
When Everything Competes for Attention
Building sustained focus, one evidence-based support at a time.
"He was doing his homework — or trying to. The fan clicked. He looked up. A car passed outside. He turned to the window. I said his name four times before he found his pencil again. By then, three minutes had passed and the problem was still blank."
This is not defiance. This is not laziness. This is a brain that was never designed to filter the world the way most brains do — and it is asking for the right kind of help.
D-444
Executive Function
Ages 3–12
Pinnacle Blooms Network®
You Are Not Alone — The Numbers Are Staggering
Attention dysregulation is not a parenting failure — it is one of the most consistently documented neurodevelopmental differences across all autism and ADHD research. When your child's brain treats the ceiling fan and your spoken instruction as equivalent inputs, sustained focus becomes genuinely neurologically demanding — not a choice.
80%
Experience Attention Issues
of children with autism experience attention regulation difficulties
1 in 36
ASD Diagnosis Rate
children diagnosed with ASD in the US (CDC 2023) — India rates comparable by NIMHANS surveys
21M+
Sessions Delivered
therapy sessions delivered by Pinnacle Blooms Network® across attention and executive function
"You are among millions of families worldwide navigating this exact challenge. The loneliness you feel is disproportionate to the size of this community."
Per Indian J Pediatrics data and NIMHANS national surveys, attention regulation difficulties affect an estimated 1 in 50–70 children in India's pediatric population, with underdiagnosis particularly prevalent in non-metro regions.
What's Happening Inside Your Child's Brain
The Neuroscience
Prefrontal Cortex
The filter — struggles to suppress irrelevant stimuli; underactivated in attention challenges
Locus Coeruleus
Norepinephrine centre — over-responsive to novelty, amplifying distraction signals
Superior Colliculus
Orienting reflex — fires to every new input, pulling attention involuntarily
Thalamus
Sensory gatekeeper — reduced filtering efficiency in ADHD/ASD
What This Means in Real Life
Every sound, movement, and sensation that enters your child's environment travels through a sensory gating system in the thalamus. In most brains, this gate automatically suppresses irrelevant inputs before they reach conscious attention. In children with attention regulation differences, this gate is less selective — more stimuli pass through as "important."
The brain's orientation reflex then fires to each of these inputs, pulling the child's attention toward the new stimulus involuntarily. This is not a decision. The prefrontal cortex faces an uphill battle against a more reactive subcortical system.
This is a wiring difference. Not a behavior choice. Not defiance. Not lack of love for you.
The 9 materials in this page work by either reducing the number of inputs that trigger the orienting reflex, or by giving the prefrontal cortex scaffolding that makes executive filtering easier.

Where Attention Regulation Sits on the Developmental Map
Birth–18 Months
Basic joint attention emerges
18M–3 Years
Sustained attention begins to develop
3–5 Years
Task attention builds — Peak challenge zone begins
5–9 Years
Multi-focus demands grow; academic settings require sustained effort
9–12 Years
Self-monitoring and independent regulation targets
Ages 3–12 represent the peak demand period where academic and social settings require sustained attention that the child's executive system is still developing or specifically differs in. Easy distractibility commonly co-occurs with ASD, ADHD, Sensory Processing Disorder, Anxiety, and Learning Differences.
"Your child is here on this map. The techniques in this series build the neural scaffolding to move forward — not by forcing the brain to work differently, but by giving it the environmental support it needs while it develops."
Clinically Validated. Home-Applicable. Parent-Proven.
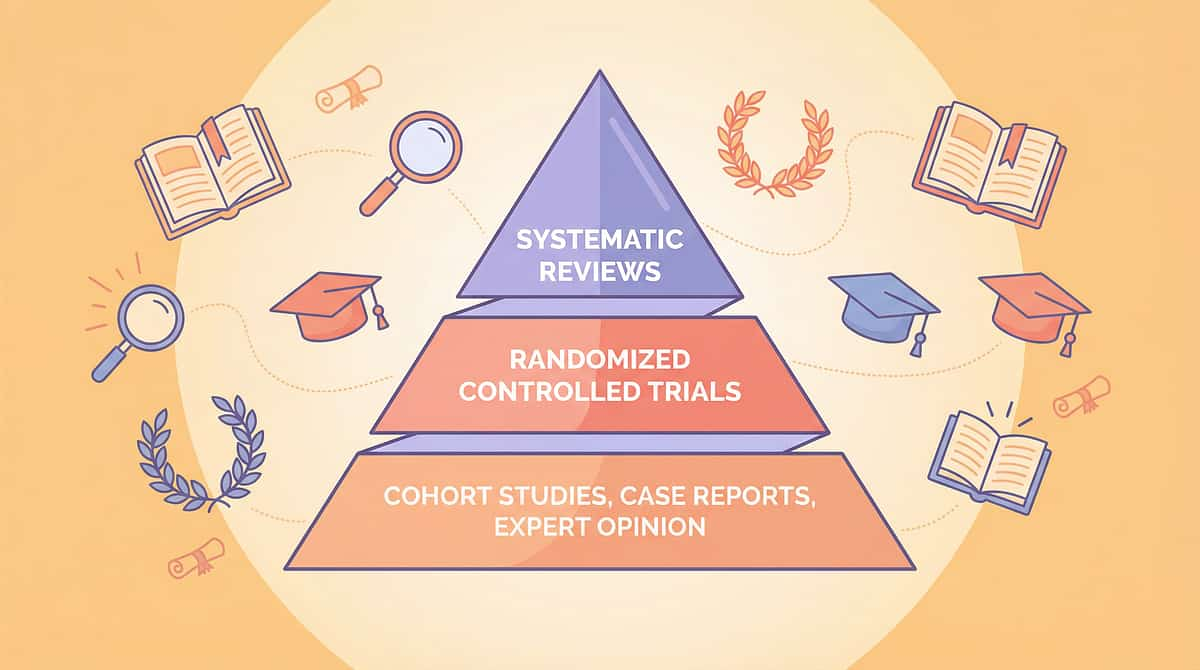
Evidence Grade I–II
Oxford CEBM
Systematic Reviews + RCTs
Systematic Review 2024
16 peer-reviewed articles (2013–2023) confirm environmental modification and material supports for attention meet evidence-based practice criteria for children with ASD. PRISMA methodology. (PMC11506176)
Meta-Analysis 2024
24 studies confirm sensory integration and attention support interventions effectively promote adaptive behavior, attention regulation, and executive function skills across pediatric populations. (PMC10955541)
Indian RCT 2019
Home-based intervention with parent-delivered material supports demonstrated statistically significant outcomes in attention and task completion in Indian pediatric populations. (Padmanabha et al., Indian J Pediatr)
Evidence Confidence
Home Applicability
Parent Deliverable
"Environmental modification and material-based attention supports — when consistently applied — produce measurable, sustained improvements in pediatric attention regulation."

Easy Distraction Support: Environmental & Material Scaffolding
"The Focus Builder" — helping your child's brain filter what matters
D-444
Executive Function
Ages 3–12
10–20 min sessions
6–8 week protocol
Easy Distraction Support is a structured approach to reducing the cognitive burden of attention regulation by modifying the environment and introducing materials that do the filtering work the child's brain struggles to perform independently. Rather than demanding the child "pay attention" — which assumes a level of executive control that may not yet be available — this approach reduces competing stimuli, provides sensory anchoring, makes time concrete, and builds motivational visibility.
The technique is grounded in three complementary clinical frameworks: Sensory Integration Theory (Ayres), TEACCH Structured Teaching, and Applied Behavior Analysis. It bridges OT's environmental modification principles, ABA's antecedent manipulation, and Special Education's structured work systems into a single, home-executable protocol.
Duration
10–20 minutes per session
Frequency
2–3 sessions per day
Setting
Home + School
Lead Discipline
OT + ABA + Special Education

Which Specialists Use This — And Why
Occupational Therapy (Primary Lead)
OTs assess the child's sensory profile and design the environmental modifications and material selection. They determine which type of distraction is dominant and match materials to the child's specific filtering challenge.
Applied Behavior Analysis (ABA / BCBA)
Behavior analysts set up reinforcement schedules linked to attention duration, use First-Then boards as contingency management tools, and train parents in data collection protocols.
Special Education (SpEd)
Special educators implement structured work systems (TEACCH methodology) and design task organization systems that reduce cognitive load, making it easier for attention to be sustained.
Speech-Language Pathology (SLP)
SLPs address how attention difficulties impact language processing. Children who can't sustain attention cannot process multi-step instructions — SLP adapts communication strategies for low-attention states.
NeuroDev Pediatrics
Neurodevelopmental pediatricians provide the diagnostic foundation, rule out medical causes (hearing, vision, seizure), and prescribe or recommend interventions within a comprehensive treatment plan.
CRO / Research Integration
Pinnacle's Clinical Research Organization monitors outcome data across the network, updating evidence-based material recommendations as new research emerges and tracking effectiveness at population scale.
"The brain does not organize itself by therapy discipline. A child's attention system is simultaneously a sensory system, a behavioral system, an executive function system, and a communication system." — Pinnacle Blooms Consortium Clinical Advisory

What Easy Distraction Support Actually Targets
Target | Before Intervention | After 6–8 Weeks | |
Sustained attention | 30–60 seconds on task | 5–15 minutes with material support | |
Prompts required | 8–12 redirections/session | 1–3 minimal cues | |
Task completion rate | <30% of tasks finished | >70% with material scaffolds | |
Self-monitoring | External only | Beginning internal awareness |

9 Materials That Help With Easy Distraction
The exact tools, why each works, and where to get them today. Every material listed below has a free DIY alternative — and a clinical-grade version when you're ready.
1. Visual Focus Frames & Attention Guides
Canon: Visual Supports | Cost: ₹100–400 | DIY Available ✓
Creates clear visual boundaries around important information, reducing visual noise that competes for attention. The brain's superior colliculus stops orienting to peripheral stimuli when the visual field is constrained.

2. Noise-Canceling Headphones & Sound Blockers
Canon: Auditory Supports | Cost: ₹1,500–5,000 | DIY Available ✓
Creates an auditory bubble where environmental sounds cannot trigger the orienting reflex. Essential for children with dominant auditory distractibility — the most common distraction type in open-plan homes and classrooms.

3. Fidget Tools & Sensory Anchors
Canon: Sensory Tools | Cost: ₹150–500 | DIY Available ✓
Provides steady, predictable proprioceptive or tactile input that satisfies the brain's need for sensory stimulation, freeing the attentional system to process the primary task. "Busy hands = focused mind" is neurologically accurate.

Materials 4–6: Time, Space & Motivation

4. Visual Timers & Time Boundaries
Canon: Time Management Materials | Cost: ₹500–1,500 | DIY Available ✓
Converts abstract time into a concrete, visible quantity. The prefrontal cortex can sustain effort more efficiently when the endpoint is visible. "5 more minutes" is meaningless to many children; a diminishing red segment is concrete. Pinnacle Recommends: Smartivity Interactive Clock — ₹673.
5. Work Station Dividers & Focus Carrels
Canon: Environmental Supports | Cost: ₹300–1,200 | DIY Available ✓
Blocks peripheral visual distractions by defining clear spatial boundaries around the workspace. The bounded space signals to the brain: "all relevant stimuli are within this zone." Visual cortex processing narrows; orienting reflex quiets.

6. First-Then Boards & Visual Task Sequences
Canon: Visual Supports | Cost: ₹200–600 | DIY Available ✓
Makes the motivational contingency visible. The prefrontal cortex sustains effort more effectively when the reward is visible and concrete. "Then preferred activity" keeps dopaminergic motivation circuits engaged during difficult focus periods.

Materials 7–9: Work Systems, Movement & Self-Monitoring

7. Structured Work Systems & Task Boxes
Canon: Work Organization Systems | Cost: ₹400–1,000 | DIY Available ✓
Eliminates task uncertainty, which is a major source of internal distraction. When a child doesn't know what to do next, working memory consumes attentional resources on task monitoring rather than task execution. TEACCH structured systems offload this to the environment.
8. Movement Break Cards & Refocus Strategies
Canon: Movement & Sensory Tools | Cost: ₹100–400 | DIY Available ✓
Scheduled movement resets the arousal system. Physical activity increases norepinephrine and dopamine availability in the prefrontal cortex — the same neurotransmitters targeted by stimulant medications for ADHD. Movement breaks are neurological refueling, not behavioral reward.

9. Self-Monitoring Checklists & Attention Tracking Tools
Canon: Self-Management Tools | Cost: ₹50–200 | DIY Available ✓
Metacognitive awareness is the highest-order attention skill — the ability to notice one's own attentional state and self-correct. Self-monitoring tools externalize this process until the child internalizes it. Research confirms self-monitoring decreases adult prompting dependency.
Comprehensive Setup Cost: ₹3,000–10,000 for all 9 materials (professional grade) | Starter Essentials (₹800–1,500): Visual Focus Frames + Visual Timer + First-Then Board

Every Material Has a ₹0 Version — Starting Today
"Every intervention on this page can be executed with household materials. WHO and UNICEF principles demand that evidence-based therapy reach every family, regardless of economic access."
Clinical Material | Household Substitute | Why It Works | |
Visual Focus Frame | Cut rectangle from old cereal box cardboard | Same principle — frames one line of text, blocks visual clutter | |
Noise-Canceling Headphones | Cotton wool balls lightly in ears, or move to quietest room | Reduces auditory input; not as effective but meaningful reduction | |
Fidget Tools | Velcro strip under desk; dried dal in a zip-lock bag; homemade putty (flour + salt + water + oil) | Same proprioceptive/tactile input principle | |
Visual Timer | Sand in a transparent water bottle (timed pour); drawn clock with erasable "pie slice" | Converts time to visible quantity | |
Work Station Dividers | Three ring-binders standing vertically around desk | Creates same visual boundary; zero cost | |
First-Then Board | Folded paper with two sections, draw or paste pictures | Contingency visibility — same motivational mechanism | |
Structured Work System | Two shoeboxes: label "TO DO" (left) and "DONE" (right) | TEACCH principle — left to right task management | |
Movement Break Cards | Index cards with movement drawings: "10 jumps," "5 stretches," "walk to door and back" | Same arousal reset mechanism | |
Self-Monitoring Checklist | Printed paper with 5 boxes per session: ✓ or ✗ "Was I paying attention?" | Same metacognitive activation |
When clinical-grade materials matter: When sensory sensitivity requires precise input calibration, when the child rejects DIY versions, or when progress has plateaued and fidelity to tool quality is the variable.
Safety Gate — Read Before You Begin
🔴 Stop
🟡 Modify
🟢 Proceed
🔴 RED ZONE — Do NOT Proceed If:
- Child is in active meltdown, crying, or showing signs of acute distress
- Child has not eaten in the past 2+ hours (hunger significantly impairs prefrontal function)
- Child is unwell, feverish, or showing signs of illness
- Significant stressor within the past 30 minutes (argument, transition trauma, sensory overload)
- Any medical professional has specifically contraindicated this activity
- Headphones: child has active ear infection or otitis media
🟡 AMBER ZONE — Modify Before Proceeding If:
- Child is tired but not exhausted (shorten session, reduce material complexity)
- Child is showing mild anxiety (skip fidget tools; prioritize focus frames + visual timer only)
- First session with a new material (introduce one material, not all nine)
- School day was particularly stressful (reduce session to 5 minutes maximum)
🟢 GREEN ZONE — Proceed With Confidence When:
- Child has been awake 1–3 hours, has eaten, and has had 15+ minutes of unstructured time
- Child is in a calm-alert state (not lethargic, not hyperactive)
- Environment is prepared and you have 15–20 minutes without interruption
STOP IMMEDIATELY if: Child shows any sign of self-harm | Child becomes inconsolably distressed | Staring spells or unresponsiveness (seizure rule-out) | Behavior escalates after 5 minutes. Call FREE Helpline: 9100 181 181 — 24×7, 18+ languages

Prepare the Focus Zone — Your Room Setup Guide
Child Position
Facing a blank wall or work station divider. Back to the room entrance. Chair at correct height — feet flat on floor, hips at 90°. Desk at elbow height.
Parent Position
Slightly behind and to the side — within reach but not in the child's visual field. Sitting, not looming. Calm body language.
Materials Tray
Pre-loaded with today's session materials only. Start with 1–2 materials per session. Introduce new materials over weeks, not days.
Work Station Divider
Place 3-sided barrier around the work area. Height: above child's eye level when seated. Introduce as "your special focus space" with positive framing.
Remove Distractors
Screen off or covered. Toys not in session: removed or out of sight. Pets outside the room. Siblings occupied elsewhere if possible.
Visual Timer Placement
Placed at child's eye level on desk edge. Set before beginning. Child sees remaining time throughout the session. Door closed; family notified session is in progress.
Environmental Checklist: Lighting: natural or warm (not fluorescent if light-sensitive) · Temperature: comfortable · Sound: background reduced · Smell: neutral · Wall behind child: plain and calm

Pre-Session Readiness Check — 60 Seconds
Before every session, run this 7-point check. A postponed session is not a failed session — it is expert-level clinical judgment.
Readiness Indicator | If NO — What to Do | ✓/✗ | |
Child has eaten within the last 2 hours | Offer a small snack; wait 15 minutes | ☐ | |
Child is not showing signs of tiredness | Postpone to after rest | ☐ | |
Child has had at least 10 min of unstructured play | Allow free play time first | ☐ | |
Child's body is calm (not hyperactive or dysregulated) | 5 min proprioceptive warm-up: wall push-ups, jumping | ☐ | |
No major stressor in last 30 minutes | Postpone; offer co-regulation support first | ☐ | |
Child makes eye contact or shows awareness of your presence | Check for medical concerns; consult if persistent | ☐ | |
You (the parent) have 15 uninterrupted minutes and are calm | Reschedule session — parent state transfers to child | ☐ |
🟢 7/7 or 6/7 — GO
Proceed to Step 1. Full session.
🟡 4–5/7 — MODIFY
5-minute session, 1 material only, lowest demand task.
🔴 3 or fewer — POSTPONE
Not today's window. Try again in 1–2 hours. Record what prevented readiness.

Step 1 of 6
STEP 1: The Invitation
⏱ Duration: 30–60 seconds
"Hey — I have something cool to show you. Want to try something with me for a few minutes? [Show material]. This is your focus frame / special timer / focus spot."
Acceptance Cues — Child IS Interested
- Looks at the material
- Reaches toward it or moves closer
- Vocalizes interest
- Sits down near the workspace
Resistance Cues — Child Is NOT Ready
- Turns away and moves to another activity
- Pushes the material away firmly
- Vocalizes protest or distress
- Engages in repetitive behavior intensification
If resistance: Say: "Okay, no problem. We can try later." Return to the readiness check. Resistance is data, not failure.
ABA Principle: This is the Pairing phase — establishing yourself and the materials as predictors of positive experience before any demand is placed.
Step 2 of 6
STEP 2: The Engagement
⏱ Duration: 1–3 minutes
Introduce the first material by doing it together, not instructing the child to do it. Show how it works with your own hands first. The child observes, then participates. Do not rush to the task — 1–3 minutes of material exploration is productive therapeutic time, not delay.
For Focus Frame
"Watch — I put this over the page like this and now we can only see this one problem. Cool, right? Want to try?"
For Visual Timer
"This red part shows how much time we have. See it go down? When it's all gone, we're done for today."
For Fidget Tool
"This is yours to hold while you work. You can squish it / twist it / rub it any time you want."
For Work Station Divider
"This is your focus space — it's YOUR special thinking spot. Only the good stuff is in here."
Reinforcement cue: The moment the child touches, explores, or approaches the material: "Yes! That's it. You've got it." Immediate, specific, warm — not effusive.

Step 3 of 6
STEP 3: The Therapeutic Action
⏱ Duration: 5–12 minutes (core focus period)
Prompting Hierarchy (if needed — in order)
- Visual prompt — tap the focus frame or timer
- Gestural — point toward task without speaking
- Positional — move slightly closer
- Verbal — whisper: "Back to your work"
- Physical proximity increase — only if all else fails
Session Length by Attention Baseline
- Baseline 30–60 sec: Set timer for 2–3 minutes
- Baseline 1–3 min: Set timer for 4–6 minutes
- Baseline 3–5 min: Set timer for 7–10 minutes
- Never extend beyond current maximum + 20%
Common Execution Errors:❌ Sitting too close in the visual field | ❌ Prompting every 10–15 seconds | ❌ Task too long for current attention capacity | ❌ Too many new materials at once

Step 4 of 6
STEP 4: Repeat & Vary
⏱ Duration: 3–5 minutes per block × 2–3 blocks
"3 successful focus blocks per session > 10 forced, distressed attempts."
Block 1
Introduce material + task → Focus period → Reinforce → 2-min free break
Block 2
Same material + new task → Focus period (slightly longer) → Reinforce → 2-min free break
Block 3
Same material + child's choice of task → Focus period → Reinforce → Session close
Sandwich structure for tasks: Preferred subject → Less-preferred subject → Preferred subject. This maintains motivational engagement across all three blocks.
Satiation Indicators — the child has had enough: Quality of engagement declining despite material support | Fidget tool becoming a distraction | Increased time to return after drift | Physical signs of fatigue (slumping, head on hand)

Step 5 of 6
STEP 5: Reinforce & Celebrate
⏱ Timing: Within 3 seconds of desired behavior
"Timing matters more than magnitude. A whispered 'Yes!' delivered within 2 seconds is more powerful than a sticker chart updated the next morning."
Social Reinforcement
High five, hug, fist bump, thumbs up, celebratory look — immediate and genuine, matching the child's enthusiasm level
Token Economy
Sticker on chart → trade for preferred item after X stickers. Rosette Imprint Reward Jar — ₹589 | 1800+ Reward Stickers — ₹364
Activity Reinforcement
5 minutes of preferred activity — the "then" from the First-Then board, delivered immediately
Celebrate the attempt: "You tried to come back to your work. I saw that. That counts." Even imperfect engagement receives reinforcement. Graduated reinforcement builds approach behavior. Behavior occurs → 0–3 seconds → Reinforcement delivered. This window is non-negotiable.

Step 6 of 6
STEP 6: The Cool-Down
⏱ Duration: 2–3 minutes
No session ends abruptly. Abrupt endings create transition resistance that bleeds into the next session. A structured cool-down teaches the child that endings are safe, predictable, and followed by something enjoyable.
2-Minute Warning
"Two more — then all done for today. You've done a great job."
1-Minute Warning
"One more. When the timer goes, we're done and it's [preferred activity] time."
Material Put-Away Ritual
Child participates in tidy-up as transition ritual. 30-second heavy work if arousal remains elevated (carry books to shelf, push chair in).
Connecting Moment
Brief non-task conversation or shared observation. A small transition object (fidget tool, sticker) can accompany the child as a physical bridge.
If child resists ending: Do not extend session — this reinforces resistance. Countdown: "5... 4... 3... 2... 1... All done! Great work." Update First-Then board to reflect what comes next.

60 Seconds of Data Now — Hours of Clarity Later
Fill in these three fields immediately after every session. This data is the difference between hope and evidence.
Field 1 — Session Date & Duration
[Date] | [Minutes completed] — record immediately while memory is fresh
Field 2 — Focus Quality Rating (1–5)
- 1 = Child could not engage / session abandoned
- 2 = Brief engagement only (<1 minute sustained)
- 3 = Moderate engagement, frequent prompts needed
- 4 = Good engagement, 1–3 prompts, most task completed
- 5 = Excellent engagement, self-corrected attention, task completed
Field 3 — Notable Observation
One sentence. What worked? What didn't? Which material helped most today?
Week 1 data compared to Week 6 data shows you — with evidence, not hope — that progress is happening. When the child has a hard day, you look at the data and remember: "3 weeks ago, we couldn't get through 2 minutes. Today was 8 minutes." That is the antidote to despair.

Session Didn't Go as Planned? Here's Your Immediate Fix.
"Session abandonment is not failure — it is data. Every imperfect session teaches you something that makes the next one better. Pinnacle's therapists have imperfect sessions too."
Child refused to sit at the focus station
Why: New environment/materials often trigger initial avoidance. Fix: Don't demand sitting today. Let the child explore from standing or floor. Tomorrow: sit for 30 seconds only, heavily reinforced. Build duration from 30 seconds up.
Child watched the fidget tool instead of the task
Why: Visual fidgets become competing distractors for visual learners. Fix: Switch to tactile-only fidget (under-desk Velcro, therapy putty out of sight). Fidget must be automatic, not visual.
Child took off the headphones within 1 minute
Why: Sensory tolerance to headphones requires gradual habituation. Headphones may be too tight, too heavy, or uncomfortable. Fix: Start with headphones worn for 30 seconds off-task, then build. Try lighter ear defenders or loop earplugs.
Visual timer increased anxiety ("Is it almost over?")
Why: Some children with anxiety find visible countdowns anxiety-provoking. Fix: Turn timer away from the child, switch to a sand timer the child controls, or remove timer entirely and use verbal "2 more minutes."

More Troubleshooting: Common Scenarios
Child completed 1 task then immediately asked for the "then" activity
Why: The "then" is too proximal and too salient — pulling attention toward reward rather than task. Fix: Extend the "first" requirement: "First finish all 3 problems, then iPad." Use a checklist showing 3 tasks to complete before reward delivery.
Child became more distractible when all materials were introduced
Why: Too much novelty at once. New materials require attentional resources to process — defeating their purpose. Fix: One new material per week. Maintain all others as familiar tools. Novelty and attention support cannot coexist in early implementation.
Parent became frustrated during the session
Why: Parent frustration is a real, documented phenomenon. It is also contagious — children read parent emotional state and mirror it. Fix: Stop the session warmly. "Let's take a break. We'll try again later." This is not failure — this is the most clinically skilled thing a parent can do. Call 9100 181 181 for parent support.
📞FREE National Autism Helpline: 9100 181 181 — 24×7 · 18+ Languages. Call anytime — for your child or for yourself.
Every Child Is Different — Here's How to Tune the Protocol
Easier Modifications
For bad days, first weeks, high anxiety
- Session duration: 2–3 minutes maximum
- Materials: 1 only (start with visual timer)
- Task demand: zero demand ("just sit here with me")
- Reinforcement: continuous every 30 seconds
- Parent proximity: close
Harder Modifications
For weeks 5–8, strong progress
- Session duration: 15–20 minutes
- Materials: 3–4 in combination
- Task demand: grade-level academic material
- Reinforcement: intermittent every 3–4 minutes
- Parent proximity: across room
Age | Primary Materials | Session Length | Reinforcement | |
3–5 years | Visual timer + First-Then board | 3–5 minutes | Every 1–2 min | |
5–8 years | All 9 materials as appropriate | 8–12 minutes | Every 3–5 min | |
8–12 years | Self-monitoring + structured work systems | 12–20 minutes | Natural + intermittent |
Weeks 1–2: What "Progress" Actually Looks Like
Most parents expect visible change in week 1. Here is what actually happens — and why it counts as real, measurable neurological progress.
Protocol Progress
Weeks 1–2 position in the 8-week protocol
✓ Progress in Weeks 1–2 Looks Like:
- Child accepts one material without active rejection
- Child sits at the focus station for 1–2 minutes (up from 30 seconds)
- Child glances at the visual timer during work
- Parent completes 2–3 sessions without escalation
- One session out of five goes smoothly — that is the neural seed
✗ What Is NOT Expected Yet:
- Sustained independent focus
- Generalizing to school
- Task completion without prompting
- Reduced prompts (may actually increase as child explores new materials)
"If your child tolerates the focus frame for 30 more seconds than last week — that is measurable neurological adaptation. That is the brain forming new pathways. Write it down."

Weeks 3–4: The Neural Pathways Are Forming
Protocol Progress
Weeks 3–4 consolidation phase
Routine Anticipation
Child anticipates the focus station routine — moves toward it, picks up familiar material unprompted
Reduced Resistance
From active avoidance to neutral acceptance at session start — a significant behavioral shift
Self-Return to Task
Occurring before parent prompt at least once per session — the executive function skill is beginning to internalize
Generalization Seeds
Child uses a material in a novel context — asks for "the focus frame" for homework without being asked
Frequency Recommendation for Weeks 3–4: Increase to 3 sessions per day if Weeks 1–2 showed tolerance and acceptance. More exposure during consolidation phase accelerates neural pathway strengthening.
"You may notice you are more confident. You know the protocol. You know the materials. You are becoming the expert on your child's attention system. That confidence transfers."
"You may notice you are more confident. You know the protocol. You know the materials. You are becoming the expert on your child's attention system. That confidence transfers."

Weeks 5–8: Mastery — The Moment the Skill Belongs to Your Child
Protocol Progress
Weeks 5–8 — Mastery Zone Approaching 🏆
Mastery Criteria — Specific, Observable, Measurable
10+ Minutes Sustained
Child sustains attention for 10+ minutes with material support during structured sessions
1–2 Prompts per Session
Adult prompts reduced from 8–12 at baseline to just 1–2 per session
Independent Tool Use
Child independently reaches for attention support material before starting tasks without adult reminder
Self-Monitoring Active
Self-monitoring checklist used without prompting at least 50% of sessions
70%+ Task Completion
Task completion rate exceeds 70% of assigned work; at least one generalization observed in school
🏆 "When your child reaches self-monitoring mastery, they own an executive function skill that will serve them for life. Not a crutch — a capability."

🎉 You Did This.
Your child grew because of your commitment, your consistency, and your refusal to accept that "this is just how they are."
Where You Started
- Constant adult prompting every session
- Frequent task abandonment
- Active session resistance
- No independent tool use
Where You Are Now
- Material-supported sustained focus
- Reduced prompts — 1 to 2 per session
- Task completion exceeding 70%
- Early self-monitoring emerging
In 6–8 weeks, you built a focus scaffolding system from scratch. You learned 9 materials and their neuroscience. You executed a clinical protocol — the same one Pinnacle's therapists use — at home, in your own space, with your own child.
📸"Take a photo of your child at their focus station today. In 6 months, you will show them this photo and say: 'This is where you learned to focus. This is where you became yourself.'"
🚨 Red Flags — When to Pause and Seek Professional Guidance
"Even in the progress zone, these specific signs mean stop and consult. Not because something is wrong — because something specific needs professional attention."
🔴 Staring Spells or Unresponsiveness
Child "blanks out" — stares with no response to name, voice, or touch for 10+ seconds. Absence seizures can mimic attention difficulties. Do: Stop all intervention. Consult pediatrician immediately. Video the episode if possible.
🔴 Sudden Dramatic Change in Attention
Child who was improving suddenly shows marked regression within days. Often has a medical cause (illness, ear infection, medication change). Do: Rule out medical causes first. Pause protocol. Consult healthcare provider.
🔴 Attention Problems Only in Specific Environments
Child focuses well at home but not at school — or vice versa — consistently. Suggests the environment, not the child's attention system, is the issue. Do: Request school-based OT/behavioral assessment.
🔴 Self-Harm During or After Sessions
Child head-bangs, bites self, or engages in self-injurious behavior. Session demands may be exceeding the child's regulatory capacity. Do: Stop sessions immediately. Call 9100 181 181.
🔴 No Improvement After 8 Weeks
Data shows no improvement despite consistent implementation. Protocol may not match this child's specific attention profile. Do: Book AbilityScore® assessment at nearest Pinnacle center.
🔴 Attention Challenges Interfering with Safety
Distractibility causes safety incidents (running toward roads, not responding to safety cues). Requires clinical-grade intervention, not home protocol alone. Do: Immediate professional consultation.
D-444 in the Executive Function Journey — Your Developmental GPS
Highly Effective + Generalizing
→ Move to D-445 (Losing Track of Time)
Worked but Task Initiation Remains
→ Move to D-446 (Task Initiation Difficulties)
Mastered but Material-Dependent
→ Self-Monitoring advanced tracks within D-444 before progression
Long-term developmental goal: All executive function techniques feed into Independent Study Skills → Academic Self-Management → Lifelong Adaptive Functioning.
Related Techniques — Your Attention & Executive Function Series
The materials you've already acquired from D-444 carry forward — your investment extends across the entire executive function pathway.
Technique | Focus Area | Difficulty | Materials You Already Have | |
D-441 | Understanding Attention Differences | 🟢 Intro | Knowledge-based — no new materials | |
D-442 | Attention Duration Building | 🟡 Core | Visual timer ✓ from D-444 | |
D-443 | Multi-Step Direction Following | 🟡 Core | First-Then board ✓ from D-444 | |
D-445 | Losing Track of Time | 🟡 Core | Visual timer ✓ from D-444 | |
D-446 | Task Initiation | 🔴 Advanced | Work system ✓ from D-444 | |
D-450 | Working Memory Challenges | 🔴 Advanced | Focus frame ✓ from D-444 |
✅ Materials from D-444 cover 4 of the next 5 techniques in this series. Your investment in these 9 materials extends across the entire executive function pathway.
D-444 in Your Child's Complete Developmental Landscape
Primary Domain
Executive Function → Attention & Focus
Secondary Domain
Learning Readiness — attention is the foundation of all learning
Tertiary Domains
Social Communication + Emotional Regulation — competence in focus reduces frustration meltdowns
GPT-OS® Integration: D-444's data contributes to your child's Learning & Academic Readiness Index and is reviewed by your assigned clinical team. Your home session data is clinical evidence — not just family record-keeping.
→ View your child's full developmental profile at pinnacleblooms.org/gpt-os
→ View your child's full developmental profile at pinnacleblooms.org/gpt-os
Three Families. Three Stories. One Journey.
Note: Anonymized. Names changed. Outcomes verified from Pinnacle Network centers. Individual results vary.
Rohan, Age 6, Hyderabad — ASD Level 2
Before: "Rohan's homework took 3 hours every evening. He would start a problem, look at his pencil, put the pencil down, look at his brother's room, call out for water — and we would be back at problem 1. I cried more evenings than I didn't."
After 8 weeks: "He does his homework in 35 minutes now. He now asks for the timer before we even set it up. He says 'red goes down, then iPad' and he stays."
Therapist's Note: 340% increase in task-completion rate from Week 1 to Week 8.
Ananya, Age 9, Mumbai — ADHD + Learning Differences
Before: "The noise in the classroom was just everywhere for her. She'd come home completely drained from the effort of holding herself together all day."
After 8 weeks + school implementation: "Ananya now wears ear defenders during independent work. Her grades are not the point — she comes home with energy left. That is the point."
Therapist's Note: Generalization to school setting within 6 weeks using noise-canceling headphones + self-monitoring checklist.
Vikram, Age 5, Bengaluru — ASD Level 1
Before: "He couldn't sit for even 2 minutes. Everything called to him — the ceiling fan, a sound outside, his own fingers. We felt like we were failing him every single day."
After 8 weeks: "He says 'Am I paying attention?' out loud to himself when he drifts. He is 5 years old and he is his own attention coach. I still can't believe that's my son."
Therapist's Note: Self-monitoring introduced in Week 6, following 5 weeks of environmental support.
📞FREE National Autism Helpline: 9100 181 181 — 24×7 · 18+ Languages

You Are Not Doing This Alone
D-444 Parent WhatsApp Group
Parents navigating attention regulation challenges. Share what works, ask questions, support each other's hard days. Join the group
Pinnacle Online Forum
Discussion threads specific to executive function and attention regulation, moderated by Pinnacle clinical staff. pinnacleblooms.org/forum
Local Parent Meetups
70+ centers across India host monthly parent support sessions. Find your nearest center's next meetup
Peer Mentoring Program
Connect with a parent who has completed the D-444 protocol — living-room wisdom, not clinical authority. Request a peer mentor
"Your experience helps others. The parent who read this page in terror 6 months ago is the expert that the parent who found it today needs. Consider sharing your journey when you're ready."

Home + Clinic = Maximum Impact
70+ Pinnacle centers across India operate under GPT-OS® clinical standards. Every center uses the same materials, the same evidence framework, the same data system — ensuring what you do at home and what happens in clinic are synchronized.
🔵 Occupational Therapists
Sensory profile assessment and environmental modification design for D-444
🟢 BCBAs / ABA Therapists
Reinforcement protocols and attention data tracking
🟡 Special Education Specialists
Structured work system design and academic adaptation
Not near a center? Teleconsultation available for material selection guidance, protocol troubleshooting, data review, and parent training. Insurance and funding options available — ask your nearest center.
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 18+ Languages
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 18+ Languages
The Science Behind D-444 — For the Curious Parent
PRISMA Systematic Review (Children, 2024)
16 peer-reviewed articles (2013–2023) confirm environmental modification meets evidence-based practice criteria for attention support in ASD. PubMed: PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
24 studies confirm attention and behavioral support interventions promote adaptive behavior and executive function skills across pediatric populations. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT (Indian J Pediatrics, 2019)
Home-based parent-delivered material interventions show statistically significant outcomes in Indian children with developmental challenges. DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al.
WHO Care for Child Development (2023)
Age-specific caregiver-delivered interventions proven in 54 LMICs, establishing the evidence base for parent-delivered home protocols. PMC9978394
NCAEP Evidence-Based Practices (2020)
Confirms visual supports, structured work systems, self-monitoring, and reinforcement as evidence-based practices for autism spectrum disorders. NCAEP Report 2020

Your Data. Your Child's Progress. The World's Learning.
What GPT-OS® Learns from D-444
- Which of the 9 materials showed strongest correlation with attention improvement
- Rate of attention duration increase per week
- Environmental and time-of-day factors affecting session quality
- Parent implementation fidelity patterns
Privacy Assurance
- 🔒 Data encrypted (ISO/IEC 27001 compliant)
- 🔒 Child data never sold or shared
- 🔒 Parent is the data controller; delete anytime
- 🔒 DPIIT DIPP8651 registered (Government of India)
"When you log today's session, you are doing two things: tracking your child's progress, and contributing to the collective intelligence that helps every child like yours, everywhere. Your data has reach you cannot imagine."

Frequently Asked Questions
Generated from Pinnacle center clinical FAQ database and parent community query patterns.
My child already uses materials in the clinic. Does this page add anything?
Yes. The clinic context is controlled. Home — where the child spends 90% of waking hours — is the generalization environment. Clinic + home consistency is the formula for outcomes.
My child has both autism and ADHD. Do I use the same materials?
Yes — the 9 materials address attention regulation regardless of diagnosis. ADHD profiles typically respond strongly to movement breaks and visual timers; ASD profiles often respond strongest to structured work systems and visual focus frames. Start with the full protocol — the data will show you which materials to prioritize.
My child is 12 — isn't this too young-focused?
The materials scale. A 12-year-old uses noise-canceling headphones and self-monitoring checklists — not the same format as a 4-year-old's picture-based First-Then board. See Card 25 for specific age adaptations.
How do I know if it's the material that helped or just a good day?
The data. One session is a data point. Eight weeks of data is a pattern. If focus quality ratings trend upward over 6–8 weeks and correlate with material use, the materials are working.
My child's school refuses to allow noise-canceling headphones in class.
Request an OT assessment letter from your Pinnacle therapist. A formal recommendation from a licensed OT carries weight that parent preference does not. Many states have provisions under the Rights of Persons with Disabilities Act 2016 for reasonable accommodation of assistive materials in educational settings.
My child is non-speaking. Do these materials still work?
Yes — all 9 materials are non-verbal. They work through environmental and sensory mechanisms, not linguistic understanding. Non-speaking children often show the strongest responses to visual and sensory materials because they rely on environmental information more heavily.
Preview of 9 materials that help with easy distraction Therapy Material
Below is a visual preview of 9 materials that help with easy distraction therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

Your Child's Focus Journey Starts Now.
Not after the assessment. Not after the school meeting. Now. With what you have. In your home.
🔵 OT
Occupational Therapy
🟢 ABA
Behavior Analysis
🟡 SLP
Speech-Language Pathology
🟠 SpEd
Special Education
🔴 NeuroDev
Neurodevelopmental Pediatrics
⚡ CRO
Clinical Research Organization
"From fear to mastery. One technique at a time." — Pinnacle Blooms Network®
Next Technique:D-445: Losing Track of Time — If your child can't tell when 5 minutes has passed or when to stop, the next page was written for you.
This content is for educational purposes only. It does not constitute medical diagnosis, clinical assessment, or a substitute for evaluation by a licensed occupational therapist, behavior analyst, speech-language pathologist, or physician. Individual results vary based on child profile, implementation consistency, and clinical factors.
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: Udyog Aadhaar TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All Rights Reserved. | techniques.pinnacleblooms.org
📞9100 181 181 · 24×7 · FREE · 18+ Languages · care@pinnacleblooms.org