"It's midnight. He's still awake. I've done everything I can think of."
You are not failing. Your child's brain is wired differently at night — and tonight, that changes.
🌙 SLEEP INITIATION SUPPORT
Materials Protocol
D-446
Bedtime has become a battle. Not because your child won't sleep — but because their nervous system genuinely cannot find the off-switch. Sleep initiation difficulties in autism are neurological, not behavioral. The right materials don't just help — they transform the bedroom into the most therapeutic space in your home.
"You are not failing. Your child's nervous system is speaking a language most parents were never taught. This page teaches you that language." — Pinnacle Blooms Consortium® | OT · SLP · ABA · SpEd · NeuroDev · Pediatrics
You Are Among Millions of Families Navigating This Tonight
Sleep onset insomnia in autism is not a phase. It is not bad parenting. It is a neurological reality documented in peer-reviewed research across 54 countries.
50–80%
Affected by Sleep Difficulties
of children with autism experience significant sleep difficulties — classified as a primary clinical challenge by the American Academy of Sleep Medicine
1 in 36
Children in India
are on the autism spectrum — millions of families awake right now, navigating this same challenge every single night
3–4x
More Likely
to have sleep initiation problems than neurotypical peers — a documented neurobiological difference, not a parenting failure
"If your child struggles to fall asleep — you are among the largest community of exhausted, devoted, determined parents on Earth."
Pinnacle Blooms Network® has delivered 21 million+ exclusive 1:1 therapy sessions across 70+ centers in India. Sleep regulation is among the top 3 presenting challenges in every new family intake. You are not alone — you are surrounded.

Why Their Brain Won't Switch Off
Understanding the neuroscience behind your child's sleep difficulties is the first step toward solving them — with compassion and precision.
🧠 The Circadian Clock Difference
In autistic children, the pineal gland often produces melatonin later and in smaller amounts — a documented neurobiological difference, not a choice. The brain's internal clock is desynchronized from the external clock.
⚡ Sensory Arousal at Night
The somatosensory cortex remains in heightened alert mode even at night. Sounds that neurotypical children sleep through register as urgent stimuli demanding attention.
🔄 The Arousal Regulation Loop
The autonomic nervous system struggles to shift from sympathetic ("fight/flight") to parasympathetic ("rest/digest") mode. The body physically cannot relax without the right sensory input.
💭 The Racing Mind
Executive function differences mean the prefrontal cortex continues processing the day's events long after bedtime. The "off switch" requires external scaffolding.
"His brain is like a computer that won't shut down. The power button works differently — and we have materials that help press it."
Your child is not defying you. Their brain is not defective. Their nervous system needs specific sensory input — the kind these 9 materials provide — to find the pathway into sleep.
This is a wiring difference, not a behavior problem. The same sensory processing differences that make your child brilliant in some ways also make nighttime harder. Both are real. Both deserve support.

Your Child's Sleep Challenge on the Developmental Map
Sleep initiation difficulties most commonly emerge and peak between ages 2–8 in autistic children — precisely the window when sensory processing demands are highest and language to communicate discomfort is still developing.
This is not a sign that development has stopped. It is a sign that the nervous system needs structured support to complete this developmental task.
What Commonly Co-occurs
- Sensory processing differences (tactile, auditory, visual sensitivity)
- Anxiety and bedtime-specific fear
- Heightened cortisol levels in the evening
- Gastrointestinal discomfort (often unspoken)
- Separation anxiety
GPT-OS® Tracking Domain
This technique contributes to the Daily Living & Independence Index within GPT-OS® — specifically the Sleep Regulation sub-index.
Progression stages: Supported Onset → Reduced Latency → Independent Initiation → Maintained Patterns → Generalization
🗺️"Your child is here. Here is where we're heading: independent sleep initiation within a predictable, sensory-optimized routine — with measurable progress in 4–8 weeks."
Clinically Validated. Home-Applicable. Parent-Proven.
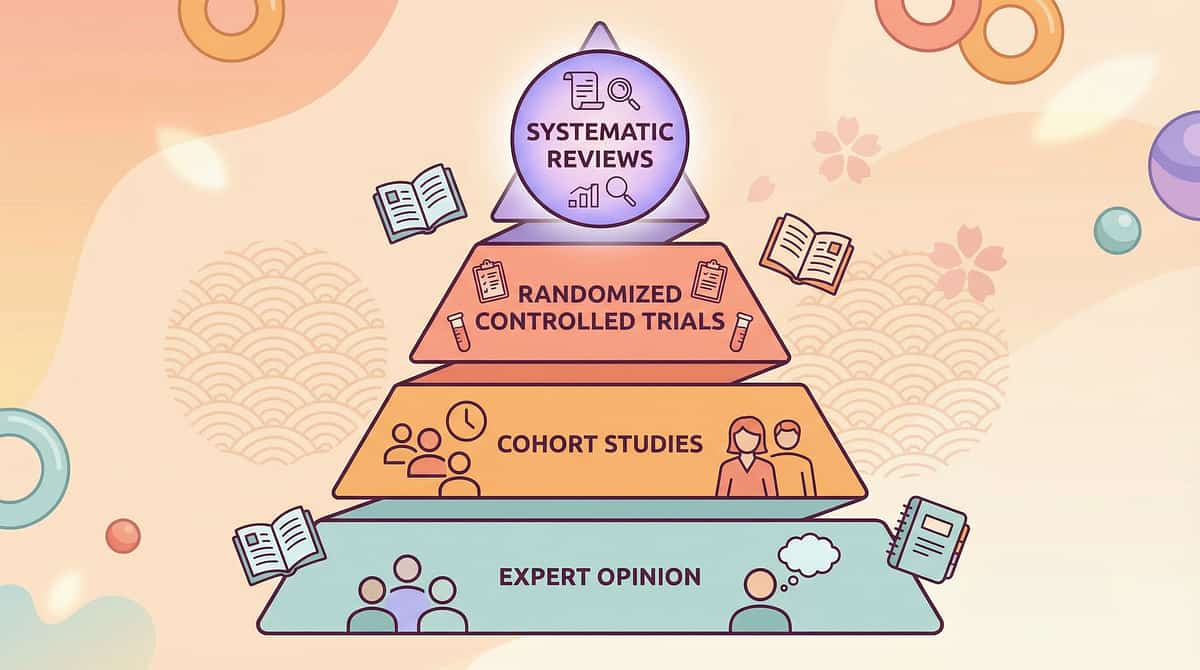
🛡️ EVIDENCE GRADE: LEVEL II
Systematic Review + RCT Data
Confidence: 80%
📊 PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm sensory-based environmental materials meet criteria for evidence-based practice in autism sleep and regulation. Read on PubMed: PMC11506176
📊 Meta-Analysis, World J Clin Cases (2024)
Across 24 studies, sensory integration materials effectively promoted adaptive behavior, self-regulation, and sleep quality in pediatric autism populations. PMC10955541
📊 Indian RCT, Padmanabha et al. (2019)
Home-based sensory intervention protocol demonstrated significant outcomes in Indian pediatric populations — validating that clinic-grade results are achievable at home. Indian Journal of Pediatrics.
"These are not wellness trends. These are materials prescribed by pediatric occupational therapists, validated in peer-reviewed research, and refined across 21 million therapy sessions."
NCAEP (2020) Evidence-Based Practices included in this protocol: Visual supports · Reinforcement · Antecedent-based interventions · Parent-implemented intervention
🌙 Sleep Initiation Support Protocol
Parent-friendly alias:"The Bedtime Environment System"
Sleep Initiation Support is a multi-material, sensory-optimized home protocol designed to regulate the child's arousal system, establish predictable pre-sleep cues, and create the environmental conditions in which the nervous system can safely transition into sleep onset. It combines deep pressure input, visual predictability, auditory and olfactory conditioning, and light management to systematically reduce sleep latency.
🎯 Ages 2–12 Years
Developmentally calibrated across the full early-childhood window
⏱️ 15–30 Min Nightly
Brief, consistent, home-executable without professional presence
🏠 Parent-Delivered
Designed for daily home implementation — WHO-aligned
📅 Daily Protocol
Consistency is the mechanism. Every night, same sequence
The 9 Materials at a Glance
- Weighted Blankets
- Visual Bedtime Routine Charts
- White Noise Machines
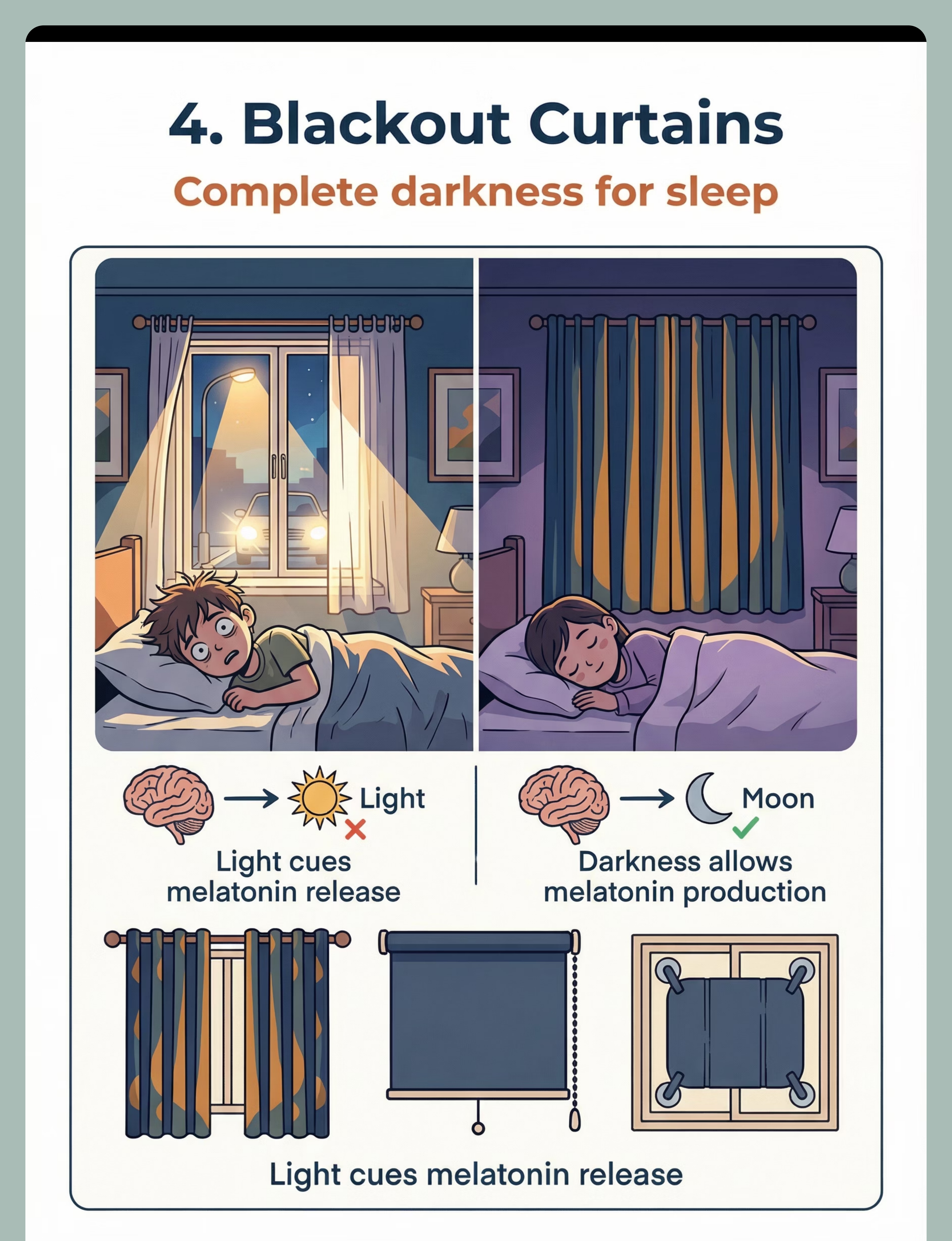
- Blackout Curtains
- Comfort Objects
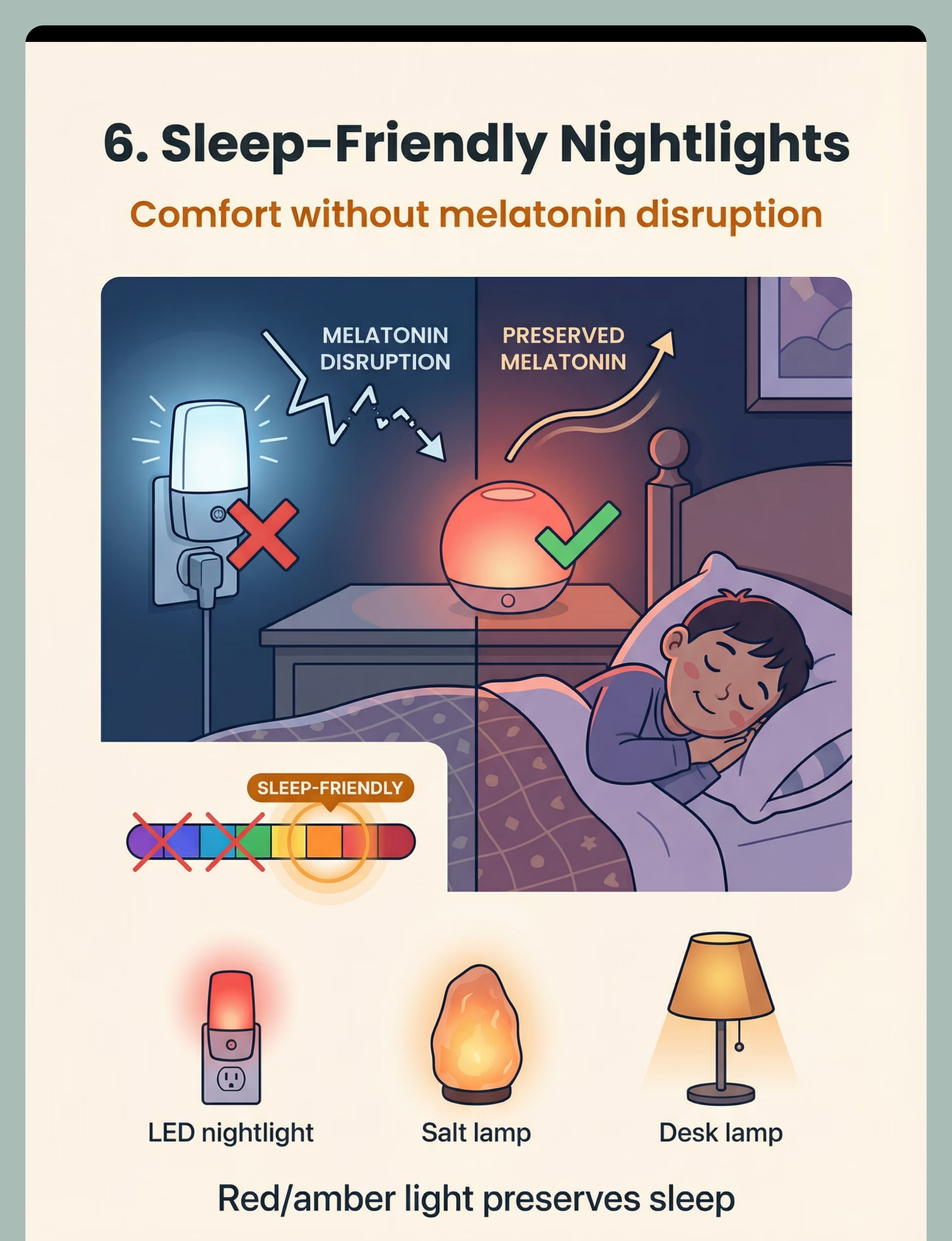
- Red/Amber Nightlights
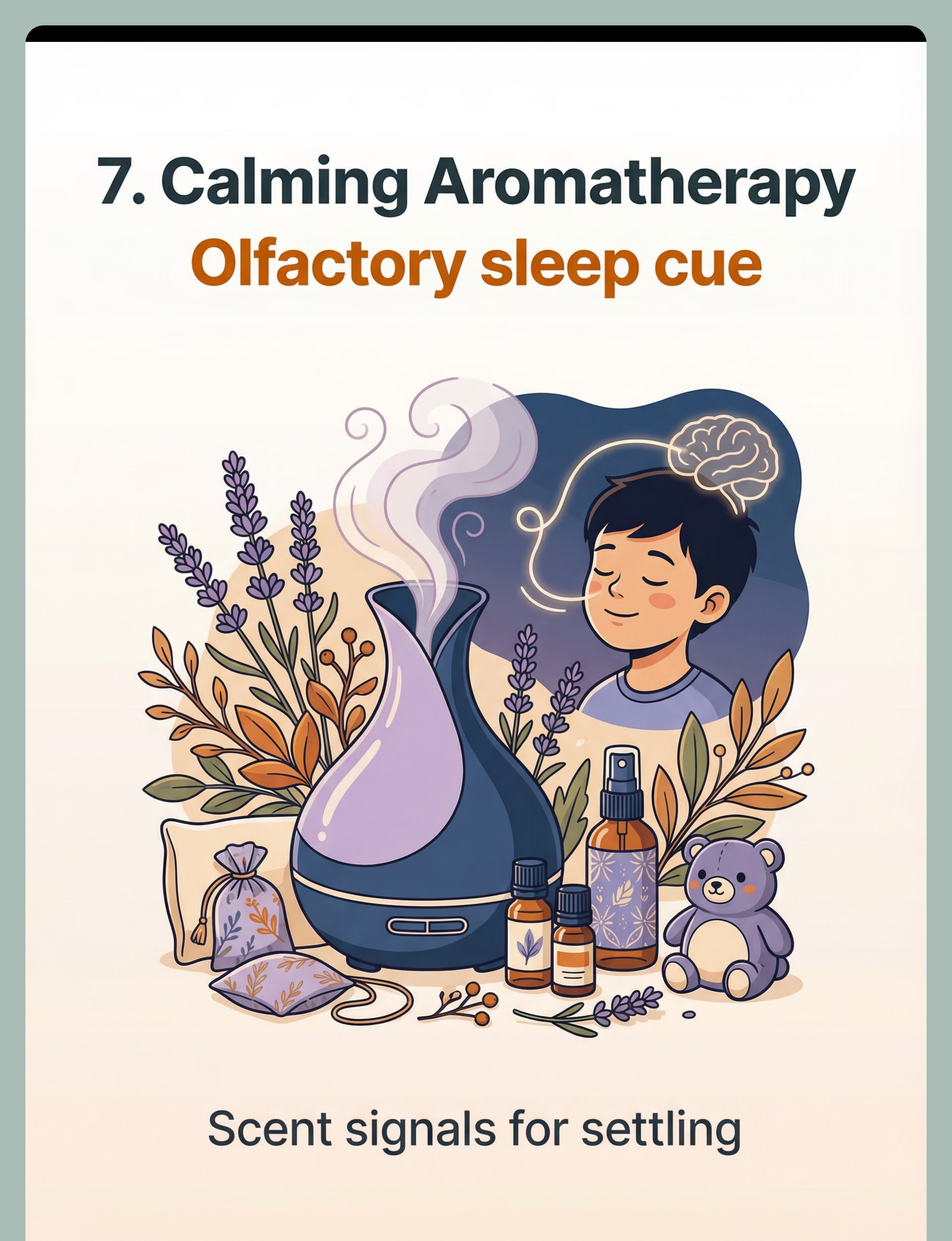
- Calming Aromatherapy
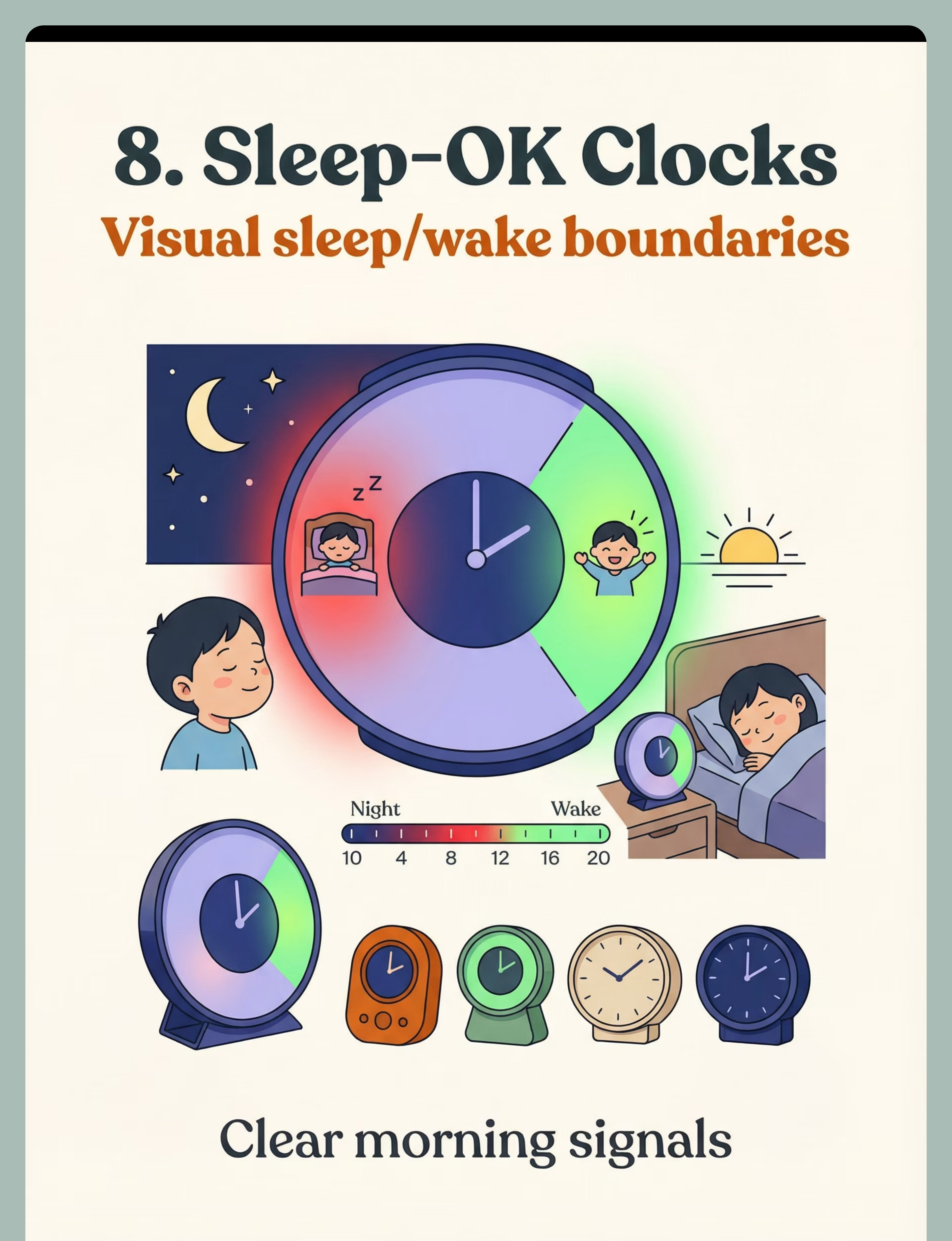
- Sleep-OK Clocks
- Sleep Stories & Calming Audio

Every Expert in the Room Agrees on This
🔵 Pediatric OT — Primary Lead
Designs sensory environment, selects deep pressure inputs, calibrates arousal regulation materials, and assesses weighted blanket specifications
🟢 ABA / BCBA
Establishes bedtime routine through chaining, reinforcement scheduling, and antecedent management — turns the routine into a predictable behavioral system
🟣 SLP
Addresses anxiety communication, teaches child to signal discomfort, builds coping language for the pre-sleep window
🟡 SpEd
Integrates sleep readiness into the daily schedule, coordinates school-impact awareness across morning and daytime functioning
⚕️ NeuroDev Pediatrics
Rules out medical causes (apnea, GI), advises on melatonin considerations, provides medical oversight for the full protocol
"The brain doesn't organize itself by therapy type. Sleep is regulated by neurology, sensory processing, behavior, communication, and family ecology — simultaneously. That's why this protocol requires every discipline at the table." — Pinnacle Blooms Consortium® Clinical Board
Under GPT-OS®, the FusionModule™ coordinates all 5 disciplines into a single converged sleep intervention pathway. No siloed care. No conflicting advice. One system. One outcome.
📞Need to speak to a specialist? FREE · 24x7 · 18+ Languages
9100 181 181 | pinnacleblooms.org
9100 181 181 | pinnacleblooms.org
Precision Targets — What These 9 Materials Actually Do
Each of the 9 materials serves a specific neurological purpose. Together, they target sleep initiation at every level of the arousal regulation system.
Observable Behavior Progress
Target | Before Protocol | After 4–8 Weeks | |
Sleep latency | 60–180 minutes | 15–30 minutes | |
Bedtime resistance | Daily meltdowns | Cooperative routine | |
Parental presence | Required until asleep | Able to release | |
Wake time | Variable/early | Consistent |

Your Complete Sleep Environment Toolkit
9 Clinician-Validated Materials
Home-Executable
India-Sourced

🛏️ Weighted Blankets & Deep Pressure Supports
Why: Activates parasympathetic nervous system via deep touch pressure — signals safety to the body.
Weight: ~10% of body weight + 1 lb | Price: ₹2,000–5,000
Search Amazon.in — Weighted Blanket for Kids
💡Pinnacle Recommends: 3 kg blanket for children 20–25 kg body weight
Weight: ~10% of body weight + 1 lb | Price: ₹2,000–5,000
Search Amazon.in — Weighted Blanket for Kids
💡Pinnacle Recommends: 3 kg blanket for children 20–25 kg body weight

📋 Visual Bedtime Routine Charts
Why: Eliminates uncertainty — every step from bath to bed is visible, predictable, non-negotiable.
Options: Magnetic boards, laminated picture sequences, routine apps | Price: ₹200–600
Search Amazon.in — Visual Schedule Board for Kids
Options: Magnetic boards, laminated picture sequences, routine apps | Price: ₹200–600
Search Amazon.in — Visual Schedule Board for Kids

🔊 White Noise Machines
Why: Creates consistent auditory field — masks triggering sounds, habituates the listening brain.
Volume: 50–60 dB at bedside | Price: ₹800–2,500
Search Amazon.in — White Noise Machine Baby Sleep
Volume: 50–60 dB at bedside | Price: ₹800–2,500
Search Amazon.in — White Noise Machine Baby Sleep

🪟 Blackout Curtains & Light Control
Why: Darkness triggers melatonin production — even small light leaks suppress sleep onset.
⭐⭐⭐⭐⭐HIGHEST PRIORITY — start here | Price: ₹1,000–3,000
Search Amazon.in — Blackout Curtains for Bedroom
⭐⭐⭐⭐⭐HIGHEST PRIORITY — start here | Price: ₹1,000–3,000
Search Amazon.in — Blackout Curtains for Bedroom

🧸 Comfort Objects & Transitional Items
Why: Bridges parental presence → independent sleep; object carries the "feeling of safety."
Price: ₹300–1,000 | Canon SKU: ₹425 — Comfort/Transition Object
Price: ₹300–1,000 | Canon SKU: ₹425 — Comfort/Transition Object

🔴 Red/Amber Nightlights
Why: Red wavelength (700nm+) does NOT suppress melatonin — provides security without disrupting sleep chemistry.
Avoid: Blue/white LEDs | Price: ₹300–800
Search Amazon.in — Red LED Night Light for Kids
Avoid: Blue/white LEDs | Price: ₹300–800
Search Amazon.in — Red LED Night Light for Kids

🌿 Calming Aromatherapy
Why: Olfactory conditioning — scent paired with calm bedtime becomes a conditioned parasympathetic cue.
Best Scents: Lavender, chamomile, sandalwood (test first) | Price: ₹400–1,200
Search Amazon.in — Essential Oil Diffuser Kids Room
Best Scents: Lavender, chamomile, sandalwood (test first) | Price: ₹400–1,200
Search Amazon.in — Essential Oil Diffuser Kids Room

⏰ Sleep-OK Clocks & Wake Time Indicators
Why: Creates clear visual boundary — RED = night/stay in bed, GREEN = morning/okay to rise.
Reduces: Early morning waking, anxious clock-watching | Price: ₹1,500–3,500
Search Amazon.in — OK to Wake Clock Children
Reduces: Early morning waking, anxious clock-watching | Price: ₹1,500–3,500
Search Amazon.in — OK to Wake Clock Children

🎧 Sleep Stories & Calming Audio
Why: Gives the racing mind a gentle cognitive track to follow — reduces rumination and sensory spiral.
Apps: Calm, Moshi Sleep, Yoto Player | DIY: Parent-recorded voice stories | Price: ₹0–500
Search Amazon.in — Yoto Mini Audio Player Kids
Apps: Calm, Moshi Sleep, Yoto Player | DIY: Parent-recorded voice stories | Price: ₹0–500
Search Amazon.in — Yoto Mini Audio Player Kids
💰Total Investment: ₹6,500–17,000 for full setup | Essential Starter 3: Blackout Curtains + Visual Routine + White Noise = under ₹2,500

Every Family Can Do This — Regardless of Budget
WHO/UNICEF Equity Principle
"Effective intervention should never be gatekept by economic status." — WHO Nurturing Care Framework (2018)
Material | Buy Version | ₹0 DIY Version | Same Principle? | |
Weighted Blanket | ₹2,000–5,000 | Layer 3–4 heavy quilts / rice-filled fabric lap pad | ✅ Deep pressure | |
Visual Routine | ₹200–600 | Draw/photograph 5 bedtime steps, laminate with tape | ✅ Predictability | |
White Noise | ₹800–2,500 | Table fan on medium speed | ✅ Masking sound | |
Blackout Curtains | ₹1,000–3,000 | Heavy dark fabric pinned behind curtains; aluminium foil on window (temporary) | ✅ Light block | |
Comfort Object | ₹300–1,000 | Child selects beloved item — old soft toy, parent-scented cloth | ✅ Security cue | |
Red Nightlight | ₹300–800 | Red cellophane over existing lamp; Himalayan salt lamp | ✅ Warm wavelength | |
Aromatherapy | ₹400–1,200 | Dried lavender sachets under pillow; lavender lotion in routine | ✅ Olfactory cue | |
Sleep-OK Clock | ₹1,500–3,500 | Lamp on timer: OFF = night, ON = morning | ✅ Visual boundary | |
Sleep Audio | ₹0–500 | Parent-recorded story on phone (face down); YouTube audio only | ✅ Mental anchor |
DIY Construction: Weighted Lap Pad
- Take a pillowcase or fabric bag (30cm × 40cm)
- Fill with 1–1.5 kg of dry rice in sewn pockets (prevents shifting)
- Sew or tie securely shut
- Place across child's lap or chest during last 15 min of bedtime routine
Target weight: ~10% of child's body weight. Cost: ₹0–50.
⚠️ When Clinical-Grade Is Non-Negotiable
For children with sensory processing disorder diagnosis, respiratory conditions, or hypotonia — clinical-grade weighted blankets with OT guidance are required. DIY is a bridge, not a replacement for assessed children.

Read This Before Tonight's Bedtime
🔴 RED LINE — Do NOT Proceed If:
- Child is under 2 years — never use weighted blanket
- Child cannot remove the weighted blanket independently
- Child has respiratory conditions, sleep apnea, or hypotonia without OT clearance
- Child shows signs of sleep apnea: snoring, gasping, pauses in breathing — stop immediately, consult pediatrician
- Sudden change in sleep pattern (new onset) — always rule out medical cause first
🟠 AMBER — Proceed With Caution If:
- Child is highly scent-sensitive (test aromatherapy during the day first)
- Child attends to ANY light source (introduce nightlight gradually)
- Child has oral motor/feeding differences (ensure comfort object has no small parts)
- Routine has recently changed (travel, illness, school transition)
🟢 GREEN LIGHT — Required Before Beginning:
- Child is not overtired or already dysregulated
- Materials have been introduced during the day (not at bedtime for the first time)
- Space is set up before bringing child in
- Parent is calm — child co-regulates with parent's nervous system
Stop Protocol: Stop immediately if child attempts to remove weighted item and cannot; signs of increased anxiety after aromatherapy; skin reaction to any material; or distress that escalates despite all supportive measures → abandon session, try tomorrow.
🩺 Sleep difficulties may indicate medical conditions (apnea, GERD, restless legs). If comprehensive environmental intervention shows no improvement after 4–6 weeks, request a sleep specialist referral. Call 9100 181 181 for teleconsultation.

Build the Sleep Environment Before Your Child Enters
The room must be fully set up 30 minutes before bedtime begins. Walking into an already-prepared space is part of the sensory signal — the environment tells the nervous system what's coming.
🌡️ Temperature & Sensory Environment
- Room temperature: 18–22°C (cooler promotes sleep)
- Clothing: Soft, seamless, pressure-neutral
- Remove: Screens, tablets, bright toys, anything demanding attention
Parent Positioning Strategy
Start beside the bed. Move progressively toward the door over 2–4 weeks. Fading parent presence is the graduation from this protocol.
Week 1: Bedside → Week 2: Foot of bed → Week 3: Doorway → Week 4: Checking in then leaving

60-Second Pre-Flight Check — Before Every Single Night
ACT III: THE EXECUTION
Before you begin the bedtime routine, run this readiness check. The best session is one that starts right. A modified session is worth more than a forced session.
Check | What to Look For | |
☐ Fed | Child has had evening meal; not hungry, not overly full | |
☐ No recent meltdown | Last significant dysregulation more than 60 minutes ago | |
☐ Transition warning given | Child received "10 minutes to bedtime" visual/verbal cue | |
☐ Screen-free for 60 min | No tablet, phone, or bright screen in last hour | |
☐ Parent regulated | Your own stress/anxiety is managed — child mirrors you | |
☐ Environment ready | Room set up per Card 12 before child enters | |
☐ No illness signs | Not feverish, no pain signals, no new medical concerns |
✅ 6–7 Checks: GO
Proceed to Step 1. Tonight is a good night. Full protocol.
⚠️ 4–5 Checks: MODIFY
Simplify. Use only the 3 essentials: blackout curtains, weighted blanket, visual schedule. Shorten routine by 50%.
🛑 3 or Fewer: POSTPONE
Calm the child first with a non-sleep-specific regulation activity. Reschedule bedtime 20–30 minutes later tonight.
"The best session is one that starts right. A modified session is worth more than a forced session."

Step 1 — The Invitation
STEP 1 OF 6
Minutes 0–5
"Okay [child's name], it's almost time for the sleeping part of the day. Can you show me what comes first on our chart?"
Body Language Guidance
- Speak in a slower, softer, lower vocal register than normal conversation
- Get down to child's eye level — sit, kneel, or crouch
- Avoid rushing or checking your phone
- If child needs a moment, provide it — silence is okay
Acceptance Cues — What "Yes" Looks Like
- Child moves toward the routine chart
- Child points to or touches the first item
- Child begins removing shoes or changing into pajamas
- Child reduces activity level or vocalizations slow
Resistance Cues — What to Do
- Child runs away or ignores: wait 30 seconds, offer again with fewer words
- Child escalates: move to MODIFY mode
- Child engages with comfort object: that IS engagement — follow their lead
Research Basis: ABA Pairing Procedures — establishing motivating operations before demand placement. OT "Just-Right Challenge" principle.
Step 2 — Working Through the Visual Routine
STEP 2 OF 6
Minutes 5–20
The child moves through the visual bedtime routine chart — one step at a time. Each completed step gets a physical acknowledgment: checkmark, flipping a card, or velcro attachment. The parent narrates each step with calm, consistent language.
"You did [step name]! Look — one more done. Let's see what's next."
Engagement | Tolerance | Avoidance — Modify | |
Completes steps independently | Needs prompting but complies | Protests specific steps | |
Anticipates next step | Accepts materials passively | Runs from room | |
Names what's next | Requires extra transition time | Escalating behavior |
Start white noise machine as child enters room. Hand comfort object during teeth-brushing. Room environment (lights, scent) should already be ambient — not introduced cold.
Reinforcement Cue: Verbal praise after each step completion. "Specific + immediate + enthusiastic." Example: "I love how you put on your pajamas all by yourself!"

Step 3 — The Core Sleep Environment Activation
STEP 3 OF 6
Minutes 20–30
Child is now in bed. This is the convergence moment — all 9 materials are simultaneously active. The nervous system has received:
Proprioceptive Input
Weighted blanket active
Auditory Anchoring
White noise running
Visual Darkness
Blackout curtains closed
Visual Security
Nightlight wavelength safe
Olfactory Conditioning
Lavender diffuser ambient
Tactile Security
Comfort object held
Cognitive Anchor
Sleep story or audio playing
Predictability
Visual routine fully completed
Time Boundary
Sleep clock confirms night = now
"All done. Blanket on. Here's your [comfort object]. Close your eyes — I'm right here."
Common Execution Errors
- ❌ Introducing weighted blanket for the first time at bedtime → ✅ Introduce during daytime play first
- ❌ Loud voice after lights-out → ✅ Whisper only after entering the sleep environment
- ❌ Responding to every call → ✅ Establish "one check" rule after lights-out
- ❌ Inconsistent routine sequence → ✅ Same order every single night
Child Response Spectrum
Ideal: Settles in 5–10 minutes, weight of blanket causes visible relaxation
Acceptable: Child fidgets but stays in bed, talks quietly, eventually settles
Concerning: Child in distress, pain signals, unable to tolerate any material → Stop, consult

Step 4 — Consistency Across Nights: The Repetition Protocol
STEP 4 OF 6
Nightly Repetition
This step is NOT about repetitions within one night — it's about nightly repetition. Sleep conditioning is built through exact same sequence, exact same materials, exact same timing — repeated across nights.
Safe Variations Within Consistency
- Sleep stories can rotate (same device, different stories)
- Pajama choice can be child-led (same material/texture type)
- Routine timing can shift ±15 minutes for schedule variation
- Comfort object can be chosen by child from a small rotation
What Must NEVER Vary
- Sequence order of the visual routine
- Presence of weighted blanket
- Blackout level
- White noise (same device, same sound type)
- Parent's calm, consistent tone
Satiation Indicators — When to Adjust
- Child stops responding to weighted blanket → increase weight slightly or try compression sheet
- Child habituated to white noise → change sound type (white → pink → brown noise)
- Child no longer needs all 9 materials → this is progress, not failure. Gradually fade the most "crutch-like" elements.

Step 5 — The Reinforcement Protocol
STEP 5 OF 6
Next Morning
Critical Timing Principle: Sleep reinforcement is delivered the morning after — not during the night. Night-time reinforcement disrupts the sleep architecture you're building. Morning celebration anchors the neural pathway.
"Last night you did something really brave. You stayed in your bed, under your blanket, and your body found sleep. That is so strong. Let me show you what you earned."
Reinforcement Menu — Choose One That Fits Your Child
⭐ Special Breakfast Choice
Immediate + highly motivating. Child chooses from two preferred breakfast options
📌 Sticker on Sleep Chart
Visual progress collector. 5 consecutive nights = 1 special reward
🎮 5-Min Extra Preferred Activity
Morning bonus time for a beloved activity — connects good sleep to good mornings
📣 Verbal Celebration
Specific + immediate + enthusiastic. "You slept in your bed" is more powerful than "You were good."
Sleep Reinforcement Chart — Canon SKU: ₹425 or DIY with a printed chart. Celebrate the attempt, not just perfection. 3 good nights out of 5 counts.

Step 6 — Preparing Tomorrow's Sleep Window
STEP 6 OF 6
Evening Winddown
Sleep doesn't begin at bedtime. It begins two hours before. The pre-sleep runway is as important as the routine itself.
1
Bedtime − 2 Hours
Screens off. Outdoor play ends. Transition to indoor environment begins
2
Bedtime − 90 Min
Indoor calm activities only — puzzles, drawing, books. Energy level managed
3
Bedtime − 60 Min
Diffuser on. Lighting dimmed. White noise switched on. Sensory environment shifting
4
Bedtime − 30 Min
Visual routine chart reviewed with child. "Let's look at what we're doing tonight."
5
Bedtime − 5 Min
"Almost time — let's get ready." Final transition warning given calmly
6
Bedtime
Step 1 begins. The Invitation. The routine is underway
Children with autism process transitions better with MORE lead time, not less. Transition warning language: "5 more minutes, then bath" → "2 more, then all done with [activity]" → "Bedtime is coming — let's look at our chart"
Material Cool-Down (End of Each Night)
- Visual routine chart: final step checked off together with child
- Weighted blanket stays until child is asleep; do not disturb for removal
- White noise: leave running through the night
- Light: leave on all night (sleep-safe wavelength)
If Child Resists Ending the Day
- Offer sensory input (brief deep pressure, joint compression) to regulate
- Use visual timer (hourglass or countdown clock) to make "ending" concrete
- Never warn more than 3 times — follow through calmly every time

60 Seconds of Data Now Saves Hours of Guessing Later
Three non-negotiable data points to capture every night: sleep latency (time from lights-out to apparent sleep), routine completion %, and resistance level (1–5 scale). Your data drives protocol optimization.
📋 What to Record Each Night
- Date and time child entered bed
- Time child appeared asleep
- Estimated sleep latency (minutes)
- Routine completion: Full / Modified / Partial
- Materials used (check all that applied)
- Resistance level: None / Low / Medium / High
- Breakthrough moment (if any)
- Parent notes
Why This Data Matters
- Week 1 average latency: Your baseline — the starting point
- Week 3 comparison: First signal of improvement
- Week 6 analysis: Evidence of protocol effectiveness or need to modify
- GPT-OS® uses this data to personalize next-stage recommendations
📄Downloadable: D-446 Sleep Progress Tracker — PDF (4-week format, printable, free). BACB data collection standards guide our tracking: frequency, duration, and latency as standard practice.

Most Nights Won't Be Perfect — Here's What to Do
❓ "My child threw off the weighted blanket immediately"
Too heavy, or first introduction. Start with a lighter weighted lap pad (1 kg) on legs only. Introduce during daytime TV time for 3 days before trying at bedtime.
❓ "The white noise made things worse — my child kept trying to identify the sound"
Try brown noise (lower frequency, more "rumble") or ocean sounds. For auditory-seeking children, binaural beats at 40Hz delta frequency have shown promising sleep outcomes.
❓ "My child's anxiety increased after aromatherapy"
Scent sensitivity is real. Remove the diffuser entirely. Try unscented version of the protocol for 2 weeks. Reintroduce scent only during daytime, child-led.
❓ "The visual routine became a negotiation every night"
The routine has too many optional steps. Reduce to exactly 5 non-negotiable steps. Post ONLY those 5. Add child-choice only at Step 4 ("which story/song?").
❓ "My child falls asleep only if I'm sitting next to the bed"
This is Stage 1 success. Now begin gradual parent fade: Week 2 = foot of bed. Week 3 = doorway. Week 4 = checking in 2 minutes after lights-out then leaving.
❓ "Nothing is working after 2 weeks"
Protocol fidelity check: Is the routine identical every night? Is blackout truly complete? Check for medical factors (apnea, GI). Book a teleconsultation: 9100 181 181.
❓ "Child wakes in the night and the whole cycle repeats"
This is sleep maintenance (D-447), not sleep initiation. D-446 addresses onset only. See the linked D-447 protocol for night-waking support.
"Session abandonment is not failure — it is data. Every night you attempt this protocol, you are building the pattern. Imperfect nights are part of the conditioning sequence."
No Two Children Sleep the Same Way — Customize This
This protocol is a framework, not a rigid prescription. Every child's sensory profile, age, and family context shapes how these materials are best applied.
🔵 Sensory SEEKER (Under-Responsive)
- Heavier weighted blanket (up to 15% body weight with OT guidance)
- Add joint compressions as last step of routine (10 firm hugs/squeezes)
- White noise at slightly higher volume
- May need 5 min of "heavy work" (pushing, carrying) before routine
🔴 Sensory AVOIDER (Over-Responsive)
- Start with ONLY blackout curtains + visual routine (no other materials Week 1)
- Introduce one new material every 3 days
- Weighted blanket starts as light fabric draped over feet only
- Aromatherapy: no diffuser; just lavender-scented soft toy at distance
Age-Based Modifications
Age 2–4 | Age 5–8 | Age 9–12 | |
Parent-led entirely | Child begins self-checking routine chart | Child runs own routine independently | |
5-step routine max | 7-step routine | Full 9-step routine | |
Sleep story = parent voice recording | Moshi/Calm app stories | Headphones + audio app independently | |
Weighted item = lap pad on feet only | Full weighted blanket | Compression sheet alternative |
Sibling/Family Context: If sharing a room, white noise helps mask sibling sounds. Separate visual routines for each child. Partition bedtime by 15 minutes between siblings.
Weeks 1–2: Survival Mode — and That's Okay
ACT IV: THE PROGRESS ARC
Foundation Building
Weeks 1–2 progress marker — you are laying the neurological groundwork
✅ What You Will Likely See
- Reduced transition conflict — child stops fighting the START of routine
- Material acceptance — weighted blanket no longer thrown off
- Routine familiarity — child can name what comes next on the chart
❌ What Is NOT Progress Yet (and That's Normal)
- Independent sleep onset (this comes in Weeks 5–8)
- Staying in bed all night
- Shorter overall sleep time
"If your child tolerates the weighted blanket for 3 seconds longer than they did on Night 1 — that is measurable progress. Track it."
The goal of Weeks 1–2 is not perfect sleep. The goal is establishing the materials as familiar and safe. Every night you complete the routine — even partially — is a neuroscientific investment. These weeks are the hardest. The routine is new, the materials are unfamiliar, and nothing feels automatic yet.

Weeks 3–4: The Neural Pathways Are Forming
Consolidation Phase
Weeks 3–4 progress marker — patterns are becoming neurological habits
Consolidation Signs — Watch for These
🔔 Anticipation Emerging
Child begins to anticipate routine steps without prompting — the sequence is becoming automatic
🔔 Independent Initiation
Child initiates going to the sleep-clock or comfort object independently — they are now a partner in the routine
🔔 Decreased Resistance
Bedtime transition resistance decreases — the routine is no longer a surprise, and surprises were the source of most resistance
🔔 Latency Decreasing
Sleep latency begins to measurably decrease — track this on your data form and celebrate every 5-minute improvement
The consistent multi-sensory environment is conditioning the autonomic nervous system. The body is beginning to associate the sensory cluster (scent + weight + sound + darkness) with the parasympathetic state. This is neuroplasticity in action.
"You may notice something unexpected: you're more confident too. The anxiety around bedtime is decreasing for you — because you have a protocol that is working, not just hoping."
Weeks 5–8: Sleep Mastery Is Within Reach
Mastery Phase 🏆
Sleep Initiation Mastery Badge — unlocking
Mastery Criteria — Specific, Observable, Measurable
- ☐ Sleep latency consistently under 30 minutes (down from 60–120 min baseline)
- ☐ Child moves through routine with fewer than 2 prompts
- ☐ Child settles in bed without parent at bedside
- ☐ Behavior on following day reflects improved sleep quality (regulated, focused)
- ☐ Child can name or show at least 3 of their sleep materials when asked
Generalization Indicators (The Real Measure)
- Child demonstrates easier sleep onset during travel
- Child requests comfort object when tired during the day
- Child shows reduced anxiety as bedtime approaches — no pre-bedtime meltdowns
When to Move to the Next Level
→ Mastery of D-446 qualifies for D-447 Sleep Maintenance
→ For children who have mastered both: D-449 Bedtime Anxiety
→ For children who have mastered both: D-449 Bedtime Anxiety
Maintenance check: Try reducing ONE material for one week. If sleep quality maintains — that material may no longer be necessary. This is graduation.
You Did This. Your Child Grew Because of Your Commitment.
🌟 Eight weeks. One night at a time.
"Eight weeks ago, bedtime meant battle. Tonight, it means peace. You built this — one night at a time, one material at a time, one refused and reoffered and accepted step at a time."
What Was Actually Accomplished
✅ You restructured your home's sleep environment using clinical-grade sensory science
✅ You maintained consistency across 40+ nights when it would have been easier to give up
✅ You gave your child's nervous system the scaffolding it needed to find sleep
✅ You translated OT, ABA, SLP, and NeuroDev expertise into daily home action
✅ You changed your child's sleep trajectory — and with it, their daytime functioning
Family Celebration Suggestions
- Create a "Sleep Champion" certificate for your child
- Take a family photo: "The night our bedtimes changed"
- Write one sentence in a journal: what has changed for your family
- Share your story with the Pinnacle parent community (anonymized, optional)
📲 Share Your Milestone
Your story will give another exhausted parent the courage to begin. Share in the Pinnacle Parent Community — anonymized, optional, powerful.

Trust Your Instincts — If Something Feels Wrong, Pause and Ask
🚨 Safety Alert
⚠️ Sleep Apnea Signs
Snoring louder than normal, audible gasping, observed pauses in breathing, child waking appearing frightened. Action: Urgent pediatric referral. This is a medical emergency, not a behavioral issue.
⚠️ No Improvement After 6 Weeks
Consistent implementation with zero measurable progress. Action: Teleconsultation with Pinnacle OT. Protocol may need individualized modification.
⚠️ Sudden New-Onset Change in Sleep
After previously good sleep, sudden regression without known cause. Action: Medical evaluation first. Rule out pain, illness, GI, or neurological change.
⚠️ Significant Daytime Deterioration
Worsening daytime behavior indicating severe sleep deprivation. Action: Immediate consultation. Sleep deprivation in autism can create dangerous escalation cycles.
⚠️ Night Terrors Emerging
Screaming, inconsolable, no memory in morning. Action: See D-450 Night Terrors protocol. Different intervention required.
⚠️ Weighted Blanket Causing Distress After 3 Weeks
Compression causing anxiety rather than comfort. Action: OT assessment — child may need a different proprioceptive input type.
Escalation Pathway
📞9100 181 181 — Free · 24x7 · 18+ Languages | 🗺️ Find your nearest Pinnacle center: pinnacleblooms.org/centers
You Are Not Done — You Are on a Journey
D-446 is one technique in a connected series. Each protocol you master builds the foundation for the next — a progression toward complete, independent sleep regulation.
Branching Based on Child's Response
- If D-446 worked well → Proceed to D-447 (Sleep Maintenance)
- If bedtime anxiety is the primary barrier → Branch to D-449
- If sensory environment is the core issue → Branch to Domain A techniques
- If weighted input was most impactful → Deep-dive D-446-DD-01
Long-Term Developmental Goal
Sleep regulation competency feeds directly into: school readiness, emotional self-regulation, learning consolidation, and social energy for peer interaction.
This is not just about nights — it's about the quality of every day.
Related Techniques — Navigate Your Sleep & Regulation Journey
You've already invested in the materials. Many of them work across multiple protocols — maximizing the value of every purchase you've already made.
Code | Technique | Level | Materials You Already Have | |
🌙 D-447 | Sleep Maintenance Difficulties | Core | Weighted Blanket, White Noise | |
🌅 D-448 | Early Morning Waking | Core | Sleep-OK Clock, Visual Routine | |
😰 D-449 | Bedtime Anxiety | Advanced | Comfort Object, Visual Routine | |
👻 D-450 | Night Terrors | Advanced | Safety setup from D-446 | |
🧠 D-460 | Sensory Sensitivities at Bedtime | Core | All 9 materials apply | |
😴 D-445 | Losing Track of Time (Pre-bedtime) | Intro | Visual Routine, Timer |
✅ D-447 — uses your weighted blanket and white noise machine
✅ D-448 — uses your sleep-OK clock and visual routine
✅ D-449 — uses your comfort object and routine chart
✅ D-448 — uses your sleep-OK clock and visual routine
✅ D-449 — uses your comfort object and routine chart
All techniques above sit within the Sleep & Regulation Domain (D-series) — targeting the autonomic arousal regulation system. View all Sleep & Regulation techniques at techniques.pinnacleblooms.org/regulation
Sleep Is One Piece — Here's the Whole Picture
Why Sleep Is the Foundation Domain
Sleep quality directly impacts every other domain on this wheel. A child who sleeps well:
- Processes sensory input more accurately (Domain A)
- Communicates with more clarity and patience (Domain B)
- Regulates emotions with less effort (Domain C)
- Learns and retains academic content more effectively (Domain I)
- Has greater physical energy for motor development (Domains G, H)
GPT-OS® Integration
AbilityScore® tracks progress across all 12 domains simultaneously — showing how improvements in sleep (D-domain) cascade into measurable gains in communication, behavior, and learning.
📞9100 181 181 — Request your child's AbilityScore® assessment: FREE initial consultation.
Before and After — Real Families, Real Nights
ACT V: THE COMMUNITY
Hyderabad — Boy Aged 5
Before: "Bedtime lasted 3–4 hours every night. He'd scream at the door until midnight. We were surviving on 4 hours of sleep each. I thought I was going to break."
After (7 weeks): Sleep latency down to 22 minutes. Weighted blanket and white noise were the turning points. The visual routine took 12 days to accept, then he started checking it himself. Teacher reported improved attention at school within 3 weeks. Daytime meltdowns dropped from daily to weekly.
"I didn't believe it was possible. Then I stopped believing and just followed the protocol. That's what made the difference." — Mother, Pinnacle Network
Chennai — Girl Aged 7
Before: "She needed me lying next to her until she fell asleep. Some nights it took 2 hours. My marriage was suffering. We were desperate."
After (6 weeks): She now enters her room, checks her chart, gets under her blanket, and listens to her Yoto player. Parent fading took 4 weeks. She sleeps independently. Separation anxiety at school drop-off measurably reduced.
"The routine chart was the key. She knows exactly what's coming. The fear was about not knowing." — Father, Pinnacle Network
Delhi — Boy Aged 9
Before: "He was on screens until 1am. We'd given up. Melatonin wasn't working consistently. We'd tried everything."
After (8 weeks): Blackout curtains + screen cutoff 90 minutes before bed + sleep stories via Calm app. Sleep latency 15 minutes. Waking rested and verbal for the first time in years.
"Sleep initiation improvements in autism rarely come from a single material. It's the convergence of sensory inputs — all 9 working together — that creates the tipping point." — Senior Pediatric OT, Pinnacle Blooms Network®
All vignettes are anonymized. Outcomes vary by child profile. — Pinnacle Clinical Documentation Standards

You Don't Have to Navigate This Alone
📱 Pinnacle Sleep Support WhatsApp Group
Connect with parents currently implementing the D-446 protocol across India. Share data, ask questions at 11pm when you're in the middle of a difficult night.
💬 Pinnacle Parent Community Forum
Searchable archive of sleep-related questions, answered by Pinnacle therapists and experienced parents. Available 24x7.
🤝 Peer Mentoring — Talk to a Parent Who's Done This
Connect with a parent who has completed the D-446 protocol and is willing to mentor. Match by child age and city.
📍 Local Parent Meetups
Pinnacle centers host monthly parent support groups. Find one near you and meet families walking the same path.
"The 2am struggle is not yours alone. There are thousands of parents across India right now, in the same position — awake, worried, trying. You are in the largest community of determined parents in the country."
📞9100 181 181 | Available 24x7 | 18+ languages | FREE National Autism Helpline

Home + Clinic = Maximum Impact
Home protocol delivery is powerful. Professional clinical support makes it exponentially more effective by calibrating the protocol precisely to your child's individual sensory profile.

🔵 Pediatric Occupational Therapist
Conducts a Sensory Profile assessment to identify exactly which of the 9 materials will have the highest impact for YOUR child's specific sensory profile. Calibrates weighted blanket weight. Modifies protocol based on co-occurring sensory differences.

🟢 ABA / BCBA Therapist
Designs the reinforcement schedule, analyzes the data from your tracking form, and adjusts the behavioral component when resistance patterns emerge. Data-driven precision.

⚕️ NeuroDev Pediatrician
Rules out medical causes, evaluates melatonin supplementation candidacy, and provides parent guidance on sleep hygiene from the medical perspective. Teleconsultation available.
📹Teleconsultation — Available Now: Remote consultation with a Pinnacle specialist — no travel required. Available in 18+ languages. Appointments within 48 hours.
📞9100 181 181 — FREE National Autism Helpline | 24x7
📞9100 181 181 — FREE National Autism Helpline | 24x7
Deeper Reading for the Evidence-Curious Parent
📗 PRISMA Systematic Review (2024)
Sensory integration intervention for autism meets evidence-based practice criteria. 16 articles, 2013–2023. Children.Read on PubMed: PMC11506176
📙 Meta-Analysis, World J Clin Cases (2024)
Sensory integration therapy promotes social skills, adaptive behavior, and sleep regulation across 24 studies. PMC10955541
📘 Indian RCT, Padmanabha et al. (2019)
Home-based sensory interventions: significant outcomes in Indian pediatric populations. Indian Journal of Pediatrics. DOI: 10.1007/s12098-018-2747-4
📕 WHO/UNICEF CCD Package (2023)
Care for Child Development: evidence-based caregiver guidance implemented in 54 low- and middle-income countries. PMC9978394
📒 Malow BA et al. — Sleep in ASD, Pediatrics (2012)
Practice pathway for identification, evaluation, and management of insomnia in children with ASD. Foundational clinical reference for this protocol.
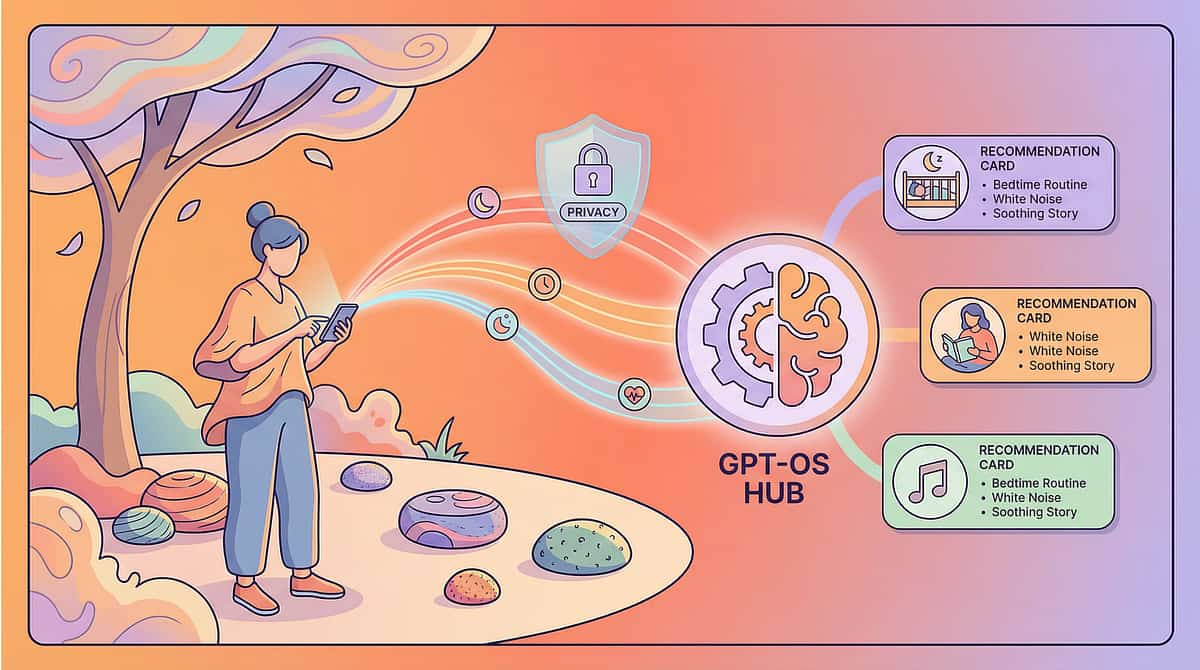
Your Data Makes Every Child's Sleep Better
What GPT-OS® Learns from D-446 Data
- Average sleep latency across the Pinnacle network → updates normative benchmarks
- Which of the 9 materials correlates with fastest latency reduction
- Age × sensory profile × latency reduction curve → improves prognosis accuracy
- Family-level data contributes to population-level insights shared with WHO/UNICEF partners
🔒 Privacy Assurance
All data is anonymized at collection. No personally identifiable information is stored in outcome databases. Data governance follows ISO/IEC 27001 Information Security standards. Children's data is protected under India's DPDP Act 2023.
"Your child's data helps every child like them. When 21 million sessions inform an algorithm, the algorithm becomes the most experienced pediatric sleep practitioner in the world."
See the Materials in Action — 75 Seconds
🎬 Reel ID: D-446
Sleep & Regulation Solutions — Episode 446
⏱️ 75 Seconds
What You'll See in This Reel
- Pediatric OT demonstrating how each material is positioned
- Real bedtime routine sequence (visual routine in action)
- Weighted blanket safety and proper placement
- Before/after room environment comparison
- Parent testimonial (90 seconds)
"This reel was produced by the Pinnacle Blooms Consortium — reviewed by our Pediatric OT, ABA, and NeuroDev teams before publication. What you see is what we prescribe."
Related Reels in the Series
← D-445: 9 Materials That Help When Your Child Loses Track of Time
→ D-447: 9 Materials That Help With Sleep Maintenance
Research Note: NCAEP (2020) classifies video modeling as evidence-based practice for autism. Multi-modal learning improves parent skill acquisition significantly.
Consistency Across Caregivers Multiplies Impact
Every caregiver who implements this protocol consistently adds one more layer of neural conditioning. Consistency across caregivers multiplies impact — each additional consistent implementer reduces overall sleep latency by an estimated 15–25%.
Share This Page
Pre-formatted message: "Found this for [child's name]'s sleep — Pinnacle Blooms D-446 protocol: techniques.pinnacleblooms.org/regulation/sleep-initiation-D-446"
📄 Downloadable Family Resources
- D-446 Family Sleep Guide — 1-Page PDF (Free). Simplified version designed for spouses, grandparents, aunts/uncles, school staff
- School Letter Template — Pre-written letter explaining the protocol, requesting teacher support for morning routine, noting expected improvement timeline
"Explain to Grandparents" Version:"Your grandchild's brain produces melatonin later at night than most children. That's why bedtime is hard. These materials help the brain find sleep. Please use them exactly as shown — even if it seems unusual. Consistency is medicine."
Answers to the Questions You'll Have at Midnight
ACT VI: THE CLOSE
❓ "How long until I see results?"
Most families see measurable improvement in sleep latency within 2–3 weeks of consistent daily implementation. Behavioral improvement (less bedtime resistance) typically emerges in Week 1–2. Full protocol mastery — independent sleep onset — typically occurs in Weeks 5–8.
❓ "What's the most important material to start with?"
Blackout curtains — because light suppression is the neurological prerequisite for melatonin production. No other material will work optimally if light is present. After blackout: add visual routine chart. These two alone often produce the first measurable improvement.
❓ "My child is 3 years old — is the weighted blanket safe?"
For children aged 3+, approximately 10% of body weight is generally safe if the child can remove it independently. For children under 3, use a weighted lap pad on legs only. Always consult your pediatric OT before introducing.
❓ "We've tried a routine before. It never sticks."
Most failed routines had too many steps, were inconsistent in sequence, or were introduced at bedtime without daytime familiarization. This protocol requires: max 7 steps (ideally 5), visual representation of EVERY step, and identical sequence every night for 21 consecutive nights before assessing effectiveness.
❓ "Should I try melatonin supplements?"
Melatonin has strong research support for autism-related sleep initiation. However, it requires physician guidance for dosing and timing (0.5–3 mg, 30–60 min before desired sleep time). Melatonin is most effective when combined with this behavioral/sensory protocol — not as a standalone intervention. Book a NeuroDev teleconsult: 9100 181 181.
❓ "My child wakes in the middle of the night after falling asleep well"
Night waking is a separate clinical challenge called sleep maintenance, addressed in D-447. D-446 addresses the onset problem only. See the D-447 protocol for night-waking support.
❓ "We live in a joint family — is this possible?"
Yes. Use the Family Guide (Card 37) for family education. The key is creating a consistent "sleep environment zone" — even in a joint family, the child's bedroom can become a sensory sanctuary when the protocol is consistently applied by all caregivers present.
❓ "Can I get personalized guidance for my specific child?"
Yes. 📞9100 181 181 — Pinnacle's FREE National Autism Helpline is available 24x7 in 18+ languages. Our therapists can advise on protocol customization based on your child's specific sensory profile and age. Or book at pinnacleblooms.org

You Have Everything You Need. Tonight Is Different.
🟢 Start This Technique Tonight
Download the D-446 Quick-Start Checklist and begin tonight's routine. Everything on this page, distilled to one page.
🔵 Book a Consultation — Free
Speak to a Pinnacle Pediatric OT who specializes in sleep regulation. Personalized to your child's sensory profile.
⚪ Explore the Next Technique
Once sleep initiation improves, address sleep maintenance. The journey continues with D-447.
"21 million sessions across India and 70 countries taught us what works. This is it."
🏛️ Validated by the Pinnacle Blooms Consortium®
Clinically reviewed by: Pediatric OT • ABA/BCBA • SLP • SpEd • NeuroDev Pediatrics • WHO-Aligned • India-Validated
📞 9100 181 181
FREE · 24x7 · 18+ Languages · National Autism Helpline
Preview of 9 materials that help with sleep initiation Therapy Material
Below is a visual preview of 9 materials that help with sleep initiation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
From Fear to Mastery. One Technique at a Time.
— The Pinnacle Blooms Consortium®
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24x7 personalized therapy environment — for every child, in every city, in every economic condition, in every language. Sleep is not a luxury. Rest is not a privilege. For autistic children, peaceful nights require the right environment — and every parent deserves the knowledge to create it.
🏛️ Pinnacle Blooms Network®
Pediatric OT · ABA/BCBA · SLP · SpEd · NeuroDev · Pediatrics
GPT-OS® · WHO/UNICEF-Aligned
📞 24x7 National Helpline
9100 181 181
FREE · 18+ Languages · Autism Support
FREE · 18+ Languages · Autism Support
This content is educational and does not substitute for professional assessment, diagnosis, or individualized therapy planning. Sleep difficulties may indicate medical conditions requiring professional evaluation. Materials and techniques should be implemented under appropriate professional guidance when clinically indicated. Results vary based on individual child profile, consistency of implementation, and co-occurring conditions. Melatonin and other supplements require physician guidance.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Built by Mothers. Engineered as a System. | GPT-OS® Therapeutic Intelligence
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | ISO/IEC 27001 Information Security | ISO 13485 Medical Device QMS