
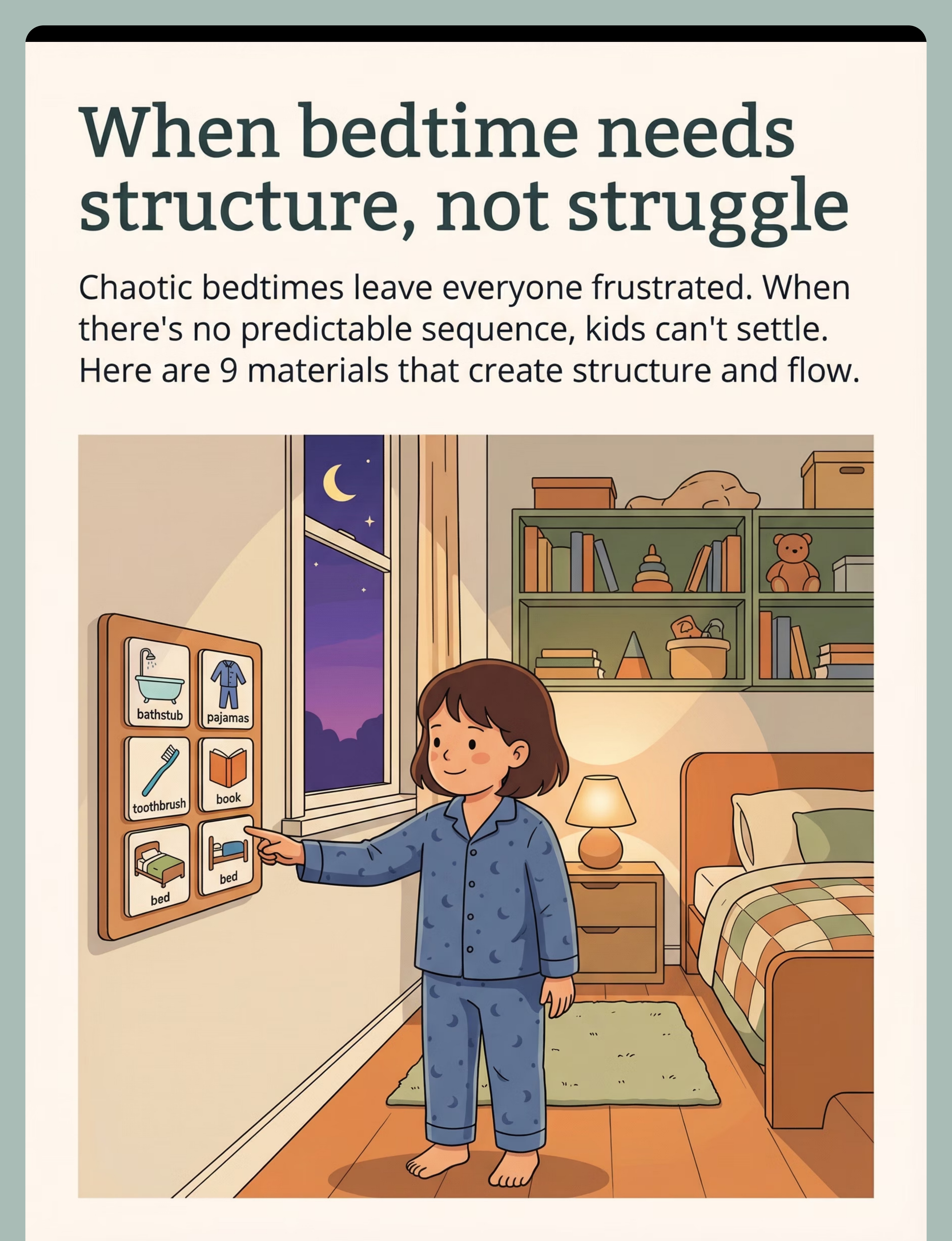
9 Materials That Help With Sleep Routine
Evidence-based bedtime structure for children ages 2–12. Visual boards, timers, progress trackers, calm-down kits, and more — engineered by India's largest therapy consortium.
D-449
Sleep / Self-Care Series
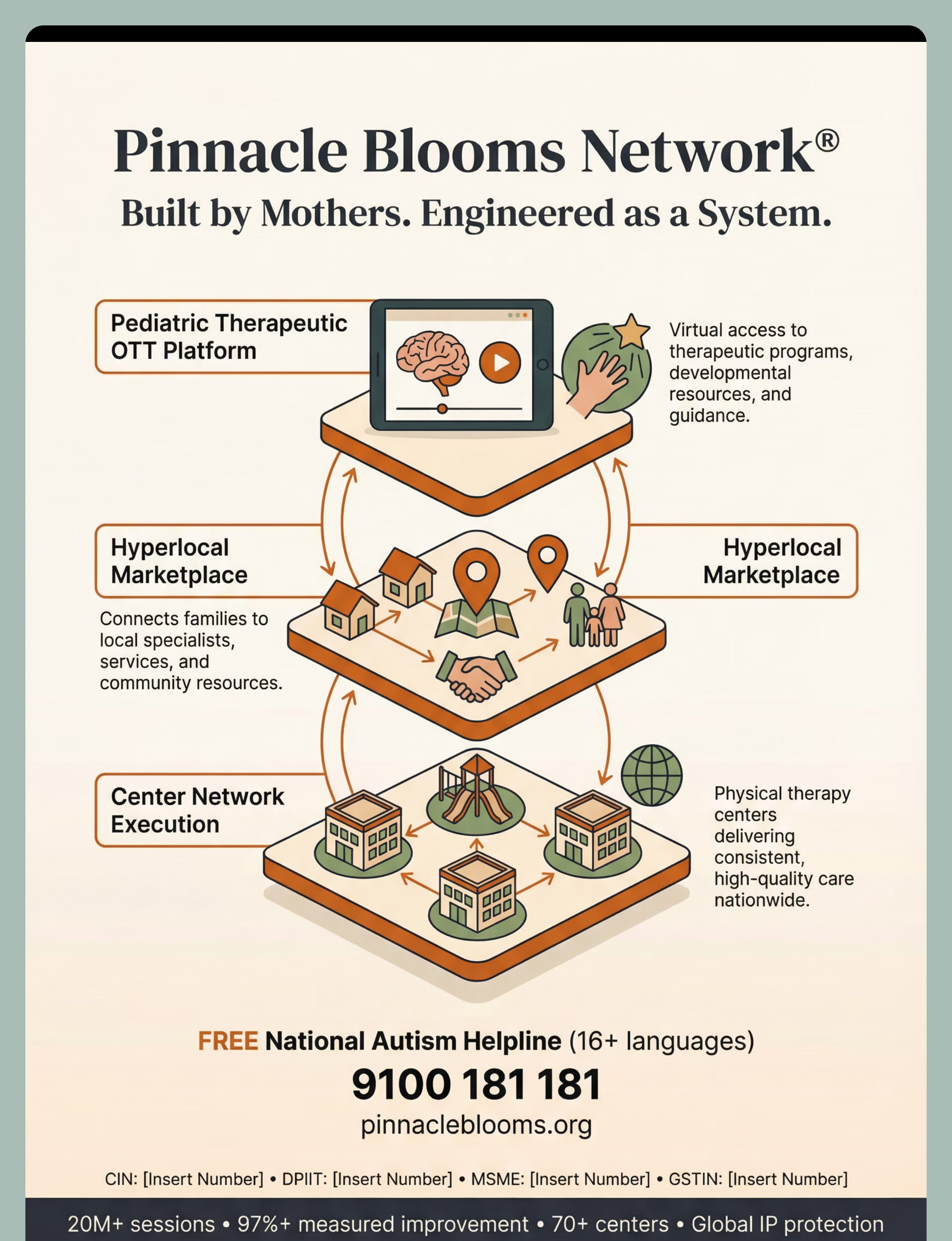
Pinnacle Blooms Network®
It's 10 PM again. Everyone's exhausted.
The bedtime routine that was supposed to take 30 minutes somehow took 90. Again. Chaotic evenings without predictable structure leave children dysregulated and parents depleted. Sleep Routine Establishment is the bridge — and it starts with the right materials in place.
"You are not a disorganized parent. Your child's nervous system needs external structure to do what yours does automatically." — Pinnacle Blooms OT Consortium
⬡ SLEEP ROUTINE ESTABLISHMENT — D-449
Visual Structure + Time Architecture + Environmental Design → Predictable Bedtime Flow
WHO Nurturing Care Framework (2018): "Consistent, responsive caregiving routines in the first 12 years establish lifelong self-regulation capacity."
📞FREE National Autism & Development Helpline: 9100 181 181 | Available 24×7 | 16+ Languages
Visual Structure + Time Architecture + Environmental Design → Predictable Bedtime Flow
WHO Nurturing Care Framework (2018): "Consistent, responsive caregiving routines in the first 12 years establish lifelong self-regulation capacity."
📞FREE National Autism & Development Helpline: 9100 181 181 | Available 24×7 | 16+ Languages

You Are Not Alone: The Numbers
When bedtime has no predictable structure, the nervous system cannot downshift into sleep-ready state. This is physiologically true — not a parenting failure. The circadian system learns from repeated, consistent cue sequences. Millions of families across India and 70+ countries are on this exact same journey.
50–80%
Children with Autism
experience significant sleep difficulties. Cortesi et al., J Sleep Research 2010
44%
Indian Children Ages 2–12
lack a consistent bedtime routine. NFHS-5 | Sleep Health India 2023
3×
Faster Sleep Onset
for children with consistent visual bedtime routines. Mindell et al., SLEEP 2015
Across Pinnacle's 70+ centers and 20M+ therapy sessions, sleep routine challenges rank among the top-5 parent concerns in the Occupational Therapy intake assessment. You are not struggling alone.

What's Happening in Your Child's Brain
When bedtime has no consistent sequence, your child's brain does not receive the chemical signal to prepare for sleep. The materials in this guide address three core systems: visual structures cue the SCN, external boards substitute for the immature PFC, and consistent predictability calms the amygdala.
Suprachiasmatic Nucleus (SCN)
The brain's circadian clock. Requires consistent behavioral cues to trigger melatonin release. Without routine cues → clock stays confused.
Prefrontal Cortex
Governs sequencing and self-regulation. In children under 10: still developing. External visual structures substitute for immature PFC.
Amygdala
Threat-detection center. Unpredictable transitions = perceived threat. Predictable routines calm the amygdala before sleep.
This is a wiring difference, not a behavior choice.
Your child's circadian clock learns from repeated behavioral cues — the same bath, the same brush, the same story, the same hug. When those cues vary nightly, the clock stays confused and melatonin doesn't release on time.
The prefrontal cortex is immature in all children under 10, and significantly more so in children with autism or ADHD. Your child literally cannot hold a 7-step sequence in working memory without external support. This is neurology, not defiance.
Frontiers in Integrative Neuroscience (2020) | Jan et al. (2010) | NCAEP (2020)
Where This Sits in Development
The 2–12 year window is the optimal intervention window for permanent routine internalization. Understanding where your child sits on the developmental timeline helps you calibrate expectations and choose the right materials.
0–24 Months
Circadian rhythm emerges; parent-regulated sleep. Sleep routine capacity begins at 12–24 months; protest behaviors peak.
2–4 Years ★
Routine rigidity peak in autism; visual support most powerful here. Highlighted intervention window.
4–6 Years
Emerging self-monitoring; checklist-based routines become effective.
6–8 Years
Independence possible with systematic fading of prompts.
8–12 Years
Audio/timer-based systems replace visual boards for most children.
12+ Years
Internalized routines (if foundations built); adolescent circadian shift begins.
Sleep routine challenges commonly co-occur with: Autism Spectrum Disorder (routine rigidity + transitions) · ADHD (time blindness + sequencing deficits) · Sensory Processing Disorder (environmental sensitivities) · Anxiety (fear of the dark, separation anxiety) · Executive Function Delays (multi-step sequence difficulty)
The Evidence Behind This Technique
Level I Evidence
Systematic Review + Multiple RCTs
Clinically validated. Home-applicable. Parent-proven. Children with consistent nightly routines fall asleep significantly faster, sleep longer, and wake fewer times — regardless of diagnostic status. The routine itself is therapeutic.
Study | Finding | Evidence Level | |
Mindell et al., SLEEP (2015) | Nightly bedtime routine reduced sleep onset by avg 15 mins; improved child mood next day | Level I RCT | |
Cortesi et al., J Child Psychol (2012) | Visual routine supports improved sleep in 78% of children with ASD | Level II RCT | |
NCAEP (2020) | Visual schedules = evidence-based practice for autism across 28 studies | Level I Systematic Review | |
Jan et al., Paediatr Child Health (2008) | Behavioral sleep interventions 94% effective; visual structure cited as key component | Level I Meta-Analysis | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based structured routines showed significant outcomes in Indian pediatric population | Level II RCT |
📞 Questions about your child's sleep profile? FREE Helpline: 9100 181 181

The Technique: What It Is
D-449
Self-Care Series
Ages 2–12
Sleep Routine Establishment
"The Predictable Bedtime System"
A structured, consistent sequence of pre-sleep activities — supported by visual materials, time structures, and environmental design — performed in the same order every night to train the nervous system to prepare for sleep.
How It Works
Externalize the Sequence
Visual board puts the routine on the wall — never in a parent's head. Available regardless of which caregiver is present or how tired anyone is.
Create Time Architecture
Each step has clear time boundaries so transitions are predictable and non-negotiable.
Organize the Environment
Dedicated stations and visual labels ensure nothing derails the sequence mid-routine.
Build Positive Reinforcement
Reward systems motivate cooperative completion night after night.
🏷 Domain: Sleep / Self-Care
OT Primary
ABA Reinforcement
Ages 2–12
Daily Frequency
Home-Executable
Who Uses This Technique
This technique crosses therapy boundaries. Your child's brain doesn't organize by therapy type. At Pinnacle's 70+ centers, every sleep routine case receives a multi-disciplinary FusionModule™ assessment — OT, ABA, SpEd, and NeuroDev in one converged plan.
Occupational Therapy — PRIMARY
OTs assess daily living skills, sensory contributions to bedtime difficulty, and executive function capacity. They design the visual system, evaluate environmental organization, and grade the independence ladder.
Applied Behavior Analysis — SECONDARY
BCBAs design the reinforcement system, conduct functional assessment of resistance behaviors, and fade prompts systematically. They create transition warning protocols and reward chart design.
Special Education — TERTIARY
SpEd specialists adapt visual boards for the child's comprehension level, calibrate first-then language, and train classroom generalization of routine skills.
NeuroDev Pediatrics — ESCALATION
When routine resistance has medical underpinnings. Pediatricians assess for delayed sleep phase syndrome, melatonin dysregulation, co-occurring ADHD, or medication effects on sleep architecture.
What This Targets
This isn't a random bedtime activity. It's a precision instrument targeting 3 developmental layers — from immediate sleep onset to long-term family well-being.
Observable indicator: Child completes 80%+ of routine steps independently within 4 weeks · Child checks visual board proactively by Week 3 · Faster sleep onset → better next-day regulation, attention, and behavior across all domains

9 Materials. One System. Peaceful Bedtimes.
These nine materials form a complete sleep routine system. Each serves a specific therapeutic function — from externalizing the sequence to regulating the nervous system for sleep onset.

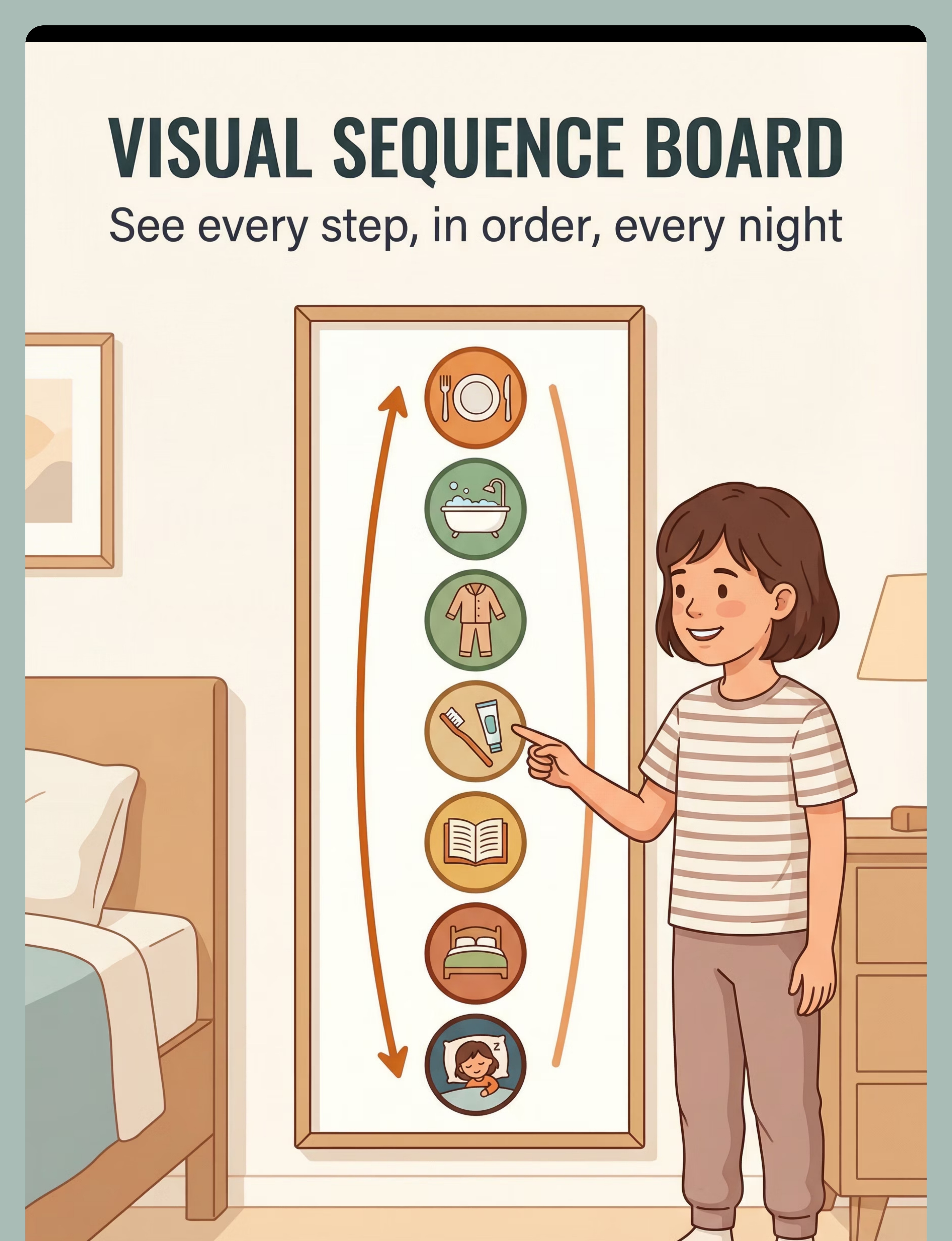
📋 Material 1: Visual Sequence Board
A-4 to A-3 laminated board with 5–8 bedtime sequence picture cards. The anchor of the entire system. ₹200–1,000
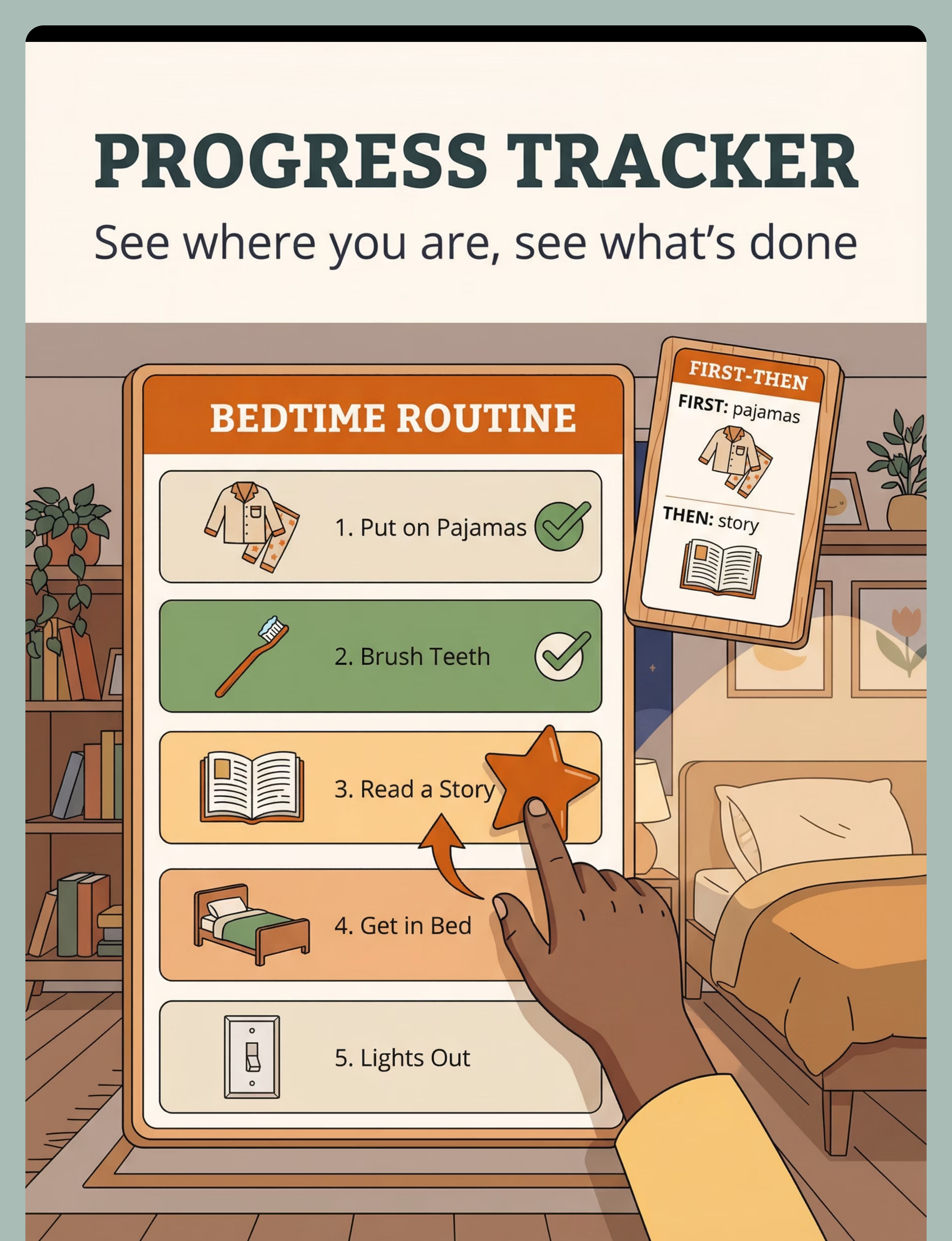
📍 Material 2: Progress Tracker + First-Then Cards
Velcro or magnetic tracker that advances through bedtime steps. Includes First-Then card pairs. ₹100–500

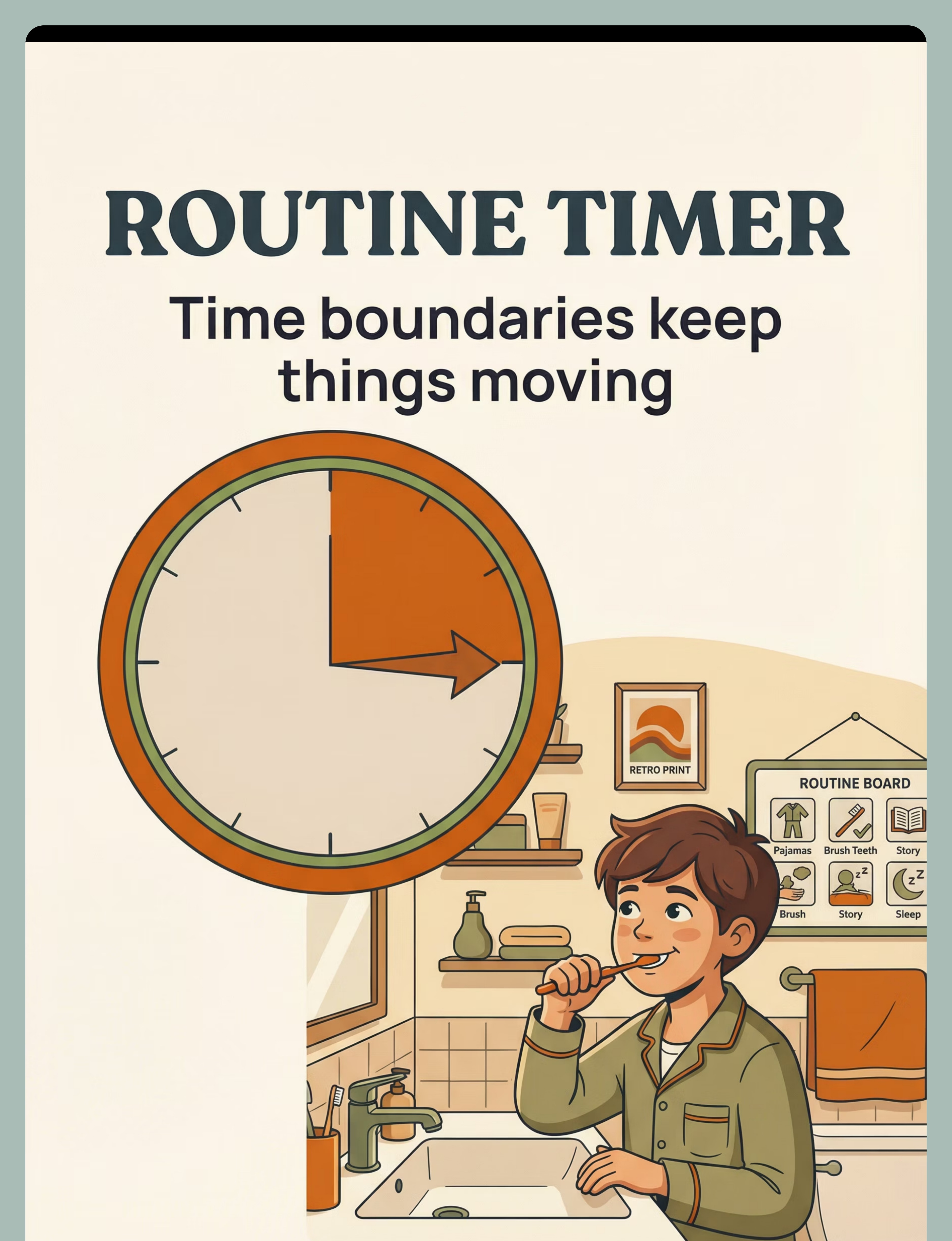
⏱ Material 3: Visual Countdown Timer
Time Timer or sand timer showing remaining time graphically. 30-minute capacity recommended. Also: Smartivity Interactive Clock ₹673. ₹200–800

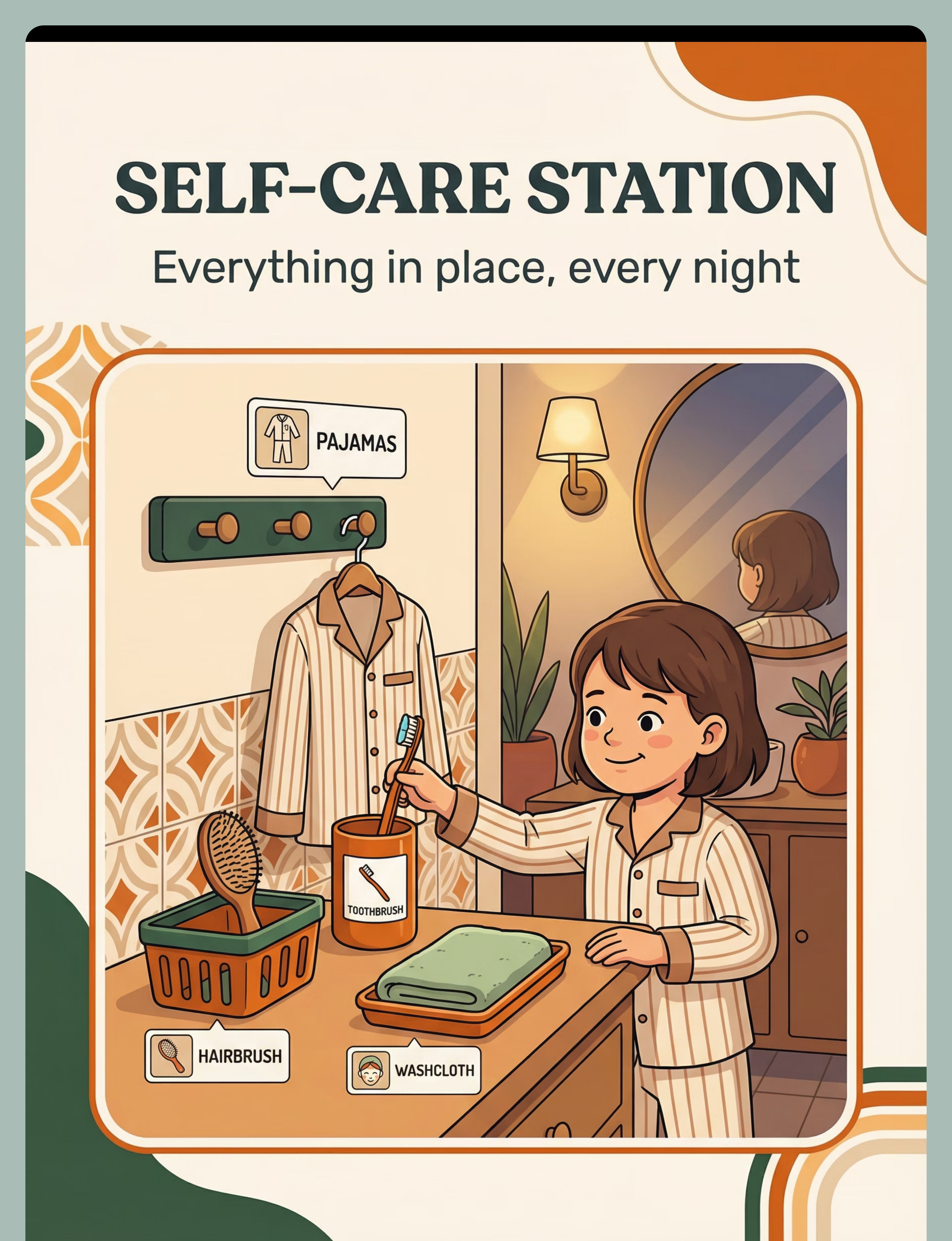
🗂 Material 4: Self-Care Station Organizer
Child-height bin + hook system for bathroom and bedroom. Picture labels for non-readers. ₹300–1,500
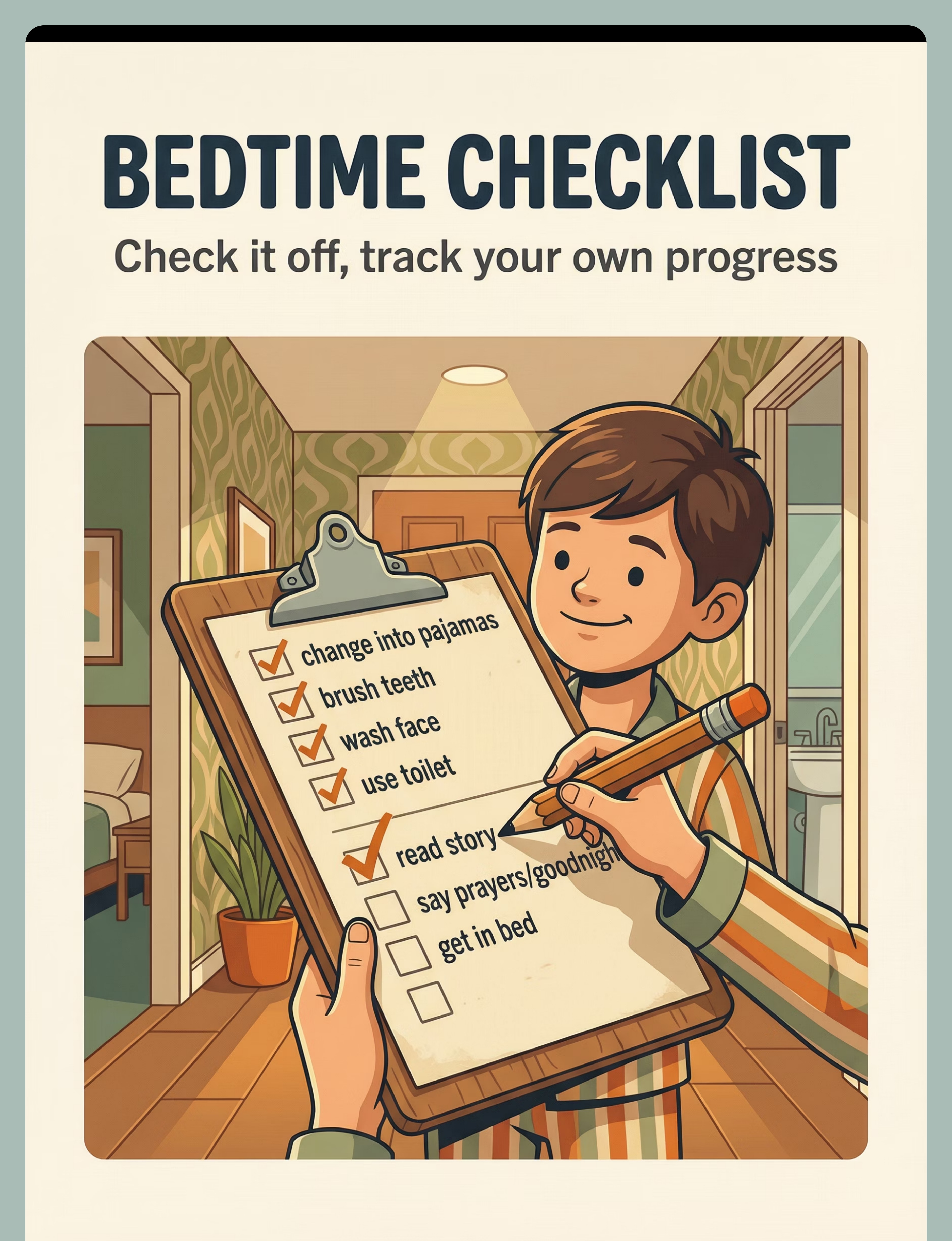
✅ Material 5: Bedtime Routine Checklist (Laminated)
Laminated A4 checklist with dry-erase checkbox system. Portable for whole-house use. Print free from pinnacleblooms.org/resources. ₹50–200

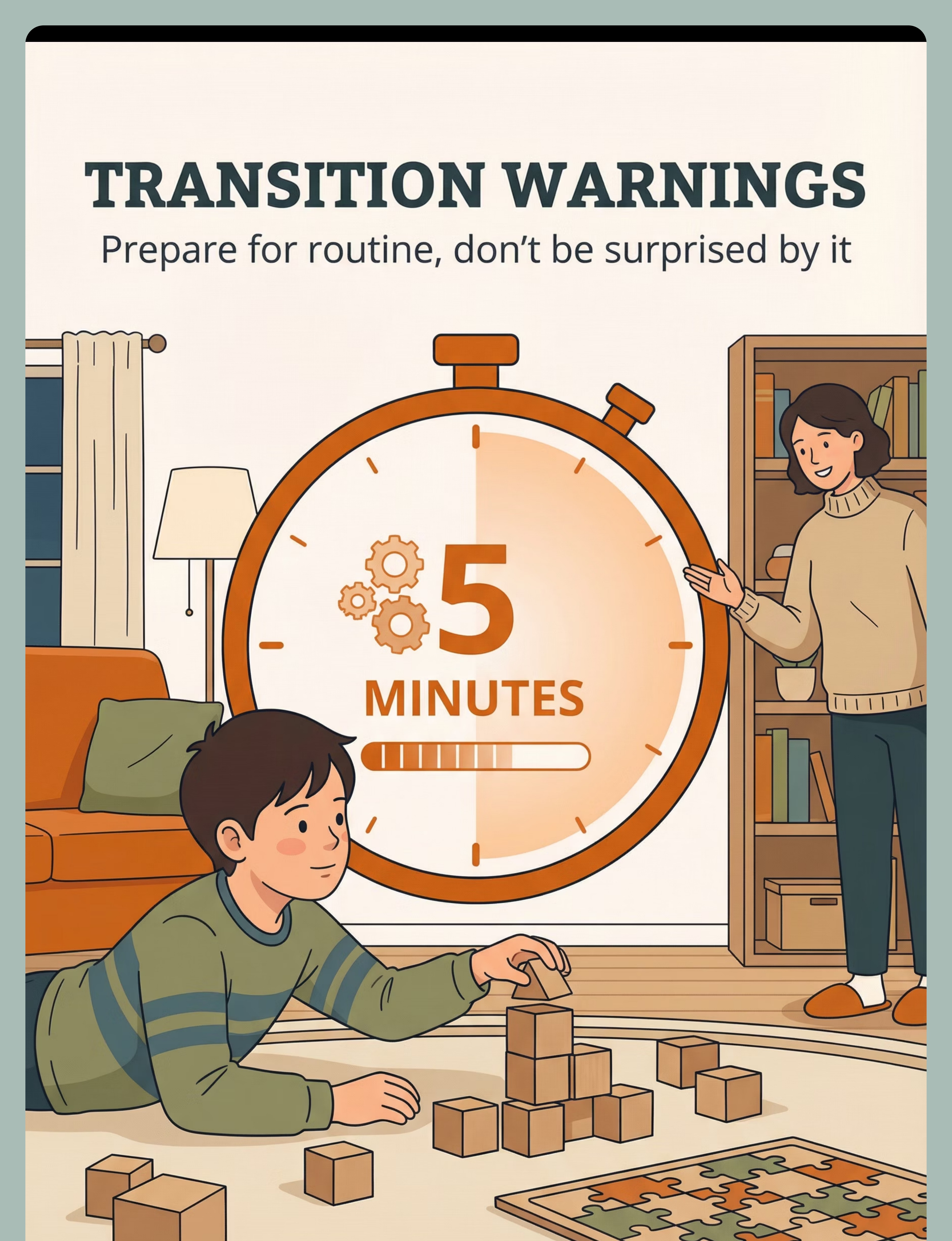
⏰ Material 6: Transition Warning Timer
Countdown timer visible from play area for 15/10/5-minute pre-routine warnings. ₹0–500

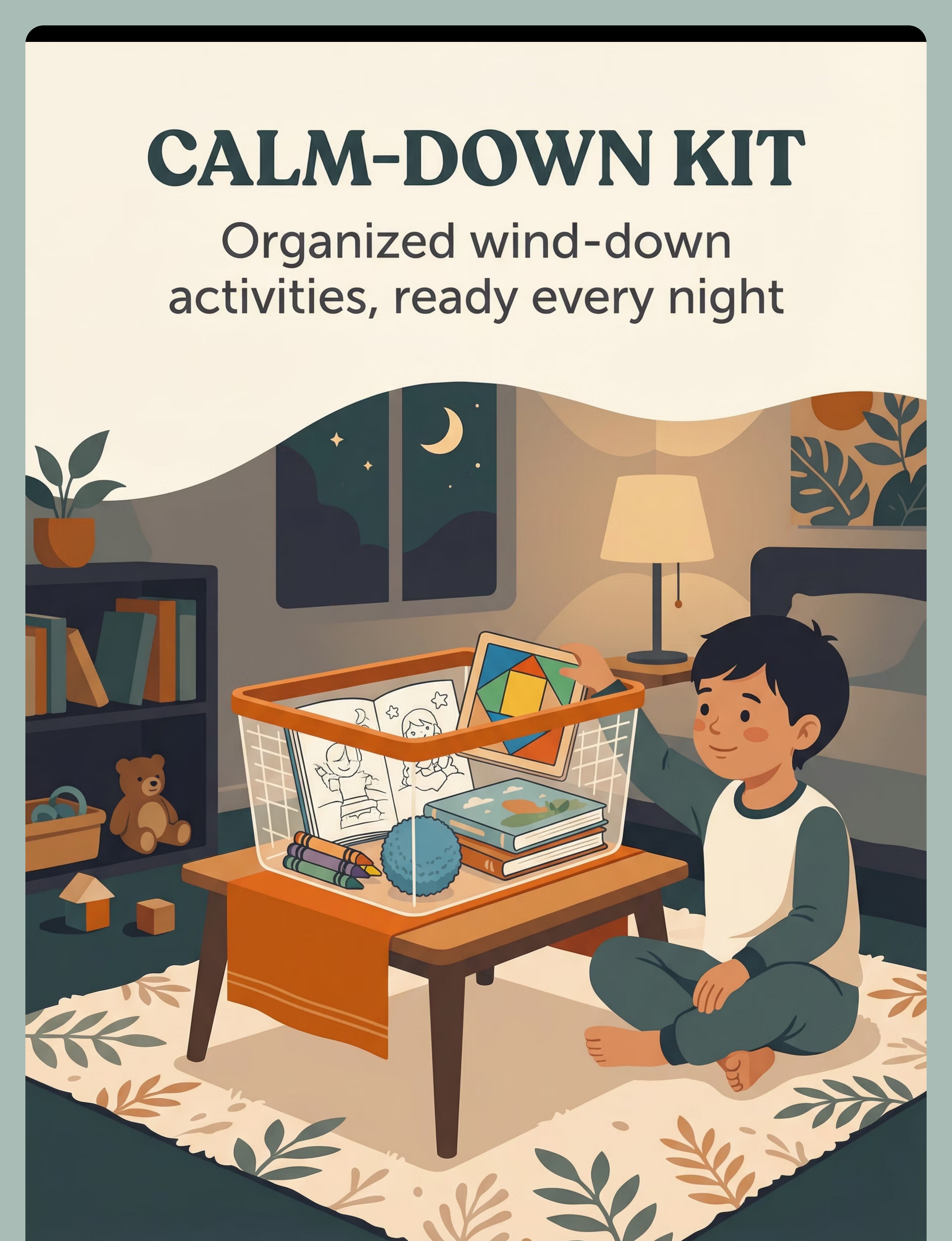
🧺 Material 7: Calm-Down Activity Kit
Dedicated container with calming activities: puzzles, coloring, quiet sensory items. Also: Animal Soft Toys ₹425. ₹200–1,000

🔊 Material 8: Bluetooth Speaker for Audio Routine
Portable speaker for bedtime playlist or recorded audio routine guide. ₹0–300

⭐ Material 9: Reward Chart + Sticker System
💡PINNACLE STARTER RECOMMENDATION: Begin with just 3: Visual Sequence Board + Progress Tracker + Reward Chart. Add materials as routine strengthens. Over-engineering Week 1 is the #1 mistake.
DIY & Substitute Options
Every family can execute this technique. Regardless of budget. Starting today. WHO Nurturing Care Framework (2018) established that effective child development interventions must be equity-accessible. These alternatives carry the same therapeutic mechanism as commercial equivalents.
Material 1 — Visual Board
Buy: ₹200–1,000
Make: Print A4 pages or cut magazine pictures. Paste on cardboard. Cover with cling wrap. Attach to bedroom door at child's eye level.
Cost: ₹0–30 | Works identically.
Make: Print A4 pages or cut magazine pictures. Paste on cardboard. Cover with cling wrap. Attach to bedroom door at child's eye level.
Cost: ₹0–30 | Works identically.
Material 2 — Progress Tracker
Buy: ₹100–500
Make: Draw the routine on cardboard. Attach a paperclip that slides down each step. Use stickers as "done" indicators.
Cost: ₹0 | Works identically.
Make: Draw the routine on cardboard. Attach a paperclip that slides down each step. Use stickers as "done" indicators.
Cost: ₹0 | Works identically.
Material 3 — Visual Timer
Buy: ₹200–800
Make: Draw a clock face on cardboard. Move a cut-out red "pie slice" to show remaining time. Free phone apps: "Visual Timer" (Android/iOS).
Cost: ₹0 | Works for most children.
Make: Draw a clock face on cardboard. Move a cut-out red "pie slice" to show remaining time. Free phone apps: "Visual Timer" (Android/iOS).
Cost: ₹0 | Works for most children.
Material 4 — Self-Care Station
Buy: ₹300–1,500
Make: Repurpose old bowls and containers. Label with handwritten picture labels. Use command strips for hooks.
Cost: ₹0 | Material accessibility is the mechanism.
Make: Repurpose old bowls and containers. Label with handwritten picture labels. Use command strips for hooks.
Cost: ₹0 | Material accessibility is the mechanism.
Material 5 — Checklist
Buy: ₹50–200
Make: Print from pinnacleblooms.org/resources free printables. Or draw in a notebook. Re-draw each week as routine solidifies.
Cost: ₹0 | Equally effective.
Make: Print from pinnacleblooms.org/resources free printables. Or draw in a notebook. Re-draw each week as routine solidifies.
Cost: ₹0 | Equally effective.
Material 9 — Reward Chart
Buy: ₹364–589
Make: Draw 7 boxes on paper. Child puts a hand-drawn star in each box after a successful night. Trade 5 stars for a family-chosen experience reward.
Cost: ₹0 | ABA reinforcement mechanism is identical.
Make: Draw 7 boxes on paper. Child puts a hand-drawn star in each box after a successful night. Trade 5 stars for a family-chosen experience reward.
Cost: ₹0 | ABA reinforcement mechanism is identical.
"Zero-cost implementation is not a compromise. The mechanism is the structure, not the material cost. A cardboard board at eye level is as powerful as a ₹1,000 laminated version — because the child's brain responds to the visual sequence, not the finish." — Pinnacle OT Consortium, aligned with WHO/UNICEF Equity Principles

Safety First: Before You Begin
Read this before your first night. Every point matters. This traffic-light safety system ensures the intervention is used appropriately and protects both children and caregivers.
🔴 DO NOT PROCEED IF:
- Child is currently severely dysregulated, mid-meltdown, or had a major sensory crisis within the past 2 hours
- Child has an undiagnosed medical condition affecting sleep (suspected sleep apnoea, restless legs, epilepsy at night) → Seek NeuroDev/Paediatric evaluation first
- Family is in acute crisis (domestic instability, recent trauma)
- Visual materials include small pieces for children under 3 with oral exploration tendencies (choking risk)
🟡 MODIFY BEFORE PROCEEDING:
- If child has high anxiety about visual boards: introduce board during daytime roleplay before nighttime use
- If routine resistance is extreme: start with just ONE step on the board, build the sequence over 2 weeks
- Medications affecting sleep architecture → consult prescribing doctor before changing bedtime timing
- Check that pajama textures, lighting levels, and sound environment won't trigger sensory overload
🟢 YOU'RE READY WHEN:
- Child is baseline regulated (not post-meltdown, reasonably fed)
- Materials are age-appropriate with no small parts hazard
- Environment set up with 2+ hours before board goes up
- All caregivers who do bedtime have seen the system
🚨STOP THIS SESSION IMMEDIATELY IF: Child shows signs of acute panic, breathing difficulty, extreme self-injurious behavior, or complete shutdown. Do not force completion.
📞Call 9100 181 181 if distressed. Free. 24×7.
📞Call 9100 181 181 if distressed. Free. 24×7.

Set Up Your Space
The environment is half the intervention. Set it up once. The room does the work every night. Spatial precision prevents 80% of session failures. When a child can see every element of the routine without being told, the routine runs itself.
Position 1 — Visual Sequence Board
Bedroom door or hallway wall at child's eye level. Not adult eye level — child must point and check independently.
Position 2 — Self-Care Station
Bathroom counter, organized. Toothbrush in labeled cup, pajamas laid out, face cloth accessible, hairbrush in holder.
Position 3 — Visual Timer
Visible from both bathroom and bedroom. Child should be able to see it throughout the entire routine.
Position 4 — Calm-Down Kit
On bedroom floor or table, accessible. Designated "quiet zone" spot. Contents rotated for novelty, always calming category.
Position 5 — Reward Chart
Bedroom wall, child-visible and within reach for sticker placement after routine completion.
Position 6 — Speaker/Audio Device
Bedroom, low volume position. Dimmed lighting: hallway to 50%, bedroom to warm/low. Temperature: 20–22°C ideal for sleep onset.

Is Your Child Ready? The 60-Second Check
A quick readiness check before beginning every night prevents failed sessions and protects the child's positive association with the routine. Run through all seven indicators before starting.
✓ Readiness Indicators
- Child is fed — not hungry, not overfull
- Child has been in a regulated state for at least 30 minutes
- No major transition difficulty in the last 60 minutes
- Environment is set up: board, station, timer, kit in place
- No signs of illness: fever, ear pain, unusual irritability
- Caregiver is regulated and genuinely ready to follow calmly
- Device-free period has started: screens off for 30+ minutes
🟢 ALL 7 CHECKED → GO
Begin with transition warning sequence.
🟡 5–6 CHECKED → MODIFY
Begin routine but simplify to 3 core steps: Pajamas → Teeth → Bed. Skip wind-down activities tonight.
🔴 4 OR FEWER → POSTPONE
Do a connection activity instead: read together, quiet cuddle. Attempt full routine tomorrow. Record tonight as "postponed — [reason]." This is not failure. It is data.
"The best session is one that starts right. You are not behind. You are being precise."

Step 1: The Transition Warning
Step 1 of 6
Starts 15 minutes before routine
ABA + OT | Antecedent Management
Every routine begins before it begins. The warning IS the first step. Delivering structured, predictable warnings trains the child's nervous system to begin downshifting before the routine even starts.
"[Child's name], 15 more minutes. When the timer goes off, it's our bedtime routine time. What do we do first? [Point to board] — that's right, pajamas!"
15 Minutes
"15 minutes until routine time."
10 Minutes
"10 more minutes — start finishing up."
5 Minutes
"5 minutes — almost time."
1 Minute
"1 minute — find a stopping place."
Timer Sounds
Routine begins. No exceptions. Point to visual board.
Resistance Response: If the child protests the warning — validate, don't negotiate. "I know you want more time. The timer says routine time. Let's do pajamas first, then story." Do NOT extend the timer in response to protests. The warning loses power if it becomes negotiable.
Body Language: Get down to child's level · Calm, warm tone — not urgent · Point to visual board as you give the verbal warning
Body Language: Get down to child's level · Calm, warm tone — not urgent · Point to visual board as you give the verbal warning

Step 2: The Sequence Begins
Step 2 of 6
Following the Visual Board
The board is now the authority. You are the support, not the commander. Shifting authority to the visual board removes the child's ability to negotiate with a person — the board simply is what it is.
"Okay, timer went off. Let's check your board — what's the first thing? [Child checks/points] Yes! Pajamas! Where are they? [Child finds them at self-care station] You know exactly where they are."
How to Use the Board During Routine
- Ask "What does your board say is next?" — don't tell
- Wait 5 full seconds for child to process and respond
- If no response after 5s: point to current step card, wait 3 more seconds
- If still no response: light physical prompt (guide hand to touch card)
- Never skip steps, even on difficult nights
Typical 7-Step Sequence
- Calm-down activity kit (15–30 min wind-down)
- Bath/face wash
- Pajamas on (from self-care station)
- Teeth brushing (timer for 2 minutes)
- Toilet visit
- Story/quiet connection time
- Final settling ritual → Lights out
Praise each step completion immediately: "You did it! Pajamas on. Moving the marker now!" [Child moves progress tracker to next step] · Full sequence 25–40 minutes.

Step 3: The Therapeutic Action — Wind-Down
Step 3 of 6
Calm-Down Phase | 15–20 Minutes
This is the step most families skip. It's the step that changes everything. The wind-down phase is the neurological preparation for sleep. It transitions the nervous system from the day's sensory load to rest-ready state. This is not "free time" — it is structured, calm, regulated activity that actively lowers cortisol and begins melatonin release.
Simple Floor Puzzles
5–10 pieces for young children; 50–100 for older. Hands-on, visually focused, inherently calming.
Coloring Books + Crayons
Non-stimulating colors and themes. Provides fine motor engagement while lowering arousal.
Soft Sensory Items
Comfort toy ₹425, sensory ball, soft book. Tactile regulation through proprioceptive input.
Audiobook or Quiet Music
Via speaker — no screen. Auditory calm without blue-light stimulation. Maintains low arousal throughout.
Parent role during wind-down: Sit nearby — available but not directing · Model calm: read your own book · Low lighting during this phase · No stimulating conversation
Concerning sign: Child is more aroused after 10 min than before → Sensory OT evaluation recommended
Concerning sign: Child is more aroused after 10 min than before → Sensory OT evaluation recommended

Step 4: Self-Care Tasks
Step 4 of 6
Self-Care Independence | 10–15 Minutes
3 good repetitions of correct teeth brushing beats 10 rushed ones. The routine is the dosage. Repetition IS the therapy — nightly execution builds the neural pathway for independent self-care across the lifespan.
Pajamas — 3–5 Minutes
Child finds and puts on pajamas independently from self-care station. Allow child to choose between 2 pre-selected options. Independence goal: achieved without instruction by Week 4.
Face Wash / Bath — 5–10 Minutes
Water temperature, washcloth texture, and soap scent consistent and child-preferred. Variation for sensory-sensitive: face wipe instead of full wash.
Teeth Brushing — 2-Minute Timer
Set countdown for exactly 2 minutes. When timer ends: done. Use specific "teeth brushing song." Mirror sticker showing "brush all 4 zones." Electric toothbrush for sensory-seeking children.
Toilet Visit — 3–5 Minutes
Ensure this is in routine regardless of whether child "needs" it. Prevents middle-of-night disruptions. Non-negotiable step.
Progress Tracker Movement: After each self-care task, child moves progress marker on board. "You brushed your teeth! Move your marker — you're almost done!"
Repetition guidance: "3 good nights in a row of independent pajama selection is more valuable than 10 nights of guided selection."
Repetition guidance: "3 good nights in a row of independent pajama selection is more valuable than 10 nights of guided selection."

Step 5: Reinforce & Celebrate
Step 5 of 6
Reinforcement Phase | 1–2 Minutes
Celebrate the attempt, not just the success. Timing matters more than magnitude. The reinforcement system is what makes the routine sustainable across weeks and months — it keeps the child motivated through the harder nights.
Deliver reinforcement WITHIN 3 SECONDS of completed step. Not after the whole routine. Not "good job tonight." IMMEDIATELY after each step completes.
After Pajamas On
"Amazing — you got your pajamas yourself! I love that!"
After Teeth Done
"Your teeth are SO clean. You did the whole 2 minutes!"
Board Checked Proactively
"You checked your own board! That's incredible."
Full Routine Complete
"You did your WHOLE bedtime routine tonight! You are someone who takes care of themselves. That's powerful."
Reward Chart Mechanics
After routine completion: child places sticker on reward chart → 1800+ Reward Stickers ₹364. Goal: 5 consecutive successful nights = family-chosen experience reward (special breakfast, extra story, choose Friday's movie — NOT a purchased toy).
→ Rosette Imprint Reward Jar ₹589: Child places token in jar after each successful night. When jar fills to the line → family celebration event.
Reinforcement Fading Plan
Weeks 1–2: Reinforce every step + full routine completion
Weeks 3–4: Reinforce every 2 steps + full routine
Weeks 5–6: Reinforce full routine completion only
Weeks 7–8: Move to natural reinforcers only (story = reward for routine)
Weeks 3–4: Reinforce every 2 steps + full routine
Weeks 5–6: Reinforce full routine completion only
Weeks 7–8: Move to natural reinforcers only (story = reward for routine)
"Habit formation is complete when the routine itself is the reinforcer."

Step 6: The Cool-Down Into Sleep
Step 6 of 6
Settling Phase | 10–15 Minutes
No routine ends abruptly. The last step signals: everything is safe. Sleep is coming. The settling sequence is the neurological landing — the bridge between the structure of the routine and the surrender of sleep.
Story / Quiet Connection — 10 Minutes
In bed. Warm light only. Parent reads OR child looks at picture book independently. Connection time, not instruction time. Calm voice, low volume, slow pace. "The story voice IS the sleep cue."
Final Ritual — 1–2 Minutes (NEVER Changes)
Choose ONE and execute identically every night: Hug + kiss + specific phrase · Gratitude moment · Quiet back rub + same song hummed · Prayer or cultural ritual. "The final ritual tells the nervous system: everything is complete, everyone is safe, sleep is permitted."
Lights Out Procedure
Pre-agree and stay consistent from Night 1: Night light (yes/no, color, position) · Door (open, cracked, or closed) · Sound (silence, white noise, quiet music). Transition warning: "One more page, then lights out." No negotiation post lights-out.
Resistance at end (most common failure point):
• "One more story" → "Board says all done. Board is the rule."
• Child gets out of bed → Silent, zero-attention return. No discussion. No second hug.
• "I'm scared" → Pre-establish "scaries protocol" during daytime: worry box, checking routine, reassurance phrase.
Progress Tracker — Final Move: Child moves tracker to "ALL DONE ★" position. Celebrate it every night.
• "One more story" → "Board says all done. Board is the rule."
• Child gets out of bed → Silent, zero-attention return. No discussion. No second hug.
• "I'm scared" → Pre-establish "scaries protocol" during daytime: worry box, checking routine, reassurance phrase.
Progress Tracker — Final Move: Child moves tracker to "ALL DONE ★" position. Celebrate it every night.
Capture the Data: Right Now
Within 60 seconds of lights out. Not tomorrow morning. Now. 60 seconds of data now saves hours of guessing later. After 14 days of data, patterns emerge — which nights are hardest, which steps take longest, whether resistance is decreasing week over week.
📊 Data Point 1: Routine Completion Score
How many steps did the child complete independently (without direct instruction)?
0 = None | 1–3 = Some | 4–6 = Most | 7+ = All
Record as a number. Takes 5 seconds.
0 = None | 1–3 = Some | 4–6 = Most | 7+ = All
Record as a number. Takes 5 seconds.
📊 Data Point 2: Resistance Level
Scale: 0 (no resistance) → 1 (mild, recovered quickly) → 2 (moderate) → 3 (significant, routine incomplete) → 4 (routine abandoned).
Circle one number. Takes 3 seconds.
Circle one number. Takes 3 seconds.
📊 Data Point 3: Lights-Out Time
Write the actual time lights went out tonight. Compare against target time. Track trend weekly.
Takes 5 seconds.
Takes 5 seconds.
Paper Tracker Sheet
Print from pinnacleblooms.org/resources
Notes App on Phone
"449 — [date] — [score/resistance/time]"
GPT-OS® App Data Capture
Links progress to TherapeuticAI® recommendations → pinnacleblooms.org/track/d449
📞Data showing no improvement after 2 weeks? Call 9100 181 181 for clinical review. Free. 24×7.
What If It Didn't Go As Planned?
Most nights don't go perfectly. That's not failure — that's data about what to adjust. Session abandonment is not failure. Record what happened. Adjust one variable for tomorrow. Not everything. One variable.
🔧 Problem 1: Routine takes 90+ minutes
Why: One step consumes disproportionate time, often wind-down or teeth brushing.
Fix: Add per-step visual timer. The timer — not the parent — signals when to move on. Teeth: 2-minute timer. Calm-down kit: 20-minute timer. Non-negotiable.
Fix: Add per-step visual timer. The timer — not the parent — signals when to move on. Teeth: 2-minute timer. Calm-down kit: 20-minute timer. Non-negotiable.
🔧 Problem 2: Child refuses to start when warnings given
Why: Transition difficulty; current activity has very high motivation value.
Fix: Earlier first warning (20 min). Create "routine launch ritual" child enjoys (special music). Ensure preferred activity — story — is at end as motivator.
Fix: Earlier first warning (20 min). Create "routine launch ritual" child enjoys (special music). Ensure preferred activity — story — is at end as motivator.
🔧 Problem 3: Works for me but not other caregivers
Why: Board exists but other caregivers don't use it.
Fix: "The board is the routine, not you." All caregivers point to board and follow it. Send caregivers to this page. Audio routine guide removes individual variation entirely.
Fix: "The board is the routine, not you." All caregivers point to board and follow it. Send caregivers to this page. Audio routine guide removes individual variation entirely.
🔧 Problem 4: Child ignores the visual board
Why: Board not at eye level, not interactive, not being referenced.
Fix: Move board to eye level. Add interactive element (velcro, progress clip). Make it a game: "I wonder what the board says is next?" Replace pointing-by-parent with pointing-by-child.
Fix: Move board to eye level. Add interactive element (velcro, progress clip). Make it a game: "I wonder what the board says is next?" Replace pointing-by-parent with pointing-by-child.
🔧 Problem 5: Routine complete but child can't fall asleep
Why: This is a DIFFERENT problem — bedtime resistance or sleep onset difficulty, not routine structure.
Fix: See D-448 (Bedtime Resistance) and D-446 (Falling Asleep Independently).
Fix: See D-448 (Bedtime Resistance) and D-446 (Falling Asleep Independently).
🔧 Problem 6: Works 1 week then falls apart
Why: Novelty effect fades; reinforcement may have been removed too early.
Fix: Ensure reward chart is still active. Check routine hasn't been adjusted. Re-introduce with caregiver consistency audit.
Fix: Ensure reward chart is still active. Check routine hasn't been adjusted. Re-introduce with caregiver consistency audit.
🔧 Problem 7: Child severely distressed at one step
Why: Sensory sensitivity, specific phobia, or negative history with that step.
Fix: Address that step separately, outside bedtime routine. OT for sensory-based dental hygiene resistance. Do not let one step derail the entire routine.
Fix: Address that step separately, outside bedtime routine. OT for sensory-based dental hygiene resistance. Do not let one step derail the entire routine.

Adapt & Personalize
No two children are identical. Your routine needs to fit your child's profile. The technique remains constant; the intensity, steps, and reinforcement density flex to match where your child is on any given night and across developmental weeks.
EASIER — Bad Days / Early Weeks
3-step routine: Pajamas → Teeth → Bed. Parent walks through each step. Immediate reinforcement after every step. Zero expectation of board independence. Timer optional.
BASELINE — Normal Nights / Weeks 3–8
Full 7-step routine with visual board. Child checks board and moves tracker with prompting. Reinforcement after every 2 steps + completion. All timers active. Story as natural reinforcer at end.
HARDER — Mastery Phase
Child initiates routine at warning without parent instruction. Child uses board completely independently. Parent's role: connection only (story, final ritual). Use when 80%+ of steps completed independently.
Sensory Seeker
Add proprioceptive input before bed: wall push-ups, bear hug, weighted blanket. Regulates the high-arousal nervous system.
Sensory Avoider
Simplify sensory elements: face wipe, soft pajamas, dim light throughout, audio cues only — no visual clutter. Reduces sensory load.
High Anxiety
Emphasize predictability above all. Add "worry check" step: child names one worry, parent acknowledges, places in "worry box," closed until morning.
ADHD / Executive Function
Maximize time structure: visual timer for every step, per-step checklist, immediate reinforcement, no deviation from sequence. External structure compensates for time blindness.
Week 1–2: What to Expect
15% Complete
Building the Tracks
Weeks 1–2: You are building the tracks. The train hasn't left the station yet. That's exactly right. In these first two weeks, you are doing most of the work — and that is correct. You are building the external scaffold. The child's brain is quietly reorganizing around it.
Observable Indicators — Weeks 1–2
- Child tolerates the visual board being there, even if not using it
- Child can point to ONE step on the board when asked "what's next?"
- Routine takes less than 60 minutes (down from 90+)
- Child completes 1–2 steps independently without direct instruction
- Resistance at start of routine recovers within 5 minutes
- Child moves the progress tracker at least twice per night (prompted)
- Family has executed the routine 5+ nights out of 7
Not Progress Yet — Managing Expectations
- Child checking the board proactively (comes later)
- Independent routine start without warnings (comes later)
- Lights out at exact target time (takes 3–4 weeks to calibrate)
- Zero resistance (normal for first 2 weeks)
- Complete step independence (foundation first)
"If your child tolerates the routine 2 minutes longer than last week — that is real, measurable, neurological progress."

Week 3–4: Consolidation Signs
40% Complete
Neural Pathways Forming
Weeks 3–4: The neural pathways are forming. You may see things you've never seen before. These behavioral changes signal that the routine is being internalized — moving from external structure to internal habit.
Unprompted Mentions
Child mentions the routine during the day: "Is it bedtime routine time after dinner, Mummy?" This is the PFC beginning to map the routine as part of the day's architecture.
Anticipatory Behavior
Child starts moving toward the board BEFORE the warning sounds. Early internalization confirmed. Celebrate this specifically — it is neurological progress.
Child Corrects YOU
Child notices if you skip or change a step. This is neurological internalization — celebrate it enthusiastically. The routine now belongs to the child.
Independent Sticker Placement
Child places sticker on reward chart without reminder on some nights. Self-reinforcement emerging — a hallmark of internalization.
When to increase difficulty: If child is completing 70%+ of steps independently → introduce the "harder" profile from Card 22.
When to hold: If child is still at 30% independent → maintain current level, add one more reinforcement touchpoint.
Parent milestone: By Week 3–4, your confidence is visible to your child and directly affects their response.
When to hold: If child is still at 30% independent → maintain current level, add one more reinforcement touchpoint.
Parent milestone: By Week 3–4, your confidence is visible to your child and directly affects their response.

Week 5–8: Mastery Indicators
75% Complete
🏆 Mastery Zone
Weeks 5–8: The routine runs itself. You went from managing bedtime to having bedtime. These are the specific, observable, measurable criteria that confirm true mastery — not just compliance.
Board Checked Proactively
Child checks visual board proactively on 5+ consecutive nights without any parent prompt.
80%+ Independent
Child completes 80%+ of routine steps without direct instruction from any caregiver.
Consistent Timing
Routine consistently completes within 35–40 minutes. Lights out at same time ±10 minutes every night.
Resistance Resolved
Resistance at routine start absent or resolved within 2 minutes on 5+ nights per week.
Holds Across Caregivers
Routine holds when different caregiver is present. Child uses "what does my board say?" proactively regardless of who does bedtime.
Maintenance Check: At Week 8, try 1 night without the visual board. If child completes 70%+ of steps from memory → internalization confirmed. If regression → materials back, additional 2–4 weeks.
Next techniques unlocked: D-450 (Nightmares and Night Terrors) · D-446 (Falling Asleep Independently)
Next techniques unlocked: D-450 (Nightmares and Night Terrors) · D-446 (Falling Asleep Independently)
You Did This.
Five to eight weeks ago, bedtime was a battle zone. Tonight, your child knew what was coming. They found their pajamas. They brushed their teeth to the timer. They moved their tracker to "all done." They got into bed without a struggle.
That didn't happen accidentally. It happened because you set up the board. You gave the warnings. You stayed calm on the hard nights. You didn't give up when Week 1 felt impossible. Your child grew because of your commitment. Let that land.
Multi-Step Sequencing
PFC training through repeated nightly practice
Transition Readiness
Amygdala regulation through consistent predictability
Self-Care Independence
Daily living skills now owned by the child
Time Awareness
Circadian calibration through consistent cue sequences
"Tell your child specifically what they achieved. 'You have a bedtime routine now. That's yours. You did that.'"

Red Flags: When to Pause
Even in the success zone, these signs mean: pause and ask. If something feels wrong — not just hard, but wrong — trust your instincts. 📞9100 181 181. Free. 24×7.
🚨 Sleep Architecture Concern
What it looks like: Child completes full routine but wakes 4+ times per night, appears exhausted despite adequate sleep time.
Why it matters: May indicate sleep apnoea, periodic limb movement disorder, or other medical sleep disorder.
Action: NeuroDev/Paediatric sleep specialist referral → Do NOT wait more than 2 weeks.
Why it matters: May indicate sleep apnoea, periodic limb movement disorder, or other medical sleep disorder.
Action: NeuroDev/Paediatric sleep specialist referral → Do NOT wait more than 2 weeks.
🚨 Extreme Distress at One Specific Step
What it looks like: Routine runs smoothly except child has meltdown or complete shutdown at exactly the same step every night.
Why it matters: May indicate sensory defensiveness, phobia, or trauma association requiring specialized intervention.
Action: OT sensory assessment for that specific step. Continue rest of routine; bypass this step temporarily.
Why it matters: May indicate sensory defensiveness, phobia, or trauma association requiring specialized intervention.
Action: OT sensory assessment for that specific step. Continue rest of routine; bypass this step temporarily.
🚨 Routine Complete but No Sleep Onset Improvement
What it looks like: Routine completes within 40 min but child lies awake 1–2 hours after lights out every night.
Why it matters: Circadian rhythm disorder, sleep onset anxiety, or melatonin dysregulation — outside routine's scope.
Action: Separate sleep onset intervention (D-446) + Paediatric sleep consultation.
Why it matters: Circadian rhythm disorder, sleep onset anxiety, or melatonin dysregulation — outside routine's scope.
Action: Separate sleep onset intervention (D-446) + Paediatric sleep consultation.
🚨 Severe Regression After Progress
What it looks like: Child had mastery, then completely refused routine for 5+ consecutive nights.
Why it matters: May signal a change in child's life (school transition, new sibling, family change) or emerging anxiety.
Action: Functional assessment — identify trigger, do not punish regression, restart at Week 1 protocol.
Why it matters: May signal a change in child's life (school transition, new sibling, family change) or emerging anxiety.
Action: Functional assessment — identify trigger, do not punish regression, restart at Week 1 protocol.
🚨 Caregiver Burnout Signal
What it looks like: Primary caregiver showing signs of emotional exhaustion or resentment of the routine.
Why it matters: Parent dysregulation is the #1 predictor of routine failure — not child capacity.
Action: Pinnacle parent support consultation → 9100 181 181. Free. Available now.
Why it matters: Parent dysregulation is the #1 predictor of routine failure — not child capacity.
Action: Pinnacle parent support consultation → 9100 181 181. Free. Available now.

The Progression Pathway
You are not done. You are on a journey. D-449 is one milestone on a larger developmental map. Understanding what came before and what comes next helps you see where this technique fits in your child's full arc of independence.
D-447: Night Waking
Resolved night wakings before routine work began.
D-448: Bedtime Resistance
Reduced resistance before establishing sequence.
★ D-449: Sleep Routine
YOU ARE HERE. Consistent nightly routine → Self-monitoring → Independence.
D-450 or D-446
Nightmares & Night Terrors · OR · Falling Asleep Independently.
D-455: Morning Routine
Transfer visual routine skills to mornings. Same materials — new sequence.

Related Techniques in This Domain
You already have the system. These techniques use the same materials — your investment in D-449 materials unlocks 5 adjacent techniques immediately.

🌙 D-448: Managing Bedtime Resistance
Difficulty: CORE | Materials: Visual board (you own this now)
"The technique before this one. If resistance is still high, go back."
interventions.pinnacleblooms.org
"The technique before this one. If resistance is still high, go back."
interventions.pinnacleblooms.org

💤 D-446: Falling Asleep Independently
Difficulty: CORE | Materials: Visual timer + calm-down kit (you own these)
"Routine is complete. This teaches sleep onset without parent presence."
"Routine is complete. This teaches sleep onset without parent presence."

😨 D-450: Nightmares and Night Terrors
Difficulty: ADVANCED | Materials: Comfort objects + routine structure
"The next technique in the sleep series." interventions.pinnacleblooms.org
"The next technique in the sleep series." interventions.pinnacleblooms.org

⏰ D-455: Morning Routine Structure
Difficulty: CORE | Materials: Visual board (same board, morning version)
"Transfer everything you learned here to mornings." Most families master this in 2–3 weeks.
"Transfer everything you learned here to mornings." Most families master this in 2–3 weeks.

🪥 D-460: Independent Teeth Brushing
Difficulty: INTRO | Materials: Visual timer + self-care station
"Deep-dive on just the teeth brushing step."
"Deep-dive on just the teeth brushing step."

👕 D-462: Independent Dressing Routine
Difficulty: CORE | Materials: Self-care station (you own this)
"Expand independence to full dressing sequence."
"Expand independence to full dressing sequence."
Your Child's Full Developmental Map
D-449 is one technique. Your child needs a map. Sleep Routine Establishment sits in Domain D and feeds into Domains C (emotional regulation through predictability), H (cognitive skill of sequencing), and A (sensory wind-down for regulation).
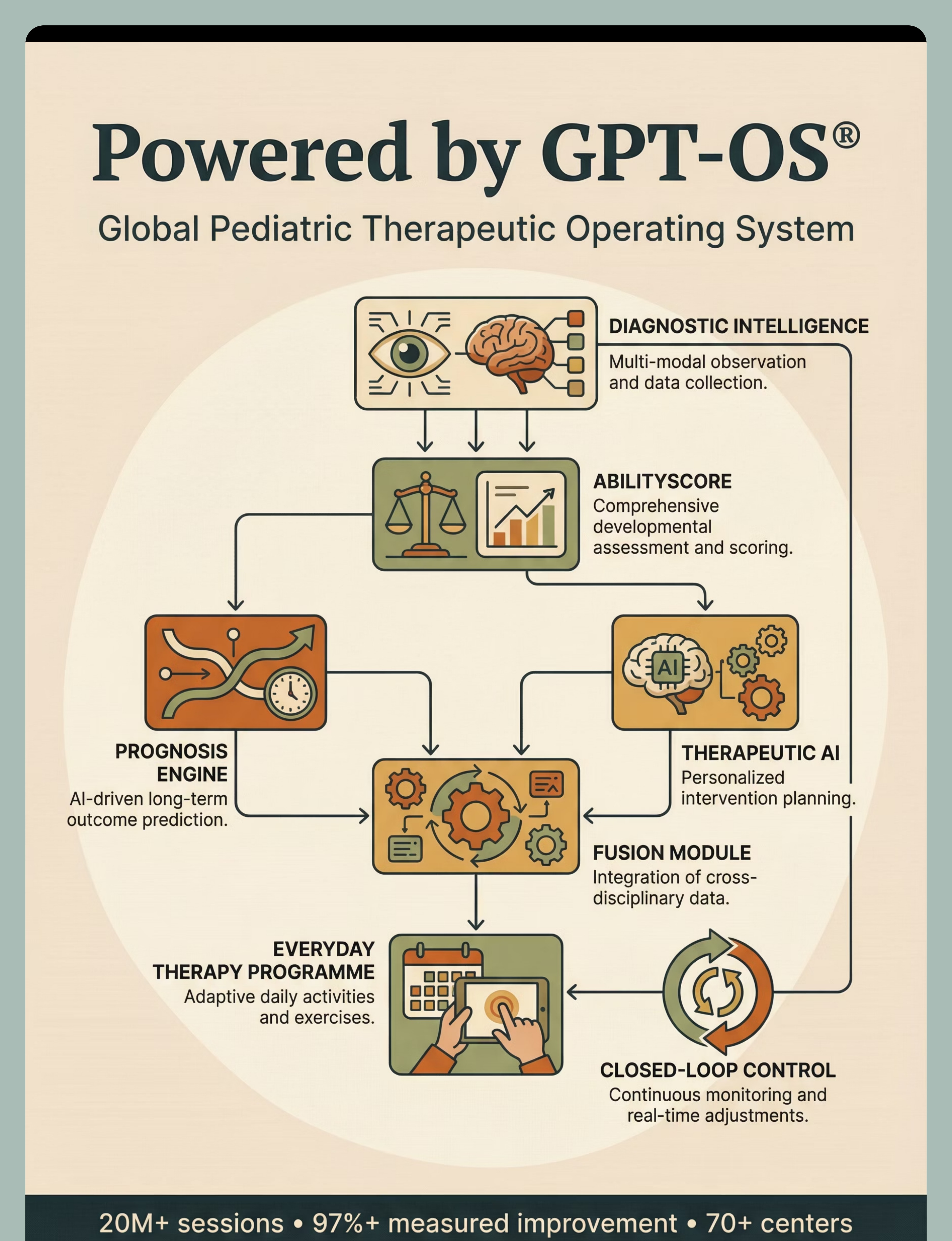
GPT-OS® Personalized Mapping
Every technique at techniques.pinnacleblooms.org maps to this wheel. Your child's journey is not random acts of therapy — it is a sequenced developmental architecture, governed by GPT-OS®, personalized by your child's AbilityScore®.
GPT-OS® Platform
12 domains × 70,000+ techniques · AbilityScore® assessment · TherapeuticAI® recommendations · EverydayTherapyProgramme™
📞Want to map your child's full profile?
FREE consultation: 9100 181 181
FREE consultation: 9100 181 181

Families Who've Been Here
These are real families. Real children. Real outcomes. Their stories reflect the aggregate experience of thousands of families across the Pinnacle network who started exactly where you are now.
Arjun, Age 6 — ASD | Hyderabad
Before: Every night was different. Bedtime took 2 hours minimum. He was still wired at 10:30 PM. We were all exhausted and dreading evenings.
After 3 weeks: Bedtime is 40 minutes. He checks his board before I even give the first warning. He moves the magnet himself. We're done by 8:45 PM and he's asleep by 9:15.
"The board changed our evenings. Not just bedtime — our whole evening has calm in it now. We're not dreading 8 PM anymore."
After 3 weeks: Bedtime is 40 minutes. He checks his board before I even give the first warning. He moves the magnet himself. We're done by 8:45 PM and he's asleep by 9:15.
"The board changed our evenings. Not just bedtime — our whole evening has calm in it now. We're not dreading 8 PM anymore."
Priya, Age 4 — Developmental Delay | Chennai
Before: Required one-to-one guidance for every single step. If any caregiver was missing, it fell apart completely.
After 6 weeks: She does her routine entirely independently except for the story. She's so proud. She shows her board to everyone who visits.
"'This is MY routine.' When she said that for the first time, I cried. She has ownership of her own life now."
After 6 weeks: She does her routine entirely independently except for the story. She's so proud. She shows her board to everyone who visits.
"'This is MY routine.' When she said that for the first time, I cried. She has ownership of her own life now."
Rohan, Age 8 — ADHD | Bangalore
Before: Gaming at 11 PM, refusing to brush teeth, still in day clothes at midnight. We had given up.
After 5 weeks: Written checklist version. He times himself. He beat his previous completion time three nights in a row. Now it's a competition with himself. Lights out by 9:30 PM.
"We told him it was a system, not a routine. He loved the word 'system.' One word changed everything."
After 5 weeks: Written checklist version. He times himself. He beat his previous completion time three nights in a row. Now it's a competition with himself. Lights out by 9:30 PM.
"We told him it was a system, not a routine. He loved the word 'system.' One word changed everything."
Illustrative cases based on aggregate outcomes. Individual results vary by child profile, intensity of implementation, and underlying needs.

Connect With Other Parents
Isolation is the enemy of adherence. 12,000+ parents are on this exact journey. Meeting one parent who has been where you are is worth 10 articles. Your experience — the hard nights, the breakthroughs, the specific adjustment that made it click for YOUR child — is valuable to every family starting tomorrow.
📱 Sleep Routine Support Group
12,000+ parents. Active. Moderated by Pinnacle therapists. Topics: visual board ideas, caregiver consistency tips, celebration posts.
Join the WhatsApp Group
Join the WhatsApp Group
💬 Pinnacle Parent Forum
Searchable archive of 50,000+ parent questions in the Self-Care & Daily Living forum.
Browse the Forum
Browse the Forum
📍 Local Parent Meetups
Monthly meetups at 70+ Pinnacle centers across India. Find your nearest center.
Find a Center
Find a Center
🤝 Peer Mentoring
Parents who have mastered D-449 and volunteered to mentor new families. Lived experience, structured support.
Request a peer mentor: 9100 181 181
Request a peer mentor: 9100 181 181
📞Need someone to talk to? FREE helpline: 9100 181 181 | 16+ Languages | 24×7
"Consider sharing your story: pinnacleblooms.org/stories"
"Consider sharing your story: pinnacleblooms.org/stories"

Your Professional Support Team
Home + clinic = maximum impact. Visual boards work. Specialist-guided visual boards work faster. Operating under a single GPT-OS® clinical standard, what you receive in Hyderabad is identical to what you receive in Chennai, Mumbai, Delhi, or Bangalore.
🏥 OT Consultation — Recommended for D-449
OTs assess: visual board design optimized for YOUR child's comprehension level · sensory contributions to bedtime difficulty · task analysis of specific resistant steps · independence ladder with graded prompt fading.
Book OT Session | 9100 181 181
Book OT Session | 9100 181 181
🧠 ABA / BCBA Consultation
BCBAs add: functional assessment of significant resistance behaviors · reinforcement system design beyond the reward chart · caregiver training for cross-family consistency · data analysis from your tracking sheets.
Book ABA session: 9100 181 181
Book ABA session: 9100 181 181
📱 Teleconsultation — All India + International
25-minute video consultation with Pinnacle specialist. Available in 16+ languages. Same-day booking available.
Fee: ₹499 first consultation | Pinnacle network families: subsidized
Book Now
Fee: ₹499 first consultation | Pinnacle network families: subsidized
Book Now
👨⚕️ NeuroDev Paediatrics
Indicated when: sleep routine difficulty co-occurring with suspected sleep disorder · medication review needed · formal developmental assessment not yet completed.
NeuroDev referral: 9100 181 181
NeuroDev referral: 9100 181 181
📞FREE National Autism & Development Helpline: 9100 181 181
Available 24×7 | 16+ Languages | No appointment needed for advice
Available 24×7 | 16+ Languages | No appointment needed for advice
The Research Library
Deeper reading for the curious parent — and the clinical mind. All techniques at techniques.pinnacleblooms.org are referenced against the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence. D-449 carries Level I–II evidence across its primary components.
Level I — Systematic Reviews & Meta-Analyses
📄NCAEP Evidence-Based Practices Report (2020): "Visual schedules: evidence-based practice for autism across 28 studies." → ncaep.fpg.unc.edu/resources
📄Mindell JA et al., SLEEP (2015): "A nightly bedtime routine: impact on sleep in young children and their mothers." Intervention group: faster sleep onset, longer total sleep, better mood → DOI: 10.5665/sleep.4880
📄PMC11506176 — PRISMA Systematic Review (2024): "16 articles 2013–2023: structured intervention meets evidence-based criteria for ASD"
📄Mindell JA et al., SLEEP (2015): "A nightly bedtime routine: impact on sleep in young children and their mothers." Intervention group: faster sleep onset, longer total sleep, better mood → DOI: 10.5665/sleep.4880
📄PMC11506176 — PRISMA Systematic Review (2024): "16 articles 2013–2023: structured intervention meets evidence-based criteria for ASD"
Level II — Randomized Controlled Trials
📄Cortesi F et al. (2012): Visual routine component: 78% improvement in sleep measures → J Child Psychol Psychiatry. 2012;53(3):225–34
📄Padmanabha S et al. (2019): Indian RCT: "Home-based structured interventions for ASD in Indian pediatric population" → DOI: 10.1007/s12098-018-2747-4
📄Padmanabha S et al. (2019): Indian RCT: "Home-based structured interventions for ASD in Indian pediatric population" → DOI: 10.1007/s12098-018-2747-4
Level III — Cohort Studies & WHO Publications
📄PMC10955541 — Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy, routine adherence
📄PMC9978394 — WHO/UNICEF CCD Package: Caregiver-implemented routines across 54 LMICs
🌐WHO Nurturing Care Framework (2018): nurturing-care.org/ncf-for-ecd/
🌐UNICEF MICS Developmental Indicators: data.unicef.org/topic/child-development
📄PMC9978394 — WHO/UNICEF CCD Package: Caregiver-implemented routines across 54 LMICs
🌐WHO Nurturing Care Framework (2018): nurturing-care.org/ncf-for-ecd/
🌐UNICEF MICS Developmental Indicators: data.unicef.org/topic/child-development
How GPT-OS® Uses Your Data
Your 60 seconds of nightly data does more than you know. When you record your 3 data points into the GPT-OS® tracker, TherapeuticAI® transforms them into personalized clinical guidance — and your anonymized data improves the journey of every child like yours.
Step 1 — Pattern Detection
TherapeuticAI® identifies: which nights are consistently harder · which steps show persistent resistance · whether resistance is decreasing week over week · time-to-mastery prediction based on your child's trajectory.
Step 2 — Personalized Recommendations
Based on YOUR child's data — not population averages: specific protocol modifications · when to increase or decrease reinforcement intensity · which next technique to attempt · red flag alerts if data shows regression patterns.
Step 3 — Population-Level Learning
Your anonymized data joins 20M+ session data points · improves TherapeuticAI® recommendations for all families · identifies new patterns in sleep routine difficulty · informs Pinnacle clinical protocol development.
✓ Data encrypted at rest and in transit · Never sold or shared with third parties · Anonymized before population-level analysis · Parent controls data deletion: pinnacleblooms.org/privacy · DPIIT recognized startup data handling standards
Watch the Reel
Reel ID: D-449 · Series: Toileting & Self-Care Independence in Children · Episode 449 · Domain: Sleep / Self-Care / Daily Living · Duration: 75–85 seconds · Therapist presentation + B-roll demonstrations
▶ Watch: 9 Materials That Help With Sleep Routine
This web page and the D-449 Reel are two entry points to the same clinical knowledge. The Reel gives you the visual overview in 60 seconds. This page gives you the complete execution system. Together: everything you need to transform your child's bedtime.
Related Reels in This Series
- D-447: 9 Materials That Help With Night Waking
- D-448: 9 Materials That Help With Bedtime Resistance
- D-450: 9 Materials That Help With Nightmares and Night Terrors
- D-451: 9 Materials That Help With Waking for Parents at Night
Full series: pinnacleblooms.org/reels/sleep-series
Share This Reel
📱WhatsApp ·
Share This With Your Family
Consistency across caregivers multiplies impact. If only one person follows the system, you get 50% results. The routine's power comes from its predictability — and predictability requires every caregiver to follow the same system every night.
Share Buttons
Pre-written WhatsApp message: "Found this for bedtime routine — follow the system on the board and we'll finally have consistent nights. Read: [link]"
For Grandparents & Helpers
- Follow the board on the wall — in order — every night
- Give warnings 15, 10, 5 minutes before starting
- Ask "what does your board say is next?" — don't tell
- Praise each step immediately: "Amazing!"
- Same story, same hug, same phrase, lights out
- No exceptions. The routine is the rule.
Teacher / School Communication Template
"Dear [Teacher], Our child is working on sleep routine establishment (D-449). The visual sequencing skills from this technique support school routines and transitions. If you notice improved sequencing behavior, it connects to this home work. Thank you for your partnership."
Family Guide PDF Contents
- Our 7-step sequence with pictures
- What to say at transition warnings
- How to use the visual board ("Ask — don't tell")
- How to give reinforcement after each step
- What NOT to do: skip steps, negotiate, give second story
- If it goes wrong: calm, neutral, silent return
📞 Help getting family on board: 9100 181 181

Frequently Asked Questions
Real questions from real parents at Pinnacle centers across India. These are the most common questions received after families begin implementing D-449.
How long does it take before the routine runs itself?
Most families see meaningful independence by Week 4–6, when the child checks the board proactively. Full independence typically takes 6–10 weeks of consistent implementation. Children with ASD or ADHD may need 3–4 months for full internalization. The board doesn't need to come down — leave it permanently.
Do we need ALL 9 materials to start?
No. Begin with 3: Visual Sequence Board + Progress Tracker + Reward Chart. Add the timer at Week 2, the self-care station at Week 1 if disorganized supplies are an issue, the calm-down kit if wind-down is a consistent problem. Build gradually.
What if my child can't understand pictures on the board?
Try real photos of YOUR child doing each step, in your bathroom and bedroom — these are more concrete than generic pictures. For children needing even more support: real objects (an actual toothbrush mounted beside the board). For SpEd guidance: 9100 181 181.
Is this approach right for autism specifically?
Yes — with adaptations: same sequence every single night (zero variation) · transition warnings are non-negotiable · ritualized ending critically important · sensory accommodations throughout · DO NOT remove the visual board even after mastery — leave it permanently.
My spouse/in-laws don't believe in "systems for bedtime." What do I do?
Share the research from Card 6. Show them your tracking data. Download the Family Guide PDF. Ask for 4 weeks of trying. "4 consistent nights beats 0." Show them the data after 4 weeks. The numbers speak for themselves.
The routine works but my child STILL won't fall asleep after lights out.
The routine and sleep onset are different challenges. D-449 prepares for sleep. If sleep onset is the remaining problem: → D-446: Falling Asleep Independently → Pinnacle NeuroDev specialist for sleep onset evaluation → 9100 181 181
Can I use the same system for morning routine?
Yes. D-455 (Morning Routine Structure) uses identical materials with a different sequence. Parents who master D-449 typically find D-455 takes only 2–3 weeks because the visual board skills fully transfer.
My child is 9 and thinks the picture board is "babyish." Now what?
Transition to written checklist. Or let your 9-year-old DESIGN the checklist themselves — ownership matters. For ADHD: frame it as a "system" or "protocol." Timer-based structure (complete routine by 8:45 PM) works better for older children than step-by-step visual boards.
Didn't find your answer? → Ask GPT-OS®: pinnacleblooms.org/ · Book : pinnacleblooms.org/enroll/
FREE helpline: 9100 181 181
Preview of 9 materials that help with sleep routine Therapy Material
Below is a visual preview of 9 materials that help with sleep routine therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Your Next Step: Start Now
Your child's bedtime routine begins tonight. Not next week. Tonight. Everything you need is on this page. The only remaining step is action.
"Every night without structure is a night your child's circadian system doesn't receive the cues it needs. Tonight is recoverable. Tomorrow is too. But the best night to start is always tonight."
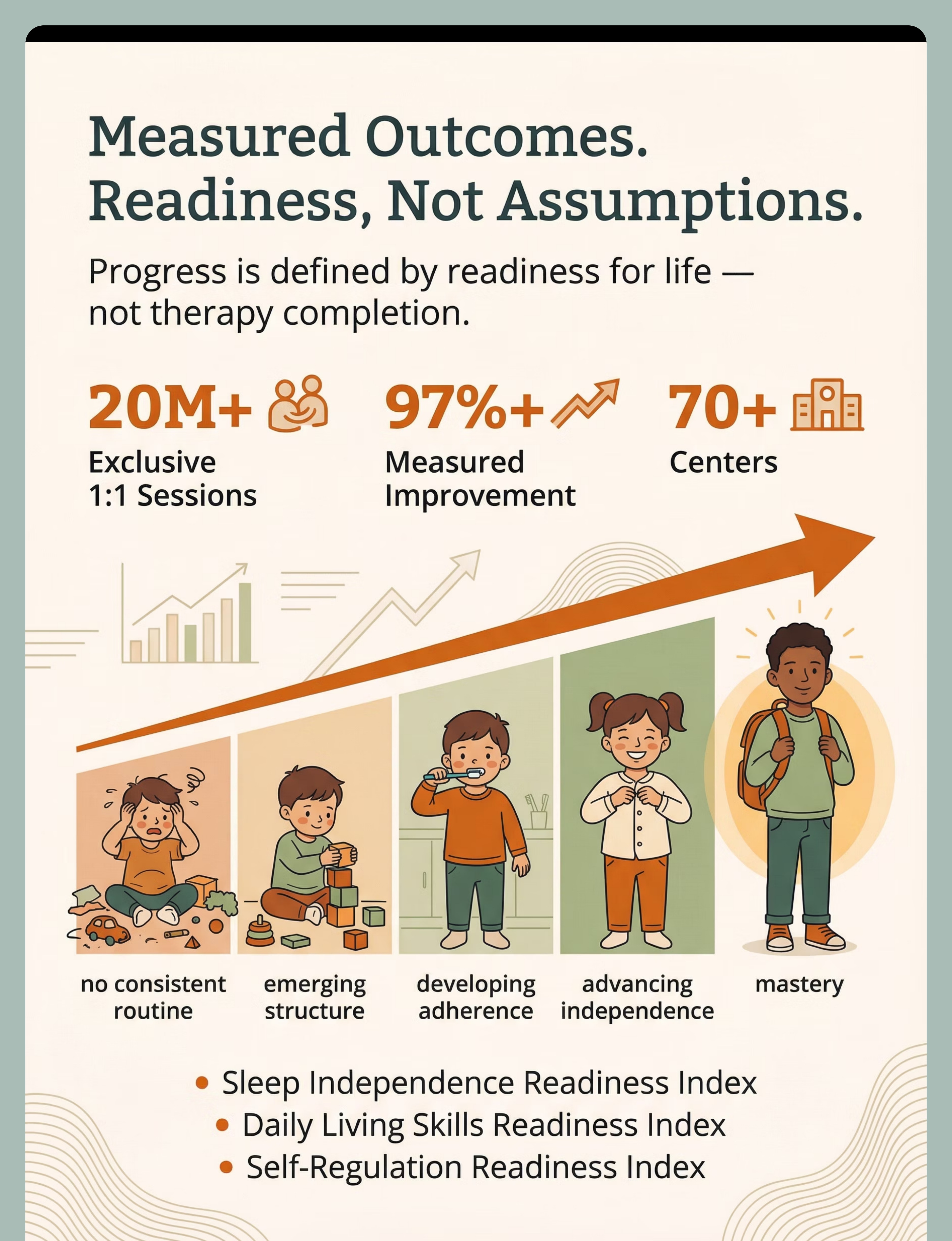
20M+
Therapy Sessions
Exclusive 1:1 sessions across the Pinnacle network
97%+
Measured Improvement
Rate across all intervention domains
70+
Centers Across India
One GPT-OS® clinical standard, nationwide
70+
Countries Served
Global families on the same journey
⬡ VALIDATED BY THE PINNACLE BLOOMS NETWORK® ⬡
OT • ABA/BCBA • SLP • SpEd • NeuroDev Paediatrics
OT • ABA/BCBA • SLP • SpEd • NeuroDev Paediatrics
📞FREE National Autism & Development Helpline: 9100 181 181
Available 24×7 | 16+ Languages | No wait. No appointment.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is for educational purposes only. It does not replace individualized assessment and intervention planning by licensed occupational therapists, behavioral specialists, and healthcare professionals. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Available 24×7 | 16+ Languages | No wait. No appointment.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is for educational purposes only. It does not replace individualized assessment and intervention planning by licensed occupational therapists, behavioral specialists, and healthcare professionals. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.