability mechanism | |
Activity Kit | 300–1,000 | Repurposed household toys in a ziplock bag — Novelty and engagement are the mechanism | |
Visual Timer | 200–1,500 | Sand from two plastic bottles — Visual time passage is the mechanism | |
Sensory Tools | 500–3,000 | Foam earplugs (₹20) + rolled-up sock fidget — Sensory input reduction is the mechanism | |
Placemat | 300–800 | Laminated A4 paper with drawn zones — Spatial definition is the mechanism | |
First-Then Board | 100–400 | Index card + drawn pictures — Sequence visualisation is the mechanism | |
Food Container | 50–200 | Any lidded container — Familiar food is the mechanism | |
Behaviour Checklist | 50–300 | Paper + pen — Visible progress tracking is the mechanism | |
Break Card | 0–200 | Index card with "I need a break" written — Communication of need is the mechanism |
⚠️When the clinical-grade material is non-negotiable: For children with profound sensory processing difficulties, quality noise-reducing headphones (not foam earplugs) may be essential. Consult your OT for assessment.
🌍 Equity-First Design
WHO NCF Compliant
UNICEF Inclusion Principles
PMC9978394 | WHO NCF Handbook (2022) — Household-material-based intervention efficacy in 54 LMICs. Accessible to families in all 28 Indian states, 8 UTs, and 70+ countries.
Read This Before Your First Restaurant Attempt With Supports
🟢 GREEN — Proceed As Planned
- Child has eaten (not hungry before entering)
- Child has had adequate rest the night before
- Child is in a regulated baseline state before leaving home
- All materials are packed and ready before arrival
- You have reviewed the social story at least 3× in the days prior
- You have chosen a sensory-friendly restaurant
- Both caregivers (if applicable) have discussed the exit plan
🟡 AMBER — Modify the Plan
- Child has had a difficult morning — shorten duration target, increase support
- Restaurant is busier than anticipated — use maximum sensory tools immediately
- Child is showing early dysregulation signs on arrival — deploy activity kit before sitting
- Familiar food unavailable at this restaurant — deploy backup food early
🔴 RED — Do Not Proceed Today
- Child is sick, running fever, or in significant pain
- Child has had a major meltdown within the last 2 hours
- Child is severely dysregulated and cannot enter the building calmly
- Caregivers are significantly stressed or have conflicting approach
🛑RED LINE — Stop and Exit If You Observe: Self-injurious behaviour (head-hitting, self-biting) | Aggressive behaviour toward others | Complete sensory shutdown (unresponsive, cannot move) | Signs of medical distress (breathing changes, vomiting) | Sustained elopement attempts (trying to run from the building)
⚠️Safety Note — Sensory Tools: Wireless headphones are safer than corded in restaurants (no trip hazard). Ensure child can still hear parent's instructions when needed — test at home first.
DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al., Indian J Pediatr (2019): Home-based intervention safety protocols for parent-administered sessions.
The Right Restaurant on the Right Day at the Right Time Is Half the Intervention
✅ Choose Restaurants With:
- Booth seating (containment, back support, defined space)
- Relatively quiet ambient noise (no live music, no open kitchens)
- Outdoor seating option (escape route; open space)
- Quick food preparation (15–20 min max wait)
- Child-friendly menu with familiar food options
- Tolerant, family-friendly atmosphere
- Proximity to restaurant exit (request corner booth)
- Off-peak hours available (3pm–5pm)
❌ Avoid Restaurants With:
- Very loud music or open-kitchen noise
- Bright or flickering lighting
- Long waits typical (trendy restaurants, no reservations)
- Formal, quiet-expected atmosphere
- Strong food smells overwhelming near the entrance
- Cramped seating with minimal egress
🪜 Graduated Exposure Ladder
- Home restaurant practice (timed table sits)
- Drive-through — no indoor sitting required
- Fast food brief (10–15 min max, controlled exit)
- Casual dining, off-peak (early dinner, outdoor seating)
- Casual dining, standard time (full support deployed)
- Gradual support fading as tolerance builds
1
Place Placemat
Place placemat immediately upon sitting
2
Position Drink
Position drink in far corner away from dominant hand
3
Set Visual Timer
Set visual timer as soon as order is placed
4
Open Activity Kit
Open activity kit BEFORE dysregulation begins — proactive, not reactive
5
Display First-Then Board
Place first-then board in child's line of sight
6
Keep Sensory Tools Accessible
Keep sensory tools accessible — not at bottom of bag. Know the bathroom/exit location before sitting.

60 Seconds Before You Walk In. The Best Outing Is One That Starts Right.
Check | Indicator | Status | |
Fed? | Child has eaten within the last 2 hours | ✅ / ❌ | |
Rested? | Normal sleep last night | ✅ / ❌ | |
Regulated? | Baseline calm state observable | ✅ / ❌ | |
Materials packed? | Full kit in bag | ✅ / ❌ | |
Story reviewed? | Social story read today or yesterday | ✅ / ❌ | |
Exit plan discussed? | Both caregivers know their roles | ✅ / ❌ |
🟢 GO — 5–6 Checked
Proceed with full protocol as planned.
🟡 MODIFY — 3–4 Checked
Shorten duration target, increase proactive support, choose easiest restaurant option. Start with 15 minutes, not 45. Use all sensory tools from the first minute.
🔴 POSTPONE — 2 or Fewer
Choose a home-based practice session instead. This is not failure — it is data. A session pushed through dysregulation teaches the brain: "restaurants = trauma."
ABA principles: Antecedent manipulation and setting events are primary determinants of session effectiveness. Readiness assessment is a standard component of ABA session protocols.

📖 Material 1 of 9
Social Stories | Visual Schedules
MATERIAL 1: Social Story & Visual Preview
Making the restaurant visit predictable — When children know what to expect, they can regulate what they feel.
What It Is
A social story is a short, first-person narrative that previews an upcoming experience — telling the child exactly what will happen from arrival to departure. Created by Carol Gray (1994) for children with autism, social stories reduce novelty anxiety by transforming an unpredictable experience into a known sequence.
Why It Works
Restaurants are anxiety-inducing because they are full of unknowns: how long will we wait? What will the seat feel like? What if I don't like the food? The social story answers every question the anxious brain would otherwise spin through. Prediction = regulation. What is known cannot ambush.
When to Use
Read aloud to the child (or child reads independently) daily for 3–5 days before the restaurant visit, and once more in the car on the way. Keep available at the table for reference.
Core Story Structure — Use or Adapt
"Today/Tomorrow, our family is going to [restaurant name]. A restaurant is a place where people go to eat food that other people cook.
When we arrive, we might wait a moment before we sit. Waiting is normal and the table will be ready soon. We will sit at a table. I will have my own space.
A server will come to take our order. I can choose what I want to eat. Then we will wait for the food to be cooked. This takes about [X] minutes. While I wait, I can use my activity kit.
When the food arrives, we will eat together. I will try to use my inside voice and stay in my seat. When we are done, we will pay and say thank you to the server. Then we will leave.
If I feel overwhelmed, I can tell Mum/Dad, or show them my break card. I can do this."
📸Photo personalisation tip: Look up the restaurant on Google Maps — Street View shows the exterior. The restaurant's website or Swiggy/Zomato listing shows the interior. Download these photos and insert them into the story. Seeing the actual location reduces novelty-triggered anxiety significantly.
💰Price: ₹100–400 (printed + laminated) | ₹0 (drawn on paper)
Gray (1994) Social Stories methodology | NCAEP (2020): Social narratives classified as evidence-based practice for autism.

🎒 Material 2 of 9
Engagement | Fine Motor Tools
MATERIAL 2: Wait-Time Activity Kit
Something to DO during the hardest part — Engaged children are regulated children. The wait is not dead time.
What It Is
A portable, curated collection of quiet, engaging activities specifically designed for restaurant wait times. Unlike a regular toy bag, the restaurant activity kit is governed by strict selection criteria: quiet, contained, mess-free, novel, and matched to this child's interests.
Why It Works
For children with ADHD, unstructured waiting is neurologically impossible — the prefrontal cortex cannot sustain attention without input. For children with autism, the anticipation anxiety of the undefined wait period escalates without an engagement channel. The activity kit provides the regulatory bridge between seated and food-arrived.
🔑Critical design principle: Reserve kit items exclusively for restaurant use. Novelty drives engagement. An item that only appears at restaurants becomes anticipated, not dreaded.
Kit Contents — 6 Categories
- 🖍Fine Motor: Mini Etch-a-Sketch, magnetic drawing board, Wikki Stix, lacing cards, tray puzzle
- 📚Visual: I Spy or Where's Waldo book, reusable sticker book, small photo album, visual illusion cards
- ✏️Quiet Creativity: Small notebook + crayons (not markers), dot-to-dot book, travel colouring book
- 🃏Thinking Games: Uno, Go Fish, Connect Four travel size, word search for older children
- 🔵Sensory (quiet): Squeeze fidget, Wikki Stix, small putty, chewable pendant
- 📱Digital (backup): Pre-downloaded content, headphones, volume limit set
Rotation Principle
Add one new item before each restaurant visit. Rotate out items the child has lost interest in. A kit with one genuinely novel item always has an engagement anchor.
💰Price: ₹300–1,000 | ₹0 (repurposed household items in a designated bag)
ABA: Antecedent engagement strategies prevent dysregulation. Prefrontal cortex maturation timeline: ADHD delays inhibitory control 30% versus peers.
⏱ Material 3 of 9
Visual Timers
MATERIAL 3: Visual Timer
Making the wait visible — "The food will come soon" means nothing. A shrinking red disk means everything.
What It Is
A visual timer makes elapsed and remaining time concretely visible — a red disk shrinking on a Time Timer, sand falling in an hourglass, or a countdown app on a phone. For children whose sense of abstract time is underdeveloped, seeing time pass transforms unbearable uncertainty into manageable anticipation.
Why It Works
Abstract language like "soon," "in a minute," or "just a little longer" is meaningless to a child who cannot conceptualise relative time. Visual timers solve this by externalising time as a shrinking visual that even a 3-year-old can understand: "When the red is gone, the food comes." The anxiety of not knowing is replaced by the calm of watching.
Restaurant Timing Protocol
- ⏱Set on order placed — estimate 15–20 minutes for typical casual dining
- ⏱If food arrives early — celebrate the pleasant surprise
- ⏱If timer ends without food — acknowledge calmly: "The kitchen is taking a little longer. Let's set 5 more minutes." Reset once.
- ⏱Chunk the wait: Menu time (5 min) → Order time (2 min) → Wait time (15 min) → Eat time (20 min) → Pay time (5 min)
Options
- 🔴Time Timer (physical device, most visually clear) — ₹800–1,500
- ⌛Sand timer (fixed durations, no batteries) — ₹200–500
- 📱Time Timer app (on phone, propped on table) — ₹0–₹200
- 📱Any visual countdown app (free, Android/iOS)
⚠️ Some children fixate on the timer, increasing rather than reducing anxiety. For these children: set the timer, then gently cover it. Check periodically.
💰Price: ₹200–1,500 | ₹0 (draw a circle on paper, shade it as time passes)
NCAEP (2020): Visual supports are evidence-based practice for autism. Time visualisation research confirms external temporal cues reduce waiting-related distress.
🎧 Material 4 of 9
Sensory Toolkits
MATERIAL 4: Sensory Support Toolkit
Creating comfort in chaos — You cannot change the restaurant's sensory environment. You can change what reaches your child.
A portable sensory toolkit — typically a small zippered bag — containing tools matched to the child's specific sensory processing profile that reduce the impact of overwhelming sensory input in the restaurant environment.
👂 Auditory
Music, dishes clattering, conversations, kitchen sounds, crying babies
Tools: Noise-reducing headphones (Loop, Bose, Sony), foam earplugs, wireless earbuds + calming playlist
👁 Visual
Bright lighting, screens, movement of staff, visual clutter
Tools: Sunglasses, baseball cap, booth seating facing wall
🤲 Tactile
Booth vinyl (sticky/cold), napkin texture, unfamiliar utensils
Tools: Familiar clothing layer, seat cushion, preferred utensils from home
👃 Olfactory
Cooking smells, cleaning products, perfumes
Tools: Scented cloth (calming essential oil), seating away from kitchen
🏋️ Proprioceptive
Need for movement input, can't sit still
Tools: Resistance band under table (push feet against), textured seat cushion, squeeze fidget
Many adults use sensory accommodations — sunglasses, ANC headphones, noise-cancelling earbuds. Frame to the child: "These headphones help your brain hear just our family, not everyone in the restaurant."
💰Price: ₹500–3,000 | Budget: foam earplugs ₹20–₹50 for immediate noise reduction
PMC11506176 — Sensory integration intervention meets evidence-based practice criteria for ASD. DOI: 10.3389/fnint.2020.556660 — Neurological basis of sensory tools for environmental adaptation.

🟣 Material 5 of 9
Boundary / Spatial Tools
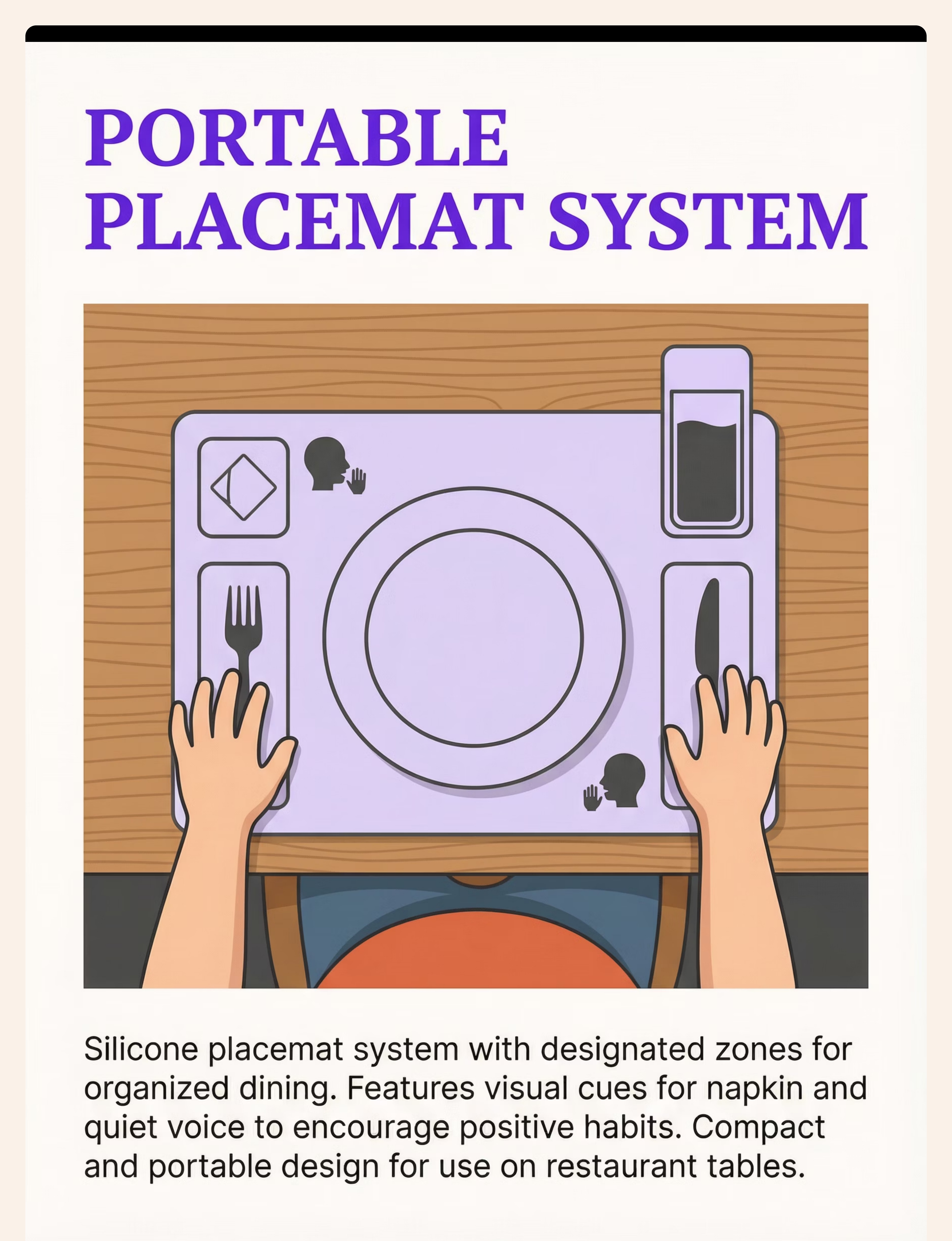
MATERIAL 5: Portable Placemat System
Defining space and expectations — Clear spatial boundaries prevent accidental spills. And stop the nagging.
What It Is
A portable silicone or laminated placemat that defines the child's personal dining space, indicates where items go (plate, drink, utensils), and optionally includes visual behaviour reminders — all within a format that rolls up and travels in a bag.
Why It Works
Restaurant tables present spatial chaos: Where does my plate go? Where does my drink go? What's my sibling's space? For children with impulsivity, poor body awareness, or motor coordination differences, unclear boundaries produce accidental spills and cross-boundary behaviour that triggers negative feedback cycles.
The placemat externalises the rules. The parent stops repeating "keep your hands in your space" because the mat shows it. External cues replace internal reminders — reducing parent-child conflict and placing the instruction in the environment, not the relationship.
Placemat Zone Design
- DRINK ZONE: Upper right corner (away from dominant hand, away from elbow swing radius)
- PLATE ZONE: Centre circle
- UTENSIL ZONES: Left (fork) | Right (knife/spoon)
- ACTIVITY ZONE: Bottom-left corner (keeps activity items in defined space)
- Optional icons: Napkin in lap | Inside voice | Stay in seat
Implementation
- Introduce at home for 2–3 meals to establish familiarity
- Bring to restaurant — familiar object in unfamiliar environment provides grounding
- Child helps place the mat — first step of settling-in ritual
- Praise use of zones ("Your drink is in its spot — great work!")
💰Price: ₹300–800 (silicone, reusable) | ₹0 (laminated A4 paper with drawn zones)
Occupational therapy spatial boundary research + ABA antecedent strategy: Environmental cues that clarify expectations reduce problem behaviour without verbal prompting.

📋 Material 6 of 9
First-Then | Visual Schedules
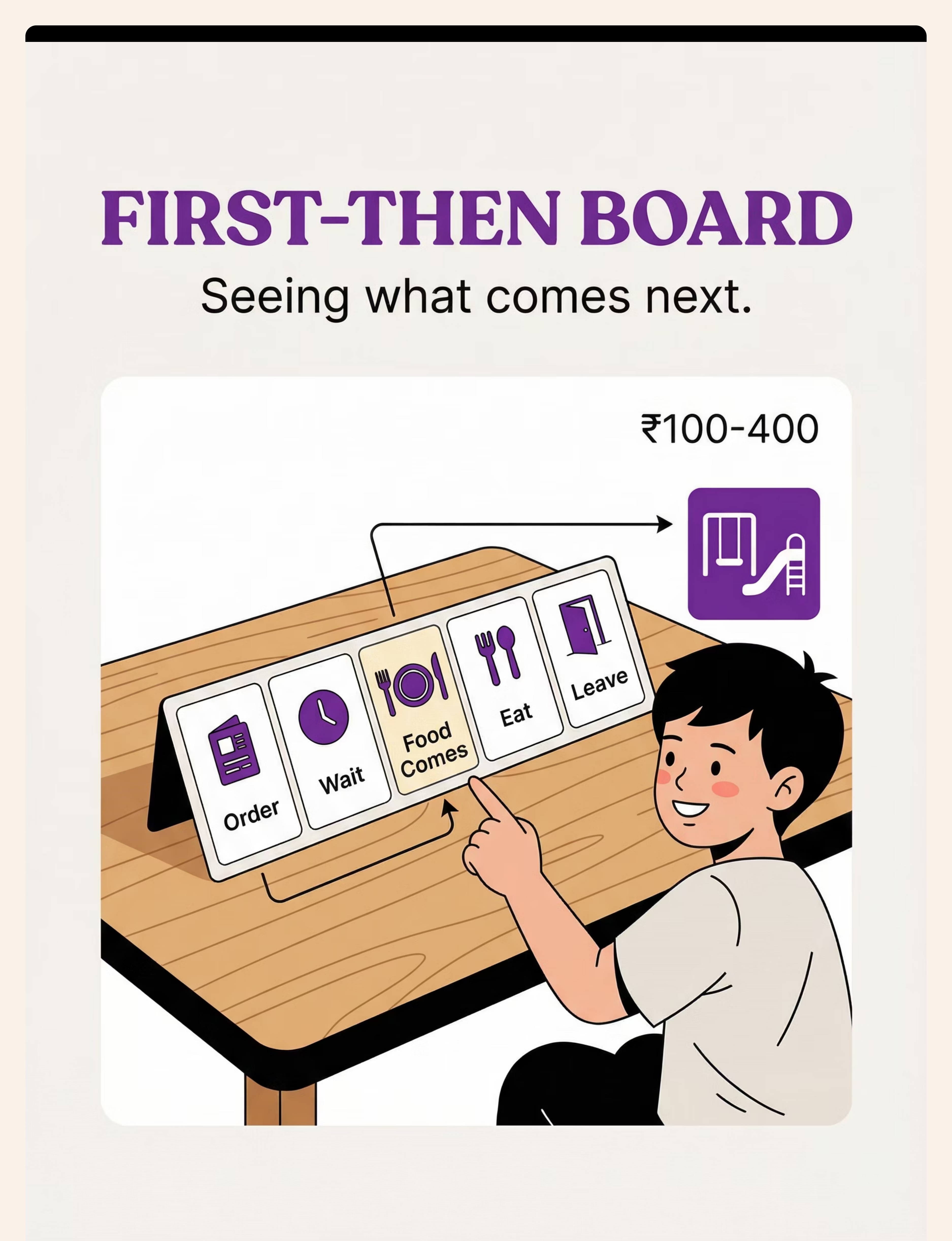
MATERIAL 6: First-Then Board
Seeing what comes next — "First wait, then food." More motivating than "Wait nicely."
A first-then board shows what is happening NOW and what comes AFTER — pairing the current demand (waiting) with its concrete outcome (food, then reward). For children with autism and ADHD, this transforms abstract waiting into a visible sequence with a visible endpoint.
How It Motivates
The first-then structure has been extensively validated in autism and ADHD intervention because it makes the contingency visible: "This hard thing (waiting) leads directly to this good thing (food)." The child can track their position in the sequence and see that every step moves toward an endpoint. The wait is not infinite — it is one step in a sequence with a clear reward.
Progression Tracking
As each step is completed, mark it (check, star, or Velcro "done" cover). The accumulating check marks become visible evidence of progress and a source of pride and motivation.
Reward Integration
Add a post-restaurant reward step if helpful: "Then we go to the park" / "Then we watch a show." The restaurant earns the reward. The child works Toward something concrete.
Size: Index card — small enough for table use, large enough to see clearly.
💰Price: ₹100–400 | ₹0 (drawn on paper)
NCAEP (2020): Visual supports are evidence-based practice for autism. ABA: First-then contingency statements function as establishing operations that increase the reinforcing value of the outcome.
🍱 Material 7 of 9
Feeding Supports
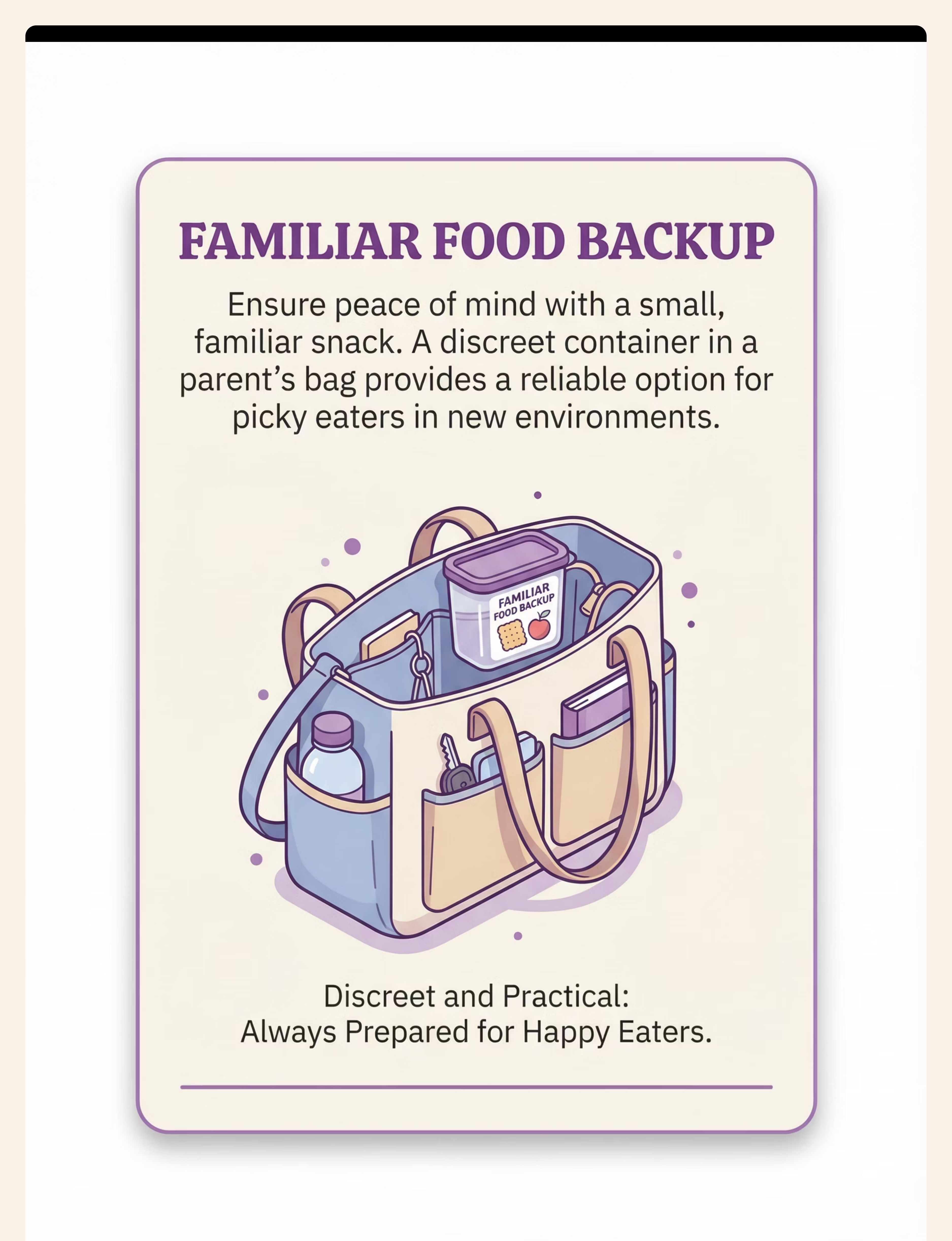
MATERIAL 7: Familiar Food Backup + Session Data Capture
Backup for picky eaters — Separate the challenges. Restaurant behaviour practice can happen even when restaurant food is not yet possible.
What It Is
A small, inconspicuous container — kept in a parent's bag, not displayed on the table — containing foods the child reliably eats. Used only if the child rejects all restaurant food options, ensuring the child can eat something and preventing the hunger + distress spiral that ends many restaurant visits.
Why It Works
Food selectivity is common in autism and sensory processing differences. Restaurant food — even theoretically identical to home food — may look different, smell different, or be presented differently. Forcing food acceptance in the high-stakes public environment produces fight-or-flight responses, not tolerance. The backup food is not defeat. It is strategic problem decomposition: address restaurant behaviour first; build food flexibility separately, in lower-stakes settings.
Implementation
- Pack small, portable, non-perishable preferred foods
- Keep in parent's bag — not visible on the table
- Order from the restaurant for yourself (support the establishment)
- Offer restaurant food first, without pressure
- If rejected: quietly provide familiar backup
- No drama, no shame, no commentary
Restaurant Approach Note
Most restaurants are accommodating of outside food for children with dietary needs. If questioned: "He has dietary restrictions — this is what he can eat." Most staff appreciate honesty and adjust without issue.
Building Food Flexibility Over Time
Separate skill from setting. Build food flexibility in low-anxiety home-based food exposure work. As flexibility increases, bring new foods to restaurants. But at early stages, the backup ensures participation continues even when food acceptance is not yet possible.
📊 DATA CAPTURE — Within 60 Seconds of Leaving
Session Log — J-845 Restaurant Visit 1. Today's restaurant: ___ 2. Total time at table: ___ minutes 3. Materials used: □ Social Story □ Activity Kit □ Timer □ Headphones □ Placemat □ First-Then □ Familiar Food □ Checklist □ Exit Plan 4. Exit required? □ Yes — returned □ Yes — did not return □ No 5. Overall regulation: □ Very challenging □ Challenging □ Manageable □ Good □ Excellent 6. One observation (free text): ___
"60 seconds of data now saves hours of guessing later."
💰Price: ₹50–200 (container cost) | ₹0 (any lidded container)
BACB data collection standards: Continuous measurement as standard ABA practice.

⭐ Material 8 of 9
Reinforcement Menus | Behaviour Checklists
MATERIAL 8: Behaviour Checklist With Reinforcement
Clear expectations, visible progress — What is tracked improves. What is made visible motivates.
What It Is
A small, portable checklist card — laminated for reuse — showing 3–4 specific, achievable restaurant behaviours with a way to mark success (star sticker, check mark, stamp). Linked to a reward at or after the meal.
Why It Works
Vague instructions ("behave nicely") are unactionable. Specific, concrete expectations ("stay in seat," "use inside voice") are observable, trackable, and achievable. The checklist externalises the expectations so the parent is not nagging — the card is the authority. The child tracks their own progress. Visible progress creates motivation and confidence.
Starter Behaviour Set (3–4 Only — Start Small)
- ✅ Stay in seat (or "ask before getting up")
- ✅ Use inside voice
- ✅ Wait nicely during wait time
- ✅ Keep hands in my space
Reinforcement Timing
- Mark behaviours in real time as they are demonstrated (not at end of meal)
- Each mark = immediate verbal praise ("I noticed your inside voice — that's a star!")
- End of meal: count stars, deliver promised reinforcement
Reinforcement Menu — Pinnacle Canon Products
🌟1,800+ Reward Stickers ₹364 — Use as in-session check markers AND take-home reward
🏆Rosette Imprint Reward Jar ₹589 — Accumulate restaurant stars in jar; milestone = special reward
🎁Natural rewards: Dessert, screen time, preferred activity after restaurant
⚠️Critical principle: If the child is consistently NOT earning stars, the expectations are too high. Reduce to 1–2 behaviours and ensure success. A checklist that documents failure produces shame, not behaviour change.
💰Price: ₹50–300 | ₹0 (paper + pen)
Token economy systems: Multiple systematic reviews confirm effectiveness in autism intervention. ABA: Immediate, specific reinforcement delivered within 3 seconds of target behaviour maximises effectiveness.
🚪 Material 9 of 9
Regulation Tools | Break Cards
MATERIAL 9: Exit Strategy & Calm-Down Plan
When it's too much, you're ready — Needing to leave is not failure. It is responsible management of your child's limits. And it sometimes allows you to return.
What It Is
A pre-agreed plan for what happens if the child becomes significantly dysregulated: where to go, who does what, how to calm down, and whether/how to return. Includes a break card the child can use to independently request a break before full dysregulation.
Why It Works
Without an exit plan, every deteriorating restaurant visit becomes a crisis because leaving feels like failure. This desperation causes parents to stay too long in deteriorating situations, making the meltdown inevitable and more severe. Knowing you can leave removes the desperation. A planned exit is faster, calmer, and more likely to allow re-entry than a crisis exit.
The Break Card
🤚"I need a break."
Child shows card to parent → parent responds calmly → take 2-minute break outside. This is not exit — it is a regulation break. Many families return to the table and complete the meal after a 2-minute outdoor break.
Caregiver Role Split (Discuss BEFORE Entering)
👤Caregiver 1: Leaves with child → regulates → assesses → returns or fully exits
👤Caregiver 2: Handles check → boxes food → gathers belongings → follows when ready
Early Warning Signs — Intervene BEFORE Full Dysregulation
Watch for: increased fidgeting beyond baseline | covering ears | voice pitch rising | repetitive vocalisations increasing | refusal to engage with activity kit | eyes darting, scanning for exits
Break vs. Full Exit
🔄BREAK (outdoor, 2 min): Early dysregulation | Child still communicating | Food not yet arrived
🚪FULL EXIT: Significant meltdown in progress | Self-injury | Aggression | Unable to re-enter without major escalation
After a Full Exit
- No shame. No punishment. No "you ruined dinner."
- Get food boxed if possible. Tip generously.
- Attend to the child in the car first.
- Debrief when calm: "What was hard? What could we do differently next time?"
Every restaurant attempt — even one that ends in the parking lot after 10 minutes — is data and practice. You are building something. It takes as long as it takes.
💰Price: ₹0–200 | ₹0 (index card + permanent marker)
ABA: Antecedent management (exit plan as prevention) is more effective than consequence management (responding to meltdown). Functional escape as a communication response.
📊 Progress Arc
15% — Beginning
Weeks 1–2: You Are Planting. You Are Not Yet Harvesting.
✅ What Progress Actually Looks Like at This Stage
- Child tolerates entering the restaurant without immediate meltdown
- Child remains at table for 10–15 minutes with full support deployed
- Child uses one sensory tool without protest
- Social story preview reduces pre-outing anxiety (you may notice this at home, before leaving)
- Child accepts activity kit as a restaurant routine
❌ What Is NOT Progress Yet
- Tolerating 45+ minutes without breaks (too early)
- Eating restaurant food without backup (too early)
- Reduced support toolkit (too early — this is maximum-support phase)
- No sensory overwhelm (environment is still challenging)
Your Role in Weeks 1–2
- 🎯 Maximum preparation (social story daily)
- 🎯 Maximum support (all tools deployed)
- 🎯 Minimum duration targets (leave before dysregulation — always)
- 🎯 Maximum celebration of any participation
If your child tolerates the restaurant for 3 minutes longer than last week — that is real, measurable neurological progress. Neural pathways are forming. The nervous system is beginning to associate "restaurant" with "manageable" rather than "overwhelming." You cannot see this — but it is happening.
PMC11506176 — Intervention outcomes emerge across 8-12 week timelines. Early phase indicators focus on tolerance and participation, not skill mastery.

📊 Progress Arc
40% — Consolidating
Weeks 3–4: The Neural Pathways Are Forming. Watch for These Signs.
By weeks 3 and 4, something is beginning to shift beneath the surface. Repeated structured exposure is doing exactly what neuroscience predicts — synaptic pathways are strengthening, and the restaurant environment is becoming incrementally more familiar and therefore less threatening to your child's nervous system.
🧠 Anticipates the Activity Kit
Child mentions the activity kit before leaving home — "Don't forget my restaurant bag" — indicating that the routine is becoming internalised and anticipated positively.
🧠 Extended Tolerance
Child tolerates 20–25 minutes at the table with moderate support. The duration target is expanding naturally.
🧠 Timer Accepted as Routine
Child accepts the visual timer as a normal part of the restaurant experience, no longer questioning or resisting it.
🧠 Reduced Pre-Outing Anxiety
Fewer protests about going. The pre-restaurant anxiety is beginning to de-escalate as predictability builds.
🧠 Spontaneous Positive Behaviour
Child attempts one new restaurant behaviour spontaneously (using napkin, saying please to server) — an early sign of social learning.
🌱Generalisation seeds: The child may begin applying restaurant skills in other waiting contexts — doctor's office, car ride, queue at the bank. This is the first evidence that the skills are becoming part of their repertoire, not just supported behaviours.
You may notice you are dreading restaurant outings less. That change in your nervous system also matters.
Neuroplasticity: Synaptic strengthening through repeated structured input follows predictable timelines in paediatric populations.

📊 Progress Arc
75% — Approaching Mastery
Weeks 5–8: Mastery Is Not Perfection. It Is Consistent, Manageable Participation.
✅ Duration
Tolerates 35–45 minutes at the restaurant with moderate support
✅ Waiting
Waits through the food-arrival period using activity kit with minimal prompting
✅ Sensory Tools
Uses 2–3 sensory tools independently (puts on headphones without being prompted)
✅ Sequence
Follows restaurant sequence with first-then board reference, not verbal reminders
✅ Behaviour Checklist
Consistently achieving 3+ of 4 target behaviours per visit
✅ Stability
No full exit required in last 3 consecutive visits
🏆Mastery Badge: "Restaurant Readiness — Stage 1 Unlocked" Your child can participate in basic restaurant dining with support toolkit. Next stage: Gradual support fading toward independent restaurant participation.
When to move forward: Stage 1 mastery → Begin fading one support at a time (first remove familiar food backup, then reduce activity kit, then fade first-then board). Do not remove sensory tools until explicitly advised by your OT.
PMC10955541 — Meta-analysis across 24 studies confirms measurable skill outcomes. Mastery criteria derived from BACB behavioural measurement standards.
You Did This. Your Child Grew Because of Your Commitment.
Weeks ago, your family avoided restaurants entirely. Today, you are dining out — with preparation, with tools, with strategy. This is not luck. This is the result of showing up consistently, learning your child's nervous system, and refusing to let isolation be the default.
1
🏆 Sensory Mastery
You learned your child's sensory profile well enough to curate a toolkit that works.
2
🏆 Nervous System Prep
You prepared your child's nervous system with social story preview before every visit.
3
🏆 Wait Management
You created a wait-management strategy that transforms the hardest 20 minutes into something manageable.
4
🏆 Clear Expectations
You defined expectations clearly enough that your child could actually succeed — not just try.
5
🏆 Life Skill Built
You built a community participation skill that will serve your child for life — in every restaurant, everywhere.
🎉 Tonight: Name It
"We did a full restaurant meal. That is hard, and we did it." Say it together.
📸 Document It
Photo at the restaurant table, smiling. Write the date on it. This is a milestone worth keeping.
💬 Share It
Share in your parent community — your progress encourages other families who are still in Week 1.
"What was the moment in this restaurant journey when I first believed we could actually do this?"
Trust Your Instincts. If Something Feels Consistently Wrong, Pause and Ask.
🚨 Distress Is Increasing, Not Decreasing
Despite 8+ weeks of consistent strategy use — may indicate unaddressed sensory processing needs requiring OT evaluation.
🚨 Self-Injurious Behaviour
Appears or increases in restaurant settings — requires immediate functional behaviour assessment (FBA) by a BCBA.
🚨 Food Restriction Worsening
Fewer safe foods, increased distress around food in all settings — requires feeding therapy evaluation beyond the materials in this series.
🚨 Anxiety Generalising
Anxiety about restaurants is spreading to anxiety about leaving home at all — may indicate anxiety disorder requiring clinical assessment beyond behavioural strategies alone.
🚨 Significant Regression
Child shows significant regression after apparent progress — possible environmental stressor, medical issue, or sensory threshold change — warrants teleconsultation.
🚨 Dramatically Different Behaviour
Other caregivers (school, grandparents) report dramatically different behaviour — inconsistency indicates function-based assessment needed.
WHO NCF Progress Report (2023): Primary health care as platform for early identification and referral pathways.
You Are Not Done. You Are at a Waypoint in a Much Larger Journey.
J-845 is one episode in a carefully sequenced series of community participation techniques. Each builds on the skills developed in the previous, and the materials you have gathered for restaurant behaviour will serve you in every technique that follows.
J-843: Public Places
Public place behaviour — foundational community access
J-844: Waiting in Lines
Prerequisite waiting tolerance skills — your starting point
J-845: Restaurant ← YOU ARE HERE
Integrated community participation — the current challenge
J-846: Grocery Store
Next community participation challenge — apply the same framework
J-847: Mall & Shopping
Advanced community participation — full sensory kit + behaviour plan
Branch pathways based on your child's primary challenge: If sensory overwhelm is primary → Domain A: Sensory Toolkit Building → Noise Sensitivity Techniques If waiting is the primary challenge → Domain B: Waiting & Transitions → Visual Schedule Deepening If food selectivity is primary → Domain E: Feeding Therapy → Food Exposure Hierarchy
Long-term developmental goal: Full community participation readiness — ability to access public spaces (restaurants, shops, transport, events) with age-appropriate independence and minimal support.
You Already Have Materials for Some of These. Explore What's Nearby.

J-844 | Waiting in Lines
🟡 Core
Visual Timers + Activity Kit. The prerequisite technique — foundational waiting tolerance skills directly transfer to restaurant behaviour.

J-846 | Grocery Store Behaviour
🟡 Core
Visual Schedules + Sensory Tools. Apply the same framework you have already built to the next community environment.

J-843 | Public Place Behaviour
🟢 Intro
Social Stories + Break Cards. The introductory technique — great for families just beginning their community participation journey.

J-847 | Mall & Shopping Behaviour
🔴 Advanced
Full Sensory Kit + Behaviour Plan. The advanced challenge — for families who have built confidence through J-845 and J-846.

G-305 | Food Selectivity & Picky Eating
🔴 Advanced
Feeding Therapy Materials. If food selectivity is the primary barrier to restaurant participation, this domain addresses it directly.
🏠 Domain J — Daily Living Skills & Community Participation
This Technique Is One Piece of a Much Larger Picture.
How Other Domains Connect to Restaurant Success
- Domain A (Sensory): Without sensory regulation tools, the restaurant is intolerable — foundational to everything
- Domain D (Behaviour): Without flexible behaviour skills, unexpected events cause crisis
- Domain I (Social): Restaurant success contributes directly to social participation skills
- Domain L (Self-Care): Dining independence is a foundational self-care skill with lifelong impact
GPT-OS® AbilityScore® Connection
GPT-OS® tracks your child's readiness across all 12 domains via AbilityScore® — a patented developmental score (0–1000) that shows exactly where your child is on every domain and what the priority intervention should be.
WHO NCF (2018): Five nurturing care components require holistic monitoring. UNICEF 2025 indicators track 42 child development markers per country.
From the Pinnacle Clinical Notes. Real Journeys. Measured Outcomes.
Story 1 — The Eighteen-Month Pause
Before: A family with an 8-year-old with ASD and sensory processing differences had stopped all restaurant outings after 18 consecutive visits ended in meltdown. The child could not tolerate the ambient noise, rejected all restaurant food, and could not wait more than 5 minutes without dysregulation.
The intervention: Weeks 1-2: Social story with photos of the specific restaurant + noise-reducing headphones + 10-minute maximum visits to a quiet outdoor café. Weeks 3-4: Gradual duration extension + activity kit introduced + familiar food backup. Weeks 5-8: First-then board added + behaviour checklist with sticker rewards.
After (Week 8): 35-minute restaurant visits, headphones worn but child engaged with family, familiar food backup used once in last 4 visits, no meltdowns requiring exit in 5 consecutive visits.
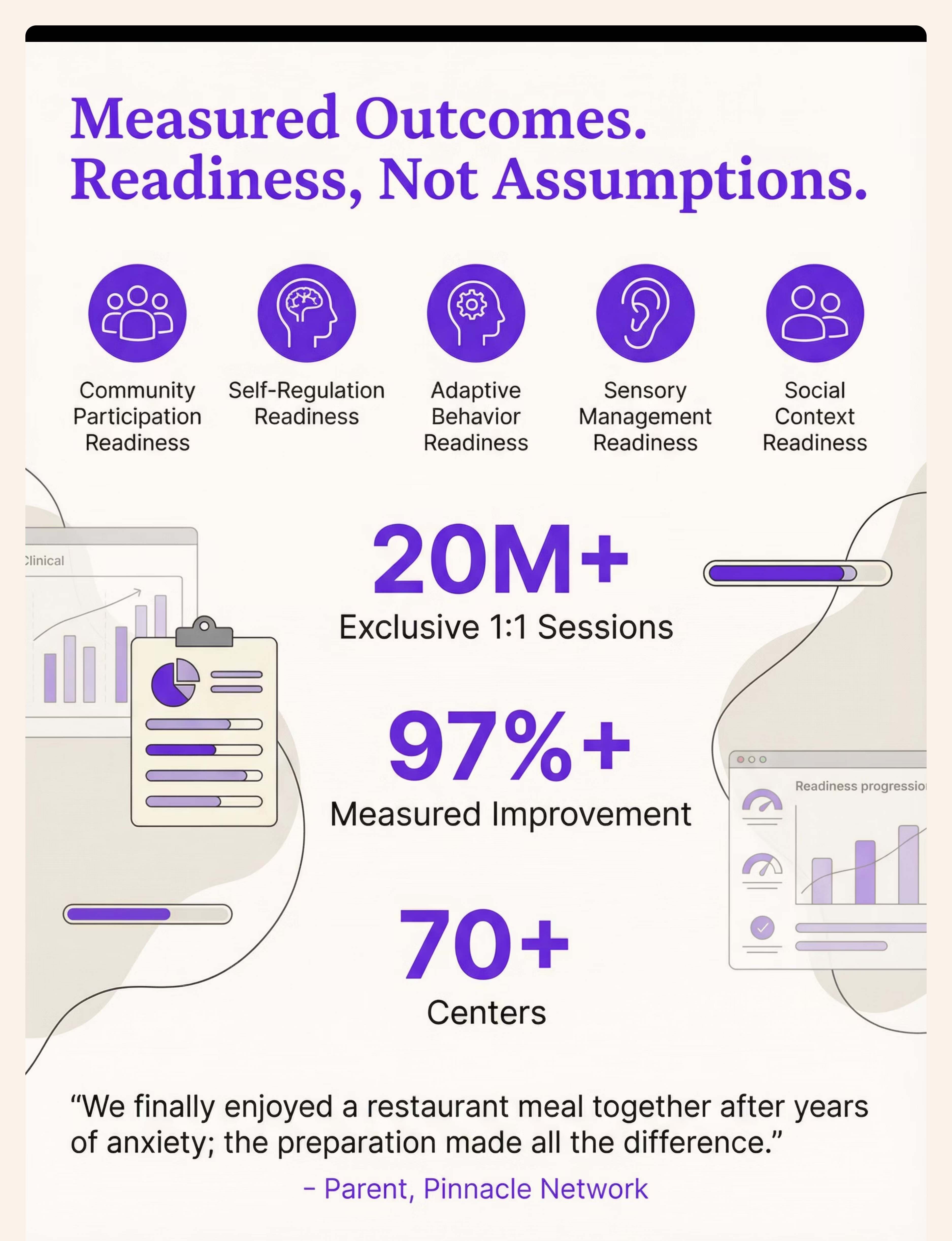
"We finally had a birthday dinner at a real restaurant. Not at home. Not takeout. A restaurant, with candles, with my mother-in-law who had been worrying about him for three years. I cried on the way home. Good tears, for the first time in a very long time." — Parent, Pinnacle Blooms Network (Hyderabad centre)
Story 2 — The ADHD Wait
Before: A 7-year-old with ADHD could not tolerate any restaurant wait. He would be under the table within 4 minutes, touching neighbouring diners' food, and requiring physical restraint to stay in the booth. The family had been asked to leave two restaurants.
The intervention: OT-designed activity kit with fidgets matched to his proprioceptive seeking profile. Visual timer set for 3-minute intervals with a small edible reinforcer at each interval. Placemat defining his physical boundary. First-then board with playground immediately after meal.
After (Week 6): 40-minute restaurant visits, activity kit used throughout wait, placemat stops the majority of reaching-across behaviour, timer check-ins replace constant verbal prompting.
"His prefrontal cortex was not failing him — we were failing to provide the external scaffolding his developing brain needed. Once we put the external structure in place, his behaviour followed." — BCBA, Pinnacle Blooms Network
Individual results vary based on child profile, diagnosis, consistency of implementation, and environmental factors. These narratives represent real clinical trajectories from the Pinnacle Network. Statistics represent aggregate outcomes across 20M+ 1:1 sessions.

Isolation Is the Enemy of Adherence. You Need a Village, Not Just a Technique.
WhatsApp Community
Community Participation & Restaurant Skills — Join other Pinnacle families working on the same challenge. Share strategies, celebrate wins, troubleshoot setbacks.
Online Forum
pinnacleblooms.org/community — Moderated discussion space for parents across all domains. Sub-forum: Daily Living Skills.
Local Parent Meetups
Organised by Pinnacle centres — monthly gatherings of parents navigating similar challenges in your city.
Peer Mentoring
Connect with a parent who has completed this technique and can share their experience directly. Request a peer mentor via the helpline.
"Over 1,000 individuals from 111 countries contributed to the WHO Nurturing Care Framework because community knowledge is irreplaceable. Your experience — your child's progress — is knowledge that helps every family who comes after you."
WHO NCF Community Engagement Principles | Parent support network research: social connection improves home intervention adherence.
Home + Clinic = Maximum Impact
These materials are most powerful when paired with professional guidance.
🟣 Occupational Therapist
Sensory profile assessment, toolkit customisation, and graduated exposure planning. OT leads the sensory integration component.
🟣 BCBA (ABA)
Behaviour checklist design, reinforcement system development, and functional behaviour assessment if needed.
🟣 Special Educator
Social story development, visual schedule design, and school-based generalisation support.
🟣 NeuroDev Paediatrician
Diagnostic confirmation, medication consultation if applicable, and prognosis guidance across domains.
Teleconsultation
📱 Book online teleconsultation for remote families — available within 48 hours, regardless of your location across India or internationally.
Primary Contact
📞FREE National Autism Helpline: 9100 181 181
🌐 pinnacleblooms.org
Available 24×7 in 16+ languages
"Primary health care is the key platform for reaching all families with essential child development interventions." — WHO NCF Progress Report 2018-2023 | PMC9978394

Deeper Reading for the Curious Parent. Every Claim on This Page Has a Source.
1. PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm sensory integration intervention meets evidence-based practice criteria for children with ASD. PMC11506176 | Children journal
2. Meta-analysis, World J Clin Cases (2024)
24 studies: Sensory integration therapy effectively promotes social skills, adaptive behaviour, sensory processing, and motor skills. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
3. NCAEP Evidence-Based Practices Report (2020)
Visual supports, social narratives, and behaviour-specific interventions classified as evidence-based practices for autism across 27 studies reviewed.
4. Indian Paediatrics RCT — Padmanabha et al. (2019)
Home-based sensory interventions in Indian paediatric populations: significant measurable outcomes. Indian J Pediatr | DOI: 10.1007/s12098-018-2747-4
5. WHO Nurturing Care Framework (2018)
Five nurturing care components framework — underpins all community participation intervention design. nurturing-care.org | WHO/UNICEF CCD Package 2023
Oxford CEBM Evidence Grading: Evidence for materials in J-845 ranges from Level I (systematic review — sensory integration, visual supports) to Level II (individual RCTs — social stories, behavioural support systems).
Your Session Data Doesn't Disappear. It Makes the System Smarter for Every Child Like Yours.
What GPT-OS® Learns from J-845 Data
- 📊 Which materials produced tolerance improvement vs. which showed no effect for this child's profile
- 📊 How duration tolerance is trending across sessions (slope of the learning curve)
- 📊 Which sensory tools are most effective for this child's specific sensory profile
- 📊 Whether food flexibility is improving alongside behaviour improvement
Privacy and Protection
- 🔒 All data stored with enterprise-grade encryption
- 🔒 Individual data never shared with third parties without explicit consent
- 🔒 Aggregate anonymised data contributes to population-level recommendations
- 🔒 DPIIT Recognised Startup | MSME Registered | All applicable Indian data protection standards
"Your data helps every child like yours. When 10,000 families track J-845 sessions, GPT-OS® learns which combinations of materials are most effective for which diagnostic profiles — and automatically adjusts recommendations for the 10,001st family."
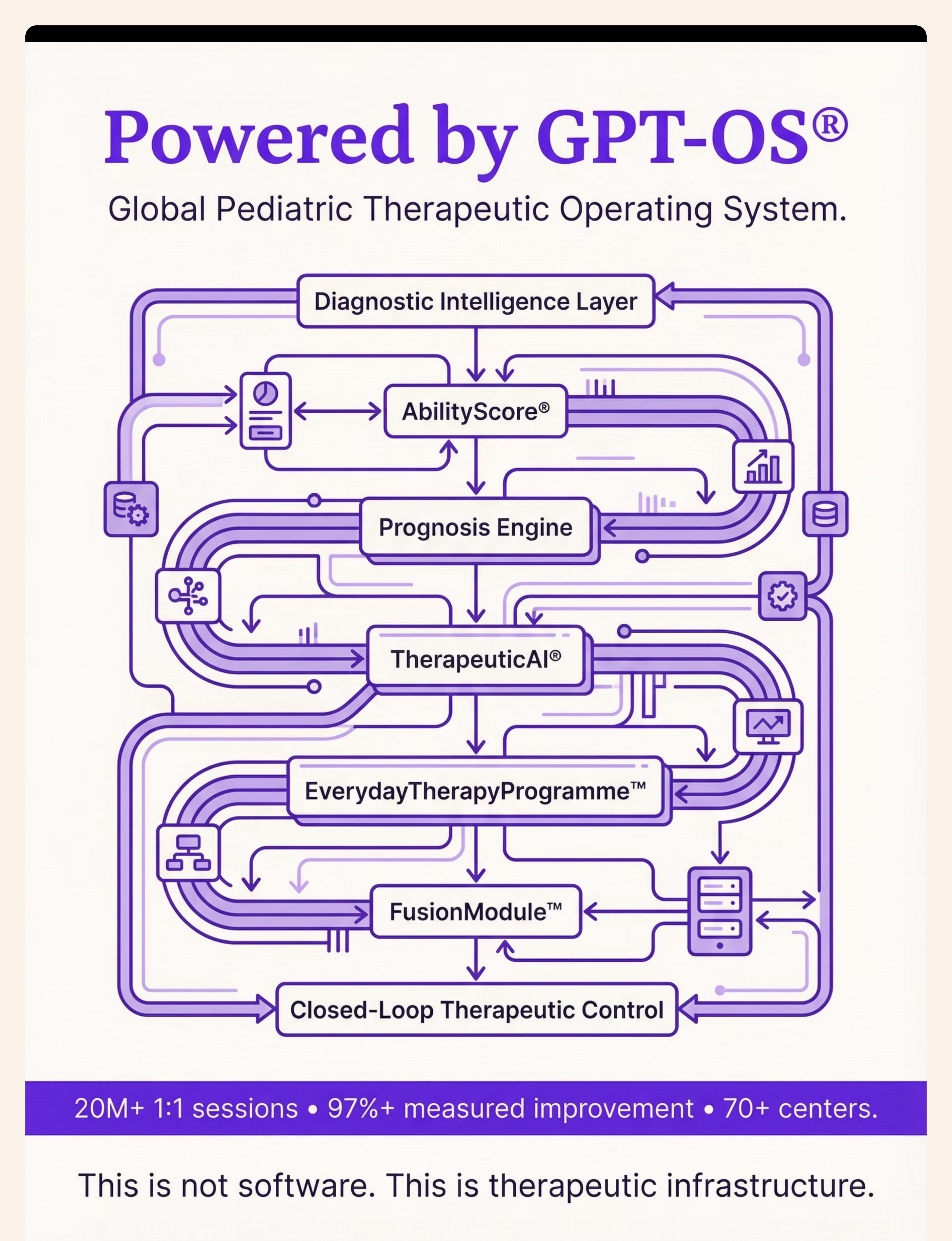
20M+
Exclusive Sessions
1:1 therapy sessions tracked and analysed
97%+
Measured Improvement
Across tracked intervention programmes
70+
Centres
Across India serving families in 70+ countries

Watch the Reel. See the Materials in Action.
🎬 Reel J-845
Daily Living Skills & Community Participation | Episode 845 of 999
About this reel: This 60-second reel walks through all 9 materials with a therapist guide and visual demonstrations of each material in a restaurant context. It is the companion visual content to this technique page — same content, different modality.
"In 60 seconds, I want to show you that restaurant dining for children with autism and ADHD is not impossible — it is under-supported. These 9 materials change that." — Pinnacle Blooms Consortium OT + ABA Team
Multi-Modal Learning Note
Research confirms that combining text/visual reading (this page) with video modelling produces significantly better parent skill acquisition than either modality alone. Watch the reel after reading for consolidation, or before for orientation.
Domain Connection
🎬 Series: Daily Living Skills & Community Participation
🏠 Domain J — Community Participation | COM-REST
Part of the Pinnacle Blooms 999 Reels Master — J-845 direct mapping confirmed.
NCAEP (2020): Video modelling is evidence-based practice for autism. Multi-modal learning improves parent skill acquisition significantly over single-modality exposure.
Consistency Across Caregivers Multiplies Impact
If only one person knows this, the strategy works once a week. If everyone knows it, it works every day.
Share This Page
📱WhatsApp: Pre-written message: "Found this for [child's name] — 9 materials that help with restaurants. Really practical. Check it out: techniques.pinnacleblooms.org/community-participation/restaurant-behavior-J-845"
📧 Share via Email | 🔗 Copy Link
📄 Downloadable Family Guide PDF
A simplified, printable version of the core protocol for grandparents, school staff, babysitters, and other caregivers. One page. Plain language. Step-by-step.
"Explain to Grandparents" Version
"We're working on helping [child's name] manage restaurants better. Before we go: we read a little story about what will happen. At the restaurant: we bring a small activity bag, a timer, and noise-reducing headphones. These help [his/her] brain stay calm in a busy place. Please don't take away the headphones or the activity bag — they are therapeutic tools, not toys or tech addiction. If you have questions, please ask us, not [child's name]."
Teacher/School Communication Template
Available on request from your Pinnacle centre. Includes context, strategy summary, and classroom generalisation suggestions.
"The WHO Care for Child Development Package emphasises multi-caregiver training as critical for intervention generalisation and maintenance." — PMC9978394
The Questions Most Parents Ask. Answered Before You Need to Ask Them.
Q1: How many of the 9 materials should I start with?
Start with 3: the social story, one sensory tool (headphones or earplugs), and the exit plan. These address the three most common restaurant failure points (unpredictability, sensory overwhelm, and crisis management). Add remaining materials gradually as you assess what's needed for your child.
Q2: My child refuses to wear headphones. What do I do?
Introduce headphones at home, not at the restaurant. Put them on during a preferred activity (favourite show, music) for 30 seconds, then remove with praise. Build duration over 1–2 weeks. Alternatively, start with foam earplugs (less intrusive) or a baseball cap (reduces visual input while the auditory solution is being built).
Q3: Is using a screen/tablet at the restaurant "cheating"?
No. Screen time as a wait-time activity is a legitimate therapeutic tool, not a parenting shortcut. The goal is a successful outing — not performative screen-free parenting. Use screens without shame while other strategies build. Gradually shift toward non-screen activities as tolerance increases.
Q4: The restaurant staff stared at us / asked us to leave. What do I do?
You are not required to explain your child's diagnosis to anyone. A brief, confident statement — "My child has sensory processing differences; we have tools to support him" — satisfies most enquiries. Restaurants that are hostile to families with special needs are not the right restaurants for this stage of training. Choose sensory-friendly options at off-peak times.
Q5: We tried once and it failed completely. Should we try again?
Yes — but with analysis, not repetition. What specifically failed? Sensory overwhelm → add tools. Wait too long → shorter visit or faster restaurant. Food refusal → bring backup. Every failed attempt contains the prescription for the next attempt's success.
Q6: How long before we see real improvement?
Weeks 1-2: tolerance of entry without meltdown. Weeks 3-4: 20+ minute visits with tools. Weeks 5-8: consistent 35-40 minute visits. These are typical trajectories — individual variation is significant.
Q7: My child has both autism and ADHD. Which materials matter most?
For the combined profile: sensory toolkit (OT-driven), activity kit (ADHD waiting support), visual timer (ADHD), and first-then board (autism predictability + ADHD motivation) are the highest-yield combination. BCBA + OT should ideally co-design your approach.
Q8: Is this approach used in Pinnacle therapy sessions?
Yes. All 9 materials are integrated into Pinnacle's EverydayTherapyProgramme™ under GPT-OS®'s FusionModule™, which coordinates OT, ABA, SLP, and SpEd contributions for each child's community participation goals. Home use mirrors and extends clinic work.

You Have Everything You Need. Your Family's Restaurant Story Is About to Change.
🚀 Start This Technique Today
Begin your personalised J-845 implementation with guided support through GPT-OS®. Launch your first session with a complete kit and a clear plan.
📞 Book a Consultation
Talk to a Pinnacle OT or BCBA within 48 hours. Personalised guidance for your child's specific profile and starting point. Call 9100 181 181.
→ Next Technique: J-846
Explore Grocery Store Behaviour — apply the same framework to the next community participation challenge when you're ready.
🏅Validated by the Pinnacle Blooms Consortium — This content is reviewed and approved by a multi-disciplinary consortium of paediatric specialists. 🟣 OT • 🟣 SLP • 🟣 ABA/BCBA • 🟣 SpEd • 🟣 NeuroDev Paediatrics • 🟣 CRO
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centres Across India
70+
Countries Served
Preview of 9 materials that help with restaurant behavior Therapy Material
Below is a visual preview of 9 materials that help with restaurant behavior therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

The Pinnacle Promise
🏅PINNACLE BLOOMS NETWORK® Multi-Disciplinary Paediatric Therapeutic Consortium OT • SLP • ABA/BCBA • SpEd • NeuroDev • Paediatrics • CRO • Mothers & Families
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® exists to transform the home of every family navigating paediatric developmental challenges into a proven, scientific, 24×7, personalised, multi-sensory, multi-disciplinary integrated therapy environment — powered by GPT-OS®, validated by 20M+ therapy sessions, and built from the wisdom of thousands of clinicians and millions of families.
Medical Disclaimer: This content is educational. It does not replace individualised assessment and treatment from licensed professionals. Children with significant behavioural challenges in community settings may benefit from occupational therapy, behavioural intervention, or other professional support. If your child's behaviour significantly limits community participation despite consistent strategy use, seek evaluation from qualified professionals. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | |
MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 |
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Unauthorised reproduction prohibited.
← Return to Top
The Recognition Moment — Card 01
→ Next Technique
J-846 — Grocery Store Behaviour
🏠 Browse All
Community Participation Techniques — techniques.pinnacleblooms.org
pinnacleblooms.org | techniques.pinnacleblooms.org | care@pinnacleblooms.org | Pinnacle Blooms Network® | GPT-OS® Content Engine | J-845 | February 2026